uptake of inhalational anaesthetics
TRANSCRIPT
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 1/25
P T A K E O F I N H A L A T I O N A L P T A K E O F I N H A L A T I O N A LA N E S T H E T I C SN E S T H E T I C S
DR.DEEPAK SOLANKIM.D. [email protected]

8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 2/25
• Pharmacokinetics: Relationship between a drug'sdose tissue concentration and elapsed time.
• Pharmacodynamics: Drug action including toxicresponses.
•• Pharmacokinetics of inhaled anesthetic involves : 1.Absorption (uptake) from alveoli into pulmonary
capillary blood. 2.Distribution in the body 3.Metabolism 4.Elimination (lungs)
•• Aging : in lean body mass, in body fat apparent
VD hepatic function and pulmonary gas exchange
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 3/25
• Principal objective of inhalational anesthesiais to achieve a constant and optimal brainpartial pressure of inhaled anesthetic
PA Pa Pbr
• PA is an indirect measurement of anestheticpartial pressure at brain.
•• There are three steps: 1.Transfer of inhaled anestetic from
machine to alveoli 2.Transfer from alveoli to arterial blood 3.Transfer from arterial blood to brain
•
• These steps are influenced by various factors.
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 4/25
• Factors affecting inspiratoryconcentration (Fi)
-Fresh gas flow rate, -volume of breathing system, -absorption by machine or breathing
circuit.
•
•Factors affecting alveolar
concentration (FA) -Uptake -Ventilation -
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 5/25
UptakeUptake
• Uptake by pulmonary circulation = b/g ×
C(A–V)×Q b/g = blood gas partition coefficient C(A–V)= difference of concentration of
anesthetic between alveolar and venousblood Q = Cardiac output
•
• Anesthetic agents are taken by pulmonarycirculation during induction. Thereforealveolar conc. lag behind inspiratory
concentration
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 6/25
• Greater uptake Slower rate of rise
of FA and alveolar partial pressure of
anesthetic slower the rate of
induction (Concentration of a gas partial
pressure)•
• The alveolar partial pressure determine
the partial pressure of anesthetic inblood and ultimately in brain.
•
• Concentration of anesthetic in brain
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 7/25
• Factors affecting anesthetic uptake A. Solubility in blood B. Alveolar blood flow C. Partial pressure difference between alveolar gas
and venous blood
•• Solubility in blood : Insoluble agents like N2O which
are taken up by blood less avidly has faster rate of induction than soluble agents like halothane.
•• The relative solubility's of anesthetic in air, blood and
tissue expressed as partition coefficient.•• Each coefficient is ratio of concentration of anesthetic
gas in each of two phases at equilibrium (equal
partial pressures) b /g = 0.47 for nitrous oxide.

8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 8/25
Partition coefficients of volatilePartition coefficients of volatile
anesthetics at 37oCanesthetics at 37oC
• Higher b/g induction is prolonged.
• Blood/gas solubility is increased by post prandial lipidemia
and is decreased by anaemia.
AgentAgent Blood/GasBlood/Gas Brain/BloodBrain/Blood Fat/BloodFat/Blood
NN2OO 0.470.47 1.11.1 2.32.3
HalothaneHalothane 2.42.4 2.92.9 6060
IsofluraneIsoflurane 1.41.4 2.62.6 4545
DesfluraneDesflurane 0.420.42 1.31.3 2727
SevofluranSevofluranee 0.650.65 1.71.7 4848

8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 9/25
(b) Alveolar blood flow(b) Alveolar blood flow•
• In absence of pulmonary shunting alveolar blood flow isequal to cardiac output
•• cardiac output anesthetic uptake slower induction
•
• Effect of cardiac output is more pronounced for more bloodsoluble anesthetic
•• Low output states predispose patients to over dosage with
soluble agents like halothane
•• Halothane may create a positive feed back loop.
•• Cerebral blood flow: It is maintained even in shock up to
moribund stage (BP<40 mmHg) and takes a greaterproportion of cardiac output, increasing the effect of inhaled anesthetic.
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 10/25
(c) Partial pressure difference(c) Partial pressure differencebetween alveolar gas andbetween alveolar gas and
venous bloodvenous blood•• This depends on tissue uptake
•• Transfer of anesthetic from blood to
tissue is determined by
(1) Tissue solubility of agent, (2) Tissue blood flow, (3) Partial pressure difference
between arterial blood and tissues
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 11/25
Tissue can be divided into 4 groups based ontheir
solubility's and blood flow.
•• Vessel rich group: (brain, heart, liver, kidney,
endocrine organ) (moderate solubility and smallvolumes), first to take up appreciable amount of
anesthetic and first to fill.•• Muscle group: (skin and muscle) (great capacity):
uptake slower and sustained for hours.
•• Fat group: tremendous solubility of anesthetic leads
to total capacity that would take days to fill.
•
• Vessel poor group: (bones, ligament, teeth, hair,
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 12/25
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 13/25
Concentration effectConcentration effect
• It include concentrating effect
and augmentation of trachealinflow.
•
• Concentrating effect reflectsconcentration of inhaled anestheticin a smaller lung volume due to
uptake of all gases in lung.
•
• At the same time, anesthetic input
via tracheal inflow is increased to
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 14/25
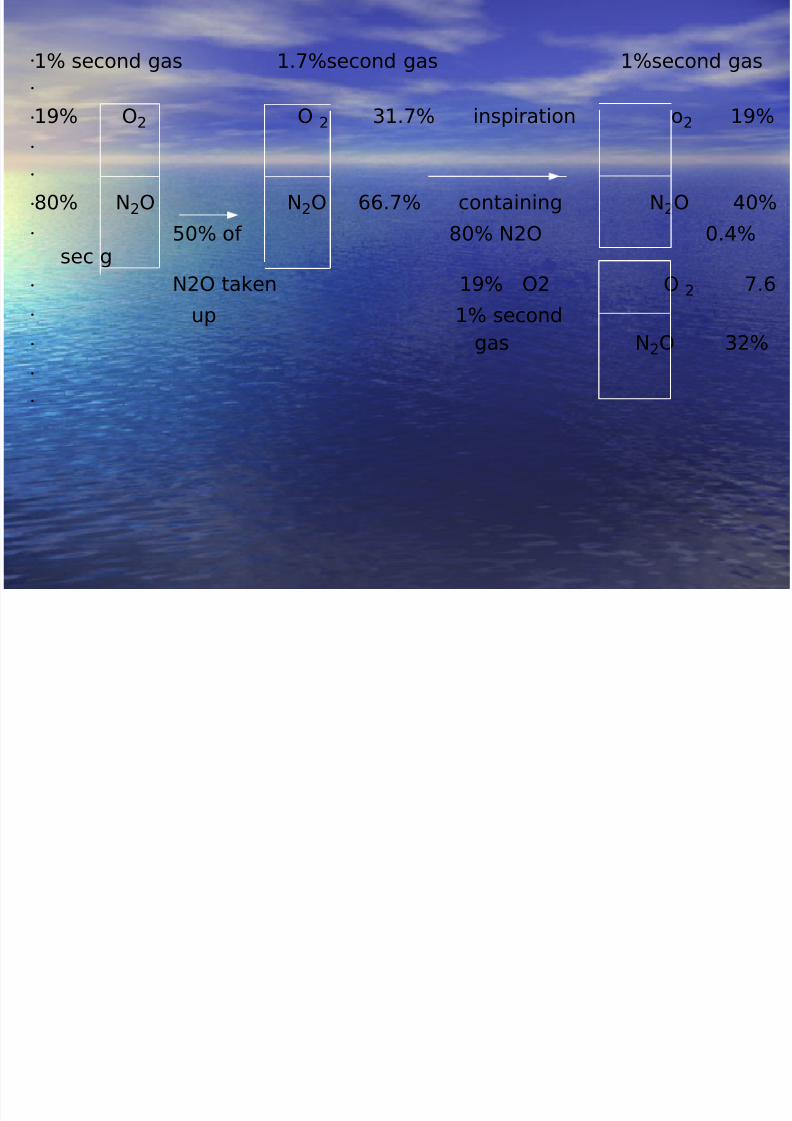
1% second gas 1.7%second gas 1%second gas
19% O2 O 2 31.7% inspiration o2 19%
80% N2O N2O 66.7% containing N2O 40%
50% of 80% N2O 0.4%sec g
N2O taken 19% O2 O 2 7.6
up 1% second
gas N2O 32%
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 15/25
• Concentration effect is more significant for nitrousoxide.
•
• Second gas effect: Reflect the ability of highvolume uptake of one gas (first gas) to acceleratethe rate of increase of alveolar partial pressure of a second concurrently administered 'Companiongas' (Second gas)
• Factors affecting arterial concentration (Fa)
•• Ideally, alveolar and arterial anesthetic partial
pressure are assumed to be equal, but in realityarterial partial pressure are consistently less thanalveolar due to venous admixture, alveolar, deadspace, ventilation perfusion mismatching.
•
• Overall effect is an increase in alveolar partial
F ff iF t ff ti
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 16/25
Factors affectingFactors affectingeliminationelimination
• Recovery depends on lowering the concentration of anesthetic in
brain tissue.
•• Elimination comprises : -Biotransformation: accounts for minimal decrease in rate of
decline of alveolar partial pressure. More important for solubleanesthetic, cytochrome P-450 group of isozymes (CYP2E1)
appears to important for some volatile anesthetic. Ex. it accountsfor halothane faster elimination than isoflurance.
- Transcutaneous loss.
-Exhalation: The most important route for elimination is alveolarfactors that speed induction also favour recovery that iselimination of rebreathing, high fresh gas flow, low anaestheticcircuit volume, high cerebral blood flow, increased ventilation.
• Elimination of N2O is so rapid that it leads to diffusion hypoxia.
– – The rate of recovery is usually faster than induction
••
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 17/25
Clinical applicationClinical application
•
• Factors that increased the speed of induction
- Greater inhaled concentration - Hyperventilation
- Poor circulation to nonvital organs- shock,dehydration old age, wasting of body tissue
- High gas flow system
• Factors that decrease speed of induction
- Respiratory obstruction, laryngospasm,bronchial secretions, lug disease. - Respiratory depression due to premedication iv
induction agent inhalational agent itself. - Increased circulation to non vital organs: in
anxiety, thyrotoxicosis, obesity, robust subjects.
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 18/25
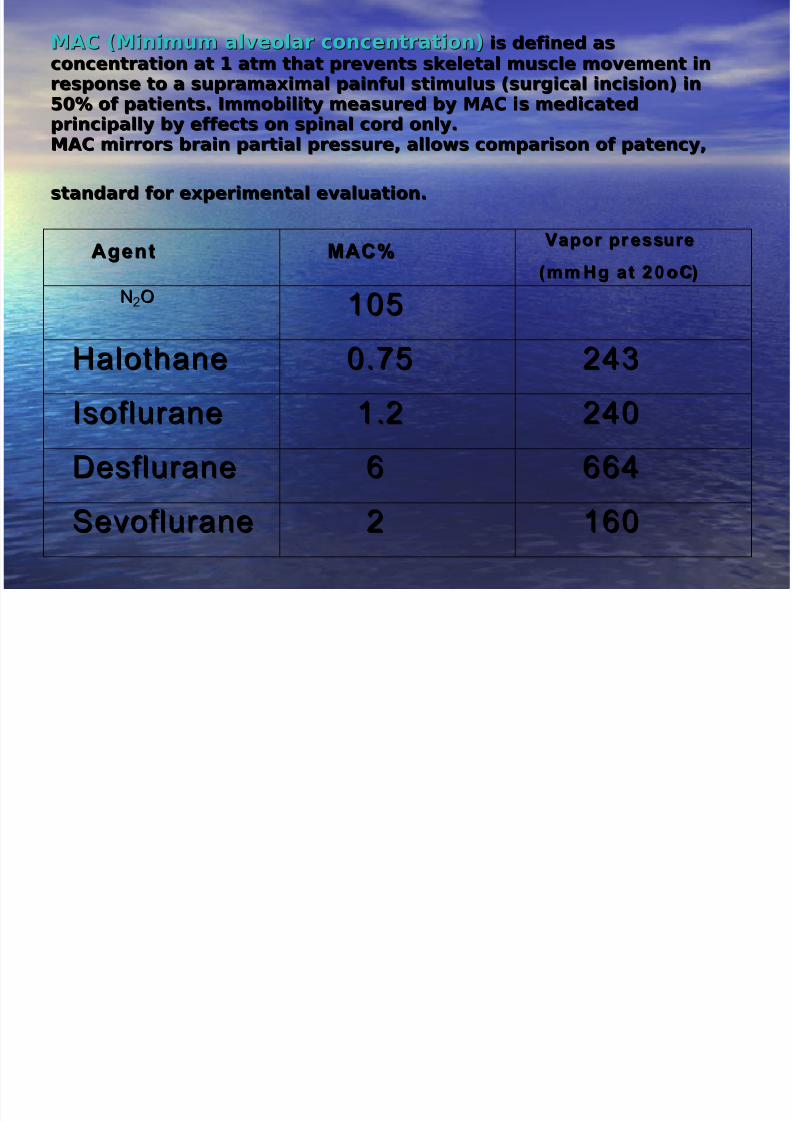
MAC (Minimum alveolar concentration)MAC (Minimum alveolar concentration) is defined asis defined as
concentration at 1 atm that prevents skeletal muscle movement inconcentration at 1 atm that prevents skeletal muscle movement inresponse to a supramaximal painful stimulus (surgical incision) inresponse to a supramaximal painful stimulus (surgical incision) in50% of patients. Immobility measured by MAC is medicated50% of patients. Immobility measured by MAC is medicatedprincipally by effects on spinal cord only.principally by effects on spinal cord only.
MAC mirrors brain partial pressure, allows comparison of patency,MAC mirrors brain partial pressure, allows comparison of patency,
standard for experimental evaluation.standard for experimental evaluation. AgentAgent MAC%MAC% Vapor pr essureVapor pr essure
(mm Hg at 20 oC)(mm Hg at 2 0oC) NN2OO 105105
HalothaneHalothane 0.750.75 243243
IsofluraneIsoflurane 1.21.2 240240
DesfluraneDesflurane 66 664664
SevofluraneSevoflurane 22 160160
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 19/25
• MAC are roughly additive for CNS depression.
•• CVS effect may not be equivalent at same MAC.
•• MAC is equivalent to median effect dose.
•
• Roughly 1.3 MAC of any volatile anesthetic has beenfound prevent movement in about 95% of patients(ED95)
•
• MAC awake: 0.3-0.4 MAC•• MAC-BAR: blockade of adrenergic response in 50% of
subjects due to surgical stimulus.
•
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 20/25
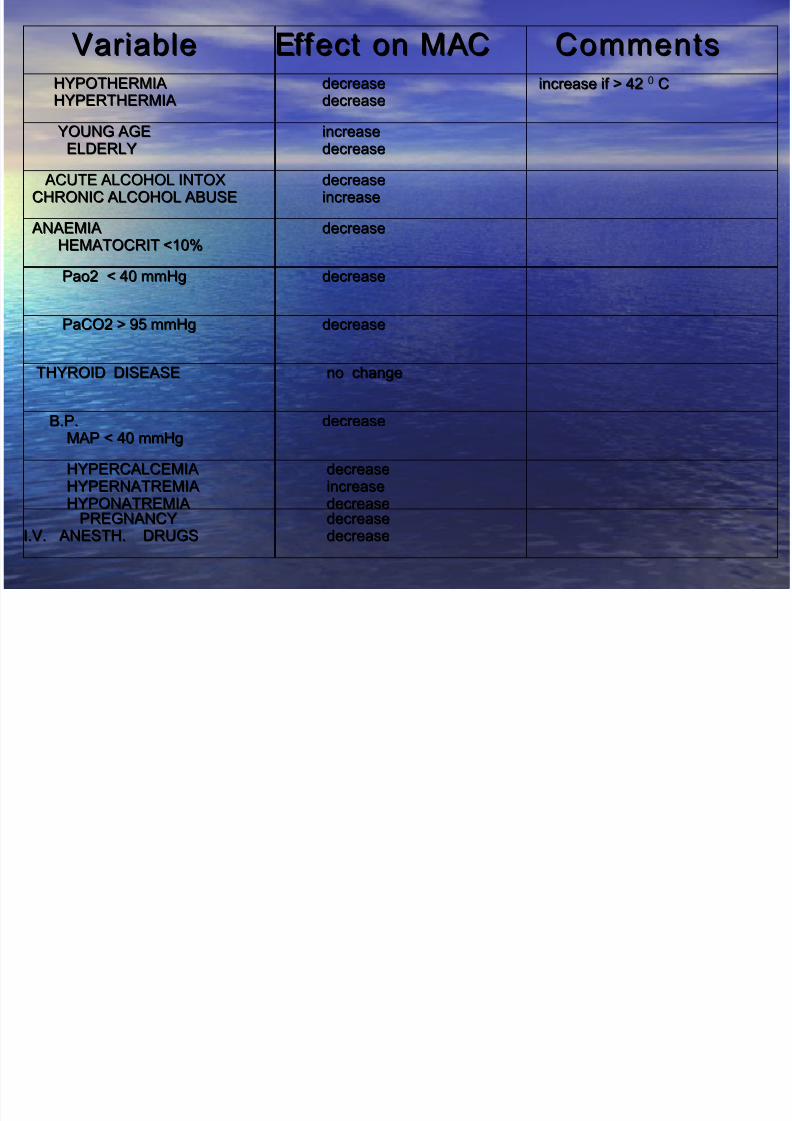
VariableVariable Effect on MACEffect on MAC CommentsCommentsHYPOTHERMIAHYPOTHERMIAHYPERTHERMIAHYPERTHERMIA
decreasedecreasedecreasedecrease
increase if > 42increase if > 42 0 CC
YOUNG AGEYOUNG AGEELDERLYELDERLY
increaseincreasedecreasedecrease
ACUTE ALCOHOL INTOXACUTE ALCOHOL INTOXCHRONIC ALCOHOL ABUSECHRONIC ALCOHOL ABUSE
decreasedecreaseincreaseincrease
ANAEMIAANAEMIAHEMATOCRIT <10%HEMATOCRIT <10%
decreasedecrease
Pao2 < 40 mmHgPao2 < 40 mmHg decreasedecrease
PaCO2 > 95 mmHgPaCO2 > 95 mmHg decreasedecrease
THYROID DISEASETHYROID DISEASE no changeno change
B.P.B.P.MAP < 40 mmHgMAP < 40 mmHg
decreasedecrease
HYPERCALCEMIAHYPERCALCEMIAHYPERNATREMIAHYPERNATREMIAHYPONATREMIAHYPONATREMIA
decreasedecreaseincreaseincreasedecreasedecrease
PREGNANCYPREGNANCYI.V. ANESTH. DRUGSI.V. ANESTH. DRUGS
decreasedecreasedecreasedecrease
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 21/25
• Among the most striking is 6% decrease in MAC per decade of age
• MAC is relatively unaffected by species, sex or duration of anesthesia
• 150
• Estimated MAC = --------------------------------------
• oil gas partition coefficient Theories of anesthetic action
• General anesthesia: loss of consciousness, analgesia, amnesia,muscle relaxation.
• Variety of substances capable of producing general anesthesia.
• Various agents probably prevalence anesthesia by different methods(agent specific theory)
• Mechanism of immobility: - due to action on spinal cord.
• Drug induced depression of excitation and enhancement of inhibition.
• Excitatory alpha amino 3AMPA and NMDA receptors and inhibitory.
• GABA and glycine receptors involved, Na ion channel also important
• Ionotropic and metabotrapic receptors Ionctropic (ligand gated ion channels) – neurestransmitter GABAreceptors.
Metabotropic receptors – Neutrotransmitter acetyl choline –activation of G protein lead to second messenger pathway.
• Glumatate (NMDA, AMPA and kainate receptors)
• Glutamate is principal excitatory neurotransmitter and - important role in immobility
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 22/25
unconsciousnessunconsciousness•• Inhaled anesthetics must act through specific interactions with target
molecule (presumably protein) in CNS
•• Unconsciousness results from action at higher centre.
•• Correlation between ability to hyperpolarize neurons and anestheticpotency.
•• Volatile anesthetic enhance inhibitory synaptic transmission especially
at synapses where GABA is major neurotransmitter in brain(especially reticular activating system)
•• Glycine is another important inhibitory neurotransmitter in spinal cord
and brain stem.
•• Presynaptic sodium ion channels and voltage gated calcium channel
also effected.•
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 23/25
• Molecular and cellular mechanism
• At molecular level, anesthetics almost
certainly ct by binding directly to proteinsrather than by pertubing lipid bilayers.
• Stereoselectively suggest existence of specificbinding sites on membrane protein. Ex.levoisomer of isoflurane is more potent.
• There is accumulating evidence the GABA andglycine receptors provide molecular bindingsites for inhaled anesthetics.
•• MAYER OVERTON THEORY (Critical
volume hypothesis)
• Unitary hypothesis – All inhalational agentsshare a common mechanism of action at
molecular level.
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 24/25
• According to this theory, there is correlation betweenlipid solubility (oil gas partition coefficient) andanesthetic potency.
•• When a sufficient number of molecules dissolve
(critical concentration) in crucial hydrophobic sitessuch as lipid cell membrane, there is distortion of channel necessary foreign flux, likewise changes in
lipid matrix produced by dissolved anestheticmolecules could alter the function of protein in cellmembrane.
•• This is supported by reversal of anesthetic effects by
high pressure (40-100 atm.)
•• Evidence against theory include:
• Effect on lipid bilayers are implausibly small and can
produced by temperature change of 1oC• Not all li id soluble dru s are anesthetic infact, some
8/6/2019 Uptake of Inhalational anaesthetics
http://slidepdf.com/reader/full/uptake-of-inhalational-anaesthetics 25/25
THANKSTHANKS