laboratory investigation guidelines for chronic kidney ... guideline.pdf · chemical pathology...
TRANSCRIPT

Chemical Pathology DisciplineNational Pathology ServicesMinistry of Health Malaysia
Laboratory InvestIgatIon guIdeLInesFor
CHronIC KIdney dIsease and utILIsatIon oF egFr In aduLts
MiNiStry of HealtH MalaySia
OCTOBER 2012
JD005805_KULIT INVESTIGATOR ndd.indd 1 10/30/12 1:59:29 PM

Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. i
CONTENTS
FOREWORD
1. National Head of Pathology Services ............................................................ 3
2. National Head of Chemical Pathology Service .............................................. 4
THE ARTICLE
1. Introduction ................................................................................................. 7-8
2. Aim of the guidelines ...................................................................................... 9
3. Guidelines for Requesting and Reporting of eGFR ................................ 10-11
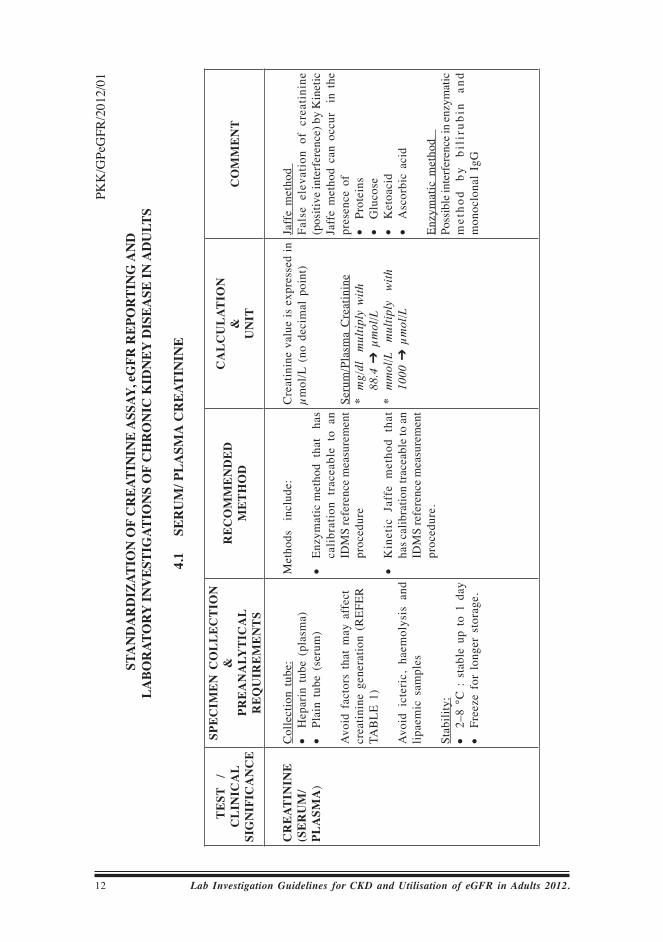
4. Standardization of Creatinine Assay, eGFR Reporting and Laboratory
Investigations of Chronic Kidney Disease (CKD) In Adults
4.1 Serum/plasma Creatinine ...................................................................... 12
4.2 Urine Albumin Creatinine Ratio (UACR) ............................................ 13
4.3 Urine Protein Creatinine Ratio (UPCR) ............................................... 14
4.4 24-Hr Urine Protein .............................................................................. 15
4.5 Creatinine Clearance (CrCl) ............................................................ 16-17
4.6 Estimated Glomerular Filtration Rate (eGFR) by Modification of Diet in Renal Disease(MDRD) ............................. 18
APPENDIX
I. Garis Panduan Permohonan dan Laporan eGFR .................................. 21-22
II. eGFR Reporting Format .......................................................................... 23
III. Table 1 : Factor That May Affect Creatinine Generation ........................ 24
IV. Table 2 : Diagnosis of Abnormal Protein or Albumin Excretion ............. 25
V. Table 3 : Staging of Chronic Kidney Disease .......................................... 26
WORKING GROUP FOR THE STANDARDISATION OF eGFR IN CKD(ADULTS) ................................................................................................... 27
REFERENCES ................................................................................................... 28
ACKNOWLEDGEMENT ..................................................................................... 29
JD005805 Kand.indd 1 10/30/12 1:49:55 PM

JD005805 Kand.indd 2 10/30/12 1:49:56 PM

FOREWORD
Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 1
FOREWORD
JD005805 Teks 1.indd 1 10/30/12 1:50:43 PM

FOREWORD
2 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
JD005805 Teks 1.indd 2 10/30/12 1:50:43 PM

FOREWORD
Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 3
The Clinical Practice Guideline (CPG) for the Chronic Kidney Disease (CKD) that was recently launched has clearly indicated the needs to standardize the formula to be adopted for eGFR (estimated Glomerular Filtration Rate) as well as to standardize reporting for eGFR (eGFR reporting format) for the whole country. The Pathology service had established a Working Group for The Standardization of eGFR in CKD for Adults from the Chemical Pathology technical group to achieve this.
Hopefully, the standardization and guidelines that has been developed will benefit the patients.
Dr.Shahnaz MuradNational Head of Pathology ServicesMinistry of Health, Malaysia.
JD005805 Teks 1.indd 3 10/30/12 1:50:44 PM

FOREWORD
4 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
The prevalence of chronic kidney disease (CKD) and end-stage renal disease (ESRD) is increasing worldwide. In Malaysia, the incidence and prevalence of patients with ESRD on dialysis had increased. As a consequence, the growing number of ESRD places an enormous human, economic and social burden on the healthcare system.
Early kidney disease is largely asymptomatic and patients often present late with complications of CKD. As such, targeted screening and early intervention will be necessary to reduce the burden of the disease. Primary care providers play a key role in the early identification, treatment and improving the outcome of patients with CKD. Awareness of CKD among primary care providers should be increased and they should be equipped to detect and to treat these patients, including referral to nephrologists for further management.
In the current Clinical Practice Guidelines (CPG) by the Ministry of Health (MOH), laboratory tests for detection and staging of CKD include estimated Glomerular Filtration Rate (eGFR) based on the Modification Diet of Renal Disease (MDRD) equation. Serum creatinine should be used in combination with eGFR in the assessment of renal function.
It is my hope that this guideline: “Laboratory Investigation Guidelines for Chronic Kidney Disease and Utilisation Of eGFR in Adults” will be used by MOH Pathology laboratory as a platform to help laboratorians to implement and use a standardised formula to calculate and, thus to report eGFR.
Hopefully, the reporting of eGFR by the MOH Pathology Service will further improve the detection and staging of CKD in Malaysia.
Dr. Muhammad Arif Mohd. HashimNational Head of Chemical Pathology and Head of Pathology DepartmentHospital Kuala Lumpur
JD005805 Teks 1.indd 4 10/30/12 1:50:44 PM

FOREWORD
Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 5
THE ARTICLES
JD005805 Teks 1.indd 5 10/30/12 1:50:44 PM

FOREWORD
6 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
JD005805 Teks 1.indd 6 10/30/12 1:50:44 PM

INTRODUCTION
Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 7
Chronic kidney disease (CKD) is an irreversible loss of renal function for at least three months and poses a major public health problem. The prevalence of CKD and end-stage renal disease (ESRD) is increasing worldwide. The estimated prevalence of CKD in the US was 16.8% while in Asia the prevalence ranged from 12.1% to 17.5%. In Malaysia, the incidence and prevalence of patients with ESRD on dialysis had increased from 88 and 325 per million population (pmp) respectively in 2001 to 170 and 762 pmp respectively in 2009. The increase in ESRD was largely driven by the increasing incidence of diabetic kidney disease (DKD) accounting for 58% of new patients accepted for dialysis. As a consequence, the growing number of ESRD places an enormous human, economic and social burden on the healthcare system.
Early kidney disease is largely asymptomatic and patients often present late with complications of CKD. As such, targeted screening and early intervention will be necessary to reduce the burden of the disease. Primary care providers play a key role in the early identification, treatment and improving the outcome of patients with CKD. Awareness of CKD among primary care providers should be increased and they should be equipped to detect and to treat these patients, including referral to nephrologists for further management.
The Clinical Practice Guidelines (CPG) was recently launched by the Ministry of Health (MOH) with the objectives to provide recommendations on the following:
a) Prevention and reduction in risk of developing chronic kidney disease (CKD)
b) Screening and early detection of CKDc) Treatment of early CKD to prevent its progression to end-stage renal
diseased) Reduction in risk of cardiovascular disease
Patients with early stage of CKD are generally asymptomatic. Many of such cases remain undiagnosed and later progress to ESRD. To reduce the prevalence of ESRD, effective screening and treatment methods for CKD should be established. Early detection and intervention of high risk groups may prevent the development and progression of CKD. For instance, patients with diabetes mellitus and/or hypertension should be screened at least yearly for chronic kidney disease (CKD). Screening can also be considered for high risk patients with:
a) Age >65 years oldb) Family history of stage 5 CKD or hereditary kidney diseasec) Structural renal tract disease, renal calculi or prostatic hypertrophyd) Opportunistic (incidental) detection of haematuria or proteinuriae) Chronic use of non-steroidal anti-inflammatory drugs (NSAIDs) or
other nephrotoxic drugsf) Cardiovascular disease (CVD)
JD005805 Teks 1.indd 7 10/30/12 1:50:44 PM

INTRODUCTION
8 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
g) Multisystem diseases with potential kidney involvement such as systemic lupus erythematosus.
In the current CPG, laboratory tests for detection and staging of CKD include estimated Glomerular Filtration Rate (eGFR) based on the Modification Diet of Renal Disease (MDRD) equation. Serum creatinine should be used in combination with eGFR in the assessment of renal function.
For many years, serum creatinine has been routinely used in clinical practice to estimate renal function. However, it is affected by many other variables (such as age, gender, ethnicity, muscle mass and protein meal) and should not be used as an independent marker of kidney function. Furthermore, serum creatinine is not a sensitive marker of early CKD as it will rise only after a reduction of renal function by at least 50%.
Due to this limitation, other formula to estimate renal function was developed including the MDRD equation. The MDRD equation has been shown to be better than Cockcroft-Gault equation in estimating renal function. However, these equations are still dependent on serum creatinine level and thus may over-estimate (such as in amputees) or under-estimate (such as in bodybuilders) renal function when muscle mass is abnormal.
With the launching of the CPG, National Pathology Service will implement the eGFR reporting from the clinician request using the standardized request form. Hopefully, the request and reporting of eGFR will improve the detection and staging of CKD and will help with the management of the patients.
In conclusion, through the link with laboratories, the public health issues of CKD detection and management will be implemented in a uniform manner. Renal experts (such as nephrologists and pathologists) will provide the interpretive expertise to allow optimal use of the laboratory results by the users of the laboratory services. The collaborative approach can provide a template for future activities where consensus approaches driven by informed experts are preferable to patchwork local implementations at the laboratory or laboratory network level. The consistent approach optimizes the use of pathology reporting services to disseminate pathology-related health interventions as widely as possible such as this eGFR reporting.
JD005805 Teks 1.indd 8 10/30/12 1:50:44 PM

Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 9
AIM OF THE GUIDELINES
The aims of these guidelines are to provide:
Guideline for request of eGFR1.
Guideline for collection of specimen for tests to support CKD2.
Recommended method and method interferences3.
Guideline for calculation and unit to be adopted for tests that support 4. CKD
Guideline for reporting of eGFR (format).5.
JD005805 Teks 1.indd 9 10/30/12 1:50:44 PM

GUIDELINES FOR REqUESTING AND REPORTING OF eGFR
10 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
1. Request form 1.1. All manual request shall use PER. PAT 301 form 1.2. Information needed • Relevant clinical history • Previous creatinine result, if available • Previous Creatinine Clearance, if available • Previous calculated eGFR result, if available
2. Only serum or plasma creatinine sample sent along with PER. PAT 301 form shall have its eGFR calculated.
3. Calculation of eGFR using previous creatinine result shall not be allowed. This is because previous eGFR result could lead to misinterpretation of the test result correlating to the current patient status.
4. Manual calculation of eGFR 4.1. eGFR can be calculated using CKD and eGFR Laboratory Tools (CELT)
software. 4.2. Transcription check shall be done.
5. Automatic calculation of eGFR via LIS 5.1. Use the adopted eGFR formula and reporting format. The formula and
reporting format should be verified by the Chemical Pathologist or designated officer prior to first time usage.
6. eGFR reporting format 6.1 The MDRD eGFR Formula is calculated in ml/min/1.73m2
175 x (Scr/88.4)-1.154 x (Age)-0.203 x (0.742 if female)
• The equation does not require weight measurement because the results are reported normalized to 1.73 m2 body surface area, which is an accepted average adult surface area.
• This equation is not applicable for African Black.
6.2 Disclaimer below shall be included in the eGFR report
LIMITATIONS OF THE MDRD eGFR The MDRD equation should not be used in some populations where it
has not been specifically validated, including: • Paediatric patients (<18 years) • Elderly patients (>70 years) • Dialysed patients • Pregnant mothers
JD005805 Teks 1.indd 10 10/30/12 1:50:44 PM

Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 11
GUIDELINES FOR REqUESTING AND REPORTING OF eGFR
• Extremes of body habi tus ie malnutr i t ion, paraplegia, quadriplegia
• Patients with skeletal muscle disorders • Vegetarians • Patients with very rapidly changing kidney function • Patients on renally excreted drugs that have significant toxicity • Severe dehydration • Patients on medications that might interfere with the creatinine
measurement • Not suitable for drugs dosing • Incomplete essential information (age, gender, race)
JD005805 Teks 1.indd 11 10/30/12 1:50:44 PM
STA
ND
AR
DIZ
ATIO
N O
F C
REA
TIN
INE
ASS
AY, e
GFR
REP
OR
TIN
G A
ND
LA
BOR
ATO
RY
INV
ESTI
GAT
ION
S O
F C
HR
ON
IC K
IDN
EY D
ISEA
SE IN
AD
ULT
S
4.1
S
ERU
M/ P
LASM
A C
REA
TIN
INE
TE
ST
/C
LIN
ICA
L SI
GN
IFIC
AN
CE
SPE
CIM
EN
CO
LL
EC
TIO
N&
PRE
AN
ALY
TIC
AL
RE
QU
IRE
ME
NT
S
RE
CO
MM
EN
DE
D
ME
TH
OD
CA
LC
UL
ATIO
N&
U
NIT
CO
MM
EN
T
CR
EAT
ININ
E (S
ER
UM
/PL
ASM
A)
Col
lect
ion
tube
:H
epar
in t
ube
(pla
sma)
•Pl
ain
tube
(se
rum
)• A
void
fac
tors
tha
t m
ay a
ffec
t cr
eatin
ine
gene
ratio
n (R
EFER
TA
BLE
1)
Avo
id i
cter
ic,
haem
olys
is a
nd
lipae
mic
sam
ples
Stab
ility
:2–
8 °C
: s
tabl
e up
to
1 da
y•
Free
ze f
or l
onge
r st
orag
e.
•
Met
hods
in
clud
e:
Enzy
mat
ic m
etho
d th
at
has
•ca
libra
tion
trac
eabl
e to
an
IDM
S re
fere
nce
mea
sure
men
t pr
oced
ure
Kin
etic
Jaf
fe m
etho
d th
at
•ha
s cal
ibra
tion
trace
able
to a
n ID
MS
refe
renc
e m
easu
rem
ent
proc
edur
e.
Cre
atin
ine
valu
e is
exp
ress
ed in
µm
ol/L
(no
dec
imal
poi
nt)
Seru
m/P
lasm
a C
reat
inin
e*
mg/
dl
mul
tipl
y w
ith
88.4
➔ µ
mol
/L*
mm
ol/L
m
ulti
ply
wit
h 10
00 ➔
µm
ol/L
Jaff
e m
etho
d Fa
lse
elev
atio
n of
cre
atin
ine
(pos
itive
inte
rfer
ence
) by
Kin
etic
Ja
ffe
met
hod
can
occu
r i
n th
e pr
esen
ce o
f Pr
otei
ns
•G
luco
se
•K
etoa
cid
•A
scor
bic
acid
• Enzy
mat
ic m
etho
d
Poss
ible
inte
rfer
ence
in en
zym
atic
m
etho
d by
bi
liru
bin
and
mon
oclo
nal
IgG
12 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
PKK
/GPe
GFR
/201
2/01
JD005805 Teks 1.indd 12 10/30/12 1:50:45 PM

Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 13
PKK
/GPe
GFR
/201
2/01
STA
ND
AR
DIZ
ATIO
N O
F C
REA
TIN
INE
ASS
AY, e
GFR
REP
OR
TIN
G A
ND
LA
BOR
ATO
RY
INV
ESTI
GAT
ION
S O
F C
HR
ON
IC K
IDN
EY D
ISEA
SE IN
AD
ULT
S
4.2
U
RIN
E A
LBU
MIN
CR
EATI
NIN
E R
ATIO
(UA
CR
)
TE
ST/
CL
INIC
AL
SIG
NIF
ICA
NC
E
SPE
CIM
EN
CO
LL
EC
TIO
N&
PRE
AN
ALY
TIC
AL
RE
QU
IRE
ME
NT
ME
TH
OD
CA
LC
UL
ATIO
N&
U
NIT
CO
MM
EN
T
UR
INE
AL
BU
MIN
C
RE
ATIN
INE
RAT
IO (
UA
CR
)
Use
ful
to
•di
agno
se
(ear
ly d
iabe
tic
neph
ropa
thy)
an
d m
onito
r ki
dney
da
mag
e
Pred
icts
•
clin
ical
end
po
ints
(C
KD
, ca
rdio
vasc
ular
di
seas
e, a
nd
mor
talit
y)
Cor
rela
tes w
ith 2
4-ho
ur a
lbum
in
excr
etio
n
Firs
t m
orni
ng u
rine
spe
cim
en
is p
refe
rred
A r
ando
m u
rine
spe
cim
en i
s ac
cept
able
if a
first
-mor
ning
urin
e sp
ecim
en i
s no
t av
aila
ble.
Stab
ility
of
urin
e al
bum
in:
2–8
°C :
sta
ble
up t
o •
1 m
onth
Froz
en a
t -2
0°C
: s
tabl
e up
•
to 6
mon
ths
Froz
en a
t -7
0°C
:
stab
le
•up
to
1 ye
ar
Pref
erab
ly a
naly
se o
n fr
esh
sam
ple
Stab
ility
of
urin
e cr
eatin
ine:
2–8
°C :
sta
ble
up t
o 4
days
•Fr
eeze
for
lon
ger
stor
age
• Pref
erab
ly a
naly
se o
n fr
esh
sam
ple
Urin
e A
lbum
inIm
mun
oass
ay m
etho
ds in
clud
e :
Turb
idim
etric
•N
ephe
lom
etric
• Cur
rent
ly, t
here
is
no r
efer
ence
m
easu
rem
ent
proc
edur
e or
sta
ndar
dize
d re
fere
nce m
ater
ial f
or
urin
e al
bum
in. M
ost c
omm
only
, ur
inar
y al
bum
in a
ssay
s ar
e st
anda
rdiz
ed a
gain
st se
rum
bas
ed
calib
rant
(C
RM
470)
.
Urin
e C
reat
inin
eM
etho
ds i
nclu
de:
Enzy
mat
ic m
etho
d
•K
inet
ic J
affe
met
hod
• Due
to la
ck o
f cer
tifie
d se
cond
ary
refe
renc
e m
ater
ial
for
urin
e cr
eatin
ine,
cal
ibra
tion
of ro
utin
e m
etho
ds o
f ur
ine
mea
sure
men
t is
ofte
n pe
rfor
med
with
ser
um
base
d re
fere
nce
mat
eria
l.
Urin
e A
lbum
in C
reat
inin
e R
atio
(U
AC
R)
is e
xpre
ssed
in
mg/
mm
ol
(1 d
ecim
al p
oint
)
To c
alcu
late
, fo
llow
the
se s
teps
:M
easu
re u
rine
albu
min
in
mg
/L1.
M
easu
re
2.
urin
e C
reat
inin
e in
m
mol
/LC
alcu
late
UA
CR
3.
U
rine
Alb
umin
(m
g/L)
=
----
----
----
----
----
----
----
U
rine
Cre
atin
ine
(mm
ol/L
)
= _
_mg/
mm
ol (
1 de
cim
al p
oint
)
Urin
e A
lbum
in*
g/L
mul
tipl
y w
ith
1000
➔ m
g/L
* µg
/ml
is e
qual
to
mg/
L
Urin
e C
reat
inin
e *
mg/
dl m
ultip
ly w
ith 0
.088
4 ➔
mm
ol/L
* µm
ol/L
div
ide
by 1
000 ➔
mm
ol/L
Inte
rpre
tati
on
of
Uri
ne
•A
lbum
in to
Cre
atin
ine
Rat
io
(REF
ER
TAB
LE
2)
An
elev
ated
UA
CR
shou
ld b
e •
conf
irmed
in
the
abse
nce
of
urin
ary
trac
t in
fect
ion
with
tw
o (2
) ad
ditio
nal
first
-voi
d sp
ecim
ens
colle
cted
dur
ing
the
next
3 t
o 6
mon
ths
Act
ivity
/con
ditio
n th
at m
ay
•in
crea
se u
rina
ry a
lbum
in
excr
etio
n o
ver
base
line
va
lues
Ex
erci
se
•Fe
ver
•H
aem
atur
ia•
Preg
nanc
y•
Post
ural
pro
tein
uria
•
Urin
ary
tract
inf
ectio
n•
JD005805 Teks 2.indd 13 10/30/12 2:35:33 PM

14 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
PKK
/GPe
GFR
/201
2/01
STA
ND
AR
DIZ
ATIO
N O
F C
REA
TIN
INE
ASS
AY, e
GFR
REP
OR
TIN
G A
ND
LA
BOR
ATO
RY
INV
ESTI
GAT
ION
S O
F C
HR
ON
IC K
IDN
EY D
ISEA
SE IN
AD
ULT
S
4.3
U
RIN
E PR
OTE
IN C
REA
TIN
INE
RAT
IO (U
PCR
)
TE
ST/
CL
INIC
AL
SIG
NIF
ICA
NC
E
SPE
CIM
EN
CO
LL
EC
TIO
N&
PRE
AN
ALY
TIC
AL
RE
QU
IRE
ME
NT
S
RE
CO
MM
EN
DE
D
ME
TH
OD
CA
LC
UL
ATIO
N&
U
NIT
CO
MM
EN
T
UR
INE
PRO
TE
IN
CR
EAT
ININ
E R
ATIO
(U
PCR
)
Use
ful
to
•di
agno
se
and
mon
itor
kidn
ey
dam
age
Pred
icts
•
clin
ical
end
po
ints
(C
KD
, ca
rdio
vasc
ular
di
seas
e, a
nd
mor
talit
y)
Cor
rela
te w
ith 2
4-H
r p
rote
in
excr
etio
n
Firs
t m
orni
ng u
rine
spe
cim
en
is p
refe
rred
.
A r
ando
m u
rine
spe
cim
en i
s ac
cept
able
if a
first
-mor
ning
urin
e sp
ecim
en i
s no
t av
aila
ble.
Stab
ility
of
urin
e pr
otei
n:2–
8 °C
: s
tabl
e up
to
7 da
ys•
Froz
en a
t -2
0°C
: s
tabl
e up
•
to 1
yea
r
Pref
erab
ly a
naly
se o
n f
resh
sa
mpl
e
Stab
ility
of
urin
e cr
eatin
ine:
2–8
°C :
sta
ble
up t
o 4
days
•Fr
eeze
for
lon
ger
stor
age
• Pref
erab
ly a
naly
se o
n f
resh
sa
mpl
e
Urin
e Pr
otei
nM
etho
ds
incl
ude:
Dye
bin
ding
(co
lorim
etric
) •
(e.g
. Py
roga
llol
Red
) Tu
rbid
imet
ric (
e.g.
•
Ben
zeth
oniu
m C
l)
Cur
rent
ly, t
here
is
no r
efer
ence
m
easu
rem
ent
proc
edur
e an
d no
st
anda
rdiz
ed r
efer
ence
mat
eria
l fo
r ur
inar
y to
tal
prot
ein.
Urin
e C
reat
inin
eM
etho
ds
incl
ude:
Enzy
mat
ic m
etho
d
•K
inet
ic J
affe
met
hod
• Due
to la
ck o
f cer
tifie
d se
cond
ary
refe
renc
e m
ater
ial
for
urin
e cr
eatin
ine,
cal
ibra
tion
of ro
utin
e m
etho
ds o
f ur
ine
mea
sure
men
t is
ofte
n pe
rfor
med
with
ser
um
base
d re
fere
nce
mat
eria
l.
Urin
e Pr
otei
n C
reat
inin
e R
atio
(U
PCR
) is
exp
ress
ed i
n m
g/m
mol
To c
alcu
late
, fo
llow
the
se s
teps
:M
easu
re
1.
urin
e Pr
otei
n in
mg
/LM
easu
re
2.
urin
e C
reat
inin
e in
m
mol
/LC
alcu
late
UPC
R
3.
U
rine
Prot
ein
(mg/
L)
= --
----
----
----
----
----
----
---
U
rine
Cre
atin
ine
(mm
ol/L
)=
__m
g/m
mol
(n
o de
cim
al p
oint
)
Urin
e Pr
otei
ng/
L m
ulti
ply
wit
h 10
00
•➔
mg/
L
Urin
e C
reat
inin
e m
g/dl
m
ultip
ly w
ith 0
.088
4 •
➔
mm
ol/L
µ•
mol
/L d
ivid
e by
100
0➔
mm
ol/L
Inte
rpre
tatio
n of
Urin
e •
Prot
ein
to C
reat
inin
e R
atio
(R
EFER
TA
BLE
2)
Act
ivity
/con
ditio
n th
at m
ay
•in
crea
se u
rinar
y pr
otei
n
over
bas
elin
e va
lues
Con
gest
ive
hear
t fa
ilure
•Ex
erci
se•
Feve
r•
Hae
mat
uria
•In
fect
ion
•M
arke
d hy
perg
lyca
emia
•Po
stur
al p
rote
inur
ia
•Pr
egna
ncy
•S
ev
ere
/ma
lig
na
nt
•hy
perte
nsio
nU
rinar
y tra
ct i
nfec
tion
•
JD005805 Teks 2.indd 14 10/30/12 2:35:33 PM

Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 15
PKK
/GPe
GFR
/201
2/01
STA
ND
AR
DIZ
ATIO
N O
F C
REA
TIN
INE
ASS
AY, e
GFR
REP
OR
TIN
G A
ND
LA
BOR
ATO
RY
INV
ESTI
GAT
ION
S O
F C
HR
ON
IC K
IDN
EY D
ISEA
SE IN
AD
ULT
S
4.4
24
- Hr U
RIN
E PR
OTE
IN
TEST
/C
LIN
ICA
L SI
GN
IFIC
AN
CE
SPEC
IMEN
CO
LLEC
TIO
N&
PREA
NA
LYTI
CA
L R
EQU
IREM
ENTS
REC
OM
MEN
DED
MET
HO
DC
ALC
ULA
TIO
N&
U
NIT
CO
MM
ENT
24- H
r UR
INE
PRO
TEIN
A ‘g
old
stan
dard
’ for
the
quan
tifica
tion
of
prot
einu
ria
Inst
ruct
ions
fo
r 24
-Hr
urin
e co
llect
ion
Day
1:
Inst
ruct
pat
ient
to
void
at
8 a
m a
nd d
isca
rd t
he s
ampl
e.
Col
lect
all
urin
e in
a 2
4-H
r urin
e co
ntai
ner f
or th
e ne
xt 2
4-H
rs.
Day
2:
Incl
ude
the
final
sam
ple
void
ed
at
8am
in
to
the
urin
e co
ntai
ner.
Kee
p sa
mpl
e in
the
ref
riger
ator
or
in
a co
ol p
lace
dur
ing
the
colle
ctio
n pe
riod.
Labe
l the
con
tain
er w
ith
Two
iden
tifier
s (N
ame
and
•N
RIC
/MR
N)
Dat
e an
d ti
me
coll
ecti
on
•st
arte
dD
ate
and
tim
e co
llec
tion
•
com
plet
ed
Met
hods
incl
ude
:
Dye
bin
ding
(col
orim
etric
) •
(e.g
. Pyr
ogal
lol R
ed)
Turb
idim
etric
(e.g
. •
Ben
zeth
oniu
m C
l)
Cur
rent
ly,
ther
e is
no
refe
renc
e m
easu
rem
ent
proc
edur
e an
d no
st
anda
rdiz
ed
refe
renc
e m
ater
ial
for u
rinar
y to
tal p
rote
in.
24-H
r Urin
e Pr
otei
n is
exp
ress
ed in
g/
24H
r
To c
alcu
late
, fol
low
thes
e st
eps :
Mea
sure
24-
Hr u
rine
vol
ume
in
1.
L/24
Hr
Mea
sure
the
urin
e pr
otei
n in
mg/
L2.
C
alcu
late
24
Hr U
rine
Prot
ein
3.
= U
rine V
olum
e x U
rine P
rotei
n
(L
/24
Hr)
(m
g/L)
= __
_ m
g/24
Hr
= __
__ g/
24 H
r (2 d
ecim
al Po
ints)
10
00
Urin
e Pr
otei
ng/
L m
ultip
ly w
ith 1
000
•➔
mg/
L
24-H
r ur
ine
colle
ctio
ns m
ay
•be
ass
ocia
ted
with
sig
nific
ant
colle
ctio
n er
rors
, la
rgel
y du
e to
im
prop
er t
imin
g an
d m
isse
d sa
mpl
es,
lead
ing
to
over
-col
lect
ion
and
unde
r-co
llect
ion.
Nor
mal
urin
e ou
tput
for
an
•ad
ult
is 0
.5
to 1
.0 m
l/kg/
Hr.
Und
er
colle
ctio
n of
24
H
r ur
ine
volu
me
may
giv
e fa
lsel
y lo
w
conc
entra
tion
of
urin
e pr
otei
n .
Inte
rpre
tatio
n of
24-
Hr
Urin
e •
Prot
ein
(REF
ER T
AB
LE 2
)
JD005805 Teks 2.indd 15 10/30/12 2:35:33 PM

16 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
PKK
/GPe
GFR
/201
2/01
STA
ND
AR
DIZ
ATIO
N O
F C
REA
TIN
INE
ASS
AY, e
GFR
REP
OR
TIN
G A
ND
LA
BOR
ATO
RY
INV
ESTI
GAT
ION
S O
F C
HR
ON
IC K
IDN
EY D
ISEA
SE IN
AD
ULT
S
4.5
C
REA
TIN
INE
CLE
AR
AN
CE
(CrC
l)
TE
ST/
CL
INIC
AL
SIG
NIF
ICA
NC
E
SPE
CIM
EN
CO
LL
EC
TIO
N&
PRE
AN
ALY
TIC
AL
RE
QU
IRE
ME
NT
S
RE
CO
MM
EN
DE
D
ME
TH
OD
CA
LC
UL
ATIO
N&
U
NIT
CO
MM
EN
T
CR
EAT
ININ
E C
LE
AR
AN
CE
(CrC
l)
The
crea
tinin
e cl
eara
nce
is a
w
idel
y us
ed
test
to
estim
ate
the
glom
erul
ar
filtra
tion
rate
(G
FR).
Cre
atin
ine
clea
ranc
e is
us
eful
whe
re
MD
RD
equ
atio
n ca
nnot
be
used
.
Sam
ple
need
ed:
Seru
m/p
lasm
a C
reat
inin
e •
shal
l be
tak
en w
ithin
24-
Hr
of
urin
e co
llect
ion
24-H
r U
rine
col
lect
ion
for
•C
reat
inin
e m
easu
rem
ent
Inst
ruct
ions
for
24-
Hr
urin
e co
llect
ion
Patie
nt P
repa
ratio
n:
Avo
id
taki
ng
inte
rfer
ing
med
icat
ions
(REF
ER T
AB
LE 1
). If
pos
sibl
e, d
rugs
sho
uld
be
stop
ped
befo
reha
nd.
Ens
ure
patie
nt d
rink
suf
fici
ent
wat
er
befo
re st
art c
olle
ctin
g and
cont
inue
go
od h
ydra
tion
thro
ugho
ut t
he
proc
edur
e. A
mea
t fr
ee d
iet
is
reco
mm
ende
d
Seru
m c
reat
inin
eM
etho
ds
incl
ude:
Enzy
mat
ic m
etho
d th
at
has
•ca
libra
tion
trac
eabl
e to
an
IDM
S re
fere
nce
mea
sure
men
t pr
oced
ure
Kin
etic
Jaf
fe m
etho
d th
at
•ha
s cal
ibra
tion
trace
able
to a
n ID
MS
refe
renc
e m
easu
rem
ent
proc
edur
e
Urin
e C
reat
inin
eM
etho
ds
incl
ude:
Enzy
mat
ic m
etho
d
•K
inet
ic J
affe
met
hod
•
Cre
atin
ine
clea
ranc
e is
exp
ress
ed i
n m
l/min
To c
alcu
late
, fo
llow
the
se s
teps
:M
easu
re 2
4-H
r ur
ine
volu
me
in
1. L/
24H
rM
easu
re
urin
e cr
eatin
ine
in
2. m
mol
/LM
easu
re
seru
m c
reat
inin
e in
3.
µmol
/LC
alcu
late
cre
atin
ine
clea
ranc
e in
4.
ml/m
in
Urin
e C
reat
inin
e x
24-h
r U
rine
Volu
me
(m
mol
/L)
(L/2
4Hr)
=
----
----
----
----
----
----
----
----
----
Se
rum
Cre
atin
ine
(µm
ol/L
)
= __
x 1,
000,
000
ml/m
in (n
o de
cimal
poin
t)
14
40
24-H
r ur
ine
coll
ecti
ons
may
be
ass
ocia
ted
with
sig
nifi
cant
co
llec
tion
er
rors
, la
rgel
y du
e to
im
prop
er t
imin
g an
d m
isse
d sa
mpl
es,
lead
ing
to
over
-col
lect
ions
and
und
er-
colle
ctio
ns.
JD005805 Teks 2.indd 16 10/30/12 2:35:33 PM

Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 17
PKK
/GPe
GFR
/201
2/01
TE
ST/
CL
INIC
AL
SIG
NIF
ICA
NC
E
SPE
CIM
EN
CO
LL
EC
TIO
N&
PRE
AN
ALY
TIC
AL
RE
QU
IRE
ME
NT
S
RE
CO
MM
EN
DE
D
ME
TH
OD
CA
LC
UL
ATIO
N&
U
NIT
CO
MM
EN
T
Day
1:
Inst
ruct
the
pat
ient
to
void
at
8 am
and
dis
card
the
sa
mpl
e. C
olle
ct a
ll ur
ine
in a
24
-Hr
urin
e co
ntai
ner
for
the
next
24-
Hrs
.
Day
2: I
nclu
de th
e fin
al s
ampl
e vo
ided
at
8am
int
o th
e ur
ine
cont
aine
r.
Kee
p sa
mpl
e in
the
refr
iger
ator
or
in
a co
ol p
lace
dur
ing
the
colle
ctio
n pe
riod.
Labe
l th
e co
ntai
ner
with
Two
iden
tifie
rs (
Nam
e an
d •
NR
IC/M
RN
)D
ate
and
tim
e co
llec
tion
•
star
ted
Dat
e an
d ti
me
coll
ecti
on
•co
mpl
eted
Due
to la
ck o
f cer
tifie
d se
cond
ary
refe
renc
e m
ater
ial
for
urin
e cr
eatin
ine,
cal
ibra
tion
of ro
utin
e m
etho
ds o
f ur
ine
mea
sure
men
t is
ofte
n pe
rfor
med
with
ser
um
base
d re
fere
nce
mat
eria
l.
Or
To c
alcu
late
, fo
llow
the
se s
teps
:M
easu
re 2
4-H
r ur
ine
volu
me
in
1. m
l/24H
rM
easu
re
urin
e cr
eati
nine
in
2. µm
ol/L
Mea
sure
se
rum
cre
atin
ine
in
3. µm
ol/L
Cal
cula
te th
e cr
eatin
ine
clea
ranc
e 4.
in m
l/min
Urin
e C
reat
inin
e x
24-h
r U
rineV
olum
e
(µm
ol/L
) (m
l/24H
r)=
---
----
----
----
----
----
----
----
----
-
Ser
um C
reat
inin
e (
µmol
/L)
= __
____
__ m
l
14
00 m
in
= __
____
__m
l/min
(no
dec
imal
poi
nt)
JD005805 Teks 2.indd 17 10/30/12 3:08:45 PM

18 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
PKK
/GPe
GFR
/201
2/01
STA
ND
AR
DIZ
ATIO
N O
F C
REA
TIN
INE
ASS
AY, e
GFR
REP
OR
TIN
G A
ND
LA
BOR
ATO
RY
INV
ESTI
GAT
ION
S O
F C
HR
ON
IC K
IDN
EY D
ISEA
SE IN
AD
ULT
S4.
6
ESTI
MAT
ED G
LOM
ERU
LAR
FIL
TRAT
ION
RAT
E (e
GFR
) by
M
OD
IFIC
ATIO
N O
F D
IET
IN R
ENA
L D
ISEA
SE (M
DR
D)
TE
ST/
CL
INIC
AL
SIG
NIF
ICA
NC
E
SPE
CIM
EN
CO
LL
EC
TIO
N&
PRE
AN
ALY
TIC
AL
RE
QU
IRE
ME
NT
S
RE
CO
MM
EN
DE
D
ME
TH
OD
CA
LC
UL
ATIO
N&
U
NIT
CO
MM
EN
T
EST
IMAT
ED
G
LO
ME
RU
LA
R
FILT
RAT
ION
R
ATE
(eG
FR)
by MO
DIF
ICAT
ION
O
F D
IET
IN
RE
NA
LD
ISE
ASE
(M
DR
D)
Sam
ple
need
ed:
Seru
m/p
lasm
a C
reat
inin
e • R
equi
rem
ent b
efor
e ap
plic
atio
n o
f M
DR
D e
quat
ion
Plea
se e
nsur
e th
e re
quir
emen
ts
belo
w a
re f
ulfil
led
Met
hod
for
seru
m/p
lasm
a •
crea
tinin
e m
easu
rem
ent
mus
t be
trac
eabl
e to
IDM
S re
fere
nce
mea
sure
men
t pr
oced
ure.
Uni
t m
easu
rem
ent
of
seru
m/
•pl
asm
a cr
eati
nine
is
in
µm
ol/L
Seru
m/P
lasm
a C
reat
inin
e*
mg/
dl m
ultip
ly w
ith 8
8.4 ➔
µm
ol/L
Met
hods
for
ser
um/p
lasm
a cr
eatin
ine
in
clud
e:
Enzy
mat
ic m
etho
d t
hat
•ha
s ca
libra
tion
trac
eabl
e to
an
IDM
S re
fere
nce
mea
sure
men
t pr
oced
ure
Kin
etic
Jaf
fe m
etho
d th
at
•ha
s ca
libra
tion
trac
eabl
e to
an
IDM
S re
fere
nce
mea
sure
men
t pr
oced
ure.
MD
RD
eG
FR v
alue
is
expr
esse
d in
m
l/min
/1.7
3m2
(no
deci
mal
poi
nt)
To c
alcu
late
, fo
llow
the
se s
teps
:
Mea
sure
se
rum
cr
eatin
ine
in
1. µm
ol/L
Age
is
expr
esse
d in
yea
rs.
2. C
alcu
late
MD
RD
eG
FR i
n 3.
ml/m
in/1
.73m
2
= 17
5 x
(Scr
/88.
4)-1
.154
x (
Age
)-0.2
03
x (0
.742
if
fem
ale)
(no
dec
imal
po
int)
The
equa
tion
does
not
requ
ire w
eigh
t m
easu
rem
ent
beca
use
the
resu
lts a
re
repo
rted
norm
aliz
ed to
1.7
3 m
2 bod
y su
rfac
e ar
ea,
whi
ch i
s an
acc
epte
d av
erag
e ad
ult
surf
ace
area
.
The
abov
e eq
uatio
n is
not
app
licab
le
for A
fric
an B
lack
. H
owev
er, t
he re
sult
can
be g
ener
ated
by
mul
tiply
ing
the
eGFR
res
ult
deriv
ed f
rom
the
abo
ve
equa
tion
with
1.2
12
Inte
rpre
tatio
n of
MD
RD
eG
FR
•va
lue
(R
EFER
TA
BLE
3)
LIM
ITAT
ION
S O
F TH
E M
DR
D
eGFR
The
MD
RD
equ
atio
n sh
ould
not
be
used
in s
ome
popu
latio
ns w
here
it
has n
ot b
een
spec
ifica
lly v
alid
ated
, in
clud
ing:
Paed
iatri
c pa
tient
s (<
18 y
ears
)•
Elde
rly p
atie
nts
(>70
yea
rs)
•D
ialy
sed
patie
nts
•Pr
egna
nt m
othe
rs•
Ext
rem
es
of
body
ha
bitu
s •
ie m
alnu
trit
ion,
par
aple
gia,
qu
adrip
legi
aPa
tien
ts w
ith
skel
etal
mus
cle
•di
sord
ers
Vege
taria
ns
•Pa
tien
ts
wit
h ve
ry
rapi
dly
•ch
angi
ng k
idne
y fu
nctio
n Pa
tient
s on
rena
lly e
xcre
ted
drug
s •
that
hav
e si
gnifi
cant
tox
icity
Seve
re d
ehyd
ratio
n •
Pati
ents
on
med
icat
ions
tha
t •
mig
ht in
terf
ere
with
the
crea
tinin
e m
easu
rem
ent
Not
sui
tabl
e fo
r dr
ugs
dosi
ng•
Inco
mpl
ete
esse
ntia
l inf
orm
atio
n •
(age
, ge
nder
, ra
ce)
JD005805 Teks 2.indd 18 10/30/12 2:35:33 PM

STA
ND
AR
DIZ
ATIO
N O
F C
REA
TIN
INE
ASS
AY, e
GFR
REP
OR
TIN
G A
ND
LA
BOR
ATO
RY
INV
ESTI
GAT
ION
S O
F C
HR
ON
IC K
IDN
EY D
ISEA
SE IN
AD
ULT
S4.
6
ESTI
MAT
ED G
LOM
ERU
LAR
FIL
TRAT
ION
RAT
E (e
GFR
) by
M
OD
IFIC
ATIO
N O
F D
IET
IN R
ENA
L D
ISEA
SE (M
DR
D)
TE
ST/
CL
INIC
AL
SIG
NIF
ICA
NC
E
SPE
CIM
EN
CO
LL
EC
TIO
N&
PRE
AN
ALY
TIC
AL
RE
QU
IRE
ME
NT
S
RE
CO
MM
EN
DE
D
ME
TH
OD
CA
LC
UL
ATIO
N&
U
NIT
CO
MM
EN
T
EST
IMAT
ED
G
LO
ME
RU
LA
R
FILT
RAT
ION
R
ATE
(eG
FR)
by MO
DIF
ICAT
ION
O
F D
IET
IN
RE
NA
LD
ISE
ASE
(M
DR
D)
Sam
ple
need
ed:
Seru
m/p
lasm
a C
reat
inin
e • R
equi
rem
ent b
efor
e ap
plic
atio
n o
f M
DR
D e
quat
ion
Plea
se e
nsur
e th
e re
quir
emen
ts
belo
w a
re f
ulfil
led
Met
hod
for
seru
m/p
lasm
a •
crea
tinin
e m
easu
rem
ent
mus
t be
trac
eabl
e to
IDM
S re
fere
nce
mea
sure
men
t pr
oced
ure.
Uni
t m
easu
rem
ent
of
seru
m/
•pl
asm
a cr
eati
nine
is
in
µm
ol/L
Seru
m/P
lasm
a C
reat
inin
e*
mg/
dl m
ultip
ly w
ith 8
8.4 ➔
µm
ol/L
Met
hods
for
ser
um/p
lasm
a cr
eatin
ine
in
clud
e:
Enzy
mat
ic m
etho
d t
hat
•ha
s ca
libra
tion
trac
eabl
e to
an
IDM
S re
fere
nce
mea
sure
men
t pr
oced
ure
Kin
etic
Jaf
fe m
etho
d th
at
•ha
s ca
libra
tion
trac
eabl
e to
an
IDM
S re
fere
nce
mea
sure
men
t pr
oced
ure.
MD
RD
eG
FR v
alue
is
expr
esse
d in
m
l/min
/1.7
3m2
(no
deci
mal
poi
nt)
To c
alcu
late
, fo
llow
the
se s
teps
:
Mea
sure
se
rum
cr
eatin
ine
in
1. µm
ol/L
Age
is
expr
esse
d in
yea
rs.
2. C
alcu
late
MD
RD
eG
FR i
n 3.
ml/m
in/1
.73m
2
= 17
5 x
(Scr
/88.
4)-1
.154
x (
Age
)-0.2
03
x (0
.742
if
fem
ale)
(no
dec
imal
po
int)
The
equa
tion
does
not
requ
ire w
eigh
t m
easu
rem
ent
beca
use
the
resu
lts a
re
repo
rted
norm
aliz
ed to
1.7
3 m
2 bod
y su
rfac
e ar
ea,
whi
ch i
s an
acc
epte
d av
erag
e ad
ult
surf
ace
area
.
The
abov
e eq
uatio
n is
not
app
licab
le
for A
fric
an B
lack
. H
owev
er, t
he re
sult
can
be g
ener
ated
by
mul
tiply
ing
the
eGFR
res
ult
deriv
ed f
rom
the
abo
ve
equa
tion
with
1.2
12
Inte
rpre
tatio
n of
MD
RD
eG
FR
•va
lue
(R
EFER
TA
BLE
3)
LIM
ITAT
ION
S O
F TH
E M
DR
D
eGFR
The
MD
RD
equ
atio
n sh
ould
not
be
used
in s
ome
popu
latio
ns w
here
it
has n
ot b
een
spec
ifica
lly v
alid
ated
, in
clud
ing:
Paed
iatri
c pa
tient
s (<
18 y
ears
)•
Elde
rly p
atie
nts
(>70
yea
rs)
•D
ialy
sed
patie
nts
•Pr
egna
nt m
othe
rs•
Ext
rem
es
of
body
ha
bitu
s •
ie m
alnu
trit
ion,
par
aple
gia,
qu
adrip
legi
aPa
tien
ts w
ith
skel
etal
mus
cle
•di
sord
ers
Vege
taria
ns
•Pa
tien
ts
wit
h ve
ry
rapi
dly
•ch
angi
ng k
idne
y fu
nctio
n Pa
tient
s on
rena
lly e
xcre
ted
drug
s •
that
hav
e si
gnifi
cant
tox
icity
Seve
re d
ehyd
ratio
n •
Pati
ents
on
med
icat
ions
tha
t •
mig
ht in
terf
ere
with
the
crea
tinin
e m
easu
rem
ent
Not
sui
tabl
e fo
r dr
ugs
dosi
ng•
Inco
mpl
ete
esse
ntia
l inf
orm
atio
n •
(age
, ge
nder
, ra
ce)
APPENDIX
JD005805 Teks 2.indd 19 10/30/12 2:35:33 PM

JD005805 Teks 2.indd 20 10/30/12 2:35:33 PM

Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 21
GARIS PANDUAN UNTUK MEMOHON DAN MELAPOR eGFR
1. Borang permohonan 1.1 Gunakan borang PER. PAT 301 1.2 Maklumat lain • Maklumat sejarah penyakit yang berkaitan • Keputusan ujian creatinine lampau, jika ada • Keputusan Creatinine Clearance lampau, jika ada • Pengiraan ujian eGFR lampau, jika ada
2. Keputusan serum/plasma creatinine yang sampelnya dihantar bersama-sama borang PER. PAT 301 sahaja akan dibuat pengiraan eGFR.
3. Keputusan creatinine yang lampau (previous results) tidak akan digunakan bagi pengiraan eGFR. Ini kerana keputusan ujian lampau eGFR boleh menimbulkan masalah dari segi intepretasi keputusan ujian mengikut keadaan semasa pesakit.
4. Pengiraan eGFR secara manual 4.1 eGFR boleh dikira menggunakan CKD and eGFR Laboratory Tools
(CELT) software. 4.2 Semakan transkripsi perlu dilakukan.
5. Pengiraan eGFR secara automatik 5.1 Gunakan formula eGFR yang disarankan dan format laporan yang
disediakan. Formula dan format laporan perlu disahkan oleh Pakar Patologi Kimia atau pegawai yang bertanggungjawab sebelum memulakan penggunaannya buat pertama kali.
6. Format Laporan eGFR 6.1 Formula pengiraan eGFR menggunakan MDRD eGFR dalam ml/
min/1.73m2 175 x (Scr /88.4)-1.154 x (Age)-0.203 x (0.742 if female)
The equation does not require weight measurement because the results are reported normalized to 1.73 m2 body surface area, which is an accepted average adult surface area.
This equation is not applicable for African Black.
6.2 Kenyataan di bawah (Disclaimer) akan dikeluarkan bersama laporan eGFR (eGFR report)
LIMITATIONS OF THE MDRD eGFR The MDRD equation should not be used in some populations where it
has not been specifically validated, including: • Paediatric patients (<18 years) • Elderly patients (>70 years)
APPENDIX I
JD005805 Teks 2.indd 21 10/30/12 2:35:33 PM

22 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
GARIS PANDUAN UNTUK MEMOHON DAN MELAPOR eGFR
• Dialysed patients • Pregnant mothers • Extremes of body habi tus ie malnutr i t ion, paraplegia,
quadriplegia • Patients with skeletal muscle disorders • Vegetarians • Patients with very rapidly changing kidney function • Patients on renally excreted drugs that have significant toxicity • Severe dehydration • Patients on medications that might interfere with the creatinine
measurement • Not suitable for drugs dosing • Incomplete essential information (age, gender, race)
APPENDIX I
JD005805 Teks 2.indd 22 10/30/12 2:35:33 PM

APPENDIX I eGFR REPORTING FORMAT APPENDIX II
��������������������
���
�����
�������
������������
�������������������������������������������������
NA
ME�
��
��
��
��
��
��
��
��
WA
RD
/ C
LIN
IC�
��
��
��
��
��
��
��
�
��
��
��
��
��
��
��
��
�R
/N�
��
��
��
��
��
��
��
�N
RIC
. N
O /
OT
HE
R I
D�
��
��
��
��
��
��
��
��
MR
N�
��
��
��
��
��
��
��
�D
AT
E O
F R
EQ
UE
ST�
��
��
��
��
��
DA
TE
RE
CE
IVE
D�
��
��
��
��
�N
AM
E O
F D
OC
TO
R�
��
��
��
��
��
��
��
��
BA
RC
OD
E N
O
��
��
��
��
��
��
��
��
��
��
��
��
�
eGF
R R
EP
OR
T
�C
RE
AT
ININ
E R
ES
UL
T�
��
�m
ol/
l�
eG
FR
VA
LU
E�
��
ml/
min
/1.7
3 m
�*�
CR
EA
TIN
INE
AS
SA
Y M
ET
HO
D�
Jaff
e K
ineti
c /
En
zy
mati
c�
�M
OD
IFIC
AT
ION
OF
DIE
T I
N R
EN
AL
DIS
EA
SE
(M
DR
D)
EQ
UA
TIO
N
�
17
5 x
(S
cr/
88
.4)-1
.154 x
(A
ge)-0
.203 x
(0
.74
2 if
fe
male
)
�
Th
e e
qu
ati
on
do
es
no
t re
qu
ire w
eig
ht
measu
rem
en
t b
ecau
se t
he r
esu
lts
are
rep
ort
ed
no
rmali
zed
to
1.7
3 m
2 b
od
y s
urf
ace
are
a, w
hic
h i
s an
accep
ted
av
era
ge a
du
lt s
urf
ace a
rea.
* T
his
eq
uati
on
is
no
t ap
pli
cab
le f
or
Afr
ican
B
lack
ST
AG
ES
OF
CK
D�
GF
R (
ml/
min
/1.7
3m
2)�
Desc
rip
tio
n
1�
>9
0�
No
rmal
or
incre
ase
d G
FR
, w
ith
oth
er
ev
iden
ce o
f k
idn
ey d
am
age�
2�
60
-89
Sli
gh
t d
ecre
ase
in
GF
R,
wit
h o
ther
ev
iden
ce o
f k
idn
ey
dam
ag
e�
3A�
45
-59
3B
30
-44
Mo
dera
te d
ecre
ase
in
GF
R, w
ith
or
wit
ho
ut
oth
er
ev
iden
ce o
f k
idney
dam
age�
4�
15
-29
Sev
ere
decre
ase
in
GF
R,w
ith
or
wit
ho
ut
oth
er
ev
iden
ce o
f k
idney
dam
age�
5�
<1
5�
Est
ab
lish
ed
ren
al
fail
ure�
��
�
LIM
ITA
TIO
NS
OF
TH
E M
DR
DeG
FR�
��
Th
e M
DR
D e
qu
ati
on
sh
ou
ld n
ot
be u
sed
in
so
me p
opu
lati
on
s w
here
it
has
no
t b
een
sp
ecif
icall
y v
ali
date
d, in
clu
din
g�
Paed
iatr
ic p
ati
en
ts (
<1
8 y
ears
)��
Veg
eta
rian
s�
Eld
erl
y p
ati
ents
(>
70
years
)��
Pati
en
ts w
ith
very
rap
idly
ch
ang
ing
kid
ney
fu
ncti
on�
Dia
lyse
d p
ati
en
ts�
�P
ati
en
ts o
n r
en
all
y e
xcre
ted
dru
gs
that
hav
e s
ign
ific
an
t to
xic
ity�
Pre
gn
an
t m
oth
ers�
�S
ev
ere
dehy
dra
tio
n�
Ex
trem
es
of
bo
dy
hab
itu
s ie
maln
utr
itio
n, p
arap
leg
ia, qu
ad
rip
leg
ia�
�P
ati
en
ts o
n m
ed
icati
on
s th
at
mig
ht
inte
rfer
e w
ith
th
e c
reati
nin
e m
easu
rem
ent�
Pati
en
ts w
ith
sk
ele
tal
mu
scle
dis
ord
ers�
�N
ot
suit
ab
le f
or
dru
gs
do
sing�
��
�
� CO
MM
EN
T:
R
EP
OR
TE
D B
Y:�
VA
LID
AT
ED
BY
:
DA
TE
:�
����������
�������
��������
��������������
JD005805 Teks 2.indd 23 10/30/12 2:35:34 PM

24 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
FACTORS THAT MAY AFFECT CREATININE GENERATION
TAB
LE
1:
F
AC
TOR
S T
HAT
MAY
AFF
EC
T C
RE
ATIN
INE
GE
NE
RAT
ION
Mec
hani
sms
Fact
ors
Red
uced
cre
atin
ine
gene
ratio
n-
Dec
reas
e se
rum
/ p
lasm
a cr
eatin
ine
Old
er A
ge•
Fem
ale
Sex
•M
alnu
tritio
n•
Mus
cle
was
ting
•A
mpu
tatio
n•
Incr
ease
d cr
eatin
ine
gene
ratio
n-
Incr
ease
ser
um /
pla
sma
crea
tinin
eA
fric
an B
lack
•In
crea
sed
mus
cle
mas
s•
Inge
stio
n of
coo
ked
mea
ts (
Tran
sien
t in
crea
se)
•
Dec
reas
ed
crea
tinin
e cl
eara
nce
by
inhi
bitin
g t
ubul
ar s
ecre
tion
of c
reat
inin
e
M
edic
atio
ns t
hat
may
inc
reas
e se
rum
/pla
sma
crea
tinin
e i
nclu
de:
Cep
halo
spor
in a
nd a
min
ogly
cosi
de a
ntib
iotic
s•
Fluc
ytos
ine
•C
ispl
atin
•C
imet
idin
e•
Trim
etho
prim
•
APPENDIX III
JD005805 Teks 2.indd 24 10/30/12 2:35:34 PM

Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 25
DIAGNOSIS OF ABNORMAL PROTEIN OR ALBUMIN EXCRETION
APPENDIX III
TAB
LE
2:
DIA
GN
OSI
S O
F A
BN
OR
MA
L PR
OT
EIN
OR
AL
BU
MIN
EX
CR
ET
ION
CL
ASS
UA
CR
(mg/
mm
ol)
UPC
R(m
g/m
mol
)U
RIN
E 2
4 H
R P
RO
TE
IN(g
/24
Hr)
Nor
mal
<2.5
(m
ale)
<3.5
(fe
mal
e)<1
5<0
.15
Trac
e pr
otei
n (M
icro
albu
min
uria
)≥
2.5
to 3
0 (m
ale)
≥3.5
to
30 (
fem
ale)
15-4
40.
15 –
0.4
4
Ove
rt P
rote
inur
ia(M
acro
albu
min
uria
)>3
0>
45>
0.45
* M
odif
ied
from
Sco
ttis
h In
terc
olle
giat
e G
uide
line
s N
etw
ork.
Dia
gnos
is a
nd m
anag
emen
t of
chr
onic
kid
ney
dise
ase.
E
dinb
urgh
: SI
GN
; 20
08
APPENDIX IV
JD005805 Teks 2.indd 25 10/30/12 2:35:34 PM

26 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
STAGING OF CHRONIC KIDNEY DISEASE
TAB
LE
3:
STA
GIN
G O
F C
HR
ON
IC K
IDN
EY
DIS
EA
SE
STA
GE
S O
F C
KD
Stag
eG
FR (
ml/m
in/1
.73m
2 )D
escr
iptio
n
1>9
0N
orm
al o
r in
crea
sed
GFR
, w
ith o
ther
ev
iden
ce o
f ki
dney
dam
age
260
-89
Slig
ht d
ecre
ase
in G
FR,
with
oth
er e
vide
nce
of k
idne
y da
mag
e
3A45
-59
Mod
erat
e de
crea
se i
n G
FR,
with
or
with
out
othe
r ev
iden
ce o
f ki
dney
dam
age
3B30
-44
415
-29
Seve
re d
ecre
ase
in G
FR,
with
or
with
out
othe
r ev
iden
ce o
f ki
dney
dam
age
5<1
5Es
tabl
ishe
d re
nal
failu
re
APPENDIX V
JD005805 Teks 2.indd 26 10/30/12 2:35:34 PM
Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 27
APPENDIX V
WORKING GROUP FOR THE STANDARDISATION OF eGFR IN CKD (ADULTS)
Chairman
Dr. Muhammad Arif Mohd. HashimSenior Consultant Pathologist andHead of Pathology DepartmentHospital Kuala Lumpur e-mail : [email protected]
Members
Dr. Baizurah Mohd. HussainSenior Consultant Pathologist andHead of Pathology DepartmentHospital Ampang e-mail : [email protected]
Dr. Siti Sharina AnasChemical PathologistHospital Putrajaya e-mail : [email protected]
Dr. Hanisah Abdul HamidChemical PathologistHospital Tengku Ampuan Rahimah, Klang e-mail : [email protected]
Dr. Nik Ahmad Zahar Nik YahChemical PathologistHospital Raja Permaisuri Bainun, Ipoh e-mail : [email protected]
En. Liew Chuan HeeScientific Officer (Biochemist)Hospital Tengku Ampuan Rahimah, Klang e-mail : [email protected]
En. Abdul Rahim bin OsmanScientific Officer (Biochemist)Hospital Kuala Lumpur e-mail : [email protected]
Cik Kanchana KanthasamyScientific Officer (Biochemist)Hospital Kuala Lumpur e-mail : [email protected]
Cik Lili Tresa ArulananbanMedical Laboratory TechnologistKlinik Kesihatan Tanglin e-mail : [email protected]
En. Lee Lian HoeMedical laboratory TechnologistHospital Selayang e-mail :[email protected]
JD005805 Teks 2.indd 27 10/30/12 2:35:34 PM

28 Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012.
REFERENCES
1. Ministry Of Health. Management of Chronic Kidney Disease in Adults. MOH/P/PAK/217.11(GU) ; 2011
2. W. Greg Miller, David E. Bruns et al. Current Issues in Measurement and Reporting of Urinary Albumin Excretion Clinical Chemistry 2009 ; 55(1):24–38
3. Robert M. Breslow. Evaluating Kidney Function: Impact on Clinical Decision Making for the Pharmacist Caring for the Older Adult JPSW 2011 ; 44-54
4. National Kidney Foundation : Frequently Asked Questions About GFR Estimates 2010
5. Jinn-Yuh Guh. Proteinuria versus Albuminuria in Chronic Kidney Disease. Journal Compilation Asian Pacific Society of Nephrology 2010 ; 15 : 53–56
6. Edmund J. Finlay M. et al. How should proteinuria be detected and measured? Ann Clin Biochem 2009 ; 46 : 205 – 217
7. Graham RD Jones. Laboratory reporting of Urine Protein and Albumin. Clin Biochem Rev 2011 ; 32(2) : 103-107
JD005805 Teks 2.indd 28 10/30/12 2:35:34 PM

Lab Investigation Guidelines for CKD and Utilisation of eGFR in Adults 2012. 29
ACKNOWLEDGEMENTS
The Editorial Committee wishes to thank the following for their invaluable support, guidance and direction in the preparation of this guideline, without whose provision of relevant information the production of this guidelines book would not have been possible:
Director General of Ministry of Health•
National Chemical Pathology Services•
National Nephrology Services•
Family Health Development Division•
National Public Health Laboratory•
Special thanks are also accorded to individuals who have directly or may indirectly involved in the compilation and publication of this guidelines.
JD005805 Teks 2.indd 29 10/30/12 2:35:34 PM

PRINTED BYPERCETAKAN NASIONAL MALAYSIA BERHADKUALA LUMPUR, 2012www.printnasional.com.myemail: [email protected].: 03-92366895 Fax: 03-92224773
JD005805 Teks 2.indd 30 10/30/12 2:35:34 PM

Chemical Pathology DisciplineNational Pathology ServicesMinistry of Health Malaysia
Laboratory InvestIgatIon guIdeLInesFor
CHronIC KIdney dIsease and utILIsatIon oF egFr In aduLts
MiNiStry of HealtH MalaySia
OCTOBER 2012
JD005805_KULIT INVESTIGATOR ndd.indd 1 10/30/12 1:59:29 PM