l3 4 .copd
TRANSCRIPT

DR.Bilal Natiq Nuaman,MD
C.A.B.M.,F.I.B.M.S.,D.I.M. 2016-2017
Chronic obstructivepulmonary disease
1

DefinitionChronic obstructive pulmonary disease (COPD) is
a preventable and treatable disease state characterized by airflow limitation that is not fully reversible.
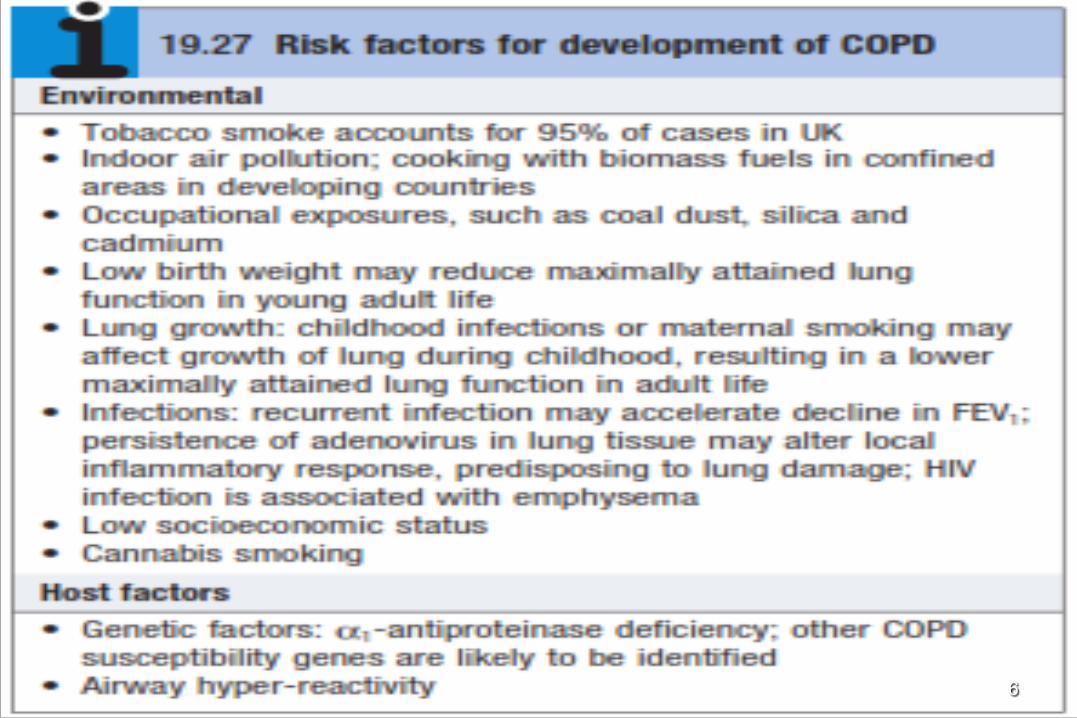
The airflow limitation is usually progressive and is associated with an abnormal inflammatory response of the lungs, primarily caused by cigarette smoking.
Although COPD affects the lungs, it also produces significant systemic consequences.
2

3

➢Major cause of death and disability ➢4th leading cause of death ➢COPD is the only chronic disease that is
showing progressive upward trend in both mortality and morbidity
➢It is expected to be the third leading cause of death by 2020
COPD GENERAL FACTS
4

% Change in Age Adjusted Death Rate
5
6
➢COPD should be suspected in any patient over the age of 35 years who presents with symptoms of persistent cough and sputum production and/or breathlessness.
➢Depending on the presentation important differential diagnoses include asthma, tuberculosis, bronchiectasis and congestive cardiac failure.
7

➢ Breathlessness usually heralds the first presentation to the health professional.
➢ In advanced disease, the presence of edema and morning headaches indicative of hypercapnia.
➢ Crackles may accompany infection but if persistent raise the possibility of bronchiectasis.
➢ Finger clubbing is not consistent with COPD and should alert the physician to potentially more serious pathology. (CA Lung)
8

➢Some patients with severe COPD may demonstrate signs consistent with corpulmonale (raised jugular venous pressure, loud P2 due to pulmonary hypertension, tricuspid regurgitation, pitting peripheral edema and hepatomegaly) and its presence usually indicates a poor prognosis.
9

Skeletal muscle wasting and cachexia may occur in advanced disease, while some patients may also be overweight.
The body mass index (BMI; weight/height²) should be calculated during the initial examination.
10
11

12
13

COPD clinical phenotypes
Chronic Bronchitis
(Blue Bloaters)
EmPhysema
(Pink Puffers)
14

15
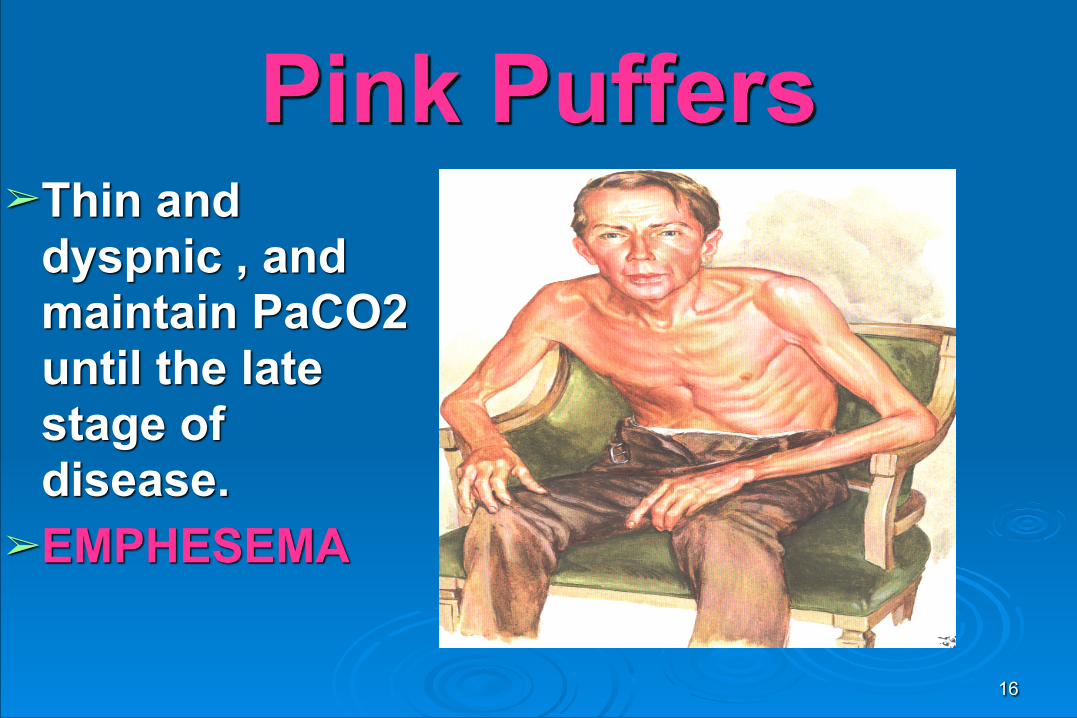
Pink Puffers➢Thin and
dyspnic , and maintain PaCO2 until the late stage of disease.
➢EMPHESEMA
16
Pursed lip breathing occur in emphysema not in chronic bronchitis
17

EMPHYSEMAPathological definition permanent dilatation of air spaces
distal to terminal bronchioles, accompanied by destruction of their walls
18

19

1. CENTRIACINAR (Centrilobular): Central part of the acinus (respiratory bronchioles)
is affected, while distal alveoli is spared. Upper lobes, particularly apical segments are involved
Cause: Cigarette smoking
2) PANACINAR (Panlobular): Entire acinus (from respiratory bronchiole to distal
alveoli affected) , Affects lower lobes Cause: α-1 antitryPsin deficiency
Types of emphysema
20
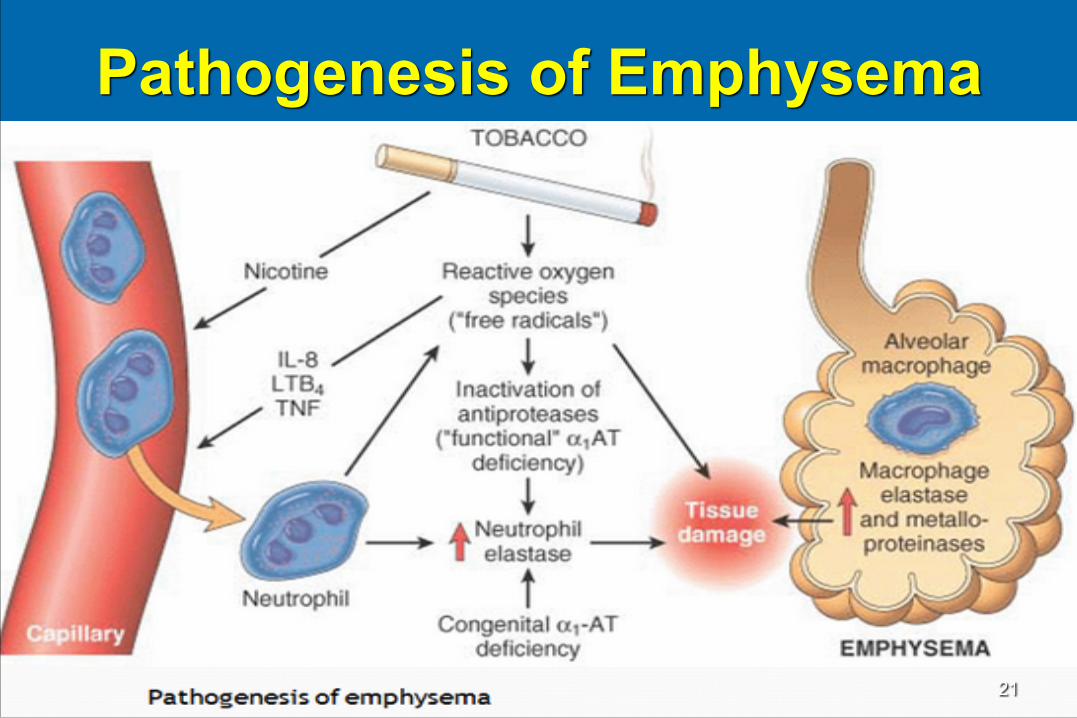
Pathogenesis of Emphysema
21

Clinical Features ➢No cyanosis (pink) ➢Presents with severe dyspnea (puffer) ➢Have a barrel chest. ➢X-ray shows large volume lung, Heart is
seems buried and diaphragm pushed down. Alveoli can rupture ! pneumothorax. ➢Don’t usually have cough or expectoration
PINK PUFFER22
23

24
BLUE BLOATER
Develop and tolerate hypercapnia earlier and may develop edema and 2‘ polycythemia.
CHRONIC BRONCHITIC
25
CHRONIC BRONCHITIS➢Defined clinically Persistent cough with sputum
production for at least 3 months in at least 2 consecutive years, with exclusion of other causes like Bronchiectasis .
26
PATHOGENESIS
SMOKING 4-10 times more common in heavy smokers ✓a smoking history of more than 20 pack years ➢Smoke and other irritants cause Hypertrophy of submucosal glands--- hypersecretion
of mucus Increase in goblet cells ↑predisposition to infection
27
Clinical Features➢Cyanosed (Blue) ➢Edematous (Bloater) ➢Productive Cough ➢CorPulmonale – heart failure ➢Usually dyspnea triggered by infection ➢Respiratory acidosis
Blue bloater
28

29

Diagnosis of COPD
SYMPTOMScough
sputumdyspnea
RISK FACTORS tobacco
SPIROMETRY EXAMINATION

Criteria of Dx 1-PFT : OBSTRUCTIVE LUNG PATTERN
➢FEV1 ↓ <80% ➢FVC low-normal 70-80% ➢FEV1/ FVC ↓ <70%
31

2-Negative reversibility test (Post-bronchodilator FEV1 <15% (200ML) increase following administration of bronchodilator or trial of corticosteroids) .
32

DLCO: Transfer Factor • Asthma high • Chronic bronchitis normal • Emphysema low
33
Other tests
➢Hemoglobin level and packed cell volume (PCV) can be elevated as a result of persistent hypoxemia causing secondary polycythemia.
➢Arterial blood gases (ABGs) determine the degree of hypoxia and hypercapnia.
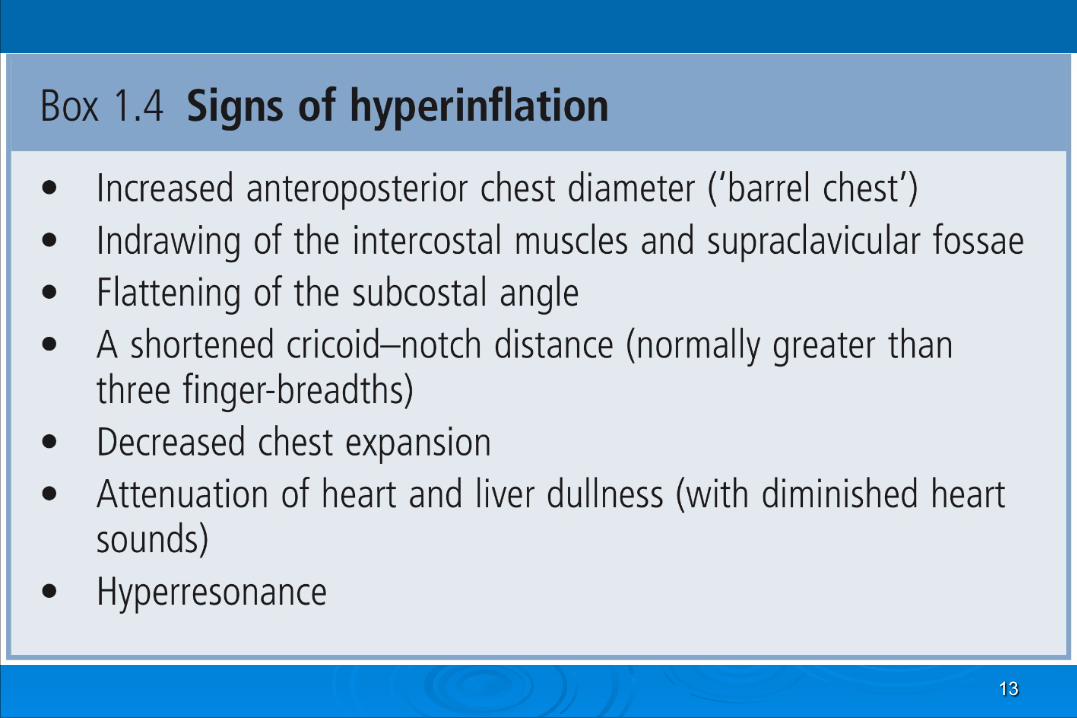
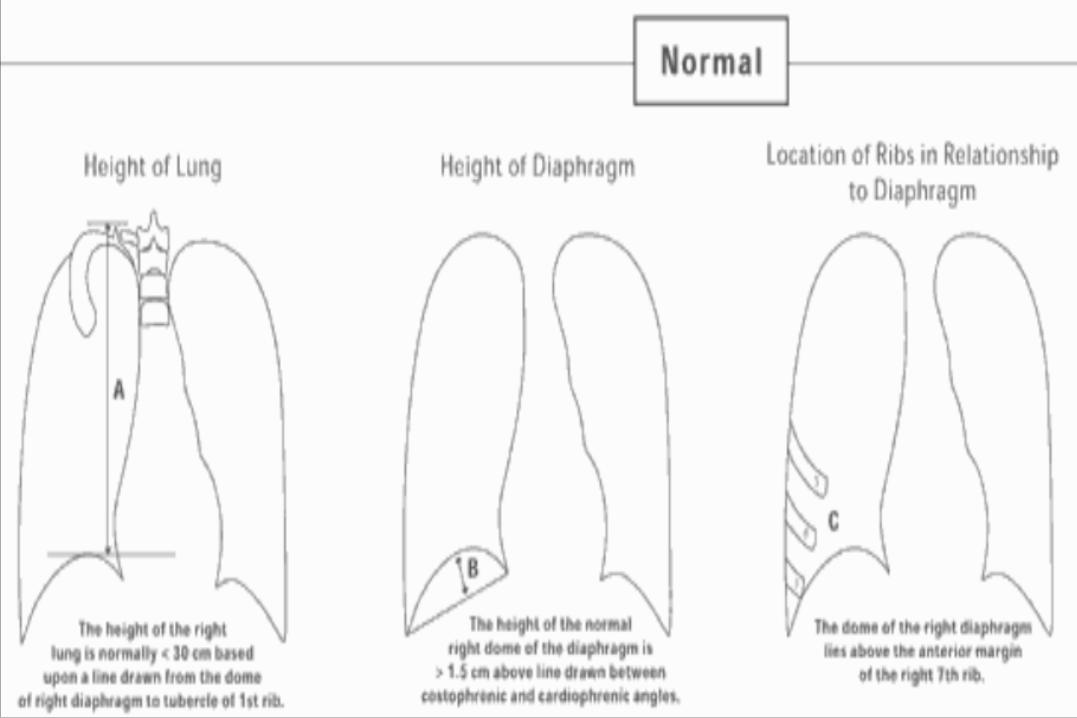
➢CXR can be normal or show hyper-expanded lung fields with low flattened diaphragms and the presence of bullae (emphysema).
➢ECG can show advanced cor pulmonale ➢ Alpha-antitrypsin level and phenotype may be helpful
(young non smokers, lower lobe emphysema, a family history of chest problems). 34
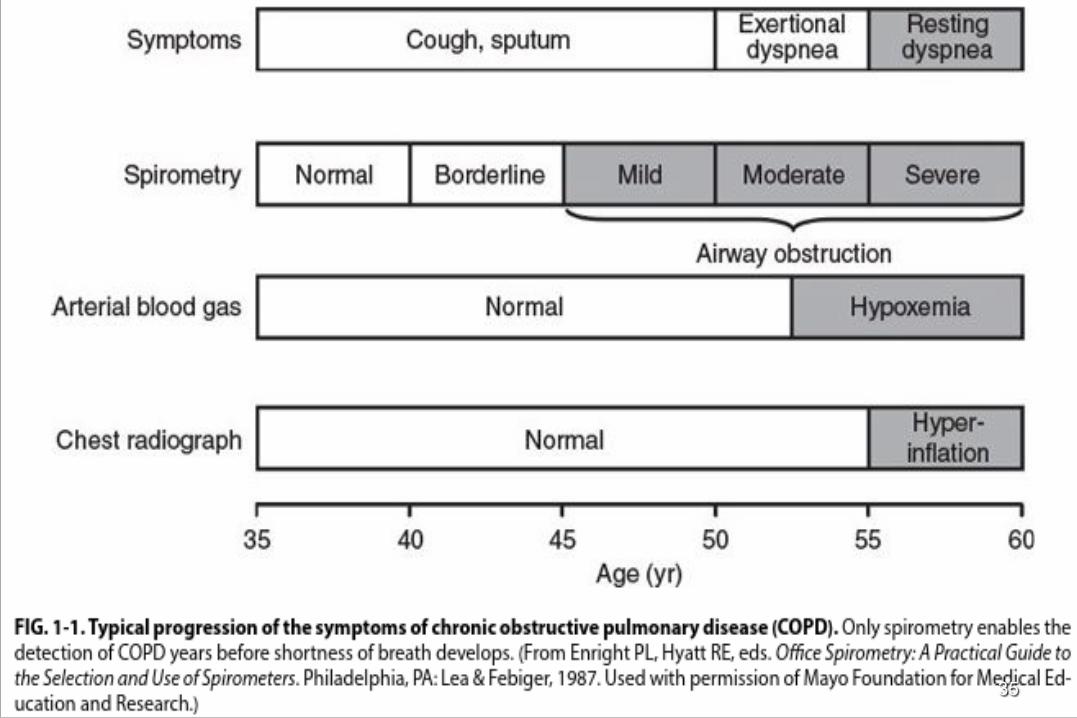
35

Disease Progression of a Patients with COPD
Symptoms
Exacerbations
ExacerbationsExacerbations
Deterioration
End of Life
36

37
Management of
COPD38
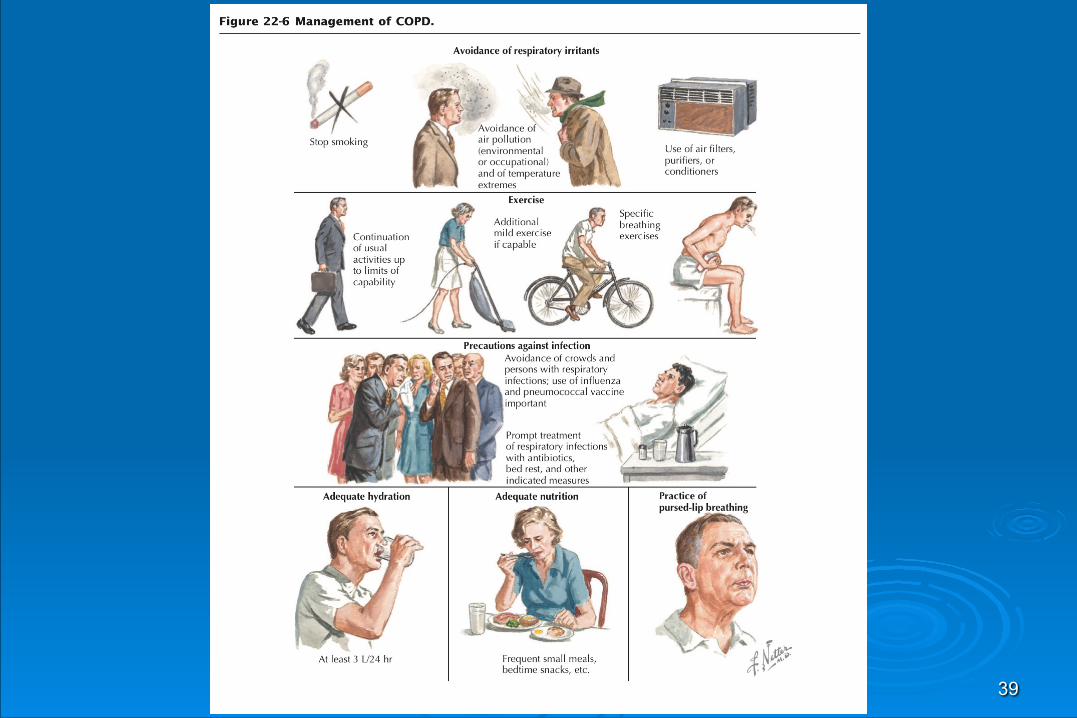
39

40
Smoking cessation
➢The only intervention proven to decelerate the decline in FEV1. 41

PharmacotherapyBRONCHODILATORS ➢Decrease airway muscle tone ➢Three types (short & long acting):
● Anticholinergics (inhaled) ● Beta-2 agonists (inhaled) ● Methylxanthines (po)
42

Bronchodilators Short Acting Beta2 Agonist (SABA)
➢e.g. Salbutamol ➢Improve pulmonary function/SOB/exercise
performance ➢Combination SABA’s and anticholinergics
produce better bronchodilation ➢For patients with MILD symptoms
● SOB on exertion
43

Bronchodilators Long Acting Beta2 Agonist (LABA)
➢e.g.– Formoterol, Salmeterol ➢For patients who still have symptoms
on SABA’s (MODERATE disease) ➢More sustained effect on PFT’s, chronic
SOB ➢Early evidence these may prolong time
between exacerbations
44

Inhaled anticholinergicsinhaled ipratropium bromide is preferred over beta-2 agonists by many as the bronchodilator of choice in COPD for the following reasons: ➢Its minimal cardiac stimulatory effects compared to those of beta agonists ➢Its greater effectiveness than either beta agonist or methylxanthine bronchodilators in most studies of patients with COPD
45

46

SteroidsInhaled steroid ➢Not recommended as first line therapy ➢No consistent effect on decreasing inflammation ➢Consider inhaled form in those with mod-severe
disease ➢Consider in those who have maximal
bronchodilator therapy ➢ Inhaled corticosteroids are currently
recommended in severe disease( FEV1 <50%) who report two or more exacerbations requiring antibiotics or oral steroids per year . 47

48

49
Additional measures ➢Vaccines. Patients with COPD should receive a single
dose of the polyvalent pneumococcal polysaccharide vaccine and yearly influenza vaccinations.
➢ a1-Antitrypsin replacement. Weekly or monthly Infusions of a1-antitrypsin have been recommended for
patients with serum levels below 310mg/L and abnormal lung function. 1
➢ Heart failure should be treated with diuretics . ➢ Secondary polycythemia requires venesection if the
PCV is >55%.
50

SURGERY➢Bullectomy : young with emphysema ➢Lung Volume reduction surgery (LVRS):
emphysema ➢Lung transplant Have been used for severe COPD
51

52
Emergency treatmentEmergency treatment
Exacerbations of COPD are characterized by an acute worsening of symptoms, with increased breathlessness, sputum volume and sputum purulence. They may occur spontaneously or as a result of infections. Mild exacerbations can be managed at home but patients with severe exacerbations require admission to hospital. key adverse features that indicate a severe exacerbation : (confusion, cyanosis, severe respiratory distress).

53
Patients admitted to hospital should have • Chest X-ray, • Arterial blood gas measurement, • ECG (to exclude comorbidities), • Full blood count and • Urea and electrolyte measurements. • Culture of sputum • Blood cultures should be taken if the patient is
pyrexial and • Theophylline level should be measured in patients
on theophylline therapy.

54
Bronchodilator therapy is usually given by nebulizer, using a combination of salbutamol 2.5 – 5.0 mg and ipratropium 500 mcg

ORAL STEROIDSORAL STEROIDS are useful during exacerbations
(rule of 15) PREDINSOLON 15 mg TWICE DAILY GIVEN FOR 15
DAYS MAY BENEFIT 15% OF PATIENTS WITH COPD EXACERBATION
55
56
Antibiotics
Common bacteria associated with COPD exacerbation include Haemophilus inluenzae, Streptococcus pneumoniae and Moraxella catarrhalis. Treatment Augmentin(amoxicillin and clavulanic acid), or doxycycline, or ciprofloxacin or clarithromycin.

57
Emergency oxygen
treatment should be commenced using controlled oxygen (e.g. 28% Venturi mask in pre-hospital care or 24% Venturi mask in hospital settings), with an initial target saturation of 88–92% pending urgent blood gas assessment to determine the patient’s ventilatory status (pH and PCO2)

58
Ventilatory support
if the pH is below the normal range (<7.35) then noninvasive ventilation (NIV) should be employed

BRONCHIECTASISA destructive lung disease characterized by:
● Abnormal & permanent dilatation of medium sized bronchi
● An associated, persistent and variable inflammatory process producing damage to bronchial elastic and muscular elements
59
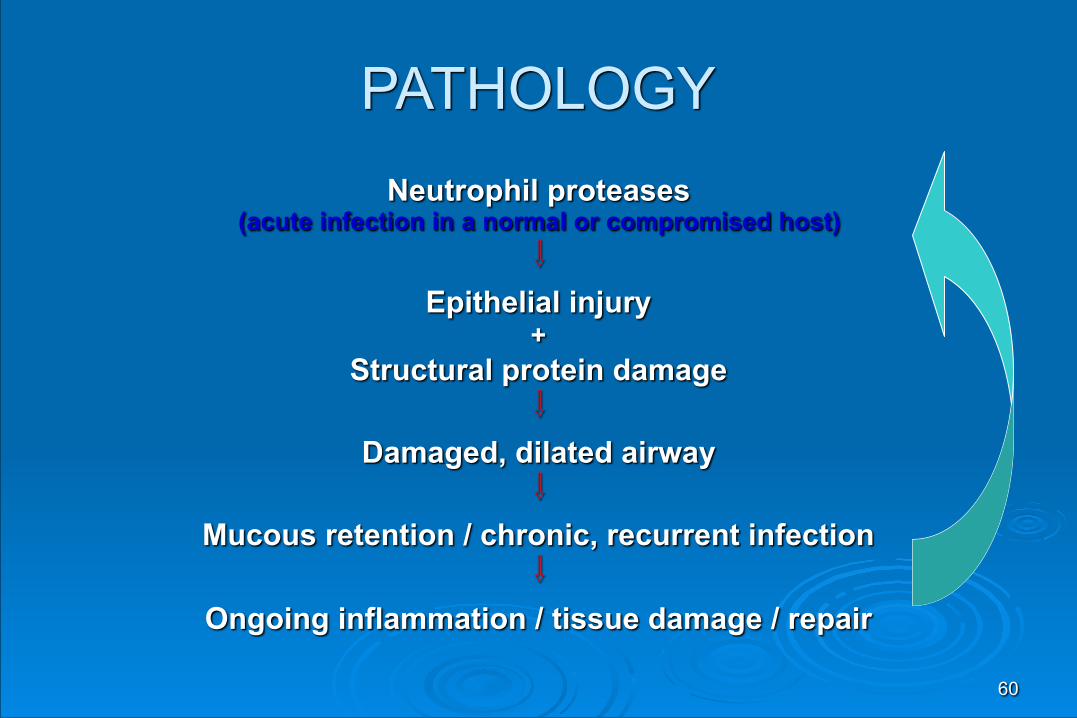
PATHOLOGYNeutrophil proteases
(acute infection in a normal or compromised host) ⇩
Epithelial injury +
Structural protein damage ⇩
Damaged, dilated airway ⇩
Mucous retention / chronic, recurrent infection ⇩
Ongoing inflammation / tissue damage / repair
60
61

62
63
Physical signs➢1-normal chest exam. If bronchiectatic airways
do not contain secretions and there is no associated lobar collapse .
➢2-coarse crackles if there is secretions . ➢3- deviated trachea toward side of lesion ,
dullness ,↓breath sound if there is collapse . ➢4- bronchial breathing : advanced scarring .
64

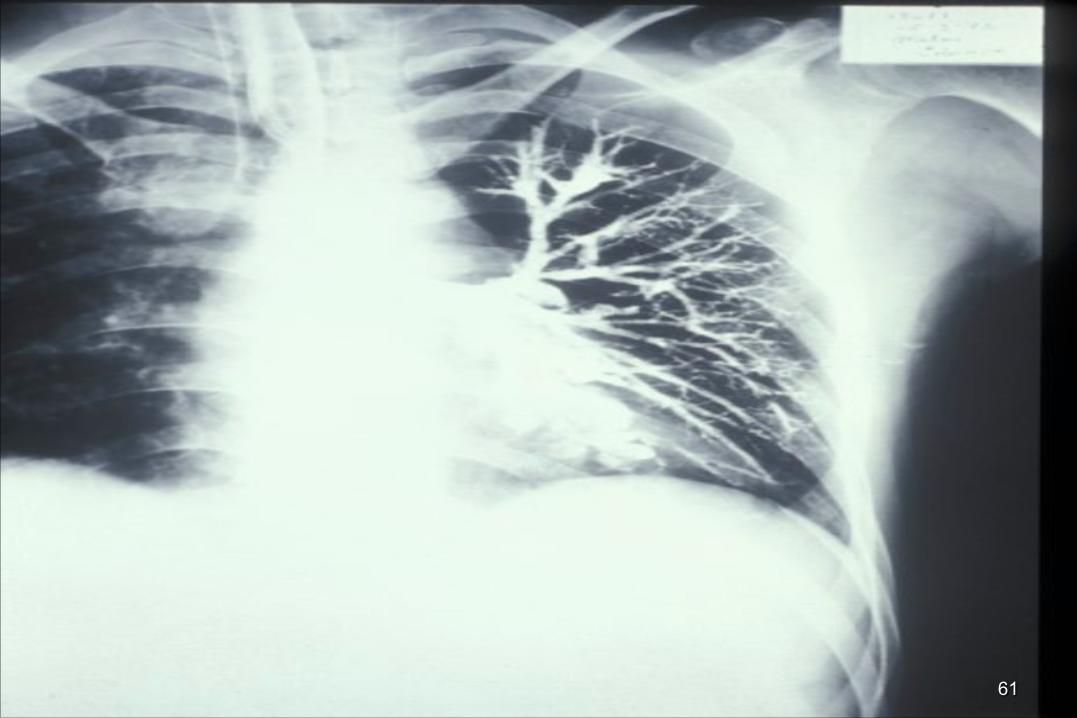
INVESTIGATIONS1-Sputum culture For pseudomonas aeruginosa , fungi , and
mycobacteria . 2- Radiology CXR : early stage normal Advanced thickened airway walls , cystic
spaces , pneumonic consolidation or collapse . SPIRAL CT SCAN of chest is much more
sensitive . 3-Assessment of ciliary function
65

management➢1-airway obstruction : inhaled bronchodilators and
corticosteroids . ➢2- physiotherapy Patients should adopt a position in which the lobe to
be drained is uppermost. Deep breathing followed by forced expiratory
maneuvers (the 'active cycle of breathing' technique) is of help in allowing secretions in the dilated bronchi to gravitate towards the trachea, from which they can be cleared by vigorous coughing.
66

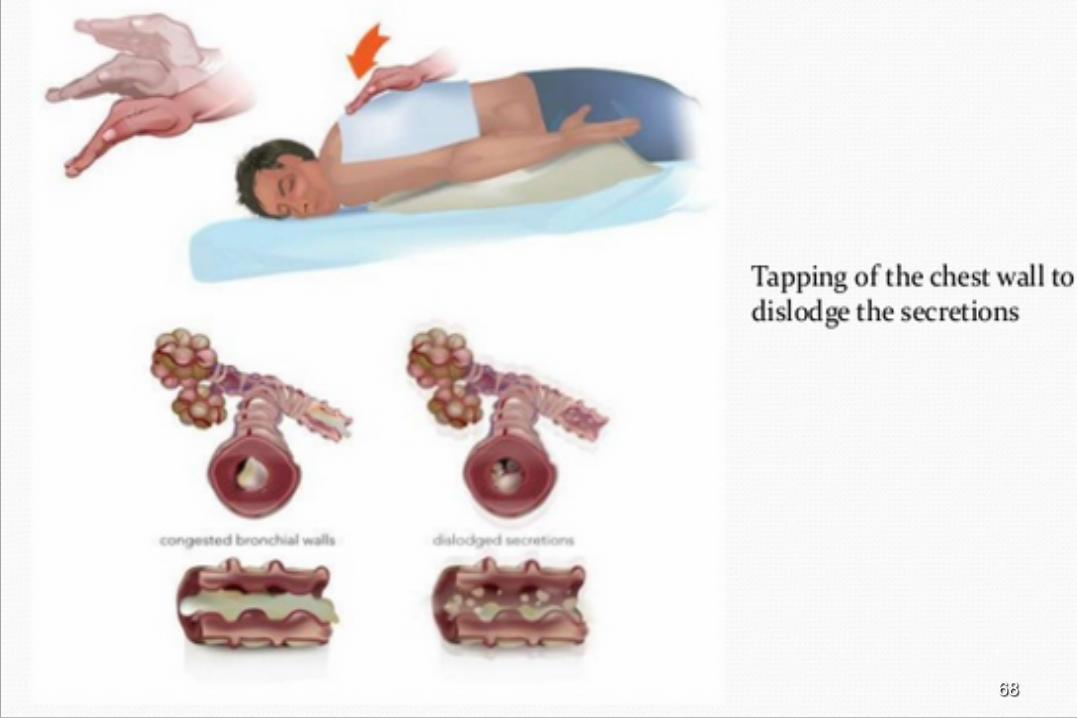
'Percussion' of the chest wall with cupped hands may help to dislodge sputum, and a number of mechanical devices are available which cause the chest wall to oscillate, thus achieving the same effect.
The optimum duration and frequency of physiotherapy depends on the amount of sputum but 5-10 minutes once or twice daily is a minimum for most patients.
67
68

3- antibiotics Oral ciprofloxacin 500-750 mg bid Or ceftazidime by IV inj. Or infusion 1-2 gm 8-
hourly. 4- surgery Only in unilateral , single lobe in young patient
69

THANK YOU70