maternal - child health · 2016-05-28 · maternal - child health abnormal colonisation that occurs...
TRANSCRIPT

203
Maternal - Child Health
Infection prevention and control strategies for mother and child are based on the principle of combined care. In many birthing centres, the mother oft en labours, delivers, and recovers in the same room. Wherever possible the mother and child are cared for together. For neonates requiring intensive care, the newborn’s environment must be clearly delineated, with spatial separation between incubators. The sharing of equipment and supplies must be preceded by thorough cleaning, and appropriate disinfection/sterilisation. The blood and body fl uids of mother and child are assumed to be potentially infectious and standard precautions should be applied for all patient care.Prevention strategies include hand hygiene, patient hygiene, environmental cleaning and immunisation.
•
•
•
•
•
Key points
Chapter 14Maternal - Child
HealthSandra Callery
204
IFIC Basic Concepts of Infection Control
Background
The World Health Organization (WHO) estimates that approximately 210 million women become pregnant each year and that 529,000 die from complications. In the immediate post-partum period, sepsis and haemorrhage are the commonest causes of maternal death. 99% of these maternal deaths occur in developing countries.
Similarly, 99% of the estimated 4 million annual neonatal deaths occur in developing countries. Severe infections cause more than one-third of deaths; these are not always carefully recorded, however the commonest are likely to be sepsis, pneumonia, tetanus, and diarrhoea.1
Neonatal Risks and Infections
Neonatal infections occur in the fi rst 28 days of life.2 These infections may be contracted:
In utero, by the transplacental route.Intrapartum, when in contact with the maternal genital tract, blood, or stool.Postpartum, when in contact with the mother, family, and visitors, other neonates in the nursery, healthcare workers, or contaminated equipment.
Risk factors for neonatal infections include:Maternal infections Foetal gestational age at the time of the infectionComplications of delivery
o Invasive procedures and interventions, such as foetal monitoring devices
o Premature rupture of membranes > 24 hours. o Caesarean section delivery (associated with respiratory distress syndrome and possible infection).
Premature infants are at increased risk for infection due to:The absence of normal microbial fl ora which increases the risk of colonisation with pathogens.The colonisation of gastrointestinal fl ora (this risk diff ers between breast-fed babies versus formula-fed babies).
••
•
•••
•
•

205
Maternal - Child Health
Abnormal colonisation that occurs most oft en in newborns in neonatal intensive care units (NICU).Fragile, underdeveloped organs that normally provide a barrier to infectious pathogens, such as the skin and lining of the lung.A poor immune (antibody) response.
Common infections for full-term newborns are superfi cial infections of the skin, eye, and mucous membranes. Additional infections occur in intensive care, such as bacteraemia associated with central lines, pneumonia, and gastrointestinal infections. Microorganisms associated with neonatal infections include Staphylococcus aureus, coagulase negative staphylococci, Group B streptococci, Escherichia coli, and Candida. Other pathogens oft en associated with outbreaks in the nursery include Klebsiella, Serratia, Enterobacter, Citrobacter, and Pseudomonas species.2
Maternal Risks and Infections
Healthcare-associated maternal infections are acquired in hospital and did not exist before admission. These infections are typically att ributable to the health care sett ing up to 10 days post-partum. Most surgical site infections are considered healthcare-associated up to 30 days post procedure.3
Maternal risk factors for infection include: 1) prolonged rupture of membranes (>24 hours), 2) obesity (interferes with wound healing), 3) diabetes mellitus, and 4) invasive tests and procedures.
Common infections include:Endometritis – infection of the lining and wall of the uterus (endometrium and myometrium).Mastitis – infl ammation and infection of the breast.Caesarean surgical site infections. Episiotomy site infections – infection at the site of the incision of the perineum.Sepsis - bloodstream infection which causes a systemic infl ammatory response.
Endometritis is oft en polymicrobial with both anaerobic and aerobic bacteria (e.g., Group A streptococcus, Group B streptococcus, Staphylococcus sp., Escherichia coli, Bacteroides, and Clostridium sp.). Staphylococcus aureus is the
•
•
•
•
•••
•

206
IFIC Basic Concepts of Infection Control
pathogen most oft en associated with mastitis. The pathogens associated with surgical site infections are typically endogenous to the patient, most oft en skin fl ora or bacterial fl ora of the lower genital tract.4
Prevention Strategies
As with all patients, use standard precautions/routine practices. Specifi c practices focused on the mother and child include:
Gloves are worn for all contact with mucous membranes, non-intact skin, and moist body substances.
a. Gloves are changed aft er each infant and/or procedure b. Gloves are not necessary for contact with the intact skin of an infant c. Gloves are worn for all diaper changes d. Gloves are worn when handling the infant aft er delivery prior to bath or adequate removal of mother’s body fl uid e. Sterile gloves are worn for the delivery f. Clean gloves are worn when handling soiled linen and waste
Gowns and/or plastic aprons are worn for holding infant to a uniform. Cohorting of infants with the same infection helps prevent spread of infections in the nursery. Parent/infant contact is encouraged, except for the occasional case when there is a risk of transmitt ing infection. Labouring mothers may shower or bathe. Post-partum, instruct patient on daily perineal care aft er toileting. Reviewing good hygienic policies with parents is vital to protect both mother and infant from acquiring or spreading infections. Additional precautions may be indicated for infants colonised or infected with microorganism(s) epidemiologically signifi cant to the facility.Suspected or confi rmed infections should be handled according to the guidelines in Table 14.1.
Mothers and infants with the following infections/microorganisms are managed using standard precautions/routine practices; mothers and infants may have contact; and breast feeding is allowed: amnionitis, Chlamydia, bacterial conjunctivitis, cytomegalovirus, endometritis (unless
1.
2.
3.
4.
5.
6.

207
Maternal - Child Health
group A streptococcus), gonococcal infections, hepatitis B and C, herpes simplex, listeria, Staphylococcus epidermidis and other coagulase negative staphylococcal infections, group B streptococci infection/colonisation, toxoplasmosis, urinary tract infection, West Nile virus, wound infection, and yeast. Also included in this group:
tuberculosis in mother (pulmonary or laryngeal on eff ective treatment, extrapulmonary, or positive skin test)mastitis/abscess due to S. aureus (for premature infants it may be prudent to withhold milk from a breast with mastitis/for breast abscess, recommended to refrain from breast feeding from aff ected breast until treated and abscess drained)S. aureus pneumonia/skin lesions in infant (during outbreak situations, additional precautions and cohorting of infants may be required)
Patients with acquired immune defi ciency syndrome, HIV or Human T-Cell Lymphotrophic Virus I/II (HTLV I/II) are cared for using standard precautions, contact is permitt ed; however mothers are not allowed to breast feed their child.
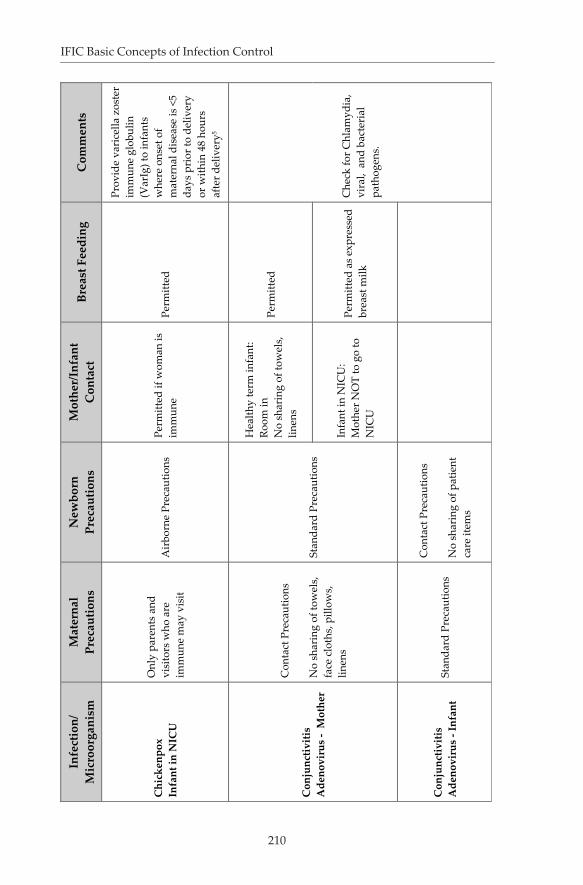
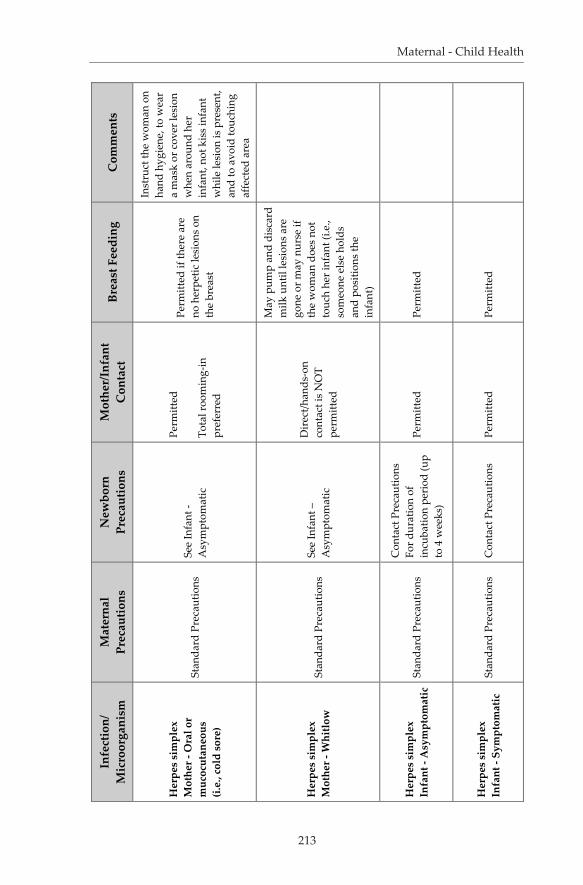
Infants and/or mothers with diagnosed or suspected infections transmitt ed by the airborne route must be placed in a single room with negative pressure and the door closed. Masks or respirators should be worn according to policy.Priority for single room accommodation should be given to mothers who soil articles in the environment with body substances and those colonised or infected with microorganism(s) epidemiologically signifi cant to the facility. Environmental cleaning – For labour and delivery suites, post-delivery remove soiled linens using gloved hands. The delivery table/bed and the immediate patient environment should be cleaned aft er each use. Use non-toxic disinfectants for cleaning neonatal equipment and incubators. Avoid phenolic disinfectants. Breast milk is protective as it provides specifi c IgA antibody and helps establish normal fl ora in the neonate. See Table 14.1 for maternal/newborn infections and recommendations for breastfeeding. Provide post-partum hygiene for the mother and infant immunisations as required. For facilities with litt le room and overcrowding, consider kangaroo mother care. This includes skin to skin positioning of the baby on the mother’s chest. Antepartum, intrapartum, and postpartum: Maintain
•
•
•
7.
8.
9.
10.
11.
12.
13.
208
IFIC Basic Concepts of Infection Control
standard precautions with designated areas for bathing, toilet, and hand washing facilities for patients. Refrain from communal use of ointments and lotions; mother should bring in her own lotions and creams. Post-partum – Encourage mothers to perform hand hygiene before breast feeding.
Prenatal assessment This is used to identify risk factors for maternal / newborn infection and focus prevention strategies.
Screen women for Group B streptococcus (GBS) at 35-37 weeks gestation. GBS-positive mothers should receive treatment if they are symptomatic. Colonised mothers should receive prophylactic penicillin at the time of delivery (ante-partum).
Screen for human immunodefi ciency virus (HIV) and Hepatitis B virus. If a mother is Hepatitis B surface antigen positive, the infant should receive hepatitis B immune globulin and the fi rst dose of Hepatitis B vaccine within the fi rst 12 hours of life. HIV positive mothers should refrain from breastfeeding unless alternatives are not available.
Antepartum - Screen mothers upon admission for symptoms of infection, such as new onset of fever and other respiratory symptoms, e.g., new onset of cough, rash, or diarrhoea. If the patient responds “yes” to the any of these conditions, initiate the appropriate additional precautions and spatial separation from other patients (> 2 metres). If airborne infections are suspected, e.g., pulmonary Mycobacterium tuberculosis or varicella, then place patient in single room with the door closed and initiate airborne precautions.

209
Maternal - Child Health
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Ant
ibio
tic R
esis
tant
M
icro
orga
nism
s -
Mot
her
Van
com
ycin
-res
ista
nt
Ente
roco
ccus
(VRE
) or
met
hici
llin-
resi
stan
t S.
aur
eus (
MRS
A):
Con
tact
Pre
caut
ions
Stan
dard
Pre
caut
ions
Pe
rmitt
ed
Perm
itted
M
RSA
- In
fant
to ro
om
with
wom
an
Ant
ibio
tic R
esis
tant
M
icro
orga
nism
s -
Infa
ntSt
anda
rd P
reca
utio
ns
VRE
or M
RSA
: Con
tact
Pr
ecau
tions
Perm
itted
Pe
rmitt
ed
MRS
A -
Sing
le ro
om
pref
erre
d. I
f ope
n co
ncep
t nur
sery
, the
n sp
atia
l sep
arat
ion
from
ot
her i
nfan
ts re
quir
ed
(>2
met
res)
Chi
cken
pox
Mot
her i
ll –
heal
thy
term
infa
nt
Air
born
e Pr
ecau
tions
Infa
nt ro
om in
with
m
othe
rPe
rmitt
ed
Perm
itted
Chi
cken
pox
Mot
her i
ll –
Infa
nt in
N
ICU
Air
born
e Pr
ecau
tions
M
othe
r may
not
vis
it th
e N
ICU
Stan
dard
Pre
caut
ions
un
til d
ay 1
0. A
s of
day
10
thro
ugh
day
28 s
tart
A
irbo
rne
Prec
autio
ns
Not
per
mitt
ed
Perm
itted
(as
expr
esse
d br
east
milk
)
Prov
ide
vari
cella
zos
ter
imm
une
glob
ulin
(V
arIg
) to
infa
nts
whe
re o
nset
of
mat
erna
l dis
ease
is <
5 da
ys p
rior
to d
eliv
ery
or w
ithin
48
hour
s af
ter d
eliv
ery5
Tabl
e 14
.1. M
ater
nal/C
hild
Infe
ctio
us D
isea
ses
and
Infe
ctio
n Pr
even
tion
and
Con
trol
Man
agem
ent (
Tabl
e ad
apte
d fr
om S
unny
broo
k H
ealth
Sci
ence
s C
entr
e, T
oron
to, O
ntar
io, 2
010)
.5-6
210
IFIC Basic Concepts of Infection Control
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Chi
cken
pox
Infa
nt in
NIC
U
Onl
y pa
rent
s an
d vi
sito
rs w
ho a
re
imm
une
may
vis
it
Air
born
e Pr
ecau
tions
Perm
itted
if w
oman
is
imm
une
Perm
itted
Prov
ide
vari
cella
zos
ter
imm
une
glob
ulin
(V
arIg
) to
infa
nts
whe
re o
nset
of
mat
erna
l dis
ease
is <
5 da
ys p
rior
to d
eliv
ery
or w
ithin
48
hour
s af
ter d
eliv
ery5
Con
junc
tiviti
sA
deno
viru
s -
Mot
her
Con
tact
Pre
caut
ions
No
shar
ing
of to
wel
s,
face
clo
ths,
pill
ows,
lin
ens
Stan
dard
Pre
caut
ions
Hea
lthy
term
infa
nt:
Room
in
No
shar
ing
of to
wel
s,
linen
s
Perm
itted
Infa
nt in
NIC
U:
Mot
her N
OT
to g
o to
N
ICU
Perm
itted
as
expr
esse
d br
east
milk
Con
junc
tiviti
sA
deno
viru
s - I
nfan
t St
anda
rd P
reca
utio
ns
Con
tact
Pre
caut
ions
No
shar
ing
of p
atie
nt
care
item
s
Che
ck fo
r Chl
amyd
ia,
vira
l, a
nd b
acte
rial
pa
thog
ens.

211
Maternal - Child Health
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Dia
rrho
ea
Mot
her -
Bact
eria
l(s
uspe
cted
or
conf
irm
ed)
Stan
dard
Pre
caut
ions
Si
ngle
room
with
toile
t St
anda
rd P
reca
utio
ns
Hea
lthy
term
infa
nt:
Perm
itted
with
St
anda
rd P
reca
utio
nsPe
rmitt
ed
Infa
nt in
NIC
U: N
ot
perm
itted
unt
il as
ympt
omat
ic fo
r 48
hour
s
Perm
itted
as
expr
esse
d br
east
milk
Dia
rrho
ea
Mot
her -
C. d
iffi
cile
Con
tact
Pre
caut
ions
Sing
le ro
om w
ith to
ilet
Stan
dard
Pre
caut
ions
Pe
rmitt
ed
Perm
itted
Dia
rrho
ea
Mot
her -
Vir
al
(e.g
., n
orov
irus
)
Con
tact
Pre
caut
ions
Sing
le ro
om w
ith to
ilet
Hea
lthy
term
infa
nt:
Perm
itted
with
St
anda
rd P
reca
utio
ns
Perm
itted
Infa
nt in
NIC
U:
Wom
an is
not
pe
rmitt
ed in
the
NIC
U
until
asy
mpt
omat
ic fo
r 48
hou
rs
Perm
itted
as
expr
esse
d br
east
milk
Con
tact
Pre
caut
ions
Sing
le ro
om w
ith to
ilet

212
IFIC Basic Concepts of Infection Control
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Dia
rrho
ea
Infa
nt -
Bact
eria
l (s
uspe
cted
or
conf
irm
ed)
Stan
dard
Pre
caut
ions
C
onta
ct P
reca
utio
ns
Perm
itted
Pe
rmitt
ed
Dia
pere
d in
fant
s re
quir
e C
onta
ct
prec
autio
ns fo
r the
du
ratio
n of
illn
ess
Dia
rrho
ea
Infa
nt -
Vir
al (e
.g.,
noro
viru
s)St
anda
rd P
reca
utio
ns
Con
tact
Pre
caut
ions
Pe
rmitt
ed
Perm
itted
Dia
pere
d in
fant
s re
quir
e C
onta
ct
Prec
autio
ns fo
r the
du
ratio
n of
illn
ess
Ente
rovi
rus
Mot
her
Con
tact
Pre
caut
ions
Sing
le ro
om
Hea
lthy
term
infa
nt:
Perm
itted
with
St
anda
rd P
reca
utio
nsPe
rmitt
ed
Infa
nt in
NIC
U:
Wom
an is
not
pe
rmitt
ed in
the
NIC
U
until
asy
mpt
omat
ic
Perm
itted
as
expr
esse
d br
east
milk
Ente
rovi
rus
Infa
ntSt
anda
rd P
reca
utio
ns
Con
tact
Pre
caut
ions
Pe
rmitt
ed
Perm
itted
Con
tact
Pre
caut
ions
Sing
le ro
om
Hep
atiti
s, ty
pe A
M
othe
rSt
anda
rd P
reca
utio
ns
Stan
dard
Pre
caut
ions
A
fter p
roph
ylax
is o
f in
fant
Afte
r pro
phyl
axis
of
infa
nt
213
Maternal - Child Health
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Her
pes
sim
plex
Mot
her -
Ora
l or
muc
ocut
aneo
us
(i.e.
, col
d so
re)
Stan
dard
Pre
caut
ions
See
Infa
nt -
Asy
mpt
omat
ic
Perm
itted
Tota
l roo
min
g-in
pr
efer
red
Perm
itted
if th
ere
are
no h
erpe
tic le
sion
s on
th
e br
east
Inst
ruct
the
wom
an o
n ha
nd h
ygie
ne, t
o w
ear
a m
ask
or c
over
lesi
on
whe
n ar
ound
her
in
fant
, not
kis
s in
fant
w
hile
lesi
on is
pre
sent
, an
d to
avo
id to
uchi
ng
affe
cted
are
a
Her
pes
sim
plex
Mot
her -
Whi
tlow
Stan
dard
Pre
caut
ions
See
Infa
nt –
A
sym
ptom
atic
Dir
ect/h
ands
-on
cont
act i
s N
OT
perm
itted
May
pum
p an
d di
scar
d m
ilk u
ntil
lesi
ons
are
gone
or m
ay n
urse
if
the
wom
an d
oes
not
touc
h he
r inf
ant (
i.e.,
som
eone
els
e ho
lds
and
posi
tions
the
infa
nt)
Her
pes
sim
plex
Infa
nt -
Asy
mpt
omat
icSt
anda
rd P
reca
utio
ns
Con
tact
Pre
caut
ions
Fo
r dur
atio
n of
in
cuba
tion
peri
od (u
p to
4 w
eeks
)
Perm
itted
Pe
rmitt
ed
Her
pes
sim
plex
Infa
nt -
Sym
ptom
atic
Stan
dard
Pre
caut
ions
C
onta
ct P
reca
utio
ns
Perm
itted
Pe
rmitt
ed
214
IFIC Basic Concepts of Infection Control
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
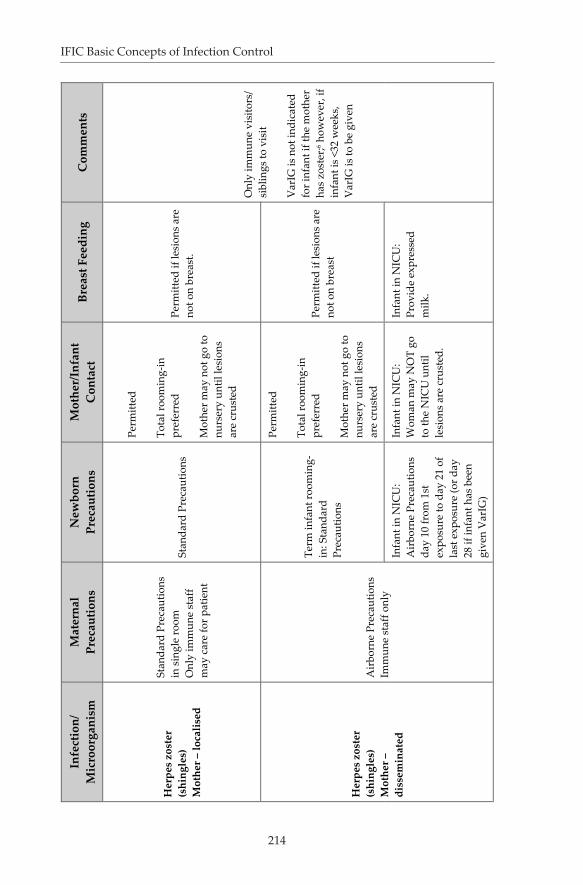
Her
pes
zost
er(s
hing
les)
Mot
her –
loca
lised
Stan
dard
Pre
caut
ions
in
sin
gle
room
O
nly
imm
une
staf
f m
ay c
are
for p
atie
nt
Stan
dard
Pre
caut
ions
Perm
itted
Tota
l roo
min
g-in
pr
efer
red
Mot
her m
ay n
ot g
o to
nu
rser
y un
til le
sion
s ar
e cr
uste
d
Perm
itted
if le
sion
s ar
e no
t on
brea
st.
Onl
y im
mun
e vi
sito
rs/
sibl
ings
to v
isit
Var
IG is
not
indi
cate
d fo
r inf
ant i
f the
mot
her
has
zost
er;6 h
owev
er, i
f in
fant
is <
32 w
eeks
, V
arIG
is to
be
give
n
Her
pes
zost
er
(shi
ngle
s)M
othe
r –
diss
emin
ated
Air
born
e Pr
ecau
tions
Im
mun
e st
aff o
nly
Term
infa
nt ro
omin
g-in
: Sta
ndar
d Pr
ecau
tions
Perm
itted
Tota
l roo
min
g-in
pr
efer
red
Mot
her m
ay n
ot g
o to
nu
rser
y un
til le
sion
s ar
e cr
uste
d
Perm
itted
if le
sion
s ar
e no
t on
brea
st
Infa
nt in
NIC
U:
Air
born
e Pr
ecau
tions
da
y 10
from
1st
ex
posu
re to
day
21
of
last
exp
osur
e (o
r day
28
if in
fant
has
bee
n gi
ven
Var
IG)
Infa
nt in
NIC
U:
Wom
an m
ay N
OT
go
to th
e N
ICU
unt
il le
sion
s ar
e cr
uste
d.
Infa
nt in
NIC
U:
Prov
ide
expr
esse
d m
ilk.
215
Maternal - Child Health
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
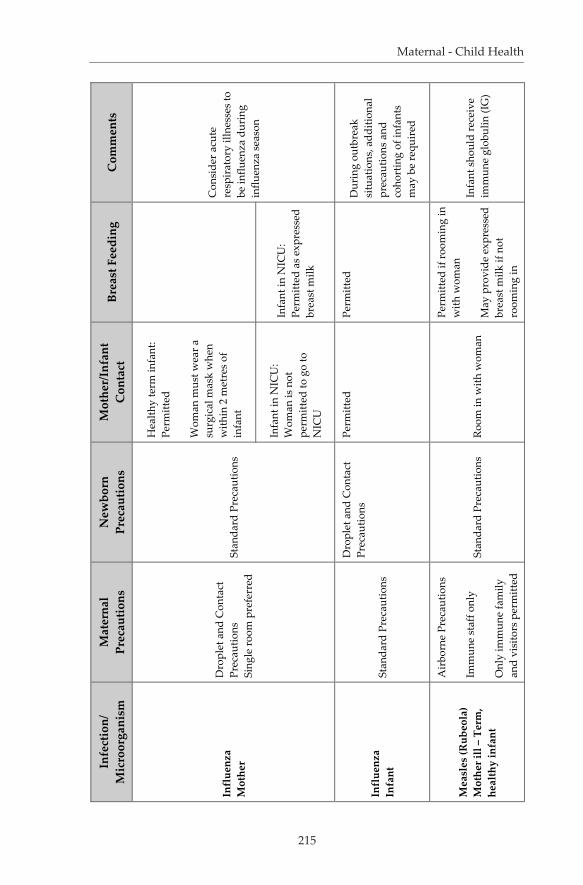
Infl
uenz
aM
othe
r
Dro
plet
and
Con
tact
Pr
ecau
tions
Si
ngle
room
pre
ferr
edSt
anda
rd P
reca
utio
ns
Hea
lthy
term
infa
nt:
Perm
itted
Wom
an m
ust w
ear a
su
rgic
al m
ask
whe
n w
ithin
2 m
etre
s of
in
fant
Infa
nt in
NIC
U:
Wom
an is
not
pe
rmitt
ed to
go
to
NIC
U
Infa
nt in
NIC
U:
Perm
itted
as
expr
esse
d br
east
milk
Infl
uenz
aIn
fant
Stan
dard
Pre
caut
ions
Dro
plet
and
Con
tact
Pr
ecau
tions
Perm
itted
Pe
rmitt
ed
Dur
ing
outb
reak
si
tuat
ions
, add
ition
al
prec
autio
ns a
nd
coho
rtin
g of
infa
nts
may
be
requ
ired
Mea
sles
(Rub
eola
) M
othe
r ill
– Te
rm,
heal
thy
infa
nt
Air
born
e Pr
ecau
tions
Imm
une
staf
f onl
y
Onl
y im
mun
e fa
mily
an
d vi
sito
rs p
erm
itted
Stan
dard
Pre
caut
ions
Ro
om in
with
wom
an
Perm
itted
if ro
omin
g in
w
ith w
oman
May
pro
vide
exp
ress
ed
brea
st m
ilk if
not
ro
omin
g in
Infa
nt s
houl
d re
ceiv
e im
mun
e gl
obul
in (I
G)
Con
side
r acu
te
resp
irat
ory
illne
sses
to
be in
fluen
za d
urin
g in
fluen
za s
easo
n

216
IFIC Basic Concepts of Infection Control
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Mea
sles
(rub
eola
) M
othe
r ill
– in
fant
in
NIC
U
Air
born
e Pr
ecau
tions
Im
mun
e st
aff o
nly
Onl
y im
mun
e fa
mily
an
d vi
sito
rs p
erm
itted
8 da
ys fr
om 1
st
expo
sure
to 1
2 da
ys
from
last
exp
osur
e -
Air
born
e Pr
ecau
tions
Wom
an n
ot p
erm
itted
in
NIC
U u
ntil
4 da
ys
afte
r the
app
eara
nce
of
the
rash
Perm
itted
as
expr
esse
d br
east
milk
onl
y un
til
wom
an n
o lo
nger
in
fect
ious
Infa
nt s
houl
d re
ceiv
e im
mun
e gl
obul
in (I
G).
Fam
ilies
& V
isito
rs:
Imm
unity
is d
efin
ed a
s pr
evio
us h
isto
ry o
f m
easl
es o
r hav
ing
rece
ived
mea
sles
va
ccin
eM
easl
es (r
ubeo
la)
Infa
nt il
l or e
xpos
ed
(i.e.
, exp
osed
in N
ICU
)St
anda
rd P
reca
utio
ns
Wom
an im
mun
e –
perm
itted
to s
ee in
fant
Perm
itted
Wom
an su
scep
tible
–
wom
an n
ot p
erm
itted
to
see
infa
nt
Perm
itted
as
expr
esse
d br
east
milk
onl
y un
til
infa
nt n
o lo
nger
in
fect
ious
Men
ingi
tis
Nei
sser
ia m
enin
giti
dis/
H
aem
ophi
lus
influ
enza
e
Dro
plet
Pre
caut
ions
un
til 2
4 ho
urs
afte
rap
prop
riat
ean
timic
robi
al th
erap
y
Con
side
r inf
ant a
co
ntac
t of t
he m
othe
r
Air
born
e Pr
ecau
tions

217
Maternal - Child Health
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Mum
psM
othe
r
Dro
plet
/Con
tact
Pr
ecau
tions
Imm
une
staf
f onl
y
Onl
y im
mun
e fa
mily
an
d vi
sito
rs p
erm
itted
Stan
dard
Pre
caut
ions
Term
infa
nt: P
erm
itted
Te
rm in
fant
: Per
mitt
ed
Infa
nt in
NIC
U:
Wom
an is
not
to g
o in
th
e N
ICU
unt
il 9
days
af
ter t
he o
nset
of t
he
paro
tid s
wel
ling
Infa
nt in
NIC
U:
Expr
esse
d br
east
milk
un
til 9
day
s af
ter t
he
onse
t of t
he p
arot
id
swel
ling
Mum
ps In
fant
in N
ICU
Ex
pose
d or
ill
Stan
dard
Pre
caut
ions
Dro
plet
/Con
tact
Pr
ecau
tions
sta
rtin
g 10
da
ys fr
om 1
st e
xpos
ure
to 2
6 da
ys fr
om la
st
expo
sure
Sing
le ro
om
Imm
une
staf
f onl
y
Onl
y im
mun
e fa
mily
an
d vi
sito
rs p
erm
itted
Wom
an im
mun
e –
perm
itted
to s
ee in
fant
Perm
itted
Wom
an su
scep
tible
–
wom
an n
ot p
erm
itted
to
see
infa
nt
Perm
itted
as
expr
esse
d br
east
milk
Fam
ilies
& V
isito
rs:
Imm
unity
is d
efin
ed
as a
pre
viou
s hi
stor
y of
mum
ps o
r hav
ing
rece
ived
mum
ps
vacc
ine
218
IFIC Basic Concepts of Infection Control
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
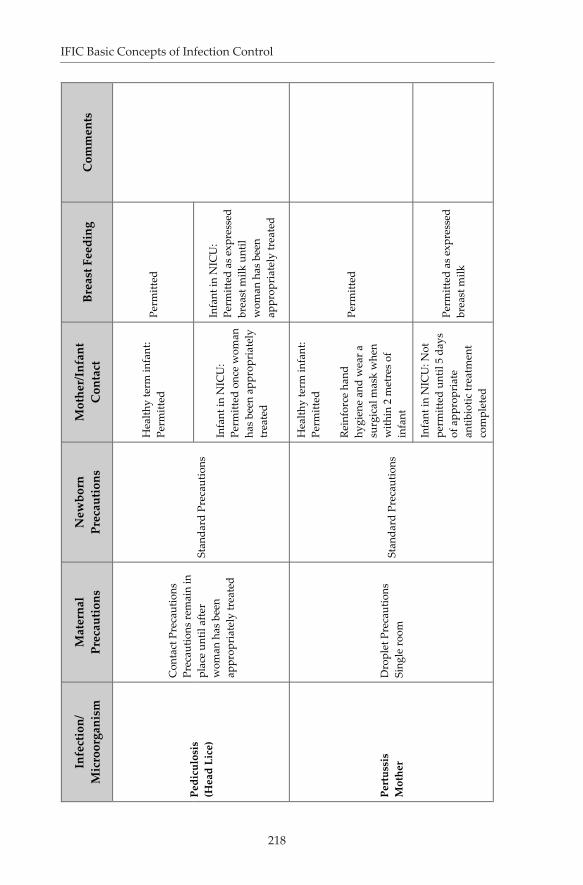
Pedi
culo
sis
(Hea
d Li
ce)
Con
tact
Pre
caut
ions
Pr
ecau
tions
rem
ain
in
plac
e un
til a
fter
wom
an h
as b
een
appr
opri
atel
y tr
eate
d
Stan
dard
Pre
caut
ions
Hea
lthy
term
infa
nt:
Perm
itted
Perm
itted
Infa
nt in
NIC
U:
Perm
itted
onc
e w
oman
ha
s be
en a
ppro
pria
tely
tr
eate
d
Infa
nt in
NIC
U:
Perm
itted
as
expr
esse
d br
east
milk
unt
il w
oman
has
bee
n ap
prop
riat
ely
trea
ted
Pert
ussi
s M
othe
rD
ropl
et P
reca
utio
ns
Sing
le ro
om
Stan
dard
Pre
caut
ions
Hea
lthy
term
infa
nt:
Perm
itted
Rein
forc
e ha
nd
hygi
ene
and
wea
r a
surg
ical
mas
k w
hen
with
in 2
met
res
of
infa
nt
Perm
itted
Infa
nt in
NIC
U: N
ot
perm
itted
unt
il 5
days
of
app
ropr
iate
an
tibio
tic tr
eatm
ent
com
plet
ed
Perm
itted
as
expr
esse
d br
east
milk

219
Maternal - Child Health
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Pert
ussi
s In
fant
Stan
dard
Pre
caut
ions
Con
tact
Pre
caut
ions
C
onsi
der c
ohor
ting
Prec
autio
ns re
mai
n in
pl
ace
until
5 d
ays
of
appr
opri
ate
antib
iotic
tr
eatm
ent h
as b
een
com
plet
ed
Perm
itted
Pe
rmitt
ed
Res
pira
tory
Vir
us
Infe
ctio
ns
Mot
her i
ll
Dro
plet
/Con
tact
Pr
ecau
tions
Sing
le ro
om
Hea
lthy
term
infa
nt:
Perm
itted
Rein
forc
e ha
nd
hygi
ene
and
wea
r a
surg
ical
mas
k w
hen
with
in 2
met
res
of
infa
nt
Infa
nt ro
omin
g-in
: Pe
rmitt
ed
Infa
nt in
NIC
U: N
ot
perm
itted
Infa
nt in
NIC
U:
Perm
itted
as
expr
esse
d br
east
milk
Res
pira
tory
Vir
us
Infe
ctio
ns
Infa
nt il
lSt
anda
rd P
reca
utio
nsD
ropl
et /C
onta
ct
Prec
autio
nsPe
rmitt
ed
Perm
itted
Dur
ing
outb
reak
si
tuat
ions
, add
ition
al
prec
autio
ns a
nd
coho
rtin
g of
infa
nts
may
be
requ
ired
.
Stan
dard
Pre
caut
ions

220
IFIC Basic Concepts of Infection Control
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Rub
ella
Mot
her
Dro
plet
pre
caut
ions
Imm
une
staf
f onl
y
Dro
plet
pre
caut
ions
Imm
une
staf
f onl
y
Hea
lthy
term
infa
nt:
Perm
itted
Hea
lthy
term
infa
nt:
Perm
itted
Fam
ilies
and
vis
itors
: Im
mun
ity is
def
ined
as
havi
ng re
ceiv
ed
rube
lla v
acci
ne o
r la
bora
tory
evi
denc
e of
im
mun
ity
Infa
nt in
NIC
U:
Wom
an c
anno
t go
into
th
e N
ICU
unt
il 7
days
af
ter t
he o
nset
of t
he
rash
Infa
nt in
NIC
U:
Expr
esse
d br
east
milk
as
the
wom
an c
anno
t go
into
the
NIC
U u
ntil
7 da
ys a
fter t
he o
nset
of
the
rash
Rub
ella
Infa
nt (C
onge
nita
l)St
anda
rd P
reca
utio
ns
Dro
plet
Pre
caut
ions
Pe
rmitt
ed
Perm
itted
C
onge
nita
lly in
fect
ed
infa
nts
may
she
d vi
rus
for u
p to
2 y
ears
.
Scab
ies
Con
tact
Pre
caut
ions
Prec
autio
ns re
mai
n in
pl
ace
until
wom
an h
as
been
app
ropr
iate
ly
trea
ted
Stan
dard
Pre
caut
ions
Hea
lthy
term
infa
nt:
Perm
itted
onc
e w
oman
ha
s be
en a
ppro
pria
tely
tr
eate
d
Perm
itted
onc
e w
oman
ha
s be
en a
ppro
pria
tely
tr
eate
d or
may
pro
vide
ex
pres
sed
brea
st m
ilk
Infa
nt in
NIC
U:
Perm
itted
onc
e w
oman
ha
s be
en a
ppro
pria
tely
tr
eate
d
Infa
nt in
NIC
U:
Perm
itted
onc
e w
oman
ha
s be
en a
ppro
pria
tely
tr
eate
d or
may
pro
vide
ex
pres
sed
brea
st m
ilk
221
Maternal - Child Health
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
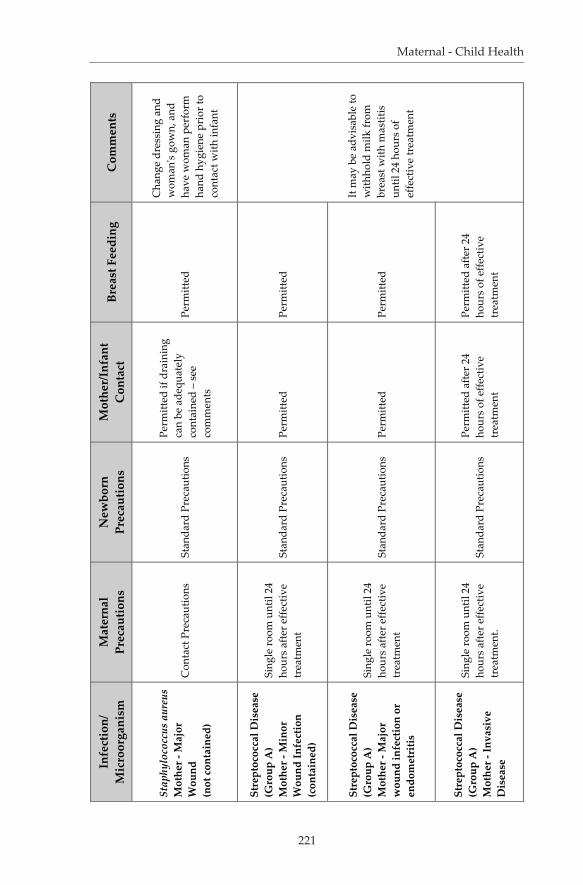
Stap
hylo
cocc
us a
ureu
s M
othe
r - M
ajor
W
ound
(not
con
tain
ed)
Con
tact
Pre
caut
ions
St
anda
rd P
reca
utio
ns
Perm
itted
if d
rain
ing
can
be a
dequ
atel
y co
ntai
ned
– se
e co
mm
ents
Perm
itted
Cha
nge
dres
sing
and
w
oman
's go
wn,
and
ha
ve w
oman
per
form
ha
nd h
ygie
ne p
rior
to
cont
act w
ith in
fant
Stre
ptoc
occa
l Dis
ease
(G
roup
A)
Mot
her -
Min
or
Wou
nd In
fect
ion
(con
tain
ed)
Sing
le ro
om u
ntil
24
hour
s af
ter e
ffect
ive
trea
tmen
tSt
anda
rd P
reca
utio
ns
Perm
itted
Pe
rmitt
ed
Stre
ptoc
occa
l Dis
ease
(G
roup
A)
Mot
her -
Maj
or
wou
nd in
fect
ion
or
endo
met
ritis
Sing
le ro
om u
ntil
24
hour
s af
ter e
ffect
ive
trea
tmen
tSt
anda
rd P
reca
utio
ns
Perm
itted
Pe
rmitt
ed
It m
ay b
e ad
visa
ble
to
with
hold
milk
from
br
east
with
mas
titis
un
til 2
4 ho
urs
of
effe
ctiv
e tr
eatm
ent
Stre
ptoc
occa
l Dis
ease
(G
roup
A)
Mot
her -
Inva
sive
D
isea
se
Sing
le ro
om u
ntil
24
hour
s af
ter e
ffect
ive
trea
tmen
t.St
anda
rd P
reca
utio
nsPe
rmitt
ed a
fter 2
4 ho
urs
of e
ffect
ive
trea
tmen
t
Perm
itted
afte
r 24
hour
s of
effe
ctiv
e tr
eatm
ent

222
IFIC Basic Concepts of Infection Control
Infe
ctio
n/M
icro
orga
nism
Mat
erna
lPr
ecau
tions
New
born
Prec
autio
nsM
othe
r/In
fant
Con
tact
Brea
st F
eedi
ngC
omm
ents
Stre
ptoc
occa
l Dis
ease
(G
roup
A)
Mot
her -
Pha
ryng
itis
(str
ep th
roat
)
Dro
plet
Pre
caut
ions
Sing
le ro
om
Stan
dard
Pre
caut
ions
Perm
itted
afte
r 24
hour
s of
effe
ctiv
e tr
eatm
ent
Perm
itted
afte
r 24
hour
s of
effe
ctiv
e tr
eatm
ent
Stre
ptoc
occa
l Dis
ease
(G
roup
A)
Infa
ntSt
anda
rd P
reca
utio
ns
Con
tact
Pre
caut
ions
Pe
rmitt
ed
Perm
itted
Syph
ilis
Mot
her -
M
ucoc
utan
eous
C
onta
ct P
reca
utio
ns
Stan
dard
Pre
caut
ions
Pe
rmitt
ed a
fter 2
4 ho
urs
effe
ctiv
e tr
eatm
ent
Perm
itted
afte
r 24
hour
s ef
fect
ive
trea
tmen
t
It m
ay b
e ad
visa
ble
to
with
hold
milk
from
br
east
with
mas
titis
un
til 2
4 ho
urs
of
effe
ctiv
e tr
eatm
ent
Syph
ilis
Infa
nt -
Con
geni
tal
Stan
dard
Pre
caut
ions
C
onta
ct P
reca
utio
ns
Perm
itted
Pe
rmitt
ed
Tube
rcul
osis
Mot
her -
Pul
mon
ary
or la
ryng
eal –
new
ly
diag
nose
d, o
n in
adeq
uate
trea
tmen
t or
non
com
plia
nt
Air
born
e Pr
ecau
tions
St
anda
rd P
reca
utio
ns
Not
per
mitt
ed u
ntil
wom
an is
no
long
er
infe
ctio
us
Mot
her m
ay p
rovi
de
expr
esse
d br
east
milk
Con
tinue
Air
born
e Pr
ecau
tions
unt
il th
e m
othe
r no
long
er
cons
ider
ed in
fect
ious

223
Maternal - Child Health
References
UNICEF. ( 2009). The State of the World’s Children-Maternal and Newborn Health. Geneva: World Health Organization. htt p://www.unicef.org/sowc09/docs/SOWC09-FullReport-EN.pdf [Accessed July 26, 2011]APIC Text Infection Control and Epidemiology, 3rd Edition (Chapters 37, 38, 39). Washington, DC: Association of Professionals for Infection Prevention and Control and Epidemiology, 2009.PIDAC. Provincial Infectious Diseases Advisory Committee - Best Practices Guidelines for Surveillance in Health Care Settings. Toronto: Ministry of Health and Long Term Care, 2008. htt p://www.oahpp.ca/resources/pidac-knowledge/best-practice-manuals/surveillance-of-health-care-associated-infections.html [Accessed July 27, 2011]Wilks D. The Infectious Diseases Manual, 2nd ed. Malden, Massachusett s: Blackwell Publishing, 2003; 249-262.National Advisory Committ ee on Immunization. (2006). Canadian Immunization Guide 7th edition. Ott awa, Canada: Public Health Agency of Canada.Committ ee on Infectious Diseases. The Red Book 28th Edition. Elk Grove Village, Illinois: American Academy of Pediatrics, 2009.
Further Reading
Provincial Infectious Diseases Advisory Committ ee (PIDAC): Best Practice Guidelines for Routine Practices and Additional Precautions – In all health care settings, Ministry of Health and Long Term Care, Toronto, Canada, 2010. htt p://www.oahpp.ca/resources/pidac-knowledge/best-practice-manuals/routine-practices-and-additional-precautions.html [Accessed July 27, 2011]World Health Organization (WHO): Practical Guidelines for Infection Control in health Care settings, WHO Regional Offi ce, India, 2004. http://www.wpro.who.int/NR/rdonlyres/006EF250-6B11-42B4-BA17-C98D413BE8B8/0/practical_guidelines_infection_control.pdf [Accessed July 26, 2011]World Health Organization (WHO): Recommendations for Routine Immunization 2010. htt p://www.who.int/immunization/policy/immunization_tables/en/index.html [Accessed July 26, 2011]World Health Organization, Geneva, 2010. Packages of Interventions for Family Planning, Safe Abortion Care, Maternal, Newborn and Child
1.
2.
3.
4.
5.
6.
1.
2.
3.
4.

224
IFIC Basic Concepts of Infection Control
Health. htt p://whqlibdoc.who.int/hq/2010/WHO_FCH_10.06_eng.pdf [Accessed July 26, 2011]