lipid metabolism in familial - athero.org · head of lipid and ldl-apheresis unit, squh president...
TRANSCRIPT

Khalid Al-Rasadi, BSc, MD, FRCPC
Head of Biochemistry Department, SQU
Head of Lipid and LDL-Apheresis Unit, SQUH
President of Oman society of Lipid & Atherosclerosis
(OSLA)
Lipid Metabolism in Familial
Hypercholesterolemia

Disclosures
• Honoraria for Speakers Bureau (Pharma)
AstraZeneca, Sanofi, Pfizer
• Advisory Boards: Sanofi, Aegerion, AstraZeneca
• Research Funding: Pfizer

Cholesterol Importance
➢ A stabilizing component of cell membranes
➢ A precursor of bile salts
➢ A precursor of steroid hormones
➢ A cholesterol precursor is converted to cholecalciferol (vit. D)


⚫ Synthesis
⚫ Primary synthetic sites are extrahepatic, but liver is key regulator of homeostasis
⚫ Absorption
⚫ Largest source is biliary secretion, not diet.
⚫ Normal absorption: 50%
⚫ For cholesterol to be absorbed it must:
⚫ undergo hydrolysis (de-esterification by esterases)
⚫ be incorporated into micelles
⚫ be taken up by cholesterol transporter
⚫ be re-esterified and incorporated into chylomicrons
NORMAL CHOLESTEROL METABOLISM

400 mg/day
1,300 mg/day
17,400 mg/day
850 mg/day
NORMAL CHOLESTEROL ABSORPTION
Oil phase

HMG CoA Reductase(More Than Cholesterol Synthesis)
Acetyl CoA
HMG CoA
Mevalonate
Farnesyl Pyrophosphate
Cholesterol
HMG CoA Reductase
Isopentenyl
adenine
(transfer RNA)
Prenylation of
signalling peptides
(ras, rho, etc.)Ubiquinones
(CoQ-10, etc.)Dolichols
Inhibition of other key products of mevalonate may relate to
nonlipid effects & rare side effects of statins.

Lipoprotein Metabolism and Atherosclerosis
LDL
clearance
Lambert et al. J. Lipid Res. 2012. 53: 2515–2524.

Receptor-Mediated Endocytosis of Lipoproteins
• LDL receptor are located at coated pits, which also contain clathrin
• Vesicles fuse with lysosome where cholesterol esters are hydrolyzed into cholesterol & re-esterified by ACAT
• This avoids damaging effects of high concentrations of free cholesterol on membrane

LDL-Receptors
Endosome Lysosome
Amino
acids
Cholesterol
LDL
Cholesteryl ester
(storage)LDL
Receptors
HMG-CoA
reductase
LDL
LDL Receptor (apoB-E receptor)
ACAT
Regulates cholesterol synthesis and plasma cholesterol levels
SREBP

PCSK9
• Proprotein convertase subtilisin/kexin type
9 (PCSK9)
• the 9th member of the proprotein
convertase family of proteins that activate
other proteins
• involved in the degradation of low-density
lipoprotein (LDL) receptors in the liver.

The LDLR Pathway

Lipoproteins
Function:
➢ Lipid transport (cholesterol, cholesterol esters, triacylglycerols, phospholipids)
Structure:
A nucleus: triacylglycerols, cholesterol esters
A shell: phospholipids, apoproteins, cholesterol

Composition of lipoproteins

Apolipoproteins
Major function:
➢ structure, solubility, activation of enzyme, ligands for receptors
Apoprotein Function
Apo A-I activates LCAT, structural component of HDL
Apo B-48 Assembly and secretion of chylomicrons
Apo B-100 VLDL assembly and secretion; structural protein
of VLDL, IDL and LDL; ligand for LDL receptor
Apo C-II Activator of lipoprotein lipase (LPL)
Apo E ligand to LDL receptor; ligand to Apo E receptor

Familial Hypercholesterolemia: Prevalence and Risk
• FH is caused by genetic mutations passed on by:
• One parent (heterozygous, HeFH)1
• Both parents (homozygous, HoFH)1
• HoFH prevalence ranges from 1 in 160,000 to 1 in 250,0002,3
• Individuals with HoFH have extremely high LDL-C levels (>500 mg/dL) and premature CV risk4
• Many with HoFH experience their first coronary event in childhood or adolescence4
• HeFH prevalence ranges from 1 in 200 to 1 in 2503
• Individuals with HeFH can present with LDL-C levels 90 to 500 mg/dL and have premature CV risk4
• On average, individuals with HeFH experience their first coronary event at age 42 (about 20 years younger than the general population)4
• Early treatment is recommended for all individuals with FH, with a goal of reducing LDL-C levels by 50% from baseline3
Abbreviations: CV, cerebrovascular; FH, familial hypercholesterolemia; HeFH, heterozygous familial hypercholesterolemia; HoFH, homozygous familial hypercholesterolemia; LDL-C, low-
density lipoprotein cholesterol.
1. Zimmerman MP. Am Health Drug Benefits. 2015;8:436-442; 2. Goldstein J, et al. The Metabolic and Molecular Bases of Inherited Disease. 7th ed. New York, NY: McGraw-Hill; 1995: 1981-
2030; 3. Bouhairie VE, et al. Cardiol Clin. 2015;33:169-179; 4. Turgeon RD, et al. Can Fam Physician. 2016;62:32-37.

laboratory tests in FH
• Secondary hypercholesterolemia causes
• Genetic diagnosis
• LDL Receptor activity
• PCSK9 levels
• Lp(a) levels


Other genetic disorders
• Lysosomal Acid Lipase deficiency
•Sitosterolemia (Phytosterolemia)
• lecithin cholesterol acyltransferase deficiency


LDL-C Overlap

Overlap of clinical and mutation diagnosis of heterozygous familial hypercholesterolaemia
Nordestgaard B G et al. Eur Heart J 2013;34:3478-3490


Plasma levels of PCSK9 and phenotypic variability in
familial hypercholesterolemia



Lipoprotein (a)
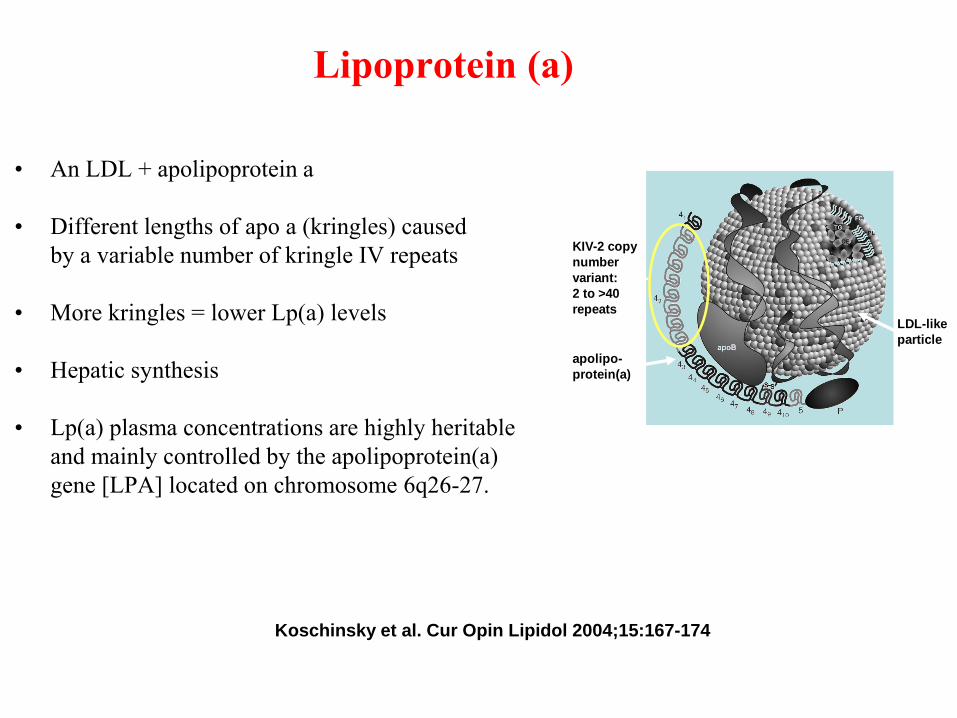
• An LDL + apolipoprotein a
• Different lengths of apo a (kringles) caused
by a variable number of kringle IV repeats
• More kringles = lower Lp(a) levels
• Hepatic synthesis
• Lp(a) plasma concentrations are highly heritable
and mainly controlled by the apolipoprotein(a)
gene [LPA] located on chromosome 6q26-27.
apolipo-
protein(a)
LDL-like
particle
KIV-2 copy
number
variant:
2 to >40
repeats
Koschinsky et al. Cur Opin Lipidol 2004;15:167-174

LIPOPROTEIN (a):
mechanisms of atherogenesis
Homology with plasminogen (= impaired fibrinolysis)
Binds to macrophages → foam cell formation
Binds to platelets (inhibition or stimulation?)
Deposition of cholesterol into plaques?

Emerging Risk Factor Collaboration. JAMA 2009; 302: 412-23

Emerging Risk Factor Collaboration. JAMA 2009; 302: 412-23

Typical distributions of lipoprotein(a) levels in the general population.
Nordestgaard B G et al. Eur Heart J 2010;31:2844-2853
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author 2010. For permissions please email: [email protected]


LIPOPROTEIN (a) MEASUREMENT
• Quantitative Lp(a) measurements
– rocket immunoelectrophoresis
– rate and endpoint nephelometry
– turbidimetry
– radio-immuno assays
– enzyme immuno assays (ELISA)
– dissociation-enhanced lanthanide fluorescent
immunoassay (DELFIA)

Lipoprotein(a) KIV-2 quartile
(mg/dL)
Multifactorially adjusted hazard ratio
(95% confidence interval)
Trend: p<0.001 Trend: p<0.001
1st
2nd
3rd
4th
50 40 30 20 10 1.0 1.5 2.0
Figure. Levels of lipoprotein(a) and risk of myocardial infarction by KIV-2 genotype.
Trend p<0.001
50 40 30 20 10
1st
2nd
3rd
4th
1.0 1.5 2.0
Lipoprotein(a)
(mg/dL)KIV-2
quartile
Hazard ratio
(95% CI)
Trend p<0.001
Risk of Myocardial Infarction
Trend p<0.001
Kamstrup et al. JAMA 2009; 301: 2331-9

Clarke et al. New Engl J Med 2009; 361: 2518-28