lower-extremity peripheral nerve blockade: essentials of ...nerves to the muscles of the anterior...
TRANSCRIPT
�
LE
FAa
TwnlnstbutciftmemescdmoTb
CsstLmCR
AE
P
4
Original Articles
ower-Extremity Peripheral Nerve Blockade:ssentials of Our Current Understanding
. Kayser Enneking, M.D., Vincent Chan, M.D., Jenny Greger, M.D.,dmir Hadzic, M.D., Ph.D., Scott A. Lang, B.Sc., M.D., F.R.C.P.C.,
nd Terese T. Horlocker, M.D.adn
LA
dcctbfDl2awitcbitnttastlcnr
L
mb
he American Society of Regional Anesthesiaand Pain Medicine introduced an intensive
orkshop focused on lower-extremity peripheralerve blockade in 2002. This review is the compi-
ation of that work. Details concerning the tech-iques described in this text are available at the webite ASRA.com, including video demonstrations ofhe blocks. Lower-extremity peripheral nervelocks (PNBs) have never been as widely taught orsed as other forms of regional anesthesia. Unlikehe upper extremity, the entire lower extremityannot be anesthetized with a single injection, andnjections are generally deeper than those requiredor upper extremity block. In addition, neuraxialechniques are widely taught and use alternativeethods for providing reliable lower-extremity an-
sthesia. Over the past decade, several develop-ents have led to an increased interest in lower
xtremity PNBs, including transient neurologicymptoms associated with spinal anesthesia, in-reased risk of epidural hematoma with the intro-uction of antithromboembolic prophylaxis regi-ens, and evidence of improved rehabilitation
utcome with continuous lower-extremity PNBs.his review will focus on the anatomy of the lum-osacral plexus and its terminal nerves, followed by
From the Department of Anesthesiology, University of Floridaollege of Medicine, Gainesville, FL (F.K.E.); Regional Anesthe-ia and Acute Pain Service, University Health Network, Univer-ity of Toronto, Ontario, Canada (V.C.); Greater Houston Anes-hesia, Houston, TX (A.H.); Department of Anesthesiology, Stuke’s/Roosevelt Hospital Center, New York, NY (J.G.); Depart-ent of Anesthesia, University of Calgary, Calgary, Alberta,anada (S.A.L.); and Department of Anesthesia, Mayo Clinic,ochester, MN.Accepted for publication October 13, 2004.Reprint requests to F. Kayser Enneking, M.D., Department ofnesthesiology, PO Box 100254, Gainesville, FL 32610-0254.-mail: [email protected]© 2005 by the American Society of Regional Anesthesia and
ain Medicine.
g1098-7339/05/3001-0002$30.00/0doi:10.1016/j.rapm.2004.10.002
Regional Anesthesia and Pain Medicine, Vol 30,
discussion of techniques and applications. In ad-ition, we will review neural localization tech-iques and potential complications.
ower-Extremity Peripheral Nervenatomy
Lower-extremity PNB requires a thorough un-erstanding of the neuroanatomy of the lumbosa-ral plexus. Anatomically, the lumbosacral plexusonsists of 2 distinct entities: the lumbar plexus andhe sacral plexus. There is some communicationetween these plexi via the lumbosacral trunk, butor functional purposes these are distinct entities.1
etails of the motor and sensory branches of theumbosacral plexus are summarized in Tables 1 and
and Figures 1 and 2. The lumbosacral plexusrises from at least 8 spinal nerve roots, each ofhich contains anterior and posterior divisions that
nnervate the embryologic ventral or dorsal por-ions of the limb. With the exception of a smallutaneous portion of the buttock (which is suppliedy upper lumbar and sacral segmental nerves), thennervation of the lower extremity is entirelyhrough branches of the lumbosacral plexus. Theerves to the muscles of the anterior and medialhigh are from the lumbar plexus. The muscles ofhe buttocks, the posterior muscles in the thigh, andll the muscles below the knee are supplied by theacral plexus. There are a multitude of approacheso each peripheral nerve block described for theower extremity. Thus, a detailed review of theourse of each of the relevant terminal peripheralerves of the lower extremity is warranted in thiseview.
umbar Plexus Anatomy
The lumbar plexus is formed within the psoasuscle from the anterior rami of T12-L4.1-4 The
ranches of this plexus, the iliohypogastric, ilioin-
uinal, genitofemoral, lateral femoral cutaneous,No 1 (January–February), 2005: p 4–35

ap3ae
bsof
bdominelectric
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 5
nd femoral and obturator nerves emerge from thesoas laterally, medially, and anteriorly (Figs 2 and). Of these, the femoral, lateral femoral cutaneous,nd obturator nerves are most important for lower-xtremity surgery.
Table 1. Lumb
NerveSpinal
Segment Motor Innervation
Iliohypogastric T12-L1 Int/ext oblique AntTransverse abdominis
Ilioinguinal L1 Int oblique Ant
Genitofemoral L1-L2 Cremaster Test
Lateral FemoralCutaneous
L2-L3 None
Femoral L2-L4Anterior division Sartorious Med
thPectineus Add
Posterior division Quadriceps Kneas
Saphenous
Obturator L2-L4Anterior division Gracilus, adductor brevis &
longus pectineusThig
Posterior division Obturator externus,adductor magnus
Thigla
Abbreviations: Int, internal; Ext, external; Ant, anterior; Abd, a*Motion observed refers to the observed motor response with
Table 2. Sacr
NerveSpinal
Segment Motor Innervation
Gluteal nerves L4-S2 Piriformis, sup/inf gemellusobturator internus,quadratus femoris
B
Sciatic, tibial L4-S3 Biceps femoris,semitendinosus,adductor magnus
H
Popliteus KP
Gastrocnemius, soleus,flexors of foot
T
Sciatic, peronealSuperficial
L4-S3 Short head of bicepsfemoris peroneuslongus, brevis
KF
Deep Extensors of foot, toes D
Sural None None NComponents from
peroneal & tibialP
Post cut nerve ofthigh
S1-S3 None N
Abbreviations: Sup, superior; Inf, inferior; Lat, lateral; Post, posterior;*Motion observed refers to the observed motor response with electric
Femoral Nerve. The femoral nerve is formedy the dorsal divisions of the anterior rami of theecond, third, and fourth lumbar nerves. The fem-ral nerve emerges from the psoas muscle in aascial compartment between the psoas and iliacus
xus Anatomy
Observed* Sensory InnervationArticular
Branches
inal wall Inferior abd wall NoneUpper lat quadrant of buttock
inal wall Inferior to medial aspect ofinguinal ligament
None
Portion of genitaliaInferior to mid portion of
inguinal ligamentNone
Spermatic cordAnterior lateral and posterior
aspects of thighterminating in prepatellarplexus
ect of the lower Anterior medial skin of thethigh
None
f thigh Nonesion, patellarn
Ant thigh Hip and knee
Medial leg from the tibia tothe medial aspect of thefoot
ction Variable, posterior medialthigh, medial knee
Hip
ction withp rotation
Knee
al; Lat, lateral.al stimulation of that nerve.
xus Anatomy
Observed* Sensory Innervation Articular Branches
with lat hipn
Upper medial aspect ofbuttock
Hip
gs with kneesion
Medial and lat heelSole of foot
Hip knee, and ankle
xionflexionion
xionersion
Distal anterior leg,dorsum of foot
Knee and ankle
ion of foot, Web space of 1st toe Ankle
Nonef, lat bordert and 5th toe
None
Distal medial quadrantof buttock perineum,post thigh includingpopliteal fossa
None
ar Ple
Motion
abdom
abdom
icular
ial aspighuctor oe extencensio
h addu
h adduteral hi
al Ple
Motion
uttocksrotatio
amstrinexten
nee flelantaroe flex
nee fleoot inv
orsiflexankle
oneost calof foo
one
Cut, cutaneous.al stimulation of that nerve.
mtlfttt
dtpnfs
otsasttwrr
tmdsmait
bsdnobs
Fp
Flt
Fiowi
6 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
uscles, in which it gives off articular branches tohe hip. It enters the thigh posterior to the inguinaligament. There it lies lateral and posterior to theemoral artery. This relationship to the femoral ar-ery exists near the inguinal ligament, but not afterhe nerve enters the thigh. As the nerve passes intohe thigh, it divides into an anterior and a posterior
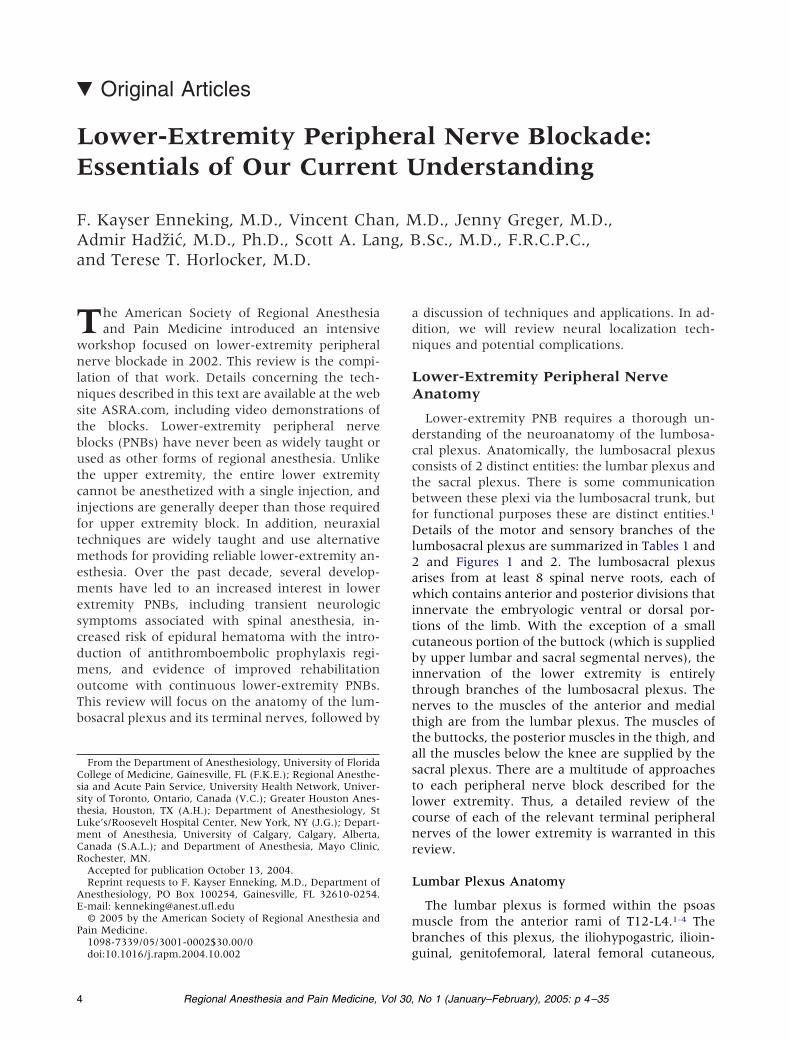
ig 1. Dermatomes and osteotomes of the lumbosacrallexus are illustrated. (Courtesy of Mayo Foundation.)
ig 2. Lumbosacral plexus. Anatomic depiction of theumbosacral plexus with the major peripheral nerves of
Ahe lower extremity. (Courtesy of Mayo Foundation.)
ivision and quickly arborizes (Fig 4). At the level ofhe inguinal ligament, there are dense fasciallanes, the fascia lata, and fascia iliaca. The femoralerve is situated deep to these fascial planes. The
emoral artery, vein, and lymphatics reside in aeparate fascial compartment medial to the nerve.
The anterior division of the femoral nerve givesff the medial and intermediate cutaneous nerveshat supply the skin of the medial and anteriorurfaces of the thigh. The muscular branches of thenterior division of the femoral nerve supply theartorius muscle and the pectineus muscle and ar-icular branches to the hip. The posterior division ofhe femoral nerve gives off the saphenous nerve,hich is the largest cutaneous branch of the femo-
al nerve, and the muscular branches to the quad-iceps muscle and articular branches to the knee.
The terminal nerves of the posterior division ofhe femoral nerve, the saphenous and the vastusedialis nerves, continue distally through the ad-
uctor canal. After leaving the adductor canal, theaphenous nerve emerges from behind the sartoriususcle, in which it gives off an infrapatellar branch
nd then continues distally to supply the cutaneousnnervation of the anteromedial lower leg down tohe medial aspect of the foot.
Obturator Nerve. The obturator nerve is aranch of the lumbar plexus formed within theubstance of the psoas muscle from the anteriorivision of the second, third, and fourth lumbarerves. It is the nerve of the adductor compartmentf the thigh, which it reaches by piercing the medialorder of the psoas and passing straight along theidewall of the pelvis to the obturator foramen.
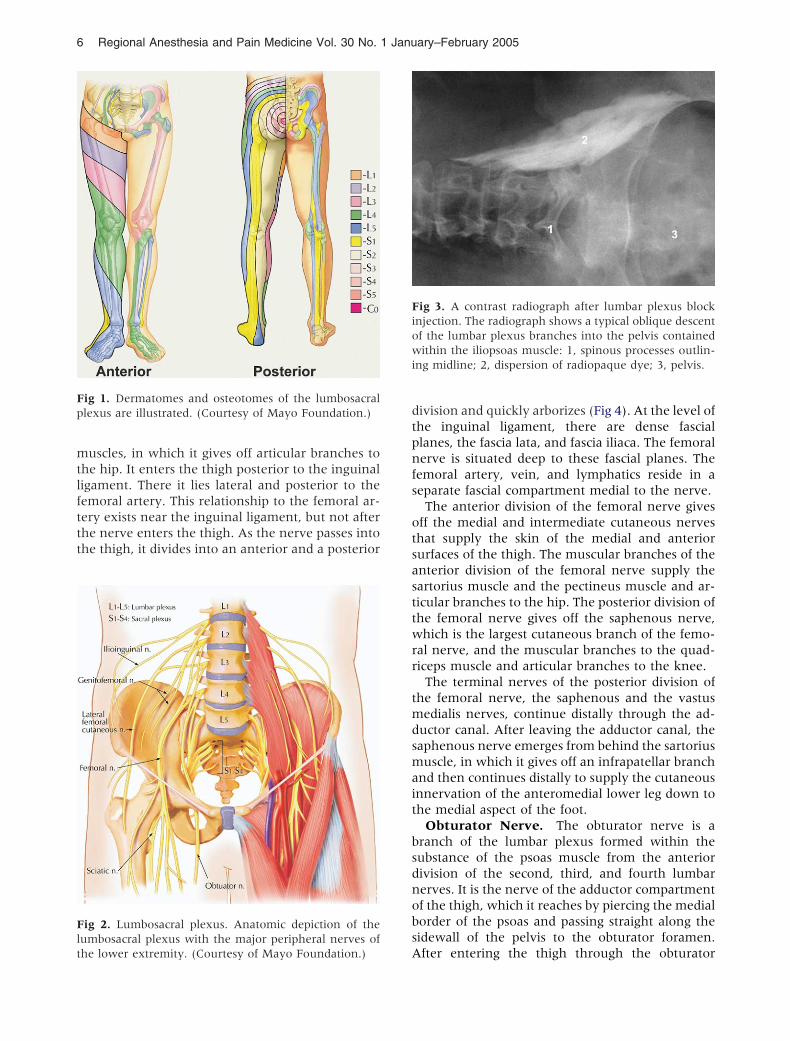
ig 3. A contrast radiograph after lumbar plexus blocknjection. The radiograph shows a typical oblique descentf the lumbar plexus branches into the pelvis containedithin the iliopsoas muscle: 1, spinous processes outlin-
ng midline; 2, dispersion of radiopaque dye; 3, pelvis.
fter entering the thigh through the obturator

gtbajtiTnbfp
mttstdeb
skbnTfsimrsoat
e
Fanmv
Ftor
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 7
roove, the nerve divides into an anterior and pos-erior division. The anterior division has threeranches including the muscular branches to thedductor muscles, an articular branch to the hipoint, and a cutaneous branch to the medial side ofhe thigh. The extent of this cutaneous sensorynnervation has been investigated by Bouaziz et al.5
hese investigators performed an isolated obturatorerve block on patients before a femoral nervelock. All the obturator nerve blocks were success-ul as shown by adductor paresis. In 57% of the
ig 4. Anatomy of the femoral nerve in the inguinalrea: 1, femoral nerve; 2, lateral femoral cutaneouserve; 3, branches of the femoral nerve to the sartoriususcle; 4, inguinal ligament; 5, femoral artery; 6, femoral
ein.
atients, there was no cutaneous sensory loss de- n
onstrable. In 23% of patients, a zone of hypoes-hesia was present on the superior medial aspect ofhe popliteal fossae. Only 20% of the patientshowed a sensory deficit on the inferior aspect ofhe medial thigh. The inconsistency of the sensoryistribution of the obturator nerve must be consid-red when evaluating reports of obturator nervelock success rates based on sensory findings only.The posterior division of the obturator nerve de-
cends with the femoral and popliteal artery to thenee joint, and forms 2 branches: a muscularranch to the external obturator and adductor mag-us muscles and an articular branch to the knee.he divergence of the obturator nerve from theemoral nerve begins as they emerge from the sub-tance of the psoas muscle. At the level of thenguinal ligament, the obturator nerve lies deep and
edial relative to the femoral nerve and is sepa-ated from it by several fascial compartments. Thiseparation at the level of the inguinal ligament isbvious in anatomic dissections (Fig 5)6 and haslso been shown both radiographically with con-rast and by magnetic resonance image.7,8
Lateral Femoral Cutaneous Nerve. The lat-ral femoral cutaneous nerve is formed by union of
ig 5. Organization of the lumbar plexus components athe level of the inguinal ligament: 1, femoral nerve; 2,bturator nerve; 3, genitofemoral nerve; 4, lateral femo-al cutaneous nerve; 5, psoas muscle; 6, ureter; 7, iliacus
erve and vein; 8, rectum.
fipllfAlpcwnipm
S
tfifblsttpphngn
amrnptttsinfitdtpparpwd
stpfpdtnSnosntevcpt
ns
Ftcst
8 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
bers from the posterior division of the anteriorrimary rami of L2 and L3. It emerges from theateral border of psoas major below the iliolumbarigament, passing around the iliac fossa on the sur-ace of the iliacus muscle deep to the iliac fascia.bove the inguinal ligament, it slopes forward and
ies inside the fibrous tissue of the iliac fascia. Iterforates the inguinal ligament approximately 1m from the anterior superior iliac spine fromhere it enters the thigh. The lateral femoral cuta-eous nerve supplies the parietal peritoneum of the
liac fascia and the skin over a widely variable as-ect of the lateral and anterior thigh.9 It has nootor innervation.
acral Plexus Anatomy
The sacral plexus is formed within the pelvis byhe merger of the ventral rami of the fourth andfth lumbar and the first 3 or 4 sacral nerves. The
ourth and fifth lumbar ventral rami are common tooth the lumbar and the sacral plexus and theumbosacral trunk.10 Of the 12 branches of theacral plexus, 5 are distributed within the pelvis andhe other 7 emerge from the pelvis to distribute tohe buttock and the lower extremity. The sacrallexus provides motor and sensory innervation toortions of the entire lower extremity including theip, knee, and ankle. The most important compo-ents of the sacral plexus for lower-extremity sur-ery are the sciatic and the posterior cutaneouserves and their terminal branches.Sciatic Nerve. The lumbosacral trunk (L4-L5)
nd anterior divisions of the sacral plexus (S1-S3)erge to form the tibial nerve, whereas the poste-
ior divisions merge to form the common peronealerve. These 2 large mixed nerves of the sacrallexus are initially bound together by connectiveissue to form the sciatic nerve. At this level, theibial component is medial and anterior, whereashe common peroneal component is lateral andlightly posterior (Fig 6). The superior gluteal arterys immediately superior and medial to the sciaticerve at the level of the piriformis. Doppler identi-cation of the superior gluteal artery has been usedo help identify appropriate needle insertion siteuring sciatic nerve block.11 The sciatic nerve exitshe pelvis via the greater sciatic notch below theiriformis muscle.12 At this level, it lies lateral andosterior to the ischial spine. As it enters the thighnd descends toward the popliteal fossa, it is poste-ior to the lesser trochanter of the femur, on theosterior surface of the adductor magnus muscleithin the posterior medial thigh compartment
eep to biceps femoris. There is no artery after a bimilar course because the chief blood supply to thehigh is through the anterior femoral artery. Theopliteal artery and vein, the continuation of theemoral artery and vein, reach the popliteal fossa byassing through the adductor hiatus and continueownward with the artery anterior to the vein. Inhe upper part of the popliteal fossa, the sciaticerve lies posterolateral to the popliteal vessels.pecifically, the popliteal vein is medial to theerve, whereas the popliteal artery is anterior, lyingn the popliteal surface of the femur (Fig 7). Theciatic nerve usually divides into its componenterves, the tibial and common peroneal nerves, athe upper aspect of the popliteal fossa. In a cadav-ric evaluation, Vloka et al.13 reported that the di-ision of the sciatic nerve into its components oc-urs at a mean distance of 6 � 3 cm above theopliteal crease. However, in this small sampling,he range was quite large (0-11.5 cm).
Tibial Nerve. In the popliteal fossa, the tibialerve lies posterior and lateral to the popliteal ves-els (Fig 8). In the lower part of the fossa, it sends
ig 6. Proximal anatomy of the sciatic nerve in the glu-eal region: 1, greater trochanter; 2, common peronealomponent of the sciatic nerve; 3, tibial component of theciatic nerve; 4, ischial tuberosity; 5, superior gluteal ar-ery; 6, inferior gluteal artery.
ranches to the major ankle plantar flexors, the

gtps
c9gtstlm
dcswndndnmsgpT(stla
Frvtca
FsnftpF
FobbmF
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 9
astrocnemius, and soleus muscles. The tibial nervehen courses on the posterior surface of the tibialisosterior muscle, along with the posterior tibial ves-els. At the ankle, the nerve and vessels enter a
ig 7. An MRI image of the popliteal fossa showing theelationship of the components of the sciatic nerve to theessels and femur: 1, femur; 2, biceps femoris; 3, semi-endinosus/semimembranosus; 4, sciatic nerve (tibial andommon peroneal components are seen); 5, poplitealrtery and vein.
ig 8. Popliteal fossa cross-sectional view. This figurehows needle position for a lateral approach to the sciaticerve in the supine patient at the level of the popliteal
ossa. Note the components of the sciatic nerve are pos-erior and lateral to the vessels. m, muscle; n, nerve; post,osterior; lat, lateral; t, tendon. (Courtesy of Mayo
toundation.)
ompartment beneath the flexor retinaculum (Fig). As it passes to the plantar aspect of the foot, itives off the lateral and medial plantar nerves. Ofhe digital nerves, those to the medial 3½ toes areupplied by the medial plantar nerve, whereashose of the lateral 1½ toes are supplied by theateral plantar nerve; a distribution similar to the
edian and ulnar nerves in the hand.Peroneal Nerve. The common peroneal nerve
iverges laterally leaving the popliteal fossa byrossing the lateral head of the gastrocnemius. It liesubcutaneously just behind the fibular head, inhich it can be easily traumatized. As it rounds theeck of the fibula, the common peroneal nerveivides into its terminal branches, the deep pero-eal nerve and the superficial peroneal nerve. Theeep peroneal nerve continues distally, accompa-ied by the anterior tibial artery, on the interosseusembrane. Nerve and artery emerge on the dor-
um of the foot between the extensor hallucis lon-us and tibialis anterior. At this level, the deeperoneal nerve is lateral to the dorsalis pedis artery.he deep peroneal nerve innervates the extensordorsiflexor) muscles of the foot and the first web-pace. The superficial peroneal nerve descends inhe lateral compartment, between the peroneusongus and brevis muscles. After supplying thesenkle evertors innervates, it emerges between them
ig 9. Ankle cross-sectional image. The figure at the levelf malleolus shows the typical distribution of the terminalranches of the sciatic nerve that comprise an anklelock. t, tendon; a, artery; v, vein; lig, ligament; n, nerve;emb, membrane; m, muscle. (Courtesy of Mayo
oundation.)
o innervate the skin of the lower leg and foot.

psSpgnplmulbalt
ntttt
A
N
patltpfattt1
tvLtatamcotttudo
pstmesTlcdattrpdvp1
cncamnetEs9Dsetetvmbttbt
tsoffcvna
10 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
Posterior Femoral Cutaneous Nerve. Theosterior femoral cutaneous nerve is a purely sen-ory nerve derived from the anterior rami of S1-3.14 It travels with the sciatic nerve out of theelvis and into the upper thigh. While deep to theluteus maximus, it gives off the inferior clunialerves (sensory nerves to the lower buttock) anderineal branches (sensory to the external genita-ia). It emerges from the lower edge of the gluteus
aximus to lie in subcutaneous tissue and contin-es down the posterior aspect of the thigh and the
eg giving off, in succession, femoral and suralranches (sensory branches to the back of the thighnd the calf). It becomes superficial near the pop-iteal fossa where its terminal branches often anas-omose with the sural nerve.
Sural Nerve. The medial and lateral suralerves are pure sensory nerves derived from theibial and common peroneal nerves, respectively, athe level of the knee joint. Together, they supplyhe posterolateral aspect of the leg and ankle andhe dorsal surface of the foot.
pproaches to the Lower Extremity
erve Blocks of the Lumbar Plexus
Psoas Compartment Block. The psoas com-artment block was first described by Chayen etl.15 in 1976. It can be performed as a single-injec-ion technique or with a catheter placed for pro-onged analgesia. It has been used to provide anes-hesia for thigh surgery. In combination witharasacral nerve block, it has been used for hipracture repair.16 It is successfully used for analgesiafter total hip arthroplasty (THA) or total knee ar-hroplasty (TKA).2,4,17,18 It has also been used in thereatment of chronic hip pain.19 The distribution ofhe psoas compartment block is shown in Figure0A.The psoas compartment block is a deep block of
he lumbar plexus from a posterior approach. Tra-ersing from posterior to anterior at the level of4-L5, the following structures would be encoun-ered: posterior lumbar fascia, paraspinous muscles,nterior lumbar fascia, quadratus lumborum, andhe psoas muscle6,20 (Fig 10D). The common iliacrtery and vein are situated anterior to the psoasuscle, which is inside a fascial sheath, the psoas
ompartment (Fig 3). Because the final positioningf the needle is within the body of the psoas musclehrough which the lumbar plexus traverses, it ishought to be the most consistent approach to blockhe entire lumbar plexus with a single injection. It isseful for providing consistent anesthesia in theistributions of the femoral, lateral femoral cutane-
us, and the obturator nerves (Fig 10A). tSeveral descriptions of the needle entry site for thesoas compartment blocks have been de-cribed.2,3,21-24 All rely on bony contact with theransverse process as a guide to depth of needle place-ent. Capedevila et al.2 described a slightly modified
ntry point based on computed tomography (CT)cans of the lumbar plexus of patients undergoingHA. They estimated the distance from the skin to theumbar plexus to be 8.35 cm in men (range 6.1-10.1m) and 7.1 cm in women (range 5.7- 9.3 cm). Theepth of the lumbar plexus correlated with gendernd body mass index. Importantly, the distance fromhe transverse process to the lumbar plexus was ex-remely consistent at a distance of less than 2 cm. Thiselationship of transverse process to the lumbarlexus was independent of body mass index or gen-er. Thus, contact with the transverse process pro-ides a consistent landmark to avoid excessive needleenetration during psoas compartment block2 (Fig0B-D).The depth of needle insertion is emphasized be-
ause of the complications associated with excessiveeedle depth including renal hematoma, pneumo-ele, total spinal anesthesia, and unintended intra-bdominal, and intervertebral disk catheter place-ent.2,25-27 To ensure the proper position of theeedle during psoas compartment block and avoidxcessive needle insertion, it is highly recommendedhat the transverse process be intentionally sought.pidural spread of local anesthetic is another commonide effect of psoas compartment block, occurring in% to 16% of adult patients3,28 (Table 3). In children,alens et al.29 reported a �90% incidence of epidural
pread when using the original landmarks of Chayent al.15 compared with no epidural spread when usinghe landmarks as modified by Winnie.29 This sideffect is usually attributed to retrograde diffusion ofhe local anesthetic to the epidural space when largeolumes of local anesthetic are used (greater than 20L). In most cases, there is residual lumbar plexus
lockade apparent after the resolution of the con-ralateral block. However, there are case reports ofotal spinal anesthesia occurring during lumbar plexuslockade and vigilance must be maintained duringhe management of this block26,30 (see complications).
Continuous Psoas Compartment Blocks. Continuousechniques have been described to provide analge-ia after a variety of operations including THA, TKA,pen reduction and internal fixation of acetabularractures, open reduction and internal fixation ofemur fractures, and anterior cruciate ligament re-onstruction.2,17,18,31,32 Interest in this block de-eloped as practitioners sought alternatives toeuraxial techniques that could provide consistentnalgesia after hip, femur, and knee surgery. One
heoretical advantage of psoas compartment block
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 11
Fig 10. Psoas compartment block. (A) The sensory distribu-tion of a psoas compartment block is shown on the right. Theosteotomes blocked by the psoas compartment block areshown on the left. (B) Landmarks for the psoas compart-ment block. Needle entry is marked 1 cm cephalad to theintercristal line, two thirds the distance from the midline tothe PSIS line. (C) Psoas compartment deep landmarks ob-served from above. Post, posterior; Ant, anterior. (D) Psoascompartment block, final needle placement. Note the struc-tures deep to the lumbar plexus including major vascularstructures, kidneys, and abdominal contents. (Courtesy ofMayo Foundation.)

oplmm
mlTpnaaa9n
iklf(matrdibfr9c
attddoic
botinbttptottoi(fotcbr
mponet
12 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
ver other continuous approaches to the lumbarlexus is the decreased likelihood of catheter dis-odgement because of the large muscle mass that
ust be traversed to reach the lumbar plexus. Theuscle mass anchors the catheter.Pandin and colleagues32 described a slightly moreedial puncture site for placement of continuous
umbar plexus blocks for postoperative analgesia.hey believed the more medial puncture site im-roved the likelihood of obtaining an obturatorerve block and optimized catheter insertion withn insertion angle of 20° to 30°. They failed to placecatheter in only 3% of their patients and reportedhigh success rate (100% femoral, 93% obturator,1% lateral femoral cutaneous) bolusing through aonstimulating catheter.32
Femoral Nerve Block. Indications for single-njection femoral nerve block include anesthesia fornee arthroscopy in combination with intra-articu-ar local anesthesia and analgesia for femoral shaftractures, anterior cruciate ligament reconstructionACL), and TKA as a part of multimodal regi-ens.33-38 Their use in complex knee operations is
ssociated with lower pain scores and fewer hospi-al admissions after same-day surgery.39 The femo-al nerve divides into the posterior and anteriorivisions shortly after it emerges from under thenguinal ligament and undergoes extensive ar-orization. Commonly, the anterior branch of theemoral nerve will be identified first. Vloka et al.40
eported this to be the first motor response elicited7% of the time. Stimulation of this branch leads to
Table 3. Success Rate of Lumbar P
Reference N Technique
Parkinson28* 27 Psoas @ L3, n.s.23 Psoas @ L4-520 Femoral paresthesia20 Femoral, n.s.†
Seeberger43 39 Femoral, n.s. 20 mL41 Femoral, n.s. 40 mL
Lang42 32 Femoral paresthesia 30 mLFarny3 45 Psoas, n.s. 1.0-0.5 mAMorau73 20 Femoral, n.s. @ 0.5 mA bolus via cathe
20 Fascia iliaca bolus via catheterTokat72 30 Psoas, n.s.
30 Femoral, n.s.Pandin32 132 Psoas n.s.@ 0.3 mA bolus via catheterCapdevila74 50 Femoral n.s. @ 0.5 mA 30 mL
50 Fascia iliaca 30 mLKaloul75 20 Femoral n.s. @ 0.5 mA bolus via cathet
20 Psoas n.s. @ 0.5 mA bolus via catheter
Abbreviations: Fem, femoral; LFC, Lateral femoral cutaneous;*Use of uninsulated needles; no mA given.†These studies reported rate of success for blocking the co
echniques and approaches to the nerves.
ontraction of the sartorius muscle on the medial o
spect of the thigh and should not be accepted, ashe articular and muscular branches derive fromhe posterior branch of the femoral nerve. The nee-le should be redirected slightly laterally and with aeeper direction to encounter the posterior branchf the femoral nerve. Stimulation of this branch isdentified by patellar ascension as the quadricepsontract.
Defining the 3-in-1 Block. During femoral nervelock, it has been advocated to use a higher volumef local anesthetic and apply firm pressure just dis-al to the needle during and a few minutes afternjection to block the femoral, lateral femoral cuta-eous, and obturator nerves, the so-named “3-in-1lock.”41 However, despite many efforts to consis-ently produce a 3-in-1 block, the effectiveness ofhese maneuvers has not been shown. In most re-orts, the femoral nerve is the only nerve consis-ently blocked with this approach.7,8,42,43 Blockadef the lateral femoral cutaneous nerve occurshrough lateral diffusion of local anesthetic and nothrough proximal spread to the lumbar plexus.8 Thebturator nerve is less frequently anesthetized dur-ng 3-in-1 block than the lateral femoral cutaneousLFC), which is not surprising given the number ofascial barriers between these structures at the levelf the inguinal ligament. Despite the lack of scien-ific support for the term 3-in-1, many authors stillontinue to refer to the anterior femoral nervelock as a 3-in-1 block. Within this text, we willefer to this approach as a femoral nerve block.
Continuous Femoral Nerve Block. Continuous fem-
Block With Different Techniques
Sensory Block Motor Block Number of Failures(Number of
Epidural Spread)Fem LFC OBT Fem OBT
95% 100% 100% 7 (4 epidural)95% 100% 100% 3 (1 epidural)95% 100% 0% None reported85% 100% 0% None reported41% 92% 62% 444% 93% 78% 396% 81% 4% 6
100% 100% 100% 5 (4 epidural)00% 70% 88% 286% 92% 55% 200% 97% 77% 80% 63% 0 (2 epidural)93% 63% 47% 73% 30% 300% 93% 91% 80% 63% 4 (2 epidural)90% 62% 52% 76% 32% 588% 90% 38% 80% 20% 6
95% 47% Not reported90% 93% Not reported
obturator; n.s., nerve stimulator.
nts of the lumbar plexus using a variety of nerve localization
lexus
ter 1
1
1
er
OBT,
ral nerve block has been shown to improve outcome

aeashotgpmeapdruaaapnnrpapfrsouw0dlmoMdteaaCccbstr
disl
astli“ttntbt
dtditiu
Fgi
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 13
fter major knee and vascular surgery of the lowerxtremity compared with intravenous narcotic ther-py or continuous infusion or injection of analge-ics.44-50 Chelly et al.46 showed a 20% reduction inospital length of stay in patients receiving continu-us femoral nerve block analgesia compared with pa-ients receiving intravenous patient-controlled anal-esia narcotics after major knee surgery. Tworospective randomized studies examined 3 differentodes of analgesia: continuous femoral nerve block,
pidural analgesia, and intravenous narcotic therapyfter TKA.47,48 These studies showed improvement inerioperative rehabilitation scores and a decreaseduration of stay in a rehabilitation center for patientseceiving the regional anesthesia techniques. Contin-ous femoral nerve block was shown to have equiv-lent analgesia with fewer side effects than epiduralnalgesia in both of these studies.47,48 However, notll investigators have been able to show these im-rovements in outcome with continuous femoralerve blocks. Hirst et al.51 found no differences inarcotic consumption or pain scores between patientseceiving a single-injection femoral nerve block andatients receiving a continuous femoral nerve blockfter TKA. The accuracy of catheter placement maylay a role in these conflicting findings. Continuousemoral nerve blocks have been associated with a highate of inaccurate catheter placement. In a prospectivetudy, Capdevila et al.52 showed that continuous fem-ral nerve block using a standard approach led tonpredictable catheter placement. Their techniqueas to elicit a vastus intermedius muscle response at.5 mA and then insert a catheter 16 to 20 cm afteristending the sheath with 5 mL saline and bolusingocal anesthetic through the catheter. Catheter place-
ent was evaluated radiographically, and only 25%f the catheters were lying near the lumbar plexus.ost of the catheters tended to course medially in the
irection of the psoas muscle or laterally in the direc-ion of the iliacus muscle. The accuracy of final cath-ter placement correlated with the degree of analgesiafter proximal lower limb surgery, although visualnalog scale values were generally low in all groups.52
omparing a stimulating catheter to a nonstimulatingatheter, Salinas and colleagues53 were able to in-rease the success rate of continuous femoral nervelock in volunteers from 85% to 100%. The role oftimulating versus nonstimulating catheters for con-inuous peripheral nerve blocks to improve successate is an active area of research at this time.
Fascia Iliacus Block. Dalens et al.55 originallyescribed the fascia iliacus block in children. Thendications for its use are the same as those foringle-injection femoral nerve block. Advocates be-
ieve its utility lies in the double pop technique for tpplying this block. The double pop refers to theensation felt as the needle traverses the fascia latahen the fascia iliaca (Fig 11). Penetration of bothayers of fascia is important for successful fascialiacus blockade. To facilitate the appreciation of theclicks” or “pops,” the use of a short bevel or pencilipped needle has been advocated to provide moreactile feedback than cutting needles. This tech-ique does not employ the use of a nerve stimula-or. Although transient femoral neuropathy haseen reported after fascia iliacus block, this appearso be a rare occurrence.56
The needle entry site for the fascia iliacus block isetermined by drawing a line between the pubicubercle and the anterior superior iliac crest andividing this line into thirds. The needle entry points 1 cm caudal to the intersection of the medial twohirds and lateral one third along this line. This sites well away from the femoral artery, making thisseful for patients in whom femoral artery punc-
ig 11. Approach to the fascia iliacus block. The needleives a discernible pop as the fascia lata, then the fascialiaca, is traversed. (Courtesy of Mayo Foundation.)
ure is contraindicated.

ifdsohttstptosArwtht
iiatdmsamdpbn
patmdtpfLrLp
wvpansb
r1wsrgn
lapTaflsintrpctc1pvrqHss
CL
PB
encpaiascnratwrn
14 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
Continuous Fascia Iliacus Blocks. Continuous fascialiacus blocks have been described for analgesia afteremur fracture and repair, femoral elongation proce-ures, skin graft harvesting, ligamentous knee recon-truction, and TKA.57,58 Much like femoral continu-us catheters, the degree of analgesia seems to beighly correlated with the final position of the cathe-er. Ganapathy et al.,57 using a modified approach tohe fascia iliacus block with a nerve stimulator,howed a high degree of catheter malpositioning. Inhis study, CT scans found only 40% of catheterslaced were ideally positioned (superior to the upperhird of the sacroiliac joint in the psoas sheath). An-ther variable examined in this study was the infu-ate, saline, 0.1% bupivacaine, or 0.2% bupivacaine.ll the patients in the study had excellent pain relief
egardless of the catheter position or infusate. Thisas attributed to the multimodal analgesic regimen
he patients received. However, the best analgesia wasighly correlated with ideal catheter tip position andhe use of 0.2% bupivacaine.
Obturator Nerve Block. Indications for a single-njection obturator nerve block are generally lim-ted to diagnostic indications or therapeutic relax-tion of the adductor muscles of the thigh.59 Despitehe significant amount of literature that has beenevoted to anesthetic sparing of this nerve withany approaches to the lumbar plexus, only 2
tudies have examined the effect of the addition ofn obturator nerve block to improve analgesia afterajor knee surgery.60,61 Both studies reported a
ecrease in opioid consumption and pain scores inatients undergoing TKA receiving obturator nervelock in addition to a femoral or femoral and sciaticerve block.LFC Nerve Block. The LFC nerve of the thigh is a
urely sensory nerve that supplies a large but vari-ble area from the inguinal ligament to the knee onhe lateral aspect of the thigh.9 LFC nerve block isost commonly used as the sole anesthetic during
iagnostic muscle biopsy and harvesting of splithickness skin grafts.62,63 It has also been used torovide analgesia in elderly patients undergoing hipracture repair.64 However, in a study comparingFC nerve block, femoral nerve block, and patientseceiving no block following femoral neck repair,FC nerve block was not as effective at controllingostoperative pain as femoral nerve block.65
Typically, this block is done as a fan techniqueith variable success. Whether this is because ofariability in the distribution of innervation or tooorly localizing the nerve is not known. Shannonnd colleagues66 compared the traditional fan tech-ique for LFC nerve block to the use of a nervetimulator technique seeking tingling in the distri-
ution of the nerve. They reported a 40% success sate with the fanning technique compared with00% with the nerve stimulating technique. Thereas no difference in the extent of the blockade in
uccessful blocks. Femoral nerve block has beeneported after LFC block.67 This is not surprisingiven the bulk of data reporting spread to the LFCerve during femoral nerve block.Saphenous Nerve Block. The saphenous nerve fol-
ows the saphenous vein to the medial malleolusnd supplies the cutaneous area of the medial as-ect of the calf and foot to the level of the midfoot.he saphenous nerve block is often combined withsciatic block to provide anesthesia and analgesia
or surgery involving the medial aspect of the lowereg and foot. The saphenous nerve is a purely sen-ory nerve and does not contribute to the bonynnervation of the foot. Approaches to the saphe-ous nerve along its entire course, from the adduc-or canal to the ankle, have been described. Successates vary widely between techniques. For exam-le, successful block is reported in 33% to 65% ofases with a field infiltration performed medially athe level of the tibial plateau,68,69 70% to 80% ofases with the trans sartorial approach,68,70 95% to00% of cases with femoral paracondylar ap-roach,70 and near 100% of cases with the para-enous approach.69 The saphenous nerve has beeneported to be selectively blocked, sparing of theuadriceps musculature, in the adductor canal.71
owever, this has not been confirmed in a largeeries of patients receiving this approach to theaphenous nerve.
omparisons of Approaches to theumbar Plexus
soas Compartment Block Versus Femoral Nervelock
Parkinson et al.,28 were the first to compare thextent of blockade after single-injection femoralerve block and psoas compartment block. Theyompared the extent of blockade of the lumbarlexus with 5 different methods: posterior approacht L3 and L4-5 with a nerve stimulator using non-nsulated needles and anterior femoral nerve blockpproaches with a paresthesia technique and nervetimulating technique.28 They reported a 100% suc-ess rate of femoral nerve blockade with all tech-iques. The lateral femoral cutaneous nerve successate was 85% to 95%. The obturator nerve, asssessed by thigh adduction, was blocked 100% ofhe time with the posterior approaches and neverith the anterior approaches. Limitations of this
eport include lack of details regarding the type oferve stimulation, the small sample size, and exclu-
ion of patients in whom femoral nerve block failed
tmoabotr
F
tbadhcwaffnfwsl
cbatbtb
CE
beoivtnr
pagpacfh
fdlc
VTusmepsp
N
P
Mapcbrastntomwtplrdscnbprtstt
C
cla
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 15
o develop. A more recent comparison has beenade between psoas compartment blocks and fem-
ral nerve blocks.72 In this study, patients receivingpsoas compartment block developed a sensory
lock of the femoral, lateral femoral cutaneous, andbturator nerves in 100%, 97%, and 77% of pa-ients versus 93%, 63%, and 47% of the patientseceiving a femoral nerve block.
emoral Nerve Block Versus Fascia Iliacus Block
Direct comparisons of the extent of blockade be-ween the fascia iliacus block and femoral nervelock has been done in both adults and children. Indults, the fascia iliaca block, performed with theouble-pop technique, provided faster onset and aigher rate of lateral femoral cutaneous nerve blockompared with femoral nerve blocks performedith a nerve stimulator.73 Both techniques provide
dequate postoperative analgesia.74 In children, theascia iliaca block is more likely to block the lateralemoral cutaneous nerve compared with a femoralerve block.54 However, the duration of analgesia
rom these single-injection techniques was some-hat shorter in the fascia iliaca group. The authors
peculated this was related to greater spread of theocal anesthetic.
A single study directly comparing continuous fas-ia iliacus blocks to continuous femoral nervelocks has been reported.73 Again, the degree ofnalgesia was highly correlated with catheter posi-ioning. Overall, there was a greater degree oflockade of the lateral femoral cutaneous nerve inhe fascia iliacus group and a greater likelihood oflocking the obturator nerve in the femoral group.
ontinuous Psoas Compartment Blocks Versuspidural Analgesia
Advantages of continuous psoas compartmentlock compared with epidural block include unilat-ral analgesia and motor block, lack of impairmentf bladder function, and improved risk/benefit ration patients anticoagulated after surgery. These ad-antages must be weighed against the disadvan-ages of incomplete blockade for anesthesia and theeed for supplementation in a balanced analgesicegimen for effective analgesia.
Turker and coworkers17 compared continuoussoas compartment block with epidural block fornalgesia after THA under combined general/re-ional technique. They showed that continuoussoas compartment block provided excellent intra-nd postoperative analgesia with a low incidence ofomplications.17 Epidural block took longer to per-orm and had a significantly higher incidence of
ypotension, whereas analgesia and patient satis- eaction provided by the 2 blocks was similar. Epi-ural block also provided more motor blockade,onger time to ambulation, and significantly moreomplications.Continuous Psoas Compartment Blocksersus Continuous Femoral Blocks. AfterKA, continuous femoral nerve block and contin-ous psoas compartment block reduce narcotic con-umption and pain scores compared to intravenousorphine usage alone.44,45,75 However, no differ-
nces in outcome were observed between the 2eripheral nerve block groups despite a more con-istent presence of obturator nerve block in thesoas compartment group.75
erve Blocks of the Sacral Plexus
arasacral Block
The parasacral nerve block (PSNB) described byansour76 in 1993 has been described as more than
n isolated sciatic nerve block.77 It has been used torovide analgesia following major foot and ankle re-onstruction. Parasacral block will consistently blockoth components of the sciatic nerve and the poste-ior cutaneous nerve of the thigh. Spread of localnesthetic may also anesthetize other branches of theacral plexus including the superior and inferior glu-eal and pudendal nerves. The pelvic splanchnicerves (S2-S4), the terminal portion of the sympa-hetic trunk, the inferior hypogastric plexus, and thebturator nerve all lie in close proximity to the ele-ents of the sacral plexus and may all be anesthetizedith this approach. For procedures about the knee,
his may provide an advantage over more distal ap-roaches to the sciatic nerve.77,78 For procedures be-ow the knee, the adductor weakness from the obtu-ator and superior gluteal nerve block may actually beisadvantageous for mobilization of the patient. Theympathetic nerve supply to the bladder is also inlose proximity but problems with voiding and theeed for bladder catheterization after PSNB have noteen reported.77 A notable difference from other ap-roaches to the sciatic nerve is the type of muscleesponse deemed acceptable as an endpoint for injec-ion. Mansour76 described contraction of the ham-tring muscles (biceps femoris, semitendinous) abovehe knee as the endpoint for PSNB with most consis-ent success.
ontinuous Parasacral Blocks
Continuous parasacral blocks have been used inombination with lumbar plexus block to provideower extremity anesthesia for TKA, above the kneemputation, ACL repair, and a variety of other lower-
xtremity procedures.78 Gaertner reported successful
ccgidt
SM
taceTnr
trapcSomthlt
aefos8ts
S
sbtptbttiq
umOrmapAnab
apblfnscaosnf
point oo lf.
16 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
atheter placement, as confirmed by radiographicontrast dye in 86 of 87 consecutive patients under-oing lower-extremity surgery, using a nonstimulat-ng catheter. All patients developed analgesia in theistribution of the tibial, peroneal, and posterior cu-aneous nerve of thigh.
ciatic Nerve Block: At the Level of the Gluteusaximus
The sciatic nerve, the largest nerve derived fromhe sacral plexus, innervates the posterior thigh andlmost the entire leg below the knee. The mostommon indications for sciatic nerve block are an-sthesia and analgesia for foot and ankle surgery.here are a variety of approaches to the sciaticerve block and their success rate is widely variable,anging from 33% to 95%.79-82
Gaston Labat83 first described, at the beginning ofhe 20th century, the sciatic nerve block that is noweferred to as the Classic Approach of Labat. Thispproach is based on the bony relationship of theosterior superior iliac spine and the greater tro-hanter with the patient positioned in a modifiedims position. Winnie79 was the first to modify theriginal description, adding in an additional land-ark, the sacral hiatus to greater trochanter dis-
ance, to more precisely account for varying bodyabituses (Table 4). Difficulty identifying these
andmarks led Chang and colleagues84 to describe aransrectal method of identifying the ischial spine.
Franco85 described a simple approach to the sci-tic nerve block in the prone position. The needlentry site is perpendicular to the floor 10-cm lateralrom the middle of the intragluteal sulcus regardlessf the patient’s gender or body mass index. Theciatic nerve was found by trainees in �3 passes in5% of the cases reported. Whether the success ofhis simple approach will be replicated in a larger
Table 4. Sciatic Nerve Block Approaches,
Approach, AuthorNumber ofPatients
At the level of the sciatic notchParasacral, Morris77 30
At the level of the ischial spineLabat, di Benedetto94 135Trans-rectal, Chang84 40
At the level of the ischial tuberosityLithotomyPosterior, Sutherland115 76
At the level of the upper thighPosterior Subgluteus, di Benedetto113 64Anterior, Chelly89 22Lateral, Guardini82 � 100
*Failures in this study were due to the inability to obtain this endf the block [12%]) rather than to the failure of the endpoint itse
ample size remains to be seen. i
ubgluteal Approaches to the Sciatic Nerve
Raj et al.80 described a supine approach to theciatic nerve in the flexed hip position, initiating thelock at the midpoint between the greater trochan-er of the femur and the ischial tuberosity. Theositioning of the patient was thought to be advan-ageous compared to the classic approach of Labaty “thinning the gluteus maximus muscles, makinghe sciatic nerve more superficial.” However, iden-ifying these bony landmarks in very obese patientss sometimes difficult and the patient position re-uires additional personnel to maintain.A lateral subgluteal approach to the sciatic nerve
sing the greater trochanter of the femur as a land-ark was first described by Ichniyanagi in 1959.86
ther investigators have described a high successate using this high lateral approach with a slightlyore caudal entry point.82 Notably, when using this
pproach the success rate of the blockade of theosterior cutaneous nerve of the thigh was 83%.lthough theoretically the posterior cutaneouserve should reliably be blocked in most proximalpproaches to the sciatic nerve, the success rate oflockade is not usually reported.The anterior approach to the sciatic nerve has the
ppeal of supine positioning and a single prep of theatient for combined femoral and sciatic nervelocks. Its popularity had long been limited by itsow success rate and relatively painful use of theemur as a deep landmark.87,88 Chelly and Delau-ay89 described a nerve stimulating technique po-itioning the needle at the level of the lesser tro-hanter as originally described by Beck. Vloka etl.90 described the importance of internal rotationf the leg if the path to the sciatic nerve is ob-tructed by the lesser trochanter. A magnetic reso-ance imaging study of the anatomy of this area
ound that in 65% of patients the sciatic nerve is
Stimulating Current And Block Success
mended Minimal Stimulatingrrent and Its Pulse Width Success Rate
A; 100 �sec pulse width 97%
A; 100 �sec pulse width 98%A; 200 �sec pulse width 92.5% (cross-over design)*
ortedmA; 100 �sec pulse width 95%
A; 100 �sec pulse width 94%A; 100 �sec pulse width 100%
orted � 94%
r to technical factors (e.g., patient movement and abandonment
Nerve
RecomCu
� 0.2 m
� 0.5 m� 0.4 m
Not rep0.3-0.5
� 0.5 m� 0.7 mNot rep
naccessible from the anterior approach at the level

onst
ttsttcCptaarcp
1tfwg1parn
SF
amahutmntnnlaeflott
fp
ct1Wvcplcce
tit(rntess
C
itatabbsatuctcwoci
ac2tocd
A
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 17
f the lesser trochanter.91 These authors suggestedeedle placement 4 centimeters lower where ob-truction to the sciatic nerve occurred in only 5% ofhe patients.
Dalens et al.92 has compared the success rate ofhe posterior, lateral, and anterior approaches tohe sciatic nerve in children. Although they had auccess rate of 90% with all approaches, the au-hors reported fewer manipulations were requiredo perform either a lateral or posterior approachompared with the anterior approach. Recently,howdary and Splinter93 reported on a medial ap-roach to the sciatic nerve at the level of the lesserrochanter in only 10 children. Advantages of thispproach are the lack of obstruction from the femurnd no muscle mass to transverse. The authorseported a 70% rate of blockade of the posteriorutaneous nerve of the thigh with this medial ap-roach.di Bendetto et al.94 described their experience in
35 consecutive patients using a posterior subglu-eal approach to the sciatic nerve. The time to per-orm the block was 41 � 25 seconds (mean � SD),ith an average of 2 needle redirections. The de-
ree of discomfort reported was very low and only6 patients (12%) reported severe pain duringlacement of the block. In contrast to this, Fanelli etl.95 reported patient discomfort in 88% of patientseceiving a classic Labat approach to the sciaticerve.
ciatic Nerve Block at the Level of the Poplitealossa
Popliteal fossa block is chiefly used for foot andnkle surgery.96-98 Short saphenous vein strippingay also be performed under combined popliteal
nd posterior cutaneous nerve block.99 The blockas also been successfully used in the pediatric pop-lation.100 Popliteal fossa block anesthetizes the en-
ire leg below the tibial plateau save the skin ofedial aspect of the calf and foot (i.e., saphenouserve distribution). Potential advantages of popli-eal block over ankle block are improved calf tour-iquet tolerance and immobile foot. The compo-ents of the sciatic nerve may be blocked at the
evel of the popliteal fossa via posterior or lateralpproaches. Patient positioning—prone, lateral (op-rative side nondependent), or supine (with legexed at the hip and knee)—may determine theptimal approach for an individual patient.101 Con-inuous techniques have been described using bothhe posterior102-104 and lateral105 approaches.
The classic posterior approach to the poplitealossa is accomplished with the patient positioned
rone (Fig 7). Traditionally, the sciatic nerve is lo- tated 5 cm above the popliteal crease.96 However,o block the sciatic nerve before its division, a 7- to0-cm distance has been recommended.97,98,106-108
ith a large-volume single-injection technique, in-ersion is the motor response that best predictsomplete neural block of the foot.109 A lateral ap-roach to blockade of the sciatic nerve in the pop-iteal fossa has been described.110-112 Because theommon peroneal nerve is located more superfi-ially than the tibial nerve, the stimulating needlencounters it first (Fig 8).Success rate with all approaches is typically 90%
o 95%, with approximately 5% of patients requir-ng supplemental general anesthesia. It is believedhat incomplete block is the result of poor diffusionbecause of the size of the sciatic nerve), the sepa-ate fascial coverings of the tibial and peronealerves, or blockade of only a single component ofhe sciatic nerve. This has led some practitioners tondorse the practice of dual stimulation to improveuccess rate110 (see Multistimulation versus single-timulation techniques).
ontinuous Sciatic Nerve Blocks
Continuous sciatic nerve blockade can theoret-cally be achieved at any place along the course ofhe sciatic nerve. These blocks have been used fornalgesia after major foot and ankle reconstruc-ion, ankle fracture fixation, and below the kneemputation.102,103,113-115 Several studies haveeen published on the use of continuous popliteallocks for analgesia after extensive foot and ankleurgery.102-104 All studies reported excellent an-lgesia with few side effects. Compared with in-ravenous analgesia or placebo infusion, a contin-ous infusion of local anesthetic via a poplitealatheter reduces pain scores and opioid consump-ion, and decreases sleep disturbances.102,103 Suc-essful catheter placement has been reportedith both lateral and posterior approaches. Thenly consistent problem reported with poplitealatheters is a high incidence (15%-25%) of kink-ng or dislodgement.102,103
di Benedetto et al.113 compared the subglutealpproach to the posterior popliteal approach forontinuous infusions in a prospective study. In the4-hour observation period after surgery, 13.3% ofhe catheters in the popliteal group were eitherccluded or dislodged compared with 6.6% of theatheters in the subgluteal group. This differenceid not reach statistical difference.
nkle and Foot Block
Indications for blockade of the terminal nerves of
he lumbosacral plexus distally, at the ankle and
mtslta
radvsoaaci
whprae
IE
u1clstgedtlf
ppcwvewipcovs2
fitmdnvCtg
fmflatcbnttat
Ct
P
sttioswggtiat
SS
bgawlHl
18 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
idtarsal levels, include anesthesia for surgery tohe foot.116,117 Diagnostic block has also been de-cribed.118 The peripheral nerves blocked at theseevels are terminal branches of both the sciatic (pos-erior tibial, superficial peroneal, deep peroneal,nd sural) and femoral (saphenous) nerves.The 5 peripheral nerves that supply the foot are
elatively easy to block at the ankle (Fig 9). Therere no important variants in the innervation of theistal musculature. However, there is considerableariation in the branching and distribution of theensory nerves of the foot. For this reason, blockadef all 5 nerves has been advocated.119 Neural block-de of the posterior tibial nerve has been describedt the supramalleolar,119-121 midmalleolar,116 sub-alcaneal,122,123 and midtarsal124 levels with no ev-dence of superiority of any technique.
Few studies evaluating perioperative outcomesith ankle block exist,125 although the techniqueas been performed for decades.83 Rather, mostublications describe variations to improve successate. Peak blood levels of local anesthetic occurround 90 minutes after blockade and are very lowven after bilateral ankle block.126
ntravenous Regional Anesthesia of the Lowerxtremity
Intravenous regional anesthesia (IVRA) may besed for foot, ankle, and knee surgery lasting up tohour.127 It may also be used for treatment of
omplex regional pain syndrome in the lowerimb.128 In a questionnaire survey,129 most re-ponding anesthesiologists (�80%) acknowledgehat lower limb IVRA is seldom performed for sur-ical anesthesia because of a lack of clinical experi-nce. Other reasons for its lack of popularity includeifficulty in locating veins in the foot or ankle, thighourniquet pain, and perceived requirement of aarger, potentially unsafe, local anesthetic dose thanor upper limb IVRA.
The technique for lower limb IVRA involves ap-lication of a double pneumatic thigh cuff afterroper padding and establishment of a venous ac-ess on the dorsum of the foot or around the ankleith a 20- to 22-G cannula. The greater saphenousein is often the most suitable vein. After limblevation for several minutes and exsanguinationith an Esmarch bandage, the proximal tourniquet
s inflated to 100 mm Hg above the limb occlusionressure (min 300 mm Hg). Most commonly, lido-aine 0.25% is injected to a maximum of 3 mg/kgver several minutes. This yields a large injectedolume of up to 1.2 mL/kg (e.g., 84 mL for a 70-kgubject).127,130 The recommended inflation time is
0 minutes minimum and 90 minutes maximum. UAlternatively, a calf tourniquet can be used foroot and ankle surgery.131 In this case, a single cuffs applied at least 3 inches below the head of fibulao avoid common peroneal nerve injury. A proxi-al “back up” cuff is placed on the thigh in case of
rug leakage. A double cuff in the calf is generallyot advisable because tapering calf curvature pre-ents a firm fit and risks accidental cuff slippage.linical experience suggests that lidocaine 0.5% up
o 3 mg/kg and 0.6 mL/kg provides consistent sur-ical anesthesia within 10 minutesAn intercuff IVRA technique has been described
or knee arthroscopy achieved successfully with 40L lidocaine 0.5%.132 This technique involves in-ation of a double-cuffed tourniquet in the thighfter exsanguination, injection of local anesthetichrough a foot cannula, then application of a singleuff in the calf, and re-exsanguination of the footefore inflation of the calf tourniquet. This tech-ique allows surgical anesthesia to be most concen-rated around the knee joint. At the end of surgery,he calf cuff is deflated first, allowing residual localnesthetic to empty into the foot before release ofhe proximal thigh cuff.
omparisons Between Approaches tohe Sacral Plexus
SNB Versus Classic Sciatic Nerve Block
Cuvillon et al.133 reported on 150 patients pre-enting for lower-extremity surgery using PNB. Forhe sciatic component of their anesthetic, the pa-ients were randomized to receive a PSNB, a single-njection sciatic nerve block as described by Winnie,r a double-injection sciatic nerve block as de-cribed by Winnie. The onset time and success rateere similar in the PSNB and double-injection
roups and were superior to the single-injectionroup in this report (Fig 12). The authors attributedhis high rate of success with the PSNB to its prox-mal location with the potential for blockade ofdditional branches of the sacral plexus, althoughhis was not evaluated in the study design.
ciatic Block at the Gluteus Maximus Versusciatic Block at the Popliteal Fossa
Kilpatrick et al.134 compared the classic sciaticlock with popliteal fossa block in patients under-oing foot surgery. All blocks were performed usingnerve stimulator technique. Popliteal fossa blocksere less painful because the sciatic nerve is no
onger covered by thick musculature at this level.owever, the success rate was lower with the pop-
iteal approach (45%) than with the classic (95%).
sing more modern techniques, a comparison of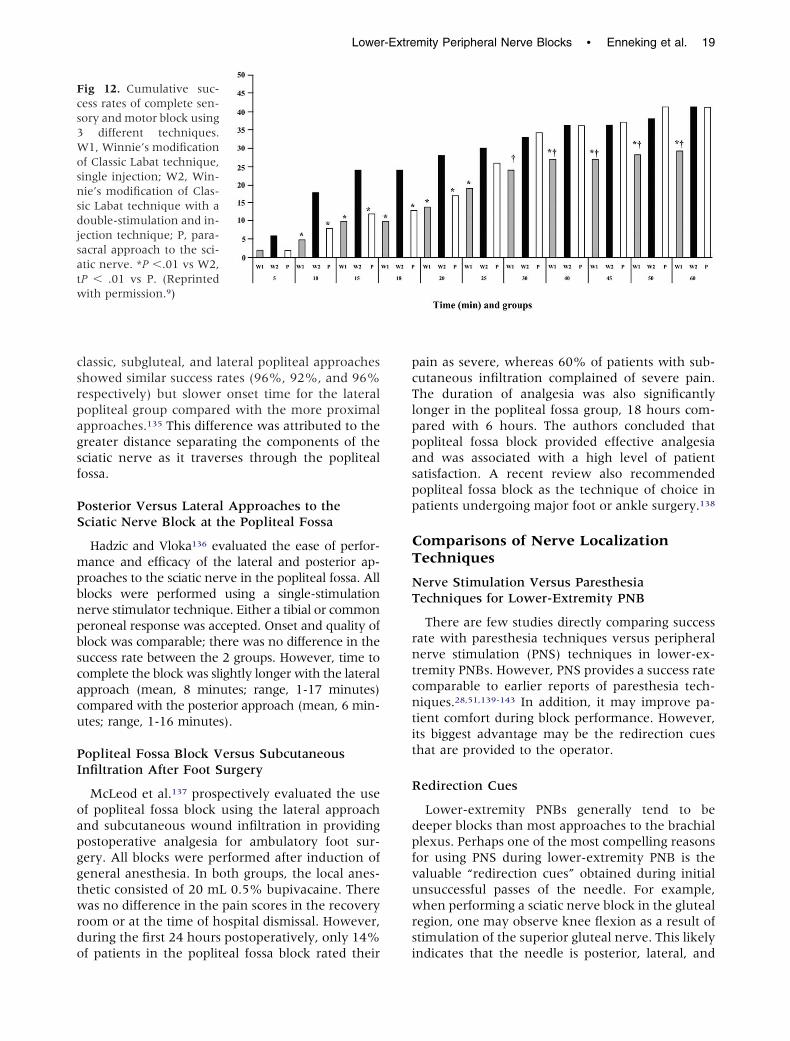
csrpagsf
PS
mpbnpbscacu
PI
oapggtwrdo
pcTlppaspp
CT
NT
rntcntit
R
dpfvuwrs
Fcs3Wosnsdjsatw
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 19
lassic, subgluteal, and lateral popliteal approacheshowed similar success rates (96%, 92%, and 96%espectively) but slower onset time for the lateralopliteal group compared with the more proximalpproaches.135 This difference was attributed to thereater distance separating the components of theciatic nerve as it traverses through the poplitealossa.
osterior Versus Lateral Approaches to theciatic Nerve Block at the Popliteal Fossa
Hadzic and Vloka136 evaluated the ease of perfor-ance and efficacy of the lateral and posterior ap-
roaches to the sciatic nerve in the popliteal fossa. Alllocks were performed using a single-stimulationerve stimulator technique. Either a tibial or commoneroneal response was accepted. Onset and quality oflock was comparable; there was no difference in theuccess rate between the 2 groups. However, time toomplete the block was slightly longer with the lateralpproach (mean, 8 minutes; range, 1-17 minutes)ompared with the posterior approach (mean, 6 min-tes; range, 1-16 minutes).
opliteal Fossa Block Versus Subcutaneousnfiltration After Foot Surgery
McLeod et al.137 prospectively evaluated the usef popliteal fossa block using the lateral approachnd subcutaneous wound infiltration in providingostoperative analgesia for ambulatory foot sur-ery. All blocks were performed after induction ofeneral anesthesia. In both groups, the local anes-hetic consisted of 20 mL 0.5% bupivacaine. Thereas no difference in the pain scores in the recovery
oom or at the time of hospital dismissal. However,uring the first 24 hours postoperatively, only 14%
ig 12. Cumulative suc-ess rates of complete sen-ory and motor block using
different techniques.1, Winnie’s modification
f Classic Labat technique,ingle injection; W2, Win-ie’s modification of Clas-ic Labat technique with aouble-stimulation and in-ection technique; P, para-acral approach to the sci-tic nerve. *P �.01 vs W2,P � .01 vs P. (Reprintedith permission.9)
f patients in the popliteal fossa block rated their i
ain as severe, whereas 60% of patients with sub-utaneous infiltration complained of severe pain.he duration of analgesia was also significantlyonger in the popliteal fossa group, 18 hours com-ared with 6 hours. The authors concluded thatopliteal fossa block provided effective analgesiand was associated with a high level of patientatisfaction. A recent review also recommendedopliteal fossa block as the technique of choice inatients undergoing major foot or ankle surgery.138
omparisons of Nerve Localizationechniques
erve Stimulation Versus Paresthesiaechniques for Lower-Extremity PNB
There are few studies directly comparing successate with paresthesia techniques versus peripheralerve stimulation (PNS) techniques in lower-ex-remity PNBs. However, PNS provides a success rateomparable to earlier reports of paresthesia tech-iques.28,51,139-143 In addition, it may improve pa-
ient comfort during block performance. However,ts biggest advantage may be the redirection cueshat are provided to the operator.
edirection Cues
Lower-extremity PNBs generally tend to beeeper blocks than most approaches to the brachiallexus. Perhaps one of the most compelling reasonsor using PNS during lower-extremity PNB is thealuable “redirection cues” obtained during initialnsuccessful passes of the needle. For example,hen performing a sciatic nerve block in the gluteal
egion, one may observe knee flexion as a result oftimulation of the superior gluteal nerve. This likely
ndicates that the needle is posterior, lateral, and
ctsir
MT
qpoprarslcgcbaabmt
oauaro2lttwnstr
lbsbtsdiaab
rWw
smrtalupbPaan
I
itmucqinnlwigpt6sArl
gbgaadouafs
20 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
ephalad to the sciatic nerve and should be reposi-ioned appropriately. Tables 1 and 2 list motor re-ponses to nerve stimulation for all the musclesnnervated by the lumbosacral plexi. These motoresponses can be used as guides for redirection cues.
ultistimulation Versus Single-Stimulationechniques
Multiple-stimulation techniques by definition re-uire individual stimulation of each component of aeripheral nerve with deposition of a small volumef local anesthetic at each site. For instance, duringerformance of a sciatic block a peroneal motoresponse is elicited first and a small volume of localnesthetic is deposited. The needle is then redi-ected medially to obtain a tibial nerve motor re-ponse with subsequent deposition of additionalocal anesthetic. Whether the search for individualomponents of a PNB versus identification of a sin-le component will become the norm for PNB is notlear. Advocates of multiple-stimulation techniqueselieve the technique increases the success rate andllows an injection of a smaller volume of localnesthetic. Advocates of single injection techniqueselieve multistimulation and injection techniquesay add risk of nerve injury during redirection of
he needle through partially anesthetized nerves.Several studies have supported the clinical utility
f multiple-stimulation technique. Paqueron etl.110 compared the block characteristics in patientsndergoing popliteal fossa block with the lateralpproach using either a single injection (inversionesponse) or a double injection (both common per-neal and tibial components identified). A total of0 mL local anesthetic was injected. Double stimu-ation was associated with a higher success ratehan single stimulation, 88% versus 54%, respec-ively. The onset time of complete sensory blockas also reduced with the double-stimulation tech-ique. Similar results were reported for multiple-timulation sciatic nerve blocks by other investiga-ors.144,145 No neurologic complications have beeneported in any of these studies.110,144,145
Casati et al.146 showed that a lower volume ofocal anesthetic could be used for femoral nervelock when comparing multi-injection technique toingle injection in a prospective randomized andlinded study. In this study, multiple stimulation ofhe femoral nerve involved injecting on each of 3timulations, the vastus medialis, vastus interme-ius, and vastus lateralis, compared with a singlenjection on a vastus intermedius stimulation. Usingstaircase method to determine the volume of localnesthetic required to produce a sensory and motor
lock within 20 minutes, the authors found a 27% neduction in volume in the multistimulation group.hether this difference in volume (total of 9 mL)ill improve safety is unknown.In each of these reports the issue of safety,
pecifically the risk of nerve injury, when using aultistimulation injection technique has been
aised. There were no reported nerve injuries inhese studies performed by experienced regionalnesthesiologists. This is in agreement with thearge cohort of patients studied by Fanelli et al.95
sing multistimulation techniques in over 2,000atients with no nerve injury attributed to nervelock. However, nerve injury is a rare event afterNB and even in a study of this size may not havelarge enough sample size to determine the rel-
tive risk of multiple versus single injection tech-iques.
maging Aids
Several investigators have examined the use ofmaging technology to improve localization of bothhe lumbar plexus and the femoral nerve. Kirch-air and colleagues147 showed the usefulness ofltrasound in localizing the psoas major using aurved array transducer at low (4-5 MHz) fre-uency. The location of the lumbar plexus is thennferred. It is not possible to distinguish peripheralerves from tendon fibers with the ultrasound tech-ology currently commercially available. The main
imitations to visualization in this volunteer studyere obesity and occasional high riding iliac crests
n male patients. In a follow-up study, ultrasounduidance was used to place needles in the lumbarlexus of cadaveric specimens.148 CT scan verifiedhe accuracy of needle placement in all cases. Of the0 attempts the psoas major was visualized in 48pecimens and the needle successfully placed in 47.gain obesity, spinal deformities, and conditions
elated to embalming of the cadavers were the mainimitations for use of this technique.
Marhofer et al.149 compared the use of ultrasounduidance to nerve stimulation during femoral nervelocks. These investigators found that ultrasounduidance was superior to nerve stimulation because itllowed the use of a smaller volume of local anestheticnd shorter latency period. The authors attributed thisifference to the ability to visualize the administrationf the local anesthetic during injection. They usedltrasound to reposition the needle when the localnesthetic spread out of the fascial plane and awayrom the nerve.149,150 It should be noted that ultra-ound failed to identify the femoral nerve in a small
umber of patients in each of these studies.
LL
P
eeabaeraglaataoacnr
itafoiaci0ewtsblsc
aeodeeocm�n
otsbjdtdsibHi5ofa
rrtuslprbstwwotcs
tPcdttdtCieunspa0st
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 21
ocal Anesthetic Choices and Dosing ofower-Extremity PNB
harmacologic Considerations
Selection of a local anesthetic solution for lower-xtremity blocks differs somewhat from that of upper-xtremity approaches because of the indications andpplications of each. For example, upper-extremitylocks are commonly performed as the intraoperativenesthetic. In addition, pain after surgery to the upperxtremity may not be as severe or protracted. As aesult, intermediate-acting local anesthetics and localnesthetic mixtures are frequently selected for sur-ery to the arm.151 These principles may not apply toower-extremity surgery in which peripheral block-de is often supplemented with a neuraxial or generalnesthetic intraoperatively, and the need for sus-ained postoperative analgesia is achieved with long-cting amides administered either as single injectionsr continuous infusions. Finally, although the use ofdjuvants such as clonidine, opioids, and ketorolac isommon during lower-extremity peripheral tech-iques, their efficacy in improving the quality or du-ation of blockade has not been consistently shown.
Local Anesthetic Selection. Few randomized stud-es have compared local anesthetics for lower-ex-remity block. Fanelli et al.152 evaluated the onsetnd duration of combined femoral-sciatic block per-ormed with 0.75% ropivacaine, 0.5% bupivacaine,r 2% mepivacaine. Ropivacaine had an onset sim-lar to that of mepivacaine but with a duration ofnalgesia between that of bupivacaine and mepiva-aine. Connelly et al.153 reported no significant clin-cal differences between 0.75% ropivacaine and.5% bupivacaine for sciatic nerve blockade. Whenquipotent (rather than equivalent) concentrationsere compared, onset times for the 2 local anes-
hetics showed no differences in onset times forensory and motor block. However, the times tolock regression and first analgesia were slightlyonger with bupivacaine.154 In a single comparativetudy of sciatic block, levobupivacaine has blockharacteristics similar to ropivacaine.155
Epinephrine. Epinephrine prolongs the durationnd quality of most local anesthetics used for lower-xtremity peripheral block. The effects are the resultf vasoconstriction of the perineural vessels, whichecreases uptake and thereby increases the neuralxposure to the local anesthetic. However, the differ-nce is only somewhat dose dependent. The additionf epinephrine 5 �g/mL (1:200,000 dilution) signifi-antly increases the duration of lidocaine from 186inutes to 264 minutes. Although epinephrine 2.5g/mL (1:400,000 dilution) prolongs the block to
early the same extent (240 minutes), it has no effect Cn nerve blood flow.156 The addition of epinephrineo local anesthetics with vasoconstrictive properties,uch as ropivacaine, may not increase block durationut would still facilitate detection of intravascular in-ection.157 The decision to add epinephrine (and theose of epinephrine) is based on the concerns relatedo cardiac or neural ischemia versus the ability toiscern an intravascular injection. In general, becauseeizures related to intravascular injection were highestn patients undergoing peripheral nerve block,158 theenefits of adding epinephrine outweigh the risks.owever, the nearly equivalent effects on block qual-
ty and duration reported with epinephrine 2.5 versus.0 �g/mL suggest that the lower concentration isptimal, particularly in patients theoretically at riskor nerve injury (diabetics, patients with chemother-py-induced neuropathy).156
Bicarbonate. The addition of bicarbonate has beenecommended to increase the speed of onset of pe-ipheral and plexus blockade. However, most studieshat have shown statistically significant differencessed commercially prepared epinephrine-containingolutions of local anesthetics (which have a muchower pH due to the addition of antioxidants) com-ared with plain local anesthetic solutions. A recenteview of the literature involving brachial plexuslock concluded that there was little reason to addodium bicarbonate with plain local anesthetics orhose with freshly added epinephrine.151 These resultsere substantiated in a study by Candido et al.,159
hich reported no difference in the onset or durationf combined lumbar plexus-sciatic block in patientshat received 0.5% bupivacaine with alkalinizationompared with those who received a non-alkalinizedolution.
Clonidine. Clonidine has been extensively inves-igated as an adjuvant for brachial plexus block.rolongation of analgesia after the addition oflonidine is most likely peripherally mediated andose dependent. During intravenous regional anes-hesia, clonidine 150 �g may improve tourniquetolerance.160 Side effects such as hypotension, bra-ycardia, and sedation do not occur with a dose lesshan 1.5 �g/kg or a maximum dose of 150 �g.lonidine as an adjuvant for lower-extremity block
s much less defined. The limited data for lower-xtremity techniques validates those of previouspper-extremity reviews.161,162 The results are mostotable with intermediate-acting agents.162 A singletudy has compared the effect of lower-extremityeripheral block with/without clonidine. Casati etl.161 reported the addition of clonidine 1 �g/kg to.75% ropivacaine for patients undergoing footurgery under sciatic-femoral block prolonged theime to first analgesia from 13.5 to 16.8 hours.
lonidine is often a component of lumbar plexus or
ssebwi
O
aeDpliotcn
O
nuidklsk
tqdatiLeoadmad
CP
bp2at
b4Tcclr
psactoaidnewabssomlrmnicrhglsisltdpissiacpa
tna
22 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
ciatic continuous infusions after hip, knee, or footurgery.45,47,102 However, the efficacy has not beenstablished. A single study involving a continuousrachial plexus infusion of ropivacaine with orithout clonidine failed to show a clinically signif-
cant effect.163
pioids
To date, there are no comparative studies evalu-ting the effect of opioids as adjuvants to lower-xtremity single-dose or continuous techniques.espite this lack of data, opioids, including mor-hine, sufentanil, and fentanyl, are often added toumbar plexus infusions.45,47 Investigations involv-ng the brachial plexus report no difference in blocknset, quality, or duration when opioids are addedo the local anesthetic solution. A recent reviewoncluded that the role of opioids in peripheralerve block is not clinically relevant.151
ther Adjuvants
Most studies investigating adjuvants such aseostigmine, hyaluronidase, and tramadol involvepper-extremity blocks.151 A single study evaluat-
ng the efficacy of nonsteroidal antiinflammatoryrugs as adjuvants reported that the addition ofetorolac to lidocaine for ankle block resulted inonger duration and improved analgesia after footurgery compared with intravenously administeredetorolac.164
In summary, selection of a local anesthetic solu-ion for lower-extremity peripheral blockade re-uires thoughtful consideration and is based on theuration of surgery, analgesic requirements, andnticipated rehabilitative efforts. The lowest effec-ive dose and concentration should be used to min-mize local anesthetic systemic and neural toxicity.ikewise, the addition of 1:200,000 or 1:400,000pinephrine is recommended to facilitate detectionf intravascular injection, as well as decrease localnesthetic levels. The role of other adjuvants is lessefined; additional studies are required to deter-ine the efficacy of clonidine, opioids, tramadol,
nd nonsteroidal antiinflammatory drugs in single-ose or continuous lower-extremity techniques.
omplications of Lower-Extremityeripheral Nerve Blocks
Complications associated with peripheral nervelockade are not common. Auroy and colleagues158
rospectively evaluated serious complications after1,278 PNBs in a 5-month period in France. Using95% confidence interval, they estimated the po-
ential for serious complications per 10,000 PNBs to s
e 0 to 2.6 deaths, 0.3 to 4.1 cardiac arrests, 0.5 to.8 neurologic injuries, and 3.9 to 11.2 seizures.here is a paucity of reports of complications spe-ifically associated with lower-extremity PNBs asompared with upper-extremity PNBs. This is mostikely related to their less common applicationather than to inherent safety of the techniques.
Local Anesthetic Systemic Toxicity. Theotential for systemic local anesthetic toxicity wouldeem to be very high for lower-extremity PNBs. Rel-tively large doses of local anesthetic are used forombined femoral and sciatic nerve blocks to anesthe-ize the entire lower extremity. However, there arenly a few case reports of local anesthetic toxicityssociated with lower-extremity PNBs. For instance,n Fanelli and colleagues’ series of 2,175 patients un-ergoing femoral sciatic combined blocks, there wereo systemic adverse local anesthetic reactions report-d.95 The apparent margin of safety seems to varyith individual block techniques. For instance, there
re no case reports of toxicity after popliteal sciaticlockade, whereas there are several case reports ofevere toxicity following lumbar plexus and proximalciatic blocks.165-169 Anatomic differences in the anat-my, primarily in the vascularity and presence of deepuscle beds in the area of blockade, are the most
ikely explanation for this discrepancy. Severe toxiceactions typically occur during the injection or im-ediately thereafter. This suggests that the mecha-ism of these events is commonly an unintentional
ntravascular injection of local anesthetic into the cir-ulation, rather than absorption.3,170-173 A forceful,apid injection of local anesthetic carries a muchigher risk of local anesthetic toxicity than a slow,entle injection.174 This is because the mean dose ofocal anesthetic that elicits the signs of central nervousystem toxicity is much less during rapid intravascularnjection as compared with that associated withlower absorption after appropriate deposition. After aower-extremity peripheral nerve block, local anes-hetic levels peak at approximately 60 minutes aftereposition170,172,173 (Fig 13). Perhaps this slow time toeak blood levels offers an explanation for the lowncidence of toxic complications associated with ab-orption. Important measures to decrease the risk ofevere toxicity include the use of epinephrine as anntravascular marker, slow methodical injection whilevoiding high-injection pressure, frequent aspiration,onstant assessment of the patient and vital signs, andrudent selection of local anesthetic concentrationnd volume.Proximal Spread (Neuraxial Block). A po-
ential needle misadventure of proximal peripheralerve blocks is intrafascicular spread of the localnesthetic proximally toward the spinal cord, re-
ulting in neuraxial blockade.26,30,175-177 This is a
pvrpwu
aclcotT2ctTwn
pdtpcDct
p5pf0d
vhplhr
citolisttmCmot
rtduhnTtwcrhu
N
pwiimrau
Ptistml
Fblc(a
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 23
articular concern with block techniques that in-olve needle placement at the level of the nerveoots or spinal nerves, such as paravertebral, andsoas compartment block. Forceful, fast injectionsithin the dural cuffs or perineurium can result innintentional spinal or epidural anesthesia.175
In their large series of severe complicationsssociated with regional anesthesia, Auroy andolleagues165 found the posterior approach to theumbar plexus to have the highest incidence ofomplications of the lower extremity PNBs. Withnly 394 posterior lumbar plexus blocks reported,here were 5 serious complications in this cohort.hree of these complications, 1 cardiac arrest andrespiratory arrests, were directly attributed to
entral placement or diffusion of the local anes-hetic to the epidural or intrathecal space.165
heir recommendation was to manage this blockith the same degree of vigilance as for aeuraxial block.Hemorrhagic Complications. Several ap-
roaches for PNBs of the lower extremity involveeep needle penetration. These approaches includehe psoas compartment approach to the lumbarlexus, the obturator nerve block, and the parasa-ral and classical approaches to the sciatic nerve.espite the proximity of these deep nerves to vas-ular and hollow viscous structures, there are rela-ively few reports of needle misadventures.
Vascular puncture during femoral nerve blocklacement has been reported to be as frequent as.6%.178 However, few complications were re-orted after unintentional vascular puncture duringemoral nerve block.179 Kent et al.180 reported a.2% (20/9,585) incidence of neuropathy after car-
ig 13. Local anesthetic levels following psoas or com-ined psoas/sciatic nerve blocks. Note the local anestheticevels peak at approximately 60 minutes. Mepi, mepiva-aine; epi, epinephrine; lido, lidocaine; bupi, bupivacaine.Data from Farney et al.,3 Odoom et al.,170, and Simon etl.173)
iac catheterization. Sixteen of these patients de- t
eloped neuropathies from large retroperitonealematomas. Twenty percent of these patients hadersistent, mild sensory, or motor neuropathy atong-term follow-up. The other 4 patients had groinematomas. In all of these patients, the neuropathyesolved.
Retroperitoneal hematoma formation after psoasompartment block has been reported by severalnvestigators.2,181,182 To reach the lumbar plexus,he needle must transverse multiple muscle andther tissue layers.183 The combination of its deep
ocation and inability to apply pressure after annadvertent puncture of deeply situated blood ves-els supplying the local muscles and other struc-ures may make this block less suitable in the set-ing of anticoagulation as compared with otherore superficial lower extremity nerve blocks.onservative management of retroperitoneal he-atoma is recommended unless the patient devel-
ps hypotension unresponsive to volume resuscita-ion.181,184
Infectious Complications. There are no caseeports of infection after single-injection, lower-ex-remity PNBs. Cuvillon et al.178 reported on the inci-ence of bacterial complications associated with these of continuous femoral nerve blocks. In their co-ort of 208 patients, 57% had positive bacterial colo-ization of the catheter at 48 hours postoperatively.hree patients had transitory symptoms of bacteremiahat resolved with removal of the catheter. Thereere no long-term sequelae related to these positive
atheter cultures. Two case reports of psoas abscessequiring drainage and intravenous antibiotic therapyas been reported in patients who received a contin-ous femoral nerve block.185,186
eurologic Complications
Although there are relatively few published re-orts of anesthesia-related nerve injury associatedith the use of PNBs,95,158,165 it is likely that the
ncidence is underestimated. The less frequent clin-cal application of lower-extremity nerve blocks
ay be the main reason that there are even fewereports of anesthesia-related nerve injury associ-ted with lower-extremity PNBs as compared withpper-extremity PNBs.187
Neurologic complications after lower-extremityNB can be related to a variety of factors related tohe block including needle trauma, intraneuronalnjection, and neuronal ischemia. However, aearch for other causes should include surgical fac-ors such as positioning, retractor injury, and he-atoma formation. In many instances, the neuro-
ogic injury may be a result of a combination of
hese factors.
MaunsttniTsfimerittls4dtpppobwn
Pabwf(lobdptlbtscgtfteatrind
tdtyatshtis
tnPdmtoiarpms
Fctei
24 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
Peripheral Nerves: Functional Anatomy andechanisms of Nerve Injury. The functional
natomy of the peripheral nerve is important fornderstanding the mechanisms of peripheralerve injury. A peripheral nerve is a complextructure consisting of fascicles held together byhe epineurium, an enveloping, external connec-ive sheath (Fig 14). Each fascicle contains manyerve fibers and capillary blood vessels embedded
n a loose connective tissue, the endoneurium.he perineurium is a multilayered epithelialheath that surrounds individual fascicles. Nervebers depend on a specific endoneurial environ-ent for their function. This is different than the
xtraneural interstitium. Peripheral nerves areichly supplied by an extensive vascular networkn which the endoneurial capillaries have endo-helial “tight junctions,” a peripheral analogy tohe “blood-brain barrier.” The entire neurovascu-ar bed is regulated by the sympathetic nervousystem and its blood flow can be as high as 30 to0 mL/100 g per minute.188 In addition to con-ucting nerve impulses, nerve fibers also main-ain axonal transport of various functionally im-ortant substances, such as proteins andrecursors for receptors and transmitters. Thisrocess is highly dependent on oxidative metab-lism. Any of these structures and functions cane deranged during a traumatic nerve injury,ith the possible result of temporary or perma-
ig 14. Organization of a peripheral nerve: 1, nerve fas-icle with endoneurium; 2, epineural sheath envelopinghe bundle of fascicles; 3, connective tissue inside thepineural sheath; 4, epineural blood vessels; 5, neighbor-ng vasculature.
ent impairment or loss of neural function. i
Direct Needle Trauma. Most needles available forNBs are manufactured as short-bevel needles (i.e.,ngles 30°-45°). The needle designs are largelyased on the work of Selander and colleagues,189
ho showed that the risk of perforating a nerveascicle was significantly lower when a short-bevel45°) needle was used compared with a standardong-bevel (12°-15°) needle. In contrast, the workf Rice and McMahon190 suggested that the short-eveled needles might cause more mechanicalamage than the long-beveled needles when pur-osefully advanced through a nerve in vitro. Inheir experiment, after deliberately penetrating theargest fascicle of rat sciatic nerves with 12° to 27°eveled injection needles, the degree of neuralrauma on histologic examination was greater withhort-beveled needles. The sharp needles producedlean cuts and the blunt needles produced noncon-ruent cuts on the microscopic images. In addition,he cuts produced by the sharper needles recoveredaster and more completely than the irregular, moreraumatic injuries caused by the blunter short-bev-led needles.190 Despite the lack of consistent datand no randomized controlled trials in humans, theheoretical advantage of short-beveled needles ineducing the risk of nerve penetration has had annfluence on manufacturers and practitioners. Mosteedles manufactured for PNB placement are, to-ay, short-beveled needles.The clinical significance of isolated, direct needle
rauma, however, remains unclear. For instance,uring femoral arterial cannulation, it is likely thathe needle is often inserted into the femoral nerve,et injuries to the nerve are rare, and are usuallyttributed to hematoma formation.184 It is possiblehat a needle-related trauma without injection re-ults in injury of a lesser magnitude, which readilyeals and may go undetected. In contrast, needlerauma coupled with injection of local anestheticnto the nerve may carry a risk for much moreevere injury.
Intraneural Injection. Little is known about howo avoid or recognize insertion of a needle into aerve or how to avoid an intraneuronal injection.ain with injection has long been cited as the car-inal sign of intraneuronal injection. However,ultiple case reports of neurologic injury suggest
hat pain may not be reliable as a sole warning signf impending nerve injury.191-194 Experimental ev-dence suggests that intraneural injection may bessociated with pain on injection but also with aesistance to needle advancement or an increasedressure on injection of local anesthetic.195 In aodel of nerve injury by Selander et al.,195 a pres-
ure of at least 19 psi was required to inject solution
nto a nerve fascicle of a rabbit sciatic nerve. Injec-
tmndstaisihTibc
aciccohsobegtnt
R
cPcwsonpaae
wtjwtdcap
btta1ltowUpcotnisiiar
tnftpfcos
EiHendTht
tticefswonsat
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 25
ion into a nerve fascicle using such high pressuresay result in rupture of the fascicle and the peri-eurium, with consequent histologic evidence ofisruption of the neural anatomy. A more recenttudy using a dog model of nerve injury suggestedhat neurologic injury with intraneural injections isssociated with high-injection pressures.196 Specif-cally, only intraneural injections resulting in pres-ures greater than 20 psi were associated with clin-cally detectable neurologic deficits as well asistologic evidence of injury to nerve fascicles.hese experiments suggest that injection pressuresn excess of 20 psi during nerve block injection maye indicative of an intraneural injection and mayarry a risk of nerve injury.
Neuronal Ischemia. The perineurium is a toughnd resistant tissue layer. An injection into thisompartment or a fascicle can cause a prolongedncrease in endoneurial pressure, exceeding theapillary perfusion pressure. This pressure, in turn,an result in endoneural ischemia.197 The additionf vasoconstricting agents theoretically can en-ance ischemia because of the resultant vasocon-triction and reduction in blood flow. The additionf epinephrine was shown in vitro to decrease thelood supply to intact nerves in the rabbit.195 How-ver, in patients undergoing lower-extremity sur-ery, the addition of epinephrine to the local anes-hetic solution used in combined femoral and sciaticerve blocks was not shown to be a risk factor forhe development of post-block nerve dysfunction.95
isk Factors for Neuropathy After PNB
Few investigations exist regarding neurologicomplications associated with lower-extremityNB. The American Society of Anesthesiologists’losed-claims analysis of nerve injury associatedith anesthesia showed a consistently low report of
ciatic (5% of nerve injury claims) or femoral (2%f nerve injury claims) injuries.198 Postoperativeeurologic complications were more frequently re-orted after general anesthesia, 61% of the claims,nd neuraxial anesthesia than after PNB. In thisnalysis, there was no specific discussion of lower-xtremity neuropathy associated with PNB.198
In the report by Auroy and colleagues,158 thereere 4 neurologic injuries reported after PNB. The
ype of block performed and the nature of the in-ury are not reported. All of the neurologic injuriesere reported within the first 48 hours postopera-
ively. All of these patients reported paresthesiasuring block placement or pain with injection. In allases, the injury had the same topography as thessociated paresthesia or pain. Fanelli et al.95 re-
orted on 2,175 combined sciatic-femoral nerve clocks performed using a nerve stimulator and aechnique of multiple injections. Consistent withhe report of Auroy and coworkers, they reportedn incidence of transient neurologic dysfunction in.7% of patients. There were no permanent neuro-ogic injuries reported in this large cohort of pa-ients. The only variable correlated with the devel-pment of postoperative neurologic dysfunctionas tourniquet inflation pressure of �400 mm Hg.nintended paresthesia was reported in 14% ofatients in the Fanelli et al. study. By study proto-ol, no local anesthetic was injected if a paresthesiaccurred.95 Univariate analysis of potential risk fac-ors for postoperative neurologic dysfunction didot demonstrate paresthesia as a risk factor. Indeed,
n a more recent study from France,165 a nervetimulator was used in 9 of 12 documented nervenjuries. This suggests that the mechanism of nervenjury may be related to some events during andfter the injection (e.g., intraneural injection),ather than to the method of nerve localization.
Blocks Performed in Anesthetized Pa-ients. There are a several individual case reports ofeuropathy after femoral or fascia iliacus block per-
ormed with a nerve stimulator or using a fascial clickechnique in anesthetized patients.56,199-201 Althoughroper sedation and analgesia are essential ingredientsor block success, maintenance of meaningful patientontact allows the patient to report pain or paresthesian injection and may provide an additional margin ofafety.
Other Etiologies of Perioperative Lower-xtremity Neurologic Complications. Nerve
njuries are frequently attributed to the use of PNBs.owever, neuropathy after abdominal or lower-xtremity surgery is relatively common. There are aumber of factors that have been implicated in theevelopment of lower-extremity neuropathy.hese factors include positioning, surgical factors,ematoma formation, compartment syndrome, andourniquet palsy.
Positioning. Positioning injuries are thoughto be caused mostly by compression or stretching ofhe nerve(s) or plexi as a result of patient position-ng. Of the sciatic nerve injury claims in the closed-laims analysis of nerve injury associated with an-sthesia, half were associated with the lithotomy orrog-leg operative positions.198 In a prospectivetudy of lower extremity neuropathies associatedith the lithotomy position, nerve injury to thebturator, lateral femoral cutaneous, and sciaticerves were observed.202 Femoral nerve palsy is as-ociated with deep hip flexion and extension associ-ted with THA and repair of acetabular frac-ures.203,204 Positioning nerve injuries are consistently
orrelated with the length of surgery.202,204-207
thrdpcAaciicfdfa
ctTlipiptsis
nlmtoiiwCtssqrrp
maputrgt
ggrrpa
EE
A
a(seei“sraPctetdlicb
D
pectPto0TaTtdpwi
F
26 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
Surgical Factors Leading to Neuropa-hy. Some surgical procedures are associated with aigh rate of nerve injury. For instance, femoral neu-opathy is associated with operations that requireeep pelvic exposure including acetabular fracture re-air, in which the femoral nerve is relatively superfi-ial and vulnerable to compression by retractors.203,206
n incidence of nerve injury as high as 17% afternkle arthroscopy has been reported.208 The superfi-ial peroneal nerve, in particular, is prone to nervenjury during ankle arthroscopy because of its prox-mity to the dorsal arthroscopy portal.209 The clini-ian’s experience using the arthroscope is anotheractor associated with a high rate of nerve injuryuring this procedure.210 This has been attributed toactors, such as joint distention, excessive traction,nd extravasation of fluid during surgery.Compartment Syndrome. A single case of
ompartment syndrome after revised forefoot ar-hroplasty under ankle block has been reported.211
he diagnosis was delayed secondary to residualocal anesthetic effects. However, prompt surgicalntervention prevented long-term sequelae. This re-ort emphasizes the need for vigilance in monitor-ng block resolution and patient positioning in theostoperative period. Consultation with the surgicaleam is of utmost importance when making a deci-ion on the use of nerve blocks and their durationn patients with a risk of developing compartmentyndrome.
Tourniquet Neuropathy. Tourniquet-inducedeuropathy is well documented in the orthopedic
iterature and ranges from mild neuropraxia to per-anent neurologic injury.211-215 The incidence of
ourniquet paralysis has been reported as 1 in 8,000perations.216 A prospective study of lower-extrem-
ty nerve blockade suggested that higher tourniquetnflation pressure (�400 mm Hg) was associatedith an increased risk of transient nerve injury.95
urrent recommendations for appropriate use ofhe tourniquet include the maintenance of a pres-ure of no more than 150 mm Hg greater than theystolic blood pressure and deflation of the tourni-uet every 90 to 120 minutes.217 Even with theseecommendations, posttourniquet application neu-opraxia may occur, particularly in the setting ofreexisting neuropathy.116,121
Compressive Hematoma. Compressive he-atoma formation leading to neuropathy has been
ssociated with both needle misadventures duringerformance of lower extremity PNB and anticoag-lation.2,185 As opposed to spinal or epidural hema-
oma, in all cases, neuropathy from this etiology hasesolved completely.181,182,218-220 Little data exist re-arding the safety of peripheral nerve block in an-
icoagulated patients. The American Society of Re- uional Anesthesia and Pain Medicine has publisheduidelines regarding this issue.221 However, theseeports emphasize the important differences in theisk-benefit ratio of peripheral nerve blocks com-ared with neuraxial blocks in patients receivingnticoagulant therapy.
valuating the Patient After Lower-xtremity Peripheral Nerve Block
ssessment of Lower-Extremity PNBs
Neal has proposed a simple and effective system forssessing the adequacy of lower-extremity PNBs220
Fig 15A-D). Based on a well-known system for as-essing the upper extremity, the lower-extremityvaluation uses 4 Ps: push, pull, pinch, and punt. Pushvaluates the adequacy of sciatic nerve block by ask-ng the patient to push against the examiner’s hand orto step on the gas” with their foot. Pull checks thetrength of the adductors of the thigh to assess obtu-ator nerve blockade. The examiner abducts the thighnd asks the patient to pull their thigh to the midline.inch refers to the evaluation of the lateral femoralutaneous nerve. A pinch on the lateral proximalhigh will check the adequacy of blockade of the lat-ral femoral cutaneous nerve. Finally, punt assesseshe degree of motor blockade in the femoral nerveistribution. The examiner supports the patient’s kneeifting it off the bed and asks the patient to punt anmaginary football. This maneuver requires quadri-eps contraction to extend the leg and will be limitedy femoral nerve blockade.
ischarge Criteria
The ability to ambulate independently is an im-ortant consideration for patients receiving lowerxtremity PNBs. Klein et al.222 have examined theontroversy of long-lasting analgesia versus poten-ial complications from insensate extremities afterNB in ambulatory surgery patients. They prospec-ively studied 1,791 patients receiving either upper-r lower-extremity nerve block with ropivacaine.5% and being discharged home the same day.here was a single complication related to a fallfter combined femoral and sciatic nerve blocks.he authors attributed the low rate of complicationso the immobilization related to the surgical proce-ure and generally cautious nature of postsurgicalatients. Sample discharge instructions for patientsith single injection and continuous lower extrem-
ty peripheral nerve blocks can be found in Table 5.
uture Directions
Lower-extremity peripheral nerve blocks provide
nquestioned superiority of analgesia after lower-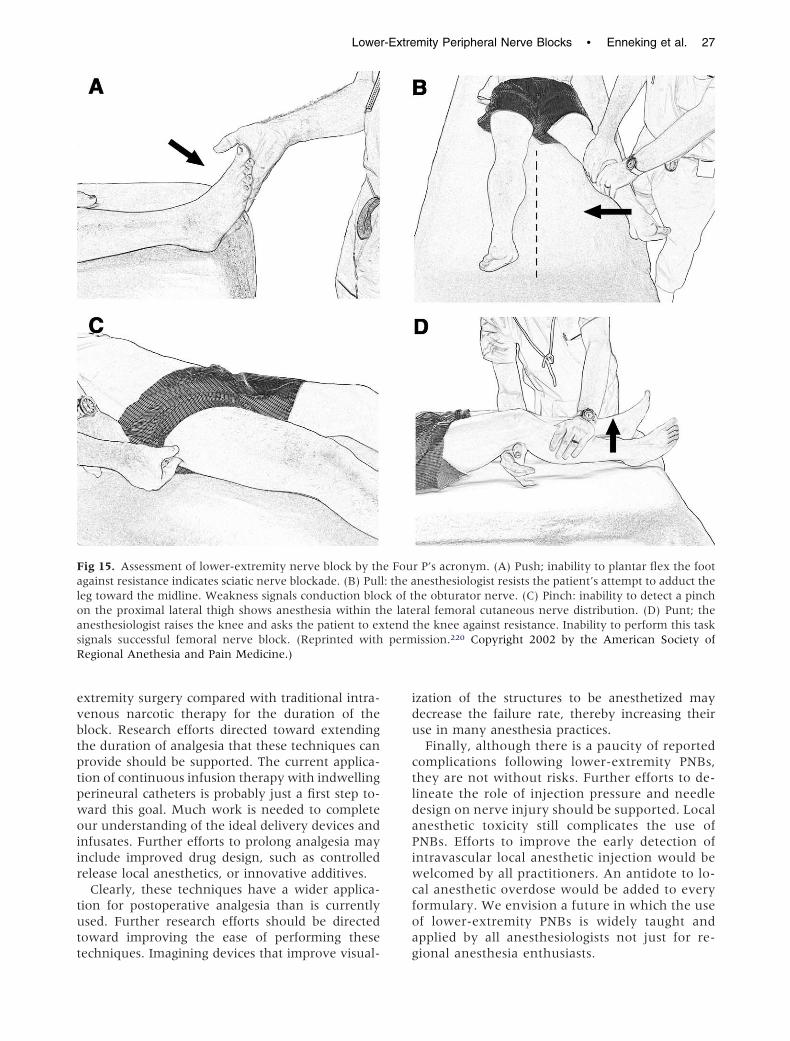
evbtptpwoiir
tutt
idu
ctldaPiwcfoa
FaloasR
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 27
xtremity surgery compared with traditional intra-enous narcotic therapy for the duration of thelock. Research efforts directed toward extendinghe duration of analgesia that these techniques canrovide should be supported. The current applica-ion of continuous infusion therapy with indwellingerineural catheters is probably just a first step to-ard this goal. Much work is needed to completeur understanding of the ideal delivery devices andnfusates. Further efforts to prolong analgesia maynclude improved drug design, such as controlledelease local anesthetics, or innovative additives.
Clearly, these techniques have a wider applica-ion for postoperative analgesia than is currentlysed. Further research efforts should be directedoward improving the ease of performing these
ig 15. Assessment of lower-extremity nerve block by thgainst resistance indicates sciatic nerve blockade. (B) Puleg toward the midline. Weakness signals conduction blocn the proximal lateral thigh shows anesthesia within thnesthesiologist raises the knee and asks the patient to exignals successful femoral nerve block. (Reprinted withegional Anethesia and Pain Medicine.)
echniques. Imagining devices that improve visual- g
zation of the structures to be anesthetized mayecrease the failure rate, thereby increasing theirse in many anesthesia practices.Finally, although there is a paucity of reported
omplications following lower-extremity PNBs,hey are not without risks. Further efforts to de-ineate the role of injection pressure and needleesign on nerve injury should be supported. Localnesthetic toxicity still complicates the use ofNBs. Efforts to improve the early detection ofntravascular local anesthetic injection would beelcomed by all practitioners. An antidote to lo-
al anesthetic overdose would be added to everyormulary. We envision a future in which the usef lower-extremity PNBs is widely taught andpplied by all anesthesiologists not just for re-
r P’s acronym. (A) Push; inability to plantar flex the footnesthesiologist resists the patient’s attempt to adduct thehe obturator nerve. (C) Pinch: inability to detect a pinchral femoral cutaneous nerve distribution. (D) Punt; the
the knee against resistance. Inability to perform this taskission.220 Copyright 2002 by the American Society of
e Foul: the ak of te latetendperm
ional anesthesia enthusiasts.

A
BvUtJsgb
28 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
cknowledgment
The authors would like to thank Anita Yeager,S, Coordinator of Information/Publications Ser-ices in the Department of Anesthesiology at theniversity of Florida, for her calm aplomb in editing
his beast of a manuscipt. The authors also thank Droseph M. Neal, Editor-in-Chief of Regional Anesthe-ia and Pain Medicine, for his patience with anduidance of this project. The authors thank youoth wholeheartedly.
References
1. Gray H. Anatomy of the Human Body. Philadelphia,PA: Lea & Fibiger; 1918.
2. Capdevila X, Macaire P, Dadure C, Choquet O,
Table 5. Patient Instructions After Lower-ExtremityNerve Block
You have received an injection near one of your nerves in yourleg to help you with your pain after surgery. Precautions thatyou should take are:
1. DO NOT DRIVE while your leg is numb.2. You must use your walker, crutches, or wheelchair until the
nerve block has worn off.3. Keep your leg elevated as much as possible for the first 24
hours after surgery to help prevent swelling.4. Keep your leg in the brace at all times except when doing
physical therapy until your surgeon tells you to take it off.5. Do not use heating pads on your leg while it is numb.6. The numbness in your leg will wear off completely about an
hour after you notice that you can feel tingling in the numbpart. Please take your pain medications when the numbnessbegins to wear off and you feel the tingling.
7. If you are ready for bed and the numbness has not worn off,please take your pain medication before you go to bed.
Instructions for Patients Receiving Continuous Lower-ExtremityBlocks
Your anesthesia doctor has placed a small tube near the nerveto your leg to decrease the pain you feel after surgery. Thisis a very effective way to control pain when it is added to theother pain medications your surgeon has given you.Precautions you should use during this treatment are:
1. DO NOT DRIVE while you have the catheter in place.2. You must use your walker, crutches, or wheelchair until the
nerve block has worn off and the catheter has beenremoved.
3. Keep your leg elevated as much as possible for the first 24hours after surgery to help prevent swelling.
4. Keep your leg in the brace at all times except when doingphysical therapy until your surgeon tells you to take it off.
5. Do not use heating pads on your leg while it is numb.6. The medication you are getting through the pump device is
not as strong as the first medicine that you got. When thenumbness begins to wear off, please push the extramedication button. Wait 15 minutes and then take your painpills if you need more pain relief. Once the initial blockwears off you should be able to wiggle your toes and makea muscle in your thigh.
7. If you have questions about the pump or your painmedications call the pager number given to you.
Biboulet P, Ryckwaert Y, D’Athis F. Continuous
psoas compartment block for postoperativeanalgesia after total hip arthroplasty: New land-marks, technical guidelines and clinical evaluation.Anesth Analg 2002;94:1606-1613.
3. Farny J, Girard M, Drolet P. Posterior approach tothe lumbar plexus combined with a sciatic nerveblock using lidocaine. Can J Anaesth 1994;41:486-491.
4. Chudinov A, Berkenstadt H, Salai M, Cahana A,Perel A. Continuous psoas compartment block foranesthesia and perioperative analgesia in patientswith hip fractures. Reg Anesth Pain Med 1999;24:563-568.
5. Bouaziz H, Vial F, Jochum D, Macalou D, Heck M,Meuret P, Braun M, Laxenaire M-C. An evaluationof the cutaneous distribution after obturator nerveblock. Anesth Analg 2002;94:445-449.
6. Available at: http://www.nlm.nih.gov/research/visible/visible_human.html. Accessed May 3, 2004.
7. Cauhepe C, Oliver M, Colombani R, Railhac N. [The“3-in-1” block: myth or reality]. Ann Fr Anesth Re-anim 1989;8:376-378.
8. Marhofer P, Nasel C, Sitzwohl C, Kapral S. Magneticresonance imaging of the distribution of local anes-thetic during the three-in-one block. Anesth Analg2000;90:119-124.
9. Hopkins PM, Ellis FR, Halsall PJ. Evaluation of localanaesthetic blockade of the lateral femoral cutane-ous nerve. Anaesthesia 1991;46:95-96.
10. Snell RS (ed). Clinical Anatomy for Medical Students.2nd ed. Boston: Little Brown and Company; 1981:272, 492, 479.
11. Hullander M, Spillane W, Leivers D, Balsara Z. Theuse of Doppler ultrasound to assist with sciatic nerveblocks. Reg Anesth 1991;16:282-284.
12. Snell RS (ed). Clinical Anatomy for Medical Students.2nd ed. Boston: Little Brown and Company; 1981:492.
13. Volka JD, Hadzic A, April E, Thys DM. The divisionof the sciatic nerve in the popliteal fossa: Anatomi-cal implications for popliteal nerve blockade. AnesthAnalg 2001;92:215-217.
14. Snell RS (ed). Clinical Anatomy for Medical Students.2nd ed. Boston: Little Brown and Company; 1981:479.
15. Chayen D, Nathan H, Chayen M. The psoas com-partment block. Anesthesiology 1976;45:95-99.
16. Ho AM, Karmakar MK. Combined paravertebrallumbar plexus and parasacral sciatic nerve block forreduction of hip fracture in a patient with severeaortic stenosis. Can J Anaesth 2002;49:946-950.
17. Turker G, Uckunkaya N, Yavascaoglu B, YilmazlarA, Ozcelik S. Comparison of the catheter-techniquepsoas compartment block and the epidural block foranalgesia in partial hip replacement surgery. ActaAnaesthesiol Scand 2003;47:30-36.
18. Luber MJ, Greengrass R, Parker T. Patient satisfac-tion and effectiveness of lumbar plexus and sciaticnerve block for total knee arthroplasty. J Arthrop-
lasty 2001;16:17-21.
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 29
19. Goroszeniuk T, di Vadi PP. Repeated psoas compart-ment blocks for the management of long-standinghip pain. Reg Anesth Pain Med 2001;26:376-378.
20. Gray H. Anatomy of the Human Body. Philadelphia,PA: Lea & Fibiger; 1918:416.
21. Brown DL: Psoas compartment block. In: Brow DL,ed. Atlas of Regional Anesthesia. 2nd ed. Philadelphia:Saunders; 1999:88-91.
22. Solanski D. Posterior lumbar plexus (psoas) block.In: Chelly JE, ed. Peripheral Nerve Blocks: A ColorAtlas. Philadelphia, PA: Lippincott, Williams &Wilkins; 1999:90-92.
23. Bridenbaugh PO, Wedel DJ. The lower extremity:Somatic blockade. In: Cousins MJ, Bridenbaugh PO(eds). Neural Blockade: in Clinical Anesthesia and Man-agement of Pain. Philadelphia, PA; Lippincott-Raven;1998:374-376.
24. Winnie AP, Ramamurthy S, Durrani Z, Radonjic R.Plexus blocks for lower extremity surgery. Anesthe-siology Rev 1974;1:11-16.
25. Aida S, Takahashi H, Shimoji K. Renal subcapsularhematoma after lumbar plexus block. Anesthesiology1996;84:452-455.
26. Pousman RM, Mansoor Z, Sciard D. Total spinalanesthetic after continuous posterior lumbar plexusblock. Anesthesiology 2003;98:1281-1282.
27. Reddy MB. Pneumocoele following psoas compart-ment block. Anaesthesia 2002;57:938-939.
28. Parkinson S, Mueller J, Little W, Bailey SL. Extentof blockade with various approaches to the lumbarplexus. Anesth Analg 1989;68:243-248.
29. Dalens B, Tanguy A, Vanneuville G. Lumbar plexusblock in children: A comparison of two proceduresin 50 patients. Anesth Analg 1988;67:750-758.
30. Muravchick S, Owens WD. An unusual complica-tion of lumbar plexus block: A case report. AnesthAnalg 1976;55:350-352.
31. Matheny JM, Hanks GA, Rung GW, Blanda JB,Kalenak A. A comparison of patient-controlled an-algesia and continuous lumbar plexus block afteranterior cruciate ligament reconstruction. Arthros-copy 1993;9:87-90.
32. Pandin PC, Vandesteene A, d’Hollander AA. Lum-bar plexus posterior approach: A catheter placementdescription using electrical stimulation. Anesth Analg2002;95:1428-1431.
33. Goranson BD, Lang S, Cassidy JD, Dust WN, McKer-rell J. A comparison of three regional anaesthesiatechniques for outpatient arthroscopy. Can J Anaesth1997;44:371-376.
34. Fletcher AK, Rigby AS, Heyes FL. Three-in-onefemoral nerve block as analgesia for fractured neckof femur in the emergency department: A random-ized, controlled trial. Ann Emerg Med 2003;41:227-233.
35. Mulroy MF, Larkin KL, Batra MS, Hodgson PS,Owens BD. Femoral nerve block with 0.25% or0.5% bupivacaine improves postoperative analgesiafollowing outpatient arthroscopic anterior cruciate
ligament repair. Reg Anesth Pain Med 2001;26:24-29.36. McCarty EC, Spindler KP, Tingstad E, Shyr Y, HigginsM. Does intraarticular morphine improve pain controlwith femoral nerve block after anterior cruciate liga-ment reconstruction? Am J Sports Med 2001;29:327-332.
37. Frost S, Grossfeld S, Kirkley A, Litchfield B, FowlerPK, Amendola A. The efficacy of femoral nerveblock in pain reduction for outpatient hamstringanterior cruciate ligament reconstruction: A double-blind, prospective, randomized trial. Arthroscopy2000;16:243-248.
38. Wang H, Boctor B, Verner J. The effect of single-injection femoral nerve block on rehabilitation andlength of hospital stay after total knee replacement.Reg Anesth Pain Med 2002;27:139-144.
39. Williams BA, Kentor ML, Vogt MT, Williams JP,Chelly JE, Valalik S, Harner CD, Fu FH. Femoral-sciatic nerve blocks for complex outpatient kneesurgery are associated with less postoperative painbefore same-day discharge. Anesthesiology 2003;98:1206-1213.
40. Vloka JD, Hadzic A, Drobnik L, Ernest A, Reiss W,Thys DM. Anatomic landmarks for femoral nerveblock: A comparison of four needle insertion sites.Anesth Analg 1999;89:1467-1470.
41. Winnie AP, Ramamurthy S, Durrani Z. The inguinalparavascular technic of lumbar plexus anesthesia:The “3-in-1 block.” Anesth Analg 1973;52:989-996.
42. Lang SA, Yip RW, Chang P, Gerard M. The femoral3-in-1 block revisited. J Clin Anesth 1993;5:292-296.
43. Seeberger M, Urwyler A. Paravascular lumbarplexus block: Block extension after femoral nervestimulation and injection of 20 vs. 40 ml mepiva-caine 10 mg/ml. Acta Anaesthesiol Scand 1995;39:769-773.
44. Singelyn F, Gouverneur JM. Extended “3-in-1”block after total knee arthroplasty: Continuous ver-sus patient-controlled techniques. Anesth Analg2000;91:176-180.
45. Singelyn F, Vanderelst P, Gouverneur JM. Extendedfemoral nerve sheath block after total hip arthrop-lasty: Continuous versus patient-controlled tech-niques. Anesth Analg 2001;92:455-459.
46. Chelly JE, Greger J, Gebhard R, Coupe K, ClyburnTA, Buckle R, Criswell A. Continuous femoralblocks improve recovery and outcome of patientsundergoing total knee arthroplasty. J Arthroplasty2001;16:436-445.
47. Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y,Rubenovitch J, d’Athis F. Effects of perioperativeanalgesic technique on the surgical outcome andduration of rehabilitation after major knee surgery.Anesthesiology 1999;91:8-15.
48. Singelyn FJ, Deyaert M, Joris D, Pendeville E,Gouverneur JM. Effects of intravenous patient-con-trolled analgesia with morphine, continuous epi-dural analgesia, and continuous “3-in-1” block onpostoperative pain and knee rehabilitation afterunilateral total knee arthroplasty. Anesth Analg
1998;87:88-92.
30 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
49. Griffith JP, Whiteley S, Gough MJ. Prospective ran-domized study of a new method of providing post-operative pain relief following femoropopliteal by-pass. Br J Surg 1996;83:1735-1738.
50. Dauri M, Polzoni M, Fabbi E, Sidiropoulou T,Servetti S, Coniglione F, Mariani P, Sabato AF.Comparison of epidural, continuous femoral blockand intraarticular analgesia after anterior cruciateligament reconstruction. Acta Anaesthesiol Scand2003;47:20-25.
51. Hirst GC, Lang SA, Dust WN, Cassidy JD, Yip RW.Femoral nerve block. Single injection versus contin-uous infusion for total knee arthroplasty. Reg Anesth1996;21:292-297.
52. Capdevila X, Biboulet P, Morau D, Bernard N, De-schodt J, Lopez S, d’Athis F. Continuous three-in-one block for postoperative pain after lower limborthopedic surgery: Where do the catheters go?Anesth Analg 2002;94:1001-1006.
53. Salinas FV, Neal JM, Sueda LA, Kopacz DJ, Liu SS.Prospective comparison of continuous femoralnerve block with nonstimulating catheter place-ment versus stimulating catheter-guided perineuralplacement in volunteers. Reg Anesth Pain Med 2004;29:212-220.
54. Dalens B, Vanneuville G, Tanguy A. Comparison ofthe fascia iliaca compartment with “3-in-1” block inchildren. Anesth Analg 1989;69:705-713.
55. Lopez S, Gros T, Bernard N, Plasse C, Capdevila X.Fascia iliaca compartment block for femoral bonefractures in prehospital care. Reg Anesth Pain Med2003;28:203-207.
56. Atchabahian A, Brown AR. Postoperative neuropa-thy following fascia iliaca compartment blockade.Anesthesiology 2001;94:534-536.
57. Ganapathy S, Wasserman RA, Watson JT, BennettJ, Armstrong KP, Stockall CA, Chess DG, Mac-Donald C. Modified continuous femoral three-in-one block for postoperative pain after total kneearthroplasty. Anesth Analg 1999;89:1197-1202.
58. Paut O, Sallabery M, Schreiber-Deturmeny E, Re-mond C, Bruguerolle B, Camboulives J. Continuousfascia iliaca compartment block in children: A pro-spective evaluation of plasma bupivacaine concen-trations, pain scores, and side effects. Anesth Analg2001;92:1159-1163.
59. Wassef M. Interadductor approach to obturatornerve blockade for spastic conditions of adductorthigh muscles. Reg Anesth 1993;18:13-17.
60. McNamee DA, Parks L, Milligan KR. Post-operativeanalgesia following total knee replacement: Anevaluation of the addition of an obturator nerveblock to combined femoral and sciatic nerve block.Acta Anaesthesiol Scand 2002;46:95-99.
61. Macalou D, Trueck S, Meuret P, Heck M, Vial F,Ouloguem S, Capdevila X, Virion J-M, Bouaziz H.Postoperative analgesia after total knee replace-ment: The effect of an obturator nerve block addedto the femoral 3-in-1 nerve block. Anesth Analg
2004;99:251-254.62. Karacalar A, Karacalar S, Uckunkaya N, Sahin S,Ozcan B. Combined use of axillary block and lateralfemoral cutaneous nerve block in upper-extremityinjuries requiring large skin grafts. J Hand Surg [Am]1998;23:1100-1105.
63. Maccani RM, Wedel DJ, Melton A, Gronert GA.Femoral and lateral femoral cutaneous nerve blockfor muscle biopsies in children. Paediatr Anaesth1995;5:223-227.
64. Jones SF, White A. Analgesia following femoralneck surgery. Lateral cutaneous nerve block as analternative to narcotics in the elderly. Anaesthesia1985;40:682-685.
65. Coad NR. Postoperative analgesia following femo-ral-neck surgery—A comparison between 3 in 1femoral nerve block and lateral cutaneous nerveblock. Eur J Anaesthesiol 1991;8:287-290.
66. Shannon J, Lang SA, Yip RW, Gerard M. Lateralfemoral cutaneous nerve block revisited. A nervestimulator technique. Reg Anesth 1995;20:100-104.
67. Sharrock NE. Inadvertent “3-in-1 block” followinginjection of the lateral cutaneous nerve of the thigh.Anesth Analg 1980;59:887-888.
68. van der Wal M, Lang SA, Yip RW. Trans-sartorialapproach for saphenous nerve block. Can J Anaesth1993;40:542-546.
69. De Mey JC, Deruyck LJ, Cammu G, De Baerde-maeker LE, Mortier EP. A paravenous approach forthe saphenous nerve block. Reg Anesth Pain Med2001;26:504-506.
70. Comfort VK, Lang SA, Yip RW. Saphenous nerveanaesthesia—A nerve stimulator technique. Can JAnaesth 1996;43:852-857.
71. Bouaziz H, Henhamou D, Narchi P. A new approachfor saphenous nerve block (letter). Reg Anesth 1996;21:490.
72. Tokat O, Turker YG, Uckunkaya N, Yilmazlar A. Aclinical comparison of psoas compartment and in-guinal paravascular blocks combined with sciaticnerve block. J Int Med Res 2002;30:161-167.
73. Morau D, Lopez S, Biboulet P, Bernard N, Amar J,Capdevila X. Comparison of continuous 3-in-1 andfascia iliaca compartment blocks for postoperativeanalgesia: Feasibility, catheter migration, distribu-tion of sensory block, and analgesic efficacy. RegAnesth Pain Med 2003;28:309-314.
74. Capdevila X, Biboulet P, Bouregba M, Barthelet Y,Rubenovitch J, d’Athis F. Comparison of the three-in-one and fascia iliaca compartment blocks inadults: Clinical and radiographic analysis. AnesthAnalg 1998;86:1039-1044.
75. Kaloul I, Guay J, Cote C, Fallaha M. The posteriorlumbar plexus (psoas compartment) block and thethree-in-one femoral nerve block provide similarpostoperative analgesia after total knee replace-ment. Can J Anaesth 2004;51:45-51.
76. Mansour N. Sub-sartorial saphenous nerve blockwith the aid of nerve stimulator. Reg Anesth 1993;
28:266-268.
1
1
1
1
1
1
1
1
1
1
1
1
1
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 31
77. Morris GF, Lang SA, Dust WN, Van der Wal M. Theparasacral sciatic nerve block. Reg Anesth 1997;22:223-228.
78. Gaertner E, Lascurain P, Venet C, Maschino X, ZamfirA, Lupescu R, Hadzic A. Continuous parasacral sciaticblock: A radiographic study. Anesth Analg 2004;98:831-834.
79. Winnie AP. Regional anesthesia. Surg Clin North Am1975;55:861-892.
80. Raj PP, Parks RI, Watson TD, Jenkins MT. A newsingle-posterior supine approach to sciatic-femoralnerve block. Anesth Analg 1975;54:489-494.
81. McNichol LR. Sciatic nerve block for children: Sci-atic nerve block by anterior approach for postoper-ative pain relief. Anaesthesia 1985;40:410-414.
82. Guardini R, Waldron BA, Wallace WA. Sciatic nerveblock: A new lateral approach. Acta AnaesthesiolScand 1985;29:515-519.
83. Labat G. Regional Anesthesia: Its Technic and ClinicalApplication. Philadelphia, PA: Saunders; 1922.
84. Chang PC, Lang SA, Yip RW. Reevaluation of thesciatic nerve block. Reg Anesth 1993;18:18-23.
85. Franco CD. Posterior approach to the sciatic nervein adults: Is Euclidean geometry still necessary? An-esthesiology 2003;98:723-728.
86. Ichiyanagi K. Sciatic nerve block: Lateral approachwith patient supine. Anesthesiology 1959;20:601-604.
87. Beck GP. Anterior sciatic nerve block. Anesthesiology1963;24:222-224.
88. Magora F, Pessachovitch B, Shoham I. Sciatic nerveblock by the anterior approach for operations on thelower extremity. Br J Anaesth 1974;46:121-123.
89. Chelly JE, Delaunay L. A new anterior approach tothe sciatic nerve block. Anesthesiology 1999;91:1655-1660.
90. Vloka D, Hadzic A, April E, Thys DM. Anteriorapproach to the sciatic nerve block: The effects of legrotation. Anesth Analg 2001;92:460-462.
91. Ericksen ML, Swenson JD, Pace NL. The anatomicrelationship of the sciatic nerve to the lesser tro-chanter: Implications for anterior sciatic nerveblock. Anesth Analg 2002;95:1071-1074.
92. Dalens B, Tanguy A, Vanneuville G. Sciatic nerveblocks in children: Comparison of the posterior, an-terior, and lateral approaches in 180 pediatric pa-tients. Anesth Analg 1990;70:131-137.
93. Chowdary K, Splinter W. Sciatic nerve block: A newapproach. Can J Anesth 2003;50:A51 (abstr).
94. di Benedetto P, Casati A, Bertini L, Fanelli G. Pos-terior subgluteal approach to block the sciatic nerve:Description of the technique and initial clinical ex-periences. Eur J Anaesthesiol 2002;19:682-686.
95. Fanelli G, Casati A, Garancini P, Torri G. Nervestimulator and multiple injection technique for up-per and lower limb blockade: Failure rate, patientacceptance, and neurologic complications. StudyGroup on Regional Anesthesia. Anesth Analg 1999;88:847-852.
96. Rorie DK, Byer DE, Nelson DO, Sittipong R, JohnsonKA. Assessment of block of the sciatic nerve in the
popliteal fossa. Anesth Analg 1980;59:371-376.97. Hansen E, Eshelman MR, Cracchiolo A. Poplitealfossa neural blockade as the sole anesthetic tech-nique for outpatient foot and ankle surgery. FootAnkle Int 2000;21:38-44.
98. Rongstad K, Mann RA, Prieskorn D, Nichelson S,Horton G. Popliteal sciatic nerve block for postoper-ative analgesia. Foot Ankle Int 1996;17:378-382.
99. Vloka JD, Hadzic A, Mulcare R, Lesser JB, Koorn R,Thys DM. Combined popliteal and posterior cutane-ous nerve of the thigh blocks for short saphenousvein stripping in outpatients: An alternative to spi-nal anesthesia. J Clin Anesth 1997;9:618-622.
00. Tobias JD, Mencio GA. Popliteal fossa block forpostoperative analgesia after foot surgery in infantsand children. J P Orthop 1999;19:511-514.
01. Vloka JD, Hadžic A, Koorn R, Thys D. Supine ap-proach to the sciatic nerve in the popliteal fossa. CanJ Anaesth 1996;43:964-967.
02. Singelyn F, Aye F, Gouverneur JM. Continuouspopliteal sciatic nerve block: An original techniqueto provide postoperative analgesia after foot sur-gery. Anesth Analg 1997;84:383-386.
03. Ilfeld BM, Morey TE, Wang RD, Enneking FK. Con-tinuous popliteal sciatic nerve block for postopera-tive pain control at home: A randomized, double-blinded, placebo-controlled study. Anesthesiology2002;97:959-965.
04. Schimek F, Deusch H. New technique of sciaticnerve block in the popliteal fossa. Eur J Anaesth1995;12:163-169.
05. Levecque JP, Borne M, Saissy JM. Analgesia withcontinuous lateral posterior tibial nerve block (let-ter). Reg Anesth Pain Med 1999;24:191-192.
06. Gouverneur JM. Sciatic nerve block in the poplitealfossa with atraumatic needles and nerve stimula-tion. Acta Anaesthesiol Belg 1985;36:391-399.
07. Singelyn F, Gouverneur JM, Gribomont BF. Popli-teal sciatic nerve block aided by a nerve stimulator:A reliable technique for foot and ankle surgery. RegAnesth 1991;16:278-281.
08. Hadzic A, Volka JD, Singson R, Santos AC, ThysDM. A comparison of intertendinous and classicalapproaches to popliteal nerve block using magneticresonance imaging simulation. Anesth Analg 2002;94:1321-1324.
09. Benzon HT, Kim C, Benzon HP, Silverstein ME,Jericho B, Prillaman K, Buenaventura R. Correla-tion between evoked motor response of the sciaticnerve and sensory blockade. Anesthesiology 1997;87:547-552.
10. Paqueron X, Bouaziz H, Macalou D, Labaille T,Merle M, Laxenaire MC, Benhamou D. The lateralapproach to the sciatic nerve at the popliteal fossa:One or two injections? Anesth Analg 1999;89:1221-1225.
11. Zetlaoui PJ, Bouaziz H. Lateral approach to the sci-atic nerve in the popliteal fossa. Anesth Analg 1998;87:79-82.
12. Vloka JD, Hadzic A, Kitain E, Lesser JB, Kuroda M,
April EW, Thys DM. Anatomic considerations for
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
32 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
sciatic nerve block in the popliteal fossa through thelateral approach. Reg Anesth 1996;21:414-418.
13. di Benedetto P, Casati A, Bertini L, Fanelli G, ChellyJE. Postoperative analgesia with continuous sciaticnerve block after foot surgery: A prospective, ran-domized comparison between the popliteal andsubgluteal approaches. Anesth Analg 2002;94:996-1000.
14. Chelly JE, Greger J, Casati A, Al Samsam T,McGarvey W, Clanton T. Continuous lateral sciaticblocks for acute postoperative pain management aftermajor ankle and foot surgery. Foot Ankle Int 2002;23:749-752.
15. Sutherland ID. Continuous sciatic nerve infusion:Expanded case report describing a new approach.Reg Anesth Pain Med 1998;23:496-501.
16. Schurman DJ. Ankle-block anesthesia for foot sur-gery. Anesthesiology 1976;44:348-352.
17. Pinzur MS, Morrison C, Sage R, Stuck R, OstermanH, Vrbos L. Syme’s two-stage amputation in insulin-requiring diabetics with gangrene of the forefoot.Foot Ankle 1991;11:394-396.
18. Harvey CK. Dilute lidocaine ankle blocks in thediagnosis of sympathetically maintained pain. J AmPodiatr Med Assoc 1997;87:473-477.
19. Delgado-Martinez AD, Marchal-Escalona JM. Su-pramalleolar ankle block anesthesia and ankle tour-niquet for foot surgery. Foot Ankle Int 2001;22:836-838.
20. Gerbert J. The location of the terminal branching ofthe posterior tibial nerve and its effect on adminis-tering a posterior tibial nerve block. J Am PodiatryAssoc 1971;61:8-11.
21. Lichtenfeld NS. The pneumatic ankle tourniquetwith ankle block anesthesia for foot surgery. FootAnkle 1992;13:344-349.
22. Colgrove RC. Posterior tibial nerve block. Foot AnkleInt 2001;22:839-840.
23. Wassef MR. Posterior tibial nerve block. A newapproach using the bony landmark of the susten-taculum tali. Anaesthesia 1991;46:841-844.
24. Sharrock NE, Waller JF, Fierro LE. Midtarsal block forsurgery of the forefoot. Br J Anaesth 1986;58:37-40.
25. Needoff M, Radford P, Costigan P. Local anesthesia forpostoperative pain relief after foot surgery: A prospec-tive clinical trial. Foot Ankle Int 1995;6:11-13.
26. Mineo R, Sharrock NE. Venous levels of lidocaineand bupivacaine after midtarsal ankle block. RegAnesth 1992;17:47-49.
27. Brown EM, McGriff JT, Malinowski RW: Intrave-nous regional anaesthesia (Bier block): Review of20 years’ experience. Can J Anesth 1989;36:307-310.
28. Ruben SS, Sklar J. Intravenous regional anesthesiawith clonidine in the management of complex re-gional pain syndrome of the knee. J Clin Anesth2002;14:87-91.
29. Henderson CL, Warriner CB, McEwen JA, MerrickPM. A North American survey of intravenous re-
gional anesthesia. Anesth Analg 1997;85:858-863.30. Lehman WL, Jones WW. Intravenous lidocaine foranesthesia in the lower extremity. A prospectivestudy. J Bone Joint Surg [Am] 1984;66:1056-1060.
31. Nusbaum LM, Hamelberg W. Intravenous regionalanesthesia for surgery on the foot and ankle. Anes-thesiology 1986;64:91-92.
32. Al Metwalli R, Mowafi HA. A modification of theinter-cuff technique of IVRA for use in knee arthro-scopy. Can J Anaesth 2002;49:687-689.
33. Cuvillon P, Ripart J, Jeannes P, Mahamat A, BoissonC, L’Hermite J, Vernes E, de la Coussaye JE. Compar-ison of the parasacral approach and the posterior ap-proach, with single- and double-injection techniques,to block the sciatic nerve. Anesthesiology 2003;98:1436-1441.
34. Kilpatrick AW, Coventry DM, Todd JG. A compar-ison of two approaches to sciatic nerve block. An-aesthesia 1992;47:155-157.
35. Taboada M, Alvarez J, Cortes J, Rodriguez J, RabanalS, Gude F, Atanassoff A, Atanassoff PG. The effects ofthree different approaches on the onset time of sciaticnerve blocks with 0.75% ropivacaine. Anesth Analg2004;98:242-247.
36. Hadzic A, Vloka JD. A comparison of the posteriorversus lateral approaches to the block of the sciaticnerve in the popliteal fossa. Anesthesiology 1998;88:1480-1486.
37. McLeod DH, Wong DH, Claridge RJ, Merrick PM.Lateral popliteal sciatic nerve block compared withsubcutaneous infiltration for analgesia followingfoot surgery. Can J Anaesth 1994;41:673-676.
38. Singelyn FJ. Single-injection applications for footand ankle surgery. Best Pract Res Clin Anaesthesiol2002;16:247-254.
39. Kaiser H, Niesel HC, Klimpel L. Influence of mini-mum current for peripheral nerve stimulation onthe latency and success rate of sciatic blockade. RegAnesth 1988;11:92-97.
40. Davies MJ, McGlade DP. One hundred sciatic nerveblocks: A comparison of localization techniques. An-aesth Intensive Care 1993;21:76-78.
41. Rosenblatt R. Continuous femoral anesthesia forlower extremity surgery. Anesth Analg 1980;59:631-632.
42. Tetzlaff JE, Andrish J, O’Hara J Jr, Dilger J, YoonHJ. Effectiveness of bupivacaine administered viafemoral nerve catheter for pain control after ante-rior cruciate ligament repair. J Clin Anesth 1997;9:542-545.
43. Singelyn F, Gouverneur JM. Postoperative analge-sia after total hip arthroplasty: IV PCA with mor-phine, patient-controlled epidural analgesia, or con-tinuous “3-in-1” block?: A prospective evaluationby our acute pain service in more than 1300 pa-tients. J Clin Anesth 1999;11:550-554.
44. Bailey SL, Parkinson SK, Little WL, Simmerman SR.Sciatic nerve block: A comparison of single versusdouble injection technique. Reg Anesth 1994;19:9-13.
45. Cuvillon P, Ripart J, Jeannes P, Mahamat A, BoissonC, L’Hermite J, Vernes E, de la Coussaye JE. Compar-
ison of the parasacral approach and the posterior ap-
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 33
proach, with single- and double-injection techniques,to block the sciatic nerve. Anesthesiology 2003;98:1436-1441.
46. Casati A, Fanelli G, Beccaria P Magistris L, AlbertinA, Torri G. The effects of single or multiple injec-tions on the volume of 0.5% ropivacaine requiredfor femoral nerve blockade. Anesth Analg 2001;93:83-86.
47. Kirchmair L, Entner T, Wissel J, Moriggl B, KapralS, Mitterschiffthaler G. A study of the paravertebralanatomy for ultrasound-guided posterior lumbarplexus block. Anesth Analg 2001;93:477-481.
48. Kirchmair L, Entner T, Kapral S, Mitterschiffthaler G.Ultrasound guidance for the psoas compartmentblock: An imaging study. Anesth Analg 2002;94:706-710.
49. Marhofer P, Schrogendorfer K, Koinig H Kapraal S,Weinstabl C, Mayer N. Ultrasonographic guidanceimproves sensory block and onset time of three-in-one blocks. Anesth Analg 1997;85:854-857.
50. Marhofer P, Schrogendorfer K, Wallner T, Koinig H,Mayer N, Kapral S. Ultrasonography guidance re-duces the amount of local anesthetic for 3-in-1blocks. Reg Anesth Pain Med 1998;23:584-588.
51. Neal JM, Hebl JR, Gerancher JC, Hogan QH. Bra-chial plexus anesthesia: Essentials of our currentunderstanding. Reg Anesth Pain Med 2002;27:402-428.
52. Fanelli G, Casati A, Beccaria P, Aldegheri G, BertiM, Tarantino F, Torri G. A double-blind comparisonof ropivacaine, bupivacaine, and mepivacaine dur-ing sciatic and femoral nerve blockade. Anesth Analg1998;87:597-600.
53. Connolly C, Coventry DM, Wildsmith JA. Double-blind comparison of ropivacaine 7.5 mg ml(-1) withbupivacaine 5 mg ml(-1) for sciatic nerve block. Br JAnaesth 2001;86:674-677.
54. Greengrass RA, Klein SM, D’Ercole FJ, Gleason DG,Shimer CL, Steele SM. Lumbar plexus and sciaticnerve block for knee arthroplasty: Comparison ofropivacaine and bupivacaine. Can J Anaesth 1998;45:1094-1096.
55. Casati A, Borghi B, Fanelli G, Cerchierini E, Santor-sola R, Sassoli V, Grispigni C, Tori G. A double-blinded, randomized comparison of either 0.5%levobupivacaine or 0.5% ropivacaine for sciaticnerve block. Anesth Analg 2002;94:987-990.
56. Neal JM. Effects of epinephrine in local anestheticson the central and peripheral nervous systems:Neurotoxicity and neural blood flow. Reg AnesthPain Med 2003;28:124-134.
57. Weber A, Fournier R, Van Gessel E, Riand N,Gamulin Z. Epinephrine does not prolong the anal-gesia of 20 mL ropivacaine 0.5% or 0.2% in afemoral three-in-one block. Anesth Analg 2001;93:1327-1331.
58. Auroy Y, Narchi P, Messiah A, Litt L, Rouvier B,Samii K. Serious complications related to regionalanesthesia: Results of a prospective survey in
France. Anesthesiology 1997;87:479-486.59. Candido KD, Winnie AP, Covino BG, Raza SM,Vasireddy AR, Masters RW. Addition of bicarbonateto plain bupivacaine does not significantly alter theonset or duration of plexus anesthesia. Reg Anesth1995;20:133-138.
60. Gentili M, Bernard JM, Bonnet F. Adding clonidineto lidocaine for intravenous regional anesthesia pre-vents tourniquet pain. Anesth Analg 1999;88:1327-1330.
61. Casati A, Magistris L, Fanelli G, Beccaria P, CappelleriG, Aldegheri G, Torri G. Small-dose clonidine prolongspostoperative analgesia after sciatic-femoral nerveblock with 0.75% ropivacaine for foot surgery. AnesthAnalg 2000;91:388-392.
62. Reinhart DJ, Stagg KS, Walker KG, Wang WP,Parker CM, Jackson HH, Walker EB. Postoperativeanalgesia after peripheral nerve block for podiatricsurgery: Clinical efficacy and chemical stability oflidocaine alone versus lidocaine plus ketorolac. RegAnesth Pain Med 2000;25:506-513.
63. Ilfeld BM, Morey TE, Enneking FK. Continuousinfraclavicular perineural infusion with clonidineand ropivacaine compared with ropivacaine alone:A randomized, double-blinded, controlled study.Anesth Analg 2003;97:706-712.
64. Reinhart DJ, Wang W, Stagg KS, Walker KG, BaileyPL, Walker EB, Zaugg SE. Postoperative analgesiaafter peripheral nerve block for podiatric surgery:Clinical efficacy and chemical stability of lidocainealone versus lidocaine plus ketorolac. Reg AnesthPain Med 2000;25:506-513.
65. Auroy Y, Benhamou D, Bargues L, Ecoffey C,Falissard B, Mercier FJ, Bouaziz H, Samii K, MercierF. Major complications of regional anesthesia inFrance: The SOS regional anesthesia hotline service.Anesthesiology 2002;97:1274-1280.
66. Pham-Dang C, Beaumont S, Floch H, Bodin J,Winer A, Pinaud M. [Acute toxic accident followinglumbar plexus block with bupivacaine]. Ann FrAnesth Reanim 2000;19:356-359.
67. Breslin DS, Martin G, Macleod DB, D’Ercole F,Grant SA. Central nervous system toxicity followingthe administration of levobupivacaine for lumbarplexus block: A report of two cases. Reg Anesth PainMed 2003;28:144-147.
68. Mullanu C, Gaillat F, Scemama F, Thibault S,Lavand’homme P, Auffray JP. Acute toxicity of localanesthetic ropivacaine and mepivacaine during acombined lumbar plexus and sciatic block for hipsurgery. Acta Anaesthesiol Belg 2002;53:221-223.
69. Petitjeans F, Mion G, Puidupin M, Tourtier JP, Hut-son C, Saissy JM. Tachycardia and convulsions in-duced by accidental intravascular ropivacaine injec-tion during sciatic block. Acta Anaesthesiol Scand2002;46:616-617.
70. Odoom JA, Zuurmond WW, Sih IL, Bovill J, OsterlofG, Oosting HV. Plasma bupivacaine concentrationsfollowing psoas compartment block. Anaesthesia 1986;
41:155-158.
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
34 Regional Anesthesia and Pain Medicine Vol. 30 No. 1 January–February 2005
71. Elmas C, Atanassoff PG. Combined inguinal para-vascular (3-in-1) and sciatic nerve blocks for lowerlimb surgery. Reg Anesth 1993;18:88-92.
72. Misra U, Pridie AK, McClymont C, Bower S. Plasmaconcentrations of bupivacaine following combinedsciatic and femoral 3 in 1 nerve blocks in open kneesurgery. Br J Anaesth 1991;66:310-313.
73. Simon MA, Gielen MJ, Lagerwerf AJ, Vree TB.Plasma concentrations after high doses of mepiva-caine with epinephrine in the combined psoas com-partment/sciatic nerve block. Reg Anesth 1990;15:256-260.
74. Scott DB. Evaluation of the toxicity of local anaes-thetic agents in man. Br J Anaesth 1975;47:56-61.
75. Selander D, Sjostrand J. Longitudinal spread of intra-neurally injected local anesthetics. An experimentalstudy of the initial distribution following intraneuralinjections. Acta Anaesthesiol Scand 1978;22:622-634.
76. Singelyn FJ, Contreras V, Gouverneur JM. Epiduralanesthesia complicating continuous 3-in-1 lumbarplexus blockade. Anesthesiology 1995;83:217-219.
77. Gentili M, Aveline C, Bonnet F. Total spinal anes-thesia complicating posterior lumbar plexus block.Ann Fr Anesth Reanim 1998;17:740-742.
78. Cuvillon P, Ripart J, Lalourcey L, Veyrat E,L’Hemite J, Boisson C, Thouabtia E, Eledjam JJ. Thecontinuous femoral nerve block catheter for post-operative analgesia: Bacteria colonization, infec-tious rate and adverse effects. Anesth Analg 2001;93:1045-1049.
79. Jöhr M. [A complication of continuous femoralnerve block.] Reg Anaesth 1987;10:37-38.
80. Kent KC, Moscucci M, Gallagher SG, DiMattia ST,Skillman JJ. Neuropathy after cardiac catheteriza-tion: Incidence, clinical patterns, and long-termoutcome. J Vasc Surg 1994;19:1008-1013.
81. Klein SM, D’Ercole F, Greengrass RA, Warner DS.Enoxaparin associated with psoas hematoma andlumbar plexopathy after lumbar plexus block. Anes-thesiology 1997;87:1576-1579.
82. Weller RS, Gerancher JC, Crews JC, Wade KL. Ex-tensive retroperitoneal hematoma without neuro-logic deficit in two patients who underwent lumbarplexus block and were later anticoagulated. Anesthe-siology 2003;98:581-585.
83. Hadzic A, Volka J. Peripheral Nerve Blocks: Principlesand Practice. New York: McGraw Hill; 2003:218-233.
84. Kent KC, Moscucci M, Mansour KA, DiMattia S,Gallagher S, Kuntz R, Skillman JJ. Retroperitonealhematoma after cardiac catheterization: Prevalence,risk factors, and optimal management. J Vasc Surg1994;20:905-910.
85. Adam F, Jaziri S, Chauvin M. Psoas abscess compli-cating femoral nerve block catheter. Anesthesiology2003;99:230-231.
86. Bernstein IT, Hansen BJ. Iatrogenic psoas abscess.Case report. Scand J Urol Nephrol 1991;25:85-86.
87. Hadzic A, Vloka JD, Kuroda MM, Koorn R, BirnbachDJ. The practice of peripheral nerve blocks in theUnited States. A national survey. Reg Anesth Pain Med
1998;23:241-246.88. Selander D. Nerve toxicity of local anesthetics. In:Lofstrom JB, Sjostrand U, eds. Local Anesthesia andRegional Blockade. Amsterdam: Elsevier Science;1988:77.
89. Selander D, Dhuner KG, Lundborg G. Peripheralnerve injury due to injection needles used for re-gional anesthesia. Acta Anaesthesiol Scand 1977;21:182-189.
90. Rice ASC, McMahon SB. Peripheral nerve injurycaused by injection needles used in regional anaes-thesia: Influence of bevel configuration, studied in arat model. Br J Anaesth 1992;9:433-438.
91. Lim EK, Pereira R. Brachial plexus injury followingbrachial plexus block. Anesthesia 1984;39:691-694.
92. Bashein G, Robertson TH, Kennedy WF. Persistentphrenic nerve paresis following interscalene bra-chial plexus block. Anesthesiology 1985;63:102-104.
93. Gillespie JH, Menk EJ, Middaugh RE. Reflex sym-pathetic dystrophy: A complication of interscaleneblock. Anesth Analg 1987;66:1316-1317.
94. Fremling MA, Mackinnon SE. Injection injury tothe median nerve. Ann Plast Surg 1996;37:561-567.
95. Selander D, Mansson GL, Karlsson L, Svanvik J.Adrenergic vasoconstriction in peripheral nerves ofthe rabbit. Anesthesiology 1985;62:6-10.
96. Hadzic A, Dilberovic F, Shah S, Mornjakovic Z,Divanovic Kucuk-Alija, Zulic I, Selak I, KulenovicA. Combination of intraneural injection and highinjection pressure leads to severe fascicular injuryand neurologic deficits in dogs. Reg Anesth Pain Med2004;29:417-423.
97. Selander D. Peripheral nerve injury after regionalanesthesia. In: Finucane BT, ed. Complications of Re-gional Anesthesia. Philadelphia: Churchill Living-stone; 1999:105-115.
98. Cheney FW, Domino KB, Caplan RA, Posner KL.Nerve injury associated with anesthesia: A closedclaims analysis. Anesthesiology 1999;90:1062-1069.
99. Bradshaw E, McHale S. Bupivacaine and femoralnerve block. Anaesthesia 1989;44:174.
00. Frerk CM. Palsy after femoral nerve block. Anaes-thesia 1988;43:167-168.
01. McNichol LR. Palsy after femoral nerve block (let-ter). Anaesthesia 1988;43:509.
02. Warner MA, Warner DO, Harper CM, SchroederDR, Maxson PM. Lower extremity neuropathies as-sociated with lithotomy positions. Anesthesiology2000;93:938-942.
03. Gruson KI, Moed BR. Injury of the femoral nerveassociated with acetabular fracture. J Bone Joint Surg[Am] 2003;85A:428-431.
04. Slater N, Singh R, Senasinghe N, Gore R, GoroszeniukT, James D. Pressure monitoring of the femoral nerveduring total hip replacement: An explanation for iat-ropathic palsy. J R Coll Surg Edinb 2000;45:231-233.
05. Gombar KK, Gombar S, Singh B, Sangwan SS, SiwachRC: Femoral neuropathy: A complication of the lithot-omy position. Reg Anesth 1992;17:306-308.
06. Dillavou ED, Anderson LR, Bernert RA, MularskiRA, Hunter GC, Fiser SM, Rappaport WD. Lower
extremity iatrogenic nerve injury due to compres-
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
Lower-Extremity Peripheral Nerve Blocks • Enneking et al. 35
sion during intraabdominal surgery. Am J Surg1997;173:504-508.
07. Nercessian OA, Macaulay W, Stinchfield FE. Periph-eral neuropathies following total hip arthroplasty.J Arthroplasty 1994;9:645-651.
08. Barber FA, Click J, Britt BT. Complications of anklearthroscopy. Foot Ankle 1990;10:263-266.
09. Ferkel RD, Heath DD, Guhl JF. Neurological com-plications of ankle arthroscopy. Arthroscopy 1996;12:200-208.
10. Lamy C, Stienstra JJ. Complications in ankle arthros-copy. Clin Podiatr Med Surg 1994;11:523-539.
11. Middleton RW, Varian JP. Tourniquet paralysis.Aust N Z J Surg 1974;44:124-127.
12. Dawson DM, Hallet M, Wilbourn AJ (eds). Entrap-ment Neuropathies. 3rd ed. Philadelphia: Lippincott-Raven; 1999:319-322.
13. Saunders KC, Louis DL, Weingarden SI, WatkibusGW. Effect of tourniquet time on postoperativequadriceps function. Clin Orthop 1979;143:194-199.
14. Sharrock NE, Savarese JJ. Anesthesia for orthopedicsurgery. In: Miller RD Cucchiara RF, Miller ED,Reves JG, Roizen MF, Savarese JJ, eds. Anesthesia.5th ed. Philadelphia: Churchill Livingstone; 2000:2118-2139.
15. Love BR. The tourniquet. Aust N Z J Surg 1978;48:
66-70.16. Jankowski CJ, Keegan MT, Bolton CF, Harrison BA.Neuropathy following axillary brachial plexusblocks: Is it the tourniquet? Anesthesiology 2003;99:1230-1232.
17. Finsen V, Kasseth AM. Tourniquets in forefoot sur-gery: Less pain when placed at the ankle. J BoneJoint Surg [Br] 1997;79:99-101.
18. Crosby ET, Reid DR, DiPrimio G, Grahovac S. Lum-bosacral plexopathy from iliopsoas haematoma af-ter combined general-epidural anaesthesia for ab-dominal aneurysmectomy. Can J Anaesth 1998;45:46-51.
19. Ho KJ, Gawley SD, Young MR. Psoas haematomaand femoral neuropathy associated with enoxapa-rin therapy. Int J Clin Pract 2003;57:553-554.
20. Neal JM. Assessment of lower extremity nerveblock: Reprise of the four P’s acronym. Reg AnesthPain Med 2002;27:618-620.
21. Horlocker TT, Wedel DJ, Benzon H, Brown DL,Enneking FK, Heit JA, Mulroy MF, Rosenquist RW,Rowlingson J, Tryba M, Yuan CS. Regional anes-thesia in the anticoagulated patient: Defining therisks. Reg Anesth Pain Med 2004;29(2 suppl):1-12.
22. Klein SM, Nielsen KC, Greengrass RA, Warner DS,Martin A, Steele SM. Ambulatory discharge afterlong-acting peripheral nerve blockade: 2382 blocks
with ropivacaine. Anesth Analg 2002;94:65-70.