length of incarceration: was there parity for mentally ill offenders?
TRANSCRIPT

International Journal of Law and Psychiatry
27 (2004) 387–393
Length of incarceration: Was there parity for mentally ill offenders?
Victoria Harrisa,*, Christos Dagadakisb
aAssistant Professor, Department of Psychiatry and Behavioural Sciences, University of Washington, Box 356560,
Seattle, WA 98195, USAbSenior Clinical Instructor, Department of Psychiatry and Behavioural Sciences, University of Washington, Seattle, WA, USA
1. Introduction
Conventional wisdom and individual (case) histories suggest that mentally ill offenders (MIOs)
are incarcerated for a longer period of time than their nonmentally ill counterparts. When matched
for crime severity, MIOs remained in a medium-sized county jail for an average of 8 days longer
than nonmentally ill offenders (NMIOs) (Steadman, 1991). The National Alliance for the Mentally
Ill (NAMI)/Public Citizens Health Research Group reported that family members strongly believe
that their sons and daughters were often being held in jail in lieu of other less restrictive placements
that would have also afforded supportive mental health services (Arons & Chavex, 1996). In fact,
the literature contains the results of a study directly addressing this issue (Axelson & Wahl, 1992).
It was found that MIOs were incarcerated for a significantly longer period of time for
misdemeanant offenses. Numerous other papers have described inherent discrimination within the
American judicial system that includes women, ethnic/racial minorities and (specifically) MIOs
(Abramson, 1972; Grekin, Jemelka, & Trupin, 1994; Sarri, 1986). From another perspective, the
disproportionate presence of major mental illnesses (compared to community rates) has also been
well documented (Lamb & Weinberger, 1998; Teplin, 1994; Teplin, Abram, & McClelland, 1996,
1997). In addition, the higher arrest rates found among psychiatric patients would also suggest that
the criminal justice system differentially deals with MIOs (Grossman, Haywood, Cavanaugh, Davis,
& Lewis, 1995; Hiday, 1991; Schellenberg, Wasylenki, Webster, & Goering, 1992; Teplin & Pruett,
1992).
Despite the weight of evidence, many questions remained: If previous criminal history were
controlled for and the sample size of the strongest previous study (Axelson & Wahl, 1992) was
greatly increased, would the results hold? How large an effect does the presence of a mental
illness have on the length of incarceration for MIOs? The purpose of this study was to answer
these questions with two groups of detainees in an American county jail: MIOs and NMIOs.
0160-2527/$ - see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.ijlp.2004.04.001
* Corresponding author. Tel.: +1-206-680-9699; fax: +1-206-543-9520.
E-mail address: [email protected] (V. Harris).
V. Harris, C. Dagadakis / International Journal of Law and Psychiatry 27 (2004) 387–393388
2. Methods
2.1. Research setting
The setting has been previously described (Harris & Koepsell, 1996a,b). Briefly, The King County
Correctional Facility (KCCF), located in Seattle, WA, has a capacity of 1623 beds, although the usual
occupancy is approximately 1900.1 It serves as the criminal justice detention center for adults in 31
municipal jurisdictions in the metropolitan area of Seattle. In addition, juveniles who have been
remanded to the adult criminal justice system are also held in the KCCF. There are approximately 60,000
bookings per year in the facility. The KCCF is classified as a medium-sized county jail (U.S. Department
of Justice, 1997).
Located within the jail is a 90-bed psychiatric unit. Its usual occupancy is about 100 inmates. Both
men and women are housed on the unit, as are both misdemeanants and felons. The Commission on
Correctional Health Care accredited this unit in 1992, using standards developed by the American
Medical Association and revised by the National Commission of Health Care. There are approximately
5600 admissions to the psychiatric unit per year. In 1990, these admissions involved 1500 different
people.
At arrest, all people are triaged for physical and mental illness in the booking area. They are referred
for psychiatric evaluation if their behaviour is considered bizarre, if they report taking psychotropic
medications, or if they report suicidality. Psychiatric staff reviews relevant paperwork and interviews the
detainee using a semistructured (nonvalidated) mental status exam. Information provided by the detainee
concerning community psychiatric providers and psychiatric medications is recorded in the detainees’
medical record. This information is verified by phoning the community psychiatric provider (if any) who
also confirms the psychiatric diagnosis. This information is also routinely recorded in the inmate’s
medical record.
2.2. Study design
A frequency matched retrospective study design was used, comparing length of incarceration of MIOs
to that of offenders who did not suffer from a mental illness.
2.3. Sample size and human subjects review
The sample size calculated for a recidivism study was also used for this study. Calculations were
based on a pilot study of 27 MIOs and 27 NMIOs (Harris & Koepsell, 1996a,b). Human subjects
approval for this study was obtained by the University of Washington and the Seattle King County
Department of Public Health. Individual consent was not obtained due to (1) the retrospective nature of
the study, (2) the transient nature of the population, and (3) the data sources (records).
1 Jail overcrowding is well documented in the literature (U.S. Department of Justice, 1997). In this situation, individuals
often sleep on mattresses on the floor until a bunk becomes available.

2.4. Study subjects and comparison group
The mentally ill group consisted of 127 randomly selected detainees2 who were housed in the
psychiatric unit at the KCCF during 1990. Psychiatric illness was determined by a combination of
information supplied by the community psychiatric provider (recorded in the medical records), and the
structured mental status exam performed by Jail Health Services psychiatric staff. Only those individuals
with a major mental illness were included, as defined by the presence of symptoms consistent with a
psychotic or affective disorder and/or the use of psychotropic medications, which would indicate one of
these illnesses in remission. Detainees with only a diagnosis of personality disorder or substance abuse
were not considered to be mentally ill.
The mentally ill subjects were frequency matched (Anderson et al., 1980) for groups of variables:
severity and type of index crime, gender, and age group with 127 detainees who were incarcerated
during 1990, but not on the psychiatric unit. The absence of a major psychiatric illness was determined
by reviewing the jail medical record.
2.5. Data collection
Demographic information, information concerning the index arrest, psychiatric information, and
previous criminal history were obtained from two sources: the criminal record of the individual,
which is available for public perusal, and the medical record kept by Jail Health Services at the
KCCF.
2.6. Analysis
Both the t test and the nonparametric Mann–Whitney U test were used to compare the length of
incarceration for the index crime between groups. Due to skewness, the t test was applied on the
transformed data to log(LOI + 1), where LOI = length of incarceration. Nineteen other independent
variables used in linear regression on the transformed data included age, gender, index crime, housing
information, and court release code. Lambda, an arrest density, was also included in the linear regression
model to account for any previous incarceration in the KCCF since the age of 16 years (Blumstein,
Cohen, & Roth, 1986).
V. Harris, C. Dagadakis / International Journal of Law and Psychiatry 27 (2004) 387–393 389
3. Results
3.1. Demographic and background information
Of the randomly selected MIOs, 84.3% (107/127) were male. Fifty-three (41.7%) were between
the ages of 21–29 years; 79.5% (101/127) of MIOs had been charged with a misdemeanor offense.
Crimes against property, including theft, trespass, and property destruction were the most common
2 Rearrest of all 254 subjects has been previously reported (Harris & Koepsell, 1996a,b).

V. Harris, C. Dagadakis / International Journal of Law and Psychiatry 27 (2004) 387–393390
crimes (40.1%). The index crime (crime of note, which resulted in arrest in 1990) was classified as
violent (including assault, menacing, rape, hit and run, harassment, violation of a no-contact order,
and obstruction) for 49 (38.8%) of the subjects.
By study design, frequency matching with the nonmentally ill group was successful for the
variables of age group, gender, crime severity, and index crime. As previously reported (Harris &
Koepsell, 1996a,b) and summarized in Table 1, MIOs and NMIOs in this study differed
significantly in the following areas: marital status, housing, prior felony arrests, and history of
alcohol abuse.
Table 1
Background information for MIOs and NMIOs at index arrest
Mentally ill (%) Nonmentally ill (%) v2 df P value
Marital status 31.96 3 < .01
Never married 57.5 26.8
No current partnera 10.2 18.1
Currently partneredb 16.5 42.5
Unavailable 15.7 12.6
Ethnicity 0.466 1 .49
African American 28.3 32.3
Caucasian 68.5 62.2
Other 3.1 5.5
Domicility 9.75 2 < .01
Homeless 31.5 16.5
Has address 60.6 67.7
Unavailable 7.9 15.7
Prior misdemeanant arrests 5.18 2 .08
None 33.9 26.0
1–4 38.6 33.1
> 4 27.6 40.9
Prior felony arrests 8.35 2 < .01
None 63.8 59.1
1–2 26.8 18.9
>2 9.4 22.0
Drug abuse history 0.16 1 .70
Yes 67.7 65.4
No 32.3 34.6
Alcohol abuse history 5.11 1 < .05
Yes 44.9 59.1
No 55.1 40.9
Court release code 6.20 3 .10
Sentence expired 41 32
Charge dismissed 20 21
Bail/Personal recognizance 55 70
Investigated and chargedc 11 4a Widowed, divorced, or separated.b Married, gay, or common law.c Applicable only for felony crimes.
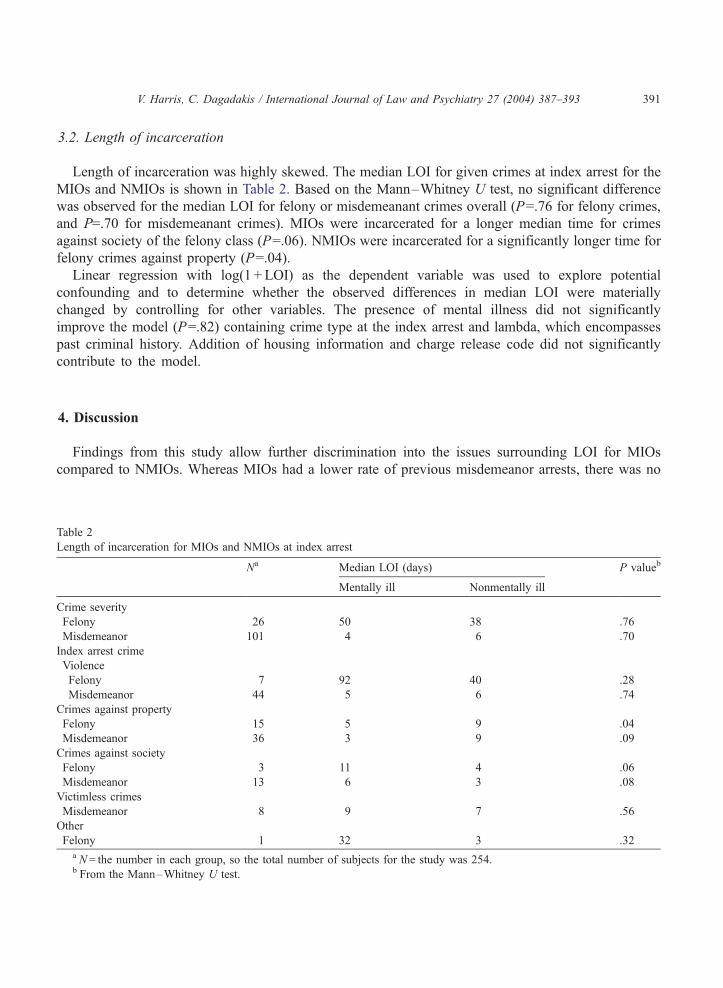
3.2. Length of incarceration
Length of incarceration was highly skewed. The median LOI for given crimes at index arrest for the
MIOs and NMIOs is shown in Table 2. Based on the Mann–Whitney U test, no significant difference
was observed for the median LOI for felony or misdemeanant crimes overall (P=.76 for felony crimes,
and P=.70 for misdemeanant crimes). MIOs were incarcerated for a longer median time for crimes
against society of the felony class (P=.06). NMIOs were incarcerated for a significantly longer time for
felony crimes against property (P=.04).
Linear regression with log(1 + LOI) as the dependent variable was used to explore potential
confounding and to determine whether the observed differences in median LOI were materially
changed by controlling for other variables. The presence of mental illness did not significantly
improve the model (P=.82) containing crime type at the index arrest and lambda, which encompasses
past criminal history. Addition of housing information and charge release code did not significantly
contribute to the model.
V. Harris, C. Dagadakis / International Journal of Law and Psychiatry 27 (2004) 387–393 391
4. Discussion
Findings from this study allow further discrimination into the issues surrounding LOI for MIOs
compared to NMIOs. Whereas MIOs had a lower rate of previous misdemeanor arrests, there was no
Table 2
Length of incarceration for MIOs and NMIOs at index arrest
Na Median LOI (days) P valueb
Mentally ill Nonmentally ill
Crime severity
Felony 26 50 38 .76
Misdemeanor 101 4 6 .70
Index arrest crime
Violence
Felony 7 92 40 .28
Misdemeanor 44 5 6 .74
Crimes against property
Felony 15 5 9 .04
Misdemeanor 36 3 9 .09
Crimes against society
Felony 3 11 4 .06
Misdemeanor 13 6 3 .08
Victimless crimes
Misdemeanor 8 9 7 .56
Other
Felony 1 32 3 .32a N= the number in each group, so the total number of subjects for the study was 254.b From the Mann–Whitney U test.

V. Harris, C. Dagadakis / International Journal of Law and Psychiatry 27 (2004) 387–393392
statistical difference found in the LOI for the index misdemeanor crime. This suggests factors other than
age, gender, current crime severity, mental illness, and previous criminal history were involved in the
determination of the LOI.
The same generalization held when previous felony history was considered. In this case,
however, the argument is strengthened. In this sample, NMIOs also had a statistically significant
more severe previous history of prior felony arrests. Yet no difference in the mean LOI was
found.
It is also noteworthy that a larger percentage of MIOs (compared to NMIOs) served their entire
sentence. Based on relative homelessness, it was (unfortunately) predictable that a lower rate of MIOs
was released on bail/personal recognizance.
Several findings in this study are in agreement with the published literature concerning mentally ill
individuals: homelessness (Abdul-Hamid & Cooney, 1997, Susser et al., 1997); the rate of never having
been married (Segal, Cohen, & Marder, 1992); and a higher proportion of Caucasians sampled (Grekin
et al., 1994; Sarri, 1986). In addition, women represented 16% of the randomly selected MIOs. Although
this is higher than the national mean for American female jail detainees, the higher proportion selected
for the study is easily understood by the high prevalence of psychiatric illness among female jail
detainees. (Lamb & Weinberger, 1998; Teplin et al., 1996, 1997). Finally, although the rate of alcohol
and drug abuse was somewhat lower than expected in both the NMIO and MIO groups (Lamb &
Weinberger, 1998; Teplin, 1994; Teplin et al., 1996), this may be an artifact of the lack of documentation
in the medical records used for this study.
This study was limited by several features inherent in the study design. Length of incarceration is
determined by several factors, including financial ability and judicial approval for release pending trial,
length of sentence after a finding of guilt, and behaviour within the county jails, which determines time
taken off the sentence. This study did not assess or control for these variables. Nonetheless, the findings
of this study are significant in terms of the lack of difference between the groups when past criminal
history is considered.
In the current judicial system, time and money (fines) have become the primary means of
punishing criminal offenders. The sentence range for a given crime is established by the state
legislature. This allows judicial discretion when an offender is sentenced. Several factors influence
the sentence imposed: crime severity, deterrence needed, time for punishment, and time for
rehabilitation (de Luca, Miller & Wiedemann, 1991). This study would suggest that when age,
gender, and crime severity are considered, mental illness per se does not statistically influence
LOI.
Nonetheless, the presence of a mental illness may easily result in a longer incarceration for an
individual. In short, it appears there was indeed a disparity in the LOI for both serious and minor crimes,
although the difference (on the whole) was not statistically different.
References
Abdul-Hamid, W., & Cooney, C. (1997). Homelessness, mental illness and the law. Medicine, Science and the Law, 37(4),
341–344.
Abramson, M. F. (1972). The criminalization of mentally disordered behavior: Possible side-effects of a new mental health law.
Hospital and Community Psychiatry, 23, 13–17.

V. Harris, C. Dagadakis / International Journal of Law and Psychiatry 27 (2004) 387–393 393
Anderson, S., Acquien, A., Hauck, W. W., Oakes, D., Vandaele, W., & Weisberg, H. (1980). Statistical methods for compar-
ative studies: Techniques for bias reduction. New York: Wiley.
Arons, B., & Chavex, N. (1996). Creating local leadership to develop mental health services: The CMHS-criminal justice
program as a model. St. Michael’s Conference.
Axelson, G. L., & Wahl, O. F. (1992). Psychotic versus non-psychotic misdemeanants in a large county jail: An analysis of
pretrial treatment by the legal system. International Journal of Law and Psychiatry, 15(4), 379–386.
Blumstein, A., Cohen, J., & Roth, J. R. (1986). Criminal careers and ‘‘career criminals’’. Washington, DC: National Academy
Press.
de Luca, M. R., Miller, T. J., & Wiedemann, C. F. (1991). Punishment vs. rehabilitation: A proposal for revising sentencing
practices. Federal Probation, 55(3), 37–45.
Grekin, P. M., Jemelka, R., & Trupin, E. W. (1994). Racial differences in the criminalization of the mentally ill. Bulletin of the
American Academy of Psychiatry and the Law, 22(3), 411–420.
Grossman, L. S., Haywood, T. W., Cavanaugh, J. L., Davis, J. M., & Lewis, D. A. (1995). State psychiatric hospital patients
with past arrests for violent crimes. Psychiatric Services, 46(8), 790–795.
Harris, V., & Koepsell, T. (1996a). Criminal recidivism among mentally ill offenders: A pilot study. Bulletin of the American
Academy of Psychiatry and the Law, 24(2), 177–186.
Harris, V., & Koepsell, T. D. (1996b). Re-arrest among mentally ill offenders. Journal of the American Academy of Psychiatry
and the Law, 26(3), 393–402.
Hiday, V. A. (1991). Arrest and incarceration of civil commitment candidates. Hospital and Community Psychiatry, 42(7),
729–734.
Kleinbaum, D. G., Kupper, L. L., & Muller, K. E. (1988). Applied regression analysis and other multivariate methods. Pacific
Grove, CA: Duxbury Press.
Lamb, H. R., & Weinberger, L. E. (1998). Persons with severe mental illness in jails and prisons: A review. Psychiatric
Services, 49(4), 483–492.
Sarri, R. C. (1986). Gender and race differences in criminal justice processing. Women and the Law [Special issue]. Women
Studies International Forum, 9(1), 89–99.
Schellenberg, E. G., Wasylenki, D., Webster, C. D., & Goering, P. (1992). A review of arrests among psychiatric patients.
International Journal of Law and Psychiatry, 15(3), 251–264.
Segal, S. P., Cohen, D., & Marder, S. R. (1992). Neuroleptic medication and prescription practices with sheltered-care residents:
A 12-year perspective. American Journal of Public Health, 82(6), 846–852.
Steadman, H. (1991). Psychiatric services at the King County Jail. (Internal report).
Susser, E., Valencia, E., Conover, S., Felix, A., Tsai, W. Y., & Wyatt, R. J. (1997). Preventing recurrent homelessness among
mentally ill men: A ‘‘critical time’’ intervention after discharge from a shelter. American Journal of Public Health, 87(2),
158–159.
Teplin, L. A. (1994). Psychiatric and substance abuse disorders among male urban jail detainees. American Journal of Public
Health, 84(2), 290–293.
Teplin, L. A., Abram, K. M., & McClelland, G. M. (1997). Mentally disordered women in jail: Who receives services?
American Journal of Public Health, 87(4), 604–609.
Teplin, L. A., Abram, K. M., & McClelland, G. M. (1996). Prevalence of psychiatric disorders among incarcerated women: I.
Pretrial jail detainees. Archives of General Psychiatry, 53(8), 505–512.
Teplin, L. A., & Pruett, N. S. (1992). Police as streetcorner psychiatrist: Managing the mentally ill. International Journal of
Law and Psychiatry, 15(2), 139–156.
U.S. Department of Justice. (1997, January). Prison and jail inmates at midyear 1996 (NCJ-162843). Bureau of Justice
Statistics Bulletin, 1–3.