mcsp activity in nigeria quarterly report
TRANSCRIPT

January–March 2017 www.mcsprogram.org
MCSP Activity in Nigeria Quarterly Report
Quarter 2 – January 01 to March 31, 2017
Submission Date: April 30, 2017 Cooperative Agreement Number: AID-OAA-A-N-00028 Activity Start Date and End Date: OCTOBER 01, 2014 to SEPTEMBER 30, 2019 [Activity Manager] Name: AORM) Activity Manager (Dr. Joseph Monehin)
Submitted by: Dr. Oniyire Adetiloye, Project Director Jhpiego Corporation Plot 971, Reuben Okoya Crescent, Off Okonjo Iweala Street, Wuye District, Abuja Tel: +234-803-446-3508 Email: [email protected]

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Activity Manager: Dr. Joseph Monehin Submitted by: Dr.Oniyire Adetiloye, Project Director
Jhpiego Corporation Plot 971, Reuben Okoya Crescent, Off Okonjo Iweala Steet, Wuye District, Abuja Tel: +234-803-446-3508 Email: [email protected]
This document was produced for review by the United States Agency for International Development Nigeria (USAID/Nigeria). “This report is made possible by the generous support of the American people through the United States Agency for International Development (USAID) under the terms of the Cooperative Agreement AID-OAA-A-N-00028. The contents are the responsibility of the Maternal and Child Survival Program and do not necessarily reflect the views of USAID or the United States Government”

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Program Overview / Summary
Program Name: MCSP-MNCH Activity in Nigeria
Activity Start Date and End Date: October 01, 2014–September 30, 2019
Name of Prime Implementing Partner: Jhpiego Corporation
[Contract/Agreement] Number: AID-OAA-A-N-00028
Name of Subcontractors/ Sub-awardees:
• Save The Children International (SCI) • Results For Development (R4D) • John Snow Incorporated (JSI) • Pediatric Association of Nigeria (PAN) • Nigerian Society of Neonatal Medicine (NISONM) • Society of Gynecology and Obstetrics of NIGERIA (SOGON) • National Association of Nigerian Nurses and Midwives (NANNM)
Major Counterpart Organizations State Ministries of Health
Geographic Coverage (cities and or countries) Ebonyi and Kogi States
Reporting Period: Jan 1, 2017 – March 31, 2017
Approved MCSP Nigeria MNCH PY1-PY3 Budget
$26,291,577
Total expenditure this quarter (Jan-March, 2017)
$1,757,098
Accrued Expenditures $477,792
Total Estimated Expenditures to Date
$11,777,714
Workplan PY1-PY3 Budget Minus Expenditures to Date
$14,513,863

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Table of Contents Acronyms ............................................................................................................................................ 5
1.0 Introduction ........................................................................................................................... 8 1.1. Program Description 8 1.2. Summary of Results to Date 9
2.0 Activity Implementation Progress ....................................................................................... 11 2.1. Maternal Health 13 2.2. Newborn Health 17 2.3. Child Health 22 2.4. Family Planning 24 2.5. Adolescent Sexual and Reproductive Health 25 2.6. Gender 26 2.7. Pre-Service Education 28 2.8. Monitoring and Evaluation 28 2.9. Operations Research 30
3.0 Stakeholders Participation / Involvement ........................................................................... 31 3.1. Professional Associations 31
3.1.1. SOGON 31 3.1.2. PAN / NISONM 32 3.1.3. NANNM 33
4.0 Management And Administrative Matters ......................................................................... 34 4.1. Appointments / Resignation 34 4.2. Team Orientation 34
5.0 Implementation Challenges / Lessons Learned .................................................................. 35 5.1. Implementations Challenges 35 5.2. Lessons Learned 35
6.0 Planned Activities For Next Quarter .................................................................................. 35
7.0 Annex 1: Detailed Progress Report Table…………………..................................................41
MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Acronyms AAP American Academy of Pediatrics
ACCESS Access to Clinical and Community Maternal, Neonatal and Women’s Health Services
ACOG American College of Obstetrics and Gynecology
ACNM American College of Nurse-Midwives
AMTSL Active Management of the Third Stage of Labor
ANC Antenatal Care
AOR Activity Officer Representative
ASRH Adolescent Sexual Reproductive Health
bCPAP bubble Continuous Positive Airway Pressure
CAII Center for Accelerating Innovation and Impact
CG Clinical Governance
CH Child Health
CHAI Clinton Health Access Initiative
CHEW Community Health Extension Worker
CHO Community Health Office
CHTWG Child Health Technical Working Group
DHIS District Health Information System
ECEB Essential Care for Every Baby
ECSB Essential Care for Small Babies
EML Essential Medicine List
ENC Essential Newborn Care
ENCC Essential Newborn Care Course
EPMCD Ending Preventable Maternal and Child Death
ETS Emergency Transport Scheme
FIGO Federation of International Gynecologists and Obstetricians
FMOH Federal Ministry of Health
FP Family Planning
FTYP First Time / Young Parent
FY Financial Year
GON Government of Nigeria
GSK Glaxo Smith Klein
HBB Helping Babies Breath
HFG Health Finance and Governance
HIV/AIDS Human Immunodeficiency Virus / Acquired Immune Deficiency Syndrome
HMIS Health Management Information System
iCCM Integrated Community Case Management of Childhood Illnesses
JHU IRB Johns Hopkins University Institutional Review Board
MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
KMC Kangaroo Mother Care
LGA Local Government Area
LOP Life of Project
LSS Life Saving Skills
MCHIP Maternal and Child Health Integrated Program
MCSP Maternal and Child Survival Program
M&E Monitoring and Evaluation
MNCH Maternal, Neonatal and Child Health
MNH Maternal and Neonatal Health
MSLC Mothers’ Savings and Loans Clubs
MSS Midwifery Service Scheme
NANNM NAPPMED
National Association of Nigerian Nurses and Midwives National Association of Patent and Propriety Medicine
NASG Non-Pneumatic Anti-Shock Garment
NHIS National Health Insurance Scheme
NiENAP Nigeria Every Newborn Action Plan
NISONM Nigerian Society of Neonatal Medicine
NPHCDA National Primary Health Care Development Agency
PAN Pediatric Association of Nigeria
PHC Primary Health Care
PMP Performance Monitoring Plan
PPFP Post-Partum Family Planning
PPH Post-Partum Hemorrhage
PPMV Patent Proprietary Medicine Vendors PPUID Post-Partum Intra Uterine Device
PSE Pre-Service Education
PY Project Year
QIT Quality Improvement Team
QIC Quality Improvement Committee
QoC Quality of Care
R4D Results for Development
RH Reproductive Health
RMC Respectful Maternal Care
SBM-R Standards-Based Management and Recognition
SCI Save the Children International
SDP Service Delivery Point
SIF Service Improvement Facilitator
SIO Strategic Information Officer
SMOH State Ministry of Health
SOGON Society of Gynecology and Obstetrics of Nigeria

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
SOML Saving One Million Lives
SPHCDA State Primary Health Care Development Agency
S&TGDA Survive and Thrive Global Development Alliance
SURE-P Subsidy Reinvestment and Empowerment Program
TOT Training of Trainers
TSHIP Targeted States High Impact Project
USAID United States Agency for International Development
USG United States Government
VOS Voluntary Obstetrics Scheme
WHO World Health Organization
YFHS Youth-Friendly Health Services

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
1.0 INTRODUCTION
1.1. Program Description The Maternal and Child Survival Program (MSCP) is a global U.S. Agency for International Development (USAID) cooperative agreement to introduce and support high-impact health interventions in 25 priority countries with the ultimate goal of ending preventable child and maternal deaths (EPMCD) within a generation. MCSP engages governments, policymakers, private sector leaders, health care providers, and civil society organizations in adopting and accelerating proven approaches to address the major causes of maternal, newborn and child mortality. It aims to improve the quality of health services from the household to the hospital.
MCSP’s Maternal, Newborn and Child Health (MNCH) project in Nigeria is focused on working with the Government of Nigeria (GoN) to improve the quality and utilization of maternal, newborn and child care services in public, private and faith-based facilities as well as in selected communities in Kogi and Ebonyi states. MCSP will be implemented over five years, subject to available funds, and builds on the work of previous USAID global programs (ACCESS and MCHIP) in northern Nigeria.
MCSP MNCH is implemented in Nigeria by four consortium partners – Jhpiego, John Snow Inc (JSI), Save the Children International (SCI) and Results for Development (R4D). The in-country partners are the Federal Ministry of Health (FMOH), National Primary Health Care Development Agency (NPHCDA), and Ministry of Health and State Primary Health Care Development Agency (SPHCDA) in both Ebonyi and Kogi states.
MCSP has sub-awards with four local professional associations: the Society of Gynecology and Obstetrics of Nigeria (SOGON), Pediatric Association of Nigeria (PAN), Nigerian Society of Neonatal Medicine (NISONM), and National Association of Nigerian Nurses and Midwives (NANNM). MCSP also partners with US-based professional associations including the American Academy of Pediatrics, American College of Obstetricians and Gynecologists, and American College of Nurse-Midwives, and with projects and partners like Clinton Health Access Initiative (CHAI), Saving One Million Lives (SOML), Survive and Thrive Global Development Alliance partners (S&TGDA), and FistulaCarePlus.
Project Objectives Life of Project (LOP) Expected Results
• To improve quality of facility-based maternal, newborn and child health care (MNCH) services and community based child health services
• To improve information systems to monitor & evaluate health outcomes
• To increase use of life-saving innovations
• 80% of staff competent to provide quality maternal, newborn and postpartum family planning (PPFP) services in all program-supported facilities
• 80% of program-supported facilities recognized for achieving quality standards in maternal, newborn and family planning (FP) services
• 80% of program-supported facilities have a minimum package of essential equipment, commodities and supplies
• Functional two-way referral systems within all program-supported clusters including pre-notification of patient transfers, use of emergency transport systems (ETS) that are enabled by savings and loans clubs as alternative financing systems
• 50% increase in percent of new graduates from nursing and midwifery schools and schools of health technology who can demonstrate competency in critical maternal, newborn and FP skills
• Increase in the utilization of skilled birth attendance (SBA) for delivery by 10% in Kogi and 20% in Ebonyi

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
1.2. Summary of Results to Date MCSP Nigeria is re-prioritizing the capacity building of healthcare workers to deliver lifesaving services following the extension and scaling up of the Program’s direct intervention and services into an additional 120 facilities (Phase II facilities) in the two states. MCSP is now supporting 240 Phase 1 and II health facilities. Between January and March 2017, 50 CHEWs from among the Phase II facilities were trained to provide basic emergency obstetric and newborn care (BEmONC). Following the training, the CHEWs are now more able to actively manage third stage of labor, do bimanual compression of the uterus and compression of abdominal aorta, manually remove retained placenta, resuscitate newborns that are not breathing, and manage maternal and newborn infections. Similarly, 51 CHEWs were trained on modified Essential Newborn Care Course (mENCC) – thus empowering them with the lifesaving skills for providing essential newborn care, care for small babies and newborn resuscitation. Furthermore, MCSP trained 23 healthcare workers in Kogi to become PP-LARC service providers and another 36 health workers in Kogi and Ebonyi as dedicated post-partum family planning counselors. The program also supported a step-down training on the Age and Life Stage counseling tools for 35 service providers in Kogi and Ebonyi states. And through the Health Workers for Change step-down training, 137 skilled and unskilled health workers were orientated on ways to offer respectful and dignified care in order to improve the quality of service being provided and thus improve the confidence of clients seeking care at these facilities. To improve pre-service education in project states, MCSP supported 10 institutions by helping to train 42 lecturers, tutors and preceptors. During the preservice education (PSE) baseline assessment, the institutions scored less than 80% SBM-R scores in the classroom and practical instruction thematic areas. MCSP played (and is still playing) an important role in developing the draft national strategy for RMNCH Quality of Care in Nigeria. The draft strategy was widely reviewed and updated with inputs from MCSP during the quarter and will be finalized in the coming months with further support from the Program. MCSP also contributed to the inauguration of the Maternal and Newborn Health Quality of Care (QoC) Steering Group & Technical Working Group (TWG) by the Minister of Health in February 2017 and the appointment of a Desk Officer for Quality Improvement in the FMOH. At the state level, MCSP supported a progress review of quality improvement interventions at the facility, local government areas (LGA) and state levels. The review provided opportunities for stakeholders to share lessons and address challenges or limitations inherent in implementing quality improvement interventions at these levels. MCSP also engaged with several other key stakeholders during the period under review to open more opportunities and prospects for achieving better outcomes for maternal, newborn and child health in the MCSP-supported states. The program organized stakeholder consultation meetings at the state and national levels through which it successfully advocated for the Pharmacists Council of Nigeria to include Amoxicillin Dispersible Tablet on the Essential Medicine List and thereafter secured approval for its inclusion in the medicine list that can be handled and dispensed by trained PPMVs thus making it more readily available at all levels of care. MCSP also engaged, sensitized and mobilized the National Union of Road Transport Workers, Ward Development Committees and relevant stakeholders towards implementing an Emergency Transport Scheme (ETS) in project states. Stakeholders agreed that the scheme, which will be initially piloted in six LGAs, will prevent/reduce the delays in reaching health facilities by pregnant women during emergencies. The women’s savings and loans clubs, are also assisting with planning for health emergencies, which have now increased to 16 (11 in Ebonyi and 5 in Kogi) and comprising 349 women members with over N650, 000 ($2,070) raised till date (an increase of 80% from last quarter). The linkages between the clubs and health facilities for health purposes are gradually becoming established – two cases of a member borrowing from her club’s emergency funds to pay for the delivery of her baby and another borrowing also from the emergency funds to treat and buy drugs for her sick baby were recorded within the reporting period. MCSP’s partnership with the professional associations led to increased access to quality facility-based healthcare for women, newborns and children during the reporting period. Through the associations’ voluntary schemes

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
(VOS and VPSS), 300 clients (mostly women and children) were reached by 36 volunteers who also mentored 58 health workers during 85 visits to 37 facilities. The major challenges/risks to the implementation of MCSP in Nigeria remain the dwindling state resources due to the current economic recession and high insecurity in the country (including project states) characterized by recurring communal clashes, kidnapping and herdsmen attacks. Even though the security situation seems to have improved slightly within this reporting period due to the efforts of the two states government, the risk is still a little high especially in Kogi State. Nonetheless, MCSP will continue to focus on improving the quality of care in the 240 health facilities. The key focused interventions of the Program scheduled for next quarter include capacity building on BEmONC and ENCC for healthcare workers in Phase II facilities, post-training follow-up, supportive supervision, mentorship and ensuring availability of essential supplies and equipment as a foundation for quality improvement in all MCSP supported sites. Figure 1 below is an infographic summarizing the facts and figures that emanate from the activities and interventions in this quarter while Table 1 is a summary of the results by standard indicators and targets. Fig 1: Program Year 3 Quarter 2 – Key facts and figures

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Table 1: Summary of results by standard indicators and targets*
Standard Indicators
Baseline FY 2014
Annual Target
Annual Achieved (Oct 16 to
Sep 17)
Q2 FY17 (Jan-Mar
2017)
Performance Achieved to
End of Reporting Period (%)
On Target?
Y/N
Sub-IR 1.1: Increased availability of EmONC and Family Planning workers Number of people trained in maternal and newborn health through USG supported programs
Ebonyi 0 150 65 (55F, 10M) 92% Y Kogi 0 150 108 (93F,
15M)
Total 0 300 173 (148F, 25M)
Sub-IR 2.1: Increased availability of EmONC and Family Planning services Number of first ANC visits supervised by Skilled Providers from USG assisted facilities
Ebonyi 77,946 55,000 10,728 36% N
Kogi 26,230 35,000 6,048
Total 104,176 90,000 16,776
Number of deliveries by SBAs
Ebonyi 6,786 12,000 2,765 44% Y
Kogi 3,133 8,000 1,247
Total 9,899 20,000 4,012
Percent of SDPs providing FP/RH counseling and/or services
Ebonyi 86% 75% (N=90 107/119 82% Y
Kogi 64% 75% (N=90) 89/121
Total 75% 75% (180) 196/240 (82%)
Couples Year of Protection (CYP) in USG supported programs
Ebonyi 2,300 8,000 2,702 60% Y
Kogi 12,504 11,000 8,735
Total 14,804 19,000 11,437
Sub-IR 3.1: Facility-based MNCH improved Number/percent of women receiving immediate post-partum Uterotonic in the third stage of labor
Ebonyi NA 12,000 2,629/3,160 (83.1%)
48% Y
Kogi NA 8,000 2,404/2,504 (96%)
Total NA 20,000 5,080/6,664 (76.2%)
Percent of births with use of Partograph in USG supported facilities
Ebonyi 20% 45% 1,139/3,160 (36%)
28% Y
Kogi 13% 45% 361/2,504 (14%)
Total 17.6% 45%
Percent of newborns receiving essential care through USG supported program
Ebonyi 65% 80% 2,327/3,012 (77.2%)
67% Y
Kogi 34% 80% 2,451/3335 (73%)
Total 51% 80%
* MCSP is presently supporting 240 health facilities in Ebonyi and Kogi states. The program implementation started with 120 health facilities and at the start of PY3, additional 120 sites were added: 119 in Ebonyi State and 121 in Kogi State.

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
MCSP Key Graphic Summary for the Reporting Period
MCSP service data are tracked and reported through DHIS2 national platform which has a mandate to report all routine data from health facilities across the country. Fig 2 below shows that the reporting rate of data from MCSP supported sites is much better when compared to the MCSP non-supported sites in Ebonyi and Kogi.
Fig 2: Reporting rates by MCSP-supported facilities vs non-supported facilities from October 2015 to March 2017
86.2% 86.1%88.8% 89.7%
92.0%
82.0%
96.0% 95.5% 96.0%100.0%
97.0%95.0%
64.7%
53.3%
64.5%
70.6%
84.0%
63.4%
83.6%
67.8%
83.1%
90.2%87.0%
78.0%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct-Dec, 2015 Jan-Mar, 2016 Apr-Jun, 2016 Jul-Sept, 2016 Oct-Dec, 2016 Jan-Mar, 2017
Ebonyi Whole state Ebonyi MCSP supported HFs Kogi Whole state Kogi MCSP supported HFs Measuring Quality of Services Provided
MCSP used service data of selected MNCH indicators to gauge the quality of services provided. Graph 1 above shows the trend in the use of Uterotonic and Partograph to monitor labour and delivery in MCSP supported health facilities from October, 2016 through March, 2017. There was an improvement in the use of Uterotonic with a drop in use of partograph to monitor labour and delivery. Graph 2 shows the percent of newborn receiving essential newborn care in MCSP supported health facilities is on the rise. MCSP will however continue to provide necessary technical supports to improve the quality of health services provided in the project states with the ultimate aim of reducing maternal, neonatal and child mortality.
71%
39%
62%
87%
62%
89%
51%
15%
27%
52%
37%
26%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct-Dec, 2015 Jan-Mar, 2016 Apr-Jun, 2016 Jul-Sept, 2016 Oct-Dec, 2016 Jan-March, 2017Uterotonic Partograph Linear (Uterotonic)
Graph 1
46%
85%
63%
93%
59%
75%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct-Dec, 2015 Jan-Mar, 2016 Apr-Jun, 2016 Jul-Sept, 2016 Oct-Dec, 2016 Jan-March, 2017
Graph 2

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
2.0 ACTIVITY IMPLEMENTATION PROGRESS
2.1. Maternal Health MCSP's strategy for maternal health emphasizes an integrated, systems-oriented approach to reducing direct and indirect causes of maternal morbidity and mortality. The interventions in the maternal health technical area include skill building on basic emergency, obstetric and newborn care (BEmONC) for health workers, quality improvement at health facilities, integrated supportive supervision, and increasing access to affordable quality care for pregnant women through a collaborative initiatives with the government at all levels and other implementing partners. 2.1.1. Capacity building on BEmONC for healthcare workers in Phase II facilities
Following the extension of direct intervention to an additional 120 health facilities (i.e. Phase II facilities) last quarter, MCSP this quarter supported 50 of the facilities by training their health workers to deliver quality BEmONC. Fifty CHEWs (one from each facility) benefitted from the training. Like previous BEmONC trainings, the health workers gained useful knowledge and skills to effectively carry out antenatal care, normal delivery, newborn resuscitation, manual removal of the placenta, bimanual compression of the uterus, abdominal compression of the aorta, use of partograph to manage labor, and preparing and giving loading dose of MgSo4 for severe pre-eclampsia and eclampsia (PE/E) before referral. The 50 health care workers were also trained on aspects of respectful maternity care.
Demonstration of newborn delivery by participants at the BEmONC training for community health extension workers in MCSP-supported Phase II facilities
2.1.2. Capacity building for BEmONC master trainers and MCSP field officers
Prior to the training of the CHEWs, MCSP collaborated with Ebonyi and Kogi SMOH and Population Council to organize a 2-day skill-building workshop to update BEmONC master trainers and MCSP’s Service Improvement Coordinators on WHO New Recommendations for ANC and Managing Complications in Pregnancy and Child Birth (MCPC) – Pre-Eclampsia/Eclampsia (PE/E) and Post-Partum Hemorrhage (PPH). The workshop provided opportunity for participants to review the new clinical guidelines from MCPC for preventing and managing PE/E and PPH; review agreement by stakeholders on priority PE/E and PPH clinical interventions and quality measures; be orientated to the use of a patient pathway facility readiness assessment tool; and build skills in PPH management (including Uterine balloon
tamponade), PE/E management (including use of anti-hypertensive for severe systolic blood pressure, timing of delivery and specialized PNC for women with severe PE/E.
A trainer practices a BEmONC skill on a model
MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Some key outcomes of the workshop included the decisions to (1) include QI skills building in future capacity-building activities, (2) incorporate QI into regular Integrated Supportive Supervision (ISS) visits, and (3) integrate QI into the focus and scope of SOGON’s Voluntary Obstetric Scheme (VOS). Furthermore, there were agreed recommendations especially for Ebonyi to (1) strengthen coordination between partners and SMOH to improve rational distribution of commodities across facilities (e.g. re-
distributing commodities that are about to expire); (2) prioritize essential RMNCH commodities for procurement as part of Saving One Million Lives campaigns (e.g. oxytocin, misoprostol, MgSO4, chlorhexidine); (3) review priority QI indicators with facility teams as part of government routine supervision (ISS); (4) prioritize and invest resources in a subset of functional facilities rather than diluting resources across multiple facilities); and (5) improve tracking and analysis of priority measures to optimize use of data for decision-making.
2.1.3. Progress review of quality improvement interventions at state level
A workshop to review progress of work around quality improvement efforts in both project states was held in Abakaliki in February 2017. Participants acknowledged progress that have been made to include regular meetings of the QI teams at the facility levels (every 1-2 weeks), tracking of prioritized phase-one (routine DoB) QI indicators, and increased clinical and QI capacity especially in sites benefitting from the low-dose high-frequency (LDHF) on the job training. The stakeholders were informed of new clinical updates on WHO ANC Recommendations and MCPC manual with focus on PE/E and PPH. They agreed priority PE/E and PPH clinical interventions and quality measures by facility level and care phases (tertiary, secondary, primary; ANC, birth, PNC) and agreed to build integrated clinical, QI and measurement skills of health care workers and managers.
They also agreed to support SMOH, SPHCDA and LGA managers to address critical health system gaps, especially for essential MNH commodities (water, soap, medications, equipment) and to introduce or strengthen existing registers and standardized patient records to capture essential data for clinical case management and quality measurement. They identified the major challenges to include stock out of essential commodities (e.g. uterotonics and MgSO4) especially in PHC and general hospitals and lack of standardized patient records (ANC, intrapartum and PNC). They plan to address lack of MNH referral protocols and processes with SMOH, LGA and SPHCDA managers, orient and support facility QI teams to begin improving PE/E and PPH care, and develop simple job aids to support better clinical decision making around PE/E and PPH management.
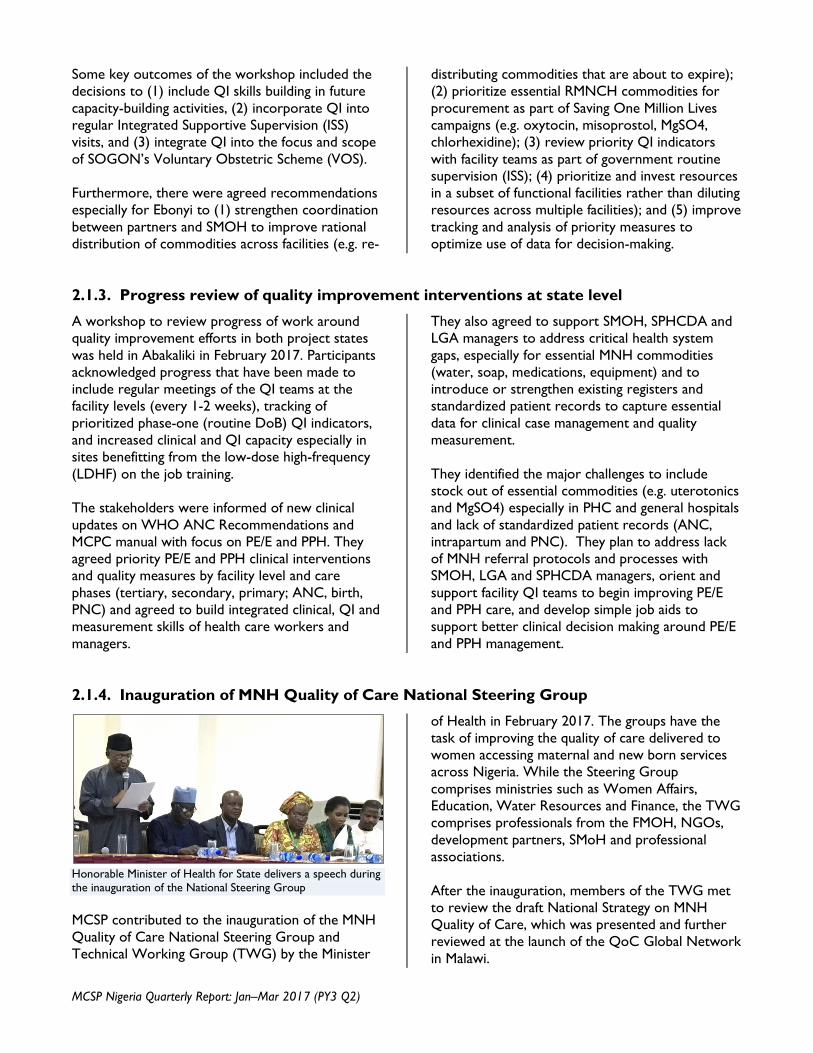
2.1.4. Inauguration of MNH Quality of Care National Steering Group
Honorable Minister of Health for State delivers a speech during the inauguration of the National Steering Group MCSP contributed to the inauguration of the MNH Quality of Care National Steering Group and Technical Working Group (TWG) by the Minister
of Health in February 2017. The groups have the task of improving the quality of care delivered to women accessing maternal and new born services across Nigeria. While the Steering Group comprises ministries such as Women Affairs, Education, Water Resources and Finance, the TWG comprises professionals from the FMOH, NGOs, development partners, SMoH and professional associations. After the inauguration, members of the TWG met to review the draft National Strategy on MNH Quality of Care, which was presented and further reviewed at the launch of the QoC Global Network in Malawi.

January–March 2017 www.mcsprogram.org
2.1.5. Launching of WHO Global Network on Maternal and Newborn Quality of Care
MCSP participated in the launch of the WHO Global Network on Quality of Care (QoC) on Maternal and Newborn Health in Malawi in February 2017. About 350 participants including representatives of the nine countries in the first phase of global MNH QoC implementation – Bangladesh, Cote d’Ivoire, Ethiopia, Ghana, India, Malawi, Nigeria, Tanzania and Uganda – shared learning and experience. Nigeria presented her work around MNH quality of care including the country’s experience in developing a national strategy for maternal and newborn quality of care. Going forward, MCSP will further support Nigeria to finalize the QoC strategy, select the demonstration states and facilities, agree on QoC measures/indicators to be prioritize, agree on method of learning platform, set milestones and start implementation.
For the Global Network, the next steps include activating a learning platform, finalizing network strategic document and monitoring, establishing coordination network mechanism, and bringing countries together for annual review and learning meeting
Nigerian delegates at the launch of the WHO Global Network on MNH Quality of Care in Malawi
2.1.6. Participation in Taking Quality of Care Forward Workshop
Nigeria’s experience in implementing quality of care with respect to MCSP’s support was also shared at a workshop organized by Jhpiego in January 2017 in Jaipur, India. The workshop with the theme Taking Quality of Care Forward helped to raise awareness about the different approaches for implementing quality of care and to learn and share achievements, challenges and lessons from quality projects across the world. Some of the important lessons shared at the workshop included: (1) a client’s experience is key
to quality improvement as the future is about the client satisfaction in all aspects of assessing quality; (2) measurement is crucial and use of information for decision making is essential; (3) it should be noted when designing quality programs that incentives can have powerful effects on performance as well as unintended consequences; and (4) taking quality to the next level requires working with the system at different levels, going to scale with projects and demonstrating impact.
2.1.7. Improving access to healthcare through the Women’s Savings and Loans Clubs
The number of women’s savings and loans clubs formed by community women in project states increased to 15 (10 in Ebonyi and 5 in Kogi) during the quarter with over 230 enrolled members. The amount contributed by members also increased from N129, 580 in December 2016 to over N650, 000 by March 2017. The sum of N435, 000 was loaned out to majority of the members with many beneficiaries utilizing their loans to start or expand their small businesses.
Through linkages with surrounding health centres, more club members were able to assess health services for themselves and their children. In Ebonyi, a member of Ugwu Ezi n’ulo club and mother of a 19-month-old baby with severe burns received N5,000 from her club’s emergency fund to treat her baby at Echialike PHC and buy the needed drugs.
“I did not have even one naira at that moment. If not for my club, my child would have died,” she said.

January–March 2017 www.mcsprogram.org
Another member of the Ugwu Ezi n’ulo club, also received N5,000 from the club’s emergency pot, which she used to pay for her delivery. Cuddling her new baby, she felt very grateful to the club for bailing her out.
See Also
Affordable healthcare: women’s savings and loans clubs to the rescue
A blog post in The Huffington Post, part of the Institutionalizing Community Health Conference blog series at the recently concluded ICHC in South Africa
2.1.8. Advocacy on establishing Emergency Transport Scheme
In parallel to the women’s savings and loans clubs, MCSP engaged relevant stakeholders including the ministries of health, women affairs and social development in Ebonyi and Kogi states as well as the National Union of Road Transport Workers and Ward Development Committees (WDCs) in both states towards establishing an Emergency Transport Scheme (ETS) for women in the states. The stakeholders were sensitized to the need for an emergency transport scheme in the states and the modalities for operating the scheme. They agreed that the scheme will help to reduce maternal
mortality and morbidity if communities and especially transport workers are effectively engaged to mitigate the delay in reaching a health facility by pregnant women during emergencies. With stakeholders now well sensitized and mobilized for the implementation of the scheme, MCSP will now pilot the scheme around 30 project supported facilities in six LGAs in both Ebonyi and Kogi states. In Ebonyi, the scheme will complement the state government’s plan to provide ambulances for transporting women and children to the hospital during emergencies – under the SOML initiative.
2.1.9. Development and production of IEC materials on maternal health
MCSP supported the project states to develop and produce educational and promotional materials on maternal health this quarter. The materials included a maternal health record booklet which will ensure that information of each mother and her newborn is captured in one document throughout the continuum of care. The maternal health record booklet also contains a copy of the partograph thus providing the opportunity for all trained health care workers to monitor progress of labor for every woman in labor. Other materials included safe motherhood posters, postnatal care posters, and birth preparedness and readiness cards. The IEC materials will be donated to the two MCSP supported states. Efforts are ongoing to see that the states make use of similar
documents in the other non-MCSP supported facilities.

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
2.1.10. Integrated Supportive Supervision Visits to LGAs and Health Facilities
In this period under review, MCSP continued to work with partners such as the SMoH, LGAs and professional associations to step-up and institutionalize the quarterly integrated supportive supervision visits to health facilities and LGAs in both states. During the quarter, 29 health facilities (19 in Ebonyi and 10 in Kogi) were visited and 45 health workers mentored. The frontline facility staff were supported to develop an action plan for addressing the gaps identified during the visits especially on how to ensure availability of essential medicines such as Chlorohexidine for umbilical cord care, dispersible Amoxicillin for acute respiratory and possible severe bacterial infections (PSBI).
2.2. Newborn Health The newborn health technical area is focused on interventions that address the three major causes of mortality in newborns in Nigeria: prematurity (29%), birth asphyxia (26%) and sepsis (23%). The intervention areas are essential newborn care, care of preterm babies and babies with respiratory distress through the use of bubble Continuous Positve Airway Pressure machine (bCPAP) where applicable, prevention and management of birth asphyxia, scale-up of use of chlorhexidine for cord care and prevention and management of newborn sepsis. 2.2.1. Training on modified Essential Newborn Care Course (mENCC)
MCSP built the capacity of 51 Community Health Extension Workers from 51 PHCs on modified Essential Newborn Care Course (mENCC) in Ebonyi and Kogi during the reporting period. The modified ENCC program, adapted from the Helping Babies Survive series developed by the American Academy of Pediatrics (AAP), is designed for CHEWs and junior CHEWs. The training modules comprise Helping Babies Breathe (HBB), Essential Care for Every Baby (ECEB) and Essential Care for the Small Baby (ECSB). The participants for the three day training were drawn from Phase II supported health facilities.
The mENCC training in Kogi State incorporated Health Workers for Change (HWFC) / Gender Sensitive and Respectful Care component into the training. The training also provided an opportunity for linking the health workers with drug representatives and marketers of chlorhexidine towards scaling up chlorhexidine in the states. At the end of the training, participants were given job aids including Action Plans and provider guides on HBB, ECEB and ECSB..
2.2.2. Orientation of health workers on Kangaroo Mother Care
MCSP oriented 41 health workers of both ECWA Hospital Egbe and Kogi State Specialist Hospital Lokoja on Kangaroo Mother Care (KMC) during the quarter. The health workers were introduced to various aspects of KMC such as the criteria for admitting babies for KMC, prolonged skin-to-skin practice, feeding and breasting feeding in KMC, monitoring babies during KMC, criteria for discharging babies from facility to the house, and criteria to discontinue KMC services.
MCSP also established KMC corners in six high volume health facilities in Kogi State namely Federal Medical Center Lokoja, General Hospitals Kabba, General Hospitals Ankpa, General Hospitals Okene, ECWA Hospital Egbe and Grimmard Hospital Anyigba. KMC centers have now been fully established 14 facilities in the state. Within this reporting period 73% of low birth weight babies in these facilities were admitted for KMC services.
2.2.3. Donation of resuscitation equipment for newborn corners
To date, MCSP has donated newborn resuscitation equipment and items to 67 facilities (37 in Kogi and 30 in Ebonyi). The items donated to the facilities
include ambu-bag, penguin suction, timer, drying cloth, wrapping cloth, cover cloth, adhesive tape, sterile gloves, mackintosh, cannula, syringes (1ml

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
and 2mls), naso- gastric tube, blanket, veronica bucket, liquid hand wash, alcohol pads, scissors and resuscitation tables. With these items, the 67 facilities now have fully set-up and functional newborn resuscitation corners in their labor rooms and are rightly equipped and trained to ensure the survival of sick neonates in their respective hospitals and thus able to prevent newborn deaths. MCSP has however continued
with his advocacy push to ensure the two states replicate these procurements for the benefit of other non-MCSP supported sites. Available records show appreciable increase in the number of asphyxiated babies who were successfully resuscitated in MCSP-supported facilities in Kogi State – from 93.7% in October 2016 to 100% in December 2016.
2.2.4. Development of action plans for Possible Severe Bacteria Infection Scale-up
MCSP organized a planning workshop on Possible Severe Bacteria Infection (PSBI) in Lokoja in February 2017. The purpose of the meeting was to share lessons learned from the Ibadan and Zaria AFRINEST study sites; understand basic principles of scaling a new intervention; agree on a common vision for the scale-up of PSBI interventions in Kogi and Ebonyi; discuss and reach consensus on a PSBI implementation strategy and develop PSBI detailed implementation plans for the two project states. MCSP supported Ebonyi and Kogi SMOH to develop detailed PSBI implementation plans and M&E frameworks for both states. PSBI implementation will be rolled out in six LGAs selected for IMCI and iCCM programs in the states. The need to revise the IMCI and ENCC training manual to include sessions on PSBI was emphasized since PSBI is not a stand-alone training. The decision of the Ebonyi SMOH that the PSBI TWG will be a sub-committee of the Child Health TWG as well as the sharing of information that Amoxicillin DT and gentamycin have been adopted by the FMOH for the management of PSBI where referral in not feasible and the presentation of the
Zimbabwe IMCI register for possible adaptation by FMOH and use in Nigeria were other key highlights of the workshop. There was a related workshop on PSBI organized by USAID team in Lusaka, Zambia to gather and share information on the latest evidence and best practices from around the globe on PSBI. Nigeria’s progress towards implementing PSBI was shared with other participants from Ethiopia, Zambia, Kenya, Nepal, Pakistan and Bangladesh. The implementation of PSBI in Bangladesh uses government established platform unlike the AFRINEST sites in Nigeria. A learning visit to Bangladesh will therefore be useful for Nigeria in the future. At the end of the meeting, country participants developed theory of change and draft concept note for a nation-wide PSBI implementation. MCSP workplan addendum and budget on PSBI implementation was submitted to USAID for approval, feedback received, MCSP will be submitting responses to the issues raised in the next quarter.
2.2.5. Scoping visit for activity on Water, Sanitation and Hygiene (WASH) for newborn sepsis reduction
A scoping visit by a researcher / consultant from the London School of Hygiene and Tropical Medicine for Phase I of the WASH for Neonatal and Maternal Sepsis Reduction was conducted in February 2017. The purpose of the scoping visit was to engage MCSP partners and gather contextual information pertinent to the development of the observational study to be conducted in Phase II. State and national Key Informant Interviews (KII) were conducted to understand ongoing efforts throughout Nigeria at
improving infection prevention and control (IPC) practices; water, sanitation and hygiene including issues around supplies in health facilities generally. Thirty key informant interviews were carried out during the visit, which identified areas for facility improvement before, during and after delivery to prevent neonatal sepsis. Some of the key findings from the scoping visit are as follows:
• Few facilities have standardized IPC protocols or regular trainings

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
• Poor water access (PHCs) • Lack of supervision & manpower • Staff indifference towards hygienic behaviors • Lack of supplies (gloves, sanitizer, gowns)
and inadequate space were challenges to standard hygiene behavior
• Limited supply of chlorhexidine in Ebonyi, more available in Kogi
• Inadequate trainings for health workers A report on the overall findings during Phase I of the activity, inclusive of a global and Nigeria-specific literature review is being finalized and will be available next quarter. Data collection for the observational study in Phase II will also begin in Q3.
2.2.6. Using Bubble CPAP to Manage Newborns Respiratory Distress Problems
Four facilities (FMC Lokoja, ECWA Hospital Egbe Mile 4 Hospital Abakaliki, and Federal Teaching Hospital Abakaliki) of the six facilities that received the donation of bCPAP machines from MCSP nine months ago have been utilizing the machines – placing 65 babies who needed critical respiratory support on the machine. Subsequently, MCSP has been engaging with the facilities to identify and address the challenges associated with the use of the machines in Nigeria. Box 1 below shows some of the major challenges identified and the actions taken or being proposed to address them. Also, MCSP participated and also supported the participation of FMOH delegates in a pre-conference workshop on neonatal mechanical ventilation at the annual PANConf in Kaduna to have learn more about bCPAP. One of the issues
discussed was the use of improvised bCPAP, which limits the promotion of bCPAP in the country. Participants at the workshop identified the need for an assessment of the implementation status of bCPAP, and called for FMOH to develop a policy framework for bCPAP and antenatal corticosteroids use. They also recommended a stakeholders’ consultative forum to address accessibility, availability, affordability and safety of bCPAP. MCSP plans to support these activities and will submit to USAID a supplementary work plan and budget for this purpose. MCSP is currently collaborating with USAID Nigeria, USAID’s Center for Innovation and Impact and Dalberg Global Development Advisor to assist the FMOH develop an action plan that will expand the reach of bCPAP in Nigeria.
Box 1: Challenges associated with the use of bCPAP machine in Nigeria and recommendations for addressing the challenges
Challenges Recommendations/Actions Taken
1. Oxygen supply is a major challenge. The hospitals are groaning under the burden of buying one oxygen cylinders at a high cost of N6, 000 ($16) each compared to the former price of N3, 000 ($8) due to the current economic situation with currency devaluation.
2. The mission hospitals have decided not to charge patients on bCPAP for the oxygen or subsidize the price of oxygen. Its use may not be sustained if they continue to buy oxygen at such a high price without the patients paying for it.
1. Support the facilities with oxygen concentrators or any affordable oxygen supply system
Key Informant Interview at the pharmacy section of a facility to understand the drug logistics systems in place

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
3. The preparedness and attitude of HCWs and acceptance of bCPAP by HCWs. For some of the facilities, the HCWs are not willing to place babies on the machine due to competence and their readiness to devout time and energy to such practice. For these HCWs, they refer anticipated preterm births and babies in severe respiratory distress to tertiary facilities. Examples are Mater Hospital, Afipko and KSSH, Lokoja.
4. Electricity is another major challenge bedeviling the use of bCPAP in the facilities. A number of these facilities cannot assure 24 hours supply of electricity whereas the PUMANI bCPAP machines require electricity at all times. One of the facilities requested a generator set from MCSP in order to be able to use the machine.
5. Data collection and entry has been a challenge. The HCWs see this as additional responsibility on their part despite their already tight schedules.
2. To hold a pre-implementation stakeholders’ meeting in order to be certain of the needs of the facilities, before donating equipment to them. This will ensure that the equipment will be put to proper use.
3. Develop a method to ensure step down trainings are conducted at the facility level
4. Advocate to the states government to support the new born unit of the institutions with dedicated power supply for the bCPAP machine alone, e.g. small generator set or solar power system
5. Special training specifically on data collection and reporting was proposed
2.2.7. Chlorhexidine Scale up
Following the launch of the national strategy to scale up the use of chlorhexidine in Nigeria in November 2016, MCSP supported the FMOH to develop a one year operational plan (with identified activities and responsible persons highlighted). MSCP will provide technical support to operationalize the plan at the national and state levels. MCSP also designed and administered a questionnaire to map and engage partners for supporting the scale up of chlorhexidine. The feedback showed that partner support (especially around procurement, distribution and training) is not available for chlorhexidine scale up in many states and these states will require technical assistance in order to ensure national scale up. At two other forums – annual conferences of Pediatrics Association of Nigeria (PAN) in Kaduna State and Association of General and Private Medical Practitioners of Nigeria (AGPMPN) in Osun State – MCSP partnered with other stakeholders to create more awareness about the use of chlorhexidine. Copies of the national strategy for the scale up of chlorhexidine were disseminated at both conferences. MCSP collaborated with SHOPS Plus, Christian Aid International, ESMPIN/SFH and PSN-PACFAH to host a forum with local manufacturers and other stakeholders with a goal to promote the availability of locally manufactured quality lifesaving childhood medicines and health related commodities specifically ORS/Zinc, chlorhexidine and Amoxicillin DT. The importance of instituting a pharmacovigilance reporting format for chlorhexidine and accelerating demand generation drive to boost utilization was noted. MCSP also secured approval from FMOH Department of Health Planning Research and Statistics to review the Labor and Delivery Register (LDR) to include a column on Chlorhexidine applied at birth. Consequently, Ebonyi and Kogi adopted the inclusion of this indicator for all health facilities in the states. By PY3, MCSP has seen an increase in the reporting on application of chlorhexidine gel at birth by the health worker (see Fig 3 below).

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Fig 3: Percent of newborns for which CHX Gel was applied by total live births in MCSP supported facilities
38194657
4228 4129
62925,464
5%8%
13%
32% 33%
40%
0
1000
2000
3000
4000
5000
6000
7000
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Oct-Dec, 2015 Jan-Mar, 2016 Apr-Jun, 2016 Jul-Sept, 2016 Oct-Dec, 2016 Jan-March, 2017
Livebirths Chlohexidine Gel Applications Linear (Chlohexidine Gel Applications)
Although there is an increase in the report on use of chlorhexidine, the number of health facilities not reporting its use is quite high. Next quarter, MCSP will provide supportive supervision to the facilities that are not reporting appropriately and on the job training on how to properly and effectively capture and report data and on the use and application of chlorhexidine. At the state level, MCSP supported Kogi State to finalize its operational plan, which takes into cognizance how to incorporate non MCSP supported facilities into chlorhexidine scale up and tracking utilization. Following advocacy by MCSP and other partners, Kogi State adopted the use of chlorhexidine gel for umbilical cord care and the national strategy to scale up chlorhexidine. The state procured 3,000 tubes of chlorhexidine which will be distributed to beneficiaries under the yet-to-be launched Health Care Plus program. The new program is aimed at revitalizing 12 PHCs facilities, supplying equipment and drugs, and providing free medical services. At a related event – the distribution of free pediatric drugs (amoxicillin suspension, antimalarial suspension, multivitamins and analgesics) to 10 secondary health facilities – the Kogi State Governor applied chlorhexidine gel to the cord to a newborn.
See Also
Nigeria Commits to Scaling Up Use of Antiseptic Gel to Reduce Newborn Deaths
An article in USAID’s Frontlines on the role of MCSP in Nigeria’s commitment to scale up the use of chlorhexidine gel to reduce neonatal mortality
Contest For Biz Students Is All About Umbilical Cords
A teaching case study written by students of Northwestern University’s Kellogg School of Management after a learning visit to understand chlorhexidine scale up in Nigeria

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
2.3. Child Health The broad objectives of the child health technical area are to (i) advance federal policies supportive of iCCM and its well-coordinated roll out across the states; (ii) improve the coverage and quality of evidence-based, high-impact child health interventions in Kogi and Ebonyi states; and (iii) improve preventive and care-seeking behavior for childhood illnesses among communities in Kogi and Ebonyi states. 2.3.1. Support to FMOH to review Child Health Policy
In support of the Child Health Division of the FMOH, MCSP identified and engaged consultants to review and finalize the recently updated National Child Health Policy and align it to the current structure of the draft National Strategic Health Development Plan. Next quarter, MCSP will support the FMOH to validate, print and disseminate the revised National Child Health Policy. 2.3.2. Develop a national-level child health advocacy plan
MCSP convened and facilitated a consensus building meeting to review the report of the national child health stakeholder analysis exercise which gained the endorsement and support of major child health stakeholders in Nigeria. Bearing in mind that most caregivers seek treatment for sick children from community pharmacists, PPMVs and PHCs, the key findings and recommendations of note include the following:
• Most responding stakeholder were in favor of a policy making AMX DT available at all levels of care • PPMVs should be an integral part of the healthcare system to contribute to addressing the gap in human
resource for health. However it is crucial to ensure adequate capacity building and sustainable access to quality commodities
Stakeholders debated the findings and recommendations from the analysis and supported the need for a National Child Health Advocacy plan after the consensus building meeting.
2.3.3. Stakeholder consultation meeting to gain approval for trained PPMVs to stock and sell AMOX DT
Effort to increase access to quality CH services at the community levels got a boost during the quarter under review following the adoption of the new national policy allowing use of AMX DT at all levels of care.
Following the ministerial directive for inclusion of Amox DT in the PPMV products list, the PCN revised and approved the PPMV products list (yet to be released) permitting PPMVs to stock and dispense AmoxDT. In Ebonyi State, the Essential Medicine List (EML) already includes Amox DT and during the next quarter MCSP will support the dissemination of the Ebonyi State EML (printed by the government.)
To enhance the availability of AmoxDT, MCSP is facilitating the linkage between the major local drug manufacturers and SMOH, SOML, Sustainable Development Goal (SDG) Office, PPMVs and other partners.

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
2.3.4. Provide Support to PPMV Associations, PCN and SMOH (PSD) to Better Support PPMVs
MCSP secured increased commitment for continued cooperation from the Pharmacist Council of Nigeria following discussions with its national leadership during the second quarter. The registrar of the PPMV regulatory agency acknowledged the need to bridge the service delivery gap by making use of available human resource such as the PPMVs. Though AMX DT has been listed on the PMV medicine list, the need for quality training and supportive supervision to ensure the quality of service delivery by PMVs was stressed. PCN indicated interest in being part of MCSP’s supportive supervision plan in project states through the involvement of the State PPMVs Supervisory Committee during supervision. Initial planning for the dissemination of the new PPMV Medicine list was discussed during the meeting and a role was identified for MCSP.
2.3.5. Selection of LGAs and health facilities
MCSP worked with the SMOH, SPDHCDA and PCN to conclude the process of LGA selection. Six LGAs were selected in each state for IMCI and iCCM implementation using the following agreed criteria:
• Population of under five in hard-to-reach communities • Geographical spread – Selection of two LGAs from each of the three senatorial districts in the state. • MCSP MNH-supported facilities • Global Fund & Saving One Million Lives Initiative supported facilities • Morbidity Statistics (using fever cases in under-five children reported in DHIS 2 as proxy) • Number of PPMVs per LGA • Willingness to partner with MCSP
Selection of health facilities for IMCI intervention is ongoing with high consideration for PHCs being supported by MCSP, SOML, Global Fund as well as hard-to-reach facilities under the recently launched Bello Health Intervention in Kogi State.
2.3.6. Entry meetings organized to increase community demand
MCSP organized entry meetings in the supported LGAs in both states to sensitize relevant stakeholders on the MCSP CH technical support and secure acceptance, participation and ownership of the program at the LGA, ward and community levels. The interactive meetings provided a platform for stakeholders to discuss and understand the iCCM strategy and to gather basic information on the health services, list of hard-to-reach communities, referral PHCs and availability of essential childhood medicines. The roles and responsibilities of the gatekeepers for the implementation of the program at the various levels were clearly explained.
2.3.7. Child Health Technical Working Group (CHTWG) meeting
MCSP along with other partners supported the SMOH to hold the first CHTWG meeting in both Ebonyi and Kogi states within this quarter. The objectives of the meeting were to update the states on the implementation status of MCSP supported child health activities, including the selection of CH focal LGAs, wards, and PPMVs as well as identify key set of child health indicators to track at the community level. The meeting was attended by Directors in the SMOH, Executive Secretary SPHCDA, a representative of the CH Division in FMOH, Program Officers, Representatives of PCN and National Association of Patent and Propriety Medicine (NAPPMED),

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
professional associations, PHC Coordinators of MCSP CH focal LGAs, community-based/civil society organizations and development partners offering child health services in the two project states. The CHTWG made the following recommendations:
• SMOH Officials should be engaged for the development of the CH AOP • National iCCM data collection tools should be used to collect iCCM data. • Trained health workers in MCSP supported PHCs, ward focal persons, LGA HMIS officers, NAPPMED
representatives, PCN and state supervisory team (consisting of SMOH, SPHCDA, and MCSP staff) should form the core of the monitoring and supervisory team for iCCM activities.
• ORT corners should be established in MCSP CH supported PHCs, with support for provision of ORT corner materials by MCSP
2.3.8. Kogi State Core Technical Committee Meeting
The core technical committee meeting was convened to review program performance. MCSP, SMOH, and professional associations (Pediatric Association of Nigeria and SOGON) presented activity updates. Poor documentation of services at PHCs and failure of some MCSP supported facilities to report data were noted as challenges to availability of quality data. Presentation by the SMOH showed that Saving One Million Lives (SOML) program had plans to employ midwives and procure commodities such as AmoxDT, chlorhexidine gel, and gentamicin for distribution to 84 PHCs supported by the program in Kogi State. An area for possible collaboration with PAN is its voluntary pediatric service scheme which currently targets seven primary and secondary health facilities. In the scheme, pediatricians provide clinical services in the target health facilities as well as mentor service providers on essential newborn care.
2.4. Family Planning MCSP is supporting Kogi and Ebonyi states to increase access to and uptake of contraceptives towards actualizing Nigeria’s commitment to achieving the global contraceptive prevalence rate (CPR) of 36% by 2020. 2.4.1. Capacity building on PP-LARC for health workers
MCSP empowered 23 health workers (nurses/midwives, CHEWs and doctors) from the labor and delivery and postpartum units of 13 health facilities with the knowledge, skills and attitude to provide quality postpartum long acting reversible contraceptive (PP-LARC) services. The health workers were trained to use the Balanced Counseling Strategy and new WHO medical eligibility criteria to support pregnant women and early postpartum women choose appropriate contraceptive methods. MCSP also supported the health workers with essential materials / equipment needed to establish PP-LARC services in their respective health facilities. Post-training follow-up and supportive supervision visits to the 13 facilities showed that PPFP counseling has been initiated in 11 facilities and implants insertions initiated in nine of the facilities.
As the training beneficiaries begin to provide PP-LARC services in their facilities, they would be increasing contraceptives access and options and reduce unmet needs for family planning among postpartum women in Nigeria. MCSP will continue to train more healthcare workers to expand PPFP services to more health facilities in Ebonyi and Kogi.
A trainer demonstrating the insertion of IUCD on a model during PP-LARC training

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
2.4.2. Training of health workers as dedicated post-partum family planning counselors
Recognizing that counseling is the bedrock of a successful FP program, and in order to further strengthen PPFP counseling during ANC interactions, MCSP identified and trained 36 health workers in Kogi and Ebonyi states as dedicated post-partum family planning counselors. The trained health workers were mainly nurses, midwives and CHEWS and were drawn from primary, secondary and tertiary facilities. To complement the training, MCSP produced and distributed dedicated counseling flip books and brooches – thus empowering and motivating the trainees to effectively counsel women and their families and support them to choose and receive the FP methods of their choice. 2.4.3. Coordination and collaboration on family planning
MCSP participated in the review and finalization of the national PPFP/LARC training manual and sponsored five health care workers from project states to participate in the training of trainers and field testing of the PPFP/PP-LARC training manual for CHEWs. The program also participated in a review meeting on task shifting policy and is providing support for the implementation of the policy in Ebonyi and Kogi states. MCSP also participated in the stakeholders planning meeting on the establishment of centers for expert removal of non- palpable implants. 2.5. Adolescent Sexual and Reproductive Health MCSP’s ASRH work aims to improve the quality of health services for adolescents and young mothers/parents by building knowledge and skills necessary to delay early childbearing, care for pregnancy, birth, and the postpartum period, including access to postnatal care, PPFP, and CH services. 2.5.1. Step-down trainings on the age and life stage counseling tools
Step-down trainings on the age and life stage (ALS) counseling tools were conducted for 35 service providers selected from FMOH, the four pilot sites, four youth-friendly centers, and pre-service institutions in Kogi and Ebonyi states. At the end of the five-day skills-based training, participants developed action plans to use the ALS for service provision and were provided with the ALS assessment tool and counseling cards to strengthen service provision. Part of the action plan developed is to see them train others in the facilities on the use of this tool to provide AYFH services. MCSP also provided assistance to FMOH for the reprint of a training manual and job aid on AYFH services provision to ensure availability at health facilities. 2.5.2. Advocate for improved coordination of ASRH services
The 4th meeting of the National Adolescent Health & Development Working Group (NAHDTWG) – a national advisory body to the FMOH on advancing the health and development of young people – was held in March 2017. The broad aim of the NAHDWG is to ensure that policy speaks to current health trends and global policy frameworks and development goals. MCSP team was well represented and contributed immensely to the discussions and consensus reached during the meeting. The objectives of the 4th meeting of the NAHDWG were to:
• Update members on the implementation status of adolescent and youth health and development (AHD) programs in Nigeria.
• Chart the way forward for AHD programming in Nigeria and improving coordination among stakeholders.
• Discuss next line of action on the draft minimum package of service and standards for Adolescent and Youth Friendly Health Services.
MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Recommendations from the meeting included:
• Mapping of agencies implementing adolescent health • Biennial report on the state of Adolescent Health and Development in Nigeria • Focusing on PHCs for adolescent health services provision • Need to leverage local resources to move AHD issues forward • Critical need for a budget line for AHD • Adolescent & Youth Friendly Health Services (AYFHS) logo needs to become national and known to all
young persons • Explore strategies to broaden access to trainings for health workers without spending huge resources
and incurring unnecessary expenses. The NAHDWG meeting is planned to be held biannually; however, the last meeting was held in 2013. The next TWG meeting is scheduled for September 2017. However, the ASRH TWG meetings funded by the SMOH could not be held within the reporting period due to conflicting schedules of the states’ ASRH desk officers. 2.5.3. Conduct implementation research (Phase I)
The analysis of data from Phase I of the formative research to identify the needs of first-time parents has been completed. Preliminary findings from the study showed that most respondents (girls/partners/relatives) believed the age of entry into marriage should be between 25 and 30. They opined that an individual within this age range would have acquired a certain level of education or skills and become an independent person with a sense of self. The cost of care was the overriding factor determining health-seeking behavior of adolescent mothers. Other factors include attitudes of health personnel, influence of mothers, and directives from spouse. The study also showed that male involvement in the reproductive health of the adolescent spouses is minimal. The final report will be disseminated next quarter. Its findings will be utilized in developing intervention packages for FTM/P in the two project states.
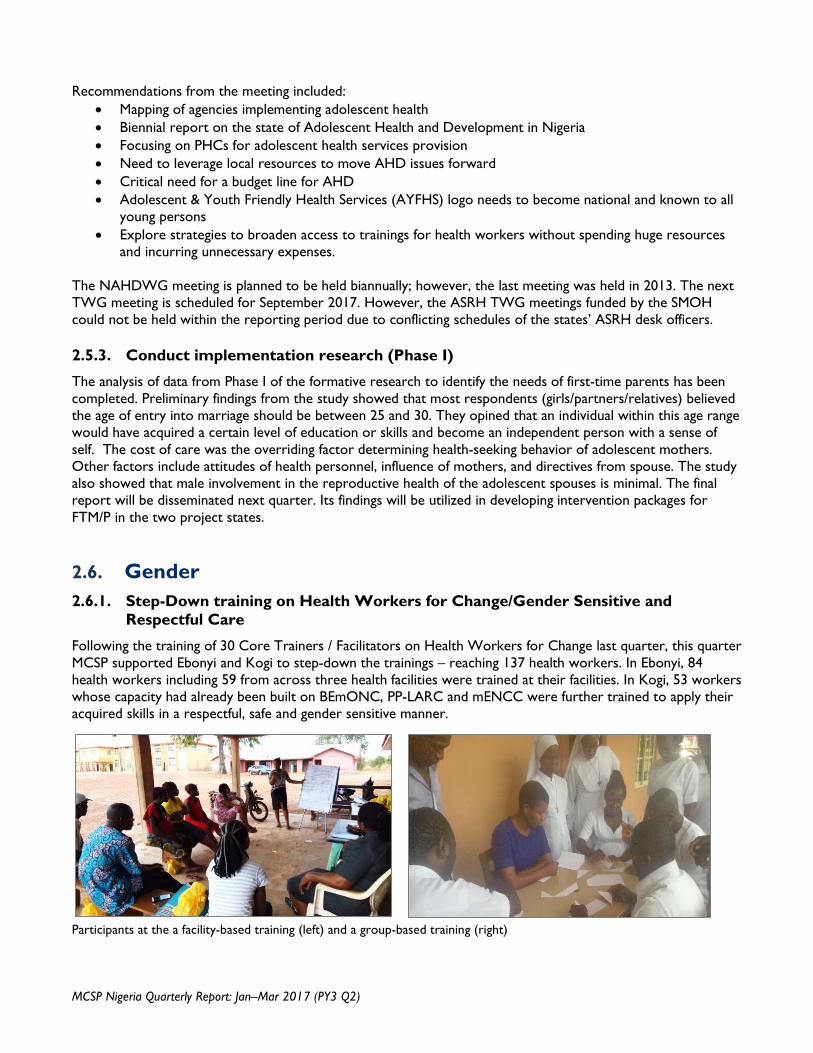
2.6. Gender 2.6.1. Step-Down training on Health Workers for Change/Gender Sensitive and
Respectful Care
Following the training of 30 Core Trainers / Facilitators on Health Workers for Change last quarter, this quarter MCSP supported Ebonyi and Kogi to step-down the trainings – reaching 137 health workers. In Ebonyi, 84 health workers including 59 from across three health facilities were trained at their facilities. In Kogi, 53 workers whose capacity had already been built on BEmONC, PP-LARC and mENCC were further trained to apply their acquired skills in a respectful, safe and gender sensitive manner.
Participants at the a facility-based training (left) and a group-based training (right)

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
The training helped to foster better commitment and involvement of health workers and local communities in ensuring quality of care especially for women and children. For instance, at Nwofe PHC, Ebonyi State, the Community Development Centre offered to provide accommodation within the health facility premises for two MSS midwives so that the facility can start providing 24-hour services. The facility staff in turn decided to change their duty roster from April 2017 to reflect a 24-hour service.
2.6.2. Establishing visual privacy
Recognizing that respect for women’s basic human rights such as the right to privacy is at the core of maternity care, MCSP is intervening to support selected facilities in Ebonyi and Kogi to establish visual privacy during care. Availability of visual privacy will also encourage and facilitate having a companion of choice during facility delivery, particularly male partners, who are often not allowed into delivery rooms due to a lack of visual privacy for other mothers. This intervention is in
line with the WHO QoC standards and the Respectful Maternity Care charter. To support the facilities and demonstrate a visual privacy model to governments and service providers, MCSP therefore carried out a needs assessment for visual privacy in 10 facilities and prepared a bill of quantities to procure needed infrastructural improvements and adjustments, which are expected to be in place next quarter.
2.6.3. Respectful Maternity Care (RMC)
For effective respectful maternity care, MCSP is collaborating with NANNM to harmonize implementation of RMC activities. At the moment, NANNM has conducted step-down trainings for health workers in the two project states – this will
be leveraged to optimize planned interventions in RMC. Similarly, MCSP will continue to engage and support White Ribbon Alliance Nigeria (WRAN) towards implementing a national advocacy on RMC with focus on Ebonyi and Kogi states.
2.6.4. Client Exit Interview
MCSP is supporting facilities in Ebonyi and Kogi to start administering client exit interviews as a measure of level of satisfaction with services received during antenatal care (ANC), labour and delivery, and postnatal care (PNC). Such feedback is critical to gathering information for improving the quality of care and experience of care at health
facilities. The clients exit interviews will also be the source of data for measuring the percentage of women who are satisfied with their experience of care during child birth in selected MCSP supported facilities – a new indicator being tracked by the program.
2.6.5. Male Engagement
A concept note on male engagement was developed during the quarter to frame a model to (1) build the capacity of health providers to effectively engage men; (2) improve facility settings to facilitate male engagement; and (3) develop resources such as job aids and IEC materials (posters and pamphlets) on male engagement. As household decision makers, men have a critical role along the RMNCAH
continuum of care and effectively engaging them will contribute to uptake of services and quality improvement. MCSP is working with the project states to include in the ANC, L&D and FP registers a performance indicator of the number of visits made by men/boys to specified sexual, reproductive and maternal, newborn or child health (MNCH) services.
An analysis of gender-related findings from the Quality of Care Study in project states was conducted within the quarter and showed that health workers in the states need further capacity building to deliver gender-sensitive, respectful care. The analysis showed that:

January–March 2017 www.mcsprogram.org
• In ANC, only 12% of providers introduced themselves to the client, and only 10% asked if she would like a male partner or companion to participate;
• In FP, in fewer than 5% of the observations was there any discussion between the health worker and the client on how she can be assisted to make informed decisions on the family planning method she will use, and only 10% of health workers strongly
think that a woman should be able to choose a FP method on her own;
• In L&D, only 36% of facilities were equipped to allow for birth companions to be present;
• About 23% of health workers do not think unmarried clients should use family planning services.
2.7. Pre-Service Education Last quarter, MCSP conducted a baseline assessment of PSE institutions and affiliated practicum sites in Ebonyi and Kogi states in order to identify existing gaps in the quality of training being rendered in the institutions. This quarter, MCSP supported the institutions to start bridging the identified gaps which included: poor classroom and clinical simulation training skills of the educators, lack of or poorly equipped clinical simulations laboratory in most of the training institutions, lack of gender sensitivity of the clinical practice sites, and lack of audio-visuals in the classrooms and simulation laboratories. Other identified gaps include lack of school library or insufficient quantities of appropriate reference training materials where the library exist, lack of computer laboratories or insufficient quantities of functional computers where they already exist, and absence of functional management committees or infrequent meetings of the committees where such exist.
Foremost, to improve pre-service education in project states, MCSP is currently supporting 10 institutions that had less than 80% SBM-R scores in the classroom and practical instruction thematic area during the PSE baseline assessment of these institutions. As part of solutions to bridging the gap, MCSP is by helping to train 42 educators (lecturers, tutors, preceptors) of the institutions. The educators were trained to effectively develop learning objectives and lesson plans, prepare the teaching environment, prepare and use visual aids, prepare and deliver interactive presentations, and facilitate group learning. They were also trained to facilitate the development of healthcare delivery skills, manage clinical practice, and prepare and use knowledge assessments. Next quarter, the educators will be trained in BEmONC and MCSP will support the institutions to equip their clinical stimulation laboratory.
2.8. Monitoring and Evaluation 2.8.1. Training of Trainers on Record Keeping, Reporting and Use of Data for decision
making
During the reporting period, MCSP conducted a ToT on record keeping, reporting and use of data for decision making. This activity was undertaken in preparation for the record keeping training for the 120 MCSP Phase 2 supported health facilities scheduled for May 2017. The training of trainers was held in Lokoja, Kogi State using a standard
training manual developed by MCSP. Fourteen selected trainers including three M&E officers from the HMIS units of Kogi and Ebonyi SMoH and MCSP staff participated in the 3-day training. Participants were introduced to the concepts of record keeping, reporting and use of data for decision making. Participants were also introduced to the current

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
NHMIS registers and forms using exercises to practice the completion of the registers, and were trained on data visualization whereby they practiced how to prepare simple charts and use these charts to make relevant decisions. The overall objective of
the ToT was to ensure that all selected trainers that will be stepping down this training to the health care providers are proficient with adequate knowledge, skills and understanding to perform the task
2.8.2. Technical support to SOGON
MCSP supported SOGON to develop data entry templates for all the national MPDSR tools. The SPSS software was used for designing the data entry templates. It is expected that the templates will
enable SOGON to effectively track the causes and number of death in the program states. The SOGON Program Officer based in Abuja has been introduced to the use of the data templates.
2.8.3. Monthly and Quarterly data collation meetings
MCSP continued to provide technical support on monthly data collation meetings for MCSP supported health facilities on a monthly basis, and for all other health facilities on a quarterly basis. Participants at the meetings included LGA Head of Departments, M&E Officers, Record Officers, and Officers-in-Charge (OIC) of health facilities and selected service providers from different service delivery points in the health facilities. During the
meetings, health facility records officers/OICs attended with approved HMIS tools from where the monthly data for service delivery are collated and validated. The meeting provided opportunity to check on the quality of routine data before they are entered into DHIS2. During the meetings, facilities with stock out of HMIS registers and forms were issued new ones and feedback given on quality of data and reporting rates.
2.8.4. Core Technical Committee Meetings and other supports to HMIS units and health facilities
MCSP Strategic Information Officers in the two program states participated in the states’ core technical committee meetings during the reporting period to discuss RMNCH indicators. Presentations were made on selected RMNCH indicators from routine generated data from MCSP supported health facilities to show progress made over specific targets. Attentions of the state HMIS units were drawn to the reporting rates and discussion held on improving the reporting rates as well as the quality of data for the two states. Other partners as well as representatives of different units in the program SMOH participated in the meetings. Since the adoption of the chlorhexidine policy in Nigeria, MCSP continues to provide necessary technical supports including M&E support at both national and state levels. During the reporting period, MCSP held discussions with the Ebonyi and Kogi States HMIS units on the need to begin to track the use of chlorhexidine in all health facilities
in the states (MCSP is tracking this in the program supported health facilities). This is imperative as it will enable the state government to have records of the quantities used which will inform future procurements. MCSP is working with and supporting the HMIS unit to develop a data template to be used for this purpose. MCSP also provided record keeping technical support to selected health facilities in the program states. It was observed that the tertiary health facilities and few of the mission health facilities were not all using the NHMIS registers to record service provisions. The Strategic Information Officers and Service Improvement Coordinators visited the health facilities and advocated for the use of the forms and registers. On-the-job trainings and orientation were provided. It is anticipated that these health facilities will continue to use the NHMIS registers and forms.

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
2.9. Operations Research The Operations Research technical area of the program involves the testing of new innovations for acceptability and feasibility in the Nigerian socio-cultural context. Some of the learning agenda includes: (1) generation of evidence from the comparison of group-based training with the Low
Dose High Frequency (LDHF) training approach in Ebonyi and Kogi States; (2) implementation research to improve reproductive health for first-time parents in Ebonyi and Kogi states; and (3) care-seeking during infancy and the post-partum period in Nigeria.
Table 2: Learning agenda updates
LDHF Study • Trained 42 master mentors and data collectors • Carried out stepdown training and data collection: 340 health workers trained till date • Completed immediate post-training assessment/data collection • Preliminary results showed significant improvement in knowledge and skills (post-
course) in both groups following BEmONC trainings • Comparison of outcomes between the two training approaches pending • M-Mentoring ongoing • Completed 3 months data collection for primary outcome in March 2017 • Data cleaning is ongoing and preliminary report expected by end of April 2017
Adolescent Study
• Completed data collection and analysis • Zero draft report developed and under finalization • Completed stakeholders meetings for the expansion of Phase I in Sokoto and Ondo;
Bauchi and Cross River states
Newborn Care-seeking Study
• MCSP supported the training of 11 qualitative interviewers and 3 state coordinators in Ibadan including 1 from Ebonyi
• Conducted learning visit with J-PAL • Data collection ongoing in Oyo but yet to start in Kaduna • Completed data collection in Ibadan and MCSP state (Ebonyi) and preparations for
analysis being made when the Kaduna piece of data collection is completed

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
3.0 STAKEHOLDERS PARTICIPATION / INVOLVEMENT 3.1. Professional Associations MCSP has sub-awards with four local professional associations – the Society of Gynecology and Obstetrics of Nigeria (SOGON), Pediatric Association of Nigeria (PAN), Nigerian Society of Neonatal Medicine (NISONM), and National Association of Nigerian Nurses and Midwives (NANNM) – being key stakeholders in the goal to end preventable child and maternal deaths in Nigeria. The contributions of the associations between January and March 2017 are highlighted as follows:
3.1.1. SOGON Updates on Voluntary Obstetric Scheme
In this quarter, nine SOGON members (five in Ebonyi and four in Kogi) visited their assigned facilities and made 20 visits (14 in Ebonyi and six in Kogi). The volunteers did consultations during ANCs and mentored and provided on the job training for 56 health workers in line with SOGON’s contractual agreement with MCSP. The notable achievements of the scheme are as follows:
• In Ebonyi, mentored 38 health workers on family planning, malaria in pregnancy, danger signs in pregnancy, AMTSL, pre-eclampsia and pregnancy induced hypertension and antenatal consultation for 111 women;
• In Kogi, conducted on-the-job training of 18 health workers on AMTSL, management of
pre-eclampsia and eclampsia including demonstration, preparation and administration of MgSO4; development and display of protocol (job aid posters) for management of pre-eclampsia and eclampsia (at General Hospital Okene); and antenatal consultation with a total of 24 women including one with pre-eclampsia.
MPDSR training for Kogi State MPDSR committee members
Twenty-eight (28) participants were trained for three days on the roles, responsibilities and processes of Maternal and Perinatal Death Surveillance and Response (MPDSR). These participants were members of the State MPDSR Steering Committee. Copies of the MPDSR Guidelines were distributed to participants as resource materials. Participants developed action
plans for the state committee in implementing MPDSR in the state. Similar training will be replicated in Ebonyi in the next quarter. The primary goal of MPDSR is to eliminate preventable maternal and perinatal mortality by obtaining and using information on each maternal and perinatal death to guide public health actions and monitor their impacts.
MPDSR training for quality improvement facilities
SOGON collaborated with MCSP and Kogi SMoH during the reporting period to train two members each from 20 MCSP Quality Improvement (QI) facilities on roles, responsibilities and process of MPDSR. Quality Improvement Committees (QIC) is fully established and functional in these 20 facilities
and MPDSR activity is coordinated by these committees on behalf of their facilities. The training was aimed at ensuring that MPDSR activities are adequately captured, reported and discussed by the facility members to learn lesson and improve the quality of services in the facility.
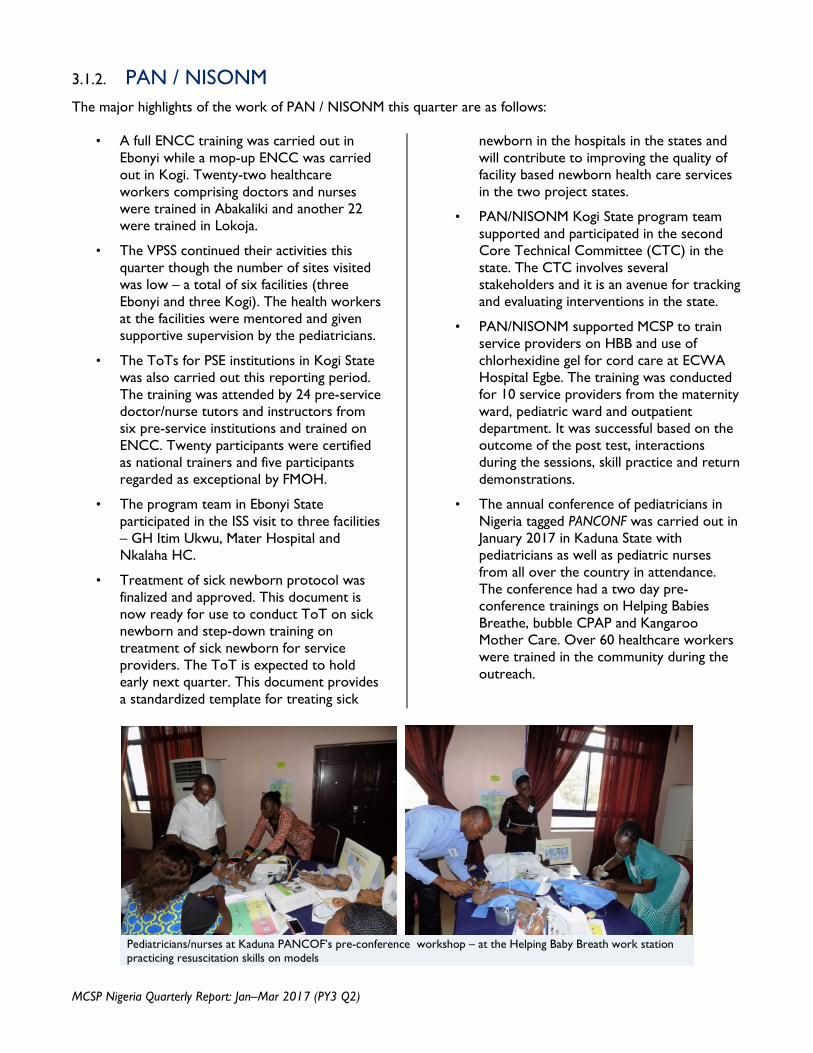
MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
3.1.2. PAN / NISONM The major highlights of the work of PAN / NISONM this quarter are as follows:
• A full ENCC training was carried out in Ebonyi while a mop-up ENCC was carried out in Kogi. Twenty-two healthcare workers comprising doctors and nurses were trained in Abakaliki and another 22 were trained in Lokoja.
• The VPSS continued their activities this quarter though the number of sites visited was low – a total of six facilities (three Ebonyi and three Kogi). The health workers at the facilities were mentored and given supportive supervision by the pediatricians.
• The ToTs for PSE institutions in Kogi State was also carried out this reporting period. The training was attended by 24 pre-service doctor/nurse tutors and instructors from six pre-service institutions and trained on ENCC. Twenty participants were certified as national trainers and five participants regarded as exceptional by FMOH.
• The program team in Ebonyi State participated in the ISS visit to three facilities – GH Itim Ukwu, Mater Hospital and Nkalaha HC.
• Treatment of sick newborn protocol was finalized and approved. This document is now ready for use to conduct ToT on sick newborn and step-down training on treatment of sick newborn for service providers. The ToT is expected to hold early next quarter. This document provides a standardized template for treating sick
newborn in the hospitals in the states and will contribute to improving the quality of facility based newborn health care services in the two project states.
• PAN/NISONM Kogi State program team supported and participated in the second Core Technical Committee (CTC) in the state. The CTC involves several stakeholders and it is an avenue for tracking and evaluating interventions in the state.
• PAN/NISONM supported MCSP to train service providers on HBB and use of chlorhexidine gel for cord care at ECWA Hospital Egbe. The training was conducted for 10 service providers from the maternity ward, pediatric ward and outpatient department. It was successful based on the outcome of the post test, interactions during the sessions, skill practice and return demonstrations.
• The annual conference of pediatricians in Nigeria tagged PANCONF was carried out in January 2017 in Kaduna State with pediatricians as well as pediatric nurses from all over the country in attendance. The conference had a two day pre-conference trainings on Helping Babies Breathe, bubble CPAP and Kangaroo Mother Care. Over 60 healthcare workers were trained in the community during the outreach.
Pediatricians/nurses at Kaduna PANCOF’s pre-conference workshop – at the Helping Baby Breath work station practicing resuscitation skills on models
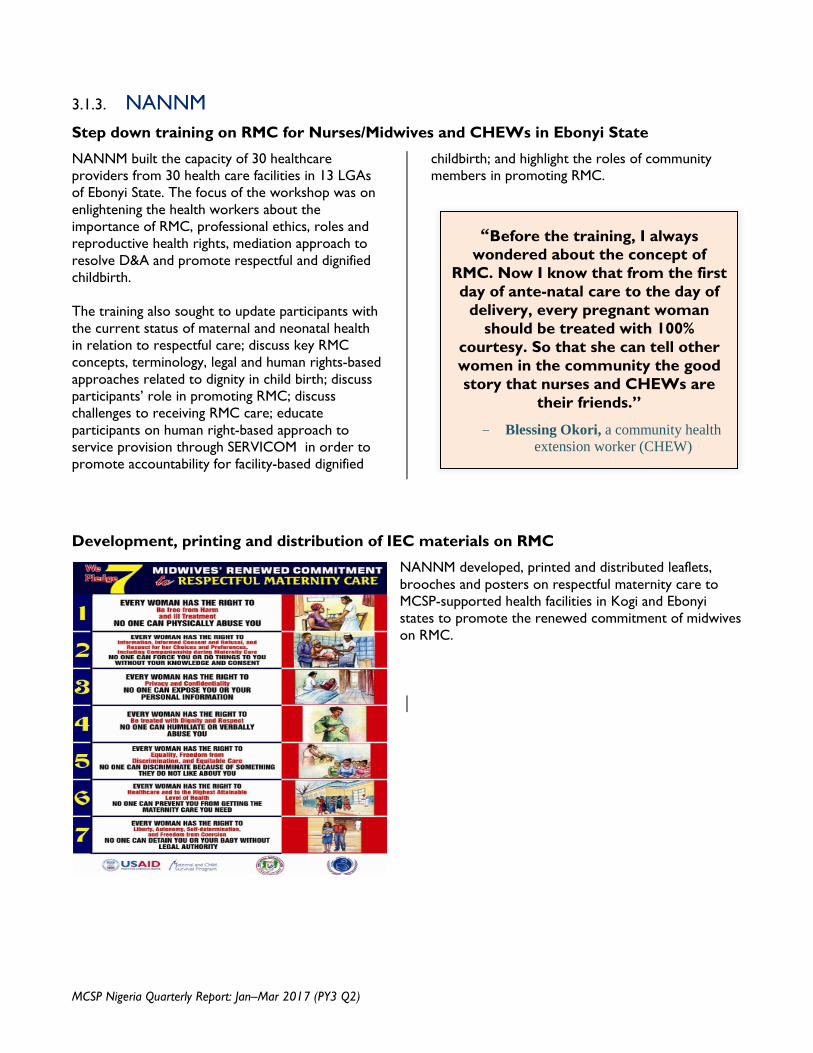
MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
3.1.3. NANNM Step down training on RMC for Nurses/Midwives and CHEWs in Ebonyi State
NANNM built the capacity of 30 healthcare providers from 30 health care facilities in 13 LGAs of Ebonyi State. The focus of the workshop was on enlightening the health workers about the importance of RMC, professional ethics, roles and reproductive health rights, mediation approach to resolve D&A and promote respectful and dignified childbirth. The training also sought to update participants with the current status of maternal and neonatal health in relation to respectful care; discuss key RMC concepts, terminology, legal and human rights-based approaches related to dignity in child birth; discuss participants’ role in promoting RMC; discuss challenges to receiving RMC care; educate participants on human right-based approach to service provision through SERVICOM in order to promote accountability for facility-based dignified
childbirth; and highlight the roles of community members in promoting RMC.
Development, printing and distribution of IEC materials on RMC
NANNM developed, printed and distributed leaflets, brooches and posters on respectful maternity care to MCSP-supported health facilities in Kogi and Ebonyi states to promote the renewed commitment of midwives on RMC.
“Before the training, I always wondered about the concept of
RMC. Now I know that from the first day of ante-natal care to the day of
delivery, every pregnant woman should be treated with 100%
courtesy. So that she can tell other women in the community the good story that nurses and CHEWs are
their friends.”
- Blessing Okori, a community health extension worker (CHEW)

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
4.0 MANAGEMENT AND ADMINISTRATIVE MATTERS 4.1. Appointments / Resignation
• New staff assumed duties between January and March 2017 to fill the following positions:
1. Driver based in Ebonyi 2. Driver based in Abuja 3. Human Resources Assistant based in Abuja 4. Procurement Officer based in Abuja 5. Quality Improvement Coordinator based in Ebonyi 6. Quality Improvement Coordinator based in Kogi 7. Monitoring & Evaluation Officer based in Abuja 8. Service Improvement Coordinator based in Ebonyi 9. Monitoring, Evaluation and Learning, Senior Manager (Child Health) in Abuja
• The successful candidate for the National Child Health Coordinator has accepted the appointment offers and will begin in the next quarter.
• Interviews were conducted for the position of Supply Chain Manager – recruitment to be completed next quarter.
• The Ebonyi State Newborn Advisor resigned her appointment in February 2017. Recruitment for a new Advisor has been initiated and will be finalized next quarter. In the interim, the State Team Leader doubles as the Newborn Advisor.
4.2. Team Orientation • Newly recruited members of the MCSP Child Health team were oriented during the quarter. The
meeting exposed participants to details on the composition of MCSP Consortium, and the operational systems/procedures of MCSP using the Local Hire Employee Manual. Other issues discussed include Overview of polices, financing, procurement, safety, security, reporting and timelines. The orientation also focused on understanding MCSP Work plan/Overview of CH Q2 PY3 Work plan activities with a focus on status and strategies for effective implementation.

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
5.0 IMPLEMENTATION CHALLENGES / LESSONS LEARNED 5.1. Implementation Challenges
1. Insecurity (characterized mostly by communal clashes, kidnapping and herdsmen attacks) hinders program implementation and activities including supportive supervision to health facilities. In Kogi, MCSP conducted an advocacy visit to the Commissioner. He reassured MCSP that the state government is working hard to reduce instability. He further offered that the police can escort MCSP team when they are traveling to crime prone areas1.
2. Dwindling government resources (due partly to current economic recession) limits funding / financial commitment by governments, e.g., procurement of commodities, health facility renovation and payment of health workers’ salaries. Irregular or non-payment of salaries in turn demotivates health workers leading to absenteeism or strikes.
3. Frequent strike actions by health workers mean closure of health facilities and slowing down, postponement or outright cancellation of program activities. Frequent strike actions often discourage clients from using facilities.
4. USAID has put on hold iCCM implementation. The Mission has requested further consultation with MCSP to discuss new strategies on how best iCCM can be implemented in the two project states.
5. There was also a hold on procurement of CH commodities as seed stock.
6. Kangaroo Mother Care: many mothers dislike having to stay back in the facilities after delivery, thus limiting the application of KMC by mothers of preterm / under weight babies. When a client refused admission after much counseling and persuasion, the choice should be respected and supported, home visits should then be conducted to ensure they receive proper KMC information.
7. Chlorhexidine scale up: plans to develop a communication campaign including radio jingles was stalled / put on hold due to FMOH’s plan to develop a combined RMNCAH+N communication strategy.
5.2. Lessons Learned Here are some of the key lessons learned in the quarter under review:
• Research projects need stakeholder involvement from conception, design, and implementation to monitoring and evaluation. More importantly, the need for quality assurance means that expert reviews will be required. It is therefore important to factor all these into planning so that there would not be unnecessary delays during implementation.
6.0 PLANNED ACTIVITIES FOR NEXT QUARTER 6.1. Maternal Health
• The second BEmONC training for health care workers from the newly added 120 Phase II health facilities in both MCSP supported States.
1 2,000 displaced in fresh Ebonyi communal clash – https://guardian.ng/news/2000-displaced-in-fresh-ebonyi-communal-clash/)
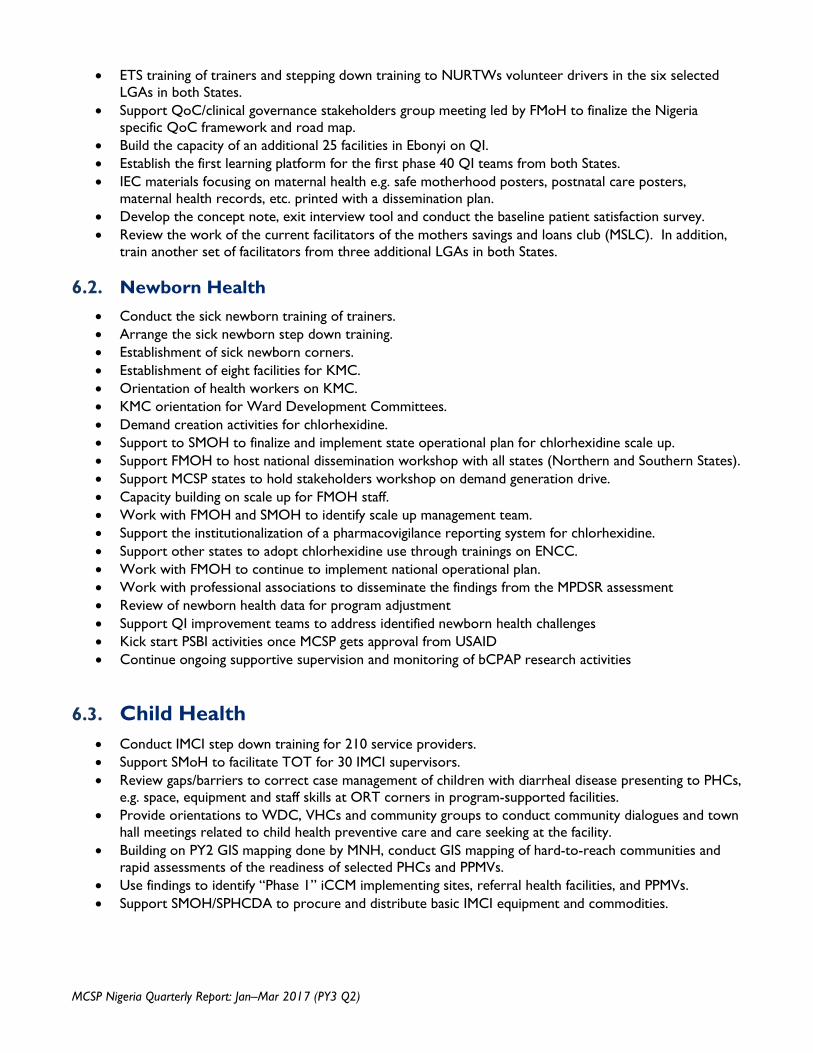
MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
• ETS training of trainers and stepping down training to NURTWs volunteer drivers in the six selected LGAs in both States.
• Support QoC/clinical governance stakeholders group meeting led by FMoH to finalize the Nigeria specific QoC framework and road map.
• Build the capacity of an additional 25 facilities in Ebonyi on QI. • Establish the first learning platform for the first phase 40 QI teams from both States. • IEC materials focusing on maternal health e.g. safe motherhood posters, postnatal care posters,
maternal health records, etc. printed with a dissemination plan. • Develop the concept note, exit interview tool and conduct the baseline patient satisfaction survey. • Review the work of the current facilitators of the mothers savings and loans club (MSLC). In addition,
train another set of facilitators from three additional LGAs in both States. 6.2. Newborn Health
• Conduct the sick newborn training of trainers. • Arrange the sick newborn step down training. • Establishment of sick newborn corners. • Establishment of eight facilities for KMC. • Orientation of health workers on KMC. • KMC orientation for Ward Development Committees. • Demand creation activities for chlorhexidine. • Support to SMOH to finalize and implement state operational plan for chlorhexidine scale up. • Support FMOH to host national dissemination workshop with all states (Northern and Southern States). • Support MCSP states to hold stakeholders workshop on demand generation drive. • Capacity building on scale up for FMOH staff. • Work with FMOH and SMOH to identify scale up management team. • Support the institutionalization of a pharmacovigilance reporting system for chlorhexidine. • Support other states to adopt chlorhexidine use through trainings on ENCC. • Work with FMOH to continue to implement national operational plan. • Work with professional associations to disseminate the findings from the MPDSR assessment • Review of newborn health data for program adjustment • Support QI improvement teams to address identified newborn health challenges • Kick start PSBI activities once MCSP gets approval from USAID • Continue ongoing supportive supervision and monitoring of bCPAP research activities
6.3. Child Health
• Conduct IMCI step down training for 210 service providers. • Support SMoH to facilitate TOT for 30 IMCI supervisors. • Review gaps/barriers to correct case management of children with diarrheal disease presenting to PHCs,
e.g. space, equipment and staff skills at ORT corners in program-supported facilities. • Provide orientations to WDC, VHCs and community groups to conduct community dialogues and town
hall meetings related to child health preventive care and care seeking at the facility. • Building on PY2 GIS mapping done by MNH, conduct GIS mapping of hard-to-reach communities and
rapid assessments of the readiness of selected PHCs and PPMVs. • Use findings to identify “Phase 1” iCCM implementing sites, referral health facilities, and PPMVs. • Support SMOH/SPHCDA to procure and distribute basic IMCI equipment and commodities.

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
6.4. Family Planning • Training of 60 service providers (L&D, PNC &FP units) on PP-LARC. • Conduct post training follow up. • Conduct FP compliance monitoring in FP supported health facilities. • On-site while-site orientation of hospital community on benefits of PPFP. • Health facility assessment for permanent method. • Provider network meeting. • Support constitution/revitalizing of FP TWG in the two project supported states. • Support MCSP Nurses/Midwives to participate in the WACN 14th Biennial General meeting and
scientific conference in Abuja. • Finalize the FP SMART advocacy concept note for training for FP champions to develop FP SMART
advocacy strategy. • Procurement of 100 dedicated counselors bags. • Training of 48 health care workers from phase two health facilities on PPFP support MCSP.
Nurses/midwives to participate in the WACN 14th Biennial General meeting and scientific conference in Abuja.
• Conduct AFP SMART advocacy training for states program officers in Kogi and Ebonyi state. 6.5. Adolescent Sexual and Reproductive Health
• Build capacity of health workers to deliver high-quality MNCH and FP services in Kogi and Ebonyi States.
• Advocate for improved coordination of ASRH services in Nigeria. • Conduct implementation research study (Phase 2) in Kogi and Ebonyi States. • Expand “Phase 1” of formative assessment for first-time parents to Bauchi, Cross River, Ondo and
Sokoto States. • Collaboration with Human Network International on AIRTEL 3-2-1 ASRH intervention.
6.6. Gender • Engage with all trained HWFC facilitators to train 120 health workers from Phase I facilities (targeting
OICs). • Conduct HWFC at health facilities focusing on the 40 QI facilities at the first instance. • Finalize male engagement job aid and resources • Develop tool and orientation workshop for first-line support for GBV survivors • Develop advocacy brief from findings of HWFC trainings and conduct stakeholders’ analysis to
commence engagement of relevant stakeholders on problems preventing health workers from doing their work efficiently.
• Conduct in collaboration with the MNH team, a clients’ exit interview questionnaire to measure “experience of care” for health facility users.
• Work with NANNM to fast track RMC implementation. • Work with White Ribbon Alliance Nigeria to promote RMC advocacy. • Work with Service Improvement Coordinators (SICs/FP/RH Coordinators/QIC) to ensure consistent
follow-up on trained service providers who made commitments to change their negative practices.
6.7. Pre-Service Education
• Conduct second batch of effective teaching skills training. • Conduct BEmONC training for PSE educators in project states.
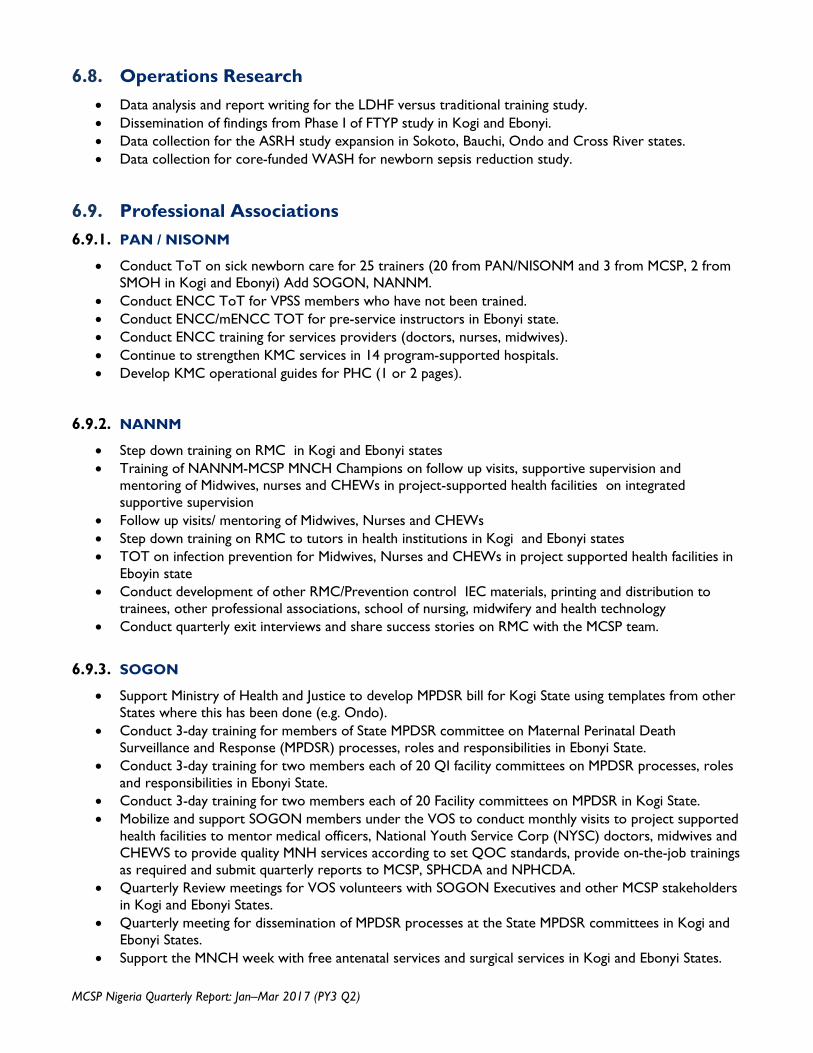
MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
6.8. Operations Research • Data analysis and report writing for the LDHF versus traditional training study. • Dissemination of findings from Phase I of FTYP study in Kogi and Ebonyi. • Data collection for the ASRH study expansion in Sokoto, Bauchi, Ondo and Cross River states. • Data collection for core-funded WASH for newborn sepsis reduction study.
6.9. Professional Associations 6.9.1. PAN / NISONM
• Conduct ToT on sick newborn care for 25 trainers (20 from PAN/NISONM and 3 from MCSP, 2 from SMOH in Kogi and Ebonyi) Add SOGON, NANNM.
• Conduct ENCC ToT for VPSS members who have not been trained. • Conduct ENCC/mENCC TOT for pre-service instructors in Ebonyi state. • Conduct ENCC training for services providers (doctors, nurses, midwives). • Continue to strengthen KMC services in 14 program-supported hospitals. • Develop KMC operational guides for PHC (1 or 2 pages).
6.9.2. NANNM
• Step down training on RMC in Kogi and Ebonyi states • Training of NANNM-MCSP MNCH Champions on follow up visits, supportive supervision and
mentoring of Midwives, nurses and CHEWs in project-supported health facilities on integrated supportive supervision
• Follow up visits/ mentoring of Midwives, Nurses and CHEWs • Step down training on RMC to tutors in health institutions in Kogi and Ebonyi states • TOT on infection prevention for Midwives, Nurses and CHEWs in project supported health facilities in
Eboyin state • Conduct development of other RMC/Prevention control IEC materials, printing and distribution to
trainees, other professional associations, school of nursing, midwifery and health technology • Conduct quarterly exit interviews and share success stories on RMC with the MCSP team.
6.9.3. SOGON
• Support Ministry of Health and Justice to develop MPDSR bill for Kogi State using templates from other States where this has been done (e.g. Ondo).
• Conduct 3-day training for members of State MPDSR committee on Maternal Perinatal Death Surveillance and Response (MPDSR) processes, roles and responsibilities in Ebonyi State.
• Conduct 3-day training for two members each of 20 QI facility committees on MPDSR processes, roles and responsibilities in Ebonyi State.
• Conduct 3-day training for two members each of 20 Facility committees on MPDSR in Kogi State. • Mobilize and support SOGON members under the VOS to conduct monthly visits to project supported
health facilities to mentor medical officers, National Youth Service Corp (NYSC) doctors, midwives and CHEWS to provide quality MNH services according to set QOC standards, provide on-the-job trainings as required and submit quarterly reports to MCSP, SPHCDA and NPHCDA.
• Quarterly Review meetings for VOS volunteers with SOGON Executives and other MCSP stakeholders in Kogi and Ebonyi States.
• Quarterly meeting for dissemination of MPDSR processes at the State MPDSR committees in Kogi and Ebonyi States.
• Support the MNCH week with free antenatal services and surgical services in Kogi and Ebonyi States.

January–March 2017 www.mcsprogram.org
7.0 Annex 1: Detailed Progress Results Table
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
IR 1: Governance of health system and institutions strengthened
Sub-IR 1.1: Increased availability of EmONC and Family Planning workers
1 Number of people trained in maternal and newborn health through USG supported program
TrainSMART Ebonyi 2015 0 150 50 (41F, 9M)
65 (55F, 10M)
92% MCSP will conduct additional trainings to meet the target during the remaining quarters
Kogi 0 150 54 (42F, 12M)
108 (93F, 15M)
Total 0 300 104 (83F, 21M)
173 (148F, 25M)
2 Number of service providers trained in BEmONC through USG supported program
TrainSMART Ebonyi NA 165 125 (102F,
23M
25 (24F, 1M)
93% The commencement of the LDHF versus traditional training approaches study was responsible for this achievement.
Kogi NA 235 202 (191F, 11M)
21 (18F, 3M)
Total NA 400 327 (293F, 34M)
46 (42F, 4M)
3 Number of people trained on FP/RH with USG funds
TrainSMART Ebonyi 2015 0 120 23 (17F; 6M)
30 (29F, 1M)
55% This include service providers trained on Age and life stage counseling & interpersonal communication skills for adolescents
Kogi 0 120 20 (18F, 2M)
58 (50F, 8M)
Total 0 240 43 (35F, 8M)
88 (79F, 9M)
4 Number of people trained on HMIS
TrainSMART Ebonyi 2015 123 120 0 5 (4F, 1M)
5.4% Only the Training of Trainers has so far been conducted trainers will be training service providers in Q3
Kogi 137 120 0 8 (4F, 4M)
Total 260 240 0 13 (8F, 5M)

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
5 Number of people trained on use of data for decision making.
TrainSMART Ebonyi 2015 0 120 0 5 (4F, 1M)
5.4% The training was conducted for trainers who will be training service providers in Q3
Kogi 0 120 0 8 (4F, 4M)
Total 0 240 0 13 (8F, 5M)
6 Number of classroom tutors and preceptors trained on clinical skills through MCSP supported funds
TrainSMART Ebonyi 2015 0 16 0 24 (11F, 13M)
163% More preceptors were trained to give room for continuity when staff are on vacations
Kogi 0 10 0 18 (13F, 5M)
Total 0 26 0 42 (24F, 18M)
7 Number of people trained through USG supported program on IMCI and iCCM
HMIS Ebonyi 850 29 (16F; 13M
0 3% Training on iCCM will continue later in the year Kogi 860 24 (12F,
12M) 0
Total 1710 53 (28F, 25M)
0
Sub-IR 1.2: Improved management of maternal and newborn services
8 Number of MCSP supported health facilities that have a systematic approach to track and display priority RMNCH indicators
Checklist Ebonyi 2015 0 20 2 10 65% Percent achieved to date was calculated based on 40 HFs selected as Phase I QI facilities.
Kogi 0 20 6 8 Total 0 40 8 18
9 Number of MCSP supported facilities with an established QI team that track at least two quality of care measures on a monthly basis
Checklist Program reports
Ebonyi 2015 NA 20 2 10 65%
MCSP established 40 QI teams (20 per state) with QI ambassador appointed for all the HFs,
Kogi NA 20 6 8 Total NA 40 8 18
10 Number of supportive supervision visits conducted to MCSP supported facilities
Checklist Program reports
Ebonyi 2015 NA 80 2 19 23% MCSP is working the SMoH to use the National ISS checklist after the initial trainings late last year. Advocacy is ongoing to improve SMoH leadership
Kogi NA 80 6 10 Total NA 160 8 29

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
11 Number of referrals for complications due to pregnancy related issues in MCSP supported facilities
Record / DHIS2
Ebonyi 2015 160 250 49 8 18% Data generated from service registers from health facilities (excludes Kogi data).
Kogi 19 150 0 14 Total 179 400 49 22
12
Percent of facilities in targeted states providing comprehensive EmONC services
Facility Assessment
2015
2.4%
80%
To be measured at the end of the program implementation.
13 Number of facilities with maternal death reviews (MDR) conducted
Reports Ebonyi 2015 4 25 4 7 42.5% This was conducted in 3 secondary health facilities (2 in Ebonyi and 1 in Kogi). Data was derived from DHIS2
Kogi 2 15 3 3 Total 6 40 7 10
14 Number of clinical skills laboratories established through MCSP support
Ebonyi 2015 NA 8 0 0 0% The baseline assessment was done in this quarter. The activity is scheduled for Q3.
Kogi NA 5 0 0 Total NA 13 0 0
15 Number/percent of PPMVs that received quarterly supportive supervision
Checklist Ebonyi 2016 NA 80% 0 0 0% Training of PPMVs will commenced as soon as agreement on implementation strategy for iCCM is reached with USAID.
Kogi NA 0 0 Total NA 0 0
16 Number of grants awarded to local non-governmental institutions to advance RMNCH services
Program report
Ebonyi 2015 0 4 (National
medical associations)
4 4 100% This is cumulative achievement. MCSP continue to support the four professional associations identified at the commencement of program start off.
Kogi Total
17 Number of local partners whose capacity MCSP has
Program report
Ebonyi 2015 0 4 (National
4 4 100% This is cumulative achievement. MCSP Kogi

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
built Total continue to support the four professional associations identified at the commencement of program start off.
Sub-IR 1.3: Effective policy, program learning and accountability for strengthening MNH fostered
18 Number of articles submitted for publication in peer reviewed journals
Program report
Ebonyi 2015 0 1 0 0 0% Most of the learning agenda are still ongoing
Kogi Total
19 Number of technical reports / papers, policy / research / program briefs and fact sheets produced and disseminated
Program report
Ebonyi 2015 0 5 4 1 100% During the reporting period a program brief on ASRH was produced
Kogi Total
IR2: Demand for quality primary health care services increased
Sub IR2.1: Increased availability of EmONC and FP services in selected LGAs
20 Number of first antenatal (ANC) visits supervised by skilled providers from USG assisted facilities
HMIS / DHIS2
Ebonyi 2015 77,946 55,000 8,973 10,728 36% Data derived from the National DHIS2 platform
Kogi 26,230 35,000 6,822 6,048 Total 104,176 90,000 15,795 16,776
21 Number of pregnant women that attended antenatal clinic for the 4th visit
HMIS / DHIS2
Ebonyi 2015 9,875 20,000 5,827 2,407 39% Kogi 10,662 10,000 1,767 1,612 Total 20,537 30,000 7,594 4,019
22 Number of deliveries with a Skilled Birth Attendants
HMIS / DHIS2
Ebonyi 2015 6,786 12,000 3,034 2,765 44% MCSP is on track to meet this target by the end of the year.
Kogi 3,113 8,000 1,758 1,247 Total 9,899 20,000 4,792 4,012
23 Number of deliveries in MCSP supported health facilities
HMIS / DHIS2
Ebonyi 2015 12,426 15,000 4,235 3,160 51% MCSP is on track to meet this target by the end of the year.
Kogi 2015 3,456 10,000 2,941 2,504 Total 2015 15,882 25,000 7,176 5,664
24 Number of Live births in MCSP supported health facilities
HMIS / DHIS2
Ebonyi Kogi
2015 NA 14,000 3,547 3,012 49% MCSP is on track to attain this target for this indicator. Kogi NA 10,000 2,745 2,452
Total NA 24,000 6,292 5,464

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
25 Number of stillbirths in MCSP supported health facilities
HMIS / DHIS2
Ebonyi 2015 NA 400 102 139 36.6% Facility stillbirth rate in MCSP supported health facilities during the reporting period was 38/1,000 based on number of livebirths in the facilities 207/5,464*1,000
Kogi NA 600 57 68 Total NA 1,000 159 207
26 Percent of C-sections performed in CEmONC facilities
HMIS / DHIS2
Ebonyi 2015 3% 5–15% 453/1693
(26.7%)
452/1,541
(29.3%)
23% The high CS rate reported which is above the globally acceptable rate of 5-15% is an indication that most women only go to the health facility when they have a life-threatening complication necessitating abdominal delivery
Kogi 3% 5–15% 332/1,758
(19%)
429/1,208
(36%)
Total 3% 5–15% 785/3,451
(23%)
881/2,749
(33%)
27 Number of Post-Natal attendees in USG supported programs
DHIS2 Ebonyi 2016 7,024 9,000 2,283 1,522 43% MCSP is on track to meet this target Kogi 2016 1,021 3,000 625 680
Total 2016 8045 12,000 2,908 2,202 28 Percent of women
who delivered in a facility that received contraception post-partum pre-discharge
HMIS / DHIS2
Ebonyi 2015 NA 15% 70/3,257 (2%)
114/2,286
(5%)
9% Calculation for this indicator was based only on total delivery in health facilities where service providers have been trained on PPFP
Kogi NA 15% 158/2368 (7%)
492/1,374
(36%)
Total NA 15% 228/5,625 (4%)
606/3,660
(17%)
29 Couples year of protection in USG supported programs
HMIS / DHIS2
Ebonyi 2015 2,300 8,000 3,860 2,702 119% MCSP achieved the target set form this indicator
Kogi 12,504 11,000 7,362 8,735 Total 14,804 19,000 11,222 11,437
30 Number post-partum HMIS / Ebonyi 2015 NA 7,000 2,522 2,195 84% MCSP is on track to

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
counselling visits for FP/RH as a results of USG
DHIS2 Kogi NA 5,000 1,826 3,517 meet this target
Total NA 12,000 4,348 5,712 31 Percent of USG
supported SDPs providing FP counseling/services
HMIS / DHIS2
Ebonyi 2015 86% 90 (75%) 107/119 (90%)
107/119 (90%)
108% Target set for this indicator already achieved Kogi 64% 90 (75%) 89/121
(76%) 89/121(
76%)
Total 75% 180 (75%) 196/240 (82%)
196/240 (82%)
32 Number of children under five referred to a high level health facility by PPMVs for treatment of severe diarrhea, pneumonia and malaria or danger signs in USG (MCSP) supported programs
DHIS2 Ebonyi 2016 NA 1,674 0 0 0% PPMVs training will be held in Quarter 3 Kogi 2016 NA 1,458 0 0
Total 2016 NA 3,132 0 0
33 Percent of confirmed malaria cases in children aged 0-59 months that received first line anti-malarial treatment (ACT)
DHIS2 Ebonyi 2016 NA 65% 124/124100%
1964/4801
(41%)
75% Data generated from DHIS2
Kogi 2016 NA 65% 766/766100-%
1300/1754
(74%)
Total 2016 NA 65% 100% 3264/6555
(50%)
IR3: Access to quality service improved
Sub-IR 3.1: Facility-based MNH improved
34 Number/percent of women receiving immediate post- partum Uterotonic in the third stage of labor
Reports / Data extraction form
Ebonyi 2015 NA 10,000 2,489/4,235
(59%)
2,629/3,160
(83%)
53% MCSP is on track to meet target for this indicator
Kogi NA 8,000 1,994/2,941
(68%)
2,404/2,505
(96%)
Total NA 18,000 4,483/7,176
(62%)
5,033/5,665
(89%)

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
35 Percent women admitted with eclampsia who received magnesium Sulphate
HMIS / DHIS2
Ebonyi 2015 NA 70% 9/9 (100%)
3/3 (100%)
100% Target achieved so far
Kogi NA 70% 0 5/5 (100)
Total NA 70% 9/9 (100%
8/8 (100%)
36 Percent of newborns receiving essential care through USG supported programs
HMIS / DHIS2
Ebonyi 2015 65% 80% 1,577/3,547
(44%)
2,327/3,012
(77%)
67% MCSP is on track to meet this target by the end of the year
Kogi 34% 80% 2,113/2,745
(77%)
2451/3335
(73%)
Total 51% 80% 3,690/6,292
(59%)
4,778/6,347
(75%)
37 Percent of babies for whom Chlorhexidine was applied to the umbilical cord at birth
L&D Register
Ebonyi 2015 NA 25% 257/2,861 (9%)
487/3,012
(16%)
37% Procurement and distribution of CHX gel to health facilities particularly through the Government of Kogi state and improved record keeping system contributed to the level of achievement so far
Kogi NA 25% 1,386/2,177
(64%)
1,725/2,452
(70%)
Total NA 25% 1,643/5,038
(33%)
2,212/5,464
(40%)
38 Percent of births monitored with a Partograph in the past quarter
HMIS / DHIS2
Ebonyi 2015 21.5% 45% 2,005/4,235
(47%)
1,139/3,160
(36%)
33% MCSP will prioritize on-the-job training on use of the Partograph in the next quarter
Kogi 38.4% 45% 675/2,941
(30%)
361/2,504
(14%)
Total 29.1% 45% 2,680/7,176
(37%)
1,500/5,664
(26%)
39 Percent of targeted health facilities with appropriate
Facility survey
Ebonyi 2015 40% 80% This indicator will be measured and Kogi 25% 80%

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
hand washing supplies in the delivery room in MCSP supported areas
Total 26.4% 80% reported at the end of the program.
40 Percent of newborns identified as having neonatal sepsis or PSBI treated in MCSP supported facilities
HMIS / DHIS2
Ebonyi 2015 NA 75% PSBI intervention is yet to commence. MCSP is working with the National HMIS unit of the FMoH and other implementing partners to institutionalize the process of capturing PSBI indicators in health facilities
Kogi NA 75% Total NA 75%
41 Percent of livebirths put to breast and kept warm within 30 minutes of birth in a health facility
HMIS / DHIS2
Ebonyi 2015 NA 70% 1,897/3,547
(53%)
2,396/3,012
(79.5%)
73% MCSP is on track to meet this indicator.
Kogi 2015 NA 7%0 1,918/2,750
(70%)
2,393/2,452
(97%)
70% 3,815/6,297
(61%)
4,789/5,464
(88%)
42 Percentage of MCSP supported facilities with functional newborn care corner established
Facility Survey
Ebonyi 2015 0 60% 30 (51%)
54% Calculation was based on the initial 120 first phase MCSP supported health facilities. Presently 65 facilities in both states (30 in Ebonyi and 35 in Kogi are equipped with newborn corners, Although, this indicator will be measured and reported at the end of the program.
Kogi 0 60% 35 (57%)
Total 0 60% 65 (54%)
43 Number of livebirth L&D Ebonyi 2015 NA 300 159 161 43% Data collected only

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
not breathing Register Kogi 2015 NA 200 57 42 from facilities MCSP provided with equipment.
Total 2015 NA 500 216 202
44 Number of Newborn not breathing at birth who were resuscitated in USG supported programs
L&D Register
Ebonyi 2015 NA 275 155 156 (97%
successfully
resuscitated)
95% of the babies not breathing at birth were successfully resuscitated
Data collected only from facilities MCSP provided with equipment.
Kogi 2015 NA 175 56 37 (95% successf
ully resuscit
ated)
Total 2015 NA 450 (90%) 211 193 45 Number of MCSP
supported facilities implementing KMC
DHIS2 / Program report
Ebonyi 2015 7 14 7 8 44% MCSP is on track to achieve this target at the end of the reporting year
Kogi 9 18 6 11 Total 16 32 13 19
46 Percent of LBW newborns admitted to facility-based KMC at MCSP supported facilities
HMIS Ebonyi 2015 NA 60% 19/27 (70%)
34/171 (20%)
73% MCSP is on track surpassing this target by end of reporting year.
Kogi NA 60% 24/32 (75%)
38/49 (97%)
Total NA 60% 43/59 (73%)
72/220 (33%)
47 Facility based Maternal Mortality Ratio
DHIS2 Ebonyi 2015 144 520/100,000 This will be measured and reported at the end of PY 3.
Kogi 256 Total 187
48 Facility Neo-natal Mortality Rate
DHIS2 Ebonyi 2015 NA 175/1,000 This will be measured and reported at the end of PY 3.
Kogi NA Total NA
49 Number of pregnant women attending ANC who received second -dose of Intermittent Preventive Treatment (IPT1) under direct
DHIS2 Ebonyi 2015 20,738 17,000 6,989/8,973
(78%)
7,966/10,728 (74%)
78% MCSP is on track to achieve this target at the end of the reporting year Kogi 5,984 13,000 4,132/6,
822 (61%)
4,434/6,048
(73%)

MCSP Nigeria Quarterly Report: Jan–Mar 2017 (PY3 Q2)
Performance Indicator Data Source State
PY 3 Quarters 1-4 Annual
Performance Achieved to
Date (%)
Notes and Comments
Baseline Data FY 2017 Quarterly Status: FY 2017
Year Value Annual Planned Target
Annual Actual Q1 Q2 Q3 Q4
observation Total 26,722 30,000 11,121/15,795 (70%)
12,400/16,776 (74%)
50 Number of pregnant women attending ANC who received second -dose of Intermittent Preventive Treatment (IPT2) under direct observation
DHIS2 Ebonyi 2015 17,119 13,600 5,694/8,973
(63%)
5740/10,728
(53.3%)
79% MCSP is on track to achieve this target at the end of the reporting year Kogi 4,830 6,400 2,553/6,
822 (37%)
1,899/6,048
(31.3%)
Total 21,949 20,000 8,247/15,795 (52%)
7,639/16,776 (46%)
51 Number/Percent of pregnant women who received at least 2 doses of Tetanus Toxoid (TT2)
DHIS2 Ebonyi 2015 14,304 15,800 6,256 3,441 68% MCSP is on track to achieve this target at the end of the reporting year
Kogi 3,815 4,200 1,953 1,978 Total 18,119 20,000 8,209 5,419
52 Number of cases of child diarrhea treated in USAID assisted program
DHIS2 Ebonyi 2016 NA 10,013 817 299 11% Data generated from DHIS2. Kogi NA 2,764 94 173
Total NA 12,777 911 472 53 Number of cases of child
pneumonia treated with antibiotics by trained facility workers or PPMVs in USG supported programs
DHIS2 Ebonyi 2016 NA 2,535 610 65 44% Data from health facilities only and generated from DHIS2. MCSP is on track to achieve this target at the end of the reporting year
Kogi NA 1,008 459 418 Total NA 3,543 1,069 483
54 Percent of women who are satisfied with their experience of care during child birth in selected MCSP supported facilities
Exit interview
Ebonyi 2015 NA 45% Data on this indicator will be reported biannually
Kogi NA 45% Total NA 45%