medtech insight › - › media › supporti… · 8 market snapshot: implantable pacemakers will...
TRANSCRIPT

FROM THE EDITORS OF: THE GRAY SHEET, CLINICA, START-UP AND MEDTECH INSIGHT NEWSLETTER
May 13, 2019
Pharma IntelligenceInformaInsight
Medtech Issue 143
medtech.pharmaintelligence.informa.com
COMMERCIAL
Boston Scientific’s Vici Venous iliac stent approved, p. 21
POLICY & REGULATION
CMS unveils favorable coding changes for medtech, p. 6
R&D
ASBrS releases mammography screening guidelines, p. 18
CONTINUED ON PAGE 11
3M Aims For Acelity In $6.7Bn Deal To Expand Wound-Care PresenceCATHERINE LONGWORTH [email protected]
I ndustrial conglomerate 3M Co. is pay-ing $6.7bn to buy Acelity LP Inc. and its KCI subsidiaries in an ambitious move
to expand its presence in the wound-care market.
San Antonio, TX-based Acelity, a maker of advanced wound-care products, gen-erated $1.5bn in revenue last year, with about 75% of sales in the Americas. 3M will acquire the company from a consor-tium of funds advised by Apax Partners and affiliates of Canada Pension Plan In-vestment Board (CPPIB) and the Public Sector Pension Investment Board (PSP
Investments) with cash along with pro-ceeds from the issuance of new debt. The deal comes after Apax, CPPIB and PSP Investments had been speaking with ad-visers about a potential public offering of Acelity, Bloomberg News reported.
In a 2 May conference call, Mike Roman, 3M’s CEO told investors Acelity's products were an ideal fit to 3M's health-care busi-ness and supported its growth strategy in the advanced wound-care market, which it is prioritizing as a key focus.
According to 3M, the advanced wound-care market is currently worth $8bn and
growing at mid-single digits, driven by rising rates of chronic health conditions such as obesity, diabetes and an aging population. That is in line with Informa's Meddevicetracker wound-care analyst report, which put the combined global market for advanced wound dressings and closure product at $7.7bn in 2017 and is expected to reach $10.6bn by 2022.
"Today, our advanced wound-care technologies include solutions that pre-vent the formation of wounds, prepare the wound for the beginning of the heal-

Stay up-to-date and get a complete view of the continually evolving medtech landscape with access to real-time market intelligence on product and company developments across the medical devices, diagnostics and advanced delivery systems markets.
Anticipate upcoming fi lings, clinical trials dates and data, and access market size information and expert forecasts all in one place, helping you assess the competition, track key events and make better-informed decisions.
Meddevicetracker: Medical Device Intelligence and Forecasts
To fi nd our more visit: ph armaintelligence.informa.com/Meddevicetracker
JN0000 MDT Advert US Letter.indd 1 2018/11/19 11:50

medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 3
inside:Cover / 3M Aims For Acelity In $6.7Bn Deal To Expand
Wound-Care Presence – 3M is betting big on wound-care maker Acelity, paying $6.7bn to buy the firm and its KCI subsidiaries in 3M's largest acquisition to date.
EDITORS' PICKS 5 Breast Implant-Makers Now Required To File Individual
Reports On Each Adverse Event, FDA Says – The agency is requiring manufacturers to file individual Medical Device Reports for each adverse event regarding implants – part of a bigger effort to end its Alternative Summary Reporting Program for all devices.
6 CMS Head Verma Unveils Favorable Coding Changes For Medtech, Pharma At MDMA Meeting – The US Centers for Medicare and Medicaid Services will allow device manufacturers to submit requests for HCPCS codes for emerging technology on a semi-annual basis.
7 John Wilkinson Stepping Down As UK MHRA Devices Director – The UK regulatory agency will now be losing two of its top-level executives this year.
8 Market Snapshot: Implantable Pacemakers Will Reach $5.3Bn by 2023 – Global sales of pacemakers are expected to reach $5.3bn by 2023, a CAGR of 5.1% from $4bn in 2017, driven largely by the rising prevalence of heart disease.
POLICY & REGULATION 9 UK Plan To Speed Access To ‘Cutting-Edge’ Products –
Changes are being made to the UK’s Accelerated Access Collaborative to help streamline access to ground-breaking medicines and diagnostic tools in areas like dementia, diabetes and cancer.
10 Preferential Treatment: US FDA Asks Patients For Their Input – As the agency continues to incorporate more patient-preference data into its regulatory process, it is asking stakeholders on the kinds of diseases and other factors it should consider when evaluating patient-preference information.
12 Rolling On: EU Makes Good Progress On Structures For New Regs Implementation – The European Commission
explore more:exclusive online contentPacemaker battery concernshttps://bit.ly/2vJA2XT
The US FDA is cautioning people implanted with particular Medtronic pacemakers to pay close attention to their device's battery level after the agency received reports of unexpected battery depletion – including one that led to a patient's death.
Resilia proves resilienthttp://bit.ly/2DTXWEt
Four-year data from the COMMENCE trial of surgical valves made of Resilia bovine pericardial tissue showed no early or late structural valve deterioration or valve thrombosis.
Execs On The Movehttps://bit.ly/2V6G8fi
Mologic’s new CMO brings program experience from Gates Foundation; former NuVasive exec is named chief commercial officer at vascular device firm Shape Memory Medical; EVP is promoted to CEO at blood products company Terumo BCT; and more.
Medtronic SCS trialhttp://bit.ly/2H8pJBS
Most patients treated for chronic leg and back pain with Medtronic’s Intellis spinal cord stimulator with the Evolve workflow in the Vectors study showed improved symptoms and function.
Approvals snapshothttp://bit.ly/2WvU1VM
The US FDA approved Boston Scientific’s Vici Venous iliac vein stent system (see related story on p. 21), and SentreHEART announced it received a CE mark for the 50mm version of the Lariat-RS system for left atrial appendage exclusion in patients with atrial fibrillation.
medtech.pharmaintelligence.informa.com
19 9 12

4 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
Medtech insightSHAWN M. SCHMITT @[email protected]
REED MILLER @[email protected]
AMANDA MAXWELL @MEDTECHAMANDA [email protected]
MARION WEBB @[email protected]
SUE DARCEY @MEDTECH_INSIGHT [email protected]
FERDOUS AL-FARUQUE @[email protected]
ELIZABETH ORR @[email protected]
CATHERINE LONGWORTH @[email protected]
ASHLEY YEO @[email protected]
MAUREEN KENNY @[email protected]
NEENA BRIZMOHUN @[email protected]
VIBHA SHARMA @[email protected]
ANDREA CHARLES CUSTOM [email protected]
JANET HANIAK SENIOR DESIGNER
GAYLE REMBOLD FURBERT DESIGN SUPERVISOR
RICHARD FAINT HEAD OF [email protected]
PHIL JARVIS MANAGING DIRECTOR
TO SUBSCRIBE, VISITmedtech.pharmaintelligence.informa.com
TO ADVERTISE, [email protected]
EDITORIAL OFFICE:601 Third Avenue, New York, NY 10158 US phone 212-520-2700
CUSTOMER CARE: [email protected] Toll-Free . . . . . . . . . . . . . . . . . . . . . . . . . . . .+1 888 670 8900US Toll . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .+1 908 547 2200UK & Europe . . . . . . . . . . . . . . . . . . . . . . . . +44 (20) 337 73737Australia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .+61 2 8705 6907Japan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .+81 3 6273 4260All stock images in this publication courtesy of www.shutterstock.com unless otherwise stated© 2019 Informa Business Intelligence, Inc., an Informa company. All rights reserved.No part of this publication may be reproduced in any form or incorporated into any information retrieval system without the written permission of the copyright owner.
has updated its EU MDR and IVDR implementation Rolling Plan to reflect the latest developments on the much-needed structures for implementing the new Regulations.
13 Day 1: US FDA Launches New 'Super Office,' Says It’s Already Proven Its Worth – At MedCon 2019, CDRH Director Jeff Shuren announced 1 May is officially the first day for the agency’s new Office of Product Evaluation and Quality.
14 ‘Disease Doesn’t Respect Silos’: Sharpless Sets Flexibility As Priority – Acting US FDA Commissioner Ned Sharpless described his vision for an efficient, adaptable agency.
14 Guidance Advises Orthopedic Firms On How To Characterize, Test Plastic Materials – Newly finalized guidance from the US FDA explains how the agency characterizes ultrahigh molecular weight polyethylene (UHMWPE) used in orthopedic products
15 Canada Finalizes Guide On Evidence Needed To License 3D-Printed Implants – Health Canada has finalized guidance representing the first phase of its 3D-printing policy.
QUALITY CONTROL & COMPLIANCE 16 Compliance Corner: When Is An Action Exempt From
FDA's Recall Reporting Requirements? – Two longtime industry experts break down the US FDA’s rules around when an action becomes reportable as a recall to the agency.
17 Q1 Recalls Snapshot: Device Corrections & Removals Are Down, But Recalls Of High-Risk Class I Units Remain A Concern – Corrections & removals of medical devices were down 41% in the first quarter of 2019, the lowest number of recalls recorded in a quarter since Q4 2017.
R&D 18 American Society Of Breast Surgeons Releases First
Mammography Screening Guidelines – The ASBrS released its first mammography screening guidelines.
19 Higher Doses Of Novocure’s TTF Help New Glioblastoma Patients – The first reported analysis demonstrating a patient-level dose response with Novocure’s Tumor Treating Fields therapy is now published.
20 Exec Chat: John Frels, VP Of Research And Development, Abbott Diagnostics – Medtech Insight caught up with Abbott's John Frels to find out more on his approach to leading innovation and growth at the company.
COMMERCIAL 21 FDA Approves Boston Scientific's Vici Venous Iliac Stent –
The approval is based on VIRTUS trial results.
21 Biotronik Begins US Rollout Of PK Papyrus For Coronary Perforations – The US FDA granted PK Papyrus a humanitarian device exemption (HDE) in late 2018, the first FDA approval of a device to treat coronary perforations since Abbott's Jomed Jostent earned an HDE in 2001.
medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 5
� E D I T O R S ’ P I C K S �
Breast Implant-Makers Now Required To File Individual Reports On Each Adverse Event, FDA SaysSUE DARCEY [email protected]
S ilicone and saline breast implant manufacturers need to file individual reports about any adverse events associated with the devices as part of broader measures being taken
by the US Food and Drug Administration to protect women.Amy Abernathy, FDA principal deputy commissioner; and
Jeff Shuren, director of the Center for Devices and Radiological Health, said on 2 May that the agency is taking steps to ensure women have access to all the information they need on the risks of breast implants.
The move is in part due to concerns raised by patients and rec-ommendations from CDRH advisors during a 25-26 March FDA General and Plastic Surgery Devices Advisory Committee meet-ing on the implants. (Also see "'Do Your Job': To The Dismay Of Pa-tients, FDA Panelists On Breast Implants Advise Better Risk Warnings, Not Recalls" - Medtech Insight, 27 Mar, 2019.)
Now silicone and saline breast implant-makers will need to file individual reports on any adverse events associated with the de-vices to FDA’s publicly available Manufacturer And User facility Device Experience (MAUDE) database.
“This is part of a larger effort to end the Alternative Summary Reporting Program for all medical devices, which we intend to complete in the coming weeks,” Abernathy and Shuren said in their announcement.
The FDA's Alternative Summary Reporting Program, which al-lows firms to submit abbreviated reports in a summarized, line-item format, was established in 1997 in an effort by the agency to review adverse events more efficiently for well-established risks. Quick, short summary reports however, were never allowed for pa-tient deaths, and unusual, unique or uncommon adverse events.
Abernathy and Shuren argue the move to individualized event reports will make the descriptions of device-related events more transparent. However, they cautioned: “Generally, the number of reports received cannot be used to determine the frequency with which a particular adverse event occurs.”
FDA recently sent warning letters to Mentor Worldwide LLC and Sientra Inc., makers of the MemoryShape and Sientra breast implants. The warning letters focused their failure to comply with post-approval study orders issued by FDA in 2013. The firms were required to enroll thousands of women who received breast im-plants in long-term studies but both failed to do so, according to the agency. (Also see "Warning Letter Roundup & Recap – March 19, 2019" - Medtech Insight, 19 Mar, 2019.)
MORE EDUCATION COMING ON BII, BIA-ALCL, TEXTURED IMPLANT RISKS“Moving forward, we plan to regularly communicate informa-tion we receive through Medical Device Reports about systemic
symptoms experienced by patients with breast implants,” Aber-nathy and Shuren said in their statement.
The agency says it will also communicate more about some re-actions to implants women are reporting for what physicians are calling “breast implant illness,” including chronic fatigue, cogni-tive issues, joint and muscle pain.
The FDA pointed to the growing discussion in regulatory agen-cies around the world, which have been considering the risk of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL), as well. BIA-ALCL is a relatively rare disease; a type of non-Hodgkin’s lymphoma that can lead to death if not treated.
INTERNATIONAL BANS SEEN ON TEXTURED BREAST IMPLANTS“A few of our international counterparts have started to initi-ate actions to ban or restrict sales of some textured breast implants, based on concerns about BIA-ALCL,” Abernathy and Shuren said.
Among those counterparts are regulatory agencies in France and Canada, who are particularly worried about the risks of tex-tured implants and their connection to BIA-ALCL. Manufacturers like to make the implants textured so they are less likely to slide around after implantation. French regulator ANSM suspended the sale of macro-textured and polyurethane-coated breast im-plants on 4 April, while Health Canada told breast implant-maker Allergan the same day it was planning to suspend licenses for the firm’s Biocell implants as a precautionary measure. (Also see "France Bans Breast Implants Linked To Rare Cancer; Canada Close Behind" - Medtech Insight, 8 Apr, 2019.)
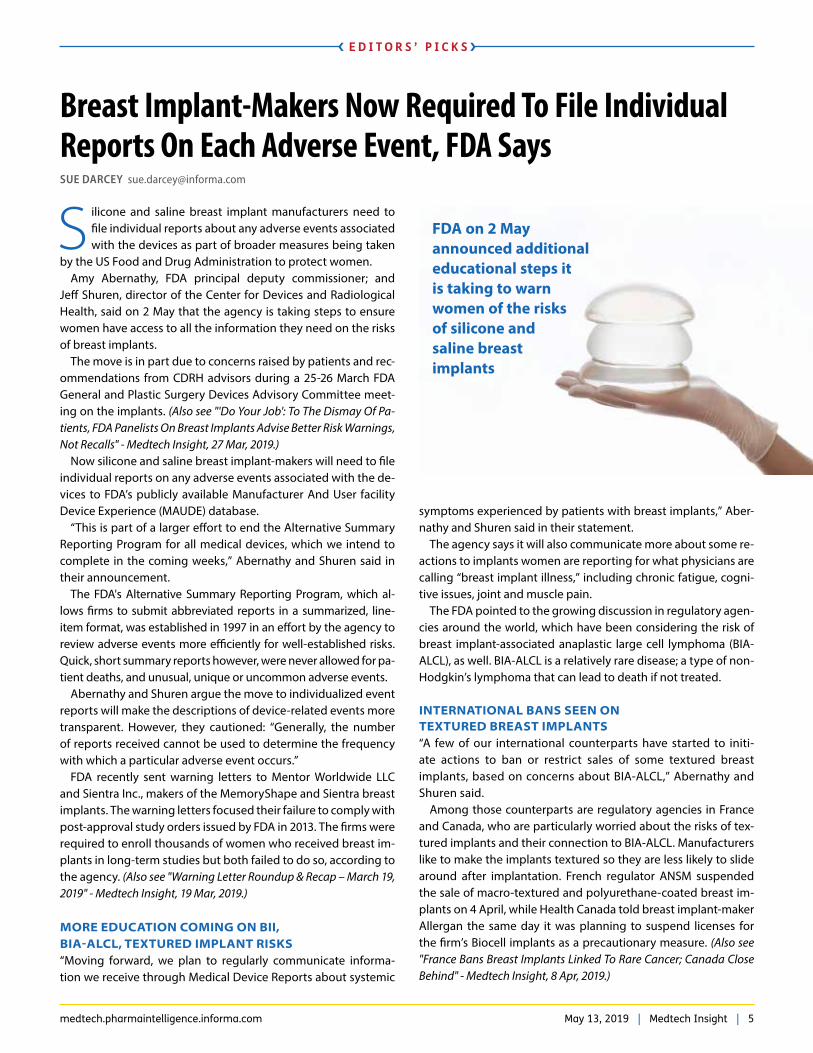
FDA on 2 May announced additional educational steps it is taking to warn women of the risks of silicone and saline breast implants

6 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
� E D I T O R S ’ P I C K S �
The FDA sent a letter about the risks of BIA-ALCL on 6 February to US medical specialists who may advise or work with patients interested in – or who already had – breast implants, in addition to OB/GYNs, plastic surgeons, general practitioners, physician assistants and nurse practitioners who are generally thought of as advising breast implant patients. (Also see "US FDA Issues Addi-tional Warnings On Breast Implants" - Medtech Insight, 12 Feb, 2019.)
“We are aware there are some health-care professionals – such as dermatologists, internists and pathologists, who may not be fully aware of all breast implant risks,” Abernathy and Shuren said.
BOXED LABELS, PATIENT DECISION CHECKLISTS PUSHEDThe FDA is also considering changes to the labeling on the im-plants (which only surgeons and other health-care providers would see) to make it a boxed warning and will push manufac-turers harder to deliver patient decision checklists – which breast implant manufacturing companies have been required to supply for many years – along with the implants.
Physicians and surgeons advising patients on the implants and their related risks are supposed to sit down with their patients and go through the checklists with them, but several speakers who had recently obtained their implants and contracted breast implant illnesses testified at the March FDA advisory committee meeting that they had never heard of the checklists, nor seen them.
FDA URGES MORE USE OF BREAST IMPLANT REGISTRIESFDA officials also emphasized the need for health-care profes-sionals to contribute more to patient data registries.
“Partnering with registries, such as the Patient Registry and Outcomes for Breast Implants and ALCL Etiology and Epidemi-ology (PROFILE), which collects real-world data on patients with BIA-ALCL diagnoses, and the new National Breast Implant Regis-try (NBIR), is one way in which we seek to gain greater insight and more comprehensive information about women’s experiences with breast implants,” Abernathy and Shuren said.
They added that the data already made available to the FDA from the PROFILE registry provided additional information about patients diagnosed with BIA-ALCL.
“However, more needs to be done to increase the number of health-care professionals in contributing to the registries. ... FDA continues to encourage stakeholders that have organized these registries to expand provider participation,” Abernathy and Shuren added. They note a good way to do this is for physicians, physician assistants and nurses to seek additional information from providers on the patient’s family history of autoimmune disorders and details of past operations.
Published online 3 May 2019
CMS Head Verma Unveils Favorable Coding Changes For Medtech, Pharma At MDMA MeetingSUE DARCEY [email protected]
U S Centers for Medicare and Medicaid Services (CMS) Ad-ministrator Seema Verma says the agency will now accept HCPCS (Healthcare Common Procedure Coding System)
coding requests for new technology twice a year. The agency chief made the announcement on 2 May at a Medical Device Manufac-turers Association (MDMA) annual meeting in Washington, DC.
Verma added that the agency will also accept submissions for codes for new pharmaceuticals on a quarterly basis. Formerly, the agency only reviewed the HCPCS coding requests for devices and drugs once a year.
“We expect this will greatly improve the ability of innovators to accelerate through the adoption curve,” Verma said.
In addition, CMS now wants regional Medicare Administrative Contractors, or MACs, to stop automatically “non-covering” tech-nologies with III CPT (Current Procedural Terminology) codes, and to instead run localized requests for coverage through the full local coverage determination (LCD) process, which requires stakeholders’ input.
These reforms were sought in legislation in the last congres-sional session, H.R. 3635, the “Local Coverage Determination
Act,” introduced by Reps. Ron Kind, D-WI, and Lynn Jenkins, R-MO. (Also see "US House Panel Passes Bill To Bring More Trans-parency To Local Coverage Determination Process" - Medtech In-sight, 6 Sep, 2018.)
“Coverage, coding and payment determinations are not al-ways made in a particular sequence,” the CMS administrator explained. “This can lead to unpredictable pathways for innova-tors with respect to review timelines and engaging with CMS. In-novators and other external stakeholders have therefore asked for better harmonization of these determination – and for more transparency into our processes.
“We’re working to enhance transparency and inter-agency co-ordination for innovators navigating CMS,” Verma added.
AT CMS, BREAKS FOR DEVICE-MAKERS JUST KEEP COMINGThe 2 May CMS decisions added to the good news for medtech manufacturers revealed by the agency last week. CMS an-nounced it will waive the requirement for “substantial clinical improvement” for FDA Breakthrough Devices Program prod-

medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 7
� E D I T O R S ’ P I C K S �
ucts for two years after they submit their requests for coverage to the agency, and those products will get automatic CMS re-imbursement. (Also see "Breakthrough Devices To Get Special US Medicare Reimbursement Under CMS Proposal" - Medtech Insight, 24 Apr, 2019.)
In announcing the decisions, Verma said the CMS will provide enhanced guidance on how its processes sync with those for FDA device approvals. She noted that the agency is “actively working with the FDA even before devices are approved to expedite cov-erage opportunities for Medicare beneficiaries.”
The CMS administrator said she had numerous conversations with former FDA Commissioner Scott Gottlieb on the issue, “and I’m looking forward to working together with acting Com-missioner [Ned] Sharpless,” she said. (Also see "‘Disease Doesn’t
Respect Silos’: Sharpless Sets Flexibility As Priority" - Medtech In-sight, 2 May, 2019.)
CMS WORKS WITH CONGRESS“We are also working with Congress on a raft of legislative chang-es to address the challenges we face in adapting the Medicare program to modern technology,” Verma said.
She reminded the MDMA audience that President Trump's 2020 budget request proposes expanding coverage of disposable de-vices, such as innovative glucose monitors and insulin pumps that substitute for durable devices. The monitors and pumps are used in the management and treatment of diabetes.
Published online 2 May 2019
John Wilkinson Stepping Down As UK MHRA Devices Director NEENA BRIZMOHUN [email protected]
J ohn Wilkinson is to retire as direc-tor of devices at the UK Medicines and Healthcare products Regulatory
Agency at the end of October, just weeks after Ian Hudson, the MHRA’s chief execu-tive, is due to leave the agency.
The MHRA announced today that Wilkinson was stepping down from his role. Hudson’s plan to leave the agency in September for personal and profes-sional reasons was announced last No-vember. (Also see "UK Agency Boss Hud-son Leaves Brexit Challenge To Successor" - Pink Sheet, 20 Nov, 2018.
Both executives are leaving the MHRA as it continues to prepare for the UK’s de-parture from the EU. The Brexit deadline has been postponed to 31 October, but it could be earlier if a withdrawal deal is agreed before then.
With regard to the MHRA finding a new director of devices, “this is currently un-der consideration,” a spokesperson for the agency told Medtech Insight. “How-ever, we will ensure that an appropriate handover of John’s work within the ex-isting workforce takes place before he leaves at the end of October,” the spokes-person added. Last year, the MHRA said recruitment for Hudson's successor was
expected to begin in early 2019.Wilkinson has been with the MHRA
since February 2012. “Since that time, he has made a significant contribution to the work of the organization, both nationally and internationally,” the agency said.
Among his achievements, the MHRA said, is that he “championed the devel-opment” of the new EU medtech legis-lation: the Medical Device Regulation (2017/745) and the In Vitro Diagnostic Regulation (2017/746).
Both regulations entered into force on 25 May 2017. Wilkinson will leave the agency before the transition periods end for each regulation: the MDR and IVDR will fully apply on 26 May 2020 and 2022, respectively.
Wilkinson has also chaired the EU’s Competent Authorities for Medical De-vices (CAMD) executive group, which seeks to enhance collaboration between the member states and the European Commission in developing and manag-ing Europe’s medical devices regulatory system, the MHRA noted.
In announcing his retirement, Wilkin-son said: “These decisions are never easy to make, and with a very heavy heart, I have now decided to step down
from my role at the agency. I felt that now was the right time for me to move on to the next stage of my life. These last seven years have been a wonderful experience for myself and I am proud to have been associated with, and worked for, the regulator.”
Before joining the MHRA, Wilkinson was chief executive of Eucomed, the European medical technology industry association.
His earlier experience included the po-sition of director general of the Associa-tion of British Healthcare Industries and a number of roles in the medical device industry, in both the UK and the US, with Becton Dickinson and the BOC Group. These were followed by a period as chief executive of an early-stage medical im-aging company.
Wilkinson was awarded an OBE for ser-vices to the medical devices industry in the 2010 New Year’s honors list.
Published online 1 May 2019

8 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
� E D I T O R S ’ P I C K S �
Source: Meddevicetracker: Interventional Cardiology, Implantable Pacemaker Products Design Credit: Janet Haniak
The global market for implantable pacemakers will reach $5.3bn by 2023, a CAGR of 5.1% from $4bn in 2017 and is driven in large part by the rising prevalence of heart disease worldwide and rising demand for better health-care services in emerging markets.
MARKET SNAPSHOT:
PACEMAKERS
GLOBAL PACEMAKER SALES ($M)
CRT-P
Single-Chamber
Dual-Chamber$2,979.8
$704.9
$3,942.4
$1,014.4
$255.60
$367.40
� 2017 � 2023
CAGR 4.8%
CAGR 6.3%
CAGR 6.2%
Will remain the dominant devices, but see moderate growth by 2023
Largest growth segment by 2023
Second-largest growth segment by 2023
Expected procedural growth of implantable pacemakers in the US
212,000 230,000
2017 2023
Procedure Cost (insured)$9,600-$19,700
High Device Cost$3,000-$11,000
Device Longevity5-15 years
LIMITERS
Implantable pacemakers growth (estimated sales RoW, excludes US, Japan and 5EU countries, $m)
1,161.7 2,267.4
2017 2023
CAGR 11.8%
PACEMAKER MARKET IS DOMINATED BY THREE PLAYERS
MEDTRONIC47.5% $1,872.3m
ABBOTT24.0% $946.4m
BOSTONSCIENTIFIC
12.1% $476.7m
OTHERS16.4% $644.0m
MARKET SHARE 2017 Revenues
Makers of leadless pacing systems on the market
Leadless pacemakers are single-chamber devices. Most patients require dual-chamber pacing to continuously regulate both chambers on the right side of the heart.
Concerns with Abbott's Nanostim leadless pacing system
Battery Failure
LostTelemetry

medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 9
� P O L I C Y & R E G U L A T I O N �
UK Plan To Speed Access To ‘Cutting-Edge’ ProductsIAN SCHOFIELD [email protected]
T he UK government says that cutting-edge medicines, di-agnostic tools and digital services will be made available on the national health service (NHS) more quickly as a
result of improvements to the Accelerated Access Collaborative.The AAC, which was set up in 2018 to speed up access to
ground-breaking products for conditions like cancer, dementia and diabetes, is to become the new “umbrella organization for UK health innovation.”
It will act as the “front door” for innovative companies seeking to have their products funded by the NHS, and will “provide support to overcome barriers that can prevent the best medical innova-tions from reaching patients,” the government said. A new unit will be established in NHS England and NHS Improvement, led by Sam Roberts, NHS England’s director of innovation, as chief executive.
The revamped AAC was announced on 2 May by health minister Nicola Blackwood, who said: “I want the NHS to be at the forefront of cutting-edge treatments and medical innovations – but often it can take too long for products to get from the bench to the bedside.”
She said the AAC would now be able to speed up this process “so patients and the NHS can be the first in the world to benefit from the most transformative technologies and treatments as part of our Long Term Plan.”
In its new incarnation, the AAC is intended to implement a system that can identify the best new innovations, “make sure the NHS is ready to make use of them,” and help the service adopt clinically and cost-effective innovations more quickly, the government said.
It will also set up a “globally leading testing infrastructure” that allows innovators to “generate the evidence they need to get their products into the NHS.”
These moves will complement efforts that have already been made to bring the NHS into the “horizon scanning” system and ensure that it is prepared for highly innovative products coming down the pipeline so that they can be made available to patients as quickly as possible, as part of the new voluntary pricing and access scheme that took effect at the beginning of this year. (Also see "ABPI Exec Lauds Innovation And Access Provisions In New UK Voluntary Scheme" - Pink Sheet, 29 Apr, 2019.)
Other objectives of the revamped AAC are:• To provide a single point of call for innovators working
inside or outside the NHS, so that they can “understand the system and where to go for support.”
• To signal the needs of clinicians and patients “so innovators know which problems they need to solve.”
• To oversee a health innovation funding strategy that “ensures public money is focused on the areas of greatest impact for the NHS and patients.”
Blackwood presented the changes at today’s conference of the Association of the British Pharmaceutical Industry, one of the member organizations of the AAC. Speaking ahead of the event,
ABPI CEO Mike Thompson said: “This is a real step forward in making sure UK patients get the latest breakthrough treatments. It sends a clear message that the UK intends to build an inno-vation-led economy alongside a more productive, innovation-ready NHS. We fully support Sam Roberts in making this a huge success that will change the lives of patients in the UK.”
HOW THE AAC WORKSAccording to health technology assessment body NICE, which hosts the AAC’s secretariat, key areas of interest for the collab-orative include products that have evidence of clinical and cost effectiveness, address a significant unmet need, treat large pop-ulations or have a high budget impact, or enable a novel mode of action or “significant changes to the care pathway.”
Products designated as high potential will receive additional support, advice and direction from the AAC, with a “tailored package of support with dedicated case management,” NICE says. This support includes running processes in parallel, gener-ating real-world evidence, the potential for flexible commercial arrangements, and pathway transformation to drive adoption of products by the NHS.
Last year, the AAC identified 12 “rapid uptake” products in seven high-potential technology areas that were to be made available more quickly to enable patients with conditions such as cancer, heart disease and multiple sclerosis to gain early access to them. NHS England said that these products “could improve the lives of around 500,000 patients and save the NHS up to £30m.”
They are as follows:• HeartFlow Inc's HeartFlow Analysis for estimating fractional
flow reserve from coronary CT angiography.• Roche Diagnostics' Elecsys immunoassay and Quidel's Triage
PIGF test for early diagnosis of suspected pre-eclampsia.• Roche Diagnostics' Elecsys Troponin and Abbott Diagnostics'
Architect STAT for early ruling out of myocardial infarction.• MAST Diagnostics' OC Sensor, Alpha Laboratories' HM-JACK-

10 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
� P O L I C Y & R E G U L A T I O N �
arc and Sysmex's FOB Gold fecal immunochemical tests for colorectal cancer.
• Teleflex's Urolift device for relieving painful urinary tract symptoms of benign prostatic hyperplasia.
• Sanofi’s alirocumab and Amgen’s evolocumab for primary hypercholesterolemia and mixed dyslipidemia.
• Merck’s Mavenclad (cladribine) for highly active relapsing-remitting multiple sclerosis.
The AAC was launched last year in response to the indepen-dently chaired Accelerated Access Review published in 2016, with the aim of making the process of getting transformative technologies to patients quicker, cheaper and easy for both in-novators and the NHS.
Its member organizations include the ABPI, the BioIndustry Association, the Association of Medical Research Charities, NHS England, the UK medtech industry group, the Association of British HealthTech Industries, and the Academic Health Sci-ence Networks (AHSN).
In March the AHSN launched a new MedTech Landscape Re-view to signpost and explain the NHS's adoption pathways and its various tools and programs, in an effort to point the way for manufacturers who want to access the service. (Also see "UK Medtech Industry Points The Signpost At Better Adoption of Innova-tion " - Medtech Insight, 4 Apr, 2019.)
Published online 2 May 2019
PREFERENTIAL TREATMENT:
US FDA Asks Patients For Their InputFERDOUS AL-FARUQUE [email protected]
T he US Food and Drug Administration wants public input that could allow patients to have more influence over the kinds of products they want to have access to.
While the agency has the final say on what devices get to mar-ket, regulators have been tasked with figuring out how to incor-porate more patient preference into their decision-making un-der the most recent user-fee deal.
On 2 May, the FDA asked stakeholders to give their thoughts on a new priority list of patient preference-sensitive areas that could be used to inform sponsors and the agency on how to de-sign and conduct trials, the acceptable benefit-risk threshold of a given product and postmarket evaluations.
"What we're looking at are those areas in technology where the patient perspective, their preferences, has a big impact on whether or not they would use that technology,” said Jeff Shuren, director of the FDA's Center for Devices and Radiological Health (CDRH), during a 2 May meeting at the Reagan-Udall Founda-tion in Washington, DC. “Those are the areas then we will devote more scientific endeavors to understand those perspectives and then to incorporate it in not only our decision-making, but hope-fully also in product development – that's the goal."
The list was developed based on patient input, and the agency hopes to provide feedback on what they learn within the coming year.
The FDA has opened a docket to get input from patients, pro-viders, academia, industry and others that could help it refine the list of patient preference-sensitive areas. The list is broken into such categories as what do patients value in diagnosis and treat-ments, and relevant clinical endpoints for specific patients. The list is also broken down by medical specialties such as cardiology, oncology and endocrinology.
“Patients are the experts in living with their disease or con-dition, the outcomes that are most important to them, and
how they weigh benefits and risks,” said Shuren in an agen-cy statement announcing the docket. “Through our Patient Preference Initiative, we’ve committed to seeking patient input on these types of topics to help inform our regulatory decision-making.
“Through better collection and understanding of information that matters to patients, we can ensure our evaluation through-out the life cycle of a medical device includes a better reflection of the patient experience,” he added.
The FDA is also asking if there are any topics on the list that need to be refined to better address certain areas. Regulators also want to know if there are areas they missed, and if there are ongoing studies or published studies that adequately address the preference-sensitive areas on the list.
“The list posted today seeks input on several parameters the agency can use to identify patient preference-sensitive areas to
Michael McCaughan (left) speaking with CDRH Director Jeff Shuren at the Reagan-Udall Foundation for FDA on 2 May
Sour
ce: F
erdo
us A
l-Far
uque

medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 11
� P O L I C Y & R E G U L A T I O N �
incorporate into medical device review, such as significant public health impact; areas where patients may value the benefits and risks of a technology or treatment differently from health-care professionals and/or caregivers; and areas where population-level differences in patient perspectives are not well understood due to a variety of factors,” said the agency.
Publishing the list fulfills the FDA’s obligations under the Medi-cal Device User Fee Act IV the agency negotiated 18 months ago with industry. (Also see "MDUFA IV (And More) Is Law: Trump Signs A Health-Care Bill" - Medtech Insight, 18 Aug, 2017.)
EVOLUTION OF PPI, STATISTICAL THRESHOLDS Patient-preference information (PPI) has been a hot topic over the past few years, and the Medical Device Innovation Consor-tium – a private-public group of medtech stakeholders – has been an integral part of that conversation.
The group has engaged the FDA and other major medtech players as the agency has started to shift its thinking to look be-yond traditional statistical thresholds and in evaluating other factors such as PPI. Over the past few years it has been working to come up with ways to change the regulatory regime in a way that is considered more encompassing and also develop statis-tical methods that can use less data. (Also see "New MDIC CEO Talks NEST, Case For Quality, CMS, And More" - Medtech Insight, 24 May, 2018.)
In early 2015, for the first time, FDA approved EnteroMedic’s Maestro implant to treat obesity that had not met its efficacy re-quirements. It is a pacemaker-like device that uses vagal block-ing therapy by stimulating the vagus nerve, which regulates the digestive system and helps suppress hunger.
The agency’s decision was based on data where patients said they accepted that the device might not work for them and there may be risks associated with not being able to use the device in conjunction with MRI scans, but they would still prefer to try it.
(Also see "EnteroMedics Eyes First Commercial Maestro Implants For Obesity After Months Of Prep" - Medtech Insight, 7 Apr, 2015.)
The approval came after the FDA finalized a guidance in the fall of 2016 on using patient-preference data to review premarket applications. The agency outlined how sponsors could use such data as well as input from providers in their submissions that would persuade it to approve or clear a product, even when it doesn’t meet its traditional safety and efficacy thresholds. (Also see "Final Guidance Encourages Use Of Patient Preference In Device Applications" - Medtech Insight, 25 Aug, 2016.)
The CDRH also announced recently it is launching patient-per-spective studies that will look at patient-preference information (PPI) and patient-reported outcomes (PRO). (Also see "The Patient Perspective: Upcoming US FDA Device Center Studies Put Device-Users In Front Seat" - Medtech Insight, 25 Apr, 2017.)
Patients will report their health status directly in the PRO stud-ies and in the PPI studies by providing information on the risk-benefit trade-offs of products under review.
The concept of using more patient-preference data to make regulatory decisions also aligns with a draft guidance, issued last year, that calls on reviewers to look beyond traditional p-values when determining whether a product meets the FDA’s regula-tory thresholds.
The guidance seeks to help agency staff decide whether the level of uncertainty presented by sponsors is reasonable based on scientific factors other than a clinical trial's p-values to deter-mine if the product should be allowed on the market. (Also see "Shuren: New Uncertainty Draft Guidance Looks Beyond p-Values" - Medtech Insight, 6 Sep, 2018.)
Stakeholders interested in commenting on FDA’s list of patient preference-sensitive areas can do so on www.regulations.gov under docket No. FDA-2019-N-1619 until July 2.
Published online 3 May 2019
ing process and protect the wound while it heals. This acquisition will help us to build out these solutions and expand our offerings, enabling us to provide greater value across the entire care pathway for patients and health-care providers. It will also allow us to apply our fundamental strengths to create unique value, espe-cially around our global reach and tech-nology development," said Roman.
3M said Acelity's approach of targeting under-penetrated segments of the market held significant opportunities for growth.
"There's new segments [in the market] such as post-acute which is growing and
a large opportunity and very low pen-etration there and we have significant opportunities," said Roman. "Geographi-cally there's an opportunity to expand and penetrate as well. And the value of this treatment and this care pathway has been proven across multiple markets. We think the opportunity to drive greater penetration and growth off of that is an important part of the coming few years."
3M, which makes Post-it notes and other consumer products will be banking on the acquisition to help turn around its struggling business. Last week the com-pany posted poor earnings and slashed its 2019 earnings guidance by 11% as
well as announcing plans to lay off 2,000 workers as part of a massive restructure. The news sent investors reeling, with 3M's stock suffering a 10% loss. The health-care unit was the only division that deliv-ered an increase in sales.
3M estimated the acquisition will cost about 35 cents on an earnings-per-share basis in the first 12 months following com-pletion of the transaction, including financ-ing costs. Excluding costs and one-time expenses, 3M expects a 25 cents-per-share benefit over the same period. The deal is expected to close in the second half of 2019.
Published online 3 May 2019
CONTINUED FROM PAGE 1
� C O V E R S T O R Y �

12 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
� P O L I C Y & R E G U L A T I O N �
Rolling On: EU Makes Good Progress On Structures For New Regs ImplementationAMANDA MAXWELL [email protected]
T he European Commission expects to adopt an imple-menting act in May 2019 on the designation of issuing entities that will be responsible for the assignment of
Unique Device Identification to medtech products. The procedure should be relatively straightforward, as no co-
mitology will be involved. Comitology is a consultation proce-dure that involves the Commission consulting a committee on which every EU member state is represented; this can, inevitably, slow adoption processes, Medtech Insight notes.
The update on UDI is included in the latest version of the Eu-ropean Commission’s MDR/IVDR implementation Rolling Plan, a tool to help implement the necessary structures that should al-low the MDR to be implemented in full, as intended, on 26 May 2020. The last regulatory update was updated in April 2019. (Also see "Eudamed - A Moving Target But On Track For March 2020 Partial Go-Live" - Medtech Insight, 7 Mar, 2019.)
The updated Rolling Plan acknowledges that: 1. A draft implementing act is now in preparation that de-
fines the detailed arrangements necessary for setting up and maintaining the Eudamed European medical device database. This implementing act is related mainly to support, change management and maintenance rules, and should be adopted by the fourth quarter of 2019.
2. There has been a slight delay in the expected adoption of the implementing acts containing Common Specifica-tions for Class D IVD products – both under the current IVD Directive and drafted under the new IVD Regulation. It is now expected that the last Common Technical Specifications (CTS) needed under the IVD Directive will be adopted under the current IVD Directive during Q2 2019, rather than in Q1. Once the CTS have been adopted under the IVDD, the Common Specifications (as the CTS will be known under the new Regula-tions) will start to be drafted under the new Regulation. CTS are needed in the context of the new IVDR in relation to the scrutiny mechanism for high-risk devices.
EUDAMED – SOME DELAYS EXPECTEDWhen it comes to Eudamed, the modules for clinical investiga-tion and market surveillance will be available later than the time of application of the MDR due to workability issues, it emerges in the April document.
Further information on the Eudamed medical device database include:
• Version 4.1 of the high-level functional specifications was
publicly issued on the DG Grow website at the beginning of March, having factored in member states’ comments, but this is “not necessarily the last version."
• Regarding the audit of functional specifications: in terms of the audit report based on which the Commission will inform the Medical Devices Coordination Group when it has veri-fied that Eudamed has achieved full functionality and meets the drawn-up functional specifications, the type of contract has now been determined. The first draft of the contract content is being finalized.
OTHER DEVELOPMENTS• Subgroups of the MDCG, made up of authority experts and
a key body supporting implementation, became opera-tional as of 1 March 2019.
• A public consultation on an opinion of the European Com-mission’s Scientific Committee on Health, Environmental and Emerging Risks (SCHEER) on guidelines for the use of phthalates in medical devices is ongoing. The opinion is expected to be made available in mid-2019.
• On the designation of the future EU medical device no-menclature to be used in the UDI database, a decision was published in March 2019.
• Standardization mandate: stakeholder feedback on the draft mandate on the conditions for developments of stan-dards was submitted before the end of March deadline, and is currently under review. A decision is expected by Q2 2019.
The European Commission’s Rolling Plan was first published on 18 October 2018. (Also see "European Commission Sheds Light On MDR/IVDR Progress In Vital Update" - Medtech Insight, 18 Oct, 2018.)
Published online 30 April 2019
List Of Essential ActionsThe Rolling Plan features the list of essential imple-menting actions and actions to be put in place by the European Commission during the transition periods to the new Regulations, together with relevant informa-tion on expected timelines and current state-of-play. The previous version was published in February.

medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 13
� P O L I C Y & R E G U L A T I O N �
Day 1: US FDA Launches New 'Super Office,' Says It’s Already Proven Its WorthFERDOUS AL-FARUQUE [email protected] SHAWN M. SCHMITT [email protected]
M ay 1 was the official first day of the US Food and Drug Administration’s Office of Product Evaluation and Qual-ity – a so-called “Super Office” that the agency hopes
will make it more efficient and effective. Regulators say the new model of workflow has already identified safety signals sooner and streamlined their work.
Speaking via video at MedCon 2019 in Cincinnati, OH, Jeff Shuren, director of the FDA's Center for Devices and Radiological Health, an-nounced the first day of the new OPEQ, which the agency has been working on as a pilot for the past year. (Also see "FDA Device Center Reorg Set To Roll Out This Week" - Medtech Insight, 18 Mar, 2019.)
"This new office brings together our premarket review, postmar-ket surveillance, compliance and quality work into what we call the Office of Product Evaluation and Quality, with a flat management structure and folks organized in teams,” he said. “They're now in di-visions overseeing particular critical disciplines and then in teams around particular types of technology, and those teams now han-dle all aspects, a full 360 [degrees] of that kind of technology. No more going to different offices; no more going to different people. You've got, if you will, a one-stop-shop with the same team.”
For the past few years, the FDA has been stressing the total product life cycle approach to overseeing medical devices that would allow it to not only review products submitted in premar-ket applications, but also follow them in the postmarket arena to better understand their safety and efficacy profile.
The agency has also been working on a new regulatory paradigm that would allow it to approve products based on less premarket data but contingent on gathering more postmarket information.
Creation of the OPEQ is meant to make those goals a reality. (Also see "'Super Office' To The Rescue: FDA's Device Center Is About To Under-go A 'Total Product Life Cycle' Makeover" - Medtech Insight, 29 Sep, 2017.)
While the agency has been using a total product life cycle ap-proach to medical devices for years, Shuren noted it was organiza-tionally not well structured to execute that oversight philosophy. As a result, they decided to develop the new office, which is meant to create a more holistic and team-based regulatory approach.
The bottom line? Sponsors and manufacturers will be able to get answers and support from a single FDA team about their product rather than having to navigate a bureaucratic maze.
IT’S ALREADY WORKINGIn a separate statement from Shuren and OPEQ Director William Maisel, the two top regulators said a pilot of the new concept has
already been fruitful in identifying serious safety signals and im-proving communication between previously disconnected FDA teams, leading to faster decision-making.
Shuren and Maisel offered an example: The agency was moni-toring two postmarket studies of an implantable eye micro stent for certain types of glaucoma when it noticed significantly more users showed loss of corneal endothelial cells, which could lead to vision reduction or loss. The premarket and postmarket teams under the new OPEQ model worked together to analyze the in-formation and quickly worked with the manufacturer to pull the device from shelves.
The agency issued a safety communication to users and pro-viders, and then followed it up with a high-risk class I recall.
“FDA staff followed up to ensure that the manufacturer sus-pended all current studies involving its device,” Shuren and Maisel said. “The swift alert enabled patients and eye-care pro-viders to speak about their treatment plans, and helped prevent additional patients from receiving the device.”
The officials also noted that the OPEQ model has helped the agency with its Medical Device Safety Action Plan that was re-leased last year. An important part of that plan was to spur in-novation that leads to safer medical products. Shuren and Maisel argued in another example that the new model helped them to do exactly that.
“During the PMA review for a first-of-a-kind medical device, the lead reviewer learned of an inspection that might result in regulatory or administrative actions being recommended for a supplier associated with the device,” they said. “Because the communication and collaboration among team members pro-vided the lead reviewer with this important information early in the process, the OPEQ team was able to consider and rec-ommend alternatives, including the suggestion to remove that supplier. This type of collaboration helps eliminate delays in getting innovative medical device technologies to the patients who need them.”
Published online 1 May 2019

14 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
� P O L I C Y & R E G U L A T I O N �
‘Disease Doesn’t Respect Silos’: Sharpless Sets Flexibility As PriorityELIZABETH ORR [email protected]
A cting US Food and Drug Administration Commissioner Ned Sharpless described a service-oriented take on his new gig during a 2 May speech at the Food & Drug Law
Institute annual conference in Washington, DC. “The relationship of a doctor and patient is like that of a lawyer
and client,” he said, referring to the lawyer-heavy crowd at FDLI. “In both cases, the relationship is one of service. At the FDA, that patient or client is the public health of Americans.”
The metaphor is natural for the oncologist, who was director of the National Cancer Institute before joining the FDA last month. He’d been a cancer researcher in academia for almost 20 years before that. The move to the FDA allows him to advocate for re-cent advances in medical technology on a larger scale, he said.
Sharpless emphasized that he doesn’t expect any major changes at the FDA under his leadership, and the recent focus on innovation and efficiency will continue.
“[Department of Health & Human Services] Secretary [Alex] Azar and the White House made it very clear to me that they have been impressed with the things that FDA has been accomplish-ing and they don’t want to disrupt this strong progress. There will be no pause at FDA,” Sharpless said.
In the medical device realm, Sharpless noted that the number of novel device approvals had reached a new high of 106 last year and continues to climb. Last year’s Medical Device Safety Action Plan will help ensure that the FDA can keep advancing device safety and in-novation, he added. (Also see "New Safety Framework Mixes Current Efforts, New Investments At US FDA " - Medtech Insight, 17 Apr, 2018.)
The plan is based around recent changes to the agency’s post-market surveillance, 510(k) and de novo review processes. It also
includes a final guidance on the Breakthrough Device Program and plans to establish a new Safer Technologies Program (STEP), Sharpless said.
In a nod to his predecessor Scott Gottlieb's unfinished priori-ties, Sharpless said he would continue to work for a legislative fix that will allow the FDA to regulate all in vitro diagnostics, includ-ing lab-developed tests (LDTs) and diagnostics produced by con-ventional manufacturers. The area has been a source of contro-versy in recent years, as a regulatory plan developed during the Obama administration was scrapped after considerable industry criticism. Current thinking at the FDA is that legislation in the books doesn’t allow the agency to regulate LDTs via guidance alone. (Also see "Unfinished Business: LDT Legislation A Top Priority For Departing FDA Chief Gottlieb" - Medtech Insight, 22 Mar, 2019.)
Sharpless concluded his remarks by calling for more efficiency and collaboration across the agency, which he said would allow new technologies to reach patients more quickly. Additionally, he said the agency should look at whether its organizational structure produces maximum efficiency.
“As a biomedical researcher, I learned that disease doesn’t re-spect or recognize the silos we’ve created between basic and ap-plied research; between clinical care and drug development; or between the disparate systems providers use to guide patient care,” he said. “If we want to harness the full potential of thera-pies to transform care, we need to become more efficient, more collaborative and more data-driven so that we can learn from ev-ery patient’s journey.”
Published online 2 May 2019
Guidance Advises Orthopedic Firms On How To Characterize, Test Plastic Materials
ELIZABETH ORR [email protected]
M anufacturers of orthopedic devices have new guidance from the US Food and Drug Administration about how the agency wants them to address ultrahigh molecular
weight polyethylene (UHMWPE) used in their products.

medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 15
� P O L I C Y & R E G U L A T I O N �
The document, issued on 26 April, describes four types of UHMWPE and outlines the information characterizing the mate-rial that the agency recommends sponsors include in submis-sions. It finalizes a draft guidance issued in February 2016. (Also see "Plastics In Artificial Joints: FDA Offers Submission Tips In Draft Guidance" - Medtech Insight, 16 Feb, 2016.)
Categories of UHMWPE described in the guidance document are:• Conventional UHMWPE;• Highly crosslinked UHMWPE (HXLPE), which has been highly
crosslinked by various methods including radiation, perox-ides or exposure to high temperatures;
• Antioxidant highly crosslinked UHMWPE (AO-HXLPE), in which Vitamin E is blended or diffused into the resin pow-der before consolidation;
• Non-conventional UHMWPE, which may include materials made from lower molecular weight polyethylenes that may or may not be extensively crosslinked, porous polyeth-ylenes, functionalized UHMWPE such as hyaluronic acid-modified UHMWPE, or polyethylenes whose surfaces have been modified.
Conventional UHMWPE, HXLPE and AO-HXLPE all may origi-nate from virgin resin powders or consolidated forms that con-form to international standard ASTM F648.
All submissions should include the starting resin, resin con-solidation method, and terminal sterilization method, the FDA says. For devices incorporating conventional UHMWPE, spon-sors should also include the material’s tensile properties, impact
resistance and density. More information is required for HXLPE, such as the radiation type, percent crystallinity, melting tem-perature and free radical concentration. The data should comply with FDA-recognized standards ASTM F2759 and ASTM F2565.
If a device uses AO-HXLPE, the submission must include the con-centration and identification of the antioxidant or other additives, the stability of the antioxidant, and the effect of the antioxidant on the wear mechanism. “The anticipated, or known, impact of the wear test results on device performance should be thoroughly dis-cussed and supported with available literature and scientific ratio-nale (eg, comparison to the control, animal studies),” the FDA says.
The agency adds that it couldn’t provide specific tips for sub-missions including non-conventional UHMWPE because the term isn’t clearly defined. Information that may need to be addressed includes the material’s compression properties, crystal size and structure, creep resistance and durability of any modified surface.
Submissions for orthopedics, including all of the materials dis-cussed, should include biocompatibility and shelf-life testing. The agency recommends real-time aging to test the effects of aging on sterility and device performance. “If you use devices subjected to accelerated aging, we recommend that you specify the way in which the device was aged and develop a rationale to explain how the results of shelf-life testing based on accelerated aging are representative of the results if the device were aged in real time,” the guidance states.
Published online 29 April 2019
Canada Finalizes Guide On Evidence Needed To License 3D-Printed ImplantsVIBHA SHARMA [email protected]
C anada has issued a final guidance document on the evi-dence manufacturers should submit to support pre‐mar-ket license applications for class III and class IV implantable
medical devices that are manufactured using 3D-printing processes. The guidance, which was finalized following a 60-day public
consultation, also offers advice on the design and manufactur-ing process, material controls, device testing and labeling of 3D-printed devices. Health Canada notes that the document does not deal with standalone software, custom‐made devices, ana-tomical models or products made through bio‐printing that in-corporate viable living cells. Read the full article here
The document clarifies that the information requested from manufacturers to support their licensing application may vary in terms of content and level of detail depending on the 3D printing processes and the risk class of the finished device.
Since the public consultation on the guideline, the document has been substantially updated to clarify several aspects. For ex-
ample, the section on device description has been expanded considerably to clarify among other things that manufacturers must submit detailed information about the finished device. They should include a photograph or drawing of the device with all functional components clearly labeled and should clarify whether the entire device or only a component of the device is 3D printed.
The device description section also says that manufacturers should include information on the starting material, the meth-odology for 3D printing (such as laser sintering, direct metal laser sintering and powder bed fusion). In addition, they should pro-vide an overview of the printing process, including post‐print-ing processing steps. There are different requirements regarding device description for products that are patient-matched rather than manufactured to pre‐determined sizes.
The final guidance elaborates on requirements for preclinical performance testing, which it says should be conducted on the final, finished device subjected to all post‐printing processing,

16 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
� P O L I C Y & R E G U L A T I O N �
cleaning and sterilization. For each test, a detailed summary is required and should include a description of the test objec-tive, samples tested, analysis of the worst case configuration of the test samples with respect to dimensions and features (eg, holes, supports, porous areas), acceptance criteria with justifi-cation, adherence to international standards where applicable, test results and a discussion/analysis of the results in terms of the test objective.
Health Canada claims that its licensing approach for im-plantable medical devices manufactured by 3D printing is well aligned with international best practices. The department adds that it is actively working and collaborating with its international
counterparts to keep pace with the research and development of 3D printing. It says that the final guidance represents the "first phase" of its 3D-printing policy. In the guideline, the department has adopted definitions developed by the International Medical Device Regulators Forum regarding personalized devices.
The final guidance is effective immediately and should be read in conjunction with Health Canada's 2012 guidance on "Support-ing evidence to be provided for new and amended licence ap-plications for class III and class IV medical devices, not including in vitro diagnostic devices."
Published online 7 May 2019
Compliance Corner: When Is An Action Exempt From FDA's Recall Reporting Requirements?ELIZABETH ORR [email protected]
I t can sometimes be tricky for device-makers to determine whether a particular action they take with their product is in-deed reportable to the US Food and Drug Administration as
a recall, two industry experts say.To wit: Despite a five-year-old guidance document from the
agency, some manufacturers are still falling down when attempt-ing to distinguish between a medical device recall and a prod-uct enhancement, Pamela Furman Forrest, a partner at law firm Covington & Burling, and Steve Niedelman, lead quality systems and compliance consultant at law firm King & Spalding, said at FDAnews' 16th Annual Medical Device Quality Congress in April.
Forrest and Niedelman explained that the 2014 guidance document from the FDA that distinguishes recalls from en-hancements still has some firms scratching their heads, trying to determine if their particular action is indeed exempt from the agency's recall regs.
Under the guidance, an enhancement is a change made to enhance a device’s quality that is not made to fix a violation of existing regulations, and therefore do not need to be reported to the agency. (Also see "US FDA drops controversial recall report idea for device enhancements" - Medtech Insight, 16 Oct, 2014.)
The key question companies should ask themselves, Forrest said, is whether their action makes a safe device better or im-proves existing safety concerns. If the action improves a de-vice’s safety, then it’s likely reportable as a recall – even if that wasn’t the primary purpose of the move.
And “if you’re making changes to improve the safety of a de-vice, you’ve likely crossed the line,” Niedelman added. “If you’re making them to build a better mousetrap or because technol-ogy has changed and improved, that might be all right.”
Also exempt from recall reporting requirements are minor cor-rections with no safety impact that the FDA calls “market with-
drawals” – for example, if a company decides to take a product off the market because an address on its labeling was incorrect. These are very similar to low-risk class III recalls, Niedelman said.
Similarly, “stock recovery,” which is a removal performed be-fore a device reaches the market, is not reportable as long as the entire affected lot is under the control of the manufacturer. If even one device has gone to a distributor, the action becomes a reportable recall, Forrest said. “Industry often is less conserva-tive than FDA in terms of whether the product is really under your control,” she noted.
Routine software updates are usually also exempt from reporting requirements, as are some prompt bug fixes that couldn’t cause significant adverse events. The FDA set the rules for those recalls and enhancements in a 2016 guidance docu-ment. (Also see "'Sharing' Organizations Stay In Final Post-Market Cybersecurity Guidance" - Medtech Insight, 29 Dec, 2016.)
AVOID 'SILENT' RECALLS Further, manufacturers are more likely to stay in the FDA’s good graces if they avoid so-called “silent” recalls, Forrest said. In these situations, a company undertakes actions in the field without realizing they need to be reported.
Such actions might include combining an upgrade with a corrective action; distributing a “market bulletin” or “technical advisory” alerting customers to recent adverse events and ex-plaining how to prevent them; or sending out sales representa-tives or maintenance staff to determine whether a fix is needed and apply it if so.
“If you’re cautioning your users as to how to more safely use your device, you’re probably in the realm of a reportable event,” Forrest said.
� Q U A L I T Y C O N T R O L & C O M P L I A N C E �
CONTINUED ON PAGE 22

medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 17
� Q U A L I T Y C O N T R O L & C O M P L I A N C E �
Source: Stericycle ExpertSOLUTIONS Q1 2019 Recall Index Design: Janet Haniak
• The average recall size was 823,126 – the highest quarter since 2006.
• At 51%, quality issues was the top recall cause based on UNITS, mostly due to one large recall. This is the first time quality issues was the top cause since Q3 2016.
• For the first time since Q3 2017, no company reported 10 or more recalls in the quarter.
CONNECTING THE DOTS
TOP RECALL CAUSES BASED ON NUMBER OF EVENTS
Sterility
15Software Issue
37Quality Issue
21Mislabeling Issue
31
OF MEDICAL DEVICE RECALLS WERE NATIONWIDE
55.5%
AVERAGE CLASS I UNITS RECALLED PER QUARTER
Q4 2018
Q1 2019
Q3 2018
1,380,706
1,388,655
14,035,195
MEDICAL DEVICE MALADIES
There were more than 1 million class I units recalled for the third consecutive quarter. The last time there were three consecutive quarters with at least 1 million units each was Q2 to Q4 2014.
MEDICAL DEVICE RECALLS & UNITS (in millions)
050
100150200250300350400
Q1 2019
Q4 2018
Q3 2018
Q2 2018
Q1 2018
Q4 2017
Q3 2017
Q2 2017
Q1 2017
0
50
100
150
200
250
SNAPSHOT: Device Recalls Q1 2019
Medtech InsightPharma intelligence |
Q1 Recalls SnapshotSHAWN M. SCHMITT [email protected]
G ood news for industry: recalls of medical devices were down 41% in the first quarter of 2019, the low-est number of recalls recorded in a quarter since Q4
2017. There were 164 recalls in Q1, compared to the 280 not-ed in Q4 2018. And there were just under 135 million units recalled in Q1 (down 16% from Q4's 161 million), consulting firm Stericycle says in its most recent recalls index. However, there was one dark spot: It was the third consecutive quar-ter in which more than 1 million high-risk class I units were recalled.
Published online 7 May 2019

18 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
� R & D �
American Society Of Breast Surgeons Releases First Mammography Screening GuidelinesMARION WEBB [email protected]
T his year nearly 268,000 women will be diagnosed with invasive breast cancer in the US alone but there are still conflicting guidelines for breast cancer screening.
The American Society of Breast Surgeons (ASBrS) on 3 May released its first screening mammography guidelines based on a patient's breast cancer risk profile with the goal to "minimize breast cancer disparities across race and ethnicity through ear-lier disease detection for all," said Shawna Willey, chair of ASBrS' board in today's statement.
"Our members are on the front lines with breast cancer patients every day guiding them through all stages of breast cancer diag-nosis and treatment," said Willey. "These new recommendations were ASBrS member driven and developed based on their unique, firsthand perspective on the disease and patient journey."
The new recommendations differ from current United States Preventive Services Task Force (USPSTF) and American Cancer Society (ACS) guidelines, which apply only to women with av-erage risk, and also factor in screening cost per diagnosis and related issues along with mortality, but are supported by the American College of Radiology (ACR), the ASBrS said.
Under the ASBrS recommendations, all women ages 25 and older should be assessed for breast cancer.
For women with average risk, the ASBrS recommends all wom-en should have annual mammograms starting at age 40, which opposes the USPSTF recommendations to delay annual screen-ing until age 50.
"Routine screening for women age 40 to 49 has been unequiv-ocally demonstrated to reduce mortality by 15%," Walton Taylor, ASBrS president said. "However, today USPSTF guidelines delay annual screening until age 50, because they are based on an ef-ficiency statistical model that also considers the impact of poten-tial screening risk."
Meanwhile, the American Cancer Society recommends that women should get annual mammograms from age 45-54, and women ages 55 and older should be screened every other year.
However, the American College of Physicians (ACP) recommends that women at average risk for breast cancer should undergo screening every other year starting between the ages of 50 and 74.
The ACP said in a statement from 9 April that these guidelines do not apply to women who have had a prior abnormal screen-ing, a previous diagnosis of breast cancer or a genetic mutation known to increase risk.
When it comes to women who are at a higher-than-average risk for breast cancer, such as women with a BRCA gene mutation or very strong family history, and other risk factors, the ASBrS also recommends an annual 3D screening mammography and supplemental imaging, preferably an MRI.
But when it comes to annual screenings for women at average risk, the two organizations still differ.
The ACP said in its statement evidence has shown that women who are screened annually receive more abnormal results than women who are screened every other year (7.0% versus 4.8%), and that annual mammograms can lead to false-positive find-ings that result in biopsies and surgeries that would otherwise not have been necessary.
When it comes to screening women older than 74, the organi-zations' recommendations also differ.
The ASBrS recommends "women with a life expectancy of at least 10 years continue yearly screening mammography," saying that prior studies have shown a survival benefit in women 74 and older who do not have severe co-morbidities.
In addition, mammographic screening in an older population would be expected to have a lower rate of false positives and unnec-essary biopsies compared to a younger population, the ASBrS said.
The USPSTF, meanwhile, concluded based on prior random-ized prospective trials of screening mammography excluding women older than 74, that there are "no definitive data to recom-mend for or against screening mammography in women ages 74 and older," the ASBrS stated.
In March, the US Food and Drug Administration also proposed a major change to mammography regulations that would re-quire mammographers to give patients more information on the limitations of mammography tests, in particular for women with denser breast tissue. (Also see "US FDA Proposes Biggest Mammog-raphy Rule Change In 20 Years" - Medtech Insight, 27 Mar, 2019.)
According to the American Cancer Society, breast cancer is the leading cancer in women worldwide and incidences continue to rise.
Mammography, while not perfect in terms of detecting can-cers, especially in dense breasts, is considered the most widely used and most cost-effective screening tool.
Nehal Patel, a radiologist at Kaiser Permanente in San Diego, told Medtech Insight earlier that "conventional mammography is the only proven method which decreases mortality in breast cancer."
Early detection for breast cancer is key to reduce mortality, and several companies are working on imaging technologies that can help physicians detect cancers earlier.
Screening mammography accounts for the largest share of the breast imaging and biopsy market and is expected to grow to $4.3bn by 2022 from $3.3bn in 2017, according to a recent Informa Medde-vicetracker report entitled "Oncology: Breast Cancer Diagnostic and Treatment Devices." (Also see "Market Intel: Breast Imaging Market Driv-en By AI, Technological Innovation " - Medtech Insight, 7 Mar, 2019.)
Published online 3 May 2019

medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 19
� R & D �
Higher Doses Of Novocure’s TTF Help New Glioblastoma PatientsREED MILLER [email protected]
N ew data from the EF-14 trial, showing a dose-response in glioblastoma patients treated with Novocure Ltd.’s Op-tune Tumor Treating Fields therapy, will help the com-
pany refine the therapy as it creates the future generations of Tumor Treating Fields technology.
Tumor Treating Fields are carefully tuned electric fields cre-ated by the Optune device to disrupt solid tumor cells’ ability to divide and propagate. (Also see "Novocure Launches INNOVATE 3 Trial Of Ovarian Cancer Therapy" - Medtech Insight, 26 Mar, 2019.)
A previous analysis of EF-14, published in the Journal of Neu-ro-Oncology in late 2018, showed Tumor Treating Fields plus temozolomide therapy improved both overall survival and survival free of cancer-progression compared to temozolo-mide therapy alone. (Also see "Results Recap: Long-Term Results Support NovoCure's Optune Brain-Cancer Technology" - Medtech Insight, 9 Dec, 2018.)
A new post-hoc analysis of 340 patients in the EF-14 trial, led by Matthew Ballo of West Cancer Center in Memphis, TN, is now published in International Journal of Radiation Oncology, Biol-ogy, Physics, known in the field as “The Red Journal.”
“This analysis provides radiation oncologists with a better un-derstanding of the relationship between Tumor Treating Fields dose and survival and can be used to help optimize outcomes for glioblastoma patients,” Ballo said.
Novocure's CEO Asaf Danziger said, “With the knowledge gained from this study, we have focused our engineering ef-forts on evolving our Optune system to improve efficacy and extend survival."
He also said the company is developing novel mapping algo-rithms to optimize treatment planning that will be incorporat-ed into the second-generation of NovoTAL, Novocure's system that creates individualized treatment maps for patients starting therapy with Optune.
Ballo and colleagues designed a simulation-based analysis to determine if increasing the Tumor Treating Fields dose at the tumor site improved patient outcomes. The investigators cre-ated realistic head models based on contrast images from pa-tients and obtained transducer array layouts for each patient from EF-14 records.
The analysis showed the median overall survival and progres-sion-free survival were significantly longer when the average local minimum dose-density in the tumor bed was more than 0.77 milliwatts per cubic centimeter. The higher-dose group lived a median of 25.2 months versus 20.4 months for the low-er-dose group. The median progression-free survival was 8.5 months in the higher-dose group versus 6.7 months for the lower-dose group.
The median overall survival and progression-free survival were also longer when the average intensity of the Tumor Treat-ing Fields was more than 1.06 volts per centimeter. The higher-intensity group’s overall survival was 24.3 months versus 21.6 months for the lower-intensity group. Progression-free survival was 8.1 months versus 7.9 months for the high-intensity and low-intensity groups, respectively.
“[This simulation-based study is] the first reported analysis demonstrating patient-level dose responses to Tumor Treating Fields,” Ballo et al explained. “We provide a rigorous definition for Tumor Treating Fields dose and set a conceptual framework for future work on Tumor Treating Fields dosimetry and treat-ment planning.”
Optune is FDA-approved for both recurrent and newly diag-nosed glioblastoma, but the company is working on applica-tions of Tumor Treating Fields for several other types of can-cer. For example, the company recently announced the start of the 540-patient INNOVATE 3 trial of Tumor Treating Fields combined with paclitaxel to treat recurrent, platinum-resistant ovarian cancer. (Also see "Novocure Launches INNOVATE 3 Trial Of Ovarian Cancer Therapy" - Medtech Insight, 26 Mar, 2019.) Re-cently published results from the Phase II STELLAR trial showed Tumor Treating Fields therapy in conjunction with chemother-apy extends survival in previously untreated mesothelioma patients. (Also see "NovoCure’s Tumor Treating Fields Help Meso-thelioma Patients Live Longer In STELLAR Trial" - Medtech Insight, 4 Apr, 2019.)
Published online 30 April 2019

20 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
� R & D �
Exec Chat: John Frels, VP Of Research And Development, Abbott DiagnosticsCATHERINE LONGWORTH [email protected]
Medtech Insight: Tell us a bit about your background and experience.
John Frels: I always knew I wanted to be involved in sci-ence, and was particularly interested in the intersection of the life sciences and new technologies, similar to what today’s STEM programs aim to build. I earned my PhD in Molecular Biology from Northwestern, and I’ve been
with Abbott for 24 years in the Diagnostics business. I spent my early years with the company as a bench scientist in Prod-uct Support and R&D where I gained an appreciation for the science that goes into our products and what our customers need and expect. Over the years, I’ve held leadership roles in Technical Support and Reagent Manufacturing in the US and Europe, as well as in R&D where I am responsible for our Core Laboratory Diagnostics new product pipeline.
How has Abbott evolved during your time at the company?
Frels: You don’t get to be a 130-year-old global organization by staying the same, and Abbott is constantly being shaped for fu-ture success. In recent decades, the company has been shaped to be much more globally diverse and balanced across geogra-phies and markets. This is true across all our businesses – Diag-nostics, Medical Devices, Nutrition and Pharmaceuticals – with each of them evolving over the years through organic execu-tion and growth, as well as some strategic acquisitions and di-vestitures. Today we provide even more breakthrough prod-ucts and innovations to help people live healthier, fuller lives, and we continue to position ourselves to be able to capitalize on future trends in health care, technology and other industries so we’re well positioned for ongoing success and growth.
What is your approach when it comes to leading innovation?
Frels: At Abbott, there is a strong commitment to investing in internal R&D, for our legacy businesses and those that we’ve acquired. This is at the heart of our strategy within Diagnos-tics where we have invested heavily over the last several years in our new Alinity family of systems, assays and informatics
solutions that are all coming to market now. While this repre-sents the culmination of many years of R&D investment, we know that to remain a strong and growing company we must continue to invest in new products and early phase concepts. We focus on developing a healthy pipeline that will deliver high-value products for many years ahead – there is no “one and done.” This always starts with a view toward what our cus-tomers want and how we can help to improve patient care. And to make it all work you need to have the right talent. We attract and retain people who have demonstrated a personal track record of achievement in science and engineering, and are curious, persistent and work well in teams. They have to be willing to try new things and take on big challenges while keeping our customers and their patients at the forefront of what we do.
What new products and launches are coming out of Abbott’s diagnostics business in 2019?
Frels: We'll continue to increase our global rollout of our advanced Alinity family of harmonized diagnostic instru-ments, and we continue to broaden our menu of assays and solutions. Alinity ci-series has launched and continues to gain traction with labs and hospital systems in [Europe and the Middle East], [Asia Pacific] and the US, and Alinity m, the lat-est in molecular technology, just received CE mark approval. We’ll also offer AlinIQ – a first-of-its-kind, holistic informatics and professional services portfolio – with additional capabili-ties and new technology across more markets. In rapid diag-nostics, we’ll introduce the first-ever rapid point-of-care test approved to diagnose diabetes. The Afinon HbA1c Dx Assay for use on the Afininon 2 Analyzer, provides results in three minutes, enabling clinicians to develop informed, individual-ized care plans during patient consultation.
What milestones is the business hoping to achieve in the coming year?
Frels: Ramping up commercialization in the U.S. is a major focus in the near term. We’ll also be looking to make invest-ments in many new products that are advancing in the pipe-line, including solutions that will benefit laboratories while also helping them to improve outcomes for doctors, patients and ultimately the entire health system.
Published online 1 May 2019
Sour
ce: A
bbot
t Lab
orat
ories

medtech.pharmaintelligence.informa.com May 13, 2019 | Medtech Insight | 21
� C O M M E R C I A L �
Biotronik Begins US Rollout Of PK Papyrus For Coronary PerforationsREED MILLER [email protected]
B iotronik SE & Co. KG has begun the US launch of the PK Pa-pyrus balloon-expandable covered stent for treating acute perforations of native coronary arteries and coronary by-
pass grafts.The US Food & Drug Administration granted a humanitarian de-
vice exemption (HDE) for PK Papyrus in September 2018. The FDA said it is the first device it has approved for this indication in 17 years.
FDA Approves Boston Scientific’s Vici Venous Iliac StentREED MILLER [email protected]
T he US Food and Drug Administration approved Boston Scientific Corp.’s Vici venous stent for treating iliofemoral venous obstructive disease on 6 May.
Venous obstructive disease causes blood to pool in the legs causing pain, swelling and ulcers. It afflicts about 40% of the US population and is caused by deep-vein thrombosis, post-thrombotic syndrome and compressive diseases, according to the company.
Vici is designed specifically to withstand the intense crushing pressures on the iliofemoral veins created by the surrounding vasculature in the pelvis.
It will compete with Bard Vascular Systems’s Venovo venous stent, which became the first stent to be approved for iliofemoral venous disease by the FDA on 14 March. (Also see "Global Device Approvals, Weekly Snapshot: FDA Approves Bard’s Venovo Stent; Abbott’s MitraClip Gets Indication-Expansion; Boston Scientific’s Watchman FLX Earns CE Mark" - Medtech Insight, 18 Mar, 2019.) Also, Cook Medical markets the Zilver vena venous stent outside the US and is evaluating it in the VIVO trial in the US.
Vici's approval was supported by the results of VIRTUS, a single-arm trial treating 170 patients with clinically significant obstruc-tions in the illiofemoral venous outflow tract, including 75% with post-thrombotic lesions and 25% with non-thrombotic lesions.
One year after treatment with Vici, 84% of the patients in the trial met the criteria for primary patency. Primary patency was defined as freedom from occlusion by thrombosis, freedom from surgical or endovascular intervention on target vessel to fix re-stenosis or stent occlusion, and freedom from in-stent restenosis blocking more than 50% of the vessel. The prespecified perfor-mance goal was 72.1%. Only 1.2% of patients in the trial had a major adverse event within the first 30 days, beating the pre-specified target of 6%. (Also see "Results Recap: Medtronic High-lights Data To Contrast With Recent Meta-Analysis That Sparked Drug-Coated Balloon Scrutiny " - Medtech Insight, 25 Jan, 2019.)
Boston Scientific added Vici to its line of peripheral vascular de-vices when it acquired Veniti Inc. for $108m upfront and $52m in milestones in August 2018. (Also see "Boston Scientific Buys Venous Stent-Developer Veniti For $160M" - Medtech Insight, 8 Aug, 2018.) Boston Scientific’s peripheral vascular devices also include the Epic and Express LD stents for the iliac arteries and Eluvia drug-eluting stent for the superficial femoral artery and popliteal ar-tery. (Also see "Eluvia Is A 'Step Ahead' Of - Not Catching Up To - Rival Peripheral DES, Says BSX" - Medtech Insight, 10 May, 2016.)
In a 6 May note, Wells Fargo analyst Larry Biegelsen pointed out that Boston Scientific believes the worldwide venous stent market is worth about $150m annually and growing at least 20% a year.
“This is despite there not being a stent with FDA approval for use in the peripheral venous system until earlier this year. In oth-er words, the market has largely been driven historically by off-label use," Biegelsen wrote.
Biegelsen suggested Vici may cannibalize sales of Boston Sci-entific’s WallStent biliary stent, which is often used off-label in the iliac vein.
Published online 6 May 2019

22 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
� C O M M E R C I A L �
The only other device approved by the FDA to treat coronary perforations is Abbott Laboratories' Graftmaster Rx coronary stent graft system, which originally earned an HDE in 2001 as the Jomed Jostent.
Coronary perforations are holes in the coronary wall. They oc-cur in fewer than 1% of the 800,000 coronary interventions per-formed in the US each year, but are life-threatening bleeding events that require immediate action, Amy Culley, Biotronik's director of vascular intervention clinical studies, told Medtech Insight. Currently, the only options for patients are emergency coronary bypass surgery or a device like Graftmaster Rx, which has a cover of expanded polytetrafluoroethylene sandwiched in between two stents of slightly different diameters.
These "sandwich stents" have a larger diameter and are more rigid than a traditional single stent, which can make delivery during emergencies challenging, Culley said.
PK Papyrus is a single PRO-Kinetic Energy cobalt chromium coronary stent covered with a unique polyurethane membrane. The stent's struts are about 60 μm thick to provide maximum flexibility and the polyurethane cover is electrospun and ex-tremely thin, which makes it flexible and low-profile.
"Biotronik saw a need to develop and rethink how to design a product to have a single stent with a single cover," Culley said. "When you have an emergency situation, you want confidence in the ability to deliver the treatment quickly and effectively. PK Papyrus delivers more like a traditional stent because it is a single-stent design."
Specifically, the HDE indicates PK Papyrus for vessels 2.5 to 5.0 mm in diameter. Graftmaster is approved for native coro-nary vessels or saphenous vein bypass grafts at least 2.75 mm in diameter.
PK Papyrus is compatible with 5 French delivery systems, which is important, according to Culley, because Graftmas-ter often requires interventionalists to "upsize" their catheter from a 5 French or 6 French to a 7 French catheter during the procedure.
"That gives [interventionalists] confidence in being able to seal perforations quickly," Culley said.
PK Papyrus has been available outside the US since 2013. The HDE is based on "real-world" data from 80 patients in Asia and Europe treated with PK Papyrus to seal coronary artery perforations.
"These are unique products and it's difficult to study them prospectively because it is not ethical to create a perforation. The only way to collect data is from the experience obtained post-use," Culley said.
In this study, PK Papyrus was successfully delivered to the perforation site in 76 of the 80 patients (95%) and successfully sealed the perforation in 73 patients (91.3%).
There were two procedural deaths during the study. One pa-tient died despite successful sealing of the perforation, but the cause of that patient's death is unknown. Another patient died of persistent intrapericardial bleeding following an unsuccess-ful attempt to seal the perforation with PK Papyrus and devel-oped electro-mechanical dissociation.
Five patients died in the hospital following successful seal-ing of the coronary perforation, and one died in the hospi-tal after a failed attempt to seal the perforation. There were two cases of stent-thrombosis, including one in a patient who died. Seven patients treated with PK Papyrus (8.8%) suffered pericardial tamponade, a build-up of fluid in the pericardium, which had to be treated with an invasive procedure to remove the fluid.
The study found no post-procedural myocardial infarctions or urgent cardiac surgeries following implantation of PK Papy-rus. Only 22 patients completed the follow-up survey, but 16 of those patients reported no complications.
"The feedback we've had is that nobody wants to be in a situ-ation where they are managing a coronary artery perforation. However, this adds confidence to their treatment of patients in [coronary intervention] procedures, knowing that they have a product that delivers like a traditional stent that will give them the ability to deliver life-saving treatment more quickly in the event of a perforation," Culley said.
Published online 2 May 2019
Other potentially risky behavior, she said, might include cor-recting devices only when a complaint is received rather than taking systemic action, or offering to exchange corrected or next-generation devices to replace faulty ones without inform-ing the FDA.
A recent example is documented in an October 2017 warning letter to Magellan Diagnostics, Forrest said. Among other issues, the company had mailed consumers new instructions for use of lead-detection diagnostics without alerting or submitting a la-beling change to FDA. (Also see "Magellen Gets Warning Letter On Lead Test Concerns" - Medtech Insight, 24 Oct, 2017.)
FDA can take regulatory action against manufacturers that fail to comply with reporting requirements, which renders their de-vices “misbranded” and makes putting them into interstate com-merce a prohibited act. Additionally, companies that don’t follow FDA’s rules could taint their relationship with the agency.
But Forrest pointed out that the harshest penalties could come from forces outside the FDA. For example, recall noncom-pliance can raise a manufacturer’s product liability risk – raising the specter of patient lawsuits that could “dwarf” the possible cost of any recall.
Published online 6 May 2019
CONTINUED FROM PAGE 16
� Q U A L I T Y C O N T R O L & C O M P L I A N C E �

Are you looking to reach and do business with senior decision makers in pharma and medtech?
To fi nd out how our team can help visit:https://pharmaintelligence.informa.com/marketing-services
We offer a range of marketing opportunities whether you are looking to:• Raise brand awareness• Produce content marketing/thought leadership content• Generate leads• Engage directly with potential clients as well as cementing existing relationships
JN723 Marketing Services Advert.indd 1 2017/11/13 6:08 PM

24 | Medtech Insight | May 13, 2019 © Informa UK Ltd 2019
Medtech InsightAwards | 2019
Medtech InsightAwards | 2019
Sponsorship and Table Booking Enquiries:Christopher Keeling
Tel: +44 (0) 20 3377 3183 | Email: [email protected]
General Enquiries:Jo Kirkpatrick
Tel: +44 (0) 20 7017 7180 | Email: [email protected]
Medtech Insight Awards
Open for Entries
Entry deadline: June 7, 2019
Monday, September 23, 2019 | State Room, Bostonhttps://pharmaintelligence.informa.com/mti_awards2019
Headline Sponsor In partnership with
JN2027 Medtech Awards 2019 Open for Entries Advert US Letter.indd 1 2019/04/17 13:17