kelley - sasmhq.org10/30/14 1 plethysmography-derived respiratory rate scott d. kelley, m.d. chief...
TRANSCRIPT

10/30/14
1
Plethysmography-derived Respiratory Rate Scott D. Kelley, M.D. Chief Medical Officer Respiratory and Monitoring Solutions Covidien
Workshop: Postoperative Monitoring
Conflict of Interest Disclosure: Covidien Employee (Salary, Equity, Op<ons)
Manufacturer Nellcor™ Respira<on Rate
Respiratory Abnormali<es: A Warning Sign
1. Hillman KM, et al. Dura<on of life-‐threatening antecedents prior to intensive care admission. Intensive Care Med. 2002;28:1629-‐34. 2. Schein RM, et al. Clinical antecedent to in-‐hospital cardiopulmonary arrest. Chest. 1990;98:1388-‐92.
Reason for 551 ICU admissions from general ward 1
Abnormality %
Respiratory 33
Cardiovascular 20
Neurologic 14
Sepsis 13
Gastrointes<nal 9
Others 6
Trauma 1
Pathophysiologic altera=ons prior to cardiopulmonary arrest 2
Altera<on %
Respiratory 38
Mul<ple abnormali<es
27
Metabolic 11
Cardiac 9
Neurologic 6
Event Odds Ra=o (95% CI)
Bradypnea (RR < 6) 14.4 (2.6 -‐ 80.0)
Tachypnea (RR > 30) 7.2 (3.9 -‐ 13.2)
Loss of consciousness 6.4 (2.9 -‐ 13.6)
Decrease of consciousness 6.4 (2.6 -‐ 15.7)
Hypotension 2.5 (1.6 -‐ 4.1)
Hypoxemia (SpO2 < 90%) 2.4 (1.6 -‐ 4.1)
Extremes in Respiratory Rate Predict Mortality
Extremes of respira=on rate are strong predictors of in-‐hospital mortality on the general ward
Buist M, et al. Associa<on between clinically abnormal observa<ons and subsequent in-‐hospital mortality: a prospec<ve study. Resuscita2on. 2004;62(2):137-‐141.
Prospec<ve study of 6,303 pa<ents on the general hospital ward.
Independent Predictors of Mortality

10/30/14
2
Gaps: Respira<on Rate Monitoring on the GCF • “The main problem iden<fied when ademp<ng to introduce an early warning system to the acute general ward areas in one hospital was the general paucity of monitoring of pa<ent observa<ons by the nursing team. ” 1 Ø Respira<on Rate: only parameter recorded <50% of the <me1
• Clinically-‐collected values miss a number of events2
1. Hogan. British Journal of Nursing. 2006;15(9):489-91.
2. Curry et al. Anesthesiology 2002; 96:A1173.
Detection & Threshold # of Events Rate (per hour)
Charted spot-check SpO2 < 90% 9 0.0037
Continuous Oximetry SpO2< 90% 1213 0.497
Respira<on Produces Photoplethysmogram Changes
Spontaneous respira=on
produces well-‐characterized PPG modula=ons1
1. Meredith DJ, Clihon D, Charlton P, Brooks J, Pugh CW, Tarassenko L. Photoplethysmographic deriva<on of respiratory rate: a review of relevant physiology. J Med Eng Technol 2012;36:1-‐7
Respira<on Related Changes in Photoplethysmogram
Baseline Modulation
Ligh
t Tra
nsm
issi
on
Frequency ModulationExpireLi
ght T
rans
mis
sion
Amplitude Modulation
Ligh
t Tra
nsm
issi
on
Central Respiratory Drive
↑ Heart Rate ↓ Stroke Volume ↑ Venous Return
↓ Intrathoracic Pressure
Diaphragm
Meredith DJ, Clifton D, Charlton P, Brooks J, Pugh CW, Tarassenko L. Photoplethysmographic derivation of respiratory rate: a review of relevant physiology. J Med Eng Technol 2012;36:1-7

10/30/14
3
Photo Pleth Signal
Respiration Features
Baseline Modula<on
Amplitude modula<on
Respiratory sinus arrhythmia
Wavelet Transform Autocorrela<on
Signal Processing
Pleth-‐based Respira<on Rate Fundamentals
Respira<on Components
Pleth-‐based Respira<on Rate Technology Algorithm-‐based Averaging Approach
= RRX+1
= RRX+2
= RRX+3
A respiration rate is calculated every 5 seconds = RRX
“Averaging window” = 45 seconds
Reported rate ( @ X+3) = Weighted average of RRX, RRX+1, RRX+2, RRX+3, with additional logic
1. Addison et al. (2012) Developing an algorithm for pulse oximetry derived respiratory rate (RRoxi): a healthy volunteer study. J Clin Monit Comput; 26(1): 45-51.
Pleth-based Respiration Rate Accuracy (General Care Floor Patients)
Distribu=on of Differences Between RRPLETH and RRETCO2
Bland-‐Altman Density Plot
Addison PS, Watson JN, Mestek ML, Ochs JP, Uribe AA, Bergese SD. Pulse oximetry-derived respiratory rate in general care floor patients. J Clin Monit Comput. May 6, 2014.
• N= 63 pa<ents • Range of respira<on rates:4.7 to 32.0 breaths per minute. • 16,980 paired observa<ons between pleth-‐based Respira<on Rate
and capnography-‐based reference
LOW
POINT DEN
SITY
HIGH

10/30/14
4
Pleth-based Respiration Rate Accuracy
Study N Setting Results (BrPM)
Mean Diff S.D. RMSD
FDA Submission Trial* 53 Hospital GCF Cohort 0.1 1.98 1.98
26 Healthy Volunteer Cohort 0.37 0.78 0.96
79 Combined GCF & Healthy 0.18 1.65 1.66
J.Clin Mon & Comp. 2012 139 Adult Healthy Volunteers -0.23 1.14 1.16
J.Clin Mon & Comp. 2014 63 GCF Patients -0.48 1.77 1.83
CHEST 2012 22 COPD 0.7 1.6 1.74
CHEST 2012 12 CHF 0.4 1.5 1.55
ASA 2012 12 PACU -0.5 0.7 0.86
ASA 2012 17 Obese volunteers 0.07 1.8 1.8
IAMPOV 2012 12 Cold Room Hypoxia Study -0.18 0.72 0.74
Pleth-‐based respira<on rate has an accuracy (mean diff) of ± 1 breaths per min when compared to respira<on rate derived from a capnography-‐based reference
* Nellcor™ Respira<on Rate Product labeling, US 510(k) cleared (K111933). Studies yielded 23,243 paired observa<ons. Range of respira<on rates observed was 4 to 34 breaths per minute. RMSD = root mean square devia<on. ClinicalTrials.gov NCT01804062 Addison et al. (2012) Developing an algorithm for pulse oximetry derived respiratory rate (RRoxi): a healthy volunteer study. J Clin Monit Comput; 26(1): 45-‐51Addison PS et al, Pulse oximetry-‐derived respiratory rate in general care floor pa<ents. J Clin Monit Comput. May 6, 2014. Mestek ML et al. Accuracy of Con<nuous Non-‐invasive Respiratory Rate Derived from Pulse Oximetry in Obese Subjects. Abstract A561, AASA 2012 Annual Mee<ng; Mestek ML et al. Accuracy of Con<nuous Noninvasive Respiratory Rate Derived From Pulse Oximetry in Conges<ve Heart Failure Pa<ents. Abstract 113A Chest. 2012;142:113A. Mestek ML et al. Accuracy of Con<nuous Noninvasive Respiratory Rate Derived From Pulse Oximetry in Chronic Obstruc<ve Pulmonary Disease Pa<ents. Abstract 142:671A. Chest. 2012
Commercially Available Pleth-based Respiration Rate Monitoring (Nellcor™ Respiration Rate Technology)
Commercially Available Pleth-based Respiration Rate Monitoring (Nellcor™ Respiration Rate Technology)
• Con=nuous, noninvasive monitoring of respira=on rate on adult pa=ents
• Yields SpO2, Pulse Rate, Respira=on Rate from a single pulse ox sensor
• Nellcor Respira=on Rate Version 1 (FDA cleared): – Respira<on Rate sohware and Adult Respiratory Sensor – Bedside Respiratory Pa<ent Monitoring System with Respira<on Rate – SpO2 PCBA with Respira<on Rate for OEM Integra<on
• Respira=on Rate Version 2 (FDA 510(k) Pending): – Algorithm changes addressing: • Time to pos<ng first Respira<on Rate measurement • Accuracy at low and high RR • Response <me to changes in RR • Reliability during disturbance condi<ons (e.g., mo<on, talking)
– User interface: Adjustable RR alarm limits (range 4-‐40 breaths/minute) – CE Mark: June 2014

10/30/14
5
700 720 740 760 780 800 820 8400
100
200
300
400
EtCO
2
700 720 740 760 780 800 820 8405
10
15
20
25
30
time (seconds)
RR
(/m
in)
TTI CO2 RR V1 V2
700 720 740 760 780 800 820 8400
100
200
300
400
EtCO
2
700 720 740 760 780 800 820 8405
10
15
20
25
30
time (seconds)
RR
(/m
in)
TTI CO2 RR V1 V2
25 breaths / min 11 breaths / min
Response Time to Changes in Respiration Rate • Pleth-‐based RespRate is not a breath by breath measure
• An averaging window (≈ 45 sec) supports overall accuracy • Response <me to step change is similar to other devices (~1 minute)
~ 1 min
*Covidien Internal Data
Variable Baseline Opioid Infusion
Detect OIRD (RR<8; SpO2↓3%)
Pleth-‐RespRate (BrPM) 13.1 ± 3.1 6.8 ± 0.8* 12/12
SpO2 (%) 99.7 ± 0.7 98.9 ± 1.8 3/12
Opioid-‐Induced Respiratory Depression1
Kelley SD, Neitenbach AM, AR Kinney AR, Mestek ML. Detec<on of Opioid-‐Induced Respiratory Depression with Pulse Oximetry-‐Derived Respiratory Rate Monitoring Abstract A095, ASA 2012 Annual Mee<ng
Remifentanil Infusion Recovery
Opioid-‐Induced Respiratory Depression -‐ Central Apnea
1500 2000 2500 30000
20
40
60
EtCO2
1500 2000 2500 3000
5
10
15
20
25
time (sec)
RR
(B
rPM
)
reference V2
1500 2000 2500 30000
20
40
60
EtCO2
1500 2000 2500 3000
5
10
15
20
25
time (sec)
RR
(B
rPM
)
reference V2~60 second apnea
Audible RR Alarms
reference PlethRR EtCO2 RR
*Covidien Internal Data
Remifentanil Infusion
Audible RR Alarms

10/30/14
6
Limita<ons of Pleth-‐based Respira<on Rate • Respira=on Rate uses the same pleth signal as SpO2 and relies on informa=on derived from Pulse Oximetry.
• A Respira=on Rate value will only be calculated if the pleth signal is sufficient for pulse oximetry.
• Challenges to SpO2 Performance – Mo<on – Low Perfusion – Electrosta<c Interference – Dyes / Nail Polish / Pigmenta<on – Strong ambient lights
Pulse Oximetry
Respiration Rate
Pleth
• Motion inherently more challenging for Respiration Rate than Pulse
Oximetry. – Pulse Oximetry can use short, intermittent periods of quiescence to attenuate
and read through neighboring interference (cardiac-gated averaging)
– Longer time intervals associated with RR monitoring means fewer sections of unperturbed pleth signal for respiration rate analysis.
• Talking (not shown here) is handled similarly to motion
Mo<on (and Talking)
490 495 500 505 510 515 520 525 530
4
4.2
4.4
4.6
4.8
5
5.2
5.4
5.6x 105
Period of calm
Period of noise
45 second window
*Covidien Internal Data
IR P
PG
Am
plitu
de
145 150 155 160 165 1700
100
200
300
400
500
600
time (seconds)
CO2
145 150 155 160 165 170
4
4.05
4.1
4.15
4.2
4.25
4.3
4.35
4.4
4.45
x 105
time (seconds)
light
inte
nsity
Respiratory Sinus Arrhythmia One breath with very large pulse amplitude and pulse period modulations
• Strong Sinus Arrhythmia provides a key respiratory-based modulation.
• Strong and frequent pulse amplitude modulations during certain arrhythmias can overpower respiratory-based modulations and decrease pleth-based Respiration Rate accuracy. (e.g. > 6 PVCs in 60 sec)
Arrhythmia
240 245 250 255 260 265 270 275 280 285 2900
50
100
150
200
250
300
350
400
time (seconds)
CO2
240 245 250 255 260 265 270 275 280 285 290
4.8
5
5.2
5.4
5.6
5.8x 105
time (seconds)
light
inte
nsity
Premature Ventricular Contractions Large, fairly regular, pulse amplitude and frequency modulations that are NOT due to breathing
*Covidien Internal Data
10/30/14
7
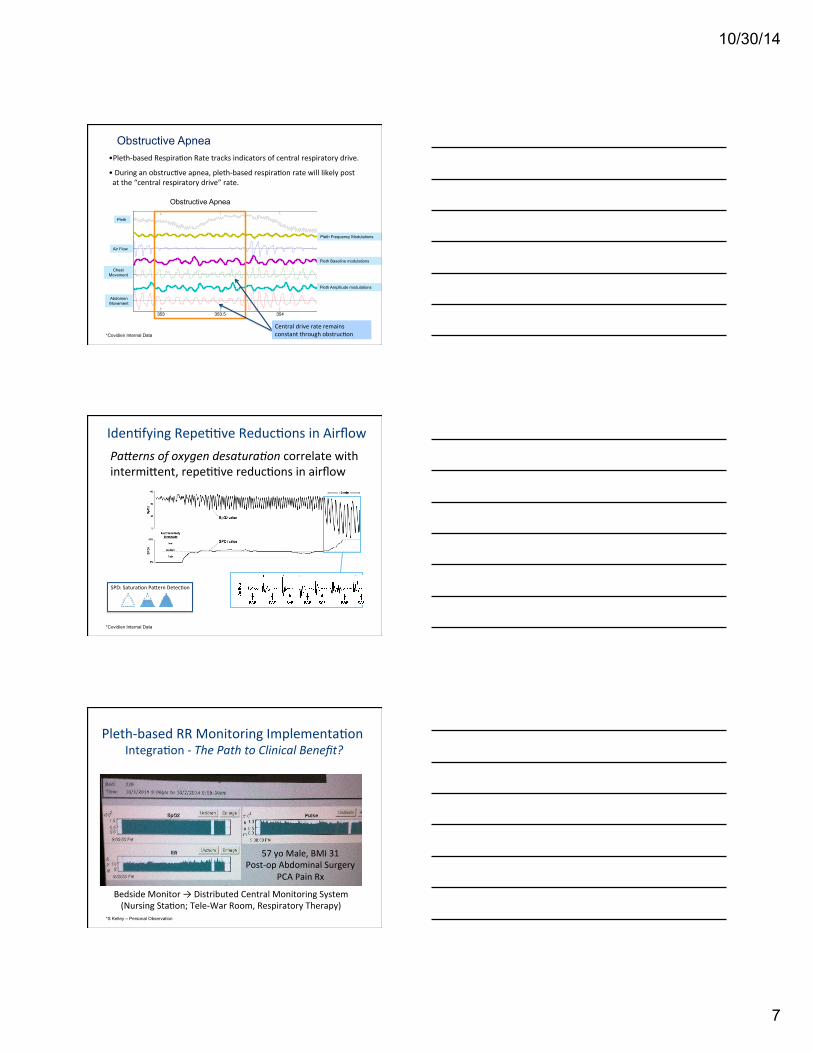
Obstructive Apnea
353 353.5 354 354.5 355
AB
Chest
Air FlowAir Flow
Pleth Frequency Modulations
Obstructive Apnea
Pleth Baseline modulations
Pleth Amplitude modulations
Chest Movement
Abdomen Movement
• Pleth-‐based Respira<on Rate tracks indicators of central respiratory drive.
• During an obstruc<ve apnea, pleth-‐based respira<on rate will likely post at the “central respiratory drive” rate.
Pleth
Central drive rate remains constant through obstruc<on *Covidien Internal Data
Iden<fying Repe<<ve Reduc<ons in Airflow Pa=erns of oxygen desatura2on correlate with intermident, repe<<ve reduc<ons in airflow
*Covidien Internal Data
SPD: Satura<on Padern Detec<on
Pleth-‐based RR Monitoring Implementa<on Integra<on -‐ The Path to Clinical Benefit?
Bedside Monitor → Distributed Central Monitoring System (Nursing Sta<on; Tele-‐War Room, Respiratory Therapy)
57 yo Male, BMI 31 Post-‐op Abdominal Surgery
PCA Pain Rx
*S Kelley – Personal Observation

10/30/14
8
Assessing Respira<on Rate /Ven<la<on Monitors
Pleth-‐RR ü ü ∅ ü ü Pending
Acous<c-‐RR
Exhaled CO2
Minute Ven<la<on
ECG-‐TTI
Manual Observa<on
Trends Re
spira<on
Single Sensor SpO 2 + R
R
Clinical Benefit Evide
nce
Comfortable
Accurate
Breath by breath
Improving Postopera<ve Monitoring
What remains to be established, however, is the level of performance (accuracy, response <me, persistence of discrepancy) required for these devices to have clinical benefits in different areas of care. However, given the current lack of respira<on rate monitoring on the general care floor, it is likely that the available devices are sufficiently accurate for implementa<on into con<nuous monitoring care strategies. The cri<cal evidence needed is to assess whether the addi<on of con<nuous respira<on rate monitoring can further enhance pa<ent safety and outcomes when u<lized.
Anesthesia & Analgesia 2014 (in press)
Pleth-based Respiration Rate: Summary
Respiration Rate – Important and overlooked! ü Predictor: Patient deterioration & demise ü Respiratory rate – even intermittent – often not charted
A pleth-based solution measures Respiration Rate ü Commercially available ü Clinically acceptable accuracy: ± 1 BrPM ü Simple integration into pulse oximetry work-flow ü Combined with oximetry: enhanced patient information ü Recognized limitations: opportunities for improvement
Continuous Respiration Rate Monitoring ü Poised to mitigate complications and thereby improve both
clinical and financial outcomes. ü Needed: evidence generation of application & value