lung cancer 101 - uk healthcare cecentral · lung cancer 101 tim mullett, md chief, ... colon &...
TRANSCRIPT
11/3/2008
1
Lung Cancer 101Lung Cancer 101
Tim Mullett, MDTim Mullett, MD,,Chief, Section of General Thoracic SurgeryChief, Section of General Thoracic SurgeryUniversity of KentuckyUniversity of KentuckyLexington, KYLexington, KY
Lung CancerLung CancerEarly DetectionEarly Detection
It is easier just to quit smoking!It is easier just to quit smoking!It is easier just to quit smoking!It is easier just to quit smoking!
Tim Mullett, MDTim Mullett, MD,,Chief, Section of General Thoracic SurgeryChief, Section of General Thoracic SurgeryUniversity of KentuckyUniversity of KentuckyLexington, KYLexington, KY
11/3/2008
2
Lung CancerLung Cancer-- Know your EnemyKnow your Enemy
Introduction to Lung CancerIntroduction to Lung Cancer Introduction to Lung CancerIntroduction to Lung Cancer Understanding the Impact of Lung Understanding the Impact of Lung
Cancer in Kentucky and the USCancer in Kentucky and the US Risk factorsRisk factors ScreeningScreening ScreeningScreening SymptomsSymptoms Importance of StageImportance of Stage
Lung Cancer: What is it?Lung Cancer: What is it?
Uncontrolled growth of malignant cells in one Uncontrolled growth of malignant cells in one or both lungs and tracheoor both lungs and tracheo--bronchial treebronchial tree
Arises from protective or ciliated cells in the Arises from protective or ciliated cells in the bronchial epitheliumbronchial epithelium
Begins as a result of repeated carcinogenic Begins as a result of repeated carcinogenic irritation causing increased rates of cellirritation causing increased rates of cellirritation causing increased rates of cell irritation causing increased rates of cell replicationreplication
Proliferation of abnormal cells leads to Proliferation of abnormal cells leads to hyperplasia, dysplasia or carcinoma in situhyperplasia, dysplasia or carcinoma in situ

11/3/2008
3
US Mortality, 2004US Mortality, 2004
1.1. Heart DiseasesHeart Diseases 652,486652,486 27.227.2
Rank Cause of DeathNo. of deaths
% of all deaths
2.2. CancerCancer 553,888553,888 23.123.1
3.3. CerebrovascularCerebrovascular diseasesdiseases 150,074150,074 6.36.3
4.4. Chronic lower respiratory diseasesChronic lower respiratory diseases 121,987 121,987 5.15.1
5.5. Accidents (Unintentional injuries)Accidents (Unintentional injuries) 112,012 112,012 4.74.7
6.6. Diabetes mellitusDiabetes mellitus 73,13873,138 3.13.1
Source: US Mortality Public Use Data Tape 2004, National Center for Health Statistics, Centers for Disease Control and Prevention, 2006.
7.7. Alzheimer disease Alzheimer disease 65,96565,965 2.82.8
8.8. Influenza & pneumoniaInfluenza & pneumonia 59,66459,664 2.52.5
9. 9. NephritisNephritis 42,48042,480 1.81.8
10.10. SepticemiaSepticemia 33,37333,373 1.4 1.4
Change in the US Death Rates* by Cause, Change in the US Death Rates* by Cause, 1950 & 20041950 & 2004
Rate Per 100,000
1950
2004
* Age-adjusted to 2000 US standard population.Sources: 1950 Mortality Data - CDC/NCHS, NVSS, Mortality Revised.2004 Mortality Data: US Mortality Public Use Data Tape, 2004, NCHS, Centers for Disease Control and Prevention, 2006
HeartDiseases
CerebrovascularDiseases
Pneumonia/Influenza
Cancer
11/3/2008
4
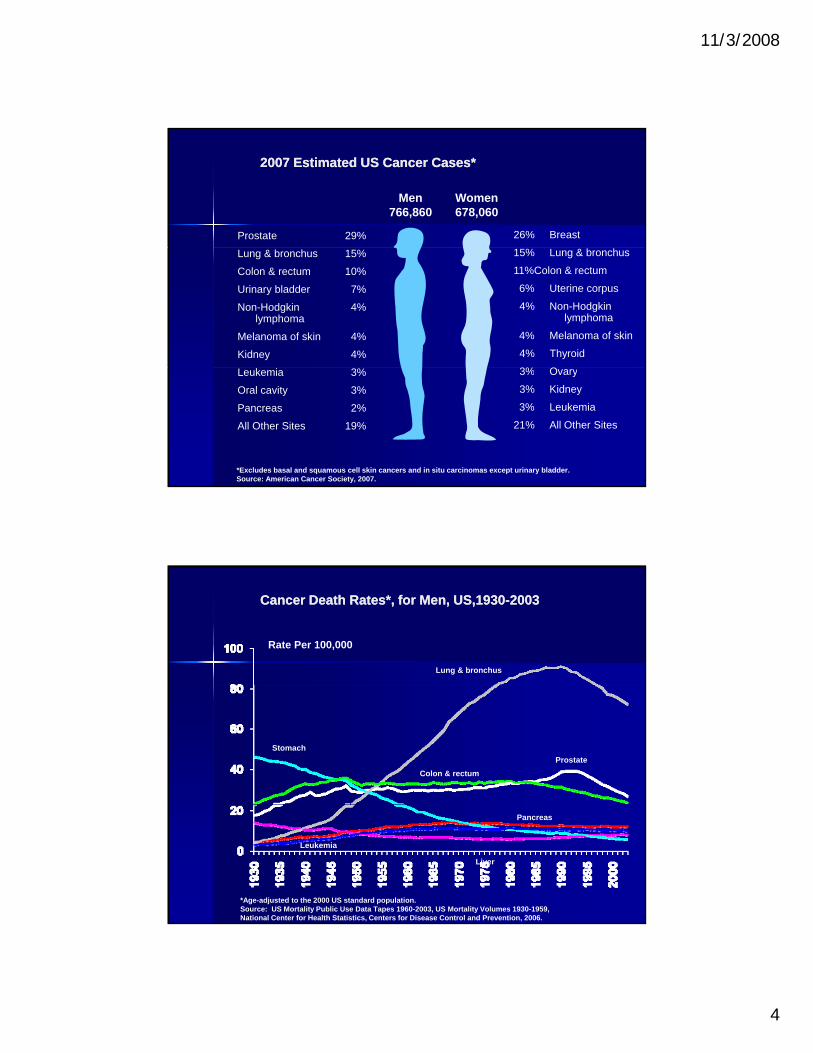
2007 Estimated US Cancer Cases*2007 Estimated US Cancer Cases*
Men766,860
Women678,060
26% BreastProstate 29%
15% Lung & bronchus
11%Colon & rectum
6% Uterine corpus
4% Non-Hodgkinlymphoma
4% Melanoma of skin
4% Thyroid
3% O
Lung & bronchus 15%
Colon & rectum 10%
Urinary bladder 7%
Non-Hodgkin 4% lymphoma
Melanoma of skin 4%
Kidney 4%
*Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder.Source: American Cancer Society, 2007.
3% Ovary
3% Kidney
3% Leukemia
21% All Other Sites
Leukemia 3%
Oral cavity 3%
Pancreas 2%
All Other Sites 19%
Cancer Death Rates*, for Men, US,1930Cancer Death Rates*, for Men, US,1930--20032003
Lung & bronchus
Rate Per 100,000
Colon & rectum
Stomach
Prostate
*Age-adjusted to the 2000 US standard population.Source: US Mortality Public Use Data Tapes 1960-2003, US Mortality Volumes 1930-1959,National Center for Health Statistics, Centers for Disease Control and Prevention, 2006.
Pancreas
Liver
Leukemia

11/3/2008
5
Cancer Death Rates*, for Women, US,1930Cancer Death Rates*, for Women, US,1930--20032003
Rate Per 100,000
Lung & bronchus
UterusBreast
*Age-adjusted to the 2000 US standard population.Source: US Mortality Public Use Data Tapes 1960-2003, US Mortality Volumes 1930-1959,National Center for Health Statistics, Centers for Disease Control and Prevention, 2006.
Colon & rectumStomach
Ovary
Pancreas
Lung Cancer in KentuckyLung Cancer in Kentucky
Kentucky has theKentucky has the 3500Kentucky has the Kentucky has the highest risk of dying highest risk of dying from ANY cancerfrom ANY cancer–– KY: 227 / 100,000KY: 227 / 100,000–– US: 199US: 199
Kentuckians dying, from Kentuckians dying, from cancer in 2005: 9 560cancer in 2005: 9 560
1500
2000
2500
3000
cancer in 2005: 9,560cancer in 2005: 9,560
Kentucky has the highest Kentucky has the highest mortality rate for LUNG mortality rate for LUNG cancercancer
0
500
1000
BrainBreast
Colon
Leukemia
LiverLung
Lymphoma O
vary
Pancreas
Prostate
11/3/2008
6
11/3/2008
7
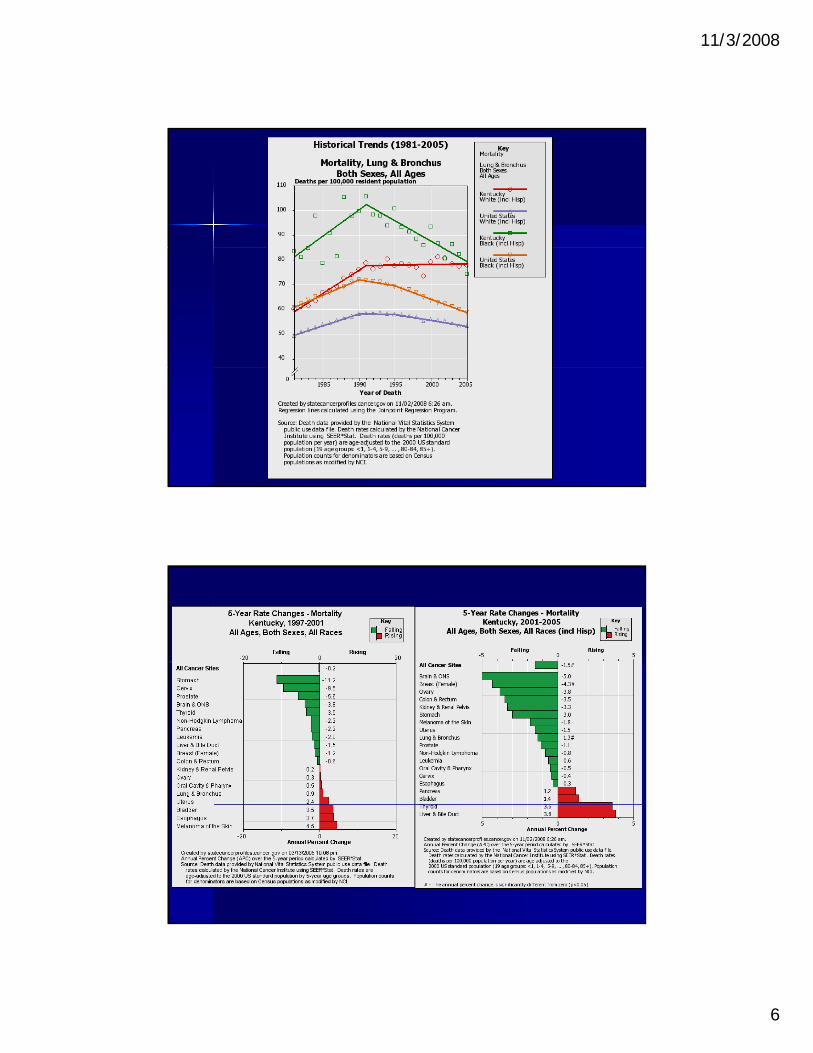
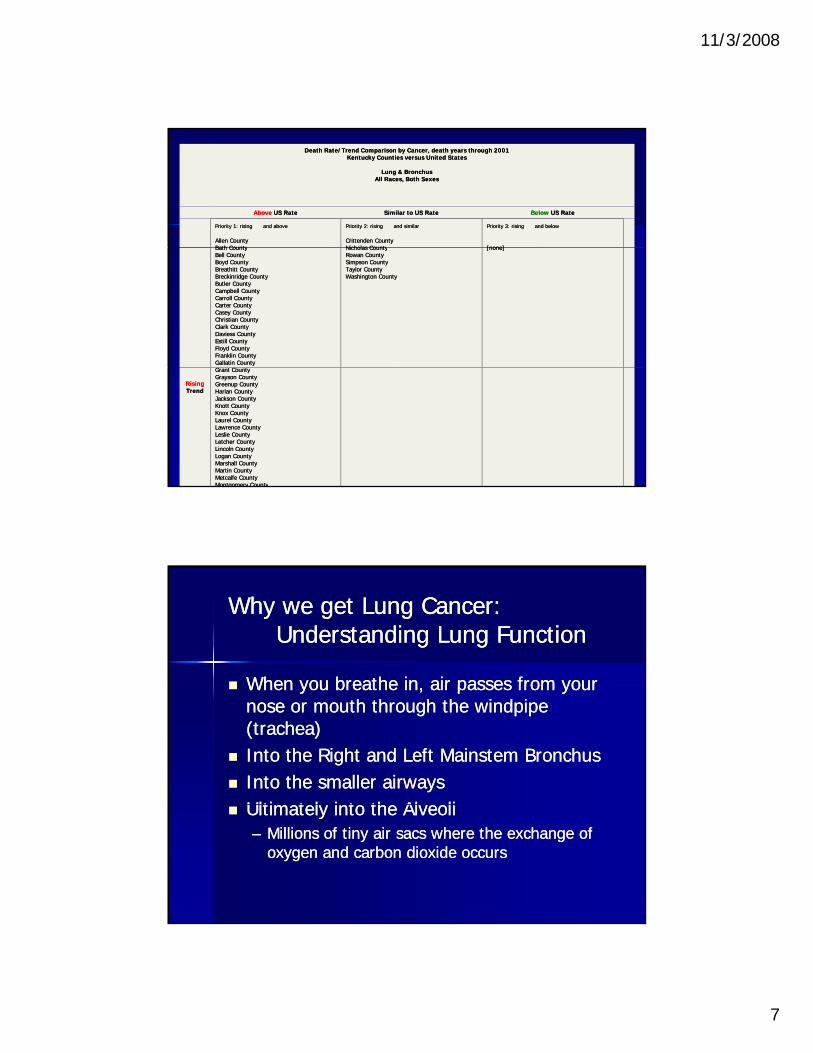
Death Rate/Trend Comparison by Cancer, death years through 2001Death Rate/Trend Comparison by Cancer, death years through 2001Kentucky Counties versus United StatesKentucky Counties versus United States
Lung & BronchusLung & BronchusAll Races, Both SexesAll Races, Both Sexes
AboveAbove US RateUS Rate Similar to US RateSimilar to US Rate BelowBelow US RateUS Rate
Priority 1: rising Priority 1: rising and above and above
Allen CountyAllen CountyBath CountyBath County
Priority 2: rising Priority 2: rising and similar and similar
Crittenden CountyCrittenden CountyNicholas CountyNicholas County
Priority 3: rising Priority 3: rising and below and below
[none][none]Bath CountyBath CountyBell CountyBell CountyBoyd CountyBoyd CountyBreathitt CountyBreathitt CountyBreckinridge CountyBreckinridge CountyButler CountyButler CountyCampbell CountyCampbell CountyCarroll CountyCarroll CountyCarter CountyCarter CountyCasey CountyCasey CountyChristian CountyChristian CountyClark CountyClark CountyDaviess CountyDaviess CountyEstill CountyEstill CountyFloyd CountyFloyd CountyFranklin CountyFranklin CountyGallatin CountyGallatin County
Nicholas CountyNicholas CountyRowan CountyRowan CountySimpson CountySimpson CountyTaylor CountyTaylor CountyWashington CountyWashington County
[none][none]
RisingRisingTrendTrend
Grant CountyGrant CountyGrayson CountyGrayson CountyGreenup CountyGreenup CountyHarlan CountyHarlan CountyJackson CountyJackson CountyKnott CountyKnott CountyKnox CountyKnox CountyLaurel CountyLaurel CountyLawrence CountyLawrence CountyLeslie CountyLeslie CountyLetcher CountyLetcher CountyLincoln CountyLincoln CountyLogan CountyLogan CountyMarshall CountyMarshall CountyMartin CountyMartin CountyMetcalfe CountyMetcalfe CountyMontgomery CountyMontgomery County
Why we get Lung Cancer:Why we get Lung Cancer:Understanding Lung FunctionUnderstanding Lung Function
When you breathe in air passes from yourWhen you breathe in air passes from your When you breathe in, air passes from your When you breathe in, air passes from your nose or mouth through the windpipe nose or mouth through the windpipe (trachea)(trachea)
Into the Right and Left Mainstem BronchusInto the Right and Left Mainstem Bronchus Into the smaller airwaysInto the smaller airways
Ultimatel into the Al eoliUltimatel into the Al eoli Ultimately into the AlveoliUltimately into the Alveoli–– Millions of tiny air sacs where the exchange of Millions of tiny air sacs where the exchange of
oxygen and carbon dioxide occursoxygen and carbon dioxide occurs

11/3/2008
8
The lungsThe lungs
Lung Cancer:Lung Cancer:What Causes It?What Causes It?
S kiS ki SmokingSmoking
Radiation ExposureRadiation Exposure
Environmental/ Occupational Environmental/ Occupational ExposureExposure–– AsbestosAsbestos
–– RadonRadon
–– Passive smokePassive smoke
11/3/2008
9
Secondhand SmokeSecondhand Smoke-- environmental tobacco smokeenvironmental tobacco smoke ((ETSETS))
Smoke from the burning end of a cigarette, cigar, Smoke from the burning end of a cigarette, cigar, g g , g ,g g , g ,or pipe, and smoke exhaled by the smoker. or pipe, and smoke exhaled by the smoker.
contains at least 60 contains at least 60 carcinogenscarcinogens–– (substances that cause (substances that cause cancercancer).).
The known health effects of exposure to secondhand smokeThe known health effects of exposure to secondhand smoke–– lunglung cancer, cancer, –– nasalnasal sinus cancer, sinus cancer, –– respiratory tractrespiratory tract infectionsinfections,,respiratory tractrespiratory tract infectionsinfections, , –– heart disease. heart disease.
Separating smokers and nonsmokers within the Separating smokers and nonsmokers within the same air space may reduce, but does not same air space may reduce, but does not eliminate, nonsmokers’ exposure to secondhand eliminate, nonsmokers’ exposure to secondhand smoke. smoke.
Lung Cancer: Lung Cancer: Smoking FactsSmoking Facts
Tobacco use is the leading cause of lung Tobacco use is the leading cause of lung g gg gcancercancer
87% of lung cancers are related to smoking87% of lung cancers are related to smoking Risk related to:Risk related to:
–– amount smoked amount smoked (pack years = # cigs/day x # yrs)(pack years = # cigs/day x # yrs)(p y g y y )(p y g y y )
–– age of smoking onsetage of smoking onset–– product smoked (tar/nicotine content, filters)product smoked (tar/nicotine content, filters)–– depth of inhalationdepth of inhalation–– gendergender
11/3/2008
10
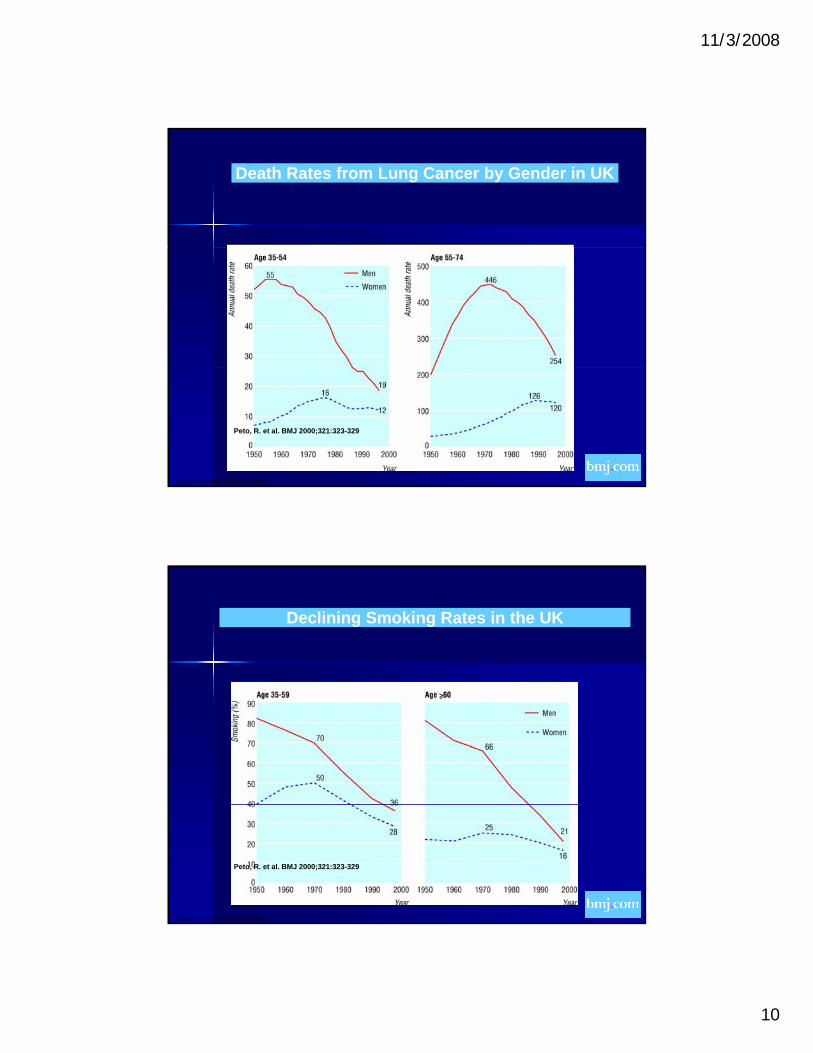
Death Rates from Lung Cancer by Gender in UK
Copyright ©2000 BMJ Publishing Group Ltd.
Peto, R. et al. BMJ 2000;321:323-329
Declining Smoking Rates in the UK
Copyright ©2000 BMJ Publishing Group Ltd.
Peto, R. et al. BMJ 2000;321:323-329
11/3/2008
11
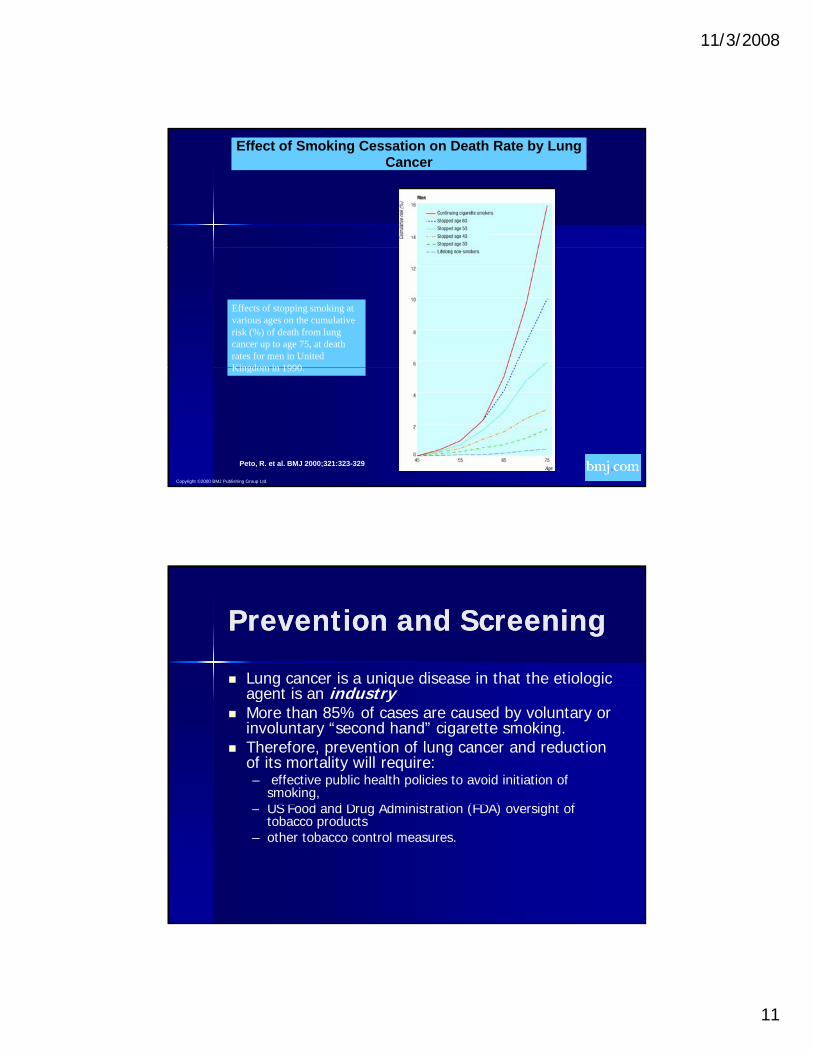
Effect of Smoking Cessation on Death Rate by Lung Cancer
Effects of stopping smoking at various ages on the cumulative risk (%) of death from lung cancer up to age 75, at death rates for men in United Kingdom in 1990
Copyright ©2000 BMJ Publishing Group Ltd.
Peto, R. et al. BMJ 2000;321:323-329
Kingdom in 1990.
Prevention and ScreeningPrevention and Screening
Lung cancer is a unique disease in that the etiologic g q gagent is an industry
More than 85% of cases are caused by voluntary or involuntary “second hand” cigarette smoking.
Therefore, prevention of lung cancer and reduction of its mortality will require:– effective public health policies to avoid initiation of
smoking, US F d d D Ad i i t ti (FDA) i ht f– US Food and Drug Administration (FDA) oversight of tobacco products
– other tobacco control measures.

11/3/2008
12
ScreeningScreening
What is screening?What is screening? What is screening?What is screening? ScreeningScreening is looking for is looking for cancercancer before before
a person has any a person has any symptomssymptoms. This can . This can help find cancer at an early help find cancer at an early stagestage. . When When abnormalabnormal tissuetissue or cancer is or cancer is found early, it may be easier to treat. found early, it may be easier to treat. By the time symptoms appear, cancer By the time symptoms appear, cancer may have begun to spread.may have begun to spread.
Why Not Screen?Why Not Screen?
Early data from Mayo Clinic Johns HopkinsEarly data from Mayo Clinic Johns Hopkins Early data from Mayo Clinic, Johns Hopkins, Early data from Mayo Clinic, Johns Hopkins, Memorial SloneMemorial Slone--Kettering indicate that there Kettering indicate that there is no reduction of the risk of dying from is no reduction of the risk of dying from lung cancer by screening with Chest Xlung cancer by screening with Chest X--ray ray or sputum.or sputum.
Concern over these trialsConcern over these trials Concern over these trials Concern over these trials –– Insensitive testsInsensitive tests–– Improper protocol for evaluating a nodule in the Improper protocol for evaluating a nodule in the
lunglung
11/3/2008
13
The Debate Rages on…The Debate Rages on…
For over 20 years the arguments haveFor over 20 years the arguments have For over 20 years, the arguments have For over 20 years, the arguments have been pursued been pursued
Intuitive advantages of screeningIntuitive advantages of screening Lack of proven benefit and concern for Lack of proven benefit and concern for
harmharm
New, more sensitive and specific tests New, more sensitive and specific tests may be availablemay be available
Complex Impact of Complex Impact of ScreeningScreening Optimal imaging device?Optimal imaging device? Optimal imaging device?Optimal imaging device?
Who will assume burden of cost?Who will assume burden of cost?
When will evidence be provided toWhen will evidence be provided to When will evidence be provided to When will evidence be provided to validate benefit?validate benefit?
11/3/2008
14
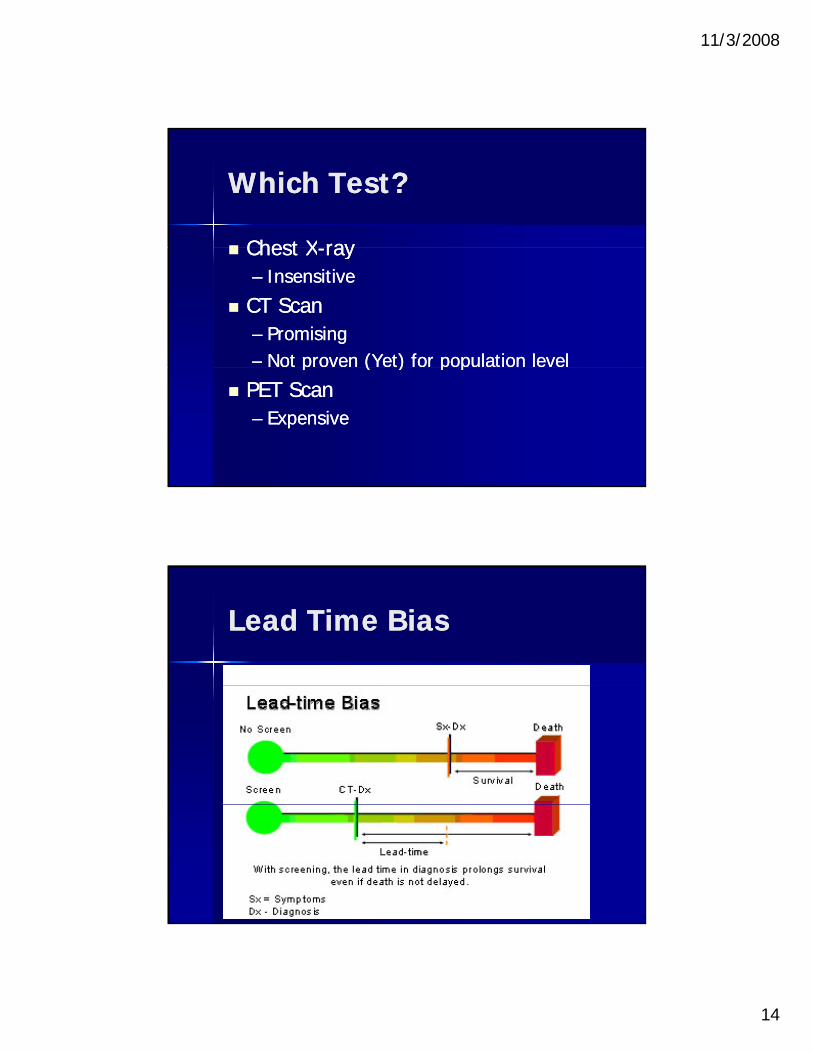
Which Test?Which Test?
Chest XChest X--rayray Chest XChest X--rayray–– InsensitiveInsensitive
CT ScanCT Scan–– PromisingPromising–– Not proven (Yet) for population levelNot proven (Yet) for population levelp ( ) p pp ( ) p p
PET ScanPET Scan–– ExpensiveExpensive
Lead Time BiasLead Time Bias

11/3/2008
15
Length BiasLength Bias
OverdiagnosisOverdiagnosis BiasBias

11/3/2008
16
Mortality not FatalityMortality not Fatality
MortalityMortality –– Mortality Mortality –– population based measure of the impact population based measure of the impact
of lung cancerof lung cancer–– The gold standardThe gold standard–– Includes all patients screenedIncludes all patients screened
Case Fatality RateCase Fatality Rate Case Fatality RateCase Fatality Rate–– Number of deaths among those with lung Number of deaths among those with lung
cancercancer–– Cannot be used since it does not account Cannot be used since it does not account
for the biases listedfor the biases listed
National Cancer InstituteNational Cancer Institute--National Lung Screening TrialNational Lung Screening Trial
Launched in 2002, NLST is comparing two ways of detecting Launched in 2002, NLST is comparing two ways of detecting lllung cancer: lung cancer: –– spiral computed tomography (CT) and standard chest Xspiral computed tomography (CT) and standard chest X--ray. ray.
Both Both chest Xchest X--rays and spiral CT scansrays and spiral CT scans have been used to find have been used to find lung cancer early. So far, neither chest Xlung cancer early. So far, neither chest X--rays nor spiral CT scans rays nor spiral CT scans have been shown to reduce a person's chance of dying from lung have been shown to reduce a person's chance of dying from lung cancer. This study will aim to show if either test is better at cancer. This study will aim to show if either test is better at reducing deaths from this disease. reducing deaths from this disease.
50,000 current or former smokers enrolled50,000 current or former smokers enrolled
The trial is slated to collect and analyze data for eight years, The trial is slated to collect and analyze data for eight years, and will examine the risks and benefits of spiral CT scans and will examine the risks and benefits of spiral CT scans compared to chest Xcompared to chest X--rays.rays.

11/3/2008
17
11/3/2008
18
What are the symptoms of What are the symptoms of Lung Cancer?Lung Cancer? a continuinga continuing coughcough or change in aor change in a a continuing a continuing coughcough or change in a or change in a
longlong--standing cough standing cough a chest a chest infectioninfection that does not get that does not get
better better increasing increasing breathlessnesbreathlessnes coughing upcoughing up bloodblood--stained phlegmstained phlegmcoughing up coughing up bloodblood stained phlegm stained phlegm
(sputum) (sputum) a dull ache or a sharp a dull ache or a sharp pain pain when you when you
cough or take a deep breath cough or take a deep breath loss of appetite loss of appetite and loss of weight.and loss of weight.
Lung Cancer: DiagnosisLung Cancer: Diagnosis
History and Physical examHistory and Physical exam History and Physical examHistory and Physical exam Diagnostic testsDiagnostic tests
–– Chest xChest x--rayray–– Biopsy (bronchoscopy, needle biopsy, surgery)Biopsy (bronchoscopy, needle biopsy, surgery)
Staging testsStaging tests–– CT chest/abdomenCT chest/abdomen–– Bone scanBone scan–– Bone marrow aspirationBone marrow aspiration–– PET scanPET scan

11/3/2008
19
Lung Cancer: Cell TypesLung Cancer: Cell Types
Non Small Cell Lung Cancer Non Small Cell Lung Cancer (NSCLC)(NSCLC)
Small Cell Lung Cancer Small Cell Lung Cancer (SCLC(SCLC))
Non Small Cell Lung Non Small Cell Lung Cancer (NSCLC)Cancer (NSCLC)
80% of all lung cancers80% of all lung cancers
Better survival rates when found inBetter survival rates when found in Better survival rates when found in Better survival rates when found in early stagesearly stages

11/3/2008
20
NSCLC: Histologic Cell NSCLC: Histologic Cell TypesTypes
Adenocarcinoma Adenocarcinoma
Squamous Cell CarcinomaSquamous Cell Carcinoma
Large Cell CarcinomaLarge Cell Carcinoma
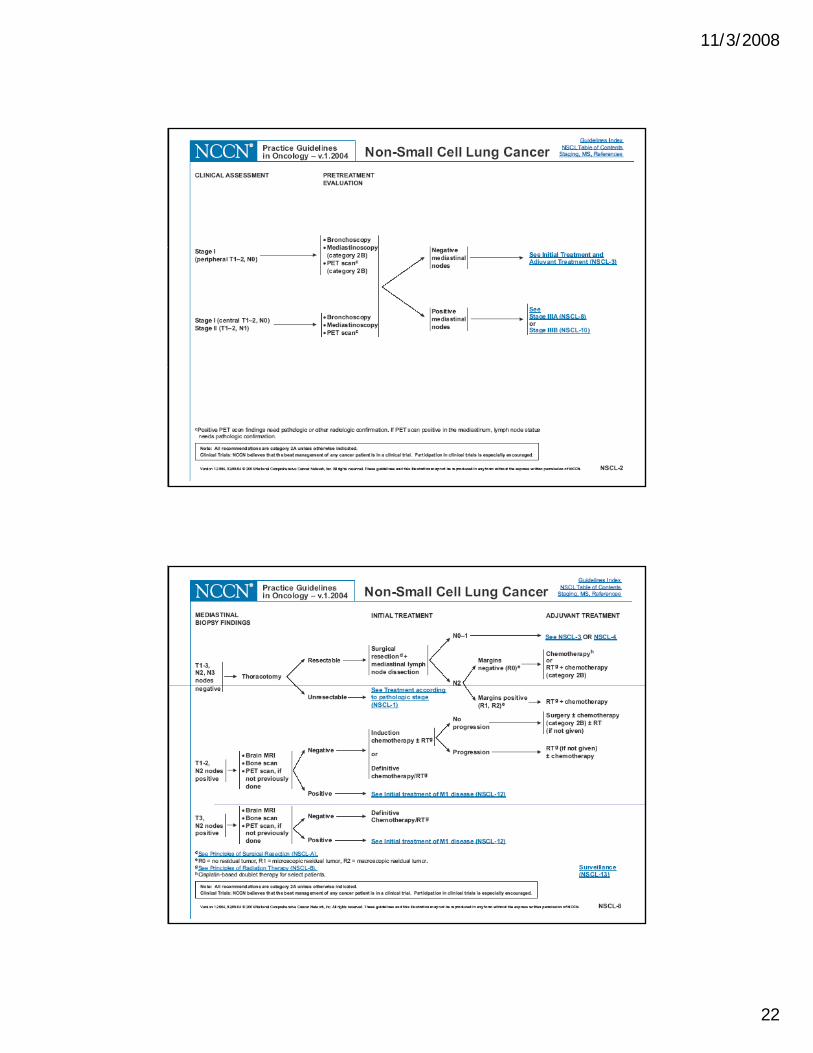
www.nccn.org
11/3/2008
21
11/3/2008
22
11/3/2008
23
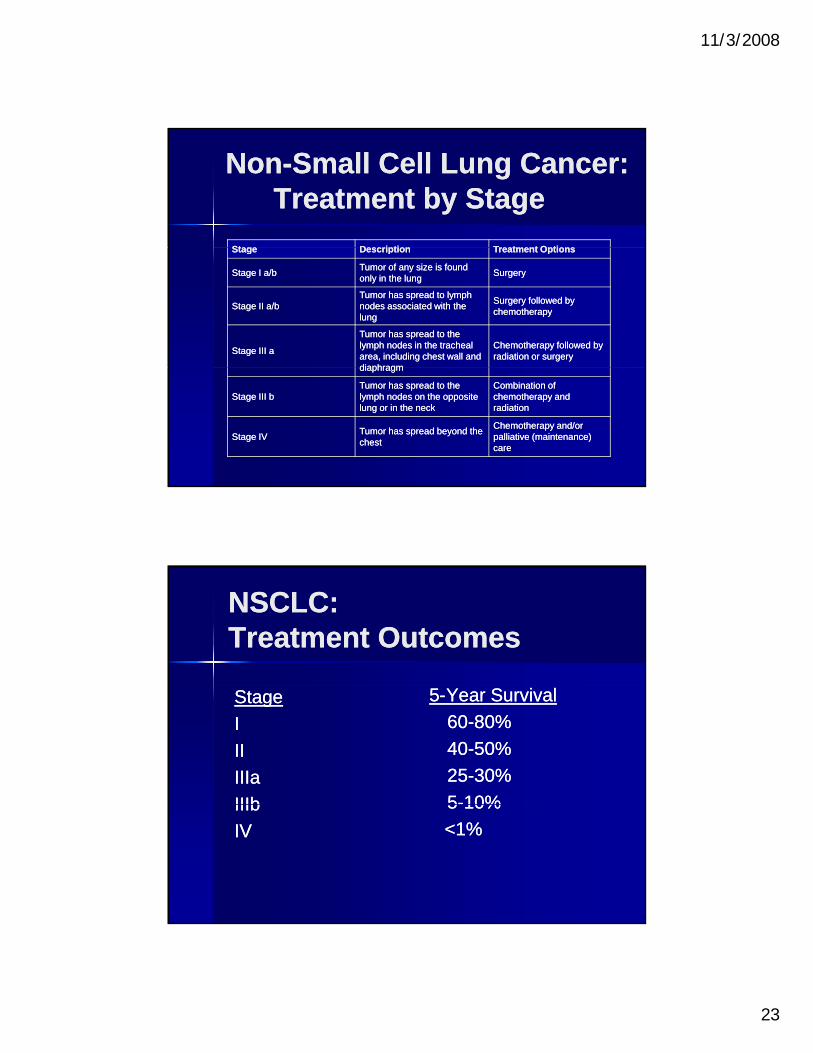
NonNon--Small Cell Lung Cancer: Small Cell Lung Cancer: Treatment by StageTreatment by Stage
StageStage DescriptionDescription Treatment OptionsTreatment OptionsStageStage DescriptionDescription Treatment OptionsTreatment Options
Stage I a/bStage I a/bTumor of any size is found Tumor of any size is found only in the lung only in the lung
SurgerySurgery
Stage II a/bStage II a/bTumor has spread to lymph Tumor has spread to lymph nodes associated with the nodes associated with the lunglung
Surgery followed by Surgery followed by chemotherapychemotherapy
Stage III aStage III a
Tumor has spread to the Tumor has spread to the lymph nodes in the tracheal lymph nodes in the tracheal area, including chest wall and area, including chest wall and diaphragmdiaphragm
Chemotherapy followed by Chemotherapy followed by radiation or surgeryradiation or surgery
diaphragmdiaphragm
Stage III bStage III bTumor has spread to the Tumor has spread to the lymph nodes on the opposite lymph nodes on the opposite lung or in the necklung or in the neck
Combination of Combination of chemotherapy and chemotherapy and radiationradiation
Stage IVStage IVTumor has spread beyond the Tumor has spread beyond the chestchest
Chemotherapy and/or Chemotherapy and/or palliative (maintenance) palliative (maintenance) carecare
NSCLC: NSCLC: Treatment OutcomesTreatment Outcomes
StageStage
II
IIII
IIIaIIIa
IIIbIIIb
55--Year SurvivalYear Survival
6060--80%80%
4040--50%50%
2525--30%30%
55--10%10%IIIbIIIb
IVIV
55 10%10%
<1%<1%
11/3/2008
24
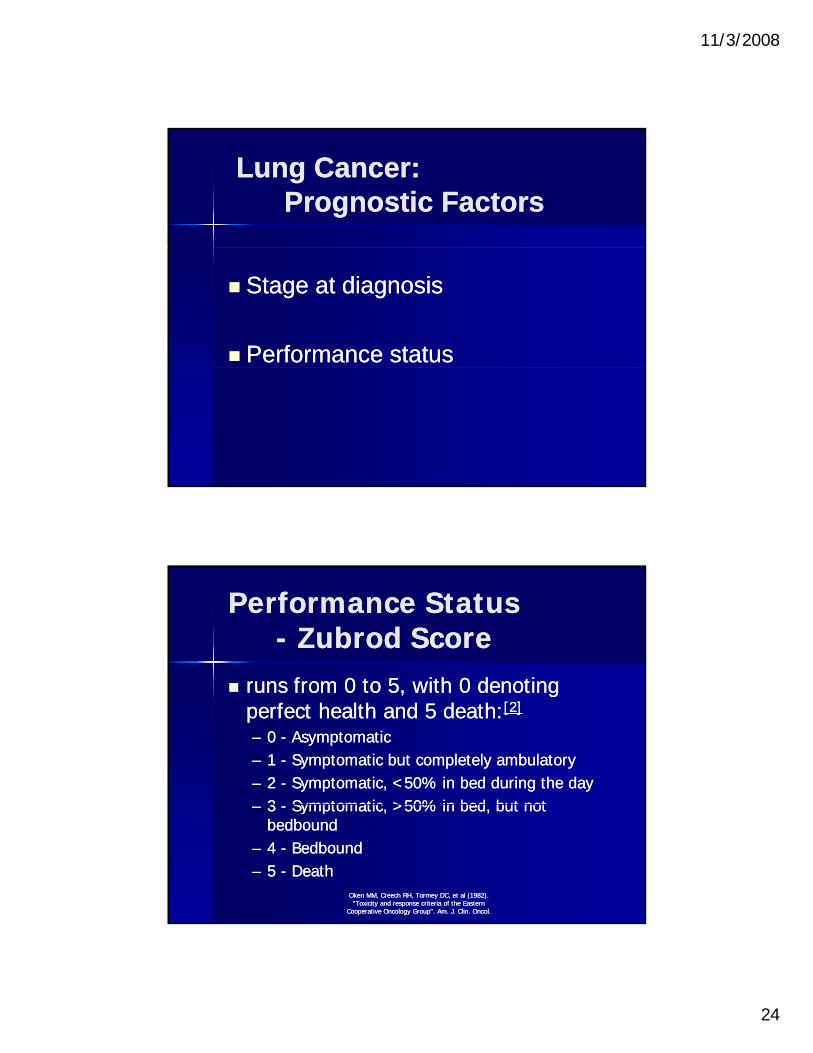
Lung Cancer: Lung Cancer: Prognostic FactorsPrognostic Factors
Stage at diagnosisStage at diagnosis
Performance statusPerformance status
Performance StatusPerformance Status-- ZubrodZubrod ScoreScore
runs from 0 to 5 with 0 denotingruns from 0 to 5 with 0 denoting runs from 0 to 5, with 0 denoting runs from 0 to 5, with 0 denoting perfect health and 5 death:perfect health and 5 death:[2][2]
–– 0 0 -- AsymptomaticAsymptomatic–– 1 1 -- Symptomatic but completely ambulatorySymptomatic but completely ambulatory–– 2 2 -- Symptomatic, <50% in bed during the daySymptomatic, <50% in bed during the day
33 Symptomatic >50% in bed but notSymptomatic >50% in bed but not–– 3 3 -- Symptomatic, >50% in bed, but not Symptomatic, >50% in bed, but not bedboundbedbound
–– 4 4 -- BedboundBedbound–– 5 5 -- Death Death
OkenOken MM, Creech RH, MM, Creech RH, TormeyTormey DC, et al (1982). DC, et al (1982). "Toxicity and response criteria of the Eastern "Toxicity and response criteria of the Eastern
Cooperative Oncology Group". Am. J. Cooperative Oncology Group". Am. J. ClinClin. . OncolOncol..
11/3/2008
25
WorkWork--Up for Suspected Up for Suspected Lung CancerLung Cancer Baseline data in most patientsBaseline data in most patients Baseline data in most patientsBaseline data in most patients
–– CXRCXR–– CT of Chest (including Liver/Adrenals)CT of Chest (including Liver/Adrenals)–– CBCCBC–– LFT, Metabolic evaluationLFT, Metabolic evaluation
–– PFT’sPFT’s Useful in any treatment due to pulmonary Useful in any treatment due to pulmonary
limitations of treatment or toxicitylimitations of treatment or toxicity
Further EvaluationFurther Evaluation
PET/CT Fusion StudyPET/CT Fusion Study PET/CT Fusion StudyPET/CT Fusion Study–– More sensitive and helpful in localizing nodes More sensitive and helpful in localizing nodes
or other suspect metastasesor other suspect metastases Differential Perfusion ScanDifferential Perfusion Scan
–– In patients with poor lung functionIn patients with poor lung function Measure of MVO2 may be helpfulMeasure of MVO2 may be helpful Measure of MVO2 may be helpfulMeasure of MVO2 may be helpful
–– Assess Assess dyspneadyspnea out of proportion to lung out of proportion to lung diseasedisease
–– More specific indicator of More specific indicator of resectabilityresectability in in smaller patientssmaller patients
11/3/2008
26
Further EvaluationFurther EvaluationCardiacCardiac
EKGEKG Stress evaluationStress evaluation
–– Usually Usually DobutamineDobutamine Stress EchoStress Echo
Ca diac cathete i ation if indicatedCa diac cathete i ation if indicated Cardiac catheterization, if indicatedCardiac catheterization, if indicated
NSCLC: ResearchNSCLC: Research
Chemotherapy/BiotherapyChemotherapy/Biotherapy Chemotherapy/BiotherapyChemotherapy/Biotherapy–– New agentsNew agents
–– Novel therapiesNovel therapies
RadiationRadiation–– Dosing and schedulingDosing and scheduling
–– New techniquesNew techniquesNew techniquesNew techniques
MultimodalityMultimodality–– Early stage and locally advanced diseaseEarly stage and locally advanced disease
–– Refining therapiesRefining therapies
11/3/2008
27
Lung Cancer: Lung Cancer: ConclusionsConclusions
S ki ti i ti l f tiS ki ti i ti l f ti Smoking cessation is essential for prevention Smoking cessation is essential for prevention of lung cancer.of lung cancer.
New screening tools offer promise for New screening tools offer promise for detection of early lung tumors.detection of early lung tumors.
Clinical trials are testing promising new Clinical trials are testing promising new treatments.treatments.
New treatments offer improved efficacy and New treatments offer improved efficacy and fewer side effects.fewer side effects.
Treatment can palliate symptoms and Treatment can palliate symptoms and improve quality of life.improve quality of life.
Vincent van GoghSkull of a skeleton with burning cigarette1885

11/3/2008
28
Oregon Coast, September 2008