mechanical ventilation & cardiopulmonary interactions deborah franzon, md pediatric critical...
Post on 22-Dec-2015
217 views
TRANSCRIPT
Mechanical ventilation &Cardiopulmonary Interactions
Mechanical ventilation &Cardiopulmonary Interactions
Deborah Franzon, MDPediatric Critical Care
Lucille Packard Children’s Hospital
Deborah Franzon, MDPediatric Critical Care
Lucille Packard Children’s Hospital

OverviewOverview
Review modes of mechanical ventilationCardiopulmonary interactionsLesion specific approachesApproach to extubation
Review modes of mechanical ventilationCardiopulmonary interactionsLesion specific approachesApproach to extubation
Overview of anatomy and respiratory physiology
Overview of anatomy and respiratory physiology

AnatomyAnatomy
Infant vs adult airways Anterior and cephalad Floppy U-shaped
epiglottis Subglottic area
narrowest Increased resistance
Poiseulle’s Law R = 1/r4) Compliant chest wall Increased VO2 (8ml/kg)
Infant vs adult airways Anterior and cephalad Floppy U-shaped
epiglottis Subglottic area
narrowest Increased resistance
Poiseulle’s Law R = 1/r4) Compliant chest wall Increased VO2 (8ml/kg)
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Mechanics of ventilationMechanics of ventilation
Inspiration Active contraction of diaphragm and
intercostal muscles Generate negative intrathoracic pressure
Expiration Passive chest wall relaxation Passive lung recoil
Inspiration Active contraction of diaphragm and
intercostal muscles Generate negative intrathoracic pressure
Expiration Passive chest wall relaxation Passive lung recoil

Respiratory failureRespiratory failure
1. Compliant chest cavity limits ability to increase gas exchange
2. Increased WOB3. Increased VO24. V/Q mismatch ensues5. Indication for assisted ventilation
1. Compliant chest cavity limits ability to increase gas exchange
2. Increased WOB3. Increased VO24. V/Q mismatch ensues5. Indication for assisted ventilation
Mechanical ventilationMechanical ventilation
Oxygenation Determined by inspired oxygen and sufficient
mean airway pressure FIO2 PIP, PEEP, i-time, flow
Carbon dioxide removal Determined by (Minute ventilation - dead
space ventilation)= alveolar ventilation Rate, TV
Oxygenation Determined by inspired oxygen and sufficient
mean airway pressure FIO2 PIP, PEEP, i-time, flow
Carbon dioxide removal Determined by (Minute ventilation - dead
space ventilation)= alveolar ventilation Rate, TV
Ventilatory supportVentilatory support
Assisted breaths determined by
Trigger: time, flow, pressureCycle: time cycled breathsLimit--volume or pressure
Assisted breaths determined by
Trigger: time, flow, pressureCycle: time cycled breathsLimit--volume or pressure
Modes of VentilationModes of Ventilation
Volume-limited(SIMV) Constant flow during inspiration Square flow wave pattern Set parameters: TV, rate, PEEP, i-time PIP--dependent variable Fixed minute ventilation
Paco2 and pH remain stable
Volume-limited(SIMV) Constant flow during inspiration Square flow wave pattern Set parameters: TV, rate, PEEP, i-time PIP--dependent variable Fixed minute ventilation
Paco2 and pH remain stable
SIMV ModeSIMV Mode
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Mechanical breath Spontaneous
breath

Modes of ventilationModes of ventilation
Pressure Limited (A/C) Set parameter: PIP, PEEP, rate, IT Pressure constant throughout Tidal volume dependent variable Decelerating flow pattern Lung compliance and airway resistance
determine gas delivery Theoretically less barotrauma
Pressure Limited (A/C) Set parameter: PIP, PEEP, rate, IT Pressure constant throughout Tidal volume dependent variable Decelerating flow pattern Lung compliance and airway resistance
determine gas delivery Theoretically less barotrauma
Volume control: flow and pressure graphs
Volume control: flow and pressure graphs
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Modes of ventilationModes of ventilation
Pressure support ventilation
Decelerating inspiratory flow Patient triggers breath Constant pressure delivered Better patient-ventilator synchrony Used with volume or pressure mode or
weaning mode
Pressure support ventilation
Decelerating inspiratory flow Patient triggers breath Constant pressure delivered Better patient-ventilator synchrony Used with volume or pressure mode or
weaning mode
SIMV + Pressure SupportSIMV + Pressure Support
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Mechanical breath
Spontaneous breath
Pressure Regulated + Volume Control (PRVC)/APV
Pressure Regulated + Volume Control (PRVC)/APV
Pressure limitedTidal volume targetedDecelerating flow waveformAchieve TV goals without barotrauma,
mean airway pressure maintained
Pressure limitedTidal volume targetedDecelerating flow waveformAchieve TV goals without barotrauma,
mean airway pressure maintained
Initial ventilator settingsInitial ventilator settings
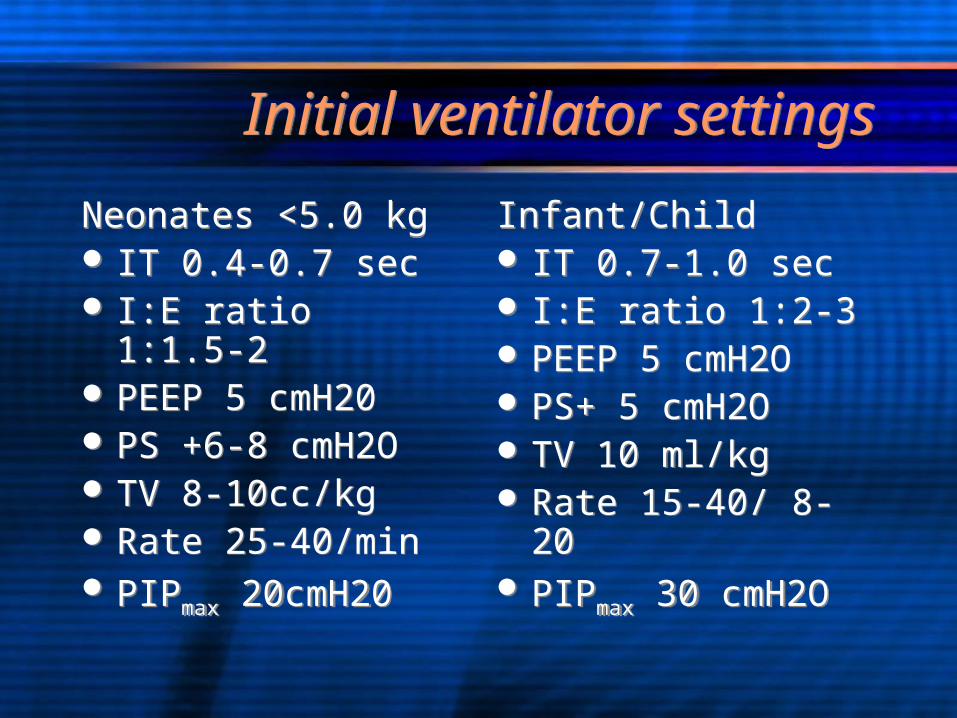
Neonates <5.0 kg IT 0.4-0.7 sec I:E ratio 1:1.5-2 PEEP 5 cmH20 PS +6-8 cmH2O TV 8-10cc/kg Rate 25-40/min PIPmax 20cmH20
Neonates <5.0 kg IT 0.4-0.7 sec I:E ratio 1:1.5-2 PEEP 5 cmH20 PS +6-8 cmH2O TV 8-10cc/kg Rate 25-40/min PIPmax 20cmH20
Infant/Child IT 0.7-1.0 sec I:E ratio 1:2-3 PEEP 5 cmH2O PS+ 5 cmH2O TV 10 ml/kg Rate 15-40/ 8-20 PIPmax 30 cmH2O
Infant/Child IT 0.7-1.0 sec I:E ratio 1:2-3 PEEP 5 cmH2O PS+ 5 cmH2O TV 10 ml/kg Rate 15-40/ 8-20 PIPmax 30 cmH2O
Pressure Volume LoopPressure Volume Loop
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.

Flow Volume LoopFlow Volume Loop
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
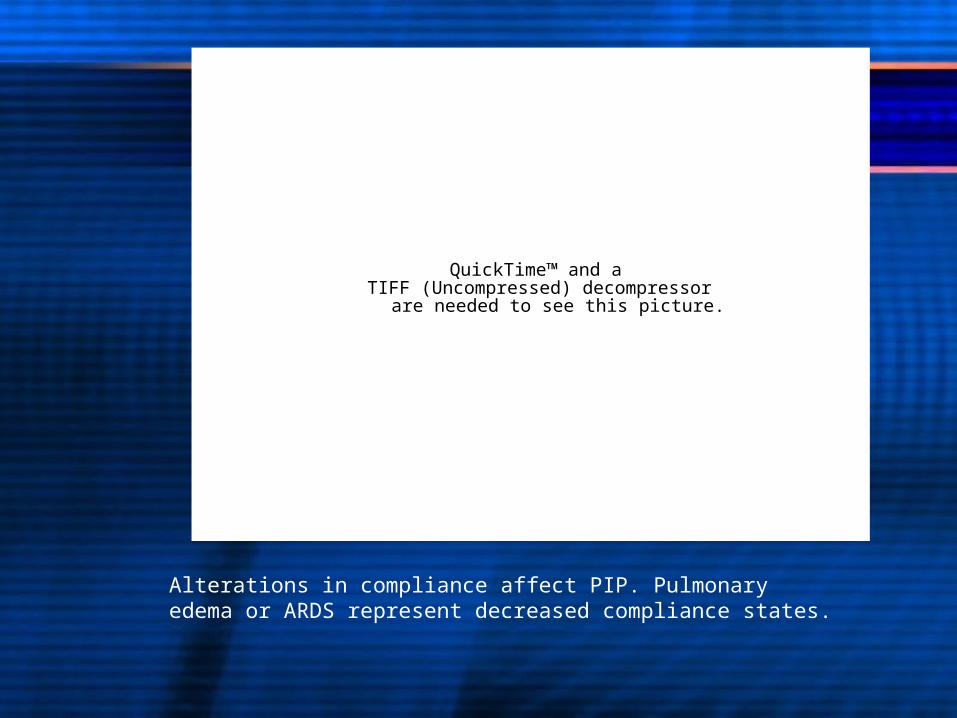
Interpreting pressure/volume loops
Interpreting pressure/volume loops
Effect of PEEPIncreased resistanceAltered complianceOverdistensionAir leak
Effect of PEEPIncreased resistanceAltered complianceOverdistensionAir leak
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
PEEP is ideally set at the point of lower inflection point on normal Volume-Pressure curve--shifting entire curve rightward
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
As resistance increases PIP increase (A to B)--Hysteresis refers to abnormal widening of PV loop
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Alterations in compliance affect PIP. Pulmonary edema or ARDS represent decreased compliance states.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
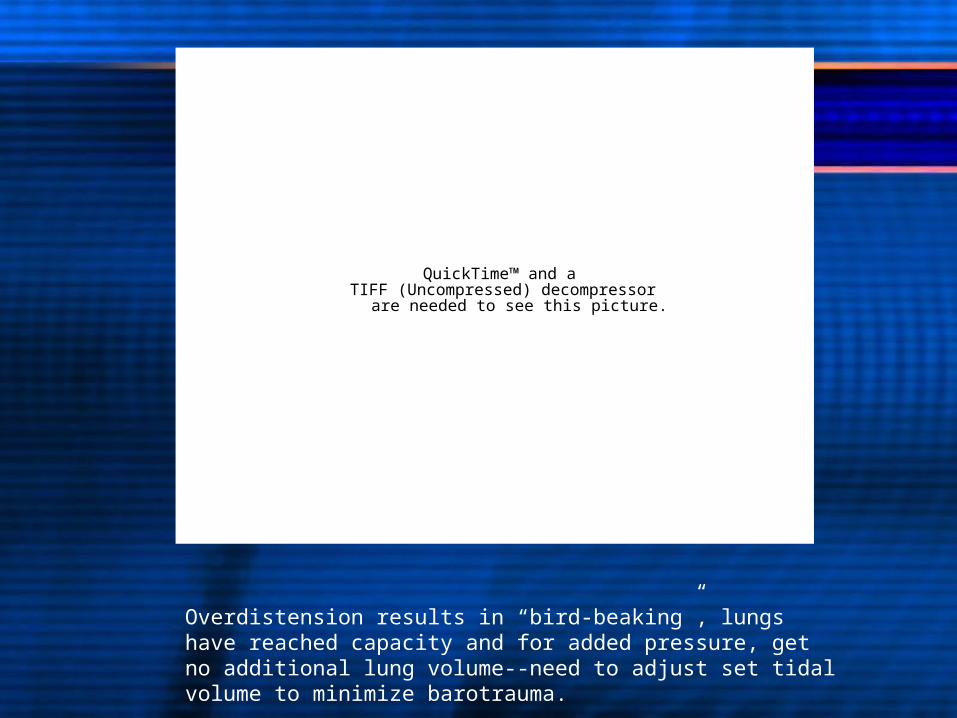
Overdistension results in “bird-beaking”, lungs have reached capacity and for added pressure, get no additional lung volume--need to adjust set tidal volume to minimize barotrauma.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
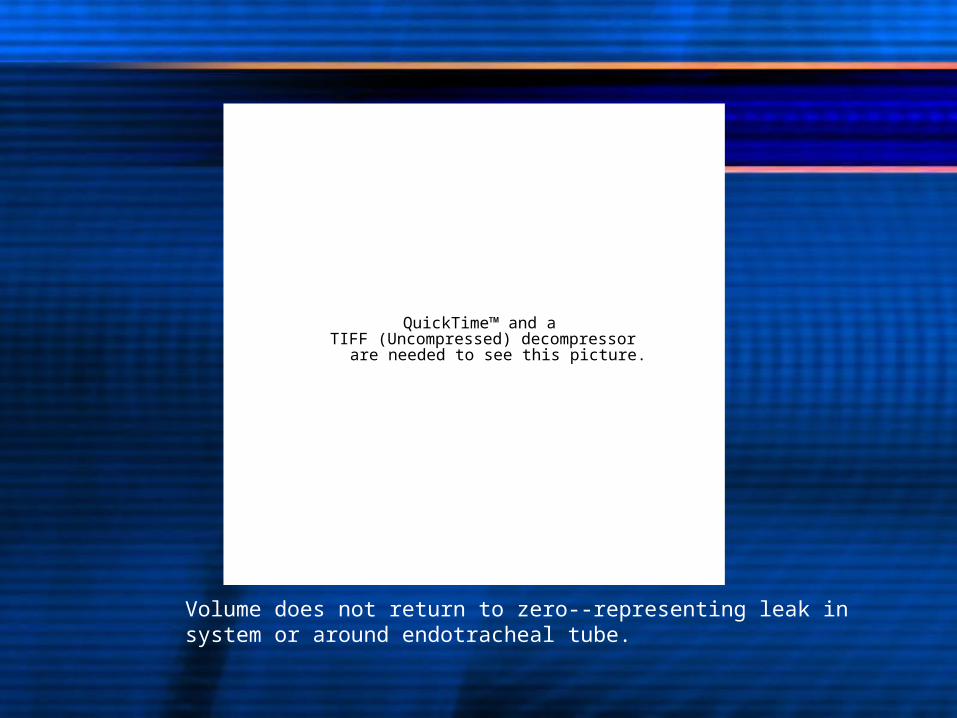
Volume does not return to zero--representing leak in system or around endotracheal tube.
High Frequency Oscillatory Ventilation
High Frequency Oscillatory Ventilation
Pistons generate frequencies of 60-3600 cpm
Tidal volumes 1-3ml/kgTidal volumes are less than dead spaceGas exchange via diffusion, convection,
penduluft and cardiogenic oscillationsSinusoidal waveformGenerally decreases oxygenation index
Pistons generate frequencies of 60-3600 cpm
Tidal volumes 1-3ml/kgTidal volumes are less than dead spaceGas exchange via diffusion, convection,
penduluft and cardiogenic oscillationsSinusoidal waveformGenerally decreases oxygenation index
HFOVHFOV
Settings: FIO2 Frequency (Hz)-- affected by patient size
and ventilatory goals Mean airway pressure--2-5mmHg higher
than on conventional ventilation Amplitude (∆P)--necessary to provide
sufficient “jiggle”
Settings: FIO2 Frequency (Hz)-- affected by patient size
and ventilatory goals Mean airway pressure--2-5mmHg higher
than on conventional ventilation Amplitude (∆P)--necessary to provide
sufficient “jiggle”

Cardiopulmonary interactionsCardiopulmonary interactions
Effects of mechanical ventilation
Effects of mechanical ventilation
Alteration of lung volumeChanges in ITP (intrathoracic pressure)Altered acid-base balanceAltered PaO2Changes in neurohormonal activity
All can affect cardiac function
Alteration of lung volumeChanges in ITP (intrathoracic pressure)Altered acid-base balanceAltered PaO2Changes in neurohormonal activity
All can affect cardiac function

Intrathoracic pressure changes
Intrathoracic pressure changes
Venous return affects RV preloadPressure gradient between CVP and
PRA
Respiratory induced changes in ITP directly effect PRA
Venous return affects RV preloadPressure gradient between CVP and
PRA
Respiratory induced changes in ITP directly effect PRA
Venous return and RV preloadVenous return and RV preload
Spontaneous inspiration PRA falls, CVP constant, intra-abdominal
pressure increases Increased pressure gradient increases VR As PRA approaches zero venous return
maximized
Spontaneous inspiration PRA falls, CVP constant, intra-abdominal
pressure increases Increased pressure gradient increases VR As PRA approaches zero venous return
maximized
Venous return and RV preloadVenous return and RV preload
Positive pressure ventilation Inhibits venous return to RA ITP (+), decreases gradient between PRA
and mean CVP, RV filling falls More pronounced in low output state
Positive pressure ventilation Inhibits venous return to RA ITP (+), decreases gradient between PRA
and mean CVP, RV filling falls More pronounced in low output state
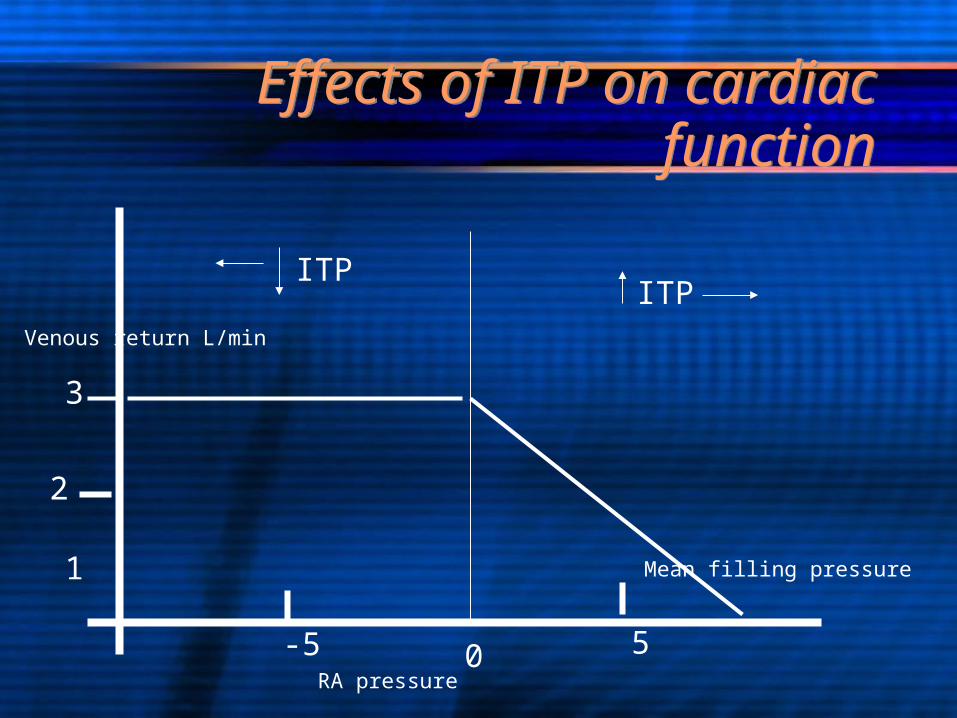
Effects of ITP on cardiac function
Effects of ITP on cardiac function
0
3
2
1
Venous return L/min
-5 5RA pressure
ITPITP
Mean filling pressure
Effect of PEEP on RV preloadEffect of PEEP on RV preload
Increases intrathoracic pressureIncreases intrathoracic volumeDiaphragm descendsIncreases both CVP and PRA
Venour return shifts to right
RV preload decreased
Increases intrathoracic pressureIncreases intrathoracic volumeDiaphragm descendsIncreases both CVP and PRA
Venour return shifts to right
RV preload decreased
LV PreloadLV Preload
Spontaneous Inspiration RV volume increases Intraventricular septum shifts leftward LV compliance and filling fall “Ventricular interdependence”
Spontaneous Inspiration RV volume increases Intraventricular septum shifts leftward LV compliance and filling fall “Ventricular interdependence”

LV PreloadLV Preload
Positive pressure ventilation Decreased VR--decreased LV filling Decreased RV volume--increased LV
compliance Increased lung volume--restricted LV filling
Positive pressure ventilation Decreased VR--decreased LV filling Decreased RV volume--increased LV
compliance Increased lung volume--restricted LV filling

LV afterloadLV afterload
Function of LV transmural pressure(SBP-Ppl)
Spontaneous inspiration Intrathoracic pressure falls and SBP
unchanged and afterload increases
Positive pressure inspiration intrathoracic pressure increases and
afterload decreases
Function of LV transmural pressure(SBP-Ppl)
Spontaneous inspiration Intrathoracic pressure falls and SBP
unchanged and afterload increases
Positive pressure inspiration intrathoracic pressure increases and
afterload decreases
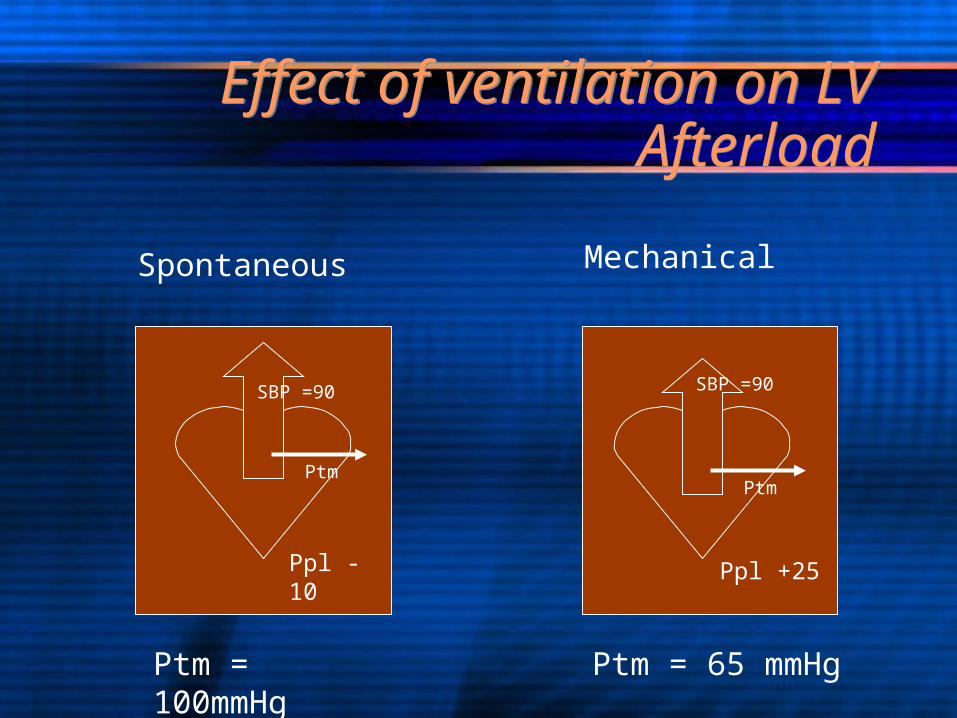
Effect of ventilation on LV Afterload
Effect of ventilation on LV Afterload
SBP =90 SBP =90
Ptm = 100mmHg Ptm = 65 mmHg
PtmPtm
Ppl -10 Ppl +25
Spontaneous Mechanical
RV AfterloadRV Afterload
Determined by Pulmonary vascular resistance (PVR)
PVR affected by lung volume via Passive compression of pulmonary vessels Hypoxic vasoconstriction
Determined by Pulmonary vascular resistance (PVR)
PVR affected by lung volume via Passive compression of pulmonary vessels Hypoxic vasoconstriction
Pulmonary vascular resistance & functional residual capacity
Pulmonary vascular resistance & functional residual capacity
PVR lowest at FRC Below FRC (atelectasis) = PVR
Extra-alveolar vessels collapse Terminal airways close--alveoli collapse--
hypoxia--Above FRC (hyperinflation) =PVR
Intralveolar vessels compressed
PVR lowest at FRC Below FRC (atelectasis) = PVR
Extra-alveolar vessels collapse Terminal airways close--alveoli collapse--
hypoxia--Above FRC (hyperinflation) =PVR
Intralveolar vessels compressed

Lung volume and PVRLung volume and PVR
Intra-alveolar vessel resistance
Total PVR
Extra-alveolar vessel resistantceFRC
Pressure
Volume
Mechanical ventilation PVRMechanical ventilation PVR
Decrease PVR Hyperventilate Alkalosis PEEP FIO2
Decrease PVR Hyperventilate Alkalosis PEEP FIO2
Increase PVR Acidosis Hypoventilation Hyperinflation/
overdistension
Increase PVR Acidosis Hypoventilation Hyperinflation/
overdistension
Lesion specific approach to mechanical ventilationLesion specific approach to mechanical ventilation
Left-to-right shuntsLeft-to-right shunts
Increasd PBFCompression of large airways can occur
due to enlarged LA and PasTOF/PA/MAPCAS--compression of
intrapulmonary bronchi by abnormal vessels Atelectasis, wheezing, poor gas exchange
Increasd PBFCompression of large airways can occur
due to enlarged LA and PasTOF/PA/MAPCAS--compression of
intrapulmonary bronchi by abnormal vessels Atelectasis, wheezing, poor gas exchange

Left-to-right shuntsLeft-to-right shunts
Bronchiolar narrowing from high flows and venous pressure
Causes pulmonary edemaIncreased PBF associated with
decreased FEV25-75%
Prominent smooth muscle narrowing seen
Bronchiolar narrowing from high flows and venous pressure
Causes pulmonary edemaIncreased PBF associated with
decreased FEV25-75%
Prominent smooth muscle narrowing seen

Single ventricle lesions: s/p Stage I Norwood
Single ventricle lesions: s/p Stage I Norwood
Goal of balancing Qp:Qs Maneuvers to increase/decrease PVR Optimize Pulmonary Blood Flow?
Hyperventilation Alkalosis Increased Fio2 Inhaled nitric oxide
Optimize cardiac output? Mild respiratory acidosis Hypoventilation Lower Fio2
Goal of balancing Qp:Qs Maneuvers to increase/decrease PVR Optimize Pulmonary Blood Flow?
Hyperventilation Alkalosis Increased Fio2 Inhaled nitric oxide
Optimize cardiac output? Mild respiratory acidosis Hypoventilation Lower Fio2
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Bidirectional Glenn--Stage IIBidirectional Glenn--Stage II
Hypoventilation improves oxygenation after bidirectional superior cavopulmonary connection.
Bradley SM, Simsic JM, Mulvihill DM.J Thorac Cardiovasc Surg. 2003 Oct;126(4):1033-9.
The effects of carbon dioxide on oxygenation and systemic, cerebral, and pulmonary vascular hemodynamics after the bidirectional superior cavopulmonary anastomosis.
Hoskote A, Li J, Hickey C, Erickson S, Van Arsdell G, Stephens D, Holtby
H, Bohn D, AdatiaJ Am Coll Cardiol. 2004 Oct 6;44(7):1501-9. I.
Hypoventilation improves oxygenation after bidirectional superior cavopulmonary connection.
Bradley SM, Simsic JM, Mulvihill DM.J Thorac Cardiovasc Surg. 2003 Oct;126(4):1033-9.
The effects of carbon dioxide on oxygenation and systemic, cerebral, and pulmonary vascular hemodynamics after the bidirectional superior cavopulmonary anastomosis.
Hoskote A, Li J, Hickey C, Erickson S, Van Arsdell G, Stephens D, Holtby
H, Bohn D, AdatiaJ Am Coll Cardiol. 2004 Oct 6;44(7):1501-9. I.
QuickTime™ and aTIFF (Uncompressed) decompressor
are needed to see this picture.
Bidirectional GlennBidirectional Glenn
Increased PCO2 (45-55 mmHg range)Permissive hypercarbia improves
systemic oxygenationImproves QsLittle effect on PVR
Increased PCO2 (45-55 mmHg range)Permissive hypercarbia improves
systemic oxygenationImproves QsLittle effect on PVR
Single ventricle: FontanSingle ventricle: Fontan
Venous return = PBF is “passive”Minimize positive pressure ventilation
and PEEPSpontaneous ventilation idealEarly extubationAdequately volume load ptSlow rate, adequate tidal volume
Venous return = PBF is “passive”Minimize positive pressure ventilation
and PEEPSpontaneous ventilation idealEarly extubationAdequately volume load ptSlow rate, adequate tidal volume
ExtubationExtubation
Ideal setting for post-op CVICU patientHemostasisOptimal cardiac outputStable hemodynamicsAppropriate mental statusNormothermia
Ideal setting for post-op CVICU patientHemostasisOptimal cardiac outputStable hemodynamicsAppropriate mental statusNormothermia
How to wean ventilator is variable:
dictated by practice style
How to wean ventilator is variable:
dictated by practice style
What are “extubatable” settings
What are “extubatable” settings
FIO2 < 0.4 with satisfactory PaO2 PEEP < 5.0 cm H2O pH > 7.35 PCO2 < 45 -50 mmHg Spontaneous TV 5-7ml/kg on PS <8 No significant grunting/flaring/ retracting on
CPAP or low rate Mechanical VT/spontaneous TV <0.4 NIF -20-30 cm H20
FIO2 < 0.4 with satisfactory PaO2 PEEP < 5.0 cm H2O pH > 7.35 PCO2 < 45 -50 mmHg Spontaneous TV 5-7ml/kg on PS <8 No significant grunting/flaring/ retracting on
CPAP or low rate Mechanical VT/spontaneous TV <0.4 NIF -20-30 cm H20
Extubation criteria (cont’d)Extubation criteria (cont’d)
Sinus rhythm or stably pacedOptimal perfusion and filling pressuresAdequate cardiac outputMinimal inotropic supportConsciousNo residual paralysisMinimal sedative within 2-4 hrsOptimal hematocrit
Sinus rhythm or stably pacedOptimal perfusion and filling pressuresAdequate cardiac outputMinimal inotropic supportConsciousNo residual paralysisMinimal sedative within 2-4 hrsOptimal hematocrit
Predictors of extubation success
Predictors of extubation success
Spontaneous breathing trial predicts successful extubation in infants and children.
Chavez A, dela Cruz R, Zaritsky A.Pediatr Crit Care Med. 2006 Jul;7(4):324-8.
Successful completion of the SBT has a 95% sensitivity for predicting successful extubation with a positive predictive value of 92% and an odds ratio of 12 (95% confidence interval, 1.3, 53.7)
Spontaneous breathing trial predicts successful extubation in infants and children.
Chavez A, dela Cruz R, Zaritsky A.Pediatr Crit Care Med. 2006 Jul;7(4):324-8.
Successful completion of the SBT has a 95% sensitivity for predicting successful extubation with a positive predictive value of 92% and an odds ratio of 12 (95% confidence interval, 1.3, 53.7)
Reasons why patients failReasons why patients fail
Pulmonary processes Effusions, pneumonia, atelectasis Diaphragm or vocal cord paralysis Airway obstruction, RAD
Cardiac reasons Residual anatomic leasion Poor function/low output
Neurologic reasons Oversedation, weakness CNS event--hypoxic ischemic encephalopathy,
intracranial hemorrhage.
Pulmonary processes Effusions, pneumonia, atelectasis Diaphragm or vocal cord paralysis Airway obstruction, RAD
Cardiac reasons Residual anatomic leasion Poor function/low output
Neurologic reasons Oversedation, weakness CNS event--hypoxic ischemic encephalopathy,
intracranial hemorrhage.