influenza causative agent –orthomyxovirus –influenza a virus –infulenza b virus ss rna virus 8...
TRANSCRIPT

Influenza
• Causative Agent– Orthomyxovirus – Influenza A virus– Infulenza B virus
• SS RNA virus • 8 linear segments • Enveloped with spikes
– H spike
– N spikes

• Signs and symptoms• Sudden high fever, pharyngitis, congestion, dry cough,
headache and myalgia
– Acute symptoms decline within a week• Cough, fatigue and generalized weakness may persist

• Acquired through respiratory droplets– Attaches via hemagglutinin
spikes• Induces phagocytosis and
replicates inside cell
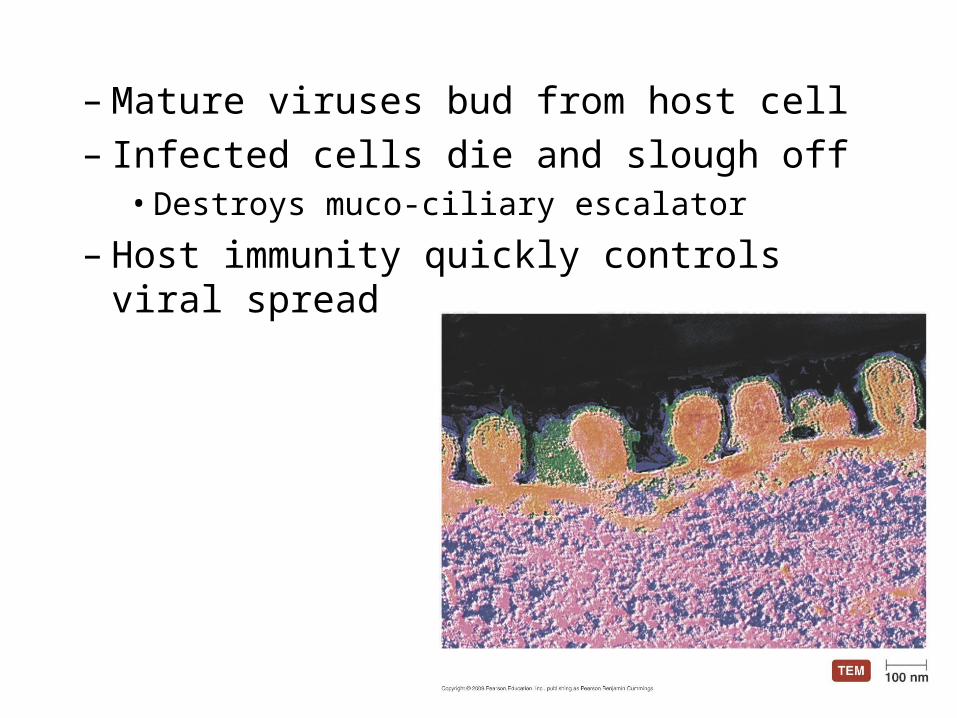
– Mature viruses bud from host cell– Infected cells die and slough off
• Destroys muco-ciliary escalator
– Host immunity quickly controls viral spread

• New strains due to hemagglutinin and neuraminidase mutations– Antigenic drift and antigenic shift
– Avian flu (H5N1)
– Swine flu (H1N1)
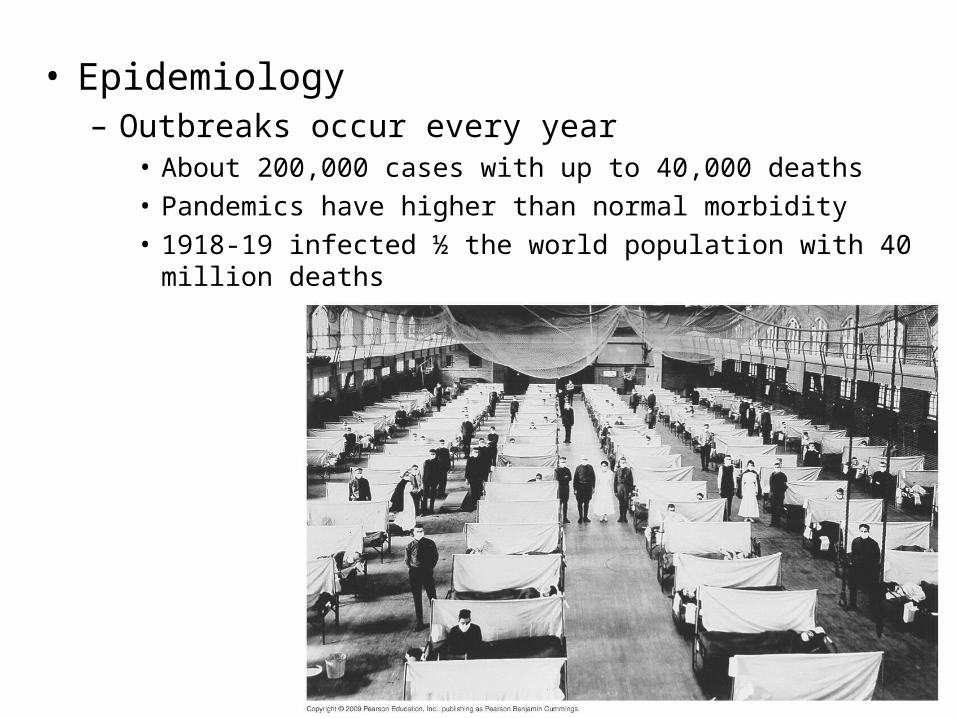
• Epidemiology– Outbreaks occur every year
• About 200,000 cases with up to 40,000 deaths• Pandemics have higher than normal morbidity• 1918-19 infected ½ the world population with 40 million deaths

Critical Swine Flu prevention tip:
Don't DO this!

• Prevention– Vaccine – New vaccine required every year
• Treatment– Antiviral medications– amantidine and rimantidine resistance common– Inhaled zanamivir mist or oral oseltamivir must be
taken with in 48 hours– No aspirin for children!

Respiratory Syncytial Virus Infection
• Most common childhood respiratory disease– Leading respiratory killer of infants
• Pathogen– Respiratory syncytial virus (RSV)– Enveloped, -ssRNA Paramyxovirus

– Signs and symptoms• Fever, runny nose, and coughing • Wheezing and difficulty breathing may occur
– Dusky skin tone
• Leading cause of bronchiolitis in children under one• Some children develop croup• May lead to pneumonia if alveoli become involved

– Epidemiology• Transmission occurs via respiratory droplet• Highly contagious• Syncytia help viruses evade immune system• Great risk of secondary infection
– Prevention • No vaccine • Aseptic technique • Isolation of infected individuals
– Treatment • Typically only supportive care• Ribavirin in extreme cases • No Aspirin!

Pneumocystis Pneumonia (PCP)• Causative Agent
– Pneumocystis jiroveci • Opportunistic fungus• Obligate parasite • Normal respiratory
flora for many

• Signs and Symptoms:– Difficulty breathing; mild anemia; hypoxia; and fever– Non-productive cough in some cases– In rare cases, extra pulmonary lesions develop in
lymph nodes, spleen, liver and bone marrow

• Acquired through respiratory droplets• In healthy individuals usually no symptoms
– Life long immunity is conferred – Some may remain carriers for life
• Fungus multiplies rapidly in immunocompromised patients and extensively colonizes lungs – Causes substantial damage

• Epidemiology– Worldwide distribution– 75% of healthy children exposed by age five
• Based on presence of antibodies– Disease limited to immunocompromised individuals
• One of the diagnostic diseases of AIDS
• Prevention– Virtually impossible due to ubiquitous nature
• Treatment– oral or IV TMP-SMX (combination of trimethoprim and
sulfamethoxazole)