inhalational anaesthetics induced cardioprotection
TRANSCRIPT

INHALATIONAL ANAESTHETICS
INDUCED CARDIOPROTECTION
Cosmin Balan
Assigning a definition
Cardioprotection is the limitation or prevention of irreversible cellular injury in heart muscle as a consequence of ischaemia/hypoxia/anoxia and reperfusion.

Assigning a context
modulation of mitochondrial function to mimicendogenous neuroprotective mechanisms found inhypoxia-tolerant species confers protection againstotherwise lethal hypoxic stresses in hypoxia-intolerantorgans and organisms
lessons gleaned from the investigation of endogenousmechanisms of hypoxia tolerance in hypoxia-tolerantorganisms may provide insight into clinical pathologiesrelated to low oxygen stress
Matthew E. PamenterMitochondria: a multimodal hub of hypoxia toleranceCanadian Journal of Zoology,2014,92(7):569-589


Learning from the bestNatural Born Survivors
Trachemys/Chrysemys TurtlesNear-suspended animation
Carassius Carassius (Crucian Carp)Still active and responsive in the absence of O2
Natural Anoxia Tolerance

Facts about these two…
4-month survival advantage without O2
outstrips a typical mammal by a factor of 1000to 10,000.
CMRO2 turtle corrected for temp is smilar to thatof a typical mammal
Half-lethal times of 45 h under anoxia at 50Cand 22h at 200C for their cousin, Car Auratus At room temperature,in anoxia, Car Car survivesfor a few days During winter, Car Car tolerates anoxia severalmonths

They, too, get preconditioned

They lived to die another dayselection for hypoxia tolerance
O2 30%
SELECTION

Different timescalessimilar outcome
The anoxic frog brain therefore experiencesthe same sequence of degenerative changes as the mammalian brain but on a greatly extended time scale. The anoxic frog brain dies very slowly.
Debra L. Knickerbocker and Peter L. LutzSlow ATP loss and the defense of ion homeostasis in the anoxic frog brainThe Journal of Experimental Biology 204, 3547–3551 (2001)
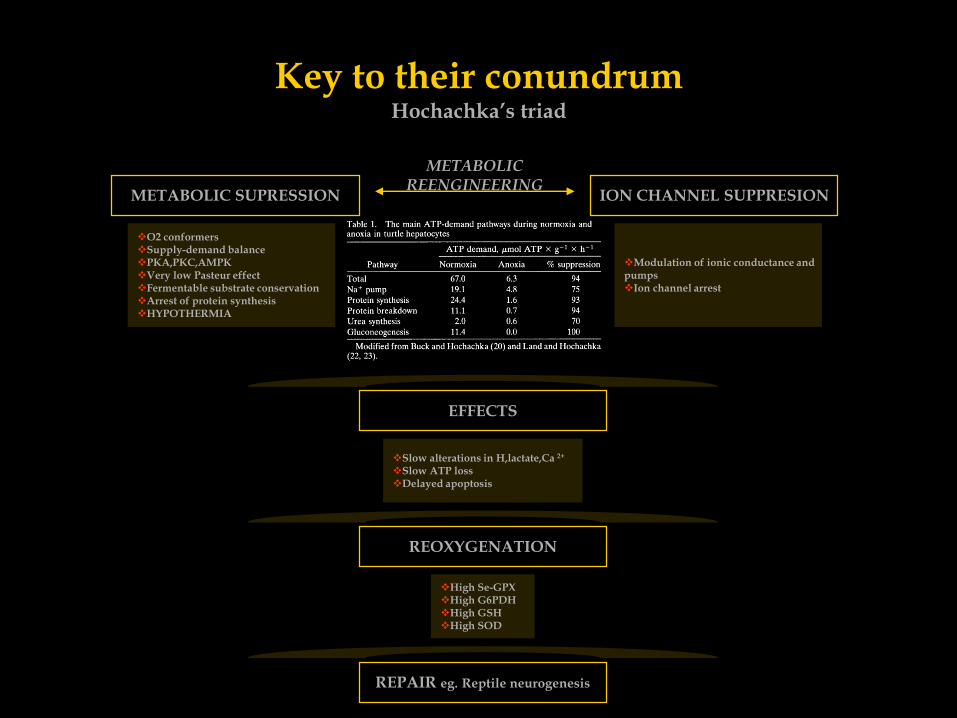
Key to their conundrumHochachka’s triad
EFFECTS
Slow alterations in H,lactate,Ca 2+
Slow ATP lossDelayed apoptosis
REOXYGENATION
High Se-GPXHigh G6PDHHigh GSHHigh SOD
REPAIR eg. Reptile neurogenesis
Modulation of ionic conductance and pumpsIon channel arrest
O2 conformersSupply-demand balancePKA,PKC,AMPKVery low Pasteur effectFermentable substrate conservationArrest of protein synthesisHYPOTHERMIA
METABOLIC SUPRESSION
METABOLICREENGINEERING
ION CHANNEL SUPPRESION

A link to human preconditioninguniversal mechanism
mKATP
AR
mKATP
Ca 2+
ROS Vanden Hoeck et al,1998, J.Biol.Chem.273:18092-98
Pain et al,2000, Circ.Res. 87:460-66
Buck LT. 2004, Comp. Biochem. Physiol. B139:401-14
Buck LT. 2005, Comp.Biochem.Physiol. A142:50-57

Impossible to emulate

Impossible to emulate

Summary model of hypoxia tolerancea second link to human preconditioning
Anaesthetic induced early PC
Anaesthetic induced late PC
Hochachka et al., Comparative Biochemistry and Physiology Part B 130 (2001). 435-459

Chasing for the Holy Grailhypoxia tolerance in humans
ISCHEMIC PRECONDITIONING
Charles E. Murry et al., Circulation 74, No. 5, 1124-1136, 1986Preconditioning with ischemia: a delay of lethal cellinjury in ischemic myocardium

Murry’s paradigmCirculation 1986
We postulated that multiple brief ischemic episodes might
actually protect the myocardium during a subsequent
sustained ischemic insult so that, in effect, we could
exploit ischemia to protect the heart from ischemic injury.
Strongest endogenous protective mechanism of the heartReduces infarct size
Improves recovery of function at reperfusion (reduced myocardial stunning)
Less reperfusion arrhytmias
Inherent to all tissues with high VO2
Has been described in the kidney, liver, small intestine, lung and brain
Universal mechanism
Endothelial and smooth muscle cells –they, too, get preconditioned
Lessens the endothelial cell damage leading to microvascular dysfunction
Two phase phenomenon-early (classic) and late (second window)

Two phases
Charles J. Lowenstein PNAS 1999;96:10953-10954
Acute memory phase Late memory phase

Chasing for the Holy Grailhypoxia tolerance in humans
ISCHEMIC POSTCONDITIONING
Circulation,Laurent Argaud et al., INSERM E 0226, Université Claude Bernard LyonPostconditioning Inhibits Mitochondrial Permeability Transition, 2005
Postconditioning delays Ca2+-induced mPTP opening
Control: ischemia, no intervention
Sham: no ischemia
PreC: 1 episode of 5 minutes of ischemiaand 5 minutes of reperfusion before the prolongedIschemia
PostC: no intervention before the 30 minuteischemia. After 1 minute of reflow after the releaseof the 30-minute occlusion, we performed 4 episodesof 1 minute of ischemia each separated by 1 minuteof reperfusion
NIM811: nonimmunosuppressive derivative ofcyclosporin A

Hormetic effect in ischemia protection in humansliving in the Goldilocks Zone
Ischemia-IPre/PostC
Hyperoxia
Mechanical-stretch
Electrical-rapid pacing
Thermal (hypothermia) /Chemical
Hormonal-remote IPreC
Pharmacological
ToxicityHormesis
DoseDet
erio
rati
on
Imp
rov
emen
tE
FF
EC
T
Gems D. et al.,Cell Metabolism 7, March 2008Stress-response Hormesis and Aging:
“That which does not kill us makes us stronger”UCL
Sublethal exposure to stressors breeds stress resistance

Pharmacological armamentariumengineered ischemia/anoxia protection
IPreC/IPostC mimetism
Inhalational anaesthetics
Opioids
H2S
Antioxidants
ACEI*
Cyclosporine(MPTP inh)
Nitroglycerine(Pre/PostC mim.)
Nicorandil(KATP)
Eniporide(Na+/H+inh)
ANP(PostC mimetic)
PDE5 inh. (Pre/PostC+MPTP)
VDR agonism(Olmesartan, D3)
Brain Sci. 2014, 4, 273-294
HORMETIC EFFECT

PROTECTION TOXICITY
engineered ischemia/anoxia protectionIPreC/IPostC mimetism

Pharmacological armamentariumengineered ischemia/anoxia protection
INHALATIONAL ANAESTHETICSSEVOFLURANE
PERIOPERATIVE CARDIOPROTECTION
► Flow-cond. demand-supply modulation
Negative inotropic & chronotropic action
Positive lusitropic action
Increased coronary bloodflow
V-A coupling modulation (ELV/EA)
Metabolic(oxidative substrate) modulation
•Oguchi , Br J Anaesthesia, 1995 May;74(5):569-75•Pagel, Anesthesiology, 1996 Jul;85(1):112-20•Takahata, Acta Anaesthesiologica Scandinavica,Vol 39, Issue 4, , 449–456, May 1995
PROTECTION DURING CARDIOPLEGIC ARREST
PARADIGM SHIFT
IA induced preconditioning IA induced postconditioning
Kersten, Anesthesiology. 1997 Aug;87(2):361-70 Chen,Acta Pharmacol Sin. 2008 Aug;29(8):931-41
Mito demand-supply
modulation-CM survival pathway

SA
RC
OL
EM
MA
AT1R M2R B2R P2YR
Gi Gi Gi Gi
NCX
NHE
Ca 2+
Na + Na +
H + H +
ENIPORIDE
LCa2+
Ca 2+
A1,A3
Gi
AgII Ach Bk ATP Ad
Redundancy
sK+ATP
HMR-1098
PLC
e/iNOS
OPIOIDS
Gi
δ,κ
PKC
EARLY
PR
ECONDIT
IONING
DESFLURANE
SEVOFLURANE
ISOFLURANE
Gi
α,β
NE
ISCHEMIC BOUTS
ISCHEMIC BOUTS
PRAZOSIN
PROPRANOLOL
PTX
PTXSPT
DPCPX
mK+ATP
ROS
εδη
CALPHOSTIN C
STAUROSPORIN
CHELERYTHRINE
5HD
GLYBURIDE
DIAZOXID
NICORANDIL
NO
NITROGLYCERINE
SNAP
cPTIO L-NAME
L-NIL
PKG
GMPc
8-Br-cGMP
Ca 2+
RYR
IP3R
Ca 2+
SERCA
IP3
PIP2
DAG
Ca 2+
RISK PATHWAY
PI3K/AKT
MEK1/2
ERK1/2
RAS/RAF
P38 & JNK
TN
FR
TNFαJAK
JAKSTAT
TRANSCRIPTION FACTOR
UPREGULATION
AP-1
STAT
NF-kB
TN
FR JAK
JAK
STATJAK
JAKTNFα
TN
FR
MPTP
MnTBAP
MPG
iNOS
AlRed
Bcl-2
HSP27/70
COX-2
MnSOD
LATE
Mito restoration of Δψ
ATP production ↑
Prevention of apoptosis
Decrease of mito Ca 2+
SARCOLEMMA

Cytoprotective Mechanismssevoflurane emulates IPC
KATP
MPTP
KATP
MPTP
SMC-RC
SMC-RC
SMC-RC
KATP
MPTP
- - - - - - - - - - - - - -++++++++++++++
- - - - - - - - - - - - - -++++++++++++++
KATP
LCa2+
LCa2+
LCa2+
KATP
KATP
NCX
NHE
Ca 2+
Na + Na +
H + H +
Ca 2+
NCX
NHE
Ca 2+
Na + Na +
H + H +
Ca 2+
NCX
NHE
Ca 2+
Na + Na +
H + H +
Ca 2+
++++++++++++++- - - - - - - - - - - - - -
ROS
ROS
ROS
ATPase3Na +
2K +
ATPase3Na +
2K +
Matrix volume dependent energy regulation
mKATP leads to depol. of the inner mito. mb.
Non linear dep. of Ca 2+ influx on mito. pot.
Mito. matrix contraction 30%
Intermembrane expansion
sKATP induced hyperpolarization
Dissociation of SMC
Modified ZAUGG, Br. J. Anaesth. (2003) 91 (4):551-565.

Myocyte Protection is Mediated by mKATP
A=control after 60 min of ischemia
5HD=5-hydroydecanoate (mKATPblocker)
HMR-1098=sKATPblocker
A=red myocytes are irreversibly damaged
Trypan blue-positive=red, damaged
ZAUGG,Anesthesiology 7 2002, Vol.97, 4-14

Sevoflurane Potentiates Diazoxide-Mediated Myocyte Protection
ZAUGG,Anesthesiology 7 2002, Vol.97, 4-14
mKATP opener

Sevoflurane only primes mKATPothers open mKATP directly
ZAUGG,Anesthesiology 7 2002, Vol.97, 4-14
Flavoprotein Oxidation-Enhanced Autofluorescence in Myocytes
The redox state of flavoproteins(FAD) reflects mitoKATP activity
The redox state of flavoproteins(FAD) is reflected by their autofluorescence
Microscope, excitation at 480 nm and emission at 530 nm
Calibration of fluorescence:2,4 dinitrophenol uncouples OxF-marker 100%

Sevoflurane’s priming is mediated by PKC
ZAUGG,Anesthesiology 7 2002, Vol.97, 4-14
Flavoprotein Oxidation-Enhanced Autofluorescence in Myocytes
CHE = Chelerythrine (PKC inhibitor)

Takahiro Kamota, J Am Coll Cardiol, 2009;53:1814–22
Lucchinetti, Zaugg, Anesth Analg, 2009;109:1117–26
Mihaela Popescu, Bogdan Pavel, Leon ZagreanRomanian Archives of Microbiology and ImmunologyVol 70 - No. 3 July - september 2011 - Dynamics ofendothelial progenitor cells following SEVOFLURANEpreconditioning
Sevoflurane-beyond the cardiomyocyte
The Recruitement of Bone Marrow Stem Cells into the Heart 1 Day after I/R Injury
J Am Coll Cardiol, 2009;53:1814–22
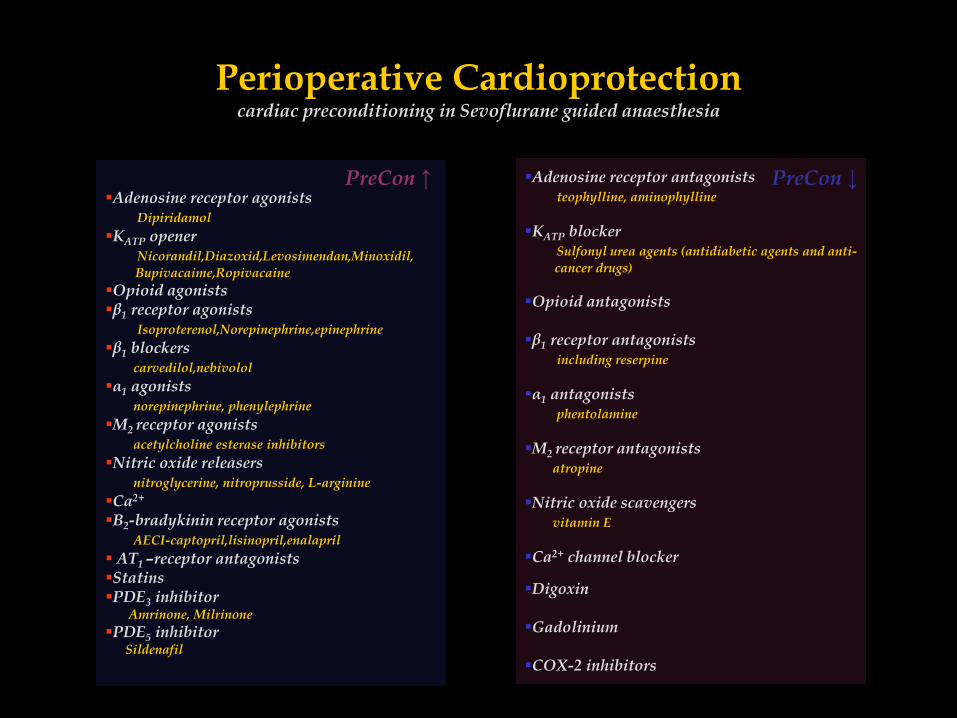
Perioperative Cardioprotectioncardiac preconditioning in Sevoflurane guided anaesthesia
Adenosine receptor agonistsDipiridamol
KATP openerNicorandil,Diazoxid,Levosimendan,Minoxidil,
Bupivacaime,Ropivacaine
Opioid agonistsβ1 receptor agonists
Isoproterenol,Norepinephrine,epinephrine
β1 blockerscarvedilol,nebivolol
α1 agonistsnorepinephrine, phenylephrine
M2 receptor agonistsacetylcholine esterase inhibitors
Nitric oxide releasersnitroglycerine, nitroprusside, L-arginine
Ca2+
B2-bradykinin receptor agonistsAECI-captopril,lisinopril,enalapril
AT1 –receptor antagonistsStatinsPDE3 inhibitor
Amrinone, Milrinone
PDE5 inhibitor Sildenafil
Adenosine receptor antagoniststeophylline, aminophylline
KATP blockerSulfonyl urea agents (antidiabetic agents and anti-
cancer drugs)
Opioid antagonists
β1 receptor antagonistsincluding reserpine
α1 antagonistsphentolamine
M2 receptor antagonistsatropine
Nitric oxide scavengersvitamin E
Ca2+ channel blocker
Digoxin
Gadolinium
COX-2 inhibitors
PreCon ↑ PreCon ↓

Perioperative Cardioprotectiondisease dependent cardioprotection efficacy
Diabetes
Increased age
High plasma cholesterol
Coronary artery disease
Arterial hypertension
Healthy Systems Breed Highly Efficient PC
Factors/Diseases Ischemic PC Sevoflurane PC
↓ ↔ ↑
↓ ↔
↓
↓ ↔
↓↔
↓
?
?
?
?

Translating Experimental Studiesclinical confounders in IA based anaesthesia
Timing and mode of adminstration
Dose
Opioids
α,β agonists/antagonists
ACEI
Statins
PDE inhibitors
Sulfonylurea medication
Cardiac versus non-cardiac surgerypredictability of ischemia
Translating Experimental Studiesdichotomy
Ischemia Predictability
Non Cardiac SurgeryCardiac Surgery

Circulation. 2007;116:1971–1996
Randomized clinical trials in patients undergoing CABG surgery indicate thatvolatile anesthetics decrease troponin release and enhance LV function comparedwith propofol, midazolam, or balanced anesthesia techniques with opioids.These data can likely be generalized to patients with CAD who are undergoing noncardiac surgery.
Recommendations for Use of Volatile Anesthetic AgentsClass IIa
It can be beneficial to use volatile anesthetic agents during noncardiacsurgery for the maintenance of general anesthesia in hemodynamicallytable patients at risk for myocardial ischemia. (Level of Evidence: B)
Landoni G, Fochi O, Bignami E, et al.Cardiac protection by volatile anesthetics in non-cardiac surgery?A meta-analysis of randomized controlled studies on clinicallyrelevant endpoints.
HSR Proc Intensive Care Cardiovasc Anesth. 2009;1:34–43.
Towards the 2014 Recommendations
No randomized study, among those which compared desflurane or sevoflurane tointravenous anesthetics, has addressed major outcomes such as myocardialinfarction or mortality. Large, multicentre, randomized clinical trials includingpatients undergoing high-risk non-cardiac surgery and reporting clinicallyrelevant outcomes such as myocardial infarction and mortality are needed.

Landoni G, Bignami E, Oliviero F, et alHalogenated anaesthetics and cardiac protection in cardiac and
non-cardiac anaesthesia.
Ann Card Anaesth. 2009
Towards the 2014 Recommendations
This review supports the evidence that the choice of an anaesthetic regimen wasshown to have an impact on patients’ outcome following cardiac surgery.
Landoni G, Biondi-Zoccai GG et al.Desflurane and sevoflurane in cardiac surgery: A meta-analysis ofrandomized clinical trials.
J Cardiothorac Vasc Anesth 2007;21:502-11
Large, multicentre, randomised clinical trials including patients high-risk non-cardiac surgery are needed to achieve a definitive demonstration of anaesthetic-induced cardioprotection: this represents a difficult task because of the low mortality rate in modern surgery and because of the number of interfering factors.

Giovanna A.L. Lurati Buse, MD; Philippe Schumacher, MD et alRandomized Comparison of Sevoflurane Versus Propofol toReduce Perioperative Myocardial Ischemia in Patients UndergoingNoncardiac Surgery
Circulation. 2012;126:2696-2704
Towards the 2014 Recommendations
Compared with propofol, sevoflurane did not reduce the incidence of myocardialischemia in high-risk patients undergoing major noncardiac surgery.The sevoflurane and propofol groups did not differ in postoperative NT-proBNPrelease, major adverse cardiac events at 1 year, or delirium.

Use of either a volatile anesthetic agent or total intravenous anesthesia is reasonable forpatients undergoing noncardiac surgery, and the choice is determined by factors other thanthe prevention of myocardial ischemia and MI.
(Level of Evidence: A)
Although the benefit of using volatile anesthetic agents has been demonstrated in cardiacsurgery, a reduction in myocardial ischemia/MI has not been demonstrated in noncardiacsurgery.
Choosing the right thing
Complex non cardiac surgery, coronary artery disease, advanced age, diabetes mellitus, chronic renal disease, hypertension.
either/or
think like a turtle
there is no either/or
there is only SEVOFLURANE
think evidence-basedthink ACC-AHA
