medical school course handbook - · pdf filereview of all assessments by external examiners is...
TRANSCRIPT

Medical SchoolCourse Handbook
A100, A101, A300, A10S, A104
2010/2011

Medicine Course Handbook 2010/11 2
CONTENTS
Welcome
Course Information
Clinical Placements
Examinations
Alternative Assessment Arrangements
Regulations for the Degree of Bachelor of Medical Sciences,Bachelor of Science (Medical Sciences) and theDegree of Bachelor of Medicine & Bachelor of Surgery
Bachelor of Medical Sciences Progression in Years 1 & 2
Bachelor of Science (Medical Sciences) Progression in Years 1 & 2
Summative Assessment for GEM
The Nottingham Medical Map
Student Conduct, Concern Form and Whistleblowing Policy
Course Co ordinators for the five year course
Module Convenors and Contact Details for the GEM (A101) Course
Pastoral Care
Introduction to Pastoral Care
Overview of Pastoral Support
Pastoral Support Pathway
The Medical Family
Tutorials/Table 2
Resources for Medical Students
Further Contacts for Support and Guidance

Medicine Course Handbook 2010/11 3
Dear Colleague
Keep this booklet in a safe place where you can get at it easily.
This is your information source covering important aspects of the Medical Course - our coursehandbook.
The specific day-to-day timetables and schedules for each phase of the course will be handed out asstudents start each phase.
The handbook covers both the BMedSci phase as well as the GEM phase - and I hope you find ituseful to know what each phase is exposed to - until the groups merge in year 3 for a commonteaching programme.
Student support and guidance is central to life as a medical student in Nottingham. This handbookcontains the important information which will guide you through how things work and who to contactwhen you have a question
While much of the content is written for reference rather than memory - you do need to read it atleast once:
* Overview of the course and the curriculum, including how theexaminations system works.
* Key contacts within the Faculty of Medicine and Health Sciences including moduleco-orindators
* How our pastoral support and tutor systems work - and where youcan expect to find help and support while on the course..
* Support in the wider University: Details of a range of pastoralsupport, both before and after qualification, are listed
One practical thing to do immediately is pay particular attention to the schedule of meetingsbetween student and tutor - read the dates, get them in your diary today, check that you areavailable and make alternative arrangements if there is a clash. The complete list of tutors and thestudents allocated to them over the five years of the course will be available at the start of term.
With best regards
Professor James LoweBMedSci BM BS DM FRCPath FHEA
Don't forget that you can also get help online in the Student Support & Guidance website for theMedical School
http://www.nottingham.ac.uk/medical-school/student_support/home.html

Medicine Course Handbook 2010/11 4
Introduction
There are two routes at Nottingham by which medical students graduate as doctors, the five yearundergraduate course (A100) and the graduate entry four year course (A101). On both courses theeducational objectives are the same, namely to acquire the knowledge, skills and behaviour to allowthe graduate to practice as a new doctor on the foundation training programme with the Bachelor ofMedicine and Bachelor of Surgery (BMBS) degrees. In addition, all students on the five year courseobtain a Bachelor of Medical Sciences (BMedSci) degree after three years.
Structure of the Medical Curriculum
Five year undergraduate course(A100)
Four year (Graduate Entry to Medicine, GEM)course(A101)
Years 1 and 2(Semesters 1-4)
o Basic Medical Sciences
o Clinical & professional development
o Some advanced biomedical science options inSemester 4 First 18 months
o Problem based learning (PBL) course
o Clinical & professional development
Year 3
Semesters 5
o Research project
o Research methodology
o Advanced biomedical science options
o Infections course
Year 3 - Semesters 6 (5yr course) & Year 2 (4yr GEM course) CLINICAL PHASE 1
Clinical practice (Medicine & Surgery) and Community follow-up project and Therapeutics.
Year 4 (5yr course) & Year 3 (4yr GEM course) CLINICAL PHASE 2
Child health, Obstetrics & Gynaecology, Psychiatry, Health Care of Elderly, Dermatology, Ophthalmology,Otorhinolaryngology, Special Study Module
Year 5 (5yr course) & Year 4 (4yr GEM course) CLINICAL PHASE 3
Advanced Clinical Experience (Medicine, Surgery, Musculoskeletal Disorders and Disability) Primary Care, SpecialStudy Module, Elective Study Period, Preparation and shadowing for Foundation Years

Medicine Course Handbook 2010/11 5
CLINICAL PLACEMENTS
For a number of years the Medical School has placed students at Trusts throughout the region. It is ofnecessity that during your Medical course you may be placed at any of our partner trusts. Theseplacements will cover hospitals, clinics and surgeries in the counties of Nottinghamshire, Derbyshire andLincolnshire. We endeavour to meet the special circumstances notified to us when placing you for theseattachments but satisfying all requests can be challenging and we expect that students will be awarethat experiencing different sites across the counties is an educational and desirable feature of yourtraining. Please bear this in mind when allocations are announced.Below you will find a map of the East Midlands. During the Clinical Phase of the course you will beallocated to various hospitals in the region.
During the Clinical Phases of your course, you should expect to go to:
The Royal Derby HospitalKingsmill Hospital, MansfieldMillbrook Hospital, MansfieldNewark Hospital, Newark on TrentLincoln County HospitalGrantham HospitalPilgrim Hospital, BostonNottingham City HospitalQueen’s Medical Centre, Nottingham

Medicine Course Handbook 2010/11 6
EXAMINATIONS

Medicine Course Handbook 2010/11 7
EXAMINATIONS - ASSESSING STUDENT PERFORMANCE AND COMPETENCE
The principles that inform our assessment strategy and policy
The University of Nottingham is committed to ensuring that methods of assessment are effective inmeasuring student attainment of intended learning outcomes and that assessment policy andpractices are effective in monitoring the validity, equity and reliability of assessment. The Universitymeets that commitment through its policies and procedures which you can review online at.[http://www.nottingham.ac.uk/quality-manual/assessment/index.htm].
The purposes of our assessments are to know whether students have achieved curricular outcomes,to help students improve their learning, and to contribute to quality assurance. Our judgementsshould be valid, reliable, objective, fair and as transparent as possible. All aspects of the assessmentprocess are managed with clear lines of communication and responsibility
Review of all assessments by external examiners is an important part of the quality assuranceprocess and contributes towards ensuring that the assessments and curriculum are credit worthy incomparison with other UK institutions.
What examination methods are used?
Based on the principles outlined above, a range of assessments are used throughout the medicineprogrammes, each of which is appropriate for testing specified learning outcomes, aligned torecognised educational understanding of the strengths and weaknesses of different forms ofassessment and their suitability to reliably assess different domains.
Both formative and summative assessments are used
Formative assessments are used to provide feedback to students, to monitor progress, toimprove their learning as well as develop skills of self-assessment. They also ensuretransparency in making sure students are familiar with assessment tasks and there are ‘nosurprises’.
A range of summative assessment tasks are used and these contribute to the process ofcertification (Pass/Fail decisions) as well providing feedback to students, improve theirlearning, and determine a student’s strengths and weaknesses. Summative assessmentapplies to both core and student-selected components of the course and contributes toprogression.
Knowledge is assessed using a range of methods, most commonly machine-marked assessments.Increasingly, online assessments are used which let us test different levels of learning (recall,understanding, application, synthesis). Outcomes typically assessed include basic and clinicalscience, patient investigation and management, clinical reasoning and judgement.
Essays, modified essays and structured short notes are used to assess knowledge, the ability toappraise evidence, critical reasoning and integration/application of knowledge and understanding atdifferent parts of the course.
Spotter assessment (Objective Structured Practical Examination) is used to test application ofknowledge in anatomy and imaging.
Objective Structured Clinical Examinations (OSCEs) are used throughout the programme to assess abroad range of specific clinical skills including communication skills, physical examination skills,clinical procedures, and analysis and integration of information.

Medicine Course Handbook 2010/11 8
Objective Structured Long Examination and Review (OSLER) is used at key points in the programmeto assess the students’ approach to the patient, communication skills, examination skills, and abilityto integrate and analyse information, clinical reasoning and formulation of a management plan.
A strategy for Mandatory Assessment of Core Clinical Skills (MACCS) is being implementedthroughout the programme in order to ensure that students have basic competence in definedessential practical skills. All students must pass each of these assessments in order to proceed withthe course,
Portfolios / logbooks are used throughout the programme
to document experience/exposure to a range of scenarios and procedures.
to record achievement of practical skills (Including MACCS).
to promote/demonstrate/document reflection on progress and to identify areas fordevelopment learning/experiences
Logbooks provide a tangible record of what learning has taken place during a placement and areconstructively aligned with the learning outcomes associated with work-based learning. They areused as supporting evidence of completion of a placement and the fidelity and veracity areconfirmed by 'sign off' by a local course teacher. They may be assessed on a completion/non-completion basis or graded excellent/completed/unsatisfactory for the purposes of progression.Outcomes assessed are typically related to clinical skills, practical procedures, patient investigation,attitudes, and personal development.
Professional attitudes and behaviour are assessed as part of portfolio and logbook signoffs. A systemfor reporting inappropriate student behaviour has been implemented, including the use of a ‘yellowcard’ system to flag issues during observed clinical interactions in OSCE/OSLER assessments. TheEarly Clinical & Professional Development logbook requires GP tutors to formally confirm that theirfirst and second year BMedSci student has behaved appropriately during their clinical visits.
Professional attitudes and behaviour are assessed as part of the PPD portfolio and by way of GPassessment evaluation at the end of year 1 and year 2. The GP assessment evaluation requires GPto comment on the students professional behaviour and attitudes during their early clinicalexperience GP visits throughout the first 18 months of the course.
Presentations, course work, project reports, dissertations, self-directed learning tasks, and case-based presentations are used to assess the ability to appraise evidence, critical reasoning andintegration/application of knowledge and understanding as well as communication skills.
Processes for setting assessment standards ensure that the appropriate students pass orfail
We rely on the expertise of academic and clinical staff, reinforced by the opinion of ExternalExaminers, to ensure that our assessment tasks are valid in the context of the relevant componentbeing assessed. External Examiner oversight is given particular weight in this respect, as specified inthe UoN Quality Manual,
Criterion-based standards are widely used in the programme aligned to the assessment of writtenwork, presentations, dissertations and course work. There is wide application of marking criteria,marking against model answers, and standardised grade descriptors. Application of such toolsincreases the reliability of assessment.
Medicine Course Handbook 2010/11 9
We apply the borderline group method of standard setting to all OSCEs throughout the programme,employing the median borderline mark as the cut-off where appropriate.
The EBEL method of standard setting is being applied to knowledge-based tasks assessed asmachine-marked assessments. The ANGOFF method is used for standard setting in GEM.
For the Mandatory Assessment of Core Clinical Skills, the minimum essential components of eachskill have been defined and agreed by expert consensus and students undertaking assessment areexpected to fully achieve all steps.
What compensation is permitted?
Compensation means being able to pass a course overall, if you have done very well in someassessments but failed in others. While this is possible in some other degree programmes it is notpossible on the medical course. No compensation is permitted in the assessment framework as it isconsidered that students need to attain the required level of achievement to provide a valid andbroadly based competence for progression into the clinical years.
In the BMedSci: all elements must be passed and resits taken on fails. No compensation is allowedfor theme D (Personal & Professional Development, Early Clinical Skills and Clinical CommunicationSkills): For other themes (ABC) the rules for progression allow for a small proportion of assessmentsas ‘soft fails’ or a single fail provided that the overall course average is above a specified thresholdand that soft fails do not signify that there is a significant area of academic weakness. This isoutlined in detail later in the booklet in the regulations for the degree and a summary diagram of therules for progression.
Assessment Feedback Policy
At the start of each year you will receive a Schedule of Assessments, giving a summary of allassessments for that academic year. You will be given guidance on the form and content ofassessments, including example questions and answers, as part of each course. This may take anyof several forms e.g. Course guide; NLE test paper, CAL program; seminars; course review session.Written and other feedback will be given.
External examiners
External examiners’ input is used throughout the programme in accordance with the University ofNottingham Quality Manual. Particular weight is given to the opinion of the External Examiner inmatters of academic oversight. All assessments are reviewed by External Examiners – and inparticular borderline and fail candidates work is reviewed. External examiners are specialists insubjects related to medicine and advise accordingly to the requirements of the University ofNottingham.
Adjustment to Examination Arrangements(Disabled students, students with dyslexia, dyspraxia or other long term medicalcondition)
Some students may require adjustments to examination arrangements. Your first point of callshould be Academic Support Unit for advice & deadlines.
http://www.nottingham.ac.uk/academicsupport/
http://www.nottingham.ac.uk/quality-manual/

Medicine Course Handbook 2010/11 10
ALTERNATIVE ASSESSMENT ARRANGEMENTS
Information relating to students who may require alternative examination arrangements.
Personal tutors and others within School who have had contact with students who may requirealternative examination arrangements should ensure that the student is aware of the deadlines andaware of their responsibility to contact Student Services for assessment by those deadlines.
Dyslexia, Disability Dyspraxia and/or Long Term Medical Conditions
Students with dyslexia, disability and/or long term medical conditions who think they requirealternative examination arrangements should contact Academic Support for assessment.Deadlines for alternative arrangements for examinations can be obtained from Academic Supportand from the GEMH office for GEM students.http://www.nottingham.ac.uk/academicsupport/
All requests for alternative arrangements should be supported by current acceptable evidence ofdisability or long-term medical condition such as a written report/assessment from: a registeredmedical practitioner; an educational psychologist; a psychiatrist.
Students who have not contacted Student Services by the deadline without good cause will notnormally be assessed for the forthcoming examination period (i.e. students not meeting the AutumnSemester deadline will not be assessed for alternative arrangements for the Autumn Semesterexaminations) and in such cases students my wish to submit an Extenuating Circumstances Form totheir School. This will not prevent the student being assessed for any later examination period.
Accidents and Short-term Illness
While students who are suffering a short-term illness, or have been involved in an accident, maycontact Student Services for support for their studies, it is not possible to make alternativeexamination arrangements for such candidates.
In such cases, options open to Schools to consider are:
i) The student misses the scheduled examination and submits an Absence Form, ExaminationForm and Extenuating Circumstances Form – the School may then recommend a resit withinthe next scheduled exam period.
ii) The student attempts the examination and submits an Extenuating Circumstances Form –and if upheld, the School would then recommend a resit within the next scheduled examperiod.
iii) The School makes alternative arrangements for the student’s examination ‘in-house’ (foradvice on this option, please contact the Assessment Manager – this option should only beused in exceptional circumstances).
The School considers setting the student an alternative form of assessment.
Medicine Course Handbook 2010/11 11
REGULATIONS FOR THE DEGREE OF BACHELOR OF MEDICAL SCIENCES/BACHELOR OFSCIENCE (MEDICAL SCIENCES) AND THE DEGREES OF BACHELOR OF MEDICINE ANDBACHELOR OF SURGERY
The following University Regulations govern the degree of Bachelor of Medical Sciences / Bachelor ofScience (Medical Sciences) and the degrees of Bachelor of Medicine and Bachelor of Surgery.
NB: These Regulations are now incorporated in the Programme Specifications (A100, A101, A104,A10S, and A300) which govern these University awards.
BMedSci/BMBSProgression from year 1 to year 2 and from year 2 to year 3 normally depends on passing allmodules in each year. University regulations state that the pass mark shall be 40%. Students whocan demonstrate mitigating circumstances to the Exam Board may be allowed to take resitexaminations as first attempts and then may repeat them one more time if they are failed.
Progression from year 3 to year 4 depends on having a classified Bachelor of Medical Sciences(Hons) degree which includes a pass in Clinical Phase 1 in Semester 6.
Candidates who have not been permitted to proceed to the following year shall normally have theright to one further opportunity to satisfy the examiners. The form of the assessment shall bedetermined by the Faculty. Any further opportunity to satisfy the examiners after the secondattempt shall be at the discretion of the Faculty, and shall be accorded only in exceptionalcircumstances.
Candidates may not normally offer themselves for reassessment in any modules which they havepassed.
For progression purposes, the higher or highest of the marks obtained by each candidate in eachmodule (whether at first attempt or upon re-assessment) shall be considered and the provisions ofthe below Rules applied accordingly.
Compensation Rules in Year 1 and Year 2Candidates who fail to pass all of their modules shall nevertheless be permitted to proceed to thefollowing year provided that they have achieved:
(i) an credit weighted average mark of at least 50%; and
(ii) pass marks in modules attracting in total at least 100 credits; and
(iii) a mark of at least 35% in each of the failed modules; and
(iv) have no failures in Theme D modules; and
(v) have no more than 10 credits of failure in a single theme (i.e. ''A'' or ''B'' or ''C'').
Candidates who have not been permitted to proceed to the following year under any of thepreceding rules shall normally have the right to one further opportunity to satisfy the examinerseither by September or in the next academic year (with or without residence).
Candidates who fail to progress from year one to year two or from year two to year three after resitexaminations may, at the discretion of the Faculty, transfer from the BMedSci degree to anapproved course of study leading to the award of the Bachelor of Science in Medical Sciences,providing they have satisfied the standard University Regulations for First Degrees. The award ofBachelor of Science in Medical Sciences does not confer eligibility to enter to the degrees of BMBS.
Progression in Clinical Phase 1 - see below and also Programme Specification for A300/A101
Medicine Course Handbook 2010/11 12
Progression in Clinical Phases 2 and 3 - see Programme Specification for A300/A101Degree Information:Award of BMedSci degreeThe Honours degree of Bachelor of Medical Sciences is awarded on successful completion of Parts Iand II of the course:
Degree weightings are:
Part I 1st Year and Part I 2nd Year 20% each
Part II 3rd Year 60%
The degree is classified as follows:
First Class - 70% and above
Upper Second Class - 60% to 69%
Lower Second Class - 50% to 59%
Third Class - 40% to 49%
Borderline candidates will be reviewed in accordance with University Guidelines. From 2005-06entry, 69% is the borderline threshold for a First class.
Course Weightings %Degree Calculation Model: Arithmetic Mean
Other Regulations A100/A101
(1) Students with failures in Clinical Phase 1 shall have further opportunities to satisfy the examinersas follows:
(i) Students who have failures in Clinical Practice:(a) KnowledgeA Student may progress to Clinical Phase 2 before taking the Knowledge resit in September. Shouldthis be failed the student continues with Clinical Phase 2 subjects until and including the DecemberCP2 assessments after which the student's CP2 course is suspended and the student must retakethe Clinical Practice module attachment at the first available opportunity and retake the Knowledgepaper. If this third attempt is failed the student's course is terminated.
(b) Skills CompetenciesAll competencies must be passed before the end of the attachment. If not passed a student may nottake the OSLER examination and does not progress to Clinical Phase 2. The student must retrain byretaking the Clinical Practice module at the first available opportunity (February of the followingsession) and be reassessed in the competencies. If this attempt is failed the student's course isterminated.
(c) Graded Skill OSLER/OSCEA student may progress to Clinical Phase 2 before taking the OSLER/OSCE resit at the first availableopportunity (usually in September). If failed again the student continues with Clinical Phase 2subjects until and including the December CP2 assessments after which the student's CP2 course issuspended and the student must retake the Clinical Practice module attachment and be reassessedat the first available opportunity in the following session. If this third attempt is failed the student'scourse is terminated.
A student who has failed at the first attempt both Knowledge and the OSLER/OSCE does notprogress to Clinical Phase 2. The student must retrain by retaking the Clinical Practice module at the

Medicine Course Handbook 2010/11 13
first available opportunity (February of the following session) and be reassessed in both Knowledgeand OSLER/OSCE. If in this attempt both are again failed the student's course is terminated.
(ii) Students who have failed Therapeutics:(a) KnowledgeA student may progress to Clinical Phase 2 before taking the Knowledge resit at the first availableopportunity (usually in September). Should this be failed the student shall be offered one finalreassessment (usually in December). If this third attempt is failed the student's course isterminated.
(iii) Students who have failed the Community Follow-up Project Module:(a) KnowledgeA student may progress to Clinical Phase 2 before taking the Knowledge resit at the first availableopportunity (usually in September). Should this be failed the student shall be offered one finalreassessment (usually in December). If this third attempt is failed the student's course isterminated.
(iv) Attitudes and Behaviour (log-book/portfolio sign-off) - A student receiving a failed end-of-coursefinal assessment will automatically be required to retake the full Clinical Practice module thefollowing year. Losing the logbook/portfolio may result in failing the attachment. The decision toallow the student to sit their Knowledge and Skills assessments prior to retaking the module will bemade on an individual basis. Students who have demonstrated inappropriate attitudes or behaviourmay be referred to the Fitness to Practise committee. Where there are concerns about patientsbeing placed at risk or the profession being brought into disrepute, the student may be excludedimmediately from clinical placements by the Dean.
Fitness to PractiseAward of BM, BS (and progression in the BMedSci course) is also dependent on fitness to practise. Ifa student is judged unfit to practise by reason of health or conduct, their course may be terminatedand the degree award refused. More details about the fitness to practise procedures are available at:http://www.nottingham.ac.uk/quality-manual/study-regulations/fitness-to-practise.pdf
Note: Award of the medical degrees (BM, BS) entitles a graduate to be provisionally registered bythe General Medical Council and to practise under supervision as a doctor. The regulation ofassessment within the course and the award of the qualification, therefore, are planned to fulfil thisvocational requirement. The award of the Bachelor of Medical Sciences degree after successfulcompletion of Semester 6 (Clinical Phase 1) does not carry any professional validation other thanprogression to the BM, BS degrees. BMedSci students who may elect to not undertake the full-timeclinical course after semester 5 are given an approved alternative modular course of study andassessments to complete their BMedSci degree at the end of semester 6 or to transfer to the BSc(Medical Sciences) degree. Such students will be required to complete 120 credits in their Part II ofthe degree course.
Progression in Clinical Phases 2 and 3 – see also Programme Specification for A300/A101Students with failures in Clinical Phase 2 shall have further opportunities to satisfy the examiners asfollows:
(a) KnowledgeA student with failures in any knowledge paper shall be offered a resit at the first availableopportunity as follows:A student failing a module Knowledge paper taken in the first half of the Clinical Phase 2 year(normally December) will be offered a resit in the second half of the same Clinical Phase 2 year(normally May).A student failing a module Knowledge paper taken in the second half of the year (normally May) willbe offered a resit at the first available opportunity (normally the following December) when theyhave progressed to Clinical Phase 3.

Medicine Course Handbook 2010/11 14
A student failing at the first available resit opportunity must retrain and retake the subject duringthe Elective period. Up to a maximum of 100 credits of Clinical Phase 2 modules may be undertakenin the Elective period.A student who is required to complete further retraining and be reassessed in Clinical Phase 2modules amounting to more than 100 credits is required to suspend their course until retraining hasbeen undertaken and reassessment taken place which shall normally be in the following academicsession.
(b) Skills Competencies (Obstetrics & Gynaecology, Child Health, Psychiatry, Health Care of theElderly, Specials) All competencies must be passed before the end of the attachment. If not passeda student will be required to undertake the following:(i) Obstetrics & GynaecologyA student shall complete retraining and be reassessed in the Elective period.(ii) Child HealthA student shall complete retraining and be reassessed in the Elective period.(iii) PsychiatryA student shall complete retraining and be reassessed in the Elective period.(iv) Health Care of the ElderlyA student failing the mini mental health state assessment shall complete retraining and bereassessed in the Elective period.(v) SpecialsA student shall complete retraining and be reassessed in the Elective period.
(c) Graded Clinical Skills OSCE/OSLERA student with failures at the first attempt in any Graded Clinical Skill shall be offered a resit at thefirst available opportunity as follows:
(i) A student failing a graded clinical skill (OSCE or OSLER) taken in the first half of the ClinicalPhase 2 year (normally December) will be offered a resit in the second half of the same ClinicalPhase 2 year (normally May).A student failing a graded clinical skill (OSCE or OSLER) taken in the second half of the year(normally May) will be offered a resit at the first available opportunity (normally the followingDecember) when they have progressed to Clinical Phase 3.A student failing at the first available resit opportunity must retrain and retake the subject duringthe Elective period. Up to a maximum of 100 credits of Clinical Phase 2 modules may be undertakenin the Elective period.
A student who is required to complete further retraining and be reassessed in Clinical Phase 2modules amounting to more than 100 credits is required to suspend their course until retraining hasbeen undertaken and reassessment taken place which shall normally be in the following academicsession.Following retraining the following shall apply:Knowledge - if a third attempt is failed the student's course shall be terminatedSkills (Competencies, Graded Skills (OSCE or OSLER)) - if a second attempt is failed the studentshall undertake retraining in that module and one further reassessment is offered. A student failingat this point shall have their course terminated.
(d) Attitudes and Behaviour (log-book/portfolio sign-off) - A student in whom attitudinal concernshave been raised should be referred to the Clinical Sub Dean. Where serious probity issues havebeen identified Fitness to Practise procedures will be invoked. The outcome of these procedures canvary but includes the power to recommend the University to suspend the student's course andclinical activities immediately.
For Clinical Phase 3 Regulations see below under 'Other Regulations'Degree Information:To qualify for the award of the degrees of Bachelor of Medicine and Bachelor of Surgery, candidatesshall follow an approved Course of Study for either four years (graduate entry medicine) or fiveyears.

Medicine Course Handbook 2010/11 15
Candidates must have passed all elements of Clinical Phases 1, 2 and 3.The award of a distinction to a candidate for the assessment in an individual Attachment shall bedetermined by the Board of Examiners who shall have discretion to consider other information inaddition to Examination marks.The degrees of Bachelor of Medicine and Bachelor of Surgery may be awarded as a pass, or a passwith Honours. A pass with Honours will be awarded to those candidates whose performance inClinical Phases 2 and 3 is considered by the Board of Examiners to be outstanding as follows:a). Performance during Clinical Practice will not be taken into account when determining the awardof Honours.b). Students will be awarded Honours based on the credit-weighted average (70% and above) of themodule marks. Each module mark is based on the combined graded knowledge and skillsassessments. Credit weighted average of Module Marks=sum of [each Module Mark x number ofcredits for the module]/sum of number of credits.c). Module marks contribute as follows:
Child Health - 50 x Total% (Knowledge:Skills 50:50 ratio)Obstetrics and Gynaecology - 50 x Total% (Knowledge:Skills 50:50 ratio)Health Care of the Elderly - 20 x Total% (Knowledge:Skills 33:67 ratio)Psychiatry - 30 x Total% (Knowledge:Skills 50:50 ratio)ACE - 180 x ACE Total% (Knowledge:OSCE1:OSCE2 50:30:20 ratio) 'Specials'- 30 x Total%(Knowledge:Skills 50:50 ratio)
e). Additional criteria yet to be determined but to include no adverse outcome of any Fitness toPractise hearing.d). The BMBS Board of Examiners may exceptionally award Honours to students not meeting theabove criteria but whose performance is nevertheless considered outstanding.NB From June 2007 the pass mark for assessments in Clinical Phases 2 and 3 is 50%.
Fitness to PractiseAward of BM, BS (and progression in the course) is also dependent on fitness to practise. If astudent is judged unfit to practise by reason of health or conduct, their course may be terminatedand the degree award refused. More details about the fitness to practise procedures are available athttp://www.nottingham.ac.uk/mhs/admissions/applying.html#fitness_to_practice and in theUniversity Quality Manual at http://www.nottingham.ac.uk/quality-manual
Course Weightings %Degree Calculation Model: Arithmetic Mean
Other Regulations A300
Students with failures at the first attempt in Clinical Phase 3 shall have further opportunities tosatisfy the examiners as follows:
(i) ACE Knowledge only - a student shall be offered a revision programme and reassessment duringthe Elective period in May.A student failing after resit shall retake the ACE module and be reassessed in the Knowledge papers.A student failing at this point shall have their course terminated.
(ii) Skills competenciesAll competencies must be passed before the end of the ACE module (usually March). If not passed astudent may not take the graded skill assessment (OSLER and OSCE) examination. The studentmust retrain by retaking the ACE module at the first available opportunity (July of the same year)and be reassessed in those competencies and if passed the student shall be assessed in the gradedskill (OSLER and OSCE). If the reassessment in competencies attempt is failed the student's courseis terminated.
(iii) Graded Clinical Skill (OSCE or OSLER or both) - a student shall be offered a revision programmeand reassessment during the Elective period in May.

Medicine Course Handbook 2010/11 16
A student failing after resit shall retake the ACE module and be reassessed in the graded ClinicalSkill(s). A student failing at this point shall have their course terminated.
(iv) ACE Knowledge and one graded Clinical skill (OSCE or OSLER) - a student shall retake the ACEmodule and be reassessed both in the Knowledge papers and the graded Clinical skill. If the studentfails this second attempt they shall be offered a revision programme and reassessment during theElective period in May. A student failing at this point shall have their course terminated.
(v) Attitudes and Behaviour (log-book/portfolio sign-off) - A student accumulating one attitudinalfailure will be offered one further opportunity only to repeat that component in the ACE moduleduring the elective period. A student failing at this point shall have their course terminated.A student accumulating more than one attitudinal failure shall:(1) invoke the Fitness to Practise procedures. Students who have demonstrated inappropriateattitudes or behaviour may be referred to the Fitness to Practise committee. Where there areconcerns about patients being placed at risk or the profession being brought into disrepute, thestudent may be excluded immediately from clinical placements by the Dean; and(2) not be eligible to take any of the end of module assessments and will have to repeat the wholeyear.
NB From June 2007 the pass mark for assessments in Clinical Phases 2 and 3 is 50%.
Fitness to PractiseAward of BM, BS (and progression in the course) is also dependent on fitness to practise. If astudent is judged unfit to practise by reason of health or conduct, their course may be terminatedand the degree award refused. More details about the fitness to practise procedures are available athttp://www.nottingham.ac.uk/mhs/admissions/applying.html#fitness_to_practice and in theUniversity Quality Manual at http://www.nottingham.ac.uk/quality-manual
Supplementary Regulations governing the degree of Bachelor of Science (BSc) Honours inMedical Sciences see Programme Specification A104
These regulations shall be subject to and read in the light of the University Regulations for First Degrees.
1. This unaccredited degree may be awarded only to those candidates who have transferred onto thecourse from the Bachelor of Medical Sciences (BMedSci) Honours degree according to the ProgrammeSpecification for that degree (A100).
2. The course of study shall be:
Year 2 Part ISemester 3 A12SF2 Human Development Structure and Function (II) 20 B
A12ASN Alimentary System & Nutrition 10 BA12REN Renal & Endocrine systems 10 B
Semester 4 A12FBN Functional and Behavioural Neuroscience 15 BA12GBP General and Biochemical Pharmacology 5 BA12PH2 Using Epidemiology in Practice 5 CLevel 3 Options (student selected from an approved list) 20 -
Year-long A12CLS Clinical Laboratory Sciences (II) 20 AA12PD2 Early Clinical & Professional Development (II) 10 D*A12CS2 Communication Skills (II) 5 D
* only taken if registered for BMedSci else an approved alternative is taken.
The Part II shall consist of:
Year 3 Part IISemester 5 A13RMx Research Methods (in school x) 10
A13HPx Research Project (Year long) (in school x) 60Level 3 Taught Courses (Student selected) 20
Semester 6 A13AMC The treatment and prevention of infection 5
Medicine Course Handbook 2010/11 17
A13THP Therapeutics 5Elective modules 20
3. The results from the Part I and Part II assessments shall decide the classification of degree to beawarded. The Board of Examiners shall attribute to Part I marks a weighting of 40% and to Part IImarks a weighting of 60%.

Medicine Course Handbook 2010/11 18
Bachelor of Medical SciencesProgression in Years 1 &2
PLEASE NOTE: THIS FLOWCHART IS FOR GENERAL GUIDANCE ONLY AND MUST BE READ IN CONJUNCTION WITHTHE REGULATIONS FOR THE BMedSci DEGREE – see Programme Specification
PASS(≥40%)MARKS INALL
MODULES?PROCEED
MARKS 35-39 INMODULES EQUIVALENTTO NO MORE THAN 20CREDITS AND NO MORETHAN 10 CREDITS IN ASINGLE THEME (ie ‘A’ or‘B’ or ‘C’)Optional modules exempt
YESSTART
FAIL ALLMODULES WITHMARKS < 40
FAIL ALLMODULES WITHMARKS < 40
FAIL ALL MODULESWITH MARKS < 40
AVERAGEMARK≥50?
ALLMARKS≥35?
PASSES INMODULESWITH≥100
CREDITS?
EXAMINATION BOARD DECISION
PASSES INALL THEMED
MODULES?IncludingOCSE
YES
NONO
NO
NO NO
NO
YESYES
YES
YES
October 2008 onwards

Medicine Course Handbook 2010/11 19
Bachelor of Science (Medical Sciences)Progression in Years 1 & 2

Medicine Course Handbook 2010/11 20
Summative Assessments for GEM (A101)
The purpose of the summative assessments is to measure competence and thereby determine progress. Thesummative assessments at the end of year 1 are a barrier to progression to year 2, and those at the end ofyear 2 are a barrier to progression to CP2 (Clinical Phase 2).
The summative assessments on GEM are:
End Year 1 End Year 2 (18 Months)
GEM Portfolio & Analysis Basic & Clinical Sciences (BCS)
Basic & Clinical Sciences (BCS)
Throughout the 18 month GEM Course
Clinical Skills

Medicine Course Handbook 2010/11 21
THE NOTTINGHAM MEDICAL MAP
PROGRAMME LEARNING OUTCOMES/OBJECTIVES FOR A100, A300, A101
This is a summary of a more detailed document, copies of which can be obtained from theMedical Course Offices.
It is the foundation of how we should plan, deliver and assess our undergraduate course. The GMC document (‘Tomorrows’ Doctors’, 2009) is used as the main reference source.
THE UNIVERSITY OFNOTTINGHAM MEDICAL
GRADUATE
(MEDICAL GRADUATE)
Doctor as Scholar& Scientist
(KNOWLEDGE ANDUNDERSTANDING)
Doctor asProfessional
(ATTITUDES)
Doctor as Practitioner
(SKILLS)
Thescientificbasis ofpractice
Communicationskills
General, genericgraduate skills
Intellectualattributes
Clinicaland
practicalskills
Teachingskills
Medico-legaland ethical
issues
Professionalattitudes andcompetencies
Disability andrehabilitation
Treatment
The workingenvironment
The healthof the public
Theindividualin society

Medicine Course Handbook 2010/11 22
WHAT THE DOCTOR SHOULD KNOW(KNOWLEDGE AND UNDERSTANDING)
Thescientificbasis ofpractice
Treatment
The workingenvironment
The healthof the public
Theindividual in
society
Core knowledge: Clinical and basic sciencesRelevant parts of behavioural and social sciencesAbility to integrate and critically evaluate evidence from all sources
Disease: Normal and abnormal structure and functionNatural history of human diseasesBody’s defence mechanismsBody’s responses to illnessDisease presentationEffects of genetic, social and environmental factors and treatment
Epidemiology: Demography and biological variabilityScientific methods relevant to medicine
Conventional: Evaluation of effectiveness and evidenceConsideration of patients’ viewsEffective and safe use of medicinesSurgical and perioperative careInitial management of certain emergenciesManagement of acute illnessManagement of recurrent and chronic illness and disabilityRehabilitation and care in institutions and the communityRelief of pain and distressPalliative care
Behavioural: Lifestyle in health and disease. Substance abuse.
Other therapies: Other non-pharmacological therapiesAlternative and complementary therapies and their interactions
The NHS: Healthcare in the UKStructures and functions of the NHSDevelopments and guiding principles in the NHS
Public health: Assessing community needs in relation to service provisionGenetic, environmental and social factors influencing diseasePromotion of health and preventing disease, surveillance and screening
Core knowledge: Social and cultural environment of medical practice in UKHuman developmentAreas of psychology and sociology relevant to medicine
Society and disease: Behaviour and relationships between patients and othersDiversity of social and cultural valuesDiffering views of healthcare and illnessSpecific issues (eg alcohol and drug abuse, domestic violence)Avoiding prejudice
The ill patient: Patients’ understanding and experience of their conditionExploring patients’ fears and concernsHelping patients understand their conditionHelping patients take active role in treatment decisions

23
WHAT THE DOCTOR SHOULD BE ABLE TODO
(SKILLS)
Communicationskills
General, genericgraduate
skills
IntellectualAttributes
Clinical andpractical
skills
Teaching skills
Organisational skills: Time and resource managementTask prioritisationTeamworkReflection and being self-critical
Personal skills: Lifelong learningRetrieving, managing and manipulating informationPresentation/communication of informationApplication of the principles of scientific research and auditStudying topics in depthEffective teachingMentoring others
Interactional skills: Dealing with uncertaintyWorking in a changing environmentRisk managementEthical decision-making
Analytical skills: Problem recognition, definition and prioritisationInformation analysis, interpretation, evaluation and prioritisationLimitations of medical knowledge; importance of professional judgement
Attitude: Reflective and inquisitive attitudeApplication of rational processesImpact of value judgements
Audit and research: Research and scientific methodologyFormulating pertinent research questionsUse of appropriate quantitative and qualitative methodologiesRigour in collecting, analysing and interpreting dataEvidence, audit, and observed variation in clinical practiceUse of research skills to understand and influence practice
Uncertainty: Inevitability of uncertainty in medicineUse of appropriate strategies to deal with uncertainty
Clinical and practical skills: Professional skills appropriate for PRHOClinical skills (specific list)Practical skills (specific list)
Teaching skills: Principles of medical educationIdentify their learning needsUse different techniques for documentationUse different teaching techniquesExhibit creativity/resourcefulness
Communication skills: Communicate with patients and relatives (listening,explaining, mediating and negotiating, handling complaints and liasing withother professionals)Awareness of other methods of communicationImportance of background and disabilityUse of interpretersPractise communicating in different waysCommunicating in difficult circumstances

24
HOW THE DOCTOR SHOULDBEHAVE
(ATTITUDES)
Medico-legaland ethical
issues
Professionalattitudes andcompetencies
Disability andrehabilitation
Core knowledge: Knowledge and understanding of the main ethical and
legal issues.
Disability: Rights of people with mental or physical disabilitiesOpportunities available to disabled people affected by society’s view ofthemPotential strengths and contributions of such individuals
GMC standards: Understanding of the principles of good practice set outin the GMC publication ‘Seeking patients’ consent: the ethicalconsiderations’
Personal practice: Self-awareness and reflectionManaging learning with respect to continuing professional developmentRecognising the pressures on themselves and colleaguesPrioritising the care of ill patientsPrioritising personal timeKeeping effective medical recordsKeeping up-to-date with current medical practice
General standards: Applying the principles of confidentiality, consent,honesty and integrityDealing effectively with complaintsBeing aware and complying with legal and professional responsibilitiesConsidering the rights of patientsUnderstanding and complying with requirements of clinical governance
GMC Standards: All the attributes to be able to function as an F1 doctorGraduates must adhere to the professional standards defined by the GMC.Their attitudes and behaviour need to be consistent with ‘Duties of aDoctor’ as defined by the GMC in ‘Good Medical Practice’
Rehabilitation: Importance of the responses to illness and providing helpto recovery, managing chronic disease and relapse, reducing or managingimpairments, disabilities and handicaps
Teamwork: Promotion of effective inter-professional activity, includinglearningWorking within the limits of responsibility and capabilityMaking decisions in partnership with colleagues and patients
Doctor/patient: Importance & therapeutic potential of patient/doctorrelationshipEmpathetic and holistic approach to patientsRespect patient autonomy and involve patients in management decisionsRespect different cultures, values, views and beliefsRespect for patients who choose alternative medical practicesNon-judgmental in all work and avoid stigmatising patientsReflective practice/audit and appraisal of their own and others’ work

25
Student Conduct, Concern Form & The Whistleblowing Policy
Student Conduct
All medical Students are expected to comply with a Code of Practice as outlined in the MedicalStudent Contract. Please visit the website given below. Any queries, please discuss this with yourPersonal Tutor
http://www.nottingham.ac.uk/MHS/undergraduate-courses/Routes/index.aspx
Concern Form
The conduct of a student is assessed both while at the University and in private life. Certain aspectsof personal conduct may give rise to cause for concern.
Any student or member of staff may report a concern about a student using the “Concern FormProcedure. This is available at:
http://www.nle.nottingham.ac.uk/websites/pastoral/docs/Concerns_Form_guidance_notes_March_10v3.doc
Whistleblowing Policy
Any student may witness something which gives them cause for concern while in the University or ina health care setting.
If discussion with one of the tutors or local supervisory team does not resolve concerns, then it ispossible to use the Whistleblowing procedure. This is available via theNLE/degree/support/Academic Pastoral Support or via the link below:
http://www.nle.nottingham.ac.uk/DEGREE/displayMediGuide.php?year=&module=DEGREE&session=2010/11

26
COURSE COORDINATORS FOR THE FIVE YEARSAND
CONTACT DETAILS

27
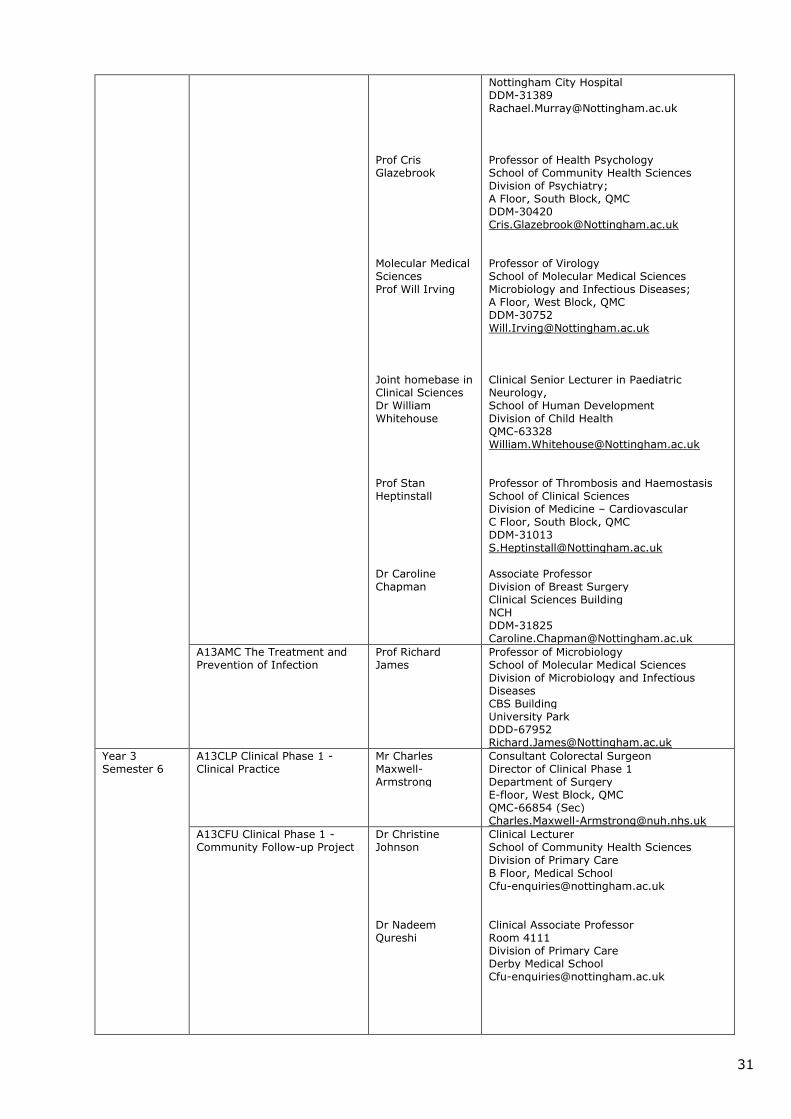
COURSE COORDINATORS FOR THE FIVE YEARS AND CONTACT DETAILS
For telephones, the prefixes quoted are -
DDD = Direct Dial University
DDI = Direct Dial University
DDM = Direct Dial Medical School
MS, TRDH = Direct Dial Medical School, The Royal Derby Hospital
QMC = (Queens Medical Centre) from University, add prefix 74
Timing Module/Course Course Co-ordinators
Contact Details
Year 1Semester 1
A11MBM Molecular Basis ofMedicine
Dr FergusDoherty
LecturerSchool of Biomedical SciencesMedical School, [email protected]
A11EXT Structure, Functionand Pharmacology ofExcitable Tissues
Prof Fran Ebling Professor of NeuroendocrinologySchool of Biomedical SciencesMedical School, [email protected]
A11HDT Human Development& TissueDifferentiation
Dr MargaretPratten
Associate ProfessorSchool of Biomedical SciencesMedical School, [email protected]
A11BHS Behavioural Sciences Prof CrisGlazebrook
Professor of Health PsychologySchool of Community Health SciencesDivision of PsychiatryA Floor, South Block, [email protected]
A11PH1 Public HealthEpidemiology
Dr Puja Myles
Dr JoLeonardi-Bee
Associate Professor in Health ProtectionDivision of Epidemiology and Public HealthClinical Sciences BuildingNottingham City [email protected]
Associate Professor in Medical StatisticsDivision of Epidemiology and Public HealthSchool of Community Health SciencesClinical Sciences BuidlingNottingham City HospitalDDM [email protected]
Year 1Semester 2
A11CLS Clinical laboratorysciences (I)
Dr Ian Todd Associate Professor & Reader in CellularImmunopathologySchool of Molecular Medical SciencesImmunologyA Floor, West Block, [email protected]

28
A11CRH Cardiovascular,Respiratory &Haematology
Dr Billy Dunn
Dr Steven Burr
Dr MichaelRandall
Associate Professor & ReaderSchool of Biomedical SciencesMedical School, [email protected]
Lecturer/Deputy Director of Biomedical SciencesTeachingSchool of Biomedical SciencesMedical School, [email protected]
Associate Professor & Reader inCardiovascular Pharmacology,School of Biomedical Sciences,Medical School, [email protected]
A11SF1 Human DevelopmentStructure andFunction (I)
Dr MargaretPratten
Dr SiobhanLoughna
Associate ProfessorSchool of Biomedical SciencesMedical School, [email protected]
LecturerSchool of Biomedical SciencesMedical School, [email protected]
General Co-ordinated by:Mrs Jane Dewse
SecretaryMedical Course OfficeMedical School, [email protected]
Year 1BothSemesters
A11CS1 ClinicalCommunicationSkills (I)
Dr VictoriaTischler
LecturerSchool of Community Health SciencesDivision of PsychiatryA Floor, South Block, [email protected]
A11PD1 Early Clinical andProfessionalDevelopment (I)
Dr Richard Knox Clinical LecturerRoom D1411,Division of Primary CareSchool of Community Health SciencesD Floor, Medical School, [email protected]
Year 2Semester 3
A12ASN Alimentary System &Nutrition
Dr Billy Dunn
Dr KostasTsintzas
Associate Professor & ReaderSchool of Biomedical SciencesMedical School, [email protected]
Associate ProfessorSchool of Biomedical SciencesMedical School, [email protected]
A12REN Renal and Endocrinesystems
Dr Vera Ralevic
Dr Sue Chan
Associate Professor & ReaderSchool of Biomedical SciencesMedical School, [email protected]
LecturerSchool of Biomedical SciencesMedical School, [email protected]

29
A12SF2 Human DevelopmentStructure andFunction (II)
Dr MargaretPratten
Dr Lopa Leach
Associate ProfessorSchool of Biomedical SciencesMedical School, [email protected]
Associate ProfessorSchool of Biomedical SciencesMedical School, [email protected]
General Co-ordinated by:Mrs Jane Dewse
SecretaryMedical Course OfficeMedical School, [email protected]
Year 2Semester 4
A12FBN Functional andBehaviouralNeuroscience
Dr Terry Parker
Prof GeorginaJackson
Associate ProfessorSchool of Biomedical SciencesMedical School, [email protected]
Professor of Cognitive NeuropsychologySchool of Community Health SciencesDivision of PsychiatryA Floor, South Block, [email protected]
A12GBP General &BiochemicalPharmacology
Dr Jeff Fry Associate Professor & ReaderSchool of Biomedical SciencesMedical School, [email protected]
General Co-ordinated by:Mrs Jane Dewse
SecretaryMedical Course OfficeMedical School, [email protected]
A12PH2 Using Epidemiologyin Practice
Dr RichardPuleston
Associate Professor in Health ProtectionSchool of Community Health SciencesDivision of Epidemiology and Public HealthClinical Sciences BuildingNottingham City HospitalDDM [email protected]
Year 2BothSemesters
A12CLS Clinical LaboratorySciences (II)
Dr Ian Todd Associate Professor & Reader in CellularImmunopathologySchool of Molecular Medical SciencesImmunologyA Floor, West Block, [email protected]
A12CS2 ClinicalCommunicationSkills (II)
Dr VictoriaTischler
LecturerSchool of Community Health SciencesDivision of PsychiatryA Floor, South Block, [email protected]
A12PD2 Early Clinical andProfessionalDevelopment (II)
Dr Richard Knox Clinical LecturerRoom D1411,School of Community Health SciencesDivision of Primary CareD Floor, Medical School, [email protected]

30
Semester 4OPTIONS
20 credits tobe chosen
A13DID Defects inDevelopment
10 credits, 48 students
Dr SiobhanLoughna
LecturerSchool of Biomedical SciencesMedical School, [email protected]
A13MDI MolecularDiagnostics
10 credits, 25 students
Prof Kevin Morgan Professor of Human Genomics andMolecular GeneticsSchool of Molecular Medical SciencesClinical ChemistryA Floor, West Block, [email protected]
A13MIA MolecularImmunology andAutoimmunity
10 credits, 30 students
Dr Ian Todd Associate Professor & Reader in CellularImmunopathologySchool of Molecular Medical SciencesImmunologyA Floor, West Block, [email protected]
A13DIT Diagnostic ImagingTechnologies
10 credits, 25 students
Dr MargaretPratten
Dr SiobhanLoughna
Associate ProfessorSchool of Biomedical SciencesMedical School, [email protected]
LecturerSchool of Biomedical SciencesMedical School, [email protected]
A13MMBMedical Microbiology
10 credits, 130 students
Dr Alan Cockayne Associate ProfessorCBS BuildingUniversity [email protected]
A13MOM Molecular Medicine
10 credits, 130 students
Dr Simon Dawson Lecturer in BiochemistrySchool of Biomedical SciencesMedical School, [email protected]
Year 3Semester 5
A13HPx Research ProjectAndA13RMx Research Methods
Sub-Dean forHonours Year:
Dr FergusDoherty
List of HomeBases in Schools& Co-ordinators:
BiomedicalSciencesDr Steven Burr
CommunityHealth SciencesDr Puja Myles
Dr RachaelMurray
Lecturer, School of Biomedical SciencesMedical School, [email protected]
LecturerSchool of Biomedical SciencesMedical School, [email protected]
Homebase Co-ordinatorAssociate Professor in Health ProtectionDivision of Epidemiology & Public HealthClinical Sciences BuildingNCHDDM- [email protected]
Projects Co-ordinatorLecturer in Health Policy and PromotionDivision of Community Medicine &EpidemiologySchool of Community Health SciencesClinical Sciences Building
31
Prof CrisGlazebrook
Molecular MedicalSciencesProf Will Irving
Joint homebase inClinical SciencesDr WilliamWhitehouse
Prof StanHeptinstall
Dr CarolineChapman
Nottingham City [email protected]
Professor of Health PsychologySchool of Community Health SciencesDivision of Psychiatry;A Floor, South Block, [email protected]
Professor of VirologySchool of Molecular Medical SciencesMicrobiology and Infectious Diseases;A Floor, West Block, [email protected]
Clinical Senior Lecturer in PaediatricNeurology,School of Human DevelopmentDivision of Child [email protected]
Professor of Thrombosis and HaemostasisSchool of Clinical SciencesDivision of Medicine – CardiovascularC Floor, South Block, [email protected]
Associate ProfessorDivision of Breast SurgeryClinical Sciences [email protected]
A13AMC The Treatment andPrevention of Infection
Prof RichardJames
Professor of MicrobiologySchool of Molecular Medical SciencesDivision of Microbiology and InfectiousDiseasesCBS BuildingUniversity [email protected]
Year 3Semester 6
A13CLP Clinical Phase 1 -Clinical Practice
Mr CharlesMaxwell-Armstrong
Consultant Colorectal SurgeonDirector of Clinical Phase 1Department of SurgeryE-floor, West Block, QMCQMC-66854 (Sec)[email protected]
A13CFU Clinical Phase 1 -Community Follow-up Project
Dr ChristineJohnson
Dr NadeemQureshi
Clinical LecturerSchool of Community Health SciencesDivision of Primary CareB Floor, Medical [email protected]
Clinical Associate ProfessorRoom 4111Division of Primary CareDerby Medical [email protected]

32
A13THP Clinical Phase 1 -Therapeutics
Dr MichaelRandall
Associate Professor & Reader inCardiovascular Pharmacology,School of Biomedical Sciences,Medical School, [email protected]
Year 4ClinicalPhase 2
A14ONG Clinical Phase 2 -Obstetrics & Gynaecology
Dr Pam Loughna Clinical Senior LecturerSchool of Human Development,Academic Division of Obstetrics &Gynaecology, Child HealthObstetrics & GynaecologyNottingham City [email protected]
A14CHH Clinical Phase 2 -Child Health
Dr Don Sharkey Clinical Associate Professor of NeonatalMedicineAcademic Child HealthSchool of Clinical SciencesE Floor, East [email protected]
A14PSY Clinical Phase 2 -Psychiatry
Dr Stuart Leask Clinical Senior LecturerSchool of Community Health SciencesDivision of PsychiatryA Floor, South Block, QMCDDM [email protected]
A14SM1 Clinical Phase 2 -Special Study Module 1
Mr K L Cheung Consultant Breast Surgeon & ClinicalAssociate ProfessorProfessorial Unit of SurgeryDivision of Breast SurgeryNCHDDM [email protected]
A14HCE Clinical Phase 2 -Health Care of the Elderly
Dr Rob Jones Clinical Associate ProfessorChair HCE Teaching CMC II, Head of Sectionof Old Age PsychiatrySchool of Community Health SciencesDivision of PsychiatryOld Age PsychiatryA Floor, South Block, [email protected]
A14DOO Clinical Phase 2 -Dermatology
Dr Stuart Cohen Consultant DermatologistDepartment of DermatologyB Floor, South BlockQueen’s Medical CentreNottinghamNG7 [email protected]
A14 DOO Clinical Phase 2 -Otorhinolaryngology
Prof John Birchall Professor of OtorhinolaryngologyOtorhinolaryngologyEyes & ENT Block, QMCQMC-44569; Clin Sec [email protected]
A14DOO Clinical Phase 2 -Ophthalmology
Mr WinfriedAmoaku
Clinical Assoc Prof & Reader inOphthalmology & Visual SciencesSchool of Clinical SciencesDivision of OphthalmologyB floor, Eyes & ENT Block, QMCClin Sec [email protected]

33
Year 5ClinicalPhase 3
A14ACE Clinical Phase 3 -Advanced Clinical Experience
Senior medicineSenior surgeryMusculo-skeletal disorders &disabilityGeneral Practice/Primary Care(Senior medicine, surgery,MDD, SSM2 & GP = The‘Advanced Clinical Experience,ACE’ Course)
Mr Jon Lund Clinical Associate ProfessorSchool of Graduate Entry Medicine andHealthThe Royal Derby HospitalMS/TDRH [email protected]
A14SM2 Clinical Phase 3 -Special Study Module 2
Mr K L Cheung Consultant Breast Surgeon & ClinicalAssociate ProfessorProfessorial Unit of SurgeryDivision of Breast SurgeryNCHDDM [email protected]
A14ACE Clinical Phase 3 -Primary Care
Dr OleysaAtkinson
LecturerDivision of Primary CareSchool of Community Health SciencesRoom 1307, Tower BuildingUniversity [email protected]
Elective (9 weeks) Clinical SubDeans
Dr BrianThompson
Professor KeithNeal
Medical Course OfficeMedical School, QMCDDM 30009
Dr Brian ThomsonClinical Associate ProfessorSchool of Molecular Medical SciencesNottingham University HospitalsDDM [email protected]
Prof Keith NealClinical ProfessorDept of Epidemiology and Public healthClinical Sciences BldgCity [email protected]
Preparation for FoundationYear Doctor 1 (FDY1)
Dr Adrian Wills Consultant NeurologistC Floor, West Block, [email protected]
-o0o-

34
GEM MODULES AND CONVENORS (A101) COURSE
ModuleCode
Module Title ModuleConvenor
Telephone Email
Year 1
A12F1G Structure,function anddefence
Dr GwenHughes
01332724688
A12R1G Respiratorysciences
Dr GwenHughes
01332724688
A12C1G Cardiovascular HannahWaterhouse
01332724726
A12M1G Limbs and Back Dr RichardTunstall
01332724644
A12A1G Alimentary Dr SusanAnderson
01332724609
A12E1G Endocrine Dr Pam Hagan 01332724726
A12P1G Personal andprofessionaldevelopment 1
Dr SharonConroy
01332724692
Year 2
A12U2G Urogenital Dr RaheelaKhan
01332724664
A12N2G Neuroscience Dr DanielMcLaughlin
01332724621
A12I2G Integrative Dr Paul Garrud 01332724616
A12P2G Personal andprofessionaldevelopment 2
Dr SharonConroy
01332724692

35
PASTORAL CARE PATHWAY
- OVERVIEW

36
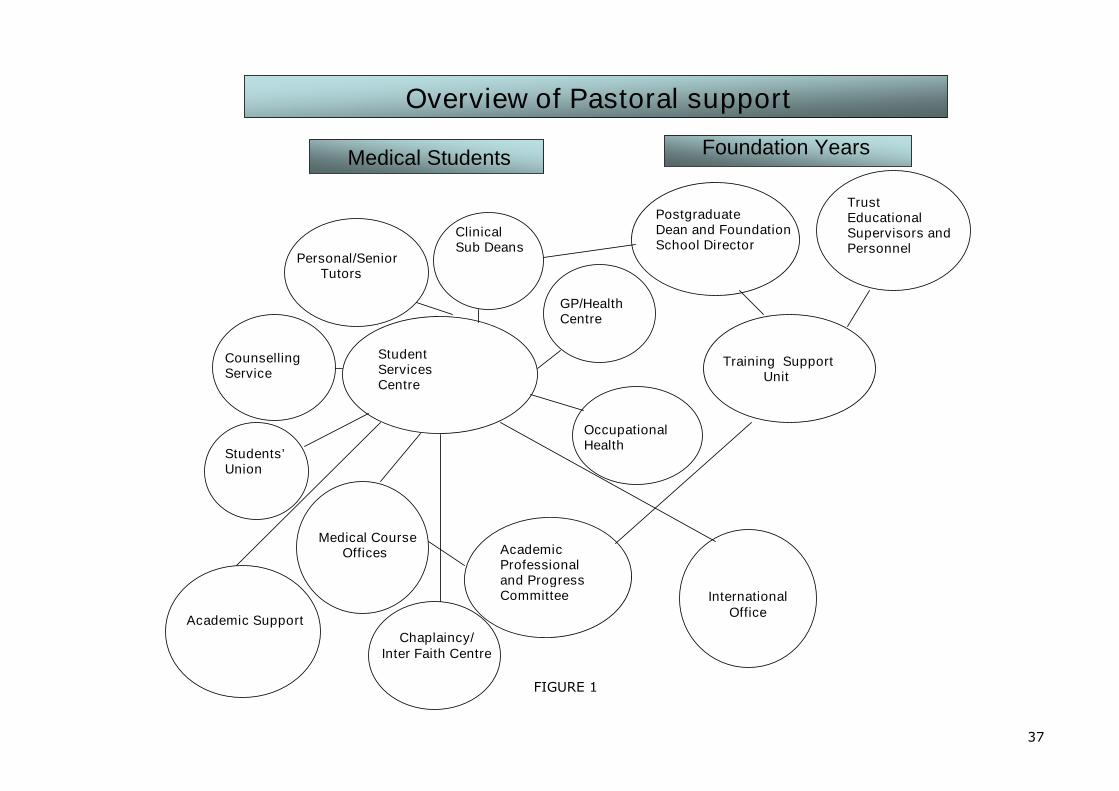
INTRODUCTION
Overview and the Pastoral Care PathwayThe Pastoral Care Pathway for medical students identifies the various forms of support that bothmedical students and F1 doctors can access and also the links between these sources of support. Itallows everyone involved in the teaching and pastoral care of students to see at a glance how theirrole fits in within the overall picture. It is illustrated in Figure 1 and table.
The interface between Medical Students and the Foundation Year 1 (F1)Any of the above undergraduate services have the responsibility of discussing appropriate problemswith the Dean Director and/or with the NHS East Midlands Healthcare Workforce Deanery Supportand Guidance Unit with a student’s agreement. This will allow a better transition of support whichwould be to the benefit of the medical student once a F1 and would provide reassurance to futureemployers within the NHS.
Difficulties may arise where there are serious concerns about a student’s fitness to practice. Undersuch circumstances, where there is a risk of harm to the individual, colleagues or patients, theClinical Sub-Dean (or others such as the Occupational Health Service or the University CounsellingService) will discuss the issues with the Dean Director so that appropriate support can be provided.Confidentiality will only be breached if there is good reason to believe that the individual or others(eg: patients) are at risk.
37
Overview of Pastoral support
Medical Students Foundation Years
Personal/SeniorTutors
ClinicalSub Deans
CounsellingService
Medical CourseOffices
GP/HealthCentre
PostgraduateDean and FoundationSchool Director
TrustEducationalSupervisors andPersonnel
Training SupportUnit
OccupationalHealth
Students’Union
AcademicProfessionaland ProgressCommittee
StudentServicesCentre
Chaplaincy/Inter Faith Centre
Academic Support
InternationalOffice
FIGURE 1

38
PASTORAL SUPPORT PATHWAYTABLE 1
STUDENTS F1
SUPPORT FOR STUDENTS AND F1 DOCTORS
Primary Care GP Tutor
Hospital Trust Educational Supervisor Associate Clinical Sub Deans UG Co ordinators
Trust Consultant Trainer Educational/
Clinical Supervisors Foundation Director Human Respources
Senior TutorsSteven BurrPamela Hagan (GEM)Jeanette LilleyMargaret PrattenVictoria Tischler
Clinical Sub DeansMargaret JonesIain McVicar Your GP
PostgraduateDean andManagingDirectorDavid SowdenFoundationSchool DirectorBridget Langham
Medical Course OfficeJudith FranklinRuth AireyJane DewseSue HallMartine LowesClaire NewburyGiorgio Vitale
Graduate Entry Medicine & HealthSchool OfficeAmanda CollettSarb AtwalVictoria BurgoyneAnne-Marie DwyerNeill MagillCathy Porter
Occupational HealthIan Aston TRUSTDavid Sherwood Jones(GEM) DERWENT
DeanIan Hall
Associate Dean for Medical EducationJames Lowe
Training Support Unit(TSU)Caroline McCarthy
Head of Schools Director of Undergraduate StudiesDanny Mclaughlin (GEM)
Student Services Centrehttp://www.nottingham.ac.uk/ssc/
Academic Progress Committee Chaplaincy/Inter-faithCentrehttp://www.nuh.nhs.uk/spiritualandpastoralcare/There is also a site at theRoyal Derby Hospital. SeeFurther Contacts forSupport and Guidance.
39
University Counsellinghttp://www.nottingham.ac.uk/counselling/
Academic Supporthttp://www.nottingham.ac.uk/academicsupport/
Students Unionhttp://www.su.nottingham.ac.uk/
International Officehttp://www.nottingham.ac.uk/international/

40
THE MEDICAL FAMILY

41
THE MEDICAL FAMILY
All new medical students are allocated to a ‘Medical Family’. The main aim of the Family is toprovide an environment for peer support.
The family normally comprises A Tutor (a member of staff (University or NHS) who has volunteered for this role) Two to four medical students from each year.
MedSoc and GEMSOC operate a ‘Parenting’ Scheme where the first year student’s parent will be astudent from the second year.
What can tutors do?
Offer SupportAll students are allocated a Personal Tutor whose role is to encourage and support them, encouragereflective practice, discuss progress with students and help with any problems they have. AtUniversity students have an opportunity to participate in a wide range of leisure activities in additionto their academic studies. Sensitive and supportive advice from their tutor can help them optimisethe balance between the two.
Nevertheless, students must feel able to turn to their tutors to talk over both academic and non-academic problems. In many cases, the tutors may be the appropriate source of advice. However,it may be more sensible and appropriate in some circumstances for the student to approach anotheragency (See Figure 1 and table 1).
Help in crisesStudents should feel able, if they wish, turn to their tutor in times of crisis such as bereavement.
Provide informationTo be able to give useful advice tutors need to be aware of the Regulations relating to the medicalcourse. Copies of the latest edition are given to each tutor annually and these are also displayed onthe University web; http://www.nle.nottingham.ac.uk/websites/pastoral/ andhttp://www.nottingham.ac.uk/quality-manual/student-support/SSD.htm
They should also be able to direct students to other agencies and appropriate sources ofinformation. A resource list of useful contacts is given later in this booklet.
Please feel free to contact the Student Support & Development Administrator for anyfurther help.
Student Support & Development AdministratorMedical Course Office, B Floor, Medical SchoolTel: 0115 82 [email protected]

42
Meet RegularlyFormal tutor/tutee meetings are compulsory throughout the Course (see table 2). These formalmeetings are opportunities to give praise and encouragement for good or improving performance.Agenda-specific details for these meetings will be provided. Students will be expected to completeactions plans for their portfolio.
For those students who are experiencing difficulties, these meetings also provide opportunities todiscuss academic issues. In cases where students are failing exams the following may be explored:
Learning styles Approach to studies Commitment to a medical career Disabilities, extenuating circumstances or other relevant factors
Represent their tuteesTutors can advise, help or represent their tutees in examination boards and if required Academicand Professional Progress Committees.
Tutors can provide references for students in connection with employment during vacations,housing, applying for electives and F1 posts.
Advise on Extenuating Circumstances ProcessThe University regulations on extenuating circumstances processes can be found at:http://www.nottingham.ac.uk/quality-manual/assessment/pro-guid-ext-cir.htm
Tutors can guide students in submitting an extenuating circumstances form. This must be submittedwithin 7 working days either side of the exam/coursework deadline. The Medical Course Offices willrequire proof of any extenuating circumstances such as a doctor’s letter/crime number etc.Extenuating circumstances are any type of personal circumstances that have or are likely to have asignificant impact on a students’ academic performance in any type of assessment. The UniversityQuality Manual lists some examples:
Illness (other than minor illnesses) Bereavement Acute personal/emotional circumstances Becoming a victim of crime Family illness
It is especially important that tutors represent their students at meetings of the Board of Examiners(either BMedSci, BSc or BMBS, GEM).
Academic SupportStudents who require special arrangements for examinations (e.g. extra time), must make anappointment with the Academic Support Centre; http://www.nottingham.ac.uk/as/ or telephone(0)115 951 3710. The student will be assessed and a formal recommendation will be sent to therelevant Medical Course Offices. The student will then be sent a personalised exam timetable at theappropriate time.
Provide formal contact for Portfolio ReviewTable 2 provides the details of the compulsory contact between students and tutor that shouldoccur. The meetings in the early part of the course are mandatory and encourage a rapport to bedeveloped between the tutor and tutee.

43
TABLE 2Tutorials
Five Year CourseBMedSci/BMBS/BSc(A100, A104, A10S)
Graduate Entry Medicine(A101)
Timing ofMeeting
Agenda for mandatory meetingswhich should be ‘face-to-face’unless otherwise stated
Timing of Meeting Agenda formandatory meetingswhich should be‘face-to-face’ unlessotherwise stated
Beginning ofterm (Sept)Yr 1
“Welcome”Meet all new students collectively(20mins) and individually (20minseach) for ‘getting to know you’ andpaperwork
Beginning of term(Sept) Yr 1
Introductory
October – endof first term.Yr1
Tutor/tutee social meeting for allyears
DecemberYr 1
Individual meetings with tutees(20mins each)See Portfolio for agenda
Yr 1A minimum of onetutorial per term isrequired
Action Plan
FebruaryYr 1
Individual meetings with tutees(20mins each)See Portfolio for agenda.
Yr1A minimum of onetutorial per term isrequired
Action Plan
April Yr 1 Individual meetings with tutees(20mins each)See Portfolio for agenda.
Yr1A minimum of onetutorial per term isrequired
Action Plan
Beginning ofterm SeptYr 2
“Welcome back”Individual meetings with student(20mins each) for general discussionabout second year
Beginning of term(Sept) Yr 2
“Welcome back”
October – endof first term.Yr2
Tutor/tutee social meeting for allyears
DecemberYr 2
Individual meetings with tutees(20mins each)See Portfolio for agenda
Yr 2 A minimum of onetutorial per term isrequired
Action Plan
FebruaryYr 2
Individual meetings with tutees(20mins each)See Portfolio for agenda
Yr 2 A minimum of onetutorial per term isrequiredJoin CP1
Action Plan
April Yr 2 Individual meetings with tutees(20mins each)See Portfolio for agenda
November Yr3 Individual meetings with tutees(20mins each)See Portfolio for agendaJoin CP1

44
CLINICAL PHASES
CP1March
Informal contact between tutor & tutee either by email or phone. A face to face meetingis advisable if there are any problems, for example academic failure.
CP2 August Informal contact between tutor & tutee either by email or phone. A face to face meetingis advisable if there are any problems, for example academic failure
CP2 January Informal contact between tutor & tutee either by email or phone. A face to face meetingis advisable if there are any problems, for example academic failure.
CP3 July Informal contact between tutor & tutee either by email or phone. Agenda provided totutor & student prior to contact. A face to face meeting is advisable if there are anyproblems, for example academic failure.
CP3 January Informal contact between tutor & tutee either by email or phone. Agenda provided totutor & student prior to contact. A face to face meeting is advisable if there are anyproblems, for example academic failure.
ObligationsBoth tutor and student have to make an effort if the relationship is to work! It is not acceptable fora student to fail to attend a previously arranged or timetabled meeting. The student should informthe tutor of any unforeseen problems and reschedule the meeting. Similarly, if the tutor cannotmake a meeting he/she should inform the student and rearrange the meeting. This emphasises theimportance of both tutors and students maintaining up to date contact details.
If a student is unhappy with their tutoring arrangements, they should do something about it. This isnot ‘complaining’. It is rather a means of improving the system for the student and future students.It is best to discuss this issue with one of the Senior Tutors; Dr Steven Burr, Dr Pam Hagan,Dr Jeanette Lilley, Dr Margaret Pratten & Dr Victoria Tischler.
AccessibilityTutors should understand the natural hesitancy of students to ‘bother them’. The earlymeetings are of importance in this regard in ensuring that tutors encourage their students to seekhelp when they feel they need it. Tutors and students should come to an arrangement as to thebest means of emergency contact. Students should recognise that tutors may not be able tosee them immediately, but will always try to do so within a reasonable time. If the tutor is notavailable ‘soon enough’ because of holidays etc, then the student must contact one of the SeniorTutors (see the Contact Details later in this booklet).
Tutors should be available to discuss examination results with their tutees in the first two years.
If a tutor cannot see the student to discuss exam results, the student should makealternative arrangements with their tutor and inform the Student Support & DevelopmentAdministrator of the alternative arrangements.
ConfidentialityTutees should be reassured that conversations with their tutors remain confidential. Therelationship is similar to that of doctor and patient. The only central record that will be made is thata meeting has taken place and this will be co-ordinated by the Medical Course Offices. Disclosure ofconfidential information, for instance to the Medical Course Offices, will only be made with theagreement of the tutee.
There may be extremely rare circumstances in which the tutor perceives an overriding need to passon information despite a lack of agreement from the tutee. This might occur in circumstancesrelating to ‘fitness to practice’. In such cases the tutor should inform the tutee of their intention and

45
initially seek advice from one of the Senior Tutors, the Medical Course Manager, or the AssociateDean for Medical Education.
There is a formal arrangement whereby the Clinical Sub-Dean will communicate details aboutstudents who will shortly qualify and become F1s to the Postgraduate Dean where there is aperceived need for special support in their F1 post.
Change of tutorOccasionally, despite everyone’s best efforts, the tutoring relationship might not flourish. Theremight, for example, be clashes of personality or difficulties in establishing a rapport. In suchcircumstances either the student or the tutor should feel able to contact one of the Senior Tutors orthe relevant Medical Course Office.
Practical IssuesWhen students first start, the geography of the Medical Schools, the campuses and the hospitals canbe quite confusing. If a student is uncertain where his/her tutor’s office is located then please feelfree to call your personal tutor directly, telephone numbers are given on the list of tutors. Failingthis, you may call into the Medical Course Offices for directions. Students from the same medicalfamily but in the year above can also help in this respect.

46
RESOURCES FOR MEDICAL STUDENTS

47
NOTES
RESOURCES FOR MEDICAL STUDENTS
Telephone numbers are as from the Medical School unless otherwise stated.
USEFUL CONTACTS
Nottingham Medical School School of Graduate Entry Medicine & Health(Derby)
DeanProfessor Ian Hall
0115 82 [email protected]
Head of SchoolProfessor Richard Donnelly
01332 724 [email protected]
Associate Dean forMedical EducationProfessor James Lowe
0115 82 30025/82 [email protected]
Director ofUndergraduate StudiesDr Danny McLaughlin
01332 724 [email protected]
Medical CourseManager and DisabilityLiaison OfficerMrs Judith Franklin
0115 82 30011/82 30008Ext 30011/[email protected]
School ManagerMrs Amanda Collett
01332 724 [email protected]
Quality AssuranceOfficerDr John Whittle
0115 82 [email protected]
Director of ClinicalSkillsDr John Frain
Director of ClinicalSkillsDr R Churchill
0115 82 [email protected]
Assistant Director ofMedical EducationDr Paul Garrud
01332 724 [email protected]
Assistant Director ofMedical EducationDr Reg Dennick
0115 82 [email protected]
Senior TutorDr Pam Hagan
01332 724 [email protected]

48
Clinical Sub-DeanDr Margaret Jones
0115 846 6919 (Primary Care)0115 927 2525 (Practice, Mon, Thurs, Friday)0115 82 [email protected]
Disability OfficerDr Pam Hagan
01332 724 [email protected]
Clinical Sub DeanMr Iain McVicar
0115 82 [email protected]
Examinations OfficerDr Richard Tunstall
Senior TutorDr Jeanette Lilley
0115 82 [email protected]
Head of PPDDr Sharon Conroy
01332 724 [email protected]
Senior TutorDr Margaret Pratten
0115 82 [email protected]
Module ConvenorsDr Gwen Hughes [email protected] Hannah Waterhouse [email protected] Richard Tunstall [email protected] Pam Hagan [email protected] Raheela Khan [email protected] Danny McLaughlin [email protected] Paul Garrud [email protected] Sharon Conroy [email protected] Saoirse O’Sullivan Saoirse.o'[email protected] Susan Anderson [email protected] Raheela Khan [email protected] Hannah Waterhouse [email protected]
Senior TutorDr Victoria Tischler
0115 82 [email protected]
Overseas StudentAdvisorDr Vince Wilson
0115 82 [email protected]
Overseas StudentAdvisorDr Jon Hardman
0115 82 [email protected]
PBL FacilitatorsMr Peter Jennings [email protected] Jennifer West [email protected] Fiona Moor [email protected] Robert Sword [email protected] Peter Cumberland [email protected] Katherine Britnell [email protected] Lorrain Pinnington [email protected] Nadeem Qureshi [email protected]
Administrative SupportNottingham Medical School
Administrative SupportSchool of Graduate Entry Medicine & Health

49
(Derby)
Office Opening Times: Monday 10.00am until 4.00pmTuesday 8.30am until 5.00pmWednesday 8.30am until 5.00pmThursday 8.30am until 9.30am
& 2.00pm until 6.00pmFriday 12noon until 2.00pm
Please respect office opening times and do notknock on the door when the office is closed. It
is imperative the staff are allowed someuninterrupted time to work.
Office Opening Times: Monday 9.30am until 4.30pmTuesday 8.30am until 4.30pmWednesday 9.30am until 1.00pmThursday 9.30am until 4.30pmFriday 8.30am until 1.00pm
Receptionist &AdmissionsAdministratorMrs Ruth Airey
0115 82 [email protected]
Course AdministratorMiss Sarb Atwal
01332 724 [email protected]
Admissions OfficerMrs Martine Lowes
0115 82 [email protected]
Admissions & FinanceOfficerMiss Cathy Porter
01332 724 [email protected]
Examinations OfficerMr Giorgio Vitale
0115 82 [email protected]
School AdministrativeOfficerMrs Anne-Marie Dwyer
01332 724 [email protected]
Clinical CourseCo-ordinator &Secretary to ClinicalSub DeansMrs Sue Hall
0115 82 [email protected]
School OfficeReceptionistMiss Victoria Burgoyne
01332 724 [email protected]
Student Support &DevelopmentAdministrator(Including PastoralCare)Mrs Claire Newbury
0115 82 [email protected]
IT OfficerNeill Magill
01332 724 [email protected]

50
TimetablingAdministratorMrs Jane Dewse
0115 82 [email protected]
Log Book & PortfolioEditorial AssistantMrs Michelle Mayer
0115 82 [email protected]
Occupational Health Occupational Health
Dr Ian Aston 0115 951 4331 Dr David Sherwood Jones 01332 868851
Career DevelopmentUndergraduate
Career Specialist Adviser Ms Jan [email protected]
Clinical Careers Leads
Secondary Care post vacant at time of printing – please contact Student Support Administrator
Primary Care Dr Caroline [email protected]
MCareer Soc [email protected]
Postgraduate
Deanery Careers Team
Foundation School Director Dr Bridget [email protected]
51
Senior Career Planning Advisor Ms Charlene [email protected]
http://www.eastmidlandsdeanery.nhs.uk/
http://www.foundationprogramme.nhs.uk/pages/home/your-career-path

52
Undergraduate Co-ordinators
The Royal Derby Hospital,Derby
Diane PfaffElaine Wright
01332 789258/01332 789259
[email protected]@Derbyhospitals.nhs.uk
King’s Mill Hospital,Mansfield
Val McCabe 01623 622515 x 4036 [email protected]
Lincoln County Hospital,Lincoln
Jeny Pell (CP3 Surgery)Khadine Cooper (CP3 SSM)Julie Evans
01522 512512 x 258701522 57319201522 512512 ext2587
[email protected]@[email protected]
Millbrook Hospital,Mansfield
Jan Allen 01623 784773 [email protected]
Nottingham City Hospital,Nottingham
Margarita Poulter & Rachael Tennant 0115 82 31832 (DDM31835)0115 9691169 x 34864
Pilgrim Hospital, Boston,Lincolnshire
Sue Warrant 01205 445333 [email protected]
Queen’s Medical Centre,Nottingham
Nick Kythreotis 0115 9249924 x 64759 [email protected]
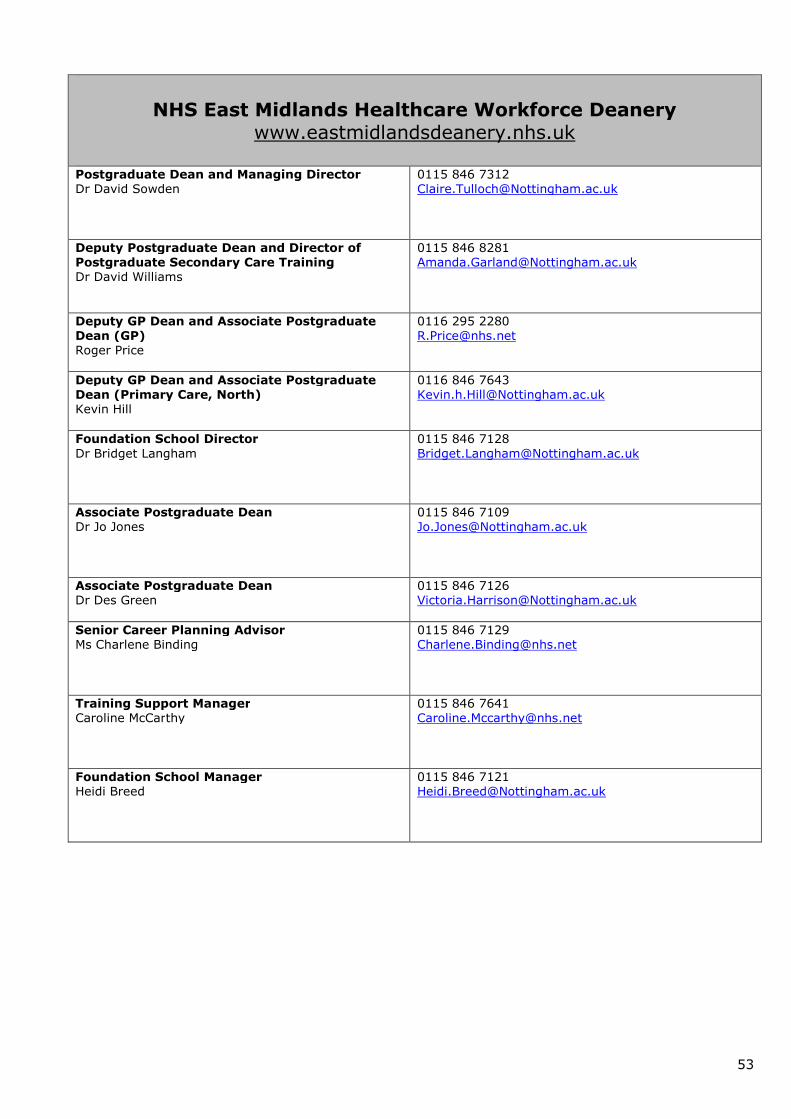
53
NHS East Midlands Healthcare Workforce Deanerywww.eastmidlandsdeanery.nhs.uk
Postgraduate Dean and Managing DirectorDr David Sowden
0115 846 [email protected]
Deputy Postgraduate Dean and Director ofPostgraduate Secondary Care TrainingDr David Williams
0115 846 [email protected]
Deputy GP Dean and Associate PostgraduateDean (GP)Roger Price
0116 295 [email protected]
Deputy GP Dean and Associate PostgraduateDean (Primary Care, North)Kevin Hill
0116 846 [email protected]
Foundation School DirectorDr Bridget Langham
0115 846 [email protected]
Associate Postgraduate DeanDr Jo Jones
0115 846 [email protected]
Associate Postgraduate DeanDr Des Green
0115 846 [email protected]
Senior Career Planning AdvisorMs Charlene Binding
0115 846 [email protected]
Training Support ManagerCaroline McCarthy
0115 846 [email protected]
Foundation School ManagerHeidi Breed
0115 846 [email protected]

54
FURTHER CONTACTS FORSUPPORT AND GUIDANCE

55
FURTHER CONTACTS FOR SUPPORT AND GUIDANCE
Student Services Centre
The Student Services Centre can provide you with information and support throughout your student life.They’re approachable, knowledgeable and most of all there to help. Go and see them if you know whatyou need or if there’s something you need to know.
The Student Services Centre is the home for Academic Support, the Disability Policy Advisory Unit,Financial Support, the majority of the Registry's front line services and Student Fees. We alsoprovide a front-line service for Graduation.
The Student Services Centre is based on Main Campus on B Floor of the Portland Building and A Floor ofthe Amenities Building at Jubilee.
Opening Hours
University Park Jubilee CampusMonday to Friday Monday to Friday
9.30am to 5.00pm 10.00am to 3.00pm
http://www.nottingham.ac.uk/ssc/
Student’s Union
Their mission statement
“To improve the experience of student life by providing quality service, representation anddevelopment opportunities for all our members.”
What they do
We represent over 35,000 students from over 140 different countries on campuses in the UK,Malaysia and China. We support 180 societies and 75 sports clubs as well as a theatre,magazine (Impact), award winning student-run radio station (URN) and fledgling TV station(NUTS). Our student fund-raising organisation, Karnival, is the largest in Europe and raised anenormous £688,458 for good causes in 2007. We also assist over 1,000 volunteers throughour Student Volunteer Centre.
To help you enjoy the social side of University life, we have a huge list of Union-run events atlocal night clubs and at our own newly refurbished venues, Mooch and The Venue. For moreday to day needs, we have Students’ Union shops at a number of sites and our own print shopand travel centre.
http://www.su.nottingham.ac.uk/

56
MEDSOC (The Medical Society)
The Medical Society is available to discuss any student/course related issues. They have allbeen through it before and so are probably the best people to ask! Tel: 0115 951 5151 ext43112.
“Student Voice” (ISC Chair) [email protected]
GEMSOC (Graduate Entry Medicine Society)
GEMSOC is available to discuss any student/course related issues.
www.gemsoc.org.uk
NIMS &Nottingham International Medics Society
The Nottingham International Medics Society (NIMS) aims to make the transition forinternational medical students to the course and life in Nottingham as smooth and fun aspossible! As you settle into your new environment, we will connect you to senior medicalstudents to give you guidance on everything UK, balancing life as an international withmedicine, maximizing your time and career opportunities in the UK, qualifying in your homecountry or places like Canada, US, Australia and others, and answering any questions youhave unique to your situation as you progress through the course! This is a great society foryou to meet and network with senior colleagues in your medical school and make contactsfrom all over the world! Get in touch by sending a quick hello to [email protected] andlet us know where you're from!
CELE (Centre for English Language)
For nearly twenty years, CELE have been providing study opportunities and support forinternational students, and teacher training programmes. Since its foundation, CELE hasgained a reputation as a student-centred organisation committed to empowering its studentsto succeed in their chosen academic and professional fields.
http://www.cele.nottingham.ac.uk/
University Counselling Service
The University Counselling Service is a free confidential service available to undergraduate andpostgraduate students and to all members of University staff.
http://www.nottingham.ac.uk/counselling/
Cripps Health Centre
The Cripps Health Centre has information relating to alcohol & drug use, as well as otherhealth issues.
www.crippshealthcentre.co.uk or Telephone: 0115 846 8888
Students who have concerns relating to alcohol or drug issues can, in the first instance discussthese with their GP at the Student Health Centre (Cripps), where they will be offered advice,assessment, information and advice about referral relating to alcohol or drug use.
57
Cripps Dental Centre
There is a Dental Centre for staff & students on main campus. Telephone: 0115 950 6781 or0115 951 3099 (extension 13099).
Nightline
This is a confidential telephone line for a friendly voice and information. It operates between7.00pm & 8.00am. It is available 24 hours a day during week one. Email:[email protected] Telephone: 0115 951 4985

58
The Department of Spiritual and Pastoral Care-QMC
The Multi-faith Centre at Queen’s Medical Centre Campus consists of the Chapel, Gurdwara, Mandir,Mosque and Synagogue, all situated on D floor, along the hospital corridor connecting the South and Eastblocks.
At City Campus the Chapel and Quiet room are on North corridor near purple entrance and there is aMuslim prayer room off South corridor.
Usually they are open day and night as places for quiet and prayer. You are very welcome to use any ofthem, whatever your beliefs – they are there for everyone.
Times for Prayer and Worship
Holy Communion is celebrated every Sunday at 10.00am in the Chapel. All welcome.
Roman Catholic Mass every Friday afternoon at 2.15pm.If you wish to attend either of these services please inform the nursing staff. If you need to be broughtin a wheelchair or bed please ask the staff to inform the chaplains. If you are unable to attend Chapeland would like to receive Holy Communion please ask; we are always willing to bring Communion to youon the ward.
Muslim Prayers (Juma Salaat) are said on Fridays at 1:30pm (summer) or 1:10pm (winter) in theMosque. Facilities for ablution and prayer mats are available.
The Derby Royal Hospital Faith Centre
GEM students and staff are welcome to use the Derby Royal Hospital Faith Centre at any time.This is located at the main hospital on level 1. Prayer rooms including washing facilities areavailable.
Faith Support & Advice – The University of Nottingham
University brings together people of many different backgrounds and faiths. It is an excellent place toreview, develop and celebrate your own beliefs, and to discover or explore the beliefs that are importantto other people. A number of resources are available to help you.
http://www.nottingham.ac.uk/chaplains/
EMERGENCIES – QMC
Fire - 2222 from a QMC switchboard phone, 74 2222 if using a University switchboardphone (in the Medical School)
Cardiac Arrest - Adult & Child 2222 from a QMC switchboard phone, 74 2222 if usinga University switchboard phone (in the Medical School)
Security/Police - Hospital security 63335 from a QMC switchboard phone for all QMCblocks except the Medical School. Whilst in the Medical School you must ring 13599 forUniversity security. Beeston Police Station can be contacted on 0115 943 0999 or a 999call can be made depending on the circumstances.
EMERGENCIES – UNIVERSITY CAMPUS
Please note; The Medical School, although based in the QMC uses the Universityswitchboard.

59
Fire, Police, AmbulanceCan be called from a University switchboard phone on 18888;(0115 951 8888 externally)
SecurityThe University Security Service is co-ordinated through the Control Office,Trent Building, Tel: 13599 (from a University switchboard), and is for problems oncampus and in the Medical School.
EMERGENCIES – GEM/THE ROYAL DERBY HOSPITAL BASE
Fire and non medical emergency
8888 (internal)
Serious Medical Emergency
9-999

60
Every attempt is made to keep the information contained in this booklet accurate andup to date.
If you have any comments, suggestions or amendments please contact:
Student Support & Development Administrator
Medical Course Office, B Floor, Medical School, QMC
Tel: 0115 82 30010