isolated medial hoffa fracture: a case series
TRANSCRIPT

IAR Journal of Medical Case Reports ISSN Print : 2709-3220 | ISSN Online : 2709-3239 Frequency : Bi-Monthly Language : English Origin : Kenya Website : https://www.iarconsortium.org/journal-info/iarjmcr
Available: https://iarconsortium.org/journal-info/iarjmcr 18
Isolated Medial Hoffa Fracture: A Case Series
Abstract: Introduction: Hoffa in 1904 first described fractures of the femoral condyle in tangential plane and are now known as Hoffa fractures. Approach to isolated medial Hoffa
fracture is, however, confusing. On reviewing literature, majority cases are operated using
parapatellar arthrotomy, some through a medial (subvastus) approach, and few was fixed percutaneously. Materials and Methods: We studied 6 patients of medial Hoffa fracture
presenting in Orthopedics department of Kalpana Chawala Government Medical College,
Karnal. They were evaluated radiologically with X-rays of knee anteroposterior and lateral
view. All patients were approached through subvastus approach, and were treated with
screws and buttress plating. The follow up of patients was done after 2 weeks, 1 month, 3 months and 6 months post operatively. Results: The age of the patients ranged from 27-31
(Mean 29 years). Mean range of motion was 125.83(range 120-130). All our patients had
radiological bony union at 6 months. Functional outcome was calculated by Knee society score which was average 84.16 (range 80-88), which comes under excellent category (80-
100). Conclusion: We concluded that outcome results of operated case of isolated medial
Hoffa’s fracture using medial subvastus approach and fixation of fracture with screws and buttress recon plate are excellent (as per knee society score).
Keywords: Hoffa’s fracture, Subvastus approach.
INTRODUCTION
Hoffa in 1904 first described fractures of the femoral condyle in
tangential plane and are now known as Hoffa fractures(Karim, A., &
Rossiter, N. 2006). They are classified as 33-B3.2 as per AO/OTA
classification(Dhillon, M. S. et al., 2012).
They can be described as intra-articular lateral or medial or bicondylar
fracture that occurs in the coronal plane of the distal femur hence
immediate needing the anatomical reduction with internal fixation as
early as possible(Karim, A., & Rossiter, N. 2006)
Lateral or bicondylar Hoffa fractures and well described in literature
in respect to classification, mechanism of injury, surgical approach,
reduction and fixation methods but Isolated coronal fracture of medial
femoral condyle, with intact lateral femoral condyle, is extremely rare and
barring a few isolated case reports(Ocguder, A. et al., 2008).
This is likely because of the often associated articular comminution,
associated injuries, the relative inaccessibility of the medial femoral
condyle articular surface, the difficulty associated with hardware
placement, and the magnitude of shear forces that must be resisted with
the fixation to avoid loss of fracture reduction(Viskontas, D. G. et al.,
2010).
The mechanism of injury for isolated medial Hoffa fracture is
controversial. Some authors described direct impact with the knee in a flexed position as the mechanism of injury, while
others have attributed the fracture to simultaneous vertical shear and twisting forces(2). Majority of these injuries are a
result of accidents two wheeler riding .The normal riding posture of the motor cyclist involves sitting with the knee
flexed at or beyond 90. In this position with slight abduction, lateral femoral condyle is the leading part of the knee to
receive a direct impact. Medial impact directly to the medial femoral condyle with the knee in greater than 90 of flexion
and an element of adduction and internal rotation can lead to medial Hoffa’s fracture(Lewis, S.L. 1989).
Diagnosis of this fracture is challenging and needs strong suspicion as this type of fracture is rare and misdiagnosis is
common. In cases of isolated fracture without any associated fractures of the knee, diagnosis should be based on physical
examination of skin lesions, oedema, effusion and careful radiological evaluation especially oblique views.
Research Art ic le
Article History
Received: 29.01.2021
Revision: 07.02.2021
Accepted: 15. 02.2021
Published: 28.02.2021
Author Details Dr. Devinder Kumar gupta1, Dr. Ambry garg*2,
Dr.Mohit Jindal3, Dr. Keerty Garg4, Dr. Varsha
Gupta5, Dr. Nikhil Gore6 and Dr. Navjyot Karda1
Authors Affiliations 1Medical Officer (Specialist) PCMS- 1, Civil
Hospital, Mohali, Punjab, India 2Senior resident, department of radiodiagnosis,
Kalpana chawla Government Medical College, Karnal Haryana, India 3Assistant professor, department of orthopedics,
Kalpana chawla Government Medical College, Karnal Haryana, India 4Assistant professor, department of Anaesthesia,
Kalpana chawla Government Medical College, Karnal Haryana, India 5Demonstrator, Department of community medicine, Kalpana Chawla Government medical college,
Karnal, Haryana, India 6Junior Resident, Department of orthopaedics, Kalpana Chawla Government medical college,
Karnal Haryana, India
Corresponding Author* Dr. Ambry garg
How to Cite the Article: Dr. Devinder Kumar gupta, Dr. Ambry garg*,
Dr.Mohit Jindal, Dr. Keerty Garg, Dr. Varsha
Gupta, Dr. Nikhil Gore & Dr. Navjyot Karda
(2021); Isolated Medial Hoffa Fracture: A
Case Series . IAR J Med Cse Rep. 2(1) 18-23.
Copyright @ 2021: This is an open-access article distributed under the terms of the Creative Commons Attribution license which permits unrestricted use, distribution, and reproduction in any medium for non commercial use (NonCommercial, or CC-BY-NC) provided the original author and source are credited.

Dr. Devinder Kumar gupta, et al., IAR J Med Cse Rep; Vol-2, Iss- 1 (Jan-Feb, 2021): 18-23
19
However, in cases with associated distal femoral
fractures, diagnosis of coronal fractures is quiet difficult
unless a strong index of suspicion is kept for the
same(Marzouki, A. et al., 2013).
The imaging evaluation of distal femoral fractures is
based primarily on radiographs. Supracondylar distal
femoral fractures may be classified as extraarticular,
unicondylar, or bicondylar, and the fractures may have
an intercondylar extension(Skaggs, D.L., & Flynn, J.M.
2014).
Nork et al., strongly recommended preoperative CT
scan in cases of supracondylar-intercondylar fractures
of the distal femur because of misdiagnosis on
conventional radiographs(Fractures, C.P. 2005).
Approach to isolated medial Hoffa fracture is,
however, confusing. On reviewing literature, majority
cases are operated using parapatellar arthrotomy, some
through a medial (subvastus) approach, and few was
fixed percutaneously(Viskontas, D. G. et al., 2010; &
Gao, M. et al., 2015).
MATERIALS AND METHODS
We studied 6 patients of medial Hoffa fracture
presenting in Orthopedics department of Kalpana
chawala government medical college, Karnal, Haryana.
They were evaluated radiologically with X-rays of knee
anteroposterior and lateral view (Figure- 3). Due to
financial constraints of patients CT scan couldn’t be
done. Of 6 patients 5 were male and one was female.
The average age of patients was 29 years (range 27-31
years).
After PAC and obtaining clearance for surgery
patients were taken up for surgery.
The operation was conducted under the guidance of
professional surgeons. The patient was placed supine on
a radiolucent table. Preoperative antibiotics and a
general or spinal anaesthetic were administered. A
tourniquet was placed around the ipsilateral thigh and
inflated at surgeon discretion. The knee was initially
placed in 20° of flexion over a towels and sheets.
All the fractures were treated by open reduction
through the medial subvastus approach is used through
an extensile longitudinal anterior skin incision
approximately 25 cm in length. (Figure-1)
Figure 1 Intra operative picture showing subvastus approach
And after exposure done the vastus medialis muscle,
sartorius muscle and saphenous nerve, which were
retracted forward to the anterior to explore the gracilis,
semimembranosus and semitendinosus muscles. After
that, the semimembranosus and semitendinosus were
retraced to the posterior and we could go through the
interval space between the gracilis muscle and caput
medial of the gastrocnemius to expose the fragment,
and then the origin of the medial collateral ligament
could be clearly exposed and protected. The intact
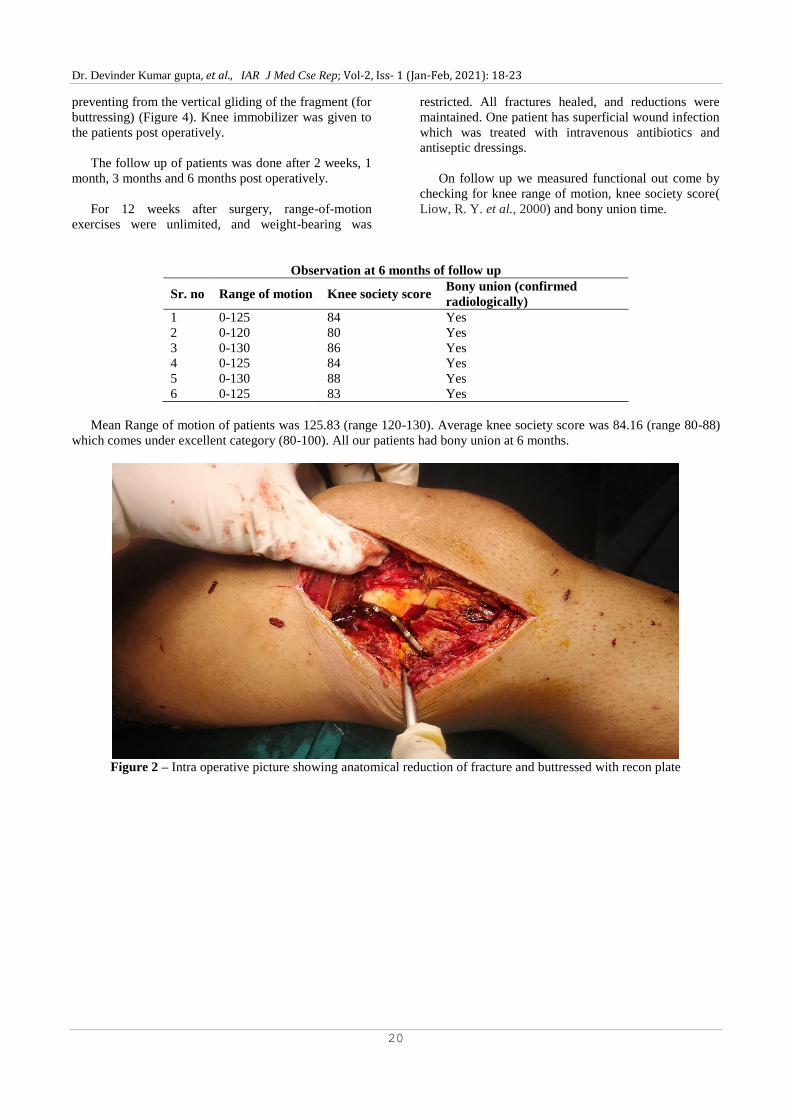
fragment of Hoffa fracture was reduced and fixed with
one or two cannulated or lag screws and meanwhile a
recon plate was anatomically contoured and used
(Figure - 2) for fixing with angular stability and also
Dr. Devinder Kumar gupta, et al., IAR J Med Cse Rep; Vol-2, Iss- 1 (Jan-Feb, 2021): 18-23
20
preventing from the vertical gliding of the fragment (for
buttressing) (Figure 4). Knee immobilizer was given to
the patients post operatively.
The follow up of patients was done after 2 weeks, 1
month, 3 months and 6 months post operatively.
For 12 weeks after surgery, range-of-motion
exercises were unlimited, and weight-bearing was
restricted. All fractures healed, and reductions were
maintained. One patient has superficial wound infection
which was treated with intravenous antibiotics and
antiseptic dressings.
On follow up we measured functional out come by
checking for knee range of motion, knee society score(
Liow, R. Y. et al., 2000) and bony union time.
Observation at 6 months of follow up
Sr. no Range of motion Knee society score Bony union (confirmed
radiologically)
1 0-125 84 Yes
2 0-120 80 Yes
3 0-130 86 Yes
4 0-125 84 Yes
5 0-130 88 Yes
6 0-125 83 Yes
Mean Range of motion of patients was 125.83 (range 120-130). Average knee society score was 84.16 (range 80-88)
which comes under excellent category (80-100). All our patients had bony union at 6 months.
Figure 2 – Intra operative picture showing anatomical reduction of fracture and buttressed with recon plate

Dr. Devinder Kumar gupta, et al., IAR J Med Cse Rep; Vol-2, Iss- 1 (Jan-Feb, 2021): 18-23
21
Figure- 3 Antero posterior and lateral radiograph of Left knee showing Isolated medial hoffas fracture
Figure 4- Immediate post operative anteroposterior and lateral radiograph of knee
Figure 5 – Anteroposterior and lateral radiograph of knee at 6 months follow up showing bony union.
DISCUSSION
An isolated coronal plane fracture of the
posteromedial distal femoral condylar was originally
described by Hoffa in 1904(Karim, A., & Rossiter, N.
2006).

Dr. Devinder Kumar gupta, et al., IAR J Med Cse Rep; Vol-2, Iss- 1 (Jan-Feb, 2021): 18-23
22
It is assumed to occur secondary to a high-energy
blunt force trauma that, applied to a flexed knee, causes
shearing of the posterior condyle (1904. HAL).
Associated injuries, which are common, occur in the
ipsilateral knee, lower extremity and more distant
locations (Viskontas, D. G. et al., 2010).
Unicondylar Hoffa fracture has been reported in
several studies (Holmes, S. M. et al., 2004; &
Ostermann, P. A. et al., 1994). However, few reports
about medial Hoffa fracture were shown in the
literature(Bali, K. et al., 2011; Chang, J. J. H. T. et al.,
2010; & Dhillon, M. S. et al., 2012).
Hoffa fractures are usually caused by motor
vehicular accidents. Until now, the injury mechanisms
of this fracture pattern have not been clearly described.
To detect the coronal fractures more accurately, CT
scanning is necessary to these fractures that might be
easily overlooked on plain radiographs. On the other
hand, CT scanning or MRI examination is essential to
find out a potential fracture and other accompanying
structure injuries ( Fractures, C.P. 2005). Ozturk
(Oztürk, A. et al., 2009) recorded a case of neglected
medial Hoffa fracture that was initially missed because
of seemingly normal anteroposterior (AP) radiographs
of the knee.
The medial Hoffa fracture is a kind of intra-articular
fracture, and most of these cases need operation
(Dhillon, M. S. et al., 2012; & Ostermann, P. A. et al.,
1994). Conservative management often leads to non-
union or loss of knee function (Oztürk, A. et al., 2009).
The surgical approaches are usually parapatellar
approaches (anteromedial), or combined with posterior
approaches, depending on the fracture classification and
fixation methods.
Several approaches and fixation methods for distal
femoral coronal fractures have been described, but most
descriptions involve treatment of lateral Hoffa
fragments. Previous descriptions of medial Hoffa
fracture surgical fixation are limited. Attempts at
fixation with a limited medial approach or a medial
parapatellar approach with the knee in extension can be
frustrating. The MCL lies over the typical coronal intra-
articular fracture plane and limits exposure and
reduction. Femoral distraction with the knee in
extension is limited in increasing visualization. In a
case report, Holmes and colleagues (Holmes, S. M. et
al., 2004) described using an anterior midline incision
with a medial parapatellar approach. Although the
parapatellar approach allows access for reduction
anteriorly, visualization of posterior comminution and
ease of reduction may be limited. A medial subvastus
approach allows extensile exposure of the articular
surface and, if needed, access to the posterior femoral
condyle— for placement of fixation in multiple planes.
The subvastus approach has been popularized by
Hofmann and colleagues (Hofmann, A. A. et al., 1991).
As far as we know, there was no clinical comparison
of different fixation methods on Hoffa fracture in the
literatures. Most of Hoffa fractures were treated with
cannulated screws or cancellous screws from anterior to
posterior or the opposite direction, and the clinical
outcomes were different (Holmes, S. M. et al., 2004;
Chang, J. J. H. T. et al., 2010; Oztürk, A. et al., 2009; &
Gavaskar, A. S. et al., 2011). It is generally accepted
that the screw heads are recessed beneath the articular
surface.
A biomechanical study showed that cannulated
screws placed from posterior to anterior provided more
stable fixation of Hoffa fractures in embalmed femurs
than anteroposteriorly placed cannulated screws(Jarit,
G. J. et al., 2006).
CONCLUSION-
We concluded that outcome results of operated case
of isolated medial Hoffa’s fracture using medial
subvastus approach and fixation of fracture with 6.5
cancellous cannulated screws and buttress recon plate
are excellent (as per knee society score). We obtained
very good range of motion (average 125.83) at 6
months follow up. We obtained radiological bony union
in 100% of our cases (fig 5).
Although conclusions about the long-term outcomes
of these injuries cannot be drawn, reduction and
fixation of these high-energy intra-articular injuries
using this surgical approach have been favourable and
may be useful for the medial Hoffa fracture.
REFERENCE
1. 1904. HAL der frakturen und L für Ä und SE. No
Title. 1904;
2. Bali, K., Mootha, A. K., Prabhakar, S., & Dhillon,
M. S. (2011). Isolated Hoffa fracture of the medial
femoral condyle in a skeletally immature
patient. Bulletin of the NYU hospital for joint
diseases, 69(4), 335–358.
3. Chang, J. J. H. T., Fan, J. C. H., Lam, H. Y.,
Cheung, K. Y., Chu, V. W. S., & Fung, K. Y.
(2010). Treatment of an osteoporotic Hoffa
fracture. Knee Surgery, Sports Traumatology,
Arthroscopy, 18(6), 784-786.
4. Dhillon, M. S., Mootha, A. K., Bali, K., Prabhakar,
S., Dhatt, S. S., & Kumar, V. (2012). Coronal
fractures of the medial femoral condyle: a series of
6 cases and review of literature. Musculoskeletal
surgery, 96(1), 49-54.
5. Fractures, C.P. (2005). Distal Femoral Fractures
and Coronal Plane Fractures. 564–569.

Dr. Devinder Kumar gupta, et al., IAR J Med Cse Rep; Vol-2, Iss- 1 (Jan-Feb, 2021): 18-23
23
6. GAO, M., Tao, J., Zhou, Z., Liu, Q., Du, L., & Shi,
J. (2015). Surgical treatment and rehabilitation of
medial Hoffa fracture fixed by locking plate and
additional screws: a retrospective cohort
study. International Journal of Surgery, 19, 95-
102. Available from:
http://dx.doi.org/10.1016/j.ijsu.2015.05.027
7. Gavaskar, A. S., Tummala, N. C., &
Krishnamurthy, M. (2011). Operative management
of Hoffa fractures—a prospective review of 18
patients. Injury, 42(12), 1495-1498.
8. Hofmann, A. A., Plaster, R. L., & Murdock, L. E.
(1991). Subvastus (Southern) approach for primary
total knee arthroplasty. Clinical orthopaedics and
related research, (269), 70-77.
9. Holmes, S. M., Bomback, D., & Baumgaertner, M.
R. (2004). Coronal fractures of the femoral
condyle: a brief report of five cases. Journal of
orthopaedic trauma, 18(5), 316-319.
10. Jarit, G. J., Kummer, F. J., Gibber, M. J., & Egol,
K. A. (2006). A mechanical evaluation of two
fixation methods using cancellous screws for
coronal fractures of the lateral condyle of the distal
femur (OTA type 33B). Journal of orthopaedic
trauma, 20(4), 273-276.
11. Karim, A., & Rossiter, N. (2006). Isolated medial
uni-condylar hoffa fracture following traumatic
knee dislocation. Injury Extra, 37(1), 12-14.
12. Lewis, S.L. (1989). Femoral accident. Surgery.
118–20.
13. Liow, R. Y., Walker, K., Wajid, M. A., Bedi, G., &
Lennox, C. M. (2000). The reliability of the
American Knee Society score. Acta Orthopaedica
Scandinavica, 71(6), 603-608.
14. Marzouki, A., Zizah, S., Benabid, M., Elassil, O.,
Lahrach, K., & Boutayeb, F. (2013). A rare case of
unicondylar medial Hoffa fracture associated with
ipsilateral vertical patella fracture. Journal of
clinical orthopaedics and trauma, 4(2), 102-105.
Available from:
http://dx.doi.org/10.1016/j.jcot.2013.01.003
15. Ocguder, A., Bozkurt, M., Kalkan, T., Ugurlu, M.,
& K? l? arslan, K. M. (2008). Hoffa fracture,
eminentia fracture and posterior cruciate ligament
damage: an unusual knee injury. Injury
extra, 39(3), 88-91.
16. Ostermann, P. A., Neumann, K., Ekkernkamp, A.,
& Muhr, G. (1994). Long term results of
unicondylar fractures of the femur. Journal of
orthopaedic trauma, 8(2), 142-146.
17. Oztürk, A., Ozkan, Y., & Ozdemir, R. M. (2009).
Nonunion of a Hoffa fracture in an adult. La
Chirurgia degli organi di movimento, 93(3), 183-
185.
18. Skaggs, D.L., & Flynn, J.M. (2014). Supracondylar
fractures of the distal humerus. Rockwood Wilkins’
Fract Child Eighth Ed. (April):2002–4.
19. Viskontas, D. G., Nork, S. E., Barei, D. P., &
Dunbar, R. (2010). Technique of reduction and
fixation of unicondylar medial Hoffa fracture. Am J
Orthop (Belle Mead NJ), 39(9), 424-428.