integrating pmtct with post natal … pmtct with post natal care...ii declaration i, maureen...
TRANSCRIPT

INTEGRATING PMTCT WITH POST
NATAL CARE SERVICES IN UGANDA:
PROCESS DOCUMENTATION AND
MONITORING OUTPUTS
BY
MAUREEN KWIKIRIZA
2012

INTEGRATING PMTCT WITH POST NATAL CARE
SERVICES IN UGANDA: PROCESS DOCUMENTATION
AND MONITORING OUTPUTS
BY
Dr. MAUREEN KWIKIRIZA
MBCHB, MSC.EPIDEMIOLOGY
MakSPH-CDC Fellow
NOVEMBER 2012

ii
DECLARATION
I, Maureen Kwikiriza do hereby declare that this programmatic activity
report titled Integrating PMTCT with post natal care services in
Uganda: Process Documentation and Monitoring outputs, has been
prepared and submitted in fulfillment of the requirements of the MakSPH-
CDC Fellowship Program and has not been submitted for any academic
qualifications.
Signed…………………………………. Date……………………..
Dr. Maureen Kwikiriza, Fellow
Signed…………………………………. Date……………………….
Dr. Francis Engwau, PM PREFA
Host Institution mentor
Signed…………………………………….. Date………………………
Dr. David Serukka, ED PREFA
Host institution mentor
Signed……………………………………. Date………………………..
Dr. Elizabeth Nabiwemba, MakSPH
Academic mentor

iii
DEDICATION
This work is dedicated to all the mothers of this nation and those who are
yet to be.
iv
ACKNOWLEDGEMENT
Great thanks to my mentors for the support and time given to me.
I would also like to thank PREFA staff especially the Program Officers of
Wakiso and Nakasongola districts for their effort during this project.
Finally, I am indebted to my family, fellow Fellows and friends for all the
support and encouragement during this project.

v
Table of contents
DECLARATION ....................................................................................... ii
DEDICATION .......................................................................................... iii
ACKNOWLEDGEMENT ......................................................................... iv
LIST OF TABLES AND FIGURES .......................................................... vi
ACRONYMS ............................................................................................ vi
OPERATIONAL DEFINITIONS ............................................................. vii
EXECUTIVE SUMMARY ..................................................................... viii
1.0 INTRODUCTION ....................................................................... 1
Table 1: PMTCT services integrated in PNC .............................................. 3
2.0 DOCUMENTATION OF THE INTEGRATION PROCESS,
MONITORINGAS WELL AS INDENTIFYING CHALLENGES ......... 4
2.1 Pilot health facilities.......................................................................... 4
Table 2: Facilities piloting the integration model ........................................ 4
2.2 Steps in the implementation of integrated PMTCT and PNC services 4
2.2.1 The assessment phase…………………………………………...6
2.2.2Planning phase…………………………………………………...9
2.2.3 Implementation and monitoring phase .......................................... 11
2.3 PMTCT indicator performance following integration ...................... 11
3.0 DISCUSSION…………………………………………………….14
3.1 Discussion of the implementation and progress of integrated PMTCT
and PNC services .................................................................................. 14
3.2 Lessons learnt from the implementation of integrated PMTCT and
PNC services ........................................................................................ 15
4.0 CONCLUSION AND RECOMMENDATIONS ............................. 17
5.1 REFERENCE ................................................................................. 18
6.0APPENDICES ................................................................................. 19
6.1 Set targets for the health facilities after the assessment……….19
6.2Checklist .......................................................................................... 22
6.3 DATA EXTRACTION TOOL................................................................ 28

vi
LIST OF TABLES AND FIGURES
Table 1: PMTCT services integrated in PNC .................................................................... 3 Table 2: Facilities piloting the integration model............................................................... 4 Table 3: Set targets and responsible persons after the assessment phase ........................... 10 Table 4 : Weaknesses and action taken for Buwambo HC IV .......................................... 19 Table 5: Action points for Nabiswera HC III following the assessment ............................ 20 Table 6: Action points for Nakasongola HC IV following the assessment ........................ 21 Table 7:Action points for Ndejje HC IV following the assessment .................................. 21 Figure 1: steps involved in implementation of integrated PMTCT and PNC
services at health facility level…………………………………………….5
Figure 2: Uptake of PMTCT services by mothers during PNC …………..12
Figure 3: Uptake of EID services in PNC ………………………………..13
ACRONYMS
AIDS Acquired Immune Deficiency Syndrome
ART Anti-Retroviral Therapy
CDC Center for Disease Control

vii
DBS Dry Blood Sample
EID Exposed Infant Diagnosis
FP Family Planning
HIV Human Immunodeficiency Virus
MNCH Maternal, Newborn and Child Health
MOH Ministry of Health
NVP Nevirapine
PCR Polymerase Chain Reaction
PEPFAR Presidential Emergency Plan For AIDS Relief
PREFA Protecting Families Against HIV/AIDS
PNC Postnatal care
PMTCT Prevention of Mother–To- Child Transmission of HIV
VHT Village Health Teams
OPERATIONAL DEFINITIONS

viii
Integration: Two or more services are offered in the same facility and by
the same health worker and a strong referral system for services which
cannot be got at that facility.
Monitoring: Supervising activities in progress to ensure they are on-course
and on-schedule in meeting the performance targets.
Processes: Sequence of activities through which inputs are converted into
outputs. All processes are directed at achieving one goal
Process Documentation: This is a descriptive, non-evaluative procedure
where data is collected on a project to identify working approaches to
challenges of implementing an effective intervention/program.
EXECUTIVE SUMMARY
This report documents the processes of implementing integrated PMTCT
with postnatal care services at health facilities in Wakiso and Nakasongola
ix
districts of Uganda. It also focuses on monitoring progress of outputs
following the implementation. The integration was a pilot conducted by
PREFA, a local NGO as recommended by Ministry of Health.
In the integration, PMTCT services are part of PNC package offered on the
same day under the same roof. The objectives of the pilot were to identify
best practices for PMTCT and PNC integration at the health facility level as
well as attempt to demonstrate the results.
The implementation of integrated PMTCT and PNC services at health
facility level involved three major steps, which are; the Participatory
assessment phase, Feedback and planning phase and Implementation and
monitoring phase.
The assessment was conducted to inform the planning phase to set targets
for the implementation of the integration services. This was done in May
2012 by PREFA program officer and district PMTCT focal person with
participation of the health workers. The areas of focus were: human
resource, support supervision, availability of key supplies, recording of data
in the registers, continued use of services, infrastructure, flow of finances
and information, education and communication materials.
The findings of this assessment were then shared with all health workers
who made suggestions for implementing integration and improving the
services. Suggestions included mentoring health workers on records
management, logistics management and follow up of mother–baby pair,
regular integrated support supervision visits, and relocating immunization
and EID clinics to PNC ward.

x
From June to August 2012, the assessment team visited the health facilities
every month to monitor performance and progress of the output. Data of
key indicators was extracted, during these visits, from the registers and
analyzed for any improvement.
More mother-baby pairs were followed up in the community with an overall
average of 15 per month compared to five in the months of March and April
before the pilot began. The number of HIV exposed infants done PCR to
determine their HIV status also increased from less than 10 in April to 14 in
June. As these babies were tested, they also received their results.
Lessons learnt include: The participatory approach to problem identification
and solving motivated health workers to work towards the improved
indicators. Also, involving the district health leaders and facility in charges
in the planning and implementation of the integrated PMTCT and PNC
services promoted ownership
Integrating PMTCT with PNC services leads to increased uptake of
PMTCT services. For maximum benefit, there should be no staff
absenteeism and adequate stocks of drugs and supplies. To ensure the latter,
training of health unit managers in logistic management should be done
urgently. For sustainability of improvements, regular support supervision to
health facilities should be conducted.

1.0 INTRODUCTION
Prevention of Mother -To- Child Transmission of HIV (PMTCT) is a
program for preventing the transmission of HIV from an infected mother to
her child. With availability of antiretroviral drugs, HIV transmission from
mother to child can be reduced to less than 5%(WHO 2010a ; AIDSTAR-
One February 2011).The PMTCT program comprises four prongs(WHO
2010a) which are:
1. Primary prevention of HIV infection among women of reproductive
age
2. Prevention of unwanted pregnancies among women living with HIV
3. Prevention of HIV transmission from pregnant women living with
HIV to their infants
4. Providing appropriate treatment, care, and support to mothers living
with HIV and - their children and families.
In Uganda, the PMTCT program was started in 2000 and by March 2011
had scaled up to 1,320 health centers, including 90% of health center III
facilities. Despite the success in increasing geographical access, many HIV
positive mothers and their babies are being lost at some point in the
PMTCT- Early Infant Diagnosis process(MOH 2009/10). This is evidenced
in 2009/2010 PMTCT review report which showed that only 8% of
mothers were offered post natal care services including family planning and
only 35% of HIV exposed infants had a Dry Blood Spot (DBS) taken for
HIV diagnosis(MOH 2009/10; UNICEF 2010), despite the high turn up of
children for immunization (over 80%). To address the above challenges,

2
the National PMTCT scale up plan 2010-2015 recommends integration of
PMTCT with the already existing Postnatal care (PNC) services.
Ministry of Health (MOH) defines integration as both PMTCT and PNC
services being available and offered at the same time by the same provider
or referred to another provider within the same premises, and a network of
providers linked by a well-developed and monitored referral system. In the
integration, PMTCT services are part of PNC package offered on the same
day under the same roof. When a woman comes for post natal examination
or family planning, her HIV status should be established and if found to be
HIV positive enrolled into HIV chronic care. Similarly, an infant born to
HIV positive mother brought for immunization is offered Early infant
diagnosis (EID) services or the other way round.
Protecting Families Against HIV/AIDS (PREFA) thus piloted integration of
PMTCT and PNC in Wakiso and Nakasongola districts. PREFA is a local
Non-governmental Organization formed in 2004 to support the government
of Uganda to develop and maintain standards in capacity building for
PMTCT service provision, implementation and monitoring of PMTCT
services and, to identify service delivery gaps and seek solutions for them.
With funds from PEPFAR through CDC, the organization supports quality
PMTCT service provision in 40 districts of Uganda.
The health workers are trained and mentored to offer quality services. Table
1 below shows PMTCT services to be integrated in to PNC.

3
Table 1: PMTCT services integrated in PNC
Period Basic services Suggested PMTCT services
to be added/integrated in the
basic services
Postnatal
care
General examination and
treatment of the mother,
Family planning
counseling and provision,
Screening for cervical and
breast cancer, Health
education and counseling,
Community Outreaches,
General examination of
the baby, growth
monitoring and
Immunization.
TB screening
Establishing HIV status of
mother, EID services, referral
for ART & Comprehensive
Care, Prevention and treatment
of opportunistic infections,
Cotrimoxazole prophylaxis for
HIV positive mothers and their
babies
The integration is dependent on improved systems at the health facility
which include: adequate and trained human resource, logistics and supplies,
well-functioning laboratories, sound health management and information
system for monitoring and evaluation; and working referral and linkage
system both within and outside the facility.
The objective of the pilot was to identify best practices for PMTCT and
PNC integration at the health facility level. This would lead to
recommending working approaches for roll out and replication to other
sites.
This report, therefore, documents the processes and monitoring outputs of
integrating PMTCT with PNC services being piloted in Wakiso and
Nakasongola districts of Uganda by PREFA.

4
2.0 DOCUMENTATION OF THE INTEGRATION PROCESS,
MONITORINGAS WELL AS INDENTIFYING CHALLENGES
This section describes the steps involved in the implementation of
integrated PMTCT and PNC services and monitoring of outputs as well as
identifying best practices.
2.1 Pilot health facilities
The health facilities where the documentation and monitoring was
conducted are included in table 2 below.
Table 2: Facilities piloting the integration model
Facility Name Facility level District
Ndejje HC IV Wakiso
Buwambo HC IV Wakiso
Nakasongola HC IV Nakasongola
Nabiswera HC III Nakasongola
2.2 Steps in the implementation of integrated PMTCT and PNC
services
The steps in the implementation of integrated PMTCT and PNC services are
summarized in the figure 1 below.

5
Figure 1: Steps involved in implementation of integrated PMTCT and PNC
services at health facility level
Participatory assessment phase
1. Orientation workshop on assessment framework and
tools
2. Complete assessment of facilities including interviews
with health workers and observation of facility functioning
3. Collection of routine PMTCT data from registers.
Feedback and planning phase
1. Review of assessment results
2. Identification of areas of weakness
3. Target setting and action plans
Implementation and monitoring phase
1. Planned interventions implemented
2. Monthly support visits by the task force to
determine progress towards targets

6
2.2.1 The assessment phase
As part of the implementation process, an assessment of obtaining
conditions in the pilot health units was first conducted. This would inform
the planning phase to set targets of what would assist the implementation of
the integration model.
The assessment was conducted by a team of three people that included the
MakSPH-CDC fellow, PREFA program officer and district PMTCT focal
person. This was to determine the capacity of the health facilities to offer
quality and integrated PMTCT and PNC services. The assessment was done
in the month of May 2012 and looked at the following domains: human
resource, support supervision, availability of key supplies, documentation of
data in the registers, continued use of services, infrastructure, flow of
finances and information, education and communication (IEC) materials.
Two data collection tools were developed and used for the assessments: a
checklist and a tool to extract data of key indicators on PMTCT and PNC
services from the registers. The findings of the assessment were as follows:
a)Human resource
i) Staff number
On average, each facility had one midwife and a nursing assistant to
manage post natal care services. However, they are also expected to give a
helping hand in antenatal and maternity wings.
ii) Staff availability
Staff absenteeism and late coming to work was common in three out of the
four facilities which increased the work load for the already stretched

7
human resource. During the monthly visits in one of the facilities a mother
lamented that; “Last week I came at about 11:00 am. The midwife told me to
go back because I was late. Today I was here by 8:00 am; it is now 11:00
am and there is no midwife to work on us”. The team arrived at this facility
at about 10:30 am and the midwife had not yet arrived, yet there were
many mothers waiting for services ranging from antenatal care, Family
planning , EID and PNC. The excuse the midwife gave for late coming was
she resides far from the facility (which was true) and transport to the facility
is sometimes difficult to get.
iii) Knowledge and skills
Each facility had at least 2 midwives and one laboratory assistant trained in
PMTCT-EID strengthening program. The nursing assistant, though not
trained in the program, benefited from the mentorship which was conducted
for the health workers at the facility.
b) Support supervision
Supervision for PMTCT and MNCH services was done separately as there
was no integrated support supervision tool. The Support supervision from
the district health team was irregular.
c) Availability of logistics and supplies
Though by the time of the assessment all the facilities were stocked with
EID supplies, family planning commodities and PMTCT antiretroviral
drugs (ARVS), only one health unit was placing in timely orders to National
Medical Stores for supplies.
There was shortage of equipment and supplies like Blood pressure
machines, Stethoscope, weighing scales, gloves, cotton, detergents, gum
boots and aprons in all the facilities.

8
d) Recording data in the registers
All the four facilities had the recommended and up to date PNC register
and EID data tools as by Ministry of Health. However, incomplete and
inaccurate documentation was common to all facilities. Post natal register is
hardly used though on observation and interviews, there are post natal
services given to both the mother and baby but not documented. In two
health facilities, EID data tools were available but kept in the cupboard. It
was difficult to trace these babies as the details of their address could not be
got from the registers.
e) Access and continued use of services
At all the health facilities, EID care point was located in a different site
(ART clinic or laboratory) from PNC. Also at 2 facilities, immunization
clinic was located in outpatient department. EID and immunization were
offered once a week while post natal care to the mother including family
planning was done upon request.
f) Infrastructure
The postnatal wing could be structured to accommodate all the service
points during postpartum period. However, the waiting areas are small and
lacked enough seats for the waiting clients.
g) IEC materials
There were few job aides for PMTCT and PNC services at the health
facilities.

9
h) Flow of finances
All the four health facilities were under local government with limited
budget allocated for PMTCT and PNC services. Funds from implementing
partners to the facilities are through the district. Three facilities had
difficulties in finance management.
2.2.2Planning phase
The analysis of the findings was done together with the health workers and
the results shared. Targets were set according to the weak areas highlighted
for integration. Some of the set targets after the assessment are included in
table 3 below.

10
Table 3: Set targets and responsible persons after the assessment phase
Weakness Action Responsible person
Staff Absenteeism Call for staff meeting and
discuss the issue
DHT/ In charge
Stock out of Nevirapine
syrup
Correct ordering of PMTCT
ARVS
Midwives/ In charge
Provide buffer PREFA
Facilities not ordering Mentor health workers on
logistic management
PREFA/DHT
Immunization clinics in
OPD
Shift immunization clinics
to PNC wing
Facility in charge
Lack weighing scales Provide adult weighing
scale
PREFA
Missed opportunity for
mothers to get PNC
Midwives should be active
and also offer PNC to
mothers. During
Immunization, a midwife
should be present to attend
to the mothers
In charges
Weak EID care point Shift EID care point from
ART clinic to MCH
Facility PMTCT focal
person
Provide another EI register PREFA
Mentor/Coach HW on EID
and the data tools
PREFA
Loss to follow up of HIV
positive mothers and
their babies
Ensure the facilitation for
follow up goes to the right
people, and coach Midwives
on how to use appointment
book to follow up mother-
baby pair
PREFA , In charge
and PMTCT focal
person
Incomplete
documentation in the
registers
Mentor/ coach health
workers on proper
documentation
PREFA
Weak community
linkages
Orient VHTs on PMTCT-
EID program
PREFA/District
Few PMTCT posters Provide with missing charts PREFA
Few internal support
supervisions
In charge to improve on
support supervisions to his
subordinates
In charge

11
2.2.3 Implementation and monitoring phase
The overall unit in charge and head of maternal and child health department
coordinated the implementation of activities to achieve the set targets at
their respective health facilities. Each month, from June to August 2012, the
monitoring team (one that led assessment) visited the pilot health facilities
to monitor performance towards the set targets; and set new targets. This
monthly follow up of performance at the health facilities constituted the
monitoring phase. In July 2012, health workers from the facilities in Wakiso
district were taken to a nearby health unit with good PMTCT indicators to
witness best practices.
Data of key indicators were extracted, during these visits, from the registers
and analyzed for any improvement. The main indicators monitored are:
number of new women tested for HIV in PNC, number of HIV positive
women receiving any modern family planning method and followed up in
the community. For HIV exposed infants, indicators were: number refilled
with nevirapine syrup, initiated on cotrimoxazole, had first PCR done and
received results.
2.3 PMTCT indicator performance following integration
Overall, the monitored indicators improved over the period of implementing
integrated PMTCT and PNC services. Mothers, who had missed HIV
counseling and testing during antenatal visits, were captured in PNC period.
More HIV positive mothers and their babies were followed up in the
communities every month following the introduction of the pilot integration

12
project. The maximum number was 25 in June, with an overall average of
15 per month compared to five in the months of March and April before the
pilot began (Figure 2). This is as a result of actively involving the Village
Health Teams (VHTS) in conducting home visits to HIV positive mothers
and their babies.
Figure 2: Uptake of PMTCT services by mothers during PNC
Similarly, more HIV exposed infants (from less than 5 in April to 9 infants
in August) were initiated on cotrimoxazole prophylaxis at 6 weeks (Figure
3). The number of infants done PCR to determine their HIV status also
increased from less than 10 in April to 14 in June. As these babies were
tested, they also received their results.
13
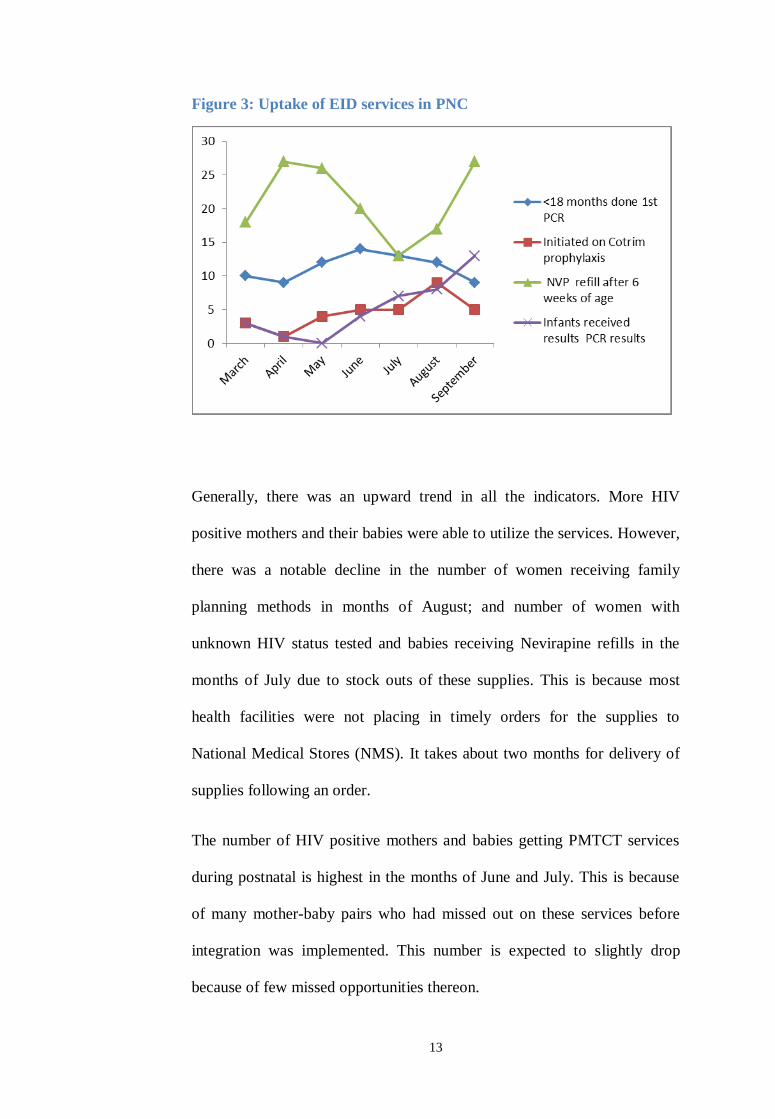
Figure 3: Uptake of EID services in PNC
Generally, there was an upward trend in all the indicators. More HIV
positive mothers and their babies were able to utilize the services. However,
there was a notable decline in the number of women receiving family
planning methods in months of August; and number of women with
unknown HIV status tested and babies receiving Nevirapine refills in the
months of July due to stock outs of these supplies. This is because most
health facilities were not placing in timely orders for the supplies to
National Medical Stores (NMS). It takes about two months for delivery of
supplies following an order.
The number of HIV positive mothers and babies getting PMTCT services
during postnatal is highest in the months of June and July. This is because
of many mother-baby pairs who had missed out on these services before
integration was implemented. This number is expected to slightly drop
because of few missed opportunities thereon.

14
3.0 DISCUSSION
3.1 Discussion of the implementation and progress of integrated
PMTCT and PNC services
The first step of assessing the capacity of health facilities made it possible
to identify bottlenecks for the implementation of integrated PMTCT and
PNC services. Involving the health workers in both assessment and setting
the targets for performance promoted ownership of the program by the
facility. In addition, it also built the capacity of the facility in charges to
conduct a simple assessment about quality of services at their respective
health units.
Identification of weak areas and implementation of a regularly supervised
participatory approach to problem solving that was data driven, resulted in
improvement of integration of PMCT/PNC services. Consequently, there
was some improvement in all indicators despite the short period of
implementation. These findings are in agreement with an intervention that
used a participatory approach in South Africa resulting in improved
PMTCT indicators(Tanya Doherty, Mickey Chopra et al. 2009). Also in
Zimbabwe, a district approach using regular team meetings was successful
in enhancing HIV testing acceptance(Perez F, Mukotekwa T et al. 2004).
The implementation process had quality improvement aspects of target
setting and monthly monitoring of performance. Continuous quality
improvement interventions have showed improvement in health services
(Center for Applied Research on Population and Development 2003;
Berwick DM 2004). Studies show that feedback on performance and small
group meetings have a positive effect on changing health worker

15
behavior(Grol R and Grimshaw J 2003). Therefore, since this intervention
involved these elements which could be part of the explanation for the
results.
The main limitation of the pilot was the short time of observation as some
set targets like orienting village health teams was not done but plans were
made to do so.
During this period of observation, there were no new health programs or
media activities taking place. It is therefore possible that the improvement
seen is due to integration of PMTCT and PNC services.
3.2 Lessons learnt from the implementation of integrated PMTCT and
PNC services
The lessons are drawn from the observation of the implementation process
of integrated PMTCT and PNC services at the health facility level. They
include the following:
Participatory approach to problem identification and solving
motivates health workers to work towards improved indicators
Technical support through supervision and mentorships enhance the
knowledge and skills of health workers
When there is linkage between service-delivery points in the facility,
there are few missed opportunities

16
With proper documentation in the registers, details for mother-baby
pair who have missed could be got and then followed up in the
communities.
Involving district health leaders and facility in charges in the
planning and implementation of integrated PMTCT and PNC
services promoted ownership of the program. Some of the set targets
were to be effected by the district health team authority.
When VHTS are facilitated, they sensitize and mobilize
communities for PMTCT and PNC services; and conduct home
visits to HIV positive mothers and their babies. This reduces
workload for the health workers.
The central supply chain system through NMS has encouraged
facilities to place in timely orders for the needed supplies. However,
lapses on the part of health units results in stock outs.
Staff absenteeism increases the workload stretching the available
health workers.

17
4.0 CONCLUSION AND RECOMMENDATIONS
Integrating PMTCT with PNC services reduces missed opportunities and
thus increase uptake of PMTCT services. Involving health workers in
monitoring progress and quality of services motivated them to implement
the new changes. However, inadequate monitoring of stocks of supplies and
drugs affects quality of care.
To ensure sustainability of improvements, regular support supervision to
health facilities should be conducted. In addition to that, staff should be
mentored on supplies management.

18
5.1 REFERENCE AIDSTAR-One (February 2011). Integrating Prevetion of Mother-To-Child Transmission
of HIV interevtions with Maternal. newborn and child health services: Technical Brief.
Berwick DM (2004). "Lessons from developing nations on improving health care." BMJ
328: 1124-1129.
Center for Applied Research on Population and Development, Ed. (2003). Using data to
improve service delivery: a self evaluation approach. . CERPOD.
Grol R and Grimshaw J (2003). " From best evidence to best practice: effective
implementation of change in patients' care. ." Lancet 362: 1225-1230.
MOH (2009/10). Uganda National PMTCT report.
Perez F, Mukotekwa T, et al. (2004). " Implementing a rural programme of prevention of
mother-to-child transmission of HIV in Zimbabwe: first 18 months of experience
" Tropical Medicine and International Health
9: 774-783.
Tanya Doherty, Mickey Chopra, et al. (2009). "Improving the coverage of the PMTCT
programme through a participatory quality improvement intervention in South Africa."
BMC Public Health 9: 406
UNICEF (2010). Uganda : PMTCT fact statistics, UNICEF.
WHO 2010a PMTCT Strategic Vision 2010–2015:Preventing mother-to-child transmission
of HIV to reach the UNGASS and Millennium Development Goals. Geneva, Switzerland:
WHO.

6.0APPENDICES
6.1 Set targets for the health facilities after the assessment
Table 4 : Weaknesses and action taken for Buwambo HC IV
Weakness Action Responsible person
Staff Absenteeism Call for staff meeting and
discuss the issue
DHT/ In charge
Missed opportunity for
mothers to get PNC
Midwives should be active
and also offer PNC to
mothers. During
Immunization, a midwife
should be present to attend
to the mothers
In charges
MCH unit lacking adult
weighing scale
Provide adult weighing
scale
PREFA
Weak EID care point Shift EID care point from
ART clinic to MCH
Facility PMTCT focal
person
Provide another EI register PREFA
Mentor/Coach HW on EID
and the data tools
PREFA
Loss to follow up of HIV
positive mothers and
their babies
Ensure the facilitation for
follow up goes to the right
people, and coach Midwives
on how to use appointment
book to follow up mother-
baby pair
PREFA , In charge
and PMTCT focal
person
Incomplete
documentation in the
registers
Mentor/ coach H/W on
proper documentation
PREFA
Weak community
linkages
Orient VHTs on PMTCT-
EID program
PREFA/Dht
Few PMTCT posters Provide with missing charts PREFA
Few support supervision
VISITS
DHT to conduct regular
support supervision visits
DHT

20
Table 5: Action points for Nabiswera HC III following the assessment
Weakness Action Responsible person
Staff Absenteeism Call for staff meeting and
discuss the issue
DHT/ In charge
Stock out of Nevirapine
syrup
Correct ordering of PMTCT
ARVS
Midwives/ In charge
Provide buffer PREFA
Missed opportunity for
mothers to get PNC
Midwives should be active
and also offer PNC to
mothers. During
Immunization, a midwife
should be present to attend
to the mothers. Shift
Immunization clinic to
MCH from OPD.
In charges
Weak EID care point Shift EID care point from
Lab to MCH
Facility PMTCT focal
person
Mentor/Coach HW on EID
and the data tools
PREFA
Loss to follow up of HIV
positive mothers and
their babies
Ensure the facilitation for
follow up goes to the right
people, and coach Midwives
on how to use appointment
book to follow up mother-
baby pair
PREFA , In charge
and PMTCT focal
person
Incomplete
documentation in the
registers
Mentor/ coach H/W on
proper documentation
PREFA
Weak community
linkages
Orient VHTs on PMTCT-
EID program
PREFA/DHT
PMTCT posters kept in
the cupboard
Hang posters on the wall In charge
Irregular support
supervision
DHT conduct regular
support supervision
DHT

21
Table 6: Action points for Nakasongola HC IV following the assessment
Weakness Action Responsible person
Missed opportunity for
mothers to get PNC
Midwives should be active
and also offer PNC to
mothers. During
Immunization, a midwife
should be present to attend
to the mothers.
Midwives
Record in PNC register Midwives
Loss to follow up of HIV
positive mothers and
their babies
Provide funds for follow up
of mother baby pair
PREFA , In charge
and PMTCT focal
person
Weak community
linkages
Orient VHTs on PMTCT-
EID program
PREFA/District
Table 7:Action points for Ndejje HC IV following the assessment
Weakness Action Responsible person
Small client waiting area Expand the waiting area/
provide a tent
District/ PREFA
Shortage of TT and DPT
vaccines
Order enough vaccines In charge
Missed opportunity for
mothers to get PNC
Midwives should be active
and also offer PNC to
mothers
Mid wives
lacking blood pressure
machine
Get the B.P machine from
the theater
In charge
PCR results given to
caregiver by lab tech
PCR results from the lab
should be taken to the EID
care point who then will
give to the caregiver
Facility PMTCT focal
person
Loss to follow up of HIV
positive mothers and
their babies
Ensure the facilitation for
follow up goes to the right
people, and coach Midwives
on how to use appointment
book to follow up mother-
baby pair
PREFA , In charge
and PMTCT focal
person
Incomplete
documentation in the
registers
Mentor/ coach H/W on
proper documentation
PREFA
Weak community
linkages
Orient VHTs on PMTCT-
EID program
PREFA/District
Few PMTCT posters Provide with missing charts PREFA
Irregular support
supervisions
DHT conduct regular
support supervisions
In charge

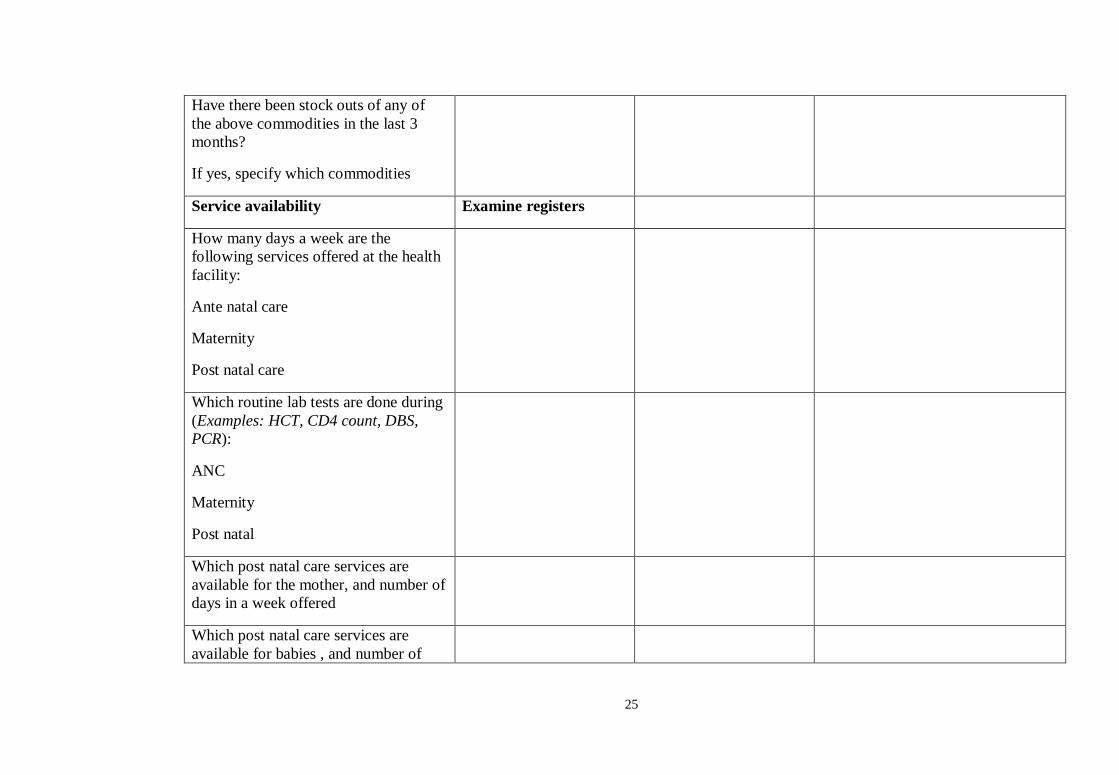
6.2Checklist This checklist will be used by the supervisors during the support visits to the health facility
Purpose: To assess the capacity of the health facility to offer quality integrated PMTCT/PNC services.
Section 1
Name of health facility…………………………………………………………………………………………..
Name of supervisors……………………………………………………………………………………………………………..
Date of visit----------/---------/--------
Indicator Means of verification YES/NO/NUMBERS Comments
Staff availability Observe facility
records, training
reports
1. Doctors
2. Clinical officers
3. Midwives
4. Nurses

23
5. Lab technician
6. Nursing aide
7. Records assistant
8. VHT
Number of staff trained in PMTCT-EID
Number of staff trained in EMOC
Number of staff trained in newborn
care
Infrastructure
The waiting area protects clients from
the sun and rain
Observation of waiting
area
The area is clean, walls and ceiling are
reasonably clean
Observation of the floor,
walls, roof/ceiling
Examination rooms are private and
privacy is maintained during
procedures
Observation of
examination rooms
The clinic has clean toilets/ latrines for
clients
Observation of the
toilets/latrines
Clinic provides adequate infection
prevention/control in area of hand
Observation of available
water and soap, and

24
washing, with soap and water available provider practice
Clinic has a container for sharps and
needles
Observation of procedure
room /injection room
Clinic has a rubbish pit for disposal of
refuse and medical waste
Observation of rubbish
pit or garbage bin
Logistics and supplies Examine stock cards,
store
Does the clinic have the following
commodities?
-Vaccines for Mother and baby
-ARVs prophylaxis
-HAART
-HIV test kits
-Family planning supplies
-Sterilization
-Gloves
-Delivery sets
-Gum boots
-Plastic sheet/ Apron
-Eye goggles
25
Have there been stock outs of any of
the above commodities in the last 3
months?
If yes, specify which commodities
Service availability Examine registers
How many days a week are the
following services offered at the health
facility:
Ante natal care
Maternity
Post natal care
Which routine lab tests are done during
(Examples: HCT, CD4 count, DBS,
PCR):
ANC
Maternity
Post natal
Which post natal care services are
available for the mother, and number of
days in a week offered
Which post natal care services are
available for babies , and number of

26
days in a week offered
Partnerships and referrals Examine referral
forms, registers
Where do they refer their patients
What is the procedure of referral
Is there any communication means to
where they refer clients (provide
ambulance, feedback)
Records management Examine recording
tools
Do staffs use recommended HMIS
forms?
Do staffs use recommended HMIS
forms?
IEC materials Observe on walls, clinic
rooms for charts
-Which IEC materials are available
-In which languages?
--Are there materials you could use that
you do not have?

27
Conclusions Summarize your findings as below
Strengths
Weaknesses/ Areas that need strengthening
Recommendations/ Action points

28
6.3 DATA EXTRACTION TOOL
This form will be used to extract data of key indicators that monitor progress of PMTCT/PNC integrated services at the health facilities.
Information will be got from PNC register, PMTCT-dispensing log, HIV test register, Referral books, Exposed Infant register, clinical
charts and Child Health cards.
Section 1:
Name of health facility……………………………………………………………………………..
Reporting month …………………… Year…………………………..
Section 2: Information about mother
2.1 Number of women attending post natal care-----------
2.2 Number of women with known HIV status--------------------
2.3 Number of women attending post natal care with unknown HIV status--------------
2.4 Number of women attending post natal care with unknown HIV status tested for HIV--------------------
2.5 Number of women attending post natal care counseled about modern family planning method------------------------
2.6 Number of women supplied with any method of family planning---------------------------
2.7 Number of HIV positive women on ART---------------------

29
2.8 Number of HIV positive women referred for HIV chronic care-----------------
Section 3; Information about Infants
3.1 Number of babies attending immunization clinic----------
3.2 Number of children confirmed HIV positive ----------
3.3 Number of children born to HIV positive mothers--------------
3.4 Number of HIV exposed children refilled for Septrin------------
3.5 Number of HIV exposed children refilled with Nevirapine syrup----------
3.6 Number of HIV exposed children PCR done at 6 weeks------------
3.7 Number of HIV exposed babies first PCR done after 6 weeks-------------
3.8 Number of children HIV results returned at the health facility--------------
3.9 Number of children received HIV results-------------
3.10 Number of HIV exposed children turned HIV positive--------------
3.11 Number of HIV positive children referred for HIV chronic care--------------
3.12 Number of referred HIV positive children enrolled into pre-ART care------------