management of knee dislocations - continuprint, inc. of knee dislocations thomas j. gill, md ......
TRANSCRIPT

6/10/2011
1
Management of Knee Dislocations
Management of Knee Dislocations
Thomas J. Gill, MDChief, Sports Medicine ServiceMassachusetts General Hospital
Associate Professor of Orthopedic SurgeryHarvard Medical School
Thomas J. Gill, MDChief, Sports Medicine ServiceMassachusetts General Hospital
Associate Professor of Orthopedic SurgeryHarvard Medical School
Multi-Ligament InjuriesMulti-Ligament Injuries
•• ComplexComplex
•• ChallengingChallenging
•• Variable outcomesVariable outcomes
•• ComplexComplex
•• ChallengingChallenging
•• Variable outcomesVariable outcomes
•• Can be devastatingCan be devastating
•• Easily overlookedEasily overlooked
•• Can be devastatingCan be devastating
•• Easily overlookedEasily overlooked
Knee DislocationKnee Dislocation
• Epidemiology» Thought to be rare
» 14 cases at Mayo from 1911 – 1960
26 t MGH i 28 i d
• Epidemiology» Thought to be rare
» 14 cases at Mayo from 1911 – 1960
26 t MGH i 28 i d» 26 cases at MGH in 28-year period» 26 cases at MGH in 28-year period

6/10/2011
2
Knee DislocationsKnee Dislocations
• Most common causes» MVA #1
» Sports #2
» Falls #3
• Most common causes» MVA #1
» Sports #2
» Falls #3
• 50% reduce spontaneously
• Anterior most common (40%)
• 50% reduce spontaneously
• Anterior most common (40%)
Knee DislocationKnee Dislocation
• > 2 ligaments injured to dislocate
» not necessarily both cruciates
» PCL status critical for w/u
• > 2 ligaments injured to dislocate
» not necessarily both cruciates
» PCL status critical for w/u» PCL status critical for w/u» PCL status critical for w/u
Physical ExamPhysical Exam
• Lachman
• Pivot shift
• Posterior drawer
• Sag test
• Lachman
• Pivot shift
• Posterior drawer
• Sag test• Sag test
• Valgus stress 0°/30°
• Varus stress 0°/30°
• Recurvatum with ER
• Tibial ER 30°/90°
• Sag test
• Valgus stress 0°/30°
• Varus stress 0°/30°
• Recurvatum with ER
• Tibial ER 30°/90°

6/10/2011
3
ImagingImaging
• XR
• MRI
• ? MRA
? A i
• XR
• MRI
• ? MRA
? A i• ? Angio• ? Angio
LCLrupture
MCLrupture
AnatomyAnatomy• Medial side
» Superficial MCL
» Posterior Oblique Ligament
» Deep MCL
• Medial side» Superficial MCL
» Posterior Oblique Ligament
» Deep MCL
» Semi-membranosis and expansions
» Sartorius, gracilis, semi-tendinosis
» Medial gastrocnemius
• Valgus» ER
» medial and lateral translation
» Semi-membranosis and expansions
» Sartorius, gracilis, semi-tendinosis
» Medial gastrocnemius
• Valgus» ER
» medial and lateral translation
Vascular AnatomyVascular AnatomyPopliteal artery
adductor hiatus
fascial arch of proximal soleus
Types of Injury• Contusion• Stretch• Intimal flap tearp• Rupture
6/10/2011
4
Vascular InjuryVascular Injury
• 14% Vascular injuries » Diagnosis critical
» High index of suspicion
• Detailed neurovascular exam
• 14% Vascular injuries » Diagnosis critical
» High index of suspicion
• Detailed neurovascular exam» Manual pulses
» Doppler
» ABI
• Devastating complications» Compartment Syndrome
» Ischemia
» Manual pulses
» Doppler
» ABI
• Devastating complications» Compartment Syndrome
» Ischemia
Vascular AssessmentVascular Assessment
Angiography - Is it necessary?
• Physical exam adequate» 8 normal exams – 0/8 required surgery
» 11 abnormal exams – 7/11 required surgery
Angiography - Is it necessary?
• Physical exam adequate» 8 normal exams – 0/8 required surgery
» 11 abnormal exams – 7/11 required surgeryq g y
(Hollis et al JOT 2005)
• Abnormal pedal pulse not sensitive enough » Sensitivity 0.79, Specificty 0.91, PPV 0.75, NPV 0.93
(Barnes et al JOT 2002)
• ABI has excellent predictive value» Sensitivity, specificity and PPV of ABI < 0.90 is 100%
» NPV of ABI > 0.90 is 100%(Mills at al JOT 2004)
q g y
(Hollis et al JOT 2005)
• Abnormal pedal pulse not sensitive enough » Sensitivity 0.79, Specificty 0.91, PPV 0.75, NPV 0.93
(Barnes et al JOT 2002)
• ABI has excellent predictive value» Sensitivity, specificity and PPV of ABI < 0.90 is 100%
» NPV of ABI > 0.90 is 100%(Mills at al JOT 2004)
Functional Anatomy of Lateral SideFunctional Anatomy of Lateral Side
• LCL
» Varus, ER
» biceps helps tension in flexion
C
• LCL
» Varus, ER
» biceps helps tension in flexion
C• PLC
» ER, varus, posterior translation
• Popliteus (popliteofibular lig)
» Dynamic IR of tibia
» Static restraint to posterior translation, varus, ER
• PLC
» ER, varus, posterior translation
• Popliteus (popliteofibular lig)
» Dynamic IR of tibia
» Static restraint to posterior translation, varus, ER

6/10/2011
5
Peroneal NervePeroneal Nerve
• 14% Peroneal N. injury• 14% Peroneal N. injury
Nerve InjuryNerve Injury
Incidence: variable (16-40%)
1/3 will recover completely
Nerve Injuries
Peroneal nerve
Travels around proximal fibula from posterior to anterior
Traction injury: Lateral and Posterolateral disruptions
Foot drop
Tibial nerve less common
NFL Experience 1995-2005
NFL Experience 1995-2005
• 19 dislocations» 13 MCL
» 6 LCL
• 19 dislocations» 13 MCL
» 6 LCL
• 19/19 had surgery
• Lost time (73, 310)
• 19/19 had surgery
• Lost time (73, 310)

6/10/2011
6
NFL ExperiencePosition
NFL ExperiencePosition
• DB - 4
• N/A - 3
• QB - 2
• WR 2
• DB - 4
• N/A - 3
• QB - 2
• WR 2• WR - 2
• TE - 2
• OL - 2
• DL - 2
• RB - 1
• LB - 1
• WR - 2
• TE - 2
• OL - 2
• DL - 2
• RB - 1
• LB - 1
NFL ExperienceActivity
NFL ExperienceActivity
• Blocked 10» “Cut” 3
• Tackled 7
• Non-contact 2
• Blocked 10» “Cut” 3
• Tackled 7
• Non-contact 2
• Game 14
• Practice 5
• 4/11 on special teams
• Game 14
• Practice 5
• 4/11 on special teams
NFL ExperienceSurface
NFL ExperienceSurface
• Grass 12
• Turf 7» Field 4
• Grass 12
• Turf 7» Field 4
» Astro 3 » Astro 3

6/10/2011
7
Key to successKey to success
• Accurate diagnosis» Understand anatomy
» Careful physical exam
» Appropriate imaging
• Accurate diagnosis» Understand anatomy
» Careful physical exam
» Appropriate imaging» Appropriate imaging
• Treatment options» Conservative
» Surgical
» Acute
» Immediate
» Delayed
» Appropriate imaging
• Treatment options» Conservative
» Surgical
» Acute
» Immediate
» Delayed
Questions to be AnsweredQuestions to be Answered
• Timing of Surgery» Acute vs. delayed (criteria?)
» Medial vs. lateral (different?)
» Role for non-op treatment of MCL?
• Timing of Surgery» Acute vs. delayed (criteria?)
» Medial vs. lateral (different?)
» Role for non-op treatment of MCL?
• Repair vs. Reconstruction» Cruciates
» Collaterals
• Peroneal nerve / Vascular exam
• Rehabilitation philosophy
• Return to play criteria
• Repair vs. Reconstruction» Cruciates
» Collaterals
• Peroneal nerve / Vascular exam
• Rehabilitation philosophy
• Return to play criteria
Surgical DecisionsSurgical Decisions
• Timing
• Immediate» Open dislocation
• Timing
• Immediate» Open dislocation
» Vascular injury
» Repair collaterals
» Delay cruciates
» Uncontrolled instability
» Ex-fix x 5-10 days
» Vascular injury
» Repair collaterals
» Delay cruciates
» Uncontrolled instability
» Ex-fix x 5-10 days

6/10/2011
8
Surgical DecisionsSurgical Decisions
• Acute <14 days
» Lateral side + ACL or PCL
» ACL/PCL, PLC or MCL III
All t lli t b id
• Acute <14 days
» Lateral side + ACL or PCL
» ACL/PCL, PLC or MCL III
All t lli t b id• Allow acute swelling to subside
• Restore ROM!
• Give capsule chance to seal
• Collaterals easier to repair
• PLC typically tears distally, retracts proximally and scars
• Allow acute swelling to subside
• Restore ROM!
• Give capsule chance to seal
• Collaterals easier to repair
• PLC typically tears distally, retracts proximally and scars
Surgical DecisionsSurgical Decisions
• Elective
• ACL/PCL with MCL grade I, II » Allow MCL to heal
• Elective
• ACL/PCL with MCL grade I, II » Allow MCL to heal
» Reconstruct (not “repair”) cruciates
• Grade III MCL» Distal tears can retract
» Stenner lesion of knee
» Poor healing, chronic instability
» Check stability after cruciate reconstruction
» Reconstruct (not “repair”) cruciates
• Grade III MCL» Distal tears can retract
» Stenner lesion of knee
» Poor healing, chronic instability
» Check stability after cruciate reconstruction
Graft ChoicesGraft Choices
•• AutograftAutograft»» RareRare
»» Usually only for lateral sideUsually only for lateral side
•• AllograftAllograft
•• AutograftAutograft»» RareRare
»» Usually only for lateral sideUsually only for lateral side
•• AllograftAllograft»» CruciatesCruciates
»» CollateralsCollaterals
»» PMC, PLCPMC, PLC
•• Chronic casesChronic cases»» Generally poorer resultsGenerally poorer results
»» Compomised secondary restraintsCompomised secondary restraints
»» Err on side of more reconstructions (“corners”)Err on side of more reconstructions (“corners”)
»» CruciatesCruciates
»» CollateralsCollaterals
»» PMC, PLCPMC, PLC
•• Chronic casesChronic cases»» Generally poorer resultsGenerally poorer results
»» Compomised secondary restraintsCompomised secondary restraints
»» Err on side of more reconstructions (“corners”)Err on side of more reconstructions (“corners”)
6/10/2011
9
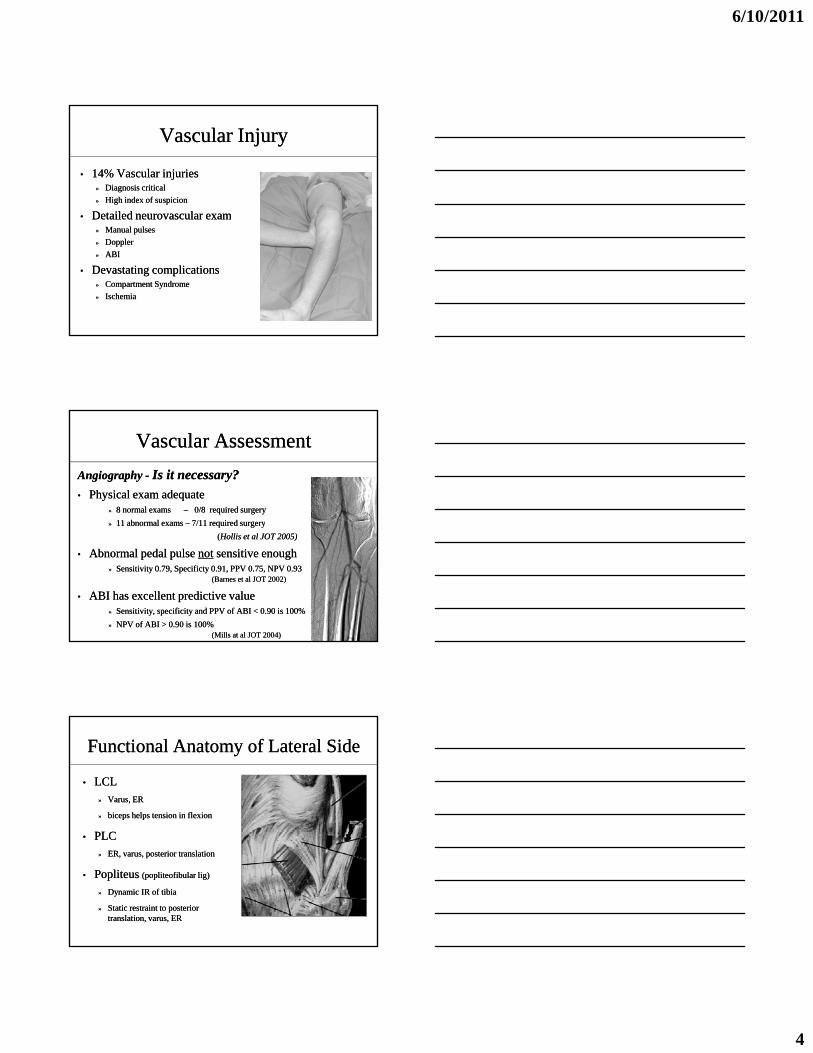
My (Current) PCL PreferenceMy (Current) PCL Preference
• Trans-tibial tunnel
• Single bundle
• Achilles allograft
• Trans-tibial tunnel
• Single bundle
• Achilles allograftgg
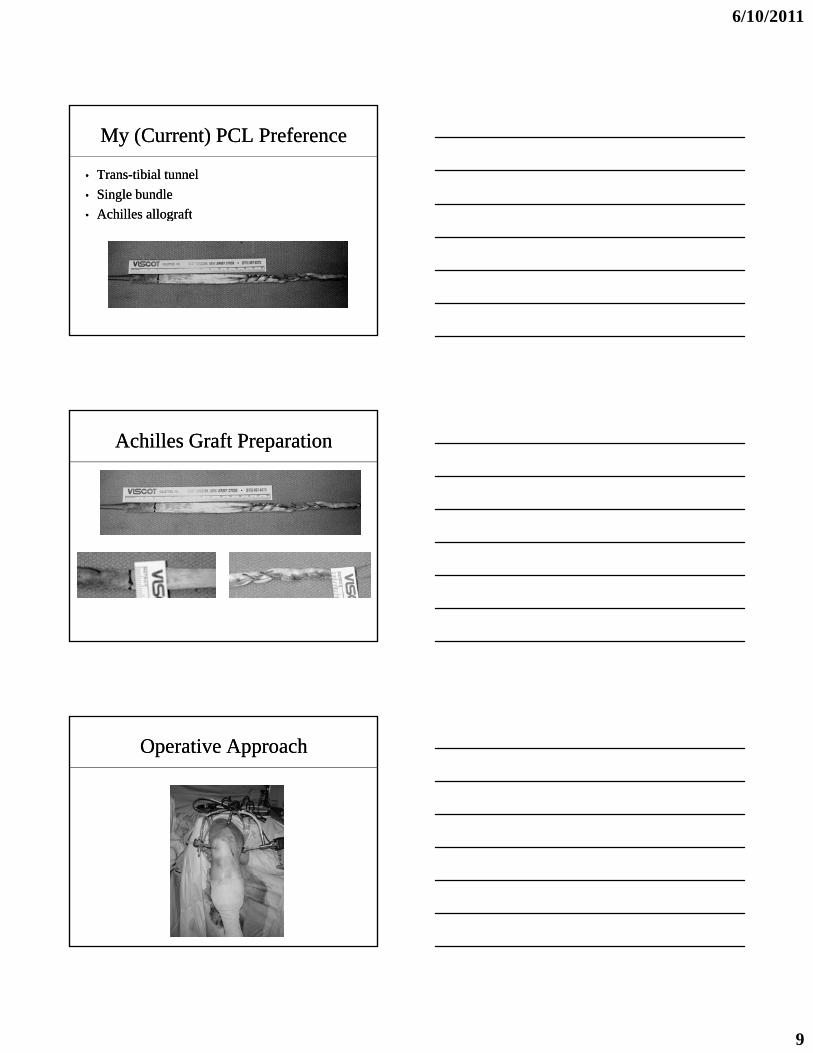
Achilles Graft PreparationAchilles Graft Preparation
Operative ApproachOperative Approach
6/10/2011
10
Establish PM PortalEstablish PM Portal
Expose Posterior TibiaExpose Posterior Tibia
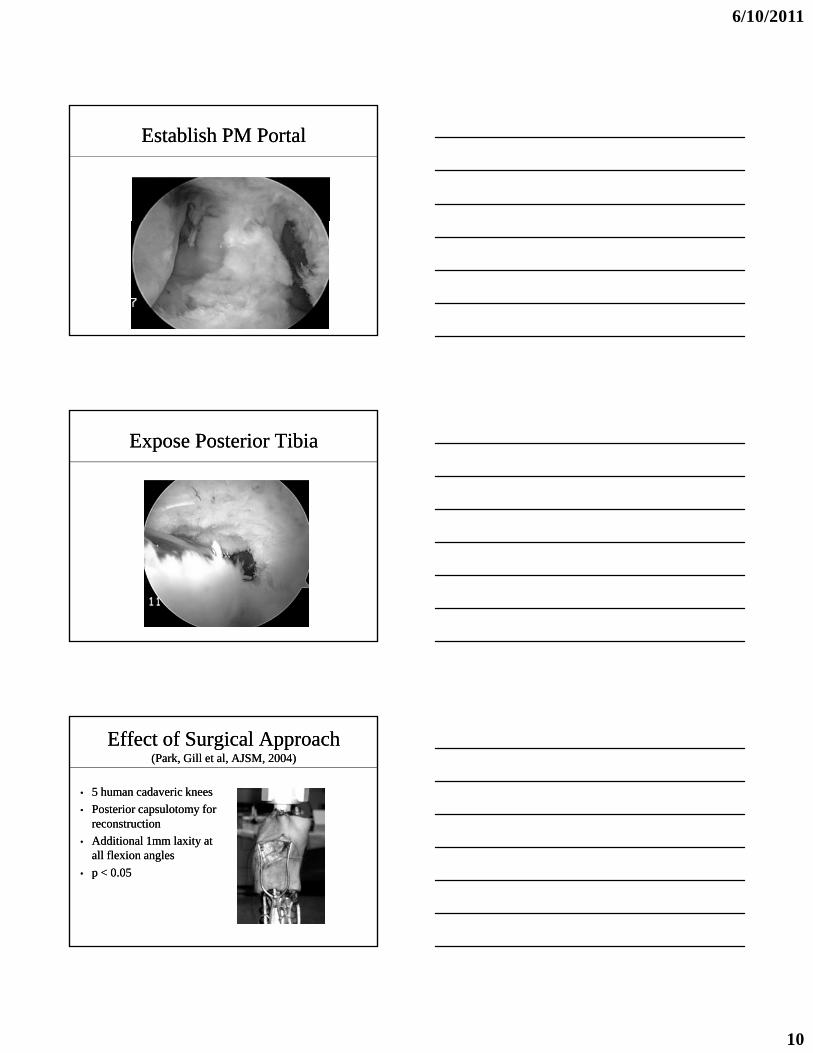
Effect of Surgical Approach(Park, Gill et al, AJSM, 2004)
Effect of Surgical Approach(Park, Gill et al, AJSM, 2004)
• 5 human cadaveric knees
• Posterior capsulotomy for reconstruction
• 5 human cadaveric knees
• Posterior capsulotomy for reconstruction
• Additional 1mm laxity at all flexion angles
• p < 0.05
• Additional 1mm laxity at all flexion angles
• p < 0.05

6/10/2011
11
Influence of Tibial Tunnel Position
Influence of Tibial Tunnel Position
• Just lateral to midline
• 10mm distal to joint surface
• 70 degree angle
Medial tunnel
Lateral tunnel
Knee center
Placement of Tibial GuidePlacement of Tibial Guide
Drilling Tibial TunnelDrilling Tibial Tunnel

6/10/2011
12
Drilling Tibial TunnelDrilling Tibial Tunnel
PCL Femoral TunnelPCL Femoral Tunnel
• Femoral tunnel» “2-incision” avoids killer angle
» Half-way from medial trochlea to epicondyle
• Femoral tunnel» “2-incision” avoids killer angle
» Half-way from medial trochlea to epicondyle
» Stay proximal
» 6mm posterior to articular surface
» 12:30pm
» Stay proximal
» 6mm posterior to articular surface
» 12:30pm
Femoral Guide PlacementFemoral Guide Placement

6/10/2011
13
Suture PasserSuture Passer
Passing GraftPassing Graft
Graft Fixation:Does Location Matter?
Graft Fixation:Does Location Matter?
• 5 human cadaveric Achilles tendons
• 3 different lengths studied» 75mm (long) = mid-tunnel fixation for TTT
» 48mm (medium) = inlay tibia mid femur
• 5 human cadaveric Achilles tendons
• 3 different lengths studied» 75mm (long) = mid-tunnel fixation for TTT
» 48mm (medium) = inlay tibia mid femur» 48mm (medium) = inlay tibia, mid-femur
» 34mm (short) = articular fixation
» 48mm (medium) = inlay tibia, mid-femur
» 34mm (short) = articular fixation
(DeFrate, AJSM, 2004)

6/10/2011
14
Optimal Graft LengthOptimal Graft Length
• MTS
• Preconditioned
• Displaced at 100 mm/min
• MTS
• Preconditioned
• Displaced at 100 mm/min
Crosshead
Clamp
• 400N load applied
• Force-displacement data
• Linear stiffness at each length
• 400N load applied
• Force-displacement data
• Linear stiffness at each lengthBone Cement
Graft
Optimal Graft LengthOptimal Graft Length
• Increasing length caused decrease in stiffness of 29±30%
f l iff
• Increasing length caused decrease in stiffness of 29±30%
f l iff250300350400450
(N)
Long Medium Short
• Long graft 85±28% less stiff than short graft
• All diffs p<0.05
• Consider your fixation site!
• Long graft 85±28% less stiff than short graft
• All diffs p<0.05
• Consider your fixation site!
050
100150200250
0 2 4 6Elongation (mm)
Fo
rce
(
Figure 2. Force-elongation curve
Linear Stiffness of Grafts
150
200
250
s (N
/mm
)
**
0
50
100
150
Short Medium Long
Lin
ear
Sti
ffn
ess

6/10/2011
15
Clinical SignificaneClinical Significane
• Two tibial screws to shorten effective length
• Composite screw posteriorly (60mm)
M l i l
• Two tibial screws to shorten effective length
• Composite screw posteriorly (60mm)
M l i l• Metal screw anteriorly
• ? Need for Inlay
• Metal screw anteriorly
• ? Need for Inlay
ACLACL
• Single Bundle
• Patellar tendon allograft
• Single Bundle
• Patellar tendon allograft
ACL Tibial TunnelACL Tibial Tunnel
• 50-55 degree angle
• 2 cm bone bridge
• Medial on anterior tibia
• 50-55 degree angle
• 2 cm bone bridge
• Medial on anterior tibia
• Just posterior to AHLM• Just posterior to AHLM

6/10/2011
16
ACL Femoral TunnelACL Femoral Tunnel
• “Anatomic position”
• Low on notch (10 o’clock)
• 2-pin passer
• “Anatomic position”
• Low on notch (10 o’clock)
• 2-pin passer
• Composite screw• Composite screw
LCLLCL
• Approach depends on location of tear
• Usually avulsed with biceps
• Primary repair preferred
• Approach depends on location of tear
• Usually avulsed with biceps
• Primary repair preferred
LCL / PLC RepairLCL / PLC Repair
• LCL and biceps form “V”
• Tag peroneal nerve
• Whipstich tendon
• 3 drill holes (2 0mm)
• LCL and biceps form “V”
• Tag peroneal nerve
• Whipstich tendon
• 3 drill holes (2 0mm)• 3 drill holes (2.0mm)
• Popliteus
• Capsule!!» Arcuate ligaments
• 3 drill holes (2.0mm)
• Popliteus
• Capsule!!» Arcuate ligaments

6/10/2011
17
LCL / PLC ReconstructionLCL / PLC Reconstruction
• Mid-substance tear
• Split Achilles allograft
• Drill hole (5mm) in fibular head
• Popliteal by-pass
• Mid-substance tear
• Split Achilles allograft
• Drill hole (5mm) in fibular head
• Popliteal by-passPopliteal by passPopliteal by pass
LCL / PLC ReconstructionLCL / PLC Reconstruction
• “Docking” procedure (Asnis technique)
• Tibialis anterior allograft
• Pass P to A through fib head
• “Docking” procedure (Asnis technique)
• Tibialis anterior allograft
• Pass P to A through fib head• Pass P to A through fib head
• “Dock” free ends into 8mm tunnel
• Interference screw
• Tie free ends medially over bridge
• Pass P to A through fib head
• “Dock” free ends into 8mm tunnel
• Interference screw
• Tie free ends medially over bridge
MCL RepairMCL Repair• < 2-3 weeks
• Femoral avulsion
» Beware stiffness
• Tibial avulsion
• < 2-3 weeks
• Femoral avulsion
» Beware stiffness
• Tibial avulsion• Tibial avulsion
» Beware laxity
• Bone screw
• Suture anchors
• Don’t forget PM Corner / POL!!
• Tibial avulsion
» Beware laxity
• Bone screw
• Suture anchors
• Don’t forget PM Corner / POL!!

6/10/2011
18
MCL ReconstructionMCL Reconstruction
• Check after other procedures done
• Rare
• Be prepared
I
• Check after other procedures done
• Rare
• Be prepared
I• Isometry
• Capsule
• Stiffness…
• Isometry
• Capsule
• Stiffness…
Order and Method of FixationOrder and Method of Fixation
• Pass PCL» Fix femoral side with composite screw
• Pass ACL» Fix femoral side with composite screw
• Pass PCL» Fix femoral side with composite screw
• Pass ACL» Fix femoral side with composite screw
• Fix PCL tibial tunnel» 90 degrees, anterior drawer
» Composite screw posteriorly (60-65mm)
» Metal screw anteriorly
• Fix ACL tibial tunnel» Full extension (!)
» Metal screw
• Fix PCL tibial tunnel» 90 degrees, anterior drawer
» Composite screw posteriorly (60-65mm)
» Metal screw anteriorly
• Fix ACL tibial tunnel» Full extension (!)
» Metal screw
Order and Method of FixationOrder and Method of Fixation
• LCL with valgus stress» #2 fiberwire
» Composite screw and medial bridge
• LCL with valgus stress» #2 fiberwire
» Composite screw and medial bridge

6/10/2011
19
Order and Method of FixationOrder and Method of Fixation
• MCL» Check isometry
» Anterior limb to tibia
» Posterior limb to POL
• MCL» Check isometry
» Anterior limb to tibia
» Posterior limb to POL
Ten Commandments of Knee Dislocations(modified from Schenk, 2001)
Ten Commandments of Knee Dislocations(modified from Schenk, 2001)
1. …treat all traumatic PCL + collateral ligament injuries as potential knee dislocations
2. …classify by anatomy rather than direction
1. …treat all traumatic PCL + collateral ligament injuries as potential knee dislocations
2. …classify by anatomy rather than direction
Thou Shalt…
2. …classify by anatomy rather than direction3. …use angiography appropriately4. …use MRI for preoperative planning 5. …apply external fixators liberally in polytrauma 6. …repair collateral ligamentous avulsions7. …use allografts liberally8. …fix what’s torn9. …restore ROM pre-operatively when possible10. …individualize rehabilitation program
2. …classify by anatomy rather than direction3. …use angiography appropriately4. …use MRI for preoperative planning 5. …apply external fixators liberally in polytrauma 6. …repair collateral ligamentous avulsions7. …use allografts liberally8. …fix what’s torn9. …restore ROM pre-operatively when possible10. …individualize rehabilitation program
RehabilitationRehabilitation• Brace in full ext / quad rehab 2 - 4 wks
• Protected ROM 4 - 8 wks
• Crutches 6 - 8 wks
• PREs 8 wks
S t 9 12
• Brace in full ext / quad rehab 2 - 4 wks
• Protected ROM 4 - 8 wks
• Crutches 6 - 8 wks
• PREs 8 wks
S t 9 12• Sports 9 - 12 mo• Sports 9 - 12 mo

6/10/2011
20
Multi-Ligament InjuriesMulti-Ligament Injuries
• Conclusions» Complex cases
» Very challenging
» Fraught with pitfalls and complications
• Conclusions» Complex cases
» Very challenging
» Fraught with pitfalls and complicationsg p p
» Understand the anatomy
» Fix what’s torn
» Have a plan
» Don’t rush rehab!!
» 1 year to return…
g p p
» Understand the anatomy
» Fix what’s torn
» Have a plan
» Don’t rush rehab!!
» 1 year to return…