meeting coc standards - oncolog
TRANSCRIPT


Meeting CoC Standards
Chapter 4
Patient Outcomes
Sheryl Daugherty. RHIT, CTR
Senior Client Relationship Manager
Sharon Metzger, CTR
Director of Consulting Services

Welcome
Thank you for joining us today for our webinar
We will take questions and comments at the end of the
presentation
You may enter your questions into the “Question” box on
the GoToWebinar screen

FYI
This webinar has been awarded 1 CEU by NCRA
You must be registered and logged in to receive a
Certificate of Attendance which will be emailed to you
within 3 weeks
This webinar is being recorded and the recording, slide
deck and Q&A will be made available at our website:
Oncolog.com “VIEW OUR WEBINARS” within 2 weeks

Goals for Today
Review the requirements to meet the standards in
Chapter 4
Identify requirements for documentation and compliance
Share examples, offer suggestions and provide clarification

Required Documentation
CoC accredited cancer programs document cancer program
activity using multiple sources, including policies, procedures,
manuals, tables and grids; however, cancer committee
minutes are the “primary source” for all documentation of
cancer program activities*.
All meeting minutes should contain sufficient detail to
accurately reflect the activities of the cancer committee, as
well as demonstrate compliance with the CoC standards.*
• *Cancer Program Standards: Ensuring Patient-Centered Care page 11

Chapter 4: Patient Outcomes
Standard 4.1 Cancer Prevention Programs
Standard 4.2 Cancer Screening Programs
Standard 4.3 Cancer Liaison Physician Responsibilities
Standard 4.4 Accountability Measures
Standard 4.5 Quality Improvement Measures
Standard 4.6 Monitoring Compliance with Evidence-
Based Guidelines
Standard 4.7 Studies of Quality
Standard 4.8 Quality Improvements

Standard 4.1 Cancer Prevention Programs
Each calendar year, the cancer committee organizes and offers
at least one cancer prevention program designed to reduce the
incidence of a specific cancer type and targeted to meet the
prevention needs of the community. Each prevention program is
consistent with evidence-based national guidelines for cancer
prevention.

Definition and Requirements
Cancer prevention requires cancer programs to identify risk factors
within their community and patient population, and use strategies
to modify attitudes and behaviors to reduce the chance of
developing cancer.
Annually, the cancer committee identifies the cancer prevention
needs of the community and offers at least one cancer prevention
program focused on reducing the number of diagnoses of a specific
type of cancer.
The prevention program must be consistent with evidence-based
national guidelines for cancer prevention.
The program can be provided on-site or may be coordinated with
other facilities and/or local agencies as long as it is under the
direction of the cancer committee.

Examples of Cancer Prevention Programs
Education material on risk awareness for a specific cancer
type
Skin cancer prevention (UV rays, tanning bed use)
Smoking/chewing tobacco cessation
Smoking prevention in adolescents
Radon education and testing (related to lung cancer
prevention)
Nutrition, physical activity, and weight loss programs
(specifically related to cancer prevention)
Vaccine/Human papillomavirus (HPV)

Role of the Community Outreach Coordinator
Appointed each calendar year
Required member of the Cancer Committee
Monitors the prevention and screening activities
Reports annually to the cancer committee
Recommends corrective action if activity falls below the
annual goal or requirements
Responsible for overseeing compliance for Standards 1.8, 4.1
and 4.2
A cancer registrar CANNOT be selected to fulfill this role
Resources for Evidence-Based National Guidelines
Related to Cancer Prevention
Agency for Healthcare Research and Quality
American Cancer Society
Cancer Control P.L.A.N.E.T.
Centers for Disease Control and Prevention
National Cancer Institute
The Community Guide

Clarification
The need and planning discussion of the Prevention program must be documented
in the cancer committee minutes prior to the event and include evidence-based
guidelines.
The impact of the prevention program is evaluated and documented.
Prevention programs count for the year in which the event is held.
Prevention programs may be repeated if justified by a review of the community
needs assessment.
Prevention education provided via newspaper article, television interview, or
social media without any actual interaction with the participants is not compliant
with this standard.

SAR Documentation
For each year of the survey cycle complete the following information:
PREVENTION PROGRAM ACTIVITY
Year: 2016
Date Prevention needs assessed by the cancer committee: 1/15/16
Cancer site selected based on prevention needs Breast
Type of prevention activity offered: Education and cancer
risk assessment
Date prevention activity held: 10/22/16
Number of participants 465
National Guidelines used to design the prevention activity American Cancer
Society

Rating Compliance
Each calendar year, the program fulfills all of the
following compliance criteria:
The cancer committee assessed the cancer prevention needs of the
community and patient population.
The cancer committee organizes and offers at least one cancer
prevention.
The cancer prevention program is consistent with evidence-based
national guidelines and evidence-based interventions.
The cancer committee minutes document the assessment of
community needs, the prevention program offered and the number
of participants.

Standard 4.2 Cancer Screening Programs
Each calendar year, the cancer committee organizes and
offers at least one cancer screening program that is designed
to decrease the number of patients with late-stage
disease and is targeted to meet the screening needs of the
community. Each screening program is consistent with
evidence-based national guidelines and interventions and
must have a formal process developed to follow up on all
positive findings.

Definition and Requirements
Cancer screening programs apply screening guidelines to detect cancers at
an early stage, which improves the likelihood of increased survival and
decreased morbidity.
Each calendar year, the cancer committee organizes and offers at least
one cancer screening program focused on an identified cancer screening
need within the community, and designed to decrease the number of
patients with late-stage disease.
The screening program must be consistent with evidence-based national
guidelines and interventions.
The cancer committee and designated community outreach coordinator
must have a mechanism in place to ensure that all positive findings
identified are addressed.
Cancer screening programs may be provided on-site or coordinated with
other facilities or local agencies as long as it is under the direction of the
cancer committee.

Examples of Cancer Screening Programs
Breast: Screening Mammograms and Physical Examination
Colon: Colonoscopy, Flexible Sigmoidoscopy, or Fecal Occult
Blood Testing (FOBT)
Cervical: Papanicolaou (PAP) testing with or without Human
Papillomavirus (HPV DNA) testing
Skin: Total-body Skin Exams
Lung: Low-dose computed tomography

Resources for Evidence-Based National
Guidelines and Evidence-Based Interventions
Agency for Healthcare Research and Quality
American Cancer Society
American Society of Clinical Oncology
National Comprehensive Center Network
National Cancer Institute
National Colorectal Cancer Roundtable
Clarification
The need and planning discussion of the screening program must be documented in
the cancer committee minutes prior to the event and include evidence-based
guidelines.
The impact of the screening program is evaluated and documented and must
include how positive findings will be addressed.
Screening programs must screen for the detection of actual cancer- not just a risk.
Screening programs may be repeated if justified by a review of the community
needs assessment.
The standard does not require that a physician perform screenings and follow-up.
That decision should be made by the cancer committee based on the site,
screening procedures, staff’s clinical experience and follow-up process

SAR Documentation
For each calendar year within the survey cycle, the following data items must be documented in
the SAR:
Cancer Screening Program Activity
Year: 2016
Date screening needs were assessed by the cancer
committee:
2/15/16
Type of screening activity: Mammography
Cancer Site selected based on screening needs: Breast
Date activity held: 10/14/16
Number of participants: 254
National guidelines used to design screening activity; NCCN
Define follow-up process for positive findings: Results of mammogram were mailed to
each participant and the primary physician
identified by the patient. All BIRAD 4s
were contacted by the Breast Center and
follow-up was documented

Rating Compliance
The cancer committee identifies the cancer screening needs of their
community and patient population annually.
The cancer committee organizes and offers at least one cancer screening
program per calendar year.
The screening program is consistent with evidence-based national
guidelines and evidence-based interventions.
Each screening program has a process developed to follow up on all
positive findings.
Each calendar year, the program uploads cancer committee minutes
documenting the planning and provision of at least one annual cancer
screening program organized and offered by the cancer committee.
Standard 4.3 Cancer Liaison Physician Responsibilities
A Cancer Liaison Physician (CLP) serves in a leadership
role within the cancer program and is responsible for
evaluating, interpreting, and reporting the cancer
program’s performance using National Cancer Data Base
data. The CLP, or an equivalent designee, reports the
results of this analysis to the cancer committee at least
four times each calendar year.

Liaison Physician Selection Criteria
The Cancer Liaison Physician (CLP) is a required role in CoC-
accredited cancer programs.
Serves a three-year term with eligibility to serve an unlimited
number of terms based on performance as assessed by the
CoC and the cancer committee.
Is an active member of the medical staff.
Authorized to access facility-specific information that is
maintained in CoC Datalinks.
May also fulfill a leadership position on the cancer committee
such as chair, vice-chair, or quality improvement coordinator.

Liaison Physician Educational Requirements
Required to complete CLP orientation within three months
of initial appointment and on reappointment every three
years.
Will view all web-based CLP education programs provided
by the CoC each year. All CLP education is located in the
Cancer Liaison Program section of the CoC website.
Liaison Physician Primary Responsibility
At least four times each calendar year, the CLP reports and discusses
the facility’s performance as related to the accountability and quality
improvement measures in the Cancer Program Practice Profile Reports
(CP3R), and on data from additional NCDB reporting tools such as the
Cancer Quality Improvement Program (CQIP), the Rapid Quality
Reporting System (RQRS), Hospital Comparison Benchmark Reports, or
Survival Reports.
A quality-related audit is initiated for any of the accountability and
quality improvement measures that fall below required levels of
compliance.
Discussions related to facility performance are documented in the
cancer committee minutes and subsequently shared with the medical
staff and administration.
CLP reports do not fulfill the requirements for Standards 4.6 or 4.7.

Liaison Physician Secondary Responsibilities
Reports on CoC activities, initiatives, and priorities to the
cancer committee
Serves as liaison between the cancer program, the CoC, and
the American Cancer Society
Attends the CoC accreditation on-site survey and meets
with the surveyor to discuss the NCDB Quality Reporting
Tools and CLP responsibilities
Completes the CLP Activity Report annually
Uploads a copy of each CLP report presented to the cancer
committee into the SAR

Clarification
CLP or designee, MUST report at 4 separate meetings per
calendar year. If the CLP prepares the report, he/she can
designate another physician member to give the verbal
report.
The CLP can fulfill one additional leadership position within
the cancer committee(chair, coordinator) and represent one
of the required physician specialties.
Your CLP’s cancer committee report must include your
facilities data from the NCDB Reporting Tools (CQIP, CP3R,
RQRS, Survival Reports, or Hospital Comparison Benchmark
Reports).
SAR Documentation
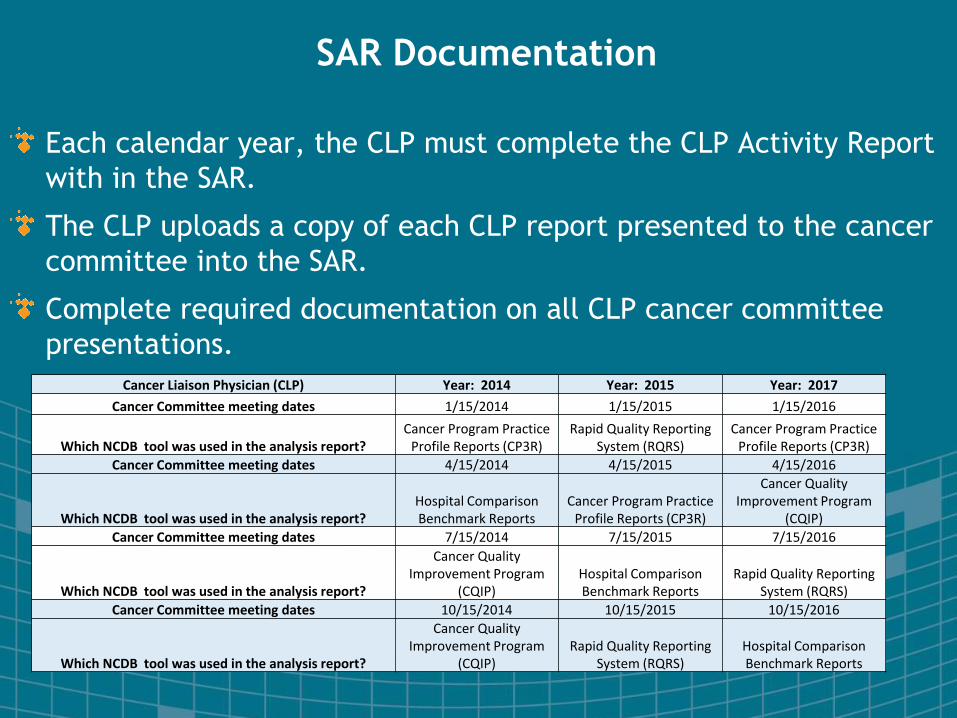
Each calendar year, the CLP must complete the CLP Activity Report
with in the SAR.
The CLP uploads a copy of each CLP report presented to the cancer
committee into the SAR.
Complete required documentation on all CLP cancer committee
presentations.
Cancer Liaison Physician (CLP) Year: 2014 Year: 2015 Year: 2017
Cancer Committee meeting dates 1/15/2014 1/15/2015 1/15/2016
Which NCDB tool was used in the analysis report?Cancer Program Practice
Profile Reports (CP3R)Rapid Quality Reporting
System (RQRS)Cancer Program Practice
Profile Reports (CP3R)
Cancer Committee meeting dates 4/15/2014 4/15/2015 4/15/2016
Which NCDB tool was used in the analysis report?Hospital Comparison Benchmark Reports
Cancer Program Practice Profile Reports (CP3R)
Cancer Quality Improvement Program
(CQIP)
Cancer Committee meeting dates 7/15/2014 7/15/2015 7/15/2016
Which NCDB tool was used in the analysis report?
Cancer Quality Improvement Program
(CQIP)Hospital Comparison Benchmark Reports
Rapid Quality Reporting System (RQRS)
Cancer Committee meeting dates 10/15/2014 10/15/2015 10/15/2016
Which NCDB tool was used in the analysis report?
Cancer Quality Improvement Program
(CQIP)Rapid Quality Reporting
System (RQRS)Hospital Comparison Benchmark Reports
Rating Compliance
For each calendar year:
The CLP generates reports that evaluate and interpret the
cancer program’s performance using NCDB data.
The CLP, or an equivalent designee, reports this information
to the cancer committee a minimum of four times.
The CLP is present during the CoC accreditation survey and
meets with the surveyor to discuss CLP activities and
responsibilities.
Cancer committee minutes are uploaded that document at
least four CLP reports on NCDB data, including actions and
response.

Standard 4.4 & 4.5 Accountability and Quality
Improvement Measures
Each calendar year, the expected Estimated Performance
Rates (EPR) is met for each accountability and quality
improvement measure as defined by the Commission on
Cancer
Definition and Requirements
Facilities are required to treat cancer patients according to nationally
accepted accountability and quality improvement measures as described
by the Cancer Program Practice Profile Reports (CP3R).
Accountability measures are standards of care derived from evidence-
based data and promote improvements in care delivery by demonstrating
provider accountability and promoting transparency.
Quality improvement measures are supported by evidence from
experimental studies. They monitor the need for quality improvement or
remediation of treatment provided. QI measures are intended for internal
monitoring of performance within a cancer program.
A corrective action plan must be developed and executed for any measure
not meeting the estimated performance rate (EPR).
Monitoring of all is measures documented in the cancer committee
minutes.

Standard 4.4 Accountability Measures
2012 2013 2014
BCSRT - Radiation is administered within 1 year (365 days)
of diagnosis for women under the age of 70 receiving breast
conservation surgery for breast cancer
90% 90% 90%
HT – Tamoxifen or third generation aromatase inhibitor is
considered or administered within 1 year (365 days) of
diagnosis for women with AJCC T1c or Stage II or Stage III
hormone receptor positive breast cancer
90% 90% 90%
MASTRT- Radiation therapy is considered or administered
following any mastectomy within 1 year (365 days) of
diagnosis of breast cancer for women with >= 4 positive
regional lymph nodes
90% 90% 90%
MEASURE EXPECTED EPR

Standard 4.5 Quality Improvement Measures
2012 2013 2014
nBx- image or palpation-guided needle biopsy (core or
FNA) is performed to establish diagnosis of breast cancer
80% 80% 80%
G15RLN-At least 15 regional lymph nodes removed and
pathologically examined for resected gastric cancer
N/A 80% 80%
12RLN-At least 12 regional lymph nodes are removed and
pathologically examined for resected colon cancer
85% 85% 85%
LCT- Systemic chemo is administered within 4 months to
day preoperatively of day of surgery to 6 months
postoperatively, or is considered for surgically resected
cases with (pN1) and (pN2) NSCLC
N/A 85% 85%
LNoSurg- Surgery is not the first course of treatment for
cN2, M0 lung cases
N/A 85% 85%
RECRTCT – Preop chemo and radiation are administered
for clinical AJCC T3N0, T4N0 or Stage III; or treatment is
considered; for patients under the age of 80 receiving
resection for rectal cancer
N/A 85% 85%
MEASURE EXPECTED EPR

Compliance Based on the Upper Limit of the
Confidence Interval
.

Non- Compliance Based on the Upper Limit of the
Confidence Interval
.

Specifications & Exceptions by Category
All programs fulfill both standards as written except programs in all
categories undergoing initial survey and PCP facilities.
Programs undergoing initial survey and PCP facilities are exempt from
these standards.
Expected EPRs for facilities that are part of an Integrated Network Cancer
Program (INCP) are evaluated individually and as an INCP as a whole.

Standard 4.4 and 4.5 Clarifications
All quality and accountability measures do not need to be
discussed at the same cancer committee meeting.
The Surveillance measures do not need to be discussed by
the cancer committee to meet Standards 4.4 and 4.5.
If the measure compliance issue is due to low patient
volume or the patient refused that piece of the treatment,
then noting that the issue was investigated and a reason
identified would be appropriate documentation in
replacement of an action plan.

SAR Documentation Std. 4.4
.

SAR Documentation Std. 4.5
.

Rating Compliance
For Each calendar year:
The cancer committee monitors the program’s expected EPR
for all accountability and quality improvement measures using
the CP3R.
The monitoring activity is reported and documented in the
cancer committee minutes.
For each, the quality reporting tools show a performance rate
equal to or greater than the expected Estimated Performance
Rates specified by the CoC, or the program has implemented
an action plan that reviews and addresses program
performance below the expected EPR.
Standard 4.6 Monitoring Compliance with
Evidence-Based Guidelines
Each calendar year, the cancer committee designates a
physician member to complete an in-depth analysis to
assess and verify that cancer program patients are
evaluated and treated according to evidence-based
national treatment guidelines. Results are presented to the
cancer committee and documented in cancer committee
minutes.

Definition and Requirements
Each calendar year, a physician member of the cancer committee
performs an in-depth review to examine the evaluation and
treatment of patients and ensure that it is compliant with evidence-
based national guidelines using AJCC stage or other appropriate
staging system, including prognostic indicators.
The analysis must aim to determine if the diagnostic evaluation is
adequate and the treatment plan is concordant with a recognized
guideline.
Any problems identified with the diagnostic evaluation or treatment
planning process may serve as a source for performance
improvement.
The completion of this analysis and treatment discussions of
patients at cancer conferences do not fulfill the requirement for
this Standard.

Annual In-Depth Analysis
Sources for the Assessment
A cancer site-specific sample
Review of a single treatment regimen for a specific cancer site
A determination that the first course of therapy is concordant
with evidence based national treatment guidelines and/or
prognostic indicators.
A reporting format that permits analysis and provides an
opportunity to recommend performance improvements based
on data from the analysis.
The formal report with the analysis results is presented to the
cancer committee and documented in the cancer committee
minutes.

Clarifications
Studies can be completed by any physician on the cancer
committee.
Studies count for the year they are completed and reported to
the cancer committee.
Review of data that are required for Standards 4.4 and 4.5
cannot be used to satisfy this requirement.

SAR Documentation
Cancer committee minutes that document presentation of the results of
the analysis are uploaded to the SAR.
The site included in the analysis, the name of the physician completing the
analysis and the date of presentation to cancer committee are
documented in the SAR.
All studies are uploaded to the SAR.
Date Analysis was
Reported to the
Cancer Committee
Name of Physician
Member from the Cancer
Committee Selected to
Complete Analysis
Cancer Site
Reviewed
4/11/2014 Stan Smith, MD Breast
10/14/2015 Mark Brewer, MD Prostate
10/12/2016 Leslie Carpenter, MD Colorectal

Rating Compliance
For Each calendar year:
A physician member of the cancer committee is selected to
conduct an in-depth analysis to ensure that evaluation and
treatment provided to patients is compliant with evidence-
based national treatment guidelines and is appropriate for
AJCC stage or other appropriate staging system, including
prognostic indicators.
The analysis results are reported to the cancer committee.
The analysis results are documented in the cancer committee
minutes.

Standard 4.7 Studies of Quality
Each calendar year, the cancer committee, under the
guidance of the Quality Improvement Coordinator,
develops, analyzes, and documents the required number of
studies (based on the program category) that measure the
quality of care and outcomes for cancer patients.

Quality Improvement Coordinator
Monitors, reports and recommends activity related to the
quality improvement program
Reports regularly to the cancer committee
Recommends corrective actions if any area falls below
acceptable norms or when undesirable performance is
identified
The recommendations and improvements are reported to the
cancer committee and documented in the minutes
A Cancer Registrar CANNOT be named as your Quality
Improvement Coordinator

Definition and Requirements
Annual evaluation of care provides a baseline to measure quality
and an opportunity to correct or enhance care and quality
outcomes.
Quality improvement efforts focus on evaluating areas of cancer
care and must include multidisciplinary representation from
clinical, administrative, and patient perspectives.
Study topics must be selected based on a problematic quality-
related issue relevant to the cancer program and local cancer
patient population, and used as a means to identify a potential
issue or understand why a problem is occurring.
Quality studies can evaluate various spectrums of cancer care,
including diagnosis, treatment, and supportive care of patients.
Includes issues related to structure, process, and outcomes.

Required Quality Study Components
Study topic that identifies a problematic quality-related issue
within the cancer program
Define methodology and criteria for evaluation, including data need
to evaluate or answer the quality-related question
Conduct the study according to the identified measures and
methodology
Summary of the study findings
Comparison to national benchmarks or guidelines
Corrective action plan based on evaluation of the data
Follow-up steps to monitor the actions implemented

Specifications
Studies that do not meet the requirements for this standard
include:
Quality studies that duplicate topics or studies from year-to-year
Ongoing monitoring activities following a completed quality study
Survival studies and the in-depth analysis used in Standard 4.6
Review of data presented in the NCDB data reports and tools
A study that is required by an outside, recognized
organization related to oncology is acceptable if it follows the
required study criteria outlined in the previous slides.

Specifications by Category
All programs fulfill the standard as written. The number of studies
required is based on Program Category.
7 Steps to Completing a Study of Quality
Appoint a Quality Improvement Coordinator (QIC) to oversee study
activities.
Identify a Problem.
Define how the study will be conducted.
Conduct the study according to the identified. methodology and
measures, and organize the data collection.
Prepare an analysis summary of the study findings and results.
Compare the data results obtained following the completion of the
quality study with an applicable national benchmark or guideline.
Design a corrective action plan (quality improvement) based on
evaluation of the data.

Clarifications
Standard 4.7 is about identifying a problematic quality-related issue
and conducting a study to understand what is causing the problem.
Studies count for the year they are completed and reported to the
cancer committee. Discussion at a sub-committee does not fulfill
this requirement.
Studies that are duplicative of a previous quality study or ongoing
monitors done over multiple years do not meet the requirements for
this standard.
A benchmark is a standard or a measure against which the
performance/data can be compared. If national benchmarks such as
NCCN Guidelines are not available, related published articles may
be used.

SAR Documentation
Rating Compliance
For Each calendar year:
Based on category, the Quality Improvement Coordinator,
under the direction of the cancer committee, develops and
conducts the required number of quality studies.
The results of the required number of quality studies are
analyzed.
The results of the required number of quality studies are
reviewed by the cancer committee and documented in the
meeting minutes.

Standard 4.8 Quality Improvements
Each calendar year, the cancer committee, under the
guidance of the Quality Improvement Coordinator,
implements two cancer care improvements. One
improvement is based on the results of a quality study
completed by the cancer program that measures the quality
of cancer care and outcomes. One improvement can be
based on a completed study from another source. Quality
improvements are documented in the cancer committee
minutes and shared with medical staff and administration.
Definition and Requirements
Quality or performance improvements are the actions taken,
processes implemented, or services created to improve cancer
care.
Sources for quality improvements may include:
Actions based on analysis and findings of a quality study under Standard
4.7
Actions to address substandard patient care or process performance
Changes to improve upon acceptable patient care or process
performance
Each year, one improvement must be based on the results of a
quality study completed by the cancer program that measures
the quality of cancer care and outcomes.

Clarifications
A quality improvement is an improvement affecting cancer
patient care that has been implemented based on evidence from
either a quality study or another relevant data source.
Quality improvements count for the year in which they are
implemented.
Documentation in the cancer committee minutes must include
when the improvement was implemented and when the
improvement was communicated to administration and the
medical staff.
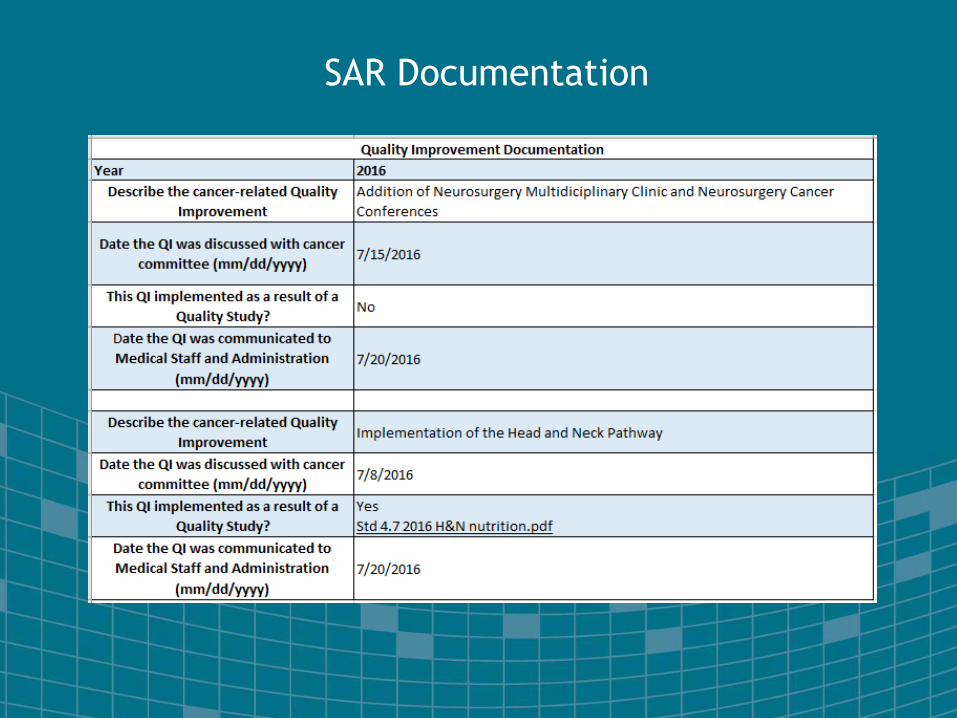
SAR Documentation
.

Rating Compliance
For Each calendar year:
The cancer committee, under the guidance of the Quality
Improvement Coordinator, implements one cancer care
improvement based on the results of a completed quality
study.
The cancer committee, under the guidance of the Quality
Improvement Coordinator, implements on cancer care
improvement based on any study or data source.
The quality improvements are reviewed by the cancer
committee and documented in the minutes.
The quality improvements are shared with medical staff and
administration.

Required Documentation for Chapter 4: Patient Outcomes
STANDARD DOCUMENTATION COMMENT
4.1: Cancer Prevention Programs Cancer committee minutes documenting the cancer
committee identifying the cancer prevention needs of the
community and documentation that the committee offered
at least one cancer prevention activity that is focused on
decreasing the number of diagnoses of a specific type of
cancer. The documentation includes references to the
national guidelines used.
Complete and upload for each
calendar year.
4.2: Cancer Screening Programs Cancer committee minutes documenting the cancer
committee identifying the cancer screening needs of the
community and documentation that the committee offered
at least one cancer screening activity focused decreasing
late stage disease of a specific type of cancer. The
documentation includes references to the national
guidelines and interventions used and the process in
place to follow up on positive findings.
Complete and upload for each
calendar year.
4.3: Cancer Liaison Physician
Responsibilities
Cancer committee minutes and the CLP reports on
NCDB data that are presented to the cancer committee at
four separate meetings each calendar year.
Complete and upload for each
calendar year.
4.4 and 4.5: Accountability
Measures & Quality Improvement
Measures
• Cancer committee minutes that demonstrate the
monitoring of the accountability and quality improvement
measures from the CP3R.
• If necessary, the action plan that was developed and
executed if the program’s performance rates were
observed to be below the expected EPRs established by
the CoC.
Complete and upload for each
calendar year
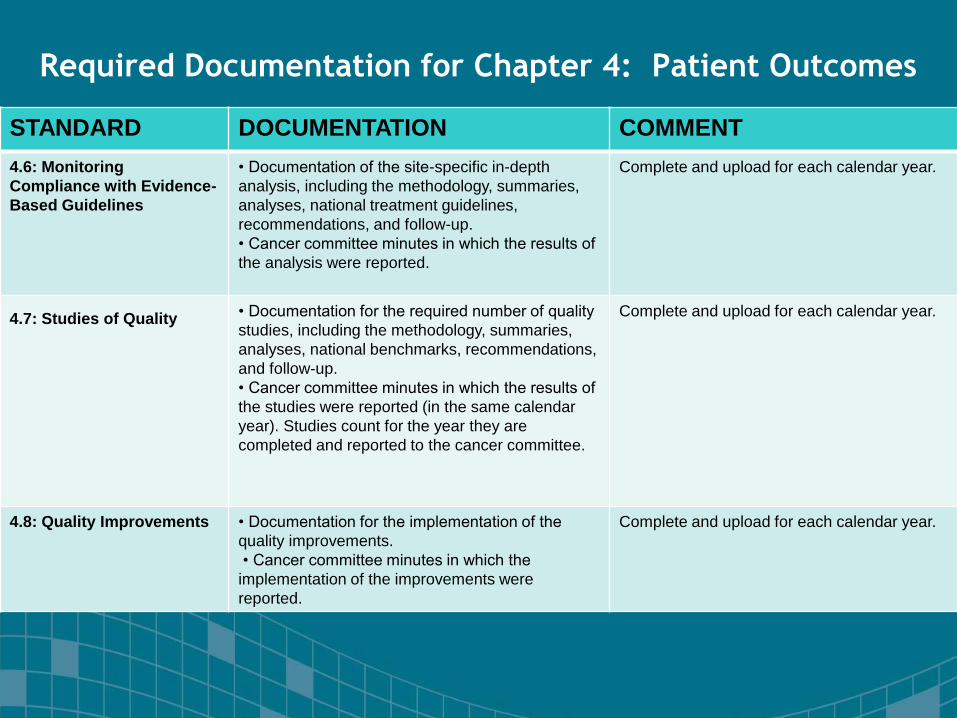
Required Documentation for Chapter 4: Patient Outcomes
STANDARD DOCUMENTATION COMMENT
4.6: Monitoring
Compliance with Evidence-
Based Guidelines
• Documentation of the site-specific in-depth
analysis, including the methodology, summaries,
analyses, national treatment guidelines,
recommendations, and follow-up.
• Cancer committee minutes in which the results of
the analysis were reported.
Complete and upload for each calendar year.
4.7: Studies of Quality • Documentation for the required number of quality
studies, including the methodology, summaries,
analyses, national benchmarks, recommendations,
and follow-up.
• Cancer committee minutes in which the results of
the studies were reported (in the same calendar
year). Studies count for the year they are
completed and reported to the cancer committee.
Complete and upload for each calendar year.
4.8: Quality Improvements • Documentation for the implementation of the
quality improvements.
• Cancer committee minutes in which the
implementation of the improvements were
reported.
Complete and upload for each calendar year.

Documentation Requirements Resources
CAnswer Forum http://cancerbulletin.facs.org/forums/
Standards Resource Library
http://cancerbulletin.facs.org/forums/CAnswerForumHome/StandardResourc
eLibrary
Cancer Program Standards: Ensuring Patient-Center Guidelines 2016

QUESTIONS
FYI
This webinar has been awarded 1 CEU by NCRA
You must be registered and logged in to receive a
Certificate of Attendance which will be emailed to you
within 3 weeks
This webinar is being recorded and the recording, slide
deck and Q&A will be made available at our website:
Oncolog.com “VIEW OUR WEBINARS” within 2 weeks

Next Webinar
Meeting CoC Standards
Chapter 5
Data Quality
February 21, 2018

Thank you
We appreciate your time today.
To schedule a demo of
Oncolog Registry software or speak to someone, please call
800-345-6626.
Visit us at: www.oncolog.com
To schedule a demo of
OncoNav Nurse Navigation software or speak to someone, please call
888-369-1791