intergenerational health correlations: is it genes or is...
TRANSCRIPT
Intergenerational health correlations: Is it genes or is it
income?
Ana Llena-Nozal
a*
Maarten Lindeboom b
Bas van der Klaauw c
January 2006
Very preliminary and incomplete
Abstract: This paper investigates how much of health is transmitted across generations through
genetics and how much through behavior and socio-economic status (SES). Low SES children
start adulthood with lower education and health and this may constrain their economic position in
adulthood. The intergenerational correlation of income may be linked to health but it is not clear
what mechanisms are driving this. Low SES parents may face financial constraints that lower
parental investment, they may have lower parenting skills, or they may have worse health
outcomes that constraint economic opportunities and these may be transmitted across generations.
Both unobserved heterogeneity and parental health need to be accounted for in order to
disentangle the correlation. We use a cohort study, the National Child Development Study, which
follows individuals since their birth in 1958 until their 40s. We exploit the richness of the data
and incorporate information on twins, adoptees and the cohort members’ own children to
disentangle the nature and nurture components. Our findings suggest that parental income
significantly reduces the risk of ill health in children. Individuals not having a natural father are
more prone to poor health but experience a similar mitigating impact of income. Income appears
to no longer be significant when we control for parental health and time investment. On the other
hand, when financial difficulties are used to measure poverty, the effects persist, even after
controlling for individual unobserved heterogeneity.
a: Free University Amsterdam & Tinbergen Institute.
b. Free University Amsterdam, Tinbergen Institute, HEB, IZA & Netspar.
* Correspondence: Department of Economics and Business Administration, Free University of Amsterdam,
De Boelelaan 1105, 1081 HV Amsterdam, The Netherlands. E-mail: [email protected]

c. Free University Amsterdam, Tinbergen Institute, Scholar & CEPR.

1. Introduction
There exists a strong positive association between health and socio-economic status (SES) at
adult ages. Whilst there is agreement on the strength of the association between health and SES,
little is known about the underlying mechanisms. Causality can run both ways: from poor health
to lower income or from low income to poorer health. Many studies point out that the gradient in
health status has its antecedents in childhood and in recent years there has been a growing
literature exploring the association between SES and health in childhood. Looking at child’s
health instead of adult health has the additional advantage that it rules out problems of reverse
causality. Indeed, in Western countries, children do not contribute to family income and one can
therefore focus solely on the adverse effects of poverty on health. There are several reasons why
parental income might be associated with offspring’s health. One possibility is that parents from a
lower socio-economic background suffer from financial constraints and invest less in their
children's education, nutrition and environment. Financial constraints might results in parents
from lower incomes purchasing less health care or other goods affecting child’s health. Parental
decisions such as prenatal care and nutrition can be affected by parental income and wealth and
may have a strong influence in the health of their children even as they enter adulthood. In
addition, lower income can influence health through the effects of the environment such as
neighborhood and housing conditions. Secondly, health behavior is correlated with income and
worse health habits (drinking, smoking and exercise) might be transmitted across generations.
Finally, health problems might be genetically transmitted across generations. In particular, some
studies have shown the association between parental mortality from cardiovascular disease and
offspring’s birth weight (Davey Smith et al., 1997) and between parental diabetes and offspring’s
birth weight (Hypponen et al., 2003). Genetic endowments might also explain why some
individuals are both healthier and wealthier. Both unobserved heterogeneity and parental health
need to be accounted for in order to disentangle the correlation.
Recent research has looked at the possible transmission mechanisms between income and
child’s health. Most studies point out that: 1) Permanent income appears to be more important
than current income; 2) it is the level rather than the changes in income which matter; and 3) that
it is persistent poverty rather than transitory or occasional poverty which matters (Benzeval &
Judge, 2001). Case, Lubotsky and Paxson (CLP-2002) suggest that the relationship can be partly

explained by the fact that children in higher-income households experience less chronic
conditions and their parents manage those conditions better. Higher income children have higher
health stocks for any given chronic conditions and low-income children have more adverse
effects from poor health at birth. They also find that the income effect for children living with
birth and non-birth parents is not significantly different. Nevertheless, controlling for health at
birth, parental health, health insurance and maternal labor supply does not completely eliminate
the effect of income and do not account for the income gradient in childhood health. Currie et al.
(2004) replicate the analysis with pooled data from the UK (HSE) and find that the size of the
gradient is significantly smaller and does not increase with child age. Using additional data on
nutrition and lifestyle, they find that consumption of vegetables and parental exercise are
important but do not reduce the income gradient in child heath. On the other hand, family income
is not important in determining health measured by blood tests results. Currie & Stabile (2003)
pursue this analysis further using panel data and find that children from both low and high SES
recover similarly from past health shocks. Their analysis shows that the gradient occurs because
low SES children receive more shocks.
Most studies on child health and income do not control for unobserved heterogeneity and
parental health. The methods used have generally looked at the association between parental
income and child health, controlling for a set of variables which attempt to capture the child’s
health endowment and as much as possible the parents own health and the parents’ production of
child health. Doyle et al. (2005) question to what extent the income (or education/SES) effects on
child’s health are the result of a spurious correlation due to the correlation with some
unobservable variables. The study by Kebede (2003) uses a fixed-effects specification to remove
the bias caused by the correlation between income and the unobservables. Kebede (2003)
examines the determinants of child health in rural Ethiopia and finds no significant correlation
between children’s health and per capita expenditures. Parental health is highly significant and
appears to influence child health through genetic rather than behavioral factors. On the other
hand, Burgess et al. (2005) question whether the use of fixed-effects for children is appropriate
since the individual effects at early ages might not be fixed. They use a cohort data from the UK
and find that, controlling for maternal health and parental choice of health inputs in early
childhood, there is almost no effect of income on child health. Their results also suggest that the
transmission mechanism from income to child health operates through maternal health (in
particular mental health) rather than through health related behaviors. Doyle et al. (2005) identify
the effect of parental education on child health using the exogenous variation in schooling caused
by the raising of the minimum school leaving age (for those born after September 1957) and

grandparent’s smoking histories as instrument for parental income. They find that the use of
instruments eliminates the effects of parental income and education.
In this paper we investigate how much of health is transmitted across generations through
genetics and how much through pregnancy-related growth, parental and own health behavior and
socio-economic status. We use the intergenerational information of a cohort study, the National
Child Development Study, which follows individuals since their birth in 1958 until their 40s. We
use the information on the parental background, health and behavior and income, and the
individual’s own information while exploiting the panel data nature of the data and the
information on the cohort member’s own children. This issue is particularly relevant for policy as
it provides further evidence on whether increasing parental income through different benefits
substantially contributes to children’s outcomes. In addition, it throws light on the process of
intergenerational mobility by examining what is the role of health transmission in the
intergenerational correlation of earnings or to what extent is the transmission of social
disadvantage merely a reflection of poor health transmitted across generations.
2. The model and empirical specification of the model
2.1 The Model
We base our conceptual framework on the demand for health model developed by Grossman
(1972, 1999) since it is the most relevant theoretical framework to explain an individual's health
status. Health is defined as a durable capital stock that produces an output of healthy time
(Grossman, 1972). The demand for health corresponds to two reasons: for consumption and for
investment purposes. It represents a consumption commodity because sick days produce
disutility. Health can be viewed as an investment commodity because it influences the time
available for market and nonmarket activities. Indeed, an increase in the stock of health may
increase economic resources through an increase in time available for work. Individuals are
supposed to inherit an initial stock of health, which depreciates with age and increases with health
investments.
In this paper, we focus on how health is transmitted from the parents. In this case, health
of offspring at birth might be due to a genetic component, but also partly the result of the
optimizing behavior of parents. Parents make decisions in terms of how to allocate the resources
in the households and invest in the child’s human and health capital. The health outcome of
children is thus a result of the parental maximization problem, where parents maximize the

expected value of an intertemporal utility function that has as arguments children's health,
commodities and health inputs. The household's utility function in each period follows
(Rosenzweig & Schultz, 1983; Rosenzweig & Wolpin, 1988):
U �U�X it,Z it,Hit;S�
where H is the health of the child, Z are health-related inputs (health behavior, health
environment, use of medical services), X are other commodities. Utility may also be affected by
household characteristics ( S� such as education and age (representing life cycle position and
preferences). Fertility decisions are taken as given and we ignore the problems of how decisions
are taken in the household. Preferences are assumed to be intertemporally additive and the utility
function is increasing and concave in its arguments (individuals are risk-averse). Households use
certain inputs and transform them through a production technology into the health of their
offspring. The production if child health is specified by the production function
H �h�Z it,��
where � represents family-specific health endowments known to the family but not
controlled by them and child characteristics such as inherent healthiness/immunity. Child health
is a function of such health inputs as nutrition, parental time and health care use, and of parental
health productivity (i.e. the ability to translate those inputs into the production of child health).
Production of health is also a function of past health. Parental decisions unknown to the
researcher affect this process. This is the case, for instance, if parental behavior responds to
unanticipated health outcomes as indicated by Rosenzweig & Wolpin (1988). The production of
child health (the health technology or productivity) is thus influenced by the characteristics of the
child, parental characteristics and the health environment. Income may affect the behavior of
parents in the case of credit constraints as poor parents may not be able to invest optimally.
On the other hand, the effect of income might also act through and impact on the quality of
parenting.
The budget constraint for the household is:
F ��
t
Wtp t
where F is exogenous money income, pt are exogenous prices and W �X�Z.
The reduced form demand function for the health outcome is:
H ���p,F,��.
Reduced form expressions relate the impact of exogenous factors on a variable representing
child’s health. To examine the relationship between health outcomes and health inputs, hybrid or
quasi-structural equations are used. The reason is the lack of available data.
H �� �Zm ,p l,F,��
where Ym corresponds to one input and the other are the determinants of all other inputs.
Nevertheless, "hybrid" functions give biased estimates according to Rosenzweig and Schultz
(1983) because they are unable to differentiate between the properties of the health production
function and the characteristics of the household preferences.
2.2. Empirical specification
In this paper we estimate a household health production function using information on several
health and morbidity indicators and a set of determinants such as parental characteristics and
parental health behavior.
Direct estimation of the production function will most likely lead to biased coefficient
estimates. The reason for the bias is that a mother may have information regarding her health
endowment that may influence her choice of inputs (health behavior for instance), leading to an
endogeneity of certain health inputs. The error term, containing household heterogeneity is likely
to be correlated with the health outcome-- thus OLS estimates will be inconsistent. Indeed, the
observed association between the variables and the measures of the child’s health will overstate
the consequences for the child’s health.
Consistent estimates of the health production can be obtained estimating a structural
demand system identifying the underlying preference parameters. Given the absence of all prices
and household expenditures, Rosenzweig and Schultz (1983) suggest that a two-stage least
squares. They estimate first the demand equations for behavioral input variables which are then
used for the second-stage estimates of the health production parameters. In our paper, we
combine different approaches to obtain as much information as possible on the relative
importance of factors that contribute to the intergenerational transmission of health. Firstly, we
will examine the association between income and child health at birth and during childhood and
adolescence. We will exploit the richness of our dataset and introduce several measures of
parental health and behavior in an attempt to capture as much heterogeneity as possible. We will
also exploit the panel data nature of the data to estimate individual fixed-effects for an indicator
for chronic illnesses. Secondly, we will look at three generations health outcomes since the
dataset contains information on the children of the cohort members and examine the effects of
grandparents’ and parents’ factors on the cohort member’s children while exploiting the variation
among siblings. Thirdly, we will use data on twins to difference out any correlation attributable to
genetics. Identical twins possess identical genetic endowments and share the same pre-natal
environment. Differences in the health of their children will be informative. Finally, we will use
adoptees to try to get a causal relation between health behavior and income. Children are
randomly placed with adoptive parents and thus the relationship between parental health and
children’s health cannot reflect genetic factors.
2.2.1 Fixed-effects
The indicator for the offspring health is regressed on time-variant covariates and the fixed-effects
are estimated. We will then regress the estimated individual fixed-effects on a series of variables
representing prenatal inputs, parental behavior in early life/Perinatal care inputs, parental health
productivity, and a set of own characteristics. We also take into account birth order and number
of siblings since it has been found to affect parental choice of other inputs since parents have to
make decisions about the distribution of those inputs across siblings. The fixed-effects model
controls for sample selection due to fertility and mortality selection. We are well aware that for
children individual characteristics (particularly in health) might not be fixed but rather develop
over time. Differencing might not therefore remove all the individual fixed effects. We
nevertheless perform the estimation as a comparison method with the OLS estimates; where the
health variable of the child at the different ages is regressed on a set of parental characteristics
(see part 3).
2.2.2. Siblings fixed-effects (for twins also)
We use differences in parental behaviors between births to estimate a so-called “sibling fixed-
effects” model. The sibling fixed-effect model is estimated by taking deviations of health from
the family mean. For this, we need data on health outcomes of siblings and parental behavior to
estimate the effects of parental behavior, the variance of health endowments and the variance in
measurement errors for each outcome. The sibling fixed-effects model requires that the
heterogeneity parameter is constant across births.
The reduced form health outcome of a child is:
ijjiji XXH ε++=

Where Hi is the child’s health measure, X ij are the k variables on individual I in household j
and X j are the k2 household variables (e.g. parental characteristics) and ij is the error term.
The error term is the sum of a household specific component (equal across siblings) and a person-
specific component. The person-specific component represents unobservable personal
characteristics such as health endowments.
ij �☺i ��ij
“The household-specific term reflects unobserved variation in the health environment of
households, the infant health technology and household preferences “(Pitt, Rosenzweig, 1990).
2.2.3. OLS for adoptees
3. Data
The National Child Development Study (NCDS) is a longitudinal study of 17,000 babies born in
Great Britain in the week of 3-9 March 1958. NCDS data are available for secondary analysis
from The Data Archive at the University of Essex. The study started as the “Perinatal Mortality
Survey (PMS)” and surveyed the economic and obstetric factors associated with stillbirth and
infant mortality. Since the first wave, cohort members have been traced on six other occasions to
monitor their physical, educational and social circumstances. The waves were carried out in 1965
(age 7), 1969 (age 11), 1974 (age 16), 1981 (age 23), 1991 (age 33) and 1999 (age 42). The first
three surveys were augmented with immigrants born in the same week, but no attempt to include
immigrants was made since 1974. In addition to the main sweeps, information about the public
examinations was obtained from the schools in 1978. For the birth survey, information was
gathered from the mother and the medical records. For the surveys during childhood and
adolescence, interviews were carried out with parents, teachers, and the school health service,
while ability tests were administered. The subsequent surveys included information on
employment and income, health and health behavior, citizenship and values, relationships,
parenting and housing, education and training of the respondents.

3.1 Prenatal care and birth
The PMS contains some information on the birth mother during the pregnancy with respect to her
health input utilization, problems experienced during the pregnancy and background. The main
measures of health at birth included are birthweight (in ounces), birthweight by gestational age
and sex (in standard deviations) and an indicator of whether the child experienced an illness in the
first week of life. Background information that might be related to child’s health include mother’s
age, height and pre-pregnancy weight (in bands), mother’s marital status, father’s age and social
class (based on occupation), grandparent’s social class. Some information on maternal behavior
during the pregnancy is also available. Prenatal care has been found in a number of studies
(Rosenzweig & Schultz, 1982, Frank et al, 1992, Brown et al., 2001) to be relevant for birth
outcomes and child health at birth. We therefore use the information on delay in seeking prenatal
care (first week of mother’s visit) and on the number of prenatal care visits of the mother.
Maternal smoking during the pregnancy, an indicator of whether the mother was working during
the pregnancy and in which week she stopped are also available. There is also information on
multiple births and the NCDS contains a small sample of 438 twins. Previous obstetric records
show whether the mother has had previous births, stillbirths and ectopic abortions. Finally,
problems during the pregnancy such as pleclampsia, bleeding, toxemia and low hemoglobin
levels are available.
3.2 Child health
During childhood and adolescence parents are asked questions about their children’s record of
illnesses, psychological problems, accidents and hospitalizations. A medical examination is
performed by a physician who records the child’s specific medical problems. Using this
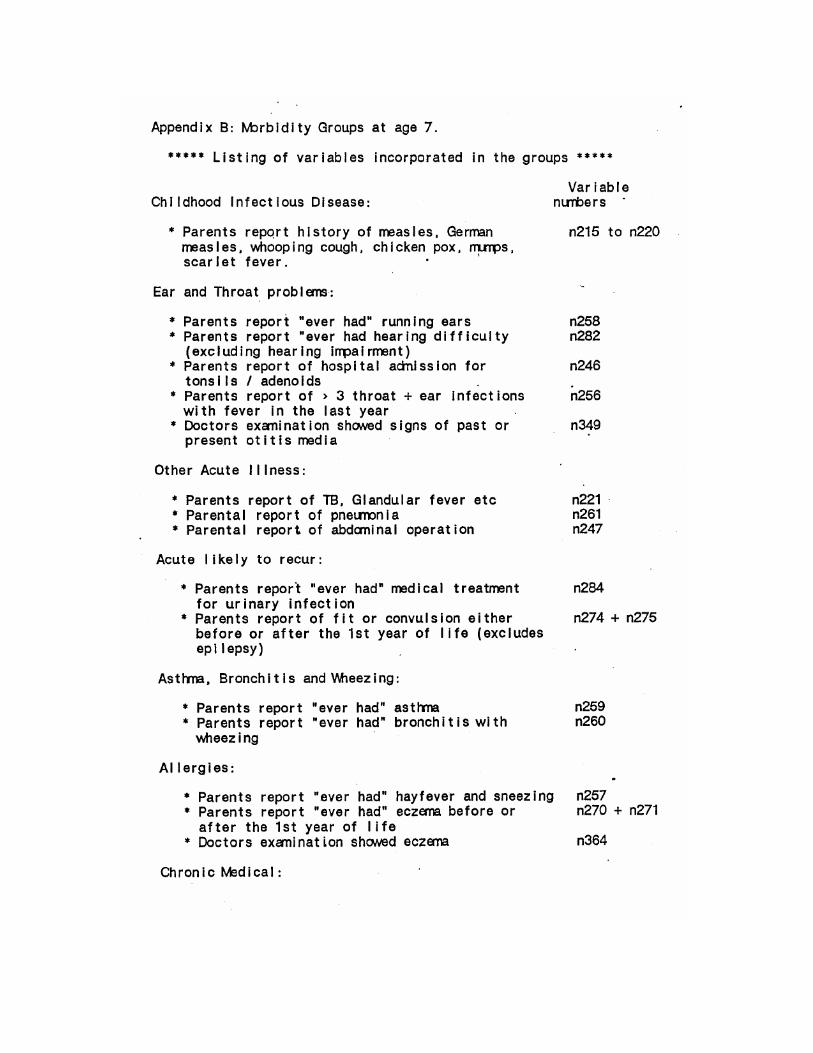
information we develop several measures of child’s health. The first one is a measure of
morbidity based on the number of conditions the child has experienced at ages 7, 11 and 16. The
conditions are categorized under 13 groups (see Power & Pecham and Appendix, 1987) and the
group of infectious diseases is excluded from the morbidity index as most children experience
them. The prevalence of conditions is as follows:
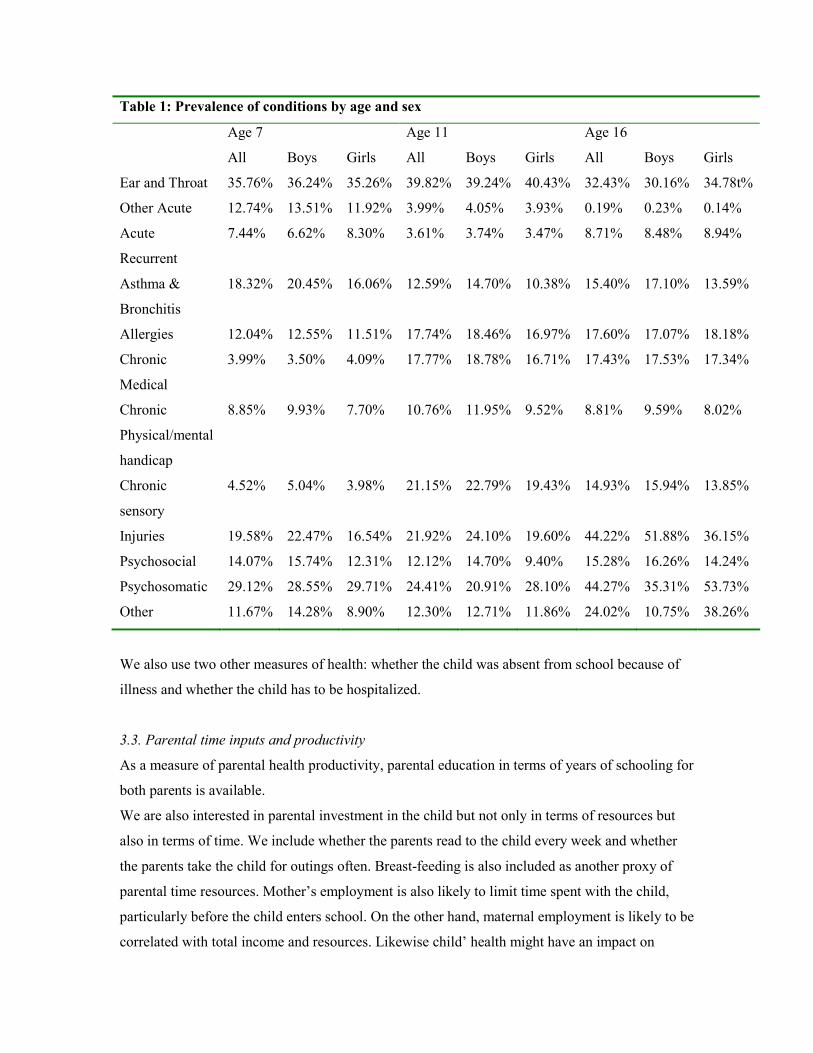
Table 1: Prevalence of conditions by age and sex
Age 7 Age 11 Age 16
All Boys Girls All Boys Girls All Boys Girls
Ear and Throat 35.76% 36.24% 35.26% 39.82% 39.24% 40.43% 32.43% 30.16% 34.78t%
Other Acute 12.74% 13.51% 11.92% 3.99% 4.05% 3.93% 0.19% 0.23% 0.14%
Acute
Recurrent
7.44% 6.62% 8.30% 3.61% 3.74% 3.47% 8.71% 8.48% 8.94%
Asthma &
Bronchitis
18.32% 20.45% 16.06% 12.59% 14.70% 10.38% 15.40% 17.10% 13.59%
Allergies 12.04% 12.55% 11.51% 17.74% 18.46% 16.97% 17.60% 17.07% 18.18%
Chronic
Medical
3.99% 3.50% 4.09% 17.77% 18.78% 16.71% 17.43% 17.53% 17.34%
Chronic
Physical/mental
handicap
8.85% 9.93% 7.70% 10.76% 11.95% 9.52% 8.81% 9.59% 8.02%
Chronic
sensory
4.52% 5.04% 3.98% 21.15% 22.79% 19.43% 14.93% 15.94% 13.85%
Injuries 19.58% 22.47% 16.54% 21.92% 24.10% 19.60% 44.22% 51.88% 36.15%
Psychosocial 14.07% 15.74% 12.31% 12.12% 14.70% 9.40% 15.28% 16.26% 14.24%
Psychosomatic 29.12% 28.55% 29.71% 24.41% 20.91% 28.10% 44.27% 35.31% 53.73%
Other 11.67% 14.28% 8.90% 12.30% 12.71% 11.86% 24.02% 10.75% 38.26%
We also use two other measures of health: whether the child was absent from school because of
illness and whether the child has to be hospitalized.
3.3. Parental time inputs and productivity
As a measure of parental health productivity, parental education in terms of years of schooling for
both parents is available.
We are also interested in parental investment in the child but not only in terms of resources but
also in terms of time. We include whether the parents read to the child every week and whether
the parents take the child for outings often. Breast-feeding is also included as another proxy of
parental time resources. Mother’s employment is also likely to limit time spent with the child,
particularly before the child enters school. On the other hand, maternal employment is likely to be
correlated with total income and resources. Likewise child’ health might have an impact on

maternal decision on whether to work or not and on mother’s labor supply.
Based on teacher’s assessment, there is some information on the level of interested of parents in
their child’s schooling. Another indication of investment is the information on parental wishes
about their offspring continuing their education.
In wave 3, parents report their cigarette consumption and this can also be a proxy of parental
attitudes towards health and health habits that can be transmitted.
3.4 Parental health
The NCDS records parental weight and height when the child is age 11. This information can be
transformed to obtain the Body mass Index (BMI) which is a measure of obesity. In addition,
chronic conditions for the father, mother and/or relatives is recorded in all waves during
childhood and adolescence. At age 7, the information is quite limited and it is only known
whether a relative had a congenital heart condition, diabetes or convulsions. At ages 11, the father
and the mother’s chronic condition is categorized according to the following groups:
Table 2: Parental chronic conditions
Age 11 Age 16
Mother Father Mother Father
Respiratory 12.55% 20.20% 14.86% 22.17%
Psychiatry 26.16% 11.94% 25.00% 10.06%
Subnormality 1.58% 0.20% 0.43%
Urogenital 9.28% 2.29% 3.43% 2.29%
Alimentary 6.33% 12.54% 5.57% 7.54%
Locomotory 11.71% 16.42% 11.57% 19.20%
Neurology 3.80% 5.17% 5.57% 4.91%
Infectious 0.84% 0.80% 1.14% 1.83%
Special 1.58% 2.495 3.57% 3.20%
Cardiovascular 14.56% 19.90% 12.14% 19.31%
Dermatological 1.58% 1.29% 1.43% 1.14%
Other 10.02% 6.77% 15.29% 8.34%
948 1005 700 875

Finally, when the cohort members are adults they are asked in wave 4 and 5 whether the father
and the mother are still alive.
3.5 Parental income
The information collected by the NCDS only contains one measure of family income when the
child is 16. This might not be a reflection of living standards earlier in childhood nor of persistent
poverty problems. For this reason, the data holders developed a measure of permanent income.
Using grouped dependent variable techniques and variables representing parental education,
occupation, age and region, they predicted permanent income. Because of the estimation
technique, this variable is therefore correlated with other variables of interest. In addition, there
are many missing cases because the following cases are excluded from the analysis: cases where
occupational class is missing and cases where the children are not living with either natural parent
at age 16.
We therefore experiment with several measures of income including whether the family had
serious financial difficulties, whether the child received free meals at school, and parental
socioeconomic status based on occupation.
3.6 Background characteristics
The dataset contains other additional information on the children’s background such as the sex,
number of siblings, birth order, region, and household composition, that is, whether the child had
one parental figure or not and which one (natural, adopted, foster, etc).
The NCDS includes a reduced number of children who have been adopted (around 200).
Adoption is assumed to be random and children are placed with the adoption family 3 months
after birth. This removes the potential bias that parents in better health select those children in
better health for adoption. The NCDS adoptees are illegitimate children who are randomly placed
for adoption. Because of this, we do have some information on both the birth mother and the
adoptive parents. Because of the nature of the data we have some information on the birth mother
and the adoptive parents, which is unusual and not often found in data.
3.7 Cohort member’s children
In addition, wave 5 includes information about the cohort members’ children. The sample
consists of 4207 children, of which 23 are adopted. This includes some information about the
pregnancy and the delivery (smoking, problems during labor, etc). The mother also reports
information on the child’s infectious illnesses (measles, chicken pox), hearing problems, speech

difficulties, as well as other conditions such as asthma, epilepsy, hay fever, eczema, migraine,
diabetes and behavioral problems. Two assessment tests are given to the children to evaluate their
reading and math abilities (Ppvt reading test and piat math test). They are nevertheless not the
same as those previously administered to the cohort members. There is only information at one
point in time for those children and it is done at a young age. In addition, there are issues of
selection since older children will be typically those from teenage mothers. The data would only
allow us to look at the correlation between parental illnesses and children’s illnesses but we won’t
be able to disentangle the genetic part and the environmental part. Because of the children’s age
we cannot look at variables such as years of education and labor market outcomes correlation
with the parents’.
4. Results
4.1 Prenatal factors and health at birth
Prenatal care shows to have a positive impact on the baby’s weight. Maternal smoking is
associated with lower birthweight. High socio-economic status or higher income appears to have
a positive impact on birthweight. Mother’s own physical characteristics such as height and weight
are as expected highly correlated with the baby’s own weight. Mother schooling appears to
increase birthweight only when gestation time is not taken into account. Problems during the
pregnancy such as bleeding and toxemia have a negative impact on health at birth. Obstetric
history also appears to matter as indicated by the negative effect pas stillbirths and a too short
interval between this birth and the previous one, while having more children increases the weight
of the subsequent children. Nevertheless these results do not take into account the potential
endogeneity of variables such as prenatal care choice, smoking, etc.
Table 3: Health at birth and maternal care
Estimated birthweight Log of estimated birthweight
number of prenatal
care visits
0.617 0.164 0.446 0.006 0.001 0.004
(19.46)** (5.48)** (11.34)** (20.27)** (4.57)** (11.59)**
Parity 1.331 1.100 1.180 0.011 0.009 0.010
(9.01)** (8.01)** (6.44)** (7.64)** (6.67)** (5.97)**
sex of child -4.658 -4.950 -4.931 -0.041 -0.044 -0.043
(14.66)** (17.08)** (12.67)** (12.71)** (15.75)** (12.32)**
mother's age -0.190 -0.047 -0.080 -0.002 -0.000 -0.001
(5.01)** (1.35) (1.70) (4.77)** (0.77) (1.62)

Mother smoking –
medium
-4.098 -3.330 -4.049 -0.038 -0.029 -0.035
(9.06)** (8.05)** (7.21)** (8.32)** (7.37)** (7.09)**
Mother smoking –
heavy
-6.150 -5.569 -6.220 -0.056 -0.050 -0.056
(12.20)** (12.08)** (9.91)** (11.08)** (11.13)** (9.93)**
high ses 1.467 1.257 0.014 0.011
(3.66)** (3.47)** (3.40)** (3.12)**
Permanent income 4.757 0.044
(4.14)** (4.28)**
Week of 1s mother
prenatal visit- 1st-
3rd
-13.198 -8.277 0.954 -0.162 -0.108 0.009
(4.17)** (2.91)** (0.23) (5.08)** (3.93)** (0.25)
Week of 1s mother
prenatal visit- 36
week
8.372 3.868 6.702 0.093 0.045 0.064
(3.75)** (1.78) (2.12)* (4.11)** (2.13)* (2.26)*
Mother’s weight
in stones >=15st
12.814 10.271 10.143 0.107 0.082 0.083
(5.54)** (4.69)** (3.46)** (4.60)** (3.86)** (3.17)**
Mother’s weight
in stones: under 7
-7.355 -6.749 -6.320 -0.075 -0.068 -0.058
(6.12)** (6.14)** (4.05)** (6.16)** (6.37)** (4.14)**
past stillbirths and
neonatal deaths
-4.267 -2.454 -1.758 -0.048 -0.028 -0.016
(7.03)** (4.42)** (2.28)* (7.93)** (5.14)** (2.32)*
Bleeding -2.250 -1.371 -0.382 -0.027 -0.017 -0.003
(6.28)** (4.21)** (0.86) (7.50)** (5.42)** (0.77)
Toxaemia -2.127 -1.839 -2.108 -0.023 -0.019 -0.021
(6.23)** (5.93)** (5.04)** (6.65)** (6.44)** (5.57)**
Interval between
births <=1 year
-4.730 -0.627 -2.058 -0.053 -0.010 -0.020
(4.39)** (0.61) (1.50) (4.89)** (0.98) (1.61)
Scotland 2.313 2.807 2.325 0.019 0.024 0.020
(3.87)** (5.12)** (3.20)** (3.11)** (4.46)** (3.05)**
Mother stayed in
school after
minimum age
1.333 0.470 0.687 0.015 0.006 0.007
(3.40)** (1.33) (1.42) (3.82)** (1.61) (1.67)
height of mum in
inches
0.776 0.826 0.787 0.006 0.007 0.007
(10.85)** (12.67)** (8.93)** (8.72)** (10.70)** (8.36)**
Gestationalperiod
in days
0.668 0.008 4.157
(62.12)** (73.36)** (58.08)**
Constant 75.256 -115.243 48.340 4.421 2.255 7497
(15.88)** (21.75)** (6.02)** (92.62)** (44.03)** 0.137
Observations 13797 12685 7497 13797 12685
R-squared 0.136 0.340 0.142 0.121 0.385

4.2 Child health and parental income
Our primary estimates for child health are presented in Table 4. Here we used the number of
chronic illnesses at 3 different ages (corresponding to the 3 waves) as a measure of health. We
also include another measure of health available at ages 11 and 16: whether the child was absent
from school due to illness. The estimates for chronic illnesses are obtained using OLS while those
for absence from school are obtained through a probit. We observe that the coefficient for the log
of permanent parental income is negative and significant for all measures except at age 7. The
size of the coefficient also increases with age, indicating that the income gradient becomes more
pronounced with age, which is in line with the results found by Case et al. (2002) using US data
but not with Currie et al. (2005) using British data. Compared to Case et al. (2002) our coefficient
for income is smaller at ages 7 and 11 while being larger at age 16. The inclusion of additional
controls such as family size and sex does not change primarily the results1.
1 We do not include additional controls such as the age of the parents, the absence of the father or mother, parental education, occupation or region because the permanent income was predicted using those variables. For all tables in
this section, we include only the relevant variables and/or those significant at least the 5% level.
Table 4: Health status and family income
Number of chronic illness School absences due to illness
Age 7 Age 11 Age 16 Age 11 Age 16
predicted
permanent
parental income
-0.119 -0.211 -0.493 -0.432 -1.169
(1.43) (2.26)* (5.02)** (5.90)** (11.34)**
Constant 2.388 3.170 5.056 1.866 4.580
(5.71)** (6.77)** (10.28)** (5.09)** (8.93)**
Observations 8478 8050 7757 8890 8890
R-squared 0.000 0.001 0.003
Controls for Sex and Family size
predicted
permanent
parental income
-0.155 -0.228 -0.436 -0.440 -1.060
(1.82) (2.39)* (4.41)** (5.88)** (10.09)**
Sex of child -0.182 -0.137 0.316 0.150 0.217
(5.87)** (3.93)** (7.12)** (5.52)** (5.94)**
Constant 2.905 3.501 4.237 1.679 3.540
(6.65)** (7.10)** (8.44)** (4.33)** (6.71)**
Observations 8466 8039 7743 8866 8870
R-squared 0.005 0.003 0.015
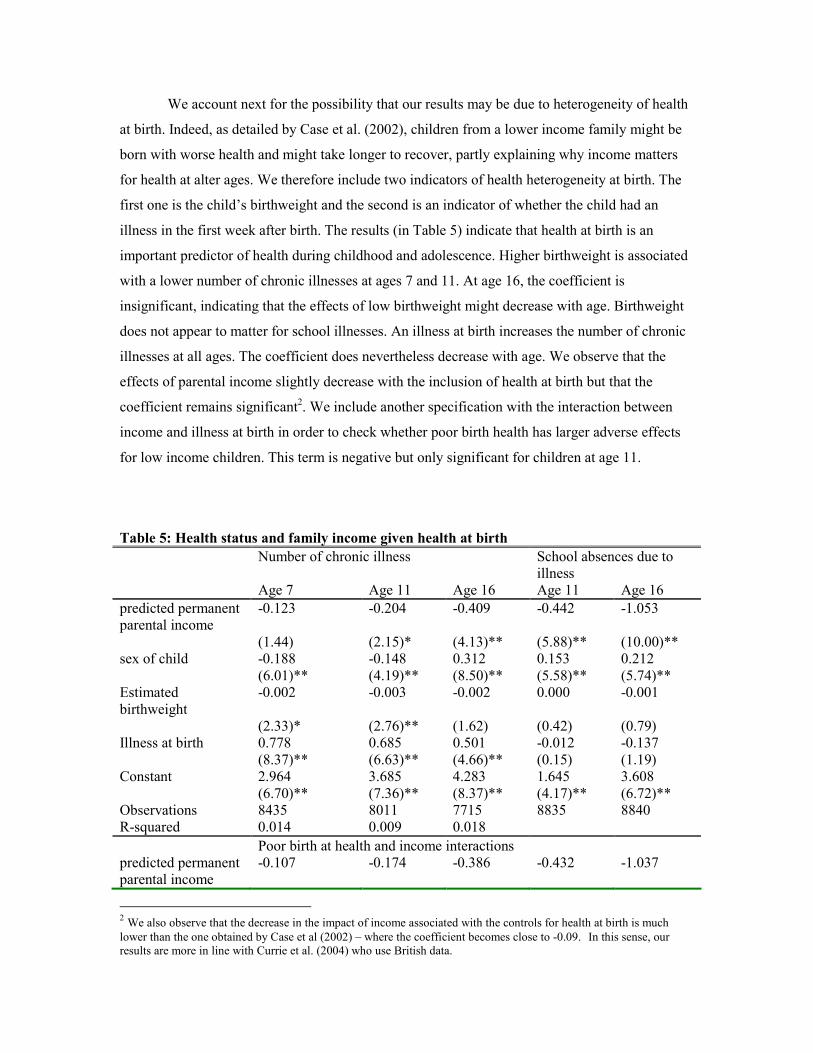
We account next for the possibility that our results may be due to heterogeneity of health
at birth. Indeed, as detailed by Case et al. (2002), children from a lower income family might be
born with worse health and might take longer to recover, partly explaining why income matters
for health at alter ages. We therefore include two indicators of health heterogeneity at birth. The
first one is the child’s birthweight and the second is an indicator of whether the child had an
illness in the first week after birth. The results (in Table 5) indicate that health at birth is an
important predictor of health during childhood and adolescence. Higher birthweight is associated
with a lower number of chronic illnesses at ages 7 and 11. At age 16, the coefficient is
insignificant, indicating that the effects of low birthweight might decrease with age. Birthweight
does not appear to matter for school illnesses. An illness at birth increases the number of chronic
illnesses at all ages. The coefficient does nevertheless decrease with age. We observe that the
effects of parental income slightly decrease with the inclusion of health at birth but that the
coefficient remains significant2. We include another specification with the interaction between
income and illness at birth in order to check whether poor birth health has larger adverse effects
for low income children. This term is negative but only significant for children at age 11.
Table 5: Health status and family income given health at birth
Number of chronic illness School absences due to
illness
Age 7 Age 11 Age 16 Age 11 Age 16
predicted permanent
parental income
-0.123 -0.204 -0.409 -0.442 -1.053
(1.44) (2.15)* (4.13)** (5.88)** (10.00)**
sex of child -0.188 -0.148 0.312 0.153 0.212
(6.01)** (4.19)** (8.50)** (5.58)** (5.74)**
Estimated
birthweight
-0.002 -0.003 -0.002 0.000 -0.001
(2.33)* (2.76)** (1.62) (0.42) (0.79)
Illness at birth 0.778 0.685 0.501 -0.012 -0.137
(8.37)** (6.63)** (4.66)** (0.15) (1.19)
Constant 2.964 3.685 4.283 1.645 3.608
(6.70)** (7.36)** (8.37)** (4.17)** (6.72)**
Observations 8435 8011 7715 8835 8840
R-squared 0.014 0.009 0.018
Poor birth at health and income interactions
predicted permanent
parental income
-0.107 -0.174 -0.386 -0.432 -1.037
2 We also observe that the decrease in the impact of income associated with the controls for health at birth is much lower than the one obtained by Case et al (2002) – where the coefficient becomes close to -0.09. In this sense, our results are more in line with Currie et al. (2004) who use British data.
(1.24) (1.81) (3.86)** (5.68)** (9.75)**
sex of child -0.187 -0.146 0.313 0.154 0.213
(5.98)** (4.14)** (8.53)** (5.60)** (5.75)**
Estimated
birthweight
-0.002 -0.003 -0.002 0.000 -0.001
(2.33)* (2.76)** (1.63) (0.42) (0.81)
Illness at birth 3.975 6.602 5.427 2.002 3.484
(1.51) (2.24)* (1.69) (0.84) (0.96)
Illness at
birth*family income
-0.641 -1.185 -0.987 -0.404 -0.733
(1.21) (2.01)* (1.53) (0.85) (1.00)
Constant 2.883 3.533 4.166 1.595 3.531
(6.45)** (6.98)** (8.05)** (4.00)** (6.51)**
Observations 8435 8011 7715 8835 8840
R-squared 0.014 0.010 0.018
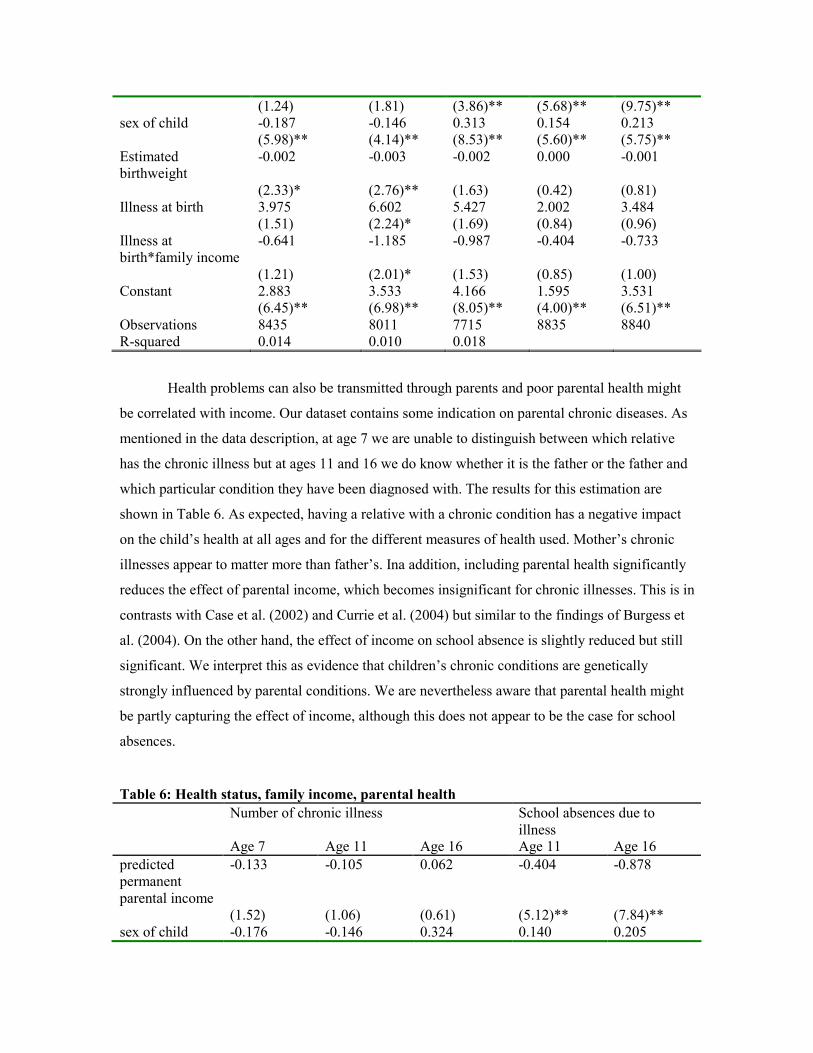
Health problems can also be transmitted through parents and poor parental health might
be correlated with income. Our dataset contains some indication on parental chronic diseases. As
mentioned in the data description, at age 7 we are unable to distinguish between which relative
has the chronic illness but at ages 11 and 16 we do know whether it is the father or the father and
which particular condition they have been diagnosed with. The results for this estimation are
shown in Table 6. As expected, having a relative with a chronic condition has a negative impact
on the child’s health at all ages and for the different measures of health used. Mother’s chronic
illnesses appear to matter more than father’s. Ina addition, including parental health significantly
reduces the effect of parental income, which becomes insignificant for chronic illnesses. This is in
contrasts with Case et al. (2002) and Currie et al. (2004) but similar to the findings of Burgess et
al. (2004). On the other hand, the effect of income on school absence is slightly reduced but still
significant. We interpret this as evidence that children’s chronic conditions are genetically
strongly influenced by parental conditions. We are nevertheless aware that parental health might
be partly capturing the effect of income, although this does not appear to be the case for school
absences.
Table 6: Health status, family income, parental health
Number of chronic illness School absences due to
illness Age 7 Age 11 Age 16 Age 11 Age 16
predicted
permanent
parental income
-0.133 -0.105 0.062 -0.404 -0.878
(1.52) (1.06) (0.61) (5.12)** (7.84)**
sex of child -0.176 -0.146 0.324 0.140 0.205

(5.57)** (4.09)** (9.02)** (5.00)** (5.39)**
Family illnesses 0.356
(7.27)**
Father chronic
illness
0.357 1.034 0.163 0.203
(4.95)** (15.09)** (2.91)** (3.14)**
Mother chronic
illness
0.577 1.327 0.208 0.323
(7.62)** (16.71)** (3.52)** (4.49)**
Bmi father -0.022 -0.019 -0.007 0.003 -0.003
(4.26)** (3.18)** (1.17) (0.59) (0.52)
Bmi mother 0.007 0.009 0.006 0.009 0.017
(1.77) (2.02)* (1.28) (2.53)* (3.74)**
Constant 3.141 3.124 1.597 1.245 2.268
(6.52)** (5.64)** (2.88)** (2.84)** (3.78)**
Observations 7963 7553 7262 8328 8320
R-squared 0.014 0.016 0.063
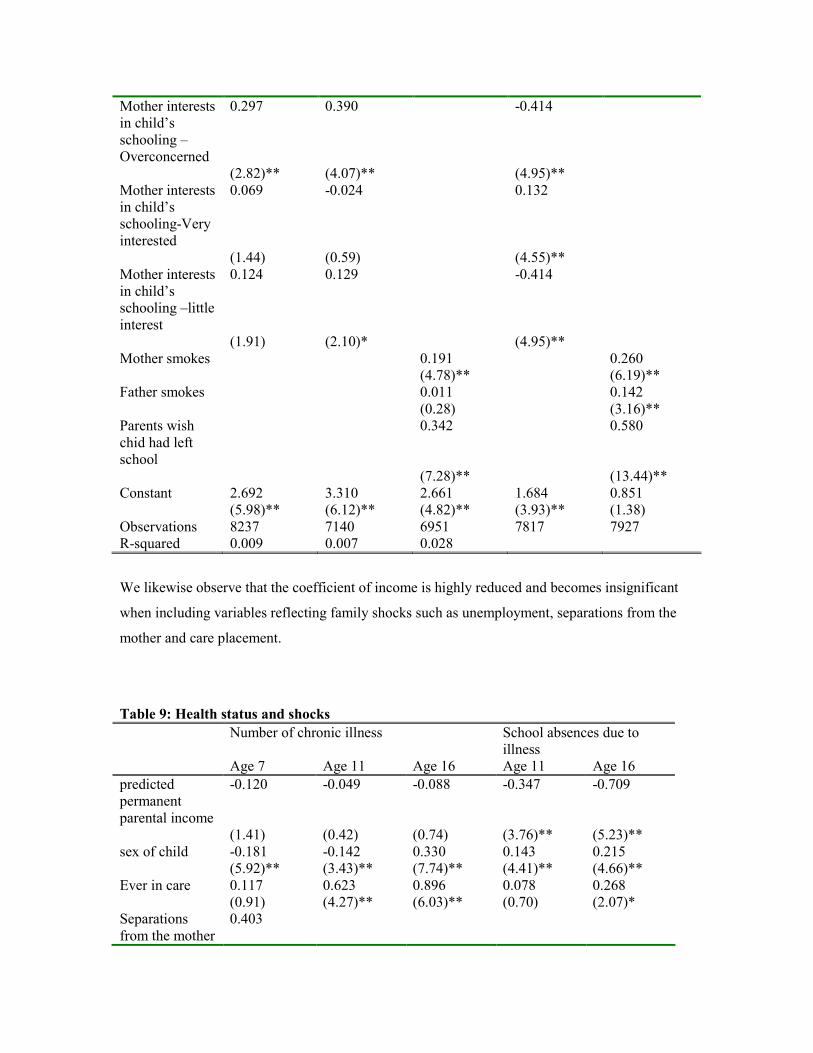
We are also interested in the effects of parental time and parental health behavior on
child’s health. We present the results on Table 7. We observe again that adding parental behavior
does reduce the impact of income on health and that the gradient disappears for the number of
chronic illnesses. Income does still matter for school absences due to illness. Father’s outing with
the child significantly reduces the number of chronic illnesses at age 7 but not at 11. Parental over
concern with schooling as assessed by the teacher appears to be positively correlated with the
number of chronic illnesses. Surprisingly children whose parents were over concerned with their
education and those whose parents showed little interest were less likely to miss school due to
illnesses. Parental wishes for lower education are associated with lower child’s health. Maternal
smoking is also significantly correlated with poor health.
Table 7: Health status, family income, parental behavior
Number of chronic illness School absences due to illness
Age 7 Age 11 Age 16 Age 11 Age 16
Predicted
permanent
parental income
-0.108 -0.187 -0.160 -0.414 -0.608
(1.21) (1.77) (1.49) (4.95)** (5.02)**
sex of child -0.191 -0.113 0.333 0.132 0.240
(6.10)** (3.06)** (8.74)** (4.55)** (5.89)**
Mother outings
with the child
0.090 -0.042 -0.414
(1.68) (0.67) (4.95)**
Father outings
with the child
-0.144 -0.083 0.132
(3.52)** (1.34) (4.55)**
Mother interests
in child’s
schooling –
Overconcerned
0.297 0.390 -0.414
(2.82)** (4.07)** (4.95)**
Mother interests
in child’s
schooling-Very
interested
0.069 -0.024 0.132
(1.44) (0.59) (4.55)**
Mother interests
in child’s
schooling –little
interest
0.124 0.129 -0.414
(1.91) (2.10)* (4.95)**
Mother smokes 0.191 0.260
(4.78)** (6.19)**
Father smokes 0.011 0.142
(0.28) (3.16)**
Parents wish
chid had left
school
0.342 0.580
(7.28)** (13.44)**
Constant 2.692 3.310 2.661 1.684 0.851
(5.98)** (6.12)** (4.82)** (3.93)** (1.38)
Observations 8237 7140 6951 7817 7927
R-squared 0.009 0.007 0.028
We likewise observe that the coefficient of income is highly reduced and becomes insignificant
when including variables reflecting family shocks such as unemployment, separations from the
mother and care placement.
Table 9: Health status and shocks
Number of chronic illness School absences due to
illness
Age 7 Age 11 Age 16 Age 11 Age 16
predicted
permanent
parental income
-0.120 -0.049 -0.088 -0.347 -0.709
(1.41) (0.42) (0.74) (3.76)** (5.23)**
sex of child -0.181 -0.142 0.330 0.143 0.215
(5.92)** (3.43)** (7.74)** (4.41)** (4.66)**
Ever in care 0.117 0.623 0.896 0.078 0.268
(0.91) (4.27)** (6.03)** (0.70) (2.07)*
Separations
from the mother
0.403

for more than a
week
(12.94)**
Domestic
problems
0.593
(7.85)**
Father
unemployed
0.022
(0.21)
Number of
Weeks dad off
work due to
illness
0.013 0.018 0.006 0.013
(4.71)** (6.05)** (3.06)** (5.21)**
Number of
Weeks dad off
work due to
unemployment
0.008 0.001 0.007 0.011
(2.06)* (0.26) (2.41)* (3.32)**
Number of
Weeks dad off
work due to
other causes
0.027 -0.002
(2.04)* (0.23)
Constant 2.579 2.608 2.378 1.251 1.676
(5.93)** (4.35)** (3.93)** (2.63)** (2.44)*
Observations 8425 5660 5498 6201 6223
R-squared 0.034 0.012 0.029
Finally, we compare different specifications for parental wealth: parental income, father’s
socioeconomic status (SES) at birth of the child and whether the family experienced financial
difficulties3. After inclusion of all the controls, neither parental income nor SES remain
significant. Financial difficulties however are significant at all ages and have a much higher
coefficient.
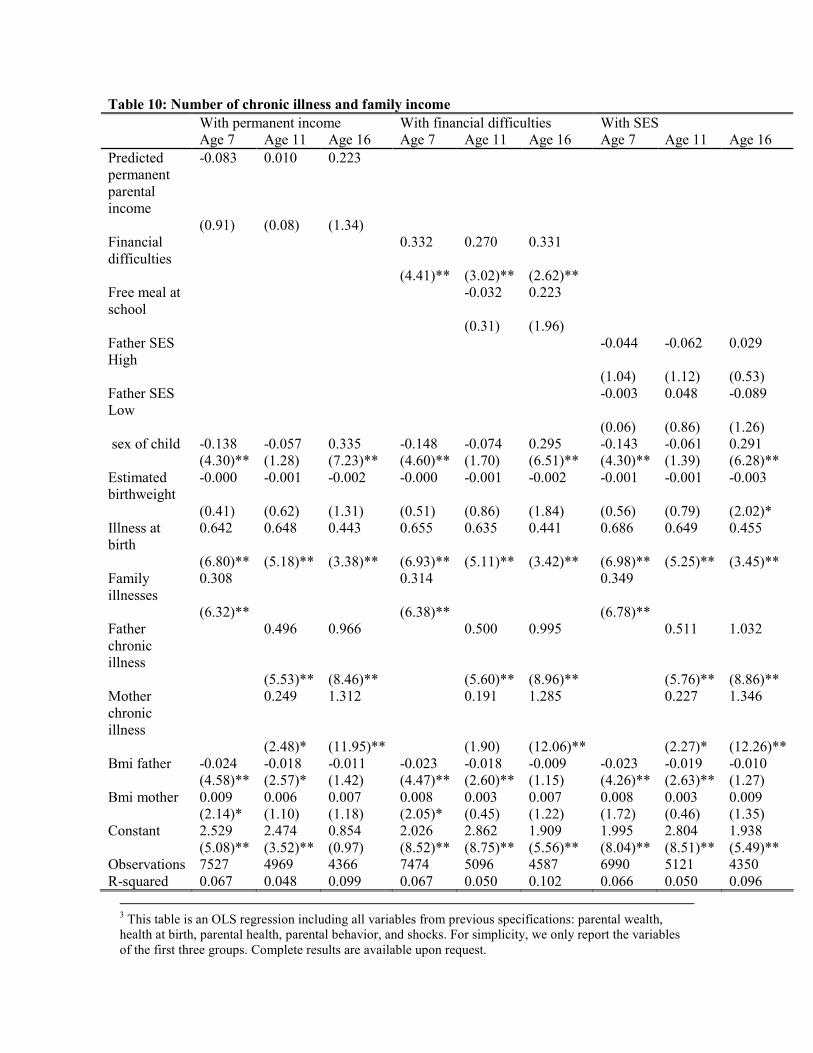
Table 10: Number of chronic illness and family income
With permanent income With financial difficulties With SES
Age 7 Age 11 Age 16 Age 7 Age 11 Age 16 Age 7 Age 11 Age 16
Predicted
permanent
parental
income
-0.083 0.010 0.223
(0.91) (0.08) (1.34)
Financial
difficulties
0.332 0.270 0.331
(4.41)** (3.02)** (2.62)**
Free meal at
school
-0.032 0.223
(0.31) (1.96)
Father SES
High
-0.044 -0.062 0.029
(1.04) (1.12) (0.53)
Father SES
Low
-0.003 0.048 -0.089
(0.06) (0.86) (1.26)
sex of child -0.138 -0.057 0.335 -0.148 -0.074 0.295 -0.143 -0.061 0.291
(4.30)** (1.28) (7.23)** (4.60)** (1.70) (6.51)** (4.30)** (1.39) (6.28)**
Estimated
birthweight
-0.000 -0.001 -0.002 -0.000 -0.001 -0.002 -0.001 -0.001 -0.003
(0.41) (0.62) (1.31) (0.51) (0.86) (1.84) (0.56) (0.79) (2.02)*
Illness at
birth
0.642 0.648 0.443 0.655 0.635 0.441 0.686 0.649 0.455
(6.80)** (5.18)** (3.38)** (6.93)** (5.11)** (3.42)** (6.98)** (5.25)** (3.45)**
Family
illnesses
0.308 0.314 0.349
(6.32)** (6.38)** (6.78)**
Father
chronic
illness
0.496 0.966 0.500 0.995 0.511 1.032
(5.53)** (8.46)** (5.60)** (8.96)** (5.76)** (8.86)**
Mother
chronic
illness
0.249 1.312 0.191 1.285 0.227 1.346
(2.48)* (11.95)** (1.90) (12.06)** (2.27)* (12.26)**
Bmi father -0.024 -0.018 -0.011 -0.023 -0.018 -0.009 -0.023 -0.019 -0.010
(4.58)** (2.57)* (1.42) (4.47)** (2.60)** (1.15) (4.26)** (2.63)** (1.27)
Bmi mother 0.009 0.006 0.007 0.008 0.003 0.007 0.008 0.003 0.009
(2.14)* (1.10) (1.18) (2.05)* (0.45) (1.22) (1.72) (0.46) (1.35)
Constant 2.529 2.474 0.854 2.026 2.862 1.909 1.995 2.804 1.938
(5.08)** (3.52)** (0.97) (8.52)** (8.75)** (5.56)** (8.04)** (8.51)** (5.49)**
Observations 7527 4969 4366 7474 5096 4587 6990 5121 4350
R-squared 0.067 0.048 0.099 0.067 0.050 0.102 0.066 0.050 0.096
3 This table is an OLS regression including all variables from previous specifications: parental wealth,
health at birth, parental health, parental behavior, and shocks. For simplicity, we only report the variables
of the first three groups. Complete results are available upon request.
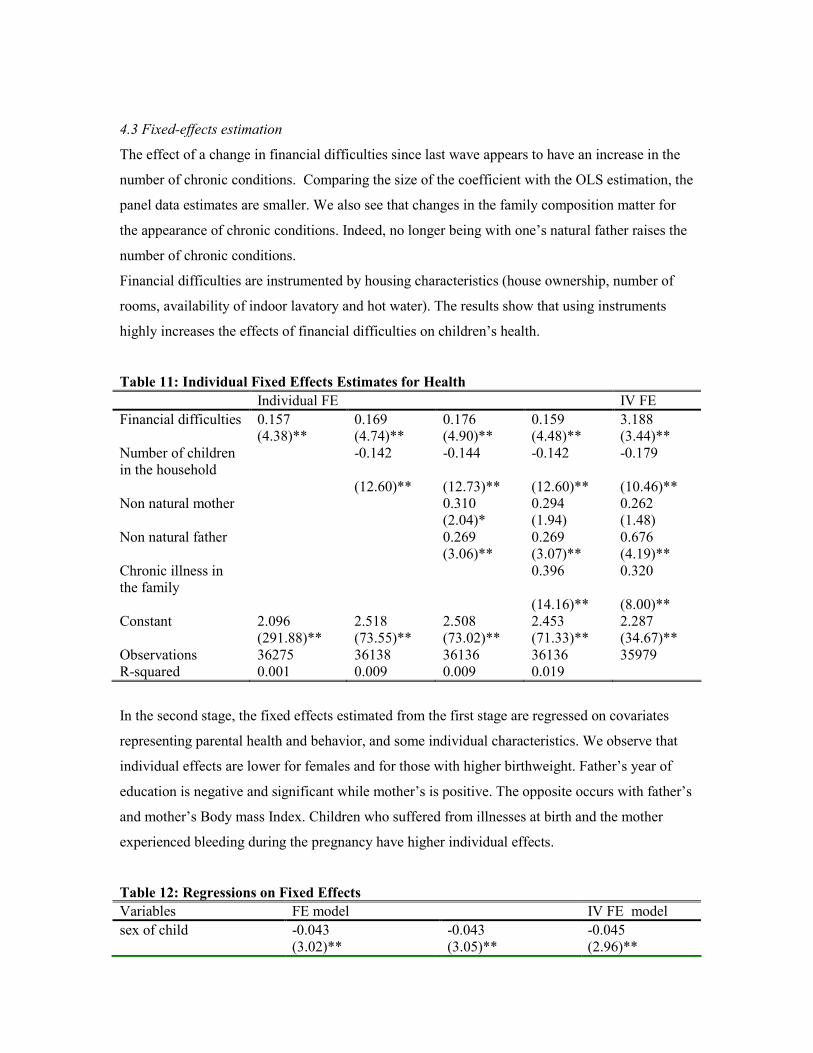
4.3 Fixed-effects estimation
The effect of a change in financial difficulties since last wave appears to have an increase in the
number of chronic conditions. Comparing the size of the coefficient with the OLS estimation, the
panel data estimates are smaller. We also see that changes in the family composition matter for
the appearance of chronic conditions. Indeed, no longer being with one’s natural father raises the
number of chronic conditions.
Financial difficulties are instrumented by housing characteristics (house ownership, number of
rooms, availability of indoor lavatory and hot water). The results show that using instruments
highly increases the effects of financial difficulties on children’s health.
Table 11: Individual Fixed Effects Estimates for Health
Individual FE IV FE
Financial difficulties 0.157 0.169 0.176 0.159 3.188 (4.38)** (4.74)** (4.90)** (4.48)** (3.44)**
Number of children
in the household
-0.142 -0.144 -0.142 -0.179
(12.60)** (12.73)** (12.60)** (10.46)**
Non natural mother 0.310 0.294 0.262
(2.04)* (1.94) (1.48)
Non natural father 0.269 0.269 0.676
(3.06)** (3.07)** (4.19)**
Chronic illness in
the family
0.396 0.320
(14.16)** (8.00)**
Constant 2.096 2.518 2.508 2.453 2.287
(291.88)** (73.55)** (73.02)** (71.33)** (34.67)**
Observations 36275 36138 36136 36136 35979
R-squared 0.001 0.009 0.009 0.019
In the second stage, the fixed effects estimated from the first stage are regressed on covariates
representing parental health and behavior, and some individual characteristics. We observe that
individual effects are lower for females and for those with higher birthweight. Father’s year of
education is negative and significant while mother’s is positive. The opposite occurs with father’s
and mother’s Body mass Index. Children who suffered from illnesses at birth and the mother
experienced bleeding during the pregnancy have higher individual effects.
Table 12: Regressions on Fixed Effects
Variables FE model IV FE model
sex of child -0.043 -0.043 -0.045
(3.02)** (3.05)** (2.96)**

Parity 0.028 0.028 -0.023
(5.76)** (5.81)** (4.41)**
Bleeding during
pregnancy
0.147 0.148 0.160
(9.37)** (9.45)** (9.52)**
Toxemia -0.066 -0.066 -0.045
(4.52)** (4.52)** (2.88)**
Illness at birth 0.612 0.612 0.674
(14.85)** (14.87)** (15.23)**
Estimated birthweight -0.002 -0.002 -0.001
(5.32)** (5.37)** (1.49)
Bmi father -0.012 -0.012 -0.009
(5.00)** (5.05)** (3.27)**
Bmi mother 0.016 0.016 0.011
(8.30)** (8.35)** (5.57)**
Father’s years of
education
-0.019 -0.019 -0.001
(3.12)** (3.16)** (0.15)
Mother’s years of
education
0.020 0.019 0.037
(2.81)** (2.77)** (4.90)**
Family illnesses 0.422
(20.00)**
Breastfed 0.069 0.067 0.093
(4.53)** (4.46)** (5.72)**
Maternal smoking during
pregnancy
0.135 0.136 0.043
(8.92)** (9.03)** (2.67)**
bsag total score 0.014 0.014 0.006
(16.35)** (16.27)** (6.89)**
Constant -0.020 0.042 -0.314
(0.18) (0.38) (2.66)**
Observations 32102 32102 31973
R-squared 0.052 0.038 0.029
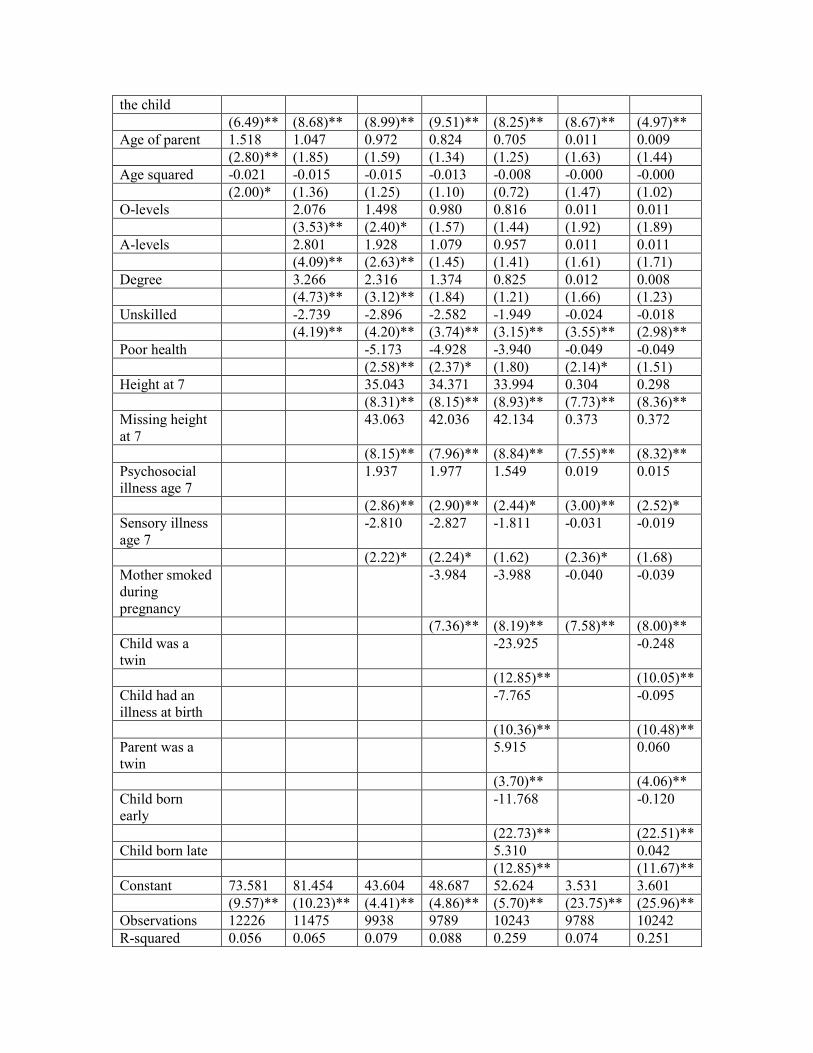
4.4 Cohort members and their children
Table 13: Regression of children’s Birthweight on parental birthweight and other parental
characteristics
With Birthweight With log of BW
Sex -10.238 -11.064 -11.493 -11.837 -7.169 -0.308 -0.172
(2.90)** (3.13)** (3.15)** (3.16)** (2.05)* (2.19)* (1.29)
Birthweight 0.148 0.140 0.122 0.124 0.123 0.145 0.141
(6.05)** (5.89)** (4.92)** (4.78)** (4.95)** (6.34)** (6.82)**
Sex*BW 0.099 0.105 0.108 0.106 0.075 0.066 0.040
(3.36)** (3.58)** (3.56)** (3.41)** (2.59)** (2.25)* (1.43)
Sex of the child -1.123 -1.380 -1.573 -1.460 -2.006 -0.011 -0.017
(2.68)** (3.22)** (3.43)** (3.19)** (4.78)** (2.48)* (4.05)**
Birth order of 1.717 2.375 2.687 2.920 2.394 0.025 0.018
the child
(6.49)** (8.68)** (8.99)** (9.51)** (8.25)** (8.67)** (4.97)**
Age of parent 1.518 1.047 0.972 0.824 0.705 0.011 0.009
(2.80)** (1.85) (1.59) (1.34) (1.25) (1.63) (1.44)
Age squared -0.021 -0.015 -0.015 -0.013 -0.008 -0.000 -0.000
(2.00)* (1.36) (1.25) (1.10) (0.72) (1.47) (1.02)
O-levels 2.076 1.498 0.980 0.816 0.011 0.011
(3.53)** (2.40)* (1.57) (1.44) (1.92) (1.89)
A-levels 2.801 1.928 1.079 0.957 0.011 0.011
(4.09)** (2.63)** (1.45) (1.41) (1.61) (1.71)
Degree 3.266 2.316 1.374 0.825 0.012 0.008
(4.73)** (3.12)** (1.84) (1.21) (1.66) (1.23)
Unskilled -2.739 -2.896 -2.582 -1.949 -0.024 -0.018
(4.19)** (4.20)** (3.74)** (3.15)** (3.55)** (2.98)**
Poor health -5.173 -4.928 -3.940 -0.049 -0.049
(2.58)** (2.37)* (1.80) (2.14)* (1.51)
Height at 7 35.043 34.371 33.994 0.304 0.298
(8.31)** (8.15)** (8.93)** (7.73)** (8.36)**
Missing height
at 7
43.063 42.036 42.134 0.373 0.372
(8.15)** (7.96)** (8.84)** (7.55)** (8.32)**
Psychosocial
illness age 7
1.937 1.977 1.549 0.019 0.015
(2.86)** (2.90)** (2.44)* (3.00)** (2.52)*
Sensory illness
age 7
-2.810 -2.827 -1.811 -0.031 -0.019
(2.22)* (2.24)* (1.62) (2.36)* (1.68)
Mother smoked
during
pregnancy
-3.984 -3.988 -0.040 -0.039
(7.36)** (8.19)** (7.58)** (8.00)**
Child was a
twin
-23.925 -0.248
(12.85)** (10.05)**
Child had an
illness at birth
-7.765 -0.095
(10.36)** (10.48)**
Parent was a
twin
5.915 0.060
(3.70)** (4.06)**
Child born
early
-11.768 -0.120
(22.73)** (22.51)**
Child born late 5.310 0.042
(12.85)** (11.67)**
Constant 73.581 81.454 43.604 48.687 52.624 3.531 3.601
(9.57)** (10.23)** (4.41)** (4.86)** (5.70)** (23.75)** (25.96)**
Observations 12226 11475 9938 9789 10243 9788 10242
R-squared 0.056 0.065 0.079 0.088 0.259 0.074 0.251

4.5 Children’s health by household composition
Table 13: Health status, family income, type
Number of chronic illness at age
7
Number of chronic illness at age
11
Number of chronic illness at age
16
Singletons Twins Adoptees Singletons Twins Adoptees Singletons Twins Adoptees
Estimated
birthweight
-0.003 -0.012 0.002 -0.004 -0.021 -0.000 -0.002 -0.009 0.005
(4.91)** (2.51)* (0.36) (4.42)** (3.20)** (0.00) (2.50)* (1.30) (0.58)
sex of child -0.242 0.035 -0.585 -0.198 -0.040 -0.410 0.278 0.199 -0.231
(9.67)** (0.21) (2.65)** (6.72)** (0.18) (1.48) (8.25)** (0.83) (0.75)
Constant 2.546 2.744 2.365 2.822 4.051 2.837 2.462 3.059 2.446
(26.82)** (5.04)** (2.96)** (25.27)** (5.60)** (2.68)** (19.06)** (3.98)** (2.20)*
Observations 13348 310 170 11415 254 134 9280 193 107
R-squared 0.008 0.021 0.042 0.005 0.039 0.017 0.009 0.014 0.010


References
Benzeval M, Judge K. Income and Health: The Time Dimension, Social Science and Medecine,
2001; 52: 1371-1390.
Burgess S, Propper C, Rigg J, the ALSPAC Study Team. The Impact of Low-Income on Child
Health: Evidence from a Birth Cohort Study, CMPO Working Paper Series, Working Paper
04/098, 2004.
Case A, Lubotsky M, Paxson C. Economic Status and Health in Childhood: The Origins of the
Gradient, American Economic Review, 2002; 92(5): 1308-1334.
Currie A, Shields MA, Wheatley Price S. Is the Child Health / Family Income Gradient
Universal? Evidence from England, IZA Discussion Paper Series, Discussion Paper No. 1328,
2004.
Currie J, Moretti E. Biology as Destiny? Short and Long-Run Determinants of Intergenerational
Transmission of Birth Weight, NBER Working Papers Series, Working Paper 11567, 2005.
Currie J, Stabile M. Socioeconomic Status and Child Health: Why Is the Relationship Stronger
for Older Children? American Economic Review 2003; 93(5): 1813-1823.
Davey Smith G, Hart C, Ferrell C, Upton M, Hole D, Hawthorne V, Watt G. Birth weight of
offspring and mortality in the Renfrew and Paisley study: prospective observational
study, British Medical Journal, 1997; 315: 1189-1193.
Doyle O, Harmon C, Walker I. The Impact of Parental Income and Education on the Health of
their Children, IZA Discussion Paper Series, Discussion Paper No. 1832, 2005.
Grossman M. On the concept of health capital and the demand for health. Journal of Political
Economy 1972; 80: 223-255.
Hyppönen E, Davey Smith G, Power C. Parental diabetes and birth weight of offspring:
intergenerational cohort study, British Medical Journal, 2003; 326: 19-20.
Kebede B. Genetic Endowments, Parental and Child Health in Rural Ethiopia. Scottish Journal of
Political Economy, 2005; 52(2): 194-221.
Power C, Peckham C. Childhood Morbidity and Adult Ill-Health, National child Development
Study User Support Group, Working Paper No. 37, 1987.
Rosenzweig MR, Schultz TP. Estimating a Household Production Function: Heterogeneity, the
Demand for Health Inputs, and Their Effect on Birth Weight, The Journal of Political Economy,
1983; 91(5): 723-746.
Rosenzweig MR, Wolpin KI. Heterogeneity, Intrafamily Distribution, and Child Health. The

Journal of Human Resources, 1988; 23(4): 437-461.

Appendix A
Table A1: Health information by generation
Generation1: Parents of the
cohort members
Generation 2: Cohort
members
Generation 3: children of the
cohort members
1) Before and/or during
pregnancy
a) Mother’s Height
b) Mother’s Weight
c) Prenatal care
d) Maternal smoking
e) Pregnancy-related
problems
(pleclampsia,
bleeding, toxemia and
low hemoglobin)
2) After pregnancy
a) Height and weight
b) Chronic conditions (in
wave 1- only 3
categories- and wave
2)
c) Date of death
d) Parental smoking
1) Health at birth
a) Birthweight (by
gestational age and
sex)
b) Illness in the first
week of life
2) During childhood
a) Accidents
b) Hospitalizations
c) Chronic conditions
(physical)
d) Acute conditions
e) Psychological
problems
3) In adulthood
a) SAH
b) Disability/LSI
c) Health behavior:
smoking, drinking,
exercise, nutrition
d) Height and weight
(self-reported)
1) Pregnancy information
2) Birthweight
3) Motor problems, chronic
conditions (asthma,
epilepsy, hay fever,
eczema, migraine,
diabetes), behavioral.