in this issue 2015 annual meeting programs show why no … · 2015 annual meeting programs show why...
TRANSCRIPT

www.osseo.org
2015 Annual Meeting programsshow why no one personcan manage all patient needs
A quarterly publication of the Academy of OsseointegrationVolume 25, Number 4 • 2014
In This Issue
President’s Message: No better venue than San Francisco . . . . . . . . . . . . . . .2
Editor’s E-Mailbag, letters from readers . . . . . . . . . . .3
AO returns to romantic “city by the Bay” . . . . . . . . . . . .5
Over 310 E-posters, 75 researchpresentations to be featured . . . .7
AO Charter Chapter meetings in Italy, Spain successful . . . . . . .8
AO Summit brings world’s topscientists to management of edentulous maxilla . . . . . . . . . . .9
A view of the implant treatment process, as seen by Lars Hansson, CDT . . . . . . . . . .10
Dollars and Sense: Implants and malpractice . . . . . . . . . . . .11
Editor’s Editorial: In AO we trust…(and no one else) . . .14
Academy NewsAcademy of Osseointegration85 W. Algonquin Road, Suite 550Arlington Heights, IL 60005847/439-1919
EditorBruce K. Barr, DDS
Board LiaisonMichael R. Norton, BDS, FDS, RCS(Ed)
Editorial ConsultantsEdward M. Amet, DDS, BS, MSDLouis R. Guenin, BDS, LDS, RCSArchie A. Jones, DDSHarriet K. McGraw, DDSPaige Warren Miller, DDSNavid Rahmani, DDSRobert L. Schneider, DDS, MS
Staff EditorRichard Bragaw, MA
© The Academy of Osseointegration. All rights reserved.
From its Opening Session, “The Power ofCollaboration and the Team Approach,”the 2015 AO Annual Meeting programs
will show whyunderstanding thepatient’s needs andappreciating theabilities and limita-tions of everymember of theteam are the keysto the best implanttreatment.
The theme for the program is “Science,Collaboration and Clinical Excellence for30 Years.” It will be held Thursday, March12, through Saturday, March 14, at theMoscone West Convention Center, SanFrancisco, CA.
“This program is coming at a time whenmany dentists, surgeons as well as restora-tive dentists, could be confused, becausesome in industry are saying you can do itall yourself – drill the hole, do the restora-tion. From a different perspective, if youare a surgeon, why not just scan theimplant at placement and fill out a lab slipto order a final restoration? No problem,they say, it’s all done for you. What do youneed a team for when it’s all so simple now,
right?” says Annual Meeting ProgramChair Dr. Donald S. Clem, Fullerton, CA.
“That one person approach might be fineif you’re working with models, but we areworking with patients who want to livelonger and better. Our patients are becom-ing more complex, not simpler. I remindresidents and students that you become anexpert in your field by commitment, not byconvenience,” Dr. Clem says.
“The fact is no one person can manage allthe patient’s needs. AO more than anyorganization has been dedicated to thatprinciple, and this year’s program, plannedon the occasion ofthe Academy’s 30thanniversary, willshow very clearlywhy the teamapproach is essen-tial and how tomake it work.
“Restorative den-tists need to under-stand the surgical aspects. They need tounderstand what the surgeon’s limitationsare. In the same way, the surgeon needs tounderstand the restorative aspects to create
…continued on page 13The purpose of the Academy of Osseointegration is to advance the science and application of tissue replacement in oral and facial care.
Dr. Donald S. Clem
…continued on page 5
Dr. Daniel Alam

The Academy will return to San Francisco’s Moscone WestConvention Center, the nation’s premier meeting location, forour 30th Annual Meeting, March 12-14, 2015. After making arecent visit to the site, I can assure you that we could not havea better venue for this historic meeting. The center is adjacentto the Intercontinental Hotel and across the street from ourheadquarters hotel, the Marriott Marquis. For those whoattended the 2004 Annual Meeting, it will be familiar, thoughupdated and enhanced.
During the site visit, we selected the Exploratorium as the sitefor Friday’s President’s Reception. I am sure you will bethrilled, as I was, to walk through this outstanding sciencemuseum and participate in its interactive exhibits, while enjoy-ing the level of reception hospitality we have come to expectat AO. It will be a night to remember. We chose theExploratorium, whose stated mission is to change the way theworld learns, after considering a host of other outstandingpossible venues for the reception, including the DeYoungMuseum and AT&T Park.
The theme for the 2015 Annual Meeting is “Science,Collaboration, and Clinical Excellence for 30 Years.” The pro-gram will examine what the Academy has learned through its30-year history and summarize current recommendations toaddress the most challenging conditions in implant dentistry.Annual Meeting Program Chair Dr. Donald S. Clem and hiscommittee have created a scientific program that will take whatthe profession has learned and show how we can apply theseconcepts in new ways to solve clinical conditions and dilemmas.
A highlight of the program will be the Focus on South KoreaSymposium, moderated by AO members Drs. David M. Kimand Brian M. Chang. All three organizations specializing inimplant dentistry in South Korea – the Korean Academy ofOral & Maxillofacial Implantology (KAOMI), the KoreanAcademy of Implant Dentistry (KAID), and the KoreanAcademy of Osseointegration (KAO) – have provided speakersfor the AO Symposium, our second program dedicated to asingle country.
More details about these individual presenters, as well as allsessions and speakers, are available in an article that begins onpage 1 and on our website. Take a few minutes to see foryourself the outstanding program that is in store for you inSan Francisco.
It was my special pleasure as your President to travel to SouthKorea with Dr. Kim to plan the symposium. Our busy itiner-ary included visits with all the symposium speakers, three out-standing dental schools, and the leaders of the three SouthKorean organizations specializing in implant dentistry. Wealso visited three excellent dental product companies –
Shinhung Company, DentiumManufacturing, and Osstem – “and toured two very interesting private practices.
My impression of the schools, the companies, and the prac-tices was that they equal the quality one might find anywhereelse in the world. These are world class schools and compa-nies. We would feel completely comfortable in either of thedental practices. One of the practices we visited was huge –seven stories with glass enclosed offices. I had never seen anything on that scale in the Philadelphia area. The secondpractice was a boutique operation, more like what we areaccustomed to in the U.S.
We also took time to include an interview with South Koreandental magazine reporters. They were interested in knowinghow South Korean implant dentistry compares with the U.S. Itold them that except for the difference in language, we wouldhave thought we were in the U.S.
My wife, Janice, and I enjoyed an eight-day tour of SouthKorea. We found that the best part about the country is itspeople, who were absolutely wonderful to us. The fact thatJanice was using a cane after a recent operation and I havewhite hair may have helped, but we were treated with caringrespect everywhere we went. South Koreans are phenomenallyindustrious. We know the country suffered heavy damage inwar, but we were delighted to find it beautifully reforested.We visited the DMZ, which is only 20 miles from Seoul, andenjoyed a rice-based drink called soju, the world’s largest sell-ing alcoholic beverage.
Since my last President’s message, AO conducted a very suc-cessful Summit, “Current Best Evidence for MinimalIntervention in the Management of the Edentulous Maxilla,”under the leadership of Co-Chair Dr. Clark M. Stanford.(See the report on page 9 of this newsletter). Results will bepublished in supplement to the International Journal of Oral &Maxillofacial Implants (IJOMI). In addition, Dr. Stanford willreport on the Summit results on an Annual Meeting program.
The mobile app for this year’s meeting will be available soon.You will be able to access a complete listing of programevents, organize your meeting itinerary, view speaker eventsand bios, maps and local attractions, customized access tosocial media, and much more – all in the palm of your hand!The mobile app is free and will be available on our website.
I’m sure you won’t want to miss our historic 30th AnnualMeeting in the beautiful city by the bay, San Francisco,California. I look forward to seeing you there!
President’s Message
No better venue than San Franciscofor historic 30th Annual MeetingBy Joseph E. Gian-Grasso, DMD
2
Dr. Joseph Gian-Grasso

3
Editor’s E-Mailbag
Academy News welcomes letters from readerscommenting on articles that have appeared “Please Exit through the gift shop,” Editor’s Editorialby Dr. Bruce Barr, Volume 25, Number 2, 2014
• Dr. Franklin D. Niver, Encino, CA, wrote: “Wonderful edi-torial. Thank you for the mirth and underlying sophisticatedstory. I have been a periodontist for 45 years and involved inimplants for 27+ years, so I have seen and heard a lot of thisbut not so eloquently stated.”
• Dr. Stanley M. Weinstock, New York, NY, said: “What adelight to read your editorial. Skewering with finesse, greatwit and wonderful insight. Loved it.”
Issue Volume 25, Number 3, 2014
• Dr. Kevin T. McNally, Culver City, CA, wrote: “Nice issueof the News. Great to see the committee members con-tributing to the content. Well done!”
AO certification program, page 1, Volume 25, Number 3, 2014
• Dr. Paul A. Schnitman, Wellesley Hills, MA, wrote: “It iswith encouragement, applause, and respect that I writeregarding the ‘new program to offer Certificate in implantdentistry,’ announced in the last issue of Academy News.
“It is admirable that our Board of Directors is instituting acertification process by which our members may demon-strate their core knowledge and competence in the field ofimplant dentistry. This will be especially beneficial for thegeneral dentist practicing implant dentistry who has not hadthe benefit of an advanced education program in one of therecognized specialties providing implant care. In turn, atleast initially, it will also allow the Academy to attract thesedentists to membership.
“Certification could also be seen as especially beneficial forthe ‘single solution specialist providers’ within the AOActive membership. Could this lead to fragmenting themembership? We could end up with two classes of member-ship within each specialty – oral and maxillofacial surgery,periodontics, and prosthodontics.
“While I applaud the Task Force of the AO Board for con-sidering this new program, many questions arise when a cer-tification process like this is being contemplated. Let me lista few of the questions that come to mind.
• After an initial influx of members, could this actually slowthe growth of the Academy because potential membersmay not wish to go through the certification process?
• Could this turn into a new class of membership, and whateffect would that have on existing members?
• Will current Active members who do not wish to partici-pate become disenfranchised and as a result be dispirited?
• Could this put the Academy at risk of fragmentation, ifeveryone does not seek certification?
• Would this process deter potential new members, becausethe hill might appear too steep to climb and stimulatethem to seek membership in other implant organizations?
• Will this be a laddered process, so members early in theircareers will have the opportunity to progress graduallythrough the process?
• Will certification be for both restoration and surgery oronly one aspect of implant dentistry, and how will thataffect current members who wish to practice only oneaspect of implant dentistry?
• How will current Active members achieve certificationshould they wish to pursue it?
• Will this require Academy oversight to assure the publicdoes not confuse this credential with Board Certificationwhen members wish to market their credentials?
• Should the Board of Directors separate itself from thiscredentialing process by creating an independent creden-tialing committee/board within the Academy?
“Deliberation by the communities of interest on these andother issues would be prudent to ensure that the establishmentof an organizational certification process will be successful.”
Official Response to Dr. Paul Schnitman from the AO Board of Directors:
“Thank you so much for your email and for your thought-provoking consideration of the recent announcement of theAO Certificate in Implant Dentistry. I am sure you voice thesame concerns that will be in the minds of many of our mem-bers so allow me this opportunity to address those concerns.
“The Certificate is the result not just of recent efforts onbehalf of the Task Force but the culmination of many years ofdeliberation at Board level, which has often resulted in thepast to the proposal being voted down. This is in no small partdue to recognition by the Board that providing any form ofcertification is not to be entered into lightly. However timeschange and the Board recognizes that the market is shiftingtoward a more dominant provision of implant therapy by gen-eral dentists, who represent approximately 20% of AO’s mem-bership today.
“The AO has always been the natural home for those who areboard certified in the mono-specialties due to the high stan-dards we uphold and encourage as well as the high regard inwhich both our annual meeting and journal, the InternationalJournal of Oral & Maxillofacial Implants are held. The Boardhopes and believes that this status will be unaffected by our
…continued on page 9
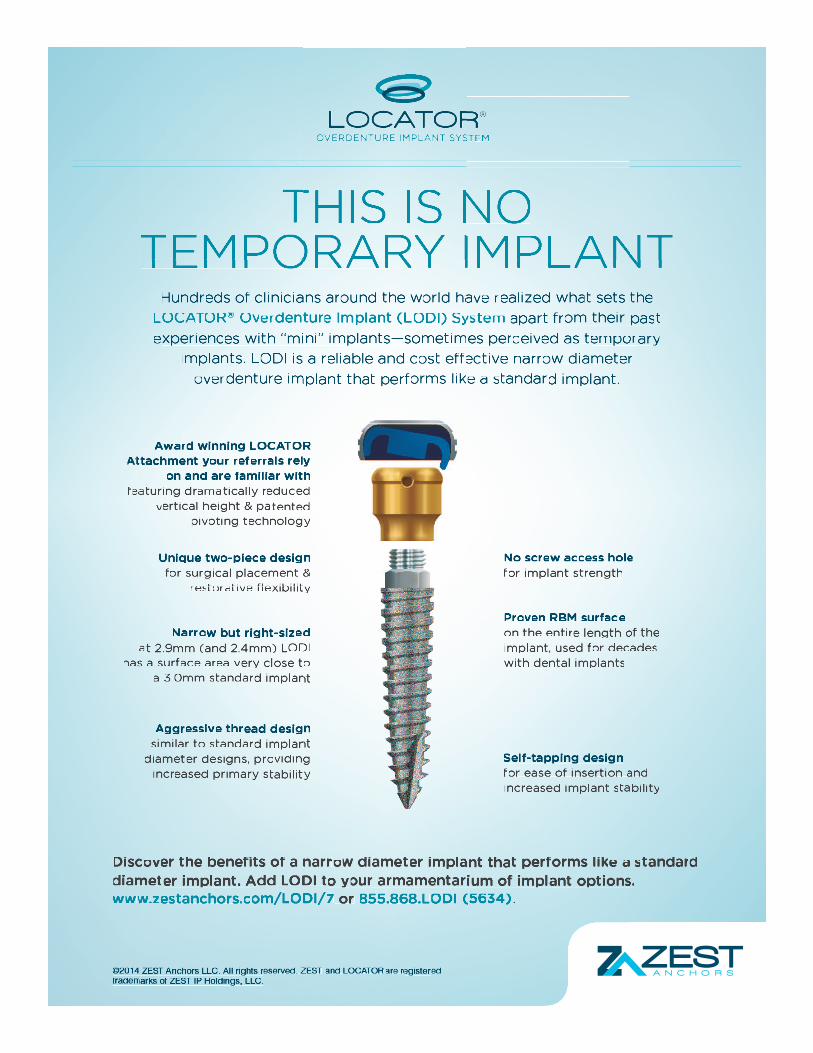
THIS IS NO TEMPORARY IMPLANT
Hundreds of clinicians around the world have realized what sets the
LOCATOR® Overdenture Implant (LODI) System apart from their past
experiences with “mini” implants—sometimes perceived as temporary
implants. LODI is a reliable and cost effective narrow diameter
overdenture implant that performs like a standard implant.
Award winning LOCATOR Attachment your referrals rely
on and are familiar with featuring dramatically reduced
vertical height & patented pivoting technology
Aggressive thread design similar to standard implant
diameter designs, providing increased primary stability
Narrow but right-sized at 2.9mm (and 2.4mm) LODI
has a surface area very close to a 3.0mm standard implant
Unique two-piece design for surgical placement &
restorative flexibility
No screw access hole for implant strength
Proven RBM surface on the entire length of the implant, used for decades with dental implants
Self-tapping design for ease of insertion and increased implant stability
©2014 ZEST Anchors LLC. All rights reserved. ZEST and LOCATOR are registered trademarks of ZEST IP Holdings, LLC.
Discover the benefits of a narrow diameter implant that performs like a standard diameter implant. Add LODI to your armamentarium of implant options. www.zestanchors.com/LODI/7 or 855.868.LODI (5634).

5
The Academy returns to the “city by theBay” after an 11-year hiatus. At thetime, the 2004 Meeting was the highestattended meeting in the Academy’s 19-year history and set a new exhibitorattendance record as well. The MosconeWest Convention Center had only beenopen for a few months and the AO wasthe first dental/medical meeting to takeplace in this new facility. The popularityof its location in the heart of one of theworld’s most iconic cities will continueto draw attendance for AO’s 30thanniversary meeting. A lot has changedsince 2004 for both the Academy andSan Francisco.
Our 2015 attendance is expected toreach near record numbers. As an earlyindicator, AO headquarters has receivedan unprecedented number of clinical
and scientific abstract submissions,which may be attributed to the newly-offered electronic poster sessions thathave created a buzz, adding to theexcitement of this year’s meeting.
Complimentary to all registered guests,the highly anticipated President’sReception will take place Friday eveningat the Exploratorium, founded by physi-cist and educator Frank Oppenheimer. Ithas been described by the New York
Times as the most important sciencemuseum to have opened since the mid-20th century. Wikipedia describes it as“a mad scientist’s penny arcade, a scien-tific funhouse, and an experimental labo-ratory all rolled into one. Theparticipatory nature of its exhibits andits self-identification as a center forinformal learning has led to it beingcited as the prototype for participatorymuseums around the world.” The newExploratorium building is also workingto showcase environmental sustainabilityefforts as part of its goal to become thelargest net-zero museum in the country.Have fun strolling through the galleriestinkering with the interactive exhibitswhile enjoying live entertainment andfood stations displayed in various loca-tions around the facility.
The Academy has contracted with alocal tour company to provide a tourdesk available throughout the meetingand conveniently located in theMoscone West Convention lobby forattendees and guests to convenientlybook specially discounted tours withinthe San Francisco area. After the meet-ing, bring your family and journey northinto Napa and Sonoma Valley, two ofthe most prized wine regions ofNorthern California and enjoy winetasting and exclusive estate tours andfavored wineries.
Stroll through 1,000-year-old ancientredwood trees towering 260 feet at thefamous Muir Woods NationalMonument and on the way back beforecrossing the Golden Gate Bridge, stopat beautiful Sausalito and stay for a fewextra hours and take the Return Ferryback to San Francisco. For those who
want a more scenic visit, book a day-tripto Yosemite National Park, the “CrownJewel” of America’s National Park sys-tem. Also Travel Highway 1 and experi-ence California‘s rugged coastline bytaking the Monterey/Carmel Tour andenjoy the 17-Mile Drive, Monterey’sCannery Row, Silicon Valley, PebbleBeach and more.
Of course, your trip to San Franciscowouldn’t be complete without walkingthrough Fisherman’s Wharf with itsmany fine dining establishments andunique shopping. It’s also the locationwhere you can book a Ferry to Alcatraz,formerly a maximum-security peniten-tiary and now one of San Francisco’smost popular tourist attractions. Also,riding San Francisco’s famous cable carsthroughout the city and shopping atUnion Square is a must.
There is no shortage of things to seeand do in the San Francisco area, butmost importantly, Dr. Donald Clemand his Annual Meeting planning com-mittee have assembled an impressivelineup of speakers with topics thatshould be critically important to all dental practitioners.
AO returns to romantic “city by the Bay” By Kevin P. Smith, MA, MBA, Executive Director
a surgical result that compliments the restoration, not compli-cates it,” explains Dr. Clem.
The keynote speaker at the Opening Session is Daniel Alam,MD, a member of the multidisciplinary team of doctors at theCleveland Clinic, Cleveland, OH, who performed the firstnear-total face transplant in the U.S. “He will speak to thecritical importance of different disciplines coming together to
support patients’ medical, surgical and emotional needs tomake them whole again,” Dr. Clem says. Dr. Alam recentlytransferred to Queens Medical Center, Honolulu, HI, wherehe is Head and Neck Cancer and Reconstructive Surgeon andholds an appointment as Clinical Professor of Surgery at theUniversity of Hawaii John A. Burns School of Medicine.
2015 Annual Meeting programs …continued from page 1
…continued on page 6
Photo by Pius Lee © All rights reserved
Photo by Gayle Laird © Exploratorium, All rights reserved

6
“We can learn much from medicineabout managing the patient as a wholeperson,” Dr. Clem explains. “Patientswant to be cared for. We want to showthat when a patient is missing a part ofthe body, it is a very personal, emotionaljourney. We can take the message of Dr.Alam’s team and dial it down to whatour implant patients need.
“We have put together an internationalgroup of clinicians who will thendemonstrate how the team approach canbe applied to implant dentistry toachieve the finest in surgical andrestorative care.”
Following Dr. Alam on Thursday’sOpening Session program are:
• “The Team Approach for Success:Implant Aesthetics-New Approaches,Limitations and Challenges”: SoniaLeziy, DDS, Vancouver, BC, Canada,and Brahm Miller, DDS, Vancouver,BC, Canada
• “The Quest for the Esthetic ImplantReconstruction”: Adriano Piattelli,DDS, MD, Chieti, Italy, and MarcoDegidi, DDS, MD, Bologna, Italy
• “Managing the Failing Dentition”:Dennis P. Tarnow, DDS, New York,NY, and Stephen Chu, DMD, MSD,CDT, New York, NY.
“We will take a step back, reviewingwhere we’ve been over 30 years, wherewe are now, and where we are going.Our goal is to take what the professionhas learned and show how we can applythese concepts in new ways to solvetoday’s clinical conditions and dilem-mas,” Dr. Clem says.
A program innovation, “Morning withthe Masters,” leads the Friday programbright and early at 7 a.m., with “an out-standing group of experts to give youpearls you can use when you return tothe office Monday morning. Your per-spective on your current approaches willsurely be challenged,” says Dr. Clem.The first morning pearls will come fromDr. Sascha A. Jovanovic, Los Angeles,whose topic will be “The Current Statusof GBR: What are the Options?”
Following Dr. Jovanovic on the“Morning with the Masters” are:
• “Masters on the Teeth and ImplantEsthetics”: Fereidoun Daftary, DDS,Beverly Hills, CA
• “Current Status of Surgical/Restorative Treatment Options for theEdentulous Maxilla”: AO PastPresident Michael S. Block, DMD,Metairie, LA
• “Management of Bone Loss aroundImplants”: Bradley S. McCallister,DDS, PhD, Tualatin, OR
• “Restorative/LaboratoryConsiderations in AchievingPredictable Outcomes”; Markus B.Blatz, DMD, PhD, Philadelphia, PA,and Michael Bergler, CDT, MDT,Philadelphia, PA
• “Morning with the Masters” concludeswith a presentation by Dr. Steven E.Eckert, AO Past President andEditor-in-Chief of the InternationalJournal of Oral & Maxillofacial Surgery(IJOMI), who identifies six IJOMI arti-cles “that may change your thinking.”
“It’s been veryexciting to watchthe journal grow.Our idea in ask-ing Dr. Eckert totake the podiumis to pick out sixarticles thatexemplify howlooking carefullyat the evidence-based approach may change the way weapproach patients in our practices. Wewant to give our members a real sense ofwhat the literature is teaching us,” Dr. Clem adds.
The program retains many very popularfeatures, beginning with the CorporateForums Thursday morning. This year’sparticipants are BioHorizons, Biomet3i, DENTSPLY Implants, GeistlichBiomaterials, Intra-Lock, KeystoneDental, Millennium DentalTechnologies, Inc., J. Morita USA,Nobel Biocare, OraPharma, andZimmer Dental.
The new E-Poster Presentations will beintroduced Thursday afternoon, justbefore the Welcome Reception, held inthe exhibit area. Oral Abstract ResearchPresentations and Clinical InnovationsPresentations will be presented Friday,followed by the President’s Reception,to be held in the Exploratorium (seearticle on page 5).
The Surgical Track and the RestorativeTrack will run concurrently from 8 a.m.to noon on Friday. The TEAMProgram (formerly called Allied StaffProgram) and the LaboratoryTechnician Program will be heldSaturday. The popular Lunch & LearnSessions return Saturday at noon.
Speakers for Friday morning’s parallelSurgical and Restorative Tracks (inorder of their presentations) includeDrs. Mark I. Handelsman, SantaMonica, CA, Jaime L. Lozada, LomaLinda, CA, Otto Zuhr, Freising,Germany, István Urbán, Budapest,Hungary, Hugo De Bruyn, Ghent,Belgium, Frank L. Higginbottom,Dallas, TX, Brody J. Hildebrand,Dallas, TX, Markus B. Blatz, DMD,PhD, Philadelphia, PA, MichaelBergler, CDT, MDT, Philadelphia, PA,Curtis Becker, Denver, CO, GarySolnit, Beverly Hills, CA, Michael R.Norton, London, England, and RobertC. Vogel, Palm Beach Gardens, FL.
Another program highlight will beFriday afternoon’s “Focus on SouthKorea Symposium,” the second of theAcademy’s feature programs dedicated toa single country. “The meeting is on theWest Coast at a time when cliniciansfrom the Pacific Rim are becoming anever more vital part of the AO member-ship. This program is an important partof our outreach to colleagues in thePacific Rim,” Dr. Clem says.
AO members Drs. David M. Kim,Harvard School of Dental Medicine,Boston, MA, and Brian M. Chang,Cleveland Clinic, Cleveland, OH, willmoderate the symposium.
Here is a brief overview of the program:
2015 Annual Meeting programs …continued from page 5
…continued on page 7
Dr. Adriano Piattelli

This year, AO had a record number of over 75 submissions fororal clinical research presentations. Our judges are in the
process of choosing the best submis-sions to be featured at the OralClinical and Oral Scientific sessionsduring the Academy’s 30th AnnualMeeting in San Francisco March 12-14, 2015. In addition to state of the artoral research presentations, theAcademy’s 2015 Annual Meeting willfeature the new E-poster format forover 310 E-posters.
The new format will allow the submitters to display theirposters on the AO website and meeting app in addition to pre-senting their poster during the poster sessions onsite, accord-ing to Dr. Mehrdad Favagehi, Falls Church, VA, Chair of theResearch Submissions Committee.
AO will become one of the first organizations in dentistry tointroduce electronic posters at the meeting and the first dental organization to go 100% paperless. “It’s a hugechange, and we’re all very excited about our bold and pio-neering transition to E-Posters,” says Dr. Favagehi. “It will
solve problems for us and deliver significant benefits for sub-mitters”. Submitters will have until March 1, 2015 to makeany changes to their E-poster.
“Our policy has been to never say ‘no’ to a poster. Membersof the Research Submission Committee will now be able toaccess the abstracts online for review and judging. With E-posters, submitters won’t have to print and carry theirposters to the meeting,” he says.
“As in the past, Annual Meeting attendees will be able to seethe final posters and meet with the submitters to discuss theirwork, as the E-Posters will be displayed on 52 inch monitors.After the meeting, attendees and those unable to attend theAnnual Meeting will be able to access posters online, insteadof only in the Program Guide. Also, the quality of posters willbe much better. They will be in digital format, making forbetter quality graphics.” he adds.
“We plan to have a moderator for every E-poster station. EachE-poster will be presented at a pre-set time, so the meetingattendees can interact and review the posters with the submit-ters ” Dr. Favagehi says.
7
Over 310 E-posters, 75 oral clinical researchpresentations to be featured at 2015 Annual Meeting
Dr. Mehrdad Favagehi
• “Managementof an InjuredInferiorAlveolar Nerveduring DentalImplantPlacement,”Jong-Ho Lee,DDS, Seoul,South Korea
• “Tissue Engineering and RegenerativeMedicine for Dental Implants: Presentand Future,” Bu-Kyu Lee, DDS,PhD, Seoul, South Korea
• “Chairside Preparation of Tooth-Osteoplant (TOP) Graft for BoneRegeneration: The Development of anIndividual Tooth Bank,” Eun-SukKim, DDS, PhD, Seoul, South Korea
• “Peri-implant Bone Loss,” SungtaeKim, DDS, PhD, Seoul, South Korea
• “Management of Implant FailureAssociated with Bisphosphonate-relat-ed Osteonecrosis of the Jaw,” Sun-Jong Kim, DDS, MSD, PhD, Seoul,South Korea
• “Food Impaction and Retention afterDental Implant Restoration,” Yang-Jin Yi, DDS, MSD, PhD, Seoul,South Korea
• “Anytime Loading: The Long TermSuccess Points,” Young-Ku Heo,DDS, MSD, PhD, Seoul, South Korea
For the Closing Symposium on Saturday,Dr. Clem and his committee haveplanned an interactive session headed,“Putting it All Together: Two MissingAdjacent Teeth in the Esthetic Zone,Options for Treatment.” Missing adjacentteeth in the esthetic zone is a fairly com-mon situation, and one of the more diffi-cult clinical challenges to treat in anesthetic manner, according to Dr. Clem.
“Some patients come to us thinking thatevery tooth can be replaced with animplant. Implants are not just replace-ments for teeth. They should be carefullyplanned, with health, function and esthet-ics in mind. It’s important that theseaspects be communicated to the patientin a manner which brings the patient intothe treatment decision. When a patient
understands thelimitations oftreatment – therisks that treat-ment may pre-sent – the resultsof treatment willbe much betterappreciated,” hesays.
The Closing Symposium will be fullyinteractive, giving attendees the oppor-tunity to vote on keypads to give theiropinions on various treatment optionsfor presented cases. Moderators will beMaurizio Tonetti, DMD, PhD,Genova, Italy, and Paul S. Rosen,DMD, MS, Yardley, PA. Participantsinclude Oded Bahat, BDS, MSD,Beverly Hills, CA, Bobby L. Butler,DDS, Seattle, WA, Fereidoun Daftary,DDS, Beverly Hills, CA, AO PastPresident Kenneth F. Hinds, DDS,Laguna Niguel, CA, Robert A. Levine,DDS, Philadelphia, Pa, and Craig M.Misch, DDS, MDS, Sarasota, FL.
2015 Annual Meeting programs …continued from page 6
Dr. Young-Ku HeoDr. Bu-Kyu Lee
…continued on page 9

I am delighted to report that the Charter Chapter meetings inMilan, Italy, in September and Madrid, Spain in Novemberwere both highly successful, with 100 attendees in Italy and115 in Spain, including many delegates who joined or plan tojoin AO. Our lead speaker in Milan was AO Past PresidentDr. Peter K. Moy, LosAngeles, CA, while AOBoard Member Dr.Lyndon F. Cooper, ChapelHill, NC, was the keynotespeaker in Madrid.
The Italian meeting wasorganized by AO MemberDr. Ruggero Rodriquez yBaena, Pavia, Italy. Theprogram title was “StemCells: the Future of BoneRegeneration?” In additionto a presentation on AOand all its benefits, Dr. Moy presented on “The Use of StemCell Constructs and Growth Factors for Hard and SoftTissue Augmentation.”
Organizer for the Spanish meeting was Dr. Fernando Rojas-Vizcaya, who planned an outstanding program and obtainedsubstantial corporate support to offset the costs.
Next on the agenda for AO’s Global Program DevelopmentCommittee, Charter Chapter program, is the first Japanesemeeting. Preparations are now in full flow with Dr. TakashiSumi, Ichinomiya-City, Aichi, Japan, who is organizing theCharter Chapter to take place in Tokyo on July 24 – 26, 2015.A venue contract has been signed, and we will now be lookingat working on the program, with an impressive selection oftop Japanese speakers. AO board member Dr. Tara Aghaloo,Los Angeles, CA. has agreed to join me to represent the boardand to give a keynote lecture.
In addition to the above, Dr. Tolga Fikret Tozum, Ankara,Turkey, continues to express an interest in running a CharterChapter meeting in Turkey, and we have re-commenced a dia-log to see how we might best execute this in late 2015 or early2016. Any other members reading this article who reside in acountry outside of the U.S. and would like to help organize aCharter Chapter in their own country may contact the AOoffice by phone or email or me by email at [email protected].
The 2014 FDI meeting in New Delhi was a huge success withthe AO symposium once again being filled to capacity witharound 400 delegates listening to presentations by Drs. Zvi
Artzi, Tel Aviv, Israel, Mete I. Fanuscu, Istanbul, Turkey, andSaphal M. Shetty, Karnataka, India. At the end of the meet-ing, Dr. D. Gopal who was in attendance also made anannouncement about the forthcoming Outreach Symposiumin Pune, India in 2015.
The AO Indian Outreach Symposium, “Innovation & Practicein Modern Implant Therapy,” is set for January 22-24.Speakers will include Drs. Rojas-Vizcaya, Georgios E.Romanos, Stony Brook, NY, and Hugo De Bruyn, Ghent,Belgium, as well as Dr. Jocelyne Feine, who has been invitedindependently of AO.
AO President Dr. Joseph E. Gian-Grasso, Philadelphia, PA,will be joining us in India to promote the global educationalaspirations as well as the many benefits of the Academy of Osseointegration.
In order not to rest on our laurels and in our quest to makeAO a truly global brand, your Board of Directors recentlyapproved a second Outreach Symposium after extensive corre-spondence with Dr. Blackie Swart, Cape Town, South Africa.Dr Swart who also represents the South African Association ofOsseointegration (SAAO), approached AO last year abouttheir desire to have AO sponsor a whole session at their 2016annual meeting. The SAAO is the only implant organizationin South Africa and shares the same mission and ethos as theAO. As such, it was felt that there was considerable potentialto disseminate the values and benefits of the Academy in thehope of attracting a number of new members to AO fromwithin South Africa, while spreading the reputation of the AObrand to this part of the world.
Finally, I am pleased to report that our collaboration with theInternational Association for Dental Research (IADR), whichincludes a significant annual grant from AO, continues tounderpin our support for high quality research in a global arena.
8
Keynoter Dr. Lyndon Cooper (center, left) and meeting organizer Dr. Fernando Rojas-Vizcaya (center, right) with speakers at AO'sCharter Chapter meeting in Madrid, Spain.
AO news from around the globe
AO Charter Chapter meetings in Italy, Spain successful;now on to Japan, Turkey, India, South AfricaBy Dr. Michael R. Norton, Chair, Committee on Global Program Development

9
The 2014 AO Summit on Current Best Evidence forManaging the Edentulous Maxilla was held in Chicago fromAugust 6-9, 2014. This Summit brought together a panel of world class academic and clinical scientists along with leading private practice clinicians in the area of surgical andprosthetic rehabilitation. Representatives came from manycountries worldwide.
At this very busy Summit, the five task groups reported on thesystematic reviews prepared for the Summit and the draftClinical Practice Guidelines or CPG (3-5/group) and follow-ing lengthy and often vigorous debate, each CPG was votedon, using the SORT Criteria for evidence, and scored on the
strength of the evidence and how the strength of the evidencesupported (or not) the respective CPG. The entire audiencethen voted on the level of training and experience needed bythe team to apply the evidence and obtain results similar tothat in the literature.
The Summit was a lively event with much debate and collegialinteractions! The Summit organizing committee wants tothank all of the participants and especially the sponsors, suchas the OF Foundation, for their generous support of thisSummit! The various systematic reviews and the CPG will bepublished shortly in the International Journal of Oral andMaxillofacial Implants (IJOMI).
AO Summit brings world’s top scientiststo management of edentulous maxillaBy Clark M. Stanford, DDS, PhD, Summit Co-Chair
Dr. Clem has often had the opportunityto ask his referring dentists to join himat AO. Also, the Annual Meeting expe-rience has significantly broadened theresources he turns to when doing litera-ture reviews or preparing presentations.
His 30 years of attending AO AnnualMeetings has been a very valuable per-sonal and professional experience,according to Dr. Clem. “My conversa-tions and learning experiences at AOhave emphasized the advantage of sitting
down with colleagues from all disciplinesand seeing things from a broader per-spective than strictly within my periodon-tal field. I have enjoyed the opportunityto expand my network of colleagues andprofessional friends,” he says.
2015 Annual Meeting programs …continued from page 7
decision to launch the certificate. However the Board must ofcourse continue to be responsive to the ever changing face ofimplant dentistry as well as the flux within its membership.We believe that it is imperative that we encourage more gen-eral dentists to join forces with their specialist colleagues in anendeavour that applauds education, skill, competence, highquality and ethics in the field. We should not sit idly by whileothers offer what are possibly less rigorous courses or certifi-cates that do not necessarily encourage genuine education andthe acquisition of integrated core competencies.
“The Task Force had the unenviable job of creating a certifi-cate that would not require formal education or credentialingto be provided by AO. This is based upon the recognition thatsuch education and credentialing would fall outside the scopeof CODA and the Board do not believe that AO has theauthority to do this. To this end the certificate will clearlystate that this is not a qualification or a conferring of specialiststatus/Board certification and the certificate will only be validfor one year and subject to renewal on renewal of AO mem-bership. At the same time, however, we felt it was possible tocreate a vehicle by which we could assess and evaluate educa-tion and training that has been completed outside of AO andgive it the recognition it deserves. We see no reason why thisshould be exclusive or deny others the chance to attain thesame recognition. To this end we do not believe it will slowgrowth of the Academy but rather stimulate it. We also do notbelieve that it will create a new class of membership, in much
the same way as Fellows are still the same membership catego-ry as all other Active members, so will those who are awardedthis certificate. Similarly there are many members who are notFellows but we do not believe they feel disenfranchised, so wesee no reason why this should happen.
“The certificate is purposefully intended to be rigorous whileat the same time being an achievable goal. This is a very diffi-cult balance to strike but to this end the need for a minimumone year institutional based course was seen as central, thwart-ing the short comings of just relying on CERPS which can beobtained through weekend courses, company courses and alike.The newly appointed Accreditation Committee under the chairof Dr. Amerian Sones will shoulder the responsibility of eval-uating these institutional based courses to ensure they meet thestandards expected by AO and this committee will also beresponsible for the evaluation of all future applications bymembers. The Task Force under my Chair has now been dis-banded and the Board will not shoulder any of the day to dayresponsibility for evaluation and award of the certificate.
“We very much hope that you and all the membership will support this new venture within AO and that it will prove tobe fruitful and of value both to our members and to AO as a whole.”
Dr. Michael R. Norton, for the AO Board of Directors
Editor’s E-Mailbag …continued from page 3

10
Lars Hansson, CDT, is a board certified master dental tech-nician from Malmo, Sweden, who as Chair of the AO AlliedProfessional Staff Education subcom-mittee, is dedicated to exposing laboratory technicians and dentists toeach other’s world.
Mr. Hansson followed his brother intothe field. In Europe, it takes four toeight years to become a master techni-cian, and training takes place alongsidethe clinicians, with involvement in lotsof clinical trials. Over the years, he hasstudied and worked with Drs. Per-Ingvar Brånemark, PeteDawson, Charles English, John Kois, Carl Misch, AvishaiSadan, and many more to learn the doctor’s side of implanttreatment. In America, laboratory training is often a differentstory, with very few seeking the less stringent certification spon-sored by the National Association of Dental Laboratories.
After working in Hawaii and Boston, he moved to VirginiaBeach, VA, about 15 years ago to head the Bay View DentalLaboratory implant department. He has immersed himself inthe study of dentistry. He is a Fellow member of theInternational Congress of Oral Implantologists, assistant lectur-er for the Mid-Atlantic Center for Advanced Dental Studies,the Dawson Academy, and Virginia Commonwealth University.
Mr. Hansson has published many articles on implant dentistryand communication between the clinicians and the laboratory.Several implant manufacturers have employed him as a specialconsultant. He is involved with Misch International ImplantInstitute, serves on the editorial advisory board for IDT(Inside Dental Technology), and is a presenter for Dental XP.Somehow, he also has time for his family, competing in worldcup windsurfing tournaments, and playing drums in a rockand roll band.
With over 25 years of experience, he has seen what works andwhat does not. He knows where dental technology is headed.Quite simply, he believes for the best outcome, the lab tech-nician needs to know what the dentist knows and the dentistneeds to know what the dental lab technician knows. In manyrespects, the technician is far ahead of the dentist in regard to what can be accomplished with what materials in theevolving technology.
The Academy of Osseointegration Annual Meeting, with itshigh standard for lectures, is a venue Mr. Hansson, as theChair of the Allied Professional Staff Education subcommit-tee, encourages technicians and dentists to attend and, if pos-sible, present lectures. Even with the special tuition pricingfor this meeting for the Allied Professional Staff program on
Saturday, it has had disappointing attendance. Less than 1%of A0 members are laboratory technicians and, for most meet-ings, due to cost it is the practice owners alone who attend.
By knowing how each member of a team has to work andwhat each needs to create the best product for the patient,many pitfalls and mistakes can be avoided. In saying this, Mr.Hansson believes the dental technician needs to be involved ineach implant case from start to finish. He prefers to dothe initial CBCT planning himself, and then present it to thesurgeon and restorative dentist. The restorative dentist andtechnician can then perform the smile design for the patientand help each other in the process.
New dental technology has brought the technician, surgeonand restorative dentist together. Digital dentistry is well under-stood and utilized by the laboratory technician. Simply out-sourcing design to some anonymous third party in another stateor country, using generic tooth libraries with no awareness ofbiotype or occlusion, is not the same as having the dentist andtechnician plan each step together, with both having a sense ofownership for the case and, ultimately, the patient.
For example, when performing All on Four case hybrid designs,as opposed to milled zirconium frameworks, the lab technicianneeds 18mm from bone to occlusion. The surgeon needs toknow this, so that, if necessary, they can take away enoughbone. If they do not, then the restorative aspect becomes a res-cue case and the prosthesis is weakened. Treatment planningand communication between all parties is essential.
Dentists are now working on patients with failing pros -theses, supported by implants, some of which are no longer inproduction. Retreating and redesigning these cases can becomplicated, but with the new technology and communicationof all parties, treatment can be orchestrated more smoothly.
Education of the clinician and technician is the key. The tech-nician needs to know the many implant systems, how todesign an abutment (according to Mr. Hansson, in reality, amedical device) to maintain healthy gingival architecture, andhe or she must understand biology. The clinician must under-stand what the technician needs to make a strong prosthesisthat will create the smile that has been designed for thepatient. Everyone – surgeon, restorative dentist, and techni-cian – needs to take more ownership in the patient.
Clinical Technique
A view of the implant treatment process, as seen by Lars Hansson, CDT, educatorBy Dr. Paige W. Miller, New Bern, NC, Academy News Editorial Consultant
Lars Hansson, CDT
Update member contact info at osseo.orgDo we have your most current information for the 2015Membership Directory? Members may update their contact information online at www.osseo.org, or emailBarbara Hartmann, [email protected].

11
Dental implants are common procedures in many practicestoday. Unfortunately, with increased use comes the possibil-ity of increased liability concerns. It has been established
that the number one concern withmedical legal dental negligence iscomplications due to extractions, followed by complications due toendodontic procedures, followed bycomplications due to implant proce-dures – primarily un-restorableimplants and nerve damage.
As a prosthodontist in an academicinstitution for over 20 years, I am
occasionally asked to be an “expert” witness in implant relat-ed malpractice issues. The vast majority of the time, I amhappy to defend the dentist, following initial review of thepatient complaint. Generally, the dentist has tried to do theright thing and followed some form of a reasonable treatmentplan. However, there is the occasion when the patient hasbeen blatantly mistreated, in my opinion, and does deservesome sort of recourse, such as a refunded fee or frequentlyjust a referral to a qualified specialist.
I have found, following review and participation as an“expert” witness in several of these cases, one of the firstthings I ask for is the diagnostic work-up information fromthe treating doctor. Unfortunately, it appears that many ofthese patients have not even had a minimal attempt at a diag-nostic evaluation, which include mounted diagnostic casts,diagnostic wax-up, and surgical guides, not to mention ade-quate radiographic evaluation and accurate medical/dentalhistory. With that being said, recently an OMS colleague andI participated in the support of a patient suing a general den-tist from another state for failed implant treatment and nervedamage. Let me give you the “Cliff’s Notes” version, and youcan be the judge.
In 2005, a 65-year old female with hypertension and type IIdiabetes was referred to me by her general dentist for treat-ment of her mandibular failing dentition. An OMS colleagueand I collaborated in her treatment, after the patient signed aconsent for a five implant retained mandibular fixed partialdenture. Treatment included a thorough review of her med-ical history, radiographic analysis, mounted diagnostic castsand wax-up, and fabrication of a surgical guide. She was alsoinformed she should continue with periodontal recall for herremaining maxillary teeth which had previously been restoredwith fixed restorations.
Her mandibular teeth were extracted, and, following a three-four month healing period, the implants were replaced and
restored with a screw retained fixed partial denture. Healingwas uneventful, and the patient was pleased with the restora-tion. Hygiene was satisfactory and no adjustment wasrequired of the prosthesis. The patient and her husbandretired and moved out of state, with her last recall showingexcellent alveolar levels around her mandibular implants.
In 2009 the patient visited a general dentist in her new loca-tion and had two maxillary teeth extracted, and an implantplaced in one of the extraction sites and eventually restoredwith a fixed restoration. Early the next year, the restoration“fell off” and was replaced. Later that week, a maxillary anteri-or tooth was extracted and an implant placed in the site. InJune of that year, six more maxillary teeth were extracted andtwo more implants placed. The patient was informed hertreatment would consist of a maxillary overdenture withLocator abutments for retention. Attempts at denture fabrica-tion were attempted with limited successful results, due totooth placement, retention and general comfort of the patient.The patient also had some anesthesia issues from the dentalprocedures, which had to be addressed by her physician.
In 2011, the patient reported again to the treating dentistwith painful and loose maxillary implants. One maxillaryimplant was re-placed, two maxillary anterior implants wereremoved, and three more placed. Two months later on areturn check-up, she was informed one implant is coming outand an implant in the area of #8 was showing through the tis-sue. The implants were placed in the maxilla, with a two-stage surgical approach for this patient.
Due to her ongoing discomfort in the maxilla and inability toplace her maxillary implant supported overdenture over thepreviously placed implants, she self-referred herself back tome and my OMS colleague, who had treated her mandibleoriginally. My exam showed implants exposed with approxi-mately 50% bone loss and several submerged or partially sub-merged implants in the maxilla. I deemed the exposedimplants non-restorable, due to extreme facial angulation.The primary source of pain for the patient was likely animplant placed in the #8 area, which appears to be adjacent toor in the incisive foramen. These observations were con-firmed by my OMS colleague and several other surgical facul-ty. I suggested all implants be removed, and a maxillarycomplete denture be fabricated, to which the patient consent-ed. The maxillary implants were removed by an OMS resi-dent under the supervision of the OMS colleague, who hadtreated her with me earlier.
The patient ultimately was treated by removing all her maxil-lary implants, healing for six months, then fabrication of a
Dollars and Sense
Implants and malpractice:learning from a case historyBy Dr. Robert L. Schneider, Iowa City, IA, Academy News Editorial Consultant
Dr. Robert Schneider
…continued on page 13

Providing Solutions - One Patient At A Time and Smile Therapy are trademarks of BIOMET 3i LLC. ©2014 BIOMET 3i LLC.
All trademarks herein are the property of BIOMET 3i LLC unless otherwise indicated. This material is intended for clinicians only and is NOT intended for patient distribution. This material is not to be redistributed, duplicated or disclosed without the express written consent of BIOMET 3i. For additional product information, including indications, contraindications, warnings, precautions and potential adverse effects, see the product package insert and the BIOMET 3i Website: www.ifu.biomet3i.com.
Smile Beautifully Smile Confidently Smile Healthy
BIOMET 3i offers a family of synergistic system solutions to help you and your patients achieve beautiful, conf ident and healthy smiles.
Check Out The BIOMET 3i Online Store at www.shopbiomet3i.com! (US Customers Only)
For more information, please contact your local BIOMET 3i Sales Representative today!In the USA: 1-888-800-8045Outside the USA: +1-561-776-6700www.biomet3i.com | www.shopbiomet3i.com
BIOMET and your patients achieve beautiful, con
BIOMET 3i offers a family of synergistic system solutions to help you and your patients achieve beautiful, con
offers a family of synergistic system solutions to help you and your patients achieve beautiful, conf ident and healthy smiles.
offers a family of synergistic system solutions to help you dent and healthy smiles.
offers a family of synergistic system solutions to help you dent and healthy smiles.
Smile Beautifully
Check Out The BIOMET For more information, please contact your local BIOMET 3i epresentative today! Sales R Sales Representative today!
: 1-888-800-8045In the USA: +1-561-776-6700Outside the USA
dently iSmile Conf
Check Out The BIOMET 3i Online Store at wwwFor more information, please contact your local
epresentative today!
: +1-561-776-6700
dently Smile Healthy
.shopbiomet3i.com! Online Store at www Online Store at www.shopbiomet3i.com!
.shopbiomet3i.com! (US Customers Only))US Customers Only
oviding Solutions - One Patient At A TPr
ein arAll trademarks herfor patient distribution. This material is not to be r
oduct information, including indications, contraindications, warprthe BIOMET 3i Website: www W3i
ime and Smile Therapy aroviding Solutions - One Patient At A T
operty of BIOMET e the prein ar 3i LLC unless otherwise indicated. This material is intended for clinicians only and is NOT intended LLC unless otherwise indicated. This material is intended for clinicians only and is NOT intended3iedistributed, duplicated or disclosed without the exprfor patient distribution. This material is not to be r
oduct information, including indications, contraindications, war.ifu.biomet3i.com.ebsite: www
: +1-561-776-6700Outside the USA.biomet3i.com | wwwwww
e trademarks of BIOMET ime and Smile Therapy ar 3i LLC. ©2014 BIOMET
LLC unless otherwise indicated. This material is intended for clinicians only and is NOT intendededistributed, duplicated or disclosed without the expr
ecautions and potential adverse efnings, product information, including indications, contraindications, war
: +1-561-776-6700.shopbiomet3i.com.biomet3i.com | www
ecautions and potential adverse effects, see the pr
LLC. ©2014 BIOMET 3i LLC.
LLC unless otherwise indicated. This material is intended for clinicians only and is NOT intendedess written consent of BIOMET edistributed, duplicated or disclosed without the expr
oduct package insert andfects, see the precautions and potential adverse ef
LLC unless otherwise indicated. This material is intended for clinicians only and is NOT intended3i. For additional
oduct package insert and
AD032

13
maxillary complete denture. She continues to have neuro-genic maxillary pain and is taking several medications, includ-ing Vicodin. She was given the option of gabapentin blockand alcohol nerve blocks, which she has declined to thispoint. The mandibular prosthesis has been non-problematicsince initial placement, and there have been only minimalmaxillary denture adjustments required for the patient’s com-fort, but she does have limited mastication abilities, due toher compromised maxillary alveolar ridge damage. Treatmentwith anterior iliac hip graft and implants with an implant sup-ported overdenture has been recommended.
The patient initiated litigation, and diagnostic casts, wax-upor surgical guides were never produced. The general dentisthad no appreciable continuing education or experience plac-ing and/or restoring implants. The expense and time involvedin these situations is unbelievable. I was deposed twice; the
OMS colleague was deposed and had to testify at the trial,out of state; the OMS resident, now in private practice inanother state, was deposed twice, in addition to the generaldentist’s “expert” witnesses. Anybody ever involved in the liti-gation process will likely attest there are never any winners inthese situations. Let the readers make their own decision, asthis was very complex, with many various factors to be con-sidered.
AO is a leading organization that embraces the team of spe-cialist, generalist, technician and all office auxiliaries to pro-vide the highest level of continuing education and leadingedge information for all of us practitioners involved with den-tal implant treatment. This case helps to show why such anorganization has a very important role to play in assuring thebest possible care for the patient.
Implants and malpractice …continued from page 11
their company representative has taught them, if indeed theyeven have a company representative.
Dentists learn from a medley of resources, but, irrefutably,after basic education, those who truly wish to hone their skillsand sensibility require mentorship and progressive trainingwith exposure to the vanguard. There are a number of orga-nizations attempting to fulfill these needs. Should AO aggres-sively join that movement, so that “In AO We Will Trust”?
Dentistry can be an insular and solitary profession. Becausere-certification is not mandatory, a dentist could theoreticallypractice for 25 years, using primarily only techniques learnedin school. U.S. medicine attempts to uphold a standard of carein the hospital, if only to satisfy certification requirements forMedicare and insurance payments. Even with the encroach-ment of the various specialties on each other's turf, one willnever see a neurosurgeon with a few holes in his or her sched-ule try a kidney transplant right before lunch. It would hardlybe outrageous for a dentist to attempt such a procedure, ifchair time were available, provided he or she had recentlyreturned from a weekend course with a framed certificatedecreeing the status of Most Super Grand Potentate SupremeDilettante. Although many of us do fundamentally practiceimplant dentistry the way we did 25 years ago, passable obso-lescence is growing less and less tenable.
What the public believes or can be sold, may be, but is notnecessarily, different from what is respected in the profession.Some practitioners who trumpet grand-sounding, marketing-oriented implant credentials are no more than veneratedcharlatans, while, alternatively, many dentists who are seriousabout acquiring advanced knowledge become "certified" prac-titioners through humble channels. What does certificationby the various implant associations mean? Is one really betterthan another? Are these organizations simply fabricating levels of certification to attract members or justify their existence, or are they truly pursuing tiered standards for thepublic’s benefit?
It is highly improbable implant dentistry will be a recognizedADA specialty soon. Even if it were, the example of the cur-rent lack of effectiveness of the scientifically based 100 yearold American Academy of Periodontology (AAP) in control-ling the truncated level of periodontal care in the U.S. makesclear an ADA stamp of approval does not guarantee uniformquality treatment. In the meantime, will there be one organi-zation in a position to categorically establish implant standardsin a definitive legal manner, à la the American HeartAssociation? Maybe not, but protocols such as the Albrektssoncriteria of stability, the use of cone beam technology, as well asmany tried-and-true restorative and surgical approaches areaccepted as the norm, and are often used in the prosecutionand defense of implant malpractice cases. As recently as 2010,AO provided standards for implant care and has now designeda certification protocol.
There will always be dentists driven by a will to improvebeyond competence towards self-actualization. Where willthese dentists turn? Will an organization emerge as either themandated or de facto standard of care? Is AO destined tobecome this organization, or is such a notion a self-aggrandiz-ing fantasy? Stay tuned.
“In AO We Trust,” and maybe in some others, as well, to helpus get the bone, tissue, the look, and that bite that make ourcases right.
The Editor’s Editorial is intended to contribute to the dialogue onissues important to implant dentists. The views expressed in the editorial do not necessarily reflect the policy of the Academy ofOsseointegration or its Board of Directors. Readers who would liketo comment or express a point of view on the editorial are invited to write to the editor via email at [email protected]. We will endeavor to publish pertinent comments or views whenspace permits.
Editor’s Editorial …continued from page 14

14
The bone sets the tone but the tissue is the issue, and it’s the finallook and bite that makes the case right. This riff on AO member
Dr. David Garber’s famous dittyemphasizes the multifactorial aspect ofimplant dentistry and underscores whyit is so challenging for one practitionerto provide outstanding implantrestorations, especially for complexcases. The rhyme also highlightsobstacles that impede implant dentistryfrom becoming an ADA sanctioned,standalone specialty with mandatedstandards. Unquestionably, there areindividuals competent in all facets of
implant dentistry, but there are few fully-rounded expertsleveraging both state-of-the-art knowledge and mastery of theprocedure’s surgical, restorative, and laboratory components.
Experts in any given aspect of implant dentistry did not devel-op those skills and judgment from just a specialty degree or byattending a few courses, but rather through years of continu-ing education programs, by treatinghundreds of cases, and by perpetuallystaving off complacency. There’salways more to learn. As Dr. FranckRenouard so succinctly stated at lastyear’s AO meeting: If you want 20 yearsof experience, you have to work 20 years.Organizations like AO provide a forum for continuous edifica-tion. We cannot expect practitioners entering the field to pos-sess expertise or even a sense of all they don’t yet know, but wecan expect them to begin practice at a level within their owncompetence. But who is this presumptuous all-knowing “We,”claiming to be the superior moral voice of implant dentistry?
It is hardly a revelation that implants are now an integralaspect of routine dental care. Eckert’s recent editorial in theAO’s International Journal of Oral and Maxillofacial Implantsreminds us that osseointegration has been part of dentistry for60 years, and, although statistics vary widely, all concur thatincorporation into mainstream dentistry is rapidly ascendant.According to an article by Greenstein in the August ADAJournal, implants are used in 15 to 20 percent of all prostheticcases. In 2010, one to two million implants were placed. Thatnumber is projected to approach a staggering four million by2020. Industry statistics derived from a variety of sources,including a 2012 Morgan Stanley European research report byJunging, as well as a Colson report in Bloomberg, forecast anestimated $3 billion international implant market, one third ofwhich will be localized in the U.S. Further, studies anticipatean international expenditure of $6.4 billion by 2025.
Much of the growth resides in the value market targeted tothe general practitioner with little to no on-site implant com-pany representation. Danaher’s recent $2.2 billion bid to
acquire Nobel and Zimmer’s $13 billion offer to purchaseBiomet evidences the magnitude of an industry that continuesto both expand financially and consolidate, as larger compa-nies strategically stratify products based on price. An I DataResearch Incorporated project reported that in 2012, 19.4% ofgeneral dentists were placing implants, with 6.7% placingmore than 30 annually. The report said 44.5% of implantswere inserted by general dentists, and projected that numberwill climb in 2014 to approximately 50%, and by 2019, 57.5%of all implants will be placed by general dentists, with 76%cement retained.
Some seasoned implant dentists – if implant dentist is, indeed,a distinction – seem actually giddy with apocalyptic assertionsthat inexperienced dentists’ failed cases will yield a windfall oftreatment opportunities. Those who have been involved insuch repair cases, however, usually find a lack of satisfactionand profit for all involved. Dr. Robert Schneider’s article inthis edition of Academy News reinforces this reality. Thereneed not be such a "windfall."
Where will all these dentists developthe skills to deal with the bone, thetissue, the look and bite that willmake their cases right? As the articleby Dr. Archie Jones in the last AOnewsletter made clear, clinicalimplant training of dental students isnot so much uneven as non-existent.
Many dental students never even reflect a periodontal flap orperform a surgical tooth extraction, much less place animplant. Implants’ role as a major component of routine prac-tice, but not routine training, is vexing.
Restorative dentists’ recourse for the implant education deniedthem in dental school has evolved into a multimillion dollarinternational business. The “weekend wonder” courses, oftenunderwritten or hosted by implant companies, are usually ref-erenced with derision. How much consecutive time, however,can even well-established dentists devote to implant training,much less those negotiating school debt, young families, andfledgling practices?
Dentists who attend multiple courses or extended trainingover many months, as well as meetings, often complain of alack of hands-on experience. One can thus understand theappeal of Third World offshore surgical programs, where den-tists may place numerous implants in a week. Unfortunately,the value of the collaborative team approach for optimalpatient outcomes may not be stressed. Some dentists learnabout implant therapy by participating in study clubs orattending programs like AO, and some unfortunately engagein no formal training, read only throwaway journals, do notbelong to any associations, and know nothing beyond what
Editor’s Editorial
In AO we trust... (and no one else)By Bruce Barr, DDS, Newsletter Editor
…continued on page 13
Dr. Bruce Barr
“As Dr. Franck Renouard sosuccinctly stated at last year's
AO meeting: If you want 20 years of experience, youhave to work 20 years.”


Simplicity
NEW
www.dentsplyimplants.com
NEW
System EV is based on the natural dentition utilizing
System EV is based on the natural dentition utilizing
.workflowan intuitive surgical protocol and a simple prosthetic a site-specific, crown-down approach suppor
an intuitive surgical protocol and a simple prosthetic a site-specific, crown-down approach suppor
For more infor
Implant System BioManagement Complex.step remains the unique ASTRA TECH The foundation of this evolutionar
mation visit For more infor
Implant System BioManagement Complex.step remains the unique ASTRA TECH The foundation of this evolutionar
.dentsplyimplants.comwwwwww.dentsplyimplants.com
.dentsplyimplants.com