intratumoral bacillus calmette-guerin immunotherapy prior...
TRANSCRIPT

[CANCER RESEARCH 46, 5963-5968, November 1986]
Intratumoral Bacillus Calmette-Guerin Immunotherapy prior to Surgery for
Carcinoma of the Lung: Results of a Prospective Randomized TrialRichard A. Matthay', Donald A. Mahler2, Gerald J. Beck3, Jacob Loke, Arthur E. Baue4, Darryl C. Carter, andMalcolm S. Mitchell5
Pulmonary [R. A. M., D. A. M., J. L.] and Clinical Oncology [M. S. M.J Sections, Department of Internal Medicine, and the Departments of Pathology [D. C. CJ andSurgery [A. E. B.J, Yale University School of Medicine, and the School of Epidemiology and Public Health [G. J. B.J, Yale University, New Haven, Connecticut 06510
ABSTRACT
A prospective randomized trial of preoperative intratumoral therapywith Bacillus Calmette-Guérin(BCG) was conducted in non-small celllung cancer patients. Eighty-eight patients (48 BCG-treated and 40control subjects) were entered into the study; three control subjects wereremoved from data analysis because histology revealed pathology otherthan non-small cell lung cancer. There were no differences between BCG-treated and control patients in sex, age, cigarettes smoked per day, pack-years of cigarette smoking, white blood cell count, or number of peripheralblood lymphocytes. Toxicity of BCG was limited to transient malaise andfever (average peak temperature, 38.7°C).There was no significant
difference in outcome (recurrence or survival) between BCG-treated andcontrol groups with Stage I or Stage III tumors; there were too few StageII tumors for separate statistical analysis. Outcome was not affectedwithin or between the two treatment groups by tuberculin skin test status.Combining both treatment groups, Stage III patients had a worse outcomethan did Stage III patients, non-squamous cell tumor patients (large celland adenocarcinoma) had worse outcomes than did squamous cell tumorpatients, and men had a worse outcome than women. We conclude that,although preoperative intratumoral BCG therapy is safe, it does notlengthen disease-free interval or prolong survival in patients with non-small cell lung cancer.
INTRODUCTION
Lung cancer, the most common and one of the most aggressive forms of carcinoma, kills 95% of its victims within 5 years.Despite surgical intervention and radiotherapy, only about 40%of patients with resectable Stage II disease survive 5 years (I),and response of non-small cell lung cancer to chemotherapyremains under 50% in most studies of patients with establishedmetastatic disease. With the continued prevalence of smoking,the incidence of lung cancer is likely to remain high and mayincrease.
Immunocompetence may be a determining factor in survivinglung cancer. Cell-mediated and humoral immunity are compromised in cancer patients (1-5). Patients with advanced diseaseand a good delayed hypersensitivity response (skin test) todinitrochlorobenzene are likely to survive longer than patientswith a poor response to dinitrochlorobenzene (5). Likewise,lung cancer patients who respond to recall antigens have abetter prognosis than those who do not (4, 6).
Specific and nonspecific stimulation of the immune systemhas been investigated in animals and humans to determinewhether the host's natural resistance to tumor could be en-
Received 3/10/86; revised 8/6/86; accepted 8/8/86.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1To whom requests for reprints should be addressed, at Yale University Schoolof Medicine, Pulmonary Section—LCI 105, 333 Cedar Street, New Haven,CT06510.
2 Present address: Dartmouth Medical School, Hanover, New Hampshire.3 Present address: Cleveland Clinic Foundation, Cleveland, Ohio.'' Present address: St. Louis University Medical School, St. Louis, Missouri.9 Present address: University of Southern California School of Medicine, Los
Angeles, California.
hanced, thus extending disease-free intervals (7-9). BCG6 is a
nonspecific adjuvant isolated by Calmette and Guérinthroughprogressive attenuation of a virulent strain of Mycobacteriumbovis (7). BCG is a mainstay of active immunotherapy; itstimulates thymus-derived (T)-lymphocytes, macrophages, and"bursa-dependent" (B)-lymphocytes and has been effective
against cutaneous neoplasms (10-12). However, the regressionof multiple intradermal métastasesof malignant melanomaafter intralesional injection of viable BCG probably best demonstrates the efficacy of this adjuvant (13).
McKneally et al. (14, 15) reported that intrapleural BCGsignificantly increases the survival of surgically resected StageI lung cancer patients compared with concurrent randomizedcontrols. However, this therapy did not augment survival ordisease-free intervals in patients with Stage II or Stage IIIdisease. These investigators suggested that regional immunotherapy with BCG eliminates small numbers of residual tumorcells in the lymphatics and draining lymph nodes of the chest.Other trials with intrapleural BCG failed to confirm thesepositive results in lung cancer patients (16, 17), perhaps becauseof differences in the source of the microorganism.
The principal objectives of this prospective randomized trialwere to determine whether transbronchoscopic injection ofBCG into lung tumors before resectional surgery is safe andwhether this form of therapy improves survival or at leastprolongs the disease-free interval after surgery. Preliminaryresults were published (18) after about one-half of the patientshad entered the study. Preliminary data suggested that intratumoral injection of BCG in lung cancer was safe. This reportcorroborates the initial findings of safety and describes theoutcome of all patients studied.
PATIENTS AND METHODS
Patient Selection and Experimental Design
Patients with potentially resectable non-small cell carcinoma of thelung were considered for this study. Before surgery, tumor cell type wasestablished by sputum cytology, fiberoptic bronchoscopy with forceps,and/or brush biopsy (11, 19) or transthoracic needle aspiration biopsywith fluoroscopy as a guide to needle placement. Patients suspected ofhaving lung cancer were excluded if a definite diagnosis had not beenestablished before thoracotomy. Additional exclusion criteria included:(a) evidence of extrathoracic métastases,(A) previous irradiation of thethorax and/or chemotherapy, (c) cancers metastatic to the lung fromanother nonpulmonary site, (d) culture positive tuberculosis, (e) age of80 or more years, and (/) inability to tolerate pneumonectomy orlobectomy due to severity of pulmonary function abnormalities (or dueto other disease such as severe atherosclerotic cardiovascular disease).
Informed consent was obtained from patients who met the criteriafor inclusion in the study. Skin test response to the following recallantigens was determined: 5 TU of PPD (Connaught), 0.1 ml of mumpsskin test antigen (Eli Lilly), 50 PNU (0.1 ml) of trichophytin (Hollister-Stier), and 0.1 ml of streptokinase-streptodornase (Varidase; Lederle).
6 The abbreviations used are: BCG, Bacillus Calmette-Guérin;PPD, purified
protein derivative; INH, isoniazid.
5963
on July 7, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
INTRATUMORAL BCG IMMUNOTHERAPY
Patients were divided into 2 groups according to a table of randomnumbers and sealed-envelope technique in strict numerical order of
entry: BCG and surgery, or surgery only (control). Before surgery,patients were classified into Stage I or II (20) by a stratified blockrandomization method. This technique randomizes patients separatelybased upon their being Stage I or II; random assignments are made inblocks of 11 persons so that 6 persons were assigned to BCG andsurgery and 5 persons were assigned to surgery only. We anticipatedthat in some patients BCG would not be successfully injected into thetumor and that this subgroup would not be evaluated in the BCGtreatment group. Therefore, the randomization was constructed so thatthe BCG treatment group would be slightly larger. As the study progressed, it became evident that tumors could all be reached successfullywith BCG, but we decided to retain the original randomization scheme,so there were more BCG-treated than control patients.
We injected BCG (Tice strain; Chicago Research Foundation, University of Illinois) IO7 viable organisms for PPD skin test-negativepatients (14, 15, 21) and 5 x IO6 for PPD-positive patients (22), into
the tumor mass by passing a flexible fine needle (Meditech Corp.,Watertown, MA) through the fiberoptic bronchoscope. Peripherallylocated lesions, not visible through the bronchoscope, were enteredwith fluoroscopic guidance, and needle position was checked by viewingthe lung from two vantages, supine and lateral.
We obtained chest radiographs 3 days after BCG injection and 2-3weeks later (just before surgery) to determine whether BCG had causeda pulmonary infiltrate.
All control patients underwent thoracotomy immediately followingrandomization, and all BCG-treated patients underwent thoracotomy2-3 weeks after intratumoral injection of BCG. Standard criteria forresection and uniform technique were used. Immediately after surgery,a 12-week course of 300 mg INH daily was given to all patients. Liverfunction was tested serially to monitor INH side effects. The controlgroup underwent surgery promptly after randomization. After surgery,all patients were restaged according to the American Joint Committeeon Cancer Staging as modified by Mountain et al. (20). One of us (D.C.) in the Department of Pathology established the cell type in eachcase. Patients classified as Stage III (20) and those who developedmétastasesor local recurrences were treated by irradiation (300 rads x10 treatments) to all known tumor-bearing areas. Local recurrence and/or peripheral métastaseswere established by physical examination,sputum cytology, chest radiograph, and repeat bronchoscopy, whennecessary and by lung tomography or radionuclide scanning as indicated.
Statistical Analysis. Survival and time interval from resection todisease recurrence were analyzed in BCG and control groups by tumorcell type and stage using standard statistical techniques (23, 24). Thecumulative probabilities of survival and nonrecurrence were calculatedby the actuarial method of Berkson and Gage. Survival and recurrencetimes were compared with the proportional hazard model of Cox (10).This model also allows the influence of covariants (e.g., tumor cell type,stage) to be evaluated and adjusted for when comparing the survivalprobabilities of the two treatments. This covariant analysis was repeatedonly with patients receiving BCG to include a covariant for post-BCG
temperature in the patient. The Cox regression models were fit usingPROC PHGLM in the SAS statistical package (10). The best fittingmodel was determined by the iterative process. Information was incomplete for some patients on some of the covariants, and these cases wereautomatically eliminated in the Cox procedure. Covariants that wereclearly nonsignificant were then eliminated and a new model was fit,which usually included a large number of individuals. This step wasrepeated until most subjects were entered into the analysis. The forwardstepwise option was used to find the model that contained only significant terms (P < 0.05). At this point, further models were fit thatincluded interaction terms of the significant main effects or of the maineffects with other factors of special interest. The main effects corresponding to any interaction term were always included in the model,whether significant or not. Insignificant interaction terms were eliminated from the model until a final mode was produced.
RESULTS
Characteristics and Outcome of BCG-treated Patients andControls. Eighty-eight patients entered the study; 48 BCG-treated and 40 control patients. Three control patients wereremoved from data analysis because the histology of the resectedspecimen at surgery revealed small cell carcinoma, a benignadenoma, and metastatic bladder carcinoma. Therefore, resultsare reported on 85 patients: 62 men and 23 women.
Of the 85 patients evaluated, 48 were treated with BCG and37 were controls. The unequal numbers in the two groupsfavored the BCG group due to study design. In Stage I, therewere 23 BCG treated and 20 control patients; Stage II, 3 BCGand 6 controls; Stage III, 22 BCG and 11 controls. Among allthree stages, there were 44 squamous cell cancers (29 BCG, 15controls), 31 adenocarcinomas (12 BCG and 19 controls), 9large cell carcinomas (7 BCG and 2 controls), and one aden-osquamous cell (one control). Tumor cell type did not differsignificantly between BCG-treated and control patients at anyof the three stages.
Table 1 shows comparative characteristics and outcome ofBCG-treated and control patients in all three stages. There wereno differences between BCG-treated and control patients in sex,age, cigarettes smoked per day, pack-years of cigarette smoking,white blood cell count, or number of peripheral blood lymphocytes. The two groups did not differ in mean follow-up time(entry to censorship) or in mean interval between entry andrecurrence or death. Median time to recurrence was 237 daysin BCG-treated patients and 288 days in controls (NS), whereasthe median survival was 345 days in BCG-treated patients and433 days in controls (NS).
Similarly, there was no statistically significant differencebetween BCG-treated and control patients at any of the threestages in sex, age, average number of cigarettes smoked perday, package years of cigarettes, PPD skin test status, skin testanergy, remote or recent hemoptysis, or absolute (pre-BCG)lymphocyte count. There was also no difference in outcomebetween BCG-treated patients and controls due to any of theaforementioned variables.
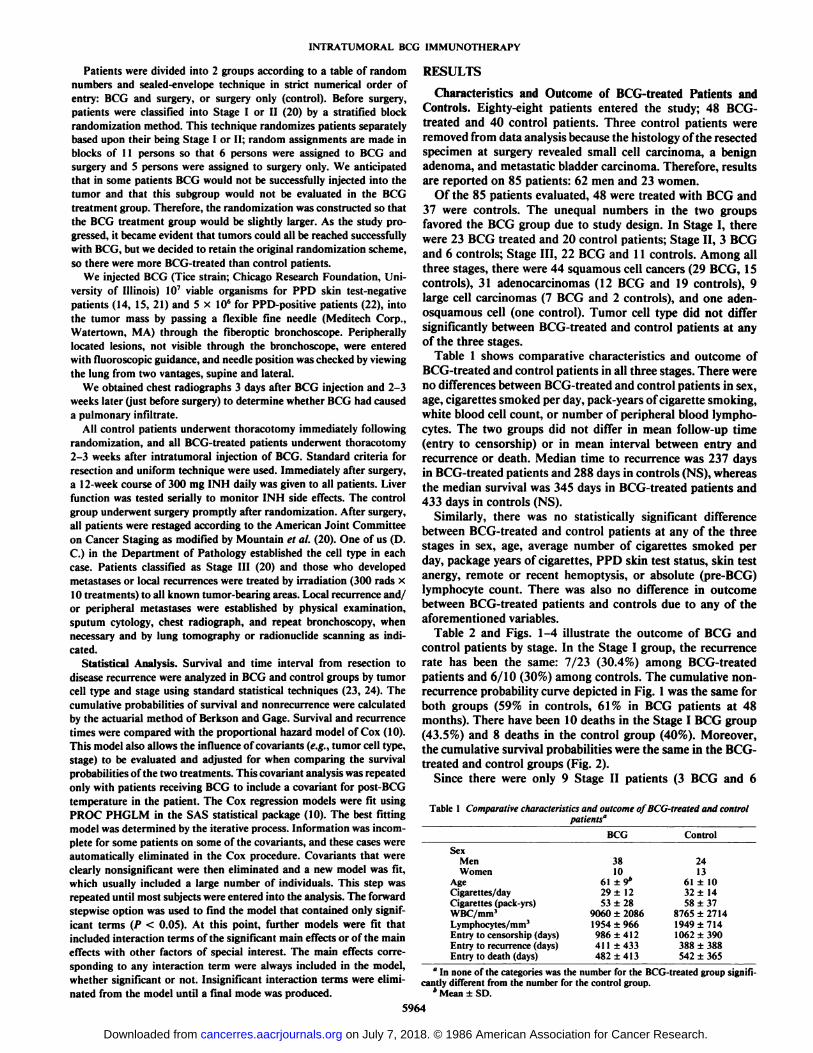
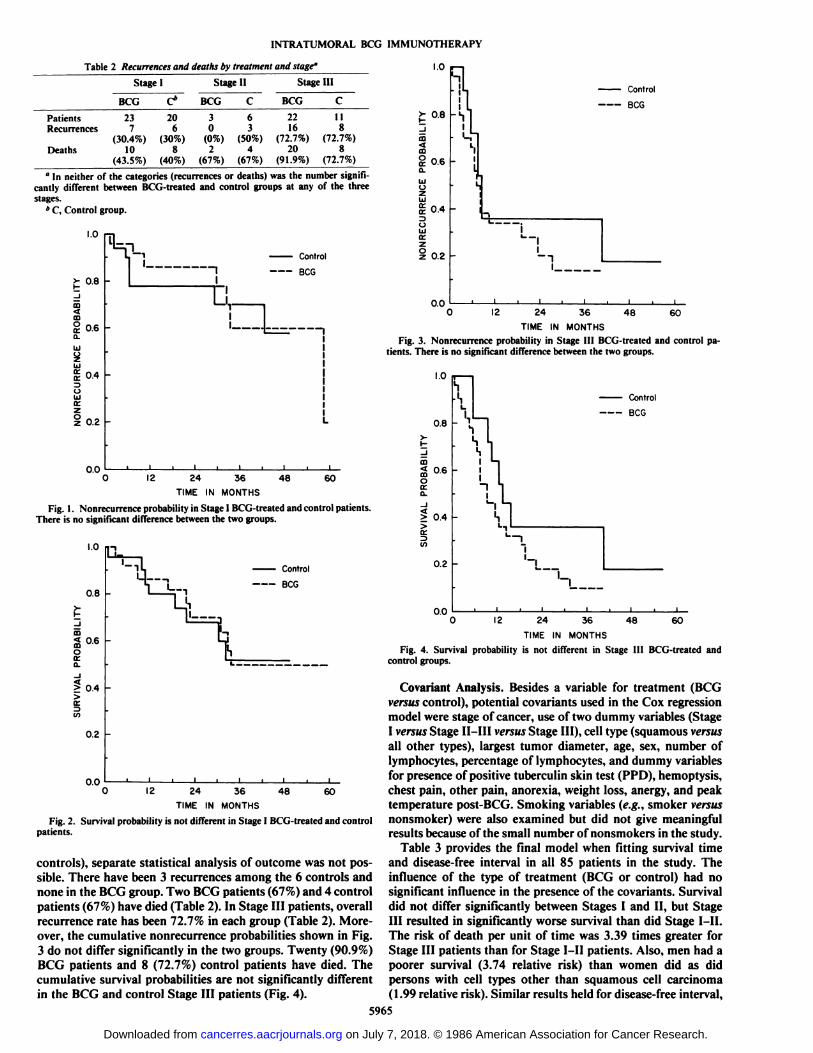
Table 2 and Figs. 1-4 illustrate the outcome of BCG andcontrol patients by stage. In the Stage I group, the recurrencerate has been the same: 7/23 (30.4%) among BCG-treatedpatients and 6/10 (30%) among controls. The cumulative non-recurrence probability curve depicted in Fig. 1 was the same forboth groups (59% in controls, 61% in BCG patients at 48months). There have been 10 deaths in the Stage I BCG group(43.5%) and 8 deaths in the control group (40%). Moreover,the cumulative survival probabilities were the same in the BCG-treated and control groups (Fig. 2).
Since there were only 9 Stage II patients (3 BCG and 6
Table 1 Comparative characteristics and outcome of BCG-treated and controlpatients"
SexMenWomenAgeCigarettes/dayCigarettes
(pack-yrs)WBC/mm3Lymphocytes/mm3Entry
to censorship(days)Entryto recurrence(days)Entryto death (days)BCG381061
±9*29
±12S3±289060
±20861954±966986±412411±433482
±413Control241361
±1032±1458
±378765±27141949
±7141062±390388
±388542±365
" In none of the categories was the number for the BCG-treated group signifi
cantly different from the number for the control group.* Mean ±SD.
5964
on July 7, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
INTRATUMORAL BCG IMMUNOTHERAPY
Table 2 Recurrences and deaths by treatment and stage'
StageIPatients
RecurrencesDeathsBCG237(30.4%)
10(43.5%)C*20
6(30%)
8(40%)Stage
IIBCG3
0(0%)
2(67%)C63
(50%)4
(67%)Stage
IIIBCG22
16(72.7%)
20(91.9%)C118(72.7%)
8(72.7%)
°In neither of the categories (recurrences or deaths) was the number significantly different between BCG-treated and control groups at any of the threestages.
* C, Control group.
1.0
?- 0.8
oocQ.
UJ
2LU
0.4
OUJCC
0.2
Control
--- BCG
12 24TIME IN
36MONTHS
48 60
Fig. 1. Nonrecurrence probability in Stage I BCG-treated and control patients.There is no significant difference between the two groups.
1.0
0.8
co
2oo:O.
> 0.4>
0.2
00
Control
12 24
TIME IN
48 6036
MONTHS
Fig. 2. Survival probability is not different in Stage I BCG-treated and controlpatients.
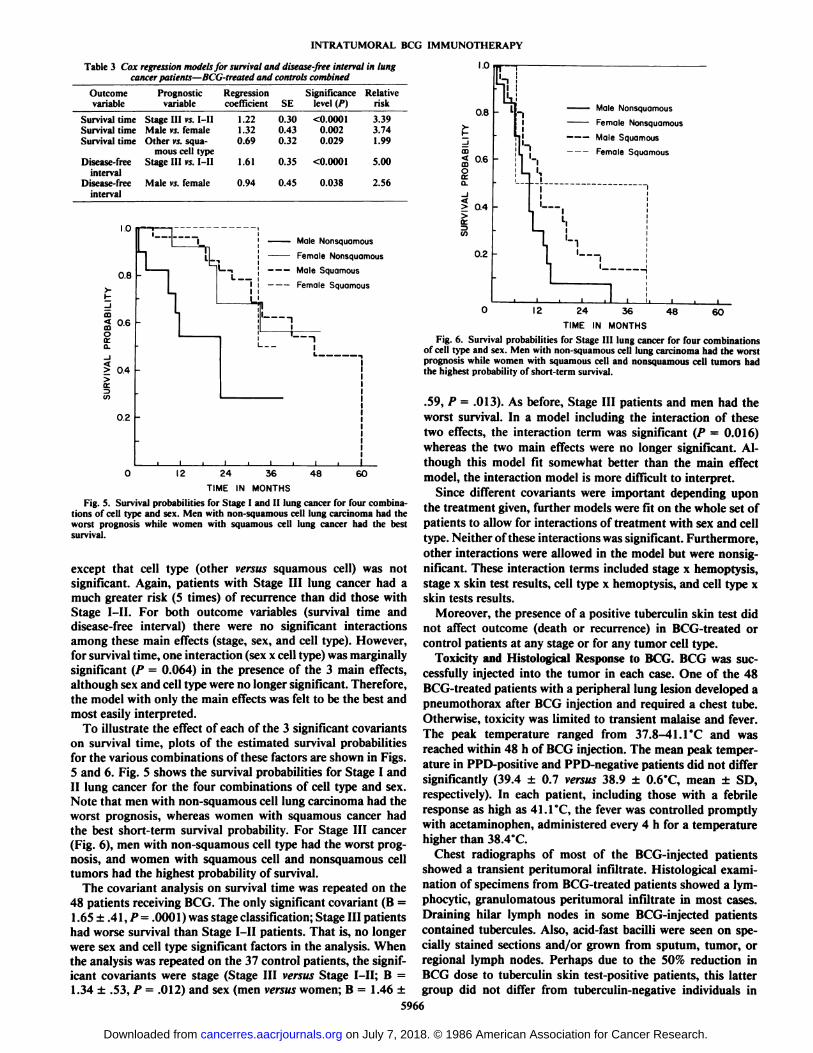
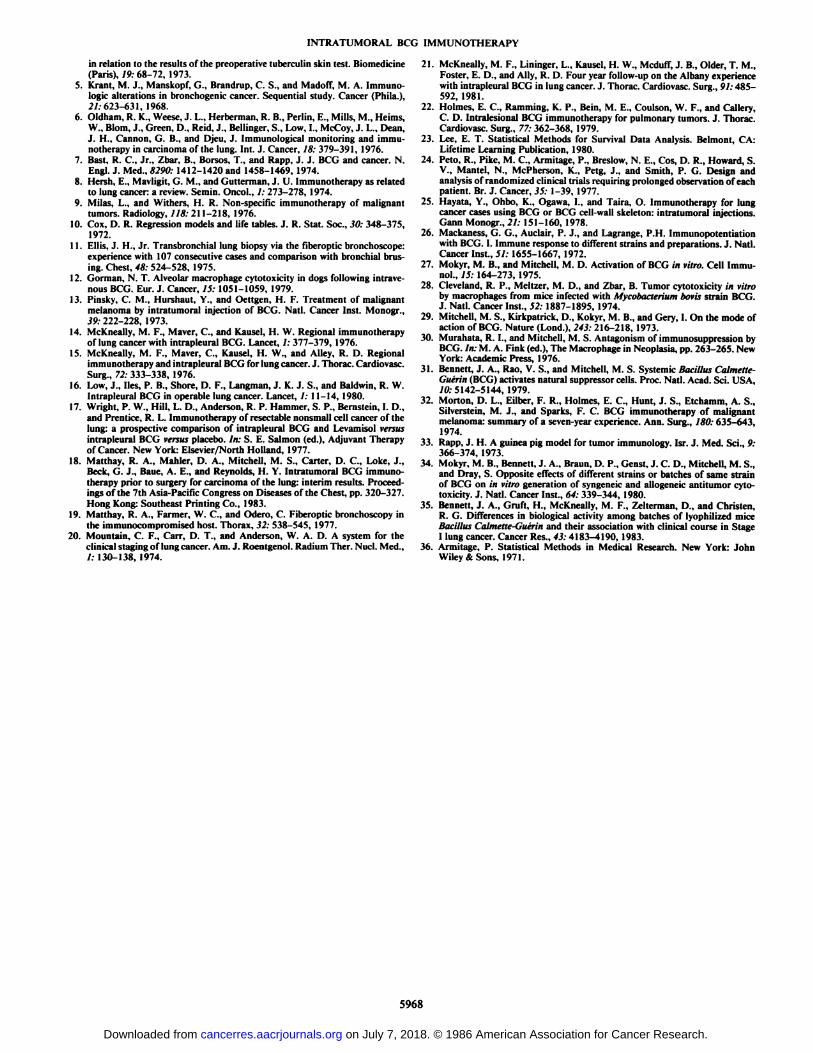
controls), separate statistical analysis of outcome was not possible. There have been 3 recurrences among the 6 controls andnone in the BCG group. Two BCG patients (67%) and 4 controlpatients (67%) have died (Table 2). In Stage III patients, overallrecurrence rate has been 72.7% in each group (Table 2). Moreover, the cumulative nonrecurrence probabilities shown in Fig.3 do not differ significantly in the two groups. Twenty (90.9%)BCG patients and 8 (72.7%) control patients have died. Thecumulative survival probabilities are not significantly differentin the BCG and control Stage III patients (Fig. 4).
I.W£0.8co<jCDg
0.6fl-UIozUJi
0.4CJUJKzi
0.2nnU.W(h].
¡UControl¡
1BCG•*lj*-hL,11lEll-
_ _.1t-
—.1-n1i
. i i i i i ,i)12 24 36 4860TIME
IN MONTHSFig. 3. Nonrecurrence probability in Stage III BCG-treated and control pa
tients. There is no significant difference between the two groups.
Control
BCG
"I
12 24TIME IN
36
MONTHS
48 60
Fig. 4. Survival probability is not different in Stage 111 BCG-treated andcontrol groups.
(mariant Analysis. Besides a variable for treatment (BCGversus control), potential covariants used in the Cox regressionmodel were stage of cancer, use of two dummy variables (StageI versus Stage 1I-III versus Stage III), cell type (squamous versusall other types), largest tumor diameter, age, sex, number oflymphocytes, percentage of lymphocytes, and dummy variablesfor presence of positive tuberculin skin test (PPD), hemoptysis,chest pain, other pain, anorexia, weight loss, anergy, and peaktemperature post-BCG. Smoking variables (e.g., smoker versusnonsmoker) were also examined but did not give meaningfulresults because of the small number of nonsmokers in the study.
Table 3 provides the final model when fitting survival timeand disease-free interval in all 85 patients in the study. Theinfluence of the type of treatment (BCG or control) had nosignificant influence in the presence of the covariants. Survivaldid not differ significantly between Stages I and II, but StageIII resulted in significantly worse survival than did Stage I-II.The risk of death per unit of time was 3.39 times greater forStage III patients than for Stage I-II patients. Also, men had apoorer survival (3.74 relative risk) than women did as didpersons with cell types other than squamous cell carcinoma(1.99 relative risk). Similar results held for disease-free interval,
5965
on July 7, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
INTRATUMORAL BCG IMMUNOTHERAPY
Table 3 Cox regression models for survival and disease-free interval in lungcancer patients—BCG-treated and controls combined
OutcomevariableSurvival
timeSurvivaltimeSurvivaltimeDisease-freeintervalDisease-freeintervalPrognostic
Regressionvariable coefficientSEStage
III >-vMlMale
vs.femaleOthervs.squa-mous
celltypeStageIII vs.MlMale
i'v female1.221.320.691.610.940.300.430.320.350.45Significance
level(/>)<0.00010.0020.029<0.00010.038Relativerisk3.393.741.995.002.56
I.Ui'h0.8
\-1>
LdcoS
0-6coo
orCL>
04or
(/>0.2---iL11
1i—1—,
L1L—
MateNonsquamousFemale
Nonsquamous——— MaleSquamousFemale
Squamous11
.n*'—ii
ilililÃ
12 24 36 48 60
TIME IN MONTHS
Fig. 5. Survival probabilities for Stage I and II lung cancer for four combinations of cell type and sex. Men with non-squamous cell lung carcinoma had theworst prognosis while women with squamous cell lung cancer had the bestsurvival.
except that cell type (other versus squamous cell) was notsignificant. Again, patients with Stage III lung cancer had amuch greater risk (5 times) of recurrence than did those withStage I-II. For both outcome variables (survival time anddisease-free interval) there were no significant interactionsamong these main effects (stage, sex, and cell type). However,for survival time, one interaction (sex x cell type) was marginallysignificant (P = 0.064) in the presence of the 3 main effects,although sex and cell type were no longer significant. Therefore,the model with only the main effects was felt to be the best andmost easily interpreted.
To illustrate the effect of each of the 3 significant covariantson survival time, plots of the estimated survival probabilitiesfor the various combinations of these factors are shown in Figs.5 and 6. Fig. 5 shows the survival probabilities for Stage I andII lung cancer for the four combinations of cell type and sex.Note that men with non-squamous cell lung carcinoma had theworst prognosis, whereas women with squamous cancer hadthe best short-term survival probability. For Stage III cancer(Fig. 6), men with non-squamous cell type had the worst prognosis, and women with squamous cell and nonsquamous celltumors had the highest probability of survival.
The covariant analysis on survival time was repeated on the48 patients receiving BCG. The only significant covariant (B =1.65 ±.41, P = .0001 ) was stage classification; Stage HI patientshad worse survival than Stage I-II patients. That is, no longerwere sex and cell type significant factors in the analysis. Whenthe analysis was repeated on the 37 control patients, the significant covariants were stage (Stage III versus Stage I-II; B =1.34 ±.53, P = .012) and sex (men versus women; B = 1.46 ±
1.0
0.8
< 0.6
O
o.
¡0.4
(E
OT
0.2 -
Male Nonsquamous
Female Nonsquamous
— Male Squamous
Female Squamous
12 24TIME IN
48 6036MONTHS
Fig. 6. Survival probabilities for Stage III lung cancer for four combinationsof cell type and sex. Men with non-squamous cell lung carcinoma had the worstprognosis while women with squamous cell and nonsquamous cell tumors hadthe highest probability of short-term survival.
.59, P = .013). As before, Stage III patients and men had theworst survival. In a model including the interaction of thesetwo effects, the interaction term was significant (P = 0.016)whereas the two main effects were no longer significant. Although this model fit somewhat better than the main effectmodel, the interaction model is more difficult to interpret.
Since different covariants were important depending uponthe treatment given, further models were fit on the whole set ofpatients to allow for interactions of treatment with sex and celltype. Neither of these interactions was significant. Furthermore,other interactions were allowed in the model but were nonsignificant. These interaction terms included stage x hemoptysis,stage x skin test results, cell type x hemoptysis, and cell type xskin tests results.
Moreover, the presence of a positive tuberculin skin test didnot affect outcome (death or recurrence) in BCG-treated orcontrol patients at any stage or for any tumor cell type.
Toxicity and Histológica! Response to BCG. BCG was successfully injected into the tumor in each case. One of the 48BCG-treated patients with a peripheral lung lesion developed a
pneumothorax after BCG injection and required a chest tube.Otherwise, toxicity was limited to transient malaise and fever.The peak temperature ranged from 37.8-41.1°C and was
reached within 48 h of BCG injection. The mean peak temperature in PPD-positive and PPD-negative patients did not differsignificantly (39.4 ±0.7 versus 38.9 ±0.6°C,mean ±SD,
respectively). In each patient, including those with a febrileresponse as high as 41.1 °C,the fever was controlled promptly
with acetaminophen, administered every 4 h for a temperaturehigher than 38.4°C.
Chest radiographs of most of the BCG-injected patientsshowed a transient peritumoral infiltrate. Histológica! examination of specimens from BCG-treated patients showed a lym-
phocytic, granulomatous peritumoral infiltrate in most cases.Draining hilar lymph nodes in some BCG-injected patientscontained tubercules. Also, acid-fast bacilli were seen on specially stained sections and/or grown from sputum, tumor, orregional lymph nodes. Perhaps due to the 50% reduction inBCG dose to tuberculin skin test-positive patients, this lattergroup did not differ from tuberculin-negative individuals in
5966
on July 7, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

INTRATUMORAL BCG IMMUNOTHERAPY
histological response to BCG. BCG did not adversely affectlung resection or healing.
Patients received 300 mg INH daily for 12 weeks to preventintra- and extrathoracic dissemination of BCG organisms, andthere was no evidence of M. bovis dissemination after intrale-sional injection. Serum glutamic-oxalacetic transaminase increased 5-fold, and lethargy developed in 2 patients. When INHwas discontinued in these patients, the serum glutamic-oxalacetic transaminase returned to normal and the lethargy reversed.
DISCUSSION
This study confirms other reports (3,22,25) that preoperativeintratumoral injection of BCG in patients with non-small celllung cancer is both feasible and safe. However, this prospective,randomized study also shows that BCG therapy neither prolongs survival nor extends the interval between surgery andtumor recurrence.
BCG was successfully injected into all lung tumors, includingperipheral tumors as small as 2 cm in diameter. Moreover, apneumothorax requiring insertion of a chest tube developed inonly one of the 48 BCG-injected patients (2%). This contrastsmarkedly with the 33% pneumothorax rate reported by Holmeset al. (3), who used the percutaneous transthoracic technique toadminister BCG into peripheral lung tumors. Fever developedin all BCG-treated patients and a postinjection, transient peri-tumoral infiltrate was evident on the chest radiograph in most.The peak temperature was the same in PPD-positive and PPD-negative patients, probably because the former group receivedone-half the dose of BCG (5 x IO6 organisms). When Holmes
et al. (3, 22) injected Glaxo strain BCG into pulmonary tumors,the highest, most prolonged fever occurred in patients with aPPD-positive skin test. Accordingly, they recommended a lowerBCG dose in PPD-positive patients (22). We followed thisrecommendation, and as a result the clinical and histologicalresponse to BCG was identical among PPD-positive and PPD-negative patients. In most patients, an inflammatory responseconsistent with tuberculous pneumonitis was adjacent to orinfiltrating the tumor. Special stains and/or culture showedtuberculin organisms in the inflammatory lesions.
The therapeutic efficacy of BCG has been ascribed to itsactivation of the lymphoreticular system. A number of studieshave demonstrated increased immunological reactivity of lymphocytes (26, 27), macrophages (12, 28, 29), and nonadherentspleen cells resembling monocytes (30) after administration ofBCG. Together, these BCG-activated cells might assist in tumorregression. However, recently Bennett et al. (31 ) showed thatBCG administered i.v. to mice activates "natural" suppressor
cells in normal bone marrow. Thus, by augmenting suppressorcell activity, BCG may suppress tumor immunity, thereby enhancing tumor growth. However, results from studies usingintralesional BCG in cutaneous melanoma and other malignancies (13, 32, 33), as well as endobronchial non-small cell lungcarcinomas (22), indicate that this agent causes tumor regression, rather than growth. Nonetheless, adverse affects of BCGon the immune system (e.g., an increase in suppressor cells)may be partially responsible for the failure of this agent toimprove outcome in our study. In fact, in the Stage III group,the poorer outcome among BCG-treated individuals approached statistical significance.
The failure of intratumoral BCG to augment disease-freeinterval or survival in this study also may have been associatedwith differences in biological activity among batches of Tice
strain BCG. Mokyr et al. (34) found striking differences in theability of various strains of BCG to augment or decrease immune responses in vitro. Bennett et al. (35) reported that batchesof BCG that protected mice against circulating tumor cells havegreater sensitivity to INH and higher viability than do batchesthat did not elicit this antitumor activity. Moreover, the cumulative disease-free interval in Stage I lung cancer patientswas longer with batches that protected mice against circulatingtumor cells than with batches that did not afford this protection.A possible solution to this "batch" problem would be use of a
nonviable immunostimulant with predictable, nonvarying anti-tumor activity.
Another possible reason for failure of intralesional BCG toimprove outcome, particularly in the Stage III group, was thelarge tumor burden. McKneally et al. (14, 15, 21) reportedsimilar negative results with postoperative intrapleural BCG inStage III lung cancer patients and attributed the results to thewide extent of tumor.
A type II error (36) may have affected our results. Accordingto this statistical concept, there may not have been enoughpatients in the Stage I or Stage III group to establish conclusively that preoperative, intralesional BCG improves or worsensthe outcome of patients with lung cancer. We doubt that a typeII error prevented us from identifying beneficial effects of BCGbecause there was no evident trend favoring BCG therapy inthe Stage I or Stage III group. However, in the Stage III group,a type II error may have prevented the demonstration of statistically significant adverse effects of BCG.
McKneally and colleagues (21) have suggested that PPD-negative patients with Stage I squamous cell lung carcinomamay benefit from postoperative intrapleural administration ofBCG. Accordingly, in our study we assessed outcome accordingto skin test status and three variables—treatment (BCG versuscontrol), stage, and cell type. Skin test status (PPD positive orPPD negative) did not significantly affect survival or recurrencefor either treatment group, any stage, or any cell type.
The Cox regression model results show (a) that Stage IIIpatients have worse outcomes than Stage I-II patients do, (b)that non-squamous cell (large cell and adenocarcinoma) tumorshave worse outcomes than squamous cell lung carcinomas do,and (c) that men have a worse prognosis than women do.
We conclude that although preoperative intratumoral BCGtherapy is well tolerated and safe in lung cancer patients, itdoes not alter the outcome of the disease. Improved understanding of the ways of selectively manipulating the host's immune
response to his tumor, utilization of a tumor-associated anti-gen(s), and targeted monoclonal antibodies may all lead toimproved results.
ACKNOWLEDGMENTS
The authors express special thanks to all Connecticut physicianswho referred patients to this study, to Joan Wallace for editorialassistance, and to Leslye Stein for secretarial assistance.
REFERENCES
1. Hersh, E. M., Gutterman, J. U., and Mavligit, G. M. Perspectives inimmunotherapy of lung cancer. Cancer Treat. Rev., /: 65-80, 1974.
2. Baldwin, W. R., and Pimm, M. V. BCG immunotherapy of local subcutaneous growth and post-surgical pulmonary métastasesof a transplanted ratepithelioma of spontaneous origin. Int. J. Cancer, 12: 420-427, 1973.
3. Holmes. E. C., Ramming, K. P.. Mink, J., Coulson, W. F.. and Morton, D.L. New method of immunotherapy for lung cancer. Lancet, 2: 586-587,1977.
4. Israel. L., Muciga, J., and Chahinian. P. H. J. Prognosis of early broncho-genie carcinoma: survival curves of 451 patients after resection of lung cancer
5967
on July 7, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
INTRATUMORAL BCG IMMUNOTHERAPY
in relation to the results of the preoperative tuberculin skin test. Biomedicine(Paris), 19: 68-72, 1973.
5. Krant, M. J., Manskopf, G., Brandrup, C. S., and Madoff, M. A. Immunologie alterations in bronchogenic cancer. Sequential study. Cancer (Phila.),21:623-631, 1968.
6. Oldham, R. K., Weese, J. L., Herberman, R. B., Perlin, E., Mills, M., Heims,W., Blom, J., Green, D., Reid, J., Bellinger, S., Low, I., McCoy, J. L., Dean,J. H.. Cannon, G. B., and Djeu, J. Immunological monitoring and iimmi-notherapy in carcinoma of the lung. Int. J. Cancer, 18: 379-391, 1976.
7. Bast, R. C, Jr., Zbar, B., Borsos, T., and Rapp, J. J. BCG and cancer. N.Engl. J. Med., «290:1412-1420 and 1458-1469, 1974.
8. Hersh, E., Mavligit, G. M., and Gutterman, J. U. Immunotherapy as relatedto lung cancer: a review. Semin. Oncol., /: 273-278, 1974.
9. Milas, I .. and Withers, H. R. Non-specific immunotherapy of malignanttumors. Radiology, 118: 211-218, 1976.
10. Cox, D. R. Regression models and life tables. J. R. Stat. Soc., 30: 348-375,1972.
11. Ellis, J. M.. Jr. Transbronchial lung biopsy via the fiberoptic bronchoscope:experience with 107 consecutive cases and comparison with bronchial brus-ing. Chest, 48: 524-528, 1975.
12. Gorman, N. T. Alveolar macrophage cytotoxicity in dogs following intravenous BCG. Eur. J. Cancer, 15: 1051-1059, 1979.
13. Pinsky, C. M., Hurshaut, Y., and Oettgen, H. F. Treatment of malignantmelanoma by intratumoral injection of BCG. Nati. Cancer Inst. Monogr.,39:222-228, 1973.
14. McKneally, M. F., Maver, C., and Kausei, H. W. Regional immunotherapyof lung cancer with intrapleural BCG. Lancet, 1: 377-379, 1976.
15. McKneally, M. F., Maver, C., Kausel, H. W., and Alley, R. D. Regionalimmunotherapy and intrapleural BCG for lung cancer. J. Thorac. Cardiovasc.Surg., 72: 333-338, 1976.
16. Low, J., lies, P. B., Shore, D. F., Langman, J. K. J. S., and Baldwin, R. W.Intrapleural BCG in operable lung cancer. Lancet, /: 11-14, 1980.
17. Wright, P. W., Hill, L. D., Anderson, R. P. Hammer, S. P., Bernstein, I. D.,and Prentice, R. L. Immunotherapy of resectable nonsmall cell cancer of thelung: a prospective comparison of intrapleural BCG and Levamisol versusintrapleural BCG versus placebo. /;;: S. E. Salmon (ed.). Adjuvant Therapyof Cancer. New York: Elsevier/North Holland, 1977.
18. Matthay, R. A., Mahler, D. A., Mitchell, M. S., Carter, D. C., Loke, J.,Beck, G. J., Baue, A. E., and Reynolds, H. Y. Intratumoral BCG immuno-Iherapy prior to surgery for carcinoma of the lung: interim results. Proceedings of the 7th Asia-Pacific Congress on Diseases of the Chest, pp. 320-327.Hong Kong: Southeast Printing Co., 1983.
19. Matthay, R. A., Farmer, W. C., and Odero, C. Fiberoptic bronchoscopy inthe immunocompromised host. Thorax, 32: 538-545, 1977.
20. Mountain, C. F., Carr, D. T., and Anderson, W. A. D. A system for theclinical staging of lung cancer. Am. J. Roentgenol. Radium Ther. NucÃ.Med.,/: 130-138, 1974.
21. McKneally, M. F., Lininger, L., Kausel, H. W., Mcduff, J. B., Older, T. M.,Foster, E. D., and Ally, R. D. Four year follow-up on the Albany experiencewith intrapleural BCG in lung cancer. J. Thorac. Cardiovasc. Surg., 91:485-592, 1981.
22. Holmes, E. C., Ramming, K. P., Bein, M. E., Coulson, W. F., and Gallery,C. D. Intralesional BCG immunotherapy for pulmonary tumors. J. Thorac.Cardiovasc. Surg., 77: 362-368, 1979.
23. Lee, E. T. Statistical Methods for Survival Data Analysis. Belmont, CA:Lifetime Learning Publication, 1980.
24. Peto, R., Pike, M. C., Armitage, P., Breslow, N. E., Cos, D. R., Howard, S.V., Mantel, N., McPherson, K., Petg, J., and Smith, P. G. Design andanalysis of randomized clinical trials requiring prolonged observation of eachpatient. Br. J. Cancer, 35: 1-39, 1977.
25. Hayata, Y., Ohbo, K., Ogawa, I., and Taira, O. Immunotherapy for lungcancer cases using BCG or BCG cell-wall skeleton: intratumoral injections.Gann Monogr., 21: 151-160, 1978.
26. Mackaness, G. G., Auclair, P. J., and Lagrange, P.H. Immunopotentiationwith BCG. I. Immune response to different strains and preparations. J. Nati.Cancer Inst., 51: 1655-1667, 1972.
27. Mokyr, M. B., and Mitchell, M. D. Activation of BCG in vitro. Cell Immu-nol., 15: 164-273, 1975.
28. Cleveland, R. P., Meltzer, M. D., and Zbar, B. Tumor cytotoxicity in vitroby macrophages from mice infected with Mycobacterium bovis strain BCG.J. Nail. Cancer Inst., 52:1887-1895, 1974.
29. Mitchell, M. S., Kirkpatrick, D., Kokyr, M. B., and Gery, I. On the mode ofaction of BCG. Nature (Lond.), 243: 216-218, 1973.
30. Murahata, R. I., and Mitchell, M. S. Antagonism of immunosuppression byBCG. ¡n:M. A. Fink (ed.), The Macrophage in Neoplasia, pp. 263-265. NewYork: Academic Press, 1976.
31. Bennett, J. A., Rao, V. S., and Mitchell, M. S. Systemic Bacillus Calmette-Guérin(BCG) activates natural suppressor cells. Proc. Nati. Acad. Sci. USA,10: 5142-5144, 1979.
32. Morton, D. L., Eilber, F. R., Holmes, E. C., Hunt, J. S., Etchamm, A. S.,Silverstein, M. J., and Sparks, F. C. BCG immunotherapy of malignantmelanoma: summary of a seven-year experience. Ann. Surg., 180: 635-643,1974.
33. Rapp, J. H. A guinea pig model for tumor immunology. Isr. J. Med. Sci., 9:366-374, 1973.
34. Mokyr, M. B., Bennett, J. A., Braun, D. P., Genst, J. C. D., Mitchell, M. S.,and Dray, S. Opposite effects of different strains or batches of same strainof BCG on in vitro generation of syngeneic and allogeneic anlitumor cytotoxicity. J. Nati. Cancer Inst., 64: 339-344, 1980.
35. Bennett, J. A., Gruft, H., McKneally, M. F., Zelterman, D., and Christen,R. G. Differences in biological activity among batches of lyophilized miceBacillus Calmette-Guérinand their association with clinical course in StageI lung cancer. Cancer Res., 43: 4183-4190, 1983.
36. Armitage, P. Statistical Methods in Medical Research. New York: JohnWiley & Sons, 1971.
5968
on July 7, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1986;46:5963-5968. Cancer Res Richard A. Matthay, Donald A. Mahler, Gerald J. Beck, et al. Randomized TrialSurgery for Carcinoma of the Lung: Results of a Prospective
Immunotherapy prior toBacillus Calmette-GuérinIntratumoral
Updated version
http://cancerres.aacrjournals.org/content/46/11/5963
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/46/11/5963To request permission to re-use all or part of this article, use this link
on July 7, 2018. © 1986 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from