intragastrointestinal alcohol fermentation syndrome: report of two
TRANSCRIPT

COMMENTARY
Intragastrointestinal Alcohol Fermentation Syndrome: Report of Two Cases and
Review of the Literature H KAJI,* Y ASANUMA, 0 YAHARA, H SHIBUE,
M HISAMURA, N SAITO, Y KAWAKAMI and M MURAO
The First Department of Medicine, Hokkaido University School of Medicine, Nishi-7, Kita-1.5, Kita-ku, Sapporo 060, Japan
Abstract Two patients with frequent attacks of alcohol intoxication following the intake of an ordinary meal are presented. The causative agents were Candida albicans and C. krusei in the first case and C. albicans in the second. The essential factors of this syndrome were abnormal proliferation of the causative agent, abnormal stagnation of food in the alimentary tract, intake of a carbohydrate diet as the substrate for the alcohol fermentation and low threshold of the patient to alcohol. Thirty-seven other cases have been reported in Japan since 1952, with patients aged from 1 to 75 years. All those con- cerned with alcohol intoxication, especially in the forensic sciences, should bear this syndrome in mind. Key Words: Alcohol intoxication; Endogenous alcohol; Gastrointestinal moniliasis; Candida albicans; Intragastrointestinal alcohol fer- mentation.
Journal of the Forensic Science Society 1984; 24: 461-471 Received 11 October 1983
Introduction Increases in alcohol dependence, road casualties and crimes under the influence of alcohol and inebriate driving are worldwide social problems especially from the toxicological, medicolegal and criminological points of view. In postmortem examinations it is necessary to determine whether the source of blood ethanol is putrefactive alcohol production or antemortem alcohol consumption. As more sensitive analyses come into general use, trace amounts of alcohol are easily detectable in human body fluids. Thus, Harger reports normal body alcohol levels of up to 0.25 mgldl [I] and Lester
* Present address: Health Examination Center, Workmen's Accident Compensation Hospital of Iwamizawa, 4-jo, Higashi 16-chome, Iwami~awa 068, Japan.
461

reports that concentrations of up to 0.15 mgldl may be present, but whether this alcohol is endogenous is unresolved [2]. Recently, a significant increase in lower aliphatic alcohols has been demonstrated in the 24-hour urine of diabetic patients [3,4] and there may be ethanol production in infected urine
[51.
On the other hand, some cases have been reported with repeated attacks of alcoholic intoxication without prior intake of alcohol, what may be called the intragastrointestinal alcohol fermentation syndrome. This is a type of moniliasis in which patients become inebriated after the intake of an ordinary carbohydrate meal. It is caused by excessive production of ethanol by carbohydrate fermentation due to yeasts, mainly those belonging to the Candida group, which have proliferated abnormally in the gastrointestinal tract. Thus far, 37 cases have been reported in Japanese literature since the first report appeared [6]. Although, to the best of the authors' knowledge, no such case has been reported in other countries, clinician, toxicologist and forensic scientist should be aware of the significance of the syndrome.
In the present communication, two further cases of the syndrome are presented, and the characteristics of the pertinent causative factors in 39 Japanese cases are analyzed.
Methods
Measurement of ethanol concentration in breath, blood and urine The ethanol concentrations were measured by a gas chromatograph (Model GC-SAPFFp, Shimadzu, Kyoto, Japan), equipped with a flame ionization detector. Breath ethanol concentration was measured by the direct analysis of 5ml of expired alveolar air [7]. Blood, plasma and urine ethanol concentrations were also measured by GC using aqueous solutions of acetonitrile or n-propanol (Wako, Osaka, Japan) as the internal standard [8-101.
Isolation and identification of the causative agents Stomach juice, duodenal juice and faecal specimens were serially cultured using Sabouraud's glucose agar. Candida colonies appearing on this agar were purified on Sabouraud's blood agar. Thereafter, Candida groups were identified by morphological and biological examinations [ l l] .
Alcohol fermentation test in vitro Purified Candida was precultured on potato-glucose agar at 27°C for 7 days. Each suspension was adjusted to a cell number of either 4 x lo7 or 8 x lo7 in 3 ml and then innoculated into 3 ml of fermentation test medium containing 3% of yeast extract. After incubation for between 20 and 100 hours at 27°C or 37"C, the degree of alcohol fermentation activity was determined [l l] .
462
Case reports Case 1. A 24-year-old nurse, previously in good health, had, over a period of 5 months developed symptoms of faintness, nausea and sometimes vomiting 1 to 2 hours after eating. Occasionally she had fallen asleep during her night duty or fallen down while shopping in the daytime. She had deliberately avoided overeating because of the appearance of these signs and symptoms after a meal. Her diet averaged about 1800Cal per day, consumed in the Nurses' Home, with a carbohydrate content of about 78%.
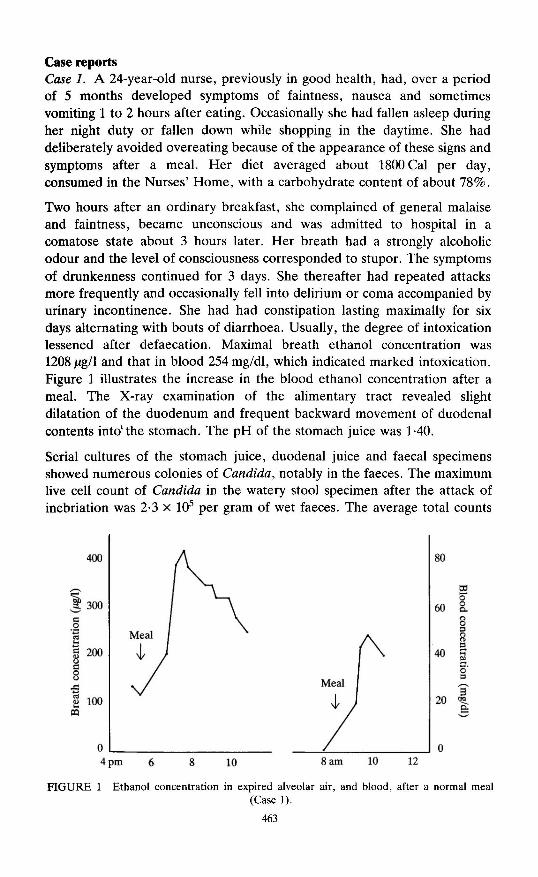
Two hours after an ordinary breakfast, she complained of general malaise and faintness, became unconscious and was admitted to hospital in a comatose state about 3 hours later. Her breath had a strongly alcoholic odour and the level of consciousness corresponded to stupor. The symptoms of drunkenness continued for 3 days. She thereafter had repeated attacks more frequently and occasionally fell into delirium or coma accompanied by urinary incontinence. She had had constipation lasting maximally for six days alternating with bouts of diarrhoea. Usually, the degree of intoxication lessened after defaecation. Maximal breath ethanol concentration was 1208 pgll and that in blood 254 mgldl, which indicated marked intoxication. Figure 1 illustrates the increase in the blood ethanol concentration after a meal. The X-ray examination of the alimentary tract revealed slight dilatation of the duodenum and frequent backward movement of duodenal contents into'the stomach. The pH of the stomach juice was 1-40.
Serial cultures of the stomach juice, duodenal juice and faecal specimens showed numerous colonies of Candida, notably in the faeces. The maximum live cell count of Candida in the watery stool specimen after the attack of inebriation was 2.3 X lo5 per gram of wet faeces. The average total counts
5 : loo m
FIGURE 1 Ethanol concentration in expired alveolar air, and blood, after a normal meal (Case 1).
463

of Candida in the stomach and the duodenal juice were 640 per ml. Candida albicans and C. krusei were identified on Sabouraud's glucose agar. C. albicans showed strong alcoholic fermentation activity, but the activity of C. krusei was only weak (Figure 2).
Since C. albicans was considered the main causative agent, an antifungal agent, Cabimicina (TrichomycinB), 10 x lo4 to 80 x lo4 unitslday, was administered orally [12, 131. Laxatives were also used and, at the same time, carbohydrates in the diet were restricted for five days from the beginning of the treatment. The drunk-like symptoms disappeared completely with this treatment.
Case 2. A 35-year-old cook had been complaining of an alcoholic odour in his breath and drunklike symptoms, such as difficulty in articulation, blurred vision and staggering or weaving gait, but denied having taken alcohol. Although these symptoms appeared several times a week sometimes lasting until midnight, they disappeared spontaneously. Seven months later, the symptoms recurred and on several occasions he lapsed into unconsciousness. Four months later he was admitted to Hospital A. Based on a provisional diagnosis of "the intragastrointestinal alcohol fermentation syndrome" he was treated with an antifungal agent, Nystatinum, 3 x lo6 unitslday orally for 11 days, and was discharged free of symptoms.
Shortly after the discharge, however, his symptoms reappeared and he was
"1 (a) (b)
20 . B
s .B 15. A
$' V
5 10. .- F .- +8
m c .s 5.. m c.
Candida albicans
8
f B
. A
Candida albicans
I
Candida krusei Candida krusei
0 0 10 20 30 40 50 60 70 80 90 100 0 10 20 30 40 50 60 70 80
Incubation time in hours FIGURE 2 Alcoholic fermentation test in vitro (Case 1). (a) Incubation at 27'C. (b)
Incubation at 37°C.

admitted to our clinic. He had a past history of appendectomy at the age of 15. Physical and biochemical examinations revealed no abnormal findings except for a slight alcoholic odour in his breath. The X-ray examination of the alimentary tract revealed no abnormal findings. The pH of the stomach juice was 6.80.
On the 13th day after admission, he felt faint during the morning and mildly drunk throughout the day. These symptoms abated by noon of the 14th day (Figure 3). During this time, microbiological examinations of stomach juice, duodenal juice and faeces were performed. The live cell counts of Candida were 1750, 820, 620 and 300 per ml in the stomach juice, 1470 per ml in the duodenal juice, and 7.4 x lo4 per gram of wet faeces. Candida colonies on Sabouraud7s glucose agar were identified as C. albicans Robins Berkhout (1853) which proved to be resistant to the Nystatinum which had been used in Hospital A. The symptoms did not re-appear in spite of taking an ordinary meal, and he was discharged without treatment, but three months later he was readmitted because of severe inebriation. This time, the live cell count of C. albicans in stomach juice was 3560 per ml. He was treated by oral administration of 1-5 x 10' unitslday of Cabimicina (TrichomycinB) for 45 days. Thereafter organisms of the Candida group were not detected in stomach juice and faeces and he is now quite healthy and completely free from the previous symptoms.
0 J
- I I I 1 I
9 lOpm 6 7 8 9 am Time
FIGURE 3 Serial ethanol concentrations in an attack of inebriation (Case 2). A -.-. A breath, 0--3 plasma, X----X urine.
465

TA
BL
E 1
. Su
mm
ary
of c
ases
of
39 p
atie
nts
with
the
intr
agas
troi
ntes
tinal
alc
ohol
ferm
enta
tion
syn
drom
e (J
apan
ese
Mei
tei-
sho)
His
tory
of
abdo
min
al o
pera
tion,
gas
troi
ntes
- C
ase
repo
rt
Age
and
sex
C
ausa
tive
agen
ts
tinal
abn
orm
aliti
es, a
nd r
elat
ed m
atte
rs
Trea
tmen
t
1952
Sa
to [
6]
46 M
ale
Can
dida
fuku
oka
Sato
ex
plor
ator
y la
paro
tom
y, p
ylor
oste
nosi
s (u
lcus
duo
deni
), p
enic
illin
ora
lly,
an-
acid
ity
1960
T
akas
ugi
[23]
46
Mal
e C
. alb
ican
s ga
stre
ctom
y (B
illr
oth
11),
ampu
lla
form
atio
n of
G
enti
ana
viol
et
Tri
chom
vcin
in
test
ine,
nor
mo-
acid
ity
(Cab
imic
ina)
ga
stre
ctom
y (u
lcus
ven
tric
uli)
, am
pull
a re
sect
ion
of
form
atio
n at
gas
troj
ejun
osto
my
ampu
llar
reg
ion
ulcu
s ve
ntri
culi
, pe
nici
llin
and
chlo
ram
phen
icol
ora
lly
-
Tak
asug
i [2
3]
41 M
ale
C. a
lbic
ans
Mur
amot
o*
41 M
ale
C. a
lbic
ans
Miy
aish
i*
28 F
emal
e C
. alb
ican
s in
test
inal
tub
ercu
losi
s, s
teno
sis
and
dila
tati
on o
f sm
all
inte
stin
e ga
stro
jeju
nost
omy,
rev
erse
d pe
rist
alsi
s of
du
oden
al C
-loo
p, a
n-ac
idity
ga
stro
jeju
nost
omy
gast
roje
juno
stom
y, p
arti
al d
ilat
atio
n of
sm
all i
ntes
tine
, an
-aci
dity
ga
stre
ctom
y (B
illr
oth
11),
inte
stin
al t
uber
culo
sis,
am
pull
a fo
rmat
ion
afte
r an
asto
mos
is
gast
rect
omy
(Bil
lrot
h I)
, di
lata
tion
of
duod
enum
-
pylo
rost
enos
is (
stom
ach
canc
er),
dil
atat
ion
of s
tom
ach,
nor
mo-
acid
ity
gast
roje
juno
stom
y -
Tri
chom
ycin
1961
K
ikuo
ka [
24]
37 M
ale
C. a
lbic
ans
& B
row
n ye
ast
Tri
chom
ycin
C. s
tello
idea
C
. tro
pica
lis
Fujis
awa*
E
zaki
[25
] 43
Mal
e 75
Fem
ale
Tri
chom
ycin
N
K 4
58,
myc
o-
stat
in
Nys
tatin
H
ashi
mot
o [2
6]
30 M
ale
Sacc
haro
myc
es
Tan
aka*
It
o*
1962
M
aeda
(20
)
61 M
ale
-
51 M
ale
C. a
lbic
ans
C. a
lbic
ans
C. t
ropi
calis
& B
row
n ye
ast
C. a
lbic
ans
gast
rect
omy
&
Tri
chom
ycin
19
63
Kam
eya*
Is
hiba
shi*
K
awab
ata
[27]
39 F
emal
e 1
Fem
ale
45 M
ale
Sacc
haro
myc
es c
ervi
siae
C
. gui
llier
mon
dii
-
Tri
chom
ycin
ch
olec
yste
ctom
y (c
hole
lith
iasi
s), n
orm
o-ac
idit
y,
peni
cilli
n an
d st
rept
omyc
in a
dmin
istr
atio
n 28
Fem
ale
C. a
lbic
ans
Yos
hika
wa*
19
64
Kun
ishi
ma*
28
Fem
ale
C. a
lbic
ans
inte
stin
al t
uber
culo
sis,
ato
nia
of s
tom
ach
and
duod
enum
di
lata
tion
of
duod
enum
co
ngen
ital
ste
nosi
s of
upp
er j
ejun
um
gast
roje
juno
stom
y
Tsu
kaha
ra*
15 M
ale
C. a
lbic
ans
Mak
unai
* 3
Fem
ale
-
-
rese
ctio
n of
ste
nosi
s

1965
Y
okot
a*
Fuk
aura
* 19
66
Iyo
[21]
Nag
ai*
Ideu
chi*
19
67
Tan
aka
[28]
Nob
oris
aka*
19
68
Mih
ara*
19
69
Taj
ima*
Wak
ana*
M
iura
* 19
71
Saka
kiya
ma
[22]
T
akah
ashi
* P
19
74
Yam
ashi
ta [
29]
8
1978
K
awan
aka
[30]
Kan
aya*
1980
T
akah
ashi
* Sh
y [3
11
20 F
emal
e C
. alb
ican
s 48
Mal
e C
. alb
ican
s 21
Fem
ale
C. a
lbic
ans
& C
. kru
sei
27 M
ale
C. t
ropi
calis
32
Mal
e C
. alb
ican
s 22
Mal
e C
. alb
ican
s
19 F
emal
e 46
Mal
e 52
Fem
ale
48 M
ale
64 M
ale
68 F
emal
e 36
Mal
e 53
Mal
e
C. t
ropi
calis
C
. tro
pica
lis
C. a
lbic
ans,
C.
stel
loid
ea
& S
acch
arom
yces
C
. alb
ican
s Sa
ccha
rom
yces
Sa
ccha
rom
yces
C
. alb
ican
s C
andi
da
2 F
emal
e To
rulo
psis
gla
brat
a
40 F
emal
e C
. alb
ican
s
70 M
ale
T. g
labr
ata
70 M
ale
C. t
ropi
calis
24 F
emal
e C
. alb
ican
s &
C. k
ruse
i
35 M
ale
C. a
lbic
ans
none
no
ne
gast
rect
omy
(Bil
lrot
h I)
, ste
nosi
s of
duo
denu
m
(par
s hor
izon
tali
s), c
hlor
amph
enic
ol o
rall
y, h
ypo-
acid
ity
none
di
lata
tion
of
duod
enum
pa
ncre
atit
is (
due
to in
test
inal
mon
ilias
is?)
none
ch
olec
yste
ctom
y, s
tom
ach
canc
er,
anac
idit
y la
paro
tom
ies
(4 t
imes
) in
clud
ing
gast
rect
omy,
bl
ind
loop
for
mat
ion
pylo
rost
enos
is
-
pylo
rost
enos
is,
gast
roje
juno
stom
y C
andi
da i
n bi
le,
an-a
cidi
ty
blin
d lo
op f
orm
atio
n af
ter
gast
roje
juno
stom
y,
mal
abso
rpti
on s
yndr
ome,
an-
acid
ity
duod
enal
dil
atio
n af
ter
duod
enoj
ejun
osto
my
due
to c
onge
nita
l st
enos
is o
f du
oden
um
lapa
roto
my,
res
ecti
on o
f co
lon
desc
ende
ns,
post
- op
erat
ive
sten
osis
of
jeju
num
, di
lata
tion
of
stom
ach
duod
enal
dil
atio
n af
ter
gast
rect
omy
hypo
-aci
dity
, ulc
us v
entr
icul
i, ir
radi
atio
n,
canc
er c
hem
othe
rapy
and
ste
roid
tre
atm
ent
for
lung
can
cer
and
derm
atom
yosi
tis
dila
tati
on a
nd r
ever
sed
peri
stal
sis
of d
uode
num
, ch
lora
mph
enic
ol a
nd c
olim
ycin
ora
lly,
con
stip
atio
n,
norm
o-ac
idit
y hy
po-a
cidi
ty
-
Tri
chom
ycin
re
-ope
rati
on (
Bill
roth
11
) -
Tri
chom
ycin
, Am
pho-
te
rici
n B
, N
ysta
tin
-
-
Nys
tatin
gast
rect
omy
(Bill
roth
I)
Tri
chom
ycin
ga
stre
ctom
y T
rich
omyc
in
-
gast
roje
juno
stom
y
gast
rect
omy
(Bill
roth
I)
-
Nys
taci
n
Tri
chom
ycin
Tri
chom
ycin
* Abs
trac
t of
the
cas
e re
port
cit
ed f
rom
the
Jap
ana
Cen
tra
Rev
uo M
edic
ina.

Discussion Although 39 cases have been reported in Japan since 1952, including our two cases, the syndrome has not yet been recognized outside the country. The syndrome is called "Meitei-sho" in Japanese, which means "the intragastro intestinal alcohol fermentation syndrome", "the alcohol autoin- toxication syndrome" or "the endogenous alcohol intoxication syndrome". A summary of case details is given in Table 1. The age distribution ranged from 1 to 75 years. The male to female ratio was 23: 15 but females predominated in the age group under 29, viz. 10 of 13 cases (76.9%), whereas males outnumbered females in patients over 30, viz. 20 out of 25 cases (80.0%).
In order to rule out surreptitious drinking, patients were strictly and continuously monitored by doctors or nurses in the sickroom for 24 hours. The patterns of ethanol concentrations in blood and in urine would seem to be of value for the differential diagnosis of intragastrointestinal fermentation from surreptitious drinking. There are several reports demonstrating breath, blood and/or urine alcohol concentration patterns following ingestion of 200, 300 and 400 ml of Japanese Sake which contains 16% vlv of ethanol. In such cases, the blood ethanol concentration reaches a peak in an hour following ingestion [14-161, but as shown in Figure 4, in the cases reported here, the blood ethanol concentration peaks two hours following the intake of an ordinary Japanese meal [15].
loo 1
Meal I/ ingestion of Sake
300 ml (n = 7) 200 rnl (n = 59)
0 1 2 3 4 5 hrs
5 6 7 8 9 10 pm Time
FIGURE 4 Plasma ethanol concentration curve after a normal Japanese meal (Case I), superimposed upon the blood ethanol concentration curves after ingestion of 200, 300 and
400 ml of Japanese Sake in healthy males [15].

Candida albicans was recovered in the majority of cases. Causative agents in descending order are: C. albicans, 21 cases; C. tropicalis, 6; Saccharomyces, 4; Torulopsis glabrata and brown yeast, 2 each; C. fukuoka Sato, C. krusei, C. guilliermondii and C. stelloidea, 1 each. As C. albicans is one of the normal flora in the human gastrointestinal tract and its presence increases in several gastrointestinal disorders [17-191, we must consider factors which appear to play important roles in the abnormal proliferation of the agents and marked alcohol fermentation occurring in certain hosts.
Most cases described have shown various gastrointestinal abnormalities. Twenty-one were cases of abdominal surgery, namely: gastrectomy (13); laparotomy (6); and cholecystectomy (2). Organic or functional disturbances of the passage of the gastrointestinal tract are also important factors, such as post-operative blind loop formation, dilatation of the duodenum or small intestine, and backflowing of duodenal content into the stomach. These abnormalities cause the stagnation of digested foods and, at the same time, possibly offer a favourable site for abnormal proliferation of the related agents and alcohol fermentation. On rare occasions, however, no gastroin- testinal abnormality was detectable. Secondary disturbances of the normal intestinal flora due to the frequent medical use of antibiotics seems to be another factor.
The optimum pH for C. albicans activity lies between 2-8 and 6.0, and it utilizes glucose, maltose and sometimes galactose as the substrates for alcohol fermentation. Therefore, hypoacidity of the stomach, the pre- digestion of carbohydrates and the back flow of duodenal contents into the stomach or the stagnation of substrate in the intestine all provide a favourable environment.
In contrast to normal gastrointestinal moniliasis, histopathological changes have not been detected [20-311. This syndrome is therefore characterized as gastrointestinal parasitism of microflora and so, in most cases, it is easily cured by the administration of antifungal agents such as Trichomycin, Amphotericin B or Mycostatin. In some cases, the symptoms disappear spontaneously. Surgical treatment to remove the site of fermentation can be effective (10 out of 39 cases).
As stated above, the intragastrointestinal alcohol fermentation syndrome consists of the following essential factors: parasitism and abnormal proliferation of the causative agent, mainly the Candida group, which is capable of alcohol fermentation in the alimentary tract; abnormal stagnation of foods caused by organic or functional disorders of the alimentary tract; intake of a carbohydrate diet as the substrate for the alcohol fermentation; and a low threshold of the host patient to alcohol.
At present, such cases have been rarely reported outside Japan. Although

not a scientific paper, there was a newspaper report of an American man's memoirs in 1977, indicating he had the syndrome [32]. Additional cases should exist in many other countires. All those concerned with alcoholic intoxication in clinical toxicology and in forensic medicine must bear this syndrome in mind and should consider mycological examination as well as sensitive biochemical analyses.
References 1. Harger RN. Perennial claims of endogenous alcohol or alcohol-like substances. In:
Proceedings of the Fourth International Conference on Alcohol and Traffic Safety. Bloomington: Indiana University, 1965: 182-189.
2. Lester D . The concentration of apparent endogenous alcohol. Quarterly Journal of Studies on Alcohol 1962: 23: 17-25.
3. Liebich HM, Al-Babbili 0 , Zlatkis A and Kim K. Gas chromatographic and mass spectrometric detection of low molecular weight aliphatic alcohols in urines of normal individuals and patients with diabetes mellitus. Clinical Chemistry 1975; 21: 1294- 1296.
4. Liebich HM, Buellow HJ and Kallmayer R. Quantification of endogenous aliphatic alcohols in serum and urine. Journal of Chromatography 1982; 239: 343-349.
5. Ball W and Lichtenwalner M. Ethanol production in infected urine. New England Journal of Medicine 1979; 301: 614.
6. Sato M. On moniliasis of the alimentary tract with alcoholic fermentation produced therein. Fukuoka Acta Medica 1952; 43: 1013-1029.
7. Kaji H, Ide H, Aikawa T and Murao M. Evaluation of the fasting level of the expired alveolar acetone concentration. Journal of the Japan Diabetic Society 1974; 17: 453-456.
8. Baker RN, Alenty AL and Zack JF, Jr. Simultaneous determination of lower alcohols, acetone and acetaldehyde in blood by gas chromatography. Journal of Chromato- graphic Science 1969; 7: 312-314.
9. Palo V and Ilkova H. Direct gas chromatographic estimation of lower alcohols, acetal- dehyde, acetone and diacetyl in milk products. Journal of Chromatography 1970; 53: 363-367.
10. Jain NC. Direct blood-injection method for gas chromatographic determination of alcohols and other volatile compounds. Clinical Chemistry 1971; 17: 82-85.
11. Lodder J and Kreger-van Rij NJW. The yeast; a taxonomic study. Amsterdam: North Holland Publishing Company, 1952.
12. Hosoya S, Komatsu N, Soeda M, Yuwaguchi T and Sonoda Y. Trichomycin, a new antibiotic with trichomonacidal and antifungal activities. Antibiotics 1952; 5: 564-566.
13. Waksman SA and Lechevalier HA. The actinomycetes. Volume 111. Baltimore: The Williams and Wilkins Company, 1962: 397.
14. Fukui Y. Gas chromatographic determination of acetaldehyde in the expired air after ingestion of alcohol. Japanese Journal of Legal Medicine 1969; 23: 24-40.
15. Hishida S, Kinoshita M, Ijiri I, Okada T , Adachi J and Mizoi Y. Studies on the ratio between alcoholic concentrations in urine and blood. Japanese Journal of Legal Medicine 1973; 27: 295-306.
16. Lindros KO, Stowell A , Pikkarainen P and Salaspuro M. Elevated blood acetaldehyde in alcoholics with accelerated ethanol elimination. Pharmacology, Biochemistry and Behavior 1980; 13 (Supplement 1): 119-124.
17. Donaldson RM, Jr. Normal bacterial populations of the intestine and their relation to intestinal function. New England Journal of Medicine 1964; 270: 938-945, 994-1001, 1050-1056.
18. Takahashi K. Etiology and pathogenesis of so-called "drunkenness disease". Report of the Hokkaido Institute of Public Health (Sapporo) 1968; 18: 50-57.
470

Finegold SM. Intestinal bacteria. The role they play in normal physiology, pathologic physiology and infection. California Medicine 1969; 110: 455-459.
Maeda M, Kobayashi J, Hashimoto H, Yabuso S, Wakamatsu M and Yanagisawa T. A case of drunkenness disease in the patient without operation of the stomach. Internal Medicine and Pediatrics (Tokyo) 1962; 17: 77-82.
Iyo S, Ikeda M, Ohashi I, Asai T, Takashima T and Yokohama S. On so-called Meitei-sho. Japanese Journal of Internal Medicine (Tokyo) 1966; 17: 881-888.
Sakakiyama Y, Shiramatsu K, Tozuka M and Suzuki A. Drunkenness disease induced by the alcoholic fermentation in the alimentary tract (stomach). Journal of the Japanese Practical Surgeon Society 1971; 32: 434-438.
Takasugi T and Takada T. Meitei-sho caused by the overgrowth of Candida albicans in the intestinal tract. Clinical All-round (Osaka) 1960; 9: 2092-2095.
Kikuoka H, Masaoka T and Akagi M. A case of Meitei-sho caused by the intragastroin- testinal alcohol fermentation. Japanese Journal of Clinics (Osaka) 1961; 19: 197-202.
Ezaki H, Funaoka H , Fukuma A and Saito H. Meitei-sho caused by the yeasts. Surgic- al Diagnostics and Treatment (Tokyo) 1961; 3: 1529-1534.
Hashimoto K, Matsuno H, Kato H and Tsuchiya N. A case of Meitei-sho caused by the overgrowth of Saccharomyces in the intestine. Chemotherapy (Tokyo) 1961; 9: 24-25.
Kawabata K, Sugawara M, Hiraga H and Takahashi K. Drunkenness-like syndrome. Japanese Transportation Medicine (Tokyo) 1963; 19: 308-314.
Tanaka K, Ideuchi H, Sakamoto S, Adachi S and Kitayama S. A case of gastrointestinal Candidiasis with elevated blood and urinary amylase values and drunk-like symptoms. Japanese Journal of Internal Medicine (Tokyo) 1967; 20: 359-362.
Yamashita Y, Inoue N, Shirabe T, Ohnishi A and Kuroiwa Y. A case of malabsorption syndrome, "Meiteisho" (endogenous ethanol intoxication) and polyneuropathy. Clin- ical Neurology (Tokyo) 1974; 14: 17-23.
Kawanaka T, Nozaki T. Nakamura K, Kajimoto T, Asai T and Kanayama T. A 2-year-old surgically treated female case of so-called Meitei-sho. Operation (Tokyo) 1978; 32: 1249-1252.
Shy CY, Sugiyama M, Eto S, Tsuchiya S and Nagaoka H. A case of gastric Candidiasis with alcoholemia. Japanese Journal of Gastroenterology (Tokyo) 1982; 79: 1318- 1321.
National Enquirer. 30586-2. November 1, 1977.