labouring to better effect: studies of services for … · labouring to better effect: studies of...
TRANSCRIPT

Labouring to better effect: studies of services for women in early labour The OPAL study (OPtions for Assessment in early Labour)
Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO)
November 2006
prepared by
Helen Spiby
Josephine M. Green
Clare Hucknall
Helen Richardson Foster
Alison Andrews
Mother and Infant Research Unit, Department of Health Sciences,
University of York
Address for correspondence
Helen Spiby, University of York, Area 4, Seebohm Rowntree Building,
York YO10 5DD
E-mail: [email protected]; Tel: 01904 321825

The OPAL study
©NCCSDO 2007 2
Contents
Acknowledgements 6
Executive Summary
Background 7
Objectives 7
Data collection 7
Key findings 8
Key recommendations for policy 9
Key recommendations for practice 9
The Report
Section 1 Background 11 1.1 Maternity care in the UK 11
1.1.1 Care during early labour 13
1.1.2 Women’s experiences of maternity care 15
1.1.3 Midwives and confirmation of labour 18
1.1.4 Innovations in early labour care 19
1.1.5 Triage 19
1.1.6 The All-Wales Clinical Pathway for Normal Labour 22
1.1.7 Home visits in early labour 24
1.1.8 Education and encouraging physiology 24
1.1.9 NHS Direct 25
1.1.10 Summary 26
1.2 OPAL (OPtions for Assessment in early Labour): overview of the project as planned and in practice 26
1.2.1 Context 26
1.2.2 Components 27
1.2.3 Early changes to the research plans 28
1.3 Identification of related research 29
1.4 Timetable 29
Section 2 Early labour services in England – a survey of HoMs 30
2.1 Methodology 30
2.1.1 Identification of the sampling frame 30
2.1.2 Data-collection tools 30
2.1.3 Pilot study 31
2.1.4 Main study methods 32
2.1.5 Sample size 32
2.2 HoMs England survey findings 33
2.2.1 Response 34
2.2.2 Background to Trust and service provision 34
2.2.3 Provision of early labour care 37

The OPAL study
©NCCSDO 2007 3
2.2.4 Changes to early labour services 48
2.2.5 Home assessment in early labour 55
2.2.6 Triage services 62
2.2.7 Additional options for early labour services 70
2.3 Recommendations for introducing home- or community-based assessments 72
2.3.1 Changes to commissioning 72
2.3.2 The importance of the model of midwifery care 72
2.3.3 Recommendations related to the introduction of triage areas 73
2.3.4 Recommendations related to the introduction of telephone triage 74
2.3.5 Recommendations relating to additional options for early labour care 75
2.4 Conclusion and discussion 75
Section 3 Midwives’ and women’s experiences of the All-Wales Clinical Pathway for Normal Labour 79
3.1 Background 79
3.1.1 The All-Wales Clinical Pathway for Normal Labour (the Pathway) 79
3.1.2 Part 1 of the Pathway 79
3.2 Aims 80
3.3 Methodology 80
3.3.1 Midwifery research fieldworker 81
3.3.2 Communications with stakeholders 82
3.3.3 Ethics and research governance issues 83
3.3.4 First contact with midwives 84
3.3.5 Modifications to the research plan 85
3.4 Data collection from midwives 85
3.4.1 Rationale for focus groups 85
3.4.2 Alternative data collection from midwives 86
3.4.3 Focus group arrangements 86
3.5 Midwives: findings 86
3.5.1 Documentation 87
3.5.2 Recording Part 1 information 88
3.5.3 The telephone assessment 90
3.5.4 Supporting practice and empowering midwives 91
3.5.5 Impact on workload 93
3.5.6 Perceived benefits for women 94
3.5.7 Possible disadvantages 96
3.6 Midwives: discussion 97
3.7 Data collection from women 98
3.7.1 Method of data collection 98
3.7.2 Analysis of women’s data 99
3.7.3 Development of the CATI 100
3.7.4 Early pilot work: mapping the key issues 100
3.7.5 Piloting the interview process 103
3.7.6 Target sample 104
3.7.7 Planned sample size 105
3.7.8 Recruitment in practice 105

The OPAL study
©NCCSDO 2007 4
3.7.9 Informing women about the research 106
3.7.10 Recruitment of women at discharge 109
3.7.11 Preparing community midwives for Recruitment Fortnight 109
3.7.12 Maintaining contact during Recruitment Fortnight 110
3.7.13 Arranging interviews 110
3.7.14 Recruitment response 111
3.7.15 Alternative strategies considered 112
3.7.16 Phase 2 recruitment procedures 112
3.7.17 Final recruitment figures 113
3.7.18 Sample characteristics 114
3.8 Women: findings 114
3.8.1 Descriptive information of women’s experience of Part 1 of the Pathway 115
3.8.2 Advice while staying at home 124
3.8.3 Satisfaction: statistical analyses 126
3.8.4 Satisfaction: women’s descriptions of their experiences 130
3.8.5 Satisfaction summary 144
3.8.6 Antenatal preparation and expectations 145
3.9 Women: discussion 149
3.9.1 Methodological issues 149
3.9.2 The Pathway 149
3.9.3 Professional and telephone skills of the midwife 150
Section 4 NHS Direct 152 4.1 Views of Heads of Midwifery in England 152
4.1.1 Interview data 155
4.2 Views of midwives in Wales 156
4.3 Discussion with staff of NHS Direct 157
4.4 Conclusion 157
4.5 Incorporation of structured telephone assessment for the SDO-funded Early Labour Support and Assessment (ELSA) trial 158
Section 5 Discussion and conclusion 159 5.1 Discussion 159
5.1.1 Methods 159
5.1.2 NHS Direct 163
5.1.3 England 164
5.1.4 Wales 169
5.2 Over-arching themes 171
5.3 Conclusion 172
5.4 Recommendations 173
5.4.1 Recommendations for practice 173
5.4.2 Recommendations for policy 174
5.4.3 Recommendations for future research 174
References 175

The OPAL study
©NCCSDO 2007 5
Appendices (separate document)
Appendix A National survey of early labour services in England questionnaire
Appendix B National survey of early labour services in England survey cover sheet
Appendix C Additional tables from Section 2
Appendix D Your pathway through labour leaflet
Appendix E Focus-group topic guide for midwives in Wales
Appendix F The OPAL study newsletter
Appendix G The computer-assisted telephone interview schedule
Appendix H Information sheet for potential participants
Appendix I Short proforma for every primiparous woman
Appendix J Additional tables from Section 3

The OPAL study
©NCCSDO 2007 6
Acknowledgements
For support to the research, co-grant holders:
Ms Polly Ferguson, Midwifery Officer, Welsh Assembly Government,
Professor Mary Renfrew, Director, Mother and Infant Research Unit,
Department of Health Sciences, University of York,
Professor Mary Newburn, Research and Policy Officer, National Childbirth
Trust,
Ms Janet Fyle, Professional Standards Adviser, Royal College of Midwives,
London,
Professor James Walker, Department of Obstetrics and Gynaecology, St.
James’ University Hospital, Leeds,
Mr Peter Stewart, Consultant Obstetrician and Gynaecologist, Sheffield
Teaching Hospitals NHS Trust,
Dr Brenda Leese, Reader in Primary Care, University of Leeds.
We thank Mrs Jenny Brown and Ms Jill Hunt for secretarial assistance
during the course of this research and compilation of this report.
Our thanks also to James Thomas for expertise in development of the
programme to support the computer-assisted telephone interview.

The OPAL study
©NCCSDO 2007 7
Executive Summary
Background
Care in early labour has an important contribution to make to clinical and
psychosocial outcomes of labour, and to cost-effectiveness of services.
Systematic evidence about alternative ways of organising and delivering
services in early labour is, however, sparse. The OPAL (OPtions for
Assessment in early Labour) study was developed as a suite of mixed-
method studies to examine service provision in England and Wales for
women in early labour. One specific service was of particular interest: the
All-Wales Clinical Pathway for Normal Labour (or the Pathway). This was
introduced in 2003 without formal evaluation and includes a structured
telephone assessment and the provision of telephone advice around the
time of labour onset to women considered at low obstetric risk.
A randomised controlled trial funded by the NHS Service Delivery and
Organisation (SDO) programme (ELSA, the Early Labour Support and
Assessment trial) is investigating the impact of providing midwifery
support to nulliparous women in their own home, in early labour,
compared with standard hospital care. OPAL was designed to provide
important contextual information against which the findings of this trial
could be interpreted.
Objectives
1 To map early labour services in England and explore innovations.
2 To explore the perceptions of Part 1 (the telephone component) of
the Pathway among service users and providers.
3 To obtain health care providers’ views about using NHS Direct for
early labour advice.
4 To inform the interpretation of the results of the ELSA trial.
Data collection
Information about early labour services in 178 units was obtained by
postal questionnaire survey to Heads of Midwifery; this was supported by
interviews with a purposive sub-sample of 17 who provided additional
information about local service provision.

The OPAL study
©NCCSDO 2007 8
In Wales, focus-group discussions were held with a sample of 21
midwives and computer-assisted telephone interviews were carried out
with 46 new mothers from six NHS Trusts.
Key findings
1 There has been a considerable amount of change to early labour
services in England, driven by a need to reduce the number of
women attending labour wards who are not in labour. The range of
service provision includes contact and subsequent assessment at a
maternity unit, home assessment, triage services (areas and
telephone) and early labour assessment at Birth Centres, Maternity
Units and Day Assessment Units. Change has more commonly been
effected in consultant units with a midwifery-led care area and in
larger size units.
2 The extent of service change is not matched by evaluation and
statistical information about the impact of these changes appears
scanty. Robust information related to clinical, psychosocial and
workload management impacts of these services is generally lacking.
3 Several of the service innovations require additional staffing, staff
training that should include issues of underpinning philosophy, high-
quality documentation and evidence-based guidelines to support
practice.
4 Midwives in Wales were generally positive about the telephone
component of the Pathway. Reasons given included that it: was
evidence-based; aided communication and led to women receiving
more consistent advice; and ‘gave permission’ for women to remain
at home.
5 Women’s experiences of the Pathway were varied. Satisfaction was
related to: being treated as an individual and with respect; longer
and fewer calls; and antenatal preparation, particularly the
expectation of staying at home in early labour.
6 Nearly half the sample of women in Wales were sent home after
attending hospital and this was associated with dissatisfaction.
Women were also dissatisfied when they did not feel welcome to
attend the maternity unit.
7 Receipt of the Pathway leaflet and the opportunity to discuss it with a
midwife were associated with satisfaction. Nearly one-third of the
maternity units in the Heads of Midwifery services England survey did
not offer women any written information about local arrangements
for early labour care.

The OPAL study
©NCCSDO 2007 9
Key recommendations for policy
1 The telephone service provided by NHS Direct should not be
extended to include assessment of women in early labour.
2 The potential for Children’s Centres to be a further venue for early
labour services is not yet known and should be monitored.
3 The impacts on early labour services of changes to the
commissioning process should be assessed.
Key recommendations for practice
1 Changes to early labour services should be introduced within robust
systems of evaluation that address issues of clinical outcome,
impacts on women’s experiences and labour-ward workloads.
2 Good practices in change management should be adopted that foster
staff involvement and time for discussion of new approaches.
3 The provision of early labour care for women who may not be able to
communicate in English requires particular consideration.
4 Any changes to early labour services in England should reflect the
philosophy of the maternity module of the National Service
Framework for Children, Young People and Maternity Services.
5 Statistical information should be of a quality to support evaluation
and monitoring.
6 Clinical guidelines for evidence-based care in early labour are
required.
7 Workload-management systems should be utilised to determine
impact of service changes.
8 The provision and content of written information about early labour
should be reviewed. Women should receive information about local
arrangements for early labour care and have the opportunity to
discuss it with a midwife during pregnancy so that they also
understand the underlying philosophy.
9 The use of discussion boards or other electronically based systems to
facilitate the dissemination among providers of service developments,
experiences and evaluations related to early labour care should be
explored.
10 Documentation should be completed for each episode of telephone
assessment; this documentation should be available for subsequent
care providers.

The OPAL study
©NCCSDO 2007 10
11 When women telephone in early labour, or are sent home after
attending the unit, they should be given clear advice and criteria for
further contact, and the rationale for this advice.
12 Midwives’ training needs in conducting telephone assessments should
be reviewed and training made available, where required.

The OPAL study
©NCCSDO 2007 11
Section 1 Background
1.1 Maternity care in the UK
Since the 1990s the maternity services in the UK have been subject to
changes of philosophy, location for the provision of particular components
of maternity care and in the contribution of different health professionals.
The report of the Expert Maternity Group (Department of Health, 1993)
encouraged a greater emphasis on choice within maternity care for
women, a key role for the midwife in low-risk maternity service provision
and an increase in the delivery of services in the community. The aims
included maternity service providers working in ways that would provide
women with increased continuity of care and more control over the
childbearing experience.
The recent National Service Framework for Children, Young People and
Maternity Services (NSF; Department of Health, 2005) includes one
module related to maternity care. This comprises the current main policy
driver for the NHS maternity service provision in England and requires
that
women have easy access to supportive, high-quality maternity services,
designed around their individual needs and those of their babies.
(Department of Health, 2005: p. 191).
The NSF acknowledges the need for a woman to be supported during her
labour as well as receiving high-quality clinical care. In the provision of
clinical care and public health practice, clinical guidelines, health
technology appraisals and public health guidance issued by the National
Institute for Health and Clinical Excellence (NICE) are available to
influence and underpin maternity care. Other current policy directives
that impact on maternity service provision include those that affect the
working conditions of NHS staff, including the European Working Time
Directive and Improving Working Lives (Department of Health, 2004a).
Rates of intervention during labour continue to rise, despite concerns
among health professionals and groups working with and supporting
childbearing women (Downe et al., 2001). In 2004–2005, only 48 per
cent of births could be defined as normal births (with the absence of
surgical intervention, instrumentation, induction, or regional or epidural
anaesthetic). The proportion of unassisted vaginal births has fallen from
78 per cent in 1989 to 65 per cent in 2004–2005 (NHS Maternity
Statistics, England, 2004–2005; The Information Centre, 2006). There is
currently an emphasis on supporting normality in childbearing, especially
during labour, included in the NSF (Department of Health, 2005). This has
The OPAL study
©NCCSDO 2007 12
manifested in a range of ways that include support for physiological
processes during labour (maintenance of upright positions, avoidance of
opiates or epidural anaesthesia, minimising intervention in labour) for
women at low obstetric and medical risk in, for example, the Royal
College of Midwives’ Campaign for Normal Birth.
A national survey reported by Smith and Smith (2005), undertaken prior
to publication of the NSF, identified some interesting trends in the
provision of maternity services. This survey, with an exceptionally high
response rate of 97.7 per cent, revealed an increase in home birth in
areas with a strong provision of midwifery-led care, and a reduction in the
involvement of general practitioners (GPs) in intra-partum care, resulting
in the midwife being identified more frequently than the GP as the
alternative lead professional to consultant-led maternity care. The
numbers of both consultant- and non-consultant-led units fell in England
and Wales between 1988 and 2002 (n=306 and 261 respectively).
Service changes include the closure of small, stand-alone units, the
conversion to stand-alone units of previously consultant-led units with low
delivery numbers and the consolidation of consultant-led services onto
larger sites. In particular, these large facilities appear to experience
difficulties in providing optimal early labour care due to issues of staffing
levels and facilities (Dennett and Baillie, 2002).
Most, but not all, maternity services remain under the managerial control
of the acute sector of the NHS with shared management of both
community and hospital-based midwives by one Head of Midwifery. There
are a few exceptions, with Primary Care Trust (PCT)-managed maternity
service providers, a small provision of non-NHS maternity care provided
by independent midwives available in many areas of the UK and a small
number of private consultant-led maternity units, generally in London.
Many NHS maternity service provider units and associated community
midwifery areas are also approved as training sites for pre-registration
students of midwifery, medicine and nursing.
The professions responsible for antenatal and postnatal care continue
largely unchanged; however, there is now a greater acknowledgement of
the appropriateness of midwives as lead carers for low-risk women and
settings. Obstetricians lead medically and obstetrically high-risk care and
have an increased presence on labour suites (Smith and Smith, 2005).
There are significant regional differences in the proportion of midwives
available per woman in the population, with generally higher numbers of
midwives available in the north and west of England than other areas
(Hannah, 2005). Midwifery vacancies are estimated at 2000 vacant posts,
with a requirement for a further 1000 midwives to accommodate
increases in midwifery-led care and home birth, and areas such as London
report vacancy rates above the national average. More midwives are
working part-time and employers have been encouraged to develop

The OPAL study
©NCCSDO 2007 13
employment practices that improve midwives’ working lives (Department
of Health, 2004a). Initiatives that have aimed to attract midwives back
into NHS practice have met with some limited increase in midwife
numbers (Department of Health, 2004a); however, a peak in the number
of midwives retiring is expected to occur within the next 10 years with
associated challenges for the NHS. For these reasons, the optimal
deployment of staff is essential.
The maternity service continues to receive valuable contributions from
those in roles that support both women and midwives: health care
assistants, support workers and Maternity Care Assistants (MCAs). These
people often work in ways that closely support the midwifery role in all
settings where maternity care is provided, including hospital, community-
based care and Birth Centres and release midwifery time from non-
midwifery duties (NHS Employers, 2005). The involvement of support
workers, working under midwifery jurisdiction, in providing support to
women in early labour has recently been reported (NHS Employers,
2005). The Royal College of Midwives has defined a set of competencies
for the role of maternity support workers. Recent policy has encouraged
approaches targeted at women and families in situations of poverty and
disadvantage (midwives and health visitors work in SureStart
partnerships and will subsequently work in Children’s Centres) to improve
the health of children under five (Department for Education and Skills,
2004). A small proportion of women receive additional support from
doulas (an experienced trained helper who provides continuous comfort,
companionship and emotional support to a woman during labour and
delivery); these are generally hired independently by pregnant women
but also available in some pilot SureStart initiatives.
1.1.1 Care during early labour
The importance of the timing of admission to the hospital labour ward is
demonstrated in the midwifery and obstetric literature. The importance of
avoiding hospital admission for women whose cervix has not reached full
effacement or where little dilatation has been achieved comprises one of
the lessons learned from workshops conducted in the USA that aimed to
share experiences of reducing rates of caesarean section (Flamm et al.,
1998). There are suggestions that repeated visits to the labour suite for
women at or near term should be viewed as a cause for concern among
maternity professionals as they can be associated with a higher chance of
caesarean section (Summers et al., 1991). Negative associations with
repeated episodes of false labour include subsequent incoordinate uterine
action (Schauberger, 1986), increased risk of fetal distress, and
augmentation of labour and operative births (Arulkumaran et al., 1987),
although Quinn and colleagues (1981) found no such associations if
labour onset did not occur within 48 h.
The OPAL study
©NCCSDO 2007 14
There is limited research available related to care in early labour and the
studies that do exist often lack appropriate control groups. Admission to
the hospital labour ward at higher cervical dilatation with care provided by
certified nurse-midwives was associated with lower rates of unassisted
vaginal delivery in a hospital in California (Jackson et al., 2003). Women
booked at a UK GP unit where home assessment was a part of the care
package used less Pethidine, had fewer epidurals, and less electronic fetal
monitoring, augmentation, fetal distress and forceps than women who
gave birth at a consultant unit where care did not include home
assessment (Klein et al., 1983). The generalisability of the findings of that
study is limited by the retrospective nature of the research, small
numbers and atypical setting and potential for selection bias. A small
Canadian trial evaluated a triage area in a general hospital where
delivery-room nurses, following a strict protocol, assessed women on
admission (McNiven et al., 1998). Women found not to be in labour were
allocated randomly to either the experimental approach where they could
return home until labour was established or the standard care that
comprised immediate admission to delivery suite. Whereas this study
lacked statistical power to detect a difference in caesarean section rates
between the two groups, women admitted later in labour were found to
have lower rates of augmentation of labour and epidural anaesthesia. A
retrospective study of nulliparous women admitted to an Ottawa teaching
hospital found fewer amniotomies and episiotomies among women who
attended at cervical dilatations between 4 and 10 cm compared to women
who attended with a cervical dilatation of 0–3 cm (Holmes et al., 2001).
Data collected from a retrospective review of records at a university
hospital in Finland found that, following adjustment for speed of labour,
women who arrived earlier at the delivery suite had more interventions
during labour and a higher rate of caesarean section (Hemminki and
Simukka, 1986). There are, therefore, suggestions that timing of
admission to a labour ward is important for the subsequent outcome of
labour.
The importance of environment is increasingly acknowledged in maternity
care. The provision of home-like settings for the entire labour and birth
have been evaluated and found to be associated with improved outcomes
including less analgesia and less augmentation, increased satisfaction
with the childbearing experience and fewer babies delivered using
instrumentation (Hodnett et al., 2005). The National Childbirth Trust
(NCT) conducted surveys in 2003 and 2005 to determine women’s
preferred characteristics for the birth environment and have made
recommendations for labour and birth facilities that are to be incorporated
into NHS building recommendations (Singh and Newburn, 2006).
In the UK, when a woman booked for hospital birth (97 per cent women
in the UK) feels that she may be going into labour and requires advice,
the usual arrangement for maternity care requires her to telephone the

The OPAL study
©NCCSDO 2007 15
labour suite of the unit where she is booked to have her baby. The advice
given to the majority of women is to attend the hospital labour suite for
assessment. At this point, a midwife will take a history of the labour,
perform a clinical examination and provide advice on subsequent options
for care. The woman may then be advised to either return to her home
and await events or remain on the labour suite or antenatal ward to await
labour onset or augmentation. These women do, however, require care
and this impacts significantly on the work of a labour and delivery suite
and reduces the staff available to provide care to women in established
labour. Consequently all women may experience a reduced quality of care
and units may also have difficulty in achieving the recommended staffing
ratios for women in established labour (Royal College of Obstetricians and
Gynaecologists and Royal College of Midwives, 1999).
The consequences of admission to a hospital setting prior to established
labour include possible embarrassment for women and their companion if
found not to be in labour, increased cost to families of repeated travel or
costs to the NHS if an ambulance is required. Women may also feel
anxious about being asked to leave the perceived security of the hospital
and be unsure of what signs to look for when they had previously
considered that there were signs of labour. Staying in hospital prior to
established labour brings difficulties in allocating beds and the associated
costs to the NHS of an inpatient stay, an increased propensity for
intervention either suggested by clinicians or requested by the woman,
and a lack of facilities for birth companions to remain with the woman
leading to feelings of isolation at a time when support is crucial. Between
10 and 33 per cent of admissions to a delivery suite may be from women
not found to be in established labour (category X; Ball 1996). However,
women require confirmation that labour has started likely timescales and
advice on coping with labour. If the woman is advised to remain in
hospital, she may be assessed by either midwifery and medical staff, or
both, thus contributing to the work of both staff groups and adding to
work that may be avoidable in the context of reductions in junior doctors’
hours.
1.1.2 Women’s experiences of maternity care
Previous studies of women’s satisfaction with maternity care have
demonstrated repeatedly that women are usually fairly positive and would
wish to use again or recommend the model or components of care
already experienced, rather than approaches to care that they have not
used personally (van Teijlingen et al., 2003). This offers challenges in
measurement of satisfaction and discussion of preferences, for example,
for subsequent births.
Recent large-scale evaluations of women’s experiences of maternity care
have, however, clearly indicated factors that are important to women,

The OPAL study
©NCCSDO 2007 16
including their perceptions of support and being in control and their
involvement in decision-making and choice (Green et al., 1990, 1998).
Using qualitative approaches, it has been suggested that women’s
involvement in decision-making might fall within four typologies;
unilateral decision-making on the part of care-givers, contested by
women; unilateral decisions made by health professionals with agreement
by women; non-engagement in the decision-making process while letting
the events of labour unfold and lastly shared decision-making between
the woman and her care-giver. Women’s responses to the different
experiences of involvement had significant impacts on their emotional
well-being (Vande Vusse, 1999). Communications that take place
between labouring women and their care-givers play a key role in
women’s overall experience of labour. Continuous midwifery support has
been demonstrated to improve obstetric outcomes in terms of less
intervention, less pharmacological pain relief and fewer operative births
(Hodnett et al., 2005). However, it has also been demonstrated that
women may receive less support in certain aspects of intra-partum care
than they had hoped for during their pregnancy, for example, in use of
coping strategies (Spiby et al., 1999). Research that informed the
recommendations of the NSF suggests that significant numbers of women
are worried by feeling unsupported by maternity care providers during at
least part of their labour (Garcia et al., 1998). Some women may be
reassured only by assessment or admission to hospital, whereas others
may feel supported at home through house visits by midwives.
The emotional consequences of childbearing remain a significant concern
for maternity service providers. Psychiatric illness comprises the most
common cause of maternal death in the UK (CEMACH, 2004). Accurate
memories of labour and birth and of the impressions of the attitudes of
care-givers are retained for many years (Simkin 1991) and these
contribute to women’s perceptions of satisfaction about their experience
of childbearing. Post-traumatic stress disorder related to childbirth is now
acknowledged as a distinct disorder with up to 5.6 per cent of women
reporting symptoms at 4–6 weeks postpartum (Creedy et al., 2000).
Whereas effective treatment is available in the form of cognitive
behavioural therapy, posttraumatic stress disorder is a condition that may
often remain undiagnosed but impact on women’s subsequent decisions
related to method of subsequent deliveries (Ryding, 1993) and future
childbearing (Goldbeck-Woods, 1996).
Women’s views of early labour services have previously been largely
unexplored in surveys of experiences of care in labour. Smith (2001)
reports the development and preliminary use of an instrument designed
to measure women’s satisfaction with the quality of different models of
intra-partum maternity care in the UK. Response rates of 70 per cent
were achieved. Dimensions of the labour experience identified as
important included professional support, pain in labour, environment and

The OPAL study
©NCCSDO 2007 17
home assessment in early labour. A statistically significant association
was found between absence of a home visit and risk of postnatal
depression (identified using the Edinburgh Postnatal Depression Scale).
Further testing of the instrument was recommended in groups outside
those included during development of the instrument (predominantly
middle class, mainly white and moderately highly educated women in
supportive relationships). Smith (2001) suggests that this instrument
could be used in comparisons of satisfaction with intra-partum care
delivered within different models or settings. A national survey of
women’s experience of maternity care in England is in progress and will
report in 2007.
Women booked for low-risk care may sometimes require transfer between
settings if labour deviates from the normal or if there are concerns about
maternal and fetal well-being. The disappointment felt by women
transferred to hospital care following booked community care was
described (Creasy, 1997) and women’s feelings of loss of choice and
control, together with anger and disappointment when transferred to
consultant unit care following booking in midwifery–led facility (Walker,
2000). Admission to hospital has been identified as a time of disruption to
women’s use of coping strategies (breathing, relaxation and postural
change) in labour (Spiby et al., 1999). Martin and Jomeen (2004)
identified a lower internal locus of control at labour onset among women
who had a period of expectant management at home, following prelabour
rupture of membranes, compared with those who remained in hospital.
Using conjoint analysis, Langworth and colleagues (2001) found that
different factors were important for women who chose hospital and home
birth. Women who preferred hospital birth valued, among other factors,
the avoidance of transfer between care settings if problems occurred with
labour.
Women may also need to be referred in labour if a unit has no spare
capacity; the closure of units to admission of labouring women occurs in
the UK. In a study carried out in Sweden, a group of women for whom
this occurred in labour utilised more opiates and epidurals during their
labour and had a higher level of episiotomy than a group who received
care at their planned birth unit (Wiklund et al., 2002). The women
diverted away from their planned birth unit also described more feelings
of stress and of not feeling welcome at the unit where they laboured
compared with those who gave birth in their planned unit. The perception
of being unwelcome at the labour unit was considered by women to
constitute a difficult and negative start to their labour and associated with
feelings of panic and fear (Wiklund et al., 2002). The points of admission
to and transfer between labour settings have, therefore, been
demonstrated to contribute significantly to women’s experiences of their
labours.

The OPAL study
©NCCSDO 2007 18
1.1.3 Midwives and confirmation of labour
In the UK, the confirmation of labour and provision of advice to women
rests within the sphere of practice of the midwife in cases of low-risk
maternity. In complicated pregnancies, midwives also provide advice on
appropriate times for admission to labour suites for assessment and
advice, while working in a multi-disciplinary team. It appears likely that
confirmation of labour onset will remain a midwifery role for the
foreseeable future, as it is designated within the role of the midwife and
supported by secondary legislation (Nursing and Midwifery Council,
2004).
The extent to which midwifery training adequately prepares midwives to
provide high-quality care in early labour is unclear due to the dearth of
recent evaluations. It is also important to state that the emphasis of
midwifery training, hitherto, has been on face-to-face assessment and
discussion with a woman in labour; this has been the case in both UK and
North American pre-registration programmes (DeVore, 1999). Guidance
on making such assessments and providing appropriate support and
advice by telephone is available in the contemporary midwifery literature
(DeVore, 1999; Baston, 2003) but it may be that there is a skills deficit in
this area. Baston (2003) details the steps in providing advice by
telephone to women in labour. These steps include discussion of coping
strategies used and whether alternative methods may be useful,
providing advice about when a woman should contact the birth unit again,
if she decides to remain at home.
Sookhoo and Biott (2002) explore methods of learning in the clinical
setting among midwives. It is suggested that a range of factors including
intuition, use of diagnostic markers and confidence in making assessment
without using intrusive procedures all contribute to learning and will
develop with increasing midwifery practice; the concept of coping with
uncertainty is important in this aspect of practice and needs to be
developed by novice practitioners.
Additional concerns for midwives if not seeing women face-to-face include
those related to negative outcomes for the woman or her baby if there is
an unexpectedly rapid labour that culminates in an emergency and a
possibly professionally unattended birth. Such births are associated with a
higher rate of neonatal morbidity than planned home birth and
considerable anxiety and emotional distress for the family. The midwife
will have concerns for the family’s well-being but may also fear enquiry
into her professional practice, complaint or litigation (Webb, 2004). For
those reasons, it may feel ‘safer’ to advise a woman to attend the
maternity unit for examination and assessment.
In a focus group conducted predominantly with midwives pursuing a
Master’s programme, Burvill (2002) explored midwives’ confirmation of

The OPAL study
©NCCSDO 2007 19
labour onset. Issues identified by focus-group participants included
difficulties of defining labour onset, the restrictions imposed by
terminology, incorporating intuition and using observation of physical
signs to arrive at a midwifery confirmation of labour onset. The fact that
labour is a continuum, rather than the clearly defined three-stage process
conventionally described in the midwifery and obstetric texts, is also
highlighted (Burvill, 2002). A recent report identified the various
processes and factors that affect midwives’ decision-making about labour
onset (Cheyne et al., 2006); this work was conducted as a precursor to a
randomised controlled trial. Factors that had a bearing on decisions
around early labour management included an interaction between the key
players of midwife, mother and institution. Some factors were accorded
less importance by midwives than by women – for example, passage of
the ‘show’ – and midwives agreed that their decisions were influenced by
institutional factors. Further work investigating midwives’ decision
analysis for labour is in progress in Scotland.
Women’s recognition of the spontaneous onset of labour has been
explored by Gross and colleagues (2003). A range of symptoms were
reported by women as features of their labour onset; for women having
their first baby, these included recurrent and non-recurrent pain (32 and
27 per cent respectively), watery or blood-stained vaginal loss (15.9 and
9 per cent respectively) and other systemic and emotional signals. These
findings suggest that women experience labour in ways that do not
always reflect traditional midwifery or antenatal teaching. These
researchers suggest that the time between a women’s recognition of
labour onset (after possibly several days of discomfort) and admission to
the birth unit may influence duration of subsequent labour, but that
hypothesis requires further exploration.
1.1.4 Innovations in early labour care
Provider units have responded in a range of ways to managing the
significant proportion of women who require early labour assessment.
These have included the designation of triage areas, either within or
adjacent to main delivery suites where women reporting signs of early
labour can be assessed by a midwife and then routed appropriately,
increased information about labour and, in Wales, the adoption of a
clinical pathway supporting normal labour and birth. Most research
related to triage systems is from the USA or Canada.
1.1.5 Triage
Triage systems have their roots in battlefield medicine where the principle
was to treat casualties in an order that would maximise the number of
survivors, not necessarily by treating the most severely injured first
(Mahlmeister and van Mullem, 2000). Triage was first reported in hospital

The OPAL study
©NCCSDO 2007 20
medicine in the 1950s and 1960s to manage the pressures on North
American emergency rooms experiencing high workloads. The triage
system was used in those contexts to decide on the urgency of each
patient’s condition and to determine the order in which patients should be
treated in the acute setting, with priority given to the most seriously ill.
Triage is used to describe either approaches to assessment that take
place face to face in a designated facility or as a telephone service to
screen out enquiries that do not require face-to-face assessment. Triage
areas, units and telephone triage have all been reported in North
American maternity care. They appear to have been introduced to provide
an obstetric emergency facility and also to reduce the volume of patients
on main delivery suites (Angelini, 1999a).
In one of the earlier reports of obstetric triage, Austin’s view of its
purpose appears to differ from that of later descriptions of triage services
in the USA (Austin, 1996). Austin suggests that triage-based care differs
from that provided in other obstetric settings in that it does not require
detailed history-taking, extensive physical assessments or laboratory
investigations and that triage is not a setting where treatment will usually
be given. The focus appears to be on deciding whether admission to the
maternity unit is appropriate and, if so, to which area. DeVore (1999) has
a similar approach and stresses that the aim of triage is not to make a
diagnosis or decide on treatment but rather to assess whether a more
detailed examination is required and the degree of urgency with which it
should be carried out.
Triage is described as an activity that can take place in both high- and
low-risk maternity contexts in the USA. It is suggested that it is
particularly important to have ‘meticulous’ triage in out-of-hospital Birth
Centres (Barnes and Dossey, 1999). These authors comment on the
importance of speaking directly to labouring women when conducting
telephone triage of calls related to labour and of correctly identifying
those who require face-to-face assessment. In larger units, triage
provides a facility where all maternity patients may be reviewed, including
those with postpartum complications. The services provided in North
American triage settings where care is provided by certified midwives,
nurse-midwives, attending physicians and residents is reported to include
management of early labour, complications of pregnancy and general
advice on less-acute conditions. No reports of the introduction of triage
within randomised controlled trials have been identified in the literature
but protocols for clinical care and the perceptions of benefits to pregnant
women, care providers and services are described (Angelini, 1999b).
Using case histories, Mahlmeister and van Mullem (2000) describe clinical
and potential legal issues that might arise from triage in the context of
North American systems of care (2000). In respect of telephone triage,
they report that claims related to negligence occur most commonly due to

The OPAL study
©NCCSDO 2007 21
a failure to conduct a systematic assessment of the patient’s condition,
not recognising the condition and its seriousness, incorrect advice or
onward referral and delays in responding to calls. The education and
clinical competence of service providers, existence of and adherence to
protocols and accurate documentation are all seen as factors that would
minimise the potential for litigation. Austin and Calderon (1999) address
the issue of triage in the context of the latent phase of labour. They see
reassurance, communications and information as key, in addition to
standard approaches to assessment of maternal and fetal well-being and
confirmation (or not) of the start of labour. The importance of clarity
related to the timing of labour onset is stressed as subsequent
management decisions will flow from that.
One national survey conducted by Angelini aimed to determine and
quantify the midwifery contribution to obstetric triage in the USA, identify
and describe the midwives’ role and work, and investigate particular
aspects of triage. Fifty-nine centres fulfilled the preset criteria of being a
unit that provided care to 3000 women per annum and included a
midwifery component to services. Information was sought in the following
areas: details of unit size and facilities available, births per year,
midwifery staffing, practice guidelines, extended roles, clinical condition,
evaluation of the fetal condition, record-keeping and organisational
issues. The response rate for the survey was 71 per cent. The findings
included identifying the following issues as important in the provision of a
triage service: keeping triage in a separate area, the role of providing
care for complicated pregnancies in the latter half of pregnancy, reduced
labour-ward volume, prompt assessment of obstetric patients, reduction
in unnecessary admissions, savings in time and money, reduced waiting
time for patients, improvements in use of resources (both personnel and
beds), reductions in the volume of patients seen in emergency rooms,
acting as a ‘gate keeper’ to admissions, supporting a risk stratification for
subsequent management and general improvements in obstetric services.
The most common presenting conditions managed in the triage area were
those related to latent and preterm labour, rupture of membranes at
term, reduced fetal movements, management of post-term pregnancy
and sexually transmitted diseases and urinary-tract infections. Angelini
(1999a) suggests that further research is required to explore midwives’
decision-making in triage areas, how the potential for litigation can be
reduced and further exploration of the triage-related aspects of the
midwifery role.
In another report describing the midwifery contribution to obstetric triage
in 10 USA settings, a range of activities and services are described in a
series of vignettes (Angelini, 1999b). Midwifery responsibilities in triage
varied between units but included the opportunity to provide patient
education, protocol development, some extended role duties and the
opportunity for the clinical teaching of students. Although the interface

The OPAL study
©NCCSDO 2007 22
with medical staff varied between units, as did the populations served and
their access to health care (Medicaid or privately insured), there was a
general cut-off point that women less than 16–20 weeks pregnant would
receive care within the gynaecology services. Angelini (1999b)
recommends triage as a useful primary care role for the midwife, offering
a potential to increase multi-disciplinary working, and triage is observed
to extend the midwifery role but it is suggested that a greater emphasis
on obstetric triage is required within midwifery education. There are
significant differences in both professional roles and boundaries between
the USA and UK settings and also different financial resourcing and
drivers between the two health care systems.
Responding to a range of enquires from pregnant women and their
families has traditionally been a part of labour-ward work in the UK but it
can cause interruptions to the care of women in established labour.
Midwives may feel concerned about responding to requests for advice
without face-to-face assessment due to inexperience and concerns about
potential litigation (Webb, 2004). Experiences of introducing delivery-
suite triage have been reported in UK settings. Telephone triage using a
specially developed proforma was seen as a means of dealing with
enquires in the context of excessive workload on busy delivery suites with
the potential for women to attend, if required. Triage was considered to
offer good clinical experience for midwives and a means of providing
women with continuity during early labour (Webb, 2004). Dennet and
Baillie (2002) reported the introduction of a midwifery triage service in
2001; the objectives of the service were to provide an assessment facility
including an out-of-hours service, referral for women with complicated
pregnancies, pre-operative care, the provision of advice and reassurance
and reduction of workloads on central labour wards. The service was
considered to have a beneficial impact on labour-ward workload and to
provide interesting midwifery experience.
1.1.6 The All-Wales Clinical Pathway for Normal
Labour
Whereas the provision of triage areas has been adopted as one solution to
providing appropriate assessment in early labour, a different approach
was developed in Wales, supported by funding from the Welsh Assembly
Government, and involved midwife, service-user, obstetric and midwifery
educator representation. The All-Wales Clinical Pathway for Normal
Labour (known as the Pathway) was introduced throughout Wales over
2003–2004 (Ferguson, 2003).
One key component of the integrated care pathway is the collaborative
care plan. This aims to optimise care through improved communications
among all members of the multi-disciplinary team using a single, shared
form of documentation. Information about assessments is shared

The OPAL study
©NCCSDO 2007 23
between care providers and the plan for care available to all team
members. The principle in collaborative care planning is that of reducing
documentation to a safe and clear minimum and of documenting in detail
only the deviations from usual care or progress (Foster, 2000).
Collaborative care planning is now used in a range of UK health care
specialties including gynaecology, paediatrics and palliative care. It has
been suggested that the utilisation of care pathways is associated with
efficient resource utilisation, support for the components of clinical
effectiveness including audit and risk management and improvement in
the patient experience through better information and the alleviation of
anxiety (Fox, 2004).
Based on the clinical-care-pathway approach, and following the successful
introduction throughout Wales of a similar pathway for palliative care, the
Pathway aims to support normality in childbearing and reduce clinically
unnecessary interventions through the provision of evidence-based
telephone advice to low-risk women in early labour and a protocol for
care in established labour (Ferguson, 2004). The Pathway comprises
three components: part one telephone advice; part two initial face-to-face
assessment and part three the active labour component that utilises a
partogram for recording of labour progress. It was hoped that use of the
documentation would reduce midwifery time in completion of
documentation while maintaining a high-quality clinical record (Fox,
2004). Following introduction at two pilot sites, an audit was conducted
that focused on issues of process and correct disbursement of calls (S.
Fox, personal communication, 2004). The Pathway was subsequently
introduced throughout Wales and supported by education for midwives.
The perceived benefits of the clinical pathway have been reported widely
in the midwifery and health services literature. Audit of adherence to the
Pathway has taken place at a mainly local (unit) level with progress
reviewed by the Pathway’s Steering Group that included midwives from
each Trust in Wales. There have been no large-scale rigorous evaluations
of its impact on health outcomes but an ethnographic study is
investigating its introduction in two Trusts in Wales (B. Hunter, personal
communication, 2004) and the experiences of women who have accessed
the pathway more than once has been evaluated as part of a Master’s
programme by D. Lucy. These two studies have yet to report. NHS Trusts
in England have demonstrated interest in the Pathway approach through
invitation for presentations about the initiative at midwifery meetings in
England.
Women are provided with information about the pathway during the third
trimester of their pregnancy, although one midwifery writer questioned
whether that document might be too simplistic and commented on the
lack of planning of evaluation of the introduction of the Pathway (Hall,
2003). It was anticipated that the Pathway would be appropriate for 50
per cent of women who give birth in Wales each year (the remaining

The OPAL study
©NCCSDO 2007 24
considered ineligible due to medical or obstetric risk factors). Early
reports reflected varying usage between Trusts to the order of 30–50 per
cent of women starting on the Pathway and of the Pathway being used
throughout labour for 50–85 per cent of those women for whom its use
had been initiated. While no formal evaluations were conducted, early
reports suggested that the information leaflet had been warmly received,
with more positive reports if discussed with women by midwives
(Ferguson, 2004).
1.1.7 Home visits in early labour
Other approaches to providing early labour care in the UK include the
provision of home visits, usually from a community-based midwife. The
concept of assessment and care for early labour taking place at home has
been available previously, albeit in a limited way in the UK through the
DOMINO (domiciliary in-and-out) scheme, some of the team midwifery
schemes (Flint, 1993) and by some independent midwifery practices
(Flint, 1996). While popular with women, this service has not previously
been subjected to rigorous evaluation in the UK context, although its use
has persisted in some areas. A small randomised controlled trial
conducted in Canada compared a home visit by a hospital obstetric nurse
with standard care of telephone triage. More women in the home-care
group arrived at hospital in established labour and fewer women in the
home-care group received opiates, although there were no differences in
epidural use and babies of women in the home-visit group were less likely
to require admission to a level ll baby nursery (Janssen et al., 2003). A
randomised controlled trial of early labour support and assessment,
funded by the NHS Service Delivery and Organisation of Care programme,
is currently in progress to evaluate early labour support and assessment
at home and hospital for low-risk women having their first baby, and will
report in 2008.
1.1.8 Education and encouraging physiology
Some units have focused particularly on how women can be best be
supported in early labour and offer services such as birthing pools,
aromatherapy and postural aids with birthing balls. Anecdotal accounts of
units encouraging women to make decisions about place of delivery
during their labour following home assessment appear in a minority.
Educating women about early labour and having clear criteria for
confirming labour onset have been identified as practices that reduce
early admission to labour wards (Bonovich, 1990; Lauzon and Hodnett,
1998). Other approaches to improving early labour care include those
with education as the focus, for example Birth Talks provided during the
third trimester, often in women’s own homes, where options for labour
The OPAL study
©NCCSDO 2007 25
are considered, including a detailed discussion of management of early
labour (Sandall et al., 2001).
1.1.9 NHS Direct
The telephone service provided by NHS Direct was introduced in pilot
sites in the UK in 1998 and more widely in 2000 with two main purposes
of providing health care advice and information (Commission for Health
Improvement, 2004). NHS Direct was also seen as a means of ensuring
continuing access to the skills and experience of qualified nurses who may
be unable to provide direct clinical care, for example, due to back injury.
Algorithms were not developed with labour as a focus and the emphasis
of guidance to callers requiring advice related to labour is to contact the
maternity unit providing their care (E. Povey, personal communication,
2005). Early evaluations of NHS Direct confirmed that the service
achieved satisfactory levels for safety and high levels of acceptability
among its users; staff providing the algorithm-based service enjoyed their
work but identified clear training needs (Munro et al., 1998). An over-
cautious approach by its nurses and aversion to possible risk was
identified in early evaluations. This was ascribed by those researchers as
a ‘desirable characteristic’ but one that must be weighed against potential
inconvenience to patients of referral to other services that may not be
necessary and costly to other parts of the NHS. The action by patients on
advice provided by NHS Direct has been explored; some patients did less
than they were advised and others did more than advised. It was
suggested that callers to NHS Direct might view the advice provided as
additional information for their consideration but take actions on advice
based on their pre-existing beliefs about what action would be
appropriate. This might, of course, be the case for other telephone advice
services.
While generally considered a success, some cautioned against widening
use of NHS Direct due to the perceived conflicting policy goals of
managing demand and the need to respond to consumers; concerns
about negative impacts on the continuity usually provided in UK primary
care were also voiced (Florin and Rosen, 1999). However, the widening
use of NHS Direct was announced in 2003 and this has subsequently
included use by the Retained Organs Commission and for the reporting of
suspected drug side effects.
More recent evaluations of the NHS Direct telephone service conducted by
the then Commission for Health Improvement suggest a continuing
appreciation of the service by users with positive comments on efforts to
improve access for those with special needs or from minority ethnic
communities; staff satisfaction also remained high. The Commission for
Health Improvement (2004) did, however, suggest that risk-management
practices within NHS Direct should be developed further. The widening

The OPAL study
©NCCSDO 2007 26
use of NHS Direct must be seen in the context of a changing NHS where,
following contractual changes, the out-of-hours service previously
provided by GPs is being delivered in alternative ways by a range of care
providers and where some 999 calls are also routed through nurses in
NHS Direct. The NHS Direct online web-based enquiry service was
introduced in 2001 with advice available on preset topics. Early concerns
about this included the potential to increase inequalities in access to
service among different groups and the absence of multi-cultural
responses (Wilkinson and McPherson, 2001).
1.1.10 Summary
From the review of the literature, it is clear that a range of factors affect
and are affected by the provision of early labour care. Issues of workload
management, the need to provide a clinically safe and high-quality
maternity service that meets the needs of individual women and their
families, while avoiding unnecessary intervention, are all considerations
for maternity service providers and commissioners. The approaches
described above have different theoretical and philosophical
underpinnings; these include the provision of information and education,
workload management and improved communications through integrated
care pathways.
New innovations may rapidly become embedded in practice, often lacking
an existing evidence base and without being subjected to evaluation. This
research will contribute information to the evidence base by mapping
current early labour services in England, exploring new approaches
through information provided by Heads of Midwifery services (HoMs) and
by the evaluation of one component of a service innovation in Wales from
the perspectives of service users and providers.
1.2 OPAL (OPtions for Assessment in early Labour): overview of the project as planned and in practice
1.2.1 Context
A randomised controlled trial funded by the NHS Service Delivery and
Organisation (SDO) programme (Early Labour Support and Assessment,
or ELSA) is investigating the impact of providing midwifery support to
nulliparous women in their own home in early labour, compared with
standard care in hospital. Systematic evidence about alternative ways of
organising and delivering services in early labour is exceedingly sparse.
The OPAL (OPtions for Assessment in early Labour) study was conceived
as a further suite of studies that would examine the impact of changes in
service provision since the original trial proposal was developed and

The OPAL study
©NCCSDO 2007 27
provide important contextual information against which the findings of the
randomised controlled trial could be interpreted.
OPAL was to be overseen by the same multi-disciplinary team conducting
the ELSA trial and the proposal had the support of the Welsh Assembly
Government, NCT and Royal College of Midwives. It was intended that it
would be conducted in the same time frame as ELSA and would facilitate
the interpretation of the results of the trial, and discussion of issues of
generalisability and implementation, if the intervention is found to be
effective.
1.2.2 Components
Survey of early labour services in England
The research team was aware of developments in early labour services in
England, such as triage facilities, to manage the heavy workloads on
labour suites. There had, however, been no comprehensive mapping of
these nor exploration of services that might have been tried and
abandoned and from which others could learn. We aimed to map these
through postal questionnaires to all HoMs in England, supported by
interviews with a purposive sub-sample. This was designated as Study 3
in the original proposal and is described in Section 2 of this report.
Evaluation of Part 1 of the All-Wales Clinical Pathway for Normal
Labour
The All-Wales Clinical Pathway for Normal Labour (AWCPNL), introduced
in 2003, includes a structured telephone assessment and the provision of
advice around the time of labour onset to women deemed to be at low
obstetric risk. We aimed to explore the perceptions of women who had
used that service and of their care providers. This was designated as
Study 1 in the original proposal and is described in Section 3 of this
report.
Feasibility of the use of algorithms in early labour advice and
assessment
Based on the results of the above, the plan was that feasibility studies
would explore the possibility of incorporating structured telephone
assessment into the randomised controlled trial for women allocated to
the intervention group who go into labour at night. Additional feasibility
studies would explore the development of algorithms, as used by NHS
Direct, as none currently have normal labour as a focus. This was
designated as Study 2 in the original proposal and is described in Section
4 of this report.

The OPAL study
©NCCSDO 2007 28
1.2.3 Early changes to the research plans
The project was timed to start on 1 November 2003 and to run for
18 months. Unfortunately delays in the availability of funding meant that
we were unable start until mid-April 2004. This had implications for the
feasibility studies, described above, because our timetable no longer
fitted that of the ELSA trial. This will be discussed further in Section 4.
Staffing
The staff specified in the proposal were two part-time researchers (0.6
whole-time equivalents, wte) and a part-time secretary (0.4 wte). These
posts were advertised in February 2004. One suitable secretarial
candidate was identified and invited for interview, but she then withdrew
her application. The researcher posts were advertised as 0.6 or 0.5 wte,
since we thought it possible that we might find candidates who already
had a part-time job for whom 0.5 wte was more attractive than 0.6 wte.
This proved to be the case.
Four candidates were short-listed and interviewed for the researchers’
posts. Two candidates were considered to be appointable and were
offered posts, one preferring to work 0.5 wte. Unfortunately, the second
candidate subsequently withdrew. To maintain the impetus of the
research, we proceeded with the one part-time researcher but also
brought in an experienced health service researcher known to the team,
on a sessional basis, who provided an additional 1 day per week to the
project.
To fill some of the remaining capacity for research assistance and to
increase a sense of ownership of the project in Wales, it was felt that a
local midwifery research fieldworker based in Wales would be the ideal
complement to the Yorkshire-based research team. We advertised
accordingly, and subsequently appointed a midwife in Wales who has
been seconded to the project for 1–2 days a week and who facilitated
local contacts throughout Wales.
This staffing arrangement, although not the one that we had originally
envisaged, overall worked well. The three researchers represent an
excellent skill mix, and the midwifery secondment provided career
development for the post-holder. However, it does represent less than the
1.2-wte capacity around which the project was planned. In November
2004, the two Principal Investigators moved from the University of Leeds
to the Department of Health Sciences at the University of York. Due to
the inability to appoint to the contract researcher posts in the
configuration that we had planned, both co-Principal Investigators have
devoted more time to this research and one of the Research Officers and
the midwifery research fieldworker extended their involvement with the
project during the extension agreed by SDO.

The OPAL study
©NCCSDO 2007 29
1.3 Identification of related research
Through our preparatory work in Wales, we became aware of two other
ongoing research projects in Wales that are evaluating aspects of the All-
Wales Pathway. Dr Billie Hunter, University of Swansea, is carrying out an
ethnographic study observing the use of the Clinical Pathway for Normal
Labour documentation tool in two maternity units. At the University of
Glamorgan, Debbie Lucy, and her supervisor Dr Sandy Kirkman, are
planning to conduct 10 interviews with women who have experienced
care on the All-Wales Pathway. Their particular interest is in women who
have accessed the All-Wales Pathway more than once. We co-ordinated
our research timetable with those of the other researchers to avoid
overload at particular clinical centres. We have recently learned that
research related to midwives’ decision-making in situations of variation
from Part 2 of the All-Wales Clinical Pathway for Normal Labour has
recently commenced (C. Dowling, personal communication).
1.4 Timetable
The feasibility studies (Study 2, see Section 1.2.2) were timetabled both
to dovetail with ELSA and to be informed by the findings from the All-
Wales Pathway (Study 1). The delays in issuing the contract for OPAL, in
addition to the delays with governance processes described subsequently
compromised that and meant that the project’s timetables and objectives
required revision.

The OPAL study
©NCCSDO 2007 30
Section 2 Early labour services in England – a survey of HoMs
2.1 Methodology
2.1.1 Identification of the sampling frame
To ensure that all Heads of Midwifery services (HoMs) in England were
included in our survey a variety of data sources were used to compile a
database. Initially, the statutory mechanism of supervision of midwifery
was used, and all Local Supervising Authority Midwifery Officers were
contacted and asked to provide information of HoMs in their area. A
second phase was to cross-reference this with the information held in the
Binleys Online database (www.binleysonline.com). Finally, the third phase
of the process was to obtain details of the units within the HoM's
jurisdiction. This information was obtained through Trust websites and
also through contacting the midwifery departments by telephone and e-
mail. Many HoMs have responsibility for more than one maternity unit and
service reconfigurations make this level of up-to-date information hard to
find.
2.1.2 Data-collection tools
To reduce the burden on respondents we wished to produce a
questionnaire that was easy to complete and which could be delegated by
the HoM if desired. This seemed particularly important where a HoM was
responsible for more than one unit. We considered the possibility of
designing a questionnaire that could be answered for more than one unit,
but this idea proved impractical since unit-specific information was
required. On the other hand we did want to ask HoMs (rather than those
they delegated to) a small number of specific questions related to
different forms of telephone advice to women in early labour, specifically
the All-Wales Clinical Pathway for Normal Labour and the use of NHS
Direct. We therefore produced an eight-page questionnaire, which was to
be completed for each maternity unit by whoever the HoM designated,
and a one-page cover sheet, which was to be completed by the HoM in
person. The cover sheet asked the HoM to confirm the units for which
they had responsibility in order that the sampling frame could be verified
and to supply the contact details for the person who would complete each
questionnaire.

The OPAL study
©NCCSDO 2007 31
2.1.3 Pilot study
Introduction
The main aim of the pilot study was to test the questionnaire to be sent
to all HoMs in England. We were keen to establish how the various
documents (cover letter, information sheet, cover sheet and
questionnaire) would be perceived by the person who was likely to open
the package, and as such we targeted questions specifically in these
areas. The cover letter requested participation in the study and
explained what the separate sheets of paper were about; the
information sheet was a summary of the OPAL study with related
details specific to HoMs; the cover sheet checked information regarding
the Trusts/units for which the HOM was responsible, who was likely to
complete the questionnaire and questions specific to the HOM regarding
use of NHS Direct for early labour services; the questionnaire covered
such areas as the background of the Trust, services for women in early
labour, changes to early labour care services and the
monitoring/evaluating of early labour services.
Pilot-study methods
Eight Heads of Midwifery were approached for participation in the pilot
study. They were sent an overall covering letter explaining the purpose of
the pilot, together with copies of the various documents that would be in
the package (as above). Contact was made via their secretaries to
arrange a telephone interview. Telephone interviews, lasting no more
than 20 min, were used to identify problems, for example any questions
that were unclear or ambiguous, response options that were inappropriate
and areas or topics that were missing, and to determine whether the
general flow of questions was appropriate. We also asked specifically
about certain questions in the questionnaire about which there was some
uncertainty, for example the definitions of different models of midwifery
care. Heads of Midwifery were not asked to complete the questionnaire
(as we would wish to include them in the main study) but to read through
it and discuss with the researcher any areas of difficulty or concern.
Pilot-study findings
Seven telephone interviews and one face-to-face discussion were
conducted. The main feedback was that the questionnaire was relatively
straightforward to complete, the instructions in the cover letter were clear
and the general approach was appropriate. Specific areas and questions
were amended; in particular, questions that asked for activity figures (as
percentages) were changed, so that where data were not routinely
collected the respondent could indicate this and offer an estimate. Other
questions had options added or expanded. An additional question
regarding other local services that women in early labour could access

The OPAL study
©NCCSDO 2007 32
was inserted on the advice of respondents. The majority of the
questionnaire remained unchanged.
2.1.4 Main study methods
Data-collection tools
The final format of the survey was as described above: an eight-page
questionnaire (Appendix A), one per maternity unit which could be
completed by a suitable deputy, and a single-page cover sheet (Appendix
B) that each HoM was asked to complete in person. To help distinguish
these two tools, the eight-page questionnaire was printed on mauve
paper and each had a sticker attached specifying the maternity unit that
it concerned. Cover sheets were individually printed on white paper with
“To be completed by the Head of Midwifery Services for <name> Trust” in
red across the top.
These were accompanied by a covering letter that raised the possibility of
subsequent contact for a telephone interview to seek further details of
particular services. Our letter indicated that we would wish to conduct
follow-up interviews with a maximum of 20 HoMs whose units had
reported particular experience of innovation in early labour services (see
below).
2.1.5 Sample size
A total of 163 trusts were identified and the HoM was sent a package
containing a cover sheet (for the HoM to complete) and a mauve
questionnaire (for HoMs or delegates to complete) for each of the units
under that HoM’s jurisdiction. The total number of mauve questionnaires
sent out was 241.
Reminder strategies
To maximise response rates, a number of reminder strategies were
employed. Initially e-mail reminders were sent 3 weeks following the
initial mailout to those HoMs who had not returned the cover sheet. A
second e-mail contact was sent to all HoMs via the Royal College of
Midwives (a co-investigator to the research) thanking them for their
contributions so far and encouraging response. A third e-mail reminder
was sent out 7 weeks following the initial mailout. An additional paper
mailout was sent at this time to those Trusts who had sent back neither a
questionnaire nor a survey cover sheet. In the e-mail reminders HoMs
were given the option of completing the cover sheet and questionnaire via
e-mail. In addition, telephone calls were made to non-responders to
check they had received the initial or second paper mailout and these
were subsequently re-sent by e-mail or post if earlier mailings had not
reached them.

The OPAL study
©NCCSDO 2007 33
Data analysis
The majority of the data collected at this stage were quantitative. In
addition to the quantitative data, the HoMs also provided some qualitative
data in the form of their open responses to survey items and the
explanatory notes offered. These data were coded and analysed
manually, primarily to develop themes to add context to, and increase the
understanding of, the quantitative data. All data were entered into an
SPSS database. Frequencies and cross-tabulations are presented as
appropriate.
Follow-up interviews
Letters were sent to a purposive sample of 17 HoMs selected for follow-up
interviews; HoMs were chosen based on reports of innovative services,
both successful and otherwise. The services that we tried to explore
further included the following:
• triage units that had not been widely reported previously: a
successful one and a discontinued one;
• Birth Centres that provided assessment of all women in that
geographical area regardless of booking for birth;
• Day Assessment Units;
• ‘drop-in’ services;
• units where home assessment of early labour was offered to all
women;
• units that reported risk-assessment strategies;
• a telephone helpline;
• if exploration of the use of NHS Direct had been reported on the
cover sheet;
• discontinued services.
Letters were sent to a purposive sample of HoMs asking if they would be
willing to take part in an interview. In total 17 HoMs were interviewed
during August and September 2005; however, contact with one HoM was
difficult and the interview was finally conducted slightly later. All
interviews were tape-recorded and analysed thematically.
2.2 HoMs England survey findings
This section presents the main findings; additonal tables can be found in
Appendix C. The questionnaire is reproduced as Appendix A. This and the
next section are sub-divided into the following sub-sections: response;
background to Trust and service provision; provision of early labour care;
changes to early labour services; home assessment in early labour; triage
services; additional options for early labour services; recommendations to

The OPAL study
©NCCSDO 2007 34
other HoMs introducing home-/community-based assessments;
recommendations related to the introduction of triage areas and
telephone triage; recommendations relating to additional options for early
labour care.
2.2.1 Response
A total of 145 (89 per cent) Trusts returned data, although the data-set
from some Trusts was incomplete. Two-thirds (110) of Trusts returned
the complete data-set. Cover sheets were returned from 132 HoMs, a
response rate of 81 per cent. Of the 241 questionnaires sent out, a total
of 182 (76 per cent) were returned, representing information on 182
maternity units (including birthing centres and midwifery-led units). Four,
however, were subsequently excluded from the analysis because they did
not pertain to NHS hospitals in England.
Twelve respondents chose to return data by e-mail: five returned a
mauve questionnaire and a cover sheet, five the cover sheet only and two
the questionnaire only. The response rate for returning all questionnaires,
at Trust level, was 73 per cent (119/163), with an additional 7 per cent
(12/163) sending some of their questionnaires back. One-fifth of Trusts
(20 per cent) failed to return any questionnaire. Responses cover the
whole of England, with all areas represented.
2.2.2 Background to Trust and service provision
The following sections provide information related to unit characteristics,
the model of midwifery care in operation and population served.
Characteristics of the units
Table 2.1 Frequencies of the different types of maternity unit in the sample
Type of unit Frequency Percentage
NHS consultant unit including a midwifery-led care area 77 43.3%
NHS consultant unit without a midwifery-led care area 64 36.0%
Stand-alone Birth Centre 32 18.0%
Birth Centre alongside a consultant unit 5 2.8%
Total 178 100.0%
Table 2.1 shows the frequencies of the different types of maternity unit in
the sample. It is very difficult to know to what extent these are
representative of England as a whole, first because such information is
not available in any easily accessible form and second because, as
previous surveys have shown (Smith and Smith, 2005), there is constant
change as units are reconfigured. The number of stand-alone birth units
may appear high, but, cross-referencing against those listed on the

The OPAL study
©NCCSDO 2007 35
website www.babycentre.co.uk/pregnancy/labourandbirth/
planningyourbabysbirth/birthcentre/birthcentresbyregion/ suggests that,
if anything, they are slightly under-represented in our sample. Hospital
and community midwifery services were reported to be managed by the
same Head of Midwifery in 167/178 cases (93.8 per cent).
Table 2.2 Births per annum by unit size
Births per annum Frequency* Percentage Cumulative percentage
<1000 40 (16) 22.5% 22.5%
1001–2000 24 (27) 13.5% 36.0%
2001–3000 49 (56) 27.5% 63.5%
3001–4000 34 (49) 19.1% 82.6%
4001–5000 18 (27) 10.1% 92.7%
>5000 13 (12) 7.3% 100.0%
Total 178 (186) 100.0%
*Figures in parentheses are national figures.
Table 2.2 shows the number of births in units per annum. Again,
comparison with national figures is difficult. The website
www.igreens.org.uk/maternity_unit_mergers_in_the_nh.htm cites figures
which it credits to the Office of National Statistics (ONS) statistics for
2004–2005 (The Information Centre, 2006). The ONS source document
does not in fact present these data as a table and there are some
inaccuracies in the way that data have been extracted. Furthermore, the
ONS does note that ’only a very few Trusts currently provide information
that enables different sites to be distinguished’; in other words, ONS data
are mainly at the Trust level and should not be relied upon as a source of
information about small, individual units. This would appear to be the
explanation for the fact that we received responses from 40 small units
(i.e. <1000 births per annum) when the data given in the ONS report
identify fewer than 20. This under-representation of small units by the
ONS leads to consequent overestimation of the number of births taking
place in some consultant units, making these data of very limited value.
The survey by Smith and Smith (2005), which achieved an excellent
response rate, did not, unfortunately, report data on unit size, and is in
any case now somewhat out of date. It may therefore be that the data
that we present here on small units are unique and the best available at
this time. In view of this, it is worth noting that 90 per cent of the small
units (20.2 per cent of the whole sample) in fact had fewer than 500
births per annum (see Appendix C for details). Thirty-seven of the 40
small units are Birth Centres and three are consultant units, one with
midwifery-led care and two without.

The OPAL study
©NCCSDO 2007 36
Number of category X admissions
Category X is the term used to refer to women admitted to the labour
ward who are not in labour. Such women have been identified as making
a major contribution to labour-ward workload (Ball and Washbrook,
1996). The majority of respondents were unable to supply information
about category X rates or numbers for their unit. Only 10 per cent said
that they knew the figure and an additional 21.3 per cent were prepared
to supply an estimate. This lack of knowledge seems surprising in the
context of the apparently widespread use of Birthrate plus (a maternity
workload-management system). Figures for 2003 were supplied by 39
respondents and for 2004 by 50. The actual figures supplied ranged from
less than 10 per cent to over 100 per cent, with the modal range being
between 10 and 50 per cent. All of those who provided a figure over 100
per cent for either 2003 or 2004 were providing estimates rather than
recorded numbers.
Characteristics of the area and population served
We sought only minimal information from respondents about the
characteristics of the area and the population served because the
questionnaire was already lengthy. The majority of respondents (61.2 per
cent) said that their unit served a mixed urban/rural population, with 27.0
per cent saying ‘mainly urban’ and 11.8 per cent ‘mainly rural’. Further
details concerning the ways in which respondents characterised their
populations are given in Appendix C.
Organisation of local midwifery services
Table 2.3 Predominant organisation of midwifery services
Organisation type Frequency Percentage
Traditional, some rotation 79 44.4%
Traditional, no rotation 32 18.0%
Team midwifery: integrated teams with some core staff in hospital
32 18.0%
Team midwifery+core staff in hospitals 15 8.4%
Team midwifery 8 4.5%
Group-practice midwifery 2 1.1%
Mixed, none predominant 2 1.1%
Caseload midwifery 1 0.6%
Other: mainly community-unit model 7 3.9%
Total 178 100.0%

The OPAL study
©NCCSDO 2007 37
The midwifery workforce can be organized in various ways and it may be
that some of these approaches support particular models of service
provision. This information was, therefore, collected to act as a basic
baseline descriptor and also to support the interpretation of the findings
of the ELSA trial. Thirty-nine respondents gave more than one answer to
this question, for example there may have been different answers for
hospital and community or for different groups of community midwives.
Thirty-one respondents gave two answers and eight gave three.
‘Traditional’ organisation with some rotation was the modal response.
Table 2.3 shows the frequencies of the organisational model that was said
to be predominant.
2.2.3 Provision of early labour care
This section draws on the early labour care section of the questionnaire to
provide descriptive information about the ways in which early labour
services are provided across the country. Home assessment, triage and
additional options for early labour care are each discussed at greater
length in subsequent sections, drawing on both questionnaire and
interview data.
When a woman feels that she may be in labour, where does she
phone?
Given that the focus of the study was early labour, we were particularly
interested to know what variation existed in the first point of contact for a
woman who thinks that she may be in labour. Respondents were
therefore asked ‘When a woman feels that she may be in labour, where
does she phone?’.
Four response options were given:
1 central labour and delivery suite,
2 community midwife/team midwife,
3 triage unit/area,
4 other, please specify.
Birth units have been excluded from this analysis since these options are
not generally applicable and women will generally phone the unit directly.
Two of the remaining 141 respondents gave no answer, seven gave three
answers, and 53 gave two: responses are shown in Table 2.4. Only 8.6
per cent of respondents did not include the central labour and delivery
suite in their answer. Four of these gave community midwife/team
midwife as their first answer and six gave triage.

The OPAL study
©NCCSDO 2007 38
Table 2.4 When a woman feels that she may be in labour, where does she
phone?
Response N Responses (%) Cases (%)
Central labour and delivery suite 127 61.7% 91.4%
Community midwife/team midwife 56 27.2% 40.3%
Triage unit/area 18 8.7% 12.9%
Other, please specify 5 2.4% 3.6%
Total 206 100.0% 148.2%
Multiple responses were allowed. Birth Centres were excluded.
The most common response overall was to say that the central labour and
delivery suite was the default but that some midwives or teams of
midwives gave women the option of phoning them directly. Many of those
giving multiple responses described different mechanisms at different
times of day or for ‘high-risk’ and ‘low-risk’ women. In a small number of
cases respondents specified that there was a ‘hotline number’ so that a
woman had just one phone number that she needed, which would be
routed to different areas at different times of day or dependent upon
staffing.
Table 2.5 When a woman feels that she may be in labour, where does she
phone? by type of unit
Type of unit
Response
NHS consultant unit
including a midwifery-
led care area
NHS consultant unit
without a midwifery-
led care area Total
Central labour and delivery suite
33 (80.5%) 35 (92.1%) 68 (86.1%)
Community midwife/team midwife
1 (2.4%) 3 (7.9%) 4 (5.1%)
Triage unit/area 5 (12.2%) 0 (0.0%) 5 (6.3%)
Other, please specify
2 (4.9%) 0 (0.0%) 2 (2.5%)
Total 41 (100.0%) 38 (100.0%)
83 (100.0%)
This table excludes birth units and is limited to respondents who gave only one
answer.

The OPAL study
©NCCSDO 2007 39
To avoid the ambiguities associated with multiple responses, Table 2.5 is
restricted to those respondents who gave just one answer and cross-
tabulates this with type of unit. Here we can see that NHS consultant
units with midwifery-led care are more likely to designate a point of
contact other than the central labour and delivery suite (χ2=7.96, 3 df,
P<0.05) and that triage as the initial point of contact for all women occurs
only in such units.
Additional facilities available to women in early labour
We were interested to know to what extent changes in the wider NHS
such as walk-in centres, new GP contracts and the spread of new service
models might be having an impact on the services available to women in
early labour. This was an open-ended question with no preset response
options which was answered by 73 respondents (41 per cent). Table 2.6
shows the range of answers given based on post-hoc codings and
indicates a relative dearth of emerging community-based services.
Table 2.6 Additional facilities available to women in early labour
Type of facility Frequency Percentage
Birth Centre/midwifery-led unit 34 19.1%
Hospital-based 24 13.5%
Triage 5 2.8%
Drop in (location unspecified) 4 2.2%
Community drop in 2 1.1%
ELSA 1 0.6%
Sure Start 1 0.6%
Walk-in centre (3 days midwife input) 1 0.6%
Walk-in centres; not used 1 0.6%
Total responding 73 41.0%
Missing 105 59.0%
Total 178 100.0%
In Table 2.6, triage was allocated a separate coding to other hospital-
based facilities to reflect the fact that some triage areas are designated,
separate areas within a maternity unit. However, a few respondents
indicated that women could access community and satellite services or
‘drop in’ at a local Birth Centre, even if planning birth in the consultant
unit. Similarly, others indicated that, for example, the hospital’s Day
Assessment Unit could also be accessed on a drop-in basis. There was
little evidence of midwifery involvement in NHS walk-in centres with
midwifery support reported for only one centre.

The OPAL study
©NCCSDO 2007 40
Cross-tabulation with type of unit confirmed that the response ‘Birth
Centre/midwifery-led unit’ was largely being given by the Birth Centres
with comments indicating that women are welcome to use the Birth
Centre as a drop-in centre, such as ’Women see the Birth Centre as a 24-
hour advice centre either calling in or phoning’ (#73). However, nine
other respondents also gave this answer, including six consultant units.
These tended to be larger units in rural or semi-rural areas where
midwifery-led units were regarded as a community resource for all low-
risk women, not only those planning to give birth there:
Some women can access local birthing units to be assessed if they are low
risk but choose to deliver at main consultant unit.
(#69)
Yes, women may visit their local midwife led units at any time for
advice/guidance on any issue relative to their pregnancies.
(#113)
Early labour advice to low-risk women
Respondents were asked to consider the following scenario: ’A low-risk
nulliparous woman phones at 9 am to say that she has had a show and is
having contractions every 5–7 minutes. Her membranes are intact. She is
not distressed and she has her own transport. What would the midwives
in this unit normally say to her?’
The response options were:
• it’s time you came in now,
• make your way in when you feel ready,
• come in for a check and bring your bag just in case,
• phone again later,
• a midwife will come and visit you at home,
• other, please specify.
Four respondents omitted this question, and 42 gave more than one
answer. Multiple responses are shown in Table 2.7.

The OPAL study
©NCCSDO 2007 41
Table 2.7 Advice in early labour (multiple responses)
Responses
Advice N Percentage
Percentage of cases
It's time you came in now 5 2.3% 2.9%
Make your way in when you feel ready 79 36.6% 45.1%
Come in for a check and bring your bag just in case
9 4.2% 5.1%
Phone again later 89 41.2% 50.9%
A midwife will come and visit you at home
11 5.1% 6.3%
Other 23 10.6% 13.1%
Total 216 100.0% 123.4%
Place of assessment of women in early labour
We were aware of considerable re-configuration currently in progress
including efforts to review non-labouring women outside the labour ward.
Respondents were therefore asked, ’Once a woman has come into the
unit thinking that she may be in labour, where would she be normally be
assessed?’ Response options offered were:
•••• central labour and delivery suite,
•••• midwife-led unit/Birth Centre,
•••• triage room/area,
•••• assessment/admission area,
•••• ante-/postnatal wards,
•••• day care unit,
•••• antenatal clinic,
•••• other, please specify.
As before, we have omitted Birth Centres from this analysis because they
do not generally have the range of options. No respondents omitted this
question; 39 gave more than one answer. Up to four answers were coded.
Table 2.8 shows the responses given (multiple responses). A number of
respondents said that it would depend on the time of day and which areas
were busy. Central labour and delivery suite was the most frequent
response, but it will be seen that a quarter of the sample did not give this
as one of their responses.
Table 2.9 shows these data but coding only the predominant response for
each unit, and cross-tabulates this by type of unit. Overall, nearly one-
third of consultant units were carrying out early labour assessments
predominantly in locations other than the labour ward; units with

The OPAL study
©NCCSDO 2007 42
midwifery-led care areas are somewhat more likely to do this than those
without (39.0 compared with 25.0 per cent).
Table 2.8 Location for early labour assessment (multiple responses, Birth
Centres excluded)
Location Responses
N Percentage Percentage of cases
Central labour and delivery suite 105 54.7% 74.5%
Midwife-led unit/Birth Centre 26 13.5% 18.4%
Triage room/area 20 10.4% 14.2%
Assessment/admission area 16 8.3% 11.3%
Ante-/postnatal wards 12 6.3% 8.5%
Day-care unit 9 4.7% 6.4%
Antenatal clinic 2 1.0% 1.4%
Other 2 1.0% 1.4%
Total 192 100.0% 136.2%
Table 2.9 The usual place for labour assessment by type of unit (Birth
Centres excluded)
Type of unit
Where assessed
NHS consultant
unit including a
midwifery-led
care area
NHS consultant
unit without a
midwifery-led
care area Total
Central labour and delivery suite
47 (61.0%) 48 (75.0%) 95 (67.4%)
Midwife-led unit/Birth Centre
6 (7.8%) 1 (1.6%) 7 (5.0%)
Triage room/area 6 (7.8%) 2 (3.1%) 8 (5.8%)
Assessment/admission area
7 (9.1%) 5 (7.8%) 12 (8.5%)
Ante/postnatal wards 1 (1.3%) 3 (4.7%) 4 (2,8%)
Day-care unit 1 (1.3%) 0 (0.0%) 1 (0.7%)
Other 9 (11.7%) 5 (7.8%) 14 (9.9%)
Total 77 (100%) 64 (100.0%)
141 (100.0%)

The OPAL study
©NCCSDO 2007 43
Advice for women who attend the unit in very early labour
Respondents were asked to consider a second scenario concerning the
advice that would be given to a woman attending the unit in very early
labour.
A low-risk nulliparous woman is assessed in the unit at 9 am. Her
membranes are intact and contractions are every 10–15 minutes. She is
not distressed and she has her own transport. What would midwives in
this unit normally say to her?
The response options offered were:
• you are fine to go home but contact us again when you need to,
• you can go home and a community midwife will come and visit later
in the day,
• you should stay and be reviewed again in a couple of hours,
• other, please specify.
Responses are shown in Table 2.10. It will be seen that very few would
want to keep the woman in the unit and most would advise her to go
home and contact the unit again later.
Table 2.10 Advice for women attending the unit in very early labour
Advice Frequency Percentage
You are fine to go home but contact us again when you need to 154 86.5%
You can go home and a community midwife will come and visit 3 1.7%
You should stay and be reviewed again in a couple of hours 9 5.1%
Other 10 5.6%
Missing 2 1.1%
Total 178 100.0%
Information provided in the explanatory notes indicated that the following
factors would also be considered in offering the woman advice:
• the woman’s wishes,
• findings on vaginal examination,
• geography and distance from unit,
• invitation to contact the unit again,
• whether a home visit could be provided by a community or caseload
midwife.

The OPAL study
©NCCSDO 2007 44
Respondents were then asked, ’If this woman were sent home, what
would she be told about what to do next?’ Response options offered were:
• ring back when contractions feel stronger and 5–10 min apart or if
you experience spontaneous rupture of membranes (SROM), need
pain relief or have any concerns (e.g. blood loss, reduced fetal
movements),
• come in when contractions stronger, and 5–10 min apart, or if you
experience SROM, need pain relief or have any concerns (e.g. blood
loss, reduced fetal movements),
• a midwife will visit you later,
• a midwife will telephone you later,
• other, please specify.
Responses are shown in Table 2.11. Again there is a clear consensus that
the woman would be asked to phone back when labour was more
advanced.
Table 2.11 If this woman were sent home, what would she be told about
what to do next?
Advice Frequency Percentage
Ring back when contractions feel stronger and 5–10 min apart
147 82.6%
Come in when contractions stronger, and 5–10 min apart
24 13.5%
A midwife will visit you later 1 0.6%
A midwife will telephone you later 2 1.1%
Other 2 1.1%
Missing 2 1.1%
Total 178 100.0%
The following question asked, ‘If this woman remained in the unit, where
would she stay?’ The responses offered were:
• ante-/postnatal ward,
• central labour and delivery suite,
• midwife-led unit/Birth Centre,
• triage room/area,
• assessment/admission area,
• other.
Responses are shown in Table 2.12. Three respondents omitted this
question, but 33 gave two or more answers, so multiple responses are
shown. The majority indicate that women would go to an ante-/postnatal
ward, the main exceptions being the Birth Centres.

The OPAL study
©NCCSDO 2007 45
Table 2.12 If this woman remained in the unit, where would she stay?
(multiple responses)
Responses
N Percentage
Percentage of cases
Ante/postnatal ward 116 53.2% 66.3%
Central labour and delivery suite 36 16.5% 20.6%
Midwife-led unit/Birth Centre 45 20.6% 25.7%
Triage room/area 4 1.8% 2.3%
Assessment/admission area 9 4.1% 5.1%
Other 8 3.7% 4.6%
Total 218 100.0% 124.6%
The explanatory notes to this question elaborated that women remaining
in the unit may stay in a number of settings; these include bays
designated for women in early labour, single birthing rooms on the
maternity unit, antenatal or mixed ante- and postnatal wards, the sitting
room or canteen. Respondents indicated that the workload in the unit at
that time would be a significant factor in this decision, although areas that
allowed women to be mobile, have privacy and access to facilities were
identified. Two respondents indicated that there were no antenatal
facilities on their site and that the woman would be asked to return home.
Provision of information to women about early labour care
It might be thought that it will be easier for a unit to implement its early
labour assessment policy if women are aware of it, for example if they
know who they are meant to phone and when. Respondents were
therefore asked how information was provided to women about local
arrangements for early labour care, choosing from a list of options. As
Table 2.13 shows, most respondents gave multiple responses, which
reflects the different services that women may access, for example,
labour-ward tours and antenatal classes, where information will be
repeated. Further analysis showed that 55 units (30.9 per cent) give
women no written information about local arrangements for early labour
care. Of the remainder, 27 (15.1 per cent) cited both the unit booklet and
an information sheet; 72 (40.4 per cent) the unit booklet but no
information sheet and 24 (13.4 per cent) an information sheet but no unit
booklet.
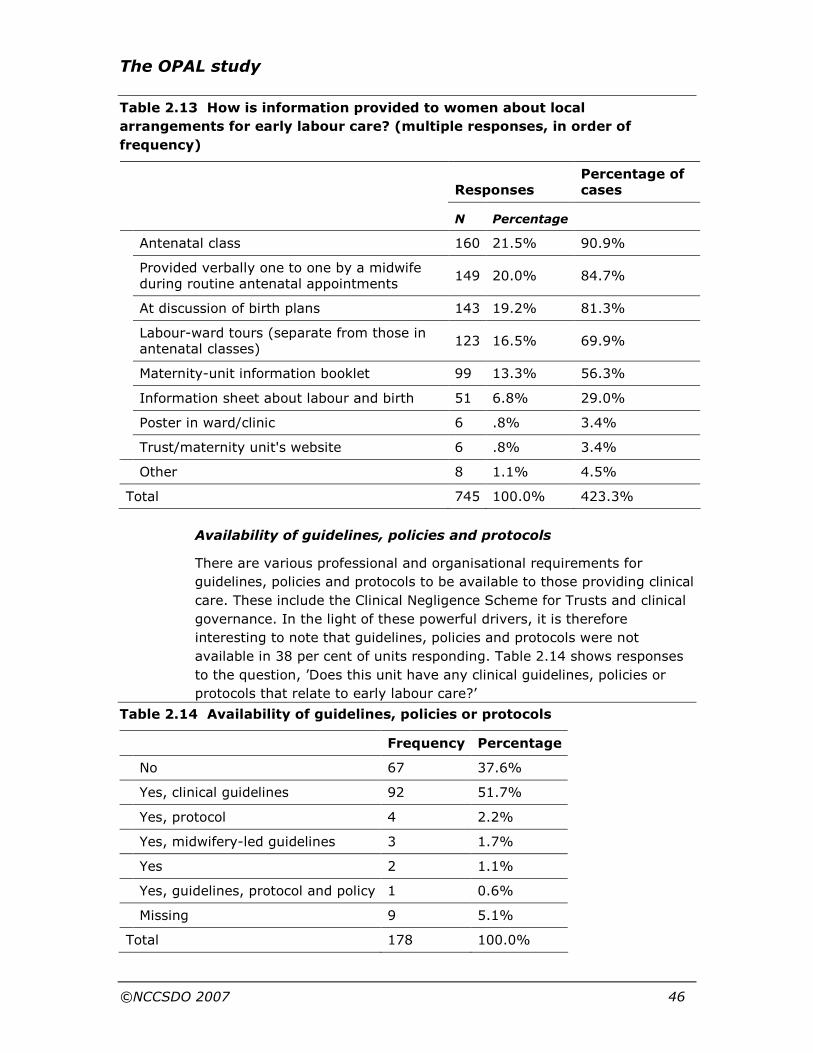
The OPAL study
©NCCSDO 2007 46
Table 2.13 How is information provided to women about local
arrangements for early labour care? (multiple responses, in order of
frequency)
Responses Percentage of cases
N Percentage
Antenatal class 160 21.5% 90.9%
Provided verbally one to one by a midwife during routine antenatal appointments
149 20.0% 84.7%
At discussion of birth plans 143 19.2% 81.3%
Labour-ward tours (separate from those in antenatal classes)
123 16.5% 69.9%
Maternity-unit information booklet 99 13.3% 56.3%
Information sheet about labour and birth 51 6.8% 29.0%
Poster in ward/clinic 6 .8% 3.4%
Trust/maternity unit's website 6 .8% 3.4%
Other 8 1.1% 4.5%
Total 745 100.0% 423.3%
Availability of guidelines, policies and protocols
There are various professional and organisational requirements for
guidelines, policies and protocols to be available to those providing clinical
care. These include the Clinical Negligence Scheme for Trusts and clinical
governance. In the light of these powerful drivers, it is therefore
interesting to note that guidelines, policies and protocols were not
available in 38 per cent of units responding. Table 2.14 shows responses
to the question, ’Does this unit have any clinical guidelines, policies or
protocols that relate to early labour care?’
Table 2.14 Availability of guidelines, policies or protocols
Frequency Percentage
No 67 37.6%
Yes, clinical guidelines 92 51.7%
Yes, protocol 4 2.2%
Yes, midwifery-led guidelines 3 1.7%
Yes 2 1.1%
Yes, guidelines, protocol and policy 1 0.6%
Missing 9 5.1%
Total 178 100.0%

The OPAL study
©NCCSDO 2007 47
Additional information about the guidelines available included use of a
labour pathway, that guidelines were under development, that guidelines
were available but that these were not specific to early labour care and
that NICE guidelines related to the management of pre-labour rupture of
membranes had been implemented.
Copies of guidelines, audits and evaluations were requested and 26
respondents provided documents including parent information leaflets,
care pathway documentation, telephone record proformas, hospital
inpatient episode and Birthrate Plus data. Guideline documents included
incorporation of evidence in the majority provided (12/14) and reference
to national guidance in 50 per cent (e.g. NICE clinical guidelines; 7/14).
One unit’s documentation acknowledged the influence of the Pathway.
Whereas some guidelines for care in normal labour had drawn on other
sources, considerable effort in total appeared to have been expended in
developing Trust or unit-specific guidelines.
Additional methods to provide women with information about local
arrangements for early labour care include the use of videos, the
maternity unit’s own website, information in the maternity record carried
by the woman and at the pre-labour discussion and birth planning around
36 weeks of pregnancy.
Monitoring and evaluation of early labour services
The final section of the questionnaire concerned monitoring and
evaluating early labour services.
Table 2.15 How is use of early labour services routinely monitored?
(multiple responses)
Responses
N Percentage
Percentage of cases
Not routinely monitored 90 33.5% 52.9%
Informally via feedback from user groups or the Maternity Services Liaison Committee
60 22.3% 35.3%
Satisfaction questionnaires to women 58 21.6% 34.1%
Audit 39 14.5% 22.9%
Uptake of service measured 13 4.8% 7.6%
Other 9 3.3% 5.3%
Total 269 100.0% 158.2%
Table 2.15 shows the multiple responses given. Informal feedback from
user groups or the Maternity Services Liaison Committee and satisfaction
questionnaires to women were each reported by over one-third of the
sample. Only 13 respondents (7.6 per cent of the sample) said that
uptake of service was measured and 39 (22.9 per cent) mentioned audit.
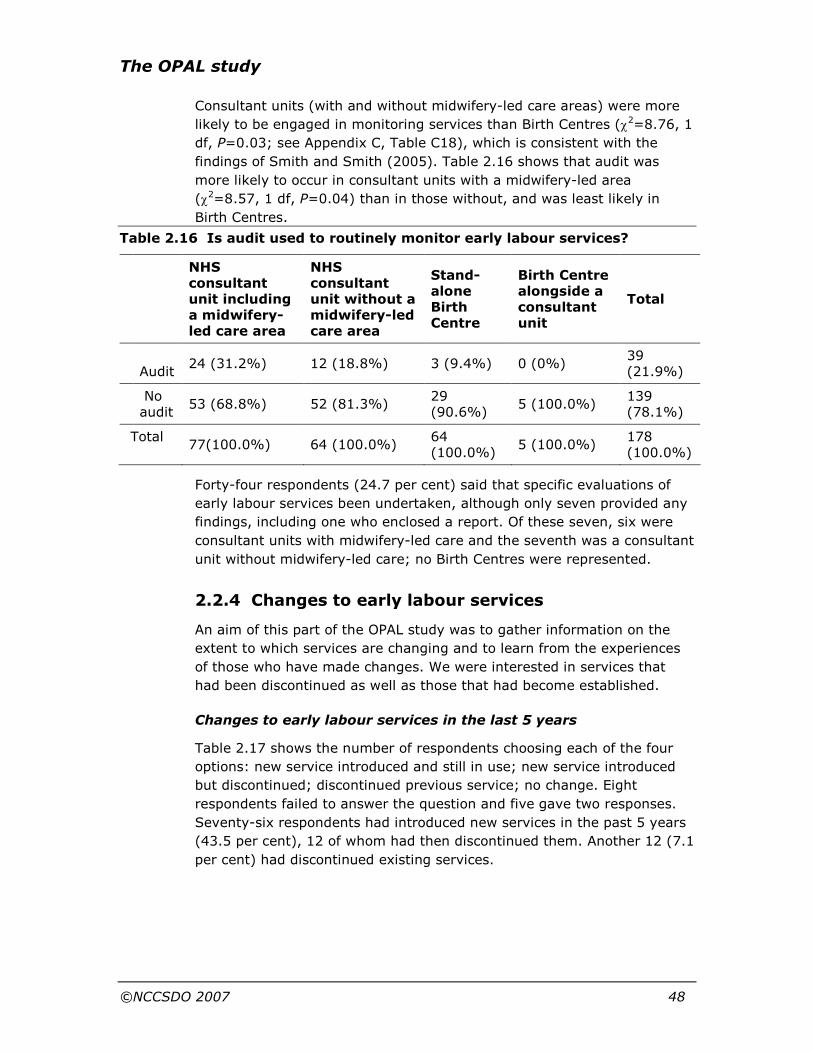
The OPAL study
©NCCSDO 2007 48
Consultant units (with and without midwifery-led care areas) were more
likely to be engaged in monitoring services than Birth Centres (χ2=8.76, 1
df, P=0.03; see Appendix C, Table C18), which is consistent with the
findings of Smith and Smith (2005). Table 2.16 shows that audit was
more likely to occur in consultant units with a midwifery-led area
(χ2=8.57, 1 df, P=0.04) than in those without, and was least likely in
Birth Centres.
Table 2.16 Is audit used to routinely monitor early labour services?
NHS consultant unit including a midwifery-led care area
NHS consultant unit without a midwifery-led care area
Stand-alone Birth Centre
Birth Centre alongside a consultant unit
Total
Audit
24 (31.2%) 12 (18.8%) 3 (9.4%) 0 (0%) 39 (21.9%)
No audit
53 (68.8%) 52 (81.3%) 29 (90.6%)
5 (100.0%) 139 (78.1%)
Total 77(100.0%) 64 (100.0%)
64 (100.0%)
5 (100.0%) 178 (100.0%)
Forty-four respondents (24.7 per cent) said that specific evaluations of
early labour services been undertaken, although only seven provided any
findings, including one who enclosed a report. Of these seven, six were
consultant units with midwifery-led care and the seventh was a consultant
unit without midwifery-led care; no Birth Centres were represented.
2.2.4 Changes to early labour services
An aim of this part of the OPAL study was to gather information on the
extent to which services are changing and to learn from the experiences
of those who have made changes. We were interested in services that
had been discontinued as well as those that had become established.
Changes to early labour services in the last 5 years
Table 2.17 shows the number of respondents choosing each of the four
options: new service introduced and still in use; new service introduced
but discontinued; discontinued previous service; no change. Eight
respondents failed to answer the question and five gave two responses.
Seventy-six respondents had introduced new services in the past 5 years
(43.5 per cent), 12 of whom had then discontinued them. Another 12 (7.1
per cent) had discontinued existing services.

The OPAL study
©NCCSDO 2007 49
Table 2.17 Have there been any changes in your early labour services in the
last 5 years? (multiple responses)
Responses
N Percentage
Percentage of cases
New service introduced and still in use 64 36.6% 37.6%
New service introduced but discontinued
12 6.9% 7.1%
Discontinued previous service 12 6.9% 7.1%
No change 87 49.7% 51.2%
Total 175 100.0% 102.9%
Characteristics of units that had introduced changes
Table 2.18 Service change by type of unit
Service change: yes
Type of unit N Percentage Total
NHS consultant unit including a midwifery-led care area
46 62.2% 74
NHS consultant unit without a midwifery-led care area
25 41.7% 60
Stand-alone Birth Centre 11 35.5% 31
Birth Centre alongside a consultant unit 1 20.0% 5
Total 83 48.8% 170
Table 2.19 Service change by unit size
Service change: yes
Size of unit (births pa) N Percentage Total
<1000 13 33.3% 39
1001–2000 11 47.8% 23
2001–3000 22 46.8% 47
3001–4000 13 40.6% 32
4001–5000 13 76.5% 17
>5000 11 91.7% 12
Total 83 48.8% 170

The OPAL study
©NCCSDO 2007 50
As Table 2.18 shows, the likelihood of changes to early labour services
varied with the type of unit. Change was most frequent in consultant
units with midwifery-led care (62.2 per cent) and least likely in alongside
Birth Centres (18.0 per cent; χ2=10.76, 3 df, P=0.013). Similarly change
was more likely in larger units, as shown in Table 2.19, with all but one of
the largest units (91.7 per cent) having made changes compared with
only one-third of the smallest units (χ2=18.71, 5 df, P=0.002).
Type of service change
Respondents were asked to give details of the service changes that they
had made. These were then grouped into post-hoc codings as shown in
Table 2.20. The first three of these: home assessment, triage and use of
a structured telephone tool, were the main categories to have appeared in
the literature and represent the main possibilities for change specific to
early labour. These will each be discussed in separate sections below. The
remaining categories represent the other answers given. Structural
change refers to changes in organisational structures, for example team
working, which respondents felt had implications for early labour care.
Clinical refers to changes in clinical guidelines which similarly had
implications for early labour care. All but one of the examples coded in
this way concerned guidelines for women with spontaneous rupture of
membranes. A further grouping of responses referred to a change in
policy (not always formalised) to delay admission until a woman was in
established labour. The final grouping referred to changes in local
facilities, such as moving to new premises or the establishment of a Day
Assessment Unit which again had implications for early labour care.
Table 2.20 Details of service changes
New, continuing
New, discontinued
Existing, discontinued
n %* n %* n %*
Home assessment 8 4.5 4 2.2 4 2.2
Triage 15 8.4 2 1.1 - -
Telephone tool 2 1.1 1 0.6 - -
Structural 5 2.8 3 1.7 1 0.6
Clinical (mainly re: SROM)
12 6.7 - - -
-
Policy to delay admission until established
5 2.8 - - -
-
Facility change 9 5.1 2 1.1 6 3.4
Total 56 31.5 12 6.7 11 6.2
*These are percentages of the whole sample.

The OPAL study
©NCCSDO 2007 51
Table 2.20 shows the categories of service which had been newly
introduced and/or discontinued for those respondents who provided
details. Triage was the most frequently introduced service (n=15)
followed by clinical policy changes particularly with regard to spontaneous
rupture of membranes. Home assessment and facility changes were the
most likely services to be discontinued.
Plans for changes to early labour practice in the near future
In addition to questions about services changes that had already
occurred, respondents were asked ‘Do you have plans to make (further)
changes to your early labour assessment and care practices in the near
future?’ Ninety-three respondents, 52.2 per cent of the sample, answered
yes to this question, indicating that early labour services are in a high
state of flux.
Characteristics of units planning changes
As with changes already implemented, consultant units were much more
likely than Birth Centres to be planning changes (χ2=20.06, 3 df,
P<0.001; see Appendix C, Table C14). NHS consultant units without a
midwifery-led care area were the most likely to be planning changes
(71.7 per cent). Similarly, there were statistically significant relationships
with size of unit (χ2=23.82, 5 df, P<0.001; Table C15): small units were
much less likely to be planning changes than medium-sized or large units.
Explanations for this could include the likelihood that small units were
more likely to be purpose-built, both in terms of facilities and model of
care. Additionally, large units appear more likely to experience as a
problem the high proportion of category-X women compared to smaller
units, where a ‘drop-in’ ethos was more frequently reported.
Type of planned service change
Eighty-nine of the 93 respondents who said that they planned service
changes gave details. Responses were coded into the same categories as
above for changes already implemented. Only one was coded per
respondent. Where more than one change was mentioned, priority was
given to those that were specific to early labour (home assessment;
triage; telephone tool) and, within those, to the change with greatest
organisational change implications (home assessment>triage>telephone
tool). Table 2.21 presents these responses alongside the corresponding
figures for service changes already implemented. It will be seen that
more than half as many again are planning changes in the areas of home
assessment, triage, or use of a telephone tool as have already made them
(28.1 compared with 18.0 per cent). These three areas constitute the
majority (56.2 per cent) of the planned changes described. The other
large category was structural change; for example, the introduction of
teams or caseload holding. The categories of clinical guidelines, policy to

The OPAL study
©NCCSDO 2007 52
delay admission until established and facility change were mentioned only
rarely compared to those that had already been implemented.
Table 2.21 Summary of details of service changes implemented and planned
Change introduced (including then discontinued)
Change planned
Service change
N
% of whole sample N % of whole
sample
Home assessment 12 6.7% 19 10.7%
Triage 17 9.6% 25 14.0%
Telephone tool 3 1.7% 6 3.4%
Structural 8 4.5% 26 14.6%
Clinical (mainly re: SROM) 12 6.7% 2 1.1%
Policy to delay admission until established
5 2.8% 1 0.6%
Facility change 11 6.2% 4 2.3%
Other – – 6 3.4%
Total 68 38.2% 89 50.00%
Table 2.22 shows that 27 per cent of the sample (n=48) had both made
changes already and planned further changes. Only 23.6 per cent of the
sample (n=42) said both that they had not made changes and that no
changes were planned, although 9 per cent (n=16) failed to answer one
or both questions. Changes, either implemented or planned, were
reported by 67.4 per cent of the sample (n=120).
Table 2.22 Service changes made by plans to make (further) changes
Q20 Do you have plans to make (further) changes?
Q19 Changes already made Yes No Missing Total
No change 40 (22.5%) 42 (23.6%) 5 (2.8%) 87 (48.9%)
Service change 48 (27.0%) 32 (18.0%) 3 (1.7%) 83 (46.6%)
Missing 5 (2.8%) 0 (0.0%) 3 (1.7%) 8 (4.5%)
Total 93 (52.2%) 74 (41.6%) 11 (6.2%) 178 (100.0%)
Reasons for introduced/planned changes
Details of reasons for service changes are given in Appendix C. ‘Local/unit
based factors’ were cited by nearly two-thirds of the sample. Both ‘service
users’ and ‘implementation of research evidence’ were cited by 43.4 per
cent of the sample. Unfortunately few respondents gave details of the
The OPAL study
©NCCSDO 2007 53
nature of the research evidence that they were implementing although
this might have been local audits or evaluation. The survey was
conducted between April and July in 2005. During that period, Birthrate
Plus, a workforce management tool was widely used by maternity units to
determine casemix and required midwifery staffing establishments. It
might therefore have been expected that Birthrate plus would be cited
more frequently as a reason for making changes.
Advantages and disadvantages of service changes
Respondents were asked to outline the main advantages and
disadvantages of their introduced or planned changes, both for service
providers and service users. Many respondents left some or all of these
blank and, conversely, those answering often gave more than one
response. In addition, many had made, or planned more than one
change, creating ambiguities which made the data less informative than
we had hoped. We will not therefore be presenting these data.
Monitoring service changes
Some 52.5 per cent of those who had made service changes reported
some form of monitoring compared with 42.9 per cent of those who had
not (see Appendix C), although this was not a statistically significant
difference (χ2=1.53, 1 df, P=0.22). Specifically, those who had made
changes were twice as likely to report the use of audit (28.9 compared
with 14.9 per cent), and this difference was statistically significant
(χ2=4.87, 1 df, P=0.03).
Implications of service changes
The final part of this section of the questionnaire asked: “Do any of these
service changes:
• require additional staffing?”
• release staff to other areas?”
• require additional non-staff resources?”
• enable a skill-mix review?”
• release non-staff resources?”
• require staff training?”
• require changes in documentation of care?”
Respondents were asked to indicate ‘yes’, ‘no’ or ‘not sure’ for each.
Despite the ‘not sure’ option, these questions were selectively missed by
many respondents who had reported service changes. Nevertheless, it is
apparent that the early labour service changes undertaken or being
contemplated have many implications. Over one-third of the sample
(n=61) described changes that required additional staffing and 70 (39.3
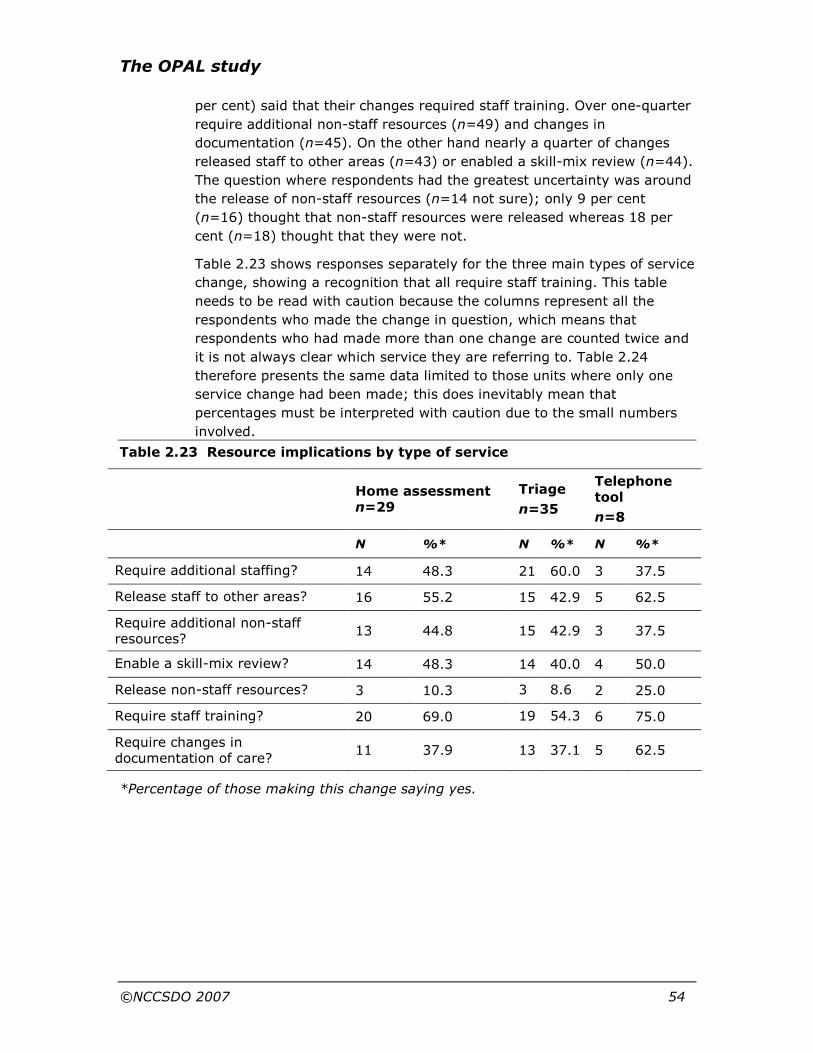
The OPAL study
©NCCSDO 2007 54
per cent) said that their changes required staff training. Over one-quarter
require additional non-staff resources (n=49) and changes in
documentation (n=45). On the other hand nearly a quarter of changes
released staff to other areas (n=43) or enabled a skill-mix review (n=44).
The question where respondents had the greatest uncertainty was around
the release of non-staff resources (n=14 not sure); only 9 per cent
(n=16) thought that non-staff resources were released whereas 18 per
cent (n=18) thought that they were not.
Table 2.23 shows responses separately for the three main types of service
change, showing a recognition that all require staff training. This table
needs to be read with caution because the columns represent all the
respondents who made the change in question, which means that
respondents who had made more than one change are counted twice and
it is not always clear which service they are referring to. Table 2.24
therefore presents the same data limited to those units where only one
service change had been made; this does inevitably mean that
percentages must be interpreted with caution due to the small numbers
involved.
Table 2.23 Resource implications by type of service
Home assessment n=29
Triage
n=35
Telephone tool
n=8
N %* N %* N %*
Require additional staffing? 14 48.3 21 60.0 3 37.5
Release staff to other areas? 16 55.2 15 42.9 5 62.5
Require additional non-staff resources?
13 44.8 15 42.9 3 37.5
Enable a skill-mix review? 14 48.3 14 40.0 4 50.0
Release non-staff resources? 3 10.3 3 8.6 2 25.0
Require staff training? 20 69.0 19 54.3 6 75.0
Require changes in documentation of care?
11 37.9 13 37.1 5 62.5
*Percentage of those making this change saying yes.

The OPAL study
©NCCSDO 2007 55
Table 2.24 Resource implications by type of service, limited to those who
only reported one change
Home assessment
n=14
Triage
n=15
Telephone tool
n=5
N %* N %* N %*
Require additional staffing? 8 57.1 9 60.0 2 40.0
Release staff to other areas? 8 57.1 6 40.0 3 60.0
Require additional non-staff resources?
6 42.9 7 46.7 1 20.0
Enable a skill-mix review? 7 50.0 7 46.7 3 60.0
Release non-staff resources? 3 21.4 1 6.7 1 20.0
Require staff training? 11 78.6 9 60.0 3 60.0
Require changes in documentation of care?
5 35.7 6 40.0 3 60.0
*Percentage of those making this change saying yes.
2.2.5 Home assessment in early labour
Home assessment in early labour is the intervention being investigated in
the ELSA trial. We were therefore particularly interested in knowing how
widespread this was in current practice, the characteristics of units
offering home assessment and the issues that had been encountered.
Availability
Table 2.25 shows the reported availability of home assessment in early
labour. Seven units (3.9 per cent) were offering home visits routinely to
all, 24 h a day, and a further 79 (44.4 per cent) said that they offered it
selectively.
Table 2.25 Availability of home assessment in early labour
Frequency Percentage
Offered selectively 79 44.4%
Routinely offered to all, 24 h/day 7 3.9%
Not available/only for home births/DOMINO 92 51.7%
Total 178 100.0%

The OPAL study
©NCCSDO 2007 56
Characteristics of units offering home visits to all
Home visiting was not associated with a particular type of unit but there
were some relationships with unit size. While selective home visiting was
found in units of all sizes, universal visiting did not occur in larger units.
Selective home visiting was also distributed across the range of ways in
which midwifery services were organised but six of the seven units
offering universal visiting were organised in teams. Surprisingly, the only
unit whose predominant form of organisation was described as the
caseload type did not offer home visits.
Criteria for selective home visiting
Respondents who indicated that home visiting was selective were asked
to expand on this by indicating which of a list of determinants applied.
Responses are shown in Table 2.26. The most frequently endorsed
response was that it was up to individual midwives, and over a third also
mentioned differences in the practice of different midwifery teams. The
most frequently mentioned formal limit on home visits was time of day
(i.e. daytime only), but limits to women at low obstetric risk were also
frequently mentioned. As will be seen from the table, many respondents
gave more than one response; for example, it might be the up to the
individual community midwife, but only during daylight hours.
Table 2.26 Criteria for selective home visiting (multiple responses)
Responses
Criterion n % of responses % of cases
Time of day 32 19.8% 42.1%
Distance 16 9.9% 21.1%
'Obstetric risk' 29 17.9% 38.2%
Parity 4 2.5% 5.3%
Variation between individual midwives 40 24.7% 52.6%
Variation between teams 26 16.0% 34.2%
Other 15 9.3% 19.7%
Total 162 100.0% 213.2%
Some respondents indicated that home assessment was available in parts
of their service – ‘some teams do it’ – but that it was not offered routinely
due to resource constraints.
Percentage of women having early labour assessment at home
Respondents were asked ’Do you know approximately what percentage of
women have early labour assessment at home, excluding women booked
for home births?’ Responses offered were yes; no, but I can provide an

The OPAL study
©NCCSDO 2007 57
estimate; and no. Seventy-five respondents (42 per cent) failed to
answer this question. These were primarily the units where home visiting
was not available, but also included one unit that offered it selectively and
eight where home visits were only available for home births and
DOMINOs. Eleven respondents who said that their unit did not offer home
visits did answer the question in order to tell us that the answer was zero.
Over two-thirds of those responding (68.9 per cent), said that they did
not know the percentage of women receiving a home visit. Only six
respondents (5.8 per cent) said that they did know, the remaining 26
(25.2 per cent) saying that they could provide an estimate. Knowing the
percentage did not appear to be related to the basis on which home
visiting was offered.
The next question asked for the actual figure, whether known or
estimated, and this was answered by 32 respondents: of the six who had
said ‘yes’ they knew the percentage, three gave the answer zero, the
remaining three offering 10, 46 and 50 per cent. Of the 26 respondents
offering an estimate, 15 suggested 5 per cent or less, with the remainder
offering estimates ranging from 6 to 95 per cent. As might be expected,
the highest estimates were from units who offer a 24-h service to all, and
all the respondents answering 10 per cent or less were offering a selective
service or none at all except for home births and DOMINOs. However,
those offering a selective service clearly covered a wide range of
possibilities with the figures offered ranging from 1 to 46 per cent.
Returning to the explanations given for the basis for selective home
visiting revealed very little pattern to explain the range. The two
‘selective’ units that were apparently visiting a substantial number of
women (#79, #106) said that visits were offered to low-risk women, and
mentioned no time or other constraints. Respondents who said that home
visits were only available at certain times often offered other constraints
as well, and tended to report only a small percentage of women receiving
home visits.
Cross-tabulation by size of unit indicates that it tends to be smaller units
who visit a high percentage of women: all five of the units that were
visiting 60 per cent or more had fewer than 2000 births per annum. This
is in keeping with the finding that offering home visits to all tends to be
less prevalent in larger units. However, those units where only a small
percentage of women were visited were spread across the size spectrum.
Discontinuation of previous home visiting
Eight respondents reported discontinuation, or reduction, of home
assessment for early labour. These are summarised below.

The OPAL study
©NCCSDO 2007 58
Table 2.27 Units which discontinued or reduced existing home assessment
Ref Type of unit
Unit size
Midwifery organisation
Type of area
Additional information
#31
Consultant unit, with no midwifery-led care area
4001–5000
Traditional, some rotation
Mix of urban/rural
Team midwives had previously provided home assessment and subsequently accompanied labouring women into the unit. Now selectively 9 am–5 pm and further service changes planned.
#33
Consultant unit, with midwifery-led care area
2001–3000
Traditional, no rotation
Mix of urban/rural
Home assessments had been offered to all in team midwifery scheme which had been discontinued. Now selectively 9 am–5 pm. Planned to move towards community-based assessments in two Birth Centres.
#152
Consultant unit, with midwifery-led care area
2001–3000
Team midwifery - integrated teams _ some cores staff in hosp
Mainly urban
Universal home visiting discontinued due to staffing difficulties, now selective. Exploring triage.
#164
Consultant unit, with midwifery-led care area
2001–3000
Traditional, no rotation
Mainly urban
Home assessment had been offered as part of DOMINO service, which had been discontinued due to funding constraints and concerns for midwives’ security when doing home visits at night. Now offered selectively (9 am–5.30 pm).

The OPAL study
©NCCSDO 2007 59
Table 2.28 Units which introduced home assessment and then discontinued
or reduced
Ref Type of unit
Unit size
Midwifery organisation
Type of area Comments
#32
Consultant unit, with no midwifery-led care area
1001–2000
Team midwifery: integrated teams, some cores staff in hospital
Mix of urban/rural
One team had previously provided home assessments but this had been discontinued.
#62
Consultant unit, with midwifery-led care area
3001–4000
Team midwifery Mix of urban/rural
Home assessment had previously been offered by a community team but this had been discontinued.
#101
Consultant unit, with midwifery-led care area
>5000
Team midwifery: integrated teams, some cores staff in hospital
Mix of urban/rural
Selective home assessment offered; would prefer universal but could not due to a need for increased staffing that was unavailable due to resource pressures.
#160
Consultant unit, with midwifery-led care area
2001–3000
Traditional, some rotation
Mix of urban/rural
Team midwives had previously provided home assessment but the teams had been disbanded as it was considered that they were not working.
One other unit had tried to provide home assessment in early labour
(#118) in one of the urban areas within its large geographical catchment.
It had subsequently been discontinued because caseloads were too heavy
to sustain this. The HoM felt that caseload size was a key determinant of
whether home visits could be provided during early labour and reported
that despite official discontinuation, some women would still telephone
their community midwife directly, who may offer home assessment if time
permits. Women booked to give birth in that unit could consult their
community midwife about early labour at the end of the midwife’s
antenatal clinics, but this was an ad-hoc arrangement.

The OPAL study
©NCCSDO 2007 60
Home- or community-based assessment in early labour: interview
data
Interviews with five senior midwives provided additional information
about home- or community-based assessments during early labour.
Home visiting during early labour had been available for some time at one
unit (#114); this unit also tries to offer a labour discussion around 36
weeks of pregnancy:
Pre-birth visits are made to give more details and discuss options for
labour at around 36 weeks. The partner may or may not be present; it is
not arranged specifically so that the partner is present. It means women
have a better idea of what is going to happen, it helps clarify for low-risk
women that they can chose home birth if they want to but they don’t have
to decide until they are in early labour. We do get some women who have
already made their mind up but we encourage them not to make their mind
up until they are in labour…. Our home birth rate is 11 per cent. The impact
of home assessment is not necessarily keeping women at home longer, it is
more that we get those who hadn’t thought about home birth deciding to
stay at home to birth.
(#114)
Another senior midwife indicated that all women were offered home visits
and that feedback from women about this service was very positive. This
unit was also planning a triage facility and modifying the Pathway for local
use. The advice of this senior midwife was to involve midwives in the
change process and to consider their job satisfaction. This unit served a
predominantly rural area and was also exploring the involvement of MCAs
in early labour support.
We introduced offering home assessment to all women in the last
6 months. We have changed our model of care from traditional to
integrated approach. Currently we are running at approximately 75 per
cent of women having home assessment, it is not 100 per cent due to
cross-border areas. If a woman has not received a home assessment it is
discussed in professional forum, why not? The managers are very keen,
and women like it, as do most of the midwives…. We are wanting to get
MCAs trained to NVQ level 3 so that there can be one MCA per team, we
want to get them out to home assessments with the team midwife, with the
possibility of leaving the MCA with the woman in early labour for the team
midwife to return later, but we are checking on the legality of this. The
midwife accompanies the woman to hospital in labour and stays with
her…
We are now getting lots of letters from women who were very positive
about their experiences of home assessment.
(#153)
Home assessment in early labour was also provided by midwives working
in group practices that provided care to a multi-racial population in an
urban area (#60). This Head of Midwifery described the provision of early

The OPAL study
©NCCSDO 2007 61
labour services and also beneficial impacts on students’ learning
experience:
Group practices cover around 35 per cent of the population. We have eight
in total, three of which are close to caseload, five to six community
midwives work with a caseload total. Out of the eight group practices,
those that work best are the individual caseloading, with 40 women per
community midwife. Women are more likely to stay at home in group
practices…. Home assessment is only available to those women in group
practices…. Group practices are based on geography and social need,
occurring in more deprived/high-social-need areas…
Also, at 36 weeks, each community midwife has a birth talk with the
woman and partner, so that they are both clear about the onset of labour,
they know that it’s Ok to phone the community midwife as often as they
need to, and it is Ok to stay at home. The birth talk was developed by the
community midwives…. Our home birth rate is 8 per cent....
The main impact on staff training is that students working with community
midwives in group practices see positive systems for advice and
communication.
(#60)
Another respondent (#126) reported an integrated team midwifery
approach operating in conjunction with a Birth Centre. This service
provided home visiting in early labour and was involving MCAs in the
support for women in early labour:
The team midwifery service was started in June and is attached to the
Birth Centre. There are two teams and each midwife is attached to a GP
practice. Women in early labour will phone the unit or community
midwives, they are offered a home assessment, now available during the
night, or to come into the unit for assessment. If they are in early labour
they go home, it depends on the time span. If they go home we phone them
back or they can come in…. All midwifery care assistants work in pairs;
they have training in all areas and are more involved than in the past.
They are involved with women in early labour but are not responsible for
them. Since team midwifery, there has been an increase in admissions to
the Birth Centre, women are more likely to change to the Birth Centre from
consultant-led unit…. It is formally on offer to have a home assessment
whereas we previously offered women to come in. Now, we say they can
have a home assessment and in most cases that happens. Women are
staying at home for longer in early labour….
The changes to home assessment were introduced as part of the change to
team midwifery, and also we were struggling to cover a midwife at night in
the Birth Centre. We have two MCAs manning the Birth Centre, and from
7.45 am to 9 pm there is a midwife present. Out of these hours there is an
on-call midwife who comes in when needed. We have needed the backing
of the MCAs; they are there caring for the postnatal women.
(#126)
One Trust was at the point of change and considering community-based
changes including team midwifery, exploring assessment at community

The OPAL study
©NCCSDO 2007 62
clinics and introducing a Care Pathway. There was currently no home
assessment of women in early labour.
It’s the logistics in relation to 110 square miles of community area, a lot is
rural. If a woman is to be assessed, it is better to set up an assessment
centre at a health centre and aim for a woman to be assessed at the health
centre rather than the midwife travel great distances. It is about being cost-
effective, if it’s in a health centre that the majority of women can get to (not
necessarily on public transport), we would be able to see more there. We
have not done feasibility studies with the PCTs yet to see which health
centres could be used. It could be in community centres. There would be no
scanning facilities but it would be closer to women in their community and
may be able to reach and engage with women who are less likely to get
into antenatal services. There are some rooms in new children centres….
(#31)
2.2.6 Triage services
Introducing triage areas
Heads of Midwifery or their designated deputies were interviewed from
two sites that identified introduction of triage areas in their questionnaire
responses (#4, #28). One unit (#4) was part of a Trust that provided
maternity services on two sites, the other was a single-site Trust. Both
were large units (approximately 4500 births per annum) serving a mixed
rural and urban population. The introduction of these triage areas had
been prompted by use of the Birthrate Plus workload-management
system and the numbers of admissions to delivery suite of women found
not to be in labour who were described as ’crippling the delivery suite’
and ’fragmenting service’.
The monthly birth rate at [unit] is approximately 370, but we always found
nearly 1000 visiting labour ward.
(#4)
In both cases the triage initiative was led by the interviewee (not
necessarily a HoM), one of whom had experience of introducing triage in a
previous post and the other a consultant midwife. Both respondents
recounted the need to ‘sell’ the idea of triage to other members of staff,
including midwives, doctors and managers:
People did need a lot of convincing.
(#28)
Both interviewees described a specific, dedicated area for triage although
the size, location, staffing establishment and facilities varied
considerably: one is a six-bedded daycare ‘ward’ in the antenatal services
area (#28) where the beds can be used when daycare closes (7 pm–8
am), and a triage-dedicated couch and recliner chair plus any vacant beds
during daycare opening hours (8 am–7 pm); the other (#4) is located in

The OPAL study
©NCCSDO 2007 63
an area built as a recovery area near theatres (with its own entrance
away from the labour ward and a seating area). One unit has five
dedicated staff (wte) employed in addition to the labour-ward staff with
one midwife and one support worker per shift (#28) and is now open 24 h
a day, 7 days a week (initially hours were limited to 12 h/day). In the
other Trust, a team of three dedicated staff was deployed from the
delivery suite without any apparent problem (#4), which enables staff to
move between delivery suite and triage. This rotation between areas,
which was viewed as ’healthy – not feeling too embedded‘ (#4), was
staffed by one midwife per shift and open between 9 am and midnight.
Lack of funding prevented the availability of a 24-h service.
The triage area quickly made an impact in both cases:
Within a month the midwives suddenly recognised that the labour-ward
activity was much more manageable. And when triage isn’t working it feels
manic…. We are now at 60 per cent seen by midwife only in triage.
(#4)
It’s gone fantastically well, it’s got all the activity off delivery suite, the
women know they are there so if they’ve got a problem in the middle of the
night, we have extended it so we deal with postnatal problems via the
telephone during the night as well, so the community midwives aren’t
disturbed…women waking up in the night can come in and get checked
over, there is a lot of telephone triaging goes on, our admission to our
inpatient ward hasn’t increased, our ratio of women attending triage and
going home is very high. We worked out that midwives spent 40-odd hours
last week just on the telephone triaging. It’s keeping women away from the
hospital that aren’t needing to come.
(#28)
Telephone triage is part of the remit of the triage area; this is seen to
take a considerable workload from the delivery suite; a specific phone
number is given for the 24-h triage service. Not all women who telephone
the triage area will subsequently attend, but having a dedicated person to
call back later was seen as helpful:
It seems to be quite nice for women if the midwife says ‘I’m on duty until 5
o’clock, call me again if something has changed or you want a chat’ and
that seems to work really well.
(#4)
However, at unit 28, if a woman phones a second time after remaining at
home after the first call, she would be encouraged to attend:
…because she is obviously not comfortable … and we need to see her. And
often it’s reassurance they need really.
(#28)
At both sites, triage is available to all women but there are clear
guidelines and criteria as to those who cannot be seen there, for example,

The OPAL study
©NCCSDO 2007 64
women at high obstetric risk or in established labour (#4), women
complaining of severe headache, blurred vision, haemorrhage, who have
collapsed or who are contracting every 2 min (#28).
The ability of the triage midwife to make decisions, both on the phone
and in the triage area, is vital to the smooth running and success of the
triage area and delivery suite:
you know … if a woman’s in labour on the phone, and that’s getting better
and better because the girls are so skilled at it now…. So the women on
delivery suite are the labourers or the ones that need to be there, the rest
are in triage.
(#28)
In addition, the triage midwife has a key role in training:
And she is a great teacher … she has a team of midwives who work with
her … and there is good teaching and hand over to them all…. We try and
get student midwives to work in there as it’s a good opportunity for them to
do decision-making and just to see the sort of queries that women have.
(#4)
Introducing a triage service also had an impact on overall training, in the
long term as well as the short term:
There has been a positive impact on training, [antenatal services] they are
no longer the Cinderella of the service, having the triage makes everyone
aware of the need to update, get training, improve skills, etc., whereas
before antenatal services wouldn’t have thought about doing that…. It had
implications with midwives doing something completely new, something
they had not thought of before. Some had done triage over the phone on
delivery suite but the easiest thing was to tell them to come in because
they had not got the time to sit and listen to them. Midwives are not just
fire-fighting on the phone, as they might have done on delivery suite; the
skill is to tease out the important stuff. We need to train, get the midwives
into a different way of thinking. For me, the training was about the triage
tool and getting the right triggers to ask. Triage is far better now, a year on.
(#28)
Documenting the care provided in triage is seen as important, but it was
suggested that appropriate documentation can be developed over time
and should not be seen as a barrier to initially implementing change:
There is no formal tool or documentation. The midwife makes notes … but
since I changed notes and records already since being in post and after
two Trusts merged, so to give them another piece of paper seemed a bit
mean. I am hoping that midwives will come up with the solution
themselves, they think that documentation would be really helpful if we
had x, y, z. It’s more important to get the service started and the midwives
confident to be looking after the women, the documentation can come later.
(#4)
Introducing the triage services had not been without teething problems.

The OPAL study
©NCCSDO 2007 65
Women were used to phoning delivery suite direct. We initially had to offer
a two-tier service, some women just turned up on delivery suite whilst
others came through triage.
(#28)
If there is no-one in triage, or it’s quiet, triage can get hijacked by day-unit
activity, which is always a problem with maternity services, we need to
mix and match a bit.
(#4)
Staffing one unit overnight had also proved a challenge, but had been
overcome:
…I think it’s [triage] had too much of a positive effect to stop but if you had
asked me 3 months ago I might have said ‘I don’t know’. I thought 3
months ago that the 24-h opening was creasing us, there was a lot of
sickness initially because people didn’t want to work the nights, but I’ve
managed those with sickness problems and they are now in there doing
the nights. I am confident now that if we can keep the staff numbers in
there that we can keep it open as a viable option.
(#28)
Overall, the introduction of triage in these two Trusts had been positive
and the long-term commitment to it was clearly evident. One positive
aspect that both interviewees reported was that they were much closer
now, after the introduction of triage, to achieving the desired one-to-one
ratio in providing care for women in established labour.
Factors associated with discontinuation of triage units
Some respondents interviewed reported only very short trials of triage
units or areas (two for less than 1 week each). In those units who had
discontinued triage (#118, #149) this was attributed primarily to a failure
to convey the philosophy and aims of a triage area to staff, leading to a
lack of support and rejection by delivery-suite staff (#118, #149);
location of triage in an area that subsequently was confirmed as
inappropriate (#118, #149); a feeling that delivery-suite midwives had
less control over the area and workload (#118); and misunderstanding of
the role of the triage midwife, who was viewed only in terms of being
taken off the delivery suite (#118, #149) rather than as seeing women
who would otherwise have required labour-suite assessment. A further
problem related to staff working in isolation at night, albeit only a short
distance away from another clinical area (#149).
There was no space on delivery suite for a triage system. The floor above
had a gynae day-case ward. We knew that triage patients usually came
after 5 pm (if they came in the day they would come to the Fetal and
Maternal Assessment Unit). As gynae day unit closed at 5 pm, we thought
we’d use their space for triage from 5 pm–7.15 am. We just looked at
patients and sent them home. It was very successful but the main problem
was location, the midwife was based upstairs on her own (and overnight),
The OPAL study
©NCCSDO 2007 66
the lone worker issue. There was also the problem of taking a midwife
away from delivery suite – reducing core staff on delivery suite. We ran it
for a week on the gynae day-case ward. We saw 56 patients. Two were in
labour, the rest were not, so there were a lot of women not going onto
delivery suite that otherwise would have.
(#149)
Sisters on the labour ward felt they didn’t have control over it, they didn’t
know who was coming in so it was abandoned … after less than a week.
A lot of it was cultural, the way they are used to working. There are a lot of
staff that have been here a long time so any change we implement is
usually fraught with challenges.
(#118)
Despite being a success in terms of the number of women seen and
‘removed’ from delivery-suite activity, there remained a problem in terms
of understanding the role of the triage midwife by the delivery-suite staff:
There were no problems selling the idea of triage – midwives were behind
the idea. Nine team leaders have been to see other units and had brought
back ideas, etc. It was an easy thing for us to do it was just using the day-
case ward upstairs….
The midwife who went and staffed it thought it was a great little job just
seeing all the antenatal admissions all night. But the other midwives on
the delivery suite were a bit peeved because it was depleting the staff on
delivery suite and we are a very busy unit with a lot of high-risk women.
(#149)
This demonstrates the importance of making sure the staff on delivery
suite are fully prepared for, and informed about, the implementation of
triage, as well as the ideas or philosophy behind it. Furthermore, the
triage midwife needs to be fully aware and confident in her role if triage is
to work:
To us, we felt that we got a lot of women home that would otherwise have
been admitted by the [Senior House Officer], and you have got to have
senior, confident midwives who can make the decision that the patient is
fine and can go straight home.
(#149)
The importance of staff acceptance and location were major factors in the
discontinuation of triage (#118):
Introduced 2–3 years ago, after we looked at audit of category X on labour
ward – we tried to take it away from labour ward, but because it’s a
purpose-built unit now (only 12 years old) there was no capacity/arranged
area for triage. We tried to use existing rooms – triage area in a four-bed
room on ante-/postnatal ward (attached to day room) also with single room
attached. Staff didn’t like it because it was away from labour ward, even
though on the same floor…. It was more difficult to relocate staff if they are
not busy…. There was a six-bedded ward for early labourers on an
interconnecting room next to labour ward and antenatal/postnatal ward.

The OPAL study
©NCCSDO 2007 67
(#118)
A number of factors prevented establishment of triage units elsewhere;
these included financial constraints at Trust level (proposed mergers, and
possible change of location, cost of adapting existing buildings) and
staffing costs (deployment of a health care assistant to address the lone-
worker issue). However, there was a balance to be reached:
You’ve got to weigh up how many would be seen in triage versus how
many would have been seen on delivery suite and sent home anyway.
(#149)
In one unit, it appears that little positive impact on workload was
perceived. This became apparent as, following an audit, it was felt that
many of the women seen in a triage area within the delivery suite could
actually be seen in the Early Pregnancy/Fetal Assessment Unit (EPFAU).
This unit planned to extend the times when EPFAU was open to
incorporate triage activity (#40), together with a policy of active
encouragement to women found not to be in labour to return home.
Telephone triage
Telephone triage has been introduced in a number of Trusts, although for
many it was a case of formalising and documenting what was already
taking place in telephone conversations between women and midwives. In
one Trust (#1), a comprehensive telephone triage tool was used
extensively at each possible point of contact with a woman in early
labour: maternal fetal assessment unit, delivery suite, midwife-led
birthing unit and with community midwives. For some Trusts, telephone
triage accompanied the introduction of on-site triage, where a dedicated
midwife would handle all calls. Reasons for introducing telephone triage
included high numbers of category-X women, prevention of BBAs (born
before arrival), standardising advice/training tool for staff answering the
telephone and clinical risk management.
One unit had introduced a telephone triage approach in 2005, where a
senior labour-ward midwife uses a locally developed protocol and specific
documentation for giving women advice related to early labour. This had
been instigated to increase the use of clinical judgment, achieve more
consistent advice and formalise the process for telephone calls. Specific
documentation was developed to support this and, again, this was seen
as supportive for the training of junior midwives. A review of the number
of women attending delivery suite was anticipated at the time of
interview. Institution of the telephone triage system was not perceived to
have any effect on staffing levels, allocation or use of non-staff resources
(#142).
In the past there had been occasions of ward clerks giving out advice over
the phone and junior midwives were uncertain as to what to say. There
was a tendency for allowing women to come in without using much clinical
The OPAL study
©NCCSDO 2007 68
judgement. We wanted to take steps to formalise how phone calls were
handled and as an aid for training.
(#142)
We are all giving phone advice now but in the past different midwives gave
different advice (for example, junior midwives versus senior midwives) and
we needed to standardise it. It is also useful for tracing calls, and advice
given out in case anything untoward happened – for example, if it is
suggested a woman calls back but they don’t and something went wrong
we have got the evidence that the woman had been asked to call. It’s
really for the protection of midwives as much as anything, as well as
standardising the advice so that all women get the same advice … one of
the reasons why we introduced the phone advice/assessment tool was
that a patient had said she had phoned up and said she was told
something by the midwife and the midwife denied it. But it’s your word
against theirs.
(#149)
In another Trust, it was noted that the PCT had an impact on a change in
practice, which has resulted in other areas of maternity care being
reviewed:
The PCT are interested in reducing unnecessary admissions, we are now
undertaking a maternity services review with the PCT, it is likely that we
will increase the hours of the Day Assessment Unit (currently used for
postnatal, reduced fetal movement, hypertension, etc.) and increase the
numbers going through there, together with any community-based
changes.
(#142)
Telephone triage was involved, but was not necessarily the focus, of
changes to practice in two Trusts interviewed. One Trust (#116) had
introduced a policy of telephone advice to stay at home, coupled with
sending women home in early labour. This approach was introduced for
two reasons: the HoM had previously worked within a team midwifery
system and was used to dealing with women over the phone, women only
going into hospital when their labour was well-established and also
because there was a need to use the beds differently:
I found it very strange that all these women were being admitted that
didn’t need to be there, as did some of other staff, and coincidentally we
needed to use the beds in a different way.
(#116)
Another Trust (#149) had introduced an information sheet for women
encouraging them to stay at home together with sending women home in
early labour and structured telephone advice or telephone triage. The
information sheet was developed in-house by the delivery-suite policy
team:
We were looking at the sort of things we wanted to tell them without
putting them off coming in altogether. We don’t want them to feel they are a

The OPAL study
©NCCSDO 2007 69
nuisance to us but obviously if they do come in too early they get interfered
with far too much…. We try and send or encourage most women in early
labour to go home. We actually say to them, even if, if they are not keen
and we are trying to get them to go home for their own benefit, we’ll say to
them ‘go home for 4 hours and then come back and I’ll check you over.’ So
we do send them home and ask them to come back later.
(#149)
However, there is reluctance on the part of some midwives to encourage
women to go home in early labour:
If you put it to the women that ‘you are in very early labour, you could go
another few hours like this, yes you can stop in hospital but you are going
to be much better off at home in the comfort of your own home’. And it’s the
confidence of the midwives, having the confidence to say that to the
patient, they get worried that they send them home and they’ll come back
at 6 cm they will be in trouble, but to me, that’s a success … that’s why I’m
saying to them to ask them to come back in 4 h, we’re trying it step by
step.
(#149)
With sufficient training and support, however, this reluctance or lack of
confidence can be overcome:
We have had to put in training for the staff. In a sense, it’s almost giving
them the permission to make that decision. It’s gone really well. At first
some of the staff were a bit reticent about doing it but now it’s become the
accepted norm. The labour-ward manager did informal training with staff,
encouraged it and acted as a role model and got the other team leaders to
act as role models as well to encourage the other staff to do this…. Initially
some people found it easier to take the plunge and send people home or
encourage them not to come in, but it seems now to be accepted practice.
(#116)
Documentation for telephone triage or telephone assessment tools is in
use in many Trusts; some has been newly devised and some has been
adapted from existing paperwork. All has been developed in-house, and a
few with some reference to the evidence-base or to the All-Wales
Pathway. In some cases guidelines are used in tandem but these are
often not specific to early labour.
The document is used to help make decisions, there are now more
questions that have to be checked off, originally it was just three boxes, but
now much more. It was developed in-house…. Guidelines are available for
established labour and problems in pregnancy (with some evidence-based
components) but none specific to early labour.
(#83)
None of the HoMs interviewed reported auditing to determine, for
example, any reduction in numbers or stage of admission of women to
the labour ward but there was a general feeling that the implementation
of telephone triage had been positive, with other notable impacts:

The OPAL study
©NCCSDO 2007 70
I think it’s part of trying to keep birth normal and we are pushing that, that
it’s very much a normal event for low-dependency women. But equally a
normal event for high-dependency women … we don’t treat them as people
on the end of a machine. So it fits in with that whole philosophy. Our
epidural rate is 14 per cent ... but it’s partly the culture here, whether
people coming in later that’s had an impact on it we don’t know, we’ve not
studied it.
(#116)
Numbers assessed in triage or other separate area
Less than a quarter of the respondents knew the approximate percentage
of women assessed in a triage or separate assessment/admission area in
their unit (see Appendix C). Among the 54 respondents who could provide
an answer or an estimate the modal response was in fact zero (n=29).
For the 22 giving a non-zero response, the range was very wide (2–100
per cent). Despite the significant amount of change in early labour
services, with only few exceptions, there was relatively little data
reported on the proportion of women assessed in triage areas.
2.2.7 Additional options for early labour services
In the interviews, some senior midwives reported a range of additional
options for providing early labour services including open access to Birth
Centres (for women of any obstetric risk status) and access during the
day to Maternity Assessment Unit or day units.
In one Trust (#26), a Birth Centre was introduced in 1986 which women
in early labour can attend for assessment. The maternity service is
developing a team midwifery model with GP practice attachment with the
aim of offering more home assessments in early labour. To support the
move to team midwifery, the role of the MCA has been developed to
provide care for postnatal women in the Birth Centre with midwifery
support available on an ‘on-call’ basis.
Funding and sustainability
One Trust had received PCT funding for a Maternity Assessment Unit as
an initiative to tackle the problem of high numbers of category-X women:
We received funding by the PCT in 04/05 for a 1.2 whole time equivalent
plus one HCA [health care assistant], now it is part of the contract with no
additional funding in 05/06…. It has reduced the numbers of category-X
women on labour ward during the day…. Those women not covered by
group practices (around 65 per cent of the population) routinely phone the
delivery suite in early labour. Early labourers are directed to the [
Maternity Assessment Unit] when it is open, and a significant proportion go
home, it is used as a triage, but it is also used by others not in early
labour. We have tried to get midwives to use a template as triage tool on
the phone but we are struggling to get midwives to record things not in
notes. Also, I am not yet convinced that phone conversations are about
The OPAL study
©NCCSDO 2007 71
giving care…. The [ Maternity Assessment Unit] is popular; we have seen
an increase in numbers attending from GP surgeries, not necessarily ones
that would have attended before…. I feel this service is sustainable; there
are no obvious threats to sustainability.
(#60)
With their multi-faceted approach, a positive effect was reported on
retention and recruitment of staff:
Despite it being a very manic labour ward, we can, we are showing staff
we are trying to make things better, e.g. [ Maternity Assessment Unit]. We
offer different ways of working, midwives move around a lot with various
things, for example maternity leaves, etc. We have very low recruitment
problems, especially given that it’s [large city], we have below 5 per cent
vacancies.
(#60)
Another Trust had introduced the change, hoping for funding
retrospectively. Funding was, for this Trust, the main threat to
sustainability:
It has gone very well. There is an assessment area on there and if women
in early labour attend the Maternal and Fetal Unit, and are low risk, they
come to the Birth Centre…. The Birth Centre has two midwives each shift,
including one consultant midwife, and one HCA [health care assistant] and
is sited downstairs from delivery suite. It is open 24 h, 7 days a week and
only closed as a last option; however, last August it was closed most
weekends due to sickness, maternity leave, staff holidays…. The main
problem is staffing…. There has been no additional staff for the Birth
Centre, we hope that with success stories we may get additional funding
from the PCT, which is the main threat to sustainability…. The MSLC
[Maternity Services Liaison Committee] have been very supportive too…. I
thought there would be more problems than there were, we have a large
percentage of junior staff but it has not seemed to cause offence.
(#1)
Issues for women whose first language is not English
Two HoMs interviewed commented on the challenges of providing early
labour support in these situations. An additional service reported by one
HoM was the introduction of a ‘buddy’ scheme to provide support during
labour and birth, if possible, together with antenatal and postnatal
contact. This scheme had been introduced in an area with high ethnic
diversity (#74) for women requiring language support or who were
vulnerable in other ways. This had been introduced a few months prior to
the interview and further developments include provision of a CD-ROM
providing information about labour in a number of languages.

The OPAL study
©NCCSDO 2007 72
2.3 Recommendations for introducing home- or community-based assessments
The following recommendations were made by HoMs during interviews
about implementation of service changes; these are subdivided into the
relevant type of service change and include issues of change
management as well as specific issues for the service change described.
The main theme of HOMs’ recommendations to colleagues related to
staffing issues: the importance of appropriate staffing levels in the
community, positive attitudes to home assessment and home birth
among midwives, considering midwives’ job satisfaction and incentives to
work in certain ways.
Need to ensure there are enough midwives in the community. You need to
look at the number in the team, make sure there are enough to provide 24
h cover within a team for intrapartum visits. You also need midwives that
are confident and passionate about homebirths, their confidence increases
the more they do.
(#114)
You need to get staffing levels so everyone is happy. You need to look at
the model of off-duty and on-call, and the incentives they give. The skill-
mix is important, you need experienced midwives. With the MCAs you need
to tread carefully, making sure the training is at a level they are happy
with.
(#126)
2.3.1 Changes to commissioning
One HoM felt that early labour care may receive attention in future
changes to the commissioning of maternity services.
There is nothing in contracts at the moment but the PCT are aware that we
provide a good service, so it may be a factor in Payment by Results in the
future but not at present.
(#114)
2.3.2 The importance of the model of midwifery care
Heads of Midwifery in most of the units offering home assessments felt
that it was only possible to do so in an integrated or other team-
midwifery model of care with enough staff, rather than the traditional
model. However, this view was not universal. One Head of Midwifery
thought it could be possible to offer home assessments in a traditional
model of midwifery but there would need to be a change in the
philosophy of the midwives:
It is a rural population … I think it is possible to provide home assessment
to all in a traditional model, but there needs to be a change in the mindset

The OPAL study
©NCCSDO 2007 73
of the midwives: it is easier in an integrated setting because everyone is
doing the same thing.
(#153)
It is difficult to offer home assessment to all in a traditional model as there
are not enough midwives.
(#114)
You can’t offer home visits if not in team midwifery, not within a traditional
model. Before, if a midwife was on call, if they went out they didn’t have to
work the following day, we couldn’t do that now.
(#126)
Trust (#1) had piloted the offer of home visits to women in early labour
during a 4-month period in four community midwife teams covering a
large geographical area. This had been discontinued, however, as there
were insufficient funds, not enough midwives and the model of care made
it difficult to operate:
Many community midwives were positive about this form of care and
understood the benefits to women but caseload constraints, patterns of
working made this a difficult option to facilitate…. Due to caseload
numbers and staffing in the community this form of care was unable to
continue at this time.
(#1)
2.3.3 Recommendations related to the introduction of
triage areas
Location
There was general agreement that there should be a dedicated area or
space near the labour ward with a separate entrance if possible. Opinion
varied over whether it should be adjacent to the delivery suite or not. The
main advantage of being adjacent is the proximity in case of clinical
problems; however, the main disadvantage is that staff can be moved to
the delivery suite when that area is busy and triage subsequently suffers:
[In a previous post where triage was attached to the delivery suite] it was
very easy when they were busy to close triage. I spent days and nights
trying to keep triage open until they finally figured that it wasn’t a midwife
doing nothing it was a midwife keeping non-labouring activity off the
delivery suite. And because here [current post] it’s not attached to delivery
suite, people don’t think of closing it so readily.
(#28)
Introducing change
In order for the philosophy of a triage area to be accepted and for that
philosophy to be operationalised, it was widely agreed that there needed

The OPAL study
©NCCSDO 2007 74
to be support from all grades of staff in planning and implementation,
including senior leadership and management as well as someone ‘on the
ground floor’. This person should be:
…a G grade or band 7 who is prepared to run with it and someone who is
credible – good midwifery skills, able to teach and lead a small team.
(#4)
A key constituency that the planning and implementation group need to
influence and involve are the core staff on delivery suite, in particular the:
team coordinator on delivery suite, if you can sell it to them, then you’ve
sold it, because if they know it’s going to be a positive effect on their
delivery of care on delivery suite, they will make it work.
(#28)
Bring on board positive labour-ward sisters so they can lead the rest.
(#118)
Another group of professionals who need to be on board are the medical
staff, as they need to be ‘compliant with it’ (#28).
Operational issues
For the triage area to function smoothly, it was felt that a number of
things need to be in place: staffing, documentation, communication,
publicity and a telephone. Staffing issues are perhaps individual to each
trust but one key feature was:
Make sure you have a dedicated person on the shop floor who is going to
lead it and isn’t sceptical, who really understands it.
(#4)
Documentation for triage was viewed as important, in particular
guidelines that should be written specifically for triage; there should also
be a means of recording triage activity.
Get paperwork and documentation sorted out. Don’t try to do it with
existing documentation – it won’t work, it’s a different area.
(#28)
Devise some decent guidelines…. Difficult to find the evidence-base for little
things. We have got some guidelines and flow charts.
(#4)
Respondents reported that it was important to communicate the aims of
triage to all staff, to be clear about which women should be seen in the
triage area and times when the service is available (#28). However, one
note of caution was raised by one respondent who felt that its availability
could be over-publicised:

The OPAL study
©NCCSDO 2007 75
Don’t overpublicise it, use it to help manage the labour ward, otherwise
you get inundated or get confused with the Day Assessment Unit.
(#4)
One issue identified was that of the provision of ‘cross-border’ care where
a Trust’s community midwives provide care for women planning to have
their baby in a different Trust. Such women would be referred to their
booking unit for early labour advice and assessment since different units
are likely to have different policies (#28).
2.3.4 Recommendations related to the introduction of
telephone triage
The need to make sure documentation is in place ‘to cover yourselves’
was highlighted (#83) and making sure that staff who are to carry out
the telephone calls are informed, happy and confident was also deemed
important.
Involve the staff; listen to what their worries are. Explain that the evidence
is that this practice is better for women, which is a big lever to make it
happen. But you need to listen to the staff and their worries and put things
in place to support them to enable it to happen.
(#116)
There were no reports to suggest that introducing telephone triage had
any negative impact on services, or on clinical or organisational issues,
staffing, or clinical risk management.
2.3.5 Recommendations relating to additional options
for early labour care
These included the need for audit, protocols or guidelines supported by
both midwives and obstetricians. The aims and philosophies of the service
need to be clear to all staff.
You need to audit who is attending, where they are coming from and
where their destination is or should be. You need clear protocols, ours were
evidence-based and devised jointly between midwives and the lead
obstetrician. Be clear that women are to spend less time in there, that the
aim is for them to go back home.
(#60)
2.4 Conclusion and discussion
The questionnaire survey achieved a satisfactory response rate that
supports generalisability in interpretation of the findings; additional
information was obtained through interviews with a purposive sample of
Heads of Midwifery, targeted for interview because of particular models of
early labour service provision.

The OPAL study
©NCCSDO 2007 76
From the questionnaire data, it was clear that, where data were available
or an estimate provided, the number of women admitted to labour wards
and discharged not in labour (category X) forms a significant workload for
maternity care providers. However, the lack of accurate data is a concern
when this component of maternity provision has contributed to the need
for a significant amount of service modification.
When women phone the maternity unit in early labour (contractions every
5–7 min) there is a variation in the advice given: the two approaches
reported most frequently – ‘make your way in when ready’ and ‘phone
again later’ – may have different implications for staffing of the maternity
unit. The majority of early labour care was reported still to take place on
labour wards but also includes an increasing range of settings,
exceptionally in SureStart facilities and some Birth Centres available for
all women to access on a ‘drop-in’ basis regardless of place where birth is
planned. Little midwifery support to NHS walk-in centres was reported.
The potential for Children’s Centres to be a further venue for early labour
services is not yet known and should be monitored. In addition, the
impact of changes to the commissioning process must still be assessed.
A large proportion of units did not have guidelines, policies or protocols
for early labour care; this is surprising given the contemporary emphasis
on the importance of evidence-based care. This issue may, of course, be
addressed in the publication in 2007 of the NICE Intra-partum Care
guideline. Women receive information about local arrangements for early
labour in a range of ways using both face-to-face discussion and written
materials, during routine antenatal care and in group sessions, for
example antenatal classes and labour-ward tours. The fact that 31 per
cent of services have no written information about early labour available
to women should be noted by service providers. A minority of units were
developing videos and CD-ROMs and providing information on their unit
website. The extent to which any of these materials is shared is unknown
and it may be that systems that support dissemination, for example,
Internet-based discussion boards would be useful.
Forty-three per cent of units reported the introduction of new early labour
provision within the last 5 years with further changes planned by over 50
per cent. Changes to early labour services were more likely to have taken
place in consultant-led units with midwifery-led areas and in larger size
units. Triggers for changes in service provision were most commonly local
factors. From interviews with HoMs key drivers to service changes
focused on managing labour-ward workloads. Planning future service
changes was more likely in NHS consultant units without a midwifery-led
care area and again, generally in the larger units. Although a significant
number of units had been engaged in making changes to early labour
care over the previous 5 years, fewer units reported evaluations of early
labour services. All new services were considered to require staff training.

The OPAL study
©NCCSDO 2007 77
Home visiting and triage required additional staffing but may also release
staff to work in other areas; however, the extent to which that occurs
may depend on local issues such as facilities and geography.
Home assessment during early labour (currently being investigated in a
large randomised controlled trial) is offered to all women in less than 4
per cent of units who responded and offered selectively in a further 44
per cent of units (excluding home birth and DOMINO deliveries). Over
two-thirds of units who provide home visits could not state the proportion
of women who received them. Discontinuation of home visiting appears
linked to staffing difficulties, discontinuation of team midwifery, concerns
about midwives’ safety and exploring new approaches.
Data related to the proportion of women assessed in a triage area were
again not easily accessible to senior staff in the maternity services.
Telephone triage, including formalizing and documenting midwives’
traditional labour-ward telephone conversations with women, was also
reported. Triage services had been discontinued due, it appears, to
difficulties in keeping triage areas open when units are busy but also due
to difficulties in communicating the philosophy. Telephone approaches to
triage also require training, good documentation and guidelines to support
staff in this approach. Some Trusts report adopting a combination of
approaches to early labour care, particularly where Birth Centres and
maternity assessment units are available. The current draft of the revised
Towards Safer Childbirth (Royal College of Midwives, 2006) suggests that
both home assessment and triage services are effective approaches to
keeping women off the labour ward. From our research, it is evident that
these approaches also bring staffing requirements and changes of
philosophy that have to be embraced. In addition, there appears no
definitive evidence of clinical benefit from providing triage areas.
The advice offered by HoMs to other HoMs thinking of implementing the
same change was specific to the type of change. For triage areas location,
documentation, a motivating midwifery leader, and staff understanding
and acceptance were key issues; telephone triage was considered easy to
implement but required good documentation, staff understanding and
confidence in its use; Birth Centres and Maternity Assessment Units work
when there is a clear understanding of their aims and philosophy in
encouraging women to return home when appropriate; home assessment
requires consideration of staffing levels, midwives’ job satisfaction, it
requires staff with positive attitudes towards home births and women
staying at home in early labour. Factors, such as the model of midwifery,
were identified that support the provision of home assessment in early
labour; the information gained in this component of the research will
inform the interpretation of the results of the SDO-funded trial of early
labour support and assessment at home.

The OPAL study
©NCCSDO 2007 78
For women whose first language is not English, increases in the
availability of interpreting and advocacy services have been described in
the revised draft Towards Safer Childbirth (Royal College of Midwives,
2006), for which consultation is currently in progress. The care of this
group of women is particularly important in the context of the Confidential
Enquiry into Maternal and Child Health report (Royal College of Obstetrics
and Gynaecologists, 2004) that identified difficulties in communication
between women and their health care professionals as contributing to the
number of maternal deaths in this group. Further exploration of service
provision for non-English speaking women appears warranted.

The OPAL study
©NCCSDO 2007 79
Section 3 Midwives’ and women’s experiences of the All-Wales Clinical Pathway for Normal Labour
3.1 Background
3.1.1 The All-Wales Clinical Pathway for Normal
Labour (the Pathway)
The website for the Pathway,
www.wales.nhs.uk/sites/page.cfm?orgid=327&pid=5786, gives the
following definition.
What is the clinical pathway for normal labour?
A clinical pathway is a template or blueprint for a plan of care. It is a guide to
usual treatment patterns, but does not compromise the need for clinical
judgement. The clinical pathway for normal labour provides support for midwives
who wish to practice evidence-based clinical care of the highest standard with
minimal unnecessary intervention. It also provides a framework to maximise the
opportunity for women in Wales to experience normal childbirth. It is not intended
to prevent clinicians from using their professional judgement in the way that they
care for individual patients. The pathway documents expected events in labour
with references to the latest evidence available. Midwives are encouraged to use
their clinical judgement and to document any variations from the anticipated path.
The pathway is designed to be shared with women so that women are both
included and informed.
A women's information leaflet, Your Pathway Through Labour (see
Appendix D), explains the care a women should expect to receive from
her midwife once she is in labour. The leaflet is considered to be an
integral part of the Pathway (P. Ferguson, personal communication) and
is downloadable from the website.
3.1.2 Part 1 of the Pathway
Part 1 of the Pathway covers the so-called latent phase of labour, prior to
admission.
The form is headed ‘Part One - Telephone Advice’ and starts with the
statement:
This clinical pathway has been developed by clinicians throughout Wales
for 100 per cent of women in normal labour. It is a guide and encourages

The OPAL study
©NCCSDO 2007 80
clinical judgement to be used and documented. The pathway aims to
reduce unnecessary intervention in normal labour.
The first page is taken up with definitions about the grading of
recommendations and Levels of Evidence pertaining to the advice
contained subsequently. Page 2 then lists the information to be
ascertained to check eligibility for the pathway, starting with ‘Have you
phoned before? If so, a pathway may be in progress’. It ends with the
injunction: ‘Facilitate as much time as is required for questions or
concerns to be raised, please document any relevant information’.
Signs of the latent phase of labour are described and the
recommendations and evidence presented regarding staying at home at
this time. The midwife documents the advice given, which can be
• advised to attend labour ward or Birth Centre,
• midwife asked to undertake home assessment,
• advised to ring back at a certain time,
• advised to ring back when labour advances.
The form continues:
For women who are advised that, at this stage, home is the most
appropriate place for them to be, advice relating to maintaining well-being
during the latent phase may be considered. Nap and rest if you are feeling
tired, although mobilising may encourage the contractions to establish
themselves. Take light diet and drink plenty. Warm showers and baths
may provide some pain relief; massage or back rubs can be helpful.
Paracetamol 1 gm 6 hourly can be taken. TENS machines, if available,
should be encouraged. The latent phase is the early part of labour,
redefining as ‘not in labour’, ‘slow labour’ or ‘niggles’ is not helpful to
women (B), a brief description of the physiology may be of assistance.
The form has space to record three telephone interactions.
3.2 Aims
The aim of this part of the study was evaluation of Part 1 (the telephone
component) of the All-Wales Clinical Pathway for Normal Labour from the
perspectives of women and of midwives. Specific objectives were:
1 to determine women’s experiences and views of the service,
2 to obtain the views of health professionals and impact on their work,
3 to identify issues of process.
3.3 Methodology
Data were collected from midwives via focus groups (and a small number
of questionnaires) and from women through computer-assisted telephone
interviews (CATI). Women were to be recruited by their community

The OPAL study
©NCCSDO 2007 81
midwife at the point of discharge to the health visitor. The original
intention had been to sample both midwives and women from every one
of the 13 NHS Trusts in Wales, but, as described below, this did not prove
possible.
3.3.1 Midwifery research fieldworker
Our team of investigators was based in Yorkshire, and, although it
included representation at the strategic level for maternity services in
Wales, we felt that the team would also benefit from the additional
contribution of a midwife with recent experience and contacts at the
service-provider level. We were able to utilise research funding to include
a midwifery research fieldworker in the team.
We envisaged that this post would:
• facilitate links with NHS Trusts and research stakeholders in Wales,
• ensure that the research team were correctly interpreting information
about the rationale and process of the recently introduced All-Wales
Pathway (the Pathway),
• utilise local knowledge of organisations, systems and key
postholders,
• facilitate the introduction of the study to midwives and other health
care professionals in Wales.
This post would also offer a research-development opportunity for an
experienced midwife reflecting the philosophy of the Mother and Infant
Research Unit to contribute to building research capacity in midwifery. We
were fortunate to be able to appoint from a strong field of experienced,
Wales-based midwives. The midwifery research fieldworker was appointed
to work one day per week throughout the preparatory and recruitment
phases of the study. We felt that it was appropriate to have one senior
midwife in this role due to the planned sampling strategy, limited
recruitment period in each Trust and the need to liaise at the strategic
level with stakeholders in Wales rather than the model used, for example,
in the ELSA trial of one local co-ordinator per Trust.
The duties of the post included: supporting introductory work at Trusts;
facilitating communications in each site; supporting recruitment of women
and assisting with data collection. More specifically, the components of
this included:
• assisting with initial contacts and liaising with staff in each of the
Trusts in Wales, including visits to each Trust,
• supporting the registration of the study within each Trust’s local R&D
Department,
The OPAL study
©NCCSDO 2007 82
• promoting the research within the midwifery and obstetric
community in Wales, including presenting the research at meetings
with midwives and others,
• acting as a contact point for professionals and participants who
became involved in the study,
• receiving and distributing supplies of study information leaflets for
women, ensuring that local knowledge is used and harnessed to
maximise recruitment within the community,
• supporting communications about the research within the hospital
and community midwifery teams,
• liaising regularly with the research team in Leeds (subsequently
York) about progress of the fieldwork,
• supporting and monitoring recruitment,
• arranging venues for, and encouraging attendance at, focus groups
for midwives,
• contributing to collection of data, including assisting with focus
groups for midwives.
3.3.2 Communications with stakeholders
Key stakeholders in the evaluation of the telephone component of the All-
Wales Pathway are service users, clinical midwives and their managers.
Polly Ferguson, Nursing Officer (Midwifery) at the National Assembly for
Wales was one of the project grant-holders. Preliminary work to involve
stakeholders included one of the principal investigators (H.S.) attending a
meeting of the All-Wales Pathway Steering Group in Cardiff, who
welcomed the research. This was followed shortly by attendance at the
Royal College of Midwives’ national conference, held in Cardiff, with the
purpose of networking with midwives based in Wales. This was successful
in allowing informal introduction to and discussion of the project by one of
the principal investigators (H.S.) with a large number of midwives
working in Wales. Fliers were distributed. Contact was also made with the
professional forum for Heads of Midwifery in Wales: information was
forwarded for inclusion at their quarterly meeting and offers of
presentations made; unfortunately their meeting schedule and full
meeting agendas prevented a presentation by any members of the
project team, although the offer remained open. All Heads of Midwifery in
Wales were contacted on an individual basis.
Contact with service users was initially achieved through the NCT,
through both their central Headquarters and Cardiff-based contacts
achieved at the Royal College of Midwives Conference. The latter resulted
in permission to contact women who had received care within the All-
Wales Pathway and who agreed to telephone discussions with members of
our research team (reported in more detail below). This allowed us to

The OPAL study
©NCCSDO 2007 83
identify aspects of the telephone component of the All-Wales Pathway
that required exploration in the main study.
3.3.3 Ethics and research governance issues
The application was approved by the Leeds West Research Ethics
Committee in October 2004. All HoMs had already been approached and
submissions were then made to the R&D departments of each of the 13
NHS Trusts in Wales. A large part of the following 6 months was devoted
to attempting to obtain the requisite clearances. At the end of that period
we still awaited final approval from five R&D departments; contact and
permission to work through the community midwives from four Heads of
Midwifery; and honorary contracts for H.S. (as principal investigator) from
four Trusts, and for the members of the research team from two Trusts.
In seeking to follow the Research Governance Framework, we
encountered the following issues:
• inconsistency between Trusts in the interpretation of the Research
Governance Framework and processes to be followed;
• uncertainty among Trust R&D staff about the interpretation of the
framework;
• confusion and a lack of clarity within Trusts in relation to which
members of the research team required honorary contracts and
conflicting advice from different departments within a Trust;
• wide variations in the process by which honorary contracts are
awarded between Trusts in respect of clearance processes; such
processes have included:
a the need for Criminal Review Board checks; this requires
submission of documentation, for example passport or driving
licence, utility bill and bank details, and the checking process takes
approximately 1 month,
b completion of lengthy occupational-health screening
questionnaires dealing with personal health and family history and
requests to attend for health screening,
c checking of professional registration, where appropriate;
• difficulties of communication between Trusts R&D and Human
Resources departments and clinical directorates;
• additional notification to general managers, Clinical Governance
Leads and Caldicott Guardians, although not stated on Trusts’ R&D
registration documentation;
• the issuing of contracts that were not specifically developed for
researchers and over which further negotiation was required;

The OPAL study
©NCCSDO 2007 84
• the allocation of supervisory staff from within the Trust when
subsequent enquiry has indicated these do not come from an
appropriate speciality;
• submission of documentation, previously approved by Multicentre
Research Ethics Committee, for R&D approval;
• exploration of issues of sponsorship and liability;
• confusion at Trust level about Multicentre Research Ethics Committee
approval and the need for site-specific assessment;
• additional peer review by Trusts’ R&D committees.
The workload involved in all of these communications was quite
disproportionate, and necessitated an average of 6 h per week each from
one of the principal investigators and the project secretary using all
possible communication methods including fax, e-mail, telephone and
letter. With one possible exception, none of the Trusts apparently had any
objection to the research being carried out in their Trust; these delays
were entirely bureaucratic. In some Trusts, R&D managers acknowledged
that their processes were not facilitative of research and that some
anomalies existed in their own systems. By June 2005, we felt that we
could not afford to wait any longer for permissions to be granted and
made a pragmatic decision to restrict the research to those Trusts in
which all permissions had been granted or were imminent. The six
participating Trusts were Gwent, North Glamorgan, Cardiff and Vale,
Swansea, Ceredigion, and Conwy and Denbighshire. In a seventh Trust
(North-East Wales) we obtained permission to approach midwives but not
women.
3.3.4 First contact with midwives
One of the fieldworker’s first tasks was to clarify how Part 1 of the
Pathway worked in different settings. Each main labour ward/Birth Centre
in Wales was contacted and asked where telephone calls of women in
early labour were directed and who completed the paperwork. This early
contact provided an opportunity to inform midwives about the study and
to gain a brief insight into the variety of midwifery care models operating
in Wales.
While we awaited Trust R&D approvals it was considered important to
maintain the momentum of the study. A decision was made to organise
meetings with midwives from the Trusts to provide an overview of the
study, its aims and objectives. Permission to undertake these initial
meetings was obtained from Heads of Midwifery, who forwarded names of
the community managers who assisted in setting up the meetings.
Meetings were organised in seven Trusts (Gwent, Cardiff, North
Glamorgan, Carmarthen, Swansea, Pontypridd, and Rhondda and
Bromorganwg). Each received a presentation about OPAL from the

The OPAL study
©NCCSDO 2007 85
midwifery research fieldworker and information regarding how the
research team would require their help. The midwives were encouraged to
ask questions and discussions took place regarding the practicalities of
identifying and recruiting eligible women for the study. Leaflets containing
study information and team contact details were distributed. The
presentations were well received by the midwives who appeared to be
interested in the study and its possible findings.
3.3.5 Modifications to the research plan
The original proposal had included the intention of collecting data from
obstetricians as well as from midwives. An early meeting with the
All-Wales Pathway Steering Group raised objections to this aspect of the
research. In particular it became clear that some midwives may not feel
comfortable attending focus groups that included obstetricians and that
recruitment to the focus groups was likely to be jeopardised by their
inclusion. It was in any case argued that the Pathway was a midwifery
issue, not an obstetric one. Clearly we needed to deal with this objection
pragmatically. It was unlikely that many obstetricians would attend even
if invited and it was the experiences and understandings of midwives
about which we particularly wanted to learn. Accordingly we agreed that
only midwives would be invited to the focus groups, although
obstetricians would still have the opportunity to make their views known
to us by other means.
The delays described in Sections 3.3.3 and 3.3.4 had two specific
implications: a reduction in the numbers of midwives and women who
were available for sampling and a reduction in the amount of time still
remaining in which to collect and analyse data. Although the SDO had
kindly agreed to a no-cost 3-month extension, modifications to the
research plan still needed to be made.
3.4 Data collection from midwives
3.4.1 Rationale for focus groups
Focus groups had been chosen as the preferred method of data collection
from midwives for a number of reasons. First, they represent a more
efficient use of researcher time than individual interviews and are likely to
seem less intimidating to the participants. Second, a group gathering
allowed us to turn the occasion into a social event, providing a light lunch
as a way of saying thank you to participants for their time, and making
the atmosphere less formal and more relaxed. In addition, focus groups
have the particular advantage that, ideally, they consist of a conversation
between the participants, not just a series of questions and answers
between the researcher and individual participants. This allows for
The OPAL study
©NCCSDO 2007 86
exploration of areas of consensus or disagreement. Finally, this was a
topic where we, the outsiders, were trying to gain understanding of
something that was a part of everyday life for the participants. A number
of our questions – for example, why things are done in a particular way –
would be issues that they would take for granted and not actually
articulate unless asked. By asking such questions we were able to create
a situation in which underlying beliefs and assumption were aired and
similarities and differences identified (Barbour and Kitzinger, 1999). The
focus-group schedule is given as Appendix E.
3.4.2 Alternative data collection from midwives
It was always evident that only a small proportion of midwives in Wales
would be able to attend a focus group. We therefore also devised a brief
questionnaire to allow any staff who were unable to attend the groups to
express their views. The questionnaire was printed as part of a Newsletter
(see Appendix F), which was distributed to all maternity units in
participating Trusts in August 2005 and invited responses from
obstetricians as well as midwives. There were ‘personalised’ newsletters
for North and South Wales, and readers were also told how to access an
electronic version of the questionnaire, if preferred. Six questionnaires
were returned in total; information obtained is included in the report of
the focus-group findings.
3.4.3 Focus-group arrangements
The plan had been to hold four focus groups for midwives in
geographically spread locations to which all local labour-suite care
providers would be invited. Following problems with obtaining necessary
permissions, only two were held: in Caerphilly in the south in August
2005 and in Rhyl in the north in September 2005. Both were held,
following negotiation, on Trust premises that were familiar and easily
accessible to local midwives, and both were held at lunchtime; this
approach was supported as the preferable option by Trusts. Midwives
from the seven Trusts participating in this part of the study were invited
to attend one of the two focus groups via an invitation sent to midwifery
managers. Potential participants were told that lunch would be provided
and that all those attending would have their name entered for a prize
draw for a £25 gift voucher.
3.5 Midwives: findings
Findings are presented in the form of a narrative account that discusses
the themes and is supported by quotations to illustrate the midwives’
perceptions of Part 1 of the Pathway. The letters and numbers in brackets
at the end of the quotes relate to the participant identification code.

The OPAL study
©NCCSDO 2007 87
3.5.1 Documentation
One of the first themes to emerge from both the focus-group and
questionnaire data concerned the documentation used to record the
telephone advice given. This arose initially in response to the opening
invitation.
Tell me about the telephone component of the Pathway. How is it different
from what you were doing before or what other units do? Is it a strict
algorithm or is there room for professional judgement?
It was clear that some respondents interpreted ‘Part 1 of the Pathway’
simply in terms of a change of documentation from that used previously,
rather than as any change in underlying philosophy. Prior to the
implementation of the Pathway, there had apparently been no standard
way of recording the telephone advice given to women in early labour;
this varied between individual midwives and maternity units. Some of the
units would record the woman’s particulars either with or without details
of advice given in a ‘telephone message’ book; other units used ‘slips of
paper’ (sic) to document the telephone call.
There was a general consensus that Part 1 of the Pathway has provided a
formalised approach by standardising the documentation in an easy
format to record advice given by midwives to low-risk women in early
labour. This standardisation has provided midwives with a clear structure
for giving advice but nevertheless was viewed more as a guide or a
prompt that complemented clinical judgement rather than a set of rules
to be strictly adhered to.
It would appear, however, that during the initial stages of implementation
there was resistance by some midwives to the change in documentation.
We had slips of paper that were used but when the Pathway came in we
had Part 1 on the side, but we got rid of the other slips of paper because
we found that some people were favouring the ‘old’ paperwork.
(N1)
The training received had varied; some midwives said that they were
given clear information on how to complete the documentation, others
relied on colleagues to help them. However, the straightforward format of
the documentation means that it is easily taught to student midwives and
new staff who have not previously worked in Wales and training was not
felt to be a major issue.
These perceived advantages of the documentation had apparently led to
widespread adoption. In one unit, Part 1 documentation was used for all
women who telephoned the labour ward for advice regardless of whether
they were eligible for the Pathway or in early labour.
This utilisation may have arisen as a way of ensuring that midwives
became familiar with completing Part 1 of the Pathway. However, because
The OPAL study
©NCCSDO 2007 88
the documentation is structured specifically for low-risk women seeking
advice in early labour, applying the framework to women outside these
criteria could be seen as inappropriate and results in duplication of
paperwork as further documentation in a different format is required.
The situations in which the documentation was likely not to be used for
low-risk women seeking advice in early labour were in the community,
and we will return to these issues below. Community midwives said they
were more likely to record advice in their diaries or the antenatal hand-
held record if they spoke to the women face to face, because they did not
necessarily carry copies of the documentation and in any case would
probably not be able to get it to the hospital to be of use to the next
person who the woman spoke to. There was ambiguity about whether it
should be used for home births.
Well I don’t tend to use it when I’m doing a home birth, I don’t tend to need
to use it for ringing, and I’m not having to write lots of bits of paper out.
(N6)
In terms of the layout of the document some expressed concern over its
length and felt it could be condensed into fewer pages. Several queried
the need to have the evidence summary on the front sheet as they
admitted to not reading it. They suggested a separate booklet containing
that information for midwives similar to the Midwives Rules and Standards
(Nursing and Midwifery Council, 2004).
3.5.2 Recording Part 1 information
There were a number of points regarding how Part 1 information was
recorded. The first concerned who recorded the information. In some
maternity units the telephone will be answered by a ward clerk during
office hours and it is they who commence the documentation before
calling a midwife to advise the woman.
They take the information, they ask some of the questions then they come
to us. Sometimes the ward clerks say our reply but other times if we feel
that we need to actually speak to them on the phone. It depends what the
call is.
(N1)
Additionally, in some instances a MCA may answer the telephone
although it would appear that they call for a midwife and do not
commence any of the documentation.
While not always possible due to shift changes or other clinical
commitments, midwives will try to offer continuity of contact:
Sometimes I’ll say do you want to ring me back in an hour, if I am not sure
what is going on, then I will give them my name then. If you can see on the
The OPAL study
©NCCSDO 2007 89
Pathway they have phoned in on this shift and the person they spoke with
is still there then we would try and get them.
(N4)
There are also occasions when a student midwife would take the
telephone call. There was a general agreement that Part 1 of the Pathway
was a useful teaching aid; the student works under the supervision of her
mentor, all documentation is countersigned, they learn to listen to women
and give appropriate advice about early labour.
In the community some Trusts have midwives who work in caseload-
holding teams. Midwives who practice in this setting are always the first
point of contact for women on their caseload who are in labour and
therefore complete the Part 1 documentation. In contrast, as we have
seen, many community midwives who work within more traditional or
integrated models will have early labour calls directed through a main
labour suite/Birth Centre and will not necessarily carry copies of the
documentation. Others may give early labour telephone advice to women
if contacted during ‘on-call’ hours, therefore completing Part 1
documentation.
Having a range of systems in place has led to diversity and sometimes
uncertainty for the community midwives regarding whether they should
complete Part 1 documentation:
I actually had a call from one of my own patients this morning who
actually said she was having niggles after I gave her a sweep yesterday. I
really wondered whether I should fill in a Part 1 for that, but I haven’t and
I suppose I should really.
(S2)
Some midwives fill in the documentation retrospectively because they do
not keep copies of Part 1 and so do not have immediate access to the
documentation or if advising a home-birth mother in very early labour.
These midwives felt they were now familiar with the Pathway and were
experienced enough to know which questions to ask. However, for some
there is a logistical issue of getting the paperwork from the midwife to the
woman’s labour notes.
And in my area I serve a 50-mile radius so she might ring me 50 miles from
where I currently actually am. I’m not going to travel 50 miles to fill in a
form.
(S3)
These issues could mean that if the woman made a later telephone call to
the birth unit/labour ward that another Part 1 would be initiated. This
raised concerns about duplication of paperwork and wasting paper;
however, there were also comments that even in hospital some women
would end up with more than one set of Part 1 documentation.

The OPAL study
©NCCSDO 2007 90
3.5.3 The telephone assessment
The midwives discussed how they conducted the telephone assessment.
Some felt that the questions on the form were no different to those many
midwives asked before implementation of the Pathway. However, it was
felt that it has assisted all midwives to ask the right questions to assess
the progress of early labour and to give appropriate advice rather than
asking all women who may (or may not) be in labour to attend labour
suite.
Although the Pathway provides guidance on questions to ask they are not
read out as a set list, midwives are incorporating them into the telephone
conversation so there is natural flow of dialogue. This suggests the
midwives are adopting an individual approach rather than using the
Pathway as an algorithm.
The duration of the telephone call can be dependent on how far the
woman’s labour is established. However, according to the midwives the
overall time spent talking to women in early labour does not appear to
have altered significantly.
But we’ve always spent a lot of time speaking to women in early labour on
the phone and we [just] never documented it.
(S6)
The midwives discussed how the telephone assessment encouraged
conversation with women and the importance of using listening skills.
They also discussed how the art of recognising and interpreting what can
be quite subtle cues from the content of the conversation, the tone of
voice or woman’s breathing develop with experience:
…having conversations with women is just the best way of learning
midwifery and it’s great that it’s brought back the conversation rather than
just ‘come in’ and put the phone down.
(S7)
One other area discussed was the importance of speaking to the woman
herself rather than having a conversation via her partner or other family
member. The midwives also spoke of occasions when there would be little
time for the telephone assessment as some calls were made to say they
were ‘coming in’ or made en route by the partner.
However, even in such circumstances the midwives said that they
endeavour to engage in conversation with the woman or partner to
undertake an assessment and obtain a minimum amount of information.
If appropriate, they may arrange for a midwife to go the woman rather
than she give birth on her way to the maternity unit.
The midwives were encouraged to debate actual or potential risk-
management issues they may have encountered in relation to the

The OPAL study
©NCCSDO 2007 91
telephone assessment and advice. It was considered that having
telephone advice documented might be assisting the risk-management
process as it provides evidence of the discussion between the woman and
the midwife, especially if problems occurred later in labour.
I think it might be preventing problems because I think in the past there
have been occasions where a woman has rung up and been give advice,
and there’s been a problem that has arisen later and there’s nothing
documented so there’s nothing to prove what the midwife said.
(S7)
Furthermore, the midwives felt that the documentation provided evidence
in the event of a complaint regarding advice given.
We’ve had a number of complaints in the past and it has provided good
evidence of when there has been disagreement with what has actually
been said over the phone.
(N1)
However, in relation to specific incidents such as a possible increase in
the number of babies born at home without the attendance of a midwife
(BBA, born before arrival), the midwives did not believe encouraging
women to stay at home in early labour had any effect.
The midwives were asked whether a limit would be put on the number of
phone calls a woman could make before being asked to attend a labour
ward/birth unit. This question was included as we had heard that one
Trust had adopted a policy that women are asked to come in after the
second call. Several midwives thought there may be a ceiling of three or
four calls, which may have arisen because the document only provides
space for recording three telephone calls. Overall there was a consensus
that no official ceiling should exist regarding the number of times a
woman could telephone for advice, as a policy to assess women after
three calls would compromise clinical judgment. However, some midwives
suggested that if a woman telephoned for advice repeatedly they might
advise her to attend the unit because it sounded as if she wanted
reassurance, although the overall clinical assessment would influence the
decision.
3.5.4 Supporting practice and empowering midwives
There was a clear perception among the midwives that the Pathway
supported their clinical practice and was an empowering tool. One of the
explanations given was that the best-practice guidance offered within the
Pathway framework was evidence-based.
It has got some of the evidence down there, in that it does guide you. It
gives you what the best practice is in terms of the current evidence and
that if they are in labour that it’s better for them to stay at home, and it
gives you grades of evidence for that.

The OPAL study
©NCCSDO 2007 92
(S3)
It was also viewed as a support to midwifery practice that could be used
flexibly to inform clinical decisions. For example, some midwives said that
they would often ask women additional questions to those listed on the
documentation if necessary.
The midwives believed that documenting the telephone advice had
improved communication. This had two elements: first in terms of the
consistency of advice the midwife and their colleagues would offer women
who telephone on more than one occasion and second it was thought to
enhance communication between shifts where there may be long periods
between telephone advice.
And particularly, say, if people phone in quite frequently with every sort of
contraction, you’ve got the continuity of advice there.
(N3)
Communication is better between the shift change as well. Because
someone can look at what was said on the previous shift and what has
changed, that’s been useful.
(N2)
In addition to improving communication, there was also the assertion that
using the Pathway had increased the midwives’ professional autonomy.
They were able to offer evidence-based advice that aimed to promote
labour as a normal physiological event rather than one that has to be
managed medically.
Whether it’s just been to enhance people’s recognition of the normal and
just to get people thinking and talking about normal birth, that to me is one
of the issues, and it’s increased midwives’ confidence.
(S11)
Moreover, not only was there a belief that professional autonomy had
improved, but also that Part 1 of the Pathway has helped midwives
develop a more positive language that emphasises the normality and
benefits for women to be at home in early labour. Midwives’ confidence in
facilitating and promoting normal birth had therefore increased, and so
they are happier to advise women to stay at home rather than suggesting
that they attend labour ward.
It’s definitely a confidence issue, you’ve got to learn to use your ears as
well, you know by the tone of a woman’s voice and what they’re saying to
you, and you know if they can talk to you happily for 10 minutes on the
phone you can guarantee that they are probably not in active labour, but if
they can’t, then…. And it’s building up that confidence, whereas before it
just like was a case of ‘oh yes, well, please make your way in’.
(S2)

The OPAL study
©NCCSDO 2007 93
It was also suggested that using Part 1 of the Pathway helped some
midwives to reflect on their practice.
And also I mean it’s a part of how I reflect on my own practice you know, if
I’ve spoken to a woman and given her particular advice about something
specific, then you want to find out the outcome, to know whether, you
know, were you correct in what you were thinking, was the advice you
gave appropriate – it’s a part of the learning yourself isn’t it, as well, I
mean I find it really helpful as a learning experience to find out what’s
happened afterwards.
(S7)
Inclusive of building midwives’ confidence and supporting their role was
the perception that the Pathway had enabled them to engage in reasoned
debate with their obstetric colleagues. It was felt that the evidence-based
guidance added weight to their arguments when discussing their rationale
of care for women with uncomplicated labours.
I think the Pathway in itself has had far more wide-reaching effects than
we probably realise, just in the debate it’s caused.
(S7)
It’s definitely generated huge debate with our obstetric colleagues and that
has to be a positive.
(S11)
3.5.5 Impact on workload
The midwives discussed how encouraging women to stay at home in early
labour had impacted on their overall workload. There was a perception
that undertaking telephone assessments for women in early labour had
resulted in a reduction of category-X women – those who are not in
established labour – on the labour ward.
Women are not coming in as early and you don’t get many women coming
in, in that latent phase, and they are more likely to be in active labour
when they do come in.
(S7)
This appeared to have created an additional benefit of freeing up
midwifery time because seeing those who attend Birth Centres/labour
ward in the early phase takes more time than reassuring and advising
women on the telephone.
I mean your phone call [has] got to be 10 minutes, whereas if you bring
them in, by the time we’ve examined them and put them on the CTG then
that’s an hour at least.
(S9)
Where I think they are is also the element of that we are spending in some
circumstances longer on the telephone with a Part 1 than we used to…..

The OPAL study
©NCCSDO 2007 94
You know, we used to just say come in and then deal with all those when
they were there, but it is quicker and easier to do it on the phone, so I think
it is freeing up a bit of time.
(S7)
This would suggest that the midwives could allocate priority and direct
resources to women in established labour. However, it was evident that
midwives still assess some women whose labours are not established but
who want the reassurance of a face-to-face assessment. In some Trusts
they are directed to a triage area away from the main labour ward.
But some of them just like to come in for reassurance I think, and that’s no
problem, they can just come into triage and go back home.
(N4)
Alternatively, community midwives who hold caseloads or book DOMINO
births offer a home assessment and/or provide additional support for
women who are experiencing a difficult latent labour phase.
Yes, we do see people who don’t know what to do. They phone for advice
and we say ‘if you want we’ll come and see what’s going on’, and they
want to stay at home a bit longer.
(N6)
Moreover, the midwives agreed that, although they inform women of the
benefits of being in their own environment, they would not discourage
anyone from attending their unit if they so wished.
An additional impact of Part 1 of the Pathway suggested in both the focus
groups and questionnaire responses is that it has a value in workload
planning for labour suites or Birth Centres. This was considered beneficial
by some midwives as they felt that completed Part 1 forms provide a
record of the number of women who are at home in early labour pending
admission.
3.5.6 Perceived benefits for women
One of the perceived benefits for women was that the Pathway was
helping to educate them that birth is a normal process. The educational
role of the midwife would appear to start with the community midwife
who is responsible for the distribution and explanation of the labour
pathway leaflet to low-risk women in pregnancy. The use of the leaflet is
considered to assist women’s understanding of the normality of the birth
experience, which is then reinforced by other midwives. This was seen as
a positive step that had wider implications for educating the public as well
as staff who worked within a model that treated birth as a medical event.
For me, my understanding of the Pathway being introduced was really to
look at the situation we were having with increasing rates of intervention
… and to impact on that positively and normalise that whole birth

The OPAL study
©NCCSDO 2007 95
experience, and to normalise it within society as well as what was actually
happening in the labour wards, so for me it’s like multi-pronged.
(S7)
The midwives suggested that the emphasis on being at home in early
labour is also beneficial to women as it reduces their likelihood of
unnecessary intervention in labour which could influence their birth
experience.
That is the big aim of the Pathway, to reduce that unnecessary
intervention.
(S9)
Moreover, the development of midwife-led care options for women had
reduced the number of women receiving conflicting advice from doctors
because midwives have adopted a consistent approach that emphasises
the normality of birth for low-risk women.
And I think with more midwife-led care, because they are seeing that
midwife all the way through and they don’t see any doctors, that they take
it from the midwife, they think it’s perfectly normal.
(N7)
There was also an opinion that midwives’ consistency in their emphasis on
the normality of labour has had the effect of increasing women’s
confidence to stay at home.
…if a woman phones up and speaks to a midwife you are actually giving
her the confidence to stay at home and know what she is experiencing is
normal … if she’s got someone at the end of the telephone she can speak to
she’s not left on her own, she can cope with the early stages without
coming to hospital really.
(S2)
The midwives were also of the view that women would consider the
telephone conversation in a positive light, because it should not appear
that the midwife is following a care pathway but that she is making an
informed assessment guided by information that the woman provides.
Some respondents saw the Pathway as empowering women because
midwives are offering them informed choices by discussing plans of care
for early labour, while the decision on whether to stay at home remains
with the woman, thus giving her the control. One community midwife said
that she told women antenatally:
…but if you feel, even if it’s 2 minutes after you come off the phone that the
contractions are stronger and you want to go in, then go in, they won’t
mind. Or even if they say don’t come in, and you want to go in, again I’d
say go in. So, if you tell them that beforehand I don’t think they feel they
have got to take exactly what is said.
(N2)

The OPAL study
©NCCSDO 2007 96
It could, of course, be argued that what these midwives are describing is
giving women permission to take an alternative course of action to that
advised by the Pathway, rather than an inherent feature of the Pathway
itself.
Finally, the midwives explained how the telephone assessment could
improve the potential for building a rapport with women. This could occur
when a woman has telephoned on more than one occasion and spoken to
the same midwife, or if the woman is admitted following telephone
advice.
I’ve often looked after women that I’ve had a telephone conversation with,
so you know when you meet her you say ‘oh yeah, I spoke to you’ and you
know there’s rapport there immediately because you’ve already had a
good conversation.
(S7)
The midwives also felt that there may be an additional benefit of
increased rapport between women and midwives because more women
are being admitted in established labour, therefore there is more
likelihood of continuity of carer for the birth.
3.5.7 Possible disadvantages
There was a general feeling that Part 1 of the Pathway is a positive
intervention for women and midwives. However, there were some
concerns highlighted in the questionnaire responses. These included a
concern that the Pathway is rigidly applied by some midwives who are
over-reliant on the format and are not exercising their clinical judgement.
This would appear to contradict the dominant view in the focus groups
that the Pathway is a flexible framework that is used to complement
clinical judgement. Furthermore, a concern was voiced that some women
may not give an accurate picture of their labour if only asked the list of
questions set out in Part 1 documentation. There is undoubtedly variation
between midwives in this regard and these concerns may reflect some
midwives’ lack of confidence or knowledge. This could suggest an
opportunity for professional development.
There was also a concern that some women may feel the telephone call to
be an impersonal question and answer session and would prefer face-to-
face contact with a midwife. Certainly, the inability to build a rapport
could pose a problem and may depend upon the individual personalities of
the woman and midwife. However, this was not an issue raised by the
focus-group midwives who asserted the positive aspects of conducting
telephone assessments.
One possible disadvantage raised both in questionnaire responses and by
focus-group participants was that some women might feel ‘put off’ and

The OPAL study
©NCCSDO 2007 97
prefer to come to the hospital/Birth Centre for an early labour
assessment:
I still do feel like some of ours feel like they are being put off.
(N1)
This is clearly a slightly sensitive area. Many focus-group participants
emphasised that they were happy for women to come in if they needed
reassurance, even though there was also recognition that it was better for
women to stay at home. However, they rejected the facilitator’s query
that this might be counter to the Pathway philosophy of discouraging
women from coming into hospital too early.
I wouldn’t say it’s to discourage them, rather to let them know it’s OK to be
at home, also that they are welcome to come in if they are concerned.
(N4)
3.6 Midwives: discussion
Only two instead of the four originally planned focus groups were
convened; thus fewer midwives contributed views than had been hoped
and only from a limited number of Trusts in Wales. Two of the Trusts
participating in the study were not represented in the focus groups and
no questionnaires were returned from those units. One limitation of the
findings of the focus groups is that some midwifery experiences of Part 1
of the Pathway may, therefore, not have been captured. It is also possible
that midwives who attended the focus group were more positive about
the Pathway; thus some element of selection bias may have occurred.
One strength of using focus groups is that it facilitates discussion among
participants, rather than obtaining their views in isolation in individual
interviews. It allows exploration of topics to determine whether views are
widely held and to check consensus. It appears that participants felt
happy to talk freely and without the guardedness that can sometimes
manifest in discussions of mixed staff groups.
Several issues related to midwives’ experiences of using Part 1 of the
Pathway emerged during the focus groups. Midwives appreciate the
Pathway as it supports midwifery practice; in particular, conversations
with labouring women. Telephone assessment for labouring women was
seen to encourage dialogue between women and midwives, which was
described as ‘bringing back the conversation in midwifery’. This enhanced
communication was also seen as an opportunity to build rapport.
Part 1 was perceived as offering a good teaching aid and documentation
of telephone conversations with women could also protect in cases of
subsequent complaint. Part I documentation appears not to be utilised in
some community settings, due to some continuing uncertainties over
when it should be used and also the practical difficulties for community-

The OPAL study
©NCCSDO 2007 98
based midwives of uniting Part 1 documentation with the main clinical
record. These practical difficulties could mean that women may not be
benefiting from the improved communication between care providers that
is a key aim of the Pathway. This issue is not reflected in hospital settings
where positive impacts on communication between women and care-
givers were perceived. Moreover, the midwives believed Part 1 acted as a
supportive framework to their clinical practice and had been instrumental
in changing midwives’ philosophy. The midwives also perceived that there
had been an overall reduction in unnecessary intervention for women as
they are less likely to attend Birth Centres or labour wards until their
labours are established. While generally acceptable to midwives, some
feel that the documentation could be shorter and it is interesting to note
that the evidence summaries included in Part 1 do not appear to be
utilised by some midwives. Midwives appear to have a range of views
about whether using Part 1 of the Pathway documentation offers a full
assessment of the woman’s situation or whether additional information is
required. The difficulties that midwives face in trying to encourage women
to remain at home while also not wishing to be seen to deny access are
clearly evident. This might mean that more work is required in providing
women with information during pregnancy about the rationale for
delaying admission until labour is established and in fulfilling what
midwives described as the education function of the Pathway. It was also
apparent that one Trust has adopted the use of Part 1 documentation to
capture all telephone data on the labour ward, irrespective of women’s
risk status and whether they are in labour.
3.7 Data collection from women
3.7.1 Method of data collection
The chosen method of data collection was via CATI. Telephone interviews
rather than questionnaires were chosen for the following reasons.
• We were interested in exploring women’s experiences and in
understanding the ways in which the process worked, or failed to
work for them. This is more easily achieved in a spoken dialogue
than with predetermined questions and responses.
• A brief telephone interview, particularly at a time nominated by the
interviewee, is less onerous for the respondent than completing a
questionnaire.
• If a woman wishes to take part but does not speak English it is easier
to find someone who can speak to her in her own language than to
produce printed questionnaires in all possible languages.
• Women who cannot read can be included.
The OPAL study
©NCCSDO 2007 99
• The sample should, ideally, be representative. Telephone interviews
yield higher response rates than self-completion questionnaires
(Crow et al., 2002) and are thus more likely to be representative.
Although telephone interviews run the risk of excluding women without
telephones, the availability of relatively cheap and easy access to pay-as-
you-go mobile phones has considerably reduced the number of women to
whom this would apply. Telephone interviews had been used previously
by members of our research team in studies involving new mothers
(Ewing and Green, 2000) and in other studies of maternity-service
provision (Statham et al., 2001). Face-to-face interviews with women
were never a realistic option given the project resources and the fact that
most of the research team were not based in Wales. However, our
previous use of telephone interviews with new mothers (Ewing and
Green, 2000) had suggested that telephone interviews were actually
preferred by mothers as being less intrusive, and thus more relaxed, and
easier to rearrange if necessary.
In addition to these advantages of telephone interviewing, the use of a
computer-assisted proforma has two major advantages: first, the
computer is able to route the interviewer to the next appropriate question
depending on the answers given. For example, if a woman made only one
phone call, she will not be taken to questions about a subsequent call.
Second, data are entered directly onto the computer so there is no need
for separate data entry. A possible disadvantage, however, is that a
woman may wish to say something that is of interest but which the
proforma does not have space for. To allow for this possibility and as a
back up, all interviews were also tape-recorded. The intention was not to
transcribe all the tapes in their entirety, but rather that the researcher
could note the sections of particular interest to be transcribed. This keeps
the workload manageable and allows us to:
• cover topics not fully covered by the CATI,
• allow verbatim quotation where this was desirable,
• check information entered into the CATI in situations where there
appeared to be conflicting information,
• be a back-up in case of computer failure.
3.7.2 Analysis of women’s data
The intention was to provide descriptive quantitative information
illustrated with direct quotations. Depending on the sample size achieved,
cross-tabulations and χ2 analyses would be carried out. In practice (see
below) the small sample size meant that only the most basic quantitative
analyses were possible and generally these required grouping categories
of responses together to avoid small cell sizes. Conversely, having less
data to analyse allowed us to give much more attention to individual

The OPAL study
©NCCSDO 2007 100
women’s experiences and we were able to go back to the tape recordings
to explore emerging themes in the data in a way that would not have
been possible with a larger sample.
3.7.3 Development of the CATI
The CATI software was developed using Microsoft Access 2000. The aim
was that the design should guide the interviewer through the interview to
ensure that all relevant questions were asked and recorded.
3.7.4 Early pilot work: mapping the key issues
Themes for investigation were developed by the research team, and
formatted into interview questions. We were keen to ensure at an early
stage that no areas of importance to women were omitted, so within the
first 3 months of the start of the project we piloted our themes and
questions with a group of postnatal women who had been to NCT
antenatal classes and were attending a postnatal reunion class. The
women were approached by the NCT leader during the reunion class, the
aims of the study and the pilot explained, and permission sought for us to
contact them by telephone. Those women agreeing to participate released
their details to us via the NCT leader. The basic eligibility criteria were
that women were primiparous; that they had not been booked for a
planned caesarean section or induction; they were well and their baby
was living with them and that a phone call had been made to the hospital
in early labour. Seven women were interviewed and their responses noted
on paper (rather than on computer).
We were aware of the possibility of some women reporting problems
during the telephone interviews that would indicate a need for support,
for example postnatal depression or breastfeeding problems. In order to
address this, the interviewers had available a list of suggested contacts
that could be drawn on for women who may need help that the
interviewers were not in a position to offer.
This list was kept for the final interviews, and contained the following:
• postnatal depression: discuss this with their health visitor or GP;
• breastfeeding: the NCT Breastfeeding Helpline can be accessed
8 am–10 pm every day on 0870 444 8708;
• bottle feeding: discuss with health visitor;
• own or baby's health: discuss with GP or health visitor;
• complaint about the maternity care they received: contact the Head
of Midwifery in the Trust where they had their baby.

The OPAL study
©NCCSDO 2007 101
This pre-pilot stage was very helpful in raising a number of issues that
needed to be resolved for the main interviews. The issues and their
resolution are listed below.
Methodological issues
• In some cases, the phone call to the hospital had been made by a
partner rather than the woman herself. This raised a dilemma about
how we dealt with third-party information. It was decided that where
the partner made the call this should be noted but that our principal
interest was in the woman’s experiences.
• A number of interviews were carried out with a baby crying in
background, which was clearly not ideal for anyone involved. This
raised issues about the time of day when interviews should be carried
out and also whether there was a need for a minimum set of
questions or more open questions that would allow key issues to
emerge if it was desirable to shorten the interview.
• Moving back and forward between pages for different phone calls
when asking questions was a challenge for the interviewers, which
underlined the desirability of a CATI which would enable this facility.
• How best to order the questions if more than one phone call was
made.
• Screening questions were devised as a check that women did meet
the eligibility criteria. These questions were to be asked prior to
setting a time and date for the telephone interview. In addition, brief
reminder information about the study and a preamble were devised,
which would be given at the start of the CATI, which included a
reminder of the interview being recorded and mention of
simultaneous entry on to the computer during the conversation.
Interview content: general
• We needed to be realistic about the level of detail that women could
be expected to recall up to 4 months after the event, for example
about the specific questions they had been asked and the advice that
they had been given.
• It was apparent that we needed to get an overview of labour to
contextualise the phone calls and timings even though we did not
require details of labour once the woman was in hospital. It was
agreed that this question would be asked first.
• Women were more inclined to want to talk about what had happened
to them after they reached hospital than about the phone calls.
However, information about the calls did seem to be available with
detailed questioning.
• It was apparent that awareness of the existence of the Pathway
varied and it was agreed that the interview would look for evidence

The OPAL study
©NCCSDO 2007 102
about this, including whether women made reference to the Pathway
leaflet and its contents. The terminology of the leaflet, for example
regarding signs of early labour, would exist as a drop-down list for
the interviewer on the computer but would not be used as a prompt
in questioning.
• Other questions which we agreed to include as a result of the pre-
pilot interviews were: demographics such as age and educational
attainment only; had the woman attended antenatal classes?; was
there a home visit from a community midwife?
Interview content: information about phone calls
• Were details to be collected on every phone call made? If not, which
were critical? After consultation with the Midwifery Officer (Welsh
Assembly Government), it was decided to collect basic information
about all phone calls that were made but to ask detailed questions
only about the first and last calls.
• Time of day of the phone call(s) should be noted.
• It was apparent that women had phoned the hospital for a variety of
reasons (e.g. to check bed availability; to notify onset of labour;
uncertainty about whether or not they were in labour; needing
advice; asking to come into hospital), and their expectations of the
call would vary accordingly.
• The pre-pilot interviews confirmed that we would want to detail the
specific advice given and to distinguish ‘advice’ from ‘assessment’.
The list of questions to be asked was further developed and reworded as
a result of the pre-pilot interviews.
In parallel with the development of the list of interview questions, an
database in Microsoft Access was developed with the assistance of IT
staff.
Key features of this were:
• drop-down menus for questions,
• capacity to add free text to certain questions,
• routing questions (if x then go to y; if not go to z),
• ability to repeat whole sections of questions (for different phone
calls),
• switch easily, using mouse and visually, between sections/windows of
interview schedule,
• data to be exportable to analysis program, e.g. SPSS.
A final check was completed by the software at completion of the
interview. The software incorporated drop-down options, rather than free
text, to aid data integrity and quantification.

The OPAL study
©NCCSDO 2007 103
3.7.5 Piloting the interview process
Prior to commencing the main study there was a need to pilot the
telephone interview questions and all post-recruitment procedures. The
midwifery research fieldworker obtained permission to attend an NHS
postnatal reunion group meeting and discuss the study with the women
present. There were 10 women in total who attended the group; four did
not meet the criteria for eligibility and the remaining six gave consent to
participate in pilot interviews. Their written consent and details were
forwarded to the research team.
The project secretary made the initial telephone contact, asking the
screening questions and then setting an agreed time and date for
interview, followed by a letter sent to the woman to confirm details. One
woman was found not to be eligible at this stage.
Since the researchers carrying out the interviews worked in part from
home, it was possible to offer a larger range of interview times (9 am–
9 pm) than would ordinarily have been the case. This was a particular
advantage in this study as it enabled women to arrange a time when their
partner would be at home and able to take over care of their baby where
necessary. In practice, the majority of interviews (in the pilot and main
data-collection phase) were carried out after 6 pm; this had an
unanticipated advantage of reducing the costs of telephone calls. Paper
versions of the CATI questions were used initially and then computer-
assisted interviews in the later cases.
Issues that arose from the main pilot phase included the following.
• There were issues around wording and drop-down menu options.
• The need to add to the preamble information about the anticipated
time the interview would take. The initial information had said 20 min
but many were taking longer than this. We also added additional
information about confidentiality, and the project’s credentials.
• The questions from the ELSA study were moved to the end as they
were found to trigger details that were going to be asked about in
other specific questions.
• Further probes were needed in the overview to get the sequence of
events, keys stages and how many times the woman went into
hospital.
• In some cases the last call consisted only of the partner phoning to
say ‘we’re on our way in’. It was agreed that in these circumstances
it would be more informative to collect detailed data on the
penultimate call but that the content of the last call would still be
noted.
• The interviewers were not always able to type answers to open-
ended questions fast enough to keep up with the conversation. It was

The OPAL study
©NCCSDO 2007 104
agreed that the CATI would be used mainly for choosing items from
the drop-down menus and for noting the number on the tape-counter
to go back and transcribe any details/specific quotes after the
interview was over.
Following this pilot, it was agreed that a final pilot stage would be useful
to test the changes to the schedule and gain practice in the computer
element of the CATI. Four women were recruited by their NCT leader at a
postnatal reunion class with the same eligibility criteria as before. The
CATI schedule is given in Appendix G.
3.7.6 Target sample
The target sample were women in Wales who had recently given birth to
their first baby and who had phoned the maternity unit at least once
when they thought that labour was starting. Women having subsequent
babies generally spend less time in early labour and they have a better
idea of the indications that they are or are not in labour. The issues are
therefore different for them. Because the ELSA trial was concerned only
with first-time mothers, it was appropriate to limit the OPAL sample in the
same way. We wanted to recruit women soon after they had given birth,
so that they would remember their early labour experiences, but to give
them time to recover from the birth and acclimatise to their new role.
Between 6 and 10 weeks after the birth was felt to meet this criterion.
This strategy for the provision of information to women and recruitment
by the women’s own community midwife was chosen for a number of
reasons: our positive experiences of community midwifery support for
recruitment in the ELSA trial, the opportunity for information to be offered
by someone known to the woman and thus avoiding potential ‘cold
calling’ associated with sampling from, for example, birth registrations,
and increased probability of avoiding distress if serious untoward events
have occurred.
The plan was that each of the 13 NHS Trusts in Wales would be asked to
recruit to the study all women at the point of discharge to the health
visitor for just one specified week (this was intended to minimise
demands on midwives). This would provide a sample of between 35 and
65 women per Trust, depending on the number of births per annum. The
weeks allocated to each Trust would be staggered over a 6-month period
to ensure a steady rate of recruitment, and thus a manageable workload
for the researchers, and to allow all women to be interviewed within 6–10
weeks of the birth. The Trusts were to be sampled in the order in which
they had introduced the Normal Labour Pathway to ensure that the
Pathway methods were established by the time of data collection. Target
women were those being discharged from the care of the community
midwives during the study week.

The OPAL study
©NCCSDO 2007 105
3.7.7 Planned sample size
The method described above should have produced a sub-population of
approximately 600 women; that is, 4 per cent of the women in Wales who
give birth within a 6-month period and who are identified within a
structured sampling frame. It was estimated that approximately 50 per
cent of these would have been eligible for the Normal Labour Pathway
(approximately 300); these were the women who were to be the focus of
our data collection. We recognised that not all would agree to take part,
but we anticipated that the response rate would be high since the burden
of participation would not be great and many women welcome the chance
to talk about their labour experiences. We thus expected between 200–
250 interviews with women who were eligible for the Pathway. The option
of asking Trusts to recruit for 2 weeks instead of one, should it become
apparent that target numbers were not being met, was included in the
original proposal.
This is a large sample size for qualitative analysis, but, unlike many
qualitative studies, we wanted the sample to be large enough to be
representative. Much of the information required was to be entered
directly on to the computer by the interviewer at the time of the
interview, and these data would be suitable for basic quantitative
analysis. However, when it became apparent that only six Trusts would be
recruiting women and that we were running short of time, we revisited
our assumptions and, in discussion with SDO, decided that a sample of
100 interviews would still meet our needs if we did not attempt analysis
at the level of individual Trusts. This would require each participating
Trust to recruit for a 2-week period: the Recruitment Fortnight.
A separate issue was that local information had suggested that more
women may fall outside the Pathway than we had previously been
advised. This underlined the need for a fortnight of recruitment rather
than 1 week. In order to be sure that the projected numbers for
recruitment were realistic, arrangements were made for a single
community midwifery team to record their total number of discharges and
the number of women who commenced Part 1 of the Pathway over a
4-week period. These were recorded on a proforma and collected by the
midwifery research fieldworker.
3.7.8 Recruitment in practice
As planned, women were recruited by their community midwife at the
point of discharge to the health visitor during a specified 2-week period,
the Recruitment Fortnight. Recruitment took place in only six NHS Trusts:
Gwent, North Glamorgan, Cardiff and Vale, Swansea, Ceredigion, and
Conwy and Denbighshire. The timing of the Recruitment Fortnight was
negotiated individually with each Trust as soon as R&D clearance was

The OPAL study
©NCCSDO 2007 106
obtained. All Trusts had been operating the Pathway for over a year by
this point. Some Recruitment Fortnights ran concurrently. The main
recruitment phase ran from the end of May until the end of August 2005.
3.7.9 Informing women about the research
Protocol 1 Women whose expected date of delivery was such that they
may be discharged from midwifery care during the Recruitment
Fortnight were given written information about the research
(Appendix H) along with the information that, we understood, they
received routinely about the Pathway, at approximately 36 weeks.
This information was to be distributed during a 4-week period,
2–6 weeks prior to the Recruitment Fortnight, to allow for variations
in gestation. Women were encouraged to contact the research team
in York for any further information or to speak with the Wales-based
midwifery research fieldworker. Flow chart 1 identifies the key steps
in recruitment, and the timescale associated with each step in
relation to the Recruitment Fortnight.
Protocol 2 The delays in obtaining R&D approval resulted in the need to
recruit during a much shorter period than the 6 months that had
been planned. Furthermore, the original protocol described above
required a substantial ‘lead time’ before recruitment because women
were being approached while still pregnant. A protocol amendment
was submitted to Multicentre Research Ethics Committee, and
approved, in which study information was distributed postnatally
rather than antenatally, in the week prior to being discharged to the
health visitor. Flow chart 2 outlines the revised format. Information
about the study was distributed by community midwives in the week
prior to the Recruitment Fortnight and during the first week of the
Recruitment Fortnight, which gave women approximately 1 week to
consider participation. The information sheets were to be given to all
primiparous women who the midwife anticipated discharging to the
health visitor during the Recruitment Fortnight. This meant that
during the first week of the fortnight there was an overlap of
information-giving and recruitment; the recruitment was of women
who had received the information in the week prior to the
Recruitment Fortnight and the information sheet was distributed to
women who were expected to be discharged during the second week
of the Recruitment Fortnight.
This procedure was modified slightly in two Trusts that were operating
selective visiting in the postnatal period. Here midwives requested a
2-week information distribution period prior to Recruitment Fortnight to
ensure that eligible women were not missed due to the length of time
between visits. During the main data-collection phase, one Trust followed
Protocol 1 (Flow chart 1) and five Trusts followed the amended format
(Flow chart 2).

The OPAL study
©NCCSDO 2007 107
Recruitment flow chart 1
Recruitment Fortnight (Recruitment Fortnight)=2 weeks during which primiparous
women will be recruited and ‘consented’ by community midwives.
Recruitment Fortnight minus 7 weeks Contact with community midwifery
staff to flag up Information Sheet distribution period (to begin in
following week for 4 weeks) and send bulk copies of information
sheet.
Recruitment Fortnight minus 6–2 weeks For next 4 weeks, women
attending antenatal appointments for their 36-week check-up will be
handed information sheet at same time they are given information
about the Pathway from the midwife.
Recruitment Fortnight minus 1 week Contact with community midwives
teams to flag up Recruitment Fortnight and explain what we need
them to do and collect. Leave bulk copies of the proformas (with
attached consent form).
Recruitment Fortnight Women are recruited by community midwives.
Proforma completed for each primiparous woman being discharged
that week into the care of health visitor (usually 10–28 days after
birth). Woman consents to take part and release details to research
team in York.
Recruitment Fortnight plus 1–2 weeks Woman contacted by research
team to book a date/time for phone interview. Woman encouraged to
contact York in meantime if any questions or changes to
arrangements or to withdraw.
Recruitment Fortnight plus 4–8 weeks One week prior to arranged phone
interview, a letter is sent to remind woman of date/time and key
areas we are interested in covering in phone interview. Option for
woman to change arranged time/date or to withdraw.
Recruitment Fortnight plus 5–9 weeks Phone interviews take place.
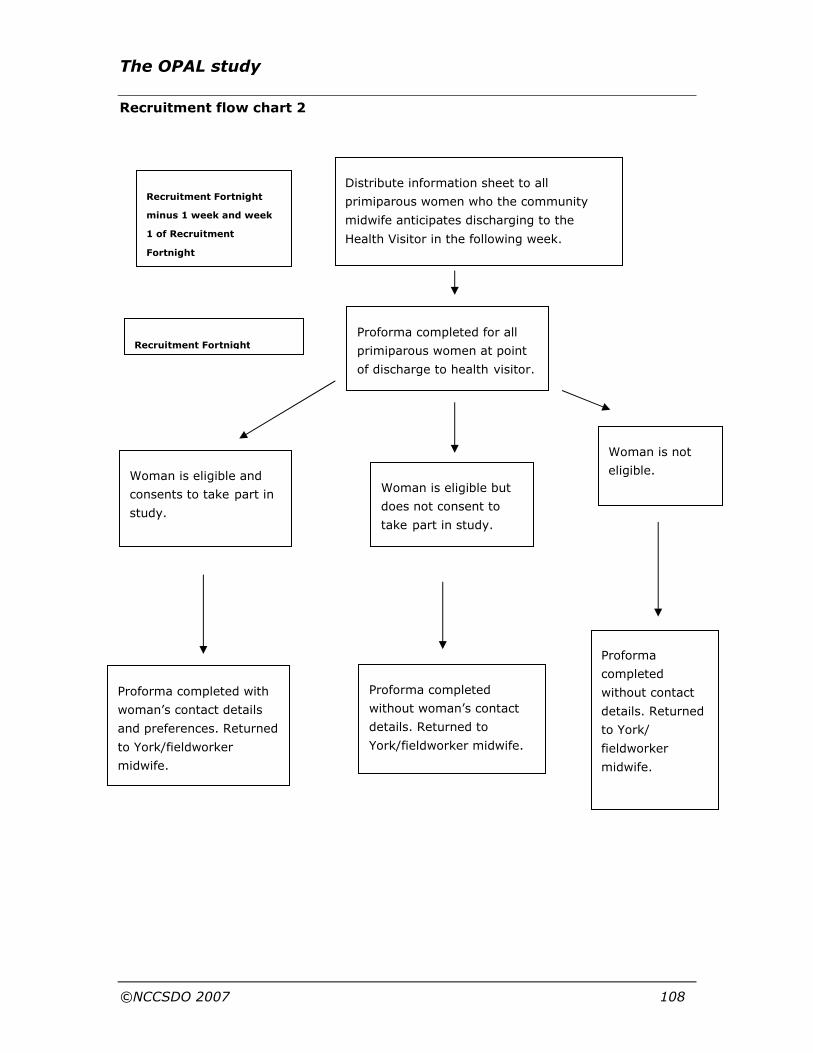
The OPAL study
©NCCSDO 2007 108
Recruitment flow chart 2
Distribute information sheet to all
primiparous women who the community
midwife anticipates discharging to the
Health Visitor in the following week.
Proforma completed for all
primiparous women at point
of discharge to health visitor.
Woman is eligible but
does not consent to
take part in study.
Proforma completed
without woman’s contact
details. Returned to
York/fieldworker midwife.
Proforma completed with
woman’s contact details
and preferences. Returned
to York/fieldworker
midwife.
Woman is eligible and
consents to take part in
study.
Proforma
completed
without contact
details. Returned
to York/
fieldworker
midwife.
Woman is not
eligible.
Recruitment Fortnight
minus 1 week and week
1 of Recruitment
Fortnight
Recruitment Fortnight

The OPAL study
©NCCSDO 2007 109
3.7.10 Recruitment of women at discharge
Following the birth and at the point of discharge to the health visitor, the
community midwife reminded women about the research (offering
another information sheet if necessary). The midwife was asked to
complete a short proforma (Appendix I) for every primiparous woman
indicating her eligibility for the Pathway (and reason for ineligibility if
appropriate) and then document whether or not she consented to
participate; women agreeing to participation signed a consent form.
For women who were eligible for the Pathway, and who consented to
participate in the study, the midwife obtained basic details to be
forwarded to the research team which included: the woman’s name;
contact telephone number; preferred time of day for a telephone call;
whether she was willing to be interviewed in English and, if not, her
preferred language; and any special circumstances that the research
team should be aware of, such as admission of the mother or her baby to
intensive care facilities around the time of birth. Contingency plans were
made for interviews to be carried out in Welsh if requested.
The names of women who did not consent to the research or who were
ineligible were not to be entered onto the proforma. However, since we
needed to monitor the number of women who fell into these categories,
midwives were asked to complete a proforma for every primiparous
woman discharged during the Recruitment Fortnight. The proformas and
completed consent forms were returned to the central community
midwifery office for Gwent following protocol 1. Other Trusts were
provided with freepost envelopes to return completed documentation
directly to the research team in York, at the end of the recruitment
fortnight. We were advised that help with translation of the information
sheet was available from the resources of the Welsh Assembly
Government.
3.7.11 Preparing community midwives for Recruitment
Fortnight
In advance of the recruitment period for each Trust, meetings were
arranged with community midwives, sometimes with considerable
difficulty due to their already full meeting agendas. Assistance was sought
from the community midwifery managers to determine suitable dates and
venues. Liaison took place through telephone calls and e-mails. The
meetings took place in order of obtaining Trust approval, and the
Recruitment Fortnight dates negotiated.
Each group of midwives was given a short PowerPoint presentation that
included an overview of the study, their role in assisting the team with
recruitment and their individual time frame for distributing information

The OPAL study
©NCCSDO 2007 110
and dates for Recruitment Fortnight. Following the presentation
information packs containing consent forms, proformas, a flow chart plus
women’s and midwives’ information sheets and stamped, addressed
envelopes for return to either the community office or research base were
distributed to the midwives and the recruitment process was explained in
detail. This further explanation gave an opportunity for clarification and
allowed for further discussion around the recruiting process. The
midwives attending the meeting tended to be the lead midwife for each of
the community teams, who were then responsible for cascading
information about OPAL to their colleagues.
The first Trust (Gwent) to participate in the study followed the original
protocol that gave an information-distribution period of 6 weeks before
their Recruitment Fortnight. Due to the length of this lead-in period there
was an opportunity to meet with at least 50 per cent of the total
community midwives. This was achieved through holding three meetings
at different venues and capitalised on fitting in with pre-arranged
meetings; this was only possible because this was the midwifery research
fieldworker’s own Trust. Subsequent Trusts followed the amended
protocol that shortened the process of information distribution and
recruitment to 3-4 weeks in total and gave less opportunity to meet
individual community midwives.
3.7.12 Maintaining contact during Recruitment
Fortnight
The ability to maintain direct contact with the midwives during the
recruitment process varied according to the proximity of the Trust to the
midwifery research fieldworker’s own workplace. North Glamorgan,
Conwy, Ceredigion and Swansea Trusts received one visit prior to their
recruitment period. Telephone and e-mail contact was maintained with
the managers to provide support and to chase up any possible
outstanding consent forms at the end of Recruitment Fortnight. Gwent
and Cardiff and Vale Trust received site visits at the end of the first week
of Recruitment Fortnight in addition to telephone contact. Site visits
appeared to be valued by the midwives as they were able to clarify the
eligibility of women who they thought may consent to the study and ask
questions about OPAL. However, only three midwives made direct
telephone contact despite being given the midwifery research
fieldworker’s and the team’s e-mail and telephone numbers plus a direct
pager number carried by one of the co-principal investigators identified as
a midwife during the re-run of the Recruitment Fortnight.
3.7.13 Arranging interviews
Some delays occurred in completed documentation being received at the
study base. On receipt of the consent forms and proformas, the research
The OPAL study
©NCCSDO 2007 111
team checked details and calculated in which weeks it would be
appropriate to interview the women, given they were to be interviewed
between 6 and 10 weeks postnatally. The initial phone call to set up the
interview was made by the project secretary or a Research Officer.
Screening questions were asked to confirm eligibility. Ineligible women
were thanked for their willingness to participate and no interview was
arranged. For all other women, an agreed time and date was set, and this
was confirmed in writing.
In a small number of cases it proved difficult to contact the woman on the
phone, and after several attempts had been made, a letter was sent to
check if the woman was still willing to participate and asking her, if
applicable, to confirm her contact details so we could make telephone
contact. A freepost envelope was included to ensure no costs were
incurred by the woman. If this letter was not returned, no further contact
was attempted.
The researcher conducting the interview phoned at the arranged time. In
some cases there was no answer, and after trying for up to 15 min after
the arranged time, the interview was abandoned on that date. A follow-up
call was made to try and arrange an alternative date and in all but one
case this was achieved. Where this was not possible, a letter similar to
the one above was sent thanking the woman for agreeing to participate
and checking whether she no longer wished to take part.
3.7.14 Recruitment response
In view of the considerable efforts invested in the recruitment process,
the response was disappointing. Only 53 forms were returned: of these
16 were not eligible and 14 did not consent, withdrew or could not be
contacted. Thus only 23 interviews could be carried out. As far as we
were able to determine, women who were asked were mostly willing to
take part but only a minority of community midwives seem to have
attempted to recruit women. This was despite a system of reminders and,
for the last two centres, an ‘on-call’ system for enquiries. The extent to
which midwives recruited did not appear to relate to the amount of input
from the midwifery research fieldworker. Two Trusts had visits during the
Recruitment Fortnight, but one of these had one of the lowest numbers of
returned proformas and consent forms whereas Conwy and Denbighshire
Trust, who were most geographically distant and who were only visited
prior to their Recruitment Fortnight, had the highest number of consent
forms per caseload number.
The poor response was discussed with midwifery managers who
expressed willingness to run a second phase of recruitment. SDO kindly
agreed to a further no-cost extension until 31 March 2006 to allow this to
take place and it was agreed that we would repeat the recruitment
strategy that we had used before, this time with a higher profile and more

The OPAL study
©NCCSDO 2007 112
support to the community midwives. We felt that the most effective
strategy was to limit this second recruitment phase to the three largest
Trusts (Gwent, Cardiff and Vale and Conwy and Denbighshire) where we
would be likely to get the highest numbers of recruits. We expected to at
least double the total number of interviews in this way. We considered a
change of recruitment strategy, but this would have required a new round
of negotiation with Multicentre Research Ethics Committee and R&D
departments which would have been time consuming.
3.7.15 Alternative strategies considered
A number of other strategies were also considered for accessing women’s
views and experiences. These included face-to-face recruitment by the
midwifery research fieldworker of women being discharged from the
postnatal ward; this was rejected as it could not be accommodated
alongside the midwifery research fieldworker’s duties in her substantive
post; it would have required submission and approval of a protocol
amendment and also precluded the continued support to other Trusts. We
were particularly attracted to the idea of focus-group discussions with
women. These had not been part of the original plan but we felt that they
might add another, richer, dimension which would augment the interview
data. These, ideally, would be carried out with pre-existing groups of
women such as a postnatal reunion of an antenatal class or groups of new
mothers in SureStart areas. The difficulty was that accessing women via
NHS routes would again necessitate a further round of negotiation with
Multicentre Research Ethics Committee and Trusts’ R&D departments,
which would have introduced substantial delays. We explored a number of
avenues for accessing women via non-NHS routes but, unfortunately,
time pressures were such that these plans had to be abandoned as
impossible within the time frame.
3.7.16 Phase 2 recruitment procedures
The community managers were re-contacted to arrange suitable dates to
meet with the community midwives. The Recruitment Fortnight dates, all
in November/December 2005, were agreed between the team and the
Trusts. All Trusts followed the second recruitment protocol. Due to time
constraints and the timing of their meetings dates, Conwy midwives did
not receive a presentation but we were assured that they were happy to
proceed without this. Following a detailed telephone conversation
between the co-principal investigator and acting manager that clarified
expectations and processes, the manager was sent recruitment packs
with covering letters to distribute to the midwives. Contact was
maintained via e-mail and telephone during their period of recruitment.
The midwifery research fieldworker made presentations to both Gwent
and Cardiff midwives to remind them of the aims of the study, the

The OPAL study
©NCCSDO 2007 113
recruiting process and provide an update on progress made. Recruitment
packs were distributed to the team leaders present. Because both Trusts
in the south ran their recruiting periods during the same weeks some of
the midwife packs were sent directly to named individuals with a covering
letter.
An addition to the midwives’ packs was a sheet of 14 stickers with the
recruiting dates printed on them. The aim of the stickers was for
midwives to place a sticker on each page of their work diary (where all
midwifery work and postnatal visits are recorded) to remind them to
inform women of OPAL and to try to recruit them to the research. As with
Conwy Trust contact was maintained via e-mail and telephone with the
managers, who were asked to remind midwives of the importance of
recruiting women and returning completed documentation.
3.7.17 Final recruitment figures
Figure 3.1 Recruitment response (phases 1 and 2 combined)
Regrettably, the response from the second recruitment phase was no
better than the first. Twenty-five forms were returned: of these six were
not eligible and five did not consent, withdrew or could not be contacted,
resulting in a further 14 interviews carried out. The final total figures are
shown in Figure 3.1. We were also able to include data from nine women
who had been interviewed as part of the pilot, yielding a final total of 47
interviews. However, one of these was with a woman having a planned
home birth who made no calls to the maternity unit, only one brief call to
Completed
proformas returned
N=78
Eligible and
Consented
N=42 (54%)
Not eligible
N=22 (28%)
Did not consent
N=14 (18%)
Withdrew, not
contactable or
failed to respond to
recontact N=4 (5%)
Interviewed
N=38 (49%)
46 valid interviews
One interview
not included*
9 pilot
interviews
included
*planned home birth, no calls to the
maternity unit

The OPAL study
©NCCSDO 2007 114
notify her community midwife of labour onset. Since most questions did
not apply to her, this interview has not been included, although we
understand that the care of women giving birth at home is included in the
Pathway.
3.7.18 Sample characteristics
Just over half the sample had an expected journey time of 15 min or less.
However, six women (13 per cent) had a journey time of 30 min or more,
reflecting the rurality of many areas of Wales. The sample is somewhat
older, and probably better educated, than first-time mothers in Wales as
a whole, as shown in Appendix J. This will, to some extent, be because
young and less-educated women are less likely to agree to participate in
research. It may also reflect selection bias at recruitment by community
midwives.
Just over half (n=24) of the births were spontaneous; instrumental
deliveries accounted for just under one-third (n=14) and six women had a
caesarean section. Table 3.1 shows the comparable figures for the whole
of Wales for 2003/2004. However, it is difficult to say to what extent our
sample is representative, since women were all low-risk primiparas. The
low number of caesarean sections, however, probably does reflect a
sampling bias.
Table 3.1 Mode of birth
Frequency Percentage
National percentage 2003/2004*
Spontaneous 24 52.2% 67.1%
Caesarian section
6 13.0% 23.8%
Instrumental 14 30.4% 8.8%
Missing 2 4.3%
Total 46 100.0%
*Taken from Health Statistics Wales (2006), www.wales.nhs.uk/page.cfm?pid=739.
3.8 Women: findings
We will first present descriptive quantitative information on women’s
experience of Part 1 of the Pathway. Following that we will focus on
women’s satisfaction and its determinants, first based on statistical
analyses and then drawing on women’s qualitative descriptions. This is
followed by a further focus on antenatal preparations and expectations
which emerged as an important issue.

The OPAL study
©NCCSDO 2007 115
Our focus is on the sequence of communications that women had with the
maternity unit from their first phone call through to going to hospital for
the last time. As we shall see, the range of experiences was substantial.
To demonstrate this and as an aid to identifying the pattern of events for
individual women we have illustrated the trajectories of all 46 women in
the flow charts given as Figures 3.2–3.6. Because women’s later
communications with the maternity unit all built on the first contact and
the advice given, we have grouped women according to the response that
they received to their first call: first the 21 women who were asked to
phone back (Figure 3.2) and then those who were asked to come in
(n=18; Figure 3.3). The two additional flow charts show the alternative
paths followed by the seven women who did not fit either of these two
main groupings. It may be helpful to refer to these flow charts in later
sections when individual women’s experiences are discussed in more
detail. Accordingly each woman’s code number (e.g. Z201) occurs at the
end of her branch on the diagram so that her route can be followed. Each
letter U–Z represents a different NHS Trust. A letter P as a prefix
indicates that the woman was interviewed as a pilot.
3.8.1 Descriptive information of women’s experience
of Part 1 of the Pathway
Process issues
Only one woman said that she had encountered problems getting through
on the telephone to the delivery suite. Over a third (n=18) said that they
received the impression that the unit was busy when they telephoned but
very few women (n=4) experienced interruptions to their phone calls.
Over two-thirds (n=32) said that they were not aware of being taken
through a preset list of questions on the phone and the vast majority
(n=40) felt they were able to raise all the issues they wanted to during
the calls. All phone calls were conducted in English, which was the
language of choice for most women, but two would have preferred Welsh.
Most women were quite happy about the conversations being on the
phone rather than face to face, but five women said that they were not
comfortable with it, saying that it was not as personal; they felt awkward
or were just unhappy about it.
Being treated as an individual and treated with respect
Women were asked if they felt that they were treated as an individual and
also whether they were treated with respect. Over three-quarters (n=36)
said they felt as if they were treated as an individual on the phone by all
staff, although six women felt treated as an individual by only a few staff
or not by any. Similar figures were reported for feeling treated with
respect: three-quarters (n=36) felt that they were treated with respect by
all staff; five by only a few staff or not at all (see Appendix J). For

The OPAL study
©NCCSDO 2007 116
subsequent analysis a new combined variable was created: women who
felt treated as an individual and with respect by all staff (n=34) and those
who did not (n=9; responses were missing for three women).
Prior awareness of the Pathway
Table 3.2 demonstrates that a little over two-thirds of the women (n=32)
said they were aware of the Pathway. Seventeen women had discussed it
with their midwife while discussing their birth plan. Twenty-seven women
said that they had attended antenatal classes and 11 said that the
Pathway had been discussed there. Women were not asked directly
whether they had received a copy of the Pathway leaflet, but, when the
qualitative analysis suggested that this might be an important variable,
we went back to each of the interviews and extracted this information.
Twenty-six women were evidently familiar with the leaflet; the remaining
20 were not, or made no reference to it. These relatively low numbers
suggest that there may be scope for improving women’s awareness of the
Pathway, and its rationale and purpose.
Table 3.2 Awareness and discussion of the Pathway
Yes No Not sure/missing/not applicable
Total
Aware of Pathway 32 (69.6%)
13 (28.3%)
1 (2.2%) 46
Discussed Pathway in birth plan*
17 (37.0%)
18 (39.1%)
11 (23.9%) 46
Attended antenatal classes
27 (58.7%)
18 (39.1%)
1 (2.2%) 46
Discussed Pathway at antenatal class
11 (23.9%)
8 (17.4%)
27 (58.7%) 46
Had a leaflet* 26 (56.5%)
– 20 (43.5%) 46
*We had not asked women directly whether they had had a Pathway leaflet (see
above).
Women's awareness of where and when to call
The vast majority of women (n=44) knew where to phone: the central
labour and delivery suite. Nearly a quarter (n=12) did not know, or were
unsure, of when it was appropriate to telephone. The Pathway leaflet (see
Appendix D) does not tell women this explicitly. The statement ‘you are
advised to contact a midwife at this stage’ appears in the column headed
‘Active Labour – 1st Stage’. It is implicit that the events in the column
headed ‘Very early labour’ have already occurred. These include
‘Contractions feel uncomfortable but are not yet regular’ ‘You may pass a
“show”; the plug of mucus is released from your cervix. It can be

The OPAL study
©NCCSDO 2007 117
streaked with blood. Your waters may break.’ Since these signs are only
‘maybes’, the only definitive sign that the Pathway leaflet offers is that in
‘Active Labour’ ‘Contractions are coming regularly about every 5 minutes
(or more frequently) and lasting 20–60 seconds’. When women were
asked what signs they were looking out for (Appendix J), it is therefore
not surprising that ‘contractions’ was the most frequently mentioned sign
(n=26; 56.5 per cent); indeed, it is perhaps surprising that more women
did not give this response.
The frequency of contractions that women were looking out for and the
frequency that actually prompted them to phone may have been different
from the guidance in the leaflet. Of the 26 respondents saying they were
looking out for contractions, half mentioned that the contractions should
be 5 min apart or less, as indicated on the Pathway leaflet; two identified
10 min as the interval; seven respondents did not mention any specific
interval between contractions, just that they were definitely occurring or
were painful, regular or stronger.
Making telephone contact in early labour
The 46 respondents made a total of 104 calls, as shown in Table 3.3. Two
calls was the modal response (n=19); just over one-third of the sample
made more than two calls (n=16). Two women made five calls. Just over
half of the women (n=24) made no contact with other sources of advice
in early labour, whereas 16 made contact with their mother or other
female relative. Over three-quarters (n=36) had their partner present
when they made the first phone call, but eight were alone. Just over half
the first calls (n=27) were made during the day, between 6 am and 6 pm.
The time interval between the first and last call was 12 h or less for 82.6
per cent of the sample (n=38; including the 11 women who only made
one call). For two women, the calls were spread over a period of 2 weeks
(see Appendix J, Tables J7–J10).
Table 3.3 How many times did you phone the hospital?
How many times Frequency Valid percentage Cumulative percentage
1 11 23.9 23.9
2 19 41.3 65.2
3 11 23.9 89.1
4 3 6.5 95.7
5 2 4.3 100.0
Total 46 100.0
What prompted the phone calls
Rupture of membranes was the most common event that prompted
women to make the first call (Table 3.4), cited by just over one-third of

The OPAL study
©NCCSDO 2007 118
women, with contractions and pain being next most common, although
contractions may not have been 5 min apart when they phoned. Pain
prompted most of the last calls (16 out of 35 with a second call), with
contractions being the next most common reason (Table 3.4).
Table 3.4 What prompted you to phone (first call and last call)?
First call Last call
n % n %
Waters broken 16 34.8 2 4.3
Contractions 10 21.7 10 21.7
Pain 9 19.6 16 34.8
Bleeding 5 10.9 – –
Concern for baby’s health
– – 1 2.2
Prearranged time to call back
n/a – 3 6.5
No second call n/a – 11 23.9
Other 6 13.0 3 6.5
Total 46 100.0 46 100.0
Details of the first and last phone calls
Table 3.5 shows that the majority of first phone calls (n=25) were of less
than 5 min duration. This is in contrast to the impression that emerged
from the focus groups with midwives and we will return to this point
below. Of the 23 cases where times were given for last calls, half (n=11)
were less than 5 min.
Table 3.5 Duration of first and last phone calls
First call Last call Call length
n % n %
<5 mins 25 54.3 11 47.8
5–10 min 20 43.5 12 52.2
10+ min 1 2.2 – –
Total 46 100.0 23 100.0
Few respondents (n=6) knew the midwife that they spoke to on the phone.
The questions asked most commonly by the midwife related to frequency
of contractions and details about the type of vaginal loss (Appendix J).
Only 28 women (60.8 per cent) said that they were asked how they were
feeling.

The OPAL study
©NCCSDO 2007 119
Advice to attend or to stay at home
First phone call
At the first phone call, just over one-quarter of the sample (n=12) were
asked to attend the unit immediately and another five to ‘make their way
in when ready’. The most common advice was to remain at home and to
phone again later (n=21). Details are shown in Appendix J.
The likelihood of being asked to come in was related to whether or not
the woman’s waters had broken. Twelve of the 17 women who were
asked to attend had ruptured membranes (eight asked to attend at once;
four ‘when ready’) in contrast to only five of the 21 who were advised to
stay at home. Women advised to stay at home were given varied
instructions about when to phone back, as Table 3.6 shows, but the most
frequent was ‘when labour advances’.
The advice and instructions given on the first call were as expected in the
majority of cases (n=27). However, just over one-third of respondents
(n=16) said that it was not what they expected or that they were unsure
about what they had expected to be told.
Table 3.6 What were you told on the first phone call?
Frequency Percentage
Asked to phone back
Ring back when labour advances 14 30.4%
Ring back at a certain time 4 8.7%
Ring back if concerned 2 4.3%
Ring back to update hospital on progress 1 2.2%
Asked to come in
Attend unit 12 26.1%
Make way in when ready 5 10.9%
Come in if you like 1 2.2%
Alternative routes
Call back/asked to come in 24 h 3 6.5%
Contacted own midwife 2 4.3%
Had planned contact with community midwife/hospital just before labour onset – asked to phone back
2 4.3%
Total 46 100.0%
Sub-headings refer to flow chart routes (Figures 3.2–3.5).

Figure 3.2 Individual women’s sequence of events: women asked to
phone back at first call (n=21)
Key
Advice given on phone call
What happened
APB
ATCI
CMW
codes (e.g. PX08)
Asked to phone back
Asked to come in
Community midwife
Participant ID
APB n=21 1st
call
CMW will visit
n=1
ATCI n=16
APB n=4
Went in, returned
home n=5
Went in and stayed
n=11*
Went in and stayed
n=1
2nd
call
Re-attended without phoning and stayed
n=2
ATCI n=3
APB n=1
3rd
call
Went in and stayed n=2
Went in, returned home
n=1
Went in and stayed n=2
Went in, returned home Re-attended without phoning and stayed n=1
ATCI n=1
ATCI n=1 4th
call
Went in and stayed n=1
ATCI n=1
5th
call
Stayed at home n=1
X201
Went in, returned home, re-attended without phoning, stayed in n=1
*went in and stayed after 2nd call
PX08, V01, W01, X205, X209, Y01, Y15, Y203, Z01, Z02, Z03
Z201 PY04 Y12
X02 Y20
U02 X211
Z16
Y03
ATCI n=3

The OPAL study
©NCCSDO 2007 121
Figure 3.3 Individual women’s sequence of events: women asked to
come in on first call (n=18)
Key: as for Figure 3.2
PY02 X210 PY01
Y17 PY05
ATCI n=18
Stayed at home n= 1
Went in and stayed n=8**
Went in, returned home
n= 9
ATCI n=1
ATCI n=3
APB n= 2
Re-attended without phoning n=4
Went in and stayed n=1
Went in and
stayed n=3
APB n=1
ATCI n=1
Went in and stayed n=1
Went in, returned home n=3
ATCI n=1
Went in and stayed n=1
Went in, returned home n=1
Re-attended without phoning and stayed n=2
ATCI n=1
APB n=1
Went in, returned home n=1
ATCI n=1
ATCI n=1
Went in and
stayed n=1 Went in and
stayed n=1
2nd
call
1st
call
3rd
call
4th
call
5th
call
Z09
Y14
Y204
Y205 Y206
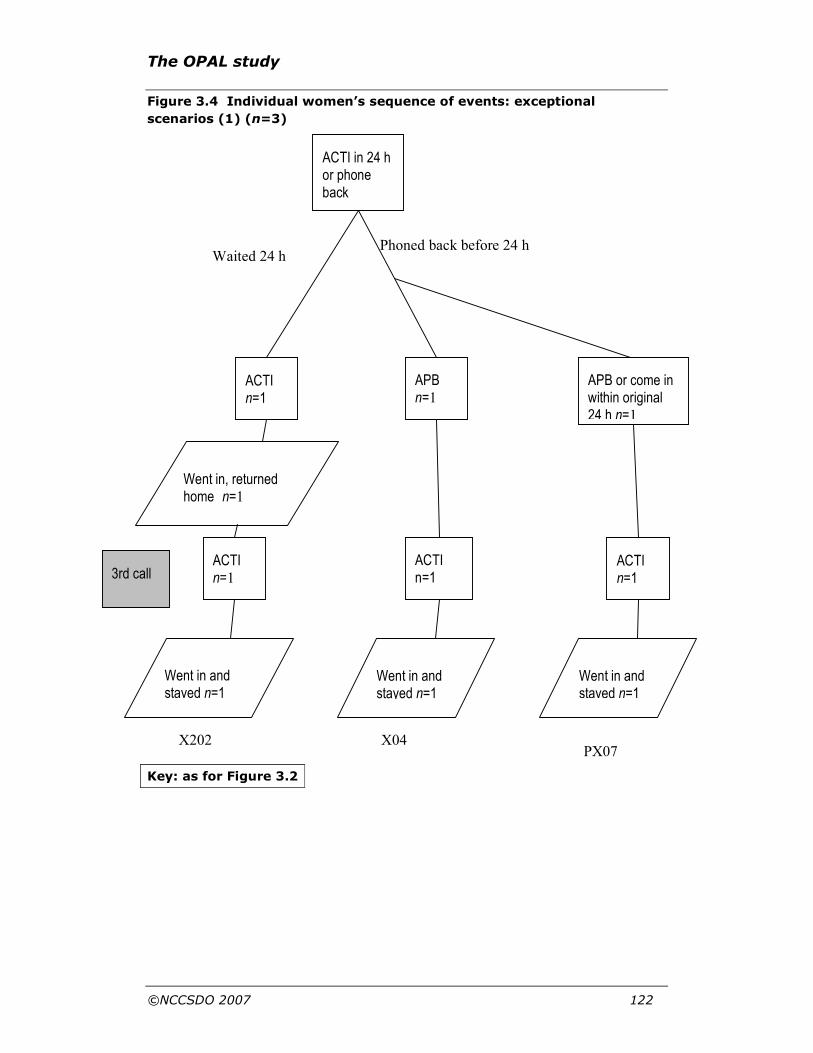
The OPAL study
©NCCSDO 2007 122
Went in, returned home n=1
ACTI n=1 3rd call
ACTI n=1
ACTI in 24 h or phone back
ACTI n=1
APB n=1
APB or come in within original 24 h n=1
Waited 24 h Phoned back before 24 h
X202 X04
Went in and stayed n=1
Went in and stayed n=1
Went in and stayed n=1
ACTI n=1
PX07
Figure 3.4 Individual women’s sequence of events: exceptional
scenarios (1) (n=3)
Key: as for Figure 3.2

The OPAL study
©NCCSDO 2007 123
Figure 3.5 Individual women’s sequence of events: exceptional
scenarios (2) (n=4)
Key: as for Figure 3.2
X204
[Prior to phone calls]
Antenatal check at home by
CMW. Attended for planned
induction
PY03
ATCI n=1
ATCI n=1
Went in and
stayed n=1
APB n=1
ATCI n=1
APB n=1
Went in,
returned home
n=1
Went in and
stayed n=1
APB n=1
Attended
without phoning,
went home n=1
APB n=1 APB n=1
Routine/planned
contact immediately
preceding early labour
n=2
4th
call
5th
call
3rd
call
X01
Contacted CMW for advice
n=2
Stayed at
home n=2
Attended without
phoning, went
home n=1
ATCI n=1 1st
call
ATCI n=1
Went in, return-
ed home n=1
ATCI n=1
Z10
Went in and
stayed n=1
Went in and
stayed n=1
2nd
call

The OPAL study
©NCCSDO 2007 124
3.8.2 Advice while staying at home
Advice for women staying at home at the first call was, most
commonly, to have a warm bath (n=19) and take paracetamol
(n=17); Table 3.7 also demonstrates that six respondents said they
had not received any or couldn’t remember what the advice was.
Table 3.7 What advice were you given on phone (first call)?
Frequency Percentage
Warm bath 19 41.3%
Paracetamol 17 37.0%
Keep active 8 17.4%
TENS machine 5 10.9%
Rest 5 10.9%
Diet/food/drink 5 10.9%
Breathing/relaxation/postural change 4 8.7%
Keep calm/take it easy 2 4.3%
Other
Regarding coming in 2 4.3%
Regarding phoning back 2 4.3%
Contact own midwife 1 2.2%
Drink cold water to stimulate fetal movement 1 2.2%
Keep eye on show 1 2.2%
This was an open-ended question. Answers are given in order of frequency. The
total is >100 per cent because women gave multiple responses.
Most women said that the advice was as expected but some had no
expectations
I was not sure what to expect as I’d not done before. I didn’t know
about paracetamol.
(Z01)
and others felt that their need for support was not met:
I think I was expecting more, I was expecting how to be advised to look
after myself. My Mum said to have a warm bath. I wasn't given any
advice about how to control the pain. I came off the phone and was like
'oh, that's all it was'. I had no advice on what to do.
(Z03)
The rationale for the advice was not always understood.
I was asked to come in in 24 hours – it wasn't explained why in
24 hours.
(PX07)

The OPAL study
©NCCSDO 2007 125
Feelings about staying at home after phoning
Thirty-four women were not asked to come in straight away on their
first call and they were asked whether they had felt confident to stay
at home. Most (n=30/34) said that they did. They were then asked an
open-ended follow-up question, ‘What do you think made you feel that
way?’ In most cases (n=18) women associated this with ‘feeling OK in
myself’. Reasons cited by the four women who did not feel confident
to be at home were: distance from hospital; being alone; not knowing
what was happening; and feeling unprepared as the antenatal classes
had been cancelled.
The majority (n=28) of the 34 women staying at home after their first
call felt they had been given enough advice from the midwife on the
phone to stay at home. Of the four women who did not feel they had
had enough advice to stay at home, one commented on the brevity of
the call as the reason why she did not feel she had enough advice on
the phone; the remaining three expressed an unmet need for
knowledge and information:
I wouldn’t have known what to do if anything had happened. You hear
about some babies being born very quick, but I wouldn't have known
what to do.
(Y12)
Of the 10 women who were not asked to come in to the unit straight
away on their last call, all were confident to stay at home: five felt
confident because of themselves and how they were feeling; two
because of their partner; one because of their mother and two
because of the midwife on the phone:
She was quite thorough, told me loads of things to be aware of, I felt
quite safe coming off the phone to her.
(X04)
In most cases (n=27) partners felt the same way about the woman
staying at home.
Feeling encouraged to be at home in early labour
All women were asked if, overall, they had felt that they were being
encouraged to stay at home as long as possible, and, if so, how they
felt about this. Most (n=32) said that they did feel encouraged to stay
at home, and comments suggested that they were generally happy
about this because it fitted with what they wanted or expected.
OK. Spoke to my friend and she had said she wanted to stay at home
as long as possible. That reassured me that it was OK to do that.
(PX07)
Fine, I’d wanted to be at home as long as possible all along, but I did
not want a home birth.
(X204)

The OPAL study
©NCCSDO 2007 126
Some also made a point of saying that they felt that they could have
gone into the unit if they had wanted to.
That was fine – I was given the choice all along but encouraged to stay
at home.
(PY01)
However the comments of 10 of these 32 women suggested that they
were unhappy about it overall and we will look at these in detail in a
later section.
Of the 12 women saying they did not feel they were being encouraged
to stay at home for as long as possible, four said it was because they
had been given a choice or been advised to stay at home until a
certain point when they would be coming in. Two said they were
happy about not being encouraged, one made no comment and only
one expressed unhappiness about not being encouraged to stay at
home, saying she wanted to stay at home longer. Four respondents
said they felt neither encouraged nor discouraged, all were happy
about this and said it was because they had been made to feel
welcome to attend if they wanted to and felt that they had been given
the choice.
Once the woman attended hospital
Nearly half (22) of the respondents had the experience of attending
the hospital in early labour and then being sent home again. As the
flow charts (Figures 3.2–3.5) show, some women had this experience
on multiple occasions. Half of these women (11/22) understood it was
appropriate to be sent home and four were happy to go home.
However, five women were disappointed to be sent home and a
further two were angry. These reactions will be discussed in more
detail below when we consider the factors associated with satisfaction.
Nine women stayed in hospital with labour not progressing. Two
women understood it was appropriate and one felt happy to be kept
in, however the rest felt a range of emotions - anger, unease,
disappointment, and frustration.
Overall, just under three–quarters of women (n=33) felt they went
into hospital at the right time – when they went and stayed in until the
baby was born – the remainder (13) of women felt they went to
hospital either too late or too early.
3.8.3 Satisfaction: statistical analyses
At the end of the interview women were asked ‘Overall, on a scale of
0–5, with 0 being very dissatisfied and 5 being very satisfied, how
satisfied were you with the telephone conversation[s] that you had?’
There were generally high levels of satisfaction, with over two-thirds
giving satisfaction scores of four or five. However, 28 per cent (n=13)
reported being less satisfied, scoring their experience as three or less
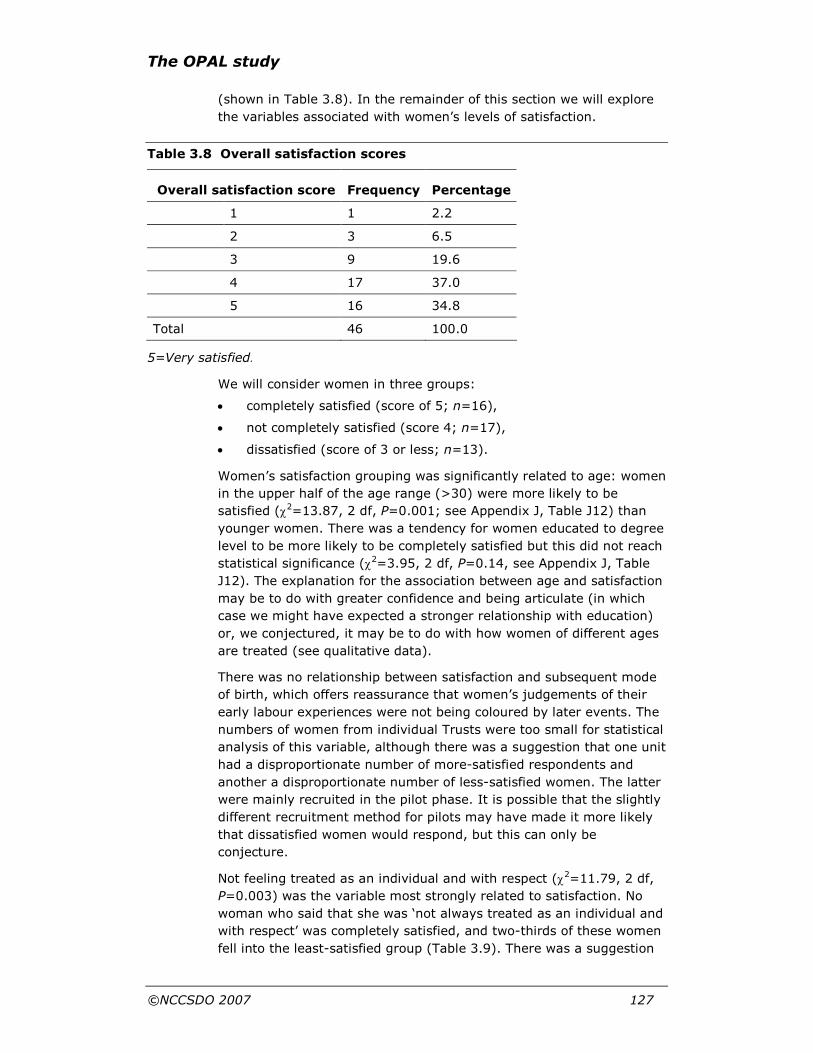
The OPAL study
©NCCSDO 2007 127
(shown in Table 3.8). In the remainder of this section we will explore
the variables associated with women’s levels of satisfaction.
Table 3.8 Overall satisfaction scores
Overall satisfaction score Frequency Percentage
1 1 2.2
2 3 6.5
3 9 19.6
4 17 37.0
5 16 34.8
Total 46 100.0
5=Very satisfied.
We will consider women in three groups:
• completely satisfied (score of 5; n=16),
• not completely satisfied (score 4; n=17),
• dissatisfied (score of 3 or less; n=13).
Women’s satisfaction grouping was significantly related to age: women
in the upper half of the age range (>30) were more likely to be
satisfied (χ2=13.87, 2 df, P=0.001; see Appendix J, Table J12) than
younger women. There was a tendency for women educated to degree
level to be more likely to be completely satisfied but this did not reach
statistical significance (χ2=3.95, 2 df, P=0.14, see Appendix J, Table
J12). The explanation for the association between age and satisfaction
may be to do with greater confidence and being articulate (in which
case we might have expected a stronger relationship with education)
or, we conjectured, it may be to do with how women of different ages
are treated (see qualitative data).
There was no relationship between satisfaction and subsequent mode
of birth, which offers reassurance that women’s judgements of their
early labour experiences were not being coloured by later events. The
numbers of women from individual Trusts were too small for statistical
analysis of this variable, although there was a suggestion that one unit
had a disproportionate number of more-satisfied respondents and
another a disproportionate number of less-satisfied women. The latter
were mainly recruited in the pilot phase. It is possible that the slightly
different recruitment method for pilots may have made it more likely
that dissatisfied women would respond, but this can only be
conjecture.
Not feeling treated as an individual and with respect (χ2=11.79, 2 df,
P=0.003) was the variable most strongly related to satisfaction. No
woman who said that she was ‘not always treated as an individual and
with respect’ was completely satisfied, and two-thirds of these women
fell into the least-satisfied group (Table 3.9). There was a suggestion

The OPAL study
©NCCSDO 2007 128
in the data that younger women were less likely to feel treated as an
individual and with respect.
Table 3.9 Satisfaction and being treated as an individual and with
respect
Satisfaction was related to the length of calls. Women who had no
calls that lasted more than 5 min were much more likely to be
dissatisfied (χ2=8.11, 2 df, P=0.02), as Table 3.10 shows.
Table 3.10 Satisfaction and length of calls
Any calls >5 min?
Completely satisfied
Not completely satisfied Dissatisfied Total
No 4 (23.5%) 4 (23.5%) 9 (52.9%)
17 100.0%)
Yes 12 (41.4%) 13 (44.8%) 4 (13.8%)
29 (100.0%)
Total 16 (34.8%) 17 (37.0%) 13 (28.3%) 46 (100.0%)
Women who perceived that the unit was busy when they phoned
appeared more likely to be dissatisfied, but this did not quite reach
statistical significance (χ2=5.02, 2 df, P=0.08).
Table 3.11 Satisfaction and number of phone calls
Number of calls
Completely satisfied
Not completely satisfied
Dissatisfied Total
1 4 5 2 11
2 7 8 4 19
3 5 2 4 11
4 0 2 1 3
5 0 0 2 2
Total 16 17 13 46
Although cell sizes are too small for statistical analysis, Table 3.11
suggests that women making more than three calls were least likely to
be completely satisfied. The same tendency is apparent if we consider
Completely satisfied
Not completely satisfied Dissatisfied Total
Not treated as an individual and with respect by all
0 (0.0%) 3 (33.3%) 6 (66.7%) 9 (100.0%)
Treated as an individual and with respect by all
16 (47.1%) 13 (38.2%) 5 (14.7%) 34 (100.0%)
Total 16 (37.2%) 16 (37.2%) 11 (25.6%) 43 (100.0%)

The OPAL study
©NCCSDO 2007 129
the mean number of calls made by women in each of the three
satisfaction groups (Table 3.12).
Table 3.12 Satisfaction and mean number of phone calls
Satisfaction
level…
Completely satisfied
Not completely satisfied Dissatisfied
Mean number of calls 2.06 2.19 2.77
Women who felt that they were being taken through a set list of
questions were no more likely to be dissatisfied.
Being sent home again after going to hospital was significantly related
to dissatisfaction (χ2=6.83, 2 df, P=0.03; see Appendix J, Table J13).
Women who were aware of the Pathway were no more satisfied than
those who were not (Table 3.13). However, other more specific
aspects of antenatal awareness and preparation did appear to relate to
satisfaction as shown in Table 3.13 and Figure 3.6. There is a notable
difference between the completely satisfied group and the rest
regarding the leaflet and discussion of the Pathway and an antenatal
expectation to stay at home in early labour. Note that there is little
difference between the groups who were ‘less than completely
satisfied’ and ‘dissatisfied’. This might indicate that antenatal
preparation is a prerequisite for complete satisfaction, but is not in
itself sufficient. We will return to the important topic of preparation in
a subsequent section.
Table 3.13 Preparation for the Pathway and satisfaction levels
Completely satisfied
Not completely satisfied Dissatisfied
All women
Aware of pathway 12 11 9 32/46
Had a leaflet 12 8 6 26/46
Discussed pathway with midwife
8 5 5 18/46
Discussed pathway at antenatal class
6 4 4 14/46
Not discussed at class
6 1 4 11/46
Did not attend antenatal class
4 10 5 19/46
Antenatal expectation to stay home in early labour
10 6 5 21/46
Total 16 17 13 46
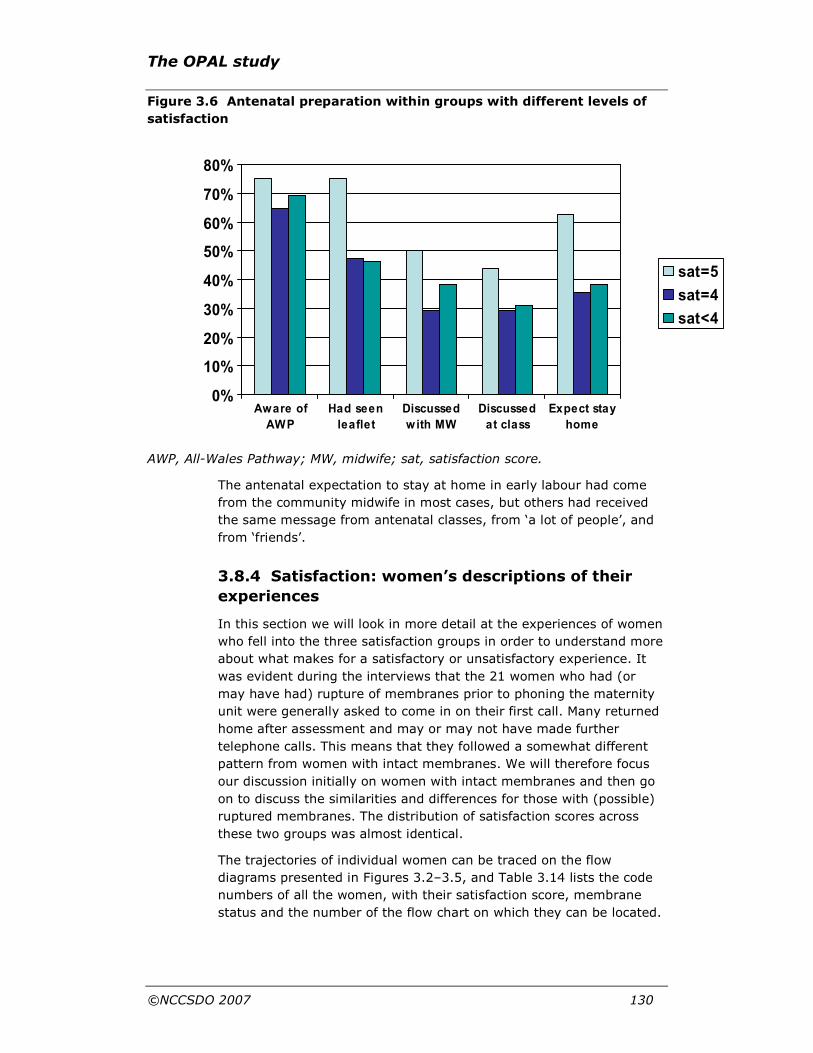
The OPAL study
©NCCSDO 2007 130
Figure 3.6 Antenatal preparation within groups with different levels of
satisfaction
AWP, All-Wales Pathway; MW, midwife; sat, satisfaction score.
The antenatal expectation to stay at home in early labour had come
from the community midwife in most cases, but others had received
the same message from antenatal classes, from ‘a lot of people’, and
from ‘friends’.
3.8.4 Satisfaction: women’s descriptions of their
experiences
In this section we will look in more detail at the experiences of women
who fell into the three satisfaction groups in order to understand more
about what makes for a satisfactory or unsatisfactory experience. It
was evident during the interviews that the 21 women who had (or
may have had) rupture of membranes prior to phoning the maternity
unit were generally asked to come in on their first call. Many returned
home after assessment and may or may not have made further
telephone calls. This means that they followed a somewhat different
pattern from women with intact membranes. We will therefore focus
our discussion initially on women with intact membranes and then go
on to discuss the similarities and differences for those with (possible)
ruptured membranes. The distribution of satisfaction scores across
these two groups was almost identical.
The trajectories of individual women can be traced on the flow
diagrams presented in Figures 3.2–3.5, and Table 3.14 lists the code
numbers of all the women, with their satisfaction score, membrane
status and the number of the flow chart on which they can be located.
0%
10%
20%
30%
40%
50%
60%
70%
80%
Aware of
AWP
Had seen
leaflet
Discussed
with MW
Discussed
at class
Expect stay
home
sat=5
sat=4
sat<4

The OPAL study
©NCCSDO 2007 131
Table 3.14 Details of individual women’s satisfaction scores, membrane
status and the flow-chart number on which she appears
Patient ID
Satisfaction score
Membranes ruptured at first call
Flow chart figure number
P06 5 No 3.3
PU09 5 Yes 3.3
PX07 4 Yes 3.4
PX08 5 Yes 3.2
PY01 5 Yes 3.3
PY02 3 Yes 3.3
PY03 3 No 3.5
PY04 3 No 3.2
PY05 1 Yes 3.3
U02 5 No 3.2
V01 4 No 3.2
W01 4 No 3.2
X01 2 Yes 3.5
X02 5 Yes 3.2
X03 4 Yes 3.3
X04 5 Yes 3.4
X201 4 No 3.2
X202 4 Yes 3.4
X204 5 No 3.5
X205 4 Yes 3.2
X209 5 No 3.2
X210 5 No 3.3
X211 3 No 3.2
Y01 4 No 3.2
Y03 4 Yes 3.2
Y12 3 No 3.2
Y14 4 No 3.3
Y15 5 No 3.2
Y17 3 Yes 3.3
Y18 3 No 3.3
Y19 4 Yes 3.3
Y20 4 No 3.2
Y201 4 No 3.3
Y203 4 No 3.2

The OPAL study
©NCCSDO 2007 132
Patient ID
Satisfaction score
Membranes ruptured at first call
Flow chart figure number
Y204 4 Yes 3.3
Y205 5 Yes 3.3
Y206 3 Yes 3.3
Z01 2 No 3.2
Z02 5 No 3.2
Z03 4 No 3.2
Z04 4 Yes 3.3
Z09 5 Yes 3.3
Z10 3 No 3.5
Z16 2 No 3.2
Z201 5 Yes 3.2
Z202 5 No 3.3
We will first present the experiences of women who were completely
satisfied (score of 5), then the experiences of women who were not
completely satisfied (score of 4) and finally the experiences of women
who were dissatisfied (score of 3 or less).
Women who were completely satisfied
Women with intact membranes (n=8)
In response to their first call, this group of women were typically
asked to phone back when labour advanced if their membranes were
intact, usually defined clearly; for example, ‘when contractions are five
minutes apart and lasting for one minute’, or at a set time, ‘in two
hours’, or ‘when you can’t cope with the pain’. Women welcomed such
exact instructions:
I was given clear instructions, not 'well it might be better', which was
what I needed…. I waited till the contractions were doing what the
midwife said then phoned, they said come in…. I took the advice they
gave and waited for it to happen…I knew it would be OK to go in.
(Z02)
They said I could stay at home but advised me that I was going to have
to come in within a couple of hours – they’d be expecting me.
(U02)
This also demonstrates the trend in these calls of an implication that
the woman would be expected to come in soon, once she had reached
the criteria for phoning back, or she could make her way in when
ready or had the choice to come in but opted to stay at home a bit
longer.
There were no comments indicating that the woman felt unwelcome,
that she was not asked to come in when she wanted to go in or that

The OPAL study
©NCCSDO 2007 133
she felt that she was being put off going into hospital. Furthermore, in
this group of women there were no comments indicating a negative
experience on the phone.
There were a number of positive comments offered, demonstrating the
women’s appreciation of the midwife’s reassurance, confidence,
information, friendliness and encouragement:
Very calm and helpful and friendly - wasn’t made to feel ‘oh, it’s
another one’.
(Z02)
She put my mind at rest, said it was all normal…. Said I was welcome
to come in.
(Y15)
I was particularly impressed, I was struck when I had the contraction
on the phone, you're on the phone and you feel the need to almost talk
but the midwife was very much saying 'Look, you don't need to talk, I
won't put the phone down, just get through it and then start talking
again' and she was talking to me, I thought she was really good.
(X209)
Two of the eight women with intact membranes were sent home but
were both aware of this possibility before going in for a check.
Although one woman asked to come back in (rather than being invited
to) on her subsequent phone call, she had been given an indication
that she would be expected back soon:
The midwife at the hospital said I’d probably be back before midnight.
(X204) Women with ruptured membranes (n=8)
Of the satisfied women with ruptured membranes, five were asked to
come in on their first call. The time at which they should attend was
not given as immediate or soon: in 3 h; within 24 h if nothing
happened; make your way in when ready. Two were asked to phone
back when labour advanced, and both were subsequently asked to
come in on their second call. One contacted her community midwife,
who went to visit after a second call. There were three examples of
women choosing to stay at home longer after being invited to attend.
As with the women with intact membranes, there were no comments
suggesting a negative experience on the phone and no evidence
indicating that the woman felt unwelcome; was not asked to come in
when she wanted to go in; or was put off going into hospital. One
respondent volunteered:
I didn't feel I was being forced to [stay at home] I felt the ball was in my
court, I didn't feel 'you’re not allowed in yet, you're not ready', they
were so lovely… ‘cos I was so relaxed they took it from me what I
wanted to do.
(X04)

The OPAL study
©NCCSDO 2007 134
In two cases (X02, X04), the woman had been telephoned by
midwives at the hospital to see how things were progressing at home.
Again, there were a number of positive comments from the majority
(n=6) of respondents referring to the midwife’s reassurance,
confidence-giving and encouragement, welcoming, information, being
given a choice and feeling confident in the midwife’s ability:
Given choice all along but encouraged to be at home…gave me
confidence.
(PY01)
Felt I was in good hands…treated as an individual…your wishes were
taken into consideration…calls were really reassuring.
(Z201)
Five of the eight women with ruptured membranes were sent home
after attending the hospital, some were given the choice to go or had
arrangements made for when they would return. One (PX08) was
disappointed to go home, she was aware of a policy that women are
invited to attend on their second call and expressed some element of
regret at having phoned too soon. However, she had been given
reassurance that it was OK to phone once she had gone home.
Women who were not completely satisfied
Women with intact membranes (n=9)
Seven of the nine women with intact membranes were asked to phone
back once labour advanced, the criteria being: contractions 5 min
apart and lasting 1 min; pains worse or not being able to cope with
the pain; or at a set time. One woman was given a choice about
whether to come in or not, another was asked to come in but she
stayed at home to have a bath before going in.
There were two examples of women being told that they were
welcome to come in but opting to stay at home.
I felt confident that they were saying you can come in when you want
to. They didn't stop me coming in, I had the option.
(V01)
Three of the nine respondents indicated that at some point they
themselves asked to come in, rather than being invited. One of these
indicated being made to feel less welcome:
…they said if you’ve got to come in, come in.
(Y01)
Six respondents had some negative comments about the advice they
were given during the phone calls. In two cases (W01, Y203) this was
because they were told that the unit was full. One woman felt she was
having to repeat information on different calls; and also wanted to be
induced on her due date but wasn’t (X201). Z03 had also wanted calls

The OPAL study
©NCCSDO 2007 135
to be in Welsh. The other three all felt that they had failed to obtain
helpful advice:
…think I was expecting more, was expecting how to be advised to look
after myself.... I wasn't given any advice about how to control the pain.
I came off the phone and was like 'oh, that's all it was'. No advice on
what to do.
(Z03)
One woman, who had previously opted to stay at home longer,
wanted to stay in hospital after attending but was told she would have
to have pain relief in order to stay. This created a dilemma for the
woman as she had wanted to avoid taking drugs where possible.
After I was examined I was only 1 cm dilated and the midwife said I
would have to go home or have – the only way to stay in hospital would
have been to have some drugs. I was against having any but didn't
want to go home. It was a half-hour journey on country lanes with
contractions every 3 min. I was offered pethidine and after much
deliberating I decided I would do that as I didn't really want to go
home.
(Y14) Women with ruptured membranes (n=8)
Five of the eight women in this group were asked to come in on their
first call: now; in 2 h; within 24 h if nothing happened. Three were
asked to phone back when labour advanced, and all were
subsequently asked to come in on their second call. There were two
examples of women choosing to stay at home longer after being
invited to attend.
One respondent commented on the advice to phone back in 24 h as
‘weird advice’, which suggests the rationale for being encouraged to
stay at home for this period had not been fully explained during the
phone call. She acknowledged that her mother had encouraged her to
go in sooner as she had had quick labours and warned her to be
watchful. This possibility had, apparently, also not been addressed
during the phone call as the woman was anxious about the midwives:
…they never seemed to think it could happen sooner…. I was assured
it wouldn't happen until next day. It would have been reassuring to
hear that I may need to go in earlier.
(PX07)
One respondent expressed relief at being asked to come in on the first
call and then being allowed to stay in:
I know they say stay at home, but to be honest with you I think I was
probably one of those people that would have benefited from going in
because I'm not very good in those [scary] situations anyway and I
have quite a low pain threshold, so I probably would have headed in
anyway. Extremely glad they told me to come in…. I think I would have
been really upset if they had said go home.
(Y19)

The OPAL study
©NCCSDO 2007 136
Negative comments about the phone calls were made by two
respondents: PX07 – quoted above – and Y204, who was asked to
come in but didn’t expect this or want to go in. Furthermore, she was
angry and annoyed at then being sent home.
Three out of eight women in this group went home after going in to
hospital. One had an arrangement to phone back at a certain time to
check if there was space for her to be admitted for induction of labour.
She went home but felt ‘a bit gutted that they were not going to just
get on with the induction’ (X202). When she phoned as planned she
went in and stayed in. Another woman (Y204) went home with a
planned return for an induction but was angry and annoyed at having
to go home, as described above. The third woman went home twice,
the second time after being told ‘women are not usually kept in until
4 cm dilated, and no pain relief is offered until 4 cm’. She was given a
choice whether or not to go home and went with a planned time to
return. Regarding going home, she admitted to feeling:
…disappointed and a bit scared, in pain, told it would get worse – the
midwife was a bit ‘off’.
(Y03)
She also commented that she felt treated with respect by ‘most’ rather
than all staff.
Women who were dissatisfied
Women with intact membranes (n=8)
Five of the eight women in this group had been advised to phone back
when labour progressed but a number had unresolved anxieties after
this first call. One woman was having pains 2 weeks prior to her due
date:
I think I expected them to ask me to go in, but they didn't. [Q: how did
you feel about that?] Erm, I think I was a bit scared ‘cos it was my first
baby as well, I didn't know what to expect…. I would have preferred to
go to hospital though. My partner felt the same. They said if I felt any
worse I could go in.
(Y12)
A second woman phoned when she was 3 days past her due date:
Short call – not enough time, I didn't feel I could say 'I want to listen to
the heartbeat' , they were not very supportive – when I called the first
time I just wanted reassurance – partner was anxious. He had had a
panic attack. Contractions were getting quicker than 15 minutes, then
10 minutes, then stopping, then 3 minutes. I felt upset after the first call
– scared and hormones, but after half-an-hour I felt better…. It would
have been reassuring to be able to hear the heartbeat. I was concerned
about losing the baby - convinced that the baby had died, especially
when it was not moving, it’s good being able to listen to the heartbeat.
(PY04)
Two others were given criteria for when to phone back that they found
imprecise. One was told:

The OPAL study
©NCCSDO 2007 137
…if you feel you can hang on a bit longer and see how you go and
update us.
(Z16)
This less-than specific criterion was, not surprisingly, confusing:
But then it was ‘well how long do you hang on a bit longer for?’ That’s
what confused me, and I was in a bit of pain and I didn’t think to say
‘well how long is a bit longer’. But she just said ‘see how long you can
hang on for’. And I thought ‘well what if I get to 1 minute apart and I’m
stuck with a 5 minute journey?’ and, I don’t know.... It [phoning back]
wasn’t so much at an agreed time; it was sort of to say how I was
getting on. So I was thinking ‘well what do I do, do I phone back in an
hour? Do I phone back when I get to so far apart?’…It would probably
have been better for one of the women [midwives] to say ‘well if they
are coming every 5 minutes now wait until they are coming every 3
minutes, or wait till you get to 2 minutes, it’s not going to happen
straight away’, but it was nothing, it was just ‘phone back if they get
closer’, that was it.
(Z16)
In both these cases the advice led on to a less-than satisfactory series
of events: the first woman (Z01) phoned back and admitted to having
‘lied about contractions, said they were stronger’ in order to be eligible
to attend; respondent Z16 complied with instructions and phoned
back:
I phoned to say they were wearing off so you probably won’t expect me
up. When I said ‘my name is [name] I’m phoning just to let you know
that my contractions are wearing off and they are 8 minutes apart’.
‘And what are you phoning for?’ was the reply and I just sort of said
‘Oh, well I was told to give you an update’, they said ‘that’s fine, OK’
and that was it. It was that short and sweet and I was left
dumbfounded really.
(Z16)
The impact of this left the woman feeling very ‘angry’ and unsure
about phoning again because of how she imagined the staff reacting:
…when I made the third one [call] I thought, all I could think of was
them thinking ‘Oh god, it’s this girl on the phone again’.
(Z16)
In view of our earlier observations on the relationship between age
and satisfaction, it is interesting that this dissatisfied woman, aged 26,
imagines that the staff saw her as a ‘girl’.
Although we asked an overall level of satisfaction with the phone calls,
some respondents, including this one, distinguished their satisfaction
with different calls:
I’d probably say 2, but that’s with the first and last not being as bad as
the second. [Q: So if you were to rate each call?] Number one I’d
probably give a 3, number 2 a 0, and number 3 a 2 or 3.
(Z16)

The OPAL study
©NCCSDO 2007 138
Two of the eight dissatisfied women offered positive comments about
the phone calls, while seven made at least one negative comment
(some three or more). These related to unmet needs: for information
or advice; for support; for having fears or anxieties allayed; and to
unmet expectations. The issues were generally the same as have
already been described. Y12 had expected to be asked to come in, she
was scared and not happy being encouraged to stay at home, feeling
she could only go in ‘if I felt worse’. Y18 felt that she was given no
advice from the maternity unit, only from her sister-in-law. PY03 was
‘shocked’ to be told that she was not in labour when contractions were
5 min apart and confused about when it would be OK to go in. She felt
that midwives were generally not supportive on the phone and
specifically mentioned that they did not offer any advice on eating
until she asked. When subsequently asked what she wished she had
been told on the phone, she replied:
What they class as being in labour – but not when actually in labour –
better to be told in antenatal class.
(PY03)
This draws attention to the importance of antenatal preparation and a
match between expectations and experiences.
PY04 complained at the briefness of the call and said that she was
‘made to feel as if I’d woken them up’. She felt upset and scared after
the first call; felt that the advice she was given was not helpful; she
was not given the name of the midwife on the phone and on the last
occasion of phoning found the line engaged for 30 min.
The last woman in this group (X211) had only one negative comment
about the phone calls; that she was ‘not made to feel welcome’. That
this was her only negative comment highlights the impact of this
dimension. She was explicit that this was what reduced her
satisfaction score to 3:
She was saying…we don't want to keep you unnecessarily and we
don't want you to be frustrated…that made me think that 'I'd better
stay at home because they may not be very patient with me,' that was
my kind of impression. So I thought I'd just carry on by myself because
I was feeling alright and I was able to manage things and I didn't feel
that there was anything wrong I just thought I'd keep on going, and
that's what I did basically…. I didn't feel that welcome anyway; it felt
like they wanted me to be really ready to give birth when I got there.
(X211)
She went on to say:
If I had felt more welcome, if they had said 'oh yes come in, even if it
takes another 12 hours, you'll be alright here' that would have been
very different, I would have been happy to go in then, it would have
been great to have had the support of another woman there, for
example, in an ideal world I would have loved that, but you know I just
know things aren't like that normally.
(X211)

The OPAL study
©NCCSDO 2007 139
Her experience was worsened after she eventually went to hospital
when she was left alone, unexamined, in a meeting room for 40 min.
She was then found to be 8.5 cm dilated.
Two women in this group reported that they asked to come in, rather
than being asked by midwife to come in. There was no evidence of
feeling welcome to attend; in one instance it was as if to pacify:
They said to come up then if I was so worried and upset, they didn’t
say to me ‘we want you to come up’ it was just – ‘if it’s concerning you
then come up’. …it was ‘if I wanted to come up, to reassure me’… she
just said ‘well if you are that teary then come up to be monitored but
there’s nothing to worry about’.
(Z16)
This respondent also described several aspects of the phone calls that
were negative. In particular was the unmet expectation of being asked
to attend once contractions were 5 min apart:
It wasn’t a very nice call really, because, when you are told by your
[community] midwife as well, ‘when you get to 5 minutes give them a
call and they’ll probably tell you to come up’, I was told to hang on and
see how long I could go. And I thought ‘yes, OK, I’m only 5 minutes
down the road but I’m a first-time mum and I didn’t have a clue what to
expect. So I wasn’t too impressed. A bit worried to say the least. I had
all my bags packed and I thought ‘is this it now?’…when I got to 5
minutes apart I was expecting to go in, so to be told to wait a bit longer,
to hang fire, a bit daunting really.
(Z16)
She went on to say:
It’s everywhere though, all the books you read, the magazines,
everything, all the information I was given about going to hospital and
what to expect, it’s all about this ‘when you get to 5 minutes apart’,
and I just think ‘either don’t print that or the hospital takes note of it’.
(Z16)
This woman also made reference to the fact that the particular call she
was concerned about was very short in length, which was also
apparent in other less satisfied respondents ‘It was about 2 minutes if
that’. The significance of shorter calls on satisfaction has already been
demonstrated. Shorter calls would seem to indicate less time available
for the more supportive aspects of the call, for example picking up on
anxieties and need for reassurance, which in a number of less satisfied
respondents was apparent:
…‘cos you read so much, with my contractions wearing off, I panicked
that not that there was something wrong but I thought, ‘well I’m going
the opposite way now’ again worrying that the baby was in distress. I
would have rather have been reassured…. I mean even if she had said
‘well it’s normal for them to branch [meaning to get less] off, get further
apart, or it’s just practice ones or if you find they are coming regular
again give us a ring back’ but that wasn’t even said.
(Z16)

The OPAL study
©NCCSDO 2007 140
Indeed, if anxieties remain unaddressed after the call then they can
feed into greater upset, fears, anxiety and misconceptions:
My stomach had gone quite hard, again, I panicked ‘was the baby
getting in distress? Was that why my contractions were getting further
apart?’ I then panicked because I couldn’t feel her moving, but that
could have been me just feeling so tense because of what was going on.
I got quite upset on the phone…. Upset to say the least, because you
think: your baby. OK, they would have said if contractions going the
wrong way and baby could be in distress, they probably would have
said, but it’s still in your mind. So I’d come off the phone upset and
phoned my Mum. To which she said ‘well, you phone back and say
that you are not happy with the way she was with you’. And I said to
her ‘I’ll hang fire for a bit’ but when I started not being able to feel the
baby moving as much, that’s when the third phone call came.
(Z16)
This case also demonstrates the likelihood of the woman feeling the
need to phone the hospital more if fears remain unaddressed. This is
consistent with the impression given by the quantitative data.
Whether or not the women’s fears were allayed is not only about
absence of any attempts to reassure but also, when attempted, the
manner in which this is made as illustrated previously.
…first-time mum you expect a bit of support really on the phone which I
don’t feel I had really.
(Z16)
A further concern expressed by this respondent and a minority of
others was about the nature of having the conversation on the phone
rather than face to face, leading to less confidence with the advice
being given or assessment being made:
I mean, even if I had gone up there and they’d have said ‘well nothing
is sort of happening so go back home and see how you get on’. At least
then I’d have seen someone face to face, they’d had a prod round and
what not, but they didn’t know what situation I was in over the phone,
so that’s what worried me a bit. …A bit worrying really, ‘cos you try
and express how much pain you are in and they obviously they can’t
see you and I know everybody is different so, you can’t really judge
one woman on what your previous woman was like, with her
contractions, erm, so a bit disappointed really that I couldn’t go in to
speak to someone or even to have someone come round to reassure me.
(Z16)
Two respondents indicated dissatisfaction with not being told the name
of the midwife they were speaking to on the phone.
The majority (six out of eight) of women in this group were sent
home, one more than once. One chose to go home; two were to
return when labour progressed (unspecified time) and one the next
morning; one was to return for induction of labour (already booked)
and the fifth went home with the expectation that she would be back
soon. PY03 was sent home more than once: she had attended without
phoning first; having been booked for an induction she went in as

The OPAL study
©NCCSDO 2007 141
planned. Her contractions were 5 min apart when she first attended
and she described her ‘shock’ at being told she was not in labour and
should go home, to return when contractions were stronger.
Her second visit was also without the preamble of a phone call, and
being sent home was not what she wanted: ‘I didn’t want to get in the
car again’. She first phoned the hospital an hour after returning home
a second time, but was left confused:
They said I could go in to be examined but suggested the best place for
me was at home. I was confused, I had no way of knowing how far
dilated I was until I was examined, but I didn't want to go in for an
exam and be sent home again…they said I needed to be at least 5 cm
dilated to be kept in. I was afraid to go in again – I didn't want to be
sent home again. It was more sort of 'pull yourself together', it didn't
feel great. I didn't feel confident to be at home – I didn't feel in danger,
but anxious as I didn't know how to find out if dilation had progressed.
(PY03)
This demonstrates that giving women a goal (5 cm dilatation) which
they cannot know they have reached is unhelpful.
She made four further phone calls to the unit before going in for the
last time. She offered additional comments about the phone calls in
early labour which underlined how she felt that they had failed to
support her at home, leading to dissatisfaction:
Questions on the phone should be longer, talk through things more. I
felt like it was just an exchange of information, efficient but not
necessarily comforting or considered. It could have been more
supportive.
(PY03)
Z16 went home after attending, was told to come back the next
morning, and admitted to feeling ‘alright’ about being sent home. She
considered the reassuring nature of the midwife, together with the
reassurance of being on the monitor had made the difference:
After being on the monitor it reassured me and the girl was lovely, and
she just explained that your contractions can wear off, didn’t actually
say why, I still don’t know to this day why, but yes, if I was able to get
home and I felt comfortable then it was probably the best place. …
Wasn’t too bad after I had spoken to someone, I’ll hold my hand up,
being reassured had made it a bit better.
(Z16)
Z16 would appear to be an example of someone who needed the
reassurance of monitoring and face-to-face contact. Women with ruptured membranes (n=5)
Three of the five women in this group were asked to come in straight
away. There was evidence of this advice being a shock; unexpected
and unwanted:
I was quite shocked at the brevity of the call, because the community
midwife was of the opinion you shouldn't go down until the last minute

The OPAL study
©NCCSDO 2007 142
so I was quite shocked when they said come straight down…a bit
shocked and panicked having to come in straight away.
(Y206)
Worst call was the first – asking me to go in to check my waters were
really broken – they didn't believe me, I was indignant. A bit panicked
too…not too happy about it, I knew my waters had gone – it was as if
they didn't believe me. I didn't see the point of going in, I knew I'd be
sent home after.
(Y17)
Another woman in this group (X01) had a series of unsatisfactory
experiences which started prior to going into labour including lack of
antenatal classes, being unsure where to phone and advice about her
clinical condition that she was not happy with. She was surprised by
the response to her first call:
I expected them to say come in. My sister-in-law said that they used to
say if your pad is wet to come in but they didn't say to come in.
(X01)
This call prior to attendance was also unsatisfactory in the way in
which questions were asked and the experience of not feeling treated
as an individual:
They said how often are the contractions? How intense are they? But I
had nothing to compare it to. They were asking me questions which I
didn’t have anything to compare it to.... No, they didn’t treat me as an
individual, did they, because they said just a general, because they
said ‘can you still talk?’ and things like that, it was just a general
outline…. I just wanted them to say like ‘come on in then’ and not
asking you millions of questions when you’re in pain.
(X01)
Her husband then made a phone call to the hospital prior to attending
which did not go well:
…phoned up and they weren’t that good. They said ‘you can’t be in
that much pain ‘cause you’re able to talk’. And my husband got quite
angry with that and said ‘what do they want you to do, to be dying?’
(X01)
Women reported that ‘the midwife was treating me as if I didn't know
what I was on about’ (PY05). ‘They do kind of make you feel a bit silly
phoning’ (Y17) and an unmet desire to be told ‘that I was not being
daft’ (PY02). There was also evidence of lack of explanation.
I don’t think a lot was explained…they didn't tell me why they wanted
me to go down, but it was really busy…. I was not told of the possibility
of being sent home, I thought that as my waters had broken I'd be kept
in…
(Y206)
As was the case for dissatisfied women with intact membranes,
women were more likely to say that they had not felt welcomed to
come in.
The OPAL study
©NCCSDO 2007 143
[Satisfaction score?] Probably about 2 really because they didn’t
encourage me to – probably because they were so busy – they didn’t
encourage me to go in at all, and if anything they were trying to put me
off which they were, more than likely, because they were so busy.
(X01)
This woman was another of the minority who expressed doubts about
the assessments being on the phone rather than being examined.
All five women in this group were sent home: two more than once.
PY02 felt:
Disappointed and angry. I felt dismissed – I was 3 cm dilated, waters
had broken in the day, I thought I may need to be induced, but then
when we got there, I was sent home.
(PY02)
There was no evidence of an arranged time for women to return, and
in three of the five cases respondents indicated a feeling of being
unwelcome to come back in: having to ask to go in or just going in
without phoning. For PY05, there was no evidence of not being
welcome to attend; the problem was rather not being able to stay.
After the first attendance she was advised to go home and take her
temperature, and if it rose or contractions got to every 3 min then she
should go straight back in, otherwise to come in at 3 pm for another
check. These instructions do not appear to have been relayed to other
staff:
I went in at 3 pm; my contractions were 5–8 mins. Midwife [second one]
was very dismissive and seemed baffled why I was in, I was told to go
home…. I was surprised that they were surprised I went in after being
told to go in.
(PY05)
She was sent home four times in total, leading to dissatisfaction and
distress:
OK about the first two times I had to go home but very unhappy at
being sent home at 11.30 pm – it was snowy and icy – that was
unacceptable and wrong. I feel I should have been kept in at 8.30 pm.
If I had been able to stay in at 11.30 pm and not sent home, baby
wouldn't have been in distress…. It was the repeated sending home
that I was not happy about…. No benefit to be sent back and forth.
(PY05)
The way that the remaining woman in this group felt treated when she
went in and was then sent home had a negative impact on her
willingness to return. Indeed, her experience meant she wanted to
delay returning so there would be different staff on duty:
…and then they sent me home in the night as well, I was in the bath
every half hour in the house and I was having contractions continually,
and I didn’t want to go back because of the way they were, they
thought I was wasting their time…. Well I was just waiting as long as I
could, until the morning staff so that the night staff would be off shift,
basically.

The OPAL study
©NCCSDO 2007 144
(X01)
She did not feel it was right to be sent home for a number of reasons:
But when they put me on the monitor, my contractions weren’t that
strong, but because I didn’t know how to breathe through them I was
hyperventilating, and the baby’s heart rate went up to 200, so they
shouldn’t have sent me home really…. I would have preferred to have
stayed in, it was horrible travelling…. Well I was frightened because
everything I’d read said you should stay in once your waters have
broken because of infection, but they sent me home…it wasn’t a
problem going in, it was going home again that was the problem.
Because I didn’t mind, once you’re in hospital you feel safe don’t you? I
was disappointed and angry…because they send you home and they
don’t know how quickly you’ll progress at home and they know you are
in labour, I mean I could have been nearly having my baby.
(X01)
This woman perceived that the unit was busy and that this had
influenced her being sent home.
3.8.5 Satisfaction summary
In summary, satisfaction was associated with:
• clear instructions about when to phone back, or return to the unit,
• choices about coming in/staying home or staying in/going home,
• not being made to feel unwelcome,
• receiving assurance, information, friendliness and
encouragement,
•••• advice given in a confident manner.
Factors contributing to dissatisfaction were:
• instructions which were less clear,
• not obviously being made to feel welcome to come in or being
invited to come in when the woman wanted to,
• being sent home when the woman did not want to go home,
• unmet expectations, particularly about timing of going to hospital,
• fear and anxieties that were not resolved by the phone calls,
• an absence of support and reassurance,
• shorter calls,
• more calls,
• midwives not understanding why a woman had phoned/attended
(according to instructions from another colleague); that is, a lack
of continuity of care.
An additional source of dissatisfaction for women with ruptured
membranes was being told to come in immediately on the first call,
leading to shock and panic. Apart from this, the factors contributing to
satisfaction or dissatisfaction for women with and without ruptured
membranes were very similar.

The OPAL study
©NCCSDO 2007 145
3.8.6 Antenatal preparation and expectations
Analysis of interviews in terms of satisfaction made it clear that
women’s expectations of early labour care were important and that
these were likely to relate to the antenatal preparation that they
received. Accordingly, we returned to the data to focus on these
aspects.
Pre-labour expectations of when to go to hospital
It is interesting to note that, in answer to this question, many women
answered in terms of their expectations of when it was appropriate to
phone the hospital. This was more noticeable in the women who were
less satisfied. Clearly this also relates to the expectation of staying at
home in early labour, which, as we have seen, was related to
satisfaction.
A small number of women had clear expectations and this had
generally come from multiple sources:
When I was not coping with pain, the piece of paper said contractions
were 4–5 mins apart, 60–90 seconds long, also [Q: Where did you get
that information?] from the Internet, magazines and the community
midwife.
(X204)
I had been given an indication from the antenatal classes that they
would assess the signs of labour and know when to tell me to come in
based on what I had told them and what advice they gave me, it would
dictate when it was appropriate for me to go into the hospital. And
perhaps that I may have to go home again…. [Q: Was there discussion
of when to phone?] At antenatal classes and my community midwife
but in more detail at the antenatal classes – they explained what would
happen where you would have to go and so on.
(X205)
The influence of such classes was missed by one respondent (PX07),
for whom the classes had been cancelled, and she was unsure of when
it was appropriate to phone the hospital. Another woman who had not
been to antenatal classes had discussed some aspects of what to
expect with the community midwife, but was not apparently aware of
the whole picture:
I was told that it was OK to phone at any time. Yes – if losing blood or
waters broken. Nothing was mentioned about contractions.
(Y204)
One of the notable sources of dissatisfaction was a mismatch between
expectations and events. Four of the dissatisfied women said that they
expected to be going into hospital by the time their contractions were
5 min apart. Although that expectation was, as we have seen,
common in other groups, within this group there was a suggestion
that women had found this misleading.

The OPAL study
©NCCSDO 2007 146
I was a bit surprised that she encouraged me to stay [at home] because
I thought that when the contractions were 5 mins apart I would be
encouraged to go in. I thought it would be time to go in. I was trying to
be brave, not too scared, I knew what I had to do, be positive.
(Y14)
Conversely one woman was asked to come in when this was what she
neither wanted nor expected.
I was not too happy about it, I knew my waters had gone – it was as if
they didn't believe me. I didn't see the point of going in, I knew I'd be
sent home after. The midwife didn't warn me that they would do a
sweep.
(Y17)
One woman highlighted the fact that this expectation is generated not
only by discussions with midwives but in written material too
(including the Pathway leaflet):
Wish I had been told to wait until every 3 mins – I expected that when
they were 5 mins I would be asked to attend – all the books, leaflets
say to call at 5 mins. It needs to be clearer that it’s not necessarily the
case that you go in at 5 mins apart.
(Z16)
Overall the aspects of antenatal preparation which appeared to relate
to satisfaction were:
• receipt of the Pathway leaflet and discussion with the community
midwife;
• specific antenatal encouragement to stay at home as long as
possible in early labour (either by community midwife, antenatal
classes or friends/relations) – almost two–thirds (10/16, 63 per
cent) of completely satisfied women had been encouraged in this
way;
• clearer expectations of when they might be admitted to hospital.
Conversely, women who were less than completely satisfied or
dissatisfied:
• were less likely to have received the Pathway leaflet or discussed
the Pathway;
• showed less evidence of specific antenatal encouragement to stay
at home for as long as possible in early labour (just over one-third
– 6/17 and 5/13 – in less-satisfied groups);
• had less obvious expectations of when they would be likely to
attend hospital;
• were more likely to comment on lack of antenatal preparation.
The role of the community midwife in preparing women was clearly
evident and very much valued where it occurred. Their influence on
expectations and knowledge about when it was appropriate to phone
and attend hospital was very strong, and notably absent in cases

The OPAL study
©NCCSDO 2007 147
where women felt they had no community support, particularly when
antenatal classes were not available. The importance of classes was
also evident in preparing women for what to expect, and in some
cases the classes appeared more influential than the individual
discussions with community midwives. It is noteworthy that so few
women reported discussing the Pathway and the leaflet in antenatal
classes.
The Pathway leaflet
The Pathway Leaflet is an important component of the Pathway, but
only 26/46 women had apparently received it. Many of those who had
were positive about it, saying that it gave them some element of
control by providing them with:
• appropriate terminology,
• a likely plan of events,
• a guide to when it was appropriate to contact the hospital.
As we have already seen, women with the maximum satisfaction score
were more likely to have had a copy of the Pathway leaflet than
others. Comments on the leaflet were offered by 5/16 of these
women, 3/17 of those who were not completely satisfied and 3/13
who were dissatisfied. The satisfied women were positive:
I kept on reading it in labour to work out where I was – to be honest my
husband was reading it more than me. I thought it was very very
useful.
(Z02)
It helps – it puts you more in control, I knew what to look for, I had
information. I was informed every step of the way – what to expect.
Good to have it in one leaflet.
(PY01)
Women who were not completely satisfied or dissatisfied were more
likely to find some shortcoming:
I had the leaflet but I was not really sure when to phone – I was
unprepared as there were no classes – they’d been cancelled. I didn't
really understand the leaflet much, I just glanced at it – I was going to
discuss it. It gave me information about the different stages, reassured
me a bit.
(PX07)
I got given that sheet.... Maybe it’s because of my profession [teacher] I
like to have things to read. If it was a normal delivery it would have
been great, because that [sheet] is what we kept consulting before we
made the decision to go down and things.
(Y206)
‘If it was a normal delivery’ is a telling phrase in that the ‘abnormality’
in Y206’s case was being asked to attend the unit to check (as she
saw it) that her membranes really had ruptured. This was clearly an
event that she saw as being treated as a divergence from the

The OPAL study
©NCCSDO 2007 148
Pathway, even though membranes rupturing is part of normal labour.
The leaflet is perhaps less clear than it might be about what women
with ruptured membranes in early labour can expect.
Y17 also highlighted another possible omission:
The Pathway leaflet didn't say that you could be in a lot of pain and
still not be in established labour.
(Y17)
Overall, few women in any of the satisfaction groups mentioned any
discussion of the Pathway. There was a tendency to equate ‘the
Pathway’ with ‘the leaflet’:
The community midwife brought it [leaflet] here when we went though
the birth plan…. My community midwife was very good, she said for
me to take paracetamol in the house, try breathing and taking my mind
off it. She said try and leave it as late as possible to go down [to the
hospital]…because the community midwife was of the opinion you
shouldn't go down until the last minute.
(Y206)
This last comment suggests that Y206 was interpreting this advice as
one midwife’s personal preference rather than a matter of evidence-
based policy.
Overall, women’s accounts of their experiences suggest there were
some elements missing from the leaflet that could have prepared
women better and possibly reduced uncertainty and dissatisfaction,
specifically:
• when you will be likely to be asked to attend the hospital;
• contractions being 5 min apart do not necessarily mean that you
will be asked to attend;
• if membranes rupture spontaneously you will be asked to attend
either immediately or within 24 h if contractions do not start, due
to risk of infection;
• in your best interests, you will be encouraged to stay at home for
as long as possible in order to reduce the likelihood of
unnecessary intervention;
• support to remain at home will be available on the phone from the
hospital and clear instructions about when to phone again will be
given;
• you may be encouraged to go home again after attending if
labour is not established but with clear instructions about when to
return;
• clearer information about likely levels of discomfort and pain
during latent or early labour.
The leaflet itself could be more specific about encouraging women to
stay at home as long as possible: currently this is not included.
Indeed, the philosophy behind the Pathway, of promoting normality of
labour, is not apparent on the leaflet. If the practical manifestation of

The OPAL study
©NCCSDO 2007 149
the philosophy of supporting normality throughout labour is to stay at
home longer in order to reduce unnecessary intervention, and it is in
the woman's best interests to do so, then this should be made more
specific in the literature and in discussions with women. In this way,
women will be made aware of the likelihood of being encouraged to
remain at home as long as possible, together with the rationale for
this. This may affect women’s experiences of labour and influence
women’s attitudes regarding staying at home for as long as possible.
3.9 Women: discussion
3.9.1 Methodological issues
The number of interviews conducted was fewer than originally planned
and we were particularly conscious of the need to avoid over-
interpretation of data from a sample of this size. We therefore
confined presentation of quantitative data to reports of frequencies in
the main and tests of significance where cell sizes warranted this. The
qualitative analysis of women’s experiences has, we feel, provided
important information on women’s experiences of the Pathway, in line
with the research objectives. We must also acknowledge the potential
for selection bias as it may be that women who agreed to participate
in the interviews were those who were particularly dissatisfied with
their experiences. However, in terms of the qualitative analysis this
should not be seen as problematic. Indeed, given the tendency for
women to express satisfaction with their maternity care (van
Teijlingen et al., 2003), it is advantageous to have had sufficient
examples of dissatisfaction to be able to extract with confidence some
common themes. The strength of the qualitative data is to identify the
features of satisfactory and unsatisfactory experiences, not to infer
prevalence.
3.9.2 The Pathway
One of the characteristics evident in those who were most satisfied
was having been made to feel welcome to attend hospital. At first
glance this would appear counter to the main philosophy behind the
All-Wales Pathway which, in promoting the normality of labour, is
encouraging women to stay at home in early labour to reduce
unnecessary interventions. However, as the data demonstrated, being
‘allowed’ to come in was not necessarily immediately followed by a
woman’s attendance: in some cases it was the safety net they needed
to have the confidence to remain at home a little longer. A further
feature in those with greatest satisfaction was the perception of
choice, so that they did not feel that they were being denied
something. In many such circumstances, the advice of the
professional was still valued and was influential in the woman’s
decision.

The OPAL study
©NCCSDO 2007 150
Being first-time mothers with no prior experience of labour, many of
the women were anxious. One of the key elements of their anxiety
was the uncertainty of when they would be ‘allowed in’. The Pathway’s
philosophy of encouraging and supporting women to remain at home
in early labour can, if not explained clearly, potentially exacerbate this
anxiety. Where uncertainty is perpetuated, for example through vague
instructions about when to phone back or a lack of indication of when
they will be likely to attend, anxiety is further worsened and
satisfaction with the phone call diminished. For a minority, having the
conversations on the phone makes this situation worse and it can lead
to feelings of uncertainty over the decisions and assessments being
made, which in turn feeds the anxiety. Where it is clear to the woman
why she is being encouraged to remain at home, and an indication
given as to when she will be asked to come in, there is greater
satisfaction, and the parallel situation is true for women who are sent
home after attending hospital. The role of antenatal information so
that women know what to expect, and why, should not be
underestimated.
Where dissatisfaction occurred in either the first or second phone call,
there was a negative impact on subsequent calls and attitudes
towards going into hospital. Each individual call needs to be managed
well if the rest of the Pathway of care is not to be jeopardised.
3.9.3 Professional and telephone skills of the
midwife
The most statistically significant finding was that women who do not
feel treated with respect and as an individual were dissatisfied. This is
in keeping with a growing body of research literature which highlights
this fundamental of communication in a wide range of settings. It may
well be that making a woman feel that she is being respected and
treated as an individual is more difficult to achieve on the telephone
where there are fewer non-verbal ways of showing this. However, the
perception of being taken through a pre-set list of questions was not
related to satisfaction, so this clearly does not preclude a midwife from
treating a woman as an individual and with respect. Women who were
more satisfied were more likely to mention that the midwife was
friendly and gave instructions in a confident manner. There was
dissatisfaction when the midwife was less friendly, and especially if
she:
• made the woman feel silly,
• made the woman feel that she was not believed,
• left the woman confused about her meaning.
In a minority of cases it was clear that the midwife responding to a
telephone enquiry was not aware of the instructions the woman had
been previously given by a colleague. This usually resulted in the
woman feeling embarrassed and dissatisfied, as well as eroding
confidence in the midwife.

The OPAL study
©NCCSDO 2007 151
Another key feature of the less satisfactory phone conversations was
the absence of reassurance by the midwife; conversely where
reassurance was given, it was associated with higher satisfaction.
Coupled with this was the importance of support and encouragement
over the phone. Where there was evidence of unmet need for
reassurance and support, there were higher rates of dissatisfaction
and residual anxiety after the call. Left unchecked, these residual
anxieties can lead to misconceptions, lack of confidence in the
assessment being made and the advice being given, and additional
need for more calls.
The length of phone calls appeared to be important: where women
reported no calls lasting 5 min or more, there was reduced
satisfaction. We must, of course, be cautious about this finding
because it is based entirely on women’s retrospective assessment of
the length of each call. However, it does seem plausible that shorter
calls are less likely to have had time spent on reassurance and
support. Time and skills need to be employed to pick up on, and
address, unmet needs for reassurance, support and information.

The OPAL study
©NCCSDO 2007 152
Section 4 NHS Direct
4.1 Views of Heads of Midwifery in England
As described in Section 2.1.4, the initial component of the survey of
HoMs in England included a cover sheet that allowed the research
team to identify all of the units within each HoM’s jurisdiction and, in
the case of delegation of completion of the main survey tool, to obtain
his/her direct response on two key issues: views related to NHS Direct
involvement in early labour services and interest in use of the
Pathway. The reason for seeking a response directly from the most
senior midwife in each Trust was that it was considered that if these
areas had been explored, it would be likely to receive the attention of
the HoM as strategic midwifery lead who usually combines a
managerial role with the statutory function of supervision of
midwifery.
The first question asked HoMs whether they had considered
introducing the telephone component of the Pathway; responses are
shown in Table 4.1.
Table 4.1 Consideration of the introduction of the telephone component
of the Pathway
Frequency Percentage
Yes 33 25.2%
No 39 29.8%
Not sure 55 42.0%
Missing 4 3.1%
Total 131 100.0%
The majority of HoMs were unsure (42 per cent); a quarter indicated
that it had been considered and 29.8 per cent that it had not.
The HoMs were asked whether there was any potential role for NHS
Direct in early labour services; whether there had been any
exploration of the use of NHS Direct for early labour services in their
local area; whether any pilot work had been carried out or was
planned and whether they had been involved in exploring the use of
NHS Direct in early labour. Questions with possible response options
are included below; boxes were incorporated to allow respondents to
provide further information on this issue; the format of the cover
sheet can be seen in Appendix B.

The OPAL study
©NCCSDO 2007 153
Responses to questions related to NHS Direct are as shown in Tables
4.2–4.4.
Table 4.2 Do you feel that there is any potential role for NHS Direct in
early labour services?
Frequency Percentage
Yes 13 9.9%
No 87 66.4%
Not sure 29 22.1%
Missing 2 1.5%
Total 131 100.0%
Table 4.3 Has there been any exploration of the use of NHS Direct in
early labour in your area?
Frequency Percentage
Valid Yes 4 3.1%
No 121 92.4%
Not sure 4 3.1%
Missing 2 1.5%
Total 131 100.0%
Of the four HoMs who reported exploration of NHS Direct in their area,
one was aware of pilot work (#10) and one had been involved in local
exploration of NHS Direct (#116). Two respondents were aware of
pilot work (#54, #162) and one HoM reported exploration of NHS
Direct in her previous post in a different Trust (#153).

The OPAL study
©NCCSDO 2007 154
Table 4.4 Concerns about use of NHS Direct for early labour services
Frequency
Who is giving advice? Professional midwifery issues 67
Negative impact on communications 28
No knowledge of individual Trust policies 24
Appropriateness of approach
Is an algorithm enough?
Difficulty in making an assessment by phone
Concerns related to IT
18
Litigation; vicarious liability; complaint; accountability* 9
What else can NHS Direct provide beyond our existing services? 9
Concerns about women at high obstetric or social risk 6
Poor experience of NHS Direct/lack of knowledge of NHS Direct’s guidelines
5
No problems/possible role for NHS Direct – as long as NHS Direct work within guidelines and algorithms are agreed
4
Whether all language needs can be met 3
Contradicts NSF and encouragement to move to caseload holding 2
Cannot comment: inadequate information/evidence 1
NHS Direct – not the answer; sort out the local service 1
*Identified as concerns by HoMs due to potential shared responsibilities between
NHS Direct and the maternity services.
Heads of Midwifery were asked to identify any particular concerns
about the use of NHS Direct for early labour services. A thematic
content analysis demonstrated a range of concerns amongst HoMs.
These are included in Table 4.4 and many HoMs provided more than
one response. Only four HoMs had no concerns or felt that there could
be a role for NHS Direct in early labour care. The most frequently
stated concern related to who would be providing such advice and a
feeling that the midwife was the most appropriate professional to do
this. Negative impacts on communication with women and the lack of
continuity were identified, together with a negative impact on
communications with labour wards and the importance of clinical areas
knowing who could be expected to attend the labour ward. A need for
advice to be tailored to the individual policies of each Trust was
stipulated. Doubts were expressed about the appropriateness of an
algorithm-based approach to providing advice that appeared reliant on
IT, together with concerns about responsibility where problems
occurred, for example, litigation or complaint. A range of other
concerns was reported less frequently.

The OPAL study
©NCCSDO 2007 155
4.1.1 Interview data
Telephone interviews were conducted with three Heads of Midwifery
who had been involved in exploration or discussion of the use of NHS
Direct for early labour services. These HoMs worked in different areas
of England; one in the north east, one Midlands, one London; two had
jurisdiction over large maternity services (4500 and 6700 births per
annum) and the other a smaller-sized unit (1250 births per annum).
A range of issues had triggered exploration of the use of NHS Direct:
…sort of reviewing all of their processes, thinking could it apply to
midwifery? Because as a unit we do get well over 10,000 women a
year coming through our triage area, so it’s a huge issue for us to look
at ‘how could we manage telephone advice better?’
(#10)
Following exploration of NHS Direct, this unit had moved towards a
telephone triage approach to women’s enquiries as it was considered
important that advice about early labour should be provided by
midwives and a view that a less structured approach than that used by
NHS Direct was preferable:
…as a midwife you ask those questions and if you’re going to follow a
set algorithm, there are some times you’d want to deviate from that, as
a midwife, depending on the answer you’ve got. It isn’t always that
you could follow one arrow or another, depending on what the woman
told you. I mean, as we know, sometimes women don’t give yes/no
answers to things so you can move on to the next box, so to speak. I
mean maybe this is just being very, very cautious but the midwives felt
that it’s better to have a freer conversation I suppose.
(#10)
Although HoMs expressed concerns about the perceived rigidity of the
NHS Direct approach, several acknowledged that they were, in fact,
exploring the use of structured tools for telephone assessment and
one commented on the apparent internal inconsistency in this.
A further HoM had been involved in a sector-wide discussion about
implementing an NHS Direct-type approach across the hospitals in
that group; this exploration had been led by consultant midwives but
had not been pursued further due to anticipated NHS re-organisation
at the Strategic Health Authority level and other competing priorities
for service development.
A further significant service consideration for this area had been the
multicultural population where 120 languages are currently spoken.
There was a concern that the advice provided might not be culturally
appropriate for the local population:
…it’s quite general the advice given and it’s not specific to the needs of
women in X [area] and so we’ve got cultural mix and the issues that we
have here – we’ve got more understanding of that. And all we would
like to pull together is, in X [area] and to be able to deliver that to these
women, given that we’ve got better understanding of what their needs
are, as opposed to, a sort of national…

The OPAL study
©NCCSDO 2007 156
(#74)
Providing early labour services for women who do not speak English
was identified as a challenge in more than one unit.
It certainly is a challenge for us, because sometimes the women arrive
and they might have called an ambulance, and how do they get home if
you don’t need to keep them, and you start on the spiral really where
they don’t need to be here but they’re in the system type of thing. And
the other type of thing is that we’re desperate for early labour facilities.
(#10)
This HoM also saw the telephone contact as fulfilling a risk-assessment
purpose and was doubtful that could be delivered by NHS Direct.
So, it was trying to risk assess them at the same time, knowing that we
had, maybe not medical concerns, but there were a lot of social
concerns with women in our area.
(#74)
One HoM reported that she had explored joint funding with
neighbouring Trusts of a midwifery post based in NHS Direct but other
Trusts had not wished to support that:
We had to have a local model that sort of reflected the way NHS Direct
worked, but we needed to fix all the cost and the logistics of it, but
what followed really had to be maternity based, as opposed to the
general one that NHS Direct took on.
NHS direct do not always give the right advice – our idea was to second
a member of staff to be employed at NHS Direct.
(#116)
4.2 Views of midwives in Wales
The concerns expressed by Heads of Midwifery in England were,
perhaps unsurprisingly, echoed by midwifery participants in focus
groups conducted in Wales related to the Pathway.
The overwhelming response from midwives regarding NHS Direct
providing early labour advice was one of rejection. The focus groups
identified several areas of concern; first there was the issue of the
professional status of the person advising women, whether they had
an active midwifery registration and whether and how they would
receive supervision of midwifery if based in NHS Direct. There was
also an opinion that if women telephoned NHS Direct for advice in
labour it would erode the midwife’s role in being the first point of
contact for women.
We’ve worked hard for the midwives to be the first point of contact,
we’ve worked very hard to have a named midwife for our women, then
to give the first phone call to NHS Direct is a big backwards step.
(S1)
The OPAL study
©NCCSDO 2007 157
In addition there was a concern about the quality and appropriateness
of advice given to women who were known to have contacted NHS
Direct.
Women do ring NHS direct, surprisingly, and they are not advised
correctly. We have had problems because they haven’t known, because
they have phoned them [NHS Direct] first and had incorrect advice.
(N9)
The midwives also expressed concern regarding how advice given by
NHS Direct would be passed on to the relevant area within the local
maternity services with the implication that care could become
fragmented resulting in a lack of consistency and continuity, all of
which would appear to be in opposition to the aims of effective service
provision. This concern appears valid in the light of the difficulties
reported by community midwives in Wales related to ensuring that
Part 1 documentation was accessible for hospital staff within the time
frame of a woman’s labour.
4.3 Discussion with staff of NHS Direct
A meeting of members of the research team with senior staff of NHS
Direct was convened to identify current processes and response to
enquiries related to labour. It was confirmed that no algorithms
specific to normal labour were currently in use or under development;
women contacting the NHS Direct telephone service for advice related
to labour would always be directed to contact their maternity service
provider. It was confirmed that the number of midwives employed by
the service was not sufficient to ensure that a midwife was on duty at
all times in the call centres. Algorithm development was reported to
require at least 6 months, following which piloting and tests for clinical
integrity would be required. No plans existed, at that stage, to extend
the service to include the provision of advice to labouring women,
although interest was expressed in the findings of this research.
4.4 Conclusion
In conclusion, the concerns reported by midwives encompassed the
importance of early labour advice being provided by midwives, risk
management, doubts about whether a telephone conversation would
allow a comprehensive assessment and the importance of meeting the
needs of women in their local community. There appeared to be no
view that NHS Direct had any potential utility in England in the
provision of early labour services and there was little interest in
further exploration of its use.

The OPAL study
©NCCSDO 2007 158
4.5 Incorporation of structured telephone assessment for the SDO-funded Early Labour Support and Assessment (ELSA) trial
Delays in the timetable described in Section 1.4, together with the
6 months required to develop and pilot algorithms or other structured
telephone tools, meant that the timetables of the two studies were no
longer running in parallel, as had been anticipated previously.
Multicentre Research Ethics Committee and research governance
approval had already been obtained and permission for a further
protocol amendment would be required to support any changes to
care for women in either arm of the trial. The time required to develop
and test a tool for structured telephone assessment would not fit into
the timescale of the trial, the preparatory work and recruitment of
which had already commenced.
Discussions with Heads of Midwifery in centres supporting the ELSA
trial had also revealed additional concerns about trying to incorporate
structured telephone assessment into the trial for women allocated to
the intervention group who laboured at night. These concerns included
the time for training in use of the new tool, potential for confusion
among midwives and women and difficulty in trying to maintain a
distinction between standard care for the unit and a different approach
to advice for the intervention group at night, thus contributing an
additional variable in the analysis.

The OPAL study
©NCCSDO 2007 159
Section 5 Discussion and conclusion
5.1 Discussion
5.1.1 Methods
The approach to identifying the sampling frame of English maternity
units by using the Local Supervising Authority Midwifery Officer’s list
appeared to work well in the context of continuing Trust
re-configurations. One potential demerit of using this approach was
that some non-NHS and island maternity facilities were identified, as
they also fall within the jurisdiction of statutory supervision of
midwifery but they did not meet our criteria for inclusion. The use of
further sources and unit websites allowed us to confirm inclusion or
exclusion of units and senior midwives also indicated if they felt that
they did not meet our criteria.
We were using the approach of a cover sheet – to be completed by the
Head of Midwifery and confirming the identity of units in her
jurisdiction – followed by a questionnaire per clinical site (hospital or
Birth Centre), for the first time. This allowed us to verify information
about the number and identity of maternity units by Trust and also to
obtain the HoM’s own view on issues of strategic importance. Further,
it appears that offering the option of delegating completion of the
questionnaire to a midwifery colleague was also acceptable to Heads
of Service and reduced demands on their time, as we are aware that
HoMs are frequently asked to participate in surveys. The use of
telephone interviews for Heads of Midwifery also seemed an
acceptable approach for all parties; the interview was easily
rearranged if the HoM had been called away at the scheduled time. We
feel that this allowed a more relaxed approach than trying to complete
face-to-face interviews when there are pressing demands on HoMs
that can arise at short notice.
Similarly, the two–stage approach of questionnaire and interview was
appropriate to map the overall service provision but also to identify
and subsequently obtain further detailed information about innovative
services. Despite pilot testing of both data-collection tools (the cover
sheet and questionnaire) we encountered problems caused by the
range of terminology used for particular service settings. For example,
small units where women give birth may be called community units,
Birth Centres and midwifery (-led) units and although we tried to
achieve clarity and avoid offence, there was always a concern that
some units may have felt that wording of some questions did not
relate to their circumstances. Although we were aware of this issue, a
satisfactory response rate was achieved across a range of sizes and
types of unit.

The OPAL study
©NCCSDO 2007 160
Although completion of core data items describing early labour service
provision was again satisfactory, it became apparent that questions
requesting statistics related to a unit were not always provided. The
reasons for this appeared to include the fact that some Trusts had
recently undergone reconfiguration, and thus any data available did
not reflect the current new service provision or population. In addition,
some Trusts appeared to have data at the Trust rather than unit level
and for some data items it appeared that HoMs did not have access to
that statistical information; for example, the proportion of women
admitted and discharged home not in labour. Whereas the poor quality
of maternity data has been recognised for some time, it is surprising
that data are not available using IT and maternity database systems;
inputting information into these systems appears to cause a significant
burden to staff in maternity units. We are aware of a small number of
further changes to maternity services that have occurred since the
data-collection period.
There were few opportunities for the core team to make meaningful
links with maternity service professionals in Wales. None of the core
research team had existing professional linkages in that area. While
efforts had been made to network with midwives in Wales at the start
of the research, significant time subsequently elapsed before
preparatory work started in the centres due to delays in governance
processes. There was also a considerable geographical distance
between the core research team in York and the Trusts in Wales, and,
for that reason, despite the efforts of the midwifery research
fieldworker, it was difficult to engender support for the research. In
addition, the model of support to the centres in this research was
different from that of the ELSA trial where a sustained period of
recruitment led to the need for an appointment of a Local Midwifery
Co-ordinator for 1 day per week in each of the six participating Trusts
throughout the recruitment period.
We were disappointed in the numbers of women recruited in Wales. In
working to meet the requirements of research governance, we
encountered a significant number of delays that impacted negatively
on the planned investigation. While we are aware that these processes
have subsequently been reviewed, the impact on this research was
significant and contributed to the small sample size. Although
alternative approaches to recruitment in Wales were explored, they
were not feasible and would have required development and
submission of protocol amendments.
The slow rate of recruitment was also rather surprising when
compared with the steady rate of recruitment to the ELSA trial by
community midwives in Yorkshire. The reasons for this were possibly
multifactoral. We had originally designed the sampling frame to allow
us to include women from all parts of Wales and to both minimise and
equalise the burden for community midwives throughout Wales, but
this was, perhaps, counter-productive. It may be that, although the
sampling strategy was methodologically robust, requesting only
The OPAL study
©NCCSDO 2007 161
2 weeks of recruitment conveys a message that the endeavour is too
transitory to be important, compared to a sustained period of
recruitment. It also offers little opportunity for midwives to become
acquainted with the system for identification and recruitment of
potential participants.
An alternative sampling frame, perhaps including fewer Trusts with a
longer period of recruitment, could have allowed consolidation of
resources, better use of the midwifery research fieldworker’s time and
more intensive communication with Trust staff. This approach may still
mean that the impact of local applications of a policy may remain
undetected. Alternatively, sampling via other systems such as birth
registration would allow the inclusion of women throughout Wales but
this approach would not ensure that the clinical characteristics
required in the sample could be met.
Two of the South Wales Trusts were also accessed in another study of
the Pathway. This may have led to research fatigue by some
midwives, or possibly a misunderstanding that these were the same
study. Furthermore, the majority of recruitment took place during the
summer months and peak holiday period. This may have impacted on
the midwives’ ability to recruit as, during peak holiday periods, they
are required to take on the work of colleagues who are on leave. In
addition to this one of the Trusts underwent a re-organisation of their
maternity services, which had an enormous impact on their
community midwives and led to a period of unsettledness. There were
also a number of areas with high levels of staff absence through
illness. All of the above factors plus an inability to provide a sustained
physical presence in Trusts may have contributed to the overall low
response rate. It may be possible that a designated midwife in each
Trust with responsibility to act as a local liaison would have achieved a
greater sense of ownership.
Although midwives are ideally placed to know the circumstances of an
individual woman’s experience and the clinical course of events during
labour and birth, their involvement in research is also difficult because
of the preparation time required. Meeting agendas, mandatory
in-service training and other routine events often lack capacity to
incorporate a further (research) component that is of lower priority
than the midwife’s other activities. Based on these experiences,
recruitment via community midwives during their provision of routine
postnatal care appears unsatisfactory and it may be too difficult for
midwives to incorporate into their current workload. Recruitment by
community midwives has the potential for selection bias and to
increase the proportion of women who decline participation. We would
not advocate use of this method of recruitment in future research
unless increased local ownership could be fostered.
Members of our research team had used telephone interviews with
new mothers previously and found this approach to be highly
acceptable (Ewing and Green, 2000). This was also found to be the
The OPAL study
©NCCSDO 2007 162
case in this research. In any project involving new mothers, it is
important to allow for the unpredictability of life with a newborn baby
and sleep deprivation is not uncommon: interview arrangements
therefore need to be flexible. The configuration of our research team
included two researchers who themselves worked in part from home;
we were therefore able to offer most of the day (9.00 am–9.00 pm),
including evenings, as a potential time for the interview to be
conducted. This appeared to suit families as, during the evening, it
was more likely that there would be another adult at home to take
care of the baby during the interview, if required. Telephone
interviewing is also useful as it avoids the potential intrusion of a
visitor in the woman’s home and any perceived need for preparation.
The CATI facilitated routing of questions and reduced the amount of
typing required compared to traditional full transcription. Piloting of
the system was essential to ensure a smooth flow through the
interview. In our pilot work, we identified that the researcher needed
to understand the overall sequence of events in the labour, in order
that subsequent enquiry could focus on the telephone component, as
this was not the element that the woman would automatically focus
on. It was essential to have available a paper version of the CATI
questions in case of computer failure during the interview. The main
benefit of CATI was that data collection and input happened largely
simultaneously. Tape-recording the interview ensured that any
information that could not be typed in at the time could be entered
later. When conducting a large number of interviews this is of huge
benefit; however, the lower-than-anticipated response rate meant that
this particular benefit was not as widely apparent. One slight
disadvantage is the delay that data entry can cause to the course of
the questioning. When listening to the tapes after the interview, the
sounds of keystrokes and pauses while typing occurred were
noticeable. Mouse clicks are a further potential distraction as the
interviewer proceeded through screens. Participants, however, seemed
generally untroubled by these issues and the pausing sometimes
meant that other information or details occurred to them and which
might otherwise have been missed could be captured and there was
also an opportunity to verify what had been said.
In planning focus groups, we wanted to learn midwives’ perceptions of
the telephone component of the Pathway from their discussions
together. Whereas all Trusts were not represented at the focus
groups, discussions flowed freely among both the community and
hospital-based midwives. We were aware of the difficulties of releasing
staff from their clinical duties to attend meetings or training and
wanted any midwives or obstetricians to be able to offer their own
perspectives on the telephone component of the Pathway. We
circulated newsletters on labour suites and other maternity areas with
a short questionnaire on the reverse that could be completed and
posted back to the research team. We also offered the opportunity for
online completion, but received few questionnaire responses. We feel
The OPAL study
©NCCSDO 2007 163
that this indicates that midwives and obstetricians did not feel
particularly strongly, either positively or negatively, about the
telephone component of the pathway, although it may be that they
have stronger views on its subsequent components.
It was interesting that the offer to use electronic methods to provide
information met with little response. This experience was mirrored in
the survey of HoMs in England where offers to provide data-collection
tools electronically were rarely taken up.
5.1.2 NHS Direct
The majority of midwives, both managerial and clinical, felt that NHS
Direct did not have a role in the provision of early labour services. The
most commonly cited reasons for this included professional concerns
about the importance of advice related to early labour being provided
by practising midwives. Additional concerns included a view that the
use of NHS Direct would have a detrimental effect on communications
with women and with the labour wards and that NHS Direct would not
be familiar with the policies of each Trust.
It appears unlikely that NHS Direct would be able to ensure midwifery
availability in all of its call centres throughout the 24-h period and,
when the pool of midwives in England is not increasing rapidly, such
appointments would inevitably reduce the numbers of midwives
available for hospital and community services.
Concerns were also expressed, albeit less frequently, about whether a
telephone assessment governed by an algorithm, perceived as an
inflexible tool, was the most appropriate method for giving advice
related to early labour. This strength of feeling was, to an extent,
surprising when, in the questionnaire responses and interviews, it
became apparent that several units were developing structured
telephone tools.
One issue appears to be that of knowing the local population, its needs
and geography and of providing advice fitting with local Trust policies.
This issue was also reflected by one of the senior midwives
interviewed; the sense of ‘our’ population being different to those of
other areas and therefore, in her view, rendering use of the Pathway
inappropriate in one English setting.
Midwives in Wales acknowledged the need to develop skills of
telephone assessment when the Pathway was introduced. One
difference between the Pathway and NHS Direct includes the access to
an existing midwifery knowledge base that can be adapted for
telephone application. There are also differences between the two
approaches; NHS Direct appears to focus on assessment and the
Pathway includes the additional component of providing evidence-
based advice.
Earlier research evaluating NHS Direct reported an over-cautious
approach in the advice given by nurses (Munro et al., 1998). Although

The OPAL study
©NCCSDO 2007 164
those researchers considered this a desirable trait, it suggests that, if
NHS Direct were to be used for early labour advice, this might result in
a duplication of resource use with women being asked to contact the
unit where they are booked, in addition to contacting NHS Direct. The
effect of this on women’s overall experience of labour and potential for
conflicting advice, previously a criticism of the maternity services
(Audit Commission 1997), would require exploration, if telephone
advice via NHS Direct became a part of service provision.
Concerns about potential negative impacts of NHS Direct on continuity
within primary care were voiced by Florin and Rosen (1999). Concerns
about disruption to communication were reported by HoMs in England
and midwives participating in focus groups in Wales. Similarly, the
difficulties of completing Part 1 documentation for community
midwives in Wales and in making that available in a timely manner to
hospital-based care providers could occur if NHS Direct was utilised for
early labour services. In the context of HoMs’ concerns about potential
litigation and responsibility in the case of complaint, efficient IT-based
mechanisms would be required to ensure communication about
labouring women with provider units.
There will also be, as identified in interviews with women in Wales,
some who will prefer and only be reassured by face-to-face advice and
assessment.
5.1.3 England
The responses to the questionnaire indicated that considerable
energies have been expended in making changes to early labour
services in England over the past 5 years. Some units that have
already made changes are planning further ones. The drivers to
change appear to have been local factors; that is, an increase in
bookings, response to staff shortages and clinical risk management. In
addition, several senior midwives interviewed identified the impact on
their workload of women attending their labour ward who are not in
labour.
Changes to services to date have occurred more frequently in
consultant units with midwifery-led care areas. It is also apparent that
changes were more likely in the larger maternity units and it is these
larger units, together with consultant units without midwifery-led care
areas, that reported planning (further) changes to their services. This
may be for a variety of reasons. Changes may have been stimulated
by the introduction of midwifery-led care; it may be that larger units
have more difficulty in dealing with large numbers of non-labouring
attenders or that smaller services have been developed with a focus
on early labour care or in premises that support its provision. No units
identified either rurality or serving a particular urban area as a trigger
for service change.
The fact that units that had already changed their early labour
services were planning further changes suggests that the anticipated

The OPAL study
©NCCSDO 2007 165
benefits of previous changes had not been realised. It was also
apparent, albeit in the context of the small amount of data for some
innovations, that service changes brought implications in terms of
requiring more staff and more training. As staff shortages were among
the local factors that triggered service changes, then careful
consideration must be given to the adoption of any new approaches.
This research was conducted at a time when changes to the
commissioning process were anticipated; a minority of questionnaire
respondents and interviewees mentioned this. In the interviews we
heard examples of maternity service providers starting to work with
Primary Care Trusts to address issues such as reducing unnecessary
admissions; this included the allocation of funding subsequently used
to develop a triage area and also of exploration of community-based
locations for early labour assessment. It was clear that HoMs expected
some impacts on service-level agreements from practice-based
commissioning (Department of Health, 2004b); further research will
be required to determine these.
It was interesting to note that despite the amount of effort expended
in service change, HoMs reported relatively little evaluation of early
labour services, even in those units where change had been effected.
It may be that in some units the changes had been implemented
relatively recently and it was considered that evaluation was not yet
appropriate or that resources to support evaluation, either financial or
skills-related, were not easily accessible. Consultant units reported
evaluation of services more frequently; this reflects the findings of a
study reporting governance procedures in different types of maternity
unit (Smith and Smith, 2006). The majority of units, but not all,
reported the availability of guidelines related to early labour care;
increases in this can be expected following publication of the NICE
Intra-partum Care guideline in 2007. Some units had changed their
services to incorporate recommendations from the NICE guideline
related to women with pre-labour rupture of membranes (Royal
College of Obstetricians and Gynaecologists, 2001a), including women
going home following initial assessment.
The ELSA trial is being conducted to evaluate the impact of offering
support and assessment at home to nulliparous women in early
labour. Although a small amount of primary research has previously
investigated the impact of this intervention, there is no high-quality
evidence derived from contemporary UK settings. It is interesting to
note, therefore, the extent to which this largely unevaluated
intervention is available in current UK maternity care, albeit selectively
in the majority of cases. One of the aims of this present study was to
inform the interpretation of the findings of the ELSA trial. If early
labour support and assessment at home is found to be a clinically
effective and cost-effective intervention, useful information has been
gained about the circumstances that support the continued provision
of a home-visiting service. This includes information related to the

The OPAL study
©NCCSDO 2007 166
model of midwifery care and the importance of adequate staffing
levels for community midwifery.
Among those units that currently provide home visiting in early labour,
a wish to delay admission to a hospital or Birth Centre during labour is
not the only outcome for such a service. Offering a woman the option
to delay the decision on place of birth until labour was a consequence
reported by one respondent whose unit’s home birth rate of 11 per
cent was considerably higher than the national average of 2 per cent
(NHS Maternity Statistics, England, 2004–2005; The Information
Centre, 2006). This was ascribed to a midwifery workforce that
appeared particularly supportive of home birth and may not occur in
other areas or workgroups. If this interesting outcome were to occur
in other areas, it is likely to require increases in community midwifery
staffing levels.
The involvement of MCAs in supporting women in early labour was
reported by one of the HoMs interviewed and is also included in the
report of new roles for maternity support workers (NHS Employers,
2005). Such approaches reflect current considerations of skill mix in
NHS maternity services. It may be that individuals other than
midwives can provide the supportive companionship that women need
as labour becomes established. Such approaches should, however, be
subjected to careful evaluation.
There appear to be an ever-increasing number of locations where
early labour services are provided. These appear as Day Assessment
Units, Maternity Assessment Units and triage areas. It is interesting to
note how the terminology used in North American settings has been
translated into the English context. While the limited descriptions of
triage areas suggest that women find them highly acceptable at the
anecdotal level, there is no evidence that they improve health
outcomes; neither is there evidence to refute the possibility of harm
and there has been no rigorous evaluation of their impact on the
psycho-social outcomes of labour. Similarly, studies of the cost-
effectiveness of such facilities were not identified in the literature. The
terminology has been adopted perhaps because new terminology
suggests innovation, but it may be that there is little difference
between Day Assessment Units, Maternity Assessment Units and
triage areas. Instead, all of these provide a service for women with
problems of pregnancy or where a woman requires reassurance. It is
unclear whether there is a distinct difference between these services
at a practical or philosophical level, although there may be variation
between units in admission criteria. One Head of Midwifery
commented on the potential for confusion between the triage and Day
Assessment Units in her area.
Triage systems were developed to determine the order of treatment
for battlefield casualties with the aim of returning the maximum
number to front-line combat. The term appears to have subsequently
been adopted for workload management in North American emergency

The OPAL study
©NCCSDO 2007 167
rooms and triage systems used to prioritise workload according to
severity of presentation, generally reflective of a high–risk approach to
maternity care. Its translation from general emergency settings to all
non-routine obstetric care raises questions about its appropriateness
for early labour care in UK settings. Although the institution of these
areas was seen, in some units but not universally, to address
workload-management issues, difficulties were reported, for example,
in issues of privacy that are key to a woman’s experience of labour.
Previous approaches to the assessment of early labour included
admission rooms, either single or multi-bedded, to which women
would be admitted while their partner or birth companion was
banished to a waiting room. A midwife would take a history of the
labour, assess maternal and fetal well-being, often including electronic
fetal monitoring, and confirm labour onset. This process may or may
not have involved consultation with a junior obstetrician. Such
admission areas fell into disuse for various reasons; a lack of privacy
for women who were in considerable discomfort and wanted to be
mobile and to assume positions of comfort in early labour; an
acknowledgement that women needed the support of a companion at
that time and a wish to avoid transfer between rooms for those
women for whom labour was confirmed. There is a danger that the
introduction of new assessment areas, however labelled, may to some
extent be re-introducing an outdated concept.
Further, if triage areas are working to prioritise admissions according
to clinical urgency, it is possible that women who are in early labour
may be restricted in movement and have their assessment delayed
while women with complications of pregnancy receive urgent
attention. It may also be difficult for midwives to provide the early
labour support, for example, discussion of coping strategies in multi-
bedded areas. If women are assessed in triage areas and found not to
be in early labour, discharge from that area will still mean that
repeated hospital attendance is required. Thus, while technically
removed from the labour suite’s category-X admissions, such women
may still be incurring personal costs for themselves and their family
and costs to the NHS from repeated journeys and admissions.
It is often the case that assessment procedures may be applied in a
universal way in any assessment area; this may include the use of
electronic fetal monitoring. This practice is not supported for routine
use on admission to labour wards for low-risk women in labour (Royal
College of Obstetricians and Gynaecologists, 2001b) thus there is a
risk that care, for some women, may return to a more routine
technological approach, counter to the emphasis on low-risk care in
the NSF (Department of Health, 2005).
One potential demerit of any new assessment area is that it requires
staffing. It is apparent from the data collected that there have been
both successes and failures in triage units, as reported by senior
midwives. Difficulties with staffing were among the problems

The OPAL study
©NCCSDO 2007 168
encountered and these appear difficult to resolve in a climate of
financial pressures.
The extent to which triage areas can be considered synonymous with
early labour care, based on the tenets of the NSF, of supporting
normality in childbearing, individualised care and equality of access is,
therefore, unclear. It therefore appears urgent that further research
explores, in detail, the care provided in triage and similar areas and
their appropriateness as a venue for early labour assessment.
The provision of drop-in services at Birth Centres, regardless of place
of booking offers a further, non-technological, location for early labour
assessment and advice. Again, there is little known about women’s
experiences of early labour services in these settings when subsequent
intra-partum care may be provided at a different site; however, this
does appear to fulfil the NSF’s requirements for ease of access and
support for normality.
One issue that figured in the description of the population served but
not as a trigger for change to early labour services was that of
language. Despite the fact that 57 units reported serving populations
that included over 5 per cent women from minority ethnic
communities and asylum seekers, only one innovative service was
identified in an interview with a Head of Midwifery. This involved a
befriending or so-called buddy scheme. It appears likely that, as
described by that HoM, without access to someone who speaks the
same language, women who do not converse in English may,
themselves, be unable to obtain early labour advice by telephone and
thus either labour unsupported at home or present at a maternity unit
when clinically inappropriate. The use of services such as language
link and, with the one exception described above, the involvement of
link workers, translators or other professional language services, were
not reported. This should not be interpreted as a lack of utilisation of
such services; it may be that in some maternity services their use is
embedded as an intrinsic part of maternity service provision. For
services where this not the case, however, it may be helpful if good
practice and innovative approaches could be reported in the
professional literature and via electronic bulletin boards to achieve the
equity in access to services for all women required by the NSF.
Some of the systems described by respondents as telephone triage do
not appear to share the theoretical underpinning of North American
triage systems. They appear to provide a more structured approach
for midwives‘ telephone conversations with women and to offer a form
of documentation that protects and is, therefore, welcomed by
midwives at a time of concerns about rising litigation (Webb, 2004).
In England, the greatest changes to early labour services have taken
place in consultant-led units and generally larger units. In addition,
local issues and a wish to provide a locally appropriate service figure
in senior midwives’ aspirations for the care provided to their
population. Any new developments in early labour care should meet

The OPAL study
©NCCSDO 2007 169
the requirements of the maternity module of the NSF and provide care
that supports normality in childbearing and that can be accessed
equally by all maternity service users. It appears likely, therefore, that
in considering optimal approaches to early labour provision, there will
not be a single solution in terms of approach but it may be that agreed
principles should be developed to underpin service delivery, however
local care is configured.
5.1.4 Wales
Women had several positive perceptions of the Pathway; these
included its helpfulness in orientating themselves and their family to
the terminology and possible sequence of events in labour and they
particularly appreciated discussion of the information leaflet with the
midwife during their pregnancy. The importance of antenatal
preparation in relation to the pathway is clear, whether it is individual
discussion between the woman and her community midwife or at
antenatal classes. Similarly women need prior information of labour-
related events that are treated as a variation from the Pathway, for
example, pre-labour spontaneous rupture of membranes at term
(which occurs in 6–19 per cent of pregnancies), in order that these do
not come as a shock and cause distress for the woman.
At the point of contact with labour suite, women had also consulted
other sources for advice and reported differences between when they
were invited to attend labour ward and what the information leaflet
had led them to expect. This mismatch may occur because it may be
that Pathway information is based on traditional views of signs of
labour, whereas it has been demonstrated by Gross and colleagues
(2003) that women experience labour onset in ways that do not
always reflect conventional professional teaching. Burvill (2002)
commented on the extent to which labour is a continuum and that the
stages of labour as experienced are not so clearly demarcated as
traditional obstetric and midwifery teaching suggests. The process of
labour varies between individuals (reflected in the various patterns of
contact with services on the trajectories Figures 3.2–3.6, Section 3). It
is therefore impossible to reflect every potential combination of labour
events in an information leaflet. It may be, however, that the leaflet
could be reviewed to avoid the disappointment caused when women
are not invited to attend the unit at the point at which they expect
that to occur. It is interesting to note that, for half of the respondents,
the Pathway did not prevent women being admitted and being sent
home without delivering their baby. This issue, in the context of an
initiative whose aim is to support women remaining at home, warrants
further investigation as some women experienced admission and
discharge (undelivered) more than once and others remained in
hospital but not in established labour.
It would appear difficult to fully realise the purpose of an integrated
care pathway for improving communications until both midwives and
women are conversant with the Pathway’s aims. It may be that the

The OPAL study
©NCCSDO 2007 170
importance of the telephone component of the Pathway could be
overlooked, as it comprises a telephone conversation, thus the
gateway to the labour ward remains as it was previously. There is,
however, the intention that there should be a clear difference between
the telephone conversations that midwives had with women prior to
institution of the pathway, that often resulted in a request to attend
the labour ward, and the current structured assessment and provision
of evidence-based advice. Midwives expressed an awareness of
tensions between supporting women to remain at home, while also
making sure that women feel welcome to attend the maternity unit
when they feel they need to. This again relates to the issues of women
being given realistic information about the Pathway and its philosophy
that being at home in early labour is considered to be in the best
interests of those women at low obstetric risk.
There appears to be a mismatch between midwives’ and women’s
perceptions of the duration of telephone calls. This may be due to the
relatively new status of the pathway when memories of the previous
shorter telephone response, generally inviting attendance, are still in
the professional consciousness. An alternative explanation of the
different perceptions of the duration of telephone conversations might
relate to the fact that a midwife may be called away from providing
care to a woman in established labour to respond to a telephone call.
It may be that concerns about leaving a labouring woman
unsupported might influence perceptions of call duration. Future
training could address this issue and improve women’s experiences of
the telephone call, in particular the amount of empathy and
reassurance provided by the midwife. Clearly, if the first telephone
conversation does not go well from the woman’s perspective,
subsequent interactions may not be successful.
Similarly, for women to benefit from the integrated care pathway
approach, midwives need to be able to access the advice given by
their colleagues on previous shifts or in other locations; thus, each
episode of early labour advice and assessment requires
documentation. This is also optimal for the midwife managing a labour
ward or Birth Centre who can consult documentation and know how
many women may be expected to attend within the next few hours,
assisting in the management of that clinical area.
Previous work has highlighted the importance to women’s experiences
of labour of being in control, involved in decision-making and of being
treated as an individual and with respect (Green and Baston, 2003).
The data collected in this research reflect this as women with higher
satisfaction scores reported feeling that they were able to make
choices and that they were being treated as an individual and with
respect. Conversely, lower satisfaction scores were associated with a
perception of being treated with a lack of respect or not as an
individual. Smith (2001) has demonstrated positive support from
professionals as a factor when evaluating women’s satisfaction with
different models of intra-partum care.

The OPAL study
©NCCSDO 2007 171
It is interesting to note the welcome that midwives have given to
telephone approaches to early labour care; midwives participating in
focus-group discussions felt that the telephone component of the
Pathway was supportive of midwives’ decision-making and useful in
the teaching of midwifery students. This was echoed by a senior
midwife in England who felt that the introduction of a structured
assessment tool supported midwives’ decision-making. Documentation
associated with this type of service change was seen as supporting the
midwife’s position, in case of subsequent clinical problem or complaint.
Further work investigating midwives’ decision-making related to
confirmation of labour onset is currently being explored in a
randomised controlled trial (Cheyne et al., 2006).
This present study has, we feel, generated a rich source of data
related to the experiences of midwives and women related to the
telephone component of the All-Wales Pathway for Normal Labour. We
have identified three current additional studies in progress in Wales
that will add to this. Data related to women’s early labour experiences
of the Pathway will provide a useful comparison to data related to
standard care and home visiting generated in the ELSA trial.
There is, however, a significant evidence gap in what is known about
the Pathway in terms of clinical outcomes for women and their babies.
We understand that data related to process (entry of women on to the
Pathway and proportion remaining on the Pathway throughout labour)
have been collated at Trust level; information on whether there are
health gains for women and babies is lacking. Although the
opportunity for evaluation through introduction in a randomised
controlled trial no longer exists in Wales, we would recommend that
any further implementation outside of Wales should take place within
a robust evaluation framework. It would, however, still be possible to
evaluate outcomes in Wales using research designs with historical
controls and we would strongly recommend further research to
address this issue.
5.2 Over-arching themes
The increasing array of options for early labour care is shown by the
range identified and the fact that, in some units, several approaches
to providing services are used concurrently. The main, although not
exclusive, driver to change relates to management of workload on
labour wards but normalising early labour; reducing interventions and
improving staffing ratios for women in established labour were also
identified.
Although several service innovations have aimed to reduce the
number of women admitted to a labour ward and subsequently
discharged home, there appears to be little evidence to demonstrate
whether this has occurred. It appears that much of the innovation in
services lacks a robust evidence base. Service changes are not
introduced within a framework of rigorous evaluation; the availability

The OPAL study
©NCCSDO 2007 172
of statistical information that allows monitoring of the impact of
change appears poor or inaccessible to senior staff in the maternity
services and for several service changes evidence of impact on clinical
outcomes is lacking.
For women’s experiences, the provision of written information about
early labour appears important but such information is not always
available and, if it is available, is not always discussed prior to labour
onset. With the exception of this current research, the impacts on
women’s psychosocial experience of different approaches to early
labour care are generally unknown.
For several of the service changes identified in this research, provision
impacts on staffing and training needs and service providers require
guidelines for practice. Midwives’ concerns about the availability of
documentation to protect their position in case of complaint remain;
clear and accessible documentation to record advice are all required
and several of the service changes identified have addressed this
(triage, telephone triage and the Pathway).
Questions remain about the extent to which a telephone conversation
can provide a complete assessment of a woman’s status at labour
onset; further exploration of this issue would be useful. Rigid
frameworks for telephone contacts were generally considered
inappropriate.
5.3 Conclusion
The NHS has instituted a range of approaches to early labour services
over the past 5 years in England and Wales without either evaluation
or ongoing audit. There is little evidence of the clinical effectiveness or
cost-effectiveness of any of these interventions. This research has
identified the range of early labour services in England, explored
particularly innovative services and gathered information that will
inform the interpretation of the results of the SDO-funded randomised
controlled trial, ELSA. Information gained about the telephone
component of the All-Wales Pathway for Normal Labour is now
available to inform both its future development and the preparation of
midwives for its use in practice. There appears little scope for
exploring the use of NHS Direct for early labour care. It is hoped that
the implementation of Best Research for Best Health (Department of
Health, 2006) and research passports will address the research
governance issues encountered in this research.
Recommendations for practice, policy and further research are listed
below.

The OPAL study
©NCCSDO 2007 173
5.4 Recommendations
5.4.1 Recommendations for practice
1 Changes to early labour services should be introduced within
robust systems of evaluation that address issues of clinical
outcome, impacts on women’s experiences and labour-ward
workloads.
2 Good practices in change management should be adopted that
foster staff involvement and time for discussion of new
approaches.
3 The provision of early labour care for women who may not be able
to communicate in English requires particular consideration.
4 Any changes to early labour services in England should reflect the
philosophy of the maternity module of the NSF (Department of
Health, 2005).
5 Statistical information should be of a quality to support evaluation
and monitoring.
6 Clinical guidelines for evidence-based care in early labour are
required.
7 Workload-management systems should be utilised to determine
impact of service changes.
8 The provision and content of written information about early
labour should be reviewed. Women should receive information
about the Pathway and have the opportunity to discuss it with a
midwife during pregnancy so that they also understand the
underlying philosophy.
9 The use of discussion boards or other electronically based
systems to facilitate the dissemination among providers of service
developments, experiences and evaluations related to early labour
care should be explored.
10 Further information about the philosophy of the Pathway should
be included in midwives’ training sessions.
11 The Pathway information leaflet should be reviewed to incorporate
information about events that will be treated as variations from
normality.
12 Documentation should be completed for each episode of
telephone assessment; this documentation should be available for
subsequent care providers.
13 Women should be given clear messages according to local policy;
for example, that they are welcome to attend a labour ward for
assessment at any time but they may be advised to go home
again to await established labour and why that may be advised.
14 Women should receive clear instructions about when they should
return to hospital if sent home.

The OPAL study
©NCCSDO 2007 174
15 Women should feel welcome to re-contact the labour ward
without feeling embarrassed.
16 Midwives need to consider spending more time on telephone
conversations with women in early labour to ensure that needs for
reassurance and information are met.
17 Midwives’ training needs in conducting telephone assessments
should be reviewed and training made available, where required.
5.4.2 Recommendations for policy
1 The telephone service provided by NHS Direct should not be
extended to include assessment of women in early labour.
2 The potential for Children’s Centres to be a further venue for early
labour services is not yet known and should be monitored.
3 The impacts on early labour services of changes to the
commissioning process should be assessed.
5.4.3 Recommendations for future research
1 The service provision and experiences of early labour for women
who are unable to communicate in English should be explored
further.
2 Clinical outcomes for women experiencing care under the Pathway
should be evaluated.
3 Women’s experiences of early labour should be explored
throughout the range of settings where care is provided; for
example, triage areas, Maternity and Day Assessment Units, and
Birth Centres.
4 The clinical effectiveness and cost-effectiveness of triage units
should be evaluated.
5 The impact of changes to the research governance framework
included in Best Research for Best Health (Department of Health,
2006) should be closely monitored.
The OPAL study
©NCCSDO 2007 175
References
Angelini, D. 1999a. Utilization of nurse-midwives as providers of
obstetric triage services. Journal of Nurse-Midwifery 44: 431–8
Angelini, D. 1999b. Obstetric triage in 10 US midwifery practices.
Journal of Nurse-Midwifery 44: 493–509
Arulkumaran, S., Michelson, J., Ingemarsson, I. et al. 1987. Obstetric
outcomes of patients with a previous episode of spurious labour.
American Journal of Obstetrics & Gynaecology 157: 17–20
Audit Commission. 1997. First Class Delivery Improving Maternity
Services in England and Wales. London: Audit Commission
Austin, D. 1996. The process of obstetric triage: management by
certified nurse-midwives. Journal of Perinatal Neonatal Nursing
10: 1–9
Austin, D. and Calderon, L. 1999. Triaging patients in the latent phase
of labor. Journal of Nurse-Midwifery 44: 585–91
Ball, J. and Washbrook, M. 1996. Birthrate Plus. Hale, Cheshire: Books
for Midwives Press
Barbour, R.S. and Kitzinger, J. 1999. Developing Focus Group
Research: Politics, Theory and Practice. London: Sage Publications
Barnes, P. and Dossey, M. 1999. Triage issues in an out-of-hospital
birth center. Journal of Nurse-Midwifery 44: 458–70
Baston, H. 2003. Admission to the hospital delivery suite. The
Practising Midwife 6: 11–15
Bonovich, L. 1990. Recognizing the onset of labour. Journal of
Obstetrics, Gynecological and Neonatal Nursing 19: 141–5
Burvill, S. 2002. Midwifery diagnosis of labour onset. British Journal of
Midwifery 10: 600–5
CEMACH. 2004. Why Mothers Die 2000-2002 Report on Confidential
Enquiries into Maternal Deaths in the UK. Plymouth: CEMACH
Cheyne, H., Dowding, D. and Hundley, V. 2006. Making the diagnosis
of labour: midwives' diagnostic judgement and management
decisions. Journal of Advanced Nursing 53: 625–35
Commission for Health Improvement. 2004. What CHI has found in:
NHS Direct Services. www.healthcarecommission.org.uk/_db
/_documents/04000053.pdf
Creasy, J. 1997. Women's experience of transfer from community-
based to consultant-based maternity care. Midwifery 13: 32–9
Creedy, D.K., Shochet, I.M. and Horsfall, J. 2000. Childbirth and the
development of acute trauma symptoms: incidence contributing
factors. Birth 27: 104–11
Crow, R., Gage, H., Hampson, S. et al. 2002. The measurement of
satisfaction with healthcare: implications for practice from a

The OPAL study
©NCCSDO 2007 176
systematic review of the literature. Health Technology
Assessment 6, no. 32
Dennett. S. and Baillie, F. 2002. From here to maternity. Health
Service Journal 37: 24–5
Department for Education and Skills. 2004. Every Child Matters,
Change for Children. Nottingham: DFES Publications
Department of Health. 1993. Changing Childbirth (1993) Part 1:
Report of the Expert Maternity Group. London: HMSO
Department of Health. 2004a. Improving Working Lives in Midwifery. A
Guide for Midwives and Managers. London: Department of Health
Department of Health. 2004b. Practise Based Commissioning:
Engaging Practices in Commissioning. London: Department of
Health
Department of Health. 2005. National Service Framework for Children,
Young People and Maternity Services. London: Department of
Health
Department of Health. 2006. Best Research for Best Health
Implementation Plan 4.1. Bureaucracy Busting: Governance,
Advice and Ethics Systems. London: Department of Health
DeVore, N.E. 1999. Telephone triage: a challenge for practicing
midwives. Journal of Nurse-Midwifery 44: 471–9
Downe, S., McCormick, C. and Lawrence Beech, B. 2001. Labour
interventions associated with normal birth. British Journal of
Midwifery 9: 602–6
Ewing, G. and Green, J.M. 2000. Infant Weaning: Lay and Professional
Accounts of the Weaning Process. Final Report to the NHS
Executive, Anglia and Oxford Regional R&D, grant no.
HSR/CCS/1095/69. Cambridge: Centre for Family Research,
University of Cambridge
Ferguson, P. 2003. Change through consensus and commitment. The
Practising Midwife 6: 4–5
Ferguson, P. 2004. The Pathway to normal labour. The Practising
Midwife 7: 4–5
Flamm, B., Berwick, D. and Kabcenell, A. 1998. Reducing Cesarean
section rates safely: lessons from a "breakthrough series"
collaborative. Birth 25: 117–24
Flint, C. 1993. Midwifery Teams and Caseloads. Oxford: Butterworth–
Heinemann
Flint, C. 1996. Home assessment in early labour. MIDIRS Midwifery
Digest 6: 169–70
Florin, D. and Rosen, R. 1999. Evaluating NHS Direct. British Medical
Journal 319: 5–6
Foster, E. 2000. Setting up a collaborative care plan. Nursing Standard
15: 40–3

The OPAL study
©NCCSDO 2007 177
Fox, S. 2004. All-Wales clinical pathway for normal labour: a way to
reducing unnecessary intervention? Midwives 7: 216–19
Garcia, J., Redshaw, M., Fitzsimons, B. and Keene, J. 1998. First Class
Delivery: a National Survey of Women’s Views of Maternity Care.
Audit Commission: London
Goldbeck-Woods, S. 1996. PTSD may follow childbirth. British Medical
Journal 313: 774
Green, J.M., Coupland, V.A. and Kitzinger, J.V. 1990. Expectations,
experiences and psychological outcomes of childbirth: a
prospective study of 825 women. Birth 17: 15–24
Green, J.M., Coupland, V.A. and Kitzinger, J.V. 1998. Great
Expectations: a Prospective Study of Women’s Expectations and
Experiences of Childbirth, 2nd edn. London: Books for Midwives
Press
Green, J., Baston, H. 2003. Feeling in control in labour: concepts,
correlates and consequences. Birth 4: 235–47
Gross, M., Haunschild, T., Stoexen, T., Methner, V. and Guenter, H.
2003. Women's recognition of the spontaneous onset of labor.
Birth 30: 267–71
Hall, J. 2003. All-Wales clinical pathway for normal labour launched.
The Practising Midwife 6: 7
Hannah, J. 2005. Maternity Care: Births in England. Midwifery and
Other Workforce Provision. London: Department of Health
Hemminki, E. and Simukka, R. 1986. The timing of hospital admission
and progress of labour. European Journal of Obstetrics &
Gynecology and Reproductive Biology 22: 85–94
Hodnett, E.D., Downe, S., Edwards, N. and Walsh, D. 2005. Home-like
versus conventional institutional settings for birth. Cochrane
Database of Systematic Reviews 1: CD000012
Holmes, P., Oppenheimer, L.W. and Wen, S. 2001. The relationship
between cervical dilation at initial presentation in labour and
subsequent intervention. British Journal of Obstetrics and
Gynaecology 108: 110–24
Jackson, D.J., Land, J.M., Ecker, J., Swatz, W.H. and Heeren, T. 2003.
Impact of collaborative management and early admission in labor
on method of delivery. Journal of Obstetrics, Gynecological and
Neonatal Nursing 32: 147–57
Janssen, P.A., Iker, C.E. and Carty, E.A. 2003. Early labour
assessment and support at home: a randomized controlled trial.
Journal of Gynaecology Canada 25: 734–41
Klein, M., Lloyd, I., Redman, C., Bull, M. and Turnbull, A.C.A. 1983.
Comparison of low risk pregnant women booked for delivery in
two systems of are: shared-care (consultant) and integrated
general practice unit. II. Labour and delivery management and
neonatal outcome. British Journal of Obstetrics & Gynaecology 90:
123–8

The OPAL study
©NCCSDO 2007 178
Langworth, L., Ratcliffe, J. and Boulton, M. 2001. Investigating
women’s preferences for intrapartum care: home versus hospital
births. Health Social Care Community 9: 404–13
Lauzon, L. and Hodnett, E. 1998. Antenatal education for self-
diagnosis of the onset of active labour at term. Cochrane
Database of Systematic Reviews 4: CD000935
Mahlmeister, L. and van Mullem, C. 2000. The process of triage in
perinatal settings: clinical and legal issues. Journal of Perinatal
Neonatal Nursing 13: 13–30
Martin, C.R. and Jomeen, J. 2004. The impact of clinical management
type on maternal locus of control in pregnant women with pre-
labour rupture of membranes at term. Health Psychology Update
13: 3–13
McNiven, P., Williams, J., Hodnett, E., Kaufman, K. and Hannah, M.
1998. An early labor assessment program: a randomised
controlled trial. Birth 25: 5–10
Munro, J., Nicholl, J., O'Cathain, A., Knowles, E. and Morgan, A. 1998.
Evaluation of NHS Direct First Wave Sites: First Interim Report of
the Phase 1 Research. Sheffield: MCRU, University of Sheffield
NHS Employers. 2005. Maternity Support Workers: Enhancing the
Work of the Maternity Team. https://www.nhsemployers.org
Nursing and Midwifery Council. 2004. Midwives Rules and Standards.
London: Nursing and Midwifery Council
Quinn, M., Murphy, A. and Gallagher, J. 1981. Spurious labour: does it
matter? Australia and New Zealand Journal of Obstetrics and
Gynaecology 21: 167–9
Royal College of Midwives. 2006. Consultation Draft: Safer Childbirth:
Minimum Standards for Service Provision and Care in Labour.
www.rcm.org.uk/views/docs/%20report.doc
Royal College of Obstetricians and Gynaecologists and Royal College of
Midwives. 1999. Towards Safer Childbirth. London: Royal College
of Obstetricians and Gynaecologists
Royal College of Obstetricians and Gynaecologists. 2001a. Induction of
Labour. London: Royal College of Obstetricians and
Gynaecologists
Royal College of Obstetricians and Gynaecologists. 2001b. The Use of
Electronic Fetal Monitoring: The Use and Interpretation of
Cardiotocography in Intrapartum Fetal Surveillance. London:
Royal College of Obstetricians and Gynaecologists
Royal College of Obstetrics and Gynaecologists. 2004. Confidential
Enquiry into Maternal and Child Health, Why Mothers Die 2000-
2002. London: Royal College of Obstetricians and Gynaecologists
Ryding, E.L. 1993. Investigation of 33 women who demanded a
caesarean section for personal reasons. Acta Obstetrica et
Gynaecologica Scandinavica 72: 280–5

The OPAL study
©NCCSDO 2007 179
Sandall, J., Davies, J. and Warwick, C. 2001. Evaluation of the Albany
Midwifery Practice, Final Report March 2001. London: Kings
College
Schauberger, C.W. 1986. False labour. Obstetrics and Gynaecology
68: 770–2
Simkin, P. 1991. Just another day in a woman’s life? Part 1. Women’s
long-term perceptions of their first birth experience. Birth 18:
203–10
Singh, D. and Newburn, M. 2006. Feathering the nest: what women
want from the birth environment. Midwives 9: 266–9
Smith, L. 2001. Development of a multidimensional labour satisfaction
questionnaire: dimensions, validity, and internal reliability.
Quality in Health Care 10: 17–22
Smith, L. and Smith, C. 2005. UK childbirth delivery options in 2001-
2002: alternatives to consultant unit booking and delivery. British
Journal of General Practice 55: 292–7
Smith, L.F. and Smith, C. 2006. Childbirth delivery options in the UK
in 2001-2: midwife care and governance. British Journal of
Midwifery 14(4): 224–8
Sookhoo, M. and Biott, C. 2002. Learning at work: midwives judging
progress in labour. Learning in Health and Social Care 1: 75–85
Spiby, H., Henderson, B., Slade, P., Escott, D. and Fraser, R. 1999.
Strategies for coping with labour: does antenatal education
translate into practice? Journal of Advanced Nursing 29: 388–94
Statham, H., Solomou, W. and Green, J.M. 2001. When a Baby has an
Abnormality: a Study of Parents' Experiences. Part 1 of the Final
Report to the NHS Executive (Mother and Child Health Initiative).
Cambridge: Centre for Family Research, University of Cambridge
Summers, P., Biswas, M.J., Malveaux, M., Moore, L., Ingraham, C. and
O'Quinn, A. 1991. Pregnancy outcome in patients with repeat
visits to the labor observation area near term. Southern Medical
Journal 84: 436–8
The Information Centre. 2006. Community Health Statistics. NHS
Maternity Statistics, England: 2004–2005. The Information Centre
Vande Vusse, L. 1999. Decision making in analyses of women's birth
stories. Birth 26: 43–52
van Teijlingen, E.R., Hundley, V., Rennie, A.-M., Graham, W. and
Fitzmaurice, A. 2003. Maternity satisfaction studies and their
limitations: "what is, must still be best". Birth 30: 75–82
Walker, J. 2000. Women's experiences of transfer from a midwife-led
to a consultant-led maternity unit in the UK during late pregnancy
and labor. Journal of Midwifery and Women's Health 45: 161–8
Webb, S. 2004. Is there a role for triage in midwifery? MIDIRS
Midwifery Digest 14: 493–5

The OPAL study
©NCCSDO 2007 180
Wiklund, I., Matthiesen, A.-S., Klang, B. and Ransjo-Arvidson, A.-B.
2002. A comparative study in Stockholm, Sweden of labour
outcome and women's perceptions of being referred in labour.
Midwifery 18: 193–9
Wilkinson, M. and McPherson, S. 2001. NHS Direct Online and the
information divide. He@lth Information on the Internet 22: 8–10

Disclaimer This report presents independent research commissioned by the National Institute for Health Research (NIHR). The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the NIHR SDO programme or the Department of Health. The views and opinions expressed by the interviewees in this publication are those of the interviewees and do not necessarily reflect those of the authors, those of the NHS, the NIHR, the NIHR SDO programme or the Department of Health Addendum This document was published by the National Coordinating Centre for the Service Delivery and Organisation (NCCSDO) research programme, managed by the London School of Hygiene & Tropical Medicine. The management of the Service Delivery and Organisation (SDO) programme has now transferred to the National Institute for Health Research Evaluations, Trials and Studies Coordinating Centre (NETSCC) based at the University of Southampton. Prior to April 2009, NETSCC had no involvement in the commissioning or production of this document and therefore we may not be able to comment on the background or technical detail of this document. Should you have any queries please contact [email protected].