knee tissue strains and effectiveness of a novel ... · ii knee tissue strains and effectiveness of...
TRANSCRIPT

Knee Tissue Strains and Effectiveness of a Novel Functional ACL Knee Brace during Dynamic In-Vitro
Loading
by
Stefan Sebastian Tomescu
A thesis submitted in conformity with the requirements for the degree of Master of Science
Institute of Medical Science
University of Toronto
© Copyright by Stefan Sebastian Tomescu, 2017

ii
Knee Tissue Strains and Effectiveness of a Novel Functional
ACL Knee Brace during Dynamic In-Vitro Loading
Stefan Sebastian Tomescu
Master of Science
Institute of Medical Science
University of Toronto
2017
Abstract
Functional knee braces are commonly prescribed to help stabilize and protect the knee after an
ACL injury or reconstruction. Newer brace designs employ a dynamic tensioning system to
apply directional forces to the knee. The purpose of this thesis was to characterize meniscal
loading under dynamic loading conditions and test the efficacy of a functional knee brace
equipped with a dynamic tensioning system to reduce ACL and meniscal strain. A combined in-
vivo/in-silico/in-vitro testing method was used to quantify tissue strains and the effect of the
brace on cadaveric specimens. Tissue strains were quantified and validated before and after
reconstruction, and the brace was found to lower tissue strains during most conditions. This work
provides supportive evidence for the use of braces with a dynamic tensioning system for patients
who are ACL deficient or following reconstruction.
iii
Acknowledgments
There are many individuals without whom this thesis may not have come to fruition. Firstly, I’d
like to thank my supervisor, Dr. Cari Whyne, and supervisory collaborator, Dr. Naveen
Chandrashekar, who have aided in overseeing and guiding all aspects of this thesis. Dr. Cari
Whyne has been both a direct supervisor of this work and a research mentor for my professional
career. Her skill and experience as a scientific researcher has helped steer this thesis in the right
direction, even when that direction wasn’t always clear. Dr. Naveen Chandrashekar, has not only
provided the necessary knowledge to complete this thesis, but continuously aided to enhance the
quality of the work being done, and the possibilities for further involvement in biomechanical
research. He also connected me with a network of support for this research and other endeavors
outside of the thesis, ensuring that I have opportunity to expand my research career under his
support. Both Cari and Naveen’s mentorship and support have made this thesis a positive
learning experience.
I’d like to also express gratitude to the other individuals that are members of my thesis
committee, Dr. Emil Schemitsch and Dr. Tyson Beach. Dr. Emil Schemitsch kindly agreed to be
part of this committee and worked on fitting each meeting into his demanding surgical and
administrative career. His critical input and expertise have contributed significantly to enriching
the work. I also thank Dr. Schemitsch for continuing to be involved even after relocating to
University of Western. Dr. Tyson Beach has offered both his time and expertise in Biomechanics
in aid of this project. His knowledge in the field added positively to discussion and helped
significantly broaden my experience in Biomechanics.
There were many people that were integral to the completion of this thesis, but none more so
than my lab mate Mr. Ryan Bakker. Ryan was instrumental in all phases of the thesis, devoting
his training, knowledge and time to aid in the computer simulations, cadaver preparation, and
testing. Without his experience, the testing may not have been successful. Additionally, Ryan
kindly spent many hours discussing and ironing out the details of the work with me. I’m glad that
in working with Ryan I have gained not only a lab mate and professional colleague, but also a
friend.
iv
Finally, I’d like to dedicate this thesis to my family, whose sacrifices, support and
encouragement have enabled me throughout this research. My parents, Drs. Mihaila and Stefan
Tomescu, and my grandmother, Mrs. Maria Traistaru, have sacrificed much to provide me with
the opportunities to pursue my career, and without them I would not be where I am today. I’d
also like to thank my wife, Mrs. Jelena Tomescu, to whom I became engaged and married in the
process of completing this thesis. She has been a supportive and enthusiastic partner, comforting
me during times of stress and celebrating with me every small accomplishment and success. I’d
also like to thank my parents in-law, Mr. Milutin and Mrs. Kata Zaric, for their generosity and
kindness. It is all these individuals and their continued support, both professional and personal,
that made this experience rewarding and enjoyable.
v
Contributions
Many lab mates, technicians, experts and helpers aided and assisted in this project both directly
and indirectly.
I’d like to thank the following for their specific contributions to this work:
Dr. David Wasserstein for connecting me with the funding partner,
Mr. Micah Nicholls, our partner at Össur Inc., for his brace insights and study design,
Mrs. Helen Chong for helping with the initial phases of data collection in the motion
capture lab,
Mr. Gajendra Hangalur and Mr. Mayank Kalra for their important contributions
throughout the preparation and testing of the cadavers,
Mr. Adam Zhang, Mr. Liu He, Ms. Ania Polak, Mr. Nokhez Qazi, Mr. Neil Griffet, and
Mr. Tom Gawel for offering a helping hand with the lab work,
and to Össur Inc for providing the necessary funding and braces to complete this work.
Additional funding was received from NSERC, the Susanne and William Holland Surgeon
Scientist Award GSEF, and the Queen Elizabeth II/Wellesley Surgeons Graduate Scholarships in
Science and Technology.
vi
Table of Contents
Acknowledgments........................................................................................................................... iii
Contributions.................................................................................................................................... v
Table of Contents ............................................................................................................................ vi
List of Appendices .......................................................................................................................... ix
List of Figures .................................................................................................................................. x
List of Tables ................................................................................................................................ xiv
List of Abbreviations ..................................................................................................................... xv
Chapter 1 Literature Review .......................................................................................................1 1
1.1 Human Body and Anatomy ......................................................................................................1
1.1.1 Anatomical Orientation............................................................................................1
1.1.2 General Knee Anatomy............................................................................................2
1.1.3 Anatomy and Function of the Anterior Cruciate Ligament .....................................3
1.1.4 Meniscal Anatomy and Function .............................................................................4
1.2 ACL injury ................................................................................................................................6
1.2.1 Risk Factors..............................................................................................................6
1.2.2 Treatment Options....................................................................................................7
1.3 Bracing......................................................................................................................................9
1.3.1 Prophylactic Braces..................................................................................................9
1.3.2 Functional Knee Braces .........................................................................................10
1.3.3 Dynamic Tensioning Systems................................................................................12
1.3.4 Neuromuscular Effects of Bracing.........................................................................13
1.4 Testing Methodologies ...........................................................................................................14
vii
1.4.1 In-Vivo ...................................................................................................................14
1.4.2 In-Silico..................................................................................................................15
1.4.3 In-Vitro...................................................................................................................15
1.4.4 Strain Measurement Techniques ............................................................................17
1.4.5 In-Vitro Knee Brace Testing..................................................................................19
Chapter 2 Hypotheses and Research Aims ...............................................................................21 2
2.1 Thesis Rationale......................................................................................................................21
2.2 Thesis Hypothesis ...................................................................................................................22
2.3 Thesis Outline .........................................................................................................................22
Chapter 3 Dynamic Meniscal and ACL Strains are Maintained Following ACL 3Reconstruction...........................................................................................................................24
3.1 Introduction.............................................................................................................................25
3.2 Methodology ...........................................................................................................................26
3.3 Results.....................................................................................................................................29
3.4 Discussion ...............................................................................................................................30
Chapter 4 Efficacy of an ACL Functional Knee Brace with a Dynamic Tension System .......40 4
4.1 Introduction.............................................................................................................................41
4.2 Materials and Methods ...........................................................................................................42
4.3 Results.....................................................................................................................................45
4.4 Discussion ...............................................................................................................................46
4.5 Summary/Conclusions ............................................................................................................50
Chapter 5 General Discussion ...................................................................................................54 5
5.1 Summary and Discussion .......................................................................................................54
5.2 Contributions ..........................................................................................................................56
5.3 Future Directions ....................................................................................................................57

viii
References .................................................................................................................................59 6
Appendix 1: Cadaver Preparation .............................................................................................76 7
7.1 Dissection ...............................................................................................................................76
7.2 Muscle Cable Insertion ...........................................................................................................77
7.3 Foaming Procedure .................................................................................................................78
7.4 Moment Arm Calculations .....................................................................................................84
Appendix 2: Pilot Testing .........................................................................................................87 8
8.1 Pilot 1 ......................................................................................................................................87
8.2 Pilot 2 ......................................................................................................................................92
8.3 Pilot 3 ......................................................................................................................................95

ix
List of Appendices
Appendix 1: Cadaver Preparation ..................................................................................................76
Appendix 2: Pilot Testing ..............................................................................................................87

x
List of Figures
Figure 1. Knee Ligament Anatomy ................................................................................................ 3
Figure 2. ACL Anatomy. ACL fibers are marked in consecutive order (A-C) with the knee in
zero degrees of flexion. Fibers reorganize as the knee flexes to 90 degrees. Apostrophe denotes
distal fiber endings. ......................................................................................................................... 4
Figure 3. Meniscal Anatomy........................................................................................................... 5
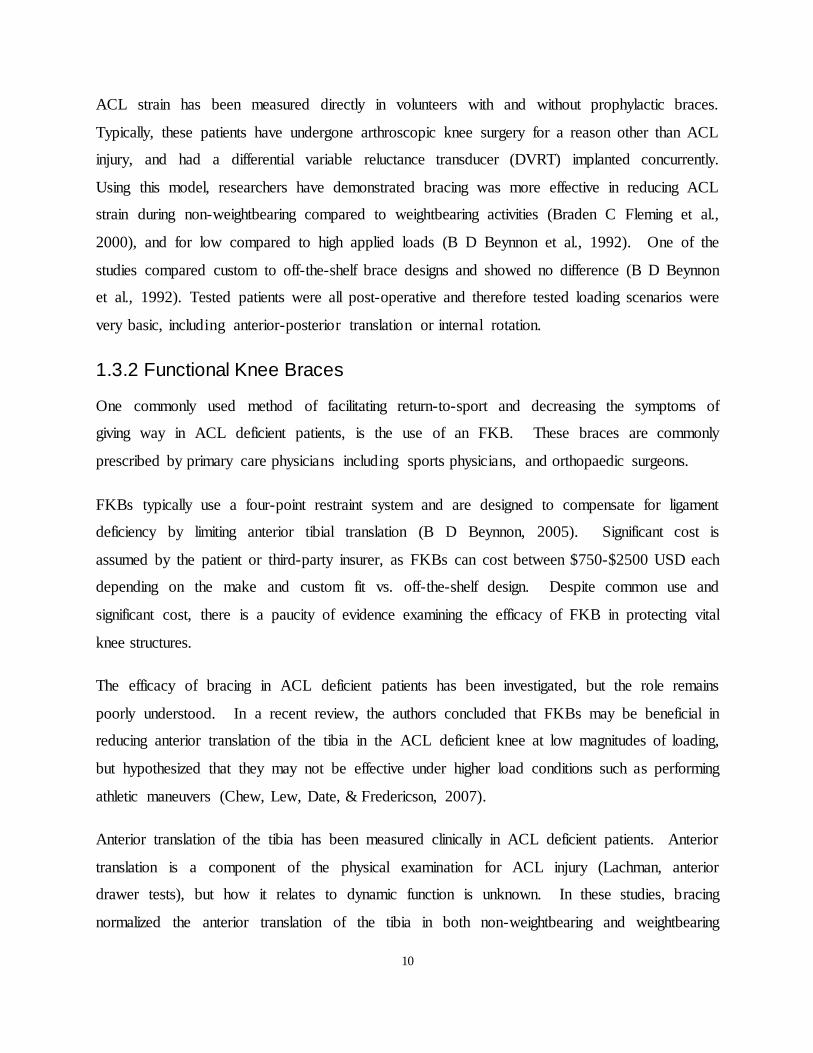
Figure 4. ACL Rebound Brace with Dynamic Tensioning System. (A) Back view. (B) side view,
(C) DTS close up, (D), adjustable torque knob ............................................................................ 13
Figure 5. Overview of In-vivo/In-Silico(Computational)/In-Vitro Method for Jump Landing.
Extracted with Permission from Bakker et al 2016. ..................................................................... 17
Figure 6. Experimental Overview. (1) In-vivo motion capture setup, (2) OpenSim
musculoskeletal model, (3) Dynamic knee simulator. .................................................................. 36
Figure 7. Motion Capture Activities. (A) Double leg squat, (B) single leg squat, (C) gait. ......... 36
Figure 8. Kinematic, Kinetic Variables and Muscle Forces Extracted from OpenSim for DSL,
SLS, and Gait. ............................................................................................................................... 37
Figure 9. Average Strain Profiles of the ACL (n=7) and Meniscus (n=5) for DSL, SLS and Gait.
ACL strain decreased during DLS and SLS and increased throughout the gait cycle. Meniscal
strain followed a similar pattern between ACL intact and reconstructed conditions. .................. 38
Figure 10. Comparison of Relative ACL strain during DLS. Both curves are presented as strain
relative to starting position rather than resting length. Current strain values (n=7) and pattern
match results of Beynnon et al (1998) (n=8). ............................................................................... 38
Figure 11. Comparison of ACL strain during the gait cycle. Current ACL strain pattern (n=7) is
similar to the findings of Taylor et al (2013) (n=32). ................................................................... 39
xi
Figure 12. Experimental overview. (1) In-vivo motion capture, (2) Musculoskeletal model, (3)
Dynamic knee simulator. .............................................................................................................. 51
Figure 13. Dynamic tensioning system. (Left) Tightening of cabling system, (Right) cable
tension translates the femur forward with respect to tibia. ........................................................... 52
Figure 14. Knee Angle and Muscle Forces Extracted from OpenSim for DSL, SLS, and Gait. HS
denotes heel strike during gait. ..................................................................................................... 52
Figure 15. Peak meniscal strain difference between braced and un-braced conditions. † = not
significant in post-hoc analysis. .................................................................................................... 53
Figure 16. Peak ACL - Strain difference between braced and un-braced conditions. .................. 53
Figure 17. Knee dissection process. (A)-(C) Removal of the skin. (D)-(J) Removal of muscle
tissue. (K)-(L) Capsule preparation. ............................................................................................. 76
Figure 18. Experimental Muscle Cable Setup. (A) Hamstring and Gastrocnemius muscle
attachments viewed from the posterior aspect of the knee (B), and from the medial aspect. (C).
Quadriceps cable attachment through the patella. ........................................................................ 78
Figure 19. Negative mold casting preparation (A) Specimen casting, (B) cast removal, (C)
location rods, (D) mold preparation. ............................................................................................. 80
Figure 20. Cadaveric integration into the mold. (A) Specimen placement, (B) stainless steel
muscle cable conduit, (C) endplate preparation. ........................................................................... 81
Figure 21. View through the end plate of a sealed mold with specimen and cable conduit in
place. ............................................................................................................................................. 82
Figure 22. Soft tissue recreation. (A) Removal from negative mold, (B) lateral view of soft
tissue, (C) fit of the custom built Rebound ACL brace on the soft tissue envelope. ..................... 83
Figure 23. Removal of restrictive joint foam. (A) Anterior view, (B) sagittal view. .................. 84

xii
Figure 24. Moment arm calculation experimental apparatus. (A) Knee specimen with an
electronic goniometer, (B) tendon length measuring apparatus with LVDT. ............................... 85
Figure 25. Example measurement of the quadriceps moment arm for one specimen. Grey dots
represent the tendon length at different flexion angles. The slope of the linear fit represents
and is the muscle moment arm (37.2mm for this knee)................................................................ 86
Figure 26. Male and female participant gait knee angle comparison with Pietraszewski et al.
Gait cycle is presented from toe-off to toe-off.............................................................................. 88
Figure 27. Male and female participant gait knee angle comparison with Liu et al. Gait cycle is
presented from toe-off to toe-off................................................................................................... 88
Figure 28. Male and female participant gait knee angle comparison with Oberg et al (1993). Gait
cycle is presented from toe-off to toe-off...................................................................................... 89
Figure 29. Muscle activation comparison during gait. (Column 1) Rectus femoris, biceps
femoris long head, medial gastrocnemius and anterior tibialis activations. (Column 2) Vastus
medialis, semimembranosus, and soleus activations. Gait cycle is presented from toe-off to toe-
off. ................................................................................................................................................. 90
Figure 30. Comparison of female participant’s knee flexion angles during double leg squat. Trial
% is from full extension through deep flexion and back to full extension. .................................. 91
Figure 31. Comparison of female participant’s knee flexion angles single double leg squat. Trial
% is from full extension through deep flexion and back to full extension. .................................. 92
Figure 32. Pilot testing strain values during double leg squat. (Left) ACL strain with and without
brace, (Right) meniscal strain with and without brace. ................................................................ 93
Figure 33. Hip upgraded attachment. (A) Hip attachment with zero degrees of femoral
angulation and (B) hip attachment with 15 degrees of femoral angulation. ................................. 93
Figure 34. Ankle upgraded attachment. (A) Previous vertical ankle attachment, (B) ankle
upgraded right angle attachment. .................................................................................................. 94
xiii
Figure 35. Patellar cable attachments. (A) Pilot study patellar attachment, (B) front view of
improved patellar attachment with patellar tunnel, (C) lateral view of improved patellar
attachment. .................................................................................................................................... 95
Figure 36 Surrogate foam muscle stiffness plots. Comparison between the female subject’s
muscle compliance corridor and three compliance measurements from SunMate liquid foam
medium-firm density..................................................................................................................... 96
xiv
List of Tables
Table 1. ACL and Meniscal Strain Values for All Activities. Strain values are presented as a
mean ± standard deviation. ANOVA P-values for ACL status are presented in horizontal
brackets. ANOVA P-values for knee angle and gait phase are presented in vertical brackets.
Knee angle and gait phase was correlated to meniscal and ACL strain for most conditions.
Meniscal strain was not statistically different between ACL-intact and reconstructed conditions.
....................................................................................................................................................... 35
Table 2. Peak and Average Tissue Strains. The brace lowered peak and mean meniscal strain
across every ACL status and activity (p<0.05). The brace lowered peak and mean ACL strain in
ACL competent knees for every activity. ..................................................................................... 51
xv
List of Abbreviations
ACL – Anterior Cruciate Ligament
ATT – Anterior Tibial Translation
BR – Braced
DF – Deep Flexion
DLS – Double Leg Squat
DTS – Dynamic Tensioning System
DVRT – Differential Variable Reluctance Transducer
EMG – Electromyography
EX – Extension
FKB – Functional Knee Brace
IMB – Intermediate bundle
LCL – Lateral Collateral Ligament
MCL – Medial Collateral Ligament
MF – Mid Flexion
NB – Not braced
OA – Osteoarthritis
PCL – Posterior Cruciate Ligament
PLB – Posterolateral Bundle
SLS – Single Leg Squat
1
Chapter 1 1Literature Review
1.1 Human Body and Anatomy
Biomechanical studies of the human body require some fundamental knowledge of basic
anatomical terms and an understanding of the structures to be studied. The first section “Human
Body and Anatomy” will get the reader up to speed with the fundamental knowledge required to
understand this thesis.
1.1.1 Anatomical Orientation
The human body can be divided into three planes used to define the directions of human
movement.
The sagittal plane divides the human body into left and right, creating two halves that are mirror
images of each other (Winter, 2009). Actions in the sagittal plane describe forward or backward
movement of the body. Examples of sagittal plane movements include: walking, running,
lunging and squatting. Additional sagittal plane movements include flexion and extension of
joints.
The frontal plane divides the human body from front to back. Movements in this plane are
termed adduction and abduction. Examples of frontal plane movements include hip abduction
and shoulder adduction. There are less abduction movements in the human body than sagittal
plane movements due to anatomical orientation of most joints.
The transverse plane separates the human body between the top and the bottom. Movements in
this plane are twisting in nature such as trunk rotations and include pronation and supination of
the foot and wrist.
In addition to the three planes, researchers define terms to identify specific locations on body
segments. Anterior and posterior define front and back of a body segment. Proximal and distal
describe which end of the body segment is nearest to the body’s center. The proximal femur is at
2
the hip joint while the distal femur is in the knee joint. Superficial and deep describe whether the
location is close to the surface or deeper internally.
1.1.2 General Knee Anatomy
The human knee is part of the primary kinematic chain (ankle, knee and hip) responsible for
human propulsion. The knee primarily operates in the sagittal plane, and therefore the primary
movements are flexion (bringing the lower leg closer to the hip) and extension (bringing the
lower leg in line with the thigh).
The knee is made up of three bones: femur, tibia and patella. The femur connects the pelvis to
the shin, and the tibia connects the thigh to the foot. Unlike the femur and tibia, the patella (often
referred to as the knee cap) acts as a fulcrum for the extensor muscles to provide a greater
extension moment.
There are three major muscle groups that cross the knee and enable flexion and extension
movements. The quadriceps muscle group consists of four muscles: the rectus femoris, vastus
lateralis, vastus intermedius and vastus medialis. All four muscles connect to the quadriceps
tendon, which inserted in the proximal patella. The quadriceps muscle group provides extension
moments about the knee, helping maintain upright stance.
The hamstring muscle group consists of four muscles: biceps femoris long head, biceps femoris
short head, semitendinosus, and semimembranosus. Hamstring muscles originate from the pelvis
and the posterior femur and insert into the proximal tibia, providing flexion moments about the
knee. The third muscle group, the gastrocnemius, also provides flexion moments about the knee.
The medial and lateral heads of the gastrocnemius originate in the posterior aspect of the distal
femur and insert on the calcaneus via the Achilles tendon.
Additional muscles that cross the knee joint are popliteus, sartorius, and gracilis. The popliteus
initiates knee flexion and provides rotational stability. The sartorius and gracilis both help flex
the knee.
A series of ligaments provide passive stability to the joint (Figure 1). There are two collateral
ligaments and two cruciate ligaments. The collateral ligaments, the lateral collateral ligament

3
(LCL) and the medial collateral ligament (MCL), are the primary restraint against abduction and
adduction forces. The cruciate ligaments, the anterior cruciate ligament (ACL) and the posterior
cruciate ligament (PCL), prevent the tibia from translating anteriorly (ACL) or posteriorly (PCL)
with respect to the femur.
Another anatomical structure of significance is the meniscus. The medial and lateral menisci
found between the femoral condyles and the tibial plateaus and consist of fibrocartilage rings
attached to the proximal tibia via coronary ligaments.
Figure 1. Knee Ligament Anatomy
1.1.3 Anatomy and Function of the Anterior Cruciate Ligament
The primary function of the ACL is to prevent anterior tibial translation (ATT) (Duthon et al.,
2006; Fu, Woo, & Ph, 1994). In addition the ACL is a restraint to tibial rotation providing
stability when pivoting or twisting (Duthon et al., 2006).
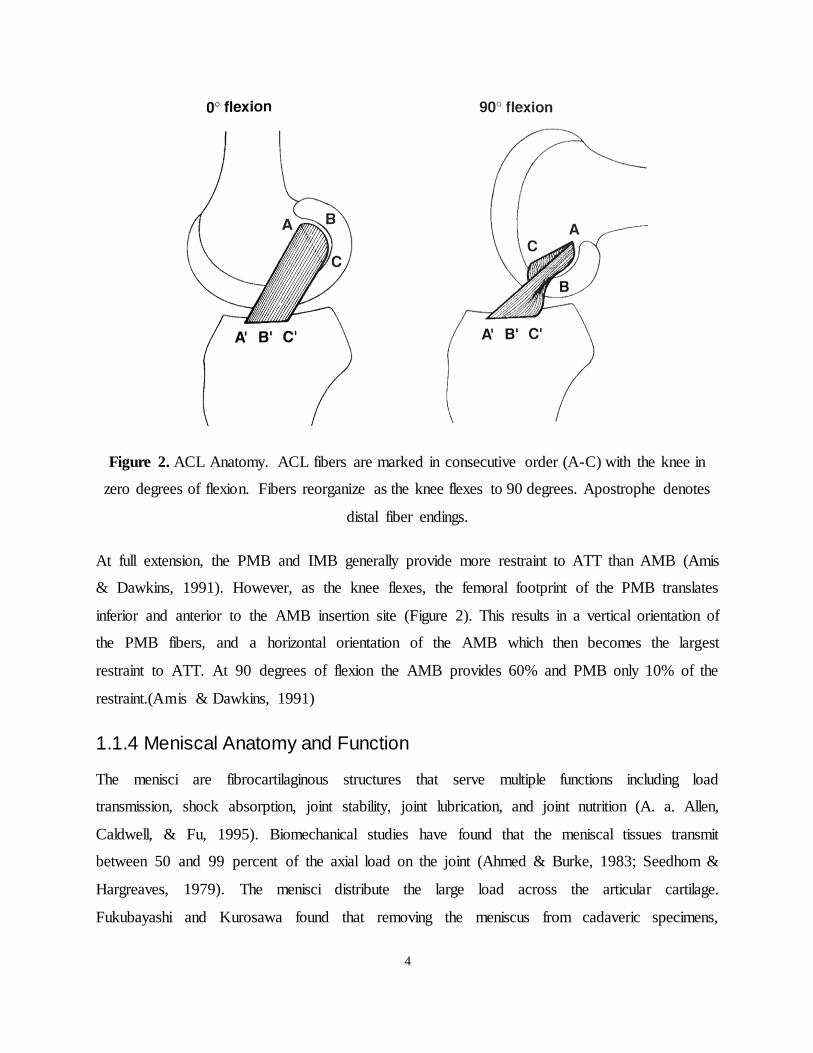
Functionally, the ACL is divided into two bundles: the anteromedial bundle (AMB) and the
posterolateral bundle (PLB) (Fu et al., 1994). Other authors have separated the ACL into three
bundles, adding an intermediate bundle (IMB) (Duthon et al., 2006). In extension, the AMB is
relatively anterior on both the tibia and femur as seen between the points A’-A in Figure 2. The
PLB has a posterior tibial footprint (C’ in Figure 2) and the IMB is located between the AMB
and PLB (B’-B in Figure 2). In flexion, the orientation of the bundles change, which alters the
relative contribution of restraint to ATT.
4
Figure 2. ACL Anatomy. ACL fibers are marked in consecutive order (A-C) with the knee in
zero degrees of flexion. Fibers reorganize as the knee flexes to 90 degrees. Apostrophe denotes
distal fiber endings.
At full extension, the PMB and IMB generally provide more restraint to ATT than AMB (Amis
& Dawkins, 1991). However, as the knee flexes, the femoral footprint of the PMB translates
inferior and anterior to the AMB insertion site (Figure 2). This results in a vertical orientation of
the PMB fibers, and a horizontal orientation of the AMB which then becomes the largest
restraint to ATT. At 90 degrees of flexion the AMB provides 60% and PMB only 10% of the
restraint.(Amis & Dawkins, 1991)
1.1.4 Meniscal Anatomy and Function
The menisci are fibrocartilaginous structures that serve multiple functions including load
transmission, shock absorption, joint stability, joint lubrication, and joint nutrition (A. a. Allen,
Caldwell, & Fu, 1995). Biomechanical studies have found that the meniscal tissues transmit
between 50 and 99 percent of the axial load on the joint (Ahmed & Burke, 1983; Seedhom &
Hargreaves, 1979). The menisci distribute the large load across the articular cartilage.
Fukubayashi and Kurosawa found that removing the meniscus from cadaveric specimens,
5
decreased the joint contact area by over 50% and significantly increased the contact pressure
(Fukubayashi & Kurosawa, 1980).
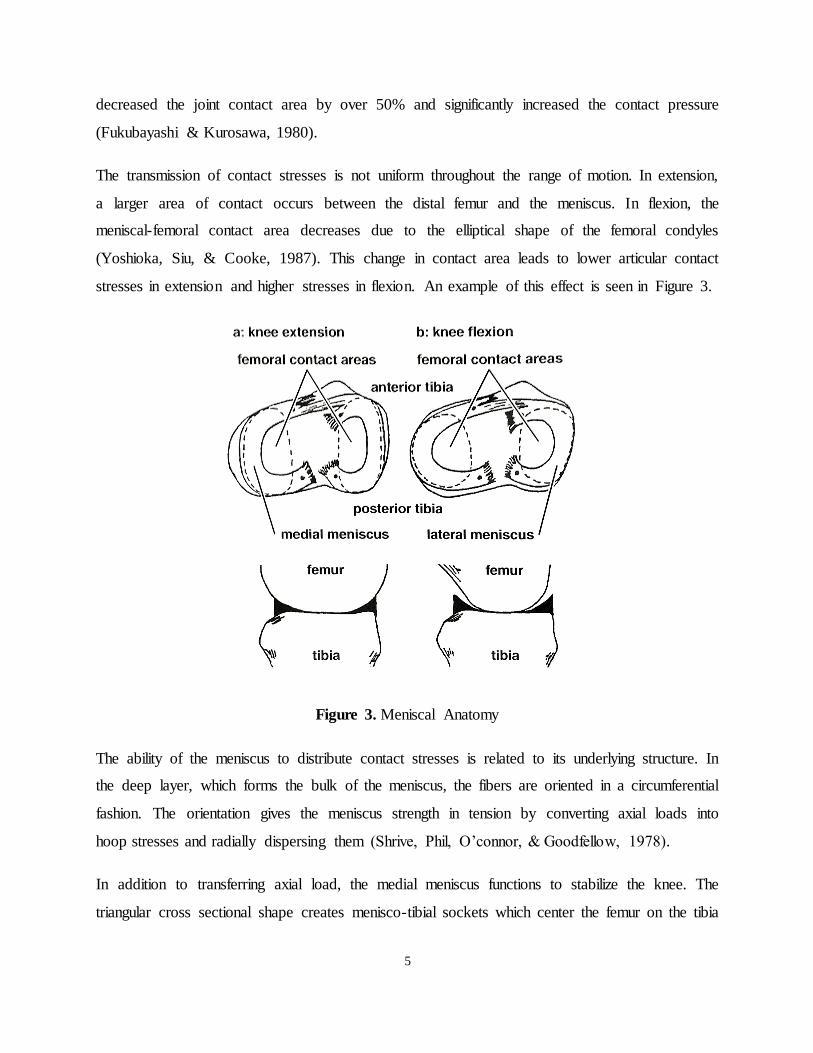
The transmission of contact stresses is not uniform throughout the range of motion. In extension,
a larger area of contact occurs between the distal femur and the meniscus. In flexion, the
meniscal-femoral contact area decreases due to the elliptical shape of the femoral condyles
(Yoshioka, Siu, & Cooke, 1987). This change in contact area leads to lower articular contact
stresses in extension and higher stresses in flexion. An example of this effect is seen in Figure 3.
Figure 3. Meniscal Anatomy
The ability of the meniscus to distribute contact stresses is related to its underlying structure. In
the deep layer, which forms the bulk of the meniscus, the fibers are oriented in a circumferential
fashion. The orientation gives the meniscus strength in tension by converting axial loads into
hoop stresses and radially dispersing them (Shrive, Phil, O’connor, & Goodfellow, 1978).
In addition to transferring axial load, the medial meniscus functions to stabilize the knee. The
triangular cross sectional shape creates menisco-tibial sockets which center the femur on the tibia
6
and resist relative translation. The meniscus is a secondary stabilizer to ATT (A. a. Allen et al.,
1995).
1.2 ACL injury
ACL injuries place a large burden on the healthcare system. In North America it is estimated that
there are 250,000 cases of ACL injury every year (Griffin et al., 2001). In addition, 100,000 of
these are reconstructed, resulting in annual costs of about $7.6Bn USD (Griffin et al., 2001;
Mather et al., 2013). The number of ACL injuries and associated costs continue to increase,
growing between 35% and 75% over the past decade (Mall et al., 2014). An adequate
understanding of ACL injury mechanisms and risk factors is essential to help prevent and
manage these injuries.
1.2.1 Risk Factors
Injury risk factors are broadly divided into intrinsic and extrinsic factors. Intrinsic factors relate
to anatomical differences, which generally cannot be changed, neuromuscular control, and
hormonal variation. Extrinsic factors refer to external causes such as weather and footwear.
Another way to categorize risk factors is according to whether or not they are modifiable.
Non-modifiable risk factors include genetics, tibial slope, (Giffin, Vogrin, Zantop, Woo, &
Harner, 2004; Hashemi et al., 2008; Levine et al., 2013; Marouane, Shirazi-Adl, Adouni, &
Hashemi, 2014; S. G. McLean et al., 2011; Yoo, Chang, Shin, Seong, & Kim, 2008) notch width,
(Domzalski, Grzelak, & Gabos, 2010; Fung & Zhang, 2003; Ireland, Ballantyne, Little, &
McClay, 2001) ligament tensile properties, (Chandrashekar, Mansouri, Slauterbeck, & Hashemi,
2006) Q angle, (Alentorn-Geli et al., 2009; Gray et al., 1985; Shambaugh, Klein, & Herbert,
1991) and sex (Timothy E Hewett, Ford, & Myer, 2006). Tibial slope, a measure of the sagittal
plane slope from anterior to posterior, has been found to increase strain and ATT, potentially
increasing an athlete’s chance of injury (Levine et al., 2013; S. G. McLean et al., 2011). The size
of the intercondylar notch may lead to impingement of the ACL and increased stress within the
ligament. Tensile properties of the ACL vary with a range of failure load between 750N and
2900N (Chandrashekar et al., 2006). Larger Q angles, the angle at which the femur and tibia
come together in the frontal plane, cause increased frontal plane moments when athletes perform

7
dynamic activities, theoretically increasing risk of injury (Alentorn-Geli et al., 2009). Variation
in all of these anatomical factors, as well as hormonal differences and landing techniques, place
females at 4 to 6 times higher risk of experiencing an ACL injury than their male counterparts
(Timothy E Hewett et al., 2006).
Modifiable risk factors involve movement mechanics, high body mass index, and playing
surface. Video analysis has found that landing with a flat foot, increased hip flexion angle, knee
abduction angles, knee valgus angles and a stiff upper body are correlated with injury (Boden,
Torg, Knowles, & Hewett, 2009; Krosshaug et al., 2007; Sasaki et al., 2015). Specifically
designed neuromuscular training programs have been shown to improve movement mechanics
and decrease rates of injury (Heidt, Sweeterman, Carlonas, Traub, & Tekulve, 2000; T E Hewett,
Lindenfeld, Riccobene, & Noyes, 1999; Myklebust et al., 2003).
1.2.2 Treatment Options
Acutely, ACL injuries result in a painful, swollen knee due to a large hemarthrosis. Once the
initial sequela resolves, patients often begin experiencing instability or a feeling of their knee
‘giving-way’, preventing them from returning to their previous level of activity. Patients may
choose to undergo ACL reconstruction surgery, or to rehabilitate using non-operative measures.
Recent level-I evidence suggests that outcomes after early rehabilitation with or without late
reconstruction have comparable subjective outcomes to early ACL reconstruction (ACLR)
(Ranstam, Lohmander, Frobell, & Roos, 2010). Previous randomized controlled trials in
different patient populations, and using historical reconstruction techniques had concluded a
benefit for early surgical reconstruction (Andersson, Odensten, Good, & Gillquist, 1989).
1.2.2.1 Non-Operative Management
Not all patients who have an ACL deficient knee choose to undergo reconstructive surgery. As
many as 150,000 patients per year in North America opt for the non-surgical treatment (Griffin et
al., 2001; Mather et al., 2013). The main non-operative treatment for ACL deficiency includes
intensive physiotherapy and knee bracing. Physiotherapy programs have been shown to be
effective at improving joint stability after an ACL injury (Carter, Jenkinson, Wilson, Jones, &
Torode, 1997).
8
Few studies have examined the natural history of knee function and injury in the ACL deficient
knee. The reported rate of eventual ACL reconstruction in these cohorts is between 22%
(Kostogiannis et al., 2007) and 37% (Scavenius et al., 1999), which suggests eventually patients
become either ‘copers’ or ‘non-copers,’ with the latter being those that have persistent instability
and elect to proceed with ligament reconstruction. Among those who remain ACL deficient, re-
operation for meniscal lesions is significant, and most are on the medial side (Kostogiannis et al.,
2007; Scavenius et al., 1999).
The concomitant knee injuries accompanying acute versus chronic ACL rupture have been
established at the time of ligament reconstruction. Lateral meniscal tears predominate in the
acute injury setting, but the majority of meniscal lesions in chronic ACL deficient knees are
severe or complex medial meniscal lesions (Cipolla, Scala, Gianni, & Puddu, 1995). This has
been hypothesized as due to the role of the medial meniscus as a secondary stabilizer to anterior
translation of the knee. Allen et al. (2000) used a force-moment sensor system in cadaveric knees
with a transected ACL and demonstrated that the minimum increase in force across the medial
meniscus was 52% at full knee extension, to a maximum of 197% at 60 degrees of flexion (C. R.
Allen et al., 2000).
In a landmark paper, Neuman et al. (2008) demonstrated the importance of meniscal preservation
in the ACL deficient knee (Neuman et al., 2008). Among a prospective cohort followed for 15
years, 13/35 patients who underwent meniscectomy developed radiographic arthritis (grade II or
higher) while none of the 44 patients without meniscal lesions developed arthritic changes. The
association of meniscal injury/loss in the ACL deficient knee and higher risk of eventual arthritic
change has been reproduced in other studies (Lohmander, Englund, Dahl, & Roos, 2007;
Louboutin et al., 2009).
1.2.2.2 Reconstruction
A significant number of patients opt for ACL reconstruction (ACLR) as a way to return-to-play
with improved joint stability. There are over 100,000 patients who undergo ACLR in North
America every year (Mather et al., 2013). Recovery from ACLR generally takes longer than
returning to play with an ACL deficient knee. Most patients require 6 to 12 months to recover
after surgery (Myer, Paterno, Ford, Quatman, & Hewett, 2006).
9
Modern ACL reconstruction techniques aim to replicate the normal anatomy of the ACL. Both
single bundle and double bundle reconstructions are used (Noyes, 2009). Typical graft materials
are autograft hamstring tendons and bone/patellar tendon/bone grafts. Allografts may also be
used. Considerable research has examined the optimal femoral and tibial insertion points to
duplicate the native ACL footprints. Graft tensioning is also an important factor in
reconstructions, both in terms of the tension value and knee angle at which tensioning is
performed. Despite best efforts, ACL reconstructions do not completely restore normal
kinematics and tissue loading (Herbort, Lenschow, Fu, Petersen, & Zantop, 2010). The long-term
risk of osteoarthritis is increased (Neuman et al., 2008). This has been hypothesized to be due to
several factors, including initial cartilage damage at the time of injury, an inability of the graft to
normalize the kinematics of the knee, and increased strain on secondary tissues.
1.3 Bracing
Knee braces have several uses in relation to ACL injuries. Functional knee braces (FKBs) are
most commonly prescribed after an ACL injury to stabilize the knee and facilitate safe return to
athletic activities. Many orthopaedic surgeons also recommend their patients wear an FKB after
ACL surgery to minimize the risk of early failure or re-injury. Lastly, prophylactic braces may
serve a role in preventing injury in high risk populations. The industry for knee bracing is
significant, with an estimated US market size of $1.6Bn USD in 2007.
1.3.1 Prophylactic Braces
Braces have been advocated for knee injury prophylaxis in uninjured athletes (Najibi, 2005). A
randomized trial in football recruits found that prophylactic brace use reduced the number of
ACL and medial collateral ligament injuries overall, but not the severity. The difference was
seen only for defensive and not offensive football players (Sitler et al., 1989). The value of
bracing for injury prophylaxis has been tested in a cadaveric model and mechanical surrogate
limb (Cawley, France, & Paulos, 1991; Paulos, Cawley, & France, 1991). Six different FKBs
protecting a cadaveric knee were tested with simple valgus impact. The braces were moderately
effective in reducing measured force, but did not influence MCL injury, and only variably
protected against ACL injury in these primitive models.
10
ACL strain has been measured directly in volunteers with and without prophylactic braces.
Typically, these patients have undergone arthroscopic knee surgery for a reason other than ACL
injury, and had a differential variable reluctance transducer (DVRT) implanted concurrently.
Using this model, researchers have demonstrated bracing was more effective in reducing ACL
strain during non-weightbearing compared to weightbearing activities (Braden C Fleming et al.,
2000), and for low compared to high applied loads (B D Beynnon et al., 1992). One of the
studies compared custom to off-the-shelf brace designs and showed no difference (B D Beynnon
et al., 1992). Tested patients were all post-operative and therefore tested loading scenarios were
very basic, including anterior-posterior translation or internal rotation.
1.3.2 Functional Knee Braces
One commonly used method of facilitating return-to-sport and decreasing the symptoms of
giving way in ACL deficient patients, is the use of an FKB. These braces are commonly
prescribed by primary care physicians including sports physicians, and orthopaedic surgeons.
FKBs typically use a four-point restraint system and are designed to compensate for ligament
deficiency by limiting anterior tibial translation (B D Beynnon, 2005). Significant cost is
assumed by the patient or third-party insurer, as FKBs can cost between $750-$2500 USD each
depending on the make and custom fit vs. off-the-shelf design. Despite common use and
significant cost, there is a paucity of evidence examining the efficacy of FKB in protecting vital
knee structures.
The efficacy of bracing in ACL deficient patients has been investigated, but the role remains
poorly understood. In a recent review, the authors concluded that FKBs may be beneficial in
reducing anterior translation of the tibia in the ACL deficient knee at low magnitudes of loading,
but hypothesized that they may not be effective under higher load conditions such as performing
athletic maneuvers (Chew, Lew, Date, & Fredericson, 2007).
Anterior translation of the tibia has been measured clinically in ACL deficient patients. Anterior
translation is a component of the physical examination for ACL injury (Lachman, anterior
drawer tests), but how it relates to dynamic function is unknown. In these studies, bracing
normalized the anterior translation of the tibia in both non-weightbearing and weightbearing
11
positions when anterior loads were applied, but not in the transition from non-weightbearing to
weightbearing (Bruce D Beynnon, Fleming, Churchill, & Brown, 2003). Similar cadaveric
testing after sectioning of the ACL, demonstrated a reduction in anterior translation with anterior
loading when braced (Anderson, Wojtys, Loubert, & Miller, 1992; E M Wojtys, Loubert,
Samson, & Viviano, 1990). Rotational control has been less reliable in cadaveric testing (E M
Wojtys et al., 1990).
Ramsey et al. placed traction pins into the femur and tibia of ACL deficient volunteers and
performed a kinematic analysis during jumping, demonstrating a mild influence of bracing on
kinematic changes (Ramsey, Lamontagne, Wretenberg, & Valentin, 2001). Others have
examined the effect of bracing on muscle activation. Ramsey et al. found decreased biceps
femoris, rectus femoris and semi-tendinosus muscle activity in four ACL deficient (ACLD)
patients wearing a FKB using EMG. Another similar study suggested hamstring muscle reflex
activity was not affected (Lam, Ng, & Chien, 2002).
Smith et al. showed delayed onset muscle activation at landing for at least 1 muscle in ACLD
patients performing a single let hop (Smith, Malanga, Yu, & An, 2003). Beynnon et al. showed
no effect of bracing on proprioception.(B D Beynnon et al., 1999)
There is only one high level clinical study that examined the efficacy of bracing in the early post-
ACL injury period (Swirtun, Jansson, Renström, & Study, 2005). An FKB significantly reduced
the number of instability episodes, but had no effect on clinical outcome. This study was limited
by a high drop-out rate due to subsequent surgery. Other clinical studies of FKBs in ACLD
patients have demonstrated improved subjective stability during activity, (Marans, Jackson,
Piccinin, Silver, & Kennedy, 1991; Mishra, Daniel, & Stone, 1989) and decreased anterior tibial
translation (Griffin et al., 2001; Jonsson & Kärrholm, 1990; Edward M Wojtys, Kothari, &
Huston, 1996) or pivot shift (Mishra et al., 1989). No difference has been found between custom
fit and off-the-shelf FKBs when tested in one study (Griffin et al., 2001).
Many clinical trials have also examined the role for FKB post-ACL reconstruction. Wright et al.
performed a meta-analysis of 12 randomized controlled trials, demonstrating no effect of knee
bracing after ACL reconstruction on pain, range-of-motion, graft stability or protection from
subsequent injury (Wright & Fetzer, 2007). More recently, Singer & Lamontagne studied the
12
effect of FKB design on lower limb mechanics of 10 normal (ACL-intact) subjects performing a
walk test (Singer & Lamontagne, 2008). The net joint moments were estimated at the ankle,
knee and hip. The authors showed that a brace altered some directional moments, but none that
they hypothesized would reduce force to the ACL.
1.3.3 Dynamic Tensioning Systems
Traditional FKBs consist of two rigid shells connected by a polycentric joint. They provide
constant restraint to tibial translation throughout the range-of-motion, with the external force
being dependent on the fit of the brace (LaPrade, Smith, Wilson, & Wijdicks, 2015).
A new brace mechanism that incorporates a dynamic tensioning system (DTS) has recently been
introduced by Össur Inc, (Foothill Ranch, CA, USA. There are two versions of the brace:
Rebound ACL (Figure 4A,B) and Rebound PCL. The DTS is a cabling system that applies forces
to the thigh and shank in order to decrease or neutralize forces in the respective cruciate ligament
(Figure 4C). A set of knobs is used to adjust the tension in the cab (Figure 4D). In addition, the
cable wraps around a post allowing the tension to change as a function of knee angle.
13
Figure 4. ACL Rebound Brace with Dynamic Tensioning System. (A) Back view. (B) side view,
(C) DTS close up, (D), adjustable torque knob
The Rebound PCL brace has recently been tested by LaPrade et al (2015) to determine the
amount of posterior force applied to the tibia by the brace (LaPrade et al., 2015). Six healthy
adult males performed three functional activities (seated unloaded knee flexion, squatting, and
stair descent) while wearing the Rebound PCL brace and a traditional static force PCL brace. A
pressure mapping technique was used to quantify the posterior force. The Rebound PCL brace
was found to apply a linearly increasing posterior force from an average of 40N at 0 degrees of
flexion to 120N at 90 degrees of flexion. The static force PCL brace applied a constant 40N of
force through the range of motion.
1.3.4 Neuromuscular Effects of Bracing
Bracing is often thought as a mechanical restraint to the knee, but braces can influence a
patient’s psychological behavior or neuromuscular response. This effect is typically measured by
a change in the patient’s movement and muscle activation patterns. This response has been
measured in both ACL-deficient (Branch, Hunter, & Donath, 1984; Nemeth, Lamontagne, Tho,
A B C
D
14
& Eriksson, 1997; Ramsey, Wretenberg, & Lamontagne, 2003) and ACL-reconstructed patients
(Nemeth et al., 1997; Rebel & Paessler, 2001) with mixed results.
Ramsey et al (2003) found that functional bracing during ACL deficiency increased rectus
femoris activity and decreased bicep femoris activity while jumping. Branch et al (1984) found
the opposite effect during cutting; hamstring activity was increased while quadriceps activity
decreased. It has also been found that functional bracing during skiing can increase hamstring
activity (Nemeth et al., 1997).
Braces have also been shown to alter the movement patterns while jumping. Rebel et al (2001)
found that bracing can increase jumping height, and improve stability when landing from jumps
(Rebel & Paessler, 2001). Patients who landed while wearing a brace had increased knee range
of motion and softer landings. It remains unclear if these neuromuscular changes vary for
different braces.
1.4 Testing Methodologies
Testing the effects of braces on tissue loads is challenging. There is no established reliable and
validated model to study ACL and meniscal strain within the knee that reflects the rigors of
athletic activity.
1.4.1 In-Vivo
Human testing, although performed previously, requires surgical implantation of strain gauges
which limits the type of activity that can be performed. In 1992, Beynnon et al used a DVRT to
measure ACL strain (B. Beynnon, Howe, Pope, Johnson, & Fleming, 1992). This technique
required a DVRT to be surgically implanted in the ACL in-vivo. Subjects performed various
tasks such as squatting, walking and stair climbing (B. Beynnon et al., 1992; B D Beynnon &
Fleming, 1998; B C Fleming et al., 1998). DVRTs have also been used to investigate the effect
of braces on ACL strain while standing with and without a brace (Bruce D Beynnon et al., 2000).
Recently dynamic fluoroscopy has also been used to analyze tissue strains in-vivo. Taylor et al
measured ACL strain during walking using this technique (K. a Taylor et al., 2011). The effect of
braces has not been studied with this method.
15
1.4.2 In-Silico
Computer models have been used to study knee mechanics during dynamic activities, including
calculating ACL strain from kinematic data after motion capture (Laughlin et al., 2011; Pflum,
Shelburne, Torry, Decker, & Pandy, 2004; K. a Taylor et al., 2011). While this approach is a
non-invasive and low-cost way to calculate intra-articular strain during dynamic activities, the
disadvantage of this approach is that important factors such as joint frictional properties, tissue
properties and joint anatomy are difficult to validate, and how this type of model relates to in-
vivo effects cannot be confirmed.
1.4.3 In-Vitro
In-vitro testing allows for easier measurement of tissue strains. Many studies have used DVRTs
to measure the strain in the collateral (C. E. Quatman et al., 2014) and cruciate ligaments
(Bakker et al., 2016; Hangalur et al., 2015; Levine et al., 2013; Oh, Lipps, Ashton-Miller, &
Wojtys, 2012), as well as the meniscus (Hollis, Pearsall, & Niciforos, 2000; Jones et al., 1996;
Pearsall, 2004). One disadvantage of DVRT strain collection is that absolute magnitudes are not
easily garnered. DVRTs can only measure the change in displacement between two pins.
Obtaining the zero-strain length of the pins to determine the absolute strain is difficult. One
method of dealing with this problem is to calculate the strain relative to a specific time or loading
condition. During jump landing Bakker et al used the time at contact as the zero strain position,
whereas Oh et al calculated relative strain from a static posture (Bakker et al., 2016; Oh et al.,
2012). Alternatively, absolute strain can be obtained in some instances with proper calibration.
Beynnon et al calculated absolute strain by examining the hysteresis curve using a Lachman test
(B. Beynnon et al., 1992).
In-vitro testing of human knees often requires advanced mechanical setups or simulators. These
simulators are custom designed equipment and are tuned to answer specific research questions.
Typically knee simulators control various kinematics and kinetics.
A number of knee simulators are static simulators, and do not apply dynamic loading to the knee
specimens. This means that these simulators are kinematically constrained and the knees do not
move during the loading process (Harris, Morberg, Bruce, & Walsh, 1999).

16
Newer static simulators have increased degrees-of-freedom. One new simulator, described in
Stephen et al, is able to apply axial loading, anterior tibial moments, posterior tibial moments,
internal rotation, external rotation and knee flexion (in 10 degree increments) (Stephen et al.,
2016). These loading conditions are applied by hanging weights from pulleys attached to each
degree-of-freedom. Although still static in nature, this increase in complexity and degree-of-
freedom allows for more in depth analysis into knee loading states. Stephen et al was able to
investigate the effect of ACL and meniscal deficiency on tibiofemoral joint laxity by combining
many of these loading options into a combined loading state.
In contrast to static simulators, dynamic simulators are able to apply dynamic loading to the
cadaveric knee specimens. Berns developed a simulator to apply dynamic loading in five
degrees-of-freedom, flexion, anterior-posterior force, medial-lateral force, varus-valgus moments
and internal-external axial moments (Berns, Hull, & Patterson, 1992). Unlike previous
simulators that hang weights to apply loads, this simulator applied forces with dynamic
actuators, allowing for electronic control and dynamic force profiles.
Significant improvements to simulators occurred in the early 1990’s when dynamic muscle
forces were introduced. Using the application of muscle forces, researchers were able to answer
more direct and applicable questions as the force development in the cadaveric models started to
resemble activities people encountered outside of the lab. Maclean et al developed one of the
earliest dynamic simulators with muscle forces in 1993 (C. a McLean & Ahmed, 1993). Instead
of loading knees in one static position at a time with a constant force, the simulator allowed for
dynamic ground reaction force simulation.
Multiple new paradigms surrounding the efficacy of in-vitro simulation study have recently
emerged in attempt to narrow the gap between in vivo measurements and in-vitro simulations.
Quatman et al suggests using a newly coined in-sim approach. This approach was developed to
help researchers validate their models in any of the three research spaces (in-vivo, in-silico, and
in-vitro) and suggests using the results from one of the three spaces to help validate and justify
the work of the other space (C. E. C. Quatman, Quatman, & Hewett, 2009).
A similar combined approach, in-vivo/in-silico/in-vitro, was described by Cassidy et al. (Cassidy,
Hangalur, Sabharwal, & Chandrashekar, 2013). This method proposes to collect kinematic,
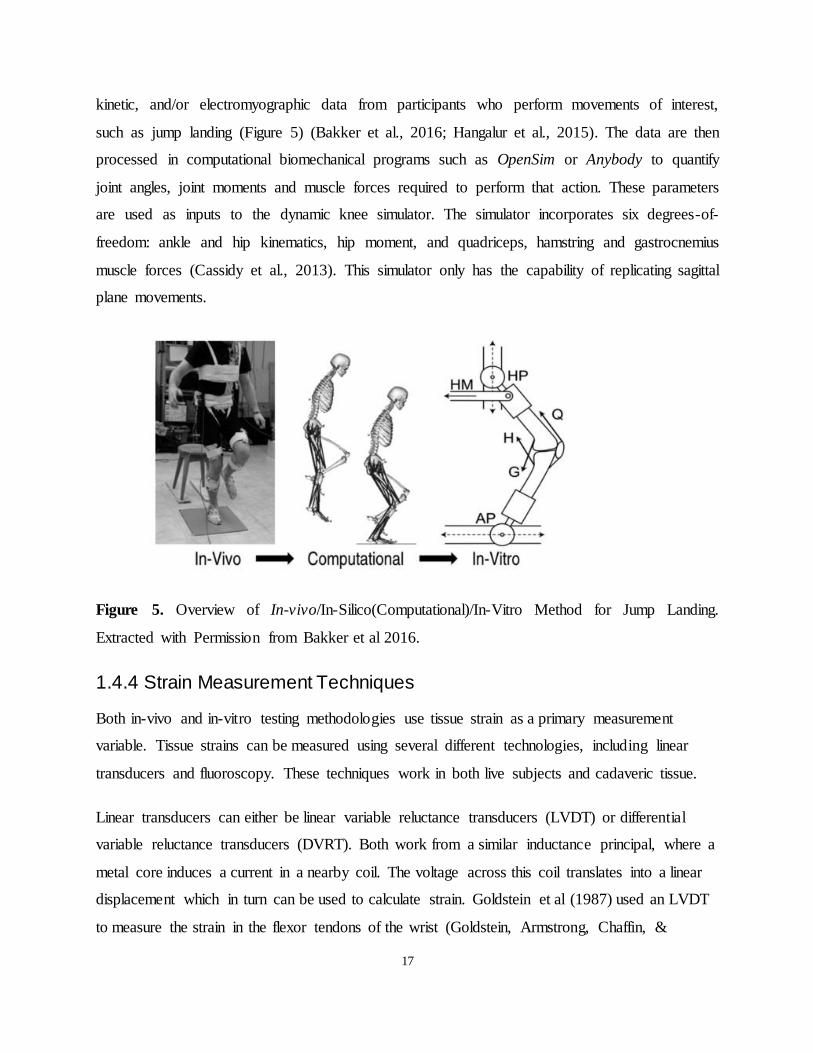
17
kinetic, and/or electromyographic data from participants who perform movements of interest,
such as jump landing (Figure 5) (Bakker et al., 2016; Hangalur et al., 2015). The data are then
processed in computational biomechanical programs such as OpenSim or Anybody to quantify
joint angles, joint moments and muscle forces required to perform that action. These parameters
are used as inputs to the dynamic knee simulator. The simulator incorporates six degrees-of-
freedom: ankle and hip kinematics, hip moment, and quadriceps, hamstring and gastrocnemius
muscle forces (Cassidy et al., 2013). This simulator only has the capability of replicating sagittal
plane movements.
Figure 5. Overview of In-vivo/In-Silico(Computational)/In-Vitro Method for Jump Landing.
Extracted with Permission from Bakker et al 2016.
1.4.4 Strain Measurement Techniques
Both in-vivo and in-vitro testing methodologies use tissue strain as a primary measurement
variable. Tissue strains can be measured using several different technologies, including linear
transducers and fluoroscopy. These techniques work in both live subjects and cadaveric tissue.
Linear transducers can either be linear variable reluctance transducers (LVDT) or differential
variable reluctance transducers (DVRT). Both work from a similar inductance principal, where a
metal core induces a current in a nearby coil. The voltage across this coil translates into a linear
displacement which in turn can be used to calculate strain. Goldstein et al (1987) used an LVDT
to measure the strain in the flexor tendons of the wrist (Goldstein, Armstrong, Chaffin, &
18
Matthews, 1987). The applications of LVDTs for strain measurement are limited due to their
relatively large size, which creates difficulties for implantation.
DVRTs have been used extensively for ligament and tissue strain measurements. Beynnon et al,
(1992) pioneered a methodology to measure ACL strain in-vivo using DVRTs. Beynnon used
this technique to measure ACL strain during a host of activities including walking, cycling, stair
climbing and squats (B. Beynnon et al., 1992; B D Beynnon et al., 1992; B D Beynnon &
Fleming, 1998; B C Fleming et al., 1998). Although it garnered valuable information about the
nature of ACL strain, the ethical restrictions due to the surgical DVRT implantation procedure
have limited widespread use of this technique. More recently, DVRTs have extensively been
used to study ligament strains in-vitro. They have been employed to measure ACL strain (Bakker
et al., 2016; Erickson, Yasuda, Beynnon, Johnson, & Pope, 1993; Hangalur et al., 2015; C. E.
Quatman et al., 2014), MCL strain (C. E. Quatman et al., 2014), and meniscal strain (Hollis et
al., 2000) among other ligaments. DVRTs are commonly used due to their relatively inexpensive
cost and ease of use.
Fluoroscopy is also used to measure tissue strains in-vivo. Fluoroscopy is a dynamic x-ray which
can be used to measure the displacement of bones throughout time during a movement. The
distance between two bones can be interpolated as the length of the ligament, and changes in this
length relate to strain. Fluoroscopy has been used to measure ACL strain during walking (K. a
Taylor et al., 2013) and jumping (Myers et al., 2012; K. A. Taylor et al., 2011; Torry et al.,
2013). This technique is considered highly accurate but requires expensive equipment and tasks
must be performed in a confined space, which makes this technique less common.
Regardless of the techniques used to measure strain, the same mathematic relationship is used for
the calculation. Strain is defined by the formula
, or the change in length divided by the resting
length of the ligament. This value is often represented as a percentage of the origina l length,
which is calculated by multiplying the original formula by one hundred percent. In many cases, it
is difficult for researchers to know or measure the resting length, because the tendons may be
pre-stressed. For these situations, researchers report relative strain which uses the original
formula with resting length replaced with reference length. Reference length is length of the
ligament with a specific reference, such as the length of the ACL at heel strike while walking.
19
This makes the relative strain at heel strike zero, and all other strains referenced to this time
point.
1.4.5 In-Vitro Knee Brace Testing
Knee simulators have been used by a few researchers to develop in-vitro brace testing models.
Erickson et al used a simulator to evaluate prophylactic bracing on lateral impacts (Erickson et
al., 1993). This simulator applied static quadriceps and hamstring loading to a cadaveric
specimen via a pulley and weight system to model co-contraction of the joint while a metal rod
was struck against the knee with and without the brace. This research failed to find any
significant reductions in ACL strain with prophylactic bracing. Similar studies have been done
on the effectiveness of knee braces and taping to reduce knee translation and rotation; (Anderson
et al., 1992) pneumatic cylinders applied anterior and rotational loads to the knees while
ligament strains were measured. Unlike Erickson et al, this experimental setup found bracing to
reduce knee translation and rotation.
A large challenge researchers face when performing in-vitro brace testing is addressing the soft
tissue envelope. Braces rely on applying forces to the musculoskeletal system to affect the strain
of knee ligaments. These forces are applied through a series of hard or soft brace straps or
material directly onto the surface of the skin. Cadaveric muscle cannot contract and thus
provides little support compared to the stiffened muscle during athletic maneuvers; this may
negatively impact the effectiveness of load transfer between the brace and the specimen.
Multiple studies solve this issue by dissecting the soft tissues from the cadaveric specimen and
replacing it with surrogate foam. Erickson et al was the first to apply this methodology in 1993
(Erickson et al., 1993). A negative mold of the musculature surrounding the knee was taken
from a subject. This mold was then placed around the cadaveric specimen and filled with
Sunmate Liquid Foam. This foam was found to have similar compliance to the stiffened muscles
of ten human participants (0.316mm/N). This new surrogate foam allowed the brace to be placed
on the cadaveric specimen in a natural way. A similar method was applied in Hangalur et al
(Hangalur et al., 2015). The only major difference between these two methods was the
application of participant-specific muscle stiffness. Hangalur et al employed subject specific
muscle forces and kinematics similar to Cassidy et al (Cassidy et al., 2013). The replication of

20
participant-specific muscle stiffness further increased the fidelity of the simulation to replicate
the motion analysis with the brace.
21
Chapter 2 2
Hypotheses and Research Aims
2.1 Thesis Rationale
The purpose of this thesis was two-fold. First, we aimed to characterize and compare in-vitro
tissue strain during dynamic activities in ACL intact and reconstructed knees. Second, we
intended to test the effectiveness of a dynamically-tensioned functional ACL knee brace in
decreasing tissue strains.
Tissue strain response in the menisci is not well understood. The menisci are recognized as
essential structures in load transmission and stabilization of the knee. Clinically, meniscal strain
is relevant in ACL-competent (ACL intact and reconstructed) and ACL-deficient knees. It has
been shown that medial meniscal strain increases following ACL transection and reduces after
ACL reconstruction in static loading scenarios. This finding has not been tested under dynamic
loading conditions. In general, no reference values for meniscal strain under dynamic loading
scenarios have been established. In this thesis, the first purpose was to address some of these
gaps in knowledge.
Functional knee braces are commonly prescribed in the non-operative treatment of ACL injuries,
and as a post-operative rehabilitation tool after ACL reconstruction. Knee brace manufacturers
continue to develop new technologies to increase the efficacy of knee braces. New designs with
dynamic tensioning systems have recently been developed to apply directional forces to the knee
via a cabling system. These braces have been designed to apply higher magnitude directional
forces than static force braces. This type of brace system theoretically reduces the tissue strain in
the knee, helping protect the ACL and posteromedial meniscus after injury or reconstruction.
The efficacy of new dynamically tensioned brace designs has not been established. The second
purpose of this thesis was to examine the effects of the new dynamic knee tensioning system on
ACL and posteromedial meniscal strain during everyday activities and rehabilitation exercises,
using an in-vivo/in-silico/in-vitro testing method.
22
2.2 Thesis Hypothesis
We hypothesized that a dynamically tensioned ACL brace would be effective in reducing peak
and average tissue strain in ACL intact, deficient and reconstructed knees during rehabilitation
activities.
2.3 Thesis Outline
The experimental testing in this thesis was completed using a combined in-vivo/in-silico/in-vitro
method. During the in-vivo and in-silico phases, we measured bodily motions and foot-ground
reaction kinetics from a single participant during three activities, quantified joint kinematics,
inter-segmental reaction forces and moments, and muscle forces using a musculoskeletal model,
and used these data as inputs for the in-vitro cadaveric simulations. Dynamic simulations of the
three activities were performed on seven cadaver specimens with and without a dynamically
tensioned ACL brace. These simulations were repeated with the ACL intact, sectioned and
reconstructed.
The results from this work have been separated into two manuscripts prepared for submission to
academic journals. The first manuscript (Chapter 3) characterizes and validates tissue strains
under dynamic loading and compares meniscal strain between ACL intact and reconstructed
conditions. The second manuscript (Chapter 4) reports the effectiveness of the functional knee
brace. Chapter 5 is a general discussion of the findings as a whole, thesis contributions, and
future directions. Chapter 5 is followed by two appendices. Appendix 1 outlines an expanded
methodology that details the procedural steps of specimen preparation. Appendix 2 outlines
motion capture analysis and pilot testing required for the completion of the thesis.
Chapter 3: Dynamic Meniscal and ACL Strains are Maintained Following ACL
Reconstruction
*Manuscript Prepared for The Knee journal
Objective: To characterize ACL and meniscal strain during dynamic activities and to compare
the strain between ACL-intact and -reconstructed conditions. Dynamic activities include double
leg squat, single leg squat, and walking gait.
23
Hypothesis: There would be no statistical differences in peak strains between the ACL-intact and
-reconstructed conditions and ACL strain patterns will match established literature strain patterns
from in-vivo subjects.
Chapter 4: Efficacy of an ACL Functional Knee Brace with a Dynamic Tension System
*Manuscript Prepared for the American Journal of Sports Medicine
Objective: To evaluate the efficacy of a functional knee brace equipped with a dynamic
tensioning system to reduce meniscal strain in ACL deficient knees, and to reduce ACL and
meniscal strain in ACL competent knees.
Hypothesis: The brace would reduce peak and average ACL and meniscal strains in all
conditions.
24
Chapter 3 3
Dynamic Meniscal and ACL Strains are Maintained Following ACL Reconstruction
Abstract
Background: Meniscal strain following ACL reconstruction during dynamic activities has not
been studied. The purpose of this study was to characterize in-vitro meniscal strain during
dynamic loading, and compare strain between ACL-intact and -reconstructed conditions.
Methods: A combined in-vivo/in-silico/in-vitro method was used to measure strain in the medial
meniscus and ACL during walking gait, a double leg bodyweight squat (DLS), and a single leg
bodyweight squat (SLS). Seven cadaveric specimens were tested using a dynamic knee
simulator.
Results: Knee angle was found to be a significant factor in the development of ACL strain
during all activities, and meniscal strain during DLS and walking gait (P<0.05). Meniscal strain
was not found to be significantly different between ACL intact and reconstructed conditions for
any of the three activities (P>0.05).
Conclusions: Tissue strains in the meniscus were maintained following ACL reconstruction.
Based on the results of this study, ACL reconstruction appears to normalize meniscal strain in
the dynamic setting during functional activities. This may be protective against meniscal injury.
25
3.1 Introduction
The goals of anterior cruciate ligament (ACL) reconstruction surgery are to improve joint
stability and allow return to function and physical activity. To achieve these goals, modern
reconstruction techniques aim to closely replicate the anatomy of the native ACL (Karlsson et
al., 2011; van Eck et al., 2010). Careful consideration is given to graft location, size, tension, and
material properties (Guler et al., 2016; Kirwan, Bourke, Chipchase, Dalton, & Russell, 2013;
Robin et al., 2015). Regardless of the type of reconstruction, the risk of developing osteoarthritis
(OA) remains increased following surgery (Barenius et al., 2014; Lohmander et al., 2007;
Struewer et al., 2013). This increased risk is multifactorial, but likely influenced by the ability of
the graft to normalize tissue loading and prevent secondary damage to the menisci and articular
cartilage (Keays, Newcombe, Bullock-Saxton, Bullock, & Keays, 2010).
The medial and lateral menisci function to transmit and distribute joint loads and to stabilize the
knee. Following a meniscal tear, patients exhibit increased joint articular pressure and higher
rates of degenerative changes (P. Allen, Denham, & Swan, 1984; Krüger-Franke, Siebert,
Kugler, Trouillier, & Rosemeyer, 1999; Ode et al., 2012). In the ACL-deficient knee, the medial
meniscus functions as a secondary restraint to anterior tibial translation (ATT) (C. Allen et al.,
2000; I. Levy, Torzilli, & Warren, 1982). Hollis et al. showed that medial meniscal strain
increases when the ACL is transected, and reduces after the ligament is reconstructed (Hollis et
al., 2000). The loading conditions in their study were static and employed small force
magnitudes in both the anterior-posterior direction and in the axial plane. It remains unknown
how meniscal strain behaves under larger loads and dynamic conditions encountered in daily
living and exercise activities.
Direct measurement of meniscal strain in-vivo is not feasible. Strain can be measured during
dynamic loading conditions using knee simulators that apply dynamic loads to cadaveric
specimens. These simulators have the capability to apply high speed joint kinematics, joint
moments and dynamic muscle force profiles (Bakker et al., 2016; Cassidy et al., 2013). This
approach allows for direct control of muscle forces and measurement of intra-articular strain.
The primary objectives of this study were to characterize meniscal strain during dynamic
activities and to compare the strain between ACL-intact and -reconstructed conditions.
26
Additionally, we compared the ACL strain for the same conditions. We examined three
movements: double leg squat (DLS), single leg squat (SLS), and walking. These tasks represent
a daily, low-demand activity (walking) and common closed chain rehabilitation exercises
(squats) used to restore flexibility and build strength after an ACL injury or reconstruction.
We hypothesized that peak strains between the ACL-intact and -reconstructed conditions would
be similar, and that ACL strain magnitudes would match established literature strain patterns
from in-vivo subjects.
3.2 Methodology
A combined in-vivo/in-silico/in-vitro method was used to quantify knee tissue strains during
dynamic activities (Figure 6; pg 36). In this approach, body segment motion and force platform
data were recorded during various dynamic tasks. These data were then input into
musculoskeletal modeling software to quantify the forces of specific lower extremity muscles.
The computed muscle forces and joint kinematics were then applied to instrumented cadaver
knees in a dynamic knee simulator system.This study was approved by the University of
Waterloo Office of Research and Ethics.
In-Vivo Motion and Ground Reaction Force Capture:
Body segment motion and foot-ground interactive kinetics were recorded from a healthy, female
subject (age: 28 years) performing three activities: walking, DLS, and SLS. Although walking is
the primary activity of a healthy individual, DLS is an exercise incorporated into early
rehabilitation after ACL injury or reconstruction, while the SLS is a more challenging, advanced
exercise initiated later in the recovery program.
Rigid body clusters with active markers were secured to the participant’s thorax, pelvis, thighs,
shanks, and feet. A total of 36 anatomical landmarks were digitized with a probe (Bakker et al.,
2016). The participant was instructed to walk across the laboratory floor at her normal, self-
selected speed. The participant then performed a DLS and a SLS by squatting down as far as
possible while maintaining balance (Figure 6; pg. 36).
27
Four Optotrak Certus (NDI, Waterloo, ON, Canada) cameras recorded marker trajectories at a
sampling frequency of 64Hz. The corresponding ground reaction forces and moments were
collected at 2048Hz using four AMTI force plates (model OR6-7- 2000). Before the simulations,
kinematic and kinetic data was low pass filtered using a 10Hz, 4th order dual pass Butterworth
filter (Bakker et al., 2016; Kristianslund, Krosshaug, & van den Bogert, 2012).
The lower extremity and torso kinematic and kinetic data from one trial was used to generate
musculoskeletal simulations of each activity in OpenSim using the Gait2392 lower extremity
model (Scott L Delp et al., 2007). The Gait2393 model has 23 degrees-of-freedom and 92
musculotendinous actuators and has previously been used to simulate walking, running, and
single leg landings (Bakker et al., 2016; Hamner, Seth, & Delp, 2010; Laughlin et al., 2011; Liu,
Anderson, Schwartz, & Delp, 2008; Mokhtarzadeh et al., 2013).
The model was first scaled and inverse kinematics and dynamics were employed. The residual
reduction algorithm was implemented to reduce residual forces and moments. Muscle forces
were then estimated using computed muscle control algorithms (Scott L Delp et al., 2007; Thelen
& Anderson, 2006).
A full gait cycle was simulated including the swing and stance phases from toe-off to toe-off.
Squats were simulated from upright stance to the lowest point in the squat and back to starting
stance.
In-Vitro Mechanical Testing:
OpenSim sagittal joint kinematics, moments, and muscle forces for the quadriceps, hamstrings,
and gastrocnemius were used to drive the dynamic knee simulator (Figure 7; pg. 36) (Bakker et
al., 2016; Cassidy et al., 2013).
Seven cadaveric specimens were tested in the mechanical simulator. The cadavers were fresh
frozen from donors less than 50 years old with no history of lower extremity trauma or surgery.
Each specimen was dissected of all muscular tissue and associated tendons around the knee with
the exception of popliteus which contributes to joint stability (LaPrade, Wozniczka, Stellmaker,
& Wijdicks, 2010). The semi-tendinosis and gracilis tendons were harvested off their tibial
28
insertion and kept for later use in reconstructing the ACL. The patella, patellar tendon, joint
capsule, menisci, cruciate ligaments and collateral ligaments were preserved.
Braided stainless steel cables were placed at the insertion of the quadriceps, hamstrings, and
gastrocnemius muscles (Cassidy et al., 2013). The moment arm of each cable was measured
through a tendon excursion method and used to adjust the estimated muscle forces from
OpenSim to apply the equivalent in-vivo knee moment to the cadaver knees (S L Delp,
Ringwelski, & Carroll, 1994).
The strain in the periphery of the postero-medial meniscus was measured using a Differential
Variable Reluctance Transducer (DVRT, Lord Microstrain Inc., Burlington, VT) as detailed by
Pearsall et al. (2004) (Pearsall, 2004). A second DVRT was inserted in the anteromedial bundle
of the intact ACL and into the ACL graft after reconstruction.
Conditions Tested:
The knees were first tested with the ACL intact for each of the three activities: DLS, SLS, and
walking. Two trials were recorded for each testing condition. The ACL was then sectioned and
reconstructed, and all tasks were re-tested in the same order.
The ACL was reconstructed with a quadruple hamstring graft using the semi-tendinosis and
gracilis tendons harvested during the initial dissection. The tibial and femoral tunnels were
drilled under direct visualization through a mini, medial parapatellar arthrotomy using an antero-
medial technique. The graft was suspended on the femur using an XO-button (ConMed Linvatec,
USA) and secured in the tibial tunnel using a metal interference screw. The button was
visualized on the cortex to confirm it had flipped appropriately.
This study was conducted as part of a larger study investigating the effects of functional bracing
on tissue strains. Additional trials were performed on the specimens with the ACL transected. All
dynamic simulations were repeated with a functional knee brace.
Statistics:
29
Strain values were measured as relative strain with respect to the initial tissue strain at the
beginning of each trial.
Strain values were first normalized by subtracting the mean and dividing by the standard
deviation for each knee (Withrow, Huston, Wojtys, & Ashton-Miller, 2006). Anatomic variables,
such as structural properties and bone geometry, prevent a direct comparison of strain between
knees. Normalizing allowed for direct comparison of strain data across the specimens. ACL and
meniscal strain values were extracted at specific knee angles. For the squats, strain was extracted
in extension (EX), mid-flexion (MF, 45 degrees), and deep flexion (DF, max flexion angle
during the trial). During gait, the strain values were separated into swing phase (toe off – heel
strike) and stance phase (heel strike – toe off). Strain values were averaged for each phase and
for the two trials in each condition.
Three separate 2-way ANOVAs were conducted for ACL strain, one for each the three activities
(DLS, SLS, Gait). For each ANOVA, the factors included knee angle and ACL status. Three
additional ANOVAs were similarly conducted for meniscal strain. Tukey’s post hoc analysis
with a familywise correction factor was used for all significant ANOVA results. An alpha value
of .05 was set to determine statistical significance for all tests.
3.3 Results
The gait parameters were representative of a normal gait pattern defined by Oberg et al.(T
Oberg, Karsznia, & Oberg, 1993; Tommy Oberg, Karsznia, & Oberg, 1994) Walking speed was
1.9 steps/second, hip range of motion was 44.5 degrees, and the knee angle during mid-swing
and mid-stance was 65.5 and 12.8 degrees respectively. The DLS had a maximum knee flexion
angle of 83 degrees and duration of 1.80 seconds. The SLS had a peak knee angle of 81 degrees
and lasted 1.82 seconds.
The sagittal plane joint angles and joint moments, and the muscle force profiles of the
quadriceps, hamstrings, and gastrocnemius, as calculated in OpenSim, are provided in Figure 8
(pg. 37) for each of the three tasks.
The seven cadaveric knee specimens (4 male, 3 female) came from donors with an average age
of 41 years (range: 24 to 50 years) and a body mass index of 25 (range: 18 to 33). No weight-
30
bearing chondral lesions or meniscal tears were noted and there were no specimen failures during
testing. Meniscal strain data was not extracted from two knees due to mechanical failure of the
DVRT. ACL strain was extracted on all seven knees.
Average meniscal and ACL strain data from the seven specimens are illustrated in Figure 9 (pg.
38) and presented in Table 1 (pg. 35). The 2-Way ANOVA tables for meniscal and ACL strain
are presented in Table 1. Interactions between knee angle and ACL status were not found to be
significant in any of the six ANOVAs.
Knee angle was found to significantly affect meniscal and ACL strain in the DLS. Post hoc
analysis of meniscal strain revealed greater strain during MF (1.7%) compared to EX (0.5%). An
opposite relationship was found for the ACL; strain was higher in extension (0.4%) than either
mid (-0.4%) or deep flexion (-6.6%). In addition, the native ACL strain was found to be
statistically lower than in the reconstructed ligament.
During SLS, ACL strain was found to be lower in DF (-11.6%) and MF (-5.4%) than in EX
(0.3%). While walking, strain in both tissues was found to be higher during stance than swing
phase (ACL: 3.0% Stance, 9.1% Swing. Meniscus: 0.2% Stance, 1.3% Swing). ACL
reconstruction was not found to significantly impact meniscal or ACL strain during SLS or
walking gait.
3.4 Discussion
The current study characterized ACL and meniscal strain during DLS, SLS, and walking gait,
and compared the strains pre and post ACL reconstruction. We found that meniscal strain was
not significantly different after the reconstruction procedure for any of three activities. Strain
patterns for the ACL matched data available in the literature.
Double-leg squats are a commonly recommended early physiotherapy exercise post ACL
reconstruction. The level of difficulty is low and the exercise is perceived as safe to the integrity
of the reconstructed ligament (Button, Roos, & Van Deursen, 2014). The ACL strain results from
this study confirm this conclusion. The average relative strain never exceeded 3% and the strain
curve mostly followed an inverse parabolic pattern (Figure 9).
31
While the ACL strain during the flexion phase of DLS decreases, the posterior-medial meniscal
strain increases up to MF and then decreases in DF. This may be counterintuitive as the meniscus
is thought to be a secondary restraint to ATT (Hollis et al., 2000), which is correlated with
increased ACL strain (Butler & Anonymous, 1989). The increase in meniscal strain is likely
explained by the elliptical shape of the condyles (Yoshioka et al., 1987). As the knee begins to
flex, the contact area of the medial condyle on the posterior meniscal horn increases therefore
straining the tissue. With further flexion, the ellipse apex is past the posterior meniscus and the
strain decreases (Figure 9).
Single-leg squats are a more demanding exercise requiring larger muscle forces. SLS showed
similar trends in the ACL strain to the DLS, decreasing in strain as the flexion angle increases.
However, this decrease in relative strain was larger than DLS. This may be explained by a 50%
larger hamstring force which provides a posterior force to the tibia (Herzog & Read, 1993).
Meniscal strain during SLS showed a similar strain pattern to DLS in the flexion phase. The
strain increases during the first 45 degrees of flexion but then decreases. The average strain was
smaller than in DLS which may again be related to a larger hamstring force.
Walking is a basic day-to-day activity that patients need to perform quickly after surgery. ACL
strain during the gait trial was almost always positive. Similar to Taylor et al, the ACL strain was
higher in stance phase than in swing (K. a Taylor et al., 2013). Meniscal strain during walking
also showed a relative increase in strain with a similar pattern between stance and swing phases.
The results from this study suggest that walking causes more strain on the ACL and meniscus
than either DLS or SLS. These results further validate the safety of DLS and SLS post-surgery
with respect to ACL and meniscal strain.
The goals of ACL reconstruction are to restore knee stability and normalize tissue loading. The
effectiveness of the graft can be evaluated by comparing ACL and meniscal strain between intact
and reconstructed states. Our results showed ACL strain was not significantly different during
walking and SLS. In DLS there was a small, 2.3% average increase following reconstruction.
Although statistically significant, this difference is not detrimental because the overall strain
decreases during the activity. The difference may be due to tensile properties mismatch between

32
the hamstring tendons and the native ACL tissue. In addition, similar strain patterns between the
intact and reconstructed conditions indicate correct geometric placement of the graft.
The current study found no significant differences in meniscal strain after ACL reconstruction
during DLS, SLS, and walking gait. Following reconstruction, meniscal strain appeared to be
lower during the stance phase of gait, but this difference was not statistically significant. A post
hoc power analysis revealed that a sample size between 20-60 knees, depending on the activity,
would be required to detect a difference in meniscal strain after ACL reconstruction. This
indicates that if there is a difference, it would be relatively small. The current study did not
investigate the effects of ACL deficiency on meniscal strain; however, previous studies report an
increase in strain in ACL-deficient knees (Hollis et al., 2000). Results from the current study
indicate ACL reconstruction was able to normalize, or possibly reduce, meniscal loading.
Although this study confirms the findings of Hollis et al that ACL surgery can help protect the
meniscus (Hollis et al., 2000), it is the first study to demonstrate this effect during dynamic
activities.
Previous cadaveric studies examining meniscal strain have used static loads that are not
necessarily representative of real world loading conditions. In the present study, we aimed to test
specimens in a dynamic knee simulator with inputs that accurately replicate the motion and
muscle forces present during walking and squatting. A set of standardized, “average” kinematic
and muscle force data is not available, nor possible to calculate, for a dynamic simulation as any
averaging would violate the equations of motions and the consistency of the system. Testing
multiple motion patterns from multiple individuals is also not feasible due to limitations in the
ability of the specimens to withstand numerous trials.
Nonetheless, it was important to select representative gait and squat patterns and validate the
simulations with previous literature. The gait trial matched the parameters reported by Oberg et
al for a normal, age-matched gait pattern (T Oberg et al., 1993; Tommy Oberg et al., 1994). The
literature lacks sets of standardized kinematic data on DLS and SLS. We chose representative
squat trials with regard to knee angle and duration of each squat.
Musculoskeletal simulations of these activities produced results that fell within the guidelines
outlined by OpenSim and Hicks et al for kinematic errors and dynamic consistencies (Hicks,
33
Uchida, Seth, Rajagopal, & Delp, 2015). The maximum kinematic rotational error found was 3.2
degrees, and the translational error was less than 1cm. Residual forces were less than 30N and
residual moments were less than 12Nm. During gait, the activation patterns of rectus femoris,
biceps femoris, and the medial gastrocnemius closely matched the respective activation patterns
reported by Liu et al (Liu et al., 2008).
Further validation of the overall methodology used in this study comes from comparing the
measured ACL strain with previous in-vivo results. Beynnon et al measured ACL strain during
DLS for eight subjects using a DVRT (B D Beynnon & Fleming, 1998). The flexion-extension
curve in Figure 10 (pg. 38) shows the similarity in strain pattern between those results and the
current ones. The strain decreases with flexion until 80 degrees and increases as the knee extends
along a path that is lower from its flexion angle counterpart.
Taylor et al. studied in-vivo ACL strain during walking using a combination of motion capture,
MRI, and fluoroscopy (K. a Taylor et al., 2013). Both the current study and Taylor et al found
maximum strain occurs close to terminal knee extension with strain values of 10.9% and 13%
respectively. The second peak in strain occurs just prior to heel strike reaching 10.6% and 10%
respectively. Although peak strain values differ by an average of 2.1%, it is important to note
that the studies were conducted using different techniques for measuring strain. Overall, the
strain patterns were similar in both the stance and the swing phase. Comparison of the strain
patterns are presented in Figure 11 (pg. 39). Direct graphical comparison of the strain
magnitudes is not possible because Taylor et al represented the data as ACL length and not
strain.
This study has several limitations. The current study investigated the effects of ACL
reconstruction on three activities using one individual’s kinematic/muscle force profiles. Thus,
the validity relies on the selection of representative movement patterns. We believe that the
careful selection of the gait and squat trials alleviates some of the concern. Furthermore, these
patterns are representative movement patterns of a healthy subject without an ACL injury. Gait
parameters can change after an injury but tend to normalize after reconstruction, returning to pre-
injury patterns after at least eight months (Knoll, Kiss, & Kocsis, 2004). The effects of early
rehabilitation pattern changes on the tissue strains was not investigated in this study. These
34
results may also depend on the quality of the reconstructions. The procedures were performed by
a fellowship trained orthopedic surgeon with experience in ACL reconstruction using modern
surgical tools. Lastly, the conditions tested were a subset of a larger study that investigated the
effects of braces. Additional tests were conducted in-between the trials, which may raise
concerns about tissue degradation. However, the results of this study found the strain in the
meniscus did not change between conditions.
In conclusion, we characterized meniscal strain during dynamic activities and compared
meniscal and ACL strain between ACL-intact and -reconstructed knees. We found that tissue
strains were higher during gait than during SLS and DLS. Meniscal strain did not differ between
ACL-intact and-reconstructed knees. These results provide insight into tissue loading following
ACL reconstruction and may help in further understanding the risk of developing osteoarthritis
after ACL injury.

35
Table 1. ACL and Meniscal Strain Values for All Activities. Strain values are presented as a
mean ± standard deviation. ANOVA P-values for ACL status are presented in horizontal
brackets. ANOVA P-values for knee angle and gait phase are presented in vertical brackets.
Knee angle and gait phase was correlated to meniscal and ACL strain for most conditions.
Meniscal strain was not statistically different between ACL-intact and -reconstructed conditions.

36
Figure 6. Experimental Overview. (1) In-vivo motion capture setup, (2) OpenSim
musculoskeletal model, (3) Dynamic knee simulator.
In-Silico Musculoskeletal Simul
A B C
Figure 7. Motion Capture Activities. (A) Double leg squat, (B) single leg squat, (C) gait.
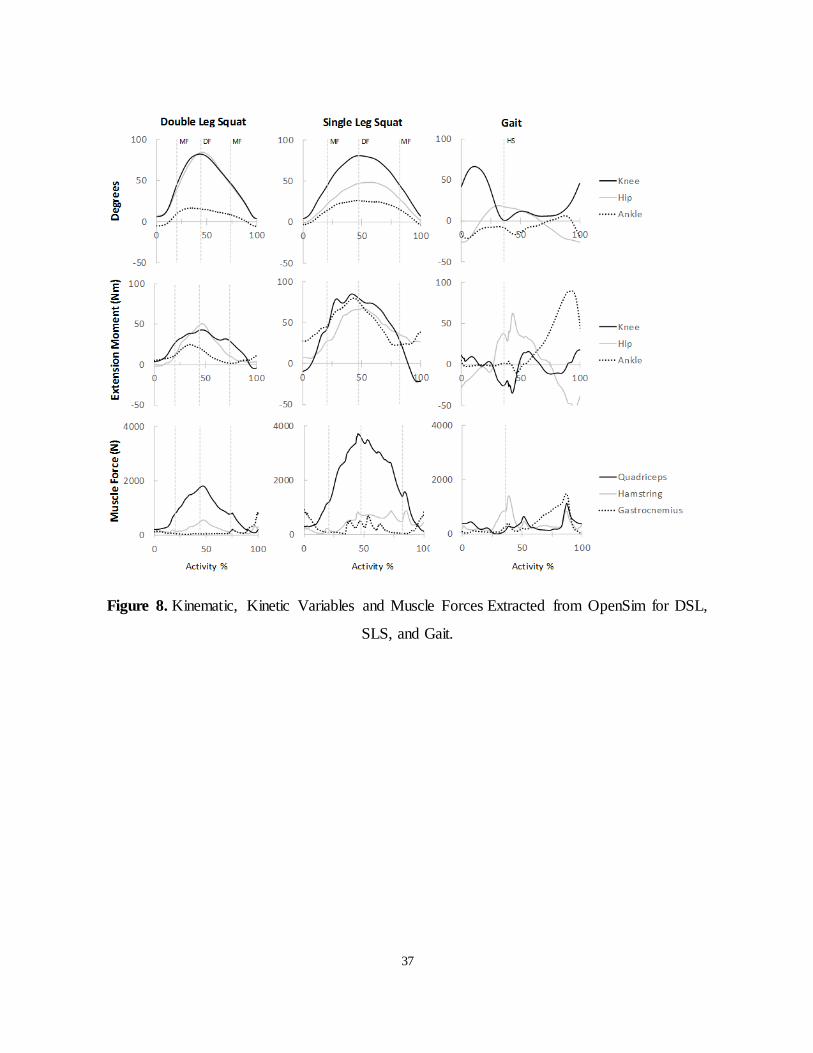
37
Figure 8. Kinematic, Kinetic Variables and Muscle Forces Extracted from OpenSim for DSL,
SLS, and Gait.
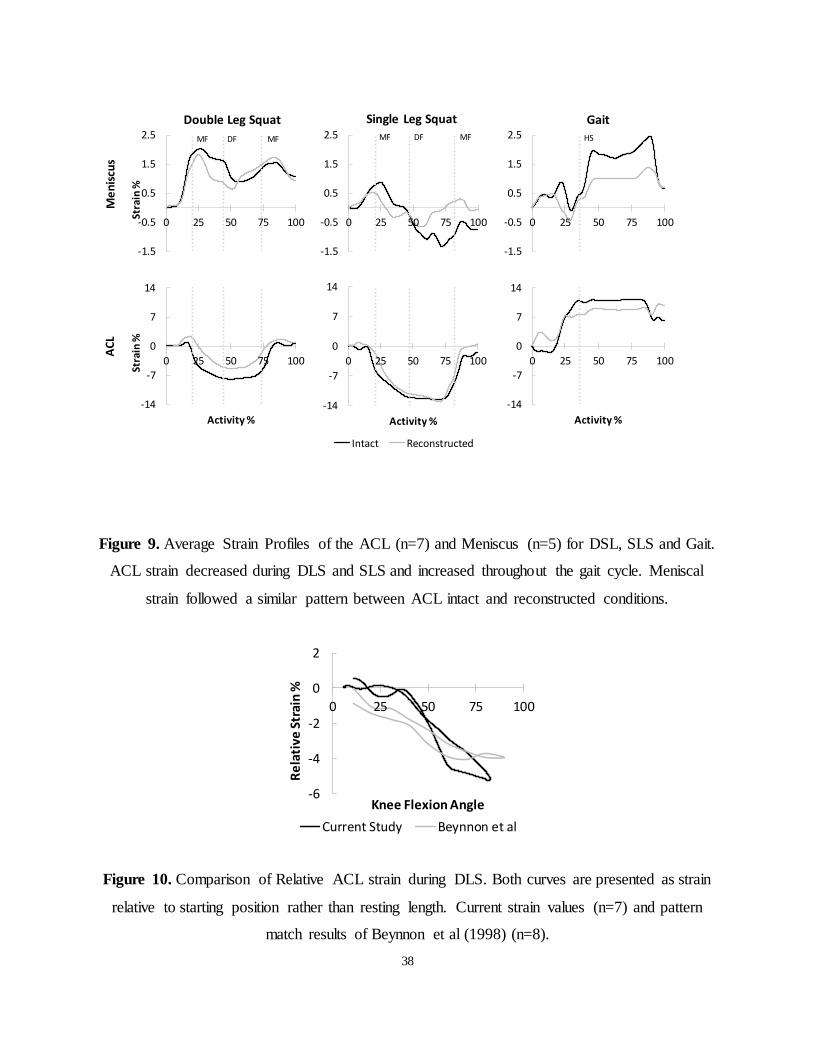
38
Figure 9. Average Strain Profiles of the ACL (n=7) and Meniscus (n=5) for DSL, SLS and Gait.
ACL strain decreased during DLS and SLS and increased throughout the gait cycle. Meniscal
strain followed a similar pattern between ACL intact and reconstructed conditions.
Figure 10. Comparison of Relative ACL strain during DLS. Both curves are presented as strain
relative to starting position rather than resting length. Current strain values (n=7) and pattern
match results of Beynnon et al (1998) (n=8).
-1.5
-0.5
0.5
1.5
2.5
0 25 50 75 100
Single Leg Squat
-14
-7
0
7
14
0 25 50 75 100
Stra
in %
Activity %-14
-7
0
7
14
0 25 50 75 100
Activity %
Intact Reconstructed
-14
-7
0
7
14
0 25 50 75 100
Activity %
-1.5
-0.5
0.5
1.5
2.5
0 25 50 75 100
Stra
in %
Double Leg Squat
-1.5
-0.5
0.5
1.5
2.5
0 25 50 75 100
GaitM
en
iscu
sA
CL
MF MFDFMF MFDF HS
-6
-4
-2
0
2
0 25 50 75 100
Re
lati
ve S
trai
n %
Knee Flexion Angle
Current Study Beynnon et al
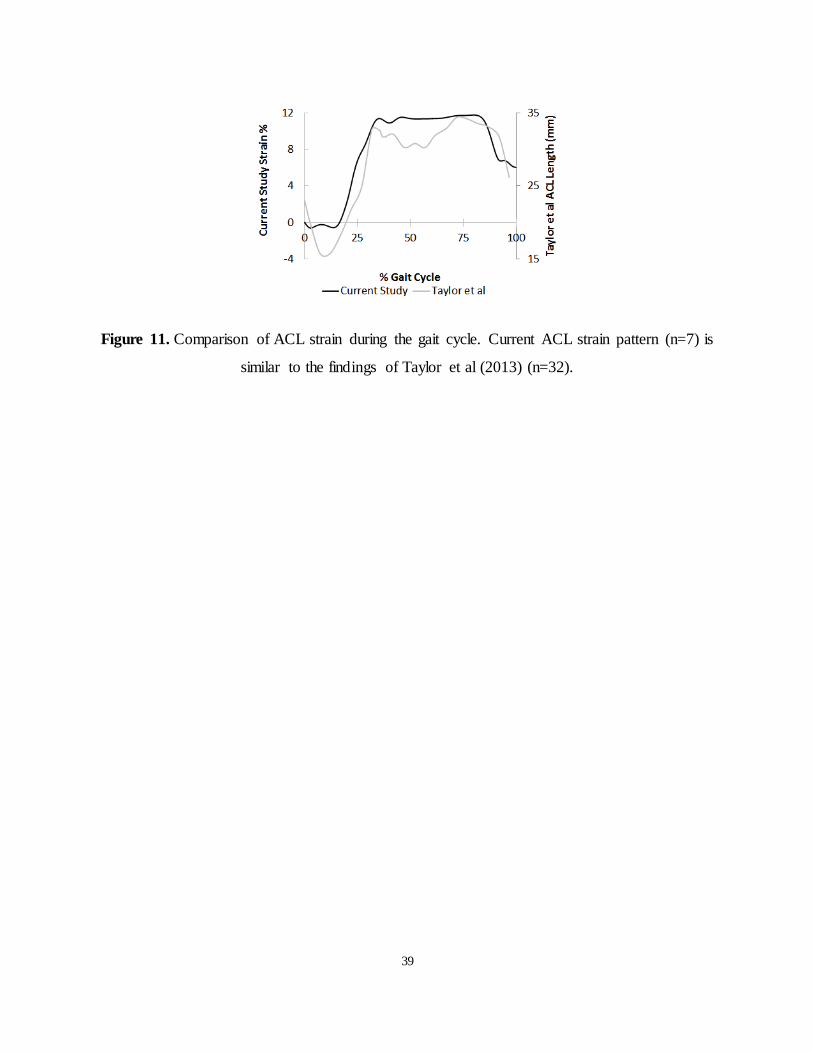
39
Figure 11. Comparison of ACL strain during the gait cycle. Current ACL strain pattern (n=7) is
similar to the findings of Taylor et al (2013) (n=32).
40
Chapter 4 4
Efficacy of an ACL Functional Knee Brace with a Dynamic Tension System
Abstract
Background: The effectiveness of ACL functional knee braces to reduce meniscal and ACL
strain remains poorly understood. A new dynamic knee tensioning brace system has been
designed to apply larger stabilizing forces to the knee. The ability of this system to reduce tissue
strains is unknown.
Purpose: The purpose of this study was to test the ability of the dynamically tensioned brace to
reduce strain in both the ACL and meniscus during dynamic activities.
Methods: A combined in-vivo/in-silico/in-vitro method was used to study three activities: gait, a
double leg squat, and a single leg squat. Medial meniscal strain and ACL strain were measured in
ACL intact, deficient and reconstructed conditions. Custom braces were fitted on seven
cadaveric specimens using surrogate foam.
Results: The brace lowered peak and average meniscal strain in ACL deficient knees (P<.05) by
an average of 1.65%. The brace was also found to lower meniscal strain in reconstructed knees
(1.07%) and lower ACL strain in ACL intact (1.34%) and ACL reconstructed knees (1.35%)
(P<.05).
Conclusions: This study supports the use of a brace equipped with a dynamic tensioning system
to lower meniscal strain in ACL-deficient knees. Its use may help decrease the risk of subsequent
meniscal tears in chronic ACL deficiency or delayed reconstruction. In ACL-intact and -
reconstructed knees, the brace may be beneficial in injury prophylaxis or in protecting the ACL
graft following reconstruction.

41
4.1 Introduction
The primary function of the anterior cruciate ligament (ACL) is to prevent anterior translation of
the tibia on the femur. Following an ACL tear, anterior tibial translation (ATT) increases,
resulting in instability (Andriacchi & Dyrby, 2005). Functional knee braces (FKB) aim to
maintain or re-establish the normal kinematic state of the knee with the ultimate goal of
providing knee stability during daily and sporting activities. Functional knee braces are
commonly prescribed to limit instability in patients with ACL deficiency, and to protect the graft
after ACL reconstruction (Chew et al., 2007). Additionally, functional bracing may be
considered for prophylactic use to prevent injury (Najibi, 2005).
The efficacy of bracing has been investigated in ACL-intact, -deficient, and -reconstructed
knees. In the intact state, prophylactic brace use in military recruits was found to reduce the
number of ACL and medial collateral ligament injuries, but not the severity (Sitler et al., 1989).
In-vivo studies using implanted strain gauges have demonstrated bracing is more effective in
reducing ACL strain during non-weight bearing compared to weight bearing activities (Braden C
Fleming et al., 2000), and for low compared to high applied loads (B D Beynnon et al., 1992).
The overall data on the effectiveness of prophylactic braces is conflicting and a recommendation
for or against their use cannot be conclusively made (Pietrosimone, Grindstaff, Linens, Uczekaj,
& Hertel, 2008).
In ACL deficient knees, the medial meniscus becomes a secondary restraint to ATT (Allen et al.
1995; Allen et al. 2000; Levy et al. 1982). As a result, the meniscus is at risk for subsequent
injury, which in the long term may be linked to the development of osteoarthritis. Cadaveric
testing after sectioning the ACL demonstrated reduced ATT when braced (Anderson et al., 1992;
Bruce D Beynnon et al., 2003; E M Wojtys et al., 1990). Clinically, patients with a torn ACL
report improved subjective stability, and experience fewer episodes of instability when wearing a
brace (Marans et al., 1991; Mishra et al., 1989). Although FKBs have been shown to reduce ATT
and subjective instability, no data exist to demonstrate whether they decrease strain in the medial
meniscus.
42
Lastly, FKBs can be prescribed during the rehabilitation period following an ACL reconstruction
to protect the graft. The graft-tunnel interface is the weakest link of the reconstruction until
osseo-integration occurs, and up to 66% of surgeons recommend braces to protect the graft
(Spindler & Wright, 2008). Clinically, functional bracing has not been shown to influence pain,
range-of-motion, or graft stability (Wright & Fetzer, 2007); however, subsequent injury may be
decreased in certain activities (Sterett, 2006).
Historically, FKBs stabilize the knee via a rigid shell and a hinge joint. Recently, a new FKB
design uses a dynamic tensioning systems (DTS) to apply directional force to the femur via a
tensioning cable (LaPrade et al., 2015). The Rebound ACL brace (Össur, Foothill Ranch, CA,
USA) applies an angle-dependent posterior force to the femur, theoretically reducing ATT. The
efficacy of the DTS system has not been biomechanically validated to stabilize ACL deficient or
ACL competent (intact and reconstructed) knees.
The objective of this study was to evaluate the efficacy of a FKB equipped with a dynamic
tensioning system to reduce meniscal strain in ACL-deficient conditions and to reduce ACL and
meniscal strain in ACL competent conditions (ACL-intact and -reconstructed) during walking
gait and squatting. We hypothesized that the brace would reduce peak and average ACL and
meniscal strains in all conditions.
4.2 Materials and Methods
A combined in-vivo/in-silico/in-vitro method (Bakker et al., 2016; Cassidy et al., 2013; Hangalur
et al., 2015) (Figure 12; pg. 51) was used to test the effectiveness of an ACL functional brace
with a DTS system during three functional activities: walking gait, double leg squat (DLS), and
single leg squat (SLS). This study was approved by the University of Waterloo Office of
Research and Ethics.
In-Vivo
Body kinematics and foot-ground reaction kinetic data was collected for a female participant
(age 28) while performing the three selected activities. An Optotrak Certus system (NDI,
Waterloo, ON, Canada) with four cameras recorded the trajectory of 36 different anatomical
landmarks (Bakker et al., 2016), and four AMTI force plates (model OR6-7- 2000) were used to

43
collect ground reaction forces and moments. Before the simulations, the kinematic and kinetic
data was low pass filtered using a 10Hz, 4th order dual pass Butterworth filter (Bakker et al.,
2016; Kristianslund et al., 2012).
The participant’s contracted thigh compliance was measured using a muscle hardness testing
apparatus (Hangalur et al., 2015). These measurements were used to replicate the soft tissue
envelope on the cadaveric specimens used in the experiments.
In-Silica
The marker trajectories were processed in OpenSim (Delp et al., 2007) to obtain the joint
kinematics and muscle force profiles of the three activities. The process involved scaling the
standardized Gait2392 model and performing inverse kinematic analysis to calculate the
kinematic trajectories of the joints. Subsequently, the Residual Reduction Algorithm was used to
reduce the dynamic inconsistencies between the kinematics and the force plate data. Lastly, the
Computed Muscle Control tool was used to calculate the muscle force profiles for each activity.
DLS and SLS trajectories were simulated from standing through deep flexion and back up to
stance. The gait trial was simulated from toe-off to toe-off. All simulations were completed
following guidelines provided in Hicks et al and from the OpenSim website (Hicks et al., 2015).
Muscle forces were corrected for the cadaveric moment arms as described in Bakker et al, and
used along with the kinematics as inputs to the in-vitro knee simulator (Figure 12) (Bakker et al.,
2016).
Specimen Preparation
Seven fresh frozen cadaver knees ranging in age from 24 to 50 years (mean = 35 years) and a
body mass index range of 18 to 33 kg/m2 (mean = 25 kg/m2) were used in this study. Prior to
dissection, a negative mold was taken of the soft tissue envelope for each specimen. All soft
tissue was removed with the exception of the popliteus muscle and tendon (LaPrade et al., 2010).
The joint capsule was preserved. Stainless steel cables were then inserted at the tendon insertion
points of the gastrocnemius, hamstrings, and quadriceps muscle groups (refer to appendix A)
(Bakker et al., 2016; Cassidy et al., 2013; Hangalur et al., 2015).
44
The specimens were placed into the respective negative molds and stainless steel conduit was
used to run the braided wire from the insertion sites to edges of the mold. Medium-firm density
SunMate liquid foam (DSI, North Carolina, USA) was mixed and poured into the negative mold.
The mixture of the foam was adjusted to match the muscle tissue compliance of the participant.
The average compliance of the foam mixture was 0.084 mm/N.
The moment arm of each of the three muscle cables was measured using a tendon excursion
method outlined (S L Delp et al., 1994). These moment arms were used to adjust the in-silica
muscle forces extracted from OpenSim to produce the same net in-vivo joint moments about the
knee (Bakker et al., 2016; Cassidy et al., 2013; Hangalur et al., 2015).
In-Vitro Testing
Custom fit Rebound ACL braces were obtained based on the specimen soft-tissue envelope and
mounted on the cadaveric specimens. Each DTS was tensioned using the torque shear knob,
which shortens the cable length and forces the femur anteriorly with respect to the tibia (Figure
13; pg. 64).
Two Differential Variable Reluctance Transducers (DVRT, Lord Microstrain Inc., Burlington,
VT) were used to measure tissue strains. One DVRT was placed on the periphery of the postero-
medial meniscus, as explained by Pearsall et al (Hollis et al., 2000). The second DVRT was
placed on the anteromedial bundle of the ACL and into the anterior strands of the reconstructed
graft.
The specimens were mounted on the dynamic knee simulator system (Jonsson & Kärrholm,
1990; LaPrade et al., 2015) and tested with and without braces. Testing was performed first with
the ACL intact for the three activities: walking gait, DLS, and SLS. The ACL was sectioned
using a scalpel and testing was repeated for each activity. Finally, the ACL was reconstructed
and the three activities were repeated. The order of bracing (braced / not braced) was randomized
within each activity, while the order of activities was tested in the same sequence each time. Two
trials were performed in each testing condition to ensure repeatability.
The ACL was reconstructed using a quadruple hamstring graft, prepared from harvested semi-
tendinosis and gracilis tendons from the same specimen. Tibial and femoral tunnels were drilled
45
under direct visualization through a mini parapatellar arthrotomy. The tibial tunnel was drilled at
45 degrees and placed at the posterior aspect of the anterior horn of the lateral meniscus and
within the stump of the native ACL. The femoral tunnel was made independent of the tibial
tunnel using an offset guide. The grafts were either 8.0 or 8.5mm in diameter and each graft was
tensioned to 60N at 30 degrees of flexion (Heis & Paulos, 2002). A titanium interference screw
was inserted in the tibial tunnel to secure the graft and a suspensory XO-button (ConMed
Linvatec, USA) was used for the femur.
Statistics
For ease of readability, the term “condition” will refer to a simulation trial of activity (DLS, SLS
or gait), ACL status (intact, deficient, reconstructed) and brace (not braced – NB, braced – BR).
Strain data for each of the two trials for every condition were averaged. Relative strain was
calculated as a percentage in reference to the initial length of the DVRT in the non-braced
condition.
Peak and average strain values were extracted for every condition. A two-way RM ANOVA was
performed for each tissue strain. The factors included the main effect of bracing on tissue strain,
the interaction between bracing and ACL status, and the interaction between bracing and
activity. The three-way interaction between brace, activity, and status was also included and
tested in the ANOVA. Any significant differences were compared using a post-hoc paired t-test
with a Bonferroni correction factor. All statistical analysis was completed using SPSS software
with an alpha value of 0.05 (Stephen et al., 2016).
4.3 Results
Kinematic and muscle force inputs extracted from OpenSim and used as simulator inputs are
shown in Figure 14 (pg. 52). Peak knee flexion angle was 83 degrees in DLS and 81 degrees in
SLS. Quadriceps muscle force peaked at 1809N in DLS and 3725N in SLS. During gait, knee
flexion during mid swing was found to be 65.5 degrees and 12.8 degrees in mid stance.
Meniscal Strain
46
The brace significantly decreased peak meniscal strain (P<.01). Peak strain difference between
braced and unbraced conditions was 0.26 with the ACL intact, 1.65 with the ACL deficient, and
1.06 following ACL reconstruction (Figure 15; pg. 53). The differences represent a percent
reduction in strain of 13%, 74%, and 60%, respectively (Table 2; pg. 51). A significant
interaction effect was found between bracing and ACL status (P=0.03). Subsequent post-hoc
pairwise comparisons showed these differences to be significant in ACL deficient (P<0.01) and
reconstructed knees (P<0.01), but not in ACL intact knees (P=0.47).
Across the three activities tested, peak meniscal strain differences for DLS, SLS, and gait were
1.27, 0.83, and 0.86, respectively. These differences respectively correspond to percent decreases
of 61%, 95%, and 29%. No interaction was found between bracing and activity (P=0.62).
Average meniscal strain was also significantly reduced by the brace (P<.01). There were no
significant interactions between the brace and ACL status or activity.
ACL Strain
The brace lowered peak and average ACL strain in both ACL intact and reconstructed knees
across every activity (P=0.01). Strain differences were found to be similar, 1.34 with the ACL
intact and 1.35 with the ACL reconstructed (Figure 16; pg. 53). These values translate to a
reduction of 24% and 22% in peak strain, respectively (Table 2). No significant interaction was
detected between brace and ACL status (P=0.99). Similarly, the brace reduced ACL strain in
every activity by 83% in DLS, 38% in SLS, and 6% in gait.
4.4 Discussion
The current study found that a dynamically tensioned ACL FKB reduces posteromedial meniscal
strain in the ACL deficient state, and reduces ACL and meniscal strain in the ACL intact and
reconstructed conditions.
The effectiveness of the brace was tested across three activities typically performed while
wearing an FKB – a low-demand activity (walking gait), and two closed-chain rehabilitation
exercises (SLS, DLS). The in-vivo kinematics, in-silica muscle forces, and in-vitro ACL strains
were compared to previous literature to assess the accuracy of the input parameters. The gait
kinematics shown in Figure 13, fell within one standard deviation of accepted normative
47
parameters (T Oberg et al., 1993; Tommy Oberg et al., 1994). Quadriceps and hamstring muscle
activations closely followed the trends published by Liu et al (Liu et al., 2008). Peak ACL strain
during gait in the ACL intact condition (12.6%) matched the peak strain (13%) reported by
Taylor et al (Taylor et al., 2013). In the DLS, the ACL strain pattern had an inverse relationship
to the knee angle, similar to the in-vivo pattern found by Beynnon et al (Beynnon & Fleming,
1998). The strain difference between stance and deep flexion was also similar: 5.7% in the
current study versus 4.1% (Beynnon & Fleming, 1998). Overall, the simulations were found to
be representative of average gait and squats.
ACL Deficient Knees
The medial meniscus has been shown to act as a secondary stabilizer in the ACL deficient state
Levy, Torzilli, & Warren, 1982). The strain in the posteromedial meniscus increases after an
ACL tear, which places the meniscus at a higher risk of tearing (Lee et al., 2006). In the long
term, chronic ACL deficient knees have a higher incidence of medial meniscal tears and
associated articular damage (Mitsou & Vallianatos, 1988). By limiting anterior translation, FKBs
stabilize the knee and theoretically reduce meniscal strain. No studies to date have investigated
whether FKBs can reduce meniscal strain. Orthopedic surgeons and primary care sports
physicians who routinely prescribe FKBs do not understand whether an FKB can be used safely
to reduce the risk of meniscal injury and the burden of subsequent post-traumatic arthritis in
patients who are awaiting ACL reconstructions, or those who choose to not to undergo
reconstruction.
The brace lowered peak meniscal strain in ACL deficient knees by 1.65%. While this represents
a large percent change (74%) in relation to the peak strain, a more meaningful comparison is to
the ultimate (failure) strain of the tissue. Hauch et al determined the ultimate strain in the menisci
of eight human cadaveric specimens to be between 9.00% and 11.35% (Hauch, Villegas, &
Donahue, 2011). The average reduction in peak strain found in this study represents a 15%
reduction in ultimate strain. Therefore the strain reduction may translate to a clinically significant
effect if the loading condition brings the tissue close to failure (tearing).
The majority of previous studies have investigated anterior-posterior laxity in non-weightbearing
conditions and have shown that braces can be effective in decreasing ATT (Anderson et al.,
48
1992; Jonsson & Kärrholm, 1990; Mishra et al., 1989). Beynnon et al. extended this work by
reproducing the loading environment in weightbearing (Beynnon et al., 2003). The authors found
braces to normalize tibial translation in both weightbearing and non-weightbearing conditions
but not during the transition between the two. This transition phase regularly occurs in dynamic
activities, such as heel strike during gait, landing from a jump, or changing direction when
pivoting. Overall, the loads tested in past studies were small and applied in a static manner,
which does not reflect the rigors of dynamic loading experienced during daily and athletic
activities. It has been hypothesized that FKBs may not be effective under higher load conditions,
when patients depend on a brace for protection (Chew et al., 2007).
We tested three activities with the aim of reproducing dynamic conditions across a variety of
loads. The peak DLS ground reaction force was 387N or 57% body weight. The load is of
similar magnitude to Beynnon et al, who applied 40% body weight (Bruce D Beynnon et al.,
2003). SLS had substantially higher forces with a peak GRF of 850N or 125% body weight and
a peak quadriceps force of 3800N. The gait simulation comprised a full cycle including the
transition from swing phase through heel strike and stance phase.
We found the brace to lower strain across all activities. There was no significant interaction
between brace and activities. The brace did appear to have a larger effect during DLS than SLS,
indicating that perhaps effectiveness may indeed be decreased under higher loads. Due to the
small sample size, however, we were underpowered to detect a difference. A post-hoc power
analysis revealed that a sample size of 188 knees would be required to detect a difference, which
indicates that if a difference exists, the magnitude of the difference would be very small.
These results may assist clinicians when prescribing braces. The observed reduction in meniscal
strain across all activities indicates that brace at least in theory may help decrease the risk of
meniscal injuries in ACL deficient knees. Braces with a dynamic tensioning system may help
alleviate the concern of a subsequent meniscal injury while awaiting reconstruction.
ACL Competent Knees
The value of bracing for injury prophylaxis or for functional protection of a newly reconstructed
graft has been thoroughly investigated. Standard functional ACL braces which rely on a rigid
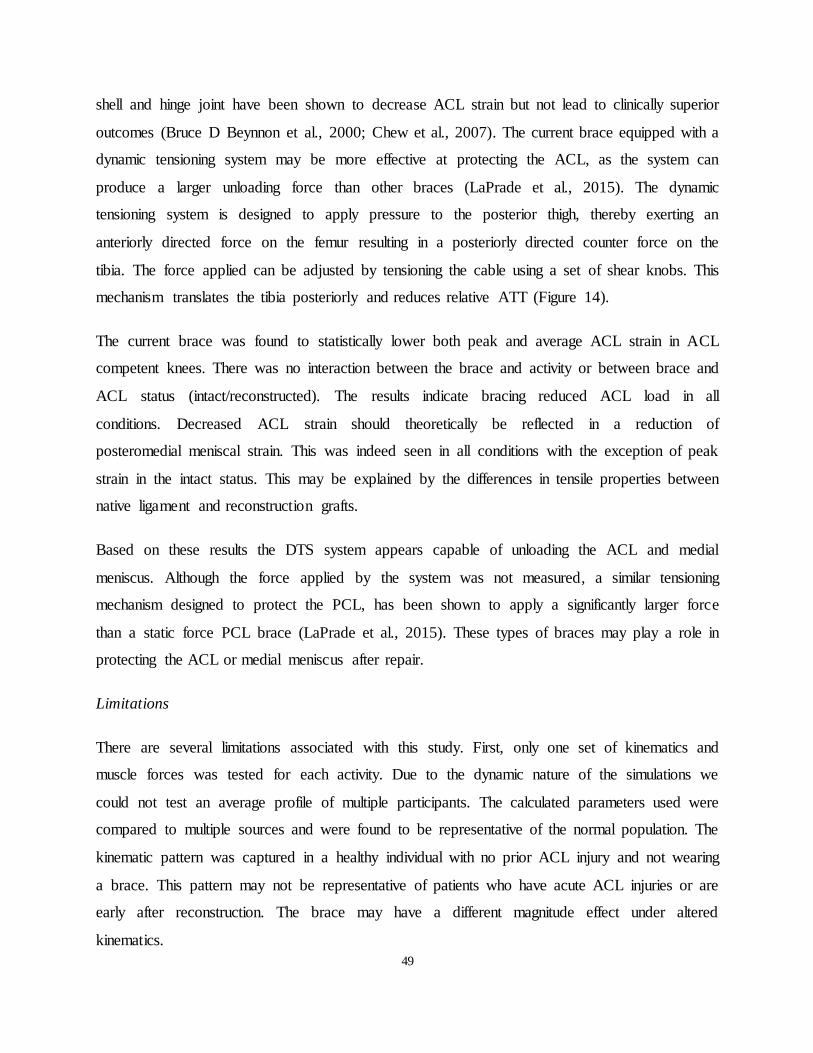
49
shell and hinge joint have been shown to decrease ACL strain but not lead to clinically superior
outcomes (Bruce D Beynnon et al., 2000; Chew et al., 2007). The current brace equipped with a
dynamic tensioning system may be more effective at protecting the ACL, as the system can
produce a larger unloading force than other braces (LaPrade et al., 2015). The dynamic
tensioning system is designed to apply pressure to the posterior thigh, thereby exerting an
anteriorly directed force on the femur resulting in a posteriorly directed counter force on the
tibia. The force applied can be adjusted by tensioning the cable using a set of shear knobs. This
mechanism translates the tibia posteriorly and reduces relative ATT (Figure 14).
The current brace was found to statistically lower both peak and average ACL strain in ACL
competent knees. There was no interaction between the brace and activity or between brace and
ACL status (intact/reconstructed). The results indicate bracing reduced ACL load in all
conditions. Decreased ACL strain should theoretically be reflected in a reduction of
posteromedial meniscal strain. This was indeed seen in all conditions with the exception of peak
strain in the intact status. This may be explained by the differences in tensile properties between
native ligament and reconstruction grafts.
Based on these results the DTS system appears capable of unloading the ACL and medial
meniscus. Although the force applied by the system was not measured, a similar tensioning
mechanism designed to protect the PCL, has been shown to apply a significantly larger force
than a static force PCL brace (LaPrade et al., 2015). These types of braces may play a role in
protecting the ACL or medial meniscus after repair.
Limitations
There are several limitations associated with this study. First, only one set of kinematics and
muscle forces was tested for each activity. Due to the dynamic nature of the simulations we
could not test an average profile of multiple participants. The calculated parameters used were
compared to multiple sources and were found to be representative of the normal population. The
kinematic pattern was captured in a healthy individual with no prior ACL injury and not wearing
a brace. This pattern may not be representative of patients who have acute ACL injuries or are
early after reconstruction. The brace may have a different magnitude effect under altered
kinematics.
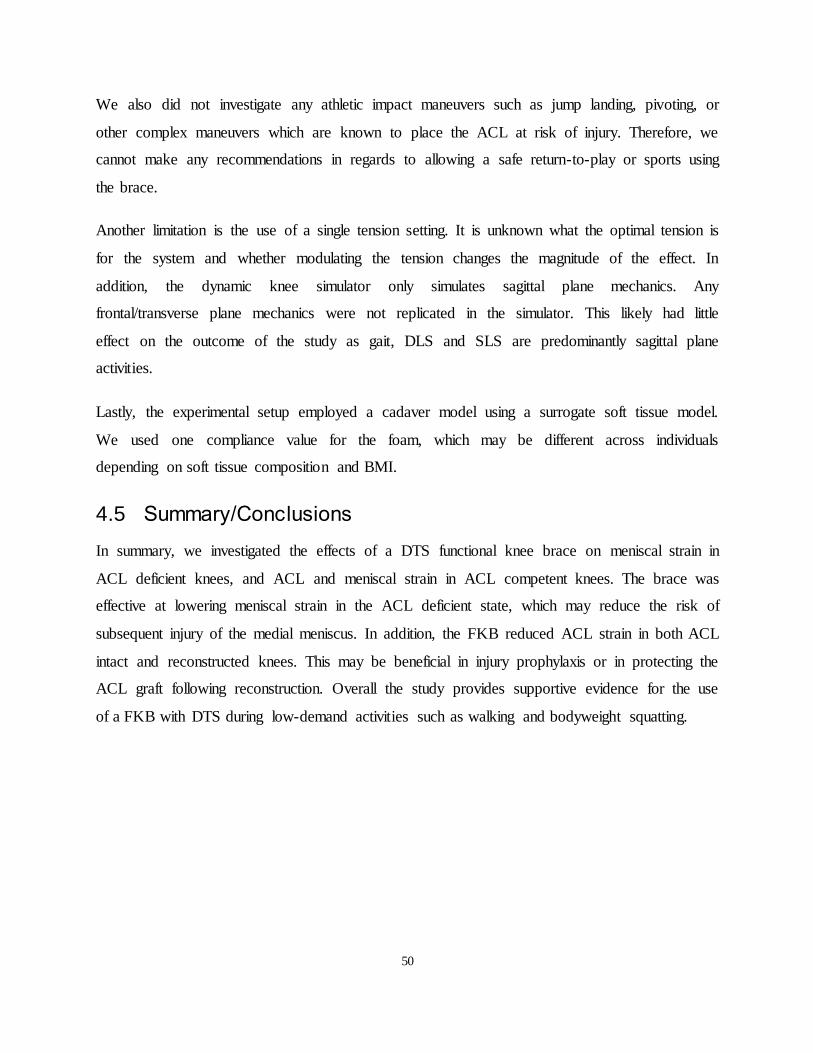
50
We also did not investigate any athletic impact maneuvers such as jump landing, pivoting, or
other complex maneuvers which are known to place the ACL at risk of injury. Therefore, we
cannot make any recommendations in regards to allowing a safe return-to-play or sports using
the brace.
Another limitation is the use of a single tension setting. It is unknown what the optimal tension is
for the system and whether modulating the tension changes the magnitude of the effect. In
addition, the dynamic knee simulator only simulates sagittal plane mechanics. Any
frontal/transverse plane mechanics were not replicated in the simulator. This likely had little
effect on the outcome of the study as gait, DLS and SLS are predominantly sagittal plane
activities.
Lastly, the experimental setup employed a cadaver model using a surrogate soft tissue model.
We used one compliance value for the foam, which may be different across individuals
depending on soft tissue composition and BMI.
4.5 Summary/Conclusions
In summary, we investigated the effects of a DTS functional knee brace on meniscal strain in
ACL deficient knees, and ACL and meniscal strain in ACL competent knees. The brace was
effective at lowering meniscal strain in the ACL deficient state, which may reduce the risk of
subsequent injury of the medial meniscus. In addition, the FKB reduced ACL strain in both ACL
intact and reconstructed knees. This may be beneficial in injury prophylaxis or in protecting the
ACL graft following reconstruction. Overall the study provides supportive evidence for the use
of a FKB with DTS during low-demand activities such as walking and bodyweight squatting.
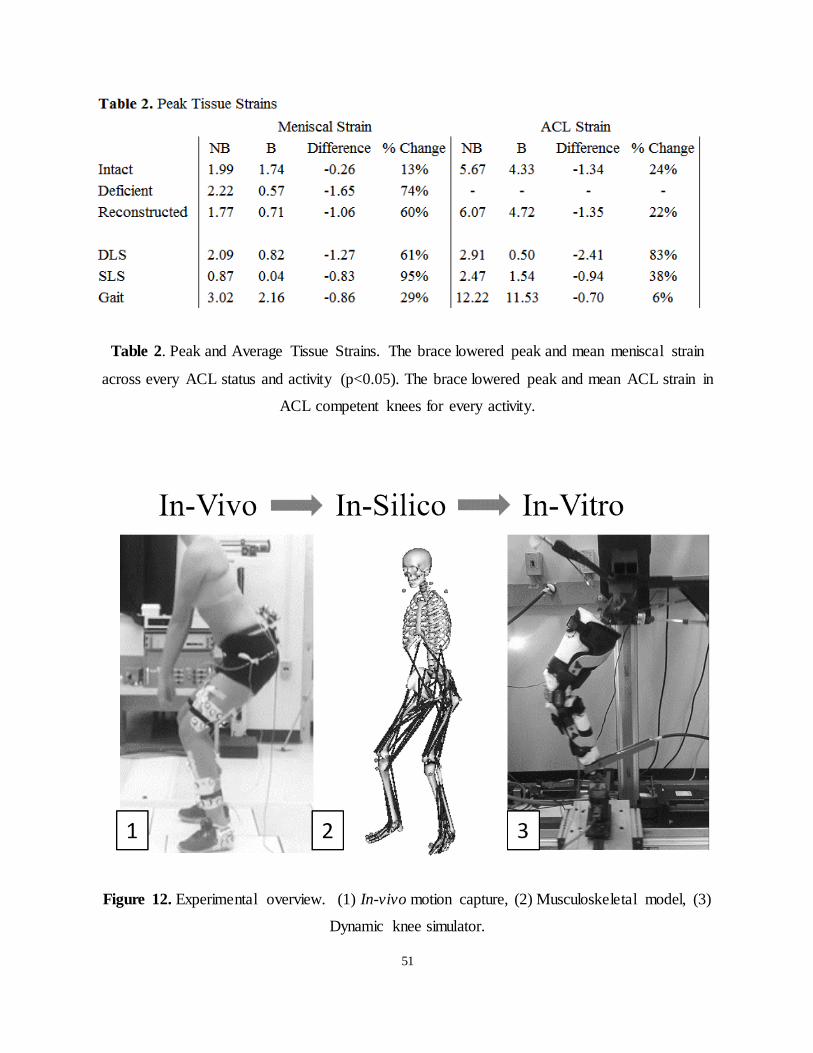
51
Table 2. Peak and Average Tissue Strains. The brace lowered peak and mean meniscal strain
across every ACL status and activity (p<0.05). The brace lowered peak and mean ACL strain in
ACL competent knees for every activity.
Figure 12. Experimental overview. (1) In-vivo motion capture, (2) Musculoskeletal model, (3)
Dynamic knee simulator.
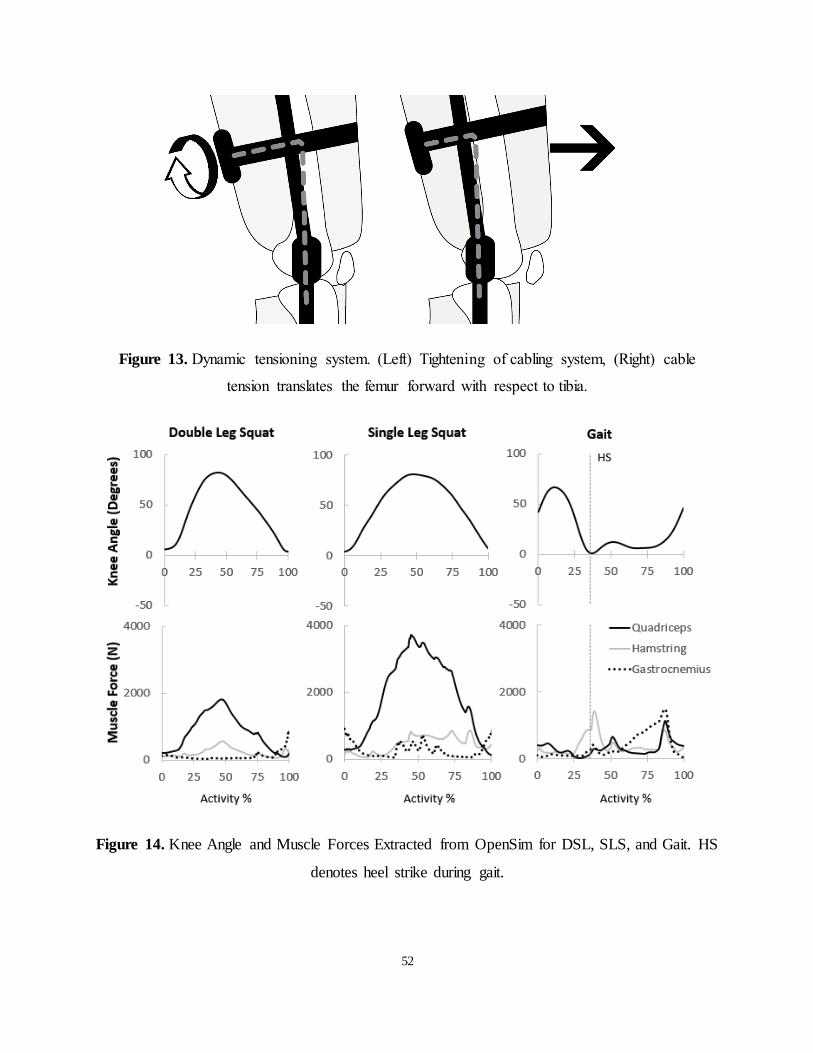
52
Figure 13. Dynamic tensioning system. (Left) Tightening of cabling system, (Right) cable
tension translates the femur forward with respect to tibia.
Figure 14. Knee Angle and Muscle Forces Extracted from OpenSim for DSL, SLS, and Gait. HS
denotes heel strike during gait.
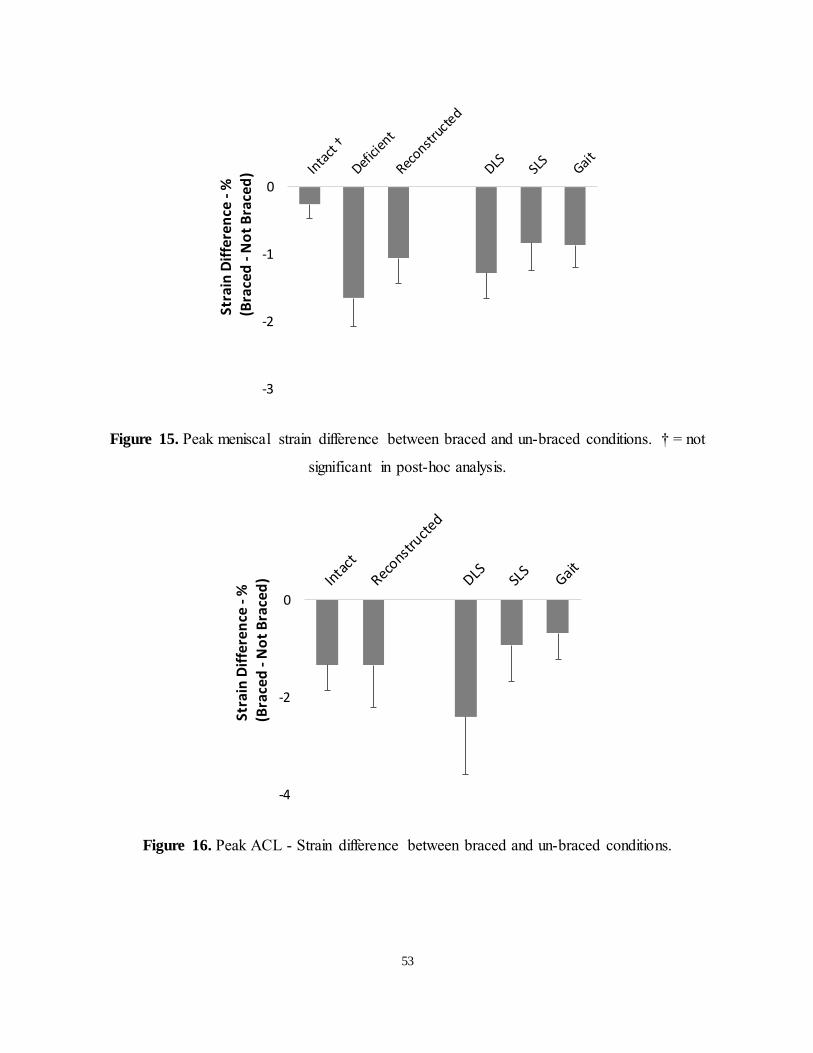
53
Figure 15. Peak meniscal strain difference between braced and un-braced conditions. † = not
significant in post-hoc analysis.
Figure 16. Peak ACL - Strain difference between braced and un-braced conditions.
-3
-2
-1
0
Stra
in D
iffe
ren
ce -
%
(B
race
d -
No
t B
race
d)
-4
-2
0
Stra
in D
iffe
ren
ce -
%
(B
race
d -
No
t B
race
d)

54
Chapter 5 5General Discussion
5.1 Summary and Discussion
In this work, we characterized and compared in-vitro tissue strain during dynamic activities in
ACL intact and reconstructed knees, and tested the effectiveness of a DTS functional ACL knee
brace in decreasing tissue strains.
The ACL strain pattern and values for the three activities tested in our study matched previously
reported results. The meniscal strain varied with the knee flexion angle and gait phase. The
meniscal and ACL strains were generally maintained following ACL reconstruction and
comparable to the ACL intact state. The DTS brace tested was effective at protecting the ACL
and posteromedial meniscus by decreasing peak tissue strains across all activities and ACL
states.
This thesis was undertaken to provide valuable data to clinicians who treat patients with ACL
injuries. It is important to know the efficacy of both operative and non-operative treatment
options. From a surgical standpoint, ACL reconstruction aims to restore tissue loading on
secondary structures in order to prevent further injury and degeneration. While meniscal strain
has been shown to normalize following reconstruction in a static loading scenario (Hollis et al.,
2000), it remains unclear if the same occurs during dynamic loading. Functional braces are
commonly prescribed as a non-operative management option following an ACL tear, as well as a
post-operative tool to protect the reconstruction. Patients may choose to not undergo
reconstruction, or have a significant delay in obtaining surgery for a variety of reasons. In this
scenario, braces may provide mechanical restraint to tibial translation and protect the medical
meniscus, which is at increased risk of injury. The effects of bracing on meniscal strain have not
previously been studied. After reconstruction, the graft may be vulnerable and braces could
theoretically offer protection during the healing phase. Although current evidence does not
support the routine use of functional braces post ACL surgery (Chew et al., 2007; Wright &
Fetzer, 2007), the majority of Orthopaedic surgeons continue to prescribe braces in an attempt to
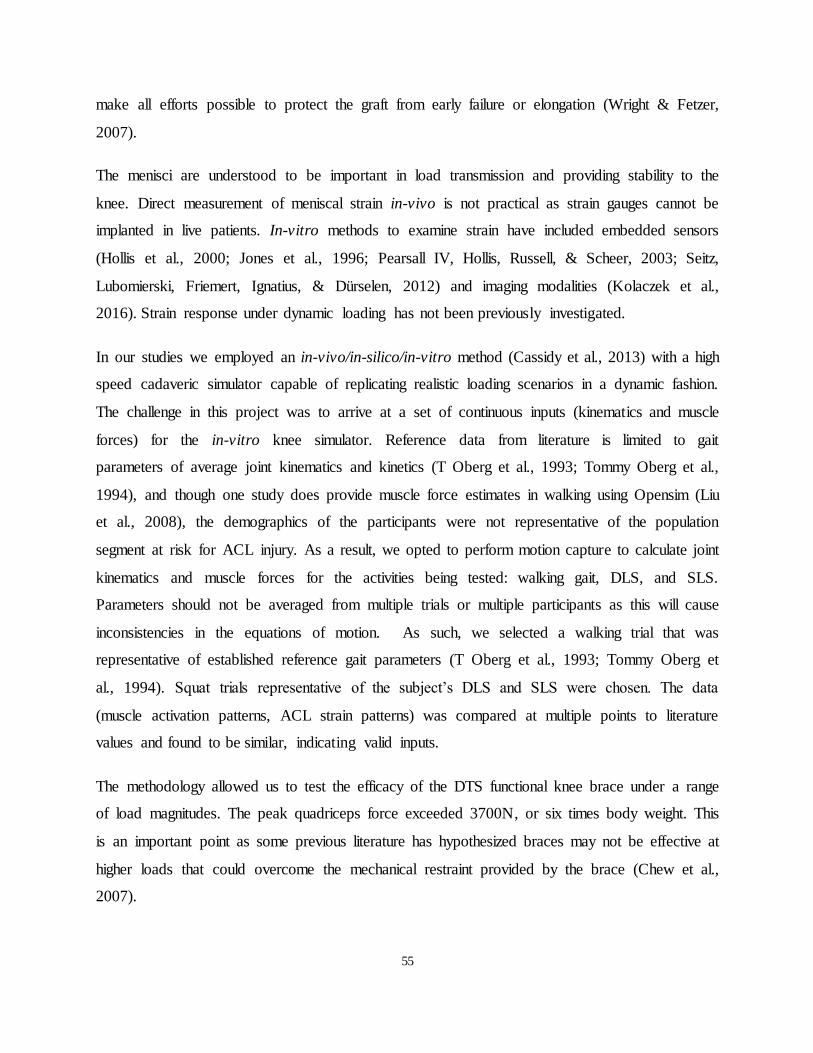
55
make all efforts possible to protect the graft from early failure or elongation (Wright & Fetzer,
2007).
The menisci are understood to be important in load transmission and providing stability to the
knee. Direct measurement of meniscal strain in-vivo is not practical as strain gauges cannot be
implanted in live patients. In-vitro methods to examine strain have included embedded sensors
(Hollis et al., 2000; Jones et al., 1996; Pearsall IV, Hollis, Russell, & Scheer, 2003; Seitz,
Lubomierski, Friemert, Ignatius, & Dürselen, 2012) and imaging modalities (Kolaczek et al.,
2016). Strain response under dynamic loading has not been previously investigated.
In our studies we employed an in-vivo/in-silico/in-vitro method (Cassidy et al., 2013) with a high
speed cadaveric simulator capable of replicating realistic loading scenarios in a dynamic fashion.
The challenge in this project was to arrive at a set of continuous inputs (kinematics and muscle
forces) for the in-vitro knee simulator. Reference data from literature is limited to gait
parameters of average joint kinematics and kinetics (T Oberg et al., 1993; Tommy Oberg et al.,
1994), and though one study does provide muscle force estimates in walking using Opensim (Liu
et al., 2008), the demographics of the participants were not representative of the population
segment at risk for ACL injury. As a result, we opted to perform motion capture to calculate joint
kinematics and muscle forces for the activities being tested: walking gait, DLS, and SLS.
Parameters should not be averaged from multiple trials or multiple participants as this will cause
inconsistencies in the equations of motion. As such, we selected a walking trial that was
representative of established reference gait parameters (T Oberg et al., 1993; Tommy Oberg et
al., 1994). Squat trials representative of the subject’s DLS and SLS were chosen. The data
(muscle activation patterns, ACL strain patterns) was compared at multiple points to literature
values and found to be similar, indicating valid inputs.
The methodology allowed us to test the efficacy of the DTS functional knee brace under a range
of load magnitudes. The peak quadriceps force exceeded 3700N, or six times body weight. This
is an important point as some previous literature has hypothesized braces may not be effective at
higher loads that could overcome the mechanical restraint provided by the brace (Chew et al.,
2007).
56
The Rebound ACL brace that was tested is manufactured by Ossur Inc. and indicated for non-
surgical treatment of ACL ruptures and for post-surgical rehabilitation. The brace is designed
with a dynamic tensioning system that applies a physiologically correct force to the posterior
thigh to counteract the load on the ACL/graft in order to optimize healing. By extension, in the
setting of ACL injury the brace has the potential to decrease load on the medial meniscus.
Traditional braces applied a static force to unload the joint and reduce tibial translation. DTS is
capable of applying a dynamic force which is higher in magnitude than typically applied by older
braces (LaPrade et al., 2015).
We found that the DTS brace significantly lowered peak and average meniscal strain in ACL
deficient knees. This finding lends support to idea that braces can mechanically stabilize the knee
and decrease load on the medial meniscus, which in turn may translate to a decreased risk of
subsequent meniscal tears in chronic ACL deficiency. The brace was also found to lower ACL
strain in ACL-intact and -reconstructed knees. Therefore, in ACL-competent knees, the brace
may be beneficial in injury prophylaxis or in protecting the ACL graft following reconstruction.
Overall, we conclude that the DTS functional ACL brace can decrease knee tissue strains during
dynamic loading.
5.2 Contributions
Contributions of the current thesis include the following:
1. Demonstrating the validity of the in-vivo/in-silico/in-vitro methodology to studying
dynamic loading conditions with cadaver specimens through comparison with in-vivo
results
2. Contributing new knowledge and reference data on meniscal loading during gait, DLS,
and SLS
3. Establishing the ability of ACL reconstructions to maintain strain in the medial meniscus
4. Demonstrating the efficacy of a DTS functional knee brace in decreasing medial meniscal
strain in ACL deficient knees
5. Demonstrating the efficacy of a DTS functional knee brace in lowering ACL and
meniscal strain in ACL competent knees
57
5.3 Future Directions
This work provided evidence for the efficacy of the DTS to stabilize the knee. There are several
future directions which would provide more clarity on its effectiveness.
The studies in this thesis had a small sample size, testing only seven specimens. While the results
of this study were significant, the standard deviations of the results were large. A larger sample
size would unlikely change the overall take-away of this thesis, but would provide more
confidence on the effect size of the brace. Larger sample sizes would also improve our ability to
make predictive statistical models about meniscal and OA injury risks.
The effect of the DTS brace was measured in terms of ACL strain and posteromedial meniscal
strain. There are several additional experimentally measurable parameters which would broaden
the understanding of the effects of the brace on other tissues. Pressure on the articular cartilage
would be a relevant measure to determine if the center of pressure is restored with the use of the
DTS brace.
The current studies evaluated the effect of the DTS during three activities: gait, DLS and SLS.
While these activities have higher forces than those previously tested, it is unknown how
effective it would be during higher impact activities, such as landing and pivoting. Patients with
ACL injuries aim to return to sports and may be at risk for further injury, especially if the ACL is
not repaired. It is important to know if the DTS can help patients return to play safely in this
scenario.
The work presented in this thesis involves using simulations of three activities from one average
participant. Future avenues of research may involve assessing multiple participants kinematics
patterns and how the variability affects the resulting tissue strains. This work would show how
different movement patterns and strategies affect knee stability during rehabilitation and may
reveal if a braced would be more effective for some groups of patients above others.
Finally, follow up studies should be conducted to investigate the clinical effects of a DTS brace.
It is hypothesized that the reduction in ligament and meniscal strain found in this thesis would
translate to positive clinical outcomes with lower rates further injury. Previous clinical studies
have investigated the effect functional braces have on re-injury rate, subjective stabilization,

58
muscle contraction, range of motion and pain. Clinical follow up studies should investigate these
clinical parameters when a DTS brace is applied.
59
References 6
Ahmed, A. M., & Burke, D. L. (1983). In-vitro measurement of static pressure distribution in
synovial joints - Part I: Tibial surface of the knee. Journal of Biomechanical Engineering,
105(3), 216–225.
Alentorn-Geli, E., Myer, G. D., Silvers, H. J., Samitier, G., Romero, D., Lázaro-Haro, C., &
Cugat, R. (2009). Prevention of non-contact anterior cruciate ligament injuries in soccer
players. Part 1: Mechanisms of injury and underlying risk factors. Knee Surgery, Sports
Traumatology, Arthroscopy : Official Journal of the ESSKA, 17(7), 705–29.
Allen, A. a., Caldwell, G. L., & Fu, F. H. (1995). Anatomy and biomechanics of the meniscus.
Operative Techniques in Orthopaedics, 5(1), 2–9.
Allen, C. R., Wong, E. K., Livesay, G. A., Sakane, M., Fu, F. H., & Woo, S. L. (2000).
Importance of the Medial Meniscus in the Anterior Cruciate Ligament-deficient Knee, 109–
115.
Allen, C., Wong, E., Livesay, G., Sakane, M., Fu, F., & Woo, S. (2000). Importance of the
medial meniscus in the anterior cruciate ligament-defi cient knee. J Orthop Res, 18, 109–15.
Allen, P., Denham, R., & Swan, A. (1984). Late Degenerative Changes After Menisectomy:
Factors Affecting the Knee After Operation. The Journal of Bone & Joint Surgery, 66(5),
666–671.
Amis, A., & Dawkins, G. (1991). FUNCTIONAL ANTERIOR ANATOMY OF THE
LIGAMENT. The Journal of Bone & Joint Surgery, 73(B), 260–267.
Anderson, K., Wojtys, E. M., Loubert, P. V, & Miller, R. E. (1992). A biomechanical evaluation
of taping and bracing in reducing knee joint translation and rotation. The American Journal
of Sports Medicine, 20(4), 416–421.
Andersson, C., Odensten, M., Good, L., & Gillquist, J. (1989). Surgical or non-surgical treatment
of acute rupture of the anterior cruciate ligament. A randomized study with long-term
follow-up. Journal of Bone and Joint Surgery. American Volume, 71(7), 965–974.
60
Andriacchi, T. P., & Dyrby, C. O. (2005). Interactions between kinematics and loading during
walking for the normal and ACL deficient knee. Journal of Biomechanics, 38(2), 293–8.
Bakker, R., Tomescu, S., Brenneman, E., Hangalur, G., Laing, A., & Chandrashekar, N. (2016).
The effect of sagittal plane mechanics on ACL strain during jump landing. Journal of
Orthopaedic Research : Official Publication of the Orthopaedic Research Society, (i), 1–9.
Barenius, B., Ponzer, S., Shalabi, A., Bujak, R., Norlén, L., & Eriksson, K. (2014). Increased risk
of osteoarthritis after anterior cruciate ligament reconstruction: a 14-year follow-up study of
a randomized controlled trial. The American Journal of Sports Medicine, 42(5), 1049–57.
Berns, G. S., Hull, M. L., & Patterson, H. A. (1992). Strain in the anteromedial bundle of the
anterior cruciate ligament under combined loading conditions. J Orthop Res, 10(6), 167–
176.
Beynnon, B. D. (2005). Treatment of Anterior Cruciate Ligament Injuries, Part I. American
Journal of Sports Medicine, 33(10), 1579–1602.
Beynnon, B. D., & Fleming, B. C. (1998). Anterior cruciate ligament strain in-vivo: a review of
previous work. Journal of Biomechanics, 31(6), 519–25.
Beynnon, B. D., Fleming, B. C., Churchill, D. L., & Brown, D. (2003). The effect of anterior
cruciate ligament deficiency and functional bracing on translation of the tibia relative to the
femur during nonweightbearing and weightbearing. The American Journal of Sports
Medicine, 31(1), 99–105.
Beynnon, B. D., Johnson, R. J., Fleming, B. C., Peura, G. D., Renstrom, P. A., Nichols, C. E., &
Pope, M. H. (2000). The effect of functional knee bracing on the anterior cruciate ligament
in the weightbearing and nonweightbearing knee. The American Journal of Sports
Medicine, 25(6), 353–359.
Beynnon, B. D., Pope, M. H., Wertheimer, C. M., Johnson, R. J., Fleming, B. C., Nichols, C. E.,
& Howe, J. G. (1992). The effect of functional knee-braces on strain on the anterior cruciate
ligament in vivo. The Journal of Bone and Joint Surgery. American Volume, 74(9), 1298–

61
312.
Beynnon, B. D., Ryder, S. H., Konradsen, L., Johnson, R. J., Johnson, K., & Renström, P. A.
(1999). The effect of anterior cruciate ligament trauma and bracing on knee proprioception.
The American Journal of Sports Medicine, 27(2), 150–5.
Beynnon, B., Howe, J. G., Pope, M. H., Johnson, R. J., & Fleming, B. C. (1992). The
measurement of anterior cruciate ligament strain in vivo. International Orthopaedics, 16(1),
1–12.
Boden, B. P., Torg, J. S., Knowles, S. B., & Hewett, T. E. (2009). Video analysis of anterior
cruciate ligament injury: abnormalities in hip and ankle kinematics. The American Journal
of Sports Medicine, 37(2), 252–9.
Branch, T., Hunter, R., & Donath, M. (1984). Dynamic analysis of anterior cruciate deficient
legs with and without bracing during cutting *. American Journal of Sports Medicine, 17(1),
35–41.
Butler, D. L., & Anonymous. (1989). Kappa Delta Award paper. Anterior cruciate ligament: its
normal response and replacement. Journal of Orthopaedic Research, 7(6), 910–921.
Button, K., Roos, P. E., & Van Deursen, R. W. M. (2014). Activity progression for anterior
cruciate ligament injured individuals. Clinical Biomechanics, 29(2), 206–212.
Carter, N. D., Jenkinson, T. R., Wilson, D., Jones, D. W., & Torode, A. S. (1997). Joint position
sense and rehabilitation in the anterior cruciate ligament deficient knee. British Journal of
Sports Medicine, 31(3), 209–12.
Cassidy, K., Hangalur, G., Sabharwal, P., & Chandrashekar, N. (2013). Combined in vivo/in
vitro method to study anteriomedial bundle strain in the anterior cruciate ligament using a
dynamic knee simulator. Journal of Biomechanical Engineering, 135(3), 35001.
Cawley, P. W., France, E. P., & Paulos, L. E. (1991). The current state of functional knee
bracing research. A review of the literature. The American Journal of Sports Medicine,
19(3), 226–33.

62
Chandrashekar, N., Mansouri, H., Slauterbeck, J., & Hashemi, J. (2006). Sex-based differences
in the tensile properties of the human anterior cruciate ligament. Journal of Biomechanics,
39(16), 2943–50.
Chew, K. T. L., Lew, H. L., Date, E., & Fredericson, M. (2007). Current evidence and clinical
applications of therapeutic knee braces. American Journal of Physical Medicine &
Rehabilitation / Association of Academic Physiatrists, 86(8), 678–686.
Cipolla, M., Scala, a, Gianni, E., & Puddu, G. (1995). Different patterns of meniscal tears in
acute anterior cruciate ligament (ACL) ruptures and in chronic ACL-deficient knees.
Classification, staging and timing of treatment. Knee Surgery, Sports Traumatology,
Arthroscopy : Official Journal of the ESSKA, 3(3), 130–134.
Delp, S. L., Anderson, F. C., Arnold, A. S., Loan, P., Habib, A., John, C. T., … Thelen, D. G.
(2007). OpenSim: open-source software to create and analyze dynamic simulations of
movement. IEEE Transactions on Bio-Medical Engineering, 54(11), 1940–50.
Delp, S. L., Ringwelski, D. A., & Carroll, N. C. (1994). Transfer of the rectus femoris: effects of
transfer site on moment arms about the knee and hip. Journal of Biomechanics, 27(10),
1201–11.
Domzalski, M., Grzelak, P., & Gabos, P. (2010). Risk factors for Anterior Cruciate Ligament
injury in skeletally immature patients: analysis of intercondylar notch width using Magnetic
Resonance Imaging. International Orthopaedics, 34(5), 703–7.
Duthon, V. B., Barea, C., Abrassart, S., Fasel, J. H., Fritschy, D., & Ménétrey, J. (2006).
Anatomy of the anterior cruciate ligament. Knee Surgery, Sports Traumatology,
Arthroscopy : Official Journal of the ESSKA, 14(3), 204–13.
Erickson, A., Yasuda, K., Beynnon, B., Johnson, R., & Pope, M. (1993). An in vitro dynamic
evaluation of prophylactic knee braces during lateral impact loading. The American Journal
of Sports Medicine, 21(1), 26–35.
Fleming, B. C., Beynnon, B. D., Renstrom, P. a, Johnson, R. J., Nichols, C. E., Peura, G. D., &
63
Uh, B. S. (1998). The strain behavior of the anterior cruciate ligament during Bicycling: an
in vivo study. Arthroscopy : The Journal of Arthroscopic & Related Surgery : Official
Publication of the Arthroscopy Association of North America and the International
Arthroscopy Association, 15(2), 185–91.
Fleming, B. C., Renstrom, P. A., Beynnon, B. D., Engstrom, B., Peura, G. D., Johnson, R. J., …
Pope, M. H. (2000). The Influence of Functional Knee Bracing on the Anterior Cruciate
Ligament Strain Biomechanics in Weightbearing and Nonweightbearing Knees. The
American Journal of Sports Medicine, 28(6), 815–824.
Fu, F. H., Woo, S. L., & Ph, D. (1994). Biomechanical Function of the Human Anterior Cruciate
Ligament. Arthroscopy : The Journal of Arthroscopic & Related Surgery : Official
Publication of the Arthroscopy Association of North America and the International
Arthroscopy Association, 10(2), 140–147.
Fukubayashi, T., & Kurosawa, H. (1980). The contact area and pressure distribution pattern of
the knee. A study of normal and osteoarthrotic knee joints. Acta Orthopaedica
Scandinavica, 51(6), 871–879.
Fung, D. T., & Zhang, L. Q. (2003). Modeling of ACL impingement against the intercondylar
notch. Clinical Biomechanics, 18(10), 933–941.
Giffin, J. R., Vogrin, T. M., Zantop, T., Woo, S. L. Y., & Harner, C. D. (2004). Effects of
increasing tibial slope on the biomechanics of the knee. The American Journal of Sports
Medicine, 32(2), 376–82.
Goldstein, S. A., Armstrong, T. J., Chaffin, D. B., & Matthews, L. S. (1987). Analysis of
cumulative strain in tendons and tendon sheaths. Journal of Biomechanics, 20(1), 1–6.
Gray, J., Taunton, J., McKenzie, D., Clement, D., McConkey, J., & Davidson, R. (1985). A
Survey of Injuries to the Anterior Cruciate Ligament of the Knee in Female Basketball
Players. International Journal of Sports Medicine, 6(6), 314–316.
Griffin, L. Y., Agel, J., Albohm, M. J., Arendt, E. A., Dick, R. W., Garrett, W. E., … Wojtys, E.

64
M. (2001). Perspectives on Modern Orthopaedics Noncontact Anterior Cruciate Ligament
Injuries : Risk Factors and Prevention Strategies, 8(3), 141–150.
Guler, O., Mahirogullari, M., Mutlu, S., Cerci, M. H., Seker, A., & Cakmak, S. (2016). Graft
position in arthroscopic anterior cruciate ligament reconstruction: anteromedial versus
transtibial technique. Archives of Orthopaedic and Trauma Surgery, 136(11), 1571–1580.
Hamner, S. R., Seth, A., & Delp, S. L. (2010). Muscle contributions to propulsion and support
during running. Journal of Biomechanics, 43(14), 2709–16.
Hangalur, G., Brenneman, E., Nicholls, M., Bakker, R., Laing, a., & Chandrashekar, N. (2015).
Can a knee brace reduce the strain in the anterior cruciate ligament? A study using
combined in vivo/in vitro method. Prosthetics and Orthotics International, 1–6.
Harris, M. L., Morberg, P., Bruce, W. J., & Walsh, W. R. (1999). An improved method for
measuring tibiofemoral contact areas in total knee arthroplasty: a comparison of K-scan
sensor and Fuji film. Journal of Biomechanics, 32(9), 951–8.
Hashemi, J., Chandrashekar, N., Gill, B., Beynnon, B. D., Slauterbeck, J. R., Schutt, R. C., …
Dabezies, E. (2008). The geometry of the tibial plateau and its influence on the
biomechanics of the tibiofemoral joint. The Journal of Bone and Joint Surgery. American
Volume, 90(12), 2724–34.
Hauch, K. N., Villegas, D. F., & Donahue, T. L. H. (2011). GEOMETRY, TIME DEPENDENT
AND FAILURE PROPERTIES OF HUMAN MENISCAL ATTACHMENTS, 43(3).
Heidt, R. S., Sweeterman, L. M., Carlonas, R. L., Traub, J. A., & Tekulve, F. X. (2000).
Avoidance of soccer injuries with preseason conditioning. The American Journal of Sports
Medicine, 28(5), 659–662.
Heis, F., & Paulos, L. (2002). Tensioning of the Anterior Cruciate Ligament Graft. Orthop Clin
North Am, 33(4), 697–700.
Herbort, M., Lenschow, S., Fu, F. H., Petersen, W., & Zantop, T. (2010). ACL mismatch
reconstructions: influence of different tunnel placement strategies in single-bundle ACL
65
reconstructions on the knee kinematics. Knee Surgery, Sports Traumatology, Arthroscopy :
Official Journal of the ESSKA, 18(11), 1551–8.
Herzog, W., & Read, L. J. (1993). Lines of action and moment arms of the major force-carrying
structures crossing the human knee joint. Journal of Anatomy, 182 ( Pt 2, 213–30.
Hewett, T. E., Ford, K. R., & Myer, G. D. (2006). Anterior cruciate ligament injuries in female
athletes: Part 2, a meta-analysis of neuromuscular interventions aimed at injury prevention.
The American Journal of Sports Medicine, 34(3), 490–8.
Hewett, T. E., Lindenfeld, T. N., Riccobene, J. V, & Noyes, F. R. (1999). The effect of
neuromuscular training on the incidence of knee injury in female athletes. A prospective
study. The American Journal of Sports Medicine, 27(6), 699–706.
Hicks, J. L., Uchida, T. K., Seth, A., Rajagopal, A., & Delp, S. (2015). Is my model good
enough? Best practices for verification and validation of musculoskeletal models and
simulations of human movement. Journal of Biomechanical Engineering, 137(February),
20905.
Hollis, J. M., Pearsall, a. W., & Niciforos, P. G. (2000). Change in Meniscal Strain with
Anterior Cruciate Ligament Injury and After Reconstruction. The American Journal of
Sports Medicine, 28(5), 700–704.
Ireland, M. L., Ballantyne, B. T., Little, K., & McClay, I. S. (2001). A radiographic analysis of
the relationship between the size and shape of the intercondylar notch and anterior cruciate
ligament injury. Knee Surgery, Sports Traumatology, Arthroscopy : Official Journal of the
ESSKA, 9(4), 200–5.
Jones, R. S., Keene, G. C. R., Learmonth, D. J. a, Bickerstaff, D., Nawana, N. S., Costi, J. J., &
Pearcy, M. J. (1996). Direct measurement of hoop strains in the intact and torn human
medial meniscus. Clinical Biomechanics (Bristol, Avon), 11(5), 295–300.
Jonsson, H., & Kärrholm, J. (1990). Brace effects on the unstable knee in 21 cases. A roentgen
stereophotogrammetric comparison of three designs. Acta Orthopaedica Scandinavica,
66
61(4), 313–8.
Karlsson, J., Irrgang, J. J., van Eck, C. F., Samuelsson, K., Mejia, H. a, & Fu, F. H. (2011).
Anatomic single- and double-bundle anterior cruciate ligament reconstruction, part 2:
clinical application of surgical technique. The American Journal of Sports Medicine, 39(9),
2016–26.
Keays, S. L., Newcombe, P. a, Bullock-Saxton, J. E., Bullock, M. I., & Keays, A. C. (2010).
Factors involved in the development of osteoarthritis after anterior cruciate ligament
surgery. The American Journal of Sports Medicine, 38, 455–463.
Kirwan, G. W., Bourke, M. G., Chipchase, L., Dalton, P. A., & Russell, T. G. (2013). Initial graft
tension and the effect on postoperative patient functional outcomes in anterior cruciate
ligament reconstruction. Arthroscopy - Journal of Arthroscopic and Related Surgery, 29(5),
934–941.
Knoll, Z., Kiss, R. M., & Kocsis, L. (2004). Gait adaptation in ACL deficient patients before and
after anterior cruciate ligament reconstruction surgery. Journal of Electromyography and
Kinesiology, 14(3), 287–294.
Kolaczek, S., Hewison, C., Caterine, S., Ragbar, M. X., Getgood, A., & Gordon, K. D. (2016).
Analysis of 3D strain in the human medial meniscus. Journal of the Mechanical Behavior of
Biomedical Materials, 63, 470–475.
Kostogiannis, I., Ageberg, E., Neuman, P., Dahlberg, L., Fridén, T., & Roos, H. (2007). Activity
level and subjective knee function 15 years after anterior cruciate ligament injury: a
prospective, longitudinal study of nonreconstructed patients. The American Journal of
Sports Medicine, 35, 1135–1143.
Kristianslund, E., Krosshaug, T., & van den Bogert, A. J. (2012). Effect of low pass filtering on
joint moments from inverse dynamics: implications for injury prevention. Journal of
Biomechanics, 45(4), 666–71.
Krosshaug, T., Nakamae, A., Boden, B. P., Engebretsen, L., Smith, G., Slauterbeck, J. R., …
67
Bahr, R. (2007). Mechanisms of anterior cruciate ligament injury in basketball: video
analysis of 39 cases. The American Journal of Sports Medicine, 35(3), 359–67.
Krüger-Franke, M., Siebert, C. H., Kugler, a, Trouillier, H. H., & Rosemeyer, B. (1999). Late
results after arthroscopic partial medial meniscectomy. Knee Surgery, Sports Traumatology,
Arthroscopy : Official Journal of the ESSKA, 7(2), 81–4.
Lam, R. Y., Ng, G. Y., & Chien, E. P. (2002). Does wearing a functional knee brace affect
hamstring reflex time in subjects with anterior cruciate ligament deficiency during muscle
fatigue? Archives of Physical Medicine and Rehabilitation, 83(7), 1009–1012.
LaPrade, R. F., Smith, S. D., Wilson, K. J., & Wijdicks, C. A. (2015). Quantification of
functional brace forces for posterior cruciate ligament injuries on the knee joint: an in vivo
investigation. Knee Surgery, Sports Traumatology, Arthroscopy, 23(10), 3070–3076.
LaPrade, R. F., Wozniczka, J. K., Stellmaker, M. P., & Wijdicks, C. a. (2010). Analysis of the
static function of the popliteus tendon and evaluation of an anatomic reconstruction: the
“fifth ligament” of the knee. The American Journal of Sports Medicine, 38(3), 543–549.
Laughlin, W. a, Weinhandl, J. T., Kernozek, T. W., Cobb, S. C., Keenan, K. G., & O’Connor, K.
M. (2011). The effects of single- leg landing technique on ACL loading. Journal of
Biomechanics, 44(10), 1845–51.
Lee, S. J., Aadalen, K. J., Malaviya, P., Lorenz, E. P., Hayden, J. K., Farr, J., … Cole, B. J.
(2006). Tibiofemoral contact mechanics after serial medial meniscectomies in the human
cadaveric knee. The American Journal of Sports Medicine, 34(8), 1334–44.
Levine, J. W., Kiapour, A. M., Quatman, C. E., Wordeman, S. C., Goel, V. K., Hewett, T. E., &
Demetropoulos, C. K. (2013). Clinically relevant injury patterns after an anterior cruciate
ligament injury provide insight into injury mechanisms. The American Journal of Sports
Medicine, 41(2), 385–95.
Levy, I. M., Torzilli, P. A., & Warren, R. F. (1982). The effect of medial meniscectomy on
anterior-posterior motion of the knee. The Journal of Bone and Joint Surgery. American
68
Volume, 64(6), 883–8.
Levy, I., Torzilli, P., & Warren, R. F. (1982). The effect of medial meniscectomy on anterior-
posterior motion of the knee. The Journal of Bone & Joint Surgery, 64(6), 883–888.
Liu, M. Q., Anderson, F. C., Schwartz, M. H., & Delp, S. L. (2008). Muscle contributions to
support and progression over a range of walking speeds. Journal of Biomechanics, 41(15),
3243–52.
Lohmander, L. S., Englund, P. M., Dahl, L. L., & Roos, E. M. (2007). The long-term
consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. The
American Journal of Sports Medicine, 35(10), 1756–69.
Louboutin, H., Debarge, R., Richou, J., Selmi, T. A. S., Donell, S. T., Neyret, P., & Dubrana, F.
(2009). Osteoarthritis in patients with anterior cruciate ligament rupture: a review of risk
factors. The Knee, 16(4), 239–44.
Mall, N. a, Chalmers, P. N., Moric, M., Tanaka, M. J., Cole, B. J., Bach, B. R., & Paletta, G. a.
(2014). Incidence and trends of anterior cruciate ligament reconstruction in the United
States. The American Journal of Sports Medicine, 42(10), 2363–70.
Marans, H. J., Jackson, R. W., Piccinin, J., Silver, R. L., & Kennedy, D. K. (1991). Functional
testing of braces for anterior cruciate ligament-deficient knees. Canadian Journal of
Surgery. Journal Canadien de Chirurgie, 34(2), 167–72.
Marouane, H., Shirazi-Adl, A., Adouni, M., & Hashemi, J. (2014). Steeper posterior tibial slope
markedly increases ACL force in both active gait and passive knee joint under compression.
Journal of Biomechanics, 47(6), 1353–9.
Mather, R. C., Koenig, L., Kocher, M. S., Dall, T. M., Gallo, P., Scott, D. J., … Spindler, K. P.
(2013). Societal and economic impact of anterior cruciate ligament tears. The Journal of
Bone and Joint Surgery. American Volume, 95(19), 1751–9.
McLean, C. a, & Ahmed, a M. (1993). Design and development of an unconstrained dynamic
knee simulator. Journal of Biomechanical Engineering, 115(2), 144–8.

69
McLean, S. G., Oh, Y. K., Palmer, M. L., Lucey, S. M., Lucarelli, D. G., Ashton-Miller, J. a, &
Wojtys, E. M. (2011). The relationship between anterior tibial acceleration, tibial slope, and
ACL strain during a simulated jump landing task. The Journal of Bone and Joint Surgery.
American Volume, 93(14), 1310–7.
Mishra, D. K., Daniel, D. M., & Stone, M. L. (1989). The use of functional knee braces in the
control of pathologic anterior knee laxity. Clinical Orthopaedics and Related Research,
(241), 213–20.
Mitsou, A., & Vallianatos, P. (1988). Meniscal injuries associated with rupture of the anterior
cruciate ligament: a retrospective study. Injury, 19(6), 429–431.
Mokhtarzadeh, H., Yeow, C. H., Hong Goh, J. C., Oetomo, D., Malekipour, F., & Lee, P. V.-S.
(2013). Contributions of the soleus and gastrocnemius muscles to the anterior cruciate
ligament loading during single- leg landing. Journal of Biomechanics, 46(11), 1913–20.
Myer, G. D., Paterno, M. V, Ford, K. R., Quatman, C. E., & Hewett, T. E. (2006). Rehabilitation
After Anterior Cruciate Ligament Reconstruction: Criteria-Based Progression Through the
Return-to-Sport Phase. J Orthop Sports Phys Ther, 36(6), 385–402.
Myers, C. a, Torry, M. R., Shelburne, K. B., Giphart, J. E., LaPrade, R. F., Woo, S. L.-Y., &
Steadman, J. R. (2012). In vivo tibiofemoral kinematics during 4 functional tasks of
increasing demand using biplane fluoroscopy. The American Journal of Sports Medicine,
40(1), 170–8.
Myklebust, G., Engebretsen, L., Braekken, I. H., Skjølberg, A., Olsen, O.-E., & Bahr, R. (2003).
Prevention of anterior cruciate ligament injuries in female team handball players: a
prospective intervention study over three seasons. Clinical Journal of Sport Medicine :
Official Journal of the Canadian Academy of Sport Medicine, 13(2), 71–8.
Najibi, S. (2005). The Use of Knee Braces, Part 1: Prophylactic Knee Braces in Contact Sports.
American Journal of Sports Medicine, 33(4), 602–611.
Nemeth, G., Lamontagne, M., Tho, K. S., & Eriksson, E. (1997). Electromyographic Activity in
70
Expert Downhill Skiers Using Functional Knee Braces After Anterior Cruciate Ligament
Injuries. American Journal of Sports Medicine, 25(5), 635–641.
Neuman, P., Englund, M., Kostogiannis, I., Fridén, T., Roos, H., & Dahlberg, L. E. (2008).
Prevalence of tibiofemoral osteoarthritis 15 years after nonoperative treatment of anterior
cruciate ligament injury: a prospective cohort study. The American Journal of Sports
Medicine, 36(9), 1717–25.
Noyes, F. R. (2009). The function of the human anterior cruciate ligament and analysis of single-
and double-bundle graft reconstructions. Sports Health, 1(1), 66–75.
Oberg, T., Karsznia, A., & Oberg, K. (1993). Basic gait parameters: reference data for normal
subjects, 10-79 years of age. Journal of Rehabilitation Research and Development, 30(2),
210–23.
Oberg, T., Karsznia, A., & Oberg, K. (1994). Joint angle parameters in gait : Reference data for
normal subjects , 10-79 years of age, (August), 199–213.
Ode, G. E., Van Thiel, G. S., McArthur, S. a, Dishkin-Paset, J., Leurgans, S. E., Shewman, E. F.,
… Cole, B. J. (2012). Effects of serial sectioning and repair of radial tears in the lateral
meniscus. The American Journal of Sports Medicine, 40(8), 1863–70.
Oh, Y. K., Lipps, D. B., Ashton-Miller, J. a, & Wojtys, E. M. (2012). What strains the anterior
cruciate ligament during a pivot landing? The American Journal of Sports Medicine, 40(3),
574–83.
Paulos, L. E., Cawley, P. W., & France, E. P. (1991). Impact biomechanics of lateral knee
bracing. The anterior cruciate ligament. Am J Sports Med, 19(4), 337–342.
Pearsall, a. W. (2004). The Effect of Posterior Cruciate Ligament Injury and Reconstruction on
Meniscal Strain. American Journal of Sports Medicine, 32(7), 1675–1680.
Pearsall IV, A. W., Hollis, J. M., Russell, G. V., & Scheer, Z. (2003). A Biomechanical
Comparison of Three Lower Extremity Tendons for Ligamentous Reconstruction about the
Knee. Arthroscopy - Journal of Arthroscopic and Related Surgery, 19(10), 1091–1096.
71
Pflum, M. a., Shelburne, K. B., Torry, M. R., Decker, M. J., & Pandy, M. G. (2004). Model
Prediction of Anterior Cruciate Ligament Force during Drop-Landings. Medicine & Science
in Sports & Exercise, 36(11), 1949–1958.
Pietraszewski, B., Winiarski, S., & Jaroszczuk, S. (2012). Three-dimensional human gait pattern
– reference data for normal men. Acta of Bioengineering and Biomechanics, 14(3), 9–16.
Pietrosimone, B. G., Grindstaff, T. L., Linens, S. W., Uczekaj, E., & Hertel, J. (2008). A
Systematic Review of Prophylactic Braces in the Prevention of Knee Ligament Injuries in
Collegiate Football Players, 43(4), 409–415.
Quatman, C. E. C., Quatman, C. E. C., & Hewett, T. E. (2009). Prediction and prevention of
musculoskeletal injury: a paradigm shift in methodology. British Journal of Sports
Medicine, 43(14), 1100–7.
Quatman, C. E., Kiapour, A. M., Demetropoulos, C. K., Kiapour, A., Wordeman, S. C., Levine,
J. W., … Hewett, T. E. (2014). Preferential loading of the ACL compared with the MCL
during landing: a novel in sim approach yields the multiplanar mechanism of dynamic
valgus during ACL injuries. The American Journal of Sports Medicine, 42(1), 177–86.
Ramsey, D. K., Lamontagne, M., Wretenberg, P. F., & Valentin, A. (2001). Assessment of
functional knee bracing : an in vivo three-dimensional kinematic analysis of the anterior
cruciate de ® cient knee m d , Gunnar N Bj o, 16, 61–70.
Ramsey, D. K., Wretenberg, P. F., & Lamontagne, M. (2003). Electromyographic and
biomechanic analysis of anterior cruciate ligament deficiency and functional knee bracing,
18, 28–34.
Ranstam, J., Lohmander, L. S., Frobell, R., & Roos, E. M. (2010). A Randomized Trial of
Treatment for Acute Anterior Cruciate Ligament Tears. New England Journal of Medicine,
4, 331–342.
Rebel, M., & Paessler, H. H. (2001). The effect of knee brace on coordination and neuronal leg
muscle control : an early postoperative functional study in anterior cruciate ligament

72
reconstructed patients, 272–281.
Robin, B. N., Jani, S. S., Marvil, S. C., Reid, J. B., Schillhammer, C. K., & Lubowitz, J. H.
(2015). Advantages and Disadvantages of Transtibial, Anteromedial Portal, and Outside-In
Femoral Tunnel Drilling in Single-Bundle Anterior Cruciate Ligament Reconstruction: A
Systematic Review. Arthroscopy : The Journal of Arthroscopic & Related Surgery : Official
Publication of the Arthroscopy Association of North America and the International
Arthroscopy Association, 31(7), 1412–1417.
Sasaki, S., Nagano, Y., Kaneko, S., Imamura, S., Koabayshi, T., & Fukubayashi, T. (2015). The
relationships between the center of mass position and the trunk, hip, and knee kinematics in
the sagittal plane: a pilot study on field-based video analysis for female soccer players.
Journal of Human Kinetics, 45(March), 71–80.
Scavenius, M., Bak, K., Hansen, S., Norring, K., Jensen, K. H., & Jorgensen, U. (1999). Isolated
total ruptures of the anterior cruciate ligament - a clinical study with long-term follow-up of
7 years. Scandinavian Journal of Medicine & Science in Sports, 9(2), 114–119.
Seedhom, B. B., & Hargreaves, D. J. (1979). Transmission of the load in the knee joint with
special reference to the role of the menisci. Part II: Experimental results, discussion and
conclusions. Eng Med, 8(4), 220–228.
Seitz, A. M., Lubomierski, A., Friemert, B., Ignatius, A., & Dürselen, L. (2012). Effect of partial
meniscectomy at the medial posterior horn on tibiofemoral contact mechanics and meniscal
hoop strains in human knees. Journal of Orthopaedic Research : Official Publication of the
Orthopaedic Research Society, 30(6), 934–42.
Shambaugh, J. P., Klein, A., & Herbert, J. H. (1991). Structural measures as predictors of injury
basketball players. Medicine and Science in Sports and Exercise, 23(5), 522–7.
Shrive, N. G., Phil, D., O’connor, J. J., & Goodfellow, J. W. (1978). Load-Bearing in the Knee
Joint. Clinical Orthopaedics and Related Research, 131, 279–287.
Singer, J. C., & Lamontagne, M. (2008). The effect of functional knee brace design and hinge

73
misalignment on lower limb joint mechanics. Clinical Biomechanics, 23(1), 52–59.
Sitler, M., Ryan, J., Hopkinson, W., Wheeler, J., Santomier, J., Kolb, R., & Polley, D. (1989).
The efficacy of a prophylactic knee brace to reduce knee injuries in football. A prospective,
randomized study at West Point. The American Journal of Sports Medicine, 18(July), 310–
315.
Smith, J., Malanga, G. A., Yu, B., & An, K. N. (2003). Effects of Functional Knee Bracing on
Muscle-Firing Patterns about the Chronic Anterior Cruciate Ligament-Deficient Knee.
Archives of Physical Medicine and Rehabilitation, 84(11), 1680–1686.
Spindler, K. P., & Wright, R. W. (2008). Anterior Cruciate Ligament Tear, 2135–2142.
Stephen, J. M., Halewood, C., Kittl, C., Bollen, S. R., Williams, A., & Amis, A. A. (2016).
Posteromedial Meniscocapsular Lesions Increase Tibiofemoral Joint Laxity With Anterior
Cruciate Ligament Deficiency, and Their Repair Reduces Laxity. The American Journal of
Sports Medicine, 44(2), 400–8.
Sterett, W. I. (2006). Effect of Functional Bracing on Knee Injury in Skiers With Anterior
Cruciate Ligament Reconstruction: A Prospective Cohort Study. American Journal of
Sports Medicine, 34(10), 1581–1585.
Struewer, J., Ziring, E., Frangen, T. M., Efe, T., Meißner, S., Buecking, B., … Ishaque, B.
(2013). Clinical outcome and prevalence of osteoarthritis after isolated anterior cruciate
ligament reconstruction using hamstring graft: Follow-up after two and ten years.
International Orthopaedics, 37(2), 271–277.
Swirtun, L. R., Jansson, A., Renström, P., & Study, A. P. R. (2005). The effects of a functional
knee brace during early treatment of patients with a nonoperated acute anterior cruciate
ligament tear: a prospective randomized study. Clinical Journal of Sport Medicine : Official
Journal of the Canadian Academy of Sport Medicine, 15(5), 299–304.
Taylor, K. A., Terry, M. E., Utturkar, G. M., Spritzer, C. E., Queen, R. M., Irribarra, L. A., …
DeFrate, L. E. (2011). Measurement of in vivo anterior cruciate ligament strain during
74
dynamic jump landing. Journal of Biomechanics, 44(3), 365–371.
Taylor, K. a, Cutcliffe, H. C., Queen, R. M., Utturkar, G. M., Spritzer, C. E., Garrett, W. E., &
DeFrate, L. E. (2013). In vivo measurement of ACL length and relative strain during
walking. Journal of Biomechanics, 46(3), 478–83.
Taylor, K. a, Terry, M. E., Utturkar, G. M., Spritzer, C. E., Queen, R. M., Irribarra, L. a, …
DeFrate, L. E. (2011). Measurement of in vivo anterior cruciate ligament strain during
dynamic jump landing. Journal of Biomechanics, 44(3), 365–71.
Thelen, D. G., & Anderson, F. C. (2006). Using computed muscle control to generate forward
dynamic simulations of human walking from experimental data. Journal of Biomechanics,
39(6), 1107–1115.
Torry, M. R., Shelburne, K. B., Myers, C., Giphart, J. E., Pennington, W. W., Krong, J. P., …
Woo, S. L.-Y. (2013). High knee valgus in female subjects does not yield higher knee
translations during drop landings: a biplane fluoroscopic study. Journal of Orthopaedic
Research : Official Publication of the Orthopaedic Research Society, 31(2), 257–67.
van Eck, C. F., Schreiber, V. M., Mejia, H. A., Samuelsson, K., van Dijk, C. N., Karlsson, J., &
Fu, F. H. (2010). “Anatomic” anterior cruciate ligament reconstruction: a systematic review
of surgical techniques and reporting of surgical data. Arthroscopy: The Journal of
Arthroscopic & Related Surgery, 26(9 Suppl), S2-12.
Winter, D. A. (2009). Biomechanics and Motor Control of Human Movement (4th ed.). John
Wiley & Sons.
Withrow, T. J., Huston, L. J., Wojtys, E. M., & Ashton-Miller, J. a. (2006). The relationship
between quadriceps muscle force, knee flexion, and anterior cruciate ligament strain in an in
vitro simulated jump landing. The American Journal of Sports Medicine, 34(2), 269–74.
Wojtys, E. M., Kothari, S. U., & Huston, L. J. (1996). Anterior Cruciate Ligament Functional
Brace Use in Sports*. The American Journal of Sports Medicine, 24(4), 539–546.
Wojtys, E. M., Loubert, P. V, Samson, S. Y., & Viviano, D. M. (1990). Use of a knee-brace for
75
control of tibial translation and rotation. A comparison, in cadavera, of available models.
The Journal of Bone and Joint Surgery. American Volume, 72(9), 1323–9.
Wright, R. W., & Fetzer, G. B. (2007). Bracing after ACL reconstruction: a systematic review.
Clin Orthop Relat Res, 455(455), 162–168.
Yoo, J. H., Chang, C. B., Shin, K. S., Seong, S. C., & Kim, T. K. (2008). Anatomical References
to Assess the Posterior Tibial Slope in Total Knee Arthroplasty: A Comparison of 5
Anatomical Axes. The Journal of Arthroplasty, 23(4), 586–592.
Yoshioka, Y., Siu, D., & Cooke, T. D. (1987). The anatomy and functional axes of the femur.
The Journal of Bone and Joint Surgery. American Volume, 69(6), 873–80.

76
Appendix 1: Cadaver Preparation 7
7.1 Dissection
Figure 17. Knee dissection process. (A)-(C) Removal of the skin. (D)-(J) Removal of muscle
tissue. (K)-(L) Capsule preparation.
77
A. An anterior incision was made along the length of specimen, and sharp disection was carried
with a scalpel though the subcutaneous tisssues. B. The skin and subcutaneous fat was
circumferentially reflected from the fascia. C. All superficial tissue layers were removed. D.
Hamstring tendons (gracilis and semi-tendinousus) were harvested for use in the ACL
reconstruction. E. Superficial and deep posterior calf muscles being removed F. Anterior tibialis
muscle dissected from the tibia. G. Quadriceps muscle tissue removed from femur. H. Vastus
medialis being carefully dissected from the capsule. I. Continued stripping of the vastus lateralis
and medialis. J. Leftover muscle tissue was scraped from the femur and tibia. K. Medial para-
patellar arthrotomy made to facilitate DVRT insertion. L. The infrapatellar fat pad was partially
resected to accommodate the DVRT cable.
7.2 Muscle Cable Insertion
Stainless steel cables were used to apply the muscle forces on the cadaveric specimens. The wire
rope used was an ultra-flexible 7 strand core x 19 core stainless steel with a maximum tensile
strength of 3,336N.
During dissection, the tendon insertions of the gastrocnemius and hamstrings were marked.
Muscle cables were placed at the location of the approximate anatomical insertion sites. The
gastrocnemius cable was looped through the femur and crimped on the posterior side as seen in
figure 18A. The hamstring cable was attached to the tibia through a stainless-steel tube which
was secured with fiberglass casting tape as seen in figure 18B. With the cables taut and the knee
flexed, the cables directed force in a line-of-action similar to their anatomic counterparts.
The quadriceps cable was attached using a different mechanism. Early testing revealed that
drilling and attaching the cable directly to the patella resulted in patellar fractures under large
loads. Instead, a 10mm hole was drilled through the long axis of the patella and a stainless-steel
tube was inserted. The stainless-steel cable was then passed through this tube and attached into
the tibial tubercle at the anatomical insertion of the patellar tendon (Figure 18C).

78
Figure 18. Experimental Muscle Cable Setup.
(A) Hamstring and Gastrocnemius muscle attachments viewed from the posterior aspect of the
knee (B), and from the medial aspect. (C). Quadriceps cable attachment through the patella.
7.3 Foaming Procedure
1. Prior to dissection, the cadaveric specimens were visually inspected. The specimens were
often frozen on a flat surface and the soft tissue envelope was irregular. These specimens
were deforested and refrozen hanging to replicate the cylindrical shape of the in-vivo
tissues.
2. All specimens were measured using the Össur SmartMeasure application for custom
bracing. The application required circumferential dimensions 7.5 and 15cm above and
below the joint line, and the medial-lateral condylar width. These dimensions along with
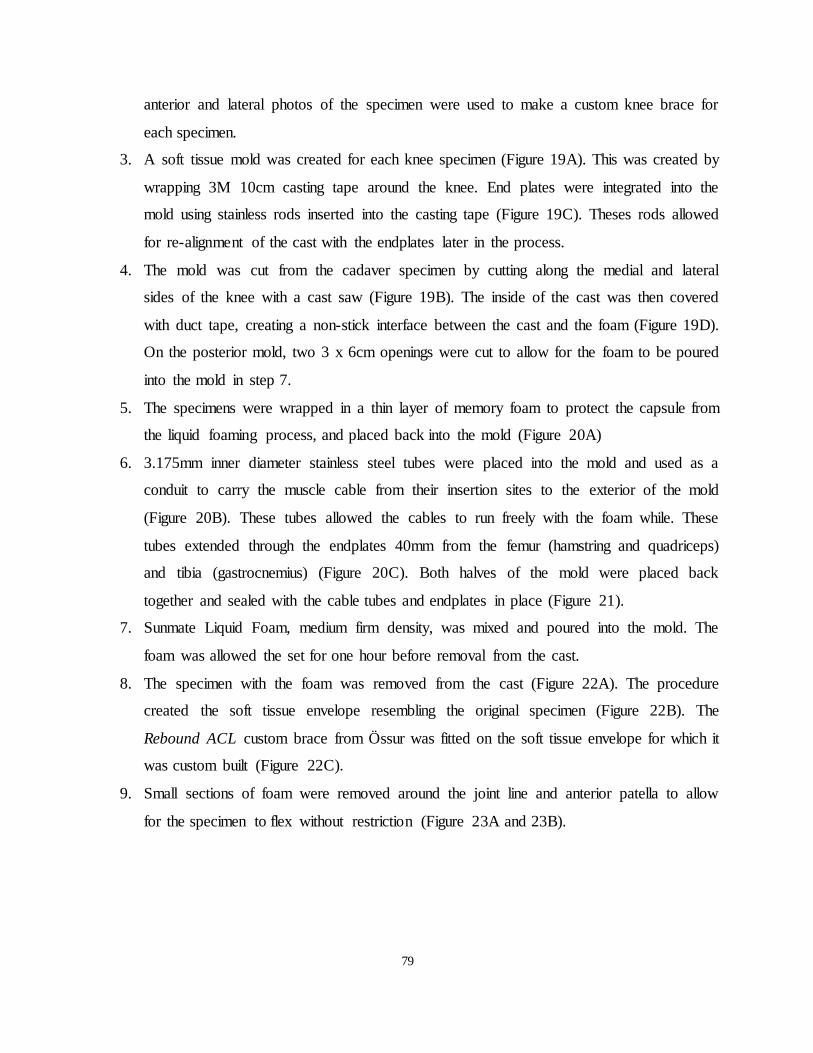
79
anterior and lateral photos of the specimen were used to make a custom knee brace for
each specimen.
3. A soft tissue mold was created for each knee specimen (Figure 19A). This was created by
wrapping 3M 10cm casting tape around the knee. End plates were integrated into the
mold using stainless rods inserted into the casting tape (Figure 19C). Theses rods allowed
for re-alignment of the cast with the endplates later in the process.
4. The mold was cut from the cadaver specimen by cutting along the medial and lateral
sides of the knee with a cast saw (Figure 19B). The inside of the cast was then covered
with duct tape, creating a non-stick interface between the cast and the foam (Figure 19D).
On the posterior mold, two 3 x 6cm openings were cut to allow for the foam to be poured
into the mold in step 7.
5. The specimens were wrapped in a thin layer of memory foam to protect the capsule from
the liquid foaming process, and placed back into the mold (Figure 20A)
6. 3.175mm inner diameter stainless steel tubes were placed into the mold and used as a
conduit to carry the muscle cable from their insertion sites to the exterior of the mold
(Figure 20B). These tubes allowed the cables to run freely with the foam while. These
tubes extended through the endplates 40mm from the femur (hamstring and quadriceps)
and tibia (gastrocnemius) (Figure 20C). Both halves of the mold were placed back
together and sealed with the cable tubes and endplates in place (Figure 21).
7. Sunmate Liquid Foam, medium firm density, was mixed and poured into the mold. The
foam was allowed the set for one hour before removal from the cast.
8. The specimen with the foam was removed from the cast (Figure 22A). The procedure
created the soft tissue envelope resembling the original specimen (Figure 22B). The
Rebound ACL custom brace from Össur was fitted on the soft tissue envelope for which it
was custom built (Figure 22C).
9. Small sections of foam were removed around the joint line and anterior patella to allow
for the specimen to flex without restriction (Figure 23A and 23B).

80
Figure 19. Negative mold casting preparation
(A) Specimen casting, (B) cast removal, (C) location rods, (D) mold preparation.
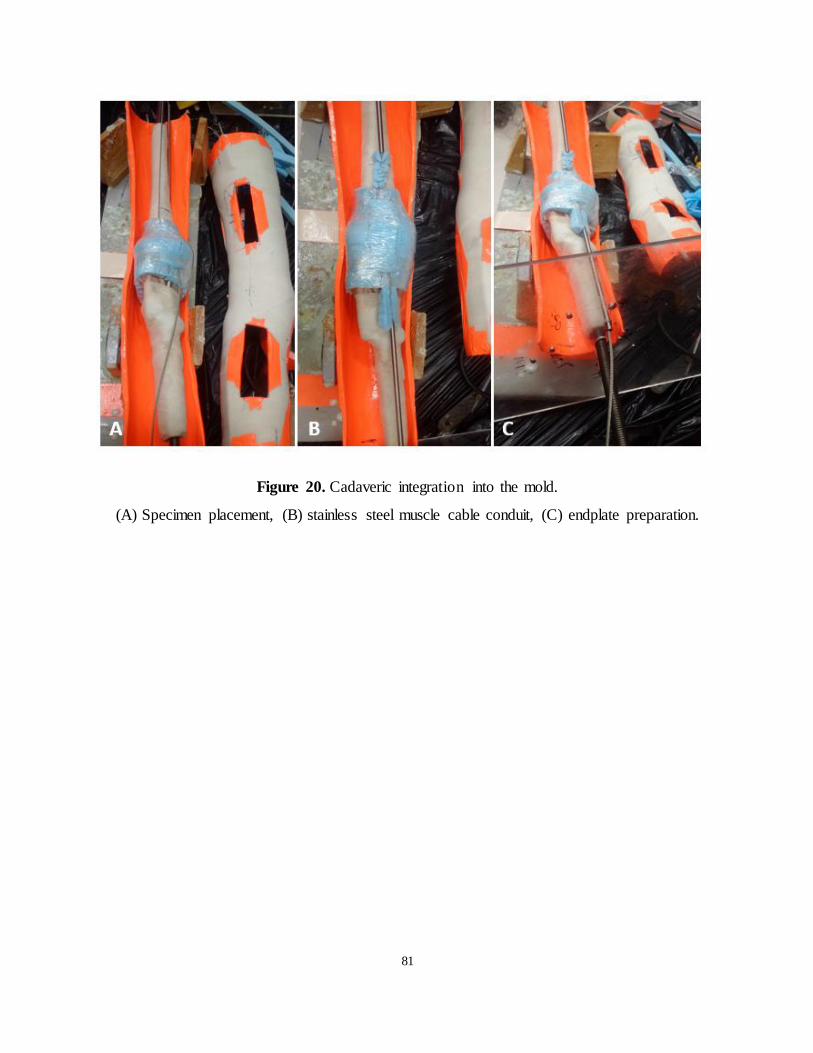
81
Figure 20. Cadaveric integration into the mold.
(A) Specimen placement, (B) stainless steel muscle cable conduit, (C) endplate preparation.

82
Figure 21. View through the end plate of a sealed mold with specimen and cable conduit in
place.
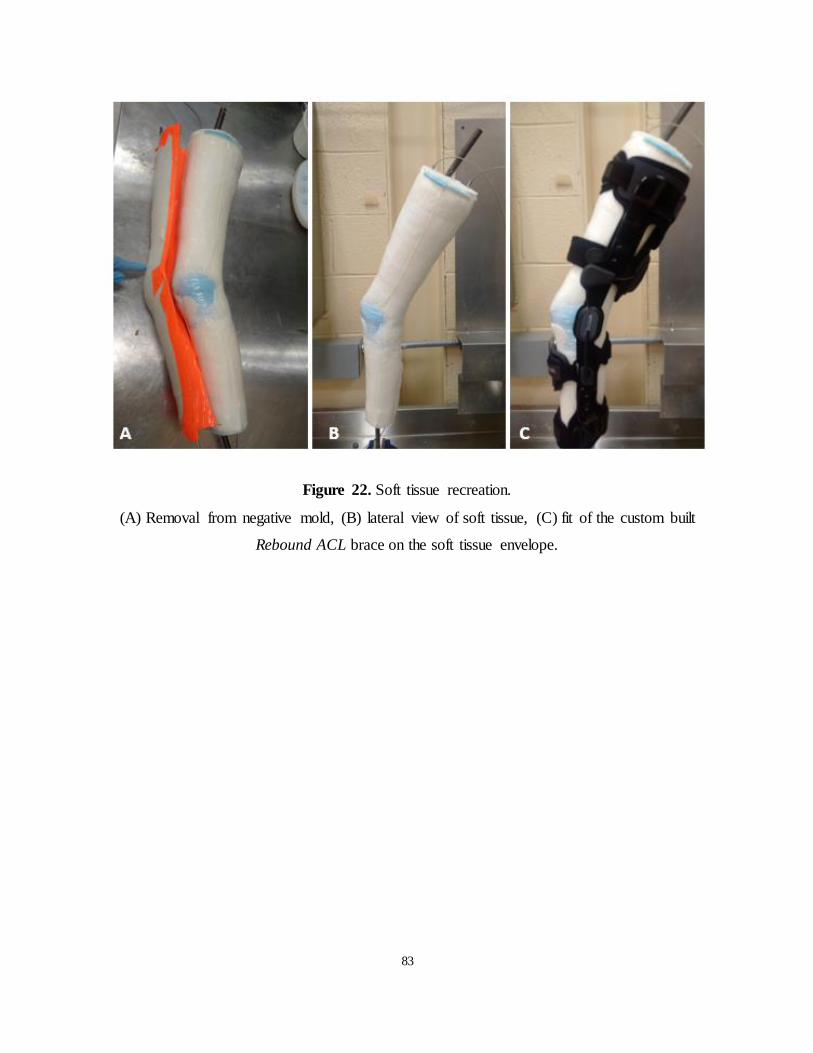
83
Figure 22. Soft tissue recreation.
(A) Removal from negative mold, (B) lateral view of soft tissue, (C) fit of the custom built
Rebound ACL brace on the soft tissue envelope.
84
Figure 23. Removal of restrictive joint foam.
(A) Anterior view, (B) sagittal view.
7.4 Moment Arm Calculations
The cadaveric moment arms for each of the three muscle groups (gastrocnemius, hamstring, and
quadriceps) were measured. Moment arms were measured using a tendon excursion method. The
tendon excursion method uses the formula
, which states that the moment arm is
equal to the slope of tendon length and knee angle.
Each knee specimen was flexed through it’s a range-of-motion of 80 degrees on a custom-built
tendon excursion apparatus. Knee flexion angle was measured using an electronic goniometer
(Figure 25A) and the change in tendon length was measured using an LVDT (Figure 25B).
These results were plotted in Excel (Microsoft Corp.), and the slope of was calculated with the
built-in fit line function (Figure 25). This slope was used to convert the OpenSim muscle forces
as outlined in Bakker et al (Bakker et al., 2016). The average moment arm calculated for the
quadriceps, hamstring, gastrocnemius was 41.6mm, 26.1mm, and 18.6mm respectively, closely
matching reported moment arms in the literature (Herzog & Read, 1993). Moment arms were
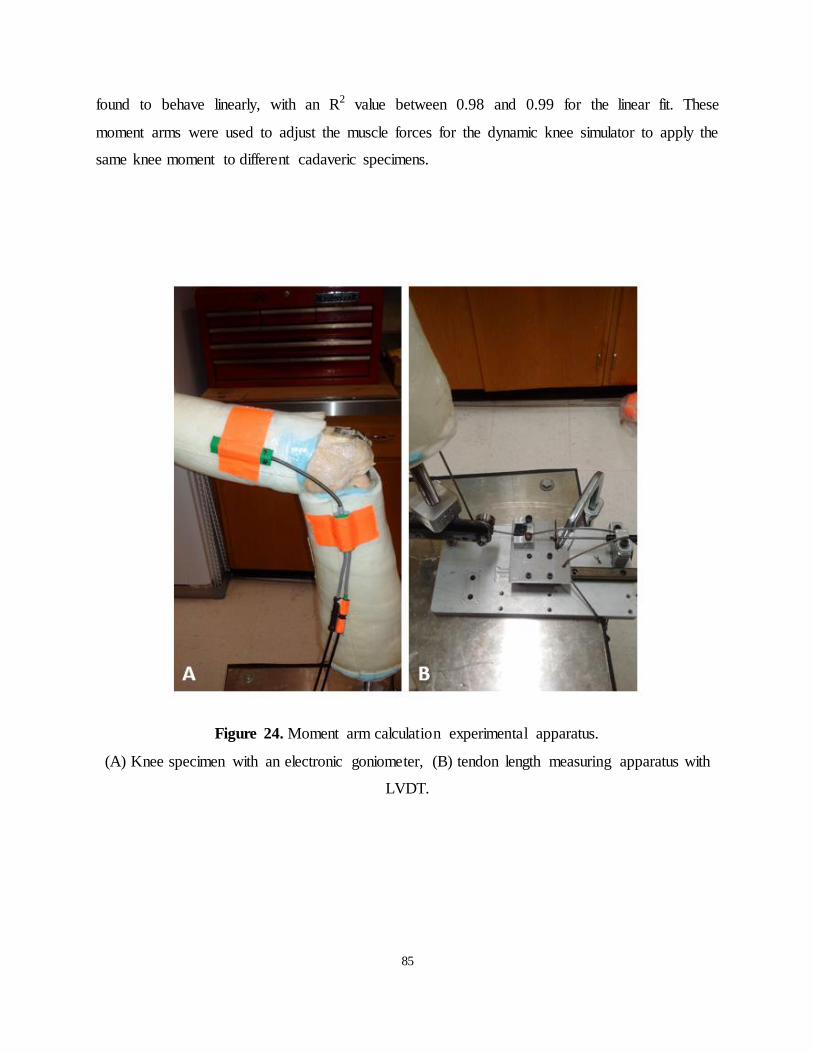
85
found to behave linearly, with an R2 value between 0.98 and 0.99 for the linear fit. These
moment arms were used to adjust the muscle forces for the dynamic knee simulator to apply the
same knee moment to different cadaveric specimens.
Figure 24. Moment arm calculation experimental apparatus.
(A) Knee specimen with an electronic goniometer, (B) tendon length measuring apparatus with
LVDT.
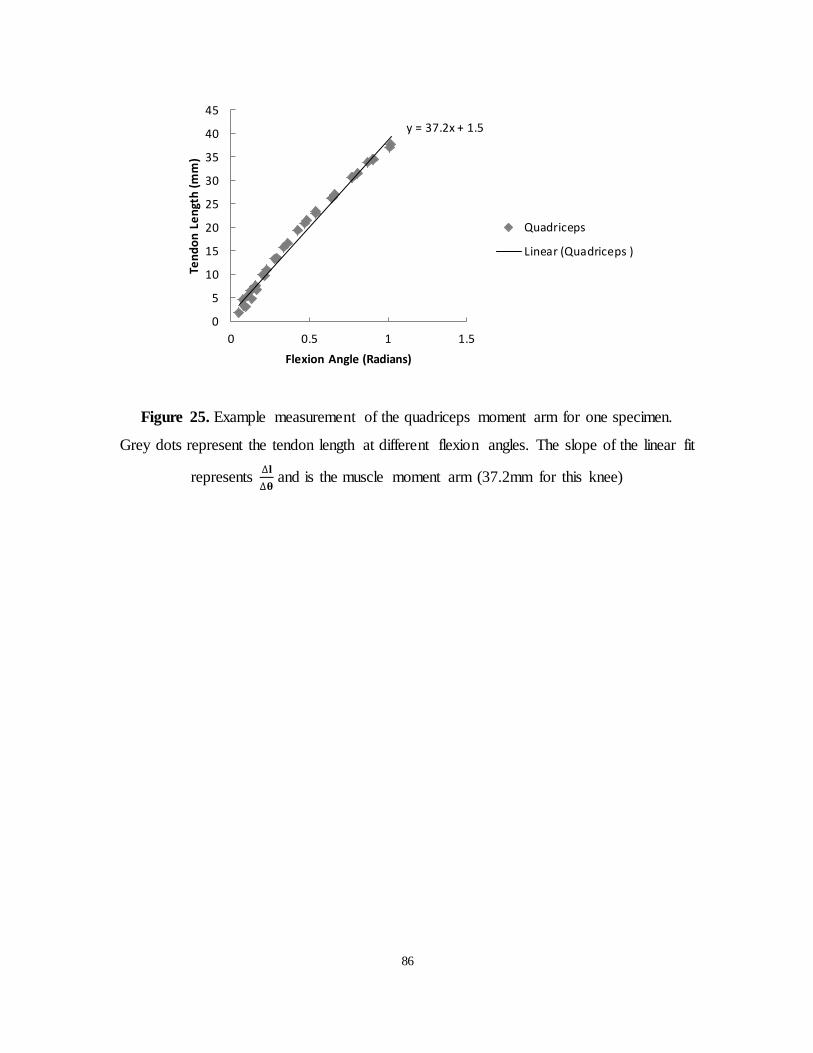
86
Figure 25. Example measurement of the quadriceps moment arm for one specimen.
Grey dots represent the tendon length at different flexion angles. The slope of the linear fit
represents
and is the muscle moment arm (37.2mm for this knee)
y = 37.2x + 1.5
0
5
10
15
20
25
30
35
40
45
0 0.5 1 1.5
Ten
do
n L
en
gth
(m
m)
Flexion Angle (Radians)
Quadriceps
Linear (Quadriceps )

87
Appendix 2: Pilot Testing 8
Prior to the beginning in-vitro data collection, several smaller experiments and pilot trials were
conducted. A brief summary of these experiments is described here.
8.1 Pilot 1
Aim 1: To select a motion capture participant and trial that represents the current literature
averages.
Methods: Motion capture was collected on one male (Age 24 years, Mass 75kg, Height 180cm)
and one female (Age 28 years, Mass 67kg, Height 175cm), performing a double leg squat, a
single leg squat and walking. Reference data was available for walking kinematics but not
squatting. Both participants gait trials were compared against three gait characterization papers.
The gait trial that best fit the papers were selected. Once the participant was selected, squatting
kinematics were extracted and the trial which best fit the average trial of the participant was
selected.
Key Findings:
Three gait trials were collected for each subject
Gait parameters were compared to three reference papers: Pietrazewski et al. , Liu
et al. and Oberg et al (Liu et al., 2008; T Oberg et al., 1993; Pietraszewski,
Winiarski, & Jaroszczuk, 2012).
Pietrazewski et al, presented only an average curve for gait data (Pietraszewski et
al., 2012). A comparison of the current knee flexion angles with Piertrazewski is
shown in Figure 26. The male participant better matched the kinematics
presented in Piertrazewski during stance while the female participant matched
closer during swing.
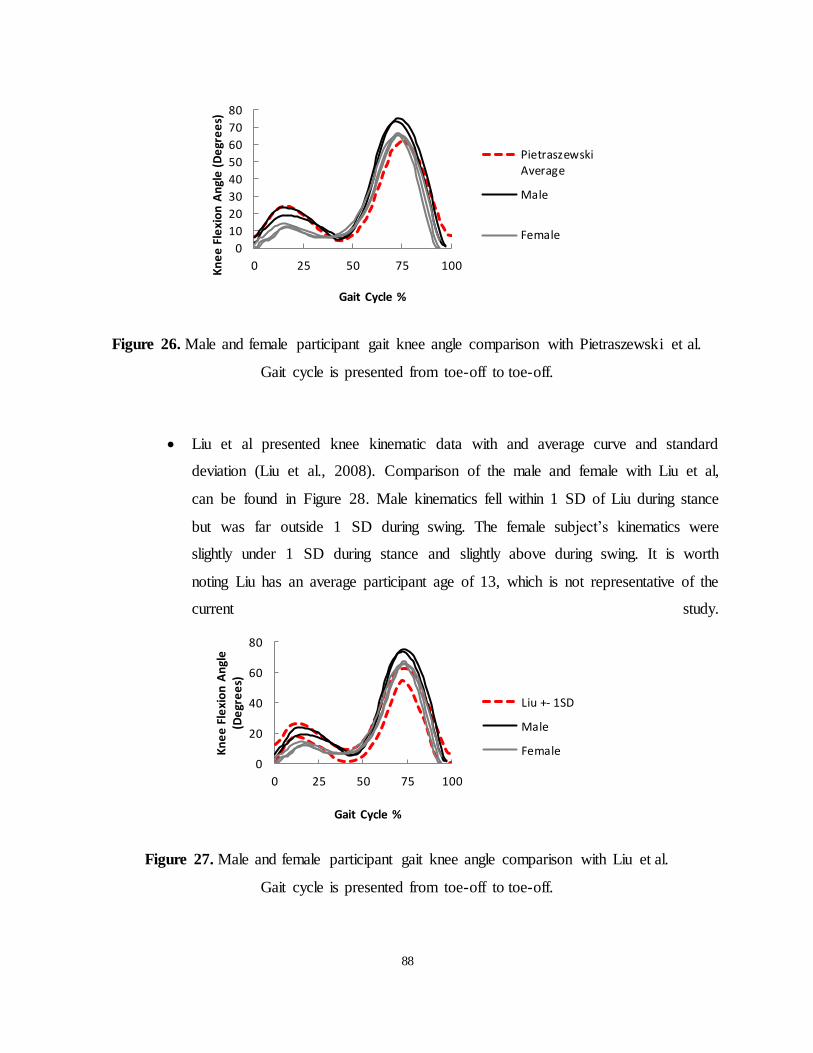
88
Figure 26. Male and female participant gait knee angle comparison with Pietraszewski et al.
Gait cycle is presented from toe-off to toe-off.
Liu et al presented knee kinematic data with and average curve and standard
deviation (Liu et al., 2008). Comparison of the male and female with Liu et al,
can be found in Figure 28. Male kinematics fell within 1 SD of Liu during stance
but was far outside 1 SD during swing. The female subject’s kinematics were
slightly under 1 SD during stance and slightly above during swing. It is worth
noting Liu has an average participant age of 13, which is not representative of the
current study.
Figure 27. Male and female participant gait knee angle comparison with Liu et al.
Gait cycle is presented from toe-off to toe-off.
0
10
20
30
40
50
60
70
80
0 25 50 75 100Kn
ee
Fle
xio
n A
ngl
e (
De
gre
es)
Gait Cycle %
PietraszewskiAverage
Male
Female
0
20
40
60
80
0 25 50 75 100
Kn
ee
Fle
xio
n A
ngl
e
(De
gre
es)
Gait Cycle %
Liu +- 1SD
Male
Female
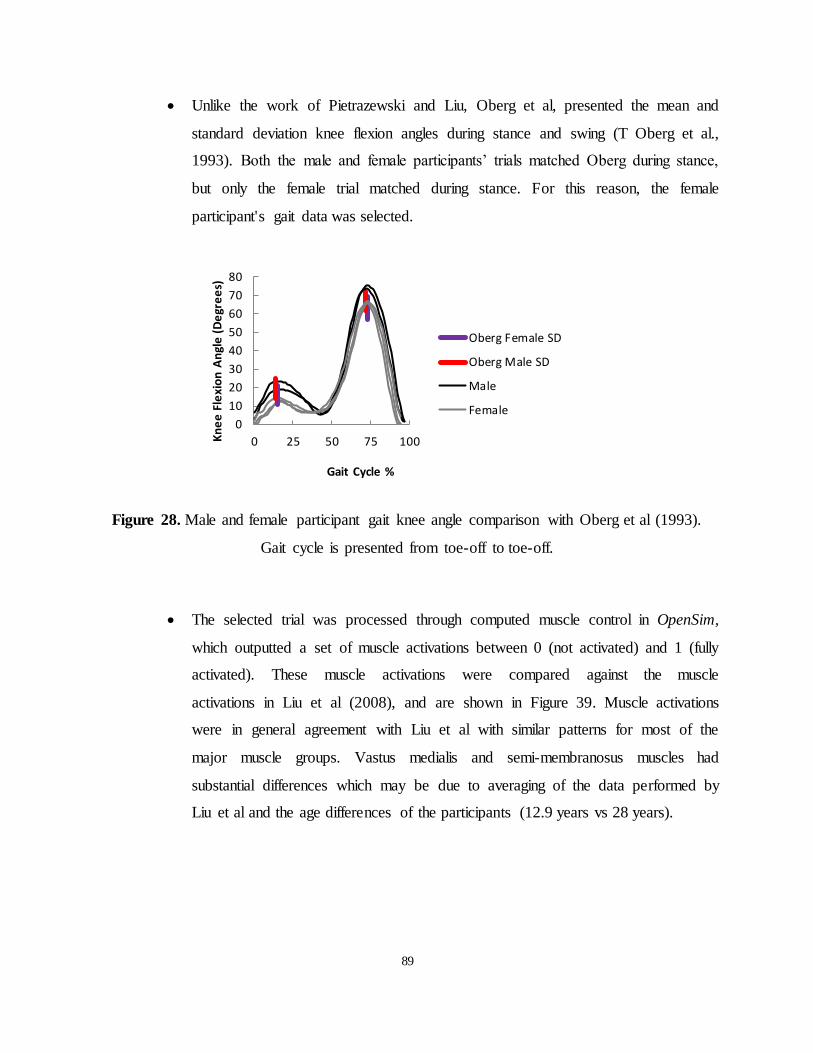
89
Unlike the work of Pietrazewski and Liu, Oberg et al, presented the mean and
standard deviation knee flexion angles during stance and swing (T Oberg et al.,
1993). Both the male and female participants’ trials matched Oberg during stance,
but only the female trial matched during stance. For this reason, the female
participant's gait data was selected.
Figure 28. Male and female participant gait knee angle comparison with Oberg et al (1993).
Gait cycle is presented from toe-off to toe-off.
The selected trial was processed through computed muscle control in OpenSim,
which outputted a set of muscle activations between 0 (not activated) and 1 (fully
activated). These muscle activations were compared against the muscle
activations in Liu et al (2008), and are shown in Figure 39. Muscle activations
were in general agreement with Liu et al with similar patterns for most of the
major muscle groups. Vastus medialis and semi-membranosus muscles had
substantial differences which may be due to averaging of the data performed by
Liu et al and the age differences of the participants (12.9 years vs 28 years).
0
10
20
30
40
50
60
70
80
0 25 50 75 100Kn
ee
Fle
xio
n A
ngl
e (
De
gre
es)
Gait Cycle %
Oberg Female SD
Oberg Male SD
Male
Female

90
Figure 29. Muscle activation comparison during gait.
(Column 1) Rectus femoris, biceps femoris long head, medial gastrocnemius and anterior tibialis
0
0.25
0.5
0.75
1
0 20 40 60 80 100
Act
ivat
ion
% Gait Cycle
Rectus Femoris Activation
Subject Liu Toe Off
0
0.25
0.5
0.75
1
0 20 40 60 80 100
Act
ivat
ion
% Gait Cycle
Semimember Activation
Subject Liu Toe Off
0
0.25
0.5
0.75
1
0 20 40 60 80 100
Act
ivat
ion
% Gait Cycle
Vastus Medialis Activation
Subject Liu Toe Off
0
0.25
0.5
0.75
1
0 20 40 60 80 100
Act
ivat
ion
% Gait Cycle
Bicepfemoris Long Head Activation
Subject Liu Toe Off
0
0.25
0.5
0.75
1
0 20 40 60 80 100
Act
ivat
ion
% Gait Cycle
Medial Gastroc Activation
Subject Liu Toe Off
0
0.25
0.5
0.75
1
0 20 40 60 80 100
Act
ivat
ion
% Gait Cycle
Soleus Activation
Subject Liu Toe Off
0
0.25
0.5
0.75
1
0 20 40 60 80 100
Act
ivat
ion
% Gait Cycle
Ant Tib Activation
Subject Liu Toe Off
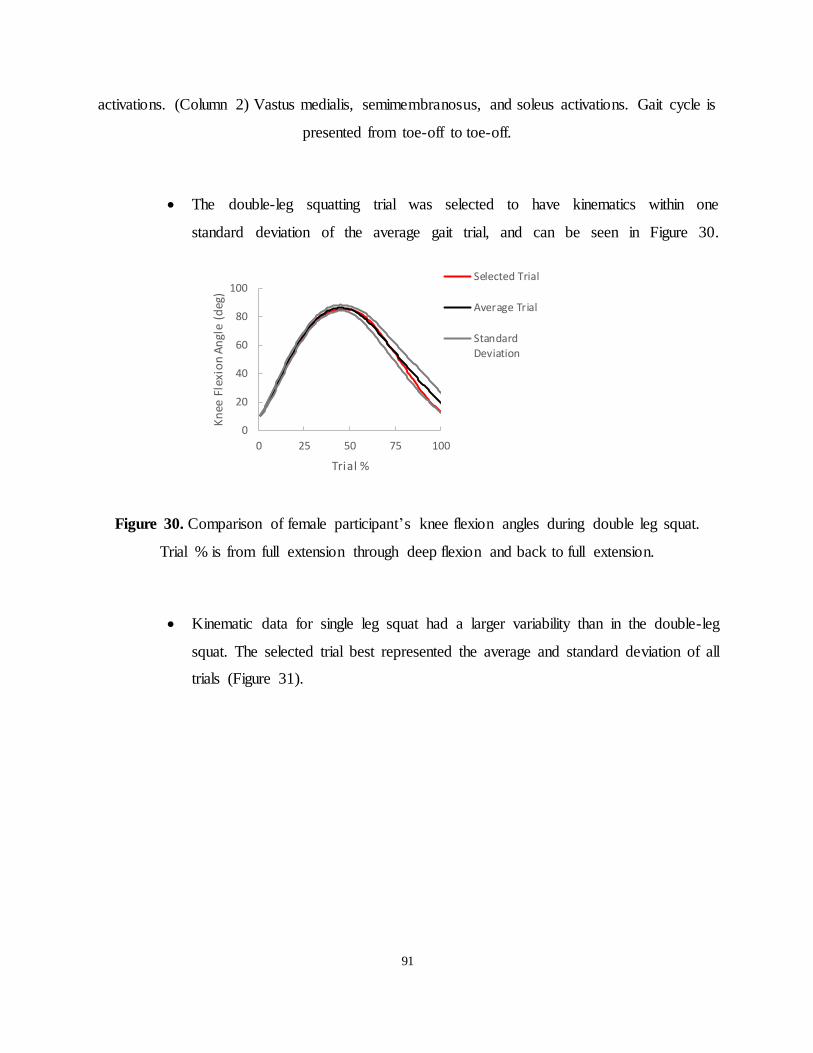
91
activations. (Column 2) Vastus medialis, semimembranosus, and soleus activations. Gait cycle is
presented from toe-off to toe-off.
The double-leg squatting trial was selected to have kinematics within one
standard deviation of the average gait trial, and can be seen in Figure 30.
Figure 30. Comparison of female participant’s knee flexion angles during double leg squat.
Trial % is from full extension through deep flexion and back to full extension.
Kinematic data for single leg squat had a larger variability than in the double-leg
squat. The selected trial best represented the average and standard deviation of all
trials (Figure 31).
0
20
40
60
80
100
0 25 50 75 100
Kn
ee F
lexi
on
An
gle
(deg
)
Trial %
Selected Trial
Average Trial
StandardDeviation

92
Figure 31. Comparison of female participant’s knee flexion angles single double leg squat.
Trial % is from full extension through deep flexion and back to full extension.
8.2 Pilot 2
Aim 2: Collect pilot data to optimize accuracy and reliability of in-vitro tests
Methods: Three cadaveric specimens were used for pilot testing. ACL and meniscal strains were
analyzed to ensure the magnitudes and patterns were within expected values.
Key Findings:
The first specimen had non-physiologic strains in both the ACL and meniscus.
Figure 32 the respective tissue strains with and without a brace during double leg
squat. Relative ACL strain was found to have a high negative strain (-15 to -35%)
and did not match the strain patterns found in the literature for squatting. The
Meniscal strain was also found to peak above 20% which is above the reported
ultimate strain of 10.25%. Several changes, reported below, were made to address
these issues.
0
20
40
60
80
100
0 25 50 75 100Kn
ee F
lexi
on
An
gle
(Deg
)
Trial %
Selected Trial
Average Trial
Standard
Deviation

93
Figure 32. Pilot testing strain values during double leg squat.
(Left) ACL strain with and without brace, (Right) meniscal strain with and without brace.
The hip attachment was found to incorrectly load the specimens by not accounting
for the angular difference between the mechanical and anatomical axis. The
attachment was redesigned to adjust the mounting position of the femur (Figure
33). The ankle attachment, which is not constrained in the medial-lateral direction
would translate laterally. This new attachment applied load vertically onto the
tibia and did not translate laterally.
Figure 33. Hip upgraded attachment.
(A) Hip attachment with zero degrees of femoral angulation and (B) hip attachment with 15
degrees of femoral angulation.
-40
-35
-30
-25
-20
-15
-10
-5
0
5
0 25 50 75 100A
CL
Stra
in %
Trial % Without Brace
With Brace
-15
-10
-5
0
5
10
15
20
25
0 25 50 75 100
Men
isca
l Str
ain
%
Trial %
Without Brace
With Brace
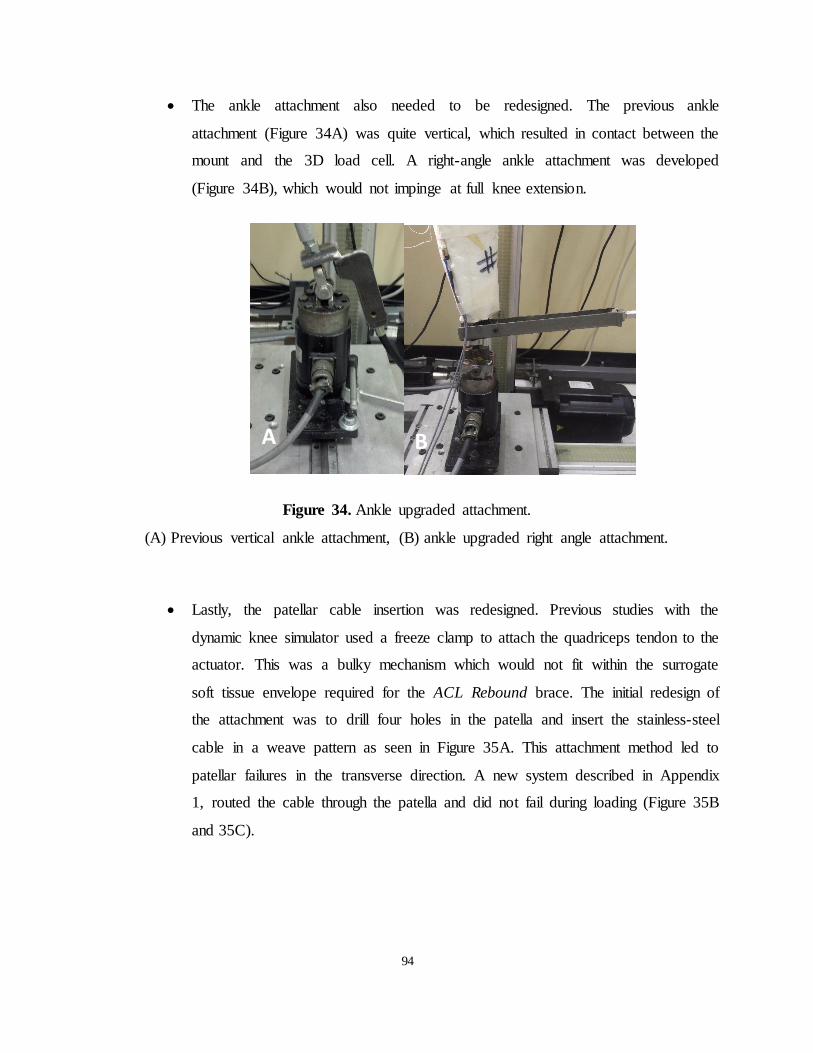
94
The ankle attachment also needed to be redesigned. The previous ankle
attachment (Figure 34A) was quite vertical, which resulted in contact between the
mount and the 3D load cell. A right-angle ankle attachment was developed
(Figure 34B), which would not impinge at full knee extension.
Figure 34. Ankle upgraded attachment.
(A) Previous vertical ankle attachment, (B) ankle upgraded right angle attachment.
Lastly, the patellar cable insertion was redesigned. Previous studies with the
dynamic knee simulator used a freeze clamp to attach the quadriceps tendon to the
actuator. This was a bulky mechanism which would not fit within the surrogate
soft tissue envelope required for the ACL Rebound brace. The initial redesign of
the attachment was to drill four holes in the patella and insert the stainless-steel
cable in a weave pattern as seen in Figure 35A. This attachment method led to
patellar failures in the transverse direction. A new system described in Appendix
1, routed the cable through the patella and did not fail during loading (Figure 35B
and 35C).
A B

95
Figure 35. Patellar cable attachments.
(A) Pilot study patellar attachment, (B) front view of improved patellar attachment with patellar
tunnel, (C) lateral view of improved patellar attachment.
8.3 Pilot 3
Aim 3: Create a soft tissue envelope with foam that best approximates in-vivo soft tissue
compliance.
Methods: A custom built indenter device was used to measure the compliance (N/mm) of the
selected subject (25.4mm diameter). The device “indents” contracted tissue, measuring both
force and displacement. Similar to previous work, liquid foam (Sunmate; Dynamic Systems Inc.,
Leicester, NC, USA) was used to create a surrogate soft tissue envelope. Multiple mixture
percentages were tested to find the best match in compliance.
Key Findings:
Compliance was measured on the participant in four different conditions:
quadriceps during a double leg squat, gastrocnemius during a double leg squat,
96
quadriceps during a maximum voluntary contraction, and gastrocnemius during a
maximum voluntary contraction. Compliance was not measured during a single
leg squat or gait because the measuring tool required a static position. Average
muscle compliance was found to be 11.4 N/mm (SD 4N/mm), shown in Figure
36.
The first mixture was Sunmate’s “semi-rigid” density. It was found that liquid
foam allowed to cure open to the air, formed a crust, which increased the stiffness
of the outer foam layers. The compliance did not match the subject’s compliance,
which was generally linear throughout. Compliance was found to be 42.5N/mm
and 30.0N/mm for the crust and inner layers respectively. These values are over
two times the stiffness of the participant.
The iso/polymer ratio was lowered from .55 to .4 to reduce the stiffness of the
foam. Compliance was found to be 12.65N/mm and 12.8N/mm for the crust and
inner layers respectively, which is within one standard deviation of the
participant’s average compliance. However, the new mixture ratio resulted in a
sticky outer texture which was undesirable for brace testing.
A new mixture “medium-firm” was ordered and tested. Unlike semi-rigid, the
medium-firm did not create an outer crust. The average compliance was found to
be 10.5N/mm, within one standard deviation of the participant’s average
compliance (Figure 36). This new mixture was the chosen mixture for all
simulations.
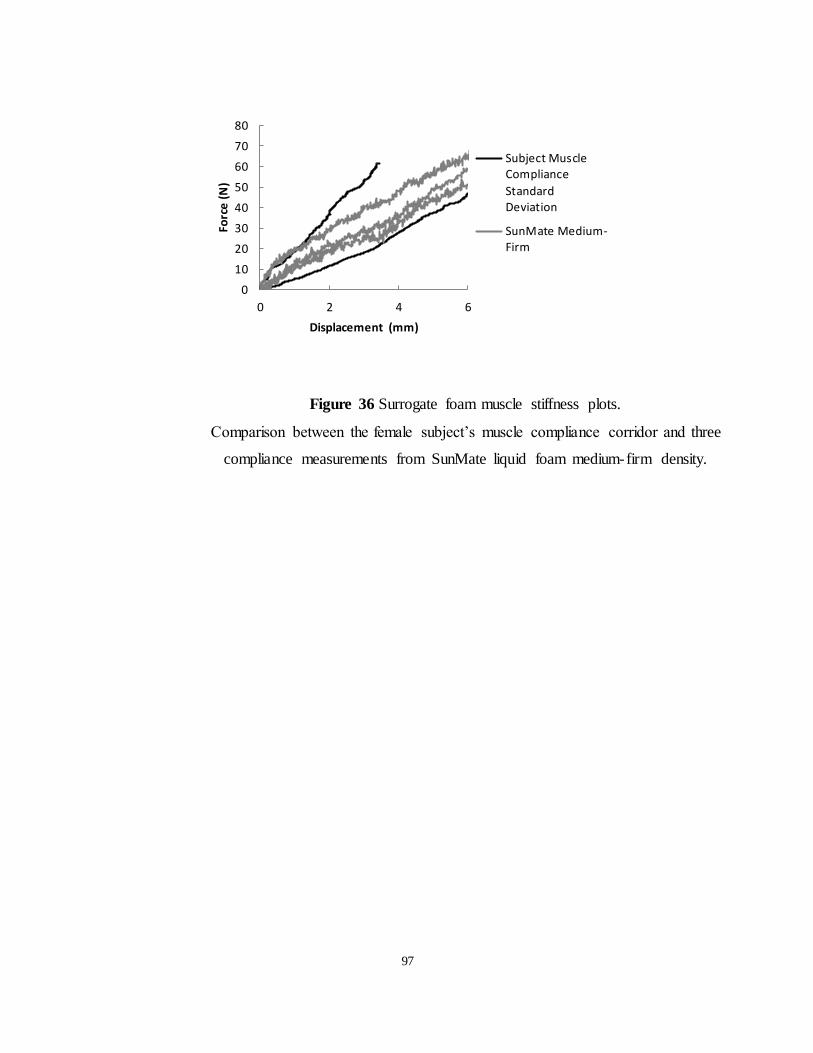
97
0
10
20
30
40
50
60
70
80
0 2 4 6
Forc
e (
N)
Displacement (mm)
Subject MuscleCompliance
StandardDeviation
SunMate Medium-Firm
Figure 36 Surrogate foam muscle stiffness plots.
Comparison between the female subject’s muscle compliance corridor and three
compliance measurements from SunMate liquid foam medium-firm density.