lao-belgian cooperation for health - ningapi.ning.com/files/gazk*efh1hkr0n3qeena54i9it2hwl7... ·...
TRANSCRIPT

Lao-Belgian Cooperation for HealthProject
Support to Health Sector Reform in the Provinces of Vientiane and Savannakhet
Developing Effective Integrated District Health Systems in
Lao PDR
Experience from Lao-Belgian Health Project Interventions 2004 – 2009
Ministry of HealthProvincial Health Office Savannakhet
Provincial Health Office Vientiane ProvinceProject Coordinating Unit, MoH
February 2009

Contents
Foreword 1
Acknowledgements 2
Abbreviations & currencies 3
Vision for provision of quality care: primary health care and local health system 4
Guiding and coaching reforms for local health system development 12
Technical elements of the local health system 18
Referral system 18
Learning and training for quality 20
Supervision 24
Performance-based subsidies and audit 26
Drug management and revolving fund 27
Monitoring and health information management 28
Financial management 29
Health equity fund 31
Overview of costs 33
Investments 33
Recurrent costs 35
Summary of costs 37
Summary: main results, lessons and challenges 39
Characteristics of Vang Vieng and Xepone Health Districts 42
References 43
1
The Local Health System (LHS) is considered by WHO (Harare, 1987) as the conceptual model to deliver Primary Health Care (Alma Ata, 1978): an integrated functional two-tier health system organization composed of first-line care health centers and a second-line referral hospital, managed by a LHS management team. This was once more underscored in the World Health Report 2008, “PHC Now More Than Ever”. The Lao Primary Health Care Policy (MoH, 2000) is fully in line, aiming at the develop-ment of health districts.
Since June 2004, the Lao-Belgian Health Project (LBHP) has been supporting the Ministry of Health (MoH) in implementing the model, according to local needs and capacities, as well as in documenting the process: potentialities, conditions and strategies for reforms, costing analysis, achievements. A referral inter-district hospital and Integrated Community Health Centers were developed in Xepone District (province of Savannakhet), and Vang Vieng District (province of Vientiane). Management teams were reinforced.
Besides hard-ware investment and technical training, the project invested heavily in improving and modernizing the management procedures of the health system. This led to important changes in attitudes and practices of staff, which in turn led to improved working conditions and output of the health services. Those changes were obtained by progressive intro-duction of innovative technical, managerial and financing methods. Many of the changes were progressively co-developed between health facility staff and project technical assistants, in agreement with provincial health offices and the MoH.
The Ministry of Health with Belgian Technical Cooperation support hosted an International Conference on District Health Systems in SE Asia (Vientiane, 2006). On this occasion, LBHP published a first brochure describing the underlying principles of “Local Health Systems” and showing the first results of their implementation in Lao PDR.
The 2008 Midterm Review of the Lao 5-year Health Sector Development Plan 2006-10 acknowledges that “Xepone and Vang-Vieng are becoming the model districts as planning and budgeting units”.
In this new brochure, the LBHP wants to share the lessons learned while developing this model, wrapped up in a tool kit showing what may be the reform processes and resources necessary in order to develop well performing public health service systems in the Lao district context. Field visits in the districts supported by the Project may make the message of the brochure more explicit.
While leaving this testimony of the work of nearly five years of very rewarding Lao-Belgian cooperation for health, we hope that our work will be useful for health officials in Laos, as an analytical framework to assess the current functioning of local health systems and plan for their further development.
Dr Frank HaegemanInternational ProjectCoordinator
Dr Danglam MahayoNational ProjectCoordinator
FOREWORD
1
The Local Health System (LHS) is considered by WHO (Harare, 1987) as the conceptual model to deliver Primary Health Care (Alma Ata, 1978): an integrated functional two-tier health system organization composed of first-line care health centers and a second-line referral hospital, managed by a LHS management team. This was once more underscored in the World Health Report 2008, “PHC Now More Than Ever”. The Lao Primary Health Care Policy (MoH, 2000) is fully in line, aiming at the develop-ment of health districts.
Since June 2004, the Lao-Belgian Health Project (LBHP) has been supporting the Ministry of Health (MoH) in implementing the model, according to local needs and capacities, as well as in documenting the process: potentialities, conditions and strategies for reforms, costing analysis, achievements. A referral inter-district hospital and Integrated Community Health Centers were developed in Xepone District (province of Savannakhet), and Vang Vieng District (province of Vientiane). Management teams were reinforced.
Besides hard-ware investment and technical training, the project invested heavily in improving and modernizing the management procedures of the health system. This led to important changes in attitudes and practices of staff, which in turn led to improved working conditions and output of the health services. Those changes were obtained by progressive intro-duction of innovative technical, managerial and financing methods. Many of the changes were progressively co-developed between health facility staff and project technical assistants, in agreement with provincial health offices and the MoH.
The Ministry of Health with Belgian Technical Cooperation support hosted an International Conference on District Health Systems in SE Asia (Vientiane, 2006). On this occasion, LBHP published a first brochure describing the underlying principles of “Local Health Systems” and showing the first results of their implementation in Lao PDR.
The 2008 Midterm Review of the Lao 5-year Health Sector Development Plan 2006-10 acknowledges that “Xepone and Vang-Vieng are becoming the model districts as planning and budgeting units”.
In this new brochure, the LBHP wants to share the lessons learned while developing this model, wrapped up in a tool kit showing what may be the reform processes and resources necessary in order to develop well performing public health service systems in the Lao district context. Field visits in the districts supported by the Project may make the message of the brochure more explicit.
While leaving this testimony of the work of nearly five years of very rewarding Lao-Belgian cooperation for health, we hope that our work will be useful for health officials in Laos, as an analytical framework to assess the current functioning of local health systems and plan for their further development.
Dr Frank HaegemanInternational ProjectCoordinator
Dr Danglam MahayoNational ProjectCoordinator
FOREWORD

2
REGIONAL SEMINAR ON DISTRICT HEALTH SYSTEMS IN S.E. - ASIA, VIENTIANE, OCTOBER 2006.
The process described in this brochure is the result of a long-term collaborative effort between health staff in both provinces together with central hospitals, ministry of health and the project team.
We acknowledge the collaboration of following persons most directly involved:
Vientiane Province: Dr Soukphathay Sopraseuth - director PHO, Dr Khamphoun Phompanya - coordinator PMU, Dr Kham-souk Souvannasy - head health financing unit PHO, Dr Virack Vidamaly - director provincial hospital, Dr Fongsalath Southam-mavong - deputy-director provincial hospital
Vang Vieng District: Dr Singthong Noula - director DHO, Dr Phetsamone Boulommavong - director district hospital, Dr.Viengkham Sinavong - head administrative office DHO, Thanouthong Chanthalangsy - deputy-director DHO
Savannakhet Province: Dr Kinta Bayavong - former director PHO, Dr Panom Phongmany - director PHO, Dr Somdy Souriya - deputy-director PHO, Dr Kaysone Mychaleun - coordinator PMU, Prof Dr Phokham Prasithideth, - director provincial hospi-tal, Dr Bounmai - deputy-director provincial hospital
Xepone District: Dr Sengchanh Koumkiengmaniseng - director DHO, Dr Khamtoun Ounliengvongsack, - director district hospital, Dr Khounmy Thongsihathep - deputy-director hospital, MA Kanha Phanthavong - deputy-director hospital
Central hospitals Vientiane: Surgeon: Dr Phetdavanh Sonnasin Gyne-obstetricians: Prof Assistant Dr Bouavanh Sene-sathid, Dr Sivanxay Chanthavongsack, Dr Boun Ouan Chansina, Dr Chaimua Suako, Dr Phoutthalad Panyasid Paediatricians:Prof Assistant Dr Bounleua Oudavong, Dr Bounlab Chittri, Dr Somchai Vinlamay Anaesthetists: Dr Aphone Sisouraj, Dr.Traichit Chanthasiri, Dr.Phouvang Thonnareth, Dr.Sisongkham Phanmany, Dr Ounkham Phanthaly, Dr Vanhpheng Nora sing Laboratory specialist: Dr Vimonh Soukkhaseum Cardiologist: Dr Pheng Sackda Psychiatrist: Dr Sisouk Vongphachanh Internists: Dr Douangdalay Milamay, Dr Simmaly Fongmany Dentist: Dr Boungnong Sidaphone X-ray technician: Mr Nousad Xaysombad
Project team: Dr Bounsavad Savattry, Dr Bounsab Voradeth, Mr Bounlam Souvannasab, Mr Virasak Phetpasak, Ms Sophavanh Thitsy, Ms Phonethip Chayavong, Ms Kindavanh Phoutsavath, Ms Nongnath Phimmeuang, Ms Phonesavanh Manipoun, Mr Viengsavanh Sourinphoumy, Dr Marlon Garcia-Lopez, Dr Danglam Mahayo, Dr Frank Haegeman
External consultants: Prof Dr Jean Macq, Dr Patrick Martiny, School Public Health University of Brussels;Ms Oumakong Sithong, Ms Prayoon Kamkhaengkwa, Mr Sawaeng Panyadee, Thai nurse-trainers; Mr Jean-Marc Thomé, health economist
All members of the Project Steering Committee, the Governors of Vientiane and Savannakhet provinces and of Vang Vieng and Xepone districts, all members of PHO of Vientiane and Savannakhet provinces, all members of DHO of districts of Vang Vieng, Phoun, Hom, Xaysomboune, Xepone and Nong.
The project team especially wants to acknowledge the continuous interest and support received by the highest authorities of the Ministry of Health.
ACKNOWLEDGEMENTS
3
ANC Ante-Natal Care
AT Anti-Tetanus vaccination
BCG Bacille Calmette Guérin (TB vaccine)
BTC Belgian Technical Cooperation
CBHI Community Based Health Insurance
CQI Continuous Quality Improvement
C/S Caesarean Section
DH District Hospital
DHMT District Health Management Team
DHO District Health Office
DTC Drug Therapeutic Committee
DTP Diphtheria -Tetanus-Pertussis vaccine
EPI Extended Program Immunization
FLHS First-Line Health Service
FP Family Planning
GOL Government of Laos
GVT Government
HA Hospital Accreditation
HC Health Center
HEF Health Equity Fund
HIV- Human Immunodeficiency Virus-
AIDS Acquired Immunodeficiency Syndrome
HMIS Health Management Information System
HZ Health Zone
IBN Impregnation of Bed Nets (program)
ICHC Integrated Community Health Center / Care
IDH Inter-District Hospital
IDRH Inter-District Referral Hospital
IEC Information, Education, Communication
IMCI Integrated Management of Childhood Illnesses
IPD In-Patient Department
IUD Intra-Uterine Device (contraceptive)
JICA Japanese International Cooperation Agency
KAP Knowledge, Attitude, Practice
LBHP Lao-Belgian Health Project
LHS Local Health System
LHS-MT Local Health System Management Team
MCH Mother and Child Health
MoH Ministry of Health
MR Minimal Requirements
NGO Non-governmental Organization
OPD Out-patient Department
PCU Project Coordinating Unit
PDCA Plan-Do-Check-Act
PHC Primary Health Care
PHD Provincial Health Department
PHO Provincial Health Office
PMU Project Management Unit
PNC Post-Natal Care
QA Quality Assurance
QI Quality Improvement
RDF Revolving Drug Fund
RH Referral Hospital
SASS State Authority Social Security
SOP Standard Operating Procedures
SSO Social Security Organization
SVK Savannakhet
SWOT Strength-Weakness-Opportunity-Threat
TA Technical Assistance
TB Tuberculosis
VTE Vientiane
VV Vang Vieng
WHO World Health Organization
5S Five “S” (organizational term)
$ 1 US = 8,500 kip (Lao currency) - February 2009
Abbreviations & currencies
4
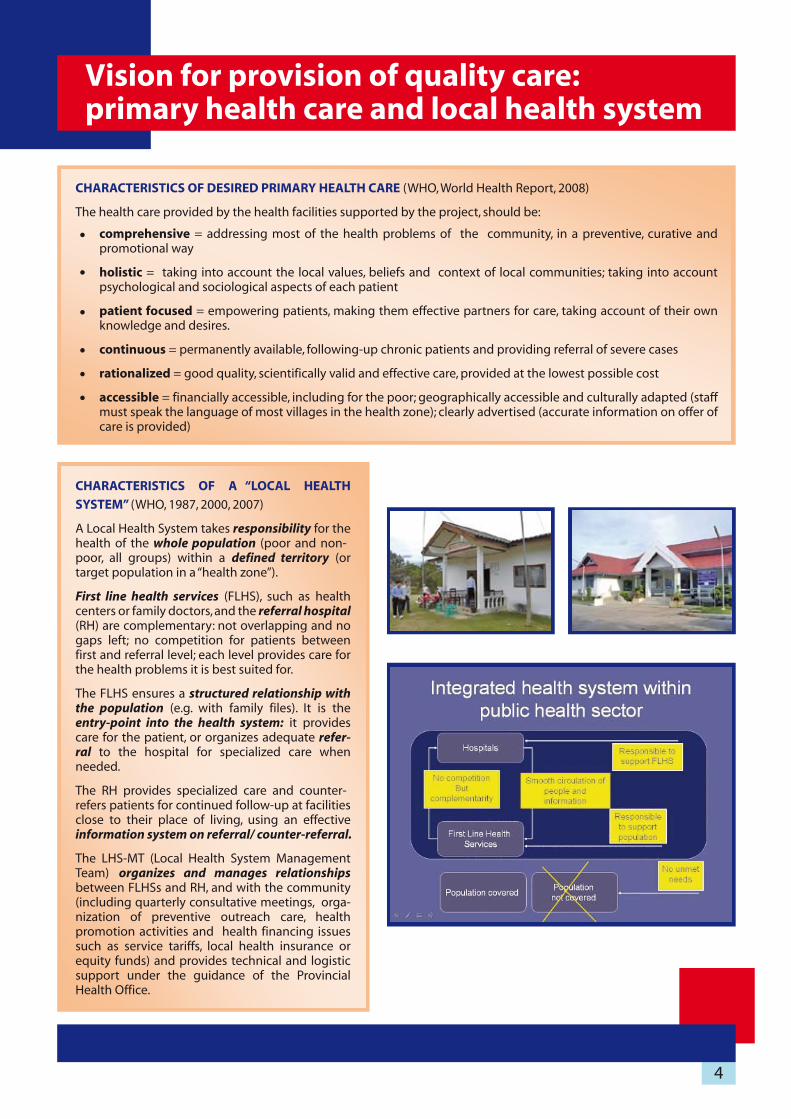
CHARACTERISTICS OF A “LOCAL HEALTH
SYSTEM” (WHO, 1987, 2000, 2007)
A Local Health System takes responsibility for the health of the whole population (poor and non-poor, all groups) within a defined territory (or target population in a “health zone”).
First line health services (FLHS), such as health centers or family doctors, and the referral hospital(RH) are complementary: not overlapping and no gaps left; no competition for patients between first and referral level; each level provides care for the health problems it is best suited for.
The FLHS ensures a structured relationship with the population (e.g. with family files). It is the entry-point into the health system: it provides care for the patient, or organizes adequate refer-ral to the hospital for specialized care when needed.
The RH provides specialized care and counter-refers patients for continued follow-up at facilities close to their place of living, using an effective information system on referral/ counter-referral.
The LHS-MT (Local Health System Management Team) organizes and manages relationshipsbetween FLHSs and RH, and with the community (including quarterly consultative meetings, orga-nization of preventive outreach care, health promotion activities and health financing issues such as service tariffs, local health insurance or equity funds) and provides technical and logistic support under the guidance of the Provincial Health Office.
CHARACTERISTICS OF DESIRED PRIMARY HEALTH CARE (WHO, World Health Report, 2008)
The health care provided by the health facilities supported by the project, should be:
comprehensive = addressing most of the health problems of the community, in a preventive, curative and promotional way
holistic = taking into account the local values, beliefs and context of local communities; taking into account psychological and sociological aspects of each patient
patient focused = empowering patients, making them effective partners for care, taking account of their own knowledge and desires.
continuous = permanently available, following-up chronic patients and providing referral of severe cases
rationalized = good quality, scientifically valid and effective care, provided at the lowest possible cost
accessible = financially accessible, including for the poor; geographically accessible and culturally adapted (staff must speak the language of most villages in the health zone); clearly advertised (accurate information on offer of care is provided)
Vision for provision of quality care: primary health care and local health system

5
First level of care: Integrated Community Health Centers (ICHC)
Health zone committee quarterly planning meetings at HC level
Composition Functions Working Procedures
HC staff
1 or 2 representatives from each village of the target zone of the HCRepresentative of the DHORepresentative of “Village Groups” (or of District Governor)
Sometimes: representative of the PHO or from the project
Discuss health situation and functioning of health center (e.g. tariffs, available services)
Present activity report of HC to population
Agree on EPI outreach calendar to each village
Quarterly meeting of 1/2 day in HC or local meeting room (e.g. in temple)
Presentation of reports
Discussion
Reimbursement transportation costs for villagers and collective meal offered
INTER-VILLAGE HEALTH COMMITTEE MEETING
MOTHER ATTENDS MCH CLINIC IN ICHCIn Vang Vieng and Xepone, the ICHC’s provide an integrated first-line
essential health care package to the population of their “health zone” (based on list of villages), using family files:
Those functions and tasks correspond to decree N° 1274/MOH of 5 Oct 2006 on health center organization
24/24 hr, 7/7 day service for treatment of most prevalent condi-tions: availability of essential drugs, small surgery, IMCI, safe delivery care or when necessary referral to hospitalpreventive care and health promotion: vaccinations (EPI), health education (IEC), mother and child health care (MCH) - ANC, birth spacing, PNC, Under-5 yrs-clinicquarterly outreach activities to each village for integrated EPI-MCH services and health promotion (mobile team / home visits)quarterly meeting of a “health zone committee” with representa-tives of each village of the zone to discuss health problems and agree on the vaccination outreach calendarsupervision and support to village health workers in the health zone, where they exist (including organizing bed net impregnation-dipping with insecticides)

Second-level of care: inter-district referral hospitals
The Xepone hospital serves 4 administrative districts with a total population of 150,000
In the Lao health system, Xepone and Vang Vieng hospitals are district hospitals Type A (with surgery).
They act as inter-district referral hospitals since they serve several administrative districts. Health Centers and district hospitals type B (in smaller districts, without surgery) refer the patients who need second line care:
24/24 hr emergency care for surgery, essential obstetric and newborn care, and medical emergenciesreferral care for all health problems that cannot be solved by the HC: second level diagnostic (laboratory, X-ray, ultrasound) and curative techniques; this includes care of communicable and non-communicable diseases, chronic or life style diseases, such as diabetes, hypertension, asthma, psychiatric problemsThe hospital comprises out-patient consulting wards, laboratory and imaging rooms, dentist room, delivery room and operating theatre, maternity and hospitalization wards, pharmacy, administration-procurement and logistic services (laundry, cleaning and maintenance, transportation)
The hospital also takes care of the nearby population for first-level care (it functions as a health center for its own health zone).
The hospital provides technical support to the health centers and hospitals type B in its “inter-district area”: training, provision of guidelines and supervision.
Specific management tools are used to manage the hospital in a transparent and accountable way and to promote quality of the organization and care for the patients through rational and effective team work. Clinical and managerial procedures, guidelines and protocols are being introduced or adapted, and their use monitored by the team, under the authority of the hospital director.
Composition Functions Working Procedures
District hospital board
Director of hospital, chief of adminis-tration unit, chief pharmacist, chief nurse of DH, accountant, chief of lab, chief of dental clinic, chief of MCH, PHO member, and temporarily a project technical assistant.
Propose and decide on staffing issues, continuous education, resources management, referral system, supervision of HC, monitor-ing, collating and disseminating health data and hospital statistics
Monthly meeting
Identification of problems
Team decisions.
Follow up implementation of decisions made
Composition Functions Working Procedures
Director of hospital, clinicians, nurses, pharmacists, accountant, administra-tive staff.
Occasionally other physicians from central hospital and project technical assistants, while present for coaching or training.
Report the overall situation of the previous day about admissions, patient’s conditions, nursing care, but also on accounting, RDF, admin-istration.Identify the opportunity for improvement. Followed by review of the patients admitted at night by doctors on duty.
Daily 8:00 – 8:30 hr
Discussions, immediate solutions or prepare the case for case confer-ences and preparation for the lectures.
Multidisciplinary team coordination.
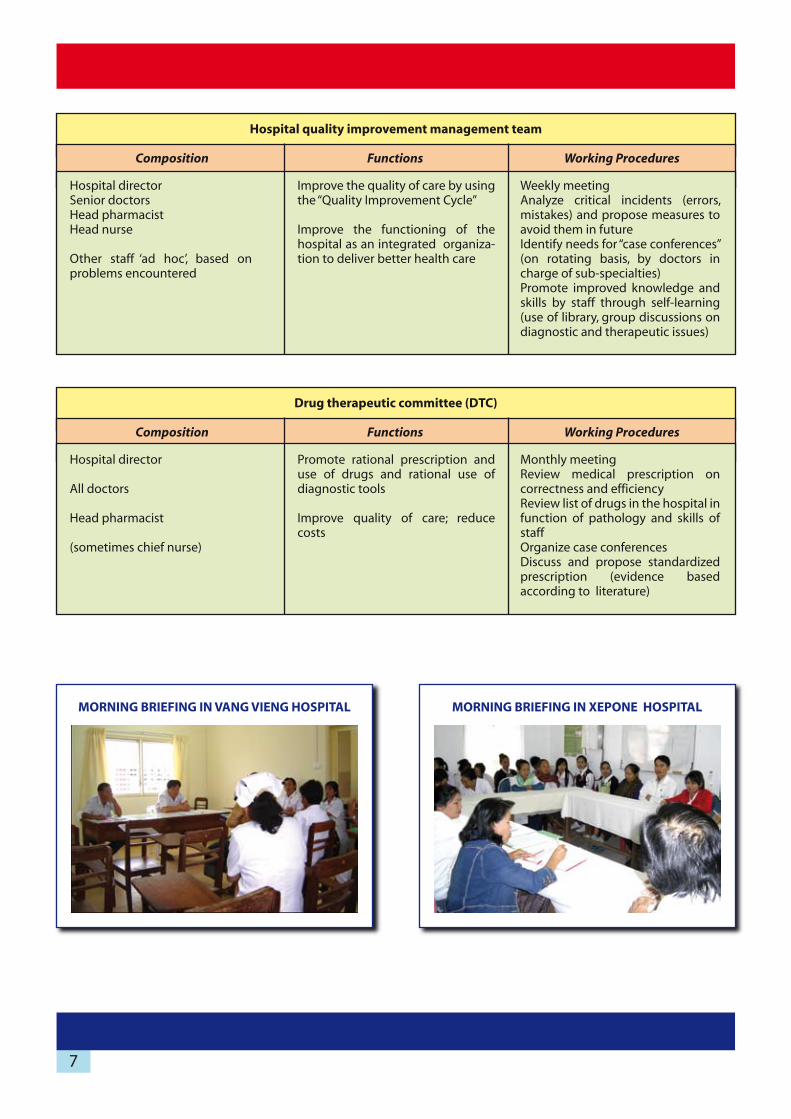
Hospital daily morning briefing (report) meeting
6
Composition Functions Working Procedures
Hospital directorSenior doctorsHead pharmacistHead nurse
Other staff ‘ad hoc’, based on problems encountered
Improve the quality of care by using the “Quality Improvement Cycle”
Improve the functioning of the hospital as an integrated organiza-tion to deliver better health care
Weekly meetingAnalyze critical incidents (errors, mistakes) and propose measures to avoid them in futureIdentify needs for “case conferences” (on rotating basis, by doctors in charge of sub-specialties)Promote improved knowledge and skills by staff through self-learning (use of library, group discussions on diagnostic and therapeutic issues)
Hospital quality improvement management team
Functions Working Procedures
Hospital director
All doctors
Head pharmacist
(sometimes chief nurse)
Promote rational prescription and use of drugs and rational use of diagnostic tools
Improve quality of care; reduce costs
Monthly meetingReview medical prescription on correctness and efficiencyReview list of drugs in the hospital in function of pathology and skills of staffOrganize case conferencesDiscuss and propose standardized prescription (evidence based according to literature)
Drug therapeutic committee (DTC)
MORNING BRIEFING IN VANG VIENG HOSPITAL MORNING BRIEFING IN XEPONE HOSPITAL
7
Composition

The District Health Management Team (DHMT) as local health system managers
The LHS team organizes, coordinates, and integrates techni-cally and administratively the 1st and 2nd level health services and the health promotion team by providing guidelines, supervision, management of human resources and drug supply.
The team works together with District Authorities, mass organizations and communities to consult, inform, and promote inter-sector work.
The team uses the health management information system (HMIS) to monitor performance indicators and evaluate health activities for decision making, budgeting and planning.
The team (co-)manages health financing schemes: Community Based Health Insurance (CBHI), Civil Servant Insurance (SASS), contracting with hospital & ICHC, Health Equity Funds for free care for the poorest people.
The team is composed of: representative of Provincial Health Office, district health officers, director of the hospital and his senior staff, some chiefs of health centers, chiefs of health promotion programs (such as EPI, MCH, and malaria control), chief of administration office.The team members attend periodic management meetings, which are publicly announced; transparency is ensured, minutes are available.
Decisions are collegial under the authority of the DHO director; tasks are clearly delegated to responsible staff.There is a clear attempt at integration of « vertical responsibilities » for health programs, into « horizontal responsibili-ties » for health services or teams.
Composition Functions Working Procedures
DHO director, DHO officers
Hospital physicians
Monitor staff’s performance, provide supportive super-vision and coaching
Solve problems on the spot, or report them to DHMT for structural solution at district level
Monthly monitoring and supervision for 1 or 2 days in each HC
Associate the specific supervisor for the specific issues such as IMCI, MCH, nursing care, DRF
District supervision team
Composition Functions Working Procedures
DHOHospital senior staffAdministration unitPHO memberAll HC chiefs(Project technical assistant)
Review activities, analyze HMIS (reporting data by each HC and by hospital)Hold quarterly planning activities for whole district (EPI, IBN, supervisions)Present budgets (from government and projects) for each facility (transparency)Report on finances of each facilityDiscuss health mattersInform, teach, introduce new procedures in the district
Quarterly meeting of 2 to 3 daysPresentation of reports by chief of each HC and units of DHO
Peer-discussion
Costs for transportation and per diem are paid
Quarterly planning meetings at (inter)-district level
8
DHMT MEETING IN XEPONE DISTRICT
QUARTERLY INTER-DISTRICT MEETING IN XEPONE
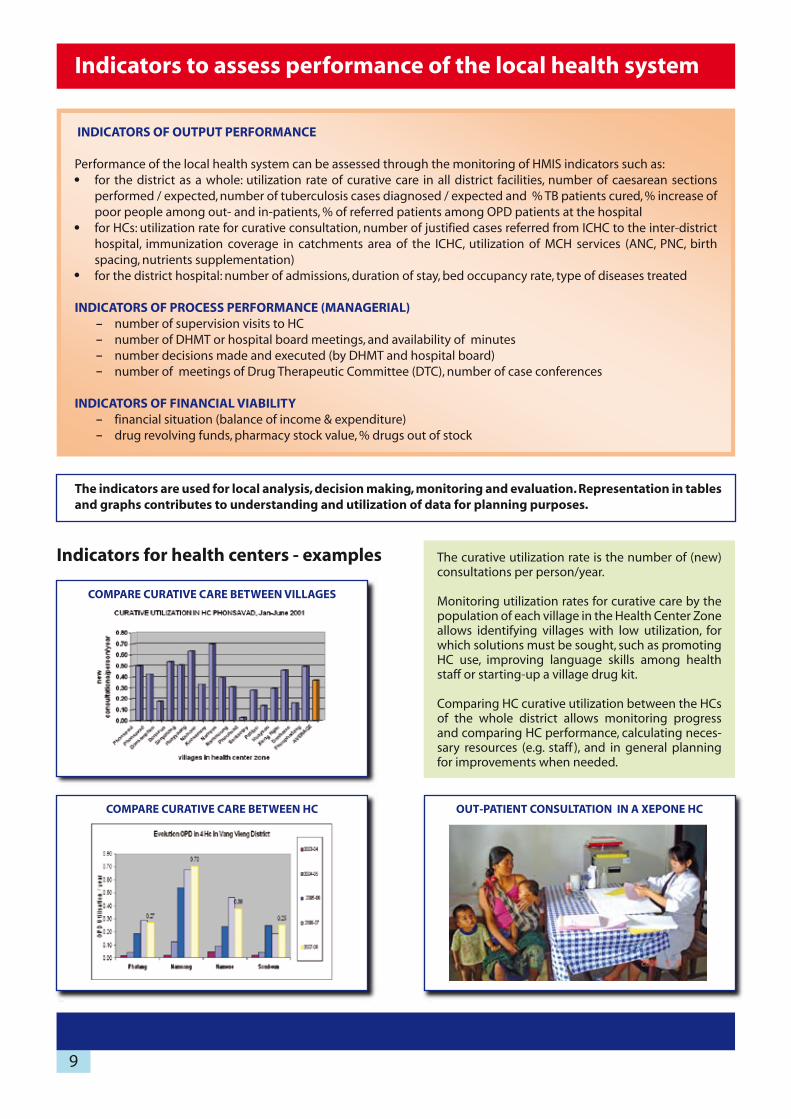
COMPARE CURATIVE CARE BETWEEN VILLAGES
COMPARE CURATIVE CARE BETWEEN HC
Indicators to assess performance of the local health system
The indicators are used for local analysis, decision making, monitoring and evaluation. Representation in tables and graphs contributes to understanding and utilization of data for planning purposes.
The curative utilization rate is the number of (new) consultations per person/year.
Monitoring utilization rates for curative care by the population of each village in the Health Center Zone allows identifying villages with low utilization, for which solutions must be sought, such as promoting HC use, improving language skills among health staff or starting-up a village drug kit.
Comparing HC curative utilization between the HCs of the whole district allows monitoring progress and comparing HC performance, calculating neces-sary resources (e.g. staff ), and in general planning for improvements when needed.
Indicators for health centers - examples
OUT-PATIENT CONSULTATION IN A XEPONE HC
INDICATORS OF OUTPUT PERFORMANCE
Performance of the local health system can be assessed through the monitoring of HMIS indicators such as:for the district as a whole: utilization rate of curative care in all district facilities, number of caesarean sections performed / expected, number of tuberculosis cases diagnosed / expected and % TB patients cured, % increase of poor people among out- and in-patients, % of referred patients among OPD patients at the hospitalfor HCs: utilization rate for curative consultation, number of justified cases referred from ICHC to the inter-district hospital, immunization coverage in catchments area of the ICHC, utilization of MCH services (ANC, PNC, birth spacing, nutrients supplementation)for the district hospital: number of admissions, duration of stay, bed occupancy rate, type of diseases treated
INDICATORS OF PROCESS PERFORMANCE (MANAGERIAL)number of supervision visits to HCnumber of DHMT or hospital board meetings, and availability of minutesnumber decisions made and executed (by DHMT and hospital board)number of meetings of Drug Therapeutic Committee (DTC), number of case conferences
INDICATORS OF FINANCIAL VIABILITYfinancial situation (balance of income & expenditure)drug revolving funds, pharmacy stock value, % drugs out of stock
9

TREND IN PREVENTIVE CARE IN HC IN XEPONE (SP)
Indicators for referral hospitals - examplesSTATISTICS OF XEPONE HOSPITAL
STATISTICS OF VANG VIENG HOSPITAL
OUTREACH VACCINATION IN XEPONE HC
10

IN XEPONE, FIRST-LINE OPD DECREASED IN THE HOSPITAL, BUT INCREASED IN THE HC
ESTIMATED AND COVERED NEED FOR CAESAREAN SECTIONS (C/S) IN TARGET AREA OF INTER-DISTRICT HOSPITAL VANG VIENG (VV) IN 2007-2008
IN VANG VIENG, CONTRACEPTIVE CARE SHIFTED FROM THE HOSPITAL TOWARDS FIRST-LINE HC
Indicators for Local Health System performance: integrated district function - examples
Indicators for inter-district hospital performance - example
Indicators for performance of DHMT- example
QUANTITATIVE PERFORMANCE OF HC SUPERVISION (NUMBERS IN 2007-08)
Xepone Vang Vieng
Planned supervisions by DHMT
Executed supervisions
Total
96 (8 HC x 12/year) 48 (4 HC x 12/year)
75
79 %
44
91 %
11

Modernizing the management of a local health system to become more effective, efficient and equitable implies a progressive change in KAP of health staff:
Knowledge: improve management skillsAttitude: improve work in team and patient-centered carePractices: respect job descriptions; be real full-time professionals
The process needs technical support (to start up, guide and coach), which consists of the following:
Identifying strengths and weaknesses, opportunities and threats (SWOT) for local health system develop-ment, based upon a vision of desired health care quality and type of health care delivery system
Building capabilities amongst health system staff, to make them take responsibility for routine activities and the development of their local health system and to communicate their experience:
Training, transmission of tools, guidelines and written instructions may be useful to improve capabilities to deal with “routine” activities that can be standardizedCoaching is more suitable to improve activities that need a high degree of human relationship and when capabilities for adaptation to change should be acquiredKnowledge management implies production and sharing of relevant information
Facilitating change and adaptation from within the system:Enhance willingness through making necessary resources and amenities available, showing that improve-ment is possible, implementing motivational strategies based on trust (cooperation, empowerment, dialogue) or control, including use of complementary performance-based financial incentivesCreate a conducive environment through brokerage (bridging between the activities of different partners in the health system), buffering (protecting the local staff from external interference) and catalyzing the changeAct at all levels of the system and for a sufficiently long duration (several years – continuously or intermit-tently): proximity and continuity of support is important to develop a necessary relationship of mutual trust through acquaintance with each other
1.
2.
3.
–
–
–
–
–
–
12
Guiding and coaching reforms for local health system development
Starting the change process
In both Xepone and Vang Vieng districts, the project found that the local health staff considered the initial situation as unsatisfactory and problematic, but that there was a willingness to improve it.
Problems identified may vary from one facility to another, but often the following shortcomings are observed in Lao health districts
Problems at health center level
Under-paid, semi-professional staff, occupied with other income generating activities, reluctant to work in HC, and often discouraged and feeling “abandoned”
Passive behavior (waiting for patients); fatalistic attitude
No or extremely low operational budget for HC functioning (except for periodic activities, such as vaccination, bed net impregnation)
Limited curative care; limited participation in EPI-vaccinations
HC is often by-passed or neglected by District
Little accountability towards population or even authorities
Problems in district hospitals
Doctors focus on private practice; high absenteeism at public work place
Low technical level; static quality situation
Individualism; networking within competing groups of staff; little accountability
Informal payments by patients are often source of conflict between underpaid staff
Equipment disappearing
Weak Drug Revolving Fund (shortage of drugs – weak accounting and stock management)
Non-transparent financial situation; chronic bankruptcy (loans to staff; payments to District Health Office)
Problems in health district management
Conflicts of interests; authoritarian decision making; arbitrary decisions because of lack of (skills to use) information (and information of poor quality)
Staff (doctor)-centered management
Non-transparent procurement and accounting procedures, mainly due to lack of skills or to ignorance
Competition between health centers and hospitals (for curative patients, for per diems to carry out vaccinations outreach)
Insufficient budget for sporadic planning, supervision and monitoring activities; DHO uses revenues from hospital for public health activities
Accountability mainly towards PHO, little towards local population
Management mainly focused on inputs, rather than on outputs or results
The following steps were taken to introduce change:
Explain to Health District core team the vision and final goal: what is quality of care, what is an integrated district health system. Seminars and some classroom teaching were organized to explain the theory and discuss its possible implementation; a brochure was produced to clarify the conceptual framework
Compose a larger « committee for change »: health staff, local district authorities and Party authorities, population representatives (village chiefs or committee, Lao Women’s Union, Lao Front for Reconstruction)
Organize study tours for this committee to already reformed facilities, or to ongoing similar experiences (e.g. visit to an existing ICHC, or to other projects such as in Xayaburi province or to a Thai “Accredited Quality district hospital”)
On return carry out a collective SWOT analysis of the current situation in order to draw a common performance assessment of the health facility and set up objectives for change
Draft a first “improvement plan” of what is feasible in current conditions
13
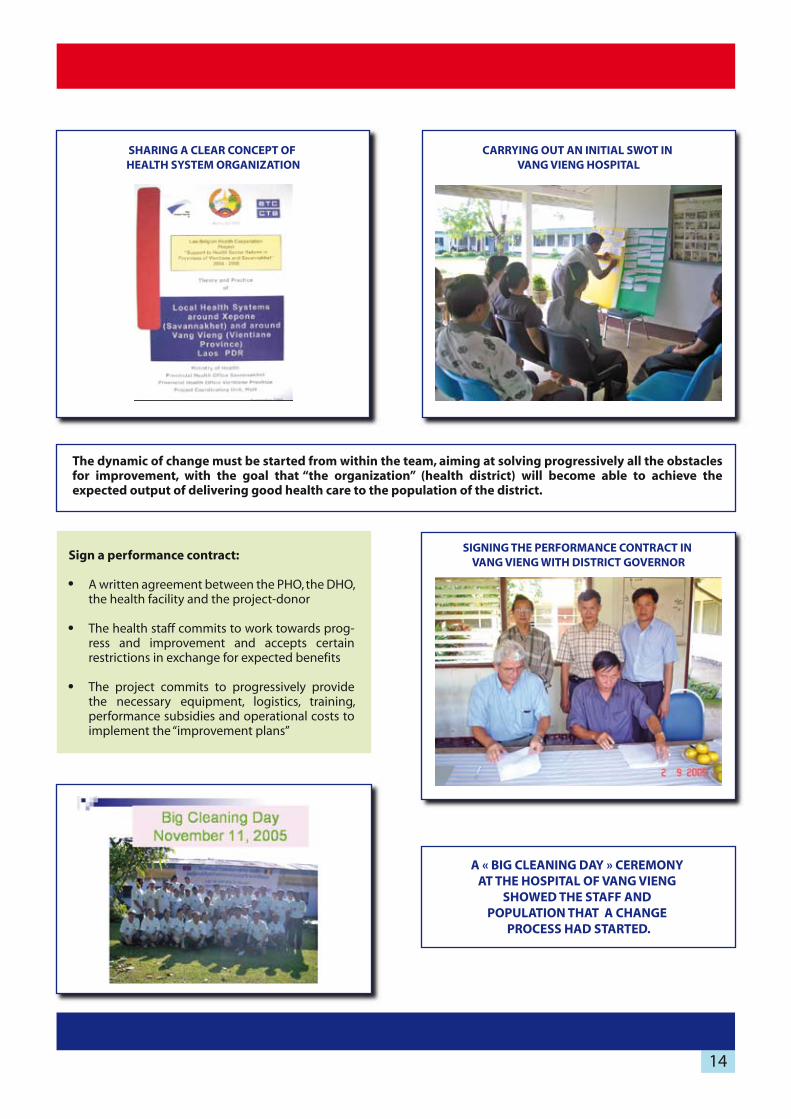
The dynamic of change must be started from within the team, aiming at solving progressively all the obstacles for improvement, with the goal that “the organization” (health district) will become able to achieve the expected output of delivering good health care to the population of the district.
CARRYING OUT AN INITIAL SWOT IN VANG VIENG HOSPITAL
SHARING A CLEAR CONCEPT OF HEALTH SYSTEM ORGANIZATION
SIGNING THE PERFORMANCE CONTRACT IN VANG VIENG WITH DISTRICT GOVERNOR
Sign a performance contract:
A written agreement between the PHO, the DHO, the health facility and the project-donor
The health staff commits to work towards prog-ress and improvement and accepts certain restrictions in exchange for expected benefits
The project commits to progressively provide the necessary equipment, logistics, training, performance subsidies and operational costs to implement the “improvement plans”
A « BIG CLEANING DAY » CEREMONY AT THE HOSPITAL OF VANG VIENG
SHOWED THE STAFF AND POPULATION THAT A CHANGE
PROCESS HAD STARTED.
14

QUARTERLY DISTRICT PLANNING IN VANG VIENG
Guiding the change process
The reform process must be continuously guided:
- Health centers are to be guided by the District Management Team- District Health Management Team is to be guided by the Provincial Health Office
This guidance focuses on achieving a dynamic for change from within the Local Health System, based upon:
Health Management Information System: used for collecting and reporting indicators on health service processes and outputs
Quarterly district review and planning meetings: with all chiefs of health centers, DHO staff, PHO representa-tive and project technical assistants. This meeting of peers in the reform process reviews and analyses data, discusses implementation problems and proposes solutions (the PDCA management cycle is used as a reference tool for analysis and decision). Information on available budgets and financial reports is shared in a transparent way
Supervision: a monthly supportive supervision aims at improving quality of the organization, skills and motiva-tion of staff by providing technical support
Audit- control: a quarterly (corrective) control, using the HMIS and qualitative indicators, monitors the perfor-mance in order to calculate financial incentive-bonus for the health facility staff
The whole process is guided by external “catalyst-persons”, and by periodically visiting technical assistants: public health experts and clinical specialists.
Remarkable synergy can be achieved through collaboration or coordination among different projects present in the health sector in a given geographical area: in Vientiane province, such a relationship between JICA (Kidsmile project), Luxembourg-Development (Health in Vientiane Province project) and BTC reinforced the message and support for change and quality improvement at all levels, under the authority and guidance of the PHO.
All must support the change process while adopting a similar vision and providing advice but also participating hands-on in clinical or management work: teaching by doing.
Experts from University Schools of Public Health can provide complementary international public health experience and knowledge, and help the PHO, DHO and project staff to reflect on the ongoing experience (monitor, review, analyze, and make new planning) and document the process. The LBHP receives such support from the Free University of Brussels, Belgium.
15

Coaching by external technical support
The tasks of technical assistants (Lao and foreign) are largely performed through coaching:- explain the concepts and provide advocacy- empower, while endorsing some (administrative and moral) responsibilities- provide scientific guidance, training and follow-up
The following table summarizes this technical support provided in the LBHP:
Coach Object ofsupport
Counterparts - targets
Possible institutionalization after
the end of the project
Project public health Technical Assistants
(Lao & international)
PHO and DHO officials
Hospital director
- planning & budgeting- quality improvement cycle- guide reform- control when needed- help draft human resource plans (work shifts, job descriptions)- supervise reporting and HMIS
- PHO- Other projects
- National Quality / hospital accreditation Unit
Nurse-trainers (Thai) Chief nurse of hospitalHospital director
HC nurses
- install nursing care quality in the hospital- 5 S program- continuous training- develop rules and procedures, e.g. on instrument inventory- supervise nursing care in HC
Nursing schools
Nursing accreditation unit
Insurance organizations
(SSO, SASS, CBHI, HEF)
Project accountant-financial trainer-advisors
Administration Unit of DHO & district hospitals
- teach computer, Excel- help in accounting- help budget planning- help reporting- help procurement
Provincial Financial-Audit Unit
RDF managers of PHO
Doctors specialists from provincial / central hospitals
Hospital doctorsprovide periodic on-the-job-training following training of staff in provincial or central hospital
Supervision of district hospitals by provincial or central hospitals
PHO project managers Guide the districtsCoordinate with PHOProvide inter-district coordination
- function in the PHO in their own technical field- implement the project
Continue
External support by School Public Health of University of Brussels
Project teamPHO teamsDept Community Medicine, University Health Sciences
Scientific-technical coaching, based on local situation (field visits) and international public health expertise
National institute of Public Health
University Health Sciences
ACCREDITATION TRAINING IN KHON KAEN UNIVERSITY, THAILAND
16

Introducing change proves to be a process of collective learning, organized team building and development and respect of rules, procedures and regulations.
A change process is often stressful for staff, inducing uncertainty, even fear and sometimes resistance: leaders fear losing power and income from informal payments, other staff fear receiving much more work and losing time for other income making activities, many staff are skeptical at the beginning (don’t believe in success), but during the process all gain in prestige, medical technical skills, monthly income and job satisfaction.
Change can be summarized as follows, comparing the situation before and after the reform process
Outcome of guiding and coaching
Before After
Individualism, focus on income generat-ing activities (private practice), passive function (waiting for instructions and for patients)
Increased professionalism, teamwork, pro-active focus on health care delivery, increased salary
Limited curative utilization and preven-tive coverage, low technical level
Integrated care, curative and preventive; higher utilization of HC and hospital; improved technical level and quality of care
Input- and staff-centered; competition between levels; arbitrary decisions
Output- and patient-centered; comple-mentarities between levels; informed decision making
Low budgets, non-transparent financial management, informal payments; unclear procurement rules
Increased budgets and cost-recovery; official user fees; transparent manage-ment for accounting, expenditures, incentives and procurement
Staff
Service delivery
Management of the health system
Financial management
DISCUSSING NURSING CARE IMPROVEMENT IN VANG VIENG HOSPITAL
WORKSHOP IN XEPONE HOSPITAL
17

Technical elements of the local health system
Referral system
The referral system manages the “pathway” of patients and related information through the different levels of the whole district health system in order to facilitate access of patients to hospital care when needed and counter-referral to health centers for follow-up. It therefore involves transportation, communication and technical skills at each level to take care of the patient in an adequate way. In the Lao context, the first-line service should be a “gate opener”: health centers advice patients to go to the hospital when needed (e.g. if need for a caesarean section), facilitate transportation (logistically or financially) and contact the hospital to improve reception of the patient on arrival.The interaction between the two levels needs therefore to be organized, both technically and financially. The challenge is to reduce both unnecessary referrals (overuse of the hospital) and missed or delayed necessary referrals (under use of the hospital) due to health center staff practice or patient behavior. Three particular delays must be avoided:
The first delay is at the village/family level where the patient and/or family delay seeking treatment at the health center, for various reasons.
The second delay is due to difficulties in reaching appropriate care i.e. lack of transportation, lack of funds for transport, lack of communication.
The third delay is due to lack of appropriate care at the health care facility which can be due to lack of qualified staff, equipment or good organization of the facility.
The referral chain can be presented as follows:
Local health systems must develop their own practical implementation procedures in the field, based on the existing national policy guidelines (see box Lao policies on next page).Each district team develops a local set of regulations ( “hand book” ) taking into account the local level of technical skills, cultural aspects, transportation facilities, the appropriate hospital to which refer different types of pathology and financial conditions of patients.
18
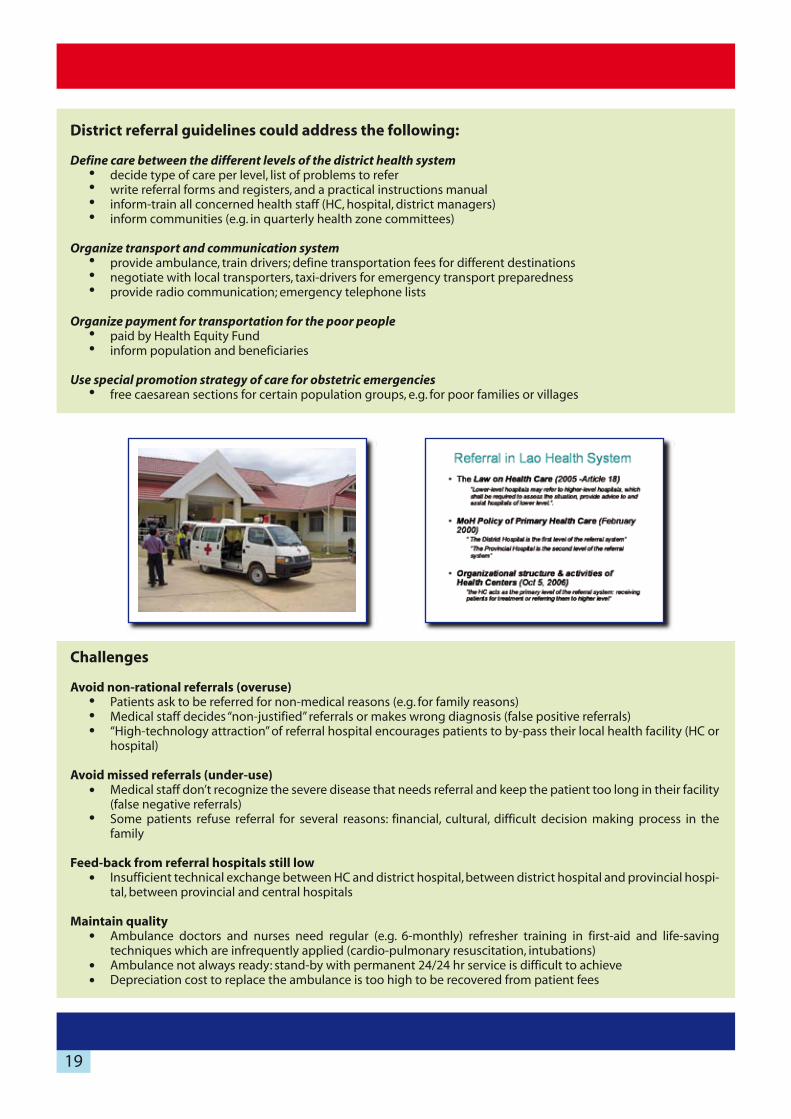
Challenges
Avoid non-rational referrals (overuse)Patients ask to be referred for non-medical reasons (e.g. for family reasons)Medical staff decides “non-justified” referrals or makes wrong diagnosis (false positive referrals)“High-technology attraction” of referral hospital encourages patients to by-pass their local health facility (HC or hospital)
Avoid missed referrals (under-use)Medical staff don’t recognize the severe disease that needs referral and keep the patient too long in their facility (false negative referrals)Some patients refuse referral for several reasons: financial, cultural, difficult decision making process in the family
Feed-back from referral hospitals still lowInsufficient technical exchange between HC and district hospital, between district hospital and provincial hospi-tal, between provincial and central hospitals
Maintain qualityAmbulance doctors and nurses need regular (e.g. 6-monthly) refresher training in first-aid and life-saving techniques which are infrequently applied (cardio-pulmonary resuscitation, intubations)Ambulance not always ready: stand-by with permanent 24/24 hr service is difficult to achieveDepreciation cost to replace the ambulance is too high to be recovered from patient fees
District referral guidelines could address the following:
Define care between the different levels of the district health system decide type of care per level, list of problems to referwrite referral forms and registers, and a practical instructions manualinform-train all concerned health staff (HC, hospital, district managers)inform communities (e.g. in quarterly health zone committees)
Organize transport and communication systemprovide ambulance, train drivers; define transportation fees for different destinationsnegotiate with local transporters, taxi-drivers for emergency transport preparednessprovide radio communication; emergency telephone lists
Organize payment for transportation for the poor peoplepaid by Health Equity Fundinform population and beneficiaries
Use special promotion strategy of care for obstetric emergencies free caesarean sections for certain population groups, e.g. for poor families or villages
19

Development of management teams at all levels (health center, hospital, district office) in collaboration with the community promotes a culture of quality: problem identification, participative decision making, sharing of responsibilities and trans-parency.The quality improvement cycle proposes solutions based upon the identification of problems: additional
funding, building, equipment, change of procedures, additional training of staff. After implementation, the changes are evaluated, and a new cycle of identification-solution-implementation-evaluation can start again.
Learning and training for quality
Health care governance is a systematic approach to quality management within a health organization; it is about moving from a culture of blame to one of learning. Emerging specific problems are continuously identified at the right level, objectives properly set, decisions made accordingly and implemented; there is evaluation of processes and results. The PDCA model of Deming (plan-do-check-act) is a useful tool to this effect. In a learning organization, learn-ing fits the needs and characteristics of the facility, it involves the team, it leads to lasting results. It is not only an intellectual process but also a social and affective one. It is part of team building.
Knowledge management concerns production, mobilization and adequate use of knowledge. Documentation of local initiatives to develop health districts may be useful for policy makers on a national scale, as well as for teaching institutions. Taking account of examples of what works elsewhere (performing experiences) may facilitate local devel-opment of health districts.
Andragogy consists of learning strategies focused on adults, laying emphasis on differences between self-directed and “taught” education. It is sustained by four simple postulates (Knowles):
Adults need to be involved in the planning and evaluation of their instruction
Experience (including mistakes) provides the basis for learning activities
Adults are most interested in learning subjects that have immediate relevance to their job or personal life
Adult learning is problem-centered rather than content-oriented
Quality improvement cycle
QAQuality Assurance
QIQuality Improvement
CQI (Continous Quality Improvement)
The process of planning for quality, by setting standards and related indicators(benchmarks) of expected quality in measurable terms, that the providers (producers) of (health) services must attain and respect
The whole process used within an organization to improve activities in order to work towards attaining the standards of quality. It is a more dynamic concept, based upon the cycle of health care implementation.
The cycle of permanent checking of quality and improvement when necessary (including technical standards and patient satisfaction)
1.
2.
3.
4.
20
Collective initiation on “Quality & Accreditation” can be provided in Khon Kaen University, Thailand, for the core district managing team in separate groups for doctors, nurses, administrators and support-logistic staff; each training lasts for three days.
This training focuses on the quality cycle, on team building, system analysis, analysis of potential for change towards improvement, blaming inadequate organizations rather than blaming insufficient individual performance.
This initiation starts a “collective learning process” for the whole team: the LHS Management Team members then become the main actors of a local “action research process”: search for appropriate actions that can be taken within the existing context.Upon return, a clear conceptual framework is shared with all staff to clarify the vision and the mission of the health service: it concerns quality of care and organization of the local health system. This is externally coached by PHO or project staff.
Defining training needs
Linking planning for additional training of staff with thequality improvement cycle is an effective way to improve skills of the existing staff for improved service delivery: the training needs are progressively identified while “the organization” develops, anchored in the local context, and training is hence directly linked towards improving activities.
Linking additional training of existing staff (of insuffi-cient quality) directly to improved activities is an efficient way to use training budgets:
staff are highly motivated, and eager to learn
upon return, all acquired skills can immediately be practiced
all necessary infrastructure, equipment and organiza-tional arrangements are meanwhile put in place, as part of the comprehensive “problem solving approach” of the Quality Improvement Cycle
Organizing quality improvement in the local health system
Create a dynamic of quality improvement in the HC or hospital team
The “5S Method” is useful for this, mainly to improve nursing care, but also for medical and administration work (see box).
An initial participative assessment of the HC or hospitalsituation (SWOT) is carried out, looking at the existing equipment, procedures and work methods. Based on this, a collective clean-up campaign is organized, all out-of-order equipment discarded and the remaining equip-ment well cleaned and put in order.
Existing work procedure and guidelines are collected and reviewed, or, when needed, new procedures (especially for nursing care) are developed. This process needs coaching.
21
Implement QI activities in the hospital
Morning briefing of all staff in the hospital is essential for team work and continuity of care for the individual patients: it allows identification of emerging clinical and organizational problems, and discussion for relevant decision making.
Case conferences: Complex critical incidents are analyzed in-depth during case conferences, drug and therapeutic committee, or management team meetings in order to set up and adopt new standards and procedures.
Peer-teaching: some doctors more specialized in a specific topic teach their colleagues for improved and standard-ized care in the hospital.
Introduce patient-information system: patient OPD files, patient IPD nursing-plan files, chronic patient’s files to provide integrated continuous care.
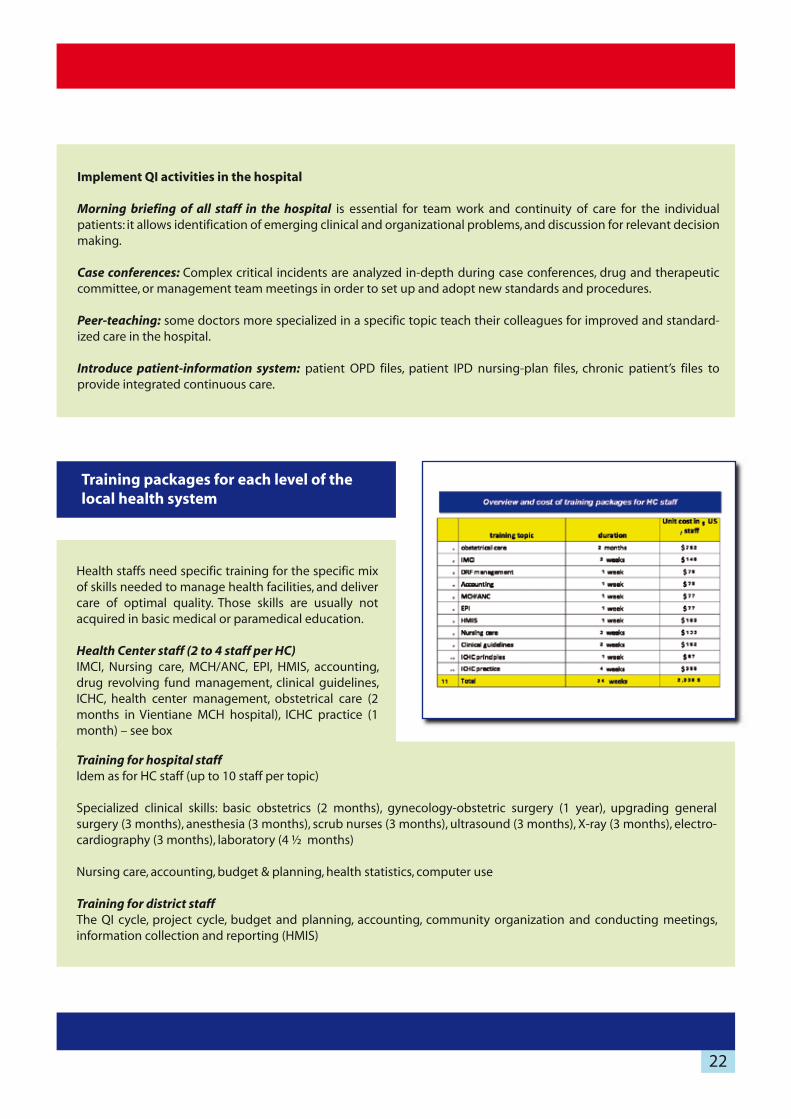
Training packages for each level of the local health system
Health staffs need specific training for the specific mix of skills needed to manage health facilities, and deliver care of optimal quality. Those skills are usually not acquired in basic medical or paramedical education.
Health Center staff (2 to 4 staff per HC)IMCI, Nursing care, MCH/ANC, EPI, HMIS, accounting, drug revolving fund management, clinical guidelines, ICHC, health center management, obstetrical care (2 months in Vientiane MCH hospital), ICHC practice (1 month) – see box
Training for hospital staff Idem as for HC staff (up to 10 staff per topic)
Specialized clinical skills: basic obstetrics (2 months), gynecology-obstetric surgery (1 year), upgrading general surgery (3 months), anesthesia (3 months), scrub nurses (3 months), ultrasound (3 months), X-ray (3 months), electro-cardiography (3 months), laboratory (4 ½ months)
Nursing care, accounting, budget & planning, health statistics, computer use
Training for district staffThe QI cycle, project cycle, budget and planning, accounting, community organization and conducting meetings, information collection and reporting (HMIS)
22
23
Types of training:
Classroom teaching: workshops or more academic courses.
Learning through practice in a referral hospital (provincial or in Vientiane Capital): hospital staff work for a given period
at the provincial or central hospital to learn through practice, according to learning objectives, the techniques and skills
needed to perform properly in their own working place. The training is hence adapted to the context where the staff
will later perform (context based learning).
Coaching: specialists in various disciplines, from provincial or central hospitals, work alternately one week in the district
hospital (maximum 3 weeks/per month): general surgery, paediatrics, gynecology-obstetrics, internal medicine, infec-
tious diseases, specialists in diabetes, hypertension or epilepsy, laboratory, X-ray, ultrasound, cardiology. Ideally, the
coaches come from the same departments where hospital staff previously received their practical training, hence
providing follow-up of the training.
The coaches also help to organize the services in the district hospital. They participate in activities, present conferences
and help produce guidelines fully adapted to the context. The district staff develops a special relation with their
coaches, and can afterwards ask advice by telephone or organize referral of patients to their “teacher”.
Library use: books and reviews are available to the staff.
Continuous learning relationship between district and provincial hospital doctors: phone calls, follow-up of patients
Challenges
Time management of staff: find a right balance between provision of care and learning/meetings
Make sure that each training is followed by immediate opportunities to practice the newly learned skills; make sure
necessary equipment is available; allow for periodic in-service follow-up of the trainee by the trainer
Guide specialist doctors to adapt their training to the working conditions in the district hospital, based on priorities,
taking into account the incidence and seriousness of different pathologies, the relevance of diagnostic tools for
decision making and the technical feasibility and costs of treatments

Content: Each supervision should have partly a standard content (the same at each supervision) and partly a specific content (different on a rotating basis), in order to make sure that all activities are gradually reviewed at least once a year. Supervisors should also be flexible and take care of any specific demands of the supervisee.
Techniques: Direct observation of the supervisee’s practice is the main feature of supervision, but a package of complementary techniques may simulta-neously be used: visit of the premises, review of docu-ments (register, family files, reports), dialogue with staff, identification and discussion of critical incidents, action for demonstration, meeting
with staff for problem analysis and decision making, interview of patients, of community representatives. Findings and resolutions should be consigned in a notebook at the health facility as a reference note.
Process: Supervision is properly prepared: choice of target activities, set up of the calendar accordingly, definition of the supervision team, mobilization of resources, review of relevant reports and documents, preparing a supervision check-list. Follow up of the supervision consists in drafting, transmitting and filing reports, holding supervisors’ meet-ings, reporting to HDMT and implementing resolutions taken.
Supportive health centre supervision is a routine periodic managerial process, which allows verifying and ensuring that work is properly done. It focuses on health care and health service organisation, with reference to a conceptual model, as well as to norms, standards and operating instructions. It is carried out in a climate of total partnership and mutual confidence. It is different from audit and monitoring, which are more control oriented procedures.
Supportive supervision of health centers comprises a situation assessment, continuous training and technical support. Supervisors and supervisees together take necessary decisions to improve the local health system. Unsolved problems are forwarded to the DHMT. Supervision reinforces the functional link between health centers and hospital and motivation of the staff.
One fixed supervisor is attached to each health center to ensure a comprehensive and continuous follow up; s/he may be assisted, on a rotating basis, by other resource persons to supervise some specific activities (curative care, pharmacy, MCH-EPI, financial management, health information system, community activities).
Supervision of health centers
Supervision is different from controls or quarterly audits. Each has a separate function but is complementary in identifying problems to be solved. The problems identified are then addressed in the management cycle of the district health system, which leads to solutions and decision to be taken.
24

Challenges
Increase technical skills of district staff to a level sufficient to allowing for supervising health center staff: increase
capacities to provide useful practical training on the spot
Improve dialogue skills between supervisors – supervised for effective communication
Provide sufficient budgets for supervision
Install a culture of “finding, reporting and solving problems”
Encourage inferior levels to report problems to higher levels, and higher levels to address the reported problems
and seek for solutions
25

A written agreement between provincial and district health offices allows health centers and district hospitals to receive performance-based subsidies for incentives, according to their performance in terms of quantity and agree upon quality standards.
The execution of the agreement is monitored quarterly by a “Control-Auditing team”, which calculates the subsidies.
Performance-based agreements for quantitative and qualitative output are a tool to motivate staff (through increased remuneration and increased job recognition), to increase working standards and to improve the health information system as well as the overall sense of responsibility of health managers for the entire Local Health System and its supervision.
Regular and objective control (audit) ensures that the commitments in the contract are respected: performance is evaluated according to a list of negotiated criteria. Performance subsidies are allocated to the facility according to quantitative criteria (based on offer and utilization of services) and qualitative criteria. The payment to individuals is calculated according to qualification and function, effective working time, respecting dress codes, behavior towards patients and individual technical performance.
ChallengesSustainability of funding the performance-based payment, related to a long term strategy to ensure adequate funding for health worker remunerationRationalization of staff numbers and staff profile in health facilities
Performance-based subsidies and audit
Health staff motivation is a condition for good performance; it is the result of a balance between negative disincentives (work load, risks, opportunity costs, discomfort) and positive incentives. Incentives may be non-financial (work characteristics, work environment, flexibility in employment conditions, career and professional development, access to services such as markets and schools), but also financial (terms and conditions of employment, complementary financial support and performance-based payments). Performance-based payments are thus not the only tool for providing incentives to staff.
On the other hand, performance-based payments not only improve the remuneration of staff but have a beneficial effect on the entire health system. A signed agreement, or “contract”, with payments based on outputs motivates health workers to do required work, or to give up inappropriate practices, in exchange for a clear reward.
Health performance contracts may involve two levels of partnership: between the “supporting body” (a project, a donor, the PHO) and a health facility (first degree contract) or between the health facility and its staff (second degree contract). Contracts may target individuals, or entire teams. Subsidies may also be used to cover operational costs of the facility.
EXAMPLE OF OUTPUT-SUBSIDY PAID BY PROJECT PERFORMANCE CONTRACTS HELP BREAK THE VICOUS CIRCLE OF LOW SERVICE DELIVERY
26
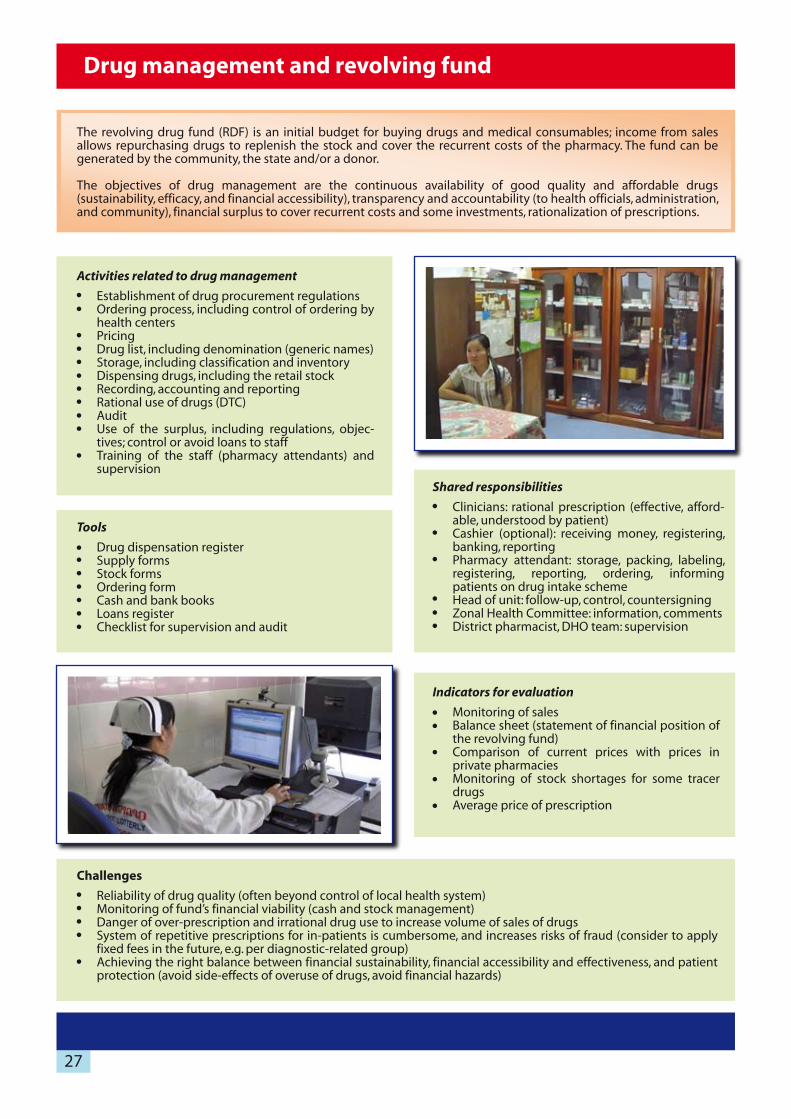
Activities related to drug management
Establishment of drug procurement regulations Ordering process, including control of ordering by health centersPricingDrug list, including denomination (generic names)Storage, including classification and inventory Dispensing drugs, including the retail stockRecording, accounting and reportingRational use of drugs (DTC)AuditUse of the surplus, including regulations, objec-tives; control or avoid loans to staffTraining of the staff (pharmacy attendants) and supervision
Tools
Drug dispensation registerSupply formsStock formsOrdering formCash and bank booksLoans registerChecklist for supervision and audit
Shared responsibilities
Clinicians: rational prescription (effective, afford-able, understood by patient)Cashier (optional): receiving money, registering, banking, reportingPharmacy attendant: storage, packing, labeling, registering, reporting, ordering, informing patients on drug intake schemeHead of unit: follow-up, control, countersigningZonal Health Committee: information, commentsDistrict pharmacist, DHO team: supervision
Indicators for evaluation
Monitoring of salesBalance sheet (statement of financial position of the revolving fund)Comparison of current prices with prices in private pharmaciesMonitoring of stock shortages for some tracer drugsAverage price of prescription
The revolving drug fund (RDF) is an initial budget for buying drugs and medical consumables; income from sales allows repurchasing drugs to replenish the stock and cover the recurrent costs of the pharmacy. The fund can be generated by the community, the state and/or a donor.
The objectives of drug management are the continuous availability of good quality and affordable drugs (sustainability, efficacy, and financial accessibility), transparency and accountability (to health officials, administration, and community), financial surplus to cover recurrent costs and some investments, rationalization of prescriptions.
Drug management and revolving fund
Challenges
Reliability of drug quality (often beyond control of local health system)Monitoring of fund’s financial viability (cash and stock management)Danger of over-prescription and irrational drug use to increase volume of sales of drugsSystem of repetitive prescriptions for in-patients is cumbersome, and increases risks of fraud (consider to apply fixed fees in the future, e.g. per diagnostic-related group)Achieving the right balance between financial sustainability, financial accessibility and effectiveness, and patient protection (avoid side-effects of overuse of drugs, avoid financial hazards)
27

Sources of information
Quantitative information is usually collected through the use of registers and reporting forms, concerning village and health facility utilization data, financial information (cash books, registers), an epidemiological surveillance system, the drug revolving fund records, inventories.Demographic data may be obtained through surveys or periodic updates of family files or other village data bases.
Qualitative information may be gathered during outreach visits to villages (e.g. for vaccination), health zone health committee meetings, feed-back from patients and population, or local authorities (e.g. patient complaint box).Supervision and control-auditing visits to health centers and the hospital provide another source of mixed qualitative-quantitative information on the health providing process.
Specific complementary information may be needed for the Quality Improvement of care: data on patient manage-ment (evidence-based diagnosis & treatment, treatment outcome) gathered through analysis of patient files.
Use of information for decision making
Demographic data on health center zones provide information about the target population for curative care and prevention: denominators. Utilization and coverage rates (e.g. vaccination) can be calculated, and interventions proposed accordingly. Financial information and on the drug revolving funds avoids depletion of drugs, keeping budgets in balance, deciding on investments or recurrent costs, proposing pricing and calculating incentives.Feed-back to the population is given in quarterly Health Zone Committee meetings: review, re-planning of activities.Feed-back to the district and peers (other staff ) is given in quarterly planning meetings at (inter-) district level: analyze indicators, discuss problems, propose solutions and analyze the functioning of the district as an integrated system.
The DHMT uses the consolidated (and eventually corrected) information of health centers and the hospital for decision making in the district (budget & planning – quarterly meetings) and for transmission of reports to the Provincial Health Office.
The Province compiles data from each district and from the provincial referral hospital. Information is processed in computerized databases. Provinces provide support to districts (Local Health System) on quality control of data, on use of the information for decision making (budgeting and planning).At provincial level, the information is used for strategic planning.
Challenges
Improve skills in data handling, calculation of rates and percentagesImprove understanding of the indicators: definition of numerators and denominators, meaning of the indicatorsUncertainty on denominator numbers due to declining birth rates (e.g. to calculate vaccination coverage)Demand by health facilities to proceed to computerization, with ensuing need for training and technical support
A Health Management Information System (HMIS) generates information produced by the health services, to be used by them for planning, monitoring and evaluation of activities.
The information is to be used in the first place at the health facility level, then by the Local Health System and finally to be reported to provincial and central levels.
The indicators mainly concern inputs, process and output-outcome, regarding curative, preventive and promotional health care; demographic and epidemiological data may be included. (See Chapter: Vision of LHS, Indicators). Financial management information and economic analysis contributes to the overall management decision process.
Monitoring and health information management
28

Financial management supports operational planning (of the district or health facility) by correctly handling funds and providing reliable information on financial transactions and the overall financial situation of health facilities to allow rational decisions on incomes and expenditure of health facilities and to ensure transparency and accountability.
Main related activities are registration of income and expenditure (archiving bills and invoices, keep registers, Excel sheets), summary and integration of information (balance sheets), supervision and audit, decision making on income and expenditure.
Financial transactions concern income and expenditures.
Sources of income are the government allocations (salary, night duty, operational budgets), payments by patients for drugs and service fees (directly out-of-pocket payment or through equity funds or health insurance), donors, national programs and other income (such as parking fees, hospital restaurant, meeting room rental).
Expenditures are allocated for staff salaries, administrative and operational costs, procurement of drugs and consum-able supplies, investments, specific health activities such as vaccination outreach rounds, health education campaigns or anti-malarial bet net impregnation.
Supervision & AuditThe District supervision team ensures monthly supervision and monitoring of accounts in the health center. Audits are carried out quarterly by the district audit team, with assistance from the PHO.
The PHO provides regular supervision to the DHO accountants and controls-audits the team of the DHO and IDRH quarterly.
Financial management
Responsibilities of the accountant and treasurer must be clearly distinguished and separated:
The accountant is in charge of the daily recording of all income and expenditure, providing summaries and reports to the head of the unit, allocating expenses, ensur-ing accuracy, transparency and account-ability.
The treasurer is in charge of the daily collection of cash (RDF, fees, donors, receiv-ables, payables), petty cash management (process of cash transaction) and weekly and monthly cash counts to ensure accuracy, transparency and accountability.
Several tools are being used such as cash books, registers, data forms, Excel sheets.
29
Challenges
Providing adequate financial and technical support (accounting, computer use, budget, planning)
Maintaining trained responsible staff in place – career prospects – salaries – professionalism
Understanding by health managers of the meaning of the obtained financial information and indicators, and
taking decisions accordingly (e.g. to avoid bankruptcy, to calculate user fees)
Consolidation by PHO of the data from different districts into a provincial health management information system
+ utilization for decision making by provincial level
Discipline (mainly in hospitals) for correct daily entering of all revenues (drug revolving fund and user fees) to
avoid leakage
To computerize or not at lower levels (HC and districts type B): it may help data collection and processing, but is a
challenge in itself (support for training in spreadsheet use, maintenance, virus cleaning)
Assure link with the HMIS: assure that there are no separate data sets, with different numbers
Outputs of financial management are simple tools:
Financial monitoring of each facility (overall availability of funds - shortage or surplus of RDF) and adequate and
clear reporting.
Allow for adequate decision making: plan activities, expenditures and prevent bankruptcy at facility level.
Provide information for budgeting and planning at district level (in Management Information System).
Provide tools of transparency and accountability to the provincial level.
Allow for economic analysis: costing analysis at provincial and national levels.
Provide needs assessment for subsidies by MoH, local administrations or donors.
30
A HEF also has a pro-active social function in encour-aging poor patients to use the opportunity of free care offered to them
Providing free care in itself is not always enough to make poor patients use the health services sufficiently. Other barriers have to be addressed by HEF managers, such as:
opportunity cost: time lost for farming or other work while attending a (remote) clinic
cultural barriers: language, taboo’s on use of western medicine, uneasiness with modern hospi-tal building and modern hospitalization room, type of food, complicated decision making process in the family regarding health seeking behavior
HEF managers also should have a role in negotiating quality and cost of care with the health care providers: use of essential drugs, rational prescribing, helpfulness and attentiveness of staff towards poor patients.
Health Equity Funds are set up to subsidize medical treatment costs and opportunity costs (transportation, lack of income while seeking care) for (very) poor families in order to improve their access to health care services.
Beneficiaries may be selected on an individual basis before (pre-identification) or at the time of care provision (post-identification) according to objective criteria and/or community representatives’ opinion. Coverage may concern whole deprived populations as well as the general population but for a specific health problem (e.g. caesarean sections, HIV-AIDS or tuberculosis patients). Selection may also target selected population groups (e.g. children, pregnant women, elderly, handicapped persons) or be geographical (e.g. for poor villages or entire districts).
The benefit package may consist of payment of user fees, provision of drugs, transportation, supplementary food, assistance to accompanier, use of basic items like soap, bed net, blanket, clothing and cooking utensils and even funeral costs.
Management of the fund may be in charge of an independent body, like a NGO, or of an administrative unit within the health sector, but requires a split between provider-purchaser functions and regular (external) audits.
The system is supported by a set of procedures (identification of benificiaries, request for reimbursement, payment, reporting, supervision and training, auditing) and operational tools (patient cards, registers, forms).
Results may be expressed in number (and %) of patients covered by the equity fund, utilization of services by poor patients compared with utilization by non-covered patients, expenditures for poor beneficiaries with distinction of overhead costs, difference of cost for patients covered by the equity fund and by other schemes.
Financing of existing HEF programs at the start-up is often provided entirely by external organizations; the base of funding could be enlarged through pooling of external resources. Economic growth may allow moving away from exclusive donor funding towards progressive global budget support from government taxation revenues (universal coverage).
Health Equity Fund (HEF): access to health care by the poor
31
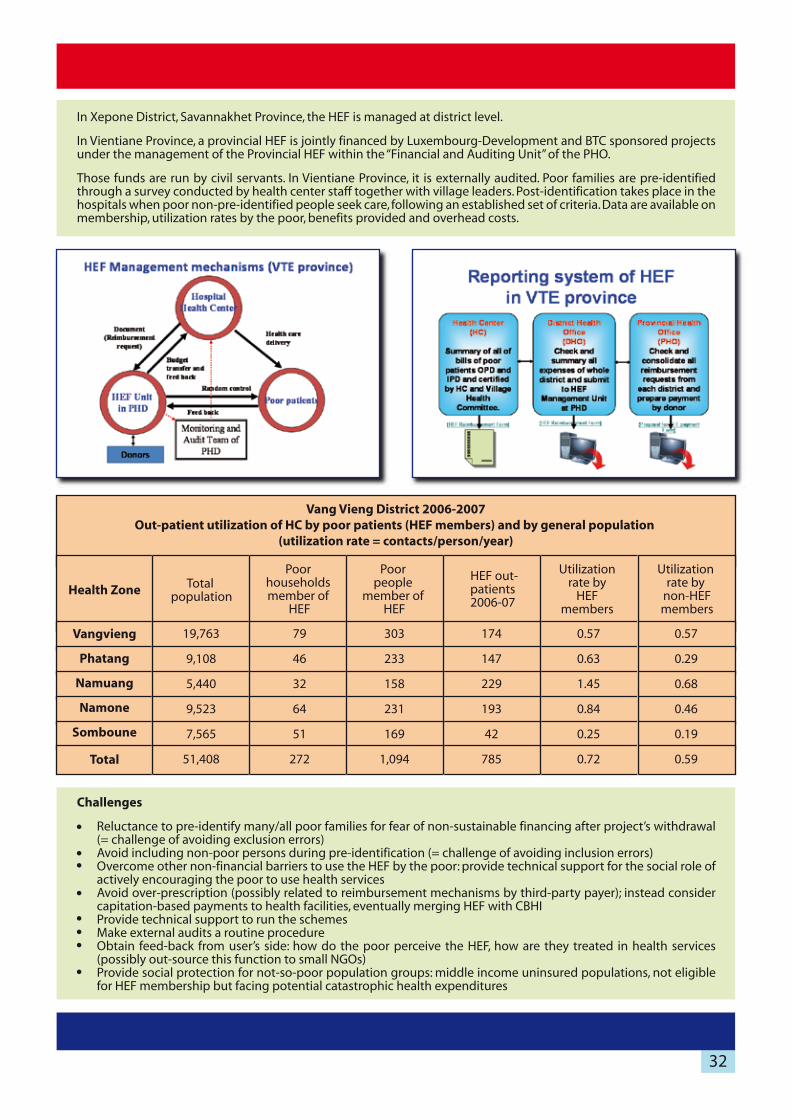
In Xepone District, Savannakhet Province, the HEF is managed at district level.
In Vientiane Province, a provincial HEF is jointly financed by Luxembourg-Development and BTC sponsored projectsunder the management of the Provincial HEF within the “Financial and Auditing Unit” of the PHO.
Those funds are run by civil servants. In Vientiane Province, it is externally audited. Poor families are pre-identifiedthrough a survey conducted by health center staff together with village leaders. Post-identification takes place in the hospitals when poor non-pre-identified people seek care, following an established set of criteria. Data are available on membership, utilization rates by the poor, benefits provided and overhead costs.
Vang Vieng District 2006-2007Out-patient utilization of HC by poor patients (HEF members) and by general population
(utilization rate = contacts/person/year)
Poor householdsmember of
HEF
Health Zone
Vangvieng
Phatang
Namuang
Namone
Somboune
Total
Total population
Poor people
member of HEF
HEF out-patients 2006-07
Utilization rate by
HEFmembers
Utilization rate by
non-HEFmembers
19,763
9,108
5,440
9,523
7,565
51,408
79
46
32
64
51
272
303
233
158
231
169
1,094
174
147
229
193
42
785
0.57
0.63
1.45
0.84
0.25
0.72
0.57
0.29
0.68
0.46
0.19
0.59
Challenges
Reluctance to pre-identify many/all poor families for fear of non-sustainable financing after project’s withdrawal (= challenge of avoiding exclusion errors)Avoid including non-poor persons during pre-identification (= challenge of avoiding inclusion errors)Overcome other non-financial barriers to use the HEF by the poor: provide technical support for the social role of actively encouraging the poor to use health servicesAvoid over-prescription (possibly related to reimbursement mechanisms by third-party payer); instead consider capitation-based payments to health facilities, eventually merging HEF with CBHIProvide technical support to run the schemesMake external audits a routine procedureObtain feed-back from user’s side: how do the poor perceive the HEF, how are they treated in health services (possibly out-source this function to small NGOs)Provide social protection for not-so-poor population groups: middle income uninsured populations, not eligible for HEF membership but facing potential catastrophic health expenditures
32
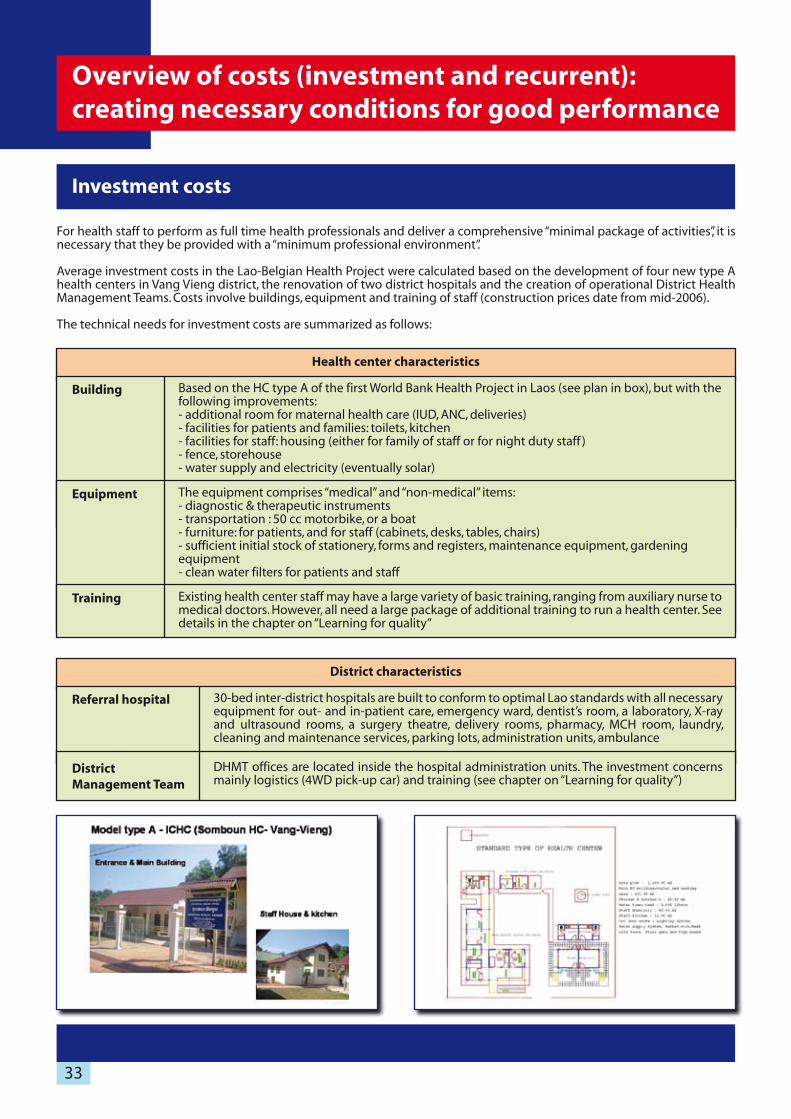
Investment costs
For health staff to perform as full time health professionals and deliver a comprehensive “minimal package of activities”, it is necessary that they be provided with a “minimum professional environment”.
Average investment costs in the Lao-Belgian Health Project were calculated based on the development of four new type A health centers in Vang Vieng district, the renovation of two district hospitals and the creation of operational District Health Management Teams. Costs involve buildings, equipment and training of staff (construction prices date from mid-2006).
The technical needs for investment costs are summarized as follows:
Health center characteristics
Building
Equipment
Training
Based on the HC type A of the first World Bank Health Project in Laos (see plan in box), but with the following improvements:- additional room for maternal health care (IUD, ANC, deliveries)- facilities for patients and families: toilets, kitchen- facilities for staff: housing (either for family of staff or for night duty staff )- fence, storehouse- water supply and electricity (eventually solar)
The equipment comprises “medical” and “non-medical” items:- diagnostic & therapeutic instruments- transportation : 50 cc motorbike, or a boat - furniture: for patients, and for staff (cabinets, desks, tables, chairs)- sufficient initial stock of stationery, forms and registers, maintenance equipment, gardening equipment- clean water filters for patients and staff
Existing health center staff may have a large variety of basic training, ranging from auxiliary nurse to medical doctors. However, all need a large package of additional training to run a health center. See details in the chapter on “Learning for quality”
District characteristics
Referral hospital
District Management Team
30-bed inter-district hospitals are built to conform to optimal Lao standards with all necessary equipment for out- and in-patient care, emergency ward, dentist’s room, a laboratory, X-ray and ultrasound rooms, a surgery theatre, delivery rooms, pharmacy, MCH room, laundry, cleaning and maintenance services, parking lots, administration units, ambulance
DHMT offices are located inside the hospital administration units. The investment concerns mainly logistics (4WD pick-up car) and training (see chapter on “Learning for quality”)
33
Overview of costs (investment and recurrent):creating necessary conditions for good performance

Health Centers Costs per capita are calculated on the basis on an average population of 7 570 for the 4 completely new HCs built in Vang Vieng.
CategoryInvestment per
HCInvestment per
capita
Depreciation years
estimate
Cost/capita/yr to maintain (*)
Equipment & drugs
Training
Total
Building $ 40,735
$ 11,666
$ 10,000
$ 62,401
$ 5.38
$ 1.54
$ 1.32
$ 8.24
$ 0.41
$ 0.15
$ 0.26
$ 0.77
15 yrs
10 yrs
5 yrs
-
CategoryAmount
(average)Investment per
capita
Depreciation years
estimate
Cost/capita/yr to maintain (*)
Equipment & drugs
Training
Total
Building $ 545,000
$ 275,000
$ 27,500
$ 847,500
$ 3.35
$ 1.69
$ 0.17
$ 5.22
$ 0.22
$ 0.17
$ 0.08
$ 0.48
15 yrs
10 yrs
2 yrs
-
CategoryAverageamount
Per capitaDepreciation
years estimate
Cost/capita/yr to maintain (*)
Equipment, furniture,
Training
Total
Car, motorbikes $ 22,932
$ 7,939
$ 22,011
$ 52,882
$ 0.46
$ 0.16
$ 0.44
$ 1.06
$ 0.05
$ 0.02
$ 0.09
$ 0.15
10 yrs
10 yrs
5 yrs
-
(*) investment/population/number of depreciation years.
Inter-district Hospitals Costs per capita are calculated on the basis of an average population of 162 000 served by the Vang Vieng and Xepone hospi-tals; this includes the population of the adjacent administrative districts which are referring patients to those “inter-district hospitals”; the investment in the hospitals type “A” is related to this whole population being served.
District Management TeamCosts per capita are calculated on the basis of an average population of 49 800 in Vang Vieng & Xepone administrative districts; this is the population served by the DHO staff – it does not include the population of neighboring administrative districts, which have their own DHO supervising health centers.
(*) investment/population/number of depreciation years.
(*) investment/population/number of depreciation years.
34

CategoryInitial investment per
capitaCost/capita/yr to
maintain or renew
Hospital (inter-district)
District team
Total
Health center $ 8.24
$ 5.22
$ 1.06
$ 14.52
$ 0.77
$ 0.48
$ 0.15
$ 1.40
Summary investment cost The overall cost per capita is based on summarizing the estimates for each level of the LHS given in the tables above.
Those costs depend on already existing resources. The investments by projects are meant to complement the existing resources to make them sufficient for providing a minimal package of quality services.
Recurrent costs
Recurrent costs of health services are composed of the following:
Salary & allowances
Supplies
Activities
Operational costs
Salaries, night duty, family allowance, performance based payments
General running costs: maintenance, stationery, transportation, electricity, water, telephone
Quarterly zone health committee meeting, integrated quarterly outreach MCH-EPI-IEC (extra per diem, transportation costs, IEC materials)Supervision (by DHO or hospital to HC; by HC to village health workers)
Essential drugs and health care consumables
35
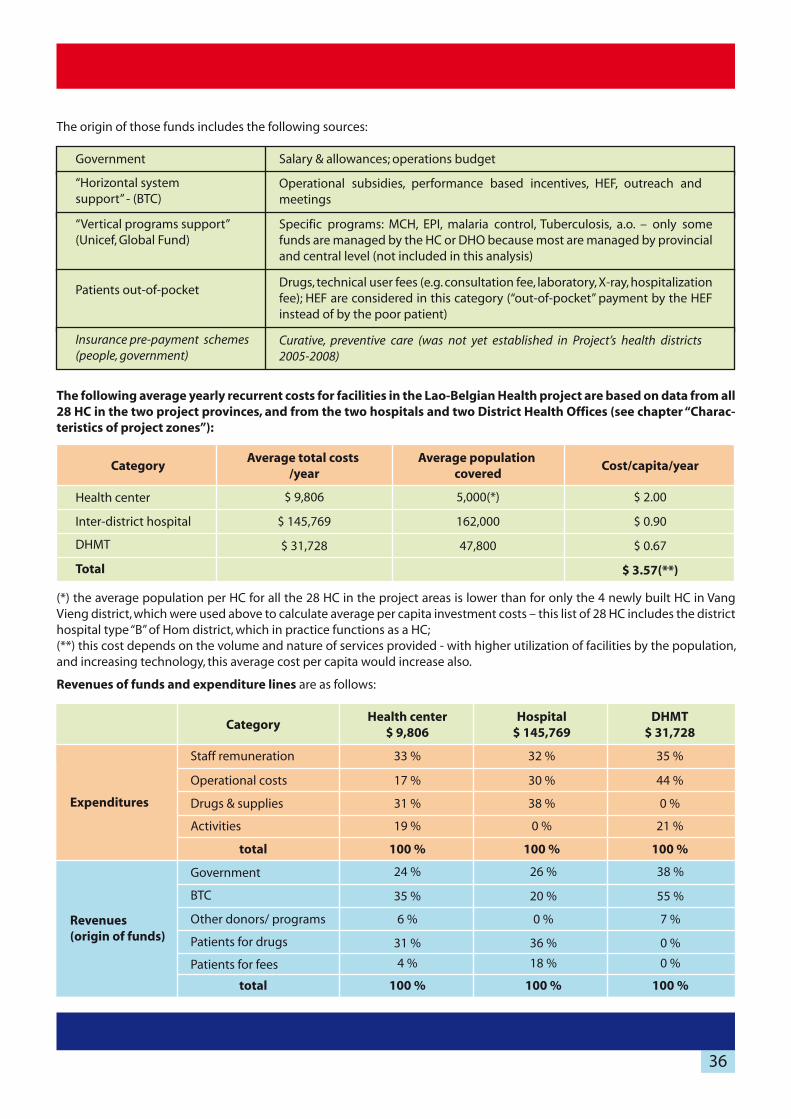
CategoryAverage total costs
/yearAverage population
coveredCost/capita/year
Inter-district hospital
DHMT
Total
Health center $ 9,806
$ 145,769
$ 31,728
5,000(*)
162,000
47,800
$ 2.00
$ 0.90
$ 0.67
$ 3.57(**)
The origin of those funds includes the following sources:
Government
“Vertical programs support” (Unicef, Global Fund)
Patients out-of-pocket
Insurance pre-payment schemes (people, government)
“Horizontal system support” - (BTC)
Operational subsidies, performance based incentives, HEF, outreach and meetings
Specific programs: MCH, EPI, malaria control, Tuberculosis, a.o. – only some funds are managed by the HC or DHO because most are managed by provincial and central level (not included in this analysis)
Drugs, technical user fees (e.g. consultation fee, laboratory, X-ray, hospitalization fee); HEF are considered in this category (“out-of-pocket” payment by the HEF instead of by the poor patient)
Curative, preventive care (was not yet established in Project’s health districts 2005-2008)
Salary & allowances; operations budget
The following average yearly recurrent costs for facilities in the Lao-Belgian Health project are based on data from all 28 HC in the two project provinces, and from the two hospitals and two District Health Offices (see chapter “Charac-teristics of project zones”):
(*) the average population per HC for all the 28 HC in the project areas is lower than for only the 4 newly built HC in Vang Vieng district, which were used above to calculate average per capita investment costs – this list of 28 HC includes the district hospital type “B” of Hom district, which in practice functions as a HC; (**) this cost depends on the volume and nature of services provided - with higher utilization of facilities by the population, and increasing technology, this average cost per capita would increase also.
Revenues of funds and expenditure lines are as follows:
CategoryHealth center
$ 9,806Hospital
$ 145,769DHMT
$ 31,728
Expenditures
Revenues(origin of funds)
Staff remuneration
Operational costs
Drugs & supplies
Activities
Government
BTC
Other donors/ programs
Patients for drugs
Patients for fees
total
total
33 %
17 %
31 %
19 %
100 %
24 %
35 %
6 %
31 %
4 %
100 %
26 %
20 %
0 %
36 %
18 %
100 %
38 %
55 %
7 %
0 %
0 %
100 %
35 %
44 %
0 %
21 %
100 %
32 %
30 %
38 %
0 %
100 %
36

Those percentages related to the overall yearly funds correspond to the following average amounts of origin of revenues per level in 2007-2008:
The “horizontal” donor BTC pays an average subsidy per HC of $ 3,432 per year. This amount allows mobilizing patient’s payments and increases the productivity of government-paid salaries while financing community participation and improved village outreach. The BTC subsidy to hospitals, on average $ 29,000 in 2007-08, shows a yearly decline while hospital recurrent costs are increasingly being financed by patients, reaching more than 50 % in 2007-08.On the other hand, the DHMT relies heavily on project subsidies, because it cannot receive income from service delivery to the population, and, besides salaries, government’s budget for operational cost is extremely low. BTC subsidizes on average $ 17,460 per year, without which little work can be done except some periodic preventive activities financed by the vertical programs.
The costs for Provincial Health Offices could not be analyzed in detail. The BTC contribution for investment (a 4WD car, computers and office equipment and some training) and operational costs (mainly supervision and meetings) amounted to $ 0.24 per capita per year (calculated on whole population in project area – see chapter “Characteristics of project zones”). This does not include costs of buildings, salaries, government budget for operational costs or subsidies by other donors and national programs.
The average recurrent cost per out-patient (OPD) and in-patient (IPD), including payments from government/donors and patients, for the 28 HC and 2 hospitals, was calculated as follows:
Compiling the data above, the following average costs are estimated for the Local Health System such as developed in the project:
Type of cost Health center Hospital
Recurrent cost per IPD case
Recurrent cost per OPD case $ 1.95
$ 21.90
$ 6.00
$ 33.27
Category Investment costs Recurrent costsTotal yearly average
cost per capita
Hospital (inter-district)
District team
Total per capita/yr
Health center $ 0.77
$ 0.48
$ 0.15
$ 1.40
$ 2.00
$ 0.90
$ 0.67
$ 3.57
$ 2.77
$ 1.38
$ 0.82
$ 4.97
Revenues of HC Revenues of hospitals Revenues of DHMT
Summary of investment and recurrent costs per capita
37

Including project management costs and subsidies to the provincial health offices, a closer estimate of overall costs per
capita per year would be as follows:
Type of cost Amount
PHO (minimum, BTC subsidy only)
Project management costs
Total cost per year/capita
District health services costs $ 4.97
$ 0.24
$ 2.90
$ 8.11
Based on this project experience, it appears that less than $ 10 per capita per year would be necessary to progressively
build and maintain a comprehensive first- and second-line health system capable of delivering a minimal package of
activities. This includes payments by the patients for drugs and services and project overhead costs. But it concerns only the
costs at the level of the LHS itself.
This figure is an underestimation of the overall costs of developing the system: it does not include most costs of the PHO
(salaries, equipment and buildings), nor vaccines, village drug kits, malaria & TBC drugs. Also, the package of care currently
provided is still not optimal. For example, the average out-patient utilization rate is about 0.50 new consultations per capita
per year, and the coverage rate of caesarean sections in Vang Vieng inter-district area is only 47%. Vaccination coverage is
estimated at approximately 80%. Higher utilization of services will entail higher costs, especially for drugs and consumables.
On the other hand, it will increase the productivity of staff.
The total project administration costs (technical assistants, cars, local staff, consultants, reporting and steering committees)
amounted to roughly $ 2,5 million over 5 years, or an average of $2,90 per capita and per year. This cost includes purchasing
an important amount of technical assistance, which might be considered as a necessary investment cost. On the other hand,
project management costs included the cost of developing a “prototype model” in two separate districts which entails
specific costs, especially for external technical assistance. Replicating this model should entail much lower operational costs,
by using economies of scale.
Finally, the calculated average costs per capita per year are based on the average numbers of inhabitants in the target health
center zones and districts. Those average numbers of population hide large variations. For other areas in Laos with large
populations, the average investment cost per capita obtained in the LBHP might be an overestimation; for low density
population areas on the contrary, this cost might be an underestimation.
For those reasons, extrapolating the average recurrent cost subsidies might be equally hazardous. Nevertheless, extrapolat-
ing the BTC subsidies of roughly $ 3,400 per HC per year to about 800 HC in Laos would entail an annual national supplemen-
tary subsidy of about $ 2,750,000. An annual DHO subsidy of $ 17,460 per year would cost about $ 2,500,000 per year for all
142 districts in Laos. An annual subsidy per inter-district hospital of $ 29,000 for 40 selected hospitals in Laos (one for 150,000
population) would entail a supplementary yearly budget of $ 1,160,000.
38

Besides hard-ware investment and technical training, the project invested heavily in improving and modernizing the management procedures of the health system. This led to important changes in attitudes and practices, which in turn led to improved working conditions and output of the health services. Those changes were obtained by progressively introducing innovative technical, managerial and financing methods. Many of the changes were progressively co-developed between health facility staff and project technical assistants, in agreement with Provincial health offices and MoH. Lessons are learned from this, but challenges remain.
Summary: main results, lessons learned and challenges
MAIN RESULTSCompared to the initial situation, following changes are observed:
Before After
Evolution in health centers
Staff reluctant to work in HC; often discouraged
Passive behavior - waiting for patients
No operational budget
Often by-passed or neglected by District
Little accountability
Pro-active community health work
Sufficient staff at HC level (+/- 1 per 1 000 capita); increased job satisfac-tion and respect from population
More professional health workers, with increased salary and spending more time on health work
Increased revenues from Government, donors, patients (user fees, income DRF)
Integrated curative and preventive care; higher utilization by popula-tion and patients
Limited curative care; limited participation in EPI-vaccinations
Considered as cornerstone of village health care; supported by District
Accountable to District and local population; organized community involvement in health matters
Under-paid, semi-professional staff, occupied with other income generating activities
Before After
Evolution in district management teams
Conflicts of interests; authoritarian decisions; arbitrary decisions
Staff (doctor)-centered management
Non-transparent procurement procedures
Management mainly of inputs
Informed decision making (quotations, technical aspects)
More collegial decisions under authority of director; decisions based on evidence (data of HMIS); decisions made public and followed-up
Patient-centered management, for better service delivery and problem solving (improved quality of care)
Complementarities between HC and hospital; support to HC from District
Competition between health centers and hospitals (for curative patients, for EPI vaccinations)
Regular activities are budgeted; public funding (donor, Government) ; DHO does not siphon income from hospital or form HC
Insufficient budget for sporadic planning, supervision and monitoring activities; DHO uses revenues from hospital
Accountability also to local authority and populationAccountability towards PHO only
Management progressively oriented towards outputs and results
Doctors focus on private practice
Low technical level; static quality situation
Focus is primarily on hospital development; private practice becomes secondary activity
Improved quality; internal quality improvement mechanism; dynamic situation
Individualism; networking within competing groups of staff; little accountability
Collegial teamwork; action taken when insufficient performance
Official user-fees complement salary of staff and operational budget; staff has increased salaries
Updated inventories and stock-keeping mechanisms introducedEquipment disappearing
Transparent financing ; sound accounting; increased income; revenue and cost analysis
Non-transparent financial situation; chronic bankruptcy (loans to staff; payments to District health Office)
Informal payments by patients are often source of conflict between underpaid staff
AfterBefore
Evolution in hospitals
39

MAIN LESSONS
Need for systemic approach
Well performing local health systems can be developed in Laos through a systemic approach: all relevant issues of the system must be simultaneously addressed – infrastructure, equipment, technical and managerial training, financing methods, referral system, supervision, information management. Those issues correspond to the “Six Building Blocks” of Health Systems (WHO, 2007): services, human resources, information system, financing, supplies, and governance.
Need for initial investment and progressively decreasing subsidies for recurrent costs
A minimum initial investment is necessary to create the conditions for quality service delivery. Once those conditions are created, and the population utilizes the services more often, the local facility can generate enough income to become nearly self-sufficient for curative care (to pay for most operational costs and some form of staff incentives for curative care). Initial subsidies for recurrent costs can hence be progressively reduced.
Preventive care and the “managing of the system” (supervisions, planning meetings, monitoring HMIS) cannot be paid for out of revenues from patients (drug sale, service fees) and other sources of funding should be explored.
Need for technical support to the reform process
Support by an external partner (catalyst) is necessary to start and guide the development process: at the beginning, this can be provided by project staff, but the role must progressively be taken over by the PHO.
This support leads to the empowerment of the local health management team and to building the necessary skills for autonomous and more effective bottom-up budgeting and planning decisions: making consensual decisions to achieve the defined objectives. Involvement and commitment of local administrative and Party authorities is important.
Flexibility in planning the improvements and in providing the funds for investments, training and activities is important to allow for a local reform dynamic, adapted to the prevailing conditions and capacities. It is best in the beginning to set only short-time goals and to aim only at “improvements” without setting too ambitious targets. If things can improve continuously, everybody is happy; if too ambitious targets cannot be met, despite real progress, then everybody risks being unhappy and the reform dynamic will suffer from less enthusiasm.
40

Sustainability of health facilities
Conditions for sustainability of the individual health facilities can be met to a large extent, namely regarding techni-cal aspects (rules, procedures, skills for clinical and managerial tasks), logistics (supply chain) and behavioral aspects (both for staff and users of health facilities).
Curative care, to a certain extent, can be auto-financed by the facility’s revenues. However, public health tasks need public funding: preventive care, system management, health care for the poor.
Sustainability and wider impact of a “pilot project”
Safeguarding the dynamics at provincial and district health offices will probably require continued external support, and additional operational funding, for several years. The lack of operational budgets for the PHO and DHO is a challenge in this respect.
How will the Lao health sector be able to get maximum benefit from this pilot experience?Use some experiences for policy or strategy decisions Use the developed districts as training grounds for practice-training for nurses and medical studentsCapitalize on the experience for teaching purposes at National Institute of Public Health-NIPH (Advanced diploma in public health) and the University of Health Sciences-UHS (Master’s degree in public health)Institutionalize certain technical aspects (supervision, quality assurance-improvement, specific training for HC staff or district managers, referral system)Further develop the concept of the inter-district Local Health System in an operational way (supervision, technical support, inter-district planning meetings).
Reproducibility of the district reform process
This reform was carried out in a specific setting, with extensive support from national and international expertise and close follow-up by MoH authorities.
Now that this “prototype” has been developed, its duplication in other districts or provinces will require fewer technical inputs. However, it might still be challenging to replicate this reform process in the more usual conditions of limited technical backstopping prevailing in the larger donor-subsidized health projects in Laos. It might be best to start in districts with the most favorable conditions; then learn from this process at provincial level, and progressively extend to other districts. Otherwise, isolated approaches may be reproduced, such as HEF or quality improvement mecha-nisms.
An intelligent balance between necessary standardization and the need for flexibility in response to context specifici-ties has to be found. Also a balance is needed between progressively introducing improved management systems in areas with most potential while also providing support to the provincial health systems as a whole. This dilemmarelated to “scaling up” is addressed in the World Health Report 2008 (WHO) pg 28-29.
Most likely, a challenge for the international donor community will be to make funds available for basic health system development instead of focusing on specific vertical programs, addressing only a part of the system, such as communi-cable disease control programs or MCH care, but which cannot be technically sustained without strengthening the Local Health System’s horizontal integrated management.
MAIN CHALLENGES
41

The following facilities were developed by the Lao-Belgian Health project
Project Health Zones in Savannakhet Province
district health zonetype
facilityPop
(2007)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
Sepone H Z
Munchi
Phonhai
Dongsavanh
Ladho
Densavanh
Salen
Phabang
Lako
subtotal
Taleo
Nasang
Nakham
Nathom
Na Yom
Nong H Z
Dongnasan
hosp A
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
hosp B
ICHC
12,278
4,796
3,109
6,509
2,255
7,365
2,687
3,224
1,965
44,188
6,228
5,525
7,909
6,700
5,444
5,447
2,345
Champhone
Xaybuly
Xayphouthong
Phin
Virabuly
Nong
Sepone
TOTAL 83,786
Project Health Zones in Vientiane Province
district health zonetype
facilityPop
(2007)
1
2
3
4
5
6
7
8
9
10
11
12
13
14
VangVieng
Phatang
Namuang
Namone
Somboune
subtotal
Hom
Phonesavad
Xiengmy
Nampoung
Sobyourk
subtotal
Bansone
Hinhouaseua
Phonthong
Naxaysavang
subtotal
hosp A
ICHC
ICHC
ICHC
ICHC
hosp B
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
ICHC
19,470
8,889
5,466
9,292
7,566
50,683
10,788
6,435
3,334
4,919
2,205
29,003
3,612
3,354
1,183
8O2
8,951
VangVieng
Hom
Xaysom- boun
TOTAL 88,637
42
Characteristics of Vangvieng and XeponeHealth Districts

Ministry of Health, Lao PDR. Policy on Primary Health Care (PHC). Vientiane, January 2000.MOH, JICA. Lao Health Master Plan Study, 2002.Lao PDR, National Assembly. Law on Health Care. Vientiane, 11 November 2005.Lao PDR, Committee for Planning and Investment. National Socio-Economic Development Plan (2006-2010). Vientiane, Oct 2006.Ministry of Health, Lao PDR. Decision of the Minister of Health on the organizational structure & activities of Health Centres. Vientiane, Oct 5, 2006.Lao PDR, MoH, Mid-term review of 6th 5-year Health Sector Plan of Lao PDR. Vientiane, 2008.Unger JP, Criel B. Principles of health infrastructure planning in less developed countries. International Journal of Health Planning and Management, 1995; 10(2):113-28.Van Lerberghe W, Lafort Y. The role of the hospital in the district; delivering or supporting primary health care? Current Concerns SHS Papers, 1990:1–36 (WHO/SHS/CC/90.2)WHO. Alma Ata declaration, (1978).WHO (1987). Report on the Interregional Meeting on Strengthening District Health Systems based on Primary Health Care. (Declaration of Harare). Harare, Zimbabwe, 3-7 August 1987.WH0, The Challenge of Implementation: District Health Systems for Primary Health Care. 1988, WHO/SHS/DHS/88.1/rev.1WHO, World Health Report 2000. Health Systems: improving performance. Geneva, 2000.WHO, World Health Report 2003. Chapter 7. Health Systems: principled integrated care. Geneva 2003.WHO, Strengthening Health Systems to improve health outcomes. Geneva, 2007.WHO, World Health Report 2008. Primary Health Care, now more than ever. Geneva.De Brouwere V, Van Balen H. Hands-on training in health district management. World Health Forum, Volume 17, Issue 3, 1996. Pages 271-273.Wasunna Owino, Paul Odundo, Timothy Oketch. Governance of the District Health Systems: A Focus on the Health Management Boards and Human Resource Development Issues, 2001, Institute of Policy Analysis and Research.Bossyns P. The Referal System: a neglected element in the health district concept. Thesis PhD, Free University of Brussels. Brussels, June 2006.Bosch-Capblanch X, Garner P (2008). Primary health care supervision in developing countries; systematic review. Trop Med Intl Health, vol 13, nr 3; pp 369-383, March 2008.Knowles, M. (1984). Andragogy in Action. San Francisco: Jossey-Bass.
WEBSITES
http://www.who.int/management/en/ (health systems management)
http://www.who.int/management/supervision/en/index.html (supervision)
http://www.wpro.who.int/health_topics/health_systems/ (WHO WPR on health systems)
http://www.afro.who.int/dsd/dhm-training/index.html (district systems)
http://www.btcctb.org/ (BTC website)
http:// www.ncqa.org/ and http://erc.msh.org/quality (quality of care)
http://en.wikipedia.org/wiki/Andragogy (adult learning)
http://en.wikipedia.org/wiki/PDCA (Mr Deming and PDCA cycle)
(1)(2)(3)(4)
(5)
(6)(7)
(8)
(9)(10)
(11)
(12)(13)(14)(15)(16)
(17)
(18)
(19)
(20)
43
REFERENCES

Editor:
Project Coordinating Unit, Lao-Belgian Health Project, Ministry of Health, PO Box 7,019, Vientiane, Laos
Tel. + 856 (0)21 216 213 ; Fax + 856 (0)21 253 029
In collaboration withSchool of Public HealthFree University of BrusselsBelgium