local bone regeneration
TRANSCRIPT

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 1/11
Review
Future of local bone regeneration e Protein versus gene therapy
J. Fischera,1, A. Kolk b,*,1, St. Wolfart a, C. Pautke b, P.H. Warnke d,e, C. Plank c, R. Smeets f
a Department of Prosthodontics, RWTH Aachen University Hospital, Pauwelsstrasse 30, D-52074 Aachen, Germanyb Department of Oral and Maxillofacial Surgery, Technische Universität München, Klinikum rechts der Isar, Ismaninger Strasse 22, D-81675 Munich, Germanyc Institute of Experimental Oncology and Therapy Research, Technische Universität München, Klinikum rechts der Isar, Ismaninger Strasse 22, D-81675 Munich, Germanyd Department of Oral and Maxillofacial Surgery, University of Kiel, Arnold-Heller-Strasse 16, 24105 Kiel, Germanye Faculty of Health Sciences and Medicine, Bond University, Gold Coast, Queensland, Australiaf Department of Oral and Maxillofacial Surgery, RWTH Aachen University Hospital, Pauwelsstrasse 30, D-52074 Aachen, Germany
a r t i c l e i n f o
Article history:
Paper received 30 July 2009
Accepted 11 March 2010
Keywords:
Bone morphogenic protein
Gene transfer
Bone regeneration
Drug delivery
Nanotechnology
a b s t r a c t
The most promising attempts to achieve bone regeneration artificially are based on the application of
mediators such as bone morphogenetic proteins (BMPs) directly to the deficient tissue site. BMPs, as
promoters of the regenerative process, have the ability to induce de novo bone formation in various
tissues, and many animal models have demonstrated their high potential for ectopic and orthotopic bone
formation. However, the biological activity of the soluble factors that promote bone formation in vivo is
limited by diffusion and degradation, leading to a short half-life. Local delivery remains a problem in
clinical applications. Several materials, including hydroxyapatite, tricalcium phosphate, demineralised
bone matrices, poly-lactic acid homo- and heterodimers, and collagen have been tested as carriers and
delivery systems for these factors in a sustained and appropriate manner. Unfortunately these delivery
vehicles often have limitations in terms of biodegradability, inflammatory and immunological rejection,
disease transmission, and most importantly, an inability to provide a sustained, continuous release of
these factors at the region of interest. In coping with these problems, new approaches have been
established: genes encoding these growth factor proteins can be delivered to the target cells. In this way
the transfected cells serve as local“
bioreactors”
, as they express the exogenous genes and secrete thesynthesised proteins into their vicinity. The purpose of this review is to present the different methods of
gene versus growth factor delivery in tissue engineering. Our review focuses on these promising and
innovative methods that are defined as regional gene therapy and provide an alternative to the direct
application of growth factors. Various advantages and disadvantages of non-viral and viral vectors are
discussed. This review identifies potential candidate genes and target cells, and in vivo as well as ex vivo
approaches for cell transduction and transfection. In explaining the biological basis, this paper also refers
to current experimental and clinical applications.
Ó 2010 European Association for Cranio-Maxillo-Facial Surgery.
1. Introduction
Despite recent progress in minimally invasive surgical proce-
dures, problems remain in the treatment of injuries due to thelimited self-healing capacity of most tissues of the musculoskeletal
system. Oral bone loss and subsequent tooth loss are substantial
worldwide health problems and in the US alone the cost has been
estimated to be $5e6 billion/year for the surgical treatments
related to oral-bone loss (Eke and Genco, 2007). The market
potential of the 16 publicly traded tissue engineering startups’amounts approx. US $2.6 billion/year (Lysaght and Reyes, 2001) and
the overall annual costs of regenerative medicine account for over
US $80 billion (Niklason and Langer, 2001).In the treatment of tissue loss, three main approaches to tissue
regeneration and engineering are defined: conduction, induction,
and cell transplantation (Langer and Vacanti,1993). The conduction
and induction techniques use the regenerative capacity of the
existing tissue to restore small amounts of tissue, but their use is
dependent on the defect size, the condition of adjacent cells, cell
migration speed, and the availability of surrounding vasculature
(Alsberg et al., 2001).
The conductive approach acts passively, allowing cells to
migrate from host tissue into a scaffold, while preventing the
invasion of unwanted cell types (Kaigler and Mooney, 2001).
* Corresponding author. Department of Oral and Maxillofacial Surgery, Techni-
sche Universität München, Klinikum rechts der Isar, Ismaninger Strasse 22, D-81675
Munich, Germany.
E-mail address: [email protected] (A. Kolk).1 These authors contributed equally to this work.
Contents lists available at ScienceDirect
Journal of Cranio-Maxillo-Facial Surgery
j o u r n a l h o m e p a g e : w w w . j c m f s . c o m
1010-5182/$ e see front matter Ó 2010 European Association for Cranio-Maxillo-Facial Surgery.
doi:10.1016/j.jcms.2010.03.016
Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e64

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 2/11
The inductive techniques use bioactive factors to stimulate tissue
regeneration and control cellular behavior. One common technique
is the delivery of soluble mediators, such as cytokines or growth
factors (Alsberg et al., 2001). The inductive method arose from the
discovery of bone morphogenetic proteins (BMPs), a sub-family of
the transforming growth factor-b (TGF-b) superfamily in 1965
(Urist, 1965). Following purification and subsequent molecular
cloning (Wozney et al., 1988; Celeste et al., 1990; Ozkaynak et al.,
1990), recombinant proteins with similar activity were identified
(Wang et al., 1990) and made available for preclinical use (Smeets
et al., 2009). These proteins are synthesised by various cells at
the defect site (e.g., fibroblasts, endothelial cells, or mesenchymal
stem cells (MSCs)) or by infiltrating repair and inflammatory cells
(e.g., platelets, macrophages, or monocytes).
Since then, many subtypes of the BMP-family have been iden-
tified, along with other growth and differentiation factors (GDFs)
that inducebone formation (Ripamonti and Reddi,1997). The major
problems of sustaining their expression and controlling their
delivery seem to have been overcome by the development and use
of carriers such as poly(D,L-lactide) (PDLLA) coating (Schmidmaier
et al., 2002, 2003; Deppe et al., 2003; Deppe and Stemberger, 2004)
or bone substitutes like hydroxyapatite, Bio-OssÓ (Terheyden et al.,
2001; Warnke et al., 2004) or calcium phosphate as a naturalrelease system (Smeets et al., 2009). However, the problems of
unwanted ectopic bone formation as well as the high costs asso-
ciated with the application of recombinant growth factors have not
yet been solved. There is increasing interest in alternative means of
exploiting the effects of growth factors. Among these potential
alternatives, one very promising procedure is gene delivery, also
called nucleic acid transfer. Instead of the respective proteins, the
DNA encoding these molecules is integrated into cells using either
in vivo or ex vivo approaches, enabling these cells to produce the
therapeutic proteins for specific periods (Bonadio et al., 1999).
The ex vivo approach represents tissue engineering in the
classical sense (Bianco and Robey, 2001). This approach, such as cell
transplantation, is required if the bone defect is extensive or lacks
active cells capable of stimulating regeneration, and is associatedwith improved results (Alsberg et al., 2001) (Fig. 1). In vivo
approaches include classic gene integration, the use of nucleicacids
to increase the expression of a target protein (De Laporte et al.,
2006).
A number of current tissue replacement strategies use
a combined approach. One example is the use of a synthetic bone
graft with a cancellous bone-like pore system, that combines
conductive properties (for strength) with an inductive potential as
a carrier for BMP (Tancred et al., 1998). Furthermore, some studies
have used transplanted cells not for ex vivo tissue formation, but
solely as carriers for inductive signals (Gysin et al., 2002).
This article reviews the use of different osteoinductive proce-
dures utilised in local bone repair and regeneration, including the
move from protein application to regional gene therapy, with an
emphasis on bone morphogenic proteins. The development of the
field of local gene transfer is described in detail. In particular, the
challenges, benefits, and risks associated with the various
gene therapy strategies and gene transfer alternatives will be
discussed.
2. Osteoinductive approaches
2.1. Bioactive mediators
Many GDFs e such as BMPs, basic fibroblast growth factor (FGF)
(bFGF), insulin-like growth factors (IGFs), TGF-b, platelet-derived
growth factor (PDGF), and vascular endothelial growth factor
(VEGF) e have been found to induce new bone through their effects
on the recruitment, proliferation, and differentiation of bone
forming cells (Hollinger et al., 2000; Oringer, 2002; Seeherman
et al., 2002).
BMPs enable skeletal tissue formation during embryogenesis,growth, and healing, as well as throughout adulthood (Reddi, 1992;
Ripamonti and Reddi, 1994; Kirker-Head, 2000). More than 30
BMPs have been identified so far. Of the known BMPs, BMP-2, -4,
and -7 are each individually able to induce de novo bone formation
at ectopic sites in vivo (Kirker-Head, 2000; Warnke et al., 2004). As
members of the TGF-b super family, BMPs themselves can be
classified into subgroups according to either their functional or
structural similarities (Ducy and Karsenty, 2000). Further studies
have shown that BMPs exhibit functions in embryogenesis that are
not restricted to skeletal development. Thus, the name “GDFs”
would be more accurate in describing this class of proteins than the
historical term (Ducy and Karsenty, 2000).
Their function is regulated from the extra-cellular compartment
by BMP-binding proteins, such as noggin and chordin, whichprevent BMPs from binding to their surface receptors. Following
the activation of a BMP receptor, the intracellular effect is trans-
mitted by Smad proteins, which induce the transcription of specific
genes (Kawabata et al., 1998). An active, mature BMP is a disul-
phide-linkeddimer that consists of eithertwo different members of
the BMP family (heterodimer), or two similar members (homo-
dimer). The dimer composition affects the function: e.g., hetero-
dimers consisting of BMP-2 (or BMP-4) and BMP-7 are more potent
morphogens than their corresponding homodimers (Kawabata
et al., 1998).
The clinical use of BMPs has been limited for years because of
the expensive and dif ficult purification process. In addition, these
proteins, isolated from allogenic or xenogenic bone, carried
potential health risks as transmission of slow virus diseases or theinduction of malignancies (Wang et al., 1988; Kirker-Head, 2000).
The identification of the corresponding human RNA and comple-
mentary DNA (cDNA) coding for human BMPs (Wozney, 1992)
allowed the production of recombinant human BMP (rhBMP)
(Kirker-Head, 2000). Despite the unlimited availability of rhBMP,
only a few human clinical studies on its use have been published
(Giannoudis et al., 2007, Schmidmaier et al., 2007). The fact that
doses far above physiological levels have to be used for bone
formation may have reduced clinical enthusiasm (Hollinger et al.,
2000). A number of animal models have demonstrated the
general beneficial effect of BMPs on the healing of bone defects. The
therapeutic potential of rhBMPs (especially rhBMP-2, -4, and -7)
has been proven in selected fracture repair models, craniomax-
illofacial-, periodontal-, and dental diseases periodontal, and dentalFig. 1. Survey of the components involved in bone formation.
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e64 55

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 3/11
diseases (Kirker-Head, 2000). Studies have revealed that different
effects of BMPs can be determined for specific cell types in a dose-
related manner (Sykaras and Opperman, 2003). For example,
increased concentrations of BMPs result in faster bone growth
(Wang, 1993), while ankylosis of teeth has been noted, dependent
on the BMP-2 dose, following application for periodontal regener-
ation (Sigurdsson et al., 1996). Studies have demonstrated the
important role of carriers in maintaining the BMP concentration at
the target site for a suf ficient period of time to promote chemotaxis
and the migration of bone-forming cells to the target site, as well as
the proliferation and differentiation of these cells (Seeherman et al.,
2002, Dai et al., 2005). Under clinical conditions, bone regeneration
requires three components: morphogenetic signals, responding
cells that are capable of assuming an osteogenic phenotype, as well
as a matrix to deliver the signal (Fig. 1). The matrix also acts, in
certain cases, as a scaffold to allow cell recruitment, attachment,
proliferation, and differentiation (Ripamonti and Duneas, 1998).
A completely new osteoinductive approach is given by the in
vivo tissue engineering techniques, such as endocultivation. They
may offer the potential to cultivate customised, vascularised bone
replacements for skeletal reconstruction. The key feature of endo-
cultivation is the use of the patient as his own bioreactor to prevent
problems with immune reactions and to allow vascularisation of the implanted matrices. Computer aided design (CAD) is used to
shape matrices for individual defects in endocultivation. The first
computer planned, complex and vascularised bone replacement e
a mandible e was grown in the latissmus dorsi muscle of man and
successfully transplanted to repair his mandibular defect (Warnke
et al., 2004). Even though this procedure was mainly successful,
drawbacks were seen and lead the focus onto developments of new
matrix designs for improved hosting of stem cells (Warnke et al.,
2006).
2.2. Delivery strategies
After the discovery of the important role of cytokines in bone
formation, much research has been invested on the controlled andcontinuous delivery of these proteins. The biological activity of
soluble factors in vivo is very short, due to proteolytic degradation
and rapid diffusion of the water-soluble factors (Winn et al., 1999;
Crombleholme, 2000). Kirker-Head (2000) defined three principle
BMP delivery strategies for clinical use: systemic administration of
BMP, delivery by means of a carrier matrix, and transfer of BMP
encoding DNA (gene therapy). The observation of elevated serum
BMP levels in growing children and decreased levels in patients
suffering from osteoporosis (Einhorn, 1992) gave rise to the idea of
the systemic application of BMPs to treat osteoporosis and poly-
traumatised patients. However, the systemic application of BMPs
still requires the development of an appropriate carrier molecule
that protects BMPs from proteolytic deactivation without impeding
their function (Kirker-Head, 2000). The major concern regardingsystemic delivery is that only a small amountof the injected protein
arrives at the diseased target tissue, while surrounding tissue
bearing BMP receptors might be adversely affected (Bonadio,
2000). In response to this, the strategy of local cytokine and
growth factor delivery directly to the target tissues was developed
(Langer, 1998). Currently, the local delivery of BMPs by carrier
matrix is at an advanced stage of development. Because of the short
lived biological activity of the factors, the ideal matrix should allow
for sustained BMP release through chemical interaction or physical
impediment, protection of the BMPs from proteolysis, rapid inva-
sion of vascular and mesenchymal cells, as well as subsequent
osteogenesis. Under clinical conditions, concentrations far above
a physiological level of osteogenic factors seem to be required to
increase the retention time and overcome the strict regulation by
inhibitors. The ef ficiency of a carrier system is often influenced by
site and species (Seeherman et al., 2002). The material used should
be non-immunogenic, non-toxic, bio-absorbable, malleable, steri-
lisable, and easily manufactured (Kirker-Head, 2000). Variousattempts have been made to develop a suitable substance that
combines all or many of these properties into one material. Organic
and inorganic materials have been used both separately and in
combination to create an appropriate matrix (Table 1).
Combinations of some of the listed materials have been used to
enhance the beneficial properties. Hydroxyapatite, as an example
of an inorganic matrix, has been used as a delivery vehicle alone
(Horisaka et al., 1991) and as a composite carrier with tricalcium
phosphate (Boden et al., 1999), collagen (Asahina et al., 1997), and
coral (Gao et al., 1996). The majoradvantages of an inorganic matrix
are its strength in supporting the surrounding tissue and
preserving bone function, and its ability to allow osteoconductive
bone formation. Additional benefits are immunological inertness
and the slow biodegradation of some of the materials. Tancredet al.(1998) demonstrated the further development of a synthetic
calcium phosphate-based material that has a cancellous bone-like
pore structure that combines optimal strength and suitability as
a carrier for BMP (Tancred et al., 1998). A novel approach was to
implant matrices that, rather than store and deliver rhBMP, actively
concentrate endogenous BMPs at the site of implantation at levels
that allow bone induction to take place. Native BMP complexes are
much more active than their constituent BMP molecules, which
means that the concentration of the native complex required for
bone induction is about 1000 times lower (De Groot, 1998;
Schliephake et al., 2005). A biodegradable, porous carrier system
is convenient for the clinician, as it limits and protects the release of
proteins or genes in a predictable and time-controlled manner,
permits cell growth, and acts transiently as an extra-cellular matrixuntil suf ficient cells are present to build a new substratum
(Hollinger and Schmitz, 1997). Among the organic matrices,
collagen and synthetic polymer delivery vehicles currently show
the greatest potential for clinical use (Kirker-Head, 2000).
Collagen, the industry’s favoured material (Hollinger et al.,
2000), has been used to create various delivery vehicles: collagen
sponges, strips, gels, membranes, and others (Kirker-Head, 2000).
In 1997, the feasibility of an rhBMP-2 absorbent collagen sponge
was evaluated for the use in local alveolar ridge preservation/
augmentation (Howell et al., 1997) and in maxillary sinus
augmentation (Boyne et al., 1997). rhBMPs bind differently to
absorbable collagen sponges, depending on their isoelectric point
(pI). It has recently been reported that rhBMP-2 and rhBMP-6 are
retained better than rhBMP-4 (Uludag et al., 1999). Unfortunately,
Table 1
Carrier matrices for delivery of BMPs (data adapted from Kirker-Head, 200 0).
Carrier matrices for delivery of BMPs
Organic Inorganic
Bone derived:
- Demineralised bone matrix
- Autolyzed antigen
extracted allogenic bone
Bone derived:
- Natural bone mineral
- Thermoashed bone mineral
Synthetic polymers:- Polylactic acid
- Polyglycolic acid homo-/
heterodimer
Metals:- Titanium
Natural polymers:
- Collagen (types I and IV)
- Non-collagenous proteins
- Fibrin
- Hydrogels
Other:
- Hydroxyapatite
- Tricalcium phosphate and other
bioceramics
- Bioactive glass
- Coral
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e6456

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 4/11
in such a delivery system, the highly potent osteoinductive heter-
odimers of the rhBMPs are less well retained than the homodimers.
A small percentage of patients develop antibodies to bovine
collagen (4e6%) or rhBMP-2 (Hollinger et al., 2000). The problems
of bovine material have been addressed with the development of
synthetic polymers, which have been made biodegradable and
assessed in various preparations (Kirker-Head, 2000). Polylactide-
co-glycolide (PLGA) not only combines the absorptive ability of
polylactide with the mechanical strength of polyglycolide (Winet
and Hollinger, 1993), making this material particularly interesting
for craniofacial surgery (Hollinger and Winn, 1999; Hollinger et al.,
2000), it can also be manufactured in various forms, depending on
the intended clinical use (Kirker-Head, 2000).
The pharmacokinetics of BMP release from a matrix is generally
characterised by two phases. After application, a short initial burst
of BMP is followed by a second phase of delayed release (Bonadio
et al., 1999; Winn et al., 1999; Kirker-Head, 2000; Sykaras and
Opperman, 2003). In the first phase, concentrations far above
a physiological level of BMP doses may diffuse, causing systemic
(Terrell et al.,1993) and local toxicity (Bonadio, 2000). Furthermore,
dose escalation seems to cause a decrease in the number of
responding cells, resulting in a slower rate of bone formation
(Seeherman et al., 2002). During the second phase, an effectivefactor level must be maintained over time, supporting mitosis and
cell differentiation, and resulting in bone formation. The long-term
delivery of BMP-2 seems to enhance the in vivo osteogenic ef ficacy
of the protein compared to short-term delivery at an equivalent
dose (Ripamonti and Duneas, 1998; Jeon et al., 2008).
These problems demonstrate the narrow therapeutic window
for the in vivo use of many recombinant cytokines and growth
factors, and provide a possible explanation for some of the disap-
pointing results in human clinical trials (Bonadio, 2000). An alter-
native strategy, regional gene therapy, attempts to overcome these
problems by providing a time- and dose-controlled delivery of
growth factors, cytokines, or morphogens for inducing bone
formation (Bonadio et al., 1999; Bonadio, 2000; Hollinger et al.,
2000; Oakes and Lieberman, 2000; Alsberg et al., 2001; Jenkinset al., 2003; Jin et al., 2003).
2.3. Gene therapy
Originally, the therapeutic application of genes was proposed
for the correction of genetic defects, such as single mutations.
Recently, gene therapy has been used to induce the expression of
molecules that are normally involved in the regenerative response
in the tissue of interest (Bonadio et al.,1999). This method provides
a potential alternative to protein therapy (Franceschi et al., 2004).
Gene therapy requires three steps to be successful: transduction
(transfection), transcription, and translation (Anderson, 1998).
The process by which the desired gene is introduced into the cellis called transduction or transfection. The introduced genes can
either integrate into the DNA of the host cell or remain in the
nucleus without integration (episomal position). In the first case,
the gene is replicated together with the host genes, and may
provide prolonged expression of the desired protein (Oakes and
Lieberman, 2000). Most research efforts have focused on trans-
duction and enhancement of its ef ficiency. Transcription, a process
while coding DNA servesas a template for mRNA synthesis in target
cells, has recently becomea focus of interest. Substantial synergistic
activity in gene therapy induced osteogenic activity is achieved by
the use of gene combination therapies to express complimentary
osteogenic signals e.g., specific combinations of BMPs, or BMPs and
their related transcription factors. The latter can regulate them-
selves and act as their own suppressor: if the transcription factor
protein binds the DNA of its own gene, it will down-regulate its
own production (Franceschi et al., 2004).
Gene therapy can be classified as in vivo or ex vivo (Fig. 4). The
desired gene can either be introduced directly into the target site
(in vivo technique), or target cells can be harvested, expanded in
culture, genetically manipulated, and (re)-implanted (ex vivo
technique) (Kirker-Head, 2000). In the ex vivo technique, cells can
be obtained from the recipient, or generated from a pre-existing
osteoprogenitor cell line (Hollinger et al., 2000).
The DNA transfer can be either native, or through a viral or non-
viral vector (Scaduto and Lieberman, 1999). The simplest trans-
duction method is the direct injection of DNA, or “naked DNA
insertion”, into the target tissue without using a vector ( Wiethoff
and Middaugh, 2003). The electroporation technique uses pulsed
electrical fields to form holes in the plasma membrane in order to
increase DNA diffusion. However, these methods are limited by
a low rate of transduction due to DNA instability and inef ficient
delivery to the target cell nucleus (Wiethoff and Middaugh, 2003).
2.4. Vector types
Most gene therapy models use vectors to enhance DNA entry
into target cell nuclei and expression of the desired genes (Scadutoand Lieberman, 1999). An ideal vector would possess the following
characteristics: avoidance of an immunological host response,
preferential binding to specific target cells, transduction of dividing
and non-dividing cells, integration of genes into cell DNA without
disruption of normal cell function, expression of genes at an
appropriate therapeutic level, ability to allow external control of
protein expression, and ease of production at a reasonable cost
(Evans and Robbins, 1995; Anderson, 1998; Oakes and Lieberman,
2000). However, the perfect vector has yet to be developed. Many
of the currently used vectors partially fulfil the above criteria. The
choice of vector for gene therapy depends on the desired duration
of protein function, anatomical location, condition to be treated,
and whether an in vivo or ex vivo approach is favoured (Oakes and
Lieberman, 200 0). The vector systems can be classified into non-viral and viral vectors.
Different viruses have been introduced as gene delivery vectors,
with adenoviruses and retroviruses among the most common,
lentiviruses and adeno-associated viruses (AAVs) are among the
more promising vectors for future therapies (Kootstra and Verma,
2003; Roth and Sundaram, 2004; Pack et al., 2005; Zhang and
Godbey, 2006). The major advantage of viral vectors is their high
frequency of transduction due to the natural tropism of viruses for
living cells ( Jenkins et al., 2003). The main disadvantages of viral
vectors are their immunogenic potential (Mahr and Gooding,1999)
and, in the case of retroviruses and certain AAVs, the threat of
disturbing normal gene function (Noguchi, 2003).
2.5. Non-viral vectors
Non-viral vectors, such as DNA plasmids, lipoplexes, or poly-
plexes mimic functions of viral cell entry but avoid many problems
associated with viral vectors, though generally possess a lower rate
of transfection (Franceschi et al., 2000; Blum et al., 2003; Wiethoff
and Middaugh, 2003). In addition, physical methods, such as
electroporation, sonoporation, magnetofection, hydrodynamic
methods, and ballistic methods (the so-called gene gun) have been
developed that support non-viral nucleic acid delivery to cells.
Naked plasmid and non-viral vectors can initiate inflammatory
responses that are different in nature and often milder than the
ones seen with viral vectors. These techniques have yet to achieve
the intrinsic ef ficiency of viral vectors. Although the induction of
bone in a non-union fracture model has been reported using the
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e64 57

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 5/11
direct transfer of plasmid DNA encoding BMP-4 and PTH (Fang
et al., 1996; Bonadio et al., 1999), the amount of plasmid DNA
necessary to induce bone in these studies was approx. 109 times
higher than the number of gene copies necessary in recent studies
using virus transduction (Franceschi et al., 2000). Nucleic acids are
complexed with cationic polymers or lipids (Spagnou et al., 2004;
Putnam and Doody, 2006), which protect them against degrada-
tion, create positively charged particles, and facilitate internal-
isation, intracellular traf ficking, and processing (De Laporte et al.,
2006; Storrie and Mooney, 2006).
Cationic lipid and adenoviral vectors have also been tested for
the delivery of BMP-2 to bone marrow stroma cells (BMSCs). Park
et al. (2003) demonstrated that both liposome- and adenoviral-
mediated BMP-2 gene transfers to primary BMSCs are suitable
methods for achieving considerable healing of critically-sized bone
defects in rats. Despite shorter healing times with adenoviral
vectors, the authors recommended liposomes as one of the most
useful vectors because of their simple preparation, the theoretically
unlimited size of the DNA insert, and fewer immunological and
safety problems (Blum et al., 2003; Park et al., 2003).
Magnetofection, another novel gene transfer method uses
magnetic force acting on gene vectors associated with magnetic
particles to enhance and target gene delivery. The major potentialof this gene transfer principle lies in the extra-ordinarily rapid and
ef ficient transfection at relatively low vector doses, and the possi-
bility of remotely controlled vector targeting in vivo (Plank et al.,
2003a,b,c). Magnetic force-derived transfection of non-viral gene
vectors is especially appropriate for cell lines that are dif ficult to
transfect, such as stem cells. By sedimenting the particles directly
onto the cells, transfection and its ef ficiency are enhanced up to
several thousand-fold compared with transfections carried out by
other gene vector procedures (Mykhaylyk et al., 2007).
Another promising non-viral gene transfer strategy uses
biodegradable structural matrix carriers to deliver plasmid DNA in
a combination referred to as a gene activated matrix (GAM) (Fang
et al., 1996). The structural matrix holds the DNA in situ until
endogenous cells, such as fibroblasts, colonise the matrix, aretransfected, and secrete the plasmid-encoded proteins that
enhance tissue regeneration (Bonadio, 2000). The carrier matrix
can gradually be replaced by the endogenous matrix deposited by
the colonising cells (Ueblacker et al., 2007). The feasibility of this
concept has been proven in animal studies. Fang et al. implanted
GAMs with genes encoding BMP-4 or human parathyroid hormone
(hPTH 1e34), resulting in bone deposition and enhanced fracture
repair, as compared to controls (Fang et al., 1996). Bonadio et al.
(1999) used a collagen sponge loaded with parathyroid hormone
cDNA in a canine tibia to improve bone formation in a dose- and
time-dependent manner. The authors argue that the retention and
expression of a plasmid gene at the site of GAM implantation is
prolonged compared to a directly delivered recombinant protein
(Bonadio et al., 1999). Despite the promising results in models(Huang et al., 2005), the delivery of DNA needs to be improved,
alternative scaffolds require evaluation, and the safety of GAM must
be further validated (Bonadio, 2002).
In general, significant technical hurdles to non-viral gene
transfer remain with regard to DNA instability, inef ficient delivery
to target cells, variable clearance by lysosomes, unpredictable
cytosolic transport, and inconsistent transcription of desired genes
(Wiethoff and Middaugh, 2003).
2.6. Viral vectors
So far, viruses are considered to be the most ef ficient vectors for
gene transfer (Chen et al., 2003). The viral vectors currently in use
are predominantly retroviruses, adenoviruses, AAVs, herpes
viruses, and lentiviruses (Evans and Robbins,1995; Anderson, 1998;
Scaduto and Lieberman, 1999; Asahara et al., 2000; Frolova-Jones
et al., 2000; Franceschi et al., 2004) in which the genes required
for viral replication are deleted and the desired gene is inserted. A
great challenge is to avoid a strong host immune response to the
viral proteins, one approach is to create a “gutless” or “gutted” virus
from which most of the viral genes are removed (Hartigan-
O’Connor et al., 1999). In current osteoinductive approaches,
retroviruses, adenoviruses, or AAVs are most commonly used to
transfer genes of bone inducing and promoting factors (Oakes and
Lieberman, 2000; Franceschi et al., 2004; Zhao et al., 2005).
The selection of its carrier is important for the direct clinical
application of a viral vector which mayprotectthe vector andenhance
its delivery to the appropriate anatomic site (Oakes and Lieberman,
2000). Schek et al. (2004) demonstrated enhanced transduction
rates and bone formation using biocompatible hydro gels as a carrier
vehicle. Other investigators have also examined strategies to tempo-
rarily control gene expression. For example, Moutsatsos et al. (2001)
reported the ability of a tetracycline-regulated vector to control
BMP-2 expression in MSCs in vitro and in vivo by administration of
doxycycline.
2.7. Retroviruses
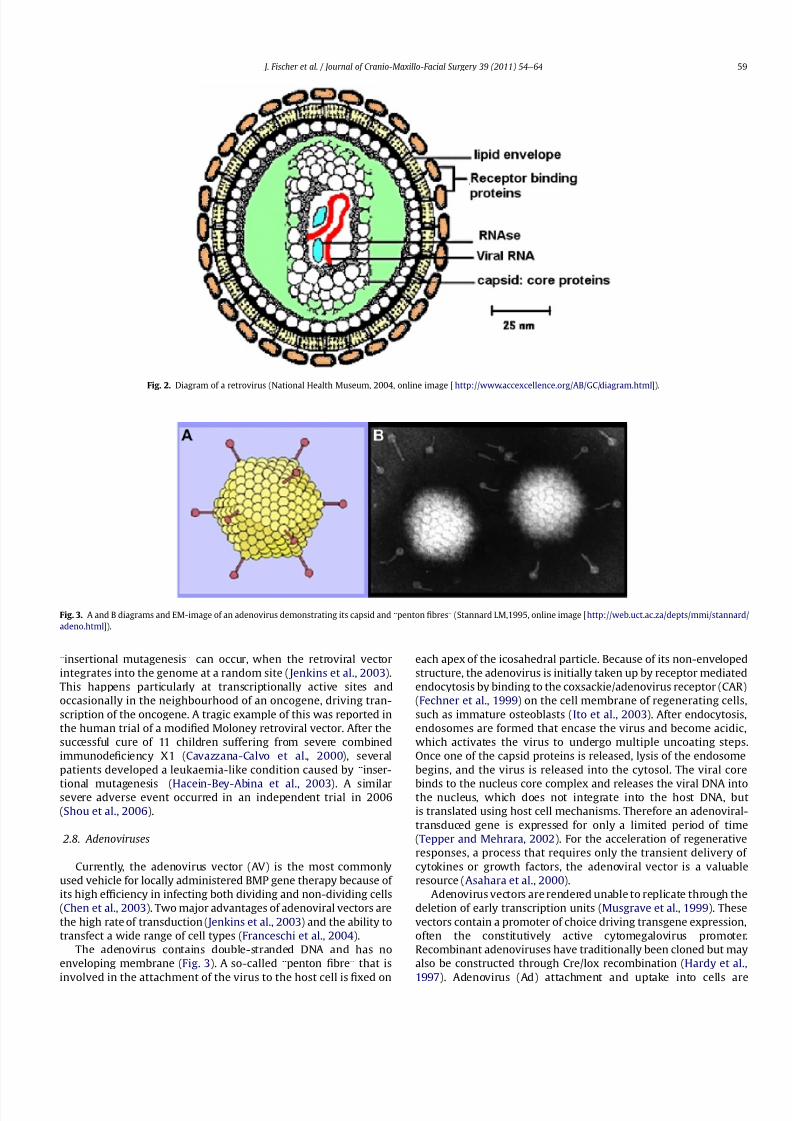
Retroviruses are an example of viruses contained in envelopes
consisting of a lipid bilayer that encloses the viral capsid containing
viral RNA and RNA transcriptase (Fig. 2).
The lipid membrane originates through budding from the
plasma membrane when the virus is released from the host cell.
The budding process is reversed when the virus attaches to target
cells through receptor-binding proteins that are anchored in its
envelope. After entering the host cell, the RNA is transcribed into
DNA by the viral reverse transcriptase, and a complementary strand
of DNA is subsequently synthesised, resulting in double-stranded
DNA that is integrated into the host cell chromosome by the viral
enzyme integrase. This allows the virus to use the replication and
translation mechanisms of the cell to assemble and release newviral particles.
Retrovirus vectors are constructed in such a way that they are
only ableto produce the desired mRNA, thus eliminating the hazard
of regaining infectiousness.
Retroviral vectors offer the advantage of being incorporated into
the host genome, providing the potential for prolonged transgene
expression (Marx et al., 1999). Furthermore, the viral proteins
produce only a weak immune response, as compared to those from
an adenoviral vector (McCormack et al., 1997). The most obvious
limitation in the application of retroviruses, e.g., the murine
leukaemia virus (MLV), is that they are only able to transfect
dividing cells (Miller et al., 1990). Rundle et al. took advantage of
this and used an MLV-based vector for direct gene therapy in
fracture repair. The vector, containing a BMP-2/4 hybrid gene, wasselectively expressed in the proliferating cells that are character-
istic for the initial stages of wound healing at the fracture site.
Although the investigators could detect an increase in the amount
of bone formed, no acceleration of the fracture union by the bone
tissue was observed (Rundle et al., 2003). Ueblacker et al. (2007)
demonstrated a highly ef ficient transduction and persistent gene
transfer to chondrocytes in vitro and in vivo by using a retroviral
based vector. Apart from this, retroviral vectors have mostly been
applied to the ex vivo transduction of target cells that show a sus-
tained expression of the incorporated BMP gene (Lieberman et al.,
1998; Breitbart et al., 1999; Gysin et al., 2002; Lee et al., 2002).
These cells, when implanted at orthotopic sites, have successfully
promoted bone healing in clinical models. Despite promising clin-
ical results, retroviral insertion can entail unexpected risks:
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e6458
8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 6/11
“insertional mutagenesis” can occur, when the retroviral vector
integrates into the genome at a random site ( Jenkins et al., 2003).
This happens particularly at transcriptionally active sites and
occasionally in the neighbourhood of an oncogene, driving tran-
scription of the oncogene. A tragic example of this was reported in
the human trial of a modified Moloney retroviral vector. After the
successful cure of 11 children suffering from severe combined
immunodeficiency X1 (Cavazzana-Calvo et al., 2000), several
patients developed a leukaemia-like condition caused by “inser-
tional mutagenesis”
(Hacein-Bey-Abina et al., 2003). A similarsevere adverse event occurred in an independent trial in 2006
(Shou et al., 2006).
2.8. Adenoviruses
Currently, the adenovirus vector (AV) is the most commonly
used vehicle for locally administered BMP gene therapy because of
its high ef ficiency in infecting both dividing and non-dividing cells
(Chen et al., 2003). Two major advantages of adenoviral vectors are
the high rate of transduction ( Jenkins et al., 2003) and the ability to
transfect a wide range of cell types (Franceschi et al., 2004).
The adenovirus contains double-stranded DNA and has no
enveloping membrane (Fig. 3). A so-called “penton fibre” that is
involved in the attachment of the virus to the host cell isfi
xed on
each apex of the icosahedral particle. Because of its non-enveloped
structure, the adenovirus is initially taken up by receptor mediated
endocytosis by binding to the coxsackie/adenovirus receptor (CAR)
(Fechner et al., 1999) on the cell membrane of regenerating cells,
such as immature osteoblasts (Ito et al., 2003). After endocytosis,
endosomes are formed that encase the virus and become acidic,
which activates the virus to undergo multiple uncoating steps.
Once one of the capsid proteins is released, lysis of the endosome
begins, and the virus is released into the cytosol. The viral core
binds to the nucleus core complex and releases the viral DNA intothe nucleus, which does not integrate into the host DNA, but
is translated using host cell mechanisms. Therefore an adenoviral-
transduced gene is expressed for only a limited period of time
(Tepper and Mehrara, 2002). For the acceleration of regenerative
responses, a process that requires only the transient delivery of
cytokines or growth factors, the adenoviral vector is a valuable
resource (Asahara et al., 2000).
Adenovirus vectors are rendered unable to replicate through the
deletion of early transcription units (Musgrave et al., 1999). These
vectors contain a promoter of choice driving transgene expression,
often the constitutively active cytomegalovirus promoter.
Recombinant adenoviruses have traditionally been cloned but may
also be constructed through Cre/lox recombination (Hardy et al.,
1997). Adenovirus (Ad) attachment and uptake into cells are
Fig. 3. A and B diagrams and EM-image of an adenovirus demonstrating its capsid and “penton fibres” (Stannard LM,1995, online image [http://web.uct.ac.za/depts/mmi/stannard/
adeno.html]).
Fig. 2. Diagram of a retrovirus (National Health Museum, 2004, online image [ http://www.accexcellence.org/AB/GC/diagram.html]).
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e64 59

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 7/11
separate but cooperative events that result from the interaction of
the viral fibre and penton base proteins with specific cell surface
receptors. The fibre knob domain mediates the primary event, cell
attachment of Ad, which projects outward from the virion and
binds to the receptor (Miura et al., 2007).
Although the standard adenoviral vector does not allow stable
integration, in vivo studies of bone regeneration have shown that
adenoviral-mediatedgenescan be expressed forup to6 weeks in bone
and upto 4 weeks in the surrounding tissue (Baltzer et al., 2000). This
is longer than has been achieved with direct delivery of the protein.
Adenovirus-mediated gene transfer has been shown to achieve
a suf ficient dose of BMPs over time in vitro and in vivo, promoting
bone formation at both ectopic and orthotopic sites (Musgrave et al.,
1999; Baltzer et al., 2000; Franceschi et al., 2000; Li et al., 2003).
These studies demonstrated the clinical potential of gene therapy for
the induction bone formation at orthotopic sites, providing a clinical
alternative to BMP protein therapy (Franceschi et al., 2004).
Despite the promising results, the immune response to the
capsid protein reduces the transduction rate (Mahr and Gooding,
1999), resulting in less or no bone formation (Musgrave et al.,
1999; Chen et al., 2002). However, the greatest concern is
the threat to the recipient, as highlighted by the 1999 death of an
18-year-old patient suffering from ornithine transcarbamoylasedeficiency who developed multiple organ failure 4 days after the
systemic administration of a recombinant adenoviral vector
(Ciment, 200 0). Local application may also generate a massive
immune response. Chen et al. (2002) reported that one of 11 rats
died after direct adenoviral mediated gene transfer on the third day
post-injection. Currently, investigators are examining new strate-
gies to encapsulate the viral vector in order to mitigate the
inflammatory response, e.g., encapsulation in an alginate micro-
sphere (Sailaja et al., 2002).
2.9. AAVs
To overcome the problems arising in immune competent indi-
viduals, the AAV-based vector has been developed, based on a non-pathogenic and replication-defective virus (Muzyczka, 1992) that
retains the advantages of a viral vector for direct gene therapy. The
recombinant AAV vector contains almost no viral-coding genes,
and therefore evades cell-mediated immunity (Monahan and
Samulski, 2000), resulting in low or no immune response (Chen
et al., 2003; Luk et al., 2003). AAV vectors are able to mediate
gene transfer to both dividing and non-dividing cells, and can
promote sustained gene expression in various tissues (Rabinowitz
and Samulski, 1998). In 2003, the AAV vector system was used to
transfer BMP-2 (Chen et al., 2003) and BMP-4 (Luk et al., 2003)
genes directly to the muscles of immune competent rats. Both
studies reported the successful transduction of cells in vitro and in
vivo, and enhanced bone formation compared to previous studies
using adenovirus vectors. The BMPs were expressed by local cellsat the end of the experiment at 8 weeks post-injection, which
is much longer than the transient expression using adenoviral
vectors. In contrast to AV vectors, adeno-associated vectors initi-
ated no detectable immunological responses (Chen et al., 2003).
Because of its safety, longevity, ef ficiency, and the ability to carry
out direct application in immune competent individuals, the AAV
vector offers a very promising option for gene transfer within the
musculoskeletal system (Luk et al., 2003). Recently, light activated
gene transduction (LAGT) has been developed to increase the
transduction of human bone marrow derived stem cells using
ultraviolet light (Ito et al., 2004). LAGT acts as a safety measure to
confine the expression of the transducted gene to the illuminated
areas, controlling the location and amount of therapeutic gene
expression.
Despite the many advantages of AAV vectors, their poor capacity
to accommodate foreign DNA is a major limitation to their use in
gene therapy. Furthermore, it is dif ficult to produce suf ficient
amounts of the virus for clinical application.
2.10. Other viral vectors
The retrovirus-mediated transduction of stem cells is restricted
by the quiescent nature and reduced receptor expression of these
cells (Havenga et al., 1997). Lentivirus-based vectors, derived from
another retrovirus subgroup, possess the ability to overcome these
limitations, and represent an alternative to retroviruses (Asahara
et al., 2000). Herpes virus saimiri (HVS)-based vectors were also
shown to infect human bone marrow stromal cells and their
progenitors (Frolova-Jones et al., 2000). In cell culture experiments,
stromal cells were susceptible to HVS-based infection in a dose-
dependent manner.
3. Candidate genes for bone regeneration
A number of genes are involved in the multiple steps of bone
regeneration and repair, and are potential candidates for gene
therapy. Beside the genes that encode for GDFs, such as PDGF, FGF,IGF, BMPs, parathyroid hormone (PTH), TGF-b, and VEGF, other
genes encode for transcription factors that are associated with
bone/cartilage-related gene expression (Runx2/Cbfal, Osterix,
Sox9), extra-cellular matrix molecules that induce or inhibit min-
eralisation (bone sialoprotein, dentin sialophosphoprotein, matrix
Gla protein, osteopontin), and receptor antagonists (soluble inter-
leukin-1 (IL-1), soluble BMP receptor) (Franceschi et al., 2004),all of
which can be considered for use in therapy.
Because of their potent induction of de novo bone formation
with a single application, rhBMP-2, -4, and -7 are preferred
candidates for local gene therapy for bone regeneration. The
earliest studies proved the feasibility of transferring single BMP
genes both ex vivo and in vivo (Lieberman et al., 1995; Fang et al.,
1996; Lieberman et al., 1998; Musgrave et al., 1999). Later, otherBMPs were sequenced and characterised, such as the novel first-
generation adenoviral constructs encoding for BMP-4 or BMP-6
developed by Jane et al. (2002) for subcutaneous injection with
which ectopic bone formation was observed. At a low vector dose,
intended to diminish the immune response to the adenoviral
vector, AdBMP-4 and -6 demonstrated a more potent induction of
bone formation when compared to the prototypical AdBMP-2
(Blum et al., 2003). Furthermore, whereas AdBMP-4 produced
ectopic bone in a manner similar to endochondral ossification,
AdBMP-6 seemed to induce both the intramembranous and
endochondral ossification pathways ( Jane et al., 2002). More
recently, Li et al. (2003) used a standardised adenovirus vector to
compare the activity of the BMP-2, -4, -6, -7, and -9 as measured by
an increase in the alkaline phosphatase activity in vitro and boneformation in vivo in athymic rats and immunocompetent Spra-
gueeDawley rats. The prototypical AdBMP-2 construct demon-
strated less bone-inducing activity than AdBMP-4, -6, and -9. The
latterdisplayed the highest osteogenic potential both in vitro and in
immunocompetent animals. Rundle et al. (2003) investigated the
effect of the substitution of a BMP-4 signal with a BMP-2 signal on
the expression of mature BMP-4. The BMP-2/4 hybrid gene induced
enhanced bone formation.
Most of the studies on gene therapy focused exclusively on
the use of a single factor. The significance of the results is,
therefore, limited by the fact that the native processes of bone
regeneration and fracture repair require the cooperation of
multiple factors in a specific temporal sequence. Fang et al.
(1996) discovered the benefi
t of the combined expression of
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e6460

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 8/11
interacting genes. A gene-activated matrix seeded with the two
plasmids, encoding for BMP-4 and hPTH 1e34, showed acceler-
ated bone formation, as compared to the administration of either
factor alone (Fang et al., 1996). More recently, multiple trans-
duction of two osteoprogenitor cell lines by AdBMP-7 and either
AdBMP-2 or AdBMP-4 resulted in a higher alkaline phosphatase
activity than expected for transduction with a single factor
(Franceschi et al., 2004). Currently, this group is investigating
these synergistic effects on bone induction in vivo. At a molec-
ular level, the BMP heterodimers possess a greater functional
activity than similar homodimers (Kawabata et al., 1998). Peng
et al. (2002) tested the interaction between an angiogenic
(VEGF) and an osteogenic (BMP-4) factor in bone formation and
demonstrated a synergistic effect when muscle-derived stem
cells were transduced with both factors.
Another approach focuses on the use of intracellular compo-
nents such as transcription factors in order to influence the activity
of osteoprogenitor cells. It has been shown that an overexpression
of the transcription factor Runx2 enhances osteoblast-specific gene
expression in mesenchymal cells (Ducy et al., 1997). Recently it has
been reported that a co-transduction of AdBMP-2 transduced cells
with AdRunx2 clearly enhanced the responsiveness to BMP-2 in
vitro and in vivo, resulting in more extensive ossification comparedto a transgene used alone (Yang et al., 2003).
4. In vivo versus ex vivo approach
Both in vivo and ex vivo methods have been successfully applied
in animal models to achieve bone regeneration. The in vivo
procedure involves the direct delivery of genes at the target site,
followed by transduction of target cells in situ (Fig. 4). Using the
appropriate delivery strategies, the in vivo gene transfer has been
shown to be a feasible, practicable, simple, minimally invasive, and
inexpensive strategy (Evans and Robbins, 1995; Bonadio et al.,
1999; Musgrave et al., 1999; Chen et al., 2003; Park et al., 2003;
Rundle et al., 2003). Although all studies have reported that
transfected cells are restricted to the injection site, it remainsdif ficult to target specific cell types for transduction (Musgrave
et al., 1999; Franceschi et al., 2004). Another disadvantage is the
dif ficulty in achieving a high transduction ef ficiency (Bonadio et al.,
1999). The first use of a retroviral vector in fracture healing showed
an adequate transduction rate but also faced the problem of
undesired extra-periosteal bone formation (Rundle et al., 2003).
The immunogenicity of adenoviral vectors remains an unresolved
problem, whereas AAV vectors appear most promising in terms of
immune compatibility and sustained gene expression (Chen et al.,
2003, Luk et al., 2003).
The ex vivo approach is a more sophisticated and expensive
technique involving target cell harvesting, expansion in cell culture,
ex vivo genetic manipulation, and (re)-implantation into target
tissue (Fig. 4). A disadvantage of the ex vivo procedure is the
morbidityassociated with cell collection from patients,when a pre-
existing cell line cannot be used (Hollinger et al., 2000). The ex vivo
expansion of cells adds considerably to the time required for the
process, and excludes this approach from the treatment of acute
conditions. However, significant advantages of ex vivo transduction
are the impossibility of uncontrolled diffusion of viral particles or
DNA complexes into the surrounding tissue, and the possibility of
selecting the target cells (Scaduto and Lieberman, 1999). Ex vivo
transduction is highly ef ficient (Oakes and Lieberman, 2000). The
successfully transduced cells can be selected and precisely
implanted at the target site using a suitable carrier matrix. If the
cells are manipulated to secrete a soluble factor, the factor can
affect other host cells (paracrine effect) or the transduced cells
themselves (autocrine effect) (Franceschi et al., 2004). To make the
most of the autocrine effect, investigators use cells for transduction
that are highly responsive to the secreted factor and can differen-
tiate into the desired tissue.
4.1. Target cells
Various cells such as gingival or dermal fibroblasts (Rutherford
et al., 2002; Hirata et al., 2003; Jin et al., 2003), periosteal cells
(Mason et al., 1998; Breitbart et al., 1999), primary articulated joint
chondroblasts (Musgrave et al., 2000), bone marrow stromal cells/
MSCs (Musgrave et al., 2000; Gysin et al., 2002; Chang et al., 2003 ),
muscle-derived stem cells (Peng et al., 2002), fat-derived stem cells
(Dragoo et al., 2003), osteoblasts, and myoblasts (Musgrave et al.,
2000; Chen et al., 2003, Luk et al., 2003) have been successfully
transduced using in vivo or ex vivo techniques and the different
vector systems.
The transduction of cells has also been shown to be dependent
on the vector dose. Baltzer et al. (2000) found that the transduction
of murine stromal cells with 108 and 109 Ad-BMP-2s increasedalkaline phosphatase activity, while 1010 particles led to cell death,
highlighting the dif ficulty of defining the therapeutic dose. Simi-
larly, Mason et al. (1998) achieved bone regeneration with BMP-7
transfected periosteal, but also showed cytotoxicity at high doses.
Hence, the therapeutic window must be defined for every target
cell type, vector type, and therapeutic gene under consideration.
This is possible for ex vivo strategies but will be exceedingly dif fi-
cult for in vivo strategies where the target cells are not well defined
and may be different depending on the site of treatment. Overall,
these studies highlight the challenges in delivering BMPs, despite
their documented usefulness in gene therapy.
5. Summary
Many clinical conditions require regeneration or implantation of
bone, while various problems with bone healing remain. Modern
therapeutic options, such as bonegrafting and protein-based therapy
donot alwaysprovidesatisfactorysolutions tothe problem of massive
bonedefects. Non-traditional approaches for bone-loss repair, suchas
gene therapy, have been investigated as a potential solution. Of the
wide range of methods used for local bone regeneration, osteoin-
ductive approaches now play a central role. They have evolved
significantly since thefirst proteins capable of inducingde novo bone
formation were discovered (Urist, 1965). Since then, various factors
have been identifiedthat influence bone formation beneficially, such
as growth factors like PDGF, FGFs, IGFs, TGF-b, and VEGF, hormones
(e.g., PTH), and bone BMPs (e.g., BMP-2, -4, -6, -7, -9). BMPs have
recently attracted great interest because of their ability to induce de
Fig. 4. Strategies for delivering therapeutic genes to target tissue: in vivo transduction
involves direct gene transfer to target cells. In an ex vivo approach, cells are harvested,
expanded in culture, transduced in vitro, and re-implanted into the target site. Gene
transfer can be achieved by viral or non-viral vectors.
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e64 61

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 9/11
novo bone formation (Schmidmaier et al., 2007). The ability to clone
andrecombinantly produce human BMPs hasopened a broadfieldfor
further research and clinical application. RhBMPs (2, 4, 6, 7, and 9)
possess a high potential for inducing ectopic and orthotopic bone, as
has been demonstrated in various animal models. Despite promising
results, futureresearchmust investigate optimal dosesand molecular
combinations, as wellas developa structureeactivityrelationship for
the different members of the BMP family in order to provide
predictable and effective clinicalapplications (De Laporte et al., 2006;
De Laporte and Shea, 2007). The biological activity of the soluble
factors that promote bone formation in vivo is transient, and sus-
tained local delivery remains a problem in clinical application.
Multiple materials including hydroxyapatite, tricalcium phosphate,
demineralised bone matrices, poly-lactic acid homo-/heterodimers,
and collagen have been tested as carriers for controlled delivery of
these factors (De Laporte and Shea, 2007). Unfortunately, many of
these delivery vehicles show limitations in terms of biodegradability,
inflammatory reaction, immunological rejection, disease trans-
mission, and, most importantly, the inability to provide a sustained
therapeutic factor level.
In response to these limitations, attempts have been made to
develop local gene therapy, in which the genes encoding the desired
proteins are delivered to the target cells rather than the proteinsthemselves. The transfected cells serve as local “bioreactors” as they
secrete the desired proteins in their vicinity. Ef ficient gene transfer,
however, requires an appropriate vector of either viral or non-viral
origin. Viral vectors have the advantage of a high transduction ef fi-
ciency (Vogt et al., 2008), and the disadvantages of a high immuno-
genic potential and, in the case of retroviruses and certain AAVs, the
threat of disturbance to normal gene function through insertional
mutagenesis. Non-viral vectors avoid these problems, but possess
a lower rate of transfection. With regard to ef ficiency and safety,
various studies conclude that adenovirus- and retrovirus-based
vectors are appropriate for an ex vivo approach, whereas AAVs are
a promising source for in vivo transduction. Nevertheless, further
studies are required to confirm the ef ficiency of lipoplexes and pol-
yplexes as non-viral vectors, which have the advantages of lowerimmunological and security risk, simple preparation, and almost
unlimited capacity for the size of genes that can be inserted.
Currently, an attempt has been made to successfully combine
the expression of different secreted factors (e.g., amongst the BMP
family, BMPþVEGF), or secreted and intracellular transcription
factors (Runx2) in order to enhance the responsiveness of target
cells (Li et al., 2009). Future research should focus on improvement
of the control of gene expression, the definition of optimal vector
dosages, and more accurate delivery of genes to the target cells in
vivo. Although promising results have been achieved in animal
defect models, human trials using gene therapy for local bone
regeneration have not yet been reported. A wide range of clinical
surgical applications is expected: correction of non-union fractures,
implant fixation, and reconstruction of skeletal defects. Additionalapplications exist in oral surgery where the successful placement of
implants often requires bone augmentation of the maxillary sinus
floor or alveolar ridge. In these clinical situations, pre-existing local
bone and surrounding tissue are extremely compromised and are,
incapable of generating an adequate biological response to either
local protein therapy or gene therapy. In these cases, further
investigation in the field of tissue engineering might provide
support for the osteoinductive approach.
References
Alsberg E, Hill EE, Mooney DJ: Craniofacial tissue engineering. Crit Rev Oral BiolMed 12: 64e75, 2001
Anderson WF: Human gene therapy. Nature 392: 25e
30, 1998
Asahara T, Kalka C, Isner JM: Stem cell therapy and gene transfer for regeneration.Gene Ther 7: 451e457, 2000
Asahina I, Watanabe M, Sakurai N, Mori M, Enomoto S: Repair of bone defect inprimate mandible using a bone morphogenetic protein (BMP)-hydroxyapatite-collagen composite. J Med Dent Sci 44: 63e70, 1997
Baltzer AW, Lattermann C, Whalen JD, Wooley P, Weiss K, Grimm M, et al: Geneticenhancement of fracture repair: healing of an experimental segmental defectby adenoviral transfer of the BMP-2 gene. Gene Ther 7: 734e739, 2000
Bianco P, Robey PG: Stem cells in tissue engineering. Nature 414: 118e121, 2001Blum JS, Barry MA, Mikos AG, Jansen JA: In vivo evaluation of gene therapy vectors
in ex vivo-derived marrow stromal cells for bone regeneration in a rat critical-size calvarial defect model. Hum Gene Ther 14: 1689e1701, 2003
Boden SD, Martin Jr GJ, Morone MA, Ugbo JL, Moskovitz PA: Posterolateral lumbarintertransverse process spine arthrodesis with recombinant human bonemorphogenetic protein 2/hydroxyapatite-tricalcium phosphate after lam-inectomy in the nonhuman primate. Spine 24: 1179e1185, 1999
Bonadio J: Tissue engineering via local gene delivery: update and future prospectsfor enhancing the technology. Adv Drug Deliv Rev 44: 185e194, 2000
Bonadio J: Genetic approaches to tissue repair. Ann N Y Acad Sci 961: 58e60, 2002Bonadio J, Smiley E, Patil P, Goldstein S: Localized, direct plasmid gene delivery in
vivo: prolonged therapy results in reproducible tissue regeneration. Nat Med 5:753e759, 1999
Boyne PJ, Marx RE, Nevins M, Triplett G, Lazaro E, Lilly LC, et al: A feasibility studyevaluating rhBMP-2/absorbable collagen sponge for maxillary sinus flooraugmentation. Int J Periodontics Restorative Dent 17: 11e25, 1997
Breitbart AS, Grande DA, Mason JM, Barcia M, James T, Grant RT: Gene-enhancedtissue engineering: applications for bone healing using cultured periosteal cellstransduced retrovirally with the BMP-7 gene. Ann Plast Surg 42: 488e495,1999
Cavazzana-Calvo M, Hacein-Bey S, Basile CD, Gross F, Yvon E, Nusbaum P, et al: Genetherapy of human severe combined immunodeficiency (SCID)-X1 disease.Science 288: 669e672, 2000
Celeste AJ, Iannazzi JA, Taylor RC, Hewick RM, Rosen V, Wang EA, et al: Identifi-cation of transforming growth factor beta family members present in bone-inductive protein purified from bovine bone. Proc Natl Acad Sci U S A 87:9843e9847, 1990
Chang SC, Chuang HL, Chen YR, Chen JK, Chung HY, Lu YL, et al: Ex vivo genetherapy in autologous bone marrow stromal stem cells for tissue-engineeredmaxillofacial bone regeneration. Gene Ther 10: 2013e2019, 2003
Chen Y, Cheung KM, Kung HF, Leong JC, Lu WW, Luk KD: In vivo new boneformation by direct transfer of adenoviral-mediated bone morphogeneticprotein-4 gene. Biochem Biophys Res Commun 298: 121e127, 2002
Chen Y, Luk KD, Cheung KM, Xu R, Lin MC, Lu WW, et al: Gene therapy for new boneformation using adeno-associated viral bone morphogenetic protein-2 vectors.Gene Ther 10: 1345e1353, 2003
Ciment J: Gene therapy experiments put on “clinical hold”. BMJ 320: 336, 2000Crombleholme TM: Adenoviral-mediated gene transfer in wound healing. Wound
Repair Regen 8: 460e472, 2000
Dai KR, Xu XL, Tang TT, Zhu ZA, Yu CF, Lou JR, et al: Repairing of goat tibial bonedefects with BMP-2 gene-modified tissue-engineered bone. Calcif Tissue Int 77:55e61, 2005
De Groot J: Carriers that concentrate native bone morphogenetic protein in vivo.Tissue Eng 4: 337e341, 1998
De Laporte L, Cruz Rea J, Shea LD: Design of modular non-viral gene therapy vectors.Biomaterials 27: 947e954, 2006
De Laporte L, Shea LD: Matrices and scaffolds for DNA delivery in tissue engi-neering. Adv Drug Deliv Rev 59: 292e307, 2007
Deppe H, Stemberger A: Effects of laser-modified versus osteopromotively coatedtitanium membranes on bone healing: a pilot study in rat mandibular defects.Lasers Med Sci 18: 190e195, 2004
Deppe H, Stemberger A, Hillemanns M: Effects of osteopromotive and anti-infectivemembranes on bone regeneration: an experimental study in rat mandibulardefects. Int J Oral Maxillofac Implants 18: 369e376, 2003
Dragoo JL, Choi JY, Lieberman JR, Huang J, Zuk PA, Zhang J, et al: Bone induction byBMP-2 transduced stem cells derived from human fat. J Orthop Res 21:622e629, 2003
Ducy P, Karsenty G: The family of bone morphogenetic proteins. Kidney Int 57:
2207e
2214, 2000Ducy P, Zhang R, Geoffroy V, Ridall AL, Karsenty G: Osf2/Cbfa1: a transcriptional
activator of osteoblast differentiation. Cell 89: 747e754, 1997Einhorn TA: Clinical applications of recombinant gene technology: bone and
cartilage repair. Cells Mat 2: 1e11, 1992Eke PI, Genco RJ: CDC periodontal disease surveillance project: background,
objectives, and progress report. J Periodontol 78: 1366e1371, 2007Evans CH, Robbins PD: Possible orthopaedic applications of gene therapy. J Bone
Joint Surg Am 77: 1103e1114, 1995Fang J, Zhu YY, Smiley E, Bonadio J, Rouleau JP, Goldstein SA, et al: Stimulation of
new bone formation by direct transfer of osteogenic plasmid genes. Proc NatlAcad Sci U S A 93: 5753e5758, 1996
Fechner H, Haack A, Wang H, Wang X, Eizema K, Pauschinger M, et al: Expression of coxsackie adenovirus receptor and alphav-integrin does not correlate withadenovector targeting in vivo indicating anatomical vector barriers. Gene Ther6: 1520e1535, 1999
Franceschi RT, Wang D, Krebsbach PH, Rutherford RB: Gene therapy for boneformation: in vitro and in vivo osteogenic activity of an adenovirus expressingBMP7. J Cell Biochem 78: 476e486, 2000
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e6462

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 10/11
Franceschi RT, Yang S, Rutherford RB, Krebsbach PH, Zhao M, Wang D: Gene therapyapproaches for bone regeneration. Cells Tissues Organs 176: 95e108, 2004
Frolova-Jones EA, Ensser A, Stevenson AJ, Kinsey SE, Meredith DM: Stable markergene transfer into human bone marrow stromal cells and their progenitorsusing novel herpesvirus saimiri-based vectors. J Hematother Stem Cell Res 9:573e581, 2000
Gao T, Lindholm TS, Marttinen A, Urist MR: Composites of bone morphogeneticprotein (BMP) and type IV collagen, coral-derived coral hydroxyapatite, andtricalcium phosphate ceramics. Int Orthop 20: 321e325, 1996
Giannoudis PV, Einhorn TA, Marsh D: Fracture healing: the diamond concept. Injury
38(Suppl. 4): S3e
S6, 2007Gysin R, Wergedal JE, Sheng MH, Kasukawa Y, Miyakoshi N, Chen ST, et al: Ex vivo
gene therapy with stromal cells transduced with a retroviral vector containingthe BMP4 gene completely heals critical size calvarial defect in rats. Gene Ther9: 991e999, 2002
Hacein-Bey-Abina S, von Kalle C, Schmidt M, Le Deist F, Wulffraat N, McIntyre E,et al: A serious adverse event after successful gene therapy for X-linked severecombined immunodeficiency. N Engl J Med 348: 255e256, 2003
Hardy S, Kitamura M, Harris-Stansil T, Dai Y, Phipps ML: Construction of adenovirusvectors through Creelox recombination. J Virol 71: 1842e1849, 1997
Hartigan-O’Connor D, Amalfitano A, Chamberlain JS: Improved production of guttedadenovirus in cells expressing adenovirus preterminal protein and DNA poly-merase. J Virol 73: 7835e7841, 1999
Havenga M, Hoogerbrugge P, Valerio D, van Es HH: Retroviral stem cell genetherapy. Stem Cells 15: 162e179, 1997
Hirata K, Tsukazaki T, Kadowaki A, Furukawa K, Shibata Y, Moriishi T, et al: Trans-plantation of skin fibroblasts expressing BMP-2 promotes bone repair moreeffectively than those expressing Runx2. Bone 32: 502e512, 2003
Hollinger JO, Schmitz JP: Macrophysiologic roles of a delivery system for vulneraryfactors needed for bone regeneration. Ann N Y Acad Sci 831: 427
e437, 1997
Hollinger JO, Winn SR: Tissue engineering of bone in the craniofacial complex. AnnN Y Acad Sci 875: 379e385, 1999
Hollinger JO, Winn SR, Hu Y, Sipe R, Buck DC, Xi. G: Assembling a bone e regen-eration therapy. In: Davies JE (ed.) Bone engineering. pp. 437e440, Toronto.
Horisaka Y, Okamoto Y, Matsumoto N, Yoshimura Y, Kawada J, Yamashita K, et al:Subperiosteal implantation of bone morphogenetic protein adsorbed tohydroxyapatite. Clin Orthop Relat Res 1991: 303e312, 1991
Howell TH, Fiorellini J, Jones A, Alder M, Nummikoski P, Lazaro M, et al: A feasibilitystudy evaluating rhBMP-2/absorbable collagen sponge device for local alveolarridge preservation or augmentation. Int J Periodontics Restorative Dent 17:124e139, 1997
Huang YC, Riddle K, Rice KG, Mooney DJ: Long-term in vivo gene expression viadelivery of PEI-DNA condensates from porous polymer scaffolds. Hum GeneTher 16: 609e617, 2005
Ito H, Goater JJ, Tiyapatanaputi P, Rubery PT, O’Keefe RJ, Schwarz EM: Light-acti-vated gene transduction of recombinant adeno-associated virus in humanmesenchymal stem cells. Gene Ther 11: 34e41, 2004
Ito T, Tokunaga K, Maruyama H, Kawashima H, Kitahara H, Horikoshi T, et al:Coxsackievirus and adenovirus receptor (CAR)-positive immature osteoblasts astargets of adenovirus-mediated gene transfer for fracture healing. Gene Ther10: 1623e1628, 2003
Jane Jr JA, Dunford BA, Kron A, Pittman DD, Sasaki T, Li JZ, et al: Ectopic osteogenesisusing adenoviral bone morphogenetic protein (BMP)-4 and BMP-6 genetransfer. Mol Ther 6: 464e470, 2002
Jenkins DD, Yang GP, Lorenz HP, Longaker MT, Sylvester KG: Tissue engineering andregenerative medicine. Clin Plast Surg 30: 581e588, 2003
Jeon O, Song SJ, Yang HS, Bhang SH, Kang SW, Sung MA, et al: Long-term deliveryenhancesin vivo osteogenicef ficacyof bonemorphogeneticprotein-2comparedto short-term delivery. Biochem Biophys Res Commun 369: 774e780, 2008
Jin QM, Anusaksathien O, Webb SA, Rutherford RB, Giannobile WV: Gene therapy of bone morphogenetic protein for periodontal tissue engineering. J Periodontol74: 202e213, 2003
Kaigler D, Mooney D: Tissue engineering ’s impact on dentistry. J Dent Educ 65:456e462, 2001
Kawabata M, Imamura T, Miyazono K: Signal transduction by bone morphogeneticproteins. Cytokine Growth Factor Rev 9: 49e61, 1998
Kirker-Head CA: Potential applications and delivery strategies for bone morpho-genetic proteins. Adv Drug Deliv Rev 43: 65e92, 2000
Kootstra NA, Verma IM: Gene therapy with viral vectors. Annu Rev PharmacolToxicol 43: 413e439, 2003
Langer R: Drug delivery and targeting. Nature 392: 5e10, 1998Langer R, Vacanti JP: Tissue engineering. Science 260: 920e926, 1993Lee JY, Peng H, Usas A, Musgrave D, Cummins J, Pelinkovic D, et al: Enhancement of
bone healing based on ex vivo gene therapy using human muscle-derived cellsexpressing bone morphogenetic protein 2. Hum Gene Ther 13: 1201e1211, 2002
Li G, Corsi-Payne K, Zheng B, Usas A, Peng H, Huard J: The dose of growth factorsinfluences the synergistic effect of vascular endothelial growth factor on bonemorphogenetic protein 4-induced ectopic bone formation. Tissue Eng Part A2009, 2009
Li JZ, Li H, Sasaki T, Holman D, Beres B, Dumont RJ, et al: Osteogenic potential of fivedifferent recombinant human bone morphogenetic protein adenoviral vectorsin the rat. Gene Ther 10: 1735e1743, 2003
Lieberman JR, Kono M, Vertelney E, Finerman GAM, Witte ON: The creation of rhBMP-2 producing cell line: retroviral gene transfer of rhBMP-2 into a stromalline. In: Trans. Orthop. Res. Soc. 41st Ann. Meeting, vol. 20; 1995, 499, 1995
Lieberman JR, Le LQ, Wu L, Finerman GA, Berk A, Witte ON, et al: Regional genetherapy with a BMP-2-producing murine stromal cell line induces heterotopicand orthotopic bone formation in rodents. J Orthop Res 16: 330e339, 1998
Luk KD, Chen Y, Cheung KM, Kung HF, Lu WW, Leong JC: Adeno-associated virus-mediated bone morphogenetic protein-4 gene therapy for in vivo boneformation. Biochem Biophys Res Commun 308: 636e645, 2003
Lysaght MJ, Reyes J: The growth of tissue engineering. Tissue Eng 7: 485e493, 2001Mahr JA, Gooding LR: Immune evasion by adenoviruses. Immunol Rev 168:
121e130, 1999Marx JC, Allay JA, Persons DA, Nooner SA, Hargrove PW, Kelly PF, et al: High-ef fi-
ciency transduction and long-term gene expression with a murine stem cellretroviral vector encoding the green fluorescent protein in human marrowstromal cells. Hum Gene Ther 10: 1163e1173, 1999
Mason JM, Grande DA, Barcia M, Grant R, Pergolizzi RG, Breitbart AS: Expression of human bone morphogenic protein 7 in primary rabbit periosteal cells: potentialutility in gene therapy for osteochondral repair. Gene Ther 5: 1098e1104, 1998
McCormack JE, Martineau D, DePolo N, Maifert S, Akbarian L, Townsend K, et al:Anti-vector immunoglobulin induced by retroviral vectors. Hum Gene Ther 8:1263e1273, 1997
Miller DG, Adam MA, Miller AD: Gene transfer by retrovirus vectors occurs only incells that are actively replicating at the time of infection. Mol Cell Biol 10:4239e4242, 1990
Miura Y, Yoshida K, Nishimoto T, Hatanaka K, Ohnami S, Asaka M, et al: Directselection of targeted adenovirus vectors by random peptide display on the fiberknob. Gene Ther 14: 1448e1460, 2007
Monahan PE, Samulski RJ: Adeno-associated virus vectors for gene therapy: morepros than cons? Mol Med Today 6: 433e440, 2000
Moutsatsos IK, Turgeman G, Zhou S, Kurkalli BG, Pelled G, Tzur L, et al: Exogenouslyregulated stem cell-mediated gene therapy for bone regeneration. Mol Ther 3:449
e461, 2001
Musgrave DS, Bosch P, Ghivizzani S, Robbins PD, Evans CH, Huard J: Adenovirus-mediated direct gene therapy with bone morphogenetic protein-2 producesbone. Bone 24: 541e547, 1999
Musgrave DS, Bosch P, Lee JY, Pelinkovic D, Ghivizzani SC, Whalen J, et al: Ex vivogene therapy to produce bone using different cell types. Clin Orthop Relat Res2000: 290e305, 2000
Muzyczka N: Use of adeno-associated virus as a general transduction vector formammalian cells. Curr Top Microbiol Immunol 158: 97e129, 1992
Mykhaylyk O, Antequera YS, Vlaskou D, Plank C: Generation of magnetic nonviralgenetransfer agents and magnetofection in vitro. NatProtoc2: 2391e2411, 2007
Niklason LE, Langer R: Prospects for organ and tissue replacement. JAMA 285:573e576, 2001
Noguchi P: Risks and benefits of gene therapy. N Engl J Med 348: 193e194, 2003Oakes DA, Lieberman JR: Osteoinductive applications of regional gene therapy: ex
vivo gene transfer. Clin Orthop Relat Res (379 Suppl.): S101eS112, 2000Oringer RJ: Biological mediators for periodontal and bone regeneration. Compend
Contin Educ Dent 23, 2002 501e504, 506e510, 512 passim; quiz 518
Ozkaynak E, Rueger DC, Drier EA, Corbett C, Ridge RJ, Sampath TK, et al: OP-1 cDNAencodes an osteogenic protein in the TGF-beta family. Embo J 9: 2085e2093,1990
Pack DW, Hoffman AS, Pun S, Stayton PS: Design and development of polymers forgene delivery. Nat Rev Drug Discov 4: 581e593, 2005
Park J, Ries J, Gelse K, Kloss F, von der Mark K, Wiltfang J, et al: Bone regeneration incritical size defects by cell-mediated BMP-2 gene transfer: a comparison of adenoviral vectors and liposomes. Gene Ther 10: 1089e1098, 2003
Peng H, Wright V, Usas A, Gearhart B, Shen HC, Cummins J, Huard J: Synergisticenhancement of bone formation and healing by stem cell-expressed VEGF andbone morphogenetic protein-4. J Clin Invest 110: 751e759, 2002
Plank C, Anton M, Rudolph C, Rosenecker J, Krotz F: Enhancing and targeting nucleicacid delivery by magnetic force. Expert Opin Biol Ther 3: 745e758, 2003
Plank C, Scherer F, Schillinger U, Bergemann C, Anton M: Magnetofection:enhancing and targeting gene delivery with superparamagnetic nanoparticlesand magnetic fields. J Liposome Res 13: 29e32, 2003
Plank C, Schillinger U, Scherer F, Bergemann C, Remy JS, Krotz F, et al: The mag-netofection method: using magnetic force to enhance gene delivery. Biol Chem384: 737e747, 2003
Putnam D, Doody A: RNA-interference effectors and their delivery. Crit Rev TherDrug Carrier Syst 23: 137e164, 2006
Rabinowitz JE, Samulski J: Adeno-associated virus expression systems for genetransfer. Curr Opin Biotechnol 9: 470e475, 1998
Reddi AH: Regulation of cartilage and bone differentiation by bone morphogeneticproteins. Curr Opin Cell Biol 4: 850e855, 1992
Ripamonti U, Duneas N: Tissue morphogenesis and regeneration by bonemorphogenetic proteins. Plast Reconstr Surg 101: 227e239, 1998
Ripamonti U, Reddi AH: Periodontal regeneration: potential role of bone morpho-genetic proteins. J Periodontal Res 29: 225e235, 1994
Ripamonti U, Reddi AH: Tissue engineering, morphogenesis, and regeneration of the periodontal tissues by bone morphogenetic proteins. Crit Rev Oral Biol Med8: 154e163, 1997
Roth CM, Sundaram S: Engineering synthetic vectors for improved DNA delivery:insights from intracellular pathways. Annu Rev Biomed Eng 6: 397e426,2004
Rundle CH, Miyakoshi N, Kasukawa Y, Chen ST, Sheng MH, Wergedal JE, et al: In vivobone formation in fracture repair induced by direct retroviral-based genetherapy with bone morphogenetic protein-4. Bone 32: 591e601, 2003
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e64 63

8/3/2019 Local Bone Regeneration
http://slidepdf.com/reader/full/local-bone-regeneration 11/11
Rutherford RB, Moalli M, Franceschi RT, Wang D, Gu K, Krebsbach PH: Bonemorphogenetic protein-transduced human fibroblasts convert to osteoblastsand form bone in vivo. Tissue Eng 8: 441e452, 2002
Sailaja G, HogenEsch H, North A, Hays J, Mittal SK: Encapsulation of recombinantadenovirus into alginate microspheres circumvents vector-specific immuneresponse. Gene Ther 9: 1722e1729, 2002
Scaduto AA, Lieberman JR: Gene therapy for osteoinduction. Orthop Clin North Am30: 625e633, 1999
Schek RM, Hollister SJ, KrebsbachPH: Deliveryand protection of adenoviruses usingbiocompatible hydrogels for localized gene therapy. Mol Ther 9: 130e138, 2004
Schliephake H, Aref A, Scharnweber D, Bierbaum S, Roessler S, Sewing A: Effect of immobilized bone morphogenic protein 2 coating of titanium implants on peri-implant bone formation. Clin Oral Implants Res 16: 563e569, 2005
Schmidmaier G, Schwabe P, Wildemann B, Haas NP: Use of bone morphogeneticproteins for treatment of non-unions and future perspectives. Injury 4(38Suppl.): S35eS41, 2007
Schmidmaier G, Wildemann B, Gabelein T, Heeger J, Kandziora F, Haas NP, et al:Synergistic effect of IGF-I and TGF-beta1 on fracture healing in rats: singleversus combined application of IGF-I and TGF-beta1. Acta Orthop Scand 74:604e610, 2003
Schmidmaier G, Wildemann B, Heeger J, Gabelein T, Flyvbjerg A, Bail HJ, et al:Improvement of fracture healing by systemic administration of growthhormone and local application of insulin-like growth factor-1 and transforminggrowth factor-beta1. Bone 31: 165e172, 2002
Seeherman H, Wozney J, Li R: Bone morphogenetic protein delivery systems. Spine27: S16eS23, 2002
Shou Y, Ma Z, Lu T, Sorrentino BP: Unique risk factors for insertional mutagenesis ina mouse model of XSCID gene therapy. Proc Natl Acad Sci U S A 103:11730e11735, 2006
Sigurdsson TJ, Nygaard L, Tatakis DN, Fu E, Turek TJ, Jin L, et al: Periodontal repair indogs: evaluation of rhBMP-2 carriers. Int J Periodontics Restorative Dent 16:524e537, 1996
Smeets R, Maciejewski O, Gerressen M, Spiekermann H, Hanisch O, Riediger D, et al:Impact of rhBMP-2 on regeneration of buccal alveolar defects during theosseointegration of transgingival inserted implants. Oral Surg Oral Med OralPathol Oral Radiol Endod 108: e3ee12, 2009
Spagnou S, Miller AD, Keller M: Lipidic carriers of siRNA: differences in theformulation, cellular uptake, and delivery with plasmid DNA. Biochemistry 43:13348e13356, 2004
Storrie H, Mooney DJ: Sustained delivery of plasmid DNA from polymeric scaffoldsfor tissue engineering. Adv Drug Deliv Rev 58: 500e514, 2006
Sykaras N, Opperman LA: Bone morphogenetic proteins (BMPs): how do theyfunction and what can they offer the clinician? J Oral Sci 45: 57e73, 2003
Tancred DC, Carr AJ, McCormack BA: Development of a new synthetic bone graft. J Mater Sci Mater Med 9: 819e823, 1998
Tepper OM, Mehrara BJ: Gene therapy in plastic surgery. Plast Reconstr Surg 109:716e734, 2002
Terheyden H, Warnke P, Dunsche A, Jepsen S, Brenner W, Palmie S, et al:Mandibular reconstruction with prefabricated vascularized bone grafts usingrecombinant human osteogenic protein-1: an experimental study in miniaturepigs. Part II: transplantation. Int J Oral Maxillofac Surg 30: 469e478, 2001
Terrell TG, Working PK, Chow CP, Green JD: Pathology of recombinant humantransforminggrowth factor-beta1 inrats andrabbits.Int RevExp Pathol34(Pt B):43e67,1993
Ueblacker P, Wagner B, Vogt S, Salzmann G, Wexel G, Kruger A, et al: In vivoanalysis of retroviral gene transfer to chondrocytes within collagen scaffoldsfor the treatment of osteochondral defects. Biomaterials 28: 4480e4487,2007
Uludag H, Friess W, Williams D, Porter T, Timony G, D ’Augusta D, et al: rhBMP-collagen sponges as osteoinductive devices: effects of in vitro sponge charac-teristics and protein pI on in vivo rhBMP pharmacokinetics. Ann N Y Acad Sci
875: 369e
378, 1999Urist MR: Bone: formation by autoinduction. Science 150: 893e899, 1965Vogt S, Ueblacker P, Geis C, Wagner B, Wexel G, Tischer T, et al: Ef ficient and stable
gene transfer of growth factors into chondrogenic cells and primary articularchondrocytes using a VSV.G pseudotyped retroviral vector. Biomaterials 29:1242e1249, 2008
Wang EA: Bone morphogenetic proteins (BMPs): therapeutic potential in healingbony defects. Trends Biotechnol 11: 379e383, 1993
Wang EA, Rosen V, Cordes P, Hewick RM, Kriz MJ, Luxenberg DP, et al: Purificationand characterization of other distinct bone-inducing factors. Proc Natl Acad SciU S A 85: 9484e9488, 1988
Wang EA, Rosen V, D’Alessandro JS, Bauduy M, Cordes P, Harada T, et al:Recombinant human bone morphogenetic protein induces bone formation.Proc Natl Acad Sci U S A 87: 2220e2224, 1990
Warnke PH, Springer IN, Acil Y, Julga G, Wiltfang J, Ludwig K, et al: The mechanicalintegrity of in vivo engineered heterotopic bone. Biomaterials 27: 1081e1087,2006
Warnke PH, Springer IN, Wiltfang J, Acil Y, Eufinger H, Wehmoller M, et al: Growthand transplantation of a custom vascularised bone graft in a man. Lancet 364:766
e770, 2004
Wiethoff CM, Middaugh CR: Barriers to nonviral gene delivery. J Pharm Sci 92:203e217, 2003
Winet H, Hollinger JO: Incorporation of polylactideepolyglycolide in a corticaldefect: neoosteogenesis in a bone chamber. J Biomed Mater Res 27: 667e676,1993
Winn SR, Uludag H, Hollinger JO: Carrier systems for bone morphogenetic proteins.Clin Orthop Relat Res (367 Suppl.): S95eS106, 1999
Wozney JM: The bone morphogenetic protein family and osteogenesis. Mol ReprodDev 32: 160e167, 1992
Wozney JM, Rosen V, Celeste AJ, Mitsock LM, Whitters MJ, Kriz RW, et al: Novelregulators of bone formation: molecular clones and activities. Science 242:1528e1534, 1988
Yang S, Wei D, Wang D, Phimphilai M, Krebsbach PH, Franceschi RT: In vitro and invivo synergistic interactions between the Runx2/Cbfa1 transcription factor andbone morphogenetic protein-2 in stimulating osteoblast differentiation. J BoneMiner Res 18: 705e715, 2003
Zhang X, Godbey WT: Viral vectors for gene delivery in tissue engineering. Adv
Drug Deliv Rev 58: 515e
534, 2006Zhao M, Zhao Z, Koh JT, Jin T, Franceschi RT: Combinatorial gene therapy for boneregeneration: cooperative interactions between adenovirus vectors expressingbone morphogenetic proteins 2, 4, and 7. J Cell Biochem 95: 1e16, 2005
J. Fischer et al. / Journal of Cranio-Maxillo-Facial Surgery 39 (2011) 54e6464