lecture 16 esophagus and stomach disorders - pathology
TRANSCRIPT

441
Esophagus & Stomach Disorders
Lecture 16
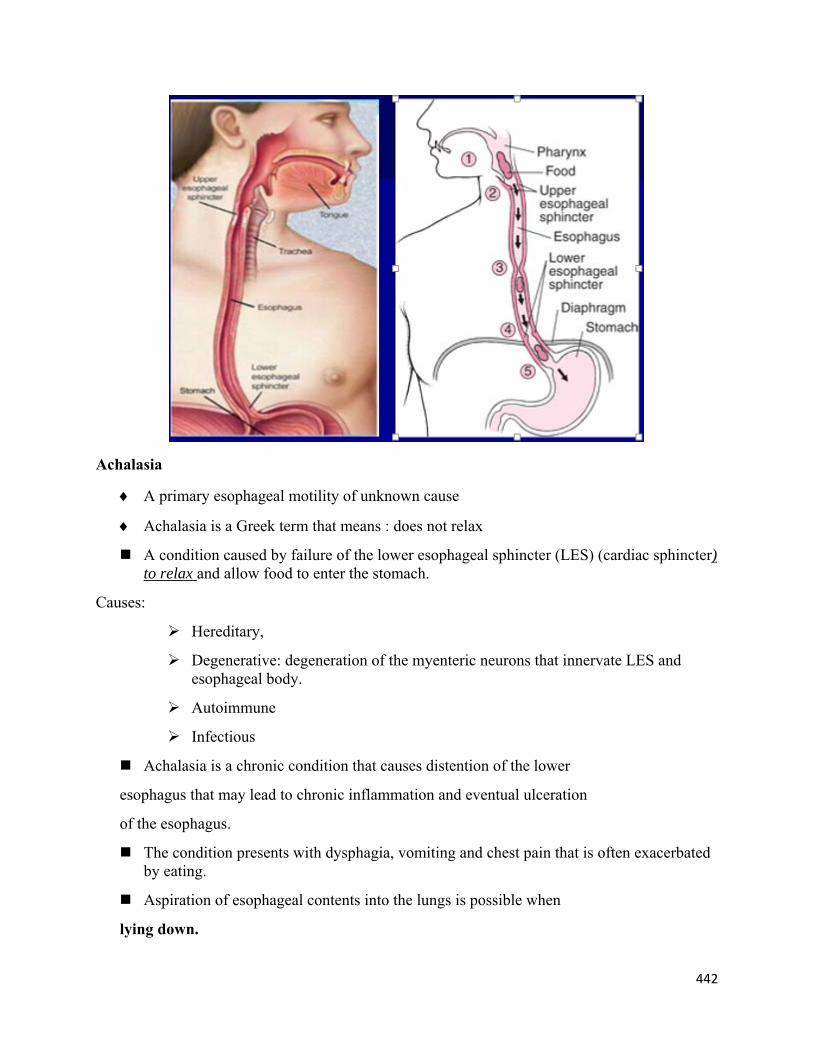
The esophagus
From mouth to stomach, the food tube consists of the oral cavity, pharynx, and esophagus.
The esophagus is very muscular and collapses when empty. It serves as a dynamic tube, pushing food toward the stomach.
The esophagus is posterior to the trachea
It is 18-25cm in length.
The esophageal lining is protected by a stratified squamous epithelium. The scattered submucosal mucous glands provide lubrication.
It serves as a wet lining capable of withstanding relatively moderate abrasive stresses.
The esophagus produces bicarbonate and mucus
The bicarbonate buffers the acid and mucus forming a “protective barrier”.
This creates an environment in the esophagus of a higher pH than that of the stomach.
The pH in the esophagus is normally about 7-8, whereas the pH in the stomach is generally 2-4.
The word esophagus which derives from the Greek word oisophagos, which means "to carry to eat."
The esophagus is divided into:
1) Upper: It has a sphincter to prevent air from entering the esophagus during respirations. The sphincter generally only opens for food to pass.
2) Lower: It has a sphincter that opens while food is being passed into the stomach. It is known as the LES, lower esophageal sphincter.
442
Achalasia
A primary esophageal motility of unknown cause
Achalasia is a Greek term that means : does not relax
A condition caused by failure of the lower esophageal sphincter (LES) (cardiac sphincter) to relax and allow food to enter the stomach.
Causes:
Hereditary,
Degenerative: degeneration of the myenteric neurons that innervate LES and esophageal body.
Autoimmune
Infectious
Achalasia is a chronic condition that causes distention of the lower
esophagus that may lead to chronic inflammation and eventual ulceration
of the esophagus.
The condition presents with dysphagia, vomiting and chest pain that is often exacerbated by eating.
Aspiration of esophageal contents into the lungs is possible when
lying down.

443
Esophageal diverticulum
Diverticula are out pocketings of the esophageal walls that occur most frequently from congenital weakness of the esophagus walls.
Food can easily become trapped in these diverticula, leading to inflammation and infection of the esophagus with possible ulceration.

444
Dyspepsia: (Indigestion)
Dyspepsia refers to persistent or recurrent epigastric pain or subjective upper abdominal discomfort that may be characterized by: Early satiety Postprandial fullness Bloating Nausea Hiccups Belching Flatulence Heartburn.
Dyspepsia is not restricted to meal-related symptoms because patients with P.U.D often report pain unrelated to meals.
Dyspepsia is characterized as:
“Reflux-like “,If heartburn or chest pain predominate.
“Ulcer-like”;if the characteristics convey the impression of P.U.D. such as epigastric pain related to meals or waking the patient from sleep . This can be confirmed by the presence of H. Pylori in the gastric antrum.
“Non-ulcer dyspepsia “describes similar symptoms in the absence of H. pylori.
Esophagitis
Inflammation of the esophagus
Starts in the mucosa
Causes: Intubation Corrosoives, irritant, acidity Chemotherapy Reflux esophagitis Hiatal hernia infections

445
Lower Esophageal Sphincter (LES)
The LES at the esophagogastric junction , is a 2 cm to 4.5 cm long, consists of tonically contracted of smooth muscle at approx. 8-20 mmHg above the gastric pressure.
At rest, the sphincter is tonically contracted with normal pressure ranging from 10 mm to 45 mm Hg.
On swallowing, the LES relaxes promptly in response to the initial neural discharge from the swallowing center. During relaxation, the pressure falls approximately to the level of gastric pressure.
The LES serves two functions: o prevents gastroesophageal reflux o relaxes with swallowing, allowing movement of ingested material into the
stomach.
Gastroesophageal Reflux Disease (GERD)
Gastroesophageal reflux is a normal physiologic phenomenon experienced intermittently by most people, particularly after a meal.
Gastroesophageal reflux disease :
o Symptoms OR mucosal damage produced by the abnormal reflux (the amount exceeds the normal limit ) of gastric contents into the esophagus
o Often chronic and relapsing
o May see complications of GERD in patients who lack typical symptoms
REFLUX is derived from Greek:
Retro – Back Flux – Flow

446
Physiologic vs Pathologic
Physiologic GERD: Postprandial, Short lived, Asymptomatic, No nocturnal symptoms.
Pathologic GERD: Symptoms, Mucosal injury, Nocturnal symptoms.
Pathophysiology of GERD
GERD occurs when there is a disruption of normal protective mechanisms.
Protective mechanisms include:
Potent Lower Esophageal Sphincter (LES): it forms a complex anti-reflux barrier located in the gastroesophageal junction. It prevents the acid reflux into the esophagus
Production of bicarbonate and saliva, which neutralize refluxed acid,
Esophageal clearance (caused by gravity and peristalsis), which minimizes the contact time between acid and the esophageal mucosa following a reflux event.
The Disruption of the normal protective mechanisms is due to:
1) Impaired lower esophageal sphincter :
o low pressures
o or frequent transient lower esophageal sphincter relaxation (TLESRs)
o or Abnormal location (Hiatal Hernia)
2) Hypersecretion of acid
3) Decreased acid clearance resulting from impaired peristalsis or abnormal saliva production
4) Delayed gastric emptying or duodenogastric reflux of bile salts and pancreatic enzymes.
5) Increase abdominal pressure:
Obesity - “excess weight puts extra pressure on the stomach & diaphragm”.
Pregnancy – “results in greater pressure on the stomach & also has a higher level of progesterone. This hormone relaxes many muscles, including the LES”.
Asthma – it is unsure why, but, is believed that the coughing leads to pressure changes on the diaphragm.
Increased gastric volume
• Smoking: lowers LES pressure and the acid-neutralising effect of saliva. • Physical activity :( running) might provoke GERD by increasing TLESRs

447
Typical Symptoms
Common symptoms most common when pH<4
• Heartburn
• Belching and regurgitation
• Hypersalivation
May be episodic or nocturnal
May be aggravated by meals and reclining position
Atypical Symptoms
Nonallergic asthma
Chronic cough
Hoarseness
Pharyngitis
Chest pain (mimics angina)

448
Hiatal Hernia
A hiatal hernia is an anatomical abnormality in which part of the stomach protrudes through the diaphragm and up into the chest.
It is present in approximately 15% of the population (symptoms in only a minority of those afflicted)
Hiatal hernias in adults are believed to have developed over many years.
Normally, the esophagus passes down through the chest, crosses the diaphragm, and enters the abdomen through a hole in the diaphragm called the esophageal hiatus.
Just below the diaphragm, the esophagus joins the stomach.
In individuals with hiatal hernias, the opening of the esophageal hiatus (hiatal opening) is larger than normal, and a portion of the upper stomach slips up or passes (herniates) through the hiatus and into the chest.
Clinical Presentation of GERD (explanation of the table)
Choking (احساس باالختناق ) : is a term frequently used to describe the feeling of food sticking in the esophagus or coughing.

449
Regurgitation : refers to the return of undigested food or liquid back to the mouth from the pharynx, or esophagus.
Belching (التجشؤ) : is the act of expelling air from the stomach through the mouth
Dysphagia :Difficulty swallowing that may be caused by obstruction of the esophagus or impaired motility of the esophageal walls.
Odynophagia :is painful swallowing
If Warning (Alarm) symptoms present, consider an endoscopy

450
Barrett’s Esophagus
Barrett esophagus is a complication of chronic GERD (5-15%) that is characterized by intestinal metaplasia within the esophageal squamous mucosa.
Barrett esophagus is defined as the replacement of the normal distal stratified squamous mucosa by columnar epithelium containing goblet cells which secrets mucus, that makes it more resistant to the acid coming up from the stomach.
Metaplastic columnar epithelium develops during healing of erosive esophagitis with continued acid reflux because columnar epithelium is more resistant to acid-pepsin damage than is squamous epithelium.

451
Barrett's esophagus is arbitrarily divided into long-segment (>2–3 cm) or short-segment (<2–3 cm) groups; long-segment disease is present in 0.5% of the population and short-segment disease may occur in up to 15%.
Barrett esophagus is a pre-malignant condition; it confers an increased risk of esophageal adenocarcinoma by 30-60 times.
It increases the risk of the esophageal strictures by 30-80%.
Diagnosis of Barrett’s Esophagus
Clinical symptoms and history
• Presenting symptoms and associated risk factors
Give empiric therapy and look for improvement (Give proton pump inhibitors (PPI’s) once daily for 4 weeks).
Ambulatory 24 hr pH Monitoring :
o Esophageal pH monitoring is the current gold standard for diagnosis of GERD.
o It provides direct physiologic measurement of acid in the esophagus and is the most objective method to document reflux disease, assess the severity of the disease and monitor the response of the disease to medical or surgical treatment.
Endoscopy if warning signs present.

452
Ambulatory 24 hr pH Monitoring
Treatment
Three phases in treatment
Phase I: Lifestyle changes – 2 weeks
o Lifestyle modifications
o Patient-directed therapy with OTC medications
Phase II: Pharmacologic intervention
o proton pump inhibitors (PPI’s) for 4-8 weeks
o May also add a prokinetic/promotility agent
Phase III: Surgical intervention
o Patients who fail pharmacologic treatment or have severe complications of GERD
o LES positioned within the abdomen where it is under positive pressure
Lifestyle Modifications
Elevate the head of the bed 6-8 inches (15-20 cm)
Decrease fat intake
Smoking cessation
Avoid recumbency for at least 3 hours post-prandial

453
Weight loss
Limit alcohol intake
Wear loose-fitting clothing
Avoidance of aggravating foods
These changes alone may not control symptoms
Anatomy of the Stomach
Anatomically divided into 4 regions:
Cardiac region: o The cardia surrounds the superior opening of the stomach by esophageal
sphincter. Fundus: Lies against the diaphragm. Body (corpus):
o large central portion of the stomach, called the body. The region of the stomach that connects to the duodenum is the pylorus.
o It has two parts, the pyloric antrum, which connects to the body of the stomach, and the pyloric canal, which leads into the duodenum.
o The pylorus communicates with the duodenum of the small intestine via the pyloric sphincter (valve).

454
Gastric Glands

455
Several kinds of cells are found in the gastric glands : o Mucous neck cells : secrets thick Mucus, alkaline in nature, which protects
the tissue from the acid content o Surface mucous cells ( Goblet Cells) : secrets Mucus o Parietal: secrets Hydrochloric acid and intrinsic factor (IF) o Chief (peptic or zymogenic cells) secrets Pepsinogen o Endocrine: secrets Gastrin, a hormone that regulates gastric secretions.
Gastrin is secreted by the G (gastrin) cells of the pyloric glands in response to the presence of proteins (usually meat).
Physiology of the Stomach
The contents of the stomach are very acidic.
This acidity provides protection to the body from infection from organisms eaten in food.
It also helps digest and break down food before it enters the small intestine (duodenum).
The lining of the stomach and duodenum is covered by a protective mucous layer (a thick, smooth fluid) which prevents the acid from injuring the wall of the stomach.
Damage to the lining from the acid can result when the stomach produces excess acid or there is insufficient mucus.
Gastritis
The highly acidic gastric environment may be one reason why infectious processes of the stomach are rare.
The term gastritis should be reserved for histologically documented inflammation of the gastric mucosa
It is may be acute or chronic gastritis.

456
Acute Gastritis
Acute gastritis refers to a transient inflammation of the gastric mucosa. It is most commonly associated with local irritants such as bacterial endotoxins (such as
the staphylococcal enterotoxins), caffeine, alcohol, and aspirin. Acute infection with H. pylori induces gastritis. However, H. pylori acute gastritis has
not been extensively studied. Depending on the severity of the disorder, the mucosal response may vary from moderate
edema and hyperemia to hemorrhagic erosion of the gastric mucosa. Neutrophils are the predominant inflammatory cell in the superficial epithelium. Clinical presentation with sudden onset of epigastric pain, nausea, vomiting, heartburn
or sour stomach. Acute gastritis usually is a self-limiting disorder; complete regeneration and healing
usually occur within several days.
Chronic Gastritis
Chronic gastritis is identified histologically by an inflammatory cell infiltrate consisting primarily of lymphocytes and plasma cells, with very scant neutrophil involvement.
The final stage of chronic gastritis is gastric atrophy; Glandular structures are lost, also there is a loss of inflammatory infiltrates.
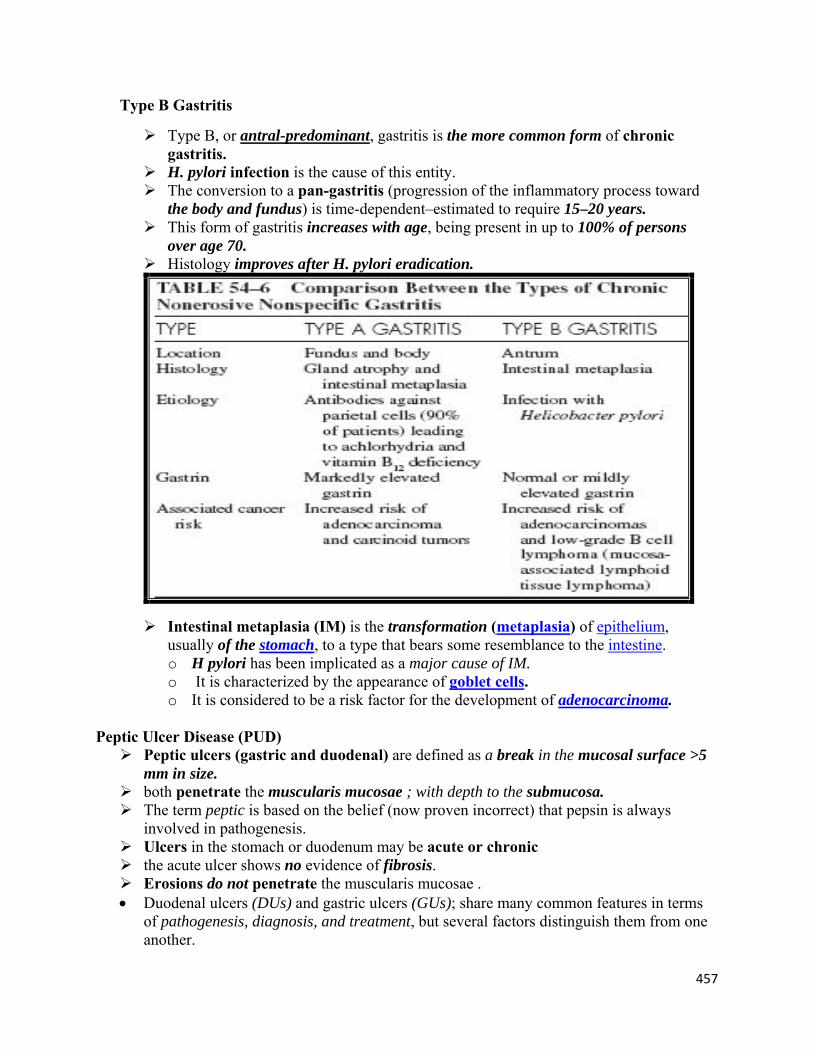
Chronic gastritis is also classified according to the predominant site of involvement: o Type A Gastritis o Type B Gastritis
Type A Gastritis
The less common of the two forms involves primarily the fundus and body, with antral sparing.
Traditionally, this form of gastritis has been associated with pernicious anemia in the presence of circulating antibodies against parietal cells and IF; thus, it is also called autoimmune gastritis.
Antibodies to parietal cells have been detected in >90% of patients with pernicious anemia and in up to 50% of patients with type A gastritis.
The parietal cell–containing gastric gland is preferentially targeted in this form of gastritis, and achlorhydria results.
Parietal cells are the source of IF, lack of which will lead to vitamin B12 deficiency and its sequelae (megaloblastic anemia, neurologic dysfunction).
Gastrin levels can be markedly elevated (>500 pg/mL) in patients with pernicious anemia. (Normal Serum gastrin levels have a reference range of 0-100 pg/mL.)
Gastrin is a peptide hormone that stimulates secretion of gastric acid (HCl) by the parietal cells of the stomach and aids in gastric motility. It is released by G cells in the antrum of the stomach, duodenum, and the pancreas.
457
Type B Gastritis
Type B, or antral-predominant, gastritis is the more common form of chronic gastritis.
H. pylori infection is the cause of this entity. The conversion to a pan-gastritis (progression of the inflammatory process toward
the body and fundus) is time-dependent–estimated to require 15–20 years. This form of gastritis increases with age, being present in up to 100% of persons
over age 70. Histology improves after H. pylori eradication.
Intestinal metaplasia (IM) is the transformation (metaplasia) of epithelium, usually of the stomach, to a type that bears some resemblance to the intestine. o H pylori has been implicated as a major cause of IM. o It is characterized by the appearance of goblet cells. o It is considered to be a risk factor for the development of adenocarcinoma.
Peptic Ulcer Disease (PUD) Peptic ulcers (gastric and duodenal) are defined as a break in the mucosal surface >5
mm in size. both penetrate the muscularis mucosae ; with depth to the submucosa. The term peptic is based on the belief (now proven incorrect) that pepsin is always
involved in pathogenesis. Ulcers in the stomach or duodenum may be acute or chronic the acute ulcer shows no evidence of fibrosis. Erosions do not penetrate the muscularis mucosae . Duodenal ulcers (DUs) and gastric ulcers (GUs); share many common features in terms
of pathogenesis, diagnosis, and treatment, but several factors distinguish them from one another.

458
Sites of P.U.D 1. Lower esophagus 2. Stomach 3. Duodenum (1st part of duodenum called duodenal bulb) 4. Jejunum after surgical anastomosis to the stomach 5. rarely, in the ileum adjacent to a Meckel's diverticulum (containing areas of ectopic
gastric mucosa) 6. Small intestine (Postbulbar :2nd part of duodenum bulb or in the Jejunum) called
Gastrinoma (Zollinger-Ellison Syndrome) characterized by: Gastric acid Hypersecretion ( Elevated level of HCl) Hypergastrinemia ( Elevated level of Gastrin) Diarrhea Severe Peptic Ulceration

459
Pathology of PUD Duodenal Ulcers DUs occur most often in the first portion of duodenum (>95%). With 90% located within 3 cm of the pylorus. They are usually 1 cm in diameter but can occasionally reach 3 to 6 cm (giant ulcer). Ulcers are sharply demarcated, with depth at times reaching the muscularis propria. The base of the ulcer often consists of a zone of eosinophilic necrosis with
surrounding fibrosis. Malignant duodenal ulcers are extremely rare.
Gastric Ulcers In contrast to DUs, GUs can represent a Malignancy. Benign GUs :
o most commonly in the antrum (60%) and at the junction of the antrum and body on the lesser curvature (25%).
o rare in the gastric fundus and are histologically similar to DUs. o Benign GUs associated with H. pylori are associated with antral gastritis.
In contrast, NSAID-related GUs are not accompanied by chronic active gastritis but may instead have evidence of a chemical gastropathy.

460
Pathophysiology of PUD P.U.D is the end result of an imbalance between aggressive and defensive factors in the
gastroduodenal mucosa. The most important contributing factors (aggressive) for developing PUD are:
1. H pylori infection. 2. NSAIDs. 3. Acid. Average basal and nocturnal gastric acid secretion appears to be increased
in DU patients. Gastric acid output (basal and stimulated) tends to be normal or decreased in GU patients.
4. Pepsin. 5. Additional aggressive factors include
1. smoking, ethanol, bile acids, 2. aspirin, steroids, and stress. (Stress – In the past, stress and emotion were felt to be a major cause of
ulcers. Now it is known that, by itself, stress rarely causes an ulcer although it probably can aggravate the symptoms)
Important protective or defensive factors are: 1. Mucus: Provides barrier from hostile factors. 2. Bicarbonate: Neutralizes acid . (Bicarbonate secretion is significantly decreased
in the duodenal bulb of patients with an active DU as compared to control subjects. H. pylori infection may also play a role in this process).
3. Mucosal blood flow: Delivers bicarbonate to surface epithelium. 4. Prostaglandins :
Prostaglandins are derived from esterified arachidonic acid, which is formed from phospholipids (cell membrane) by the action of phospholipase A2.
Prostaglandins Maintains mucosal blood flow and stimulates secretion of mucus & bicarbonate
5. Specialized acid-resistant apical surface membrane: Resist diffusion of acid into the mucosa.
6. Epithelial renewal.

461
Symptoms of PUD
Epigastric pain o Gnawing or burning o Occurs 1-3 hours after meals o Relieved by food or antacids (DU) or by Vomiting (GU) o Might occur at night o Might radiate to back (consider penetration)
Nausea Vomiting, which might be related to partial or complete gastric outlet obstruction Dyspepsia, including belching, bloating, distention, fatty food intolerance Dyspeptic symptoms that might suggest PUD are not specific because only 20-25% of
patients with symptoms suggestive of peptic ulceration are found on investigation to have a peptic ulcer.
Heartburn Chest discomfort Anorexia, weight loss Hematemesis or melena resulting from gastrointestinal bleeding

462
Epigastric pain
Helicobacter Pylori (H. pylori)
A gram – negative bacterium, microaerophilic (lives in reduced oxygen environment) Named because of its spiral or helical shape . It has up to 7 sheathed Flagella . Highly
motile. Corkscrew like movement, easy to penetrate the mucosal gel. H. pylori lives in gastric antrum; below the gastric mucus over the gastric epithelium. Re- (discovered) by Warren and Marshall in Perth( Australia) 1982. The cause of 95% of D.U., 80% of G.U. Transmission: Person –to-person; the primary route is fecal-oral route. Oral –to-Oral
transmission has not been documented. Risk factors for H. Pylori infection: Birth in developing country. Low socioeconomic
states. Crowded living and large families. Poor sanitary living condition.

463
Pathophysiology of the H. pylori infection H. pylori has multiple flagella at one end which make it motile, allowing it to burrow and
live deep beneath the mucus layer closely adherent to the epithelial surface. It uses an adhesion molecule (BabA) to bind to the Lewis b antigen on epithelial cells. Here the surface pH is close to neutral and any acidity is buffered by the organism's
production of the enzyme urease. This produces ammonia from urea and raises the pH around the bacterium and between
its two cell membrane layers. H. pylori exclusively colonizes gastric-type epithelium and is only found in the
duodenum in association with patches of gastric metaplasia.

464
Helicobacter pylori is an etiologic agent for: Gastric ulcers Duodenal ulcers Adenocarcinomas of the distal stomach Gastric mucosa associated lymphoid tissue (MALT) lymphomas Chronic Gastritis ( Active Chronic Gastritis )
H. Pylori Diagnosis: Invasive ( requires Endoscopy منظار المعدة) :
o Histology: culture biopsy (test for antibiotic sensitivity). o Biopsy urease test (CLO test; Campylobacter- Like Organisms_ it gives rapid
results). Non –invasive tests :
o Serology: detect anti-H. pylori antibody; IgG in serum, for screening purpose; indicate exposure.
o Stool :detection of H. pylori antigen in the stool o Carbon labeled breath test: extremely accurate.
14C: weakly radioactive, cheap, cannot be used in children or pregnant women, neither reliable after gastric surgery.
13C: non-radioactive, expensive requires special facilities.

465
H. Pylori Treatment: Eradication of H. pylori has been shown to be definitive cure of DU and GU.
Non steroidal anti-inflammatory drugs ( NSAIDs) NSAIDs are one of the most widely used drugs, in U.S.A. alone, 60 million prescriptions
are written each year. These highly effective analgesic and anti-inflammatory agents are used to treat:
o Rheumatoid arthritis, acute gout, ankylosing spondylitis, and osteoarthritis. NSAIDs produce their anti-inflammatory effects by blocking Prostaglandin synthesis. The cause of the Gastric mucosal damage (ulceration, bleeding, perforation) is
through the systemic effect of NSAIDs in inhibition of prostaglandin synthesis, even when administration is not oral but I.M., I.V. subcutaneous , or by rectal suppository.
Risk factors for NSAIDs gastropathy ( Damage of the gastric mucosa)are: o Advanced age. o Prior gastric ulcer o Concurrent corticosteroid use. o High dose and combination NSAIDs therapy. o Smoking.

466
PUD Complications 1) Hemorrhage
Most common complication of peptic ulcer disease Develops from erosion of Granulation tissue found at base of ulcer during healing Ulcer through a major blood vessel Patients with ulcer bleeding may report :
Hematemesis is the vomitus of bright red blood or “coffee-ground” material Melena is black, tarry stool, which is foul smelling because of the presence of
partially digested blood products. Melena implies that the blood has been in the GI tract for at least 14 hours, & that usually indicates an upper GI source, but melena may also occur with bleeding from the small bowel or the right colon.
Weakness Orthostatic syncope : a sense of passing out upon standing
Initial treatment involves rapid replacement of lost blood intravenously, usually with fluids.
Patients with persistent or severe bleeding may require blood transfusions. An endoscopy is performed to establish the site of bleeding and to stop active ulcer
bleeding with the aid of specialized endoscopic instruments

467
2) Penetration (confined perforation):
A peptic ulcer may penetrate the wall of the stomach. The adhesions prevent leakage into the peritoneal cavity. the ulcer may penetrate into the duodenum and enter another organ (eg, pancreas, liver). Pain may be intense, persistent, referred to sites other than the abdomen (usually the
back when caused by penetration of a posterior duodenal ulcer into the pancreas), and modified by body position.
CT or MRI is usually needed to confirm the diagnosis. When therapy does not result in healing, surgery is required.
3) Free perforation:
Most lethal complication of peptic ulcer Commonly seen in large penetrating duodenal ulcers that have not healed and are
located on posterior mucosal wall Perforated gastric ulcers often located on lesser curvature of stomach The patient presents with an acute abdomen. There is sudden, intense, continuous
epigastric pain that spreads rapidly throughout the abdomen, often becoming prominent in the right lower quadrant and at times referred to one or both shoulders.
4) Gastric Outlet Obstruction
Ulcers located in antrum and prepyloric and pyloric areas of stomach Obstruction leads to narrowing of pylorus Vomiting Constipation Dehydration May show swelling in upper abdomen
5) Recurrence:
Factors that affect recurrence of ulcer include : Failure to eradicate H. pylori, continued NSAID use, and smoking. The 3-yr recurrence rate for gastric and duodenal ulcers is < 10% when H. pylori is
successfully eradicated but > 50% when it is not. Thus, a patient with recurrent disease should be tested for H. pylori and treated again if the tests are positive.
Although long-term treatment with H2 blockers or proton pump inhibitors reduces the risk of recurrence, their routine use for this purpose is not recommended.
However, patients who require NSAIDs after having had a peptic and those with a marginal ulcer or prior perforation or bleeding ulcer are candidates for long-term therapy.
6) Stomach cancer:
Patients with H. pylori–associated ulcers have a 3- to 6-fold increased risk of gastric cancer later in life. There is no increased risk of cancer with ulcers of other etiology.

468
DU & GU seen by Endoscopy called Gastroscopy منظار المعدة
---------------------------------