mcs - profile of patients with chemical injury and sensitivity - ziem
DESCRIPTION
MULTIPLE CHEMICAL SENSITIVITY Protocol developed by MCS Referral & Resources. September 1995 edition.TRANSCRIPT
Profile of Patients with ChemicalInjury and SensitivityGrace Zieml and James McTamney21Occupational and Environmental Medicine, Baltimore, Maryland;2Clinical Psychologist, Lutherville, MarylandPatients reporting sensitivity to multiple chemicals at levels usually tolerated by the healthypopulation were administered standardized questionnaires to evaluate their symptoms and theexposures that aggravated these symptoms. Many patients were referred for medical tests. It is
thought that patients with chemical sensitivity have organ abnormalities involving the liver,nervous system (brain, including limbic, peripheral, autonomic), immune system, and porphyrinmetabolism, probably reflecting chemical injury to these systems. Laboratory results are notconsistent with a psychologic origin of chemical sensitivity. Substantial overlap between chemicalsensitivity, fibromyalgia, and chronic fatigue syndrome exists: the latter two conditions ofteninvolve chemical sensitivity and may even be the same disorder. Other disorders commonly seen
in chemical sensitivity patients include headache (often migraine), chronic fatigue, musculoskeletalaching, chronic respiratory inflammation (rhinitis, sinusitis, laryngitis, asthma), attention deficit,and hyperactivity (affected younger children). Less common disorders include tremor, seizures,and mitral valve prolapse. Patients with these overlapping disorders should be evaluated forchemical sensitivity and excluded from control groups in future research. Agents whoseexposures are associated with symptoms and suspected of causing onset of chemical sensitivitywith chronic illness include gasoline, kerosene, natural gas, pesticides (especially chlordane andchlorpyrifos), solvents, new carpet and other renovation materials, adhesives/glues, fiberglass,carbonless copy paper, fabric softener, formaldehyde and glutaraldehyde, carpet shampoos (laurylsulfate) and other cleaning agents, isocyanates, combustion products (poorly vented gas heaters,overheated batteries), and medications (dinitrochlorobenzene for warts, intranasally packedneosynephrine, prolonged antibiotics, and general anesthesia with petrochemicals). Multiplemechanisms of chemical injury that magnify response to exposures in chemically sensitivepatients can include neurogenic inflammation (respiratory, gastrointestinal, genitourinary), kindlingand time-dependent sensitization (neurologic), impaired porphyrin metabolism (multiple organs),and immune activation. Environ Health Perspect 105(Suppl 2):417-436 (1997)
Key words: multiple chemical sensitivity, fibromyalgia, chronic fatigue syndrome, neuropsy-chological tests, toxic encephalopathy, autoimmunity (or autoimmune diseases), immuneactivation, acquired disorders of porphyrin metabolism (or porphyria), chemically induced,pesticides, solvents, respiratory inflammation
IntroductionThe study of medicine "begins with the bodily functions. Porphyrin disturbancespatient, continues with the patient and of various types following chemical andends ... with the patient," according to heavy metal exposures were reported byWilliam Osler (1). Exposure to chemicals, several authors in a special conference onparticularly petrochemicals and combus- chemically induced porphyrinopathiestion products, has been associated in the sponsored by the New York Academy ofliterature with a variety of alterations in Sciences (2). Abnormally elevated levels of
This paper is based on a presentation at the Conference on Experimental Approaches to Chemical Sensitivityheld 20-22 September 1995 in Princeton, New Jersey. Manuscript received at EHP 6 March 1996; manuscriptaccepted 26 November 1996.
The authors gratefully acknowledge the assistance of B. Cook with record retrieval, G. Smith and C. Priggwith typing and data entry, and A. Donnay with editing and designing tables and figures. Donnay also providedmany invaluable suggestions and assistance with the content of the manuscript.
Address correspondence to Dr. G. Ziem, 1722 Linden Avenue, Baltimore MD 21217. Telephone: (410) 462-4085. alternate phone (410) 448-3319. Fax: (410) 462-1039.
Abbreviations used: AAL, Antibody Assay Laboratory; ALA-D, aminolevulenic acid dehydratase; CD, clusterof differentiation; CFS, chronic fatigue syndrome; conA, concanavalin A; CpgO, coproporhyrinogen oxidase;;EEGs, electroencephalograms; ISL, Immunosciences Laboratory; MCS, multiple chemical sensitivity; NK, nat-ural killer cell; PbgD, porphobilinogen deaminase; PHA, phytohemagglutinin; SPECT, single photon emissioncomputed tomography; WAIS-R, Wechsler adult intelligence scale-revised.
urinary coproporphyrins were reported inseveral papers, but other fecal and urinaryporphyrins could be increased as well.Specific types of heavy metal and petro-chemical exposures seem to cause specificpatterns of porphyrin disturbance in rats(3). Chlorinated benzenes can induce por-phyria in rats (4), and small exposures(such as swallowed mouthwash) can aggra-vate congenital porphyria (5). Immunedisturbances following chemical exposurehave been reported by several authors. Inthe following immune references, patientswere studied only after probable causalexposure and the results were compared tothose of laboratory normals. Impairedmitogenesis has been noted after exposureto chlordane (6) and isocyanates (7). Ahigher number of helper cells have beendescribed in workers exposed to solvents(8) and isocyanates (7), and in personsconsuming chlorinated solvents in drinkingwater (9). A greater number of immunecomplexes are reported with vinyl chlorideexposure, and scleroderma has been notedafter aromatic or chlorinated solvent expo-sure (10). Immune activation with higherlevels of TAI/CD26 has been reportedwith isocyanates (7), formaldehyde (11),formaldehyde with aliphatic amines (12),silicone (13), chlordane and chlorpyrifos(14), and sick-building exposures (15).
Higher levels of abnormalities in variousautoantibodies are described after a widevariety of chemical exposures, includingchlordane (6), solvents (16,17), chlorinatedsolvents (9), polychlorinated biphenyls andpolybrominated biphenyls (18), organo-chlorine, organophosphate and other pesti-cides (19), formaldehyde and aliphaticamines (12), silicone (13,20), chlordane(14), chlorpyrifos (14), malathion (14),and formaldehyde (11). A greater numberof chemical-specific antibodies has beennoted after exposure to building materials inremodeling (21). Suppression of mitogene-sis (22) and natural killer cell (NK) function(23) has been described following anesthesiainduced by petrochemical agents. ReducedNK function in multiple chemical sensitiv-ity (MCS) patients also has been reportedby Heuser (24).
Neurologic effects long have beenassociated with exposure to petrochemi-cals. Solvent exposure is associated withautonomic dysfunction (25), neurocogni-tive impairment (26,27), vestibular abnor-malities (28), and impaired hearing (29).In a study of the effects of solvents on 15
Environmental Health Perspectives - Vol 105, Supplement 2 * March 1997 417

ZIEM AND MCTAMNEY
industrial painters (30), impairment wasobserved on a variety of neuropsychologicalmeasures. The Halstead-Reitan Battery wasadministered and impairment was foundon the Impairment Index, Trails A, DigitSymbol, Seashore Rhythm and SpeechSounds-Perception Tests. In addition, sub-jects reported personality change anddecreased memory.
Neurological abnormalities in a groupof organophosphate-exposed subjects weredescribed using the Halstead-ReitanBattery (31). Visual retention, memorydysfunction, and constructional deficitswere reported (32).
Studies on chlorinated hydrocarbonsolvents have also shown adverse effects.Trichloroethylene in low concentrationsand for relatively brief times can lead tosignificant and prolonged impairment(33). Psychomotor speed and memorywere two of the areas most affected, withthe memory impairments characterized bystorage and retrieval difficulties.
Neuropsychological changes have beenfound among community residents livingin a supposedly benign environment suchas areas adjacent to a wood-treating plant(34). Of the 34 subjects tested, more than40% had sensory impairments, 86% hadmotor or psychomotor speed problems,and 72% had concentration difficulties.Disturbed autonomic function has beenreported with chemical sensitivity (35),and abnormal neurocognitive functionwith chemical sensitivity/cacosmia (36).
Chemical sensitivity has been reportedin the literature following exposure tochlordane (14), chlorpyrifos (37), pesti-cides (38), formaldehyde (39), tight or sickbuildings (15), and organophosphates andsolvents (40). These chemicals are notstructurally related, although all may formfree radicals and cause tissue damage.A wide range of neurologic abnormalities
[single photon emission computed tomog-raphy (SPECT), nerve conduction, electroencephalograms (EEGs), evoked potentials,neurocognitive] have been reported inchemically sensitive patients (41-43).Since depression and mood swings canoccur with solvent/hydrocarbon exposuresand with porphyrin disturbances, these arenot in themselves evidence of a psychologicetiology of MCS (40). These and otherstudies strongly suggest that chemical sen-sitivity is a physiologic not a psychologicdisorder (35,36,44).A 1994 study found that 67% of patients
with fibromyalgia and the same percentagewith chronic fatigue syndrome (CFS)
reported that their symptoms worsened onexposure to gas, paint, or solvent fumes, and46 to 64% of these groups reported sensitiv-ities to three other categories of commonchemical exposures (45). Fibromyalgiapatients have shown reduced current per-ception threshold (46) and T-cell changes(47). Chronic fatigue syndrome patientsoften meet criteria for fibromyalgia (48) andhave impaired NK function, increasedTA1/CD26, altered CD8, impaired mitoge-nesis (49,50), and vestibular and other neu-rologic abnormalities (51). Both chemicalsensitivity (52) and chronic fatigue syn-drome (53) have been postulated to involvelimbic encephalopathy.
We describe medical findings on history,physical exam, and laboratory testing forpatients who, in the wake of chemicalexposure, developed chronic illness withmulti-systemic symptoms exacerbated byexposures to multiple different chemicals atlevels usually tolerated by most healthymembers of the general population andpreviously tolerated by the patient.
MethodsZiem's medical practice has been evaluatingand caring for patients with MCS accom-panied by chronic illness for many years,assisting them with environmental controlsto reduce exposure and addressing clinicalissues related to their exposure. Typically, aninitial evaluation requires 1.5 to 2 hr formedical and exposure history, physicalexam, evaluation of environmental aggravat-ing factors, recommendations for environ-mental controls, and otherwise addressingclinical problems. Follow-up evaluationsusually require 1 to 1.5 hr. This time-inten-sive approach to the evaluation of chemi-cally injured patients contrasts with what weconsider to be a too-cursory assessmentprevalent among many industrial and acade-mic professionals. We do not believe it ispossible to evaluate and manage these disor-ders adequately in the 10 to 30 min usuallyallotted to such patients.
In the late 1980s, Ziem introduced astandardized questionnaire for initialpatient assessment to evaluate the types ofsymptoms present, possible organ systemsinvolved, and the types of chemical expo-sures perceived by these patients to beaggravating their symptoms. The full ques-tionnaire is 16 pages long with 46 detailedquestions. Reported here are the responsesto questions 14 and 6 (Appendices 1 and2) from 91 chemically sensitive patientswhose first visit occurred after the intro-duction of the questionnaire. These two
questions originally were developed byDr. Ann Davidoff of the Johns HopkinsSchool of Hygiene and Public Health aspart of a research project on chemicalsensitivity (54).
Patients responding to the question-naire came from many states from the east-ern region of the United States, with mostcoming from the mid-Atlantic area. Mostwere referred by physicians not specializingin occupational medicine or toxic sub-stances. Some were referred by patient sup-port groups, friends, or relatives, and a fewwere legal referrals (although we have nodata on the actual number in each cate-gory). Most but not all patients were wellbefore the onset of their MCS. Formerpsychiatric diagnoses and treatment wereunusual rather than typical.
In following these patients over time,Ziem's clinical impression is that patientresponses to these two questions seem tocorrelate well with the clinical severity oftheir symptoms: sicker patients appear tohave more frequent symptoms and to beaffected by more exposures. However, it wasnot possible for this presentation to confirmthis clinical impression by comparingresponse rates to exposures with clinical out-comes. This would be useful for future clini-cal studies. Symptom frequency can also bestudied as an indicator of clinical severity.
These patients filled out the question-naires at or shortly before their first visit.Some had been using some environmentalcontrols; others had not. Many but not allpatients were aware of chemical sensitivityas a potential problem for them. To assessthe frequency of 51 different symptomscommonly associated with MCS, patientswere asked in question 14 to describewhether these symptoms occur daily toalmost daily, several times a week, once aweek, several times per month, once permonth or less, rarely, if ever, or not sure. Inthe analysis below, daily or almost dailyresponses are combined with several timesa week or more responses to obtain a totalfigure for frequent symptoms.
All patients reporting increased sensi-tivity to chemicals accompanied by chronicillness were included in this analysis. Theytypically had frequent recurring or chronicsymptoms in more than one organ systemfor over 6 months before completing thequestionnaire. For some items in question14, responses were only available for 89 or90 patients: the bar graph in Figure 1 showsthe number of patients (n) answering foreach question. Outcomes are reported aspercentages of the total answering each
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997418
PATIENTS WITH CHEMICAL INJURYAND SENSITIVITY
Selected symptoms n
Headache 90Numbness, tingling 91
Weakness in a body part 91Lightheadedness, dizziness 90
Tremor or shaking 90Muscle twitching 90
Confusion, inability to concentrate 90Memory problems 90
Slurred words 90Coordination difficulties 91
Low energy, fatigue (unusual) 91Abdominal pressure, pain, cramps 90
Nausea, vomiting, bloating, gas 90Unusual thirst 90
Sneezing 90Itchy, watery eyes or nose 90
Visual changes 92Ringing ears 90
Changes in hearing 90Nasal discharge, stuffiness 90
Sinus discomfort 90Throat soreness, tightness 90
Difficulty swallowing 90Weak voice, hoarseness 89
Fever 88Reduced cold tolerance 88Reduced heat tolerance 88
Swollen glands 90Frequent infections 90
Coughing 91Chest heaviness, pain 90
Chest tightness 90Wheezing 90
Muscle discomfort, spasm 90Joint discomfort 90
Rapid pulse 90Heart palpitations 89Swelling of ankles 90
Swelling (throughout body) 90Bruising without a cause 89
Itching, rash, hives 89Flushing skin 89
Reduced bladder control 89Need to pass urine frequently 89
Flare up of yeast infection 89Insomnia 90
Other sleep disturbances 891
o 10-1 T
20 30 40 50 60
Percent reporting
_ Frequent: daily to several days/i=I1 Occasional: once/week to sevei_ Rare: less than once a month, if
E=L Not sure or unanswered
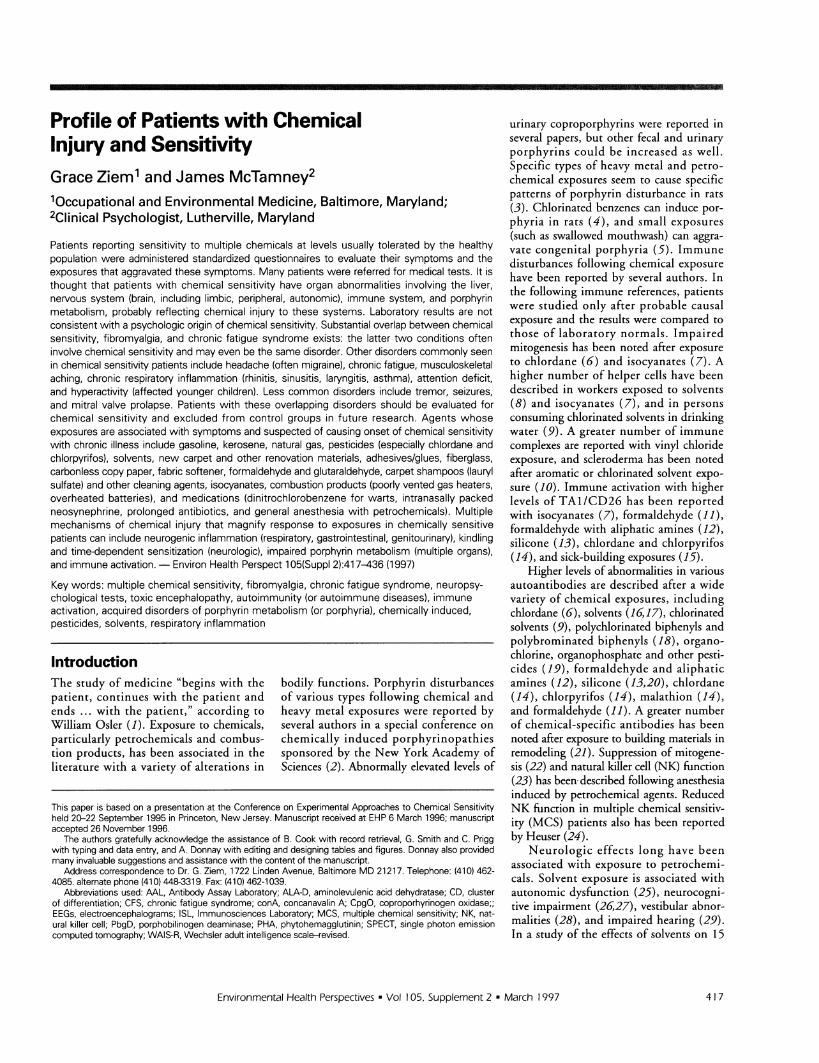
Figure 1. Relative frequency of select symptoms as reported by Ziem's MCS patients.
item. The bar for each symptom displaysseparately symptoms occurring daily to sev-eral times a week (combined totals from thefirst two columns from Appendix 1) andonce a week to several times a month (com-bined totals from columns 3 and 4 fromAppendix 1). These percents are thenadded to show the total percent with symp-toms several times a month or more (thispercent figure is shown to the right of first
bar for each symptom57% of patients had he.eral times a week andweekly to several timesof 75% of patients expseveral times a month or
Question 6 of the qfrom the Davidoff studconducted at Johns Ho1parts. In the first part, p:
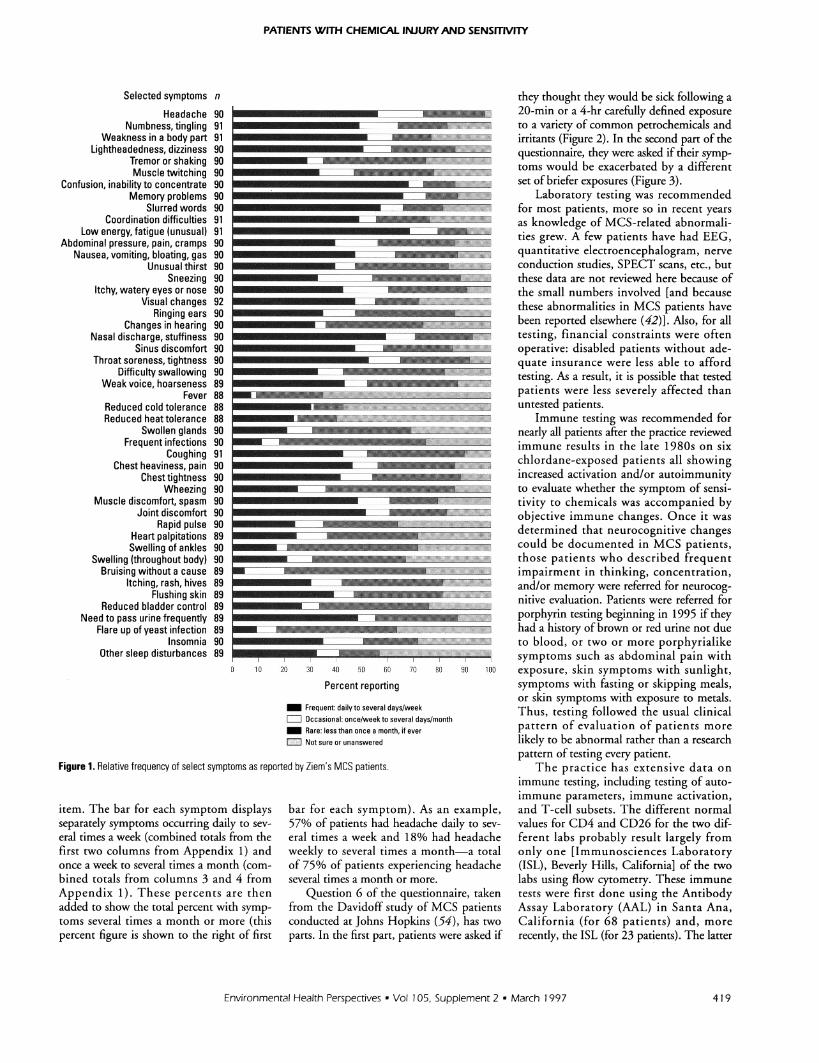
they thought they would be sick following a20-min or a 4-hr carefully defined exposureto a variety of common petrochemicals andirritants (Figure 2). In the second part of thequestionnaire, they were asked if their symp-toms would be exacerbated by a differentset of briefer exposures (Figure 3).
Laboratory testing was recommendedfor most patients, more so in recent yearsas knowledge of MCS-related abnormali-ties grew. A few patients have had EEG,quantitative electroencephalogram, nerveconduction studies, SPECT scans, etc., butthese data are not reviewed here because of
-__________________ the small numbers involved [and becausethese abnormalities in MCS patients havebeen reported elsewhere (42)]. Also, for alltesting, financial constraints were often
RMa Em operative: disabled patients without ade-quate insurance were less able to affordtesting. As a result, it is possible that testedpatients were less severely affected thanuntested patients.
Immune testing was recommended for--------------- nearly all patients after the practice reviewed
immune results in the late 1980s on sixchlordane-exposed patients all showingincreased activation and/or autoimmunity
_P-;U= to evaluate whether the symptom of sensi-tivity to chemicals was accompanied byobjective immune changes. Once it wasdetermined that neurocognitive changescould be documented in MCS patients,
.;.--: ; ] those patients who described frequentimpairment in thinking, concentration,and/or memory were referred for neurocog-nitive evaluation. Patients were referred forporphyrin testing beginning in 1995 if they
R' had a history of brown or red urine not due_-- I .IIi lI to blood, or two or more porphyrialike
f: symptoms such as abdominal pain with70 80 80 100 exposure, skin symptoms with sunlight,
symptoms with fasting or skipping meals,or skin symptoms with exposure to metals.
ral days/monthThus, testing followed the usual clinical
ever pattern of evaluation of patients morelikely to be abnormal rather than a researchpattern of testing every patient.
The practice has extensive data onimmune testing, including testing of auto-immune parameters, immune activation,
.). As an example, and T-cell subsets. The different normaladache daily to sev- values for CD4 and CD26 for the two dif-18% had headache ferent labs probably result largely froma month-a total only one [Immunosciences Laboratory
eriencing headache (ISL), Beverly Hills, California] of the twomore. labs using flow cytometry. These immune[uestionnaire, taken tests were first done using the AntibodyIy of MCS patients Assay Laboratory (AAL) in Santa Ana,pkins (54), has two California (for 68 patients) and, moreatients were asked if recently, the ISL (for 23 patients). The latter
Environmental Health Perspectives - Vol 105, Supplement 2 * March 1997
----7-r-
419
ZIEM AND MCTAMNEY
Exposures
4 hr next to someonesmoking cigarettes outside
20 min next to someonesmoking cigarettes outside4 hr driving in heavy traffic
with windows open20 min driving in heavy traffic
with windows open4 hr around workers
tarring a road20 min around workers
tarring a road4 hr driving a 1-week-old
car with the window open20 min driving a 1-week-oldcar with the window open4 hr in a room sprayed 4 hrpreviously with pesticides
20 min in a room sprayed 4 hrpreviously with pesticides
4 hr in a room painted 24 hrpreviously with water-based paint
20 min in a room painted 24 hrpreviously with water-based paint
4 hr shopping in anenclosed mall
20 min shopping in anenclosed mall
4 hr in a room with 1-week-old wall-to-wall carpet
20 min in a room with 1-week-old wall-to-wall carpet
4 hr sitting next to a personwearing perfume/cologne
20 min sitting next to a personwearing perfume/cologne
4 hr in a room newly-paneledwith wood or pressboard
20 min in a room newly-paneledwith wood or pressboard4 hr in a room with new
plastic/vinyl furniture20 min in a room with new
plastic/vinyl furniture4 hr cooking on anatural gas stove
20 min cooking on anatural gas stove
N11#1i5 "'t
-~~~~~~~C
.~~~~~~~~~~~~~~~~~~~~~D.
.MI
Bill
I AI
_-0~~
o 10 20 30 40 50 60 70 80 90
Number of respondents
Yes, aggravates symptoms L No, not aggravating Not sure or unanswered
Figure 2. Comparison of sensitivity to select exposures after 4 hr and 20 min as reported by Ziem's MCS patients.
laboratory also included tests of T- andB-cell function, which were not requestedof the AAL.
Beginning in 1995, MCS patients withneurological and/or cutaneous symptomssuggesting porphyrin disorders have beenscreened for the various biomarkers of thoseconditions that may be detected in blood,urine, and stool. Samples were collectedlocally by independent laboratories and sentfor analysis (via overnight delivery) to the
Mayo Medical Laboratories in Rochester,Minnesota. Mayo was selected both becauseof its excellent reputation and because itoffers more porphyrin-related tests thanany other commercial laboratory in theUnited States. A full panel includes testsfor five of the porphyrin-related enzymesinvolved in the heme synthesis pathway[aminolevulenic acid dehydratase (ALA-D), porphobilinogen deaminase, alsoknown as uroporphyrinogen I synthase,
uroporphyrinogen III cosynthase, uropor-phyrinogen decarboxylase, and copropor-phyrinogen oxidase], 6-aminolevulinic acidin urine, porphobilinogen in urine, quanti-tative urinary porphyrins, and fractionatedfecal porphyrins. Results are presented forsix MCS patients from Ziem's practicewho have undergone all these tests andeight others who have undergone most ofthem (Table 1). Data on the three otherpatients screened are not included, as theyeach had undergone only one or two of therecommended tests, although two patientsshowed some abnormalities-one withdecreased coproporhyrinogen oxidase (butno urine or fecal testing) and one withincreased urinary coproporphyrins (but noblood or stool testing). In terms of bothsymptoms and history, the patients testedfor porphyrin disorders were fairly repre-sentative of all chemically sensitive patientsin this medical practice and none wereknown to have any other disorder associ-ated in the literature with abnormal por-phyrin metabolism (such as lead poisoning,hepatitis C, or liver cancer).
Patients diagnosed with MCS anddescribing difficulty with thinking, concen-tration, and/or memory were referred forneurocognitive testing. Those who live nearBaltimore, Maryland, were referred to Dr.James McTamney, a clinical psychologist.As of September 1995, 13 patients hadcompleted testing with Dr. McTamney.Patients in other geographic areas some-times went elsewhere for testing, but becausetesting approaches and the tests used weredifferent, these patients' data are not ana-lyzed here. Dr. McTamney's evaluationincluded the Wechsler Adult IntelligenceScale-Revised (WAIS-R) (Table 2) and theHalstead-Reitan Battery (Table 3). TheHalstead-Reitan Neuropsychological Batteryis generally conceded to be a reliable psy-chological means of identifying patientswith brain damage. It is an individuallyadministered battery composed of the fol-lowing tests: the Category test, the TactilePerformance test, the Seashore Rhythm test,the Speech Sounds Perception test, theFinger Oscillation test, and Trails A and B.
The Category test is a complex test ofnew problem solving, judgment, abstractreasoning, concept formation, mental flexi-bility, and mental efficiency. It requires anumber of higher order functions suchas the ability to note similarities anddifferences among stimuli and to formulatehypotheses regarding the principle thatdetermines the correct answer. It is also atest of learning ability utilizing nonverbal
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997420

PATIENTS WITH CHEMICAL INJURYAND SENSITIVITY
Exposure
Drink one glassof city water
Try on newly dry-cleaned clothing
Walk down detergentaisle in grocery
Use self-serve at thegas station
Use a bathroom with ascented air freshner
Read a freshlyprinted paper
Wear synthetic fabrics
Swim 20 min in achlorinated pool
Wear clothing launderedin chlorine bleach
Wear clothing launderedwith perfumed soap
Use chlorine bleachto clean toilet
Wear clothing dried witha fabric softener
0 10 20 30 40 50 60 70 80 90
Number of respondents
M Yes, aggravates symptoms L No, not aggravating M Not sure or unansweri
Figure 3. Sensitivity to other select brief exposures as reported by Ziem's MCS patients.
Trails A and B do not contribute to theHalstead Impairment index but are consid-ered a part of the Halstead-Reitan Battery.On the Trails A, the person is required toconnect 24 numbered circles distributed ina random pattern while being timed for theperformance. On Trails B, the person isrequired to connect circles numbered 1through 13 and letters A through L alter-nating from number to letter in sequence.
The overall impairment index is calcu-lated as the number of subtests withinthe impaired range divided by the overallnumber of subtests taken.
WAIS-R is a scale of an individuallyadministered composite of tests in batteryformat. For all but the most severelyimpaired adults, a WAIS-R battery consti-tutes a substantial portion of the testframework of the neuropsychologicalexamination. Eleven different subtestsmake up the WAIS-R battery. Six of thesubtests are classified as verbal tests:Information, Comprehension, Arithmetic,Similarities, Digit Span, and Vocabulary.Five are termed performance tests and mea-
~ sure nonverbal/visuospatial factors. The100 tests are Digit Symbol, Picture Completion,
Block Design, Picture Arrangement andObject Assembly.We invite independent scientific review
ed of our actual clinical data to further under-standing of these patients' chemical injuryand chemical sensitivity.
Resultsmaterial. Finally, there is a memory com-ponent to the test that requires the personto remember which principle was correctin determining the answer to an individ-ual item. This requires a longer recall ofpreviously learned correct responses.
The Tactile Performance test is a com-plex test requiring the individual to sustainadequate strength and speed of movement.It also requires the tactile perception andthe ability to form a visual map of theboard. The person, while blindfolded,must place ten blocks with the dominanthand on the first trial and then ten blockswith the nondominant hand on the secondtrial. On the third trial, the individual isallowed to use both hands together. Afterthe trials are completed, the blindfold isremoved and the person asked to draw theblocks approximating their size, shape, andrelationships to one another while theblocks are out of sight.
The Seashore Rhythm test requires theindividual to listen to 30 pairs of rhythmicbeats from a tape recording and to select
the proper response on an answer sheet asto whether the two tones in each pair arethe same or different. The test requires theindividual to discriminate between differ-ent patterns of nonverbal sounds whilemaintaining attention and concentrationthroughout the test.
On the Speech Sounds Perception test,the individual has a sheet of paper onwhich 60 groups of four nonsense wordsare listed. The individual must underlinethe correct response after hearing it on theaudio tape recording.
On the Finger Oscillation test, theindividual is required to tap as rapidly aspossible with the index finger on a smalllever attached to a mechanical counter.The person is given five consecutive 10-sectrials with the preferred hand and then fiveconsecutive trials with the nonpreferredhand. The scores in this test are the averagenumber of taps in a 10-sec period for eachhand. The cutoff point indicating impair-ment would be less than 50 taps per handon average.
The vast majority of these patients reportedsome symptoms occurring daily to almostdaily (Figure 1). Symptoms that couldreflect respiratory responses to irritantexposures were frequent (several times aweek or more): patients indicated nasalsymptoms (60%), sinus discomfort (48%),throat discomfort (53%), weak voice/hoarseness (44%), chest tightness (42%),and wheezing (25%). The higher percent-ages of patients reporting nose and throatsymptoms suggest that irritant effects maybe greatest in the upper respiratory tract-areas that first encounter respiratory irri-tants (nose, throat, etc.)-and less as theseirritants move down the respiratory tract.This is consistent with partial irritantremoval as the inhaled air moves down therespiratory tract.
Frequent symptoms that suggest neuro-logic involvement were reported by manypatients: tremor or shaking (29%), muscletwitching (33%), memory problems(67%), slurred words/difficulty findingwords (58%), coordination difficulties
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997
m
I
I
-7
421

ZIEM AND MCTAMNEY
Table 1. Disorders of porphyrin metabolism in 14 multiple chemical sensitivity patients tested by Mayo Medical Laboratories.a
Selected tests performedProbable causal exposure
Mayo Lab Mayo Lab Pt 1 Pt 2 Pt 3 Pt 4 Pt 5 Pt 6 Pt 7 Pt 8 Pt 9 Pt 10 Pt 1 1 Pt 12 Pt 13 Pt 14normal abnormal F F M F F F M F F M M M M M Outsiderange range 50y 42y 44y 53y 42y 49y 52y 49y 38y 42y 51y ily 47y 55y norm, %
8-Aminolevulinic acid in 1.5-7.5 >7.5urine (marker of ALA synthase (. 6 yr)activity), mg/dlALA-D in erythrocytes,nmol/sec/literPorphobilinogen deaminasein erythrocytes (also known asuroporphyrinogen synthase),nmol/sec/literUroporphyrinogen Illcosynthase in erythrocytes,relative units of activityUroporphyrinogendecarboxylase in erythrocytes,relative units of activityCoproporphyrinogen oxidasein erythrocytes (reticulocytes),relative units of activityPorphyrins in urine (quantitative),mg/24 hrUroporphyrins
Solv B impl Phen OP04 Unk Renov Renov Renov Tce&d Chlord Unk Unk Vocs ClagtNA NA NA NA 2.4 NA NA 2.5 1.7 26.4* 3.8 1.7 2.2 1.2 13
.4.0 <3.5 3.9* 4.0 3.6* 2.8* 4.6 3.2* 2.7* 5.3 7.2 4.7 2.7* 4.2 3.4* 5.0 50
. 7.0 <6.0 7.0 6.2* 6.3* 4.4* 6.9* 4.7* 4.1* 8.8 11.1 7.1 4.1* 7.6 8.6 8.0 50
. 40 < 10 91 83 NA 84 88 88 88 NA 91 86 88 91 86 68 0
1.00-3.00 <0.80 1.53 1.22 1.09 1.04 1.51 2.58 1.06 1.52 1.43 1.43 1.06 2.81 2.02 1.23 0
0.10-0.30 <0.06 0.14 0.10 0.04* 0.09* 0.08* 0.10 0.03* 0.11 0.12 0.05* 0.03* 0.07* 0.08* 0.03* 64
<46 M, >46 M, 8 23* 23 6 6 9 13 8 5 7 13 NA 7 7 822F 22F
Heptacarboxylporphyrins <13 M, >13 M, 2 <3 6 2 1 2 3 1 <1 2 3 NA 4 2 09F 9F
Hexacarboxylporphyrins <5 M, >5 M, <1 <3 3 1 <1 <1 2 3 <1 <1 2 NA 1 <1 04F 4F
Pentacarboxylporphyrins <4 M, >4 M, 2 <3 7* 5* 3 < 1 4 2 < 1 6* 4 NA < 1 2 233F 3F
Copro ortetracarboxylporphyrins <96 M, >96 M, 59 89* 163* 112* 62* 84* 112* 49 28 73 112* NA 89 59 5460F 60F
Porphobilinogen in urine,mg/24 hrPorphyrins in feces (fractionation),9g/24 hrCoproporphyrinsUroporphyrinsProtoporphyrins
< 1.5 >2.0 1.7* NA NA 0.4 1.2 0.1 1.1 0.8 0.8 <0.1 1.1 NA 1.1 0.7 9
<200 > 200 71 NA NA IS 397* 227* 90 170 40 111 90 NA 129 166 20= 1500 > 1500 20 NA NA IS 59* 25 23 115 18 21 23 1 1 30 146 9<1000 >1000 175 NA NA IS 486* 170 189 1206 87 288 189 175 286 1002* 18
"These are not necessarily the same patients as in Tables 2 and 3. Patients 12, 13 and 14 were added after Ziem's presentation at NIEHS Conference on ExperimentalApproaches to MCS: Profile of Patient Characteristics: Chemical Injury and Chemical Sensitivity, 20 September 1995, Princeton, New Jersey. Abbreviations: Pt, patient; F,female; M, male; y, years of age; B impl, breast implant; Chlord, chlordane; Cl agt, cleaning agents; IS, insufficient sample; NA, not available; OP04, organophosphate pesti-cide; Phen, phenol; Renov, renovation (all U.S. EPA headquarters buildings); Solv, solvents; Tce&d, trichlorethylene and Dursban; Unk, unknown; Vocs, volatile organiccompounds (offgassing from new computers). *, a result outside the Mayo reference range of normal.
Table 2. WAIS-R neuropsychological evaluation of 13 multiple chemical sensitivity patients.a
Patient Digit Compre- Picture Picture Block Object Digit IQ,ID Information scan Vocabulary Arithmetic hension Similarities completion arrangement design assembly symbol verbal/performance
1 7 8 10 8 9 12 7 8 9 9 6 104/86*2 12 3 15 9 14 11 3 10 7 7 7 106/88*3 9 12 10 11 8 8 11 8 9 12 11 98/1064 8 6 8 6 8 8 7 7 10 6 9 86/905 8 9 6 7 8 6 5 6 6 5 9 87/856 10 13 11 15 12 8 12 8 10 8 8 112/1057 12 4 11 5 11 13 5 6 7 7 2 96/78*8 8 8 9 8 9 9 9 8 8 8 9 92/949 15 8 12 14 14 10 4 5 7 7 4 118/85*10 7 8 12 5 14 9 6 7 7 10 6 95/8711 12 13 15 8 15 13 10 10 9 6 11 120/105*12 16 12 16 15 12 15 11 15 14 12 11 131/13013 12 12 16 13 14 13 10 7 8 8 6 125/100*
Percent IQ verbal/performance abnormal > 6/13 = 46%
'Same patients as in Table 3. *, significant difference between verbal and performance IQ scores.
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997422

PATIENTS WITH CHEMICAL INJURYAND SENSMVITY
Table 3. Halstead-Reitan neuropsychological evaluation of 13 multiple chemical sensitivity patients.a
Patient Tactile performance test Finger oscillation Trails ImpairmentID CAT TT DOM NDOM BH MEM LOC Rhy Ssds DOM NDOM A B index
1 63* 14'24" 4' 11" 7' 18"* 2'55" 7 4* 3 0 34* 30* 65"1* 155"1* 0.4(25") (44") (18")
2 63* 18'05'* 8'08" 5'39" 4'18" 8 2* 12* 4 21* 20* 60"* 152"* 0.7*(48") (34") (26")
3 17 18'20"* 6'55" 7'15"1* 4'10" 6 2* 5* 9* 49 51 18" 56" 0.5*(41") (43") (25")
4 26 13'05" 4'35" 4'30" 4'00" 5* 2* 2 10* 57 56 27" 82" 0.4(28") (27") (24")
5 83* 16'08"* 5'58" 5'45" 4'25" 4* 2* 8* 10* 23* 20* 66"1* 120"1* 1.0*(36") (35") (27")
6 38 13'00" 7'57" 2'59" 2'04N 7 5 9* 3 55 46 27" 72" 0.3(48") (18") (12")
7 70* 27'58"1* 14'01" 10'01" 3'56" 7 4* 14* 27* 33* 28* 86"* 162"* 0.8*(84") (60") (39")
8 71* 16'20"* 6'00" 7'30"* 2'50" 7 3* 5* 10* 44* 40* 35" 95"1* 0.8*(36") (45") (17")
9 108* 28'54"* 10'3" 13'45"* 5'06" 5* 3* 7* 8* 60 53 50"1* 101"1* 0.8*(60") (82") (30")
10 90* 16'34"* 7'52" 5'24" 3'18" 7 5 1 7 43* 40* 49"* 128"* 0.4(47") (32") (20")
11 108* 13'56" 7'33" 3'20" 3'03" 7 4* 0 4 50 43* 37" 56" 0.4(45") (20") (18")
12 19 10'54" 4'26" 3'54" 2'34" 8 4* 3 3 62 50 25" 37" 0.1(27") (23") (15")
13 55* 17'52"* 5'07" 8'33" 4'12" 8 2* 2 6 44* 43* 49"P* 1 14"* 0.5*(31") (51") (25")
% IMP 9/13 8/13 0/13 3/13 0/13 3/13 11/13 7/13 6/13 7/13 8/13 7/13 8/13 7/1369 62 0 23 0 23 85 54 46 54 62 54 62 54
Abbreviations: % IMP, percent impaired among total tested; BH, time for both hands together; CAT, category test; DOM, time for dominant hand; LOC, location; MEM, mem-ory; NDOM, time for nondominant hand; Rhy, rhythm (seashore); Ssds, speech sounds perceptions test; TT, total time. "Same patients as in Table 2. *, an impaired score.
(49%), and reduced bladder control exposure.) Symptoms suggesting inflam- and outdoor petrochemical air pollutants(27%). The latter suggests possible involve- mation such as swollen glands, muscle dis- (new carpets, pesticides, paint, scentedment of the autonomic nervous system, as comfort/spasm, and joint discomfort also products, etc.); half or more of the patientsdo some other frequently reported symp- were commonly reported to be frequent by reported symptoms when exposed to othertoms such as flushing skin (39%), rapid 21, 49, and 52% of patients, respectively. irritants such as detergents or chlorine. Inpulse (24%), palpitations (25%), reduced Frequent abdominal discomfort was expe- this group of patients, the vast majoritycold tolerance (31 %), and reduced heat rienced by 40%, consistent with abnormal- who reported symptoms with 4-hr expo-tolerance (24%). Based on patient exams ities in porphyrin metabolism, as described sures also experienced symptoms with onlyand Holter monitoring, ectopic heartbeats below. Headache and unusual fatigue were 20-min exposure. This has implications forappear more frequently during exposures frequent in 57 and 69% of patients, reasonable accommodation: requiring dailyand in sicker patients, but these data have respectively. The 40% reporting frequent commuting, work, or even brief meetingsnot been analyzed in the aggregate. Mitral unusual thirst was an unexpected finding in newly carpeted, remodeled or recentlyvalve prolapse, a probable autonomic disor- and may indicate endocrine changes in this pesticide-treated areas could aggravateder, appeared to be unusually common in group. The finding of significant muscu- symptoms in a significant proportion ofour chemically sensitive patients, possibly loskeletal aching and fatigue among MCS persons with chemical sensitivity. It also10% or more, but this too has not been patients is interesting in light of the overlap suggests that many current products andquantified in the aggregate. Murmurs in symptomatology and clinical findings practices involving chemicals (remodeling,seemed to subside with clinical improve- between MCS, fibromyalgia syndrome, deaning, repairs, pesticide application, etc.)ment in some cases. and chronic fatigue syndrome (45). present frequent problems for these patients.
Symptoms of sensory organs were also In response to question 6 (Figure 2), Ziem first encountered cellular immunereported to be frequent by a significant more than two-thirds of the patients abnormalities while evaluating a cluster ofpercentage of MCS patients: changes in reported symptoms with exposure to eight chlordane-exposed patients withhearing (32%), visual changes (48%), and combustion products such as passive ciga- chemical sensitivity in the late 1980s. Sheringing ears (36%). (Clinically, visual rette smoke and vehicle exhaust and to has checked for similar immune abnormali-changes usually involve blurred vision with many other frequently encountered indoor ties in other chemically exposed patients
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 423

ZIEM AND MCTAMNEY
with chemical sensitivity, using the AAL fortesting on the first 68 patients (Table 4).
Compared to lab normals, the majorityof those tested by AAL had increased totalCD26 (also known as TA1) cells, which isconsidered a marker of immune activation(55). Seventeen (25%) had increased CD4(helper T lymphocytes). Only five hadincreased CD8 (suppresser T lymphocytes).NK (CD57) evaluations were done on only15 patients but were reduced in number in5. B lymphocyte (CD 14) values are avail-able for 57 patients; these were reduced in18 (32%) and increased in 1 patient.Judgments of abnormal and normal rangeswere made by the laboratory, but the rawdata and the laboratory's normal referenceranges are provided for independent review.
Autoantibodies were evaluated andfound to be present in increased titer insome cases: antimyelin (nervous system)autoantibodies and antismooth muscle(liver) in about half the patients, withantiparietal (stomach), antibrush border(kidney), antimitochondrial, and antinu-clear in only a small number of patients.AAL considered myelin antibodies abnor-mal if titers were over 1.8; other autoanti-bodies were considered abnormal if titerlevels were 1:20 or greater. Exact titer levelswere not reported (by AAL) but may haveprovided additional information. Ziems'sclinical impression is that as patientsimproved, some titers fell within the labora-tory's normal range, but longitudinal datahave not been quantified in aggregate. Titerlevels facilitate comparison of changes inclinical status with increase or decline intiter levels. The striking proportion withautoantibodies against liver and nervoussystem tissue (about half the total patientstested for each) is consistent with neuro-logic effects and liver involvement, which isconsistent with porphyrin disturbance.
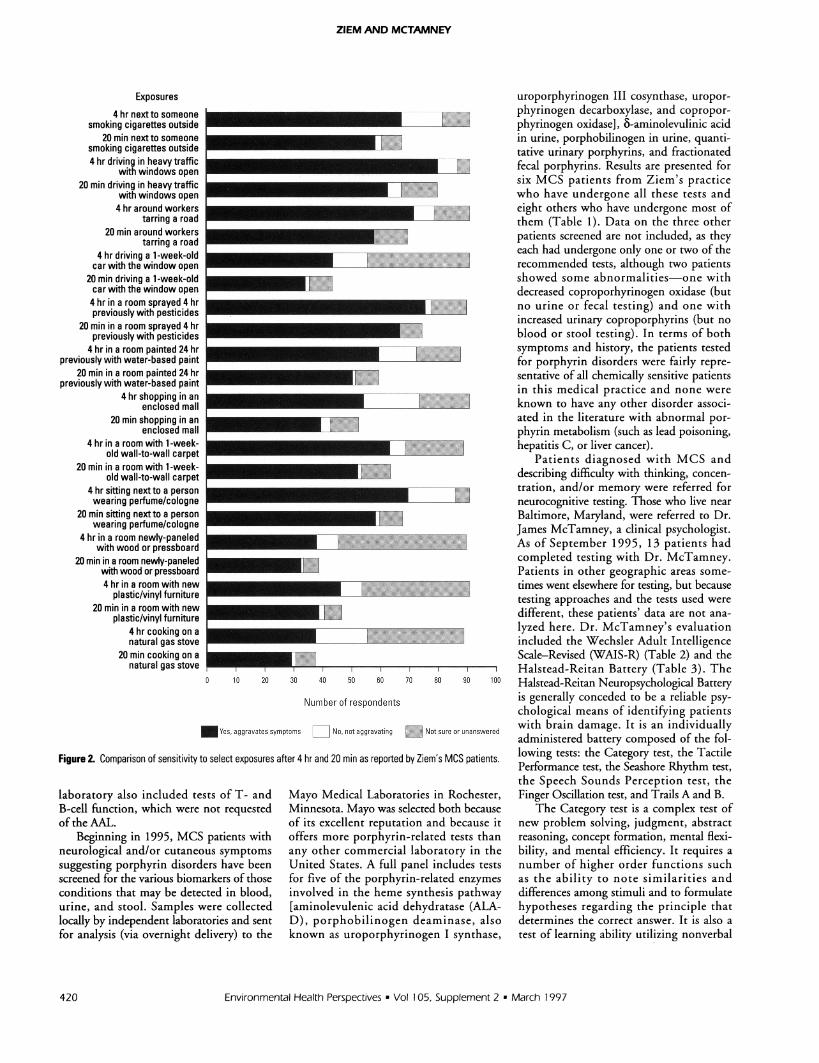
Table 4 also lists the location, situation,and chemical(s) involved in each patient'spresumed causal exposure when this couldbe determined. An exposure was consid-ered causal for this purpose if: there wereno symptoms of multiple chemical sensi-tivity accompanied by chronic illnessbefore the exposure; significant symptomsoccurred during or shortly after the expo-sure (within days); symptoms improvedaway from the exposure on at least twooccasions; and symptoms recurred on reex-posure on at least one occasion. For anyparticular products associated with causalexposures, the chemicals involved wereidentified whenever possible, usually frommaterial safety data sheets.
Over half the patients listed in Table 4were considered occupational in probablecausal exposure: 23 in the private sector(OCP in Table 4) and 14 in governmentor the public sector (OCG). Many public-sector exposures appeared to involve tightbuildings. Public sector reluctance to tacklethe chemical sensitivity problem might beaffected by a substantial number of com-pensation cases filed by public sectoremployees. School exposures accounted foreight cases, all involving pesticides, andprimarily affected students. Home expo-sures involved over a fourth of the totalcases seen by Ziem. Nearly a third of allcases were felt by Ziem to be caused bypesticide exposure.
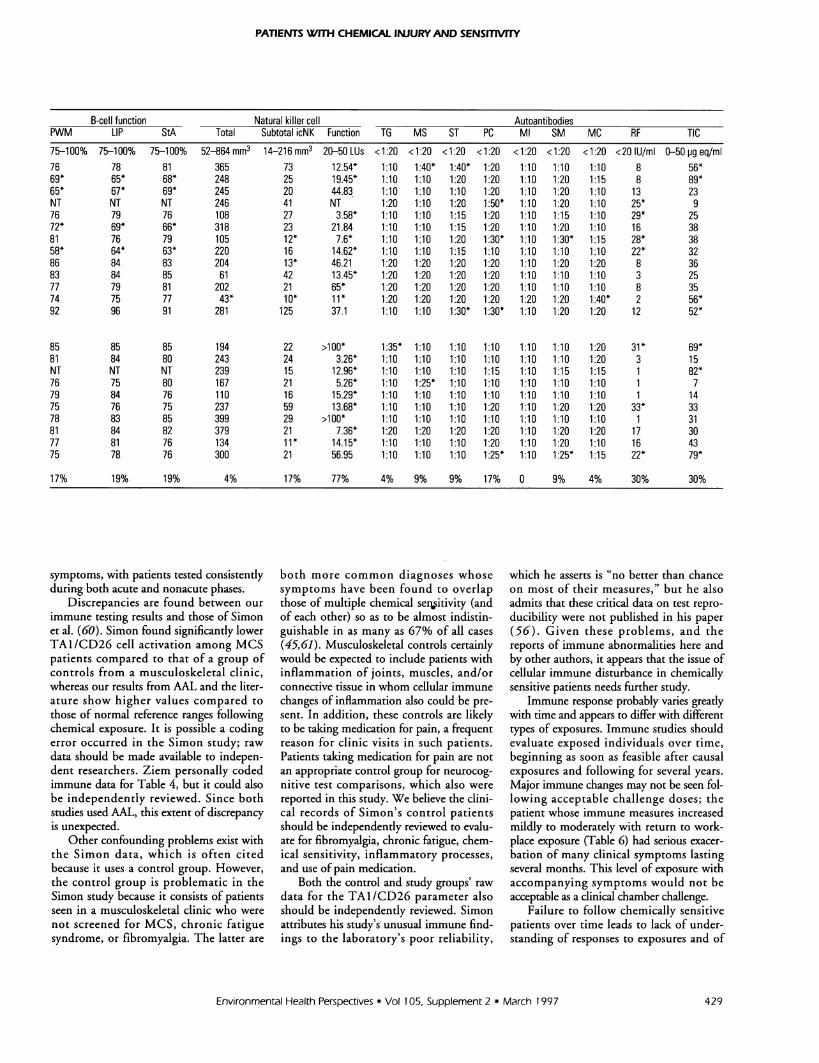
After Simon raised questions about thereliability ofAAL testing in April 1994-hesaid the results of split samples secretly sub-mitted to the laboratory showed that "thereliability on most of their measures is nobetter than chance" (56)-Ziem arrangedfor subsequent immune function testing tobe performed by the ISL. In this presenta-tion of ISL data, both normal and abnor-mal results are shown but only for thoseparticular tests done on more than half thepatients (Table 5). The only ISL dataexcluded after analysis are those on MY,GP, SG, and AS neural autoantibodies,each of which were tested in less than fivepatients, although some other parameterswere not analyzed for this paper.
Autoantibody levels were normalfor most antigens, but 7 of 21 showedincreased levels compared to laboratorynormals for both rheumatoid factor andtotal immune complex. Patients testedthrough ISL typically had normal numbersof total helper and suppresser cells (CD4,CD8) and normal CD26 (TAI) cells.Results from the two laboratories may havediffered because of different normal ranges,different patients being tested, and/or tech-niques; this merits further study. However,abnormalities in ISL tests did includehigher than expected levels of chemicalantibodies (11 of 24 patients), typicallyinvolving benzene, which is most likelyencountered as a metabolite of aromaticpetrochemicals. Reduced T-cell functionwas common (9 of 21 patients tested), with7 of the 9 being abnormal using both con-canavalin A (conA) and phylohemagglu-tinin (PHA), an indication of intratestconsistancy. Impairment of B-cell functionwas seen in five patients, of whom fourwere abnormal in all three tests (pokeweedmitogen, lipopolysaccharide, Staphalococcusaureus). This consistency across tests
increases the likelihood of their validity.While the measure of total NK cells wastypically normal, function was impaired in14 of 22 tested patients.
Immune indicators are likely to changesignificantly over time following exposure,with initial activation leading to a cascadeof other immune changes and later resolu-tion of activation. Thus, single immunemeasurements in a population with varyingtime intervals following various causal andsignificant aggravating exposures are likelyto obscure certain abnormalities. The opti-mal way to study immune changes is toobserve patients shortly after casual expo-sure and to follow them through time. Thetime interval to maximum immune activa-tion and other immune responses and toreturn to preexposure levels, if ever, at thistime is not known for chemically sensitivepatients. Further, different immune mea-sures are likely to peak at different timeintervals following onset of illness.
For a patient whose chemical sensitivitywas thought to be caused by occupationalexposure to carbonless copy paper, wecompared immune measurements beforethe patient left and after she returned toher job, which required sitting near andworking with large quantities of carbonlesscopy paper (Table 6). These data suggestthat immune measures pre- and postchal-lenge testing are unlikely to show majorchanges. The patient had been away fromexposure for many months and showed sig-nificant clinical improvement. Chemicalsensitivity has been seen in a hundredpatients with substantial occupational expo-sure to carbonless copy paper (E Panitz,personal communication).
In 1994, a few physicians began testingfor porphyrin disturbances in chemicallyinjured patients previously diagnosed withMCS. Like patients with some types ofcongenital porphyria, chemically sensitivepatients frequently describe intolerance tosmall amounts of alcohol and many syn-thetic (petrochemical) medications, inges-tion of which provokes acute outbreaks ofneurological and psychological symptomssuch as imbalance, tremor, abdominal pain,and mood swings as well as symptoms orsigns of autonomic involvement such asrapid heart rate and increased blood pres-sure. Patients also sometimes exhibit cuta-neous symptoms of photosensitivity such asskin rashes and other lesions.
Intrigued by informal reports of por-phyrin abnormalities being found in over70% of MCS patients being tested (57),Ziem and her research associate, Albert
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997424

PATIENTS WITH CHEMICAL INUURYAND SENSITMVTY
Donnay, developed a protocol for diagnos-ing disorders of porphyrin metabolism inchemically sensitive patients to try to con-trol for the many variables that may affecttesting for porphyrins and related enzymes(58). The protocol was developed in consul-tation with the porphyria laboratory of theMayo Medical Laboratories and is based onMayo's 1995 test catalog and its 1994 inter-pretive handbook. The protocol includes aone-page patient testing questionnaire(Appendix 3), most ofwhich has been incor-porated into the Health and EnvironmentalHistory Questionnaire. It was surprising tolearn from this questionnaire and verbalinterviewing that even dark brown or redurine (not attributable to blood) was rela-tively common in MCS patients duringmore severe episodes of illness.
It appears that most of the patientsquestioned experienced significant porphy-rialike neurological reactions (includingsharp abdominal pain) when exposed tosuch well-known porphyrogenic stressors asalcoholic beverages (even a single drink wasenough to trigger symptoms), usual thera-peutic doses of many synthetic pharmaceu-ticals, and fasting or skipping meals. Mostof those with skin symptoms also reportedadverse reactions to sunlight exposure.
It was found that because of problemswith memory, concentration, and generalfatigue, patients often experienced diffi-culty understanding and following the nec-essary instructions. A separate patienttesting questionnaire provided a doublecheck on such compliance (Appendix 3).Since many biomarkers of neurological andneurocutaneous porphryinopathy com-monly are known to be abnormal onlyduring periods of acute attack, patientsusually were advised to wait for testinguntil their symptoms were "worse thanusual." Unfortunately, many went for test-ing without waiting for an exacerbation oftheir illness. Of the two biomarkers inurine associated with acute attacks of neu-rological congenital porphyrias, porpho-bilinogen was normal in 10 of 11 patientstested, and 8-aminolevulinic acid was nor-mal in 7 of 8 tested. Despite lacking theseindicators of acute attack, surprisingly 12of the 14 nevertheless tested positive for avariety of other porphyrin-related abnor-malities (defined here as any result outsideMayo's range of normal).
Of the 13 patients tested for 5 differenturinary porphyrins, 8 had at least oneabnormality. Four patients had only ele-vated coproporphyrins, 1 had only elevatedpentacarboxylporphyrins, 2 had elevations
in both of these, and 1 had elevated copro-porphyrins and uroporphryins. Of the 11patients with stool evaluations, 3 showedabnormalities: 1 had only elevated copro-porhyrins, 1 had only elevated protopor-phrins, and the third patient had elevatedcopro-, uro- and protoporphyrins. Thosewith elevated fecal coproporphyrins also hadelevated urinary coproporhyrins. Onepatient submitted a stool specimen thatMayo felt was too small to represent a 24-hrsample, so this result was not included.
All patients were given blood tests forthe activity of porphyrin-related enzymes.The most common enzyme deficiency wasin the activity of coproporhyrinogen oxidase(CpgO), which was below normal in 9 ofthe 14 patients tested. CpgO was evaluatedin reticulocytes in conjunction with a reticu-locyte count which, because of lab confu-sion was done in most but not all patients.When completed, the reticulocyte countswere normal. The activity of both ALA-Dand porphobilinogen deaminase (PbgD)was below normal in 7 of the 14 patients.Uroporphyrinogen decarboxylase and uro-porphyrinogen III co-synthase activity wastested in 12 and 14 patients, respectively,and found to be normal in all cases. Onlytwo patients had no enzyme deficiencies;four had one deficiency each, four had twoeach, and four had three each (ALA-D,PbgD, and CpgO). The enzymes affectedhere occur in cytosol and mitochondria(59), and the presence of disturbed enzymesin both these compartments suggests chemi-cal injury to both mitochondrial and cytosolcellular areas.
Despite lack of a control group, it isdifficult not to conclude that porphyrindisturbances are present in a substantialpercentage of chemically sensitive patients.The multiple enzyme deficiencies found inmany of these MCS patients (6 of 14) arenot characteristically associated with any ofthe known types of congenital porphyria,which usually are marked only by a singleenzyme deficiency or with secondarycoproporphyrinuria due to other unrelatedconditions, usually an isolated abnormal-ity, unaccompanied by enzyme deficien-cies. (Because of testing techniques atMayo, when porphobilinogen deaminase isreduced, ALA-D can also appear to bereduced, so the presence of these twoabnormalities together cannot be presumedto involve two enzymes.) Given also thatnone of the patients tested had knownfamily histories of active or latent por-phyria, the fact that such relatively rareabnormalities and porphyrialike symptoms
were found in 12 of 14 patients stronglysuggests that those with MCS suffer froman environmentally acquired rather than aninherited disorder of porphyrin metabo-lism. (A genetic predisposition cannot beruled out conclusively without further test-ing the patients and family members, butstatistically such a finding is highly unlikely,since congenital porphyrias are so rare.)
Although the porphyrin disturbancesand enzyme deficiencies found in theseMCS patients appear to be milder than inthe acute types of congenital porphyriathat primarily affect heme synthesis in theliver, other organs clearly are affected incases of toxic exposure and chemical injury(e.g., irritant effects on the respiratory sys-tem, petrochemical neurotoxicity, immunedysfunction). These factors together withthe involvement of multiple enzyme defi-ciencies may account for the somewhatmore diverse symptomatology seen inMCS patients compared to those withstrictly congenital porphyria. This cer-tainly is the case with other toxicallyacquired porphyrinopathies such as thewell-recognized forms caused by overexpo-sure to lead, dioxin, and hexachloroben-zene, all of which, as neurotoxins, affectmore than just heme synthesis and causechemical injury unrelated to porphyrinabnormalities. Given all the above, it isnot unreasonable to suspect that the differ-ent patterns of porphyrinopathy evident inMCS patients may be caused and/or exac-erbated by these patients' own uniqueoverexposures to specific toxic chemicals.
On the WAIS-R neuropsychologicalevaluation done by McTamney (Table 2), 6of the 13 MCS patients tested showed a sig-nificant difference of 15 points between theverbal and performance phases of the test,all scoring higher on the verbal portion.Only one patient scored in the superiorrange for IQ with no apparent difficulties.
The Halstead-Reitan battery showed anumber of significant scores indicatingimpairment (Table 3). On the Category test,53% of patients scored in the impairedrange. On the Tactile Performance test,60% scored in the impaired range on thetotal time required to complete the threetrials. None of the patients had problemswith the dominant hand, while 30% wereslower with the nondominant hand despitethe previous trial with the dominanthand. Twenty-three percent of patientsscored in the impaired range on the mem-ory phase of the Tactile Performance test,while 84% scored in this range on theLocalization Scale.
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 425

ZIEM AND MCTAMNEY
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997
V
Co
2V
0 C C%I._,.am °;-
CDNV
LO
C,,
V
BR_
LO
~C14co
C.)
ae
LoCVco
C.,
c c
Le)
Co
Co
Co
0
.0e
U4
2 S;CD
co
0
0toa._
I0
cn
Q
to
CoW
la
0
CEa
A_
E
CD
co
0.
co
co
EEI-
426
PATIENTS WITH CHEMICAL INJURYAND SENSITITY
U Z Z:.g 2 Zi Z zX;szi ,M,I:~~~~~~C
z z z C.4
" ~~~~ ~~~~,m,,,, _.0.- >' ''j <* $ se
2t.~~~ ae 2s..::¢z.w-z 'z m sz z C s.sw.pi, Bs wS eS _.#.Rt. .............<$rws#w$|#:a...,,.s,. .w | $ t Et. j .. w , $$C
otz zt 5ez.t ......z.......z" z... z.'y''''' &'','' 's'Lt
s$5L X Z ,W '$ ,,. . ,,,Z L z SgfC CL
Environmental Health Perspectives - Vol 105, Supplement 2 * March 1997
CD
V
o v
Cv
oJ oXvC)
vC-,
CD
U,CD
C-) aR-C_
CD
C3
SLO
CC4CD
C-)
ae
0
CO4
C~
in:
Le)
C-)
*LOBe
aR L
UDat
amC=co
2= 0
0a a
-5D0
Uc
0
I'D
Co
cn
CL
6
XCDo._
g
co
cJ L6
cno
.a'na)CDX C'CD c-
Co
X zC-) Q:
' E-o
u
co *-
-0C/) -
c a)
_o M
C) m
coj.n z
Co
CD.
cocm_
m a)~2
Ecnz
coX_ a
C )
.CD
CD EE on
c' E._ e
E
co >oa)
CD
<s
'a*;:;c
a
Q-)
3S0
427

ZIEM AND MCTAMNEY
Table 5. Immune panels of 23 multiple chemical sensitivity patients tested by Immunosciences Laboratory from April 1994.
T-cell functionID Sex CD4 Total CD8 Total CD26 Total Chemical antibodies GGT SIgA D-GA conA PHA
Normals > 336-2376 192-1598 0-432 IgE,lgG<(16) IgM<(64) 5-35 U/ml 10-28 pg/ml 1-5 mol/mol crea 75-100% 75-100%1 M 1270 610 270 IgG BEN (32)* NT NT NT 85 782 F 1740 250 320 IgG BEN (24)* 232* NT NT 50* 52*3 F 1100 450 220 IgG ISO (24)*, IgG BEN (72)* 10 NT NT 58* 61 *4 M 760 660 180 IgG BEN (24)* 23 4* 5 NT NT5 F 1400 680 410 IgG TMA (24)*, IgG BEN (40)* 21 NT NT 62* 756 F 1200 660 160 IgG BEN (32)* 10 17 3 68* 65*7 F 640 370 130 IgM TMA (200)* 12 9* 5 75 788 M 660 510 820* All normal 34 4* 5 61* 62*9 F 1572 489 102 All normal 20 9* 5 88 8210 M 802 511 150 All normal 18 4* 7* 80 7511 M 1313 586 224 All normal 27 13 5 75 7812 F 1080 301 31 All normal 13 NT 5 66* 7213 F 1120 1030 250 IgG FOR (64)*, IgG ISO (64)*, 16 1* 4 88 82
IgG TMA (32)*, IgG PA (32)*,IgG BEN (64)*
14 F 1080 650 110 All normal 18 NT 4 80 7515 F 1120 900 120 All normal 22 8* 4 76 7916 M 590 620 80 All normal 20 15 6* NT NT17 F 1090 480 150 IgM BEN (96)* 18 NT NT 59* 62*18 F 790 360 130 All normal 11 NT NT 63* 65*19 M 870 570 180 All normal 9 25 4 79 7620 F 1400 800 370 All normal 6 25 4 82 8421 F 1180 300 170 IgM BEN (128)* 15 4* 5 79 7822 F 580 190 70 IgG BEN (24)* 10 NT NT 89 110*23 F 860 770 170 All normal 27 4* 4 61* 92
1053 554 209 e- Average0 0 4% < % Abnormal - 5% 64% 13% 43% 30%
Abbreviations: conA, concanavalin A; crea, creatinine; D-GA, D-glucaric acid (urine); GGT, gamma-glutamyltransferase; icNK, immunocompetent NK; LIP, lipopolysaccharide;LUs, lytic units; NT, not tested; PHA, phytohemagglutinin A; PWM, pokeweed mitogen; SIgA, secretory IgA; StA, Staphaloccoccus aureus. Autoantibody codes: MC, myocar-dial; Ml, mitochondrial; MS, microsomal; PC, parietal cell; RF, rheumatoid factor; SM, smooth muscle; ST, striated muscle; TG, thyroglobulin; TIC, total immune complex.Chemical antibody codes: BEN, benzene; FOR, formaldehyde; ISO, isocyanates; PA, phthalic anhydride; TMA, trimellitic anhydride. *, abnormal results.
Table 6. Immune panels of a multiple chemical sensitivity patient before and after exposure to carbonless copypaper.
Immune tests performed by ISL normal Before,patient's After patient'sImmunosciences Laboratory (ISL) ranges exposure, 10/10/94 exposure, 10/13/94
Lymphocytes 960-4320 1568 2088T-cells 701-3788 1150 1550T helpers 336-2376 790 1090T suppressers 192-1598 360 480B-cells 48-648 300 420Natural killer cells 52-864 110 167Immunocompetent NK cells 14-216 16 21TAl 0-432 130 150Gamma-glutamyltransferase 4-22 1 1 18IgG myelin basic protein 0-100 25 40IgM myelin basic protein 0-50 10 20IgA myelin basic protein 0-20 15 10Total immune complex 0-50 14 7IgM trimellitic anhydride* 0-64 8 32IgM benzene* 0-64 8 64PHA 75-100 65 62conA 75-100 63 59NK activity 20-50 15.29 5.26
other chemical antibodies were tested but only those shown increased.
The Rhythm Test showed 53% in theimpaired range, whereas the SpeechSounds Perception Test showed 46% inthe impaired range. On the FingerOscillation Test, 53% scored in theimpaired range with the dominant handand 61% for the nondominant hand.Trails A had 53% in the impaired range,whereas Trails B showed 61%. The overallImpairment Index scores showed 53%impairment. The most common neuro-logic changes on the physical exam werereduced vibratory perception (hands) andabnormal Romberg (suggesting vestibularneuropathy).
DiscussionChemically sensitive patients from a med-ical practice, who often have experienceddifferent initiating exposures, may havedifferent patterns of porphyrin disturbance,as was found in this study. This is the pat-tern to be expected from the literature onacquired porphyrin disturbance. Futureresearch on porphyrin abnormalitiesshould compare results by type of originalexposure and by type and level of current
Environmental Health Perspectives l Vol 105, Supplement 2 * March 1997428
PATIENTS WITH CHEMICAL INJURY AND SENSITMTY
B-cell function Natural killer cell AutoantibodiesPWM LIP StA Total Subtotal icNK Function TG MS ST PC Ml SM MC RF TIC75-100% 75-100% 75-100% 52-864 mm3 14-216mm3 20-50 LUs < 1:20 < 1:20 < 1:20 < 1:20 < 1:20 < 1:20 < 1:20 <20 IU/ml 0-50 pg eq/ml76 78 81 365 73 12.54* 1:10 1:40* 1:40* 1:20 1:10 1:10 1:10 8 56*69* 65* 68* 248 25 19.45* 1:10 1:10 1:20 1:20 1:10 1:20 1:15 8 89*65* 67* 69* 245 20 44.83 1:10 1:10 1:10 1:20 1:10 1:20 1:10 13 23NT NT NT 246 41 NT 1:20 1:10 1:20 1:50* 1:10 1:20 1:10 25* 976 79 76 108 27 3.58* 1:10 1:10 1:15 1:20 1:10 1:15 1:10 29* 2572* 69* 66* 318 23 21.84 1:10 1:10 1:15 1:20 1:10 1:20 1:10 16 3881 76 79 105 12* 7.6* 1:10 1:10 1:20 1:30* 1:10 1:30* 1:15 28* 3858* 64* 63* 220 16 14.62* 1:10 1:10 1:15 1:10 1:10 1:10 1:10 22* 3286 84 83 204 13* 46.21 1:20 1:20 1:20 1:20 1:10 1:20 1:20 8 3683 84 85 61 42 13.45* 1:20 1:20 1:20 1:20 1:10 1:10 1:10 3 2577 79 81 202 21 65* 1:20 1:20 1:20 1:20 1:10 1:10 1:10 8 3574 75 77 43* 10* 1 1 * 1:20 1:20 1:20 1:20 1:20 1:20 1:40* 2 56*92 96 91 281 125 37.1 1:10 1:10 1:30* 1:30* 1:10 1:20 1:20 12 52*
85 85 85 194 22 >100* 1:35* 1:10 1:10 1:10 1:10 1:10 1:20 31* 69*81 84 80 243 24 3.26* 1:10 1:10 1:10 1:10 1:10 1:10 1:20 3 15NT NT NT 239 15 12.96* 1:10 1:10 1:10 1:15 1:10 1:15 1:15 1 82*76 75 80 167 21 5.26* 1:10 1:25* 1:10 1:10 1:10 1:10 1:10 1 779 84 76 110 16 15.29* 1:10 1:10 1:10 1:10 1:10 1:10 1:10 1 1475 76 75 237 59 13.68* 1:10 1:10 1:10 1:20 1:10 1:20 1:20 33* 3378 83 85 399 29 >100* 1:10 1:10 1:10 1:10 1:10 1:10 1:10 1 3181 84 82 379 21 7.36* 1:20 1:20 1:20 1:20 1:10 1:20 1:20 1 7 3077 81 76 134 11* 14.15* 1:10 1:10 1:10 1:20 1:10 1:20 1:10 16 4375 78 76 300 21 56.95 1:10 1:10 1:10 1:25* 1:10 1:25* 1:15 22* 79*
17% 19% 19% 4% 17% 77% 4% 9% 9% 17% 0 9% 4% 30% 30%
symptoms, with patients tested consistently both more common diagnoses whose which he asserts is "no better than chanceduring both acute and nonacute phases. symptoms have been found to overlap on most of their measures," but he also
Discrepancies are found between our those of multiple chemical serjitivity (and admits that these critical data on test repro-immune testing results and those of Simon of each other) so as to be almost indistin- ducibility were not published in his paperet al. (60). Simon found significantly lower guishable in as many as 67% of all cases (56). Given these problems, and theTAI/CD26 cell activation among MCS (45,61). Musculoskeletal controls certainly reports of immune abnormalities here andpatients compared to that of a group of would be expected to include patients with by other authors, it appears that the issue ofcontrols from a musculoskeletal clinic, inflammation of joints, muscles, and/or cellular immune disturbance in chemicallywhereas our results from AAL and the liter- connective tissue in whom cellular immune sensitive patients needs further study.ature show higher values compared to changes of inflammation also could be pre- Immune response probably varies greatlythose of normal reference ranges following sent. In addition, these controls are likely with time and appears to differ with differentchemical exposure. It is possible a coding to be taking medication for pain, a frequent types of exposures. Immune studies shoulderror occurred in the Simon study; raw reason for clinic visits in such patients. evaluate exposed individuals over time,data should be made available to indepen- Patients taking medication for pain are not beginning as soon as feasible after causaldent researchers. Ziem personally coded an appropriate control group for neurocog- exposures and following for several years.immune data for Table 4, but it could also nitive test comparisons, which also were Major immune changes may not be seen fol-be independently reviewed. Since both reported in this study. We believe the clini- lowing acceptable challenge doses; thestudies used AAL, this extent of discrepancy cal records of Simon's control patients patient whose immune measures increasedis unexpected. should be independently reviewed to evalu- mildly to moderately with return to work-
Other confounding problems exist with ate for fibromyalgia, chronic fatigue, chem- place exposure (Table 6) had serious exacer-the Simon data, which is often cited ical sensitivity, inflammatory processes, bation of many clinical symptoms lastingbecause it uses a control group. However, and use of pain medication. several months. This level of exposure withthe control group is problematic in the Both the control and study groups' raw accompanying symptoms would not beSimon study because it consists of patients data for the TAI /CD26 parameter also acceptable as a clinical chamber challenge.seen in a musculoskeletal clinic who were should be independently reviewed. Simon Failure to follow chemically sensitivenot screened for MCS, chronic fatigue attributes his study's unusual immune find- patients over time leads to lack of under-syndrome, or fibromyalgia. The latter are ings to the laboratory's poor reliability, standing of responses to exposures and of
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 429

ZIEM AND MCTAMNEY
removal from exposure. We are followingmore than 300 chemically sensitivepatients and have observed both significantclinical improvement with reduced expo-sures and clinical exacerbation on reexpo-sure (including increased abnormalities onexam and laboratory testing). This is a clin-ical impression, although it is not quanti-fied in aggregate for this paper. It appearsthat to date the professionals who havepublished studies suggesting a psychologi-cal origin of chemical sensitivity do not fol-low these patients over time, do notremove them from exposure and observeresponses and then return them to expo-sure and observe responses. Also, theseresearchers are not physicians treatingpatients for the disorder, and therefore arenot able to observe the ongoing clinicalcourse of the illness.
We reported onset of chemical sensitivityshortly following exposure to a wide varietyof petrochemicals, combustion products,and irritants (Table 4). In some cases thesewere discrete events such as leaks, spills, orother acute exposure events. Often, espe-cially in occupational settings, exposureswere chronic. Typically, in these situationsthe illness began as a more limited sick-building syndrome, which with furtherexposure developed into chronic illness withassociated chemical sensitivity. This suggeststhat exposure controls in the early phasemay prevent the more disabling phase, andthat sick-building syndrome is a more self-limited form of chemical sensitivity.
The combined abnormalities of theimmune, respiratory, porphyrin, and ner-vous systems discussed here are incompati-ble with a psychologic etiology for chemicalsensitivity. A systematic review of ten recentstudies purporting to show a psychologicorigin for chemical sensitivity revealed seri-ous methodologic flaws in all studiesincluding the Simon study, sufficient forthe reviewing authors to conclude thatnone of the studies had the methodologicstrength to determine that chemical sensi-tivity was psychologically induced (40).
Vasospasm appears to be a problem inchemically sensitive patients. Most of ourpatients noted frequent headaches thatoften were consistent with migraine anddiagnosed as such by other evaluatingphysicians. Migraine is known to be trig-gered by chemical odors (62) and involvesabnormal vasospasm. Cerebral vasospasmwith reduced cerebral blood flow has beenreported with encephalopathy following sol-vent exposure (63) and in patients withchemical sensitivity (42,64,65). One of our
patients developed new onset of Raynaud'sphenomenon (a vasospastic disorder), whichwe observed to be triggered by double-blinded finger contact with carbonless copypaper (the probable cause of her chemicalsensitivity). Only a few patients developednew onset of high blood pressure (anothervasospastic response), which is seen primar-ily following exposure (their blood pressurereadings usually remained normal betweenexposures). These vasospastic responses mayinvolve abnormal autonomic function,which has been observed to occur withchemical sensitivity (35).
Diagnoses of fibromyalgia and chronicfatigue syndrome are common among ourMCS patients (currently 75 and 85%,respectively). We recommend furtherresearch on the incidence of chemical sensi-tivity in these groups using the types ofscreening questionnaires developed byKipen, Bell, and Davidoff. If these disor-ders are essentially the same, much of theresearch already done for fibromyalgia andchronic fatigue syndrome may also apply toMCS; this could reduce research costs andtime delays. Increased sensitivity to chemi-cals also occurs with migraine, asthma, andother disorders. However, fibromyalgia syn-drome, chronic fatigue syndrome, and por-phyrin disorders are multiple-systemdisorders involving chemical sensitivity.
Over one-third of our patients describedtremor several times or more a month(Figure 1). Several patients were told byother physicians that they were developingParkinson's disease during more seriousperiods of their illness only to have thediagnosis rescinded when they improvedafter environmental controls were put inplace to reduce exposures. Parkinson's dis-ease has been reported following pesticideexposure (66).
Nearly half our patients reportedincreased symptoms during or after swim-ming in a chlorinated pool (Figure 3),which has been associated with increasedchloroform levels (67). Patients also oftenreported reduced symptoms during andafter showering with, compared to without,an activated charcoal filter that helpsremove chloroform. Longer showers and/orthose with greater flow rates release morechloroform and other chlorinated products.Water filters that reduce chlorine thereforeappear to be a reasonable control for MCS.
In addition to filters for chlorinatedwater, other reasonable means exist tocontrol exposures that aggravate MCSsymptoms. Aggravation from vehicleexhaust (Figure 2) can be reduced by using
an auto filter device that provides activatedcharcoal filtration and by avoiding ozonat-ing devices which generate irritants.Symptom exacerbation from pesticides,cleaning products, building materials, etc.can be reduced by using less toxic prod-ucts. Reasonable accommodation at thework place, at home (apartments, condo-miniums, etc.) and at school and publicareas could be available to those with thisdebilitating condition by requesting thatless toxic products and procedures be used.Further helpful suggestions are discussed inour Environmental Control Plan (68).
In our 10-year experience with chemi-cally sensitive patients, no patients lost theirsensitivity to chemicals. No patients wereable to go to problem environments (newcarpets, recent pesticides, etc.) consistentlywithout deterioration of their conditions.Thus, MCS should be considered a perma-nent condition. Some patients were able tocontinue working if their employers pro-vided nontoxic accommodations for theirconditions. More than half the patientscontinued to be too sick to work under theprevailing conditions at the work place. Webelieve this proportion could be reduced ifsociety pays more attention to use of non-toxic products.
The large and growing epidemic ofchemical sensitivity in the United States ispartly because of inadequate exposure lim-its for chemicals. These exposure limitshave been shown to lack scientific merit(69) and to have been seriously influencedby vested interests (70-73). Exposures thatcause MCS at home or the work placesometimes reflect relatively widespreadpractices or products, some of which maybe within legal limits. Many aggravatingexposures are probably below legal limitsbut often do not provide an adequatesafety margins even for the healthy popula-tion (69). The widespread indoor use ofpesticides in U.S. schools, homes, workplaces, and public buildings is in strikingcontrast to practices in Germany andScandinavia. Major policy changes withregard to chemical product formulationand use will be necessary to reduce futurecases of permanent chemical sensitivity aswell as to reduce disability for currentlyaffected patients.
SummaryMost of our patients with symptoms ofMCS appear to have developed chronicillness following exposure to petrochemi-cals, combustion products, and other irri-tants. Symptoms and signs in patients
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997430

PATIENTS WITH CHEMICAL INJURYAND SENSIMiVITY
reporting chemical sensitivity suggestinvolvement of the immune, respiratory,limbic, and other nervous systems (central,peripheral, autonomic) as well as impairedporphyrin metabolism. This suggests thatmultiple mechanisms of chemical injuryprobably are involved, all of which canintensify response to an exposure. Immuneactivation, neurogenic inflammation (74),kindling (75), and/or time-dependent sen-sitization (76) can amplify the body'sresponse to chemical exposure in theimmune system, respiratory system, andnervous system. It is possible that impairedporphyrin metabolism reduces the amountof heme available for cytochrome P450,part of the liver's major detoxification sys-tem for foreign chemicals, which couldresult in intensified symptoms for a widerange of exposures.
Research strategies are needed that allowevaluation of multiple sites of chemical
injury and multiple mechanisms of injury-almost all studies to date focus on only onetype of chemical injury.
Immune activation also could lead toincreased response to foreign substances,such as conventional allergens. We note inour patients an apparent high rate of newonset of allergies to mold, dander, etc., fol-lowing onset of chemical sensitivity. Kipenreports what appears to be a significantlevel of sensitivity to chemicals amongasthmatics (77). Asthma also is increasedwith higher levels of indoor volatileorganic compounds (VOCs), formalde-hyde and/or limonene (78). Persons withother allergic diatheses also should bestudied for sensitivity to chemicals. Ifindeed chemical exposure via immuneactivation contributes significantly to thehigh and increasing rates of allergies,we may have the means to counter thisalarming trend.
Studies of chemically injured popula-tions should compare MCS patients withspecific and identifiable initial exposures toMCS patients who cannot identify anyspecific triggering exposure. Other patientgroups that should be studied for MCSinclude those with recurring migraines,chronic sinusitis or rhinitis, degenerativeneurologic diseases (such as acute types ofcongenital porphyria), autoimmune disor-ders (such as multiple sclerosis, autoim-mune hepatitis, rheumatoid arthritis, andlupus), hyperactive children, and patientswith attention deficit disorder. Chemicallyexposed groups also merit study, especiallythose that have avoided further occupa-tional exposures following work with pesti-cides, solvents, etc. We believe such studieswill find levels of chemical sensitivity inthese subpopulations that are considerablygreater than currently recognized.
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 431

ZIEM AND MCTAMNEY
Appendix 1. Question 14 from Ziem's Health and Environmental History Questionnaire
14. For the symptoms and health problems listed below, if you have had the problem in the last year,CIRCLE the number that best describes how often the symptom occurs, or circle 7 if not sure.
Daily to Several OnceAlmost Times/ ADaily Week Week
SeveralTimes/Month
Once/MonthOr Less
Headache1 2 3 4 5Numbness, tingling1 2 3 4 5Weakness in a body part1 2 3 4 5Lightheadedness, dizziness1 2 3 4 5Tremor or shaking1 2 3 4 5Muscle twitching1 2 3 4 5Confusion, spaciness, inability to concentrate1 2 3 4 5Memory problems1 2 3 4 5Slurred words, difficulty finding words1 2 3 4 5Coordination difficulties1 2 3 4 5Low energy, fatigue (unusual)1 2 3 4 5Dizziness when standing up after sitting1 2 3 4 5Shakiness relieved with eating1 2 3 4 5Poor appetite1 2 3 4 5Sweet Cravings1 2 3 4 5Unusual thirst1 2 3 4 5Itchy, watery eyes or nose1 2 3 4 5Visual changes1 2 3 4 5Ringing ears1 2 3 4 5Changes in hearng1 2 3 4 5Nasal symptoms (discharge, stuffiness)1 2 3 4 5Sinus discomfort1 2 3 4 5Throat discomfort (soreness, tightness)1 2 3 4 5Weak voice, hoarseness1 2 3 4 5Fever1 2 3 4 5Reduced cold tolerance1 2 3 4 5Reduced heat tolerance1 2 3 4 5Swollen glands1 2 3 4 5Coughing1 2 3 4 5Chest discomfort (heaviness, pain)1 2 3 4 5
RarelyIf Ever
NotSure
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6 7
6
6
6
6
6
6
7
7
7
7
7
7
Daily to Several Once Several Once/Almost Times/ A Times/ Month Rarely NotDaily Week Week Month Or Less If Ever Sure
Chest tightness1 2 3 4 5 6 7Wheezing1 2 3 4 5 6 7Muscle discomfort, spasm1 2 3 4 5 6 7Joint discomfort1 2 3 4 5 6 7Rapid pulse1 2 3 4 5 6 7Palpitations (rapid, violent throbbing, extra, or skipped heartbeats)1 2 3 4 5 6 7Swelling of ankles1 2 3 4 5 6 7Swelling (throughout body)1 2 3 4 5 6 7Bruising without a cause1 2 3 4 5 6 7Itching, rash, hives1 2 3 4 5 6 7Flushing skin1 2 3 4 5 6 7Reduced bladder control1 2 3 4 5 6 7Need to pass urne frequently1 2 3 4 5 6 7Insomnia1 2 3 4 5 6 7Frequent jerking in sleep1 2 3 4 5 6 7Other sleep disturbance1 2 3 4 5 6 7Fingertips turning white or blue1 2 3 4 5 6 7Menstrual Changes (women)1 2 3 4 5 6 7Impotence, reduced ability for erection (men)1 2 3 4 5 6 7Significantly reduced sex drive1 2 3 4 5 6 7Other sexual problems1 2 3 4 5 6 7Difficulty or discomfort with swallowing1 2 3 4 5 6 7Reflux of stomach acid1 2 3 4 5 6 7Nausea, vomiting, bloating, gas1 2 3 4 5 6 7Abdominal discomfort (pressure, pain, cramps)1 2 3 4 5Brown, green, or red unne-not due to blood1 2 3 4 5Symptoms increased in sunlight1 2 3 4 5Rash when exposed to sunlight1 2 3 4 5Other (specify):
6 7
6 7
6 7
6 7
1 2 3 4 5 6 7
Environmental Health Perspectives - Vol 105, Supplement 2 * March 1997432

PATIENTS WITH CHEMICAL INJURYAND SENSITMTY
Appendix 2. Question 6 from Ziem's Health and Environmental History Questionnaire
6. For each situation described below, answer the questions at the top of each column.By "sick," we mean anything that YOU consider to be either a major or a minor health problem.
a. Would you be sick if you hadto spend 4 hours...?
No A Little Moderatelv
A Lot Don'tKnow
s ^s . fi. ^ .^ -- -- ^^ --Ub. Would you be sick if you hadto spend 20 minutes ...?
No A Little Moderatelv
a Next to someone smoking l tcigarettes outside.
b. Driving in heavy traffic withwindows open.
c. Around workers taning a road.For the next questions, assume you are inside with no open windows...
d. In a room sprayed with pesticides4 hoursago.
a In a room painted 24 hours agowith water-based paint.
f. Shopping in an enclosed mall.g. In a room with
wall-to-wall carpet(1 week old).
h. Sitting next to a person wearingperfume/cologne.
l. Cooking on a stove using naturalgas.
j. Being around or using carbonlesscopy paper ___
k Sitting next to someone with fabricsoftener on clothing. I I I I
~~- -Would you be sick if you had to ..? No A Little Moderately ALot Don't Know
I. Dnnk one glass of city (chlorinated) water.
m. Try on newly dry cleaned clothing.
n. Walk down the detergent aisle at a grocery store.
o. Use self-serve at a gas station.
p. Use a bathroom with a scented air freshener.
q. Read a freshly printed newspaper.
r. Wear synthetic fabrics.S Swim for 20 minutes in a chlorinated pool.
t. Wear clothing that has been laundered in chlorine bleach.
u. Wear clothing laundered with perfumed laundry soap.
V. Use chlorine bleach in your toilet.
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997
Exposures: A Lot IDon'tKnow
433
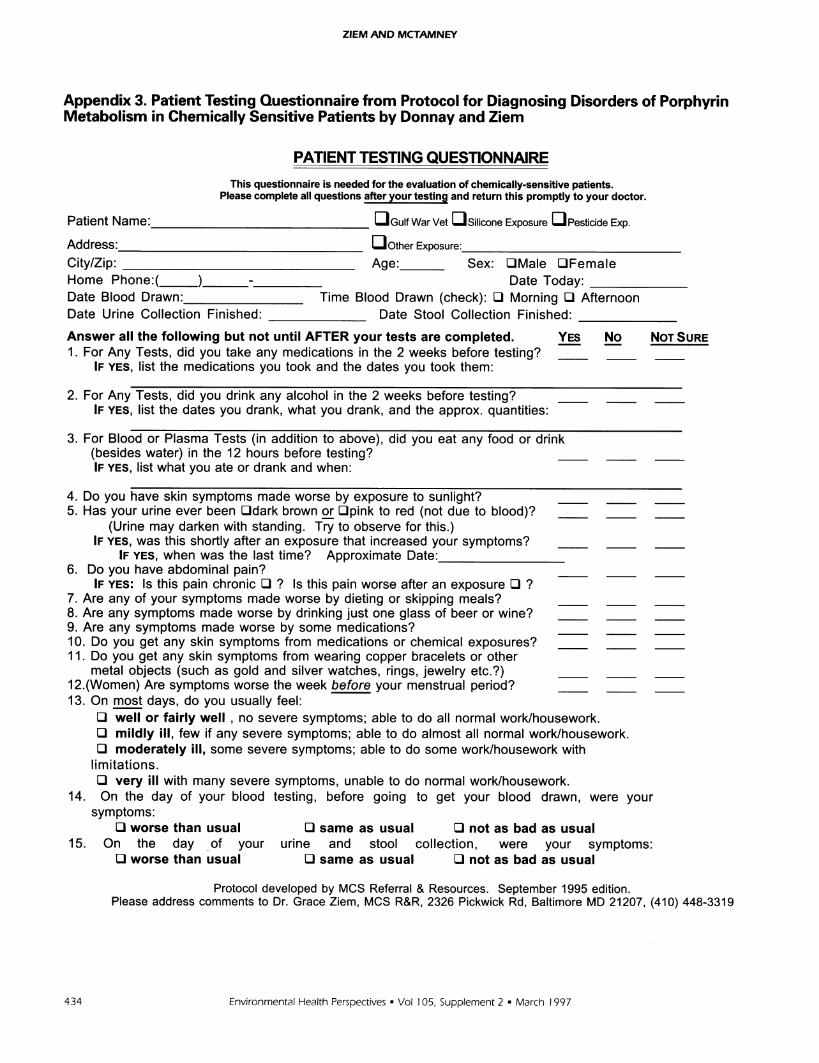
ZIEM AND MCTAMNEY
Appendix 3. Patient Testing Questionnaire from Protocol for Diagnosing Disorders of PorphyrinMetabolism in Chemically Sensitive Patients by Donnay and Ziem
PATIENT TESTING QUESTIONNAIREThis questionnaire is needed for the evaluation of chemically-sensitive patients.
Please complete all questions after your testing and return this promptly to your doctor.
Patient Name:___ Gulf War Vet u Silicone Exposure Pesticide Exp.
Address:_ O ther Exposure:_City/Zip: Age: Sex: LOMale LOFemaleHome Phone:( ) - Date Today:Date Blood Drawn: Time Blood Drawn (check): O Morning LI AfternoonDate Urine Collection Finished: Date Stool Collection Finished:
Answer all the following but not until AFTER your tests are completed. YES No NOT SURE1. For Any Tests, did you take any medications in the 2 weeks before testing?
IF YES, list the medications you took and the dates you took them:
2. For Any Tests, did you drink any alcohol in the 2 weeks before testing?IF YES, list the dates you drank, what you drank, and the approx. quantities:
3. For Blood or Plasma Tests (in addition to above), did you eat any food or drink(besides water) in the 12 hours before testing?IF YES, list what you ate or drank and when:
4. Do you have skin symptoms made worse by exposure to sunlight?5. Has your urine ever been LOdark brown or LOpink to red (not due to blood)?
(Urine may darken with standing. Try to observe for this.)IF YES, was this shortly after an exposure that increased your symptoms?
IF YES, when was the last time? Approximate Date:_6. Do you have abdominal pain?
IF YES: Is this pain chronic LI ? Is this pain worse after an exposure L ?7. Are any of your symptoms made worse by dieting or skipping meals?8. Are any symptoms made worse by drinking just one glass of beer or wine?9. Are any symptoms made worse by some medications?10. Do you get any skin symptoms from medications or chemical exposures?11. Do you get any skin symptoms from wearing copper bracelets or other
metal objects (such as gold and silver watches, rings, jewelry etc.?)12.(Women) Are symptoms worse the week before your menstrual period?13. On most days, do you usually feel:
LI well or fairly well , no severe symptoms; able to do all normal work/housework.LI mildly ill, few if any severe symptoms; able to do almost all normal work/housework.LI moderately ill, some severe symptoms; able to do some work/housework with
limitations.LI very ill with many severe symptoms, unable to do normal work/housework.
14. On the day of your blood testing, before going to get your blood drawn, were yoursymptoms:
LI worse than usual LI same as usual LI not as bad as usual15. On the day of your urine and stool collection, were your symptoms:
LI worse than usual LI same as usual LI not as bad as usual
Protocol developed by MCS Referral & Resources. September 1995 edition.Please address comments to Dr. Grace Ziem, MCS R&R, 2326 Pickwick Rd, Baltimore MD 21207, (410) 448-3319
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997434

PATIENTS WITH CHEMICAL INJURY AND SENSITMTY
REFERENCES
1. Osler W. The hospital and the college (address delivered in1903 to the New York Academy of Medicine). In: TheCollected Essays of William Osler (McGovern JP, Roland CGeds). Birmingham, AL:Classics of Medicine Library,1985;2:239-254.
2. Silbergeld EK, Fowler BA, eds. Mechanisms of chemical inducedporphyrinopathies. Ann NYAcad Sci 514:1-350 (1987).
3. Fowler BK, Oskarsson A, Woods JS. Metal- and metalloid-induced porphyrinurias: relationships to cell injury. Ann NYAcad Sci 514:172-182 (1987).
4. Rimington C. Experimental porphyria in rats induced by chlo-rinated benzenes. Biochem Pharmacol 12:1387-1397 (1963).
5. Bickers D, Miller L, Kappas A. Exacerbation of hereditaryhepatic porphyria by surreptitious ingestion of an usual provoca-tive agent-mouthwash. N Engl J Med 292:1115-1116 (1975).
6. McConnachie P, Zahalsky AC. Immune alterations in humansexposed to the termiticide technical chlordane. Arch EnvHealth 47:295-301 (1992).
7. Broughton A, Thrasher JD, Gard Z. Immunological evaluationof four arc welders exposed to fumes from ignited polyurethane(isocyanate) foam. Am J Ind Med 13:463-472 (1988).
8. Denkhaus W, von Steldem D, Botzenhardt U, Konietzho H.Lymphocyte subpopulations in solvent-exposed workers. IntArch Occup Environ Health 57:109-115 (1986).
9. Byers V, Levin AS, Ozonoff DM, Baldwin RW. Associationbetween clinical symptoms and lymphocyte abnormalities in apopulation with chronic domestic exposure to industrial sol-vent-contaminated water supply and a high incidence ofleukemia. Cancer Immunol Immunother 27:77-81 (1988).
10. Haustein UF, Ziegler V. Environmentally induced systemicsclerosis-like disorders. Int J Derm 24:147-151 (1985).
11. Thrasher J, Broughton A, Madison R. Immune activation andautoantibodies in humans with long-term inhalation exposureto formaldehyde. Arch Environ Heath 45:217-223 (1990).
12. Madison R, Broughton A, Thrasher JD. Immunologic bio-markers associated with an acute exposure to exothermicbyproducts of an urea formaldehyde spill. Environ HealthPerspect 94:219-223 (1991).
13. Editorial. Silicone implants and systemic immunologic disease.Toxicol Ind Health 8:231-237 (1992).
14. Broughton A. Chronic health effects and immunologic alter-ations associated with exposure to pesticides. CommentsToxicol 4:59-71 (1990).
15. Middaugh DA, Pinney SM, Linz DH. Sick building syndrome.J Occup Med 34:1197-1203 (1992).
16. Daniell W, Couser WG, Rosenstock L. Occupational solventexposure and glomerulonephritis. JAMA 259:2280-2283(1988).
17. Bombassei G, Kaplan AA. The association between hydrocar-bon exposure and anti-glomerular basement membrane anti-body-mediated disease (Goodpastures syndrome). Am J IndMed 21:141-153 (1992).
18. Safran M, Paul TL, Roti E, Braverman LE. Environmental fac-tors affecting autoimmune thyroid disease. Endocrinol MetabClin North Am 16:327-341 (1987).
19. Street J. Pesticides and the immune system. In: ImmunologicConsiderations in Toxicology (Sharma R, ed). Boca Raton,FL:CRC Press, 1981;49.
20. Press R, Peebles CL, Kumagai Y, Ochs RL, Tan EM.Antinuclear autoantibodies in women with silicone breastimplants. Lancet 340:1304-1307 (1992).
21. Thrasher JD, Madison R, Broughton A, Gard Z. Building-related illness and antibodies to albumin, conjugates of albu-min, toluene, diisocyanates, and trimellitic anhydride. Am JInd Med 15:187-195 (1989).
22. Slade M, Simmons RL, Yunis E, Greenberg LJ. Immuno-depression after major surgery in normal patients. Surgery78:363-372 (1975).
23. Tonneson E, Huttel MS, Christensen NJ, Schmitz 0. Naturalkiller cell activity in patients undergoing upper abdominalsurgery: relationship to the endocrine stress response. ActaAnaesthesiol Scand 28(6):654-660 (1984).
24. Heuser G. Diagnostic markers in chemical immunotoxicologyand neurotoxicology. J Occup Med Toxicol 1:v-x (1992).
25. Matikainen E, Juntunen J. Autonomic nervous system dysfunc-tion in workers. J Neurol Neurosurg Psychiatry 48:1021-1024(1985).
26. Morrow L, Ryan CM, Hodgson MJ, Robin N. Alterations incognitive and psychological functioning after organic solventexposure. J Occup Med 32:444-450 (1990).
27. Morrow L, Ryan CM, Hodgson MJ, Robin N. Risk factorsassociated with persistence of neuropsychological deficits inpersons with organic solvent exposure. J Nerv Ment Dis179:540-545 (1991).
28. Gyntelberg F, Vesterhauge S, Fog P, Isager H, Zillstorff K.Acquired intolerance to organic solvents and results of vestibu-lar testing. Am J Ind Med 9:363-370 (1986).
29. Morata T, Dunn DE, Sieber WK. Effects of occupationalexposure to organic solvents and noise on hearing. Scand JWork Environ Health 19:245-254 (1993).
30. Linz D, deGarmo P, Morton W, Weins A, Coull B, Maricle R.Organic solvent-induced encephalopathy in industrial painters.J Occup Med 28:119-125 (1986).
31. Savage EP, Keefe TJ, Mounce LM, Lewis JA, Heaton RK,Burcar PJ. Chronic neurological sequelae of acute organophos-phate pesticide poisoning. Arch Environ Health 43:38-45(1988).
32. Jusic A. Anticholinesterase pesticides of organophosphorustype: electromyographic, neurological and psychological studiesin occupationally exposed workers. In: Behavioral Toxicology:Early Detection of Occupational Hazards (Xintras C, JohnsonBL, deGrott I, eds). NIOSH 74-126. Washington:NationalInstitute for Occupational Safety and Health, 1986; 182-190.
33. Troster A, Ruff R. Neuropsychological sequelae of exposure tothe chlorinated hydrocarbon solvents trichloroethylene andtrichloroethane. Arch Clin Neuropsy 5:31-47 (1990).
34. Hartlage L, Johnson D, Burns T, Wllliams B. Neurotoxicologicalscreening in community settings. Arch Clin Neuropsy 9:139-140(1994).
35. Doty R, Deems DA, Frye RE, Pelberg R, Shapiro A. Olfactorysensitivity, nasal resistance, and autonomic function in patientswith multiple chemical sensitivity. Arch Otolaryngol HeadNeck Surg 114:1422-1427 (1988).
36. Ryan CM, Morrow LA, Hodgson M. Cacosmia and neurobe-havioral dysfunction associated with occupational exposures tomixtures of organic solvents. Amer J Psychiatry 145:1442-1445(1988).
37. Rosenthal N, Cameron CL. Exaggerated sensitivity to anorganophosphate pesticide. Am J Psychiatry 148:2 (1991).
38. Cone J, Sult TA. Acquired intolerance to solvents followingpesticide/solvent exposure in a building: a new group of work-ers at risk for mu tiple chemical sensitivities. Toxicol IndHealth 8:29-39 (1992).
39. Broughton A. Antibodies and altered cell immunity informadehyde-exposed humans. Comments Toxicol 2:155-174(1988).
40. Davidoff A, Fogarty L. Psychogenic origins of multiple chemi-cal sensitivities syndrome: a critical review of the research litera-ture. Arch Environ Health 49:316-325 (1994).
41. Callender T, Morrow L, Subramanian K, Duhon D, RistovvM. Three-dimensional brain metabolic imaging in patientswith toxic encephalopathy. Environ Res 60: 295-319 (1993).
42. Heuser G, Wodjani A, Heuser S. Diagnostic markers in chemi-cal sensitivity. In: Multiple Chemical Sensitivities: Addendumto Biologic Markers in Immunotoxicology. Washington:National Academy Press, 1992;1 17-138.
Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997 435

ZIEM AND MCTAMNEY
43. Fiedler N, Maccia C, Kipen H. Evaluation of chemically-sensi-tive patients. J Occup Med 34:529-538 (1992).
44. Meggs W, Cleveland C. Rhinolaryngoscopic examination ofpatients with multiple chemical sensitivity syndrome. ArchEnviron Health 48(1):14-18 (1993).
45. Buchwald D, Garrity D. Comparison of patients with chronicfatigue syndrome, fibromyalgia, and multiple chemical sensitiv-ities. Arch Int Med 154:2049-2053 (1994).
46. Romano T, Stiller J. Abnormal cutaneous perception in pri-mary, secondary and post-traumatic fibromyalgia patients.Arthritis Rheum 31 (Suppl 4):S99 (1988).
47. Russell IJ, Vipraio GA, Michalek J, Fletcher E. Abnormal Tcell subpopulations in fibrositis syndrome. Arthritis and Rheum31(Suppl 4):S99 (1988).
48. Golden erg D, Simms RW, Geiger A, Komaroff A. High fre-quency of fibromyalgia in patients with chronic fatigue seen ina primary care practice. Arthritis Rheum 33:381-387 (1990).
49. Klimas N, Salvato FR, Morgan R, Fletcher MA. Immunologicabnormalities in chronic fatigue syndrome. J Clin Microbiol28:1403-1410 (1990).
50. Cotton P. Treatment proposed for chronic fatigue syndrome;research continues to compile data on disorder. JAMA266:2667-2668 (1991).
51. Cheney P. Proposed pathophysiologic mechanism of CFIDS.CFIDS Chronicle, Spring 1994;1-3.
52. Bell IR. White paper: neuropsychiatric aspects of sensitivity tolow-level chemcls: a neur sensitization model. Toxicol IndHealth 10:277-312 (1994).
53. Goldstein J. The evolving hypothesis. CFS: Limbicencephalopathy in a dysfunctional neuroimmune network.CFIDS Chronicle, Fall 199 1;19-24.
54. Davidoff L. Symptoms and health status in individuals withmultiple chemical sensitivities syndrome from four reportedsensitizing exposures and a general population comparisongroup. Arch Environ Health 51:201-213 (1996).
55. Hafler D, Fox DA, Benjamin D, Weiner HL. Antigen reactivememory T cells are defined by TAI. J Immunol 137:414-418(1986).
56. Simon G. Question and answer session 3. In: Proceedings ofthe Conference on Low-Level Exposure to Chemicals andNeurobiologic Sensitivity, 6-7 April 1994, Baltimore,Maryland (Mitchell FL, ed). J Toxicol Ind Health 10:526-527(1994).
57. Baker GP. Porphyria and MCS symptoms overlap-anotherchemical connection. Townsend Letter for Doctors 144:72-73(1995).
58. Donnay A, Ziem G. Protocol for Diagnosing Disorders ofPorphyrin Metabolism in Chemically-Sensitive Patients.Baltimore, MD:MCS Referral & Resources, Inc., 1995.
59. Kappas A, Sassa S, Galbraith RA, Norman Y. The porphyrias.In: The Metabolic Basis of Inherited Disease, 6th ed. (ScriverCR, Beaudet AL, Sly WS, Valle D, eds). New York:McGraw-Hill Information Services Company, 1989; 1305-1365.
60. Simon G, Daniell W, Stockbridge H, Claypoole K, RosenstockL. Immunologic, psychological and neuropsychological factors
in multiple chemical sensitivity: a controlled study. Ann InternMed 119: 97-103 (1993).
61. Ziem G, Donnay A. Chronic fatigue, fibromyalgia and chemi-cal sensitivity: overlapping disorders. Arch Intern Med155:1913 (1995).
62. Davidoff R. Migraines: Manifestations, Pathogenesis andManagement. Philadelphia:FA Davis, 1995.
63. Hagstadius S, Orbaek P, Risberg J, Lindgren M. Regional cere-bral blood flow at the time of diagnosis of chronic toxicencephalopathy induced by organic solvent exposure and aftercessation of exposure. Scand J Work Environ Health15:130-135 (1989).
64. Callender T, Morrow L, Subramanian K, Duhon D, RistovvM. Three-dimensional brain metabolic imaging in patientswith toxic encephalopathy. Environ Res 60:295-319 (1993).
65. Callender T, Morrow L, Subramanian K. Evaluation of chronicneurological sequelae after acute pesticide exposure using SPECTbrain scans. J Toxicol Environ Health 41:275-284 (1995).
66. Bocchetta A, Corsini GU. Parkinson's disease and pesticides.Lancet 2:1163 (1986).
67. Aggazzotti G, Fantuzzi G, Tartoni PL, Predieri G. Chloroformin alveolar air of individuals attending indoor swimming pools.Arch Environ Health 45:175-179 (1990).
68. Ziem G. Dr. Ziem's Environmental Control Plan. Baltimore,MD:MCS Referal & Resources, 1995.
69. Roach SA, Rappaport SM. But they are not thresholds: a criti-cal analysis of the documentation of threshold limit values. AmJ Ind Med 17:727-753 (1990).
70. Castleman BI, Ziem GE. Corporate influence on thresholdlimit values. Am J Ind Med 13:531-559 (1988).
71. Castleman BI, Ziem GE. Toxic pollutants, science, and corpo-rate influence. Arch Environ Health 44:68,127 (1989).
72. Ziem GE, Castleman BI. Threshold limit values: historical per-spectives and current practice. J Occup Med 31:910-918(1989).
73. Castleman BI, Ziem GE. American Conference ofGovernmental Industrial Hygienists: low threshold of credibil-ity. Am J Ind Med 26:133-143 (1994).
74. Meggs WJ. Neurogenic inflammation and sensitivity to envi-ronmental chemicals. Environ Health Perspect 101(3):234-238(1993).
75. Bell I, Miller C, Schwartz G. An olfactory-limbic model ofmultiple chemical sensitivity syndrome: possible relationshipsto kindling and affective spectrum disorders. Biol Psychiatry32:218-242 (1992).
76. Sorg BA, Hooks MS, Kalivas PW. Neuroanatomy and neuro-chemical mechanisms of time-dependent sensitization.ToxicolInd Health 10:369-386 (1994).
77. Kipen H, Hallman W, Kelly-McNeil K, Fiedler N. Measuringchemical sensitivity prevalence: a questionnaire for populationstudies. Am J Public Health 85(4):574-577 (1995).
78. Norback D, Bjornsson E, Janson C, Widstrom J, Boman G.Asthmatic symptoms and volatile organic compounds,formaldehyde, and carbon dioxide in dwellings. J OccupEnviron Med 52:338-395 (1995).
436 Environmental Health Perspectives * Vol 105, Supplement 2 * March 1997