lecture 7: reproductive and developmental toxicology (yager)
TRANSCRIPT

Copyright 2008, The Johns Hopkins University and James Yager. All rights reserved. Use of these materials permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for obtaining permissions for use from third parties as needed.
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this site.

Reproductive and Developmental Toxicology
James D. Yager, PhD Johns Hopkins University

3
Outline
Introduction and general principles– Reproductive toxicology– Developmental toxicologyCase studies– 1,2-Dibromo-3-chloropropane– Estrogens– Thalidomides

Section A
General Principles of Reproductive Toxicology

5
Frequencies of Selected Reproductive Failures
Frequency Event
Per 100 Unit
Failure to conceive after one year 10–15 Couples
Spontaneous abortion 8–28 weeks 10–20 Pregnancies or women
Chromosome anomalies in spontaneous abortions, 8–28 weeks
30–40
Chromosome anomalies from amniocentesis, > 35 years 2 Amniocentesis specimen
Stillbirths 2–4 Stillbirths and live births
Birth weights < 2,500 g 7 Live births
Birth defects 2–3 Live births
Chromosome anomalies, live births 0.2 Live births
Severe mental retardation 0.4 Children to age 15 years

6
General Principles Reproductive Toxicology
What is it?– Study of the recurrence, causes,
manifestations, and sequalae of adverse effects of exogenous agents on reproduction
Reproductive ToxinsTargets for chemical toxicityReproductive toxicity endpoints

7
Reproductive Toxins: Drugs, Environmental Chemicals
Drugs that Are Gonadotoxic in Humans
Males Females
Bisulfan Bisulfan
Chlorambucil Chlorambucil
Cyclophosphamide Cyclophosphamide
Nitrogen mustard Nitrogen mustard
Adriamycin
Corticosteriods
Cystosine arabinoside
Methotrexate
Procarbazine
Vincristine
Vinblastine

8
Environmental Chemical ExposureEnvironmental Chemical Exposure Associated with Reproductive Function
Males Females Carbon disulfide Anesthetic gas (OR personnel) Chlordecone (Kepone) Aniline Chloroprene Benzene Dibromochloropropane (DBCP) Carbon disulphide Ethylene dibromide Chloroprene Ethylene oxide Ethanol consumption Ethanol consumption Ethylene oxide Glycol ethers Glycol ethers Hexane Formaldehyde Inorganic lead (smelter emissions) Inorganic lead (smelter emissions) Organic lead Organic lead Pesticides (occupational exposure) Methyl mercury Vinyl chloride Pesticides (occupational exposure) Phthalic acid esters (PAEs) Polychlorinated biphenyls (PCBs)

9
Neuroendocrine Targets for Reproductive Toxins
CNS
Hypothalamus
AnteriorPituitary
Testis/Ovary
+ GnRH
Trophic HormonesFSHLH +
Testis/Ovary-derived HormonesTestosterone
EstrogenInhibin
-
GnRH Inhibitor
-

10
Reproductive Tissue
Sertoli cells (blood-testes barrier)Leydig cells (production of testosterone)

11
Reproductive Tissue: Testis/Seminiferous Tubules
Public Domain

12
Reproductive Tissue—Testis
Histological section through testicular parenchyma of a boar.
1 = Lumen of seminiferous tubules2 = spermatids3 = spermatocytes4 = spermatogonia5 = Sertoli cell6 = Myofibroblasts7 = Leydig cells8 = capillaries
Creative Commons BY-SA. Mickael Haggestrom.

13
Reproductive Tissue
Leydig cells locatedIn this layer
Form the Blood-TestisBarrier

14
Reproductive Tissue - Testis

15
Primary FollicleThis section is from an ovary of a woman of childbearing age. It demonstrates typical swirling ovarian stroma and primary follicles, each of which consists of a primary oocyte surrounded by a single layer of cuboidal epithelial cells (granulosa cells). Two of the primary follicles are well- preserved and 2 have been distorted in tissue processing.
Image used with permission from Brown Medical School Digital Pathology. All Rights Reserved.

16
Reproductive Tissue - Ovary

17Exposure
Control
60
50
40
30
20
10
300 mg/kg 500 mg/kg
Number of small folliclesNumber of medium folliclesNumber of large follicles
Ovarian Follicle counts in MiceFed Nitrofurantoin for 43 weeks
Num
ber o
f Fol
licle
s
0
Reproductive Tissue - Ovary

18
Reproductive Toxicity Endpoints
Reproductive endpoints indicating reproductive dysfunction– Decreased libido:
Impotence– Sperm abnormalities:
Decreased number/motility: Morphology
– Subfecundity• Abnormal
gonads/ducts of external genitalia
• Abnormal pubertal development
• Infertility of male/female
• Amenorrhea• Anovulatory cycles• Delay in
conception

19
Reproductive Toxicity Endpoints
– Illness during pregnancy/parturition : toxemia: Hemorrhage
– Early fetal loss (to 28 weeks)
– Late fetal loss (after 28 weeks)/stillbirth
– Intrapartum death– Death in first week– Decreased birth
weight
– Gestational age at delivery; prematurity; postmaturity
– Altered sex ratio; chromosome abnormalities
– Multiple births; birth defects
– Infant death– Childhood morbidity;
childhood malignancies

Section B
General Principles of Developmental Toxicity
21
A birth defect is "any anomaly, functional or structural, that presents in infancy or later in life and is caused by events preceding birth, whether inherited, or acquired."
--March of Dimes
Causes of Birth Defects

22
Pregnancy& Infant Health
Social Factors
Biological Factors Environmental Factors Genetics, gender, age Diet, tobacco, chemicals, radiation
Behavior, community, medical care
Birth Defects & Developmental Disorders
March of Dimes
Causes of Birth Defects

23
Hereditary disease
20%
Cytogeneticdisease 4%
Unknowncauses 70%
Birth trauma and uterine factors 1%
Maternal metabolic factors 1%
Maternal infection 2%
Drugs, chemicals and radiation 2%
Causes of Birth Defects

24
Toxic WindowsReproductive Exposure
Gametes Blastocyst Embryo FetusNEWBORN
(normal)
Sterility Death
Death Functional Abnormalities
NEWBORN(anomalies)
REPRODUCTIVEOUTCOME
Death
Structural Abnormalities

25
Toxic Windows: Stages of Embryogenesis

26
Expected Incidence of Malformation of Different Organs and Systems

27
Radiation Infections– Rubella virus– Cytomegalovirus– Herpes virus
hominis– Toxoplasmoisis– Syphilis
Maternal metabolic imbalances– Alcoholism– Cretinism– Diabetes– Folic acid
deficiency– Hyperthermia– Phenylketonuria– Rheumatic disease
Human Developmental Toxicants

28
Human Developmental Toxicants
Drugs and chemicals– Androgenic
chemicals– Antibiotics
Anticancer drugsAnticonvulsants– Diphenylhydantoin
, trimethadione
Anti-thyroid drugsChelators– Penicillamine
Chlorobiphenyls

29
Human Developmental Toxicants
Cigarette smokeCocaineCoumarinanticogulantsDiethylstilbesterolEthanolEthylene oxide
IodidesLithiumMetals– Mercury (organic)– Lead
RetinoidsThalidomide

30
PlacentaParent compound(Lipid soluble)
Parent compound(Lipid soluble)
Parent compound(Lipid soluble)
Parent compound(Lipid soluble)
Polar metabolites
Polar metabolites
Non-polar metabolites Non-polar metabolites
Maternal compartment Fetal compartment
Distribution of Xenobiotics Between the Fetal and Maternal Compartments

31
Placenta
Parent compound(Lipid soluble)
Parent compound(Lipid soluble)
Parent compound(Lipid soluble)
No compound
Polar metabolites
Maternal compartment Fetal compartment
Non-polar metabolites
Polar metabolites
Non-polar metabolites
Elimination
Elimination
Distribution of Xenobiotics Between the Fetal and Maternal Compartments

32
Developmental Toxicity Endpoints
Type I changes – Outcomes permanent, life-threatening and
frequently associated with gross malformations• Reduction of number of live births
(litter size)• Increased number of stillbirths• Increased number of resorptions• Increased number of fetuses with
malformations

33
Developmental Toxicity Endpoints
Type II changes – Outcomes, non-permanent, non-life
threatening, and not associated with malformations• Reduced birth weights• Reduced postnatal survival• Decreased postnatal growth, reproductive
capacity• Increased number of fetuses with retarded
development

34
Developmental Toxicology – Dose-Response Patterns
Dose-Response Patterns for Different Types of Developmental Toxicants

Section C
1,2-Dibromo-3-Chloropropane

36
Structure of DBCP and Tris-BP
1,2-Dibromo-3-Chrolopropane (DBCP) Structure and Uses
Br C C C Cl
H Br H
H H HO P O
O
H C HH C BrH C H
Br
C C C Br
H Br H
H H H
Br C C C
H Br H
H H H
O
DBCP
Tris-BP

37
1,2-Dibromo-3-Chrolopropane (DBCP): Reproductive Effects
From: Whorton et al. Infertility in Male Pesticide Workers, The Lancet, Dec. 17, 1977, 1259-1261.

38
Comparison of Non-Vasectomized DBCP Workers with Very Low (A)
and Normal (B) Sperm Counts
Group A Group B
Subjects (n) 11 11
Age (yr) 37.7 26.7
Exposure (yr) 8.0 0.08
Sperm Count (x106/ml) 0.2 93
FSH (mIU/ml) 11.3 2.6
LH (mIU/ml) 28.4 14.0
Testosterone (ng/dL) 459 463

39
Neuroendocrine Feedback
Hypothalamus

40
Proposed mechanism of prokaryotic and eukaryotic
toxicity
1,2-Dibromo-3-Chrolopropane (DBCP) Metabolism and Mechanisms of Toxicity
Prokaryotic mutations2-BromoacroleinP450
CH2 Br CHBr CH2 R R: Cl or
GSH S-Transferase
Episulfonium ion Eukaryotic DNA damage
Cell necrosis
C C Ch2Br
OH
O P (O CH2 Br CH2 Br)1 or 2
O
H C C C ClH H H
S+ HG
(S-9)

Section D
Estrogens
42
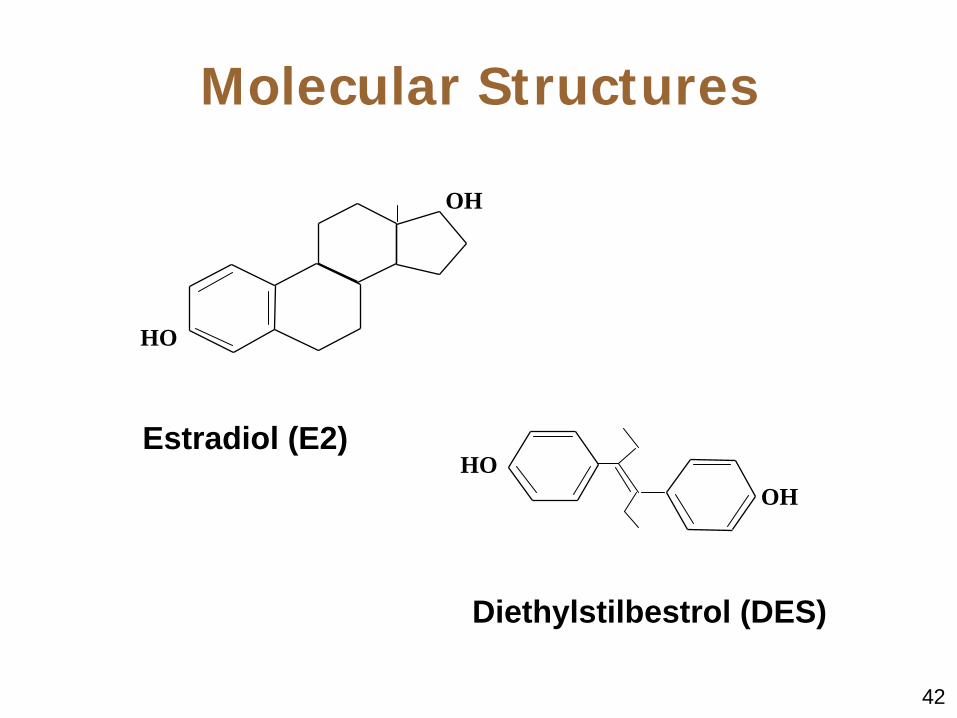
Molecular Structures
OHHO
HO
OH
Estradiol (E2)
Diethylstilbestrol (DES)

43
Diethylstilbesterol (DES)
Clinical use and adverse human health effects– Prevention of spontaneous abortion– Appearance of clear cell
adenocarcinoma of the vagina and cervix in exposed offspring of mothers treated during pregnancy
– Case-control study

44
No.Maternal Age (yr) Bleeding In This
PregnancyAny Prior
Pregnancy LossEstrogen Given In
This Pregnancy
Case Mean of 4 Controls Case Control Case Control Case Control
1 25 32 No 0/4 Yes 1/4 Yes 0/4
2 30 30 No 0/4 Yes 1/4 Yes 0/4
3 22 31 Yes 0/4 1/4 Yes 0/4
4 33 30 Yes 0/4 Yes 0/4 Yes 0/4
5 22 27 No ¼ 1/4 0/4
6 21 29 Yes 0/4 Yes 0/4 Yes 0/4
7 30 27 No 0/4 Yes 1/4 Yes 0/4
Total Mean 26.1 29.3 3/8 1/32 6/8 5/32 7/8 0/32
P <0.05 <0.01 <0.00001
DES: Case-Control Study – Summary of Data Comparing
Patients With Matched Controls

45
Diethylstilbesterol (DES)Incidence by Age of Clear Cell Adenocarcinoma at Diagnosis
among Native-born White Resident Female Subjects

46
Diethylstilbesterol (DES)
Effects of in utero exposure on human female progeny– Clear cell adenocarcinoma (malignant)– Adenosis (benign)—ectopic location of
glandular epithelium of the vagina and cervix

47
Diethylstilbesterol (DES)
Structural abnormalities of the cervicovaginal area including cervical collars, hoods, hypoplasia of the cervix– The significance of these abnormalities
is not known and some spontaneously regress with time
Structural abnormalities of the uterus

48
Diethylstilbesterol (DES)
Menstrual irregularitiesPossible adverse pregnancy outcomes including spontaneous abortions, ectopic pregnancies, and premature deliveryPossible increased risk for breast cancer (recent)

49
Diethylstilbesterol (DES)
Effects of in utero exposure on human male progeny– Anatomic abnormalities of the
reproductive tract– Altered semen including decreased
sperm density, count, and motility– Neoplasms of the reproductive tract not
widely reported

50
Human
Est
roge
n C
once
ntra
tion
Pregnancy (trimester)1 2 3
CP
Diethylstilbesterol (DES)
Mechanisms of DES toxicity: Critical period for estrogen exposure—toxicity window

51
Metabolism of Diethylstilbesterol (DES)
Mechanisms: Animal models– MouseSpecies differences in metabolism– Qualitatively similar, quantitatively
different

52
Female Genital Tract Tissue
OHHO
Phase I Metabolism
Reactive Metabolites
Robust Phase II Metabolism
Excretion
Conjugated Inactive Metabolites
OHHO
Phase I Metabolism
Reactive Metabolites
Little Phase II
Metabolism
Little conjugation and Excretion -
Retention of reactive metabolites
Liver Tissue
Metabolism of Diethylstilbesterol (DES)
Metabolism in male and female genital tract tissues– Data from mouse tissue in culture

53
Estrogenicity of DESDES is a potent estrogen
O2-•
Estrogen
2/4-OH-E2
ER
mRNAsP450sPeroxidases
ER
ER MAPK
ER = Estrogen receptor

54
Endocrine disruptors defined as:– An exogenous chemical substance or
mixture that alters the structure or function(s) of the endocrine system and causes adverse effects at the level of• Organism and its progeny• Populations• subpopulations
Environmental Endocrine Disruptors
55
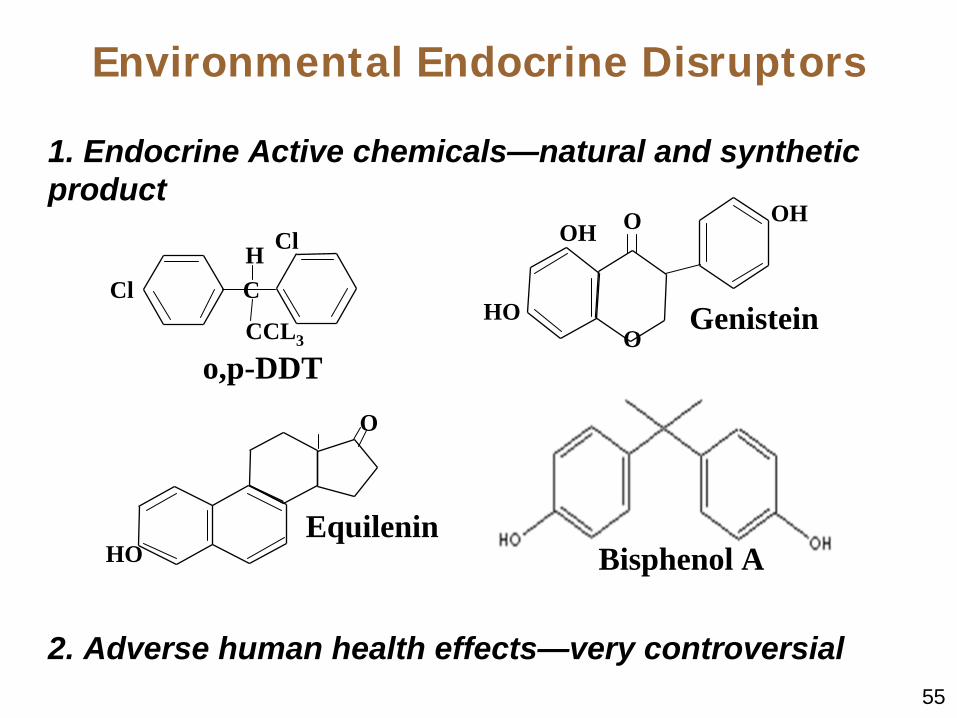
1. Endocrine Active chemicals—natural and synthetic product
2. Adverse human health effects—very controversial
Cl
Cl
C
CCL3
H
o,p-DDT
Environmental Endocrine Disruptors
OHOH
HOO
O
Genistein
HO
O
EquileninBisphenol A

56
Effects on wildlife– Alligators—Abnormal gonad
development and sex hormoneEffects on humans– Cancer?– Reproductive/developmental?Effects of combinations of environmental chemicals
Environmental Endocrine Disruptors

57
Environmental EstrogensAdverse reproductive effects
61 studies over 52 years suggest declining sperm counts. Circle size reflects relative number of subjects.
Source: adapted by CTLT from British Medical Journal, 1992.
Sper
m c
ou
nt
(x10
6 /m
l)
150
100
50
01930 1950 1970 1990

58
Environmental Endocrine Disruptors
1996 Congress passed the Food Quality Protection Act and amendments to the Safe Drinking Water ActBoth laws contained provisions requiring screening and testing of chemicals and pesticides for possible endocrine-disrupting effects– Estrogens (agonist/antagonist)– Androgens– Thyroid hormones

59
Endocrine Disruptor Screening Program
Revised Sept. 10, 1999; URL:http://www.epa.gov/scipoly/oscpendo/chart.htm
Environmental Endocrine Disruptors Prioritization for Testing
>

60
The Tier 1 Screening assays: To detect chemical substances capable of interacting with the estrogen, androgen, and thyroid hormonal systems. All known endocrine disruptor mechanisms for the estrogen, androgen and thyroid systems were included in the Tier 1 Screening battery. In Vitro assays include:
an estrogen receptor binding or reporter gene assay; an androgen receptor binding or reporter gene assay; and a steroidogenesis assay with minced testis.
In Vivo assays include: a rodent 3-day uterotrophic assay; a rodent 20-day pubertal female assay with enhanced thyroid endpoints; a rodent 5 to 7-day Hershberger assay; a frog metamorphosis assay; and a fish reproductive screening assay.
Results ->move the chemical into Tier 2 Testing or
conclude that no further screening or testing is needed at that time (Hold and periodically review).
Environmental Endocrine Disruptors Tier 1 Screening Assays

61
Tier 2 Testing: is designed to determine whether a chemical may have an effect similar to that of naturally occurring hormones and to identify, characterize, and quantify those effects for estrogen, androgen, and thyroid hormones. Conducting all five tests in the Tier 2 battery will provide the type of information necessary for endocrine disruptor hazard assessments for human health, fish, and other wildlife species.
Tier 2 tests will usually encompass two generations and will include effects on fertility and mating, embryonic development, sensitive neonatal growth and development, and transformation from the juvenile life stage to sexual maturity.
Tier 2 tests include: •a two-generation mammalian reproductive toxicity study or a less comprehensive alternative mammalian reproductive toxicity test; •an avian reproduction toxicity test; •a fish life cycle toxicity test; •an opossum shrimp (Mysidacea) or other invertebrate life cycle toxicity test; and •an amphibian development and reproduction test.
Environmental Endocrine Disruptors Tier 2 Testing

Section E
Thalidomide
63
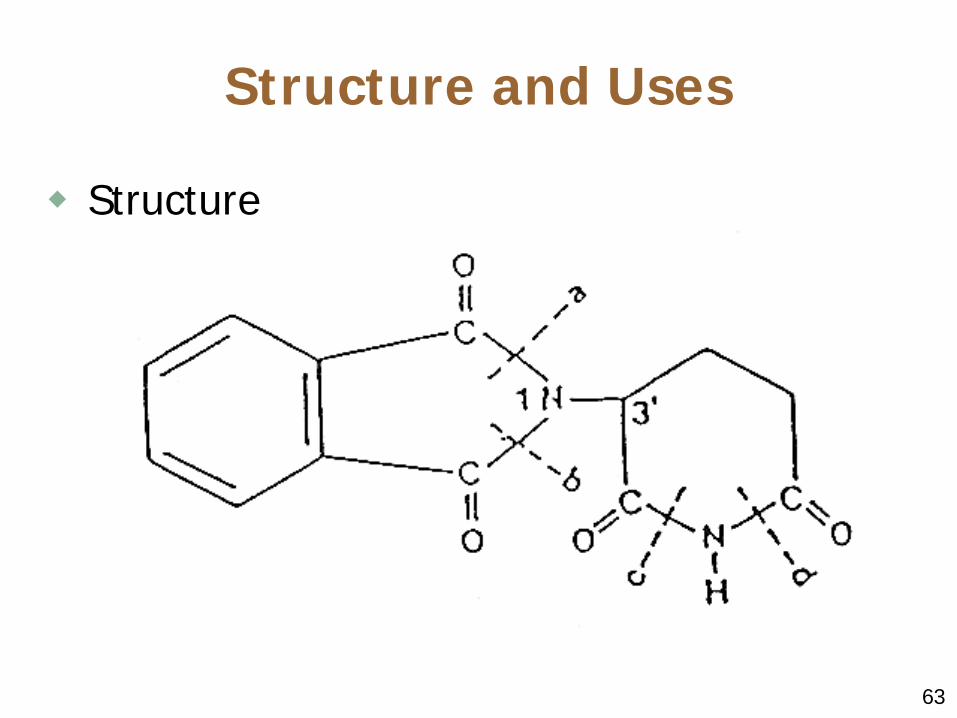
Structure and Uses
Structure

64
Structure and Uses
Chemical properties: Lipophilic, insoluble, and unstableClinical effects in rats– Sedation– Toxicity—LD 50

65
Comparison to Other Sedatives
Thalidomide was very potent, long-lasting and safe by these results
Comparison of Thalidomide to Other Sedatives
Smallest Hypnotic
Dose (mg/kg)
Start
of Effect (mins)
Duration
(mins)
Smallest Narcotic
Dose (mg/kg)
Initial
Excitation Stage
LD30
Thalidomide 100 5 240-300 >5,000 None >5,000 Luminal 40 30 300 150 ++ 300 Valamin 50 10 60 375 + 725 Doriden 75 30 200 400-500 ++ 600 Methylpentynol 150 15 210 500 + 750 Sodium bromide
500 80 360 7,000 None 800

66
Discovery of Side Effects
IntolerancePeripheral neuropathyBirth defects

67
Discovery of Side Effects

68
The Thalidomide Syndrome
10,000 childrenLimb defectsOther defects

69
Congenital Malformations Attributed to Thalidomide
In Humans System Affected Type of Malformation
Locomotor Amelia; phocomelia; micromelia, oligodactyly, syndactyly; club-hand; club-foot
Nervous Hydrocephalus; meningomyelocele; spina bifida
Cutaneous Hemangioma of the upper lip, glabella, and forehead
Ocular Microphthalmia; anophthalmia; coloboms
Auditory Deformed or absent pinna; atresia of the external canal; aplasia of the drum; low-set ears
Respiratory Choanal atresia; saddle nose; cleft palate; bilobular right lung

70
Congenital Malformations Attributed to Thalidomide
In Humans
System Affected Type of Malformation
Cardiovascular Aortic hypoplasia; transposition of the great vessels; atrial and ventricular septal defects; stenosis of the pulmonary artery; abnormal pulmonary veins
Gastrointestinal Atresia of the esophagus; pyloric stenosis; imperforate anus; absence of the gall bladder; atresia of the common bile duct
Urogenital Hypoplasia and aplasia of the kidney; horshoe kidney; hypoplasia and aplasia of the ureter; atresia of the vagina; bicornate uterus; aplasia of the uterus; recto-vaginal fistula
71
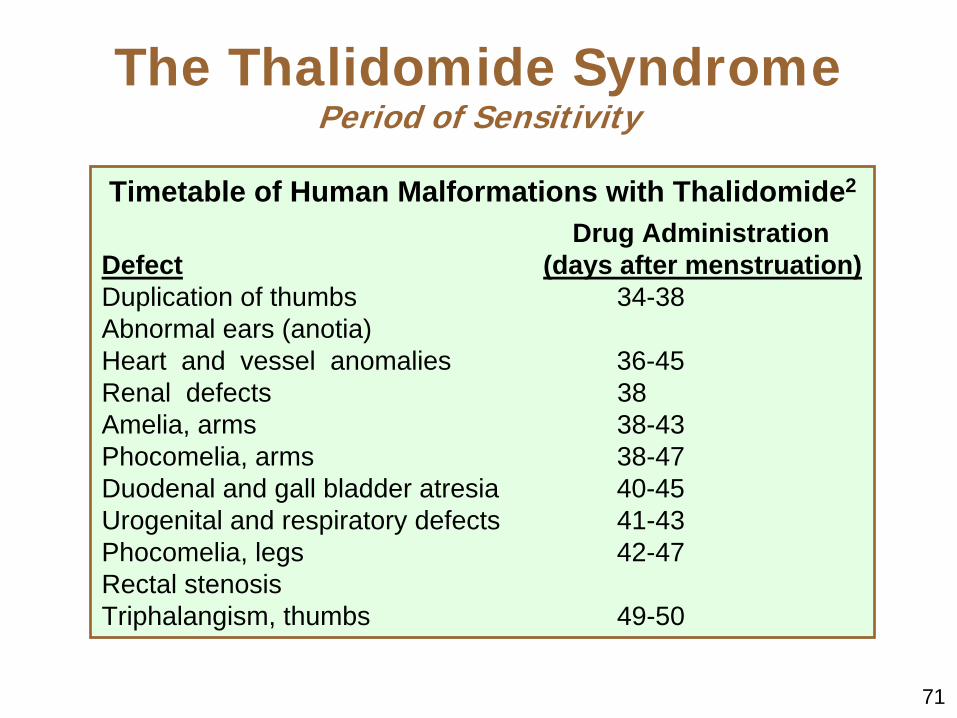
Timetable of Human Malformations with Thalidomide2
Drug Administration Defect (days after menstruation)Duplication of thumbs 34-38Abnormal ears (anotia)Heart and vessel anomalies 36-45Renal defects 38Amelia, arms 38-43Phocomelia, arms 38-47Duodenal and gall bladder atresia 40-45Urogenital and respiratory defects 41-43Phocomelia, legs 42-47Rectal stenosisTriphalangism, thumbs 49-50
The Thalidomide Syndrome Period of Sensitivity

72
The Thalidomide Syndrome
Laboratory studies: Sensitive periods of embryogenesisSpecies differences but positive in primates

73
Thailomide Syndrome
Thalidomide Teratogenesis in Primates Specie Teratogenic
dose mg/mg (oral)
Gestation days treated
Offspring with defects (type 1)
Cynomolgous monkey (crab eating) Macoca fascicularis
10 22-32 6/7 Limbs, teratomas
Rhesus monkey M. mulatta
12 24-30 3/6 Limbs
Stump-tailed monkey M. arciodes
5 24-30 5/5 Limbs and tail
Bonnet monkey M. radiata
5 24-44 13/29
Limbs and visceral
Japanese monkey M. fuscata
20 24-26 6/6 Limbs, tail and CNS

74
Thailomide Syndrome
Thalidomide Teratogenesis in Primates Specie Teratogenic
dose mg/mg (oral)
Gestation days treated
Offspring with defects (type 1)
Baboon Papio cynocephalus
5 18-44 4/10 Limbs and tail
Marmoset Callithrix jacchus
45 25-35 11/11
Limbs, ear and jaw
Green Monkey Cercopithecus aethiops
40 25-48 15/18
Limbs, skeleton and visceral
Bushbaby Galago crassicaudatus
_a 16-42 Limbs, ears
Human
2 21-36

75
Mechanisms of Action
Metabolism—Numerous spontaneous hydrolysis productsMechanisms—Trapped in fetal compartment?Current clinical uses

76
Current Clinical Uses
Thalidomide was once banned because it caused several birth defects, but researchers are discovering new uses; it:– Clears up lesions caused by a
complication of leprosy

77
– Seems to cure graft-versus-host disease in bone-marrow transplant recipients
– Appears to stop drastic weight loss in TB and AIDS patients
– Mechanism?• Immunomodulatory by unknown
mechanism
Current Clinical Uses

78
– Inhibits replication of the HIV-1 virus in vitro
– Could prevent the two leading causes of blindness• Glaucoma; Diabetic retinopathy
– May inhibit tumors– Mechanism of effect?
• Inhibition of blood vessel growth
Current Clinical Uses