making sure rotavrui s vaccni es actually get delivered to
TRANSCRIPT

Making sure Rotavirus Vaccines actually get delivered to those
who need them most
Dr. Craig Burgess, JSI Research and Training Institute Inc.Rotavirus 2018 Symposium, Minsk, 31 August, 2018

Overview1. Global trends
2. Increasing access and utilization
GRISPRED / REC principles and evolutionData issuesCommunity engagementSupply chainsMissed opportunities
3. Some thoughts for the future

Global coverage estimates, 1980-2017BCG, DTP 1st and 3rd, Measles 1st and 2nd, Rubella 1st, HepBbirth and 3rd, Hib3, Pol3, YFV, PCV3 and Rota (last dose)
Source: WHO/UNICEF coverage estimates 2017 revision, July 2018.Immunization Vaccines and Biologicals, (IVB), World Health Organization. 194 WHO Member States. Date of Slide: 15 July 2018.
RVV on different growth
trajectory

Rotavirus vaccine introduced in 97* member states
• Global coverage for RVV is only 28%
• Rotavirus vaccine introduction is lagging in Middle Income Countries
* Includes 6 countries with partial introductionSource: WHO/UNICEF coverage estimates 2017 revision, July 2018. Immunization Vaccines and Biologicals, (IVB), World Health Organization. 194 WHO Member States. Date of slide: 15 July 2018.

5
Inequities in immunization
Source: WHO Global Health Observatory / Health Equity Monitor
To improve coverage in the countries with large numbers of unvaccinated, we need to identify under-vaccinated groups and find tailored strategies to serve them

RVV do not deliver themselves!
Vaccines do not deliver themselves!
Successful, equitable introduction needs strong underlying systems: 6 building blocks + 1
Services that are:• Accessible• Available• Acceptable• Affordable• Affable
Financing
Service Delivery
Vaccines, drugs, &
commodities
Information
Human Resources
Governance
People/ Communities
Key issues with delivering RVV
1. RVV introduction may exacerbate inequities without links to:
• pro-equity health & multi sector / PHC plans; • community participation (eg. using RED / REC)
2. Timing of RVV administration is important:• First dose >15 weeks, last dose < 32 weeks• NO catch up campaigns or PIRI: only through routine delivery• HWs and parents need to know this
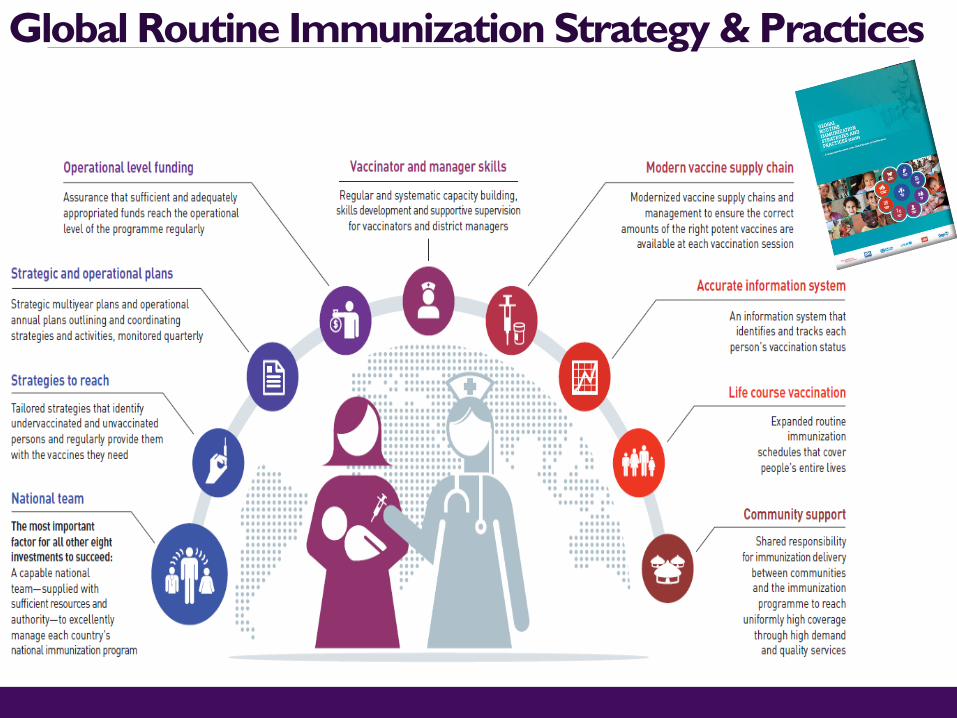
Global Routine Immunization Strategy & Practices
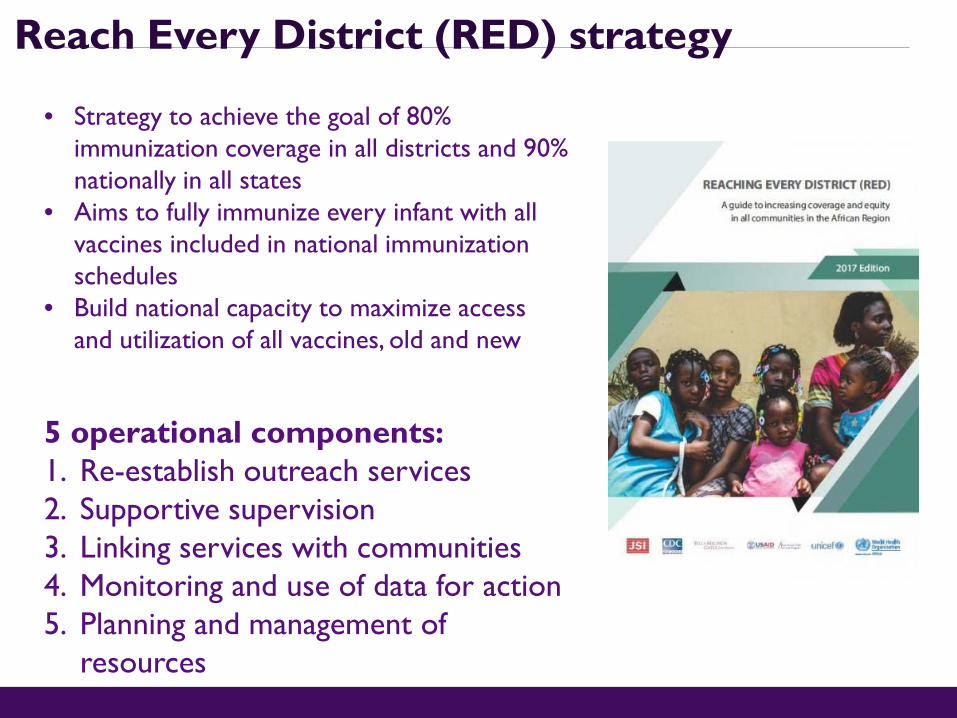
Reach Every District (RED) strategy
• Strategy to achieve the goal of 80% immunization coverage in all districts and 90% nationally in all states
• Aims to fully immunize every infant with all vaccines included in national immunization schedules
• Build national capacity to maximize access and utilization of all vaccines, old and new
5 operational components:1. Re-establish outreach services2. Supportive supervision3. Linking services with communities4. Monitoring and use of data for action5. Planning and management of
resources

RED traditionally helps identify & prioritize underperforming districts
Low drop out(<10%)
High dropout(>10%)
High Coverage with DPT1
Low dropout(<10%)
High dropout(>10%)
Low coverage with DPT1
Access to immunisation services
Interpretation
Category 1Good accessGood utilization.
Category 2Good accessPoor utilization.
Category 3Poor accessGood utilization.
Category 4Poor accessPoor utilization.

Shift to identify & prioritize under served communities
1. Fragile: displaced or living with conflict or natural disasters
2. Urban poor:either living in slums or integrated
3. Rural remote / poor
Tailored strategies addressing social barriers, life course, more integrated & increasing use of NGOs / private sector to deliver
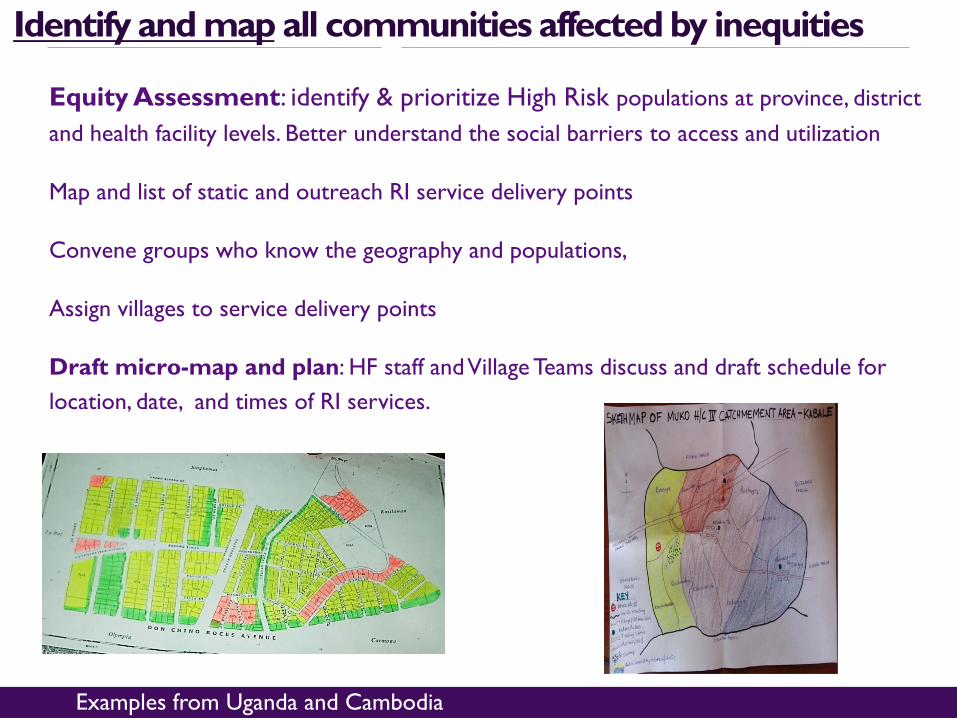
Equity Assessment: identify & prioritize High Risk populations at province, district and health facility levels. Better understand the social barriers to access and utilization
Map and list of static and outreach RI service delivery points
Convene groups who know the geography and populations,
Assign villages to service delivery points
Draft micro-map and plan: HF staff and Village Teams discuss and draft schedule for location, date, and times of RI services.
Identify and map all communities affected by inequities
Examples from Uganda and Cambodia
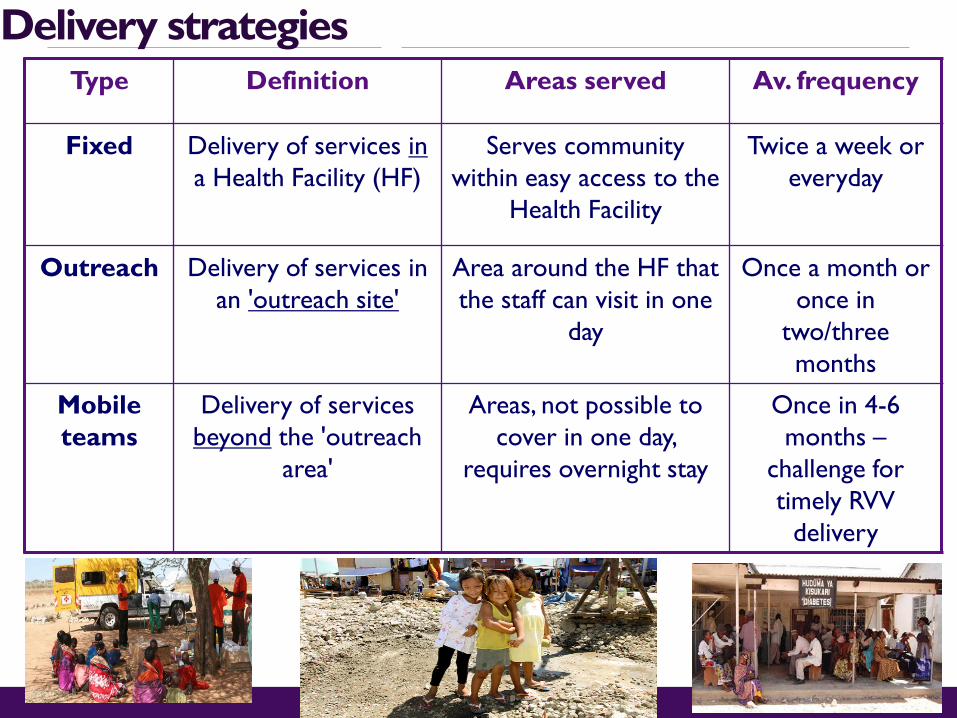
Delivery strategiesType Definition Areas served Av. frequency
Fixed Delivery of services ina Health Facility (HF)
Serves community within easy access to the
Health Facility
Twice a week or everyday
Outreach Delivery of services in an 'outreach site'
Area around the HF that the staff can visit in one
day
Once a month or once in
two/three months
Mobile teams
Delivery of services beyond the 'outreach
area'
Areas, not possible to cover in one day,
requires overnight stay
Once in 4-6 months –
challenge for timely RVV
delivery

X km
10 km
5 km
Fixed strategy
Outreach strategy
Mobile strategy
Health Center
Pop 500
Pop 221
Pop 654
Pop 1125
Pop 688
Pop 211
Pop 400
Pop 339
Pop 99
Pop 675
Pop 1898
Pop 312
Pop 89
Pop 187
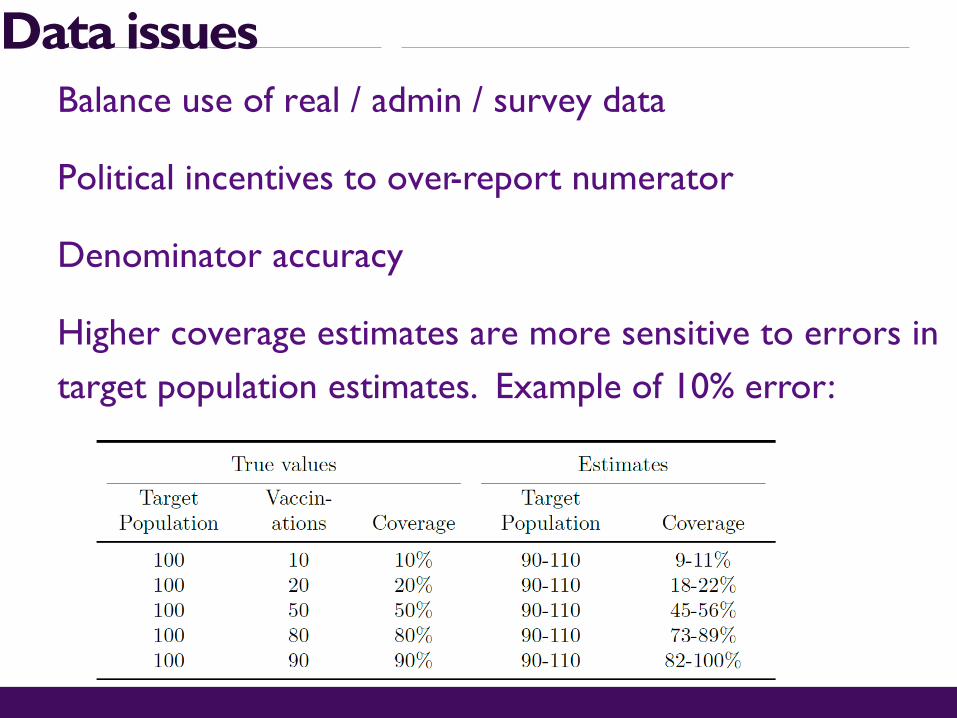
Data issuesBalance use of real / admin / survey data
Political incentives to over-report numerator
Denominator accuracy
Higher coverage estimates are more sensitive to errors in target population estimates. Example of 10% error:

Community engagementGiving voice to the ultimate customer
Joint responsibility to plan, promote and implement services to increase accountability, appropriateness, quality and sustainability of services.
Community Engagement is not just…
Communication Demand Generation Top-Down Planning One way activities
But a shift towards… Community Conversations Intersection of Supply and
Demand Partnering A dialogue

Community engagementChallenges Illustrative examples
Unclear rolesDistrust (especially vulnerable popns.)Not monitored and not remuneratedAccountabilityRepresentation (power dynamics)Quasi-legal nature of some communities
Strategic communication: interpersonal, advocacy, dispel rumoursContribute: outreach planning food, transport, crowd controlCommunity meetingsPeer educationIdentify community mobilizers announcing servicesAnalysis left outs and drop outsCase detection

Logistics & supply chains, distribution capacity
~4x ~6x
~5x ~2x
Growing volume (cm³) to vaccinate per child
Increasing number of doses
2010 2020 Introduction of more expensive vaccines
Increase in stock keeping units
Note: All figures relate to GAVI-funded vaccines1. UNICEF Supply 2012 Financial report, WHO data for Pneumo and Rota vaccines, and HPV (only for girls); 2. 2010: GAVI Shipment Data; 2020; GAVI SDF Forecast; Including volume for GAVI future graduated countries; 3. Comparison based on 2013 Price; 2020 Vaccines include: Rota, Pneumo; HPV; 2010' vaccines include:YF, Measles, DPT, OPV (UNICEF SD); 4. GAVI Background SDF Information; 2010": estimates based on 2009 data; 2020: estimates based on 2013 forecast
2010 2020

Source: Gavi Immunization Supply Chain Strategy, developed 2015
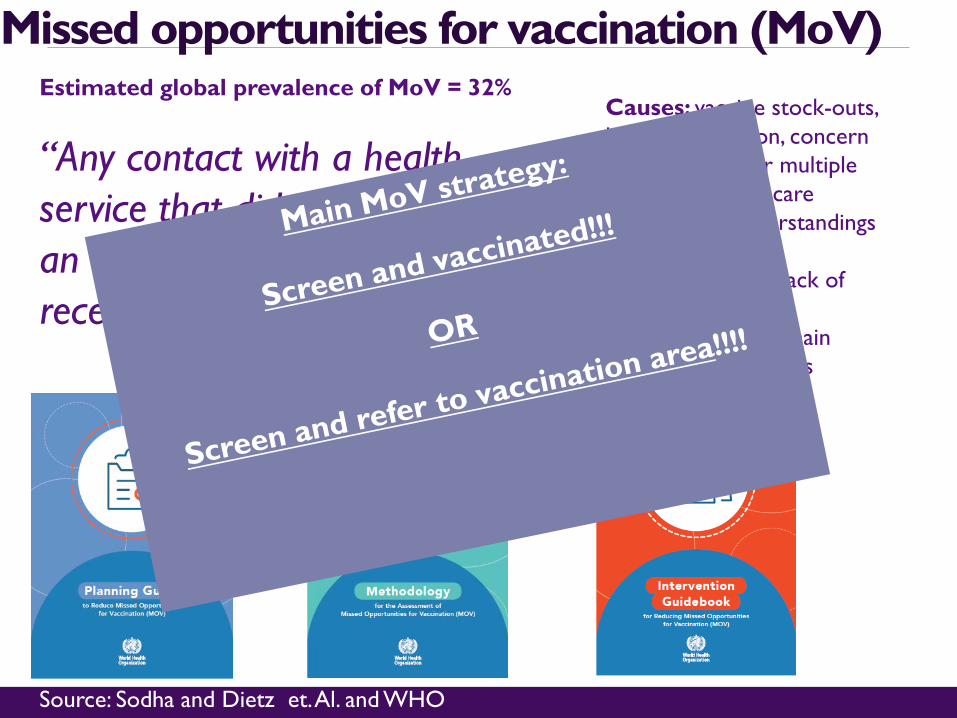
Missed opportunities for vaccination (MoV)Estimated global prevalence of MoV = 32%
“Any contact with a health service that did not result in an eligible child or woman receiving a needed vaccine”
Source: Sodha and Dietz et. Al. and WHO
Causes: vaccine stock-outs, lack of integration, concern about wastage or multiple injections, health care workers’ misunderstandings about vaccine contraindications, lack of vaccine cards, transport or cold chain failure, staff absences

MoV training in Kinshasa -West (Dec 2017) ledto in number of DTP3 doses
5,089 additional doses in 2018, compared to same period in 2017
Source- initial WHO research Kinshasa West 2017-2018 post MoV training
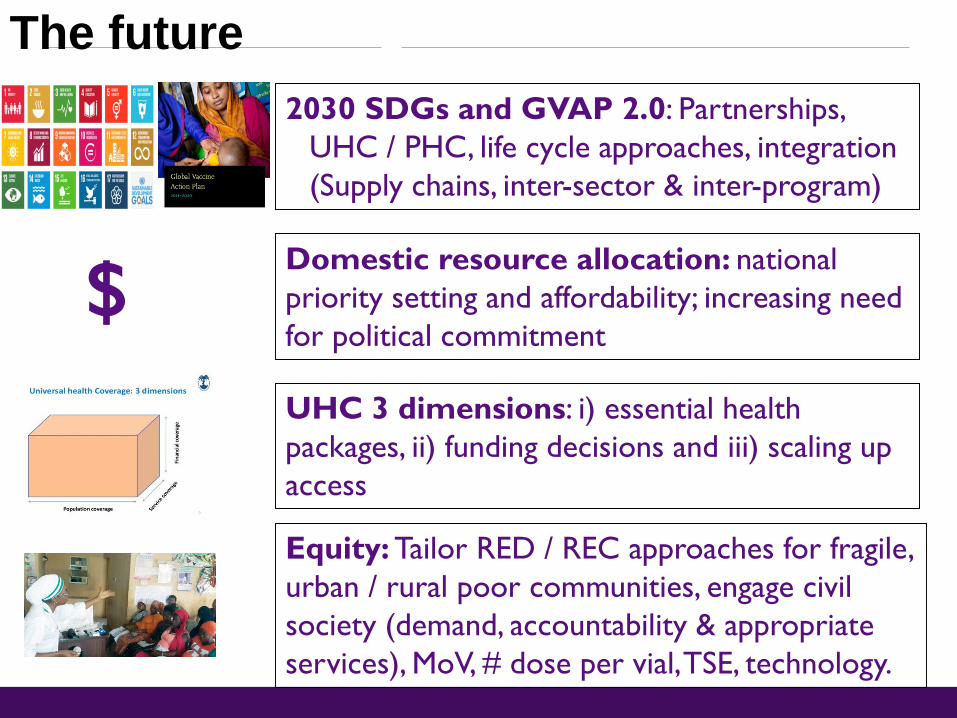
2030 SDGs and GVAP 2.0: Partnerships, UHC / PHC, life cycle approaches, integration (Supply chains, inter-sector & inter-program)
The future
$ Domestic resource allocation: national priority setting and affordability; increasing need for political commitment
UHC 3 dimensions: i) essential health packages, ii) funding decisions and iii) scaling up access
Equity: Tailor RED / REC approaches for fragile, urban / rural poor communities, engage civil society (demand, accountability & appropriate services), MoV, # dose per vial, TSE, technology.

Thank you
Acknowledgements: Robert Steinglass and Wendy Prosser (JSI), Jan Grevendonk, Marta Gacic-Dono, Ike Udo (WHO), RAVIN partnership (IVAC, CDC, BMGF, JSI)

1. Arsenault, Catherine, Sam Harper, Arijit Nandi, José M Mendoza Rodríguez, Peter M Hansen, and Mira Johri. “An Equity Dashboard to Monitor Vaccination Coverage.” Bulletin of the World Health Organization 95, no. 2 (February 1, 2017): 128–34. https://doi.org/10.2471/BLT.16.178079.Bicaba, Abel, Slim Haddad, Moussa Kabore, Emile Taminy, Marta Feletto, and Pierre Fournier. “Monitoring the Performance of the Expanded Program on Immunization: The Case of Burkina Faso.” BMC International Health and Human Rights 9, no. Suppl 1 (October 14, 2009): S12. https://doi.org/10.1186/1472-698X-9-S1-S12.2. Brearley, Lara, Rudi Eggers, Robert Steinglass, and Jos Vandelaer. “Applying an Equity Lens in the Decade of Vaccines.” Va ccine 31 (April 2013): B103–7. https://doi.org/10.1016/j.vaccine.2012.11.088.3. Chan Soeung, S., J. Grundy, R. Duncan, R. Thor, and J. B. Bilous. “From Reaching Every District to Reaching Every Communit y: Analysis and Response to the Challenge of Equity in Immunization in Cambodia.” Health Policy and Planning 28, no. 5 (August 1, 2013): 526–35. https://doi.org/10.1093/heapol/czs096.4. Deutsch, Nicole, Prem Singh, Vivek Singh, Rod Curtis, and Anisur Rahman Siddique. “Legacy of Polio —Use of India’s Social Mobilization Network for Strengthening of the Universal Immunization Program in India.” The Journal of Infectious Diseases 216, no. suppl_1 (July 1, 2017): S260–66. https://doi.org/10.1093/infdis/jix068.5. Dietz, Vance, and Felicity Cutts. “The Use of Mass Campaigns in the Expanded Program on Immunization: A Review of Reported Advantages and Disadvantages.” International Journal of Health Services 27, no. 4 (October 1997): 767–90. https://doi.org/10.2190/QPCQ-FBF8-6ABX-2TB5.6. Favin, Michael, Robert Steinglass, Rebecca Fields, Kaushik Banerjee, and Monika Sawhney. “Why Children Are Not Vaccinated: A Review of the Grey Literature.” International Health 4, no. 4 (December 2012): 229–38. https://doi.org/10.1016/j.inhe.2012.07.004.7. Goel, Sonu, Vishal Dogra, Satish Kumar Gupta, P. V. M. Lakshmi, Sherin Varkey, Narottam Pradhan, Gopal Krishna, and Rajesh Kumar. “Effectiveness of Muskaan Ek Abhiyan (The Smile Campaign) for Strengthening Routine Immunization in Bihar, India.” Indian Pediatrics 49, no. 2 (February 2012): 103–8. https://doi.org/10.1007/s13312-012-0023-7.8. Helleringer, Stephane, Patrick O. Asuming, and Jalaa Abdelwahab. “The Effect of Mass Vaccination Campaigns against Polio on the Utilization of Routine Immunization Services: A Regression Discontinuity Design.” Vaccine 34, no. 33 (July 2016): 3817–22. https://doi.org/10.1016/j.vaccine.2016.05.037.9. Hinman, Alan R., and Mark A. McKinlay. “Immunization Equity.” Vaccine 33 (November 2015): D72–77. https://doi.org/10.1016/j.vaccine.2015.09.033.10. Kc, Ashish, Viktoria Nelin, Hendrikus Raaijmakers, Hyung Joon Kim, Chahana Singh, and Mats Målqvist. “Increased Immunizat ion Coverage Addresses the Equity Gap in Nepal.” Bulletin of the World Health Organization 95, no. 4 (April 1, 2017): 261–69. https://doi.org/10.2471/BLT.16.178327.11. Sodha, S. V., and V. Dietz. “Strengthening Routine Immunization Systems to Improve Global Vaccination Coverage.” British Medical Bulletin 113, no. 1 (March 1, 2015): 5–14. https://doi.org/10.1093/bmb/ldv001.12. Steinglass, Robert. “Routine Immunization: An Essential but Wobbly Platform.” Global Health: Science and Practice 1, no. 3 (November 2013): 295–301. https://doi.org/10.9745/GHSP-D-13-00122.13. Tauil, Márcia de Cantuária, Ana Paula Sayuri Sato, and Eliseu Alves Waldman. “Factors Associated with Incomplete or Delay ed Vaccination across Countries: A Systematic Review.” Vaccine 34, no. 24 (May 2016): 2635–43. https://doi.org/10.1016/j.vaccine.2016.04.016.14. Victora, Cesar Gomes, Gary Joseph, Inacio C. M. Silva, Fatima S. Maia, J. Patrick Vaughan, Fernando C. Barros, and Aluisi o J. D. Barros. “The Inverse Equity Hypothesis: Analyses of Institutional Deliveries in 286 National Surveys.” American Journal of Public Health 108, no. 4 (April 2018): 464–71. https://doi.org/10.2105/AJPH.2017.304277.
References used for equity and coverage

Resources to use 1. Reaching Every District (RED) - A guide to increasing coverage and equity in all communities in the African Region https://www.afro.who.int/publications/reaching-every-district-red-guide-increasing-coverage-and-equity-all-communities2. Country decision making: introducing a new vaccine: http://www.who.int/immunization/programmes_systems/policies_strategies/decision_making/en/3. Missed Opportunities for Vaccination (MOV) Strategy http://www.who.int/immunization/programmes_systems/policies_strategies/MOV/en/4. Establishing and strengthening immunization in the second year of life: Practices for immunization beyond infancy http://www.who.int/immunization/documents/WHO_IVB_ISBN9789241513678/en/5. Reaching Every District strategy (WHO) http://www.who.int/immunization/programmes_systems/service_delivery/red/en/6. WHO principles and considerations when adding a new vaccine http://apps.who.int/iris/bitstream/10665/111548/1/9789241506892_eng.pdf?ua=17. Bottleneck and breakthroughs: lessons learned from new vaccine introductions in low-resource countries 2008-2013 (USAID / MCHIP) – table 7 pages 35-36http://www.jsi.com/JSIInternet/Inc/Common/_download_pub.cfm?id=15580&lid=3 8. WHO SAGE, April 2012, review of NVI on health systemshttp://www.who.int/immunization/sage/meetings/2012/april/presentations_background_docs/en/ 9. Scale up map for new vaccine introduction (JSI / MCHIP / USAID) http://www.mchip.net/files/mchip-event-documents/230348766-Scale-Up-Map-for-New-Vaccine-Introduction-in-GAVI-Supported-Countries-1.pdf 10. Explorations of inequality. Childhood immunization http://www.who.int/gho/health_equity/report_2018_immunization/en11. Global Routine Immunization Strategies and Practices (GRISP) http://www.who.int/immunization/programmes_systems/policies_strategies/GRISP/en/