in focus: a case study on diabetes mellitus. ii. physical examination a.general appearance the...
TRANSCRIPT

In Focus:
A CASE STUDY ON DIABETES MELLITUS

II. PHYSICAL EXAMINATIONA. General Appearance
The patient is bedridden, conscious and responsive to external stimuli but appears restless, with a noted depression at the left temporal area of the head, with a noted drooping and redmess of the left eye – with mild white eye discharges noted. With a noted weakness and guarding behavior at the right extremity but with active limb movements on the left arm, left and right leg.

B. Patient’s Contraptions
» Nasogastric tube Fr. 16» Foley catheter Fr. 16 to
urobag

C. Vital Signs
– Respiratory Rate :22 breaths/min– Pulse Rate :82 beats/min– Blood Pressure :120/90mmHg (Left arm)– Temperature : 36.9°C

D. Head, eyes, ears, nose, throat
Vision: - Sclera: R: White in color, some
capillaries are visible
L: Reddish in color, slightly obstructed with mild discharges; chemosis
present
E. Skin•Skin Integrity/Condition:
Generally intact with some dry areas
specifically at the lower extremities;with post operative wound at left temporal region of the head – with sinking flap noted.with healed bedsore noted at sacral area;

F. Cardiovascular
Color: FairTemperature: Warm to touchMoisture: Normal
A.Neck Veins: FlatB.Apical Pulse: Normal, 82 beats/minC.Radial Pulse: Normal, 82 beats/minD.Rhythm: RegularE.Weakness: Right aspect of the body

G. Respiratory• Chest expansion: Symmetrical• Cough: None• Breath Sounds: Clear• Use of accessory Muscles: Absent
H. GastrointestinalA.Tenderness: Rigid
B.Bowel Sounds: HypoactiveC.Diarrhea: Absent
D.Appetite: Within normal limits

I. GenitourinaryPatient is on foley catheter fr. 16 to urobag.Urine is light yellowish in color.
J. ReproductiveNo unusual bleeding or discharges noted from the penile area. No reported cases regarding the patient’s reproductive system.

K. Extremities
•Gross Deformities: Absent•Cyanosis Absent•Edema Absent•Lesion Absent•Capillary refill: Normal (<2 sec)

L. Neurological
A. Glasgow Coma ScaleEyes open: R:3 (opens eye in response to
voice)L: (Left ptosis present)
Verbal response: 2 (Incomprehensible sounds)Motor response: R:1 (No motor response)
L: 5 (Localizes painful stimuli)
Total: 9-10/15


NEUROLOGIC EXAMINATIONMental Status : Conscious, responsive
: Altered sense of attention and concentration: Incomprehensible sounds noted: Can respond to painful stimuli
Motor FunctionsRight side of the body: No
movement noted without maximum support
Left side of the body: Complete movement against maximum resistance

M. Neuromuscular
Weakness: Right side of the body

III. HISTORY OF PRESENT ILLNESS
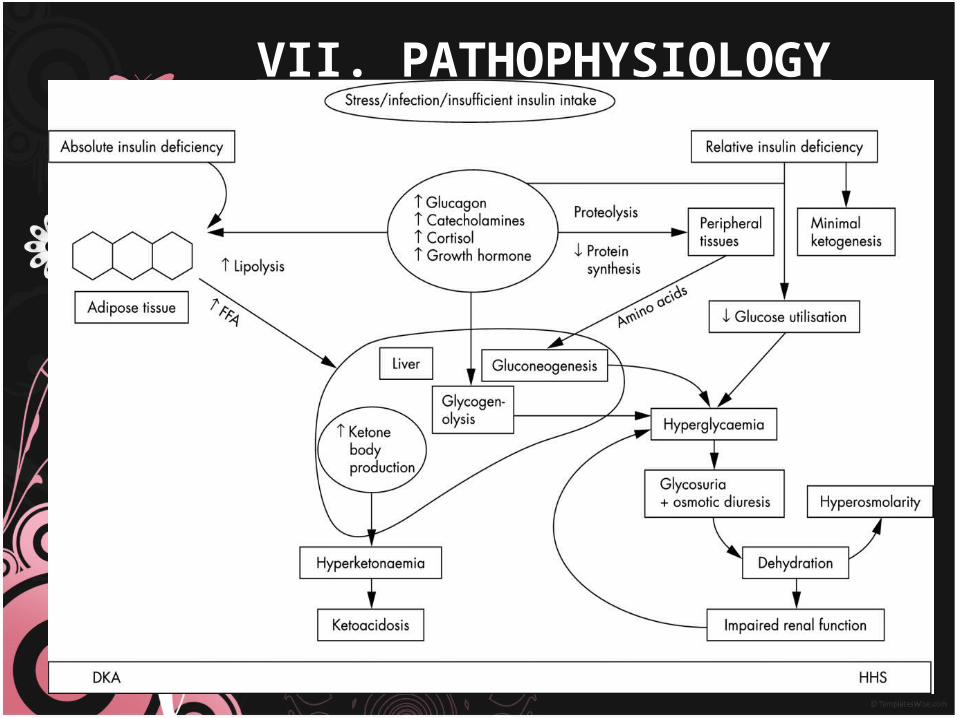
Patient was brought in emergency room in unconscious state. His blood sugar levels were high. He had severe metabolic acidosis and urinary ketones were positive which lead to the diagnosis of DKA. Treatment was started accordingly.

IV. DISCUSSION OF THE DISEASE•What is Diabetes?
•is a group of metabolic diseases in which a person has high blood sugar, either
because the pancreas does not produce enough insulin, or because cells do not
respond to the insulin that is produced.

Types of Diabetes Mellitus
•Type 1 DM results from the body's failure to produce insulin, and presently requires the person to inject
insulin or wear an insulin pump. This form was previously referred to as "insulin-dependent diabetes
mellitus" (IDDM) or "juvenile diabetes".•Type 2 DM results from insulin resistance, a condition
in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. This form
was previously referred to as non insulin-dependent diabetes mellitus (NIDDM) or "adult-onset diabetes".


V. ANATOMY AND PHYSIOLOGY

Type 1 DM : primarily inherited and can be triggered by some certain infections

Type 2 DM: primarily due to lifestyle factors and genetics

Vii. NURSING INTERVENTIONS

VIII. DIAGNOSIS
Diabetes diagnostic criteria
Condition 2 hour glucose Fasting glucose HbA1c
mmol/l(mg/dl) mmol/l(mg/dl) %
Normal <7.8 (<140) <6.1 (<110) <6.0
Impaired fasting glycaemia
<7.8 (<140)≥ 6.1(≥110) &
<7.0(<126)6.0–6.4
Impaired glucose tolerance
≥7.8 (≥140) <7.0 (<126) 6.0–6.4
Diabetes mellitus ≥11.1 (≥200) ≥7.0 (≥126) ≥6.5

IX. COMPLICATIONS

x. NURSING CARE PLAN
a. Risk for unstable blood glucose levels secondary to disease process
B. Imbalanced Nutrition Less than Body Requirments related to insufficiency of insulin, decreased oral input.

X. PRIORITIZATION•Fluid volume deficit secondary to disease process.•Imbalanced nutrition less than body requirements
related to insufficiency of insulin, decreased oral input.•Decreased cardiac output secondary to disease
process.•Impaired oral mucus membrane related to
dehydration.•Risk for constipation related to dehydration.
•Risk for infection secondary to disease process consequences.
•Risk for unstable glucose level related to inadequate endogenous insulin .
•Compromised family coping related to prolong disease.
•Body image disturbance related to disease process.•Ineffective therapeutic regimen management related
to ineffective coping with prolong disease.

XIII. CONCLUSION
Awareness and having the initiative to learn is the key in preventing or managing a chronic illness such as diabetes. The said chronic illness, when detected early, can be manageable and may prevent life threatening consequences of the disease.
Lastly, is discipline. Having a life time chronic illness such as diabetes needs the proper amount of discipline in terms of lifestyle and diet modifications to have a well rounded quality life even with the presence of the said disease.

XIV. BIBLIOGRAPHY1.^ "Diabetes Blue Circle Symbol". International Diabetes Federation. 17 March 2006. http://www.diabetesbluecircle.org.2.^ a b c d Shoback, edited by David G. Gardner, Dolores (2011). Greenspan's basic & clinical endocrinology (9th ed.). New York: McGraw-Hill Medical. pp. Chapter 17. ISBN 0-07-162243-8.3.^ a b Williams textbook of endocrinology (12th ed.). Philadelphia: Elsevier/Saunders. pp. 1371–1435. ISBN 978-1-4377-0324-5.4.^ Lambert, P.; Bingley, P. J. (2002). "What is Type 1 Diabetes?". Medicine 30: 1–5. doi:10.1383/medc.30.1.1.28264. Diabetes Symptoms edit5.^ Rother KI (April 2007). "Diabetes treatment—bridging the divide". The New England Journal of Medicine 356 (15): 1499–501. doi:10.1056/NEJMp078030. PMID 17429082.6.^ a b "Diabetes Mellitus (DM): Diabetes Mellitus and Disorders of Carbohydrate Metabolism: Merck Manual Professional". Merck Publishing. April 2010. http://www.merck.com/mmpe/sec12/ch158/ch158b.html#sec12-ch158-ch158b-1206. Retrieved 2010-07-30.7.^ Dorner M, Pinget M, Brogard JM (May 1977). "Essential labile diabetes" (in German). MMW Munch Med Wochenschr 119 (19): 671–4. PMID 406527