lung cancer
DESCRIPTION
lungTRANSCRIPT
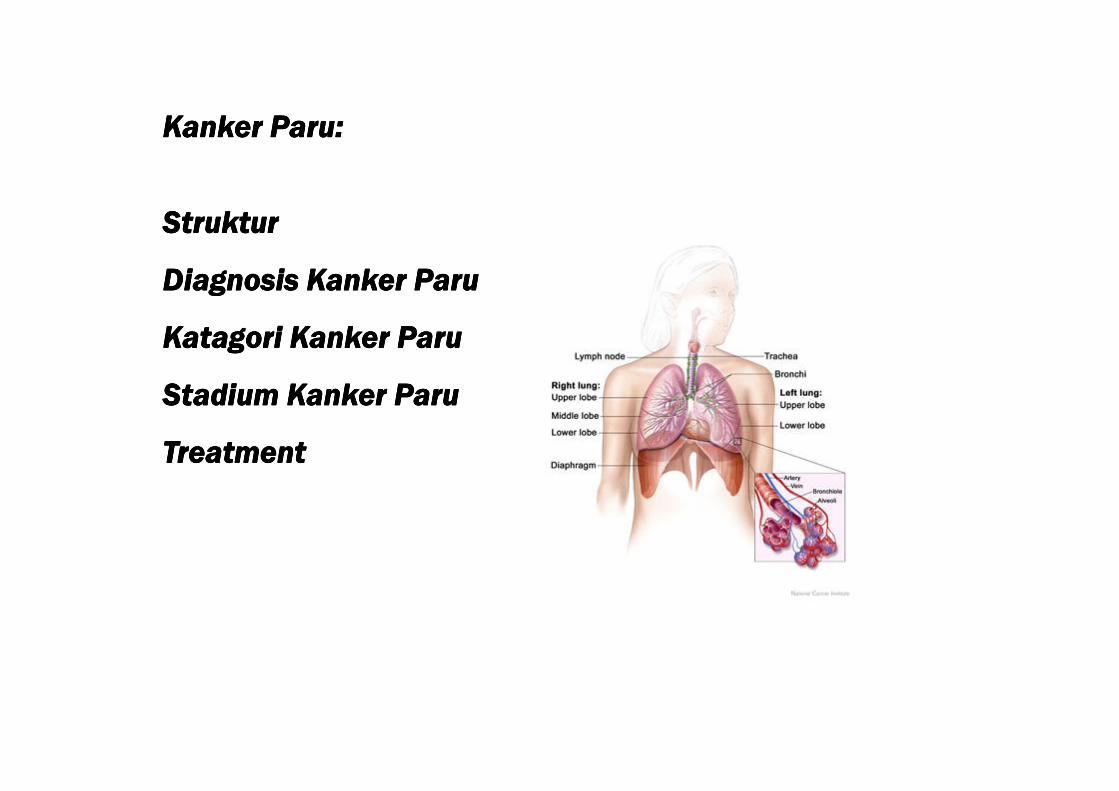
Kanker Paru:Kanker Paru:Kanker Paru:Kanker Paru:
StrukturStrukturStrukturStruktur
Diagnosis Kanker ParuDiagnosis Kanker ParuDiagnosis Kanker ParuDiagnosis Kanker Paru
Katagori Kanker ParuKatagori Kanker ParuKatagori Kanker ParuKatagori Kanker Paru
Stadium Kanker ParuStadium Kanker ParuStadium Kanker ParuStadium Kanker ParuStadium Kanker ParuStadium Kanker ParuStadium Kanker ParuStadium Kanker Paru
TreatmentTreatmentTreatmentTreatment

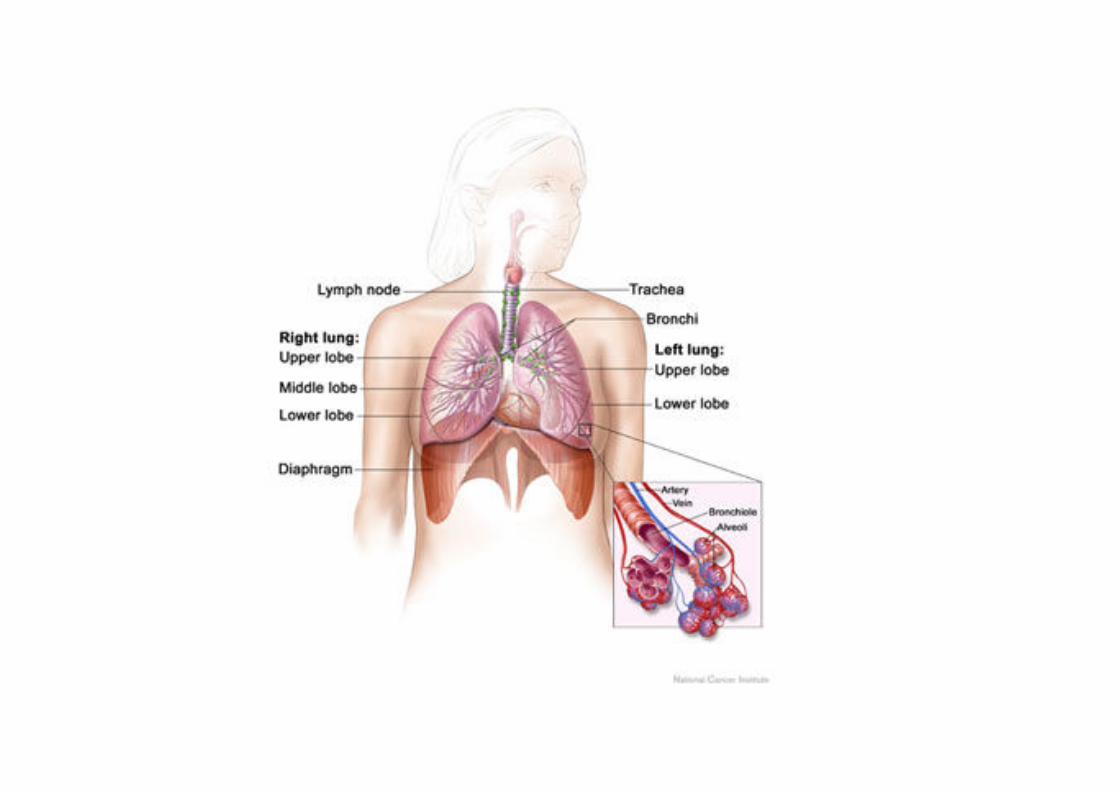
Struktur Paru-paru
The lungs are a pair of cone-
shaped breathing organs in the
chest. Each lung has sections
called lobes. The left lung has two
lobes. The right lung is slightly
larger and has three lobes. Two
tubes called bronchi lead from the
trachea (windpipe) to the right and
left lungs. The bronchi are
sometimes also involved in lung
cancer. Tiny air sacs called alveoli
and small tubes called bronchioles and small tubes called bronchioles
make up the inside of the lungs.
A thin membrane called the pleura
covers the outside of each lung and
lines the inside wall of the chest
cavity. This creates a sac called the
pleural cavity. The pleural cavity
normally contains a small amount of
fluid that helps the lungs move
smoothly in the chest when you
breathe.
Lung cancer
• Lung cancer is a major cause of morbidity and mortality that has reached epidemic proportions in many industrialized countries and is the most frequently fatal malignancy in the world.
• Although the overall 5-year survival rate for lung cancer is low, it may be curable with surgical resection if detected in the early stages, and many patients experience significant survival and symptom-relief benefits from systemic chemotherapy or radiation.patients experience significant survival and symptom-relief benefits from systemic chemotherapy or radiation.
• Patients with lung cancer may undergo surgery, chemotherapy, radiation, or multimodality therapy, depending on the histologic type of the tumor, its size and location, and the presence of metastases at diagnosis.
Risk factors for lung cancer include the following:
�Smoking cigarettes or cigars, now or in the past (83%)
�Being exposed to second-hand smoke.
�Being treated with radiation therapy to the breast or chest.
�Being exposed to PAH, asbestos (mesothelioma), radon, �Being exposed to PAH, asbestos (mesothelioma), radon,
chromium, arsenic, or tar.
�Living where there is air pollution
�Family history of cancer (The relative risk is approximately sixfold
higher for first-degree relatives of a lung cancer patient diagnosed
between the ages of 40 and 59 years)
Nutrition
• Since not all heavy smokers develop lung cancer, it is thought that nutritional factors may explain in part this variation.
• Epidemiologic studies focusing on diet and nutrition in lung cancer have shown reduced rates of lung cancer in individuals who report higher fruit and vegetable consumptionwho report higher fruit and vegetable consumption
• Recommendations to patients who are at risk owing to smoking or other factors or those who are simply interested in reducing their risk of cancer should include an increase in dietary intake of fruits and vegetables.
• The American Cancer Society estimates that cigarette smoking is responsible for about 83% of all lung cancer cases, and studies have established a dose-response relationship between the number of cigarettes smoked, the number of years an individual has smoked, the tar and nicotine content of cigarettes, and the development of lung cancer.
• Likewise, smokers with obstructive airway disease or chronic bronchitis have a three to Five fold greater risk of developing lung cancer than do smokers with normal pulmonary function.
• Cessation of smoking is associated with a gradual decrease in the risk, but a long period of time (more than 6 years) is necessary before an appreciable decline of the risk occurs.
• Antismoking campaigns, increased tobacco taxes, and smoke-free areas in many public areas and businesses, along with societal pressures have been somewhat successful in reducing the number of adult Americans who smoke.
• Passive exposure to cigarette smoke is believed to contribute to the increased risk of • Passive exposure to cigarette smoke is believed to contribute to the increased risk of lung cancer in nonsmokers living with smokers.
• Additional studies are necessary to define the role of antioxidants in lung cancer prevention.
Symptoms of Lung Cancer
Most lung cancers do not cause symptoms until cancer has spread.
The most common symptoms are:
�Persistent cough
�Coughing up blood
�Chest pain
�Hoarseness
�Sudden onset of wheezing
�Shortness of breath
�Weight loss and loss of appetite
�Recurrent respiratory infections, such as pneumonia
�Fatigue �Fatigue
Paraneoplastic syndromes occur more frequently with lung cancer than with
any other tumor.
These syndromes may be the first signs of a tumor and may prompt the
search for an underlying malignancy. Paraneoplastic syndromes that
commonly occur in association with lung cancers include cachexia,
hypercalcemia, syndrome of inappropriate secretion of antidiuretic hormone,
and Cushing’s syndrome
Screening• Chest x-rays and sputum cytology are the most commonly used screening
techniques in these older studies.
• Although several of these studies have reported that lung cancers may be detected at an earlier stage, actual mortality rates were not affected.
• Other investigations have also documented that chest x-rays are not sensitive enough to detect very small (<2 cm) lung tumors, which might account for the lack of impact of this screening technique.
• Furthermore, chest x-rays and sputum cytology may be associated with false-positive results in these high-risk individuals, leading to unnecessary and costly positive results in these high-risk individuals, leading to unnecessary and costly work-ups and anxiety.
• Low-dose spiral or helical computed tomography (CT) has detected lung tumors at sizes significantly smaller than with conventional chest x-rays (approximately 1.5 cm vs. 2 to 3 cm).
• Although evidence shows that conventional sputum cytology as an early detection tool does not lead to improvement in lung cancer outcomes
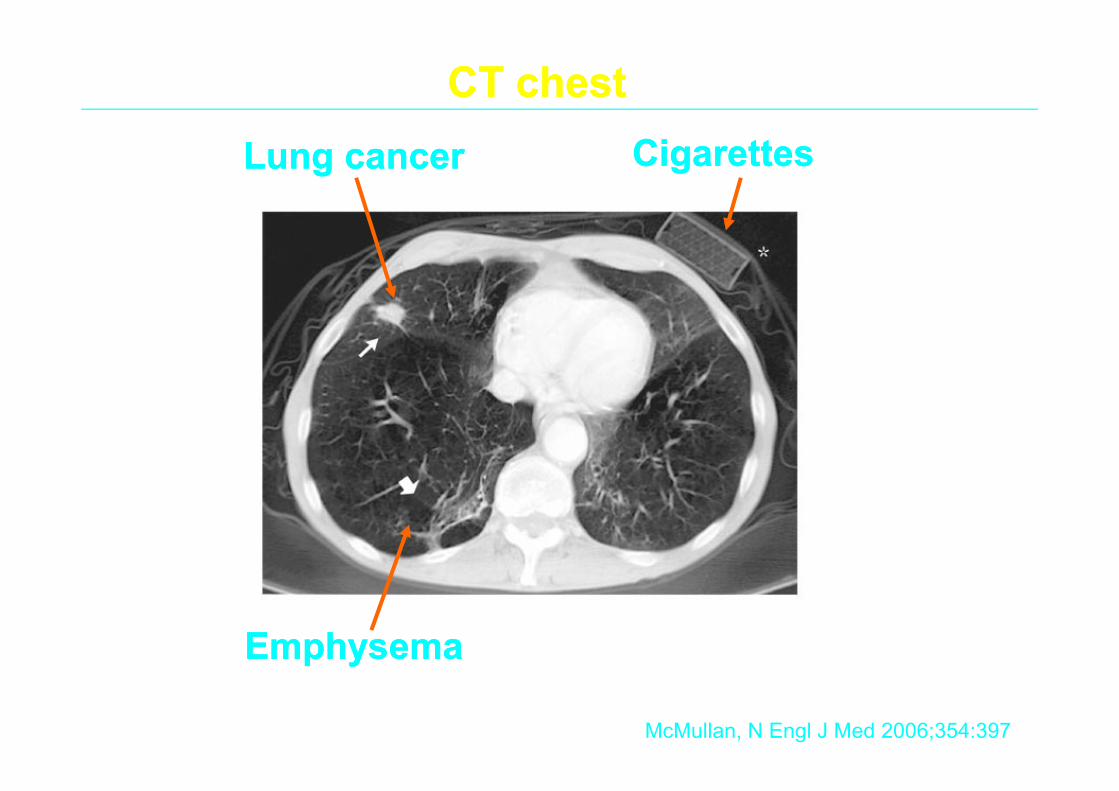
Lung cancerLung cancer
CT chestCT chest
CigarettesCigarettes
McMullan, N Engl J Med 2006;354:397
EmphysemaEmphysema
Tests for Lung Cancer
�Physical exam and history
�Thoracentesis — a sample of fluid from around the
lungs to evaluate types of cells
�Bronchoscopy — flexible camera to view the airway
and take tissue samples
�Computed tomography (CT) scan of the lungs to
identify abnormal tissue masses [CT is helpful in all identify abnormal tissue masses [CT is helpful in all
of the foregoing, as well as in evaluation of parenchymal lung
abnormalities, detection of masses only suspected on the chest
x-ray, and assessment of mediastinal and hilar lymph nodes]
�Positron emission tomography (PET) scan of the
lungs to look for cancer cells [reportedly more
accurate than CT scans in distinguishing malignant from benign
l esions, detecting mediastinal lymph node metastases, and
identifying metastatic spread]
�Bone scan to determine whether the cancer has
spread to the bones

• When there is clinical and radiologic evidence of a tumor, pathologic confirmation must be established.
• Pathologic confirmation may be accomplished by examination of sputum cytology and/or tumor biopsy by fiberoptic bronchoscopy, percutaneous needle biopsy, or open-lung biopsy.
• All patients must also have a thorough history and physical examination with emphasis on detecting signs and symptoms of the primary tumor, regional spread of the tumor, distant metastases, and paraneoplastic syndromes.
• The physical examination also aids in determining whether or not a patient may be able to withstand aggressive surgery or chemotherapy.
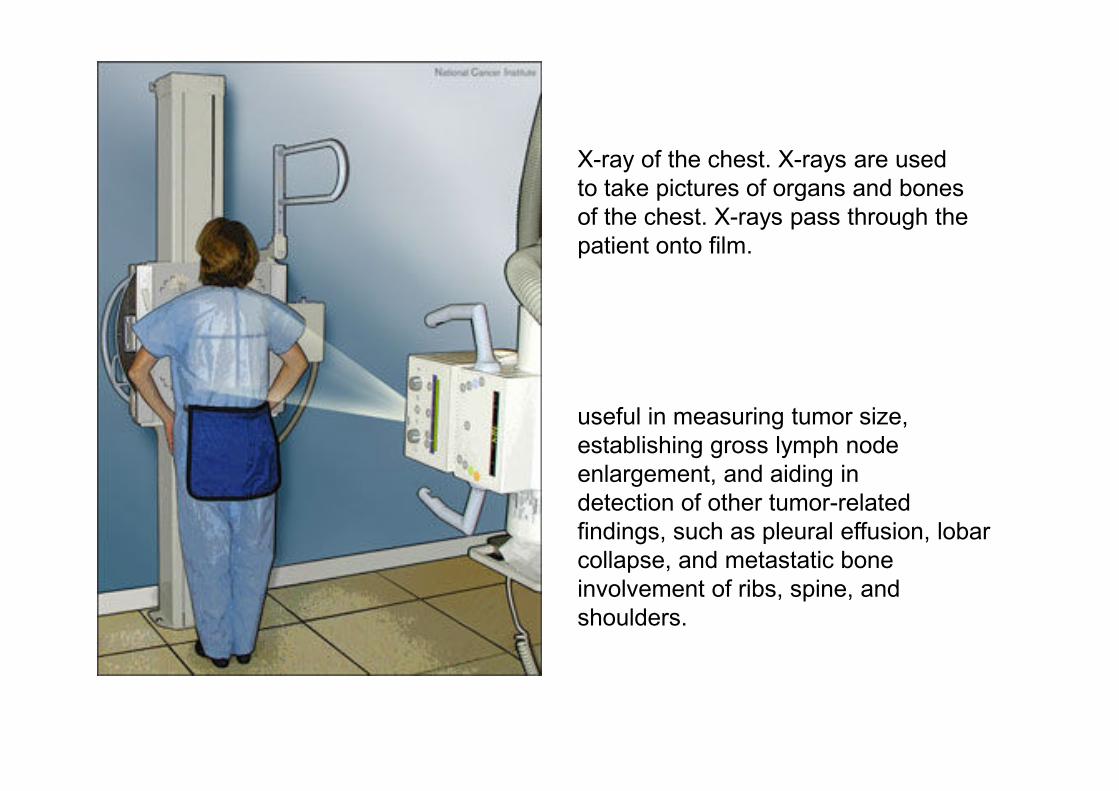
X-ray of the chest. X-rays are used
to take pictures of organs and bones
of the chest. X-rays pass through the
patient onto film.
useful in measuring tumor size,
establishing gross lymph node
enlargement, and aiding in
detection of other tumor-related
findings, such as pleural effusion, lobar
collapse, and metastatic bone
involvement of ribs, spine, and
shoulders.
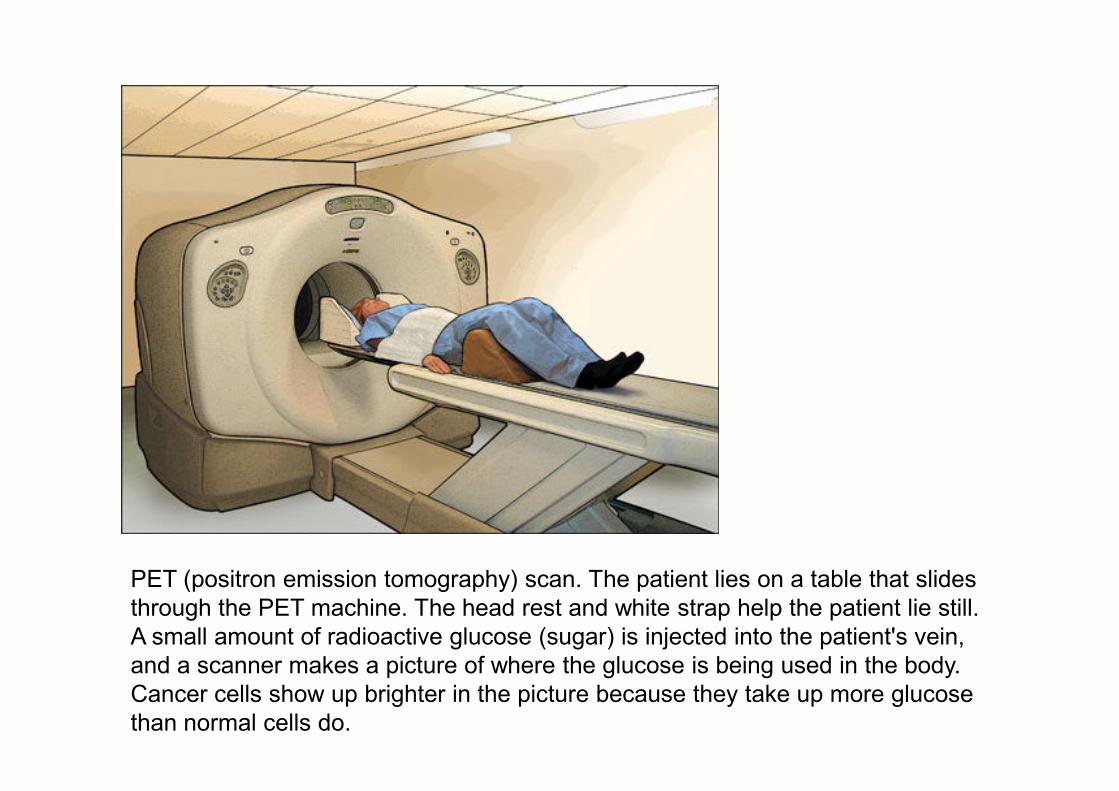
PET (positron emission tomography) scan. The patient lies on a table that slides
through the PET machine. The head rest and white strap help the patient lie still.
A small amount of radioactive glucose (sugar) is injected into the patient's vein,
and a scanner makes a picture of where the glucose is being used in the body.
Cancer cells show up brighter in the picture because they take up more glucose
than normal cells do.

Bronchoscopy. A bronchoscope is inserted
through the mouth, trachea, and major
bronchi into the lung, to look for abnormal
areas. A bronchoscope is a thin, tube-like
instrument with a light and a lens for viewing.
It may also have a cutting tool. Tissue
samples may be taken to be checked under a
microscope for signs of disease.
The prognosis (chance of recovery) and treatment
options depend on the following:
oThe stage of the cancer (the size of the tumor and
whether it is in the lung only or has spread to other
places in the body).
oThe type of lung cancer. oThe type of lung cancer.
oWhether there are symptoms such as coughing or
trouble breathing.
oThe patient’s general health.
Two main types of lung cancer: non-small cell lung cancer
(80%) and small cell lung cancer (20%).
NSCL : Slower growth rate and doubling time
Non-small cell lung cancer
�Squamous cell carcinoma : Cancer that begins in squamous
cells, which are thin, flat cells that look like fish scales.
This is also called epidermoid carcinoma.
�Large cell carcinoma: Cancer that may begin in several
types of large cells.
�Adenocarcinoma: Cancer that begins in the cells that line
the alveoli and make substances such as mucus.

• Squamous cell carcinomas (along with small cell lung cancers [SCLC]) have a much higher incidence among smokers and among males and appear to have a strong dose-response relationship to tobacco exposure.
• Adenocarcinoma is now the most common type of lung cancer in the United States, accounting for about 40% of cases. This is partly a result of the increased incidence of lung cancer in women, who tend to have more adenocarcinomas than epidermoid cancers. epidermoid cancers.
• Adenocarcinoma does not have a dose-response relationship to tobacco exposure. These tumors are usually located in the peripheral sections of the lung and are distinguished pathologically by a glandular or papillary pattern and mucin production.
• Adenocarcinoma are likely to metastasize at an early stage (often before the diagnosis of the primary tumor) and spread widely to distant sites including the contralateral lung, liver, bone, adrenal glands, kidneys, and central nervous system. As a result, adenocarcinoma has a worse prognosis than squamous cell carcinoma.

• Large cell carcinomas are anaplastic tumors that show no evidence of differentiation.
• Large cell carcinomas tumors tend to be large and bulky tumors arising in the periphery of the lung, to have a propensity to metastasize in a pattern quite similar to adenocarcinomas, and to be associated with a similar poor prognosis.
• Small cell carcinomas account for about 20% of all lung tumors. Almost all cases are associated with a history of smoking. They are distinguished by a proliferation of neoplastic cells with round to oval nuclei.
• Small cell carcinomas tend to arise in the central portion of the lung, but may also be found in the lung periphery. SCLC is a very aggressive and rapidly growing be found in the lung periphery. SCLC is a very aggressive and rapidly growing tumor with approximately 60% to 70% of patients initially presenting with disseminated disease outside of the hemithorax.
• SCLC commonly express neuroendocrine differentiation that may account for some of the paraneoplastic syndromes frequently associated with this disease.
• SCLC has a propensity to metastasize to the lymph nodes, opposite lung, liver, adrenal glands and other endocrine organs, bone, bone marrow, and central nervous system.
• Lung tumors frequently exhibit more than one histology, and it is now evident that all types of lung cancer share a common pluripotent stem cell.
• Studies of lung cancer cells have also shown that cell lines may spontaneously change phenotype, which may explain the mixed histology.
• Occasionally, patients can also have multiple lung nodules arising in different lobes or the contralateral lung. This is referred to as synchronous tumors, and the nodules may be of similar or different cell types. This usually worsens the patient’s overall prognosis.
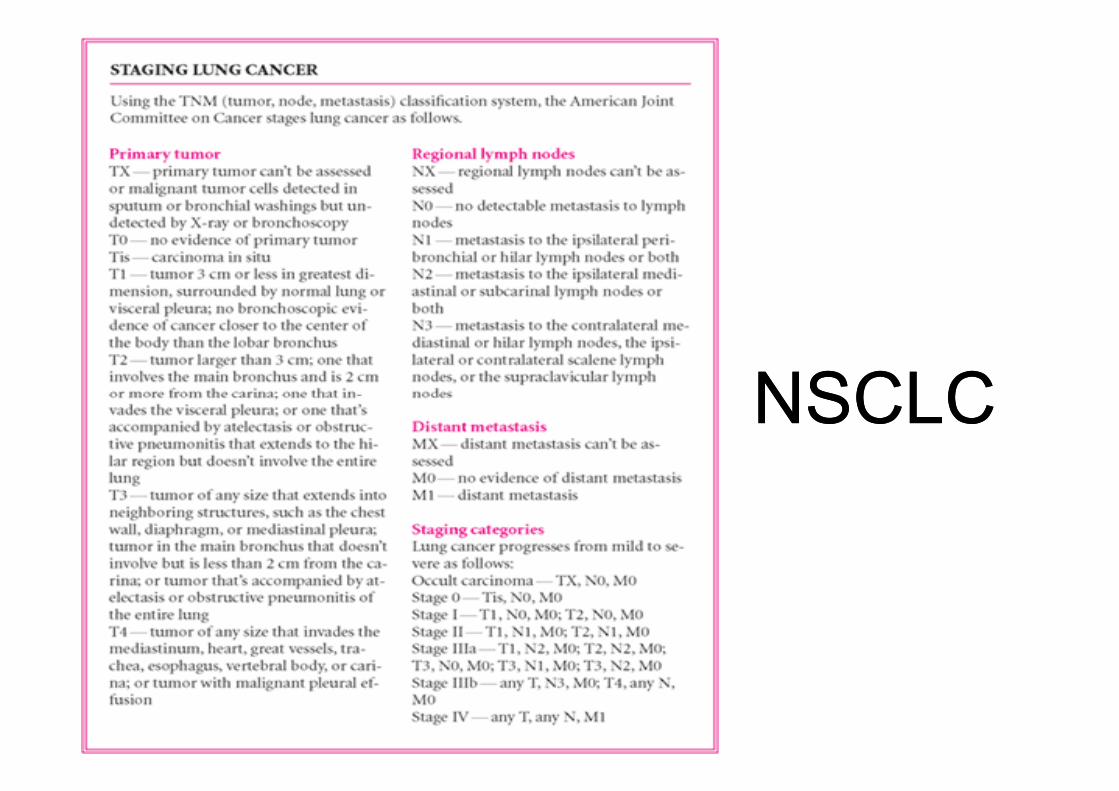
NSCLCNSCLCNSCLCNSCLC
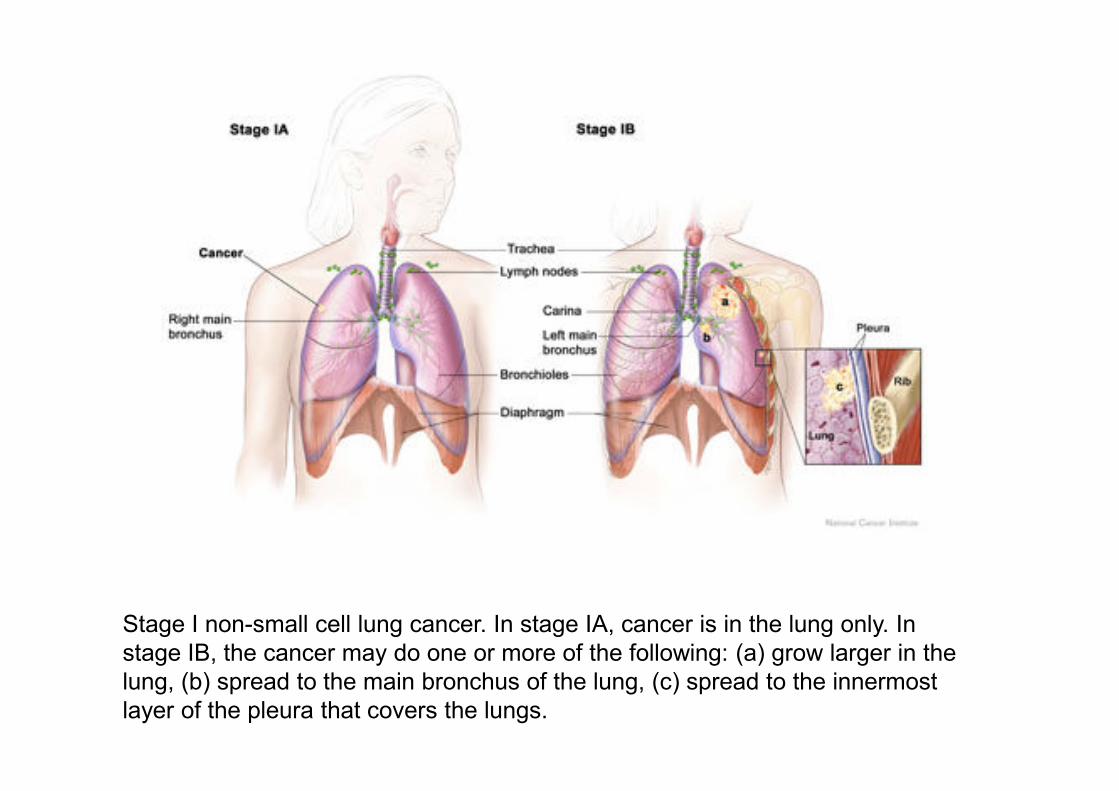
Stage I non-small cell lung cancer. In stage IA, cancer is in the lung only. In
stage IB, the cancer may do one or more of the following: (a) grow larger in the
lung, (b) spread to the main bronchus of the lung, (c) spread to the innermost
layer of the pleura that covers the lungs.

Stage II non-small cell lung cancer. In stage IIA, cancer has spread to lymph
nodes on the same side of the chest as the cancer. In stage IIB, cancer is either
the same as in stage IB and has also spread to lymph nodes on the same side of
the chest; or cancer has not spread to lymph nodes but has spread to one or
more of the following: (a) the chest wall, (b) the diaphragm, (c) the pleura
between the lungs, (d) the membrane around the heart, and/or (e) the main
bronchus.
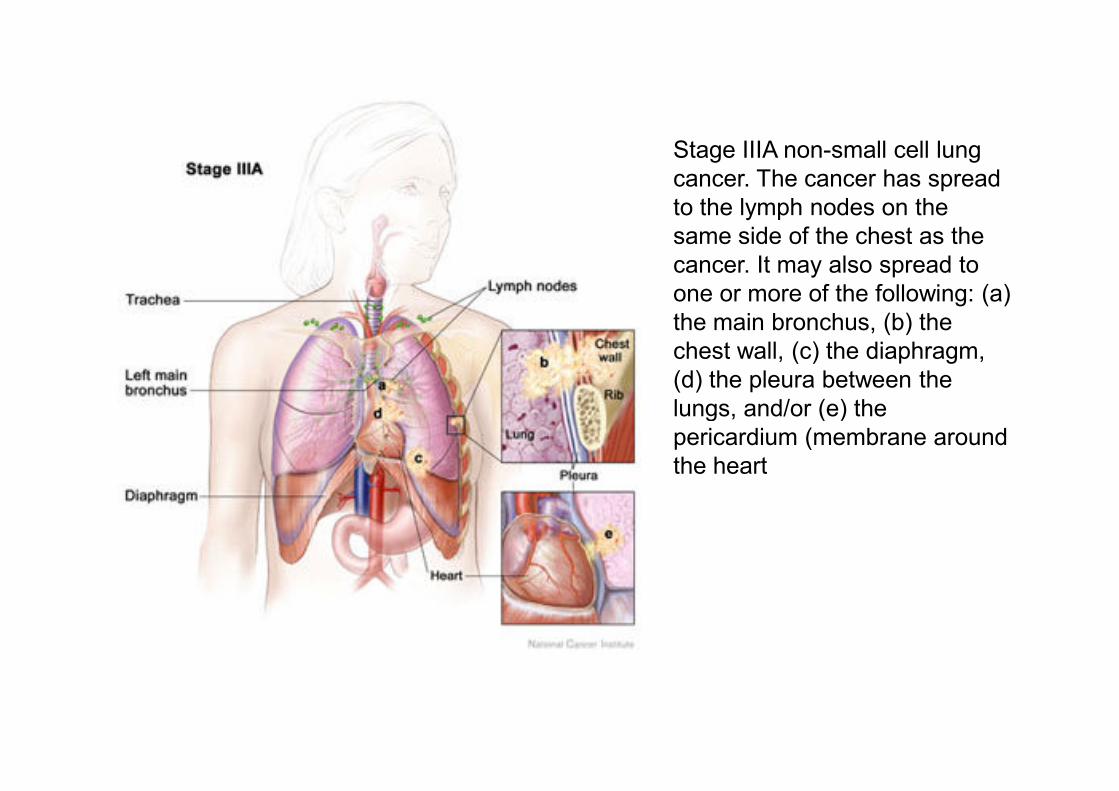
Stage IIIA non-small cell lung
cancer. The cancer has spread
to the lymph nodes on the
same side of the chest as the
cancer. It may also spread to
one or more of the following: (a)
the main bronchus, (b) the
chest wall, (c) the diaphragm,
(d) the pleura between the
lungs, and/or (e) the lungs, and/or (e) the
pericardium (membrane around
the heart
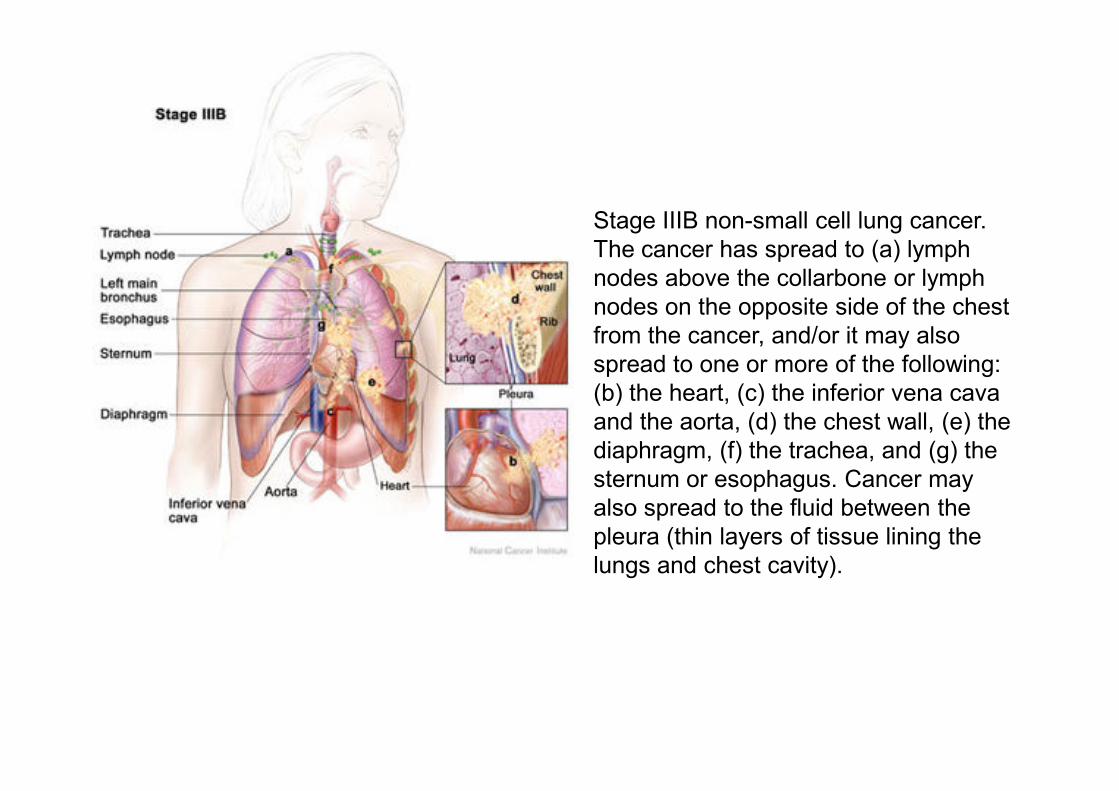
Stage IIIB non-small cell lung cancer.
The cancer has spread to (a) lymph
nodes above the collarbone or lymph
nodes on the opposite side of the chest
from the cancer, and/or it may also
spread to one or more of the following:
(b) the heart, (c) the inferior vena cava (b) the heart, (c) the inferior vena cava
and the aorta, (d) the chest wall, (e) the
diaphragm, (f) the trachea, and (g) the
sternum or esophagus. Cancer may
also spread to the fluid between the
pleura (thin layers of tissue lining the
lungs and chest cavity).

Stage IV non-small cell lung cancer. The cancer has spread to another lobe of
the same lung, to the other lung, and/or to one or more other parts of the body.
SCLC
A two-stage classification established by the Veterans
Administration Lung Cancer Study Group is widely
used in the United States to stage SCLC:
– Limited disease is classified as disease confined to one
hemithorax and to the regional lymph nodes. The tumor
and can be encompassed by a single radiation
port,
– extensive [Approximately 70% of patients]

TREATMENT
Desired Outcome and General Approach to Patient
• The treatment of lung cancer depends on tumor histology, stage of disease, and patient characteristics such as age, gender, history, and performance status.gender, history, and performance status.
• In patients with earlystage disease, a definitive cure is the primary goal of treatment, although this end point is not always met.
• Additional goals of treating lung cancer patients include prolongation of survival and improvement of quality of life through alleviation of symptoms.
Nonpharmacological Therapy
Surgery
• Of all treatment modalities, surgical resection of the affected lobe or lung leads to the greatest improvement in survival for NSCLC patients.
• If at all possible, surgery should be considered the mainstay of treatment for all patients with early-stage NSCLC (clinical stage IA, IB, or IIA) and locally advanced tumors.
• Surgery is not curative and as a general approach does not prolong • Surgery is not curative and as a general approach does not prolong survival in patients with advanced disease; however, it is an important palliative treatment that can improve some patients’ quality of life.
• Patients with small cell carcinomas are treated rarely with surgery because the results of a randomized trial published in 1969 showed that surgery did not result in any 5- or 10-year survivors, whereas radiation produced a 4% survival rate at 5 and 10 years.
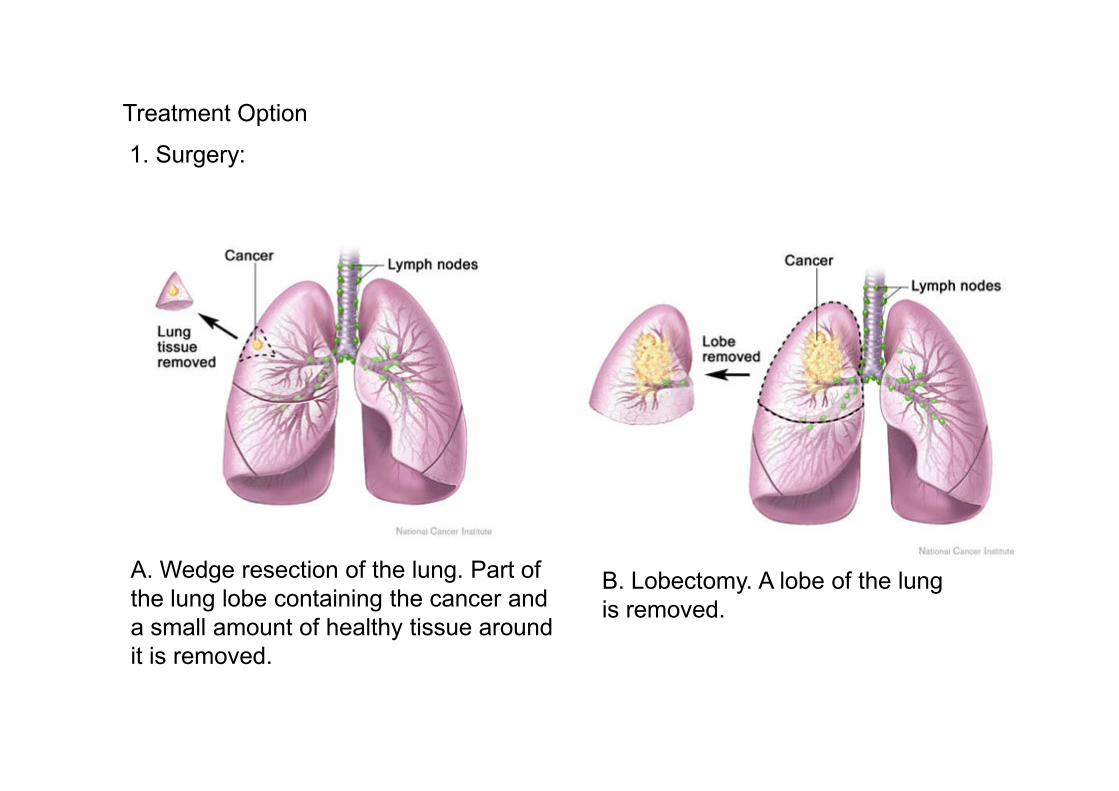
Treatment Option
1. Surgery:
A. Wedge resection of the lung. Part of
the lung lobe containing the cancer and
a small amount of healthy tissue around
it is removed.
B. Lobectomy. A lobe of the lung
is removed.
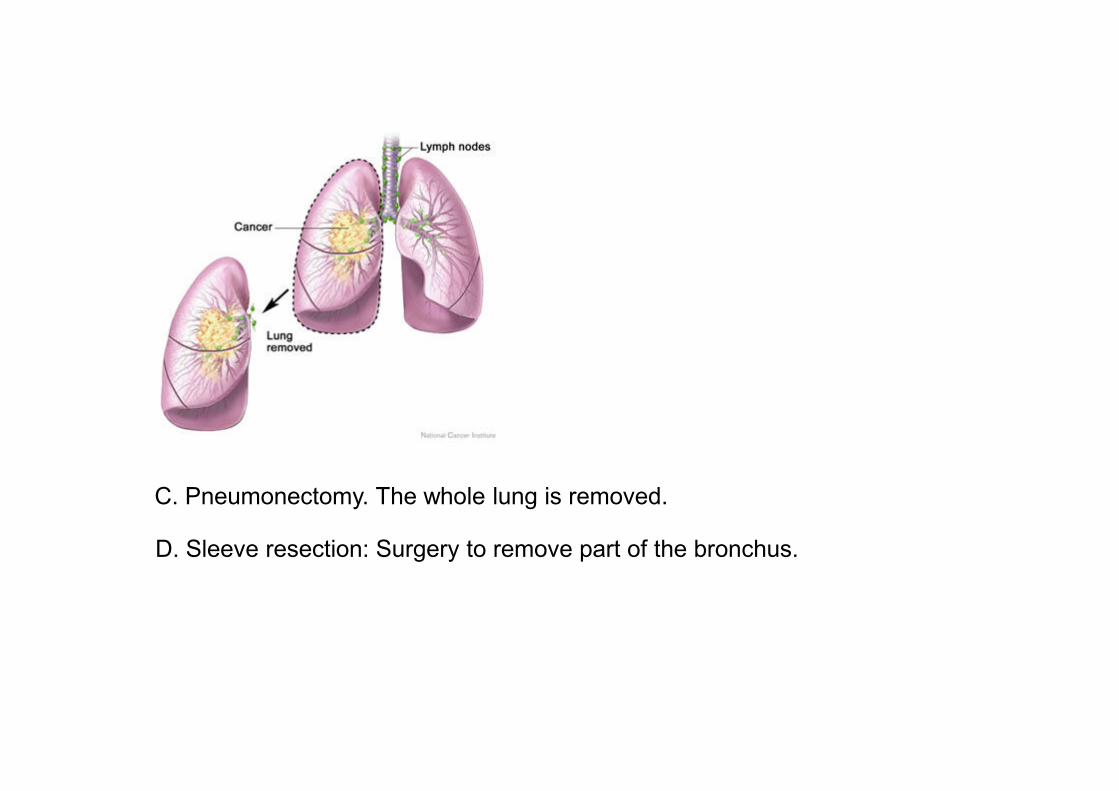
C. Pneumonectomy. The whole lung is removed.
D. Sleeve resection: Surgery to remove part of the bronchus.
Radiation therapy
• Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy. External radiation therapy uses a machine outside the body to send radiation toward the cancer. Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
• Radiotherapy is most commonly administered postsurgically (adjuvant therapy) for prevention of local disease recurrence, as well as in advanced disease for the palliation of tumor-related symptoms (i.e., control of pain from bone metastases, hemoptysis, or obstructive symptoms).
• Although radiation is less invasive than surgery, it can have marked toxicity on normal tissue, and patients may experience esophagitis, pneumonitis, cardiac abnormalities, myelopathies, and skin irritation

Radiation therapy
• radiation is the treatment of choice for
– limited-stage small cell lung cancer.
– palliation of symptoms for advanced small cell lung cancer
– Patients with inoperable localized NSCLC because of comorbidities (e.g., lung disease from smoking).
– patients with late-stage NSCLC can receive radiation therapy to palliate symptomatic metastases.
Chemotherapy
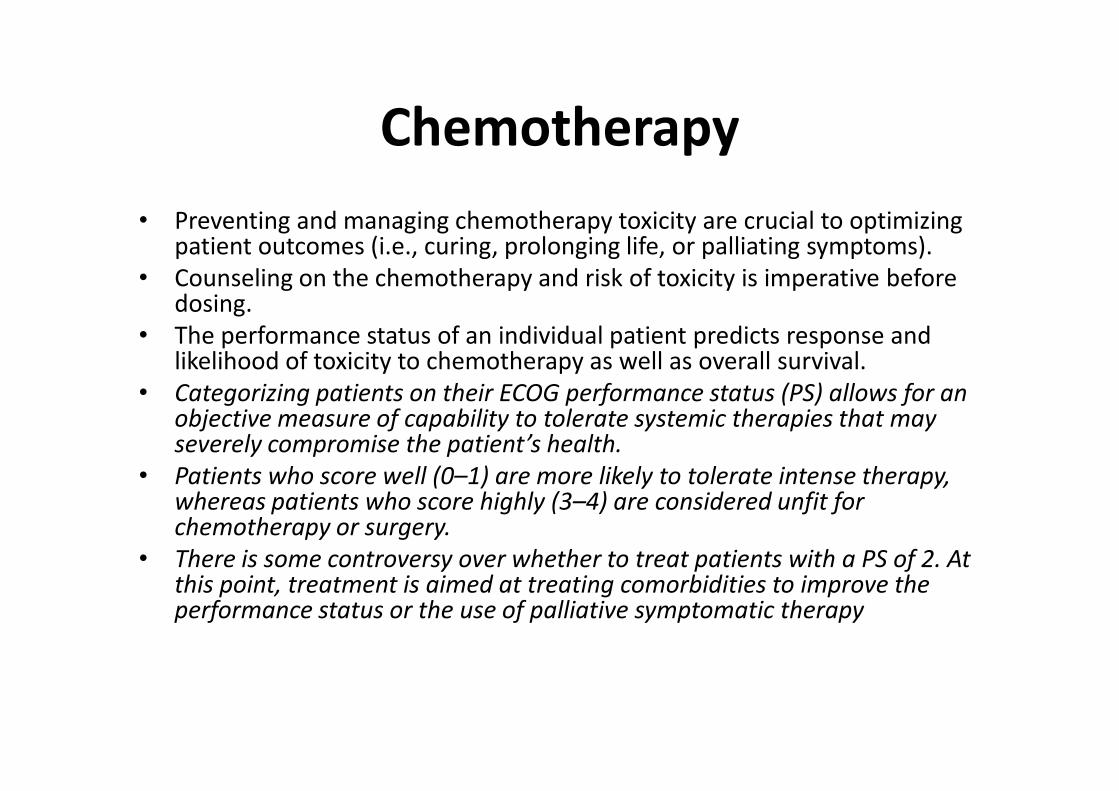
• Preventing and managing chemotherapy toxicity are crucial to optimizing patient outcomes (i.e., curing, prolonging life, or palliating symptoms).
• Counseling on the chemotherapy and risk of toxicity is imperative before dosing.
• The performance status of an individual patient predicts response and likelihood of toxicity to chemotherapy as well as overall survival.
• Categorizing patients on their ECOG performance status (PS) allows for an • Categorizing patients on their ECOG performance status (PS) allows for an objective measure of capability to tolerate systemic therapies that may severely compromise the patient’s health.
• Patients who score well (0–1) are more likely to tolerate intense therapy, whereas patients who score highly (3–4) are considered unfit for chemotherapy or surgery.
• There is some controversy over whether to treat patients with a PS of 2. At this point, treatment is aimed at treating comorbidities to improve the performance status or the use of palliative symptomatic therapy
Adjuvant Therapy
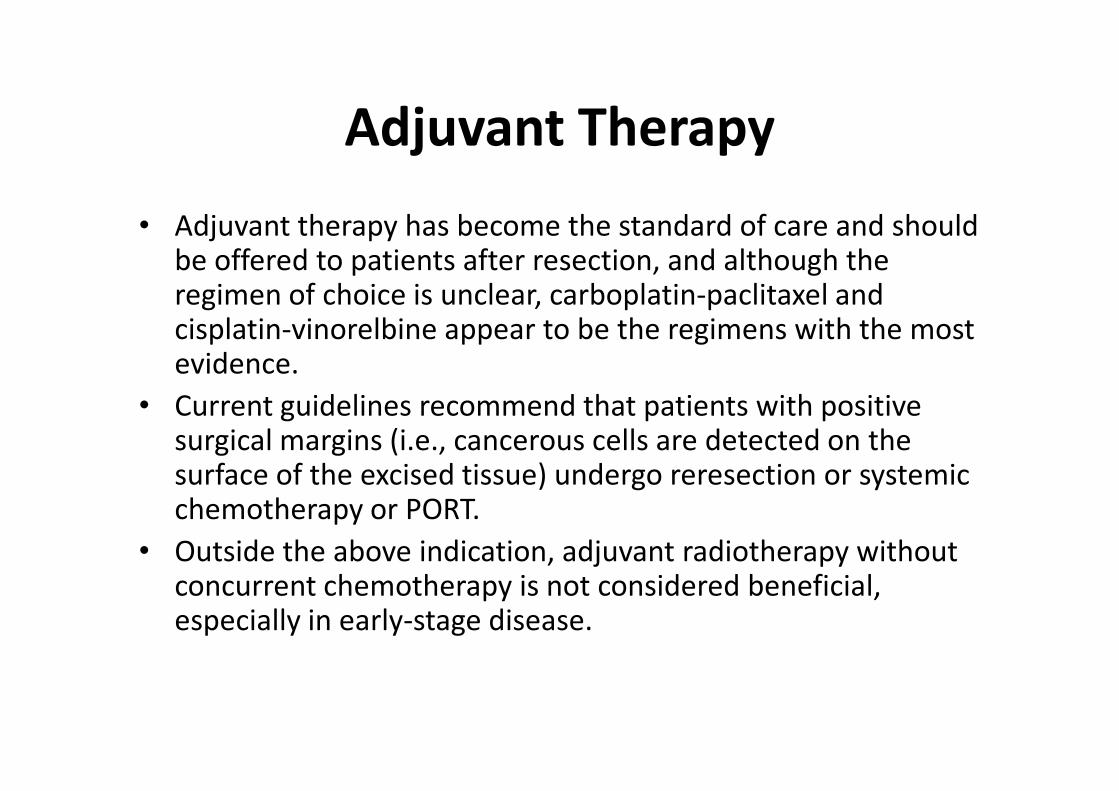
• Adjuvant therapy has become the standard of care and should be offered to patients after resection, and although the regimen of choice is unclear, carboplatin-paclitaxel and cisplatin-vinorelbine appear to be the regimens with the most evidence.
• Current guidelines recommend that patients with positive • Current guidelines recommend that patients with positive surgical margins (i.e., cancerous cells are detected on the surface of the excised tissue) undergo reresection or systemic chemotherapy or PORT.
• Outside the above indication, adjuvant radiotherapy without concurrent chemotherapy is not considered beneficial, especially in early-stage disease.
Neoadjuvant Therapy
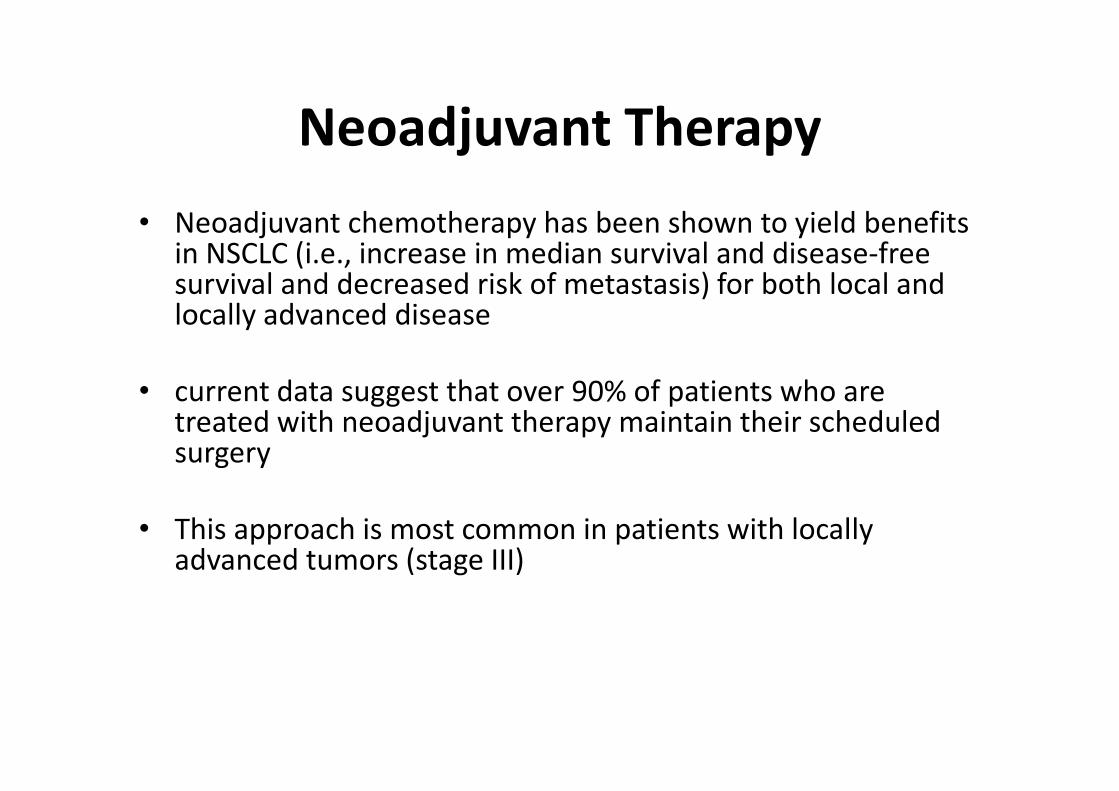
• Neoadjuvant chemotherapy has been shown to yield benefits in NSCLC (i.e., increase in median survival and disease-free survival and decreased risk of metastasis) for both local and locally advanced disease
• current data suggest that over 90% of patients who are • current data suggest that over 90% of patients who are treated with neoadjuvant therapy maintain their scheduled surgery
• This approach is most common in patients with locally advanced tumors (stage III)

Photodynamic therapy (PDT)
Photodynamic therapy (PDT) is a cancer treatment that uses a drug
and a certain type of laser light to kill cancer cells. A drug that is not
active until it is exposed to light is injected into a vein. The drug
collects more in cancer cells than in normal cells. Fiberoptic tubes are
then used to deliver the laser light to the cancer cells, where the drug
becomes active and kills the cells. Photodynamic therapy causes little
damage to healthy tissue. It is used mainly to treat tumors on or just
under the skin or in the lining of internal organs.
Watchful waiting
Watchful waiting is closely monitoring a patient’s condition without
giving any treatment until symptoms appear or change. This may be
done in certain rare cases of non-small cell lung cancer.
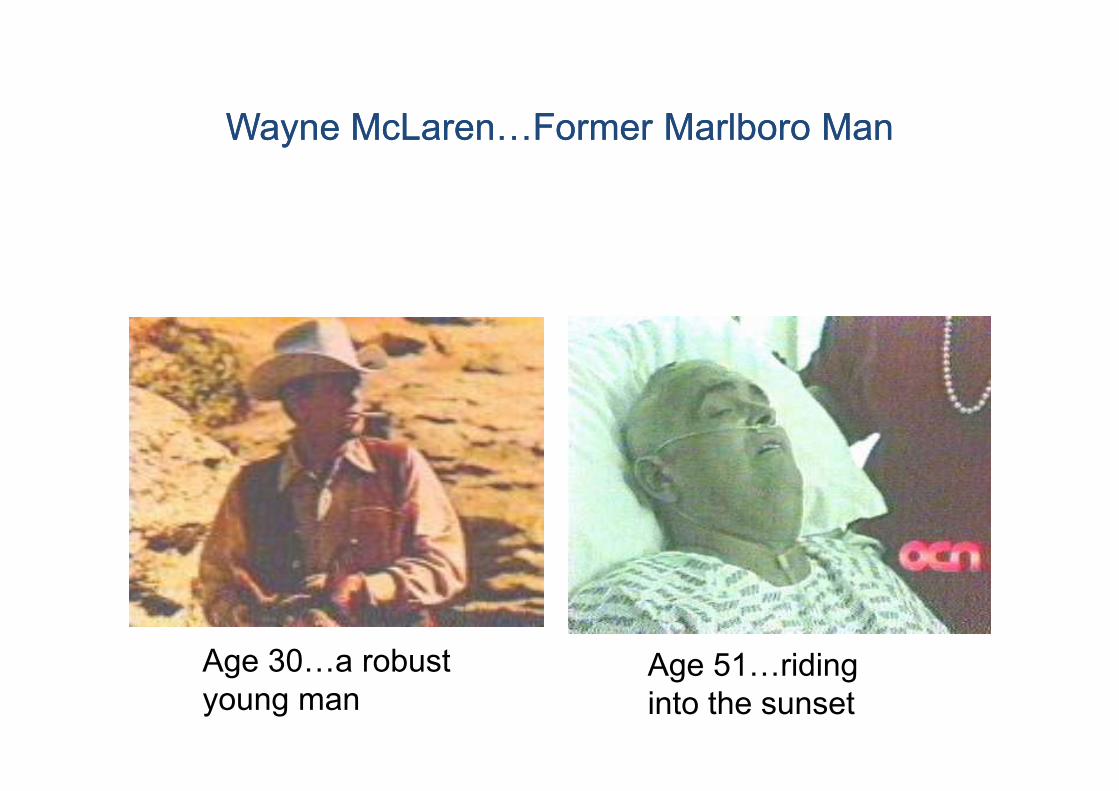
Wayne McLarenJFormer Marlboro ManWayne McLarenJFormer Marlboro Man
Age 30Ja robust
young manAge 51Jriding
into the sunset
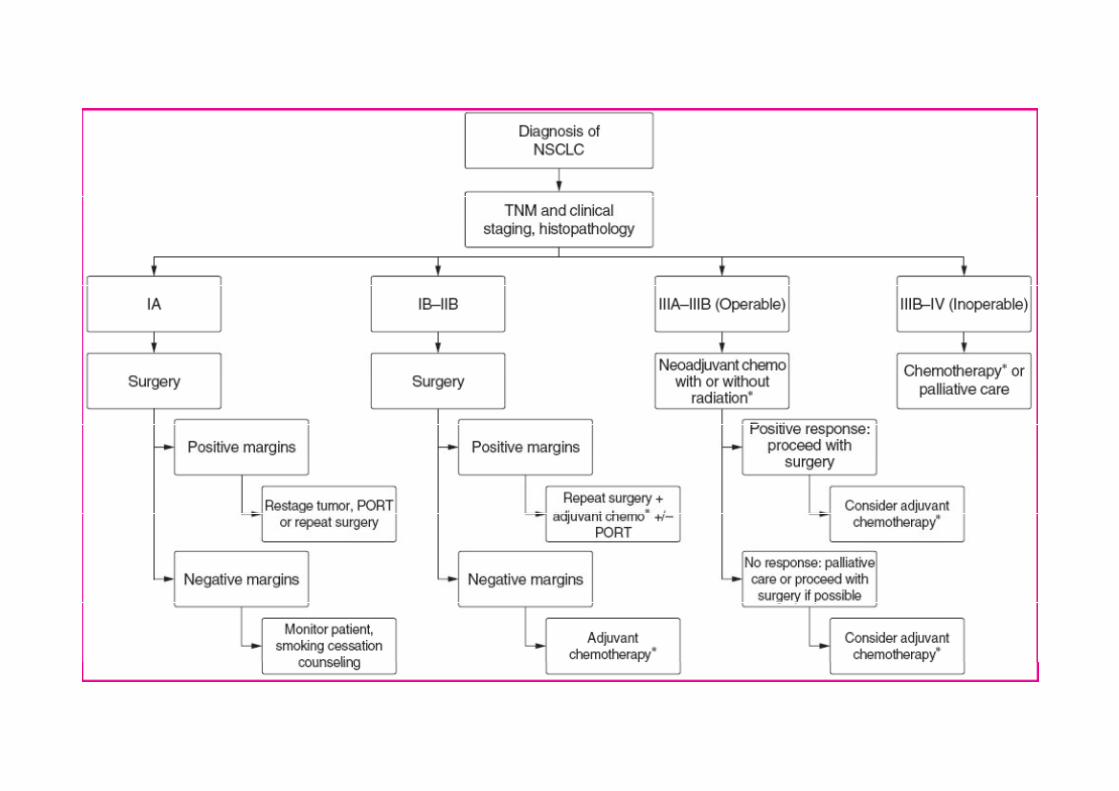
In summary
Local Disease
• Stage IA tumors are seen rarely clinically but may be treated with surgery alone.
• Stage IB, IIA, and IIB disease is treated with adjuvant chemotherapy.chemotherapy.
• The regimen of choice in this setting is not clear; however, the most benefit seen in clinical trials used carboplatin-paclitaxel or cisplatin-vinorelbine.
In summary
Locally Advanced Disease
• Patients with locally advanced disease (stages IIB and IIIA) still may be considered for surgery.
• Neoadjuvant chemotherapy with concurrent radiotherapy can be used prior to surgery
• Progression of disease during induction therapy may preclude • Progression of disease during induction therapy may preclude surgery, and the regimen should be altered if disease progresses in this time.
• If there is a response, surgery may proceed, preferably with additional adjuvant chemotherapy.
• Nonresectable locally advanced disease may be treated with both an active platinum-containing regimen and radiotherapy.

In summary
Advanced or Metastatic Disease (Stages IIIB and IV)
• Advanced disease is treated with chemotherapy if the patient has an acceptable ECOG PS score (0–1).
• NSCLC chemotherapy doublets that are considered generally equivalent include:equivalent include:– Paclitaxel-cisplatin
– Paclitaxel-carboplatin
– Cisplatin-gemcitabine
– Cisplatin-docetaxel
– Carboplatin-docetaxel
– Cisplatin-vinorelbine
– Gemcitabine-paclitaxel
– Gemcitabine-docetaxel

In summary
Recurrent (Progressive) Disease
• If the recurrence is localized, surgery options may be assessed.
• If the patient’s PS remains acceptable (0–1), second-line systemic chemotherapy has been shown to improve survival. A single-agent therapy with docetaxel, pemetrexed, or A single-agent therapy with docetaxel, pemetrexed, or erlotinib is recommended at this stage.
• Recurrences in poorly performing patients (3–4) usually are not treated with chemotherapy and are instead treated with supportive care.
• Additional recurrences (i.e., third-line therapy) may be treated with erlotinib if not used previously. Otherwise, repeat single-agent therapy or administer best supportive care.
Single agent chemotherapy:
First-line therapy for advanced-stage NSCLC and small cell
lung cancer is best done with a two-drug regimen. However,
patients who have a recurrence after the initial regimen are best
treated with a single chemotherapy agent.
Single-agent therapy
is also acceptable for poor health patients with advanced diseaseis also acceptable for poor health patients with advanced disease
because toxicities tend to be lower with one-drug regimens
Response rate 5-20%
No significant effect on overall survival
Typical agents used in monotherapy in lung cancer
include pemetrexed, erlotinib, docetaxel, gemcitabine, paclitaxel,
topotecan, and vinorelbine.
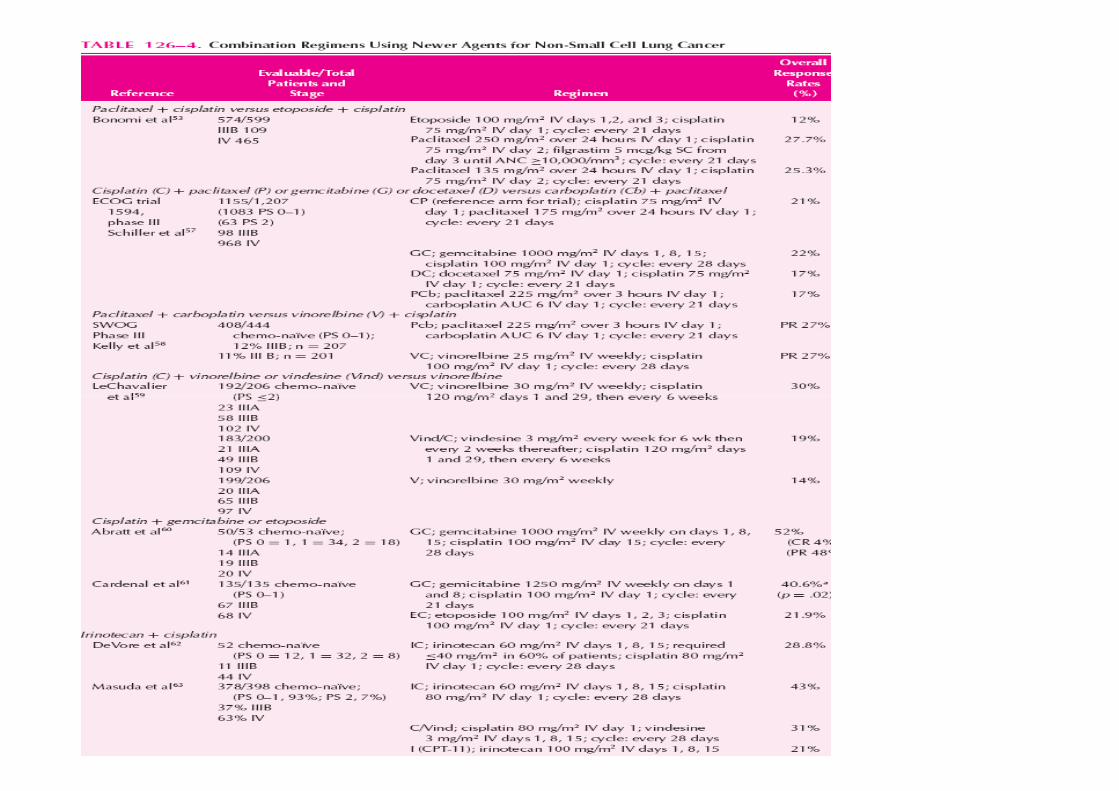
Combination chemotherapy
• Response rate better than single therapy.
• Doublet chemotherapy regimens clearly are superior in response to single-agent regimens and should be used when response to single-agent regimens and should be used when the patient can tolerate the increased toxicity. Platinum-containing regimens are the mainstay of multidrug regimens.
• guidelines still suggest that a platinum-containing doublet should be used when feasible.
• Combination ciplastin (60 – 100 mg/m2 on day 1) and etoposide (80 – 120 mg/ m2 on days 1, 2 and 3.

Monoclonal Antibodies
• Bevacizumab targets vascular endothelial-derived growth factor (VEGF), which is thought to facilitate angiogenesis, a process contributing to growth and maintenance of the tumor environment.
• bevacizumab has been shown to improve survival of advanced-stage NSCLC patients in a large phase III trial and has been incorporated into current guidelines.
EVALUATION OF THERAPEUTIC OUTCOMES
• Following initial therapy for NSCLC, patients must be monitored for evidence of disease recurrence.
• For patients who have undergone surgical resection with or without chemotherapy and/or radiation, a physical examination and chest x-ray are recommended every 3 to 4 months for the first 2 years, then every 6 months for 3 years, and then annually; and a low-dose spiral chest CT scan is recommended annually to monitor for evidence of locoregional recurrence. for evidence of locoregional recurrence.
• Suspicious symptoms or physical findings (e.g., bone pain, visual abnormalities or headache, or elevated liver function tests) should prompt an evaluation to rule out distant metastases.
• For patients with advanced disease receiving chemotherapy, diagnostic tests used in initial staging should be repeated after the second cycle to evaluate for response to determine if further therapy is warranted.
Small Cell Lung CancerSmall Cell Lung Cancer

Small Cell Lung Cancer
Without treatment, small cell carcinoma of the lung has the
most aggressive clinical course of any type of pulmonary
tumor, with median survival from diagnosis of only 2 to 4
months.
Compared with other cell types of lung cancer, small cell
carcinoma has a greater tendency to be widely
disseminated by the time of diagnosis but is much more
responsive to chemotherapy and irradiation.
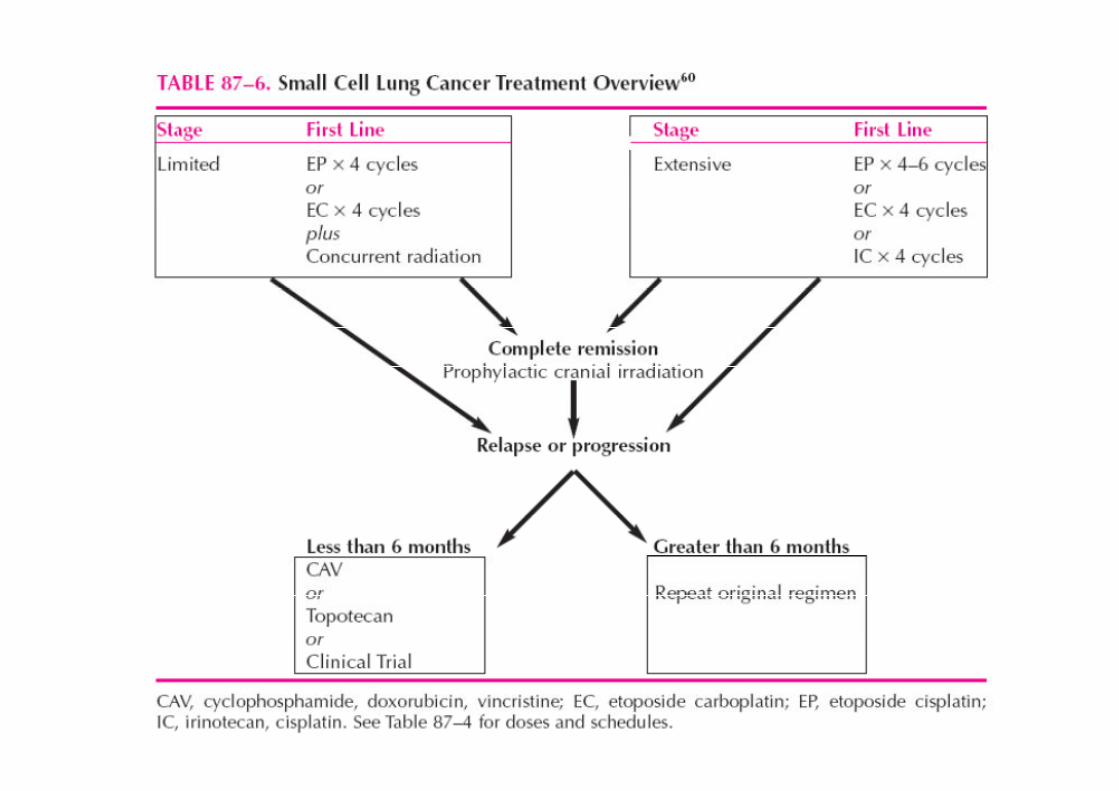
• Carboplatin may be substituted for cisplatin to reduce nausea and vomiting, nephrotoxicity, or neurotoxicity, although increased myelosuppression in the form of thrombocytopenia may result.
• patients who achieve a complete response with treatment should be offered PCI.should be offered PCI.
• A combination of irinotecan and cisplatin shows an increased median survival time by approximately 3 months over the EP regimen.
• IC showed a lower incidence`of severe neutropenic side effects but exhibited higher rates of`middle- to high-grade diarrhea.
LIMITED-STAGE DISEASE
At the time of diagnosis, approximately 30% of patients with small cell
carcinoma will have tumor confined to the hemithorax of origin, the
mediastinum, or the supraclavicular lymph nodes. These patients are
designated as having limited-stage disease, and most 2-year disease-
free survivors come from this group. In limited-stage disease, median
survival of 16 to 24 months with current forms of treatment can
reasonably be expected. A small proportion of patients with limited-
stage disease may benefit from surgery with or without adjuvant
chemotherapy; these patients have an even better prognosis.
EXTENSIVE-STAGE DISEASE
Patients with tumors that have spread beyond the supraclavicular areas
are said to have extensive-stage disease and have a worse prognosis
than patients with limited-stage disease. Median survival of 6 to 12
months is reported with currently available therapy, but long-term
disease-free survival is rare.
PROGNOSTIC FACTORS
The pretreatment prognostic factors that consistently predict for
prolonged survival include good performance status, female
gender, and limited-stage disease.
Patients with involvement of the central nervous system or liver at Patients with involvement of the central nervous system or liver at
the time of diagnosis have a significantly worse outcome.
In general, patients who are confined to bed tolerate aggressive
forms of treatment poorly, have increased morbidity, and rarely
attain 2-year disease-free survival; however, patients with poor
performance status can often derive significant palliative benefit
and prolongation of survival from treatment.
• For patients with symptomatic brain metastases, therapeutic dosages of cranial irradiation usually control the CNS disease.
• Dexamethasone (to decrease intracranial pressure) and anticonvulsants are routinely administered to patients with brain metastases for symptomatic control and seizure prevention, respectively.
• Combination chemotherapy should also be administered, with administration occurring after whole-brain irradiation in those patients with symptomatic brain metastases.
CHEMOTHERAPY FOR RELAPSED DISEASE
• After disease recurrence, the median survival is about 4 months.
• Unfortunately, when disease recurs, it is usually less sensitive to chemotherapy. The agent of choice for second-line chemotherapy is often based on the time span between completion of the induction chemotherapy regimen and relapse.
• Ifosfamide, paclitaxel, docetaxel, and gemcitabine are options for those with a good performance status (i.e., performance status 0 to 2) who relapse <3 months after induction chemotherapy was completed.
• In those who relapse between 3 and 6 months after PE or CE, options include • In those who relapse between 3 and 6 months after PE or CE, options include topotecan, irinotecan, CAV (cyclophosphamide, doxorubicin, and vincristine), gemcitabine, paclitaxel, docetaxel, oral etoposide, methotrexate, or vinorelbine.
• Topotecan administered as a second-line agent in patients with drug-resistant tumors produced objective responses and decreased symptoms in 25% to 38% of patients.
• The original chemotherapy regimen is used for those who have a long duration of disease control (i.e., >6 months between induction chemotherapy and relapse)
EVALUATION OF THERAPEUTIC OUTCOMES
• Restaging to determine the efficacy of induction therapy is done after two to three cycles of treatment.
• therapy is continued for patients with a complete or partial response or stable disease, and discontinued or changed to a non–cross-resistant regimen in patients demonstrating evidence of progressive disease.
• The induction chemotherapy regimen is administered for four to six cycles if the • The induction chemotherapy regimen is administered for four to six cycles if the SCLC disease is responsive.
• In those with a complete response, PCI is offered
• After recovery from initial therapy, follow-up visits should occur every 3 months for years 1, 2, and 3, then every 6 months for years 4 and 5, then annually for patients with either a partial or complete response.

COMPLICATIONS AND SUPPORTIVE CARE
• Patients with lung cancer frequently have numerous concurrent medical problems; paraneoplastic syndromes, chemotherapy and radiotherapy toxicity, or concomitant disease states (e.g., cardiac disease, renal dysfunction, chronic obstructive pulmonary disease, asthma, or diabetes).
• Depression is common and sometimes persistent in patients with SCLC and NSCLC and should be treated. and NSCLC and should be treated.
• The chemotherapy regimens used in the management of lung cancer are intensive and are associated with a wide variety of toxic effects; Nausea and vomiting may be severe.
• Cisplatin-containing regimens require the use of aggressive acute and delayed antiemetic regimens containing a serotonin antagonist plus dexamethasone and sometimes intravenous hydration and nutritional support.
COMPLICATIONS AND SUPPORTIVE CARE
• Other toxic effects associated with these chemotherapy regimens include Myelosuppression, Granulocytopenia mucositis, nephrotoxicity, peripheral neuropathies, and ototoxicity.
• Patients receiving radiation therapy may experience complications including severe esophagitis, fatigue, radiation pneumonitis, and cardiac toxicity. These toxicities are usually more common and severe when radiation is combined with chemotherapy. chemotherapy.
• It is readily apparent that many lung cancer patients receive complex pharmacologic regimens that may include chemotherapeutic agents, antiemetics, antibiotics, analgesics, anticoagulants, bronchodilators, corticosteroids, anticonvulsants, and cardiovascular agents.
• Such regimens necessitate intensive therapeutic monitoring in order to avoid drug-related and radiotherapy-related toxic effects and to optimize therapeutic outcome for individual patients.