management presentation february 2017 - … · 2 safe-harbor statement this presentation contains...
TRANSCRIPT

M A N A G E M E N T P R E S E N TAT I O N
F E B R U A RY 2 0 1 7
N A S D A Q : A R D M

2
Safe-Harbor Statement
This presentation contains forward-looking statements that are based on Aradigm’s current expectations and beliefs and are subject to anumber of risks, uncertainties, and assumptions that could cause actual results to differ materially from those described. All statements,other than statements of historical fact, are statements that could be deemed forward-looking statements, including estimates of revenues,operating margins, capital expenditures, cash, the extent of cash needs and the sufficiency of cash resources, other financial metrics,expected legal, arbitration, political, regulatory, or clinical results, and other such estimates and results. Forward-looking statements involvesignificant risks and uncertainties, including those discussed below and more fully described in the Securities and Exchange Commission(SEC) reports filed by Aradigm (Nasdaq: ARDM), including Aradigm’s most recent annual report on Form 10-K and most recent periodicreports on Form 10-Q and Form 8-K. Please refer to Aradigm’s most recent Forms 10-K, 10-Q, and 8-K for additional information on theuncertainties and risk factors related to our business. Unless otherwise noted, Aradigm is providing this information as of February 2, 2017and expressly disclaims any duty to update information contained in this presentation.
No forward-looking statement can be guaranteed and actual results may differ materially from those we project. Aradigm’s results may beaffected by our ability to successfully develop, partner and market our products domestically and internationally, difficulties or delays inmanufacturing our products, and regulatory developments (domestic or foreign) involving current and future products and manufacturingfacilities. Discovery or identification of new product candidates cannot be guaranteed and movement from concept to product is uncertain;consequently, there can be no guarantee that any particular product candidate will be successful and become a commercial product. Evenif product candidates appear promising at various stages of development, they may not reach the market or may not be commerciallysuccessful for a number of reasons. Such reasons include, but are not limited to, the possibilities that the potential products may be foundto be unsafe in animal or human trials, ineffective during clinical trials, may fail to receive necessary regulatory approvals, may be difficult tomanufacture on a large scale, are uneconomical to market, may be precluded from commercialization by proprietary rights of third parties,may not be purchased by government organizations for biodefense, or may not gain acceptance from health care professionals andpatients. In addition, while we routinely obtain patents for our products and technology, the protection offered by our patents and patentapplications may be challenged, invalidated, or circumvented by our competitors. Our business may be impacted by governmentinvestigations, litigation, and products liability claims.
Aradigm, Lipoquin, Pulmaquin and the Aradigm Logo are registered trademarks of Aradigm Corporation.Other names and brands may be claimed as the property of others.

Investment Opportunity
Opportunity Serving UnmetMedical Need with Long-dated Intellectual Property, Regulatory Protections and Follow-on Opportunities for Other Indications
Aradigm’s lead product candidate Pulmaquin is being developed for the unmet medical need of non-cystic fibrosis bronchiectasis (“NCFBE”) with chronic Pseudomonas aeruginosa (“PA”) infections projected by equity analysts to reach ~$1B1 in US and EU revenues by 2022 with a prevalent patient population of ~445,000 adults in these two markets
Pivotal topline Phase 3 data released on December 1, 2016 FDA pre-NDA meeting held on December 20, 2016 to discuss the application for approval of Pulmaquin
and seek additional FDA guidance; follow on meeting with FDA is scheduled, with discussions for EU approval to follow
The product has Orphan Drug, Qualified Infectious Disease Product and Fast Track designations Pulmaquin has a strong suite of intellectual property with multiple patents and patent families providing
worldwide protection through 2031 A Biodefense product candidate with compelling animal data has an abbreviated path to approval
and is being funded by DTRA through a recently awarded contract with the U.K. Defence Science and Technology Laboratory
Expansion into other diseases such as non-tuberculous mycobacteria (“NTM”) and cystic fibrosis could provide significant additional sales and could be accelerated by Pulmaquin Phase 3 data
Global Marketing Partner
Partnered with Grifols S.A. – a global biopharmaceutical company with a well-established US andEuropean specialty respiratory salesforce currently marketing Prolastin C, the leading alpha-1 antitrypsin (“A1AT”) product in the United States and having a 67% market share globally in 2016
ExperiencedManagement team
Aradigm’s executive and senior management has extensive experience in dealing with U.S. and European regulators
Orphan drug and QIDP designations for Pulmaquin have allowed for frequent and productive FDA interactions
Strong CMC focus with experience in liposomal manufacturing and aerosol R&D
Pulmaquin® - A unique proprietary product for multiple indications
3
1Ladenburg, March 2016

Snapshot of Aradigm
Founded 1991
Headquarters Hayward, CA
Employees 25
Worldwide PulmaquinPatent Expiry
Strong IP protection through 2031; 7 issued patents in US; 39 patents issued abroad
Aradigm is an emerging specialty pharmaceutical company developing and commercializing a portfolio of drugs delivered by inhalation for the treatment of severe respiratory disease
Shares outstanding(9/30/2016) 15 million
Market Capitalization(9/30/2016)(12/02/2016)
$102.8 million$32.1 million(1)
Cash Balance (9/30/2016) $28.5 million
Debt (9/30/2016) $12.8 million
Key Statistics Financial Summary
Attractive Development Pipeline
Condition Product Pre-clinical Phase 1 Phase 2a Phase 2b Phase 3
Non-CF Bronchiectasis
ARD-3150(Pulmaquin)
Cystic FibrosisARD-3100
(Lipoquin®)
Biodefense(2) ARD-1100(Pulmaquin, Lipoquin)
Non-Tuberculosis Mycobacteria
Pulmaquin, Lipoquin
Completed
Successful rodent studies
Promising preclinical data
Protocols in development for approval under the “Animal Rule”
Completed
(1) The average size of trades on the day following the release of Phase 3 data was 365 shares, with fewer than 100,000 shares of the ~1,475,000 shares being block trades(2) Indications include Tularemia, Plague, Melioidosis and Q-Fever; NIH-funded diagnostic program in humans underway as well.
ARDM will propose studies as part of Paediatric Investigation Plan for MAA
Sub group analysis of patients with NTM in completed Phase 3 BE studies will be informative
4

Experienced Executive Management Team with Excellent FDA Track Record
BackgroundTeam Member Title
Chief Medical Officer
President & Chief Executive Officer
Chief Financial Officer
Igor Gonda, Ph.D.
Juergen Froehlich, MD, MBA, FCP
Nancy Pecota
20+ years of experience in respiratory disease Has served as Aradigm’s President and CEO since 2006, and as a director since 2001 Previously served as CEO of Acrux Limited, a publicly traded specialty pharmaceutical company
located in Australia Former Senior Scientist and Group Leader at Genentech, leading inhalation development of
Pulmozyme and other products for severe respiratory disease
25+ years of industry experience in preclinical, clinical and regulatory activities Has held a variety of positions at major pharmaceutical companies involved in the commercialization
of various drugs and biologics and alliance activities with other companies. Past positions include: Vertex, Vice President and Head, Global Regulatory Affairs; Ipsen, Vice President, Clinical and Developmental Pharmacological Sciences; and BMS, Vice President, Global Medical Affairs – Sanofi Alliance
Currently a diplomat of the American Board of Clinical Pharmacology, a fellow of the American College of Clinical Pharmacology and a fellow of the Faculty of Pharmaceutical Medicine
20+ years of experience in corporate accounting and operations management Previously served as CFO for NuGEN Technologies, a life sciences tools company that provides
specialty reagents to pharmaceutical and diagnostics companies Prior to that, served as a financial consultant to early- and mid-stage life sciences companies
5
Experienced Senior Management Team in CMC, Liposomes and Aerosol R&D
BackgroundTeam Member Title
VP, Quality and Regulatory (CMC)
VP, Preclinical R&D
Bob Reed, Ph.D.
David Cipolla, Ph.D.
25+ years of industry experience in chemistry, manufacturing and control (CMC) guiding API development, drug product design and development, pharmaceutical product and process characterization, technology transfer and regulatory strategy and submissions, including 10 years with liposomal products
Has held a variety of positions (10+ years at VP level) at Merck and other global pharmaceutical and biotechnology companies including: Celsion, Vice President, CMC and Technical Operations; XenoPort, Vice President, Pharmaceutical Operations; and The Liposome Company, Research Scientist
Has supported the commercialization of over 25 drug products American Association of Pharmaceutical Scientists Fellow; Industry Advisory Board to University of the
Pacific School of Pharmacy
20+ years of industry experience in R&D, especially inhalation products and liposomes Chaired the International Pharmaceutical Aerosol Consortium on Regulation and Science (IPAC-RS) Chaired the International Society for Aerosols in Medicine (ISAM) Regulatory Affairs Working Group
and was an ISAM board member
VP, Project ManagementJanice Dahms 25+ years in product development, project and portfolio management, alliance management 10+ years as Executive Director or higher Experience extends from discovery through commercial launch Supported the development and approval of 6 marketed products
6

Recent and Upcoming Milestones
Accomplished and Near-term Milestones
Because of Orphan Drug and QIDP designations Aradigm has had the opportunity for frequent interactions with FDA as Pulmaquin has progressed through its development in the unmet medical need of NCFBE
Date Milestone
December 2016 Pre-NDA meeting held with FDA to review Phase 3 data; follow on meeting with FDA isscheduled
H1 2017 Planned submission of NDA to FDA
H2 2017 Planned submission to EMA for regulatory approval
H2 2017 Anticipated US approval of Pulmaquin for chronic treatment of NCFBE
2018 Anticipated EU approval of Pulmaquin for chronic treatment of NCFBE
7

Partnership with Grifols, S.A.
Founded 1940
Headquarters Barcelona, Spain
Employees 14,600
Strengths Prolastin (A1AT deficiency) has 67% global market share and leading market share in the US
Significant specialty respiratory salesforce in place in both US and Europe
Grifols (BME:GRF) is a biopharmaceutical company that develops, manufactures and distributes plasma derivative and respiratory products in the US and internationally
LTM Sales (9/30/2016) $4,512 million
Market Capitalization(12/02/2016) $12,012 million
Cash Balance (9/30/2016) $1,012 million
Debt (9/30/2016) $5,227 million
Key Statistics Financial Summary
Key Licensing Agreement Terms
Royalty Highlights Grifols will pay Aradigm tiered royalties on worldwide sales of products utilizing Aradigm's proprietary inhaled
ciprofloxacin formulations, plus additional payments based on specific milestones achieved
The royalty rate is 12.5% on the first $300 million of annual sales for all territories and all indications, and 20% for annual sales in excess of $300 million
The royalty rate is subject to a 50% reduction in a given country if a competitive product is approved in that country, defined as any inhaled liquid liposomal product containing ciprofloxacin
Royalties will be paid in a given country until the later of (i) patent / Orphan Drug expiry and (ii) a 10-year term from first commercial sale in that country
Collaboration Highlights Grifols was responsible for (i) all development and clinical expenses up to $65 million for the NCFBE indication and
(ii) the funding of expenses for all other indications in all territories (except for Biodefense)
Grifols is responsible for all commercialization activities, while Aradigm is responsible for manufacturing of drug product which will be sold to Grifols on a cost plus 5% margin basis
In conjunction with the licensing agreement, Grifols acquired 35% of Aradigm's common stock on a fully diluted basis for a total investment of ~$26 million on August 27, 2013
In conjunction with Aradigm’s 2016 debt financing, Grifols acquired ~$19 million in senior convertible notes due 2021 and related warrants.
Milestone Event Payment
Initiation of Phase3 clinical study $5,000,000
First filing of NDA in US or EU $5,000,000
US Regulatory Approval $5,000,000
EU Regulatory Approval $5,000,000
China Regulatory Approval $2,500,000
Japan Regulatory Approval $2,500,000
8
Key Investment HighlightsAradigm is well-positioned to generate significant royalty payments due to the ability of Pulmaquin to reduce both the morbidity and mortality of NCFBE patients with PA and the high treatment costs
Aradigm believes the NCFBE indication for Pulmaquin will exceed $500MM of sales by 2021 Ladenburg analyst projects $1B sales by 2022; Nektar
projects $750 million for their product with Bayer
Approvable endpoint achieved in ORBIT-2 –Phase 2b trial Increase in time to exacerbation is beneficial for payors
and patients
Good pulmonary safety and tolerability
US Orphan Drug Designation with no existing approved therapies
Top line Phase 3 data released in December 2016 Safety and efficacy data consistent with ORBIT-2
Persistent strong anti-pseudomonal activity
Pre-NDA meeting with FDA to discuss Phase 3 data and application for approval held in December 2016; second meeting in Q1’17
QIDP Designation and Fast Track received FDA priority review accompanies QIDP designation
Sole competitor: Bayer’s twice daily, dry powder inhaled ciprofloxacin in Phase 3 “Unencapsulated” inhaled antibiotics TOBI, Cayston and
colistin have failed in all NCFBE trials
Bayer’s first Phase 3 showed efficacy with 14 day BID cycles and failed with 28 day cycles; second Phase 3 trial results not released yet
Strong IP protection to 2031 7 patents issued in US; 39 issued patents in geographies
outside the US; plus additional patent applications pending across 20 countries
Pulmaquin once daily, with Aradigm’s unique approach: Potent antibacterial compound
Active in biofilm
Uptake by macrophages
Key Investment Highlights
9

Overview of Pulmaquin

No inhaled antibiotics approved for any disease other than Cystic Fibrosis (CF)
CF: approved inhaled antibiotics for chronic treatment of PArespiratory infections – TOBI, Cayston, Colistin
Many unsuccessful attempts with unencapsulated inhaled antibiotics in NCFBE and COPD Tobramycin (“TOBI”) Aztreonam (“Cayston”) Gentamicin Colistin
The common denominator appears to be the airway irritation caused by the unencapsulated antibiotics in NCFBE patients outweighing the benefits of the desirable antibacterial activity
Choice of drug: Ciprofloxacin Broad spectrum antibiotic – different class from approved
inhaled antibiotics, no cross-resistance Requires chronic use as PA will cause reinfection if only
treated acutely Choice of delivery: Inhalation
Rapid onset of action followed by sustained high antibiotic concentrations well above the minimal inhibitory concentration (MIC) at the sites of infections
Low blood levels – lower risk of systemic side effects and resistance
Oral and IV antibiotic treatments – negative side effects and lack of chronic suppression of PA due to high systemic concentrations, lack of durable concentrations above MIC to control “resistant” bacteria
Choice of formulation: Liposomal Encapsulation Slow release – once daily dosing Improves respiratory tolerability Facilitates penetration into microbial biofilms (PA, NTM
including M. abscessus) Enables treatment of intracellular infections (NTM, plague,
tularemia)
Pulmaquin Value Proposition
AdvantagesInhaled Antibiotics
Current acute treatment modalities with oral or IV antibiotics unable to eradicate PA, therefore only chronic treatment with an inhaled antibiotic is expected to keep PA under control long term
11

Pulmaquin Value Proposition (cont.)
Pulmaquin
Lipoquin ARD-3100 Pari LC Sprint Nebulizer
Inhaled once daily usingFDA-approved Pari LC Sprint NebulizerLiposome
(cross-section)
Ciprofloxacin
Lipoquin - CFI(Initial formulation)
Lipoquin ARD-3100
Ciprofloxacin
Pulmaquin ARD-3150
Superior antibacterial activity in sputum plus anti-inflammatory effect
Pulmaquin is a proprietary combined formulation of encapsulated and un-encapsulated ciprofloxacin that is designed to be inhaled once daily using a common and easy to use nebulizer that even patients with severely impaired lung function can use
Pulmaquin
12

Sustained Ciprofloxacin Levels in SputumVery high sustained Ciprofloxacin levels in sputum are maintained by Pulmaquin and are unachievable with oral or IV ciprofloxacin
Ciprofloxacin Concentrations in Sputum
00 55 1010 1515 2020 2525 3030
Time from last dose (hours)
10
1000
100
Cip
roflo
xaci
n (µ
g/m
l spu
tum
)
Patient 1
Patient 2
MIC(1)
(1) Moskowitz SM et al., (2004), J Clin Microb 42:1915-1922.(2) Smith MJ et al, (1986), Antimicrobial Agents and Chemotherapy, Oct 1986, p. 614-616.(3) Kontou et al. Antimicrobial Agents and Chemotherapy, Sept. 2011, p. 4149–4153.
Oral Ciprofloxacin(2)
Pulmaquin
The Minimum Inhibitory Concentration (MIC) of ciprofloxacin in sputum required to inhibit PA bacterial biofilms is estimated at 4µg/ml(1)
Oral and IV ciprofloxacin regimens fail to achieve MIC levels in sputum at standard dosages
Once-daily Pulmaquin achieves very high ciprofloxacin concentration levels in sputum above MIC while minimizing systemic exposure
IV Ciprofloxacin(3)
4
13

BE is a severe obstructive lung disease caused by previous lung infections (incl. tuberculosis and non-tuberculous mycobacteria) or other conditions (CF, COPD, PCD, chronic aspiration)
Characteristic vicious cycle of lung injury, infection, inflammation, airflow obstruction leading to recurrent episodes of acute worsening (pulmonary exacerbations) and eventually death due to respiratory complications
NCFBE is characterized pathologically by airway inflammation and permanent bronchial dilatation based on CT imaging, and clinically by productive cough and recurrent respiratory infections
NCFBE: >152,000 patients in US, >293,000 in EU who are not CF patients and whose disease is unlikely to be caused by smoking
~ 1/3 of NCFBE patients has chronic PA infections
In US Aradigm has Qualified Infectious Disease Product (QIDP) designation and orphan drug designation for Pulmaquin in NCFBE patients chronically infected with PA
Even larger populations in Asia and other parts of the world
NCFBE Overview
Overview of Disease Pathology
(1) Am J Resp Crit Care Med 2013; 188.
Bronchiectasis(1) Normal
NCFBE is a severe lung disease affecting >445,000 patients in the US and EU; it is caused by previous lung infections and other conditions and characterized pathologically by airway inflammation and permanent bronchial dilatation
14

NCFBE Overview (cont.)
British Thoracic Society defines an exacerbation as an acute deterioration with increasing sputum volume and purulence and/or systemic upset(1)
~40% of patients experience 2+ exacerbations per year and these patients have >15% 4-year mortality(1)
Pulmonary exacerbations are a key reason for the high morbidity and mortality of the disease, and a high rate of hospitalizations
Average cost: $30-40K+ per hospitalized event(2,3,4)
Most exacerbations due to respiratory infections result in admission to ICU(2)
Average ICU costs estimated between $4K - $5K per day with an average stay of 8 – 14 days(3)
Agency for Healthcare Research and Quality (AHQR)(4):
Annual age-adjusted hospitalization rate: 16.5 per 100,000 population
Annual % increases in hospitalization from 1993 to 2006: 2.45% for men, 3.0% for women.
Women >60 had highest hospital admission rates(1) American Journal of Respiratory and Critical Care Medicine Volume 189 Number 5 | March 1 2014.(2) Alizaman et al. Chest, Oct 2016; 150#4S.(3) Dasta et al. Crit Care Med. 2005 Jun;33(6):1266-71.(4) Seitz et al. Chest 2010
No specific treatment is currently approved for chronic treatment to prevent or reduce the number of
pulmonary exacerbations
Exacerbations Drive the Health and Economic Impacts of NCFBE
Acute pulmonary exacerbations impact quality of life and drive expensive hospital admissions
15

NCFBE Overview (cont.)
TIME
Finch et al, 2015:3 times higher mortality,
6.5 fold increase in hospitalizations,worse quality of life
Chronic infection with PA
More exacerbations lead to more rapid decline in lung function, which in turn leads to overall increased morbidity and mortality
16
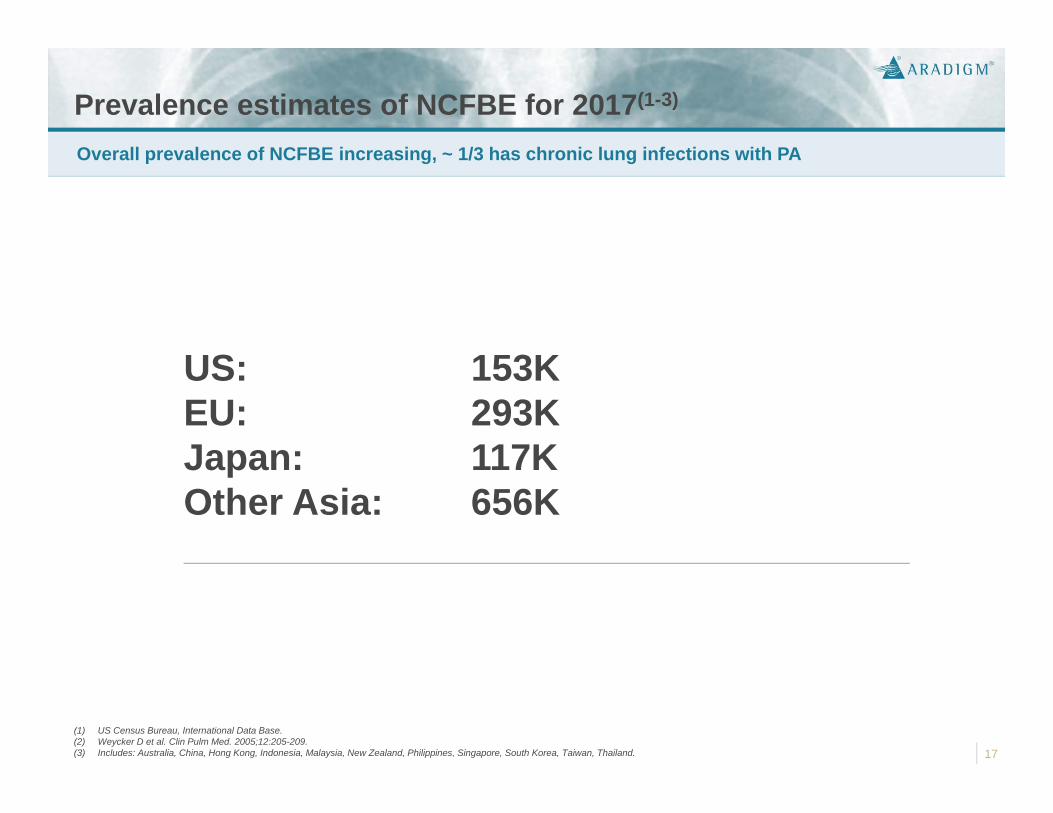
Prevalence estimates of NCFBE for 2017(1-3)
Overall prevalence of NCFBE increasing, ~ 1/3 has chronic lung infections with PA
(1) US Census Bureau, International Data Base.(2) Weycker D et al. Clin Pulm Med. 2005;12:205-209.(3) Includes: Australia, China, Hong Kong, Indonesia, Malaysia, New Zealand, Philippines, Singapore, South Korea, Taiwan, Thailand.
US: 153KEU: 293KJapan: 117KOther Asia: 656K
17

Clinical Development

NCFBE: Phase 2b ORBIT-2 StudyEnd point results were very similar to the Phase 3 trial, including excellent reduction in bacterial load of PA and 76 days of prolongation in median time to first PE with Pulmaquin
Endpoints Drug N = 20 Placebo N = 22
PA colony-forming units/Logs at 28 days (primary)
-4.44 (27,000 fold)
+0.13
Median time to first pulmonary event (secondary)
134 days 58 days
Required supplemental antibiotics (secondary)
7 patients 15 patients
Safety Better pulmonary adverse events profile in the treatment group vs. the placebo group
No significant change in lung function (FEV1)
No evidence of emergence of resistance
Randomized international double blind placebo controlled trial of once daily inhaled Pulmaquin (6 mL vs. matching placebo) of 3 cycles of 28 days on + 28 days off treatment in 42 adult BE patients
19

NCFBE: Phase 3 Study Design and ResultsAs in ORBIT-2, Pulmaquin demonstrated in the two Phase 3 studies, ORBIT-3 and ORBIT-4, good safety and tolerability. In all three trials, the median time to first PE increased by 2-3 months compared to placebo. The impact of Pulmaquin is particularly prominent on PEs that require treatment with antibiotics and/or hospitalizations (moderate and severe PEs).
Phase 3 – ORBIT-3 Phase 3 – ORBIT-4
Trial Design(1) 582 patients total (fully enrolled); 2:1 randomization on Pulmaquin:placebo
6 cycles of once daily treatment with Pulmaquin vs. placebo (6 x 28 days on + 28 days off for 48 weeks) + 28 days open label extension
Primary endpoint: time to first pulmonary exacerbation (“PE”)
Key secondary endpoint: frequency of pulmonary exacerbation’s over the 48 week study
Results Median time to first mild, moderate or severe PE was over 60% longer in the Pulmaquin treatment group as compared to the placebo group
There was a 13% reduction in the frequency of PE’s over the 48-week treatment period in the Pulmaquin treatment group as compared to the placebo group
Statistical analyses for both endpoints did not achieve significance
Median time to first mild, moderate or severe PE was over 40% longer in the Pulmaquin treatment group as compared to the placebo group
There was a 37% reduction in the frequency of PE’s over the 48-week treatment period in the Pulmaquin treatment group as compared to the placebo group
Statistical analyses for both endpoints achieved significance using non-stratified analysis (theStatistical Analysis Plan specified stratified analyses but some of the strata were too small for such analyses)
(1) The ORBIT-3 and ORBIT-4 pivotal trials were identical in design except for a pharmacokinetics sub-study that was conducted in one of the trials. 20

Consistent Prolongation of Time to First PE
ORBIT -2 ORBIT-3 ORBIT-4
Active(N= 20)
Placebo(N= 22)
Active(N=183)
Placebo(N=95)
Active(N=206)
Placebo(N=98)
Time to first PE (days) 134 58 221 135 230 163
Prolongation of median time to first PE (days)
76 85 67
Log rank p value
0.0461
0.05720.89203
0.731440.03563
0.06964
1Per Protocol Population; 2m-ITT; 3Non-stratified Analysis 4Stratified Analysis per the Statistical Analysis Plan
22
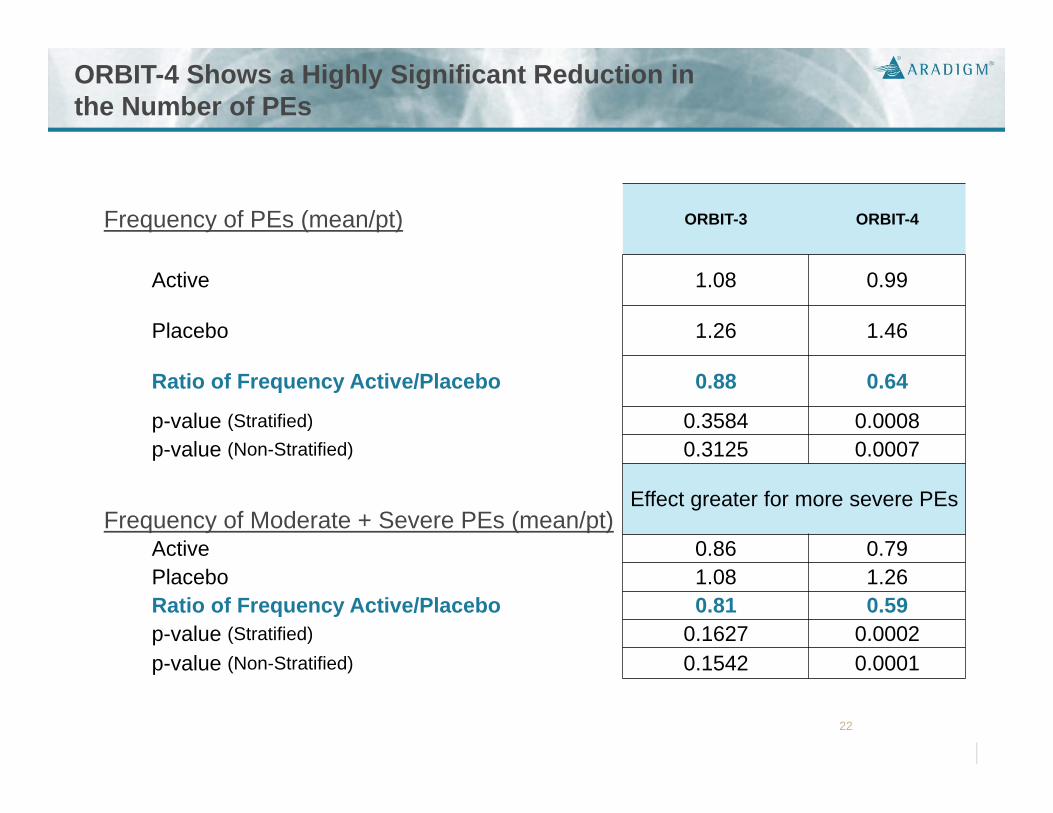
Frequency of PEs (mean/pt) ORBIT-3 ORBIT-4
Active 1.08 0.99
Placebo 1.26 1.46
Ratio of Frequency Active/Placebo 0.88 0.64
p-value (Stratified) 0.3584 0.0008p-value (Non-Stratified) 0.3125 0.0007
Frequency of Moderate + Severe PEs (mean/pt) Effect greater for more severe PEs
Active 0.86 0.79Placebo 1.08 1.26Ratio of Frequency Active/Placebo 0.81 0.59p-value (Stratified) 0.1627 0.0002p-value (Non-Stratified) 0.1542 0.0001
ORBIT-4 Shows a Highly Significant Reduction in the Number of PEs

Phase 3 Safety Results Safety SummaryPulmaquin was shown to be safe and well tolerated in both 48-week double blind Phase 3 studies, similar to the 6-month Phase 2 study
There were no differences in the changes of lung function (% FEV1 predicted and % FVC predicted) between the Pulmaquin and placebo groups at the end of the double-blind period and no airway irritation (in contrast to CF, lung function is not expected to improve but it is an important safety measure)
The incidence of all treatment emergent adverse events (“TEAE”) was similar between the Pulmaquin and placebo groups in both ORBIT-3 (Pulmaquin: 89.6%; placebo: 91.6%) and ORBIT-4 (Pulmaquin: 86.4%; placebo: 96.9%)
In ORBIT-3 the rates of serious TEAEs were 30.6% with Pulmaquin and 25.3% with placebo while in ORBIT-4 the rates were 17.0% versus 28.6%
The most frequently observed treatment related TEAEs were of respiratory / thoracic / mediastinal nature and were reported in ORBIT-3 by 25.7% of subjects with Pulmaquin and in 21.1% of subjects with placebo, while the rates in ORBIT-4 were 16.5% with Pulmaquin versus 19.4% with placebo
There were no deaths related to the study drug
8 treatment-unrelated deaths occurred in ORBIT-3 (Pulmaquin: 5 (2.7%); placebo: 3 (3.2%)) and 6 deaths in ORBIT-4 (Pulmaquin: 2 (1.0%); placebo: 4 (4.1%))
23

Other Indications and Products

Differentiating Characteristic Underlying the Severity
Patients Chronically Infected by PA
Severity of disease
Low PA burden High PA burden
Chronic PA infection is not isolated to BE patients – it is even more prevalent in CF patients, and its presence in COPD patients (although a relatively low percent) represents a large potential opportunity due to the large prevalence
Cystic FibrosisPA burden
(illustrative) 30,000
Non-CFBronchiectasis PA burden
(illustrative)>110,000
PA burden(illustrative)
30 million
Total US prevalence
COPD (chronic bronchitis,
emphysema)
25
Aradigm Opportunity in Pulmonary Non-TB Mycobacteria (“NTM”) According to the American Thoracic Society, the prevalence of NTM is believed to be greater than that of tuberculosis in the US; however, NTM is a smaller indication than NCFBE
2014 US direct medical costs of $1.7 billion, growing ~ 8% p.a.
(Strollo et al., Ann. Am. Thorac. Soc 2015 Oct;12(10):1458-64)
Frequent co-morbidity in NCFBE, CF and COPD
Almost all NTM patients have BE, ~ 30% have PA infections
Suspected to be one of the key causes of new cases of NCFBE in US
High morbidity and mortality
Current treatments have significant challenges with efficacy, emergence of resistance and tolerability, and the adherence to current guidelines is poor
Only 13% adhered to the treatment guideline for Mycobacterium Avium Complex (Adjemian J et al. Ann Am Thorac Soc 2014;11:9-16)
Burden of NTM
26
Aradigm has compelling preclinical efficacy in both M. avium and M. abscessus
Aradigm could discuss with FDA and enter directly into Phase 2b/3 program including both NTM pathogens
Differential pricing possible for NTM
NTM is expected to require continuous therapy with Pulmaquinuntil eradication of the bacteria is achieved (compared to chronic 28 day on/28 off treatment cycles to control PA)
Attractive Near-Term Option

Aradigm Opportunity in BiodefenseBARDA stocking orders are typically several hundred million dollars and represent a substantial future revenue potential
Aradigm’s inhaled liposomal ciprofloxacin has been demonstrated by scientists from the UK Defence Science and Technology Laboratory (“Dstl”) to be effective against several microbial threats in murine models:
Q-fever (Coxiella burnetii): mice were significantly protected against weight loss and showed no clinical signs of disease throughout the 14-day duration of the study (September 2012)
Pneumonic plague (Yersinia pestis): a single dose of Lipoquin administered 24 hours after exposure to a lethal dose provided full protection (November 2012)
Tularemia (Francisella tularensis): all the mice in the control group and the free ciprofloxacin group were dead within 11 days post-infection; in contrast, all the mice in the liposomal ciprofloxacin group were alive 14 days post-infection
Aradigm may be able to expeditiously complete development of liposomal ciprofloxacin for approval under the FDA’s “Animal Rule” regulations relating to new drugs or biologics for potentially fatal diseases where human studies cannot be conducted ethically or practically
These regulations allow a drug to be evaluated and approved by the FDA on the basis of demonstrated safety in humans (for which safety data from Aradigm’s NCFBE and CF programs may be used) combined with studies in animal models to show effectiveness
Aradigm intends to have liposomal ciprofloxacin considered under the Animal Rule for approval for use in prevention and treatment of a number of potential bioterrorism infections including anthrax, tularemia, Q fever and pneumonic plague
In October 2016, Aradigm announced that the UK Dstl received funding of up to $6.9 million from the US Defense Threat Reduction Agency (DTRA) for a research program investigating the efficacy of Pulmaquin and Lipoquin in animal models with respect to protection against biowarfare agents including tularemia, melioidosis, glanders and Q-fever
Biodefense Program
27
Key Investment HighlightsAradigm is well-positioned to generate significant royalty payments due to the ability of Pulmaquin to reduce both the morbidity and mortality of NCFBE patients with PA and the high treatment costs
Aradigm believes the NCFBE indication for Pulmaquin will exceed $500MM of sales by 2021 Ladenburg analysts project $1B sales by 2022; Nektar
projects $750 million for their product with Bayer
Approvable endpoint achieved in ORBIT-2 –Phase 2b trial Increase in time to exacerbation is beneficial for payors
and patients
Good pulmonary safety and tolerability
US Orphan Drug Designation with no existing approved therapies
Top line Phase 3 data released in December 2016 Safety and efficacy data consistent with ORBIT-2
Persistent strong anti-pseudomonal activity
Pre-NDA meeting with FDA to discuss Phase 3 data and application for approval held in December 2016; second meeting in Q1’17
QIDP Designation and Fast Track received FDA priority review accompanies QIDP designation
Sole competitor: Bayer’s twice daily, dry powder inhaled ciprofloxacin in Phase 3 “Unencapsulated” inhaled antibiotics TOBI, Cayston and
colistin have failed in all NCFBE trials
Bayer’s first Phase 3 showed efficacy with 14 day BID cycles and failed with 28 day cycles; second Phase 3 trial results not released yet
Strong IP protection to 2031 7 patents issued in US; 39 issued patents in geographies
outside the US; plus additional patent applications pending across 20 countries
Pulmaquin once daily, with Aradigm’s unique approach: Potent antibacterial compound
Active in biofilm
Uptake by macrophages
Key Investment Highlights
28