key contributors dr. napoleon knight dr. daniel picchietti dr. charles davies bill vogel pam...
TRANSCRIPT

Key Contributors• Dr. Napoleon Knight• Dr. Daniel Picchietti• Dr. Charles Davies• Bill Vogel• Pam Manselle• Jan Hastings• Cathy Short• Dr. Shalu Manchanda
On-going Improvements• The nursing educator is working directly with
nursing champions on the floor to continue to educate nursing staff about the need to observe patients for apnea if they desaturate and this is being tracked going forward with a report that is developed in the EMR. Further reports will also be collected directly
• Working on decreasing the Oximeter alarm volumes in patient rooms due to noise complaints (Figure 8). Thus, ensuring that RT checks carefully to make sure that when they are used on another patient the alarm limit is raised again.
• Educating our new hospitalists and physician assistants to use the sleep apnea evaluation tool, so patients who screen positive are having appropriate follow-up studies.
Data
• Created a screening tool in the EMR to evaluate patients being admitted to the hospital ( Figure 3)
• Created a documentation tool in the EMR that the hospitalists use to serve as appropriate documentation for outpatient sleep lab scheduling (Figure 4)
• Created a discharge tool in the EMR to ensure appropriate scheduling for outpatient sleep studies (Figure 5)
• Worked with our referring physician clinics to implement a sleep apnea screening tool for use in the outpatient environment
• Implemented a bridge program so patients who were placed on AutoPap machines would be allowed to use them until their sleep studies were done as an outpatient
• Changed hospital formulary substituting Zolpedam for Temazepam
Implemented Program Initiatives
• Evaluated several sleep apnea screening tools, to find one with appropriate specificity, sensitivity, and ease of use
• Utilized a nursing satisfaction tool as the screening tool was developed to make sure it was something that was easy to use
• Created a nursing, patient, and RT educational program to make family and staff members aware of the additional risk of sleep apnea for patients in the hospital environment
• Put together a support team at the time of roll out to ensure there was adequate support for nursing, RT, and physicians
• Implemented the use of AutoPap on patients with unknown sleep apnea after trialing it in the known sleep apnea population to verify its effectiveness
Program Development Outcomes• Increased the number of patients who screen
positive and are monitored on pulse oximeters (Figure 6)
• More patients and family members recognizing OSA symptoms and notifying the nursing staff
• No Code Speed events or respiratory related deaths due to suspected sleep apnea (Figure 7)
• Alarms on oximeters serve as protective feature in waking apneic patients (Figure 8)
Obstructive Sleep Apnea: An Under-Recognized Hospital Danger Carle Foundation Hospital, Urbana, Illinois
Dr. Napoleon Knight
IntroductionObstructive sleep apnea (OSA) is a
disorder that exists in a much higher percentage of patients than the general public and the medical community is aware of. It continues to be undiagnosed due to this lack of understanding and education. Contributing to the problem is the growing epidemic of obesity in this country, which adds significantly to the patient population at risk for this disorder (Figure 1). In the literature there are many studies dealing with sleep apnea in the surgical population. There are fewer studies dealing specifically with undiagnosed sleep apnea in the medical population and non-bariatric surgical population.
Source: CDC Behavioral Risk Factor Surveillance System.
1999
Obesity Trends* Among U.S. AdultsBRFSS, 1990, 1999, 2008
(* BMI 30, or about 30 lbs. overweight for 5’4” person)
2008
1990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
GoalDue to observations of patients at our
institution having morbidity and mortality from suspected unrecognized sleep apnea, as well as dollars lost in litigation, we evaluated and implemented a patient safety program to care for patients with undiagnosed sleep apnea.
Pre-Implementation DataUsed EMR data to evaluate the presenting
weights of patients being admitted or treated in our facility to demonstrate need (Figure 2).
Non-Pediatric/Non-OB BMI Data
Total Patients 51
Percentage BMI > 30 100%
Percentage BMI > 35 41.00%
Percentage BMI > 40 16.70%
Lowest BMI 30.12
Highest BMI 66.03
Average BMI 36.59
Pre-Screening Tool
ImplementationPost- Screening Tool
Implementation
July 27, 2009 thru August 10, 2009
October 1, 2009 thru October 15, 2009
Positive 34% 42%
Negative 34% 33%
Known 11% 7%
Not Screened 21% 18%
Total Volume 603 595
0.0
2.0
4.0
6.0
8.0
10.0
Pre-Screening ToolImplementation
Post-Screening ToolImplementation
Average number of AutoPaps in use per day
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
Pre-Screening ToolImplementation
Post-Screening ToolImplementation
Average Number of Patients on Oximetry per day
0
10
20
30
40
On Autopap Refused Autopap
Average Length of Longest Desaturation
Volume Comparable To
Normal room noise (daytime) 65Db Restaurant
Volume level 1+ 66Db Restaurant
Volume level 7+ 85Db City Traffic
50Db Normal Household
Codes Aug. 2009- Jan.2010
# Sleep Apnea Related
Code Speed 6 0/6
Code 99 5 0/5
Figure 3
Figure 4
Figure 5
Figure 6
Figure 7
Figure 8
Figure 1
Figure 2
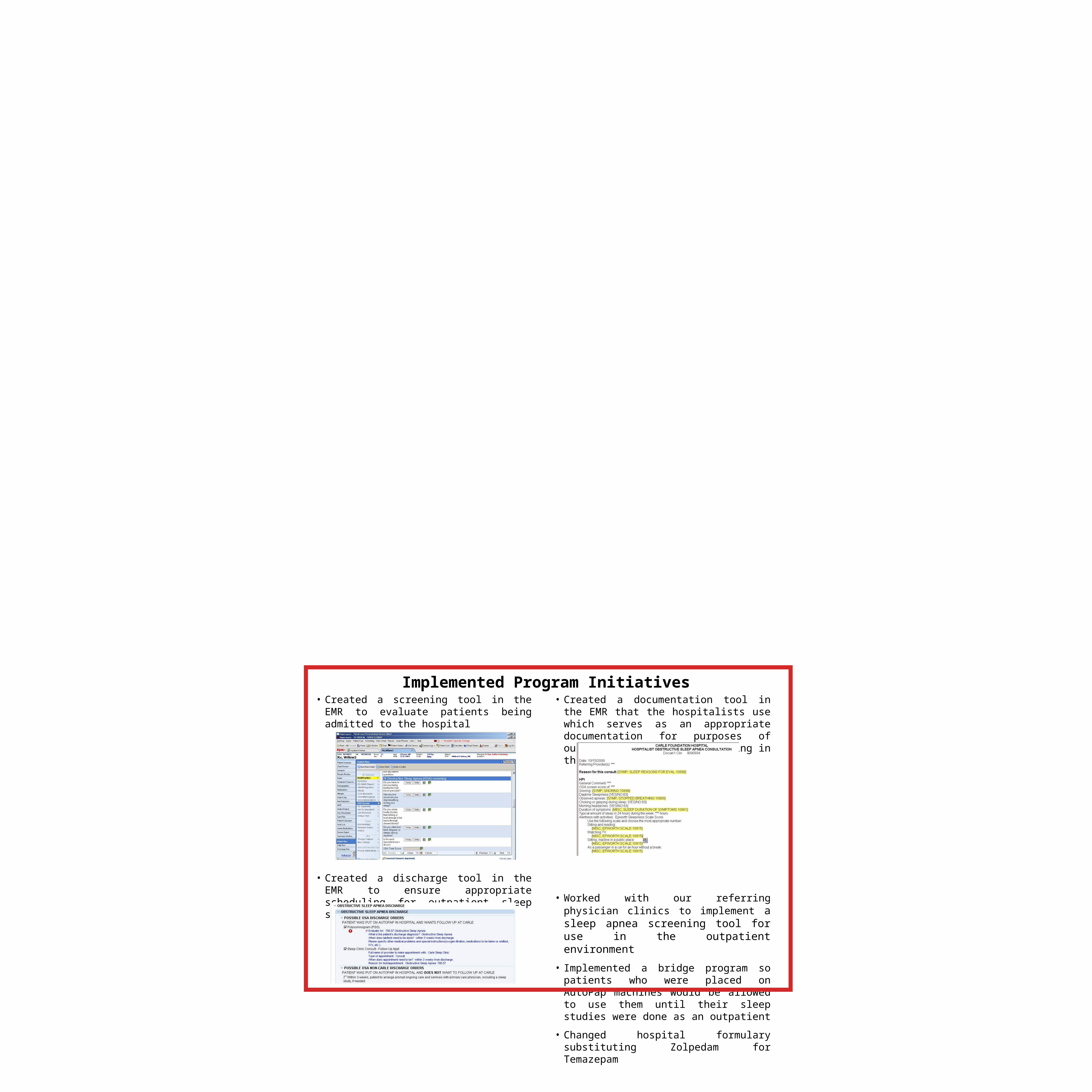
• Created a screening tool in the EMR to evaluate patients being admitted to the hospital
• Created a discharge tool in the EMR to ensure appropriate scheduling for outpatient sleep studies
• Created a documentation tool in the EMR that the hospitalists use which serves as an appropriate documentation for purposes of outpatient sleep lab scheduling in the future
• Worked with our referring physician clinics to implement a sleep apnea screening tool for use in the outpatient environment
• Implemented a bridge program so patients who were placed on AutoPap machines would be allowed to use them until their sleep studies were done as an outpatient
• Changed hospital formulary substituting Zolpedam for Temazepam
Implemented Program Initiatives