menke’s kinky hair syndrome - a spectrum of clinico-radiological findings
TRANSCRIPT

Menke’s Kinky Hair Syndrome - A Spectrum of Clinico-Radiological findings
Case Report
Menke’s kinky hair syndrome e A spectrumof clinico-radiological findings
Alka Agrawal a, P.S. Tripathi b, Abhishree Geda c,*, Neha Nischal c
aAssociate Professor, Department of Radiodiagnosis, MGMMC & MY Hospital, Indore, M.P. 452001, IndiabAssisstant Professor, Department of Radiodiagnosis, MGMMC & MY Hospital, Indore, M.P. 452001, IndiacResident, Department of Radiodiagnosis, MGMMC & MY Hospital, Indore, M.P. 452001, India
a r t i c l e i n f o
Article history:
Received 23 October 2012
Accepted 18 February 2013
Available online 26 February 2013
Keywords:
Menkes disease
Copper metabolism
Pili torti
Tortuous intracranial vessels
Cerebral atrophy
a b s t r a c t
Menkes kinky hair syndrome is a fatal rare inherited neurodegenerative disease due to
deranged copper metabolism. The manifestations begin after 2e3 months of life with
developmental delay, intractable convulsions, typical facies and pili torti. Specific imaging
findings which strongly point towards the diagnosis include symmetrical bony spurs
around the knee joints, bladder diverticulas & brain atrophy with corkscrew tortuosity of
intra & extracranial vessels. Low serum copper and ceruloplasmin are confirmatory for the
disease. Here we present an interesting case with all classical findings of Menkes disease.
Copyright ª 2013, Indraprastha Medical Corporation Ltd. All rights reserved.
1. Case report
A 7-month-old male infant presented with progressively
increasing partial seizures with secondary generalisation
since one month. The history suggested a regression of pre-
viously achieved milestones such as smiling, recognition of
faces, cooing & playing with objects. The child had never
achieved head holding. The child was born to non-consan-
guineous parents and had an institutional normal vaginal
delivery at term with history of delayed cry.
There was a positive family history of successive
births of two male children with similar appearances &
complaints to the mother’s sister. Both these children sur-
vived for 3e4 months of age & neither of them was investi-
gated.
On examination, patient had lack of visual contact and
head holding with generalized hypotonia and lethargy. There
was microcephaly with parietal bossing. There were charac-
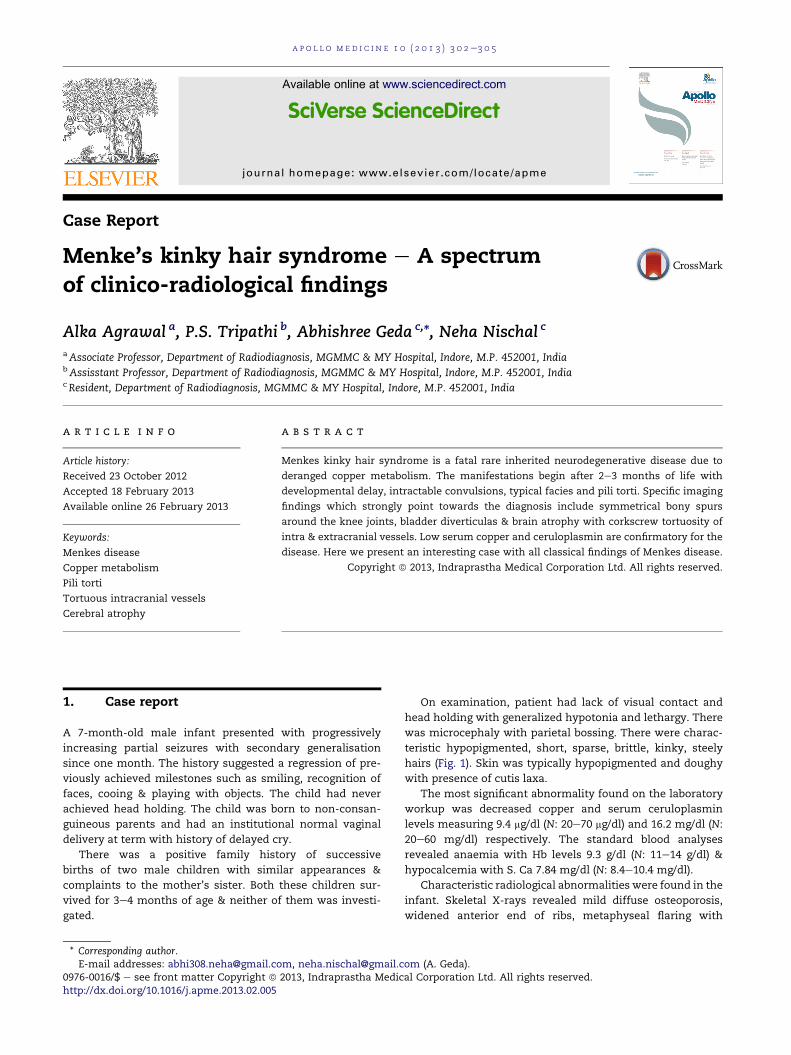
teristic hypopigmented, short, sparse, brittle, kinky, steely
hairs (Fig. 1). Skin was typically hypopigmented and doughy
with presence of cutis laxa.
The most significant abnormality found on the laboratory
workup was decreased copper and serum ceruloplasmin
levels measuring 9.4 mg/dl (N: 20e70 mg/dl) and 16.2 mg/dl (N:
20e60 mg/dl) respectively. The standard blood analyses
revealed anaemia with Hb levels 9.3 g/dl (N: 11e14 g/dl) &
hypocalcemia with S. Ca 7.84 mg/dl (N: 8.4e10.4 mg/dl).
Characteristic radiological abnormalities were found in the
infant. Skeletal X-rays revealed mild diffuse osteoporosis,
widened anterior end of ribs, metaphyseal flaring with
* Corresponding author.E-mail addresses: [email protected], [email protected] (A. Geda).
Available online at www.sciencedirect.com
journal homepage: www.elsevier .com/locate /apme
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 3 0 2e3 0 5
0976-0016/$ e see front matter Copyright ª 2013, Indraprastha Medical Corporation Ltd. All rights reserved.http://dx.doi.org/10.1016/j.apme.2013.02.005
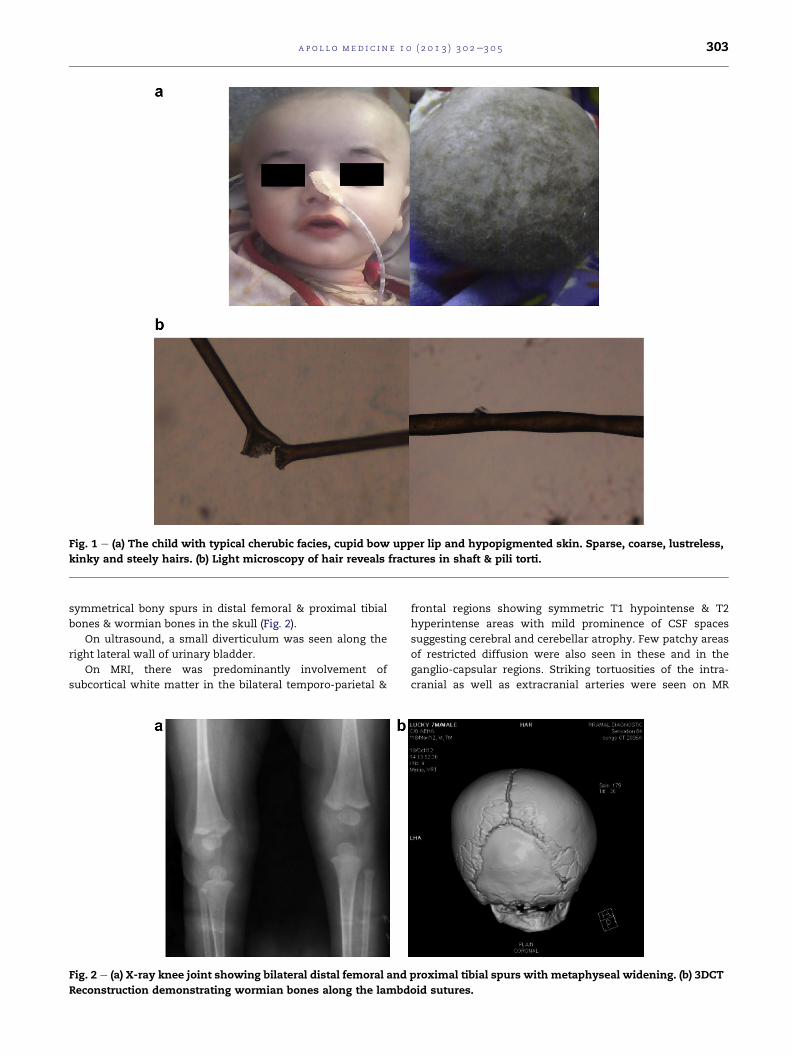
symmetrical bony spurs in distal femoral & proximal tibial
bones & wormian bones in the skull (Fig. 2).
On ultrasound, a small diverticulum was seen along the
right lateral wall of urinary bladder.
On MRI, there was predominantly involvement of
subcortical white matter in the bilateral temporo-parietal &
frontal regions showing symmetric T1 hypointense & T2
hyperintense areas with mild prominence of CSF spaces
suggesting cerebral and cerebellar atrophy. Few patchy areas
of restricted diffusion were also seen in these and in the
ganglio-capsular regions. Striking tortuosities of the intra-
cranial as well as extracranial arteries were seen on MR
Fig. 1 e (a) The child with typical cherubic facies, cupid bow upper lip and hypopigmented skin. Sparse, coarse, lustreless,
kinky and steely hairs. (b) Light microscopy of hair reveals fractures in shaft & pili torti.
Fig. 2 e (a) X-ray knee joint showing bilateral distal femoral and proximal tibial spurs with metaphyseal widening. (b) 3DCT
Reconstruction demonstrating wormian bones along the lambdoid sutures.
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 3 0 2e3 0 5 303
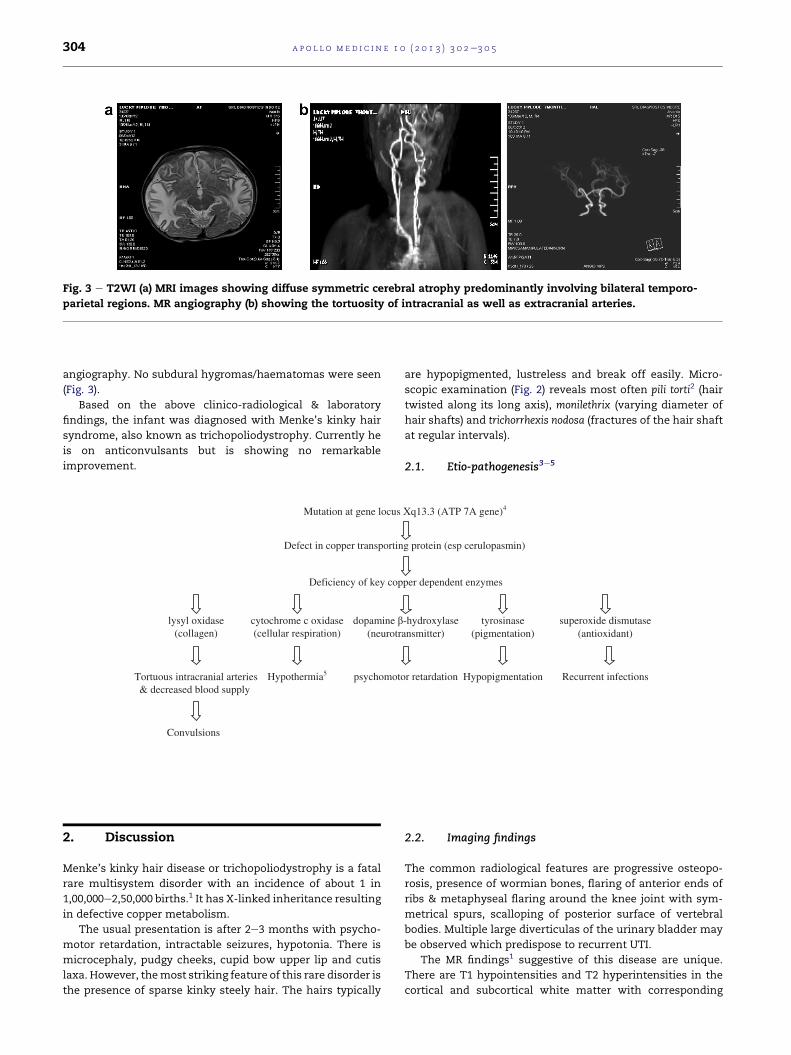
angiography. No subdural hygromas/haematomas were seen
(Fig. 3).
Based on the above clinico-radiological & laboratory
findings, the infant was diagnosed with Menke’s kinky hair
syndrome, also known as trichopoliodystrophy. Currently he
is on anticonvulsants but is showing no remarkable
improvement.
2. Discussion
Menke’s kinky hair disease or trichopoliodystrophy is a fatal
rare multisystem disorder with an incidence of about 1 in
1,00,000e2,50,000 births.1 It has X-linked inheritance resulting
in defective copper metabolism.
The usual presentation is after 2e3 months with psycho-
motor retardation, intractable seizures, hypotonia. There is
microcephaly, pudgy cheeks, cupid bow upper lip and cutis
laxa. However, themost striking feature of this rare disorder is
the presence of sparse kinky steely hair. The hairs typically
are hypopigmented, lustreless and break off easily. Micro-
scopic examination (Fig. 2) reveals most often pili torti2 (hair
twisted along its long axis), monilethrix (varying diameter of
hair shafts) and trichorrhexis nodosa (fractures of the hair shaft
at regular intervals).
2.1. Etio-pathogenesis3e5
2.2. Imaging findings
The common radiological features are progressive osteopo-
rosis, presence of wormian bones, flaring of anterior ends of
ribs & metaphyseal flaring around the knee joint with sym-
metrical spurs, scalloping of posterior surface of vertebral
bodies. Multiple large diverticulas of the urinary bladder may
be observed which predispose to recurrent UTI.
The MR findings1 suggestive of this disease are unique.
There are T1 hypointensities and T2 hyperintensities in the
cortical and subcortical white matter with corresponding
Mutation at gene locus Xq13.3 (ATP 7A gene)4
Defect in copper transporting protein (esp cerulopasmin)
Deficiency of key copper dependent enzymes
lysyl oxidase(collagen)
cytochrome c oxidase(cellular respiration)
dopamine -hydroxylase tyrosinase superoxide dismutase(neurotransmitter) (pigmentation) (antioxidant)
Hypothermia5 psychomotor retardation Hypopigmentation Recurrent infectionsTortuous intracranial arteries& decreased blood supply
Convulsions
Fig. 3 e T2WI (a) MRI images showing diffuse symmetric cerebral atrophy predominantly involving bilateral temporo-
parietal regions. MR angiography (b) showing the tortuosity of intracranial as well as extracranial arteries.
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 3 0 2e3 0 5304

hypointensities on FLAIR image, widening of CSF spaces and
prominence of cerebellar folia suggestive of severe neuronal
loss. Vascular compromise leads to demyelination of the
whitematter tracts. Theremay be areas of restricted diffusion
secondary to diffuse white matter ischaemia. Bilateral large
subdural hygromas suggests hemorrhages of different ages.
MR angiography reveals elongated and tortuous intra as
well as extracranial vessels (corkscrew pattern) which are
characteristic of the disease. MR spectroscopy shows elevated
lactate and reduced N-acetylaspartate (NAA)ecreatine (Cr)
ratio. The normalisation of MRS features suggests favourable
response to copper histidine treatment.
2.3. Laboratory findings
Low serum copper and ceruloplasmin levels5 are diagnostic
for the disease. Other supportive lab findings include hyper-
calciuria, albuminuria, aminoaciduria and increased excre-
tion of b2 microglobulin. Urinary homovanillic acid/
vanillylmandelic acid ratio �4 strongly suggests the disease
and thus could be used for screening.
2.4. Differential diagnosis
Presence of metaphyseal widening makes rickets an impor-
tant differential for this disease. Another common differential
for presence of subdural haematomas of different ages is
battered baby syndrome. However, the neurodevelopmental
history, typical hair and biochemical markers as described are
specific for Menkes syndrome.
3. Conclusion
The diagnosis in our case was made based on clinico-
radiologic and laboratory findings. Treatment of the disease
is conservative with anticonvulsants. Copper supplements
like intravenous copper or copper histidine have been tried.
Copper histidine was not given in our case due to lack of
availability.
Conflicts of interest
All authors have none to declare.
r e f e r e n c e s
1. Datta Asok K, Ghosh Taraknath, Nayak Kaustav,Ghosh Mrinalkanti. Menkes kinky hair disease: a case report.Cases J. 2008;1:158. http://dx.doi.org/10.1186/1757-1626-1-158.
2. Gandhi Rozil, Kakkar Ritu, Rajan Sajeev, Bhangale Rashmi,Desai Shrinivas. Menkes kinky hair syndrome: a rareneurodegenerative disease. Case Rep Radiol. 2012;2012:684309.
3. Kamolsilp MD Mahattana. Menkes syndrome: a case report.J Med Assoc Thai. 2005;88(suppl 3):S290eS294.
4. Tumer Zeynep, Møller Lisbeth B. Menkes disease. Eur J HumGenet. 2010 May;18(5):511e518.
5. Barzegar Mohammad, Fayyazie Afshin, Gasemie Bobollah,Shoja Mohammad Ali Mohajel. Menkes disease: report of twocases. Iran J Pediatr. 2007;17(3):388e392.
a p o l l o m e d i c i n e 1 0 ( 2 0 1 3 ) 3 0 2e3 0 5 305
Apollo hospitals: http://www.apollohospitals.com/Twitter: https://twitter.com/HospitalsApolloYoutube: http://www.youtube.com/apollohospitalsindiaFacebook: http://www.facebook.com/TheApolloHospitalsSlideshare: http://www.slideshare.net/Apollo_HospitalsLinkedin: http://www.linkedin.com/company/apollo-hospitalsBlog:Blog: http://www.letstalkhealth.in/