leveraging the power of knowledge management to transform global health and...
TRANSCRIPT

COMMENTARY
Leveraging the Power of Knowledge Management toTransform Global Health and DevelopmentTara M Sullivan,a Rupali J Limaye,a Vanessa Mitchell,a Margaret D’Adamo,b Zachary Baquetc
Good knowledge is essential to prevent disease and improve health. Knowledge management (KM)provides a systematic process and tools to promote access to and use of knowledge among health anddevelopment practitioners to improve health and development outcomes. KM tools range frompublications and resources (briefs, articles, job aids) and products and services (websites, eLearningcourses, mobile applications), to training and events (workshops, webinars, meetings) and approachesand techniques (peer assists, coaching, after-action reviews, knowledge cafés).
By its very nature, global health and developmentwork involves a multitude of actors working
toward common goals that transcend geographic,sectoral, organizational, and financial boundaries.These efforts require immediate access to the latestresearch and know-how and demand optimal use oflimited resources to achieve maximum impact.1 Knowl-edge management (KM) can improve coordination,enhance learning and knowledge application, andimprove capacity, thus heightening service quality,strengthening health systems, and, ultimately, improv-ing health and development outcomes.
The purpose of this article is to demystify KM andadvocate its increased use in global health anddevelopment projects. We first describe knowledge,define KM, and highlight some KM tools. Then wetrace the history of KM as used in the private sector andin health and development. Finally, we illustratethrough a case study from Bangladesh how KM canbe used to support health and development outcomes.
WHAT DOES KM REALLY MEAN?
Knowledge is the capacity to act effectively.2 Few wouldargue this is essential in our fight to prevent diseaseand improve health. Knowledge, or know-how, drawsfrom our experience and allows us to solve problemsusing a combination of information and contextualunderstanding.4
There are a variety of KM definitions in use. What iscommon to most definitions is that KM is a systematicor intentional process that is linked to a broader set oforganizational or project objectives. For this paper, wedefine knowledge management as the systematic processof collecting and curating knowledge and connectingpeople to it so they can act effectively.2,3
Two types of knowledge are managed: explicit andtacit. Explicit knowledge is easy to express in words andcan be shared in written documents, manuals, ordatabases.4 On the other hand, tacit knowledge—thatis, knowledge that lives ‘‘in our heads’’—is difficult toarticulate and is best shared through discussion, stories,observation, and personal interaction.5 Knowledgemanagement gives us the ability to tap into and shareexplicit and tacit knowledge and to translate thatknowledge into action.
Within global health, lack of knowledge limits thequality of health policy, programs, services, and practices,but effective knowledge management can improve thesituation. Knowledge management can be applied toboost an organization’s efficiency and effectiveness, or itcan be used to improve service delivery throughout ahealth system. The Knowledge Management for GlobalHealth Logic Model shows how KM program inputs,processes, and outputs work together to achieve intendedhealth outcomes (Figure 1). KM inputs (people, dataand information, technology, financial resources, andinfrastructure) feed into 5 processes that make up theknowledge cycle (knowledge assessment, generation,capture, synthesis, and sharing) that, in a myriad ofcombinations, creates KM outputs, or tools.5 Knowledgemanagement processes are supported by a strongKM culture and strengthened KM capacity. KM toolsare measured in terms of reach, engagement, and
a Johns Hopkins Center for Communication Programs, Baltimore, MD, USA.bUnited States Agency for International Development (USAID), Bureau forGlobal Health, Office of Population and Reproductive Health, Washington,DC, USA.c USAID Bureau for Food Security, Washington, DC, USA.
Correspondence to Tara M Sullivan ([email protected]).
Global Health: Science and Practice 2015 | Volume 3 | Number 2 150

usefulness and result in learning and action.Drawing on Rogers’ Diffusion of Innovation theoryof how people adopt a new idea,6 the logic modelillustrates how people generally move throughan ‘‘innovation-decision process’’ when puttingnew knowledge to use, from initial awareness ofthe knowledge and intention to use that knowl-edge (learning) to actually using the new knowl-edge through informed decisions, improvedpractices, and better policies (action). Theseactions translate into strengthened systems,changed behavior, and, ultimately, improved healthoutcomes.
Since development of the Knowledge Man-agement for Global Health Logic Model, KMpractitioners have come to further appreciate thecentral role of human interaction and people inthe transfer and uptake of knowledge and the keyrole that KM can play in coordinating complexglobal health work.
Knowledge management tools can be classi-fied into 4 categories, involving a range of low-to higher-end technologies: publications andresources, products and services, training andevents, and approaches and techniques (Box).Publications and resources, such as policy briefs,guidelines, journal articles, and job aids, can helpensure health professionals have the knowledgeand skills they need to do their jobs. Products andservices, many of which harness the latest digitaland mobile technologies, such as electronicrepositories of essential information (toolkitsand websites), eLearning courses, and mobileapplications, can help share information quicklyand widely. In addition, KM approaches andtechniques such as peer assists (bringing togethera group of peers to elicit feedback on a problem,project, or activity and draw lessons from theparticipants’ knowledge and experience), coach-ing, mentorship, storytelling, and online or
FIGURE 1. Knowledge Management for Global Health Logic Model
KM is a systematicprocess ofcollecting andcuratingknowledge andconnecting peopleto it so they canact effectively.
Global Health: Science and Practice 2015 | Volume 3 | Number 2 151
Knowledge Management for Global Health and Development www.ghspjournal.org

face-to-face forums such as communities ofpractice, are KM tools that can assist in enhan-cing coordination, learning, and adaptation.Other KM tools include after-action reviews(a structured debrief of an activity to learn howit can be done better in the future) and knowledgecafés (a type of meeting structure, which aims toprovide an open and creative conversation on atopic of mutual interest to surface participants’collective knowledge, share ideas and insights,
and gain a deeper understanding of the subjectand the issues involved), as well as trainings andevents such as workshops, seminars, meetings,and webinars.
HOW HAS KM EVOLVED AS A DISCIPLINE?
Practical needs for knowledge expertise andunderstanding have been present for millennia.7
However, in the last 3 decades, primarily for-profitbusinesses have transformed KM into a disciplinethat focuses on people, processes, and technologyto ensure the knowledge necessary for anorganization to succeed is captured, created,synthesized, shared, and leveraged for maximumbenefit.8
First-generation KM focused on technology,codification, and efficiency, with the goal ofproviding access to explicit knowledge.9 Thistechnology- and codification-focused approachwas intended to increase efficiency within mostlyprivate-sector organizations10–12 but paid mini-mal attention to how or why knowledge isgenerated.9 The next generation focused onlearning to maximize knowledge sharing, astechnology applications that facilitated improvedinteraction became increasingly accessible.13
However, practitioners and scholars began torecognize that, despite technology’s ability withinmany companies to successfully leverage knowl-edge in many ways, it was not the only toolneeded to deliver comprehensive knowledgemanagement.14 The current generation usespeople-focused approaches, such as after-actionreviews, peer assists, and knowledge cafés.However, it has been noted that simply focusingon people and the technologies and tools they usedoes not automatically lead to knowledge appli-cation. Rather, the interaction between thesefactors is what allows an organization to manageknowledge effectively, and this application isdependent on a nurturing environment, includ-ing capacity building.15
All these trends have pointed to the need tobetter incorporate the most critical factors of theworld we live in—human and social factors.Social knowledge management (social KM)promises to be the next generation of KM,building upon past generations while addingwhat has been the missing piece—the power ofsocial. Social KM is driven by social benefit andrecognizes the importance of social capital, sociallearning, social media, and social networks, all withinthe context of a larger social system.
BOX. Knowledge Management Tools
Publications and Resources
� Fact sheets
� Guidelines
� Handbooks
� Job aids
� Journal articles
� Manuals
� Policy or research briefs
� Project reports
Products and Services
� Databases
� eLearning platforms
� Help desks
� Mobile applications
� Resource centers or libraries
� Websites and Web portals
Training and Events
� Conferences
� Forums
� Meetings
� Seminars
� Webinars
� Workshops
Approaches and Techniques
� After-action reviews
� Coaching
� Communities of practice
� Knowledge cafes
� Peer assists
� Study tours
� Twinning
KM focuses onpeople, processes,and technology.
Social KMpromises to betterincorporatehuman and socialfactors into KMprocesses andtools.
Global Health: Science and Practice 2015 | Volume 3 | Number 2 152
Knowledge Management for Global Health and Development www.ghspjournal.org

HOW HAS KM BEEN USED IN GLOBALHEALTH AND DEVELOPMENT?
Application of KM to global health and develop-ment has evolved over time, and as a result,interest has been growing among health careprofessionals about the importance of capturing,sharing, and using explicit and tacit knowledge.16
Initially, development organizations created cen-tralized databases, such as the DevelopmentExperience Clearinghouse (DEC) from the UnitedStates Agency for International Development(USAID), and assumed users would find thedatabase and content useful. Organizations alsopushed explicit knowledge (for example, reportsand data) to potential users, which—thanks tothe expansion of the Web—was becoming easierand less expensive to do. However, limitedattention was paid to how such knowledge wouldor could be used and even less attention wasgiven to how people drove the flow of knowledgewithin groups, networks, and organizations.
The World Bank played a critical role inhighlighting the strategic importance of knowl-edge sharing, after incorporating the idea of the‘‘knowledge bank’’ as a central element of its workin the late 1990s.17 Knowledge capture, synthesis,analysis, and sharing require potential users toseek knowledge proactively and to adapt or modifyit. Understanding this, development practitionersstarted to focus more on the ways people useexpertise and less on the technology used tofacilitate sharing. The Bank was one of the first toorganize Knowledge Fairs, where thematic groupscould display their knowledge sharing activitiesand could further illustrate with concrete examplesthe benefits of working together. The KM programdirector and staff used storytelling to sensitize theorganization to the idea that sharing knowledgewould enhance its organizational performanceand, therefore, its global impact on poverty.
Many communities of practice formed aroundthis time, and USAID, for example, supported theestablishment of working groups, which provideda venue for the agency and its partners tocollaborate informally around such issues ascommunication, monitoring and evaluation(M&E), social media, and even KM itself. It wasduring this time that USAID supported thedevelopment of online and face-to-face commu-nities, including Microlinks (microfinance, 2004),FRAMEweb (environment, 2003), Agrilinks(agriculture and food security, 2011), the VirtualLeadership Development Program (management
and leadership, 2002), and the Knowledge Gate-way (global health, 2004).
Today KM continues to be an importantdiscipline that global health and developmentorganizations use to make their work moreefficient and effective through its ability totransform health care delivery systems.8 Scholarshave recognized that information is explicit andfactual, while knowledge results from the integra-tion of information with belief and context. Thisimplies that while information can flow easily,knowledge is embedded in people and must beextracted to bridge the gap between knowledgeand its application in policy and practice.18
Evaluations of global health-related KM sug-gest KM can help impact clinical practice, which, inturn, can improve health outcomes. For example,one study suggests that through eLearning, usersare able to learn at their own pace, use customizedtraining tools, and save both time and costs oftravel to attend a class, increasing the potential forknowledge gain.19 Knowledge exchange portalscreate platforms for exchanging evidence-basedinformation through online libraries, accessingepidemiological and demographic data, and creat-ing or maintaining communities of practice.20
A randomized controlled trial reported that knowl-edge exchange portals, combined with tailoredmessaging services, can be effective at encourag-ing evidence-based policy and program design.21
A recent evaluation of a community of practiceintended to build a critical mass of experts onperformance-based financing by sharing expertiseshowed the community of practice had indeedbecome the central platform for knowledge sharingon this topic.22 In addition, KM tools and processesimplemented at multiple levels of the healthsystem in Malawi yielded improvements in knowl-edge exchange and health service delivery.23
Evidence on KM thus far has primarilyfocused on the impact of eLearning, portals, andplatforms on health service delivery. The follow-ing case study from the Bangladesh KnowledgeManagement Initiative (BKMI) provides anexample of how KM, particularly in the areas oflearning and adaptation, coordination, and capa-city strengthening, has been used to supporthealth and development in Bangladesh.
A KM CASE STUDY FROM BANGLADESH
Bangladesh has a population of more than 160million people. In the last 20 years, childmortality has declined substantially (from 50 to
Knowledge resultsfrom theintegration ofexplicitinformation withbelief and context.
Global Health: Science and Practice 2015 | Volume 3 | Number 2 153
Knowledge Management for Global Health and Development www.ghspjournal.org
11 deaths per 1,000 live births between 1993/94and 2011), total fertility has dropped (from 4.3 to2.3 children per woman between 1991 and 2011),and use of modern contraception has increased(from 31% of currently married women in 1991 to52% in 2011).24 Yet deaths in the first month oflife now account for more than 60% of all under-5deaths, and the nation has among the world’shighest malnutrition rates.24
Social and behavior change communication(SBCC) for health is an evidence- and theory-based process designed to improve health behaviorand outcomes. Using communication strategies tochange knowledge, attitudes, norms, and behaviorwithin a particular socio-ecological context, SBCCpractitioners recognize that the social and culturalenvironment can influence barriers to change—and action. The most effective SBCC programs arestrategically designed and implemented so theselected mix of media approaches (for example,interpersonal, group, and mass media) results inmaximum exposure to and mutually reinforcingmessaging across all levels of the socio-ecologicalsystem.
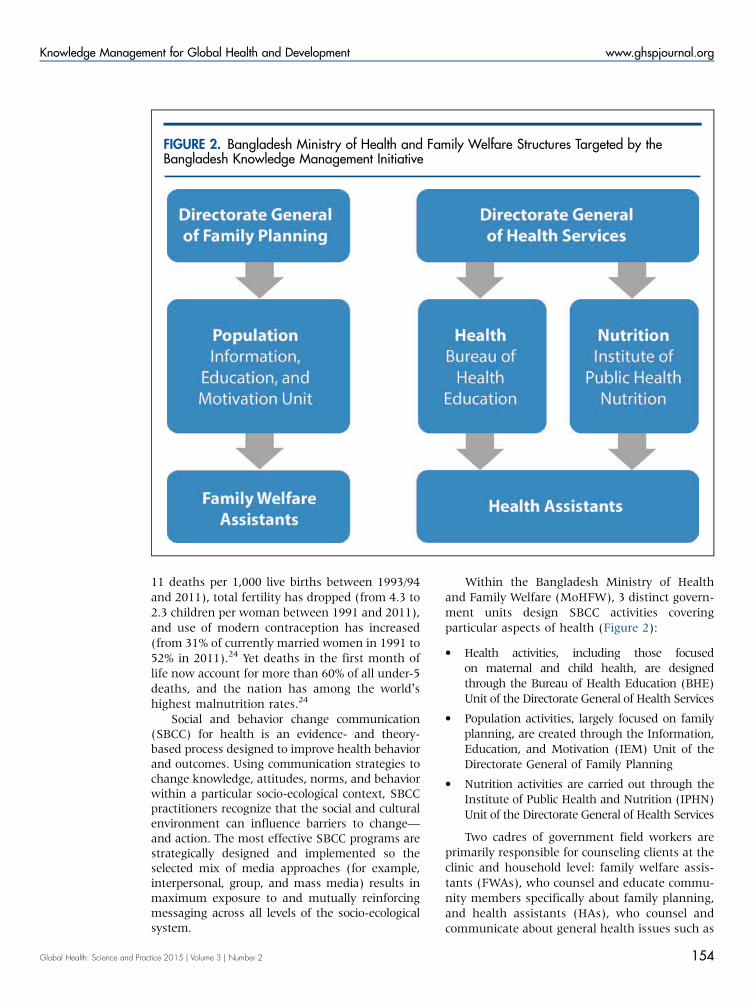
Within the Bangladesh Ministry of Healthand Family Welfare (MoHFW), 3 distinct govern-ment units design SBCC activities coveringparticular aspects of health (Figure 2):
� Health activities, including those focusedon maternal and child health, are designedthrough the Bureau of Health Education (BHE)Unit of the Directorate General of Health Services
� Population activities, largely focused on familyplanning, are created through the Information,Education, and Motivation (IEM) Unit of theDirectorate General of Family Planning
� Nutrition activities are carried out through theInstitute of Public Health and Nutrition (IPHN)Unit of the Directorate General of Health Services
Two cadres of government field workers areprimarily responsible for counseling clients at theclinic and household level: family welfare assis-tants (FWAs), who counsel and educate commu-nity members specifically about family planning,and health assistants (HAs), who counsel andcommunicate about general health issues such as
FIGURE 2. Bangladesh Ministry of Health and Family Welfare Structures Targeted by theBangladesh Knowledge Management Initiative
Global Health: Science and Practice 2015 | Volume 3 | Number 2 154
Knowledge Management for Global Health and Development www.ghspjournal.org

maternal and child health, immunizations, andnutrition. As both cadres have distinct technicalmandates, the field workers typically are not ableto address health issues outside their scope thatarise during counseling sessions.
In early 2011, the Knowledge for Health(K4Health) Project—the flagship project for KMin family planning funded by USAID’s Officeof Population and Reproductive Health—wasinvited by USAID/Bangladesh and the MoHFWin Bangladesh to undertake a scoping visit toidentify issues that could be resolved by applyingKM solutions to their SBCC work.
The project found that within each ministryunit, capacity for SBCC was low, as was overallSBCC coordination among ministry staff. Further-more, coordination of SBCC activities betweenministry units and implementing partners wasweak, leading to duplication of effort and a lack ofawareness of the scope of SBCC programs in thecountry. At the field level, government field
workers had little access to information andtraining, and they needed stronger counselingskills to communicate integrated health, popula-tion, and nutrition (HPN) messages to clients.
Subsequently, the Bangladesh KnowledgeManagement Initiative (BKMI) was implementedby K4Health from July 2011 to December 2013,focusing on 3 components to support SBCC(Figure 3):
1. Coordination of health, population, and nutri-tion SBCC programs and materials
2. Learning and application of an integratedpackage of health, population, and nutritionSBCC materials
3. Strengthening the SBCC capacity of the3 units of the MoHFW
Building on the Knowledge Management forGlobal Health Logic Model, the BKMI conceptualframework theorized that KM processes and tools
FIGURE 3. Key Components of the Bangladesh Knowledge Management Initiative.
Abbreviations: HPN, health, population, and nutrition; KM, knowledge management; MoHFW, Ministry of Health andFamily Welfare; SBCC, social and behavior change communication.
Global Health: Science and Practice 2015 | Volume 3 | Number 2 155
Knowledge Management for Global Health and Development www.ghspjournal.org

could work together to contribute to the 3 keycomponents of the project of SBCC coordination,learning and application, and capacity strength-ening (Figure 4). Coordination was an ongoingand integral part of the project that supported thelearning and application and capacity strength-ening components. Improvements in the 3 keyproject components were hypothesized to yieldenhancements in SBCC knowledge and skillsamong MoHFW stakeholders and partner orga-nizations as well as improvements in servicequality.
Coordination of Health, Population, andNutrition SBCC Activities and MaterialsThe large SBCC community in Bangladesh, madeup of government bodies, local and internationalNGOs, donor agencies, and private sector organi-zations, often worked in isolation from oneanother and was not always aligned with theMoHFW SBCC strategies. Similarly, the MoHFWwas not fully aware of all the SBCC activities inthe country, so there was a clear coordination gap.
It was common to find several organizationsworking on SBCC projects with similar objectives,similar audiences, and in similar geographicareas as a result of failure to communicate andan absence of mechanisms for coordination.This duplication of effort can slow progress, leadto financial waste, and confuse the target audi-ence with inconsistent messaging. There was aclear need for BKMI and the MoHFW to addressinconsistent, outdated, and fragmented commu-nication practices with cross-sectoral coordinationand harmonization of HPN SBCC activities.
The Bangladesh SBCC Working Group wasestablished in March 2011, following a round-table discussion in which donors, the MoHFW,and NGOs identified the need for better coordi-nation of HPN activities. When BKMI beganworking in Bangladesh in July 2011, it wasselected to serve as the secretariat for the workinggroup. Membership included the MoHFW, devel-opment partners, NGOs, and the private sector.This group met every 2 months to share knowl-edge and identify synergies among SBCC stake-holders working across HPN. Representatives
FIGURE 4. Conceptual Framework of the Bangladesh Knowledge Management Initiative
Lack ofcoordinationbetweenorganizations ledto duplication ofeffort.
Global Health: Science and Practice 2015 | Volume 3 | Number 2 156
Knowledge Management for Global Health and Development www.ghspjournal.org

from the SBCC community voluntarily andactively participated in the working group tolearn from each other and to update each otheron progress and upcoming events. BKMI sup-ported the group by convening stakeholders,developing the agenda, and arranging logistics.BKMI also hosted a website to store and sharekey documents and created a listserv for theworking group’s announcements.
Toward the end of the BKMI project, theSBCC Working Group was officially institution-alized, and the MoHFW took ownership of thegroup. A subgroup of the SBCC Working Groupbegan mapping existing HPN communicationprograms and activities in the country to helpensure coordination. A second subgroup, calledthe Strategy Review Subgroup, conducted areview of 17 SBCC strategies and 4 operationalplans with strong HPN communication compo-nents in Bangladesh to identify gaps, inconsis-tencies, synergies, and opportunities for cross-sector linkages. The last subgroup, called theHealth, Population, and Nutrition SBCC BestPractices Subgroup, began to define, identify,and share HPN best practices.
In November 2012, the SBCC Working Grouporganized a 2-day workshop to align all HPNstakeholders and partners around a country-wideshared communication implementation frameworkand to develop a plan of action that coordinatedactivities across all partners in support of theMoHFW’s Health, Population and Nutrition Sec-tor Development Program (HPN SDP), 2011–2016. Over the course of the 2 days, KM toolssuch as peer learning, small group work, andguided imagery with visual reporting were intro-duced. For example, small cross-sectoral groupswere formed at roundtables to encourage peer-to-peer learning, and the workshop facilitator tookparticipants through a guided imagery exercise aspart of the visioning for the framework. Partici-pants were tasked with imagining and thendrawing what Bangladesh would look like withimproved coordination and alignment of activitiesand SBCC messages. Participants then sharedtheir drawings at their tables, and each tableproduced a common picture that was shared in aplenary. Common themes across the pictures wereidentified, which informed the vision for theframework.
Relevant stakeholders and experts continuedto develop the framework in a participatory anditerative manner. Finalized in 2013, the frame-work is now being used to inform communication
strategies, guide resource allocation, identifyopportunities for collaboration, and guide imple-mentation of SBCC activities.
These coordination activities, aimed at insti-tuting high-quality standards and processes forthe development of SBCC programs, were alignedwith the strategic plan for the 2011–2016 HPNSDP.
Learning and Application of IntegratedHPN SBCC Activities and MaterialsBecause the FWAs and HAs addressed only asingle set of issues during their respectivecounseling sessions (FWAs focused on familyplanning while HAs covered health and nutritionissues), they missed an opportunity to educateand counsel clients comprehensively about otherimportant health issues. In the past, thesefield workers also struggled to do their jobseffectively given a number of other constraints.For example, they had little access to up-to-dateinformation, few opportunities for continuingeducation, insufficient (or, conversely, overwhelm-ing) counseling materials, and job aids that oftencontained conflicting communication messages.This resulted in confusion for both field workersand clients.
To address these challenges, BKMI conductedan eHealth pilot from May to August of 2013 in2 districts (Chittagong and Sylhet) that haverelatively high total fertility rates and low contra-ceptive prevalence rates, as well as poor maternaland child health and nutrition status, comparedwith other districts in the country. To improvefield workers’ knowledge and skills in the use ofinformation and communication technologies andtheir ability to integrate messages, including theability to counsel on the full range of HPN topics,300 field workers (150 FWAs and 150 HAs)received netbooks containing a digital HPN Toolkitand 8 video-based eLearning courses.
The Toolkit contained 116 HPN SBCC materi-als, including TV spots, flip charts, brochures,posters, and job aids, vetted by both the MoHFWand the field workers themselves. The MoHFWand subject matter experts used a standardizedassessment tool (with 9 criteria) developed by theBKMI team that measured technical accuracyand quality of the materials and alignment withMoHFW priorities. The field workers then vettedthe high-scoring materials with a separate assess-ment tool (also 9 criteria) for comprehension,appropriateness of messaging, and usability in
Global Health: Science and Practice 2015 | Volume 3 | Number 2 157
Knowledge Management for Global Health and Development www.ghspjournal.org

counseling. (See supplementary materials for theassessment tool used by subject matter expertsand the tool used by field workers.) The finalmaterials that were vetted by both the subjectmatter experts and the field workers wereuploaded into the Toolkit. The Toolkit is consid-ered the gold-standard package of HPN SBCCresources for field workers in Bangladesh.
The eLearning package, designed to addressthe training needs of the field workers, included2 family planning courses; 2 maternal, newborn,and child health courses; 2 nutrition courses; acourse on interpersonal communication andcounseling; and a course on integrated mes-saging. Courses contained 15- to 20-minute self-paced videos designed for low-literacy audiences.The project periodically assessed the field work-ers’ knowledge to measure learning from topicscovered in the courses. These KM tools (digitalToolkits and eLearning courses) connected fieldworkers to the knowledge and materials theyneeded to act effectively in their work. Prelimi-nary results indicate the package enhanced fieldworkers’ knowledge in family planning, exclusivebreastfeeding, complementary feeding, andmaternal health including danger signs.
Strengthening KM and SBCC CapacityFrom the outset, BMKI, in collaboration with theMoHFW, decided to second SBCC advisors withineach of the 3 units to provide hands-on coachingand mentorship to staff. The units had limitedcapacity to coordinate activities across HPN, aproblem that KM could solve through thissecondment. To guide this work, BKMI con-ducted a 2-part baseline assessment in each ofthe government units to: (1) understand individ-ual SBCC capacity needs, and (2) understand KMefforts currently being used to support SBCCwithin the unit. (See supplementary materials forthe SBCC and KM capacity assessment tools.)
Specifically, the SBCC assessment tool mea-sured capacity to:
� Conduct a situation analysis (including use offrameworks or models, research data todesign SBCC programs, and activity reviewsof other stakeholders to avoid duplication)
� Develop a communication strategy (includingaudience segmentation, communication objec-tives, and messaging)
� Develop materials (including creative briefs,concept testing, pretesting)
� Implement, manage, and lead programs(including work plan development, staffingplans and competencies, and supervision)
� Monitor, evaluate, and replan (including frame-works and mechanisms for measurement andthe use of results for replanning)
The KM assessment measured each unit’scapacity to:
� Create and use KM processes in support ofSBCC (including familiarity with conceptsand the existence of systems for identifyingand filling knowledge gaps and identifyingtacit knowledge among staff)
� Manage and lead SBCC programs using KM(including development of strategies to dis-seminate and promote lessons learned and useof learning to strengthen existing skills amongstaff)
� Nurture support for KM (including providingforums for knowledge sharing, fostering staffresponsibility for their own learning, anddeveloping a strategy to deliver SBCC pro-grams through digital platforms)
� Monitor, evaluate, and replan SBCC programsusing KM (including use of frameworks,M&E data, and results to assess programprogress and improve current programs)
Initially, all 3 units had low SBCC capacityand weak KM processes. Baseline data foundSBCC programs did not use evidence-baseddesign, SBCC materials and message develop-ment were of low quality, and M&E of SBCCactivities was limited. In addition, standardprocesses for KM and SBCC were nearly non-existent.
To address the identified capacity buildingneeds, BKMI, in collaboration with the unit linedirector and SBCC program managers, developedunit-specific capacity strengthening plans toimprove SBCC skills and each unit’s overallculture to support KM. To strengthen individualSBCC capacity, BKMI arranged workshops andtrainings and provided technical assistance andcontinuous coaching and mentoring. Workshopsand trainings (on message and material design,graphic design, and M&E) were provided tostaff of all 3 units together to ensure a uniformunderstanding of SBCC and to facilitate learningand collaboration across the units. Knowledgemanagement was integrated into many work-shops, both to introduce the concept to
Global Health: Science and Practice 2015 | Volume 3 | Number 2 158
Knowledge Management for Global Health and Development www.ghspjournal.org

participants and to demonstrate how it couldsupport SBCC work. For example, an SBCCcapacity strengthening training for 72 seniorand junior health officers from 64 districtsoccurred in several increments from May toSeptember 2013. As they received very little on-the-job training in this area, the 4.5-day curricu-lum covered how to design and implementstrategic communication activities, how to useSBCC materials effectively, how to design anddevelop effective messages, monitoring andsupervision for SBCC, as well as KM for SBCC.
As KM was a new concept for the healthofficers, the trainers first had to introduce theconcept and ensure the participants understoodit. After the introduction, the participants dis-cussed typical challenges in public health, such asnational guidelines not being updated or shared,program managers not being sure of which fieldworkers were performing well, field workersleaving their jobs because they were not growingprofessionally, lack of opportunity to attendtrainings, and SBCC materials being developedthat have conflicting messages. Participants thenworked in teams to discuss whether KM toolssuch as peer assist, mentorship, storytelling,online forums, and eLearning could help resolveany of these problems. The exercise helpedparticipants understand how KM could supporttheir activities and program goals.
Using a participatory assessment tool thatscored various SBCC and KM capacity compo-nents from 1 to 4 (1 = poor, 4 = excellent), base-line and endline data were compared for eachof the government units. For SBCC, in the IEMunit, the scores jumped from 1.92 to 3.42;for BHE, they increased from 1.97 to 2.64; andfor IPHN, they increased slightly from 1.97 to 2.0.For KM, the IEM unit scores rose from 1.61to 2.48; for BHE, they increased from 1.43 to 1.65;and for IPHN, they rose from 1.35 to 1.57.The IEM unit had the greatest improvementin SBCC and KM capacity compared with otherunits, and SBCC capacity scores improved morethan KM scores overall. No statistical tests wereconducted.
The endline post-assessments found that staffknowledge of how to design and implementSBCC activities had improved, and they increas-ingly used a strategic process for developingmessages and materials. Staff also demonstratedgreater ability to manage data, more appreciationfor monitoring and evaluation, and improvedleadership skills. However, BKMI staff did not
successfully put KM processes in place. Althoughthe units recognized the need, KM processes werenot prioritized. Barriers included competingdemands and limited information sharing. BKMIadvocated improved KM with the line directorsand at higher levels, including the Secretary ofHealth, specifically to develop processes and usetools that could help improve organizationaleffectiveness, knowledge sharing, and on-the-job skills. The MoHFW, however, had a greaterinterest in using external KM to improve coordi-nation between SBCC stakeholders, rather thanusing it internally at the unit level.
Lessons LearnedThe BKMI project yielded many lessons that caninform future KM initiatives in the global healthfield.
Coordination of HPN SBCC Activities and MaterialsKnowledge management in support of SBCCprograms requires time and space to shareknowledge in order to harmonize plans and alignmessages and activities within and across healthsectors and among varying SBCC stakeholders.Coordination allows SBCC stakeholders opportu-nities to collaborate, share, and validate goodpractices and lessons learned, pool resources,avoid duplication of effort, and create andimplement activities according to commonquality standards. By establishing a systematicprocess for exchanging knowledge around SBCCprograms and materials and institutionalizinga process through the working group and itsmembers, BKMI sought to create a sustainablesolution to chronic coordination issues. BKMIlearned that to institutionalize effective coordina-tion practices, it is important to take a multi-sector approach from the outset and to workclosely with the MoHFW and align coordinationactivities with the Government of Bangladesh’sstrategies and operational plans. In addition,coordination objectives and activities must beclear and inclusive of all who want to be involved.The BKMI team found that inclusiveness helpedaddress common challenges from differentangles and ensured that those implicated inSBCC activities in Bangladesh could have a voiceand contribute to the national conversationsoccurring within the health system. Furthermore,for the effort to be sustainable, the MoHFWmust take ownership of the group and drive theagenda.
Competingdemands andlimitedinformationsharing impededthe use of KMprocesses.
Global Health: Science and Practice 2015 | Volume 3 | Number 2 159
Knowledge Management for Global Health and Development www.ghspjournal.org

Learning and Application of Integrated HPN SBCCActivities and MaterialsThe eHealth pilot presented an opportunity touse new technology to deliver effective HPNcounseling to the community and improveknowledge in a standardized manner. Whilethe BKMI team had concerns about using thenetbooks with field workers, they quicklylearned how to access the digital resources,demonstrating that technology can be a usefultool for facilitating SBCC and strengtheningcounseling skills. While not its original inten-tion, field workers used the eLearning courses ascounseling tools because clients found thecourses entertaining and easy to understand.The BKMI team learned that providing fieldworkers with digital resources on netbooksempowered them, increased their confidenceon the job, and heightened their credibility inthe community. The team also learned that thefield workers would have benefitted from a morein-depth, in-person interpersonal communica-tion and counseling training on how to use thenetbook and its resources during counselingsessions. In addition, field workers would havebeen better supported if their supervisors hadbeen part of the pilot and had been available toanswer content-related questions and to helpnavigate the resources in the netbook to findthose most appropriate for a particular counsel-ing session. Finally, the project team learned thatany activity involving technology requiresongoing IT and monitoring support.
The major activities of the BKMI projectmutually reinforced each other. Capacitystrengthening efforts through 3 units of theMoHFW contributed to improved SBCC capacityof staff and increased knowledge sharing throughthe coordination activities of the SBCC WorkingGroup. All 3 units were involved in every stage ofToolkit and eLearning course development for theeHealth pilot that took place at the communitylevel. The eHealth pilot was an important activityto link national coordination and communityneeds. Applying KM processes to SBCC activities,especially in the context of coordination,improved knowledge, helped people build oneach other’s work, impacted efficiency, andultimately strengthened the health system.
Strengthening KM and SBCC CapacityGiven the high staff turnover within the MoHFW,it is important to go beyond strengthening thecapacity of individuals to focus on strengthening
the capacity of the whole organization by settingup strong processes and employing state-of-the-art tools to ensure sustainability. Furthermore,organizations need to take responsibility for theirown capacity strengthening initiatives by recog-nizing their importance and helping identifyareas for improvement. Also, given competingtime pressures, capacity strengthening plansshould support and help meet the objectivesand deliverables of operational plans. To be mosteffective, capacity strengthening efforts mustinclude the full team of SBCC staff members toachieve a common level of SBCC ability through-out the organization. Integrating new technologyas part of capacity strengthening can motivatestaff and enable them to achieve deliverablesmore efficiently. Finally, the BKMI team learnedthat changing an organization’s culture andputting KM processes in place takes time andsustained advocacy.
With regards to sustainability of the BKMIactivities, the project successfully advocated theinstitutionalization of the SBCC working group,and it continues to conduct SBCC and KMcapacity building and coordination activities inthe 3 units of the MoHFW. In addition, theproject continues to update and expand the HPNToolkit and 8 eLearning courses through a localorganization called the Bangladesh Center forCommunication Programs. The netbooks used forthe eHealth pilot were deemed to not be scalablebecause of the cost associated with the netbookitself, as well as ongoing needs for IT andmonitoring support. The netbooks loaded withthe BKMI resources were therefore given toanother USAID project in Bangladesh. Ratherthan pursuing scale-up through netbooks, theproject is now exploring how it can scale-up useof the Toolkit and the eLearning courses to morehealth service providers in Bangladesh throughthe existing infrastructure, which includes mostlydesktop computers in clinics and tablets amongthe health assistants.
CONCLUSION
Many global health programs are grappling withissues related to coordination, learning andapplication, and capacity strengthening. Address-ing these issues is critical across technical topicsand sectors, as these foundational factors, ifproperly achieved, can increase efficiency, max-imize resources, and contribute to both short- andlong-term health goals.
Field workersused theeLearning coursesas counselingtools—not bydesign butbecause clientsfound the coursesentertaining andeasy tounderstand.
Global Health: Science and Practice 2015 | Volume 3 | Number 2 160
Knowledge Management for Global Health and Development www.ghspjournal.org

The case study from Bangladesh illustrateshow KM can improve coordination by creatingand implementing a systematic process toexchange knowledge on a particular technicaltopic—in this case, SBCC programs and materi-als—as well as institutionalizing such a process toensure sustainability. Toolkits increased HPNknowledge among field workers and eLearningcourses strengthened field workers’ counselingand integrated messaging skills. These changesare hypothesized to improve service deliveryquality. From a health systems strengtheningperspective, this example illustrates that ensuringcoordination among different actors, such asthose working cross-sectorally in SBCC, support-ing learning, and investing in capacity building,can contribute to improving health and develop-ment outcomes.
Further research would be beneficial in under-standing the application of KM within the healthsector. At a minimum, more rigorous studies thatisolate KM activities and compare them to theabsence of KM activities would provide strongerevidence of its effectiveness on health outcomes.Having a deeper understanding of how healthcare organizations use KM and further testing ofvarious KM interventions within the health carecontext would be helpful in demonstrating thepotential impact.16 Within the case of BKMI, weare in the process of evaluating impact data tomore clearly make conclusions regarding theimpact of strengthening coordination, capacity,and learning and application.
The discipline of KM as applied to globalhealth and development would benefit fromadopting more systematic processes, better defin-ing the terms used to describe KM tools andprocesses, and critically examining the ‘‘how’’ tobetter integrate relevant theories into KM design,implementation, and research. Additionally,because the focus of today’s KM has shifted toKM practices for capturing knowledge that arefundamentally people-focused approaches, con-sidering human and social factors in the KMpuzzle is critical to potentially further the impactof health and development programs.
Because knowledge management has beeninformed by and used within disciplines outsidepublic health, there is a crucial need to considerhow to apply KM tools and processes from otherfields to global health. Public health practitionersmust recognize that one of the primary intangibleassets we possess is knowledge and that we allrequire knowledge to solve the world’s pressing
global health problems. The management of thatknowledge is paramount but has yet to be viewedas such.
Acknowledgments: This commentary was supported by the Knowl-edge for Health-II Project, funded by the Office of Population andReproductive Health, Bureau for Global Health, US Agency forInternational Development, Cooperative Agreement No. AID-OAA-A-13-00068. The views expressed in this document do not necessarilyreflect those of the US Agency for International Development or of theUS government. The authors wish to thank Stacey Young, SeniorLearning Advisor, Bureau for Policy, Planning and Learning Office ofLearning, Evaluation and Research, US Agency for InternationalDevelopment, for her contributions in conceptualizing thiscommentary. We also are grateful to Elizabeth Futrell from the JohnsHopkins Center for Communication Programs (CCP) for her editorialassistance and to Susan Krenn, Director of CCP, for her review of thispaper.
Competing Interests: None declared.
REFERENCES1. Ferguson J, Cummings S. Knowledge management in practice:
the case of international development. In: Koohang A, Harman K,Britz J, editors. Knowledge management: research andapplication. Santa Rosa (CA): Informing Science Press; 2008.p. 75–112.
2. Sveiby KE. The new organizational wealth: managing andmeasuring knowledge-based assets. San Francisco (CA): Berrett-Koehler Publishers; 1997.
3. Milton N. Knowledge management for teams and projects.Oxford: Chandos Publishing; 2005.
4. Brown JS, Duguid P. Organizing knowledge. Calif Manage Rev.1998;40(3):90–111. CrossRef
5. Ohkubo S, Sullivan TM, Harlan SV, Timmons BK, Strachan M.Guide to monitoring and evaluating knowledge management inglobal health programs. Baltimore (MD): Johns HopkinsBloomberg School of Public Health, Center for CommunicationPrograms; 2014. Available from: https://www.k4health.org/resources/guide-monitoring-and-evaluating-knowledge-management-global-health-programs
6. Rogers EM. Diffusion of innovations, 5th edition. New York: TheFree Press; 2003.
7. Wiig KM. Knowledge management: where did it come from andwhere will it go? Expert Syst Appl. 1997;13(1):1–14. CrossRef
8. Guptill J. Knowledge management in health care. J Health CareFinance. 2005;31(3):10–14. Medline
9. McElroy MW. Second-generation KM: a white paper.Emergence. 2000;2(3):90–100.
10. Horton D, Thiele G, Oros R, Andrade-Piedra J, Velasco C,Devaux A. Knowledge management for pro-poor innovation: thePapa Andina case. Knowl Manage Dev J. 2011;7(1):65–83.CrossRef
11. Benbya H. Knowledge management for services, operations andmanufacturing. Knowl Manage Res Pract. 2009;7(2):186–187.CrossRef
12. Sulaiman VR, Thummuru L, Hall A, Dijkman J. Tacit knowledgeand innovation capacity: evidence from the Indian livestocksector. Knowl Manage Dev J. 2011;7(1):32–44. CrossRef
13. Alavi M, Leidner DE. Review: knowledge management andknowledge management systems: conceptual foundations andresearch issues. Manage Inf Syst Q. 2001;25(1):107–136. CrossRef
Global Health: Science and Practice 2015 | Volume 3 | Number 2 161
Knowledge Management for Global Health and Development www.ghspjournal.org

14. McDermott R. Why information technology inspired but cannotdeliver knowledge management. Calif Manage Rev. 1999;41(4):103–117. CrossRef
15. Bhatt GD. Knowledge management in organizations: examiningthe interaction between technologies, techniques, and people.J Knowl Manage. 2001;5(1):68–75. CrossRef
16. Kothari A, Hovanec N, Hastie R, Sibbald S. Lessons from thebusiness sector for successful knowledge management in healthcare: a systematic review. BMC Health Serv Res. 2011;11(1):173. CrossRef. Medline
17. Kim K, McGrath S. Knowledge sharing in development agencies:lessons from four cases. Washington (DC): World Bank; 2003.Available from: http://www-wds.worldbank.org/external/default/WDSContentServer/WDSP/IB/2004/06/23/000011823_20040623121712/Rendered/PDF/293860Knowled0sharing040cases.pdf
18. Pablos-Mendez A, Chunharas S, Lansang MA, Shademani R,Tugwell P. Knowledge translation in global health. Bull WorldHealth Organ. 2005;83(10):723–723. Medline
19. Ruggeri K, Farrington C, Brayne C. A global model for effectiveuse and evaluation of e-learning in health. Telemed J E Health.2013;19(4):312–321. CrossRef. Medline
20. Quinn E, Huckel-Schneider C, Campbell D, Seale H, Milat AJ.How can knowledge exchange portals assist in knowledgemanagement for evidence-informed decision making in publichealth? BMC Public Health. 2014;14(1):443. CrossRef. Medline
21. Dobbins M, Hanna SE, Ciliska D, Manske S, Cameron R, MercerSL, et al. A randomized controlled trial evaluating the impact ofknowledge translation and exchange strategies. Implement Sci.2009;4:61. CrossRef. Medline
22. Bertone MP, Meessen B, Clarysse G, Hercot D, Kelley A, KafandoY, et al. Assessing communities of practice in health policy: aconceptual framework as a first step towards empirical research.Health Res Policy Syst. 2013;11:39. CrossRef. Medline
23. Campbell N, Schiffer E, Buxbaum A, McLean E, Perry C, SullivanTM. Taking knowledge for health the extra mile: participatoryevaluation of a mobile phone intervention for community healthworkers in Malawi. Glob Health Sci Pract. 2014;2(1):23–34.CrossRef. Medline
24. National Institute of Population Research and Training (NIPORT);Mitra and Associates; ICF International. Bangladeshdemographic and health survey 2011. Dhaka (Bangladesh):NIPORT; 2013. Co-published by Mitra and Associates and ICFInternational. Available from: http://dhsprogram.com/pubs/pdf/FR265/FR265.pdf
Peer Reviewed
Received: 2014 Dec 7; Accepted: 2015 Feb 17; First Published Online: 2015 Apr 27
Cite this article as: Sullivan TM, Limaye RJ, Mitchell V, D’Adamo M, Baquet Z. Leveraging the power of knowledge management to transformglobal health and development. Glob Health Sci Pract. 2015;3(2):150-162. http://dx.doi.org/10.9745/GHSP-D-14-00228.
& Sullivan et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricteduse, distribution, and reproduction in any medium, provided the original author and source are properly cited. To view a copy of the license, visithttp://creativecommons.org/licenses/by/3.0/. When linking to this article, please use the following permanent link: http://dx.doi.org/10.9745/GHSP-D-14-00228
Global Health: Science and Practice 2015 | Volume 3 | Number 2 162
Knowledge Management for Global Health and Development www.ghspjournal.org