meredith cook mercer cophs august, 2012. beers criteria ags and interdisciplinary panel of 11...
TRANSCRIPT
American Geriatrics Society Updated Beers Criteria for Potentially
Inappropriate Medication Use in Older Adults
Meredith CookMercer COPHS
August, 2012
Beers CriteriaAGS and interdisciplinary panel of 11 experts
in geriatrics and pharmacotherapy53 medications or medication classesThree categories:
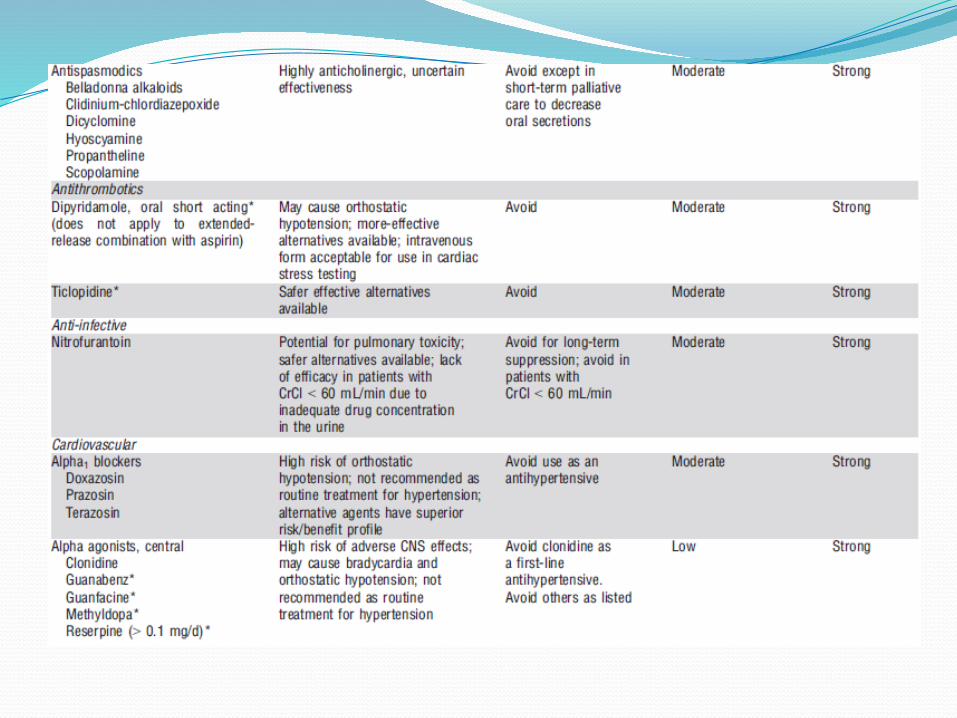
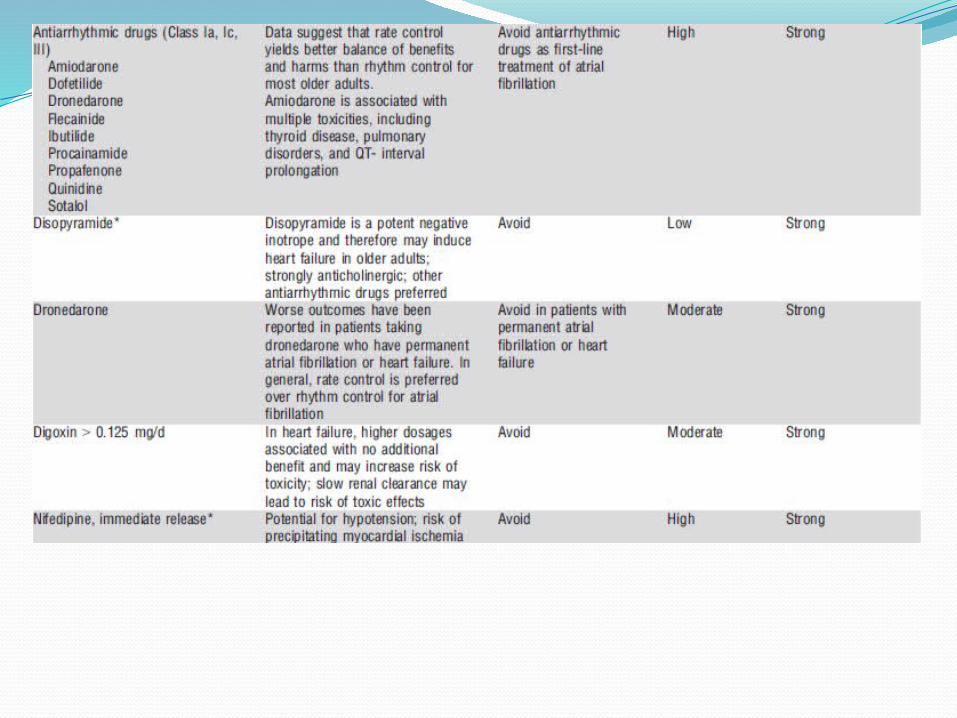
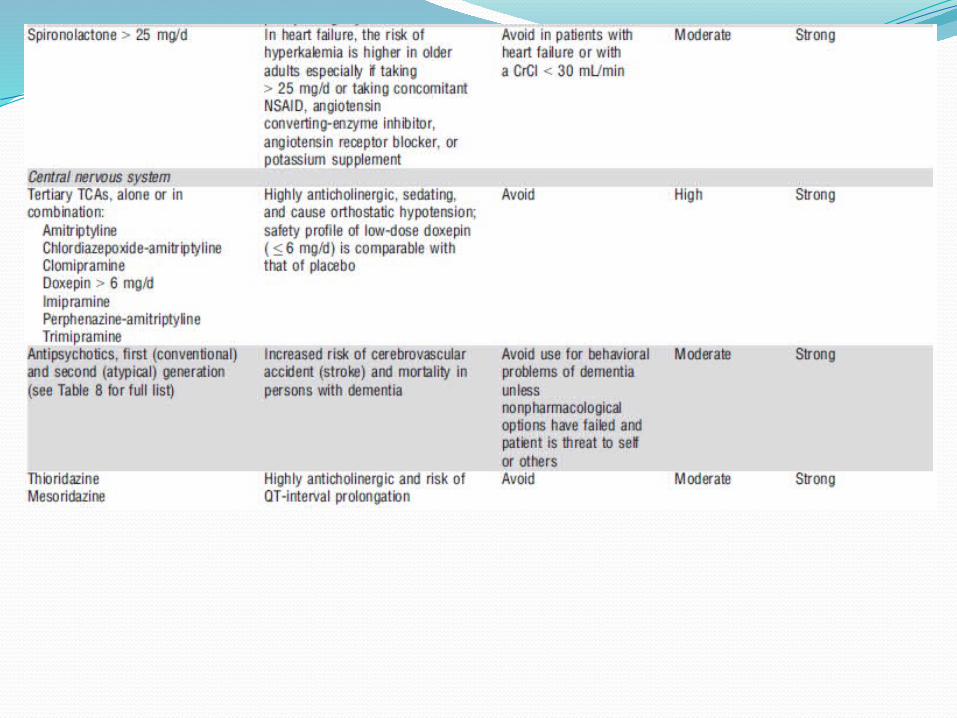
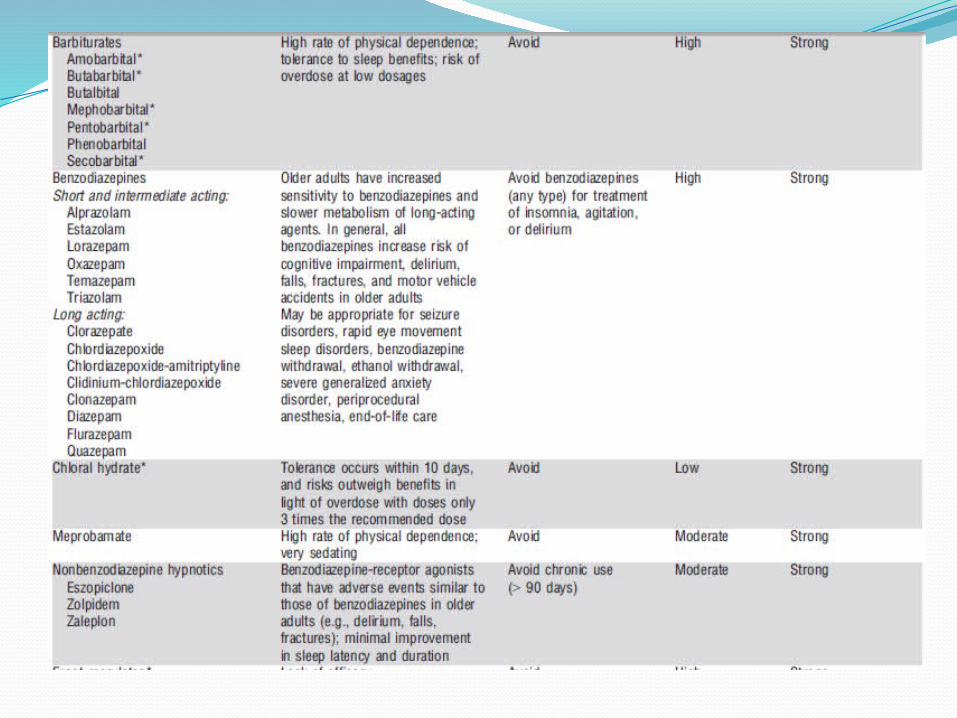
Potentially inappropriate medications and classes to AVOID in older adults
Potentially inappropriate medications and classes to AVOID in older adults with certain diseases and syndromes
Medications to be used in CAUTION in older adults
Beers CriteriaThis update will allow for:
Closer monitoring of medication useReal-time e-prescribing and interventions to
decrease adverse drug events in older adultsBetter patient outcomes
Medication Related ProblemsCommon, costly, and often preventable27% of ADE’s in primary care and 42% of
ADE’s in LTC were PREVENTABLE Most problems occurred at ordering and
monitoring stages of therapyTotal healthcare expenditures related to use
of PIMs was $7.2 billion in 2000/2001 Medical Expenditure Panel Survey
Medication Related ProblemsExplicit Criteria – unfavorable balance of risk
vs. benefit – consider alternate therapyImplicit Criteria – therapeutic duplication and
drug-drug interactions
Both of these have been taken into consideration when compiling the Beers List
PIMsLimited effectiveness in older adultsAssociated with serious problems, such as:
delirium, GI bleeding, falls, and fractures“Less is more” approachBeers List is now an important quality
measure with CMS, Medicare Part D, NCQA, HEDIS, and PQA
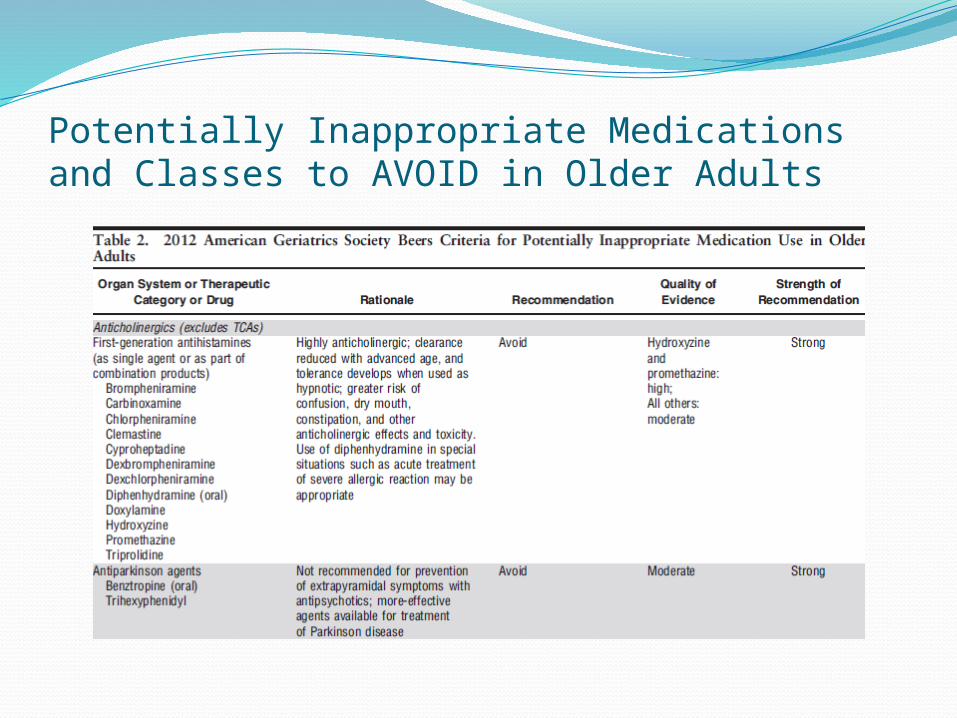
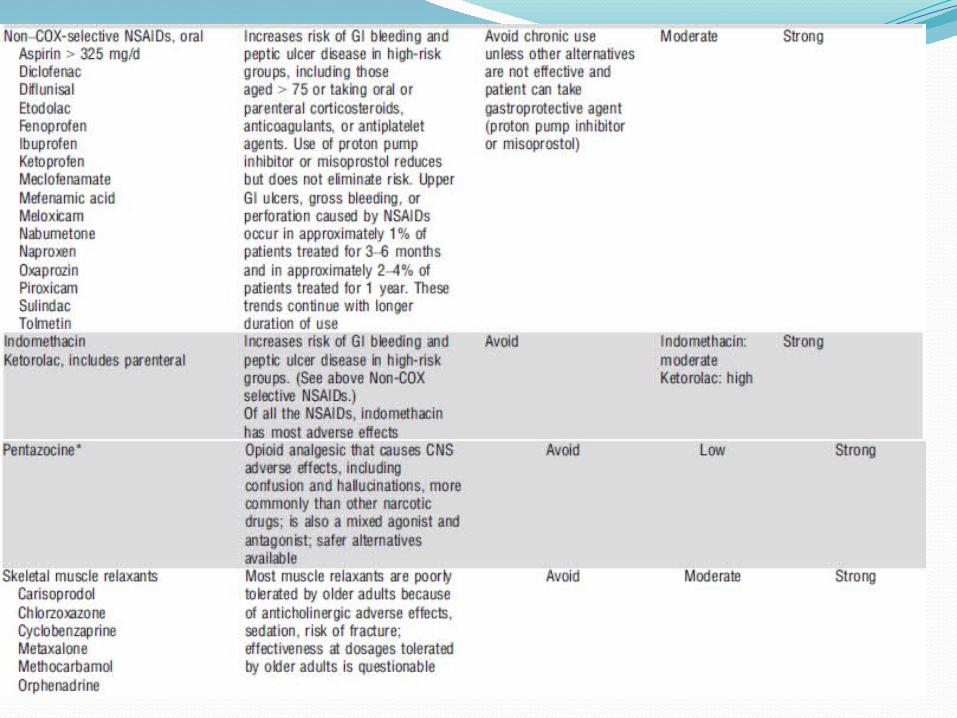
Potentially Inappropriate Medications and Classes to AVOID in Older Adults
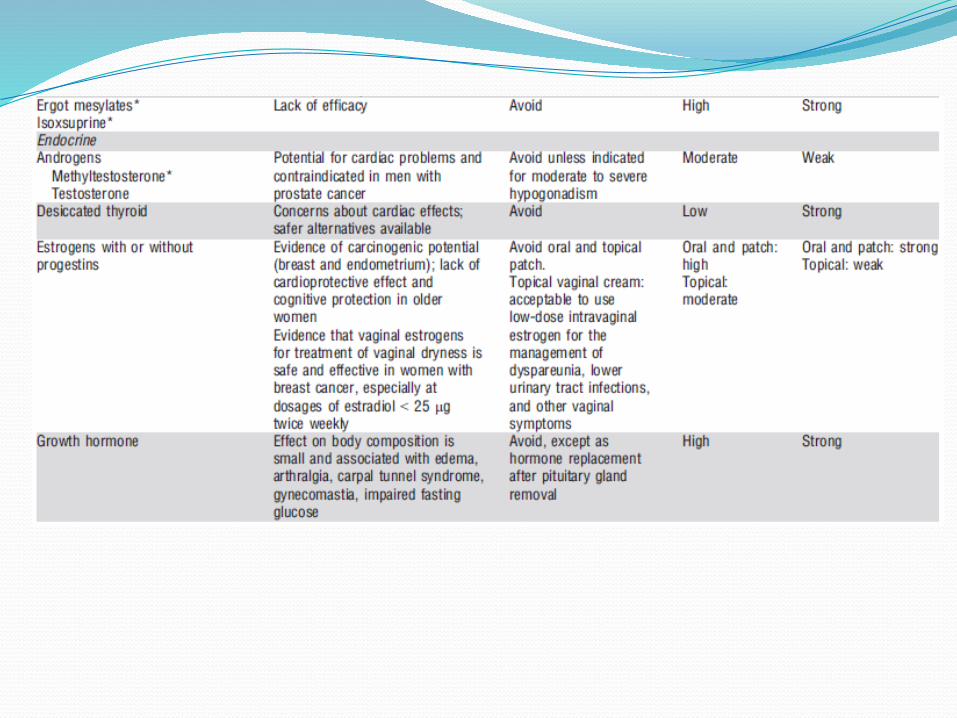
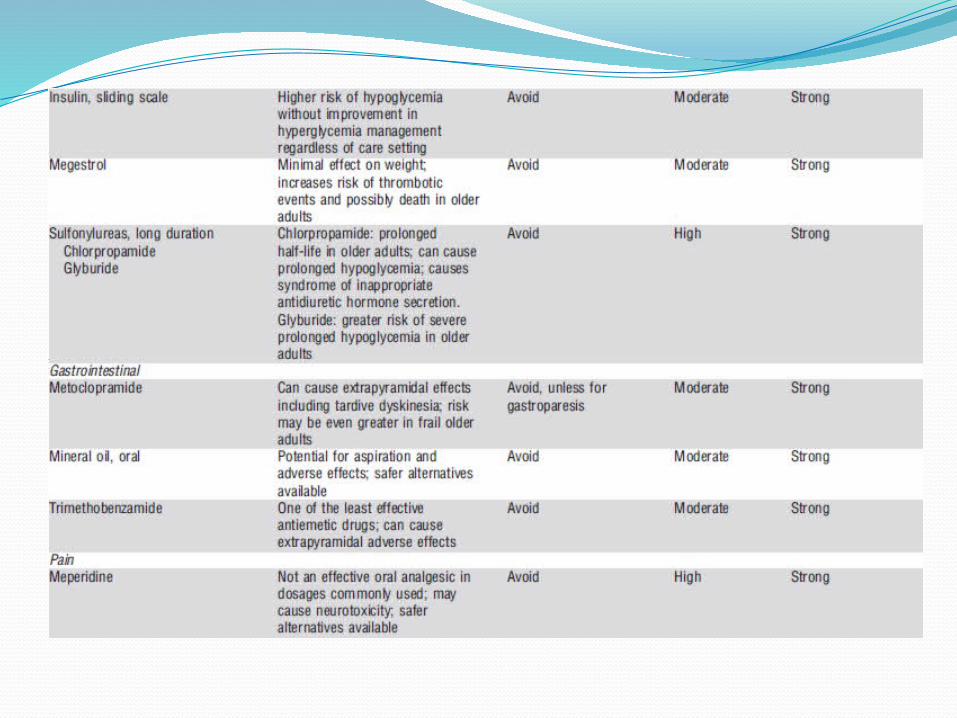
New AdditionsMegestrolGlyburideSliding-scale insulin
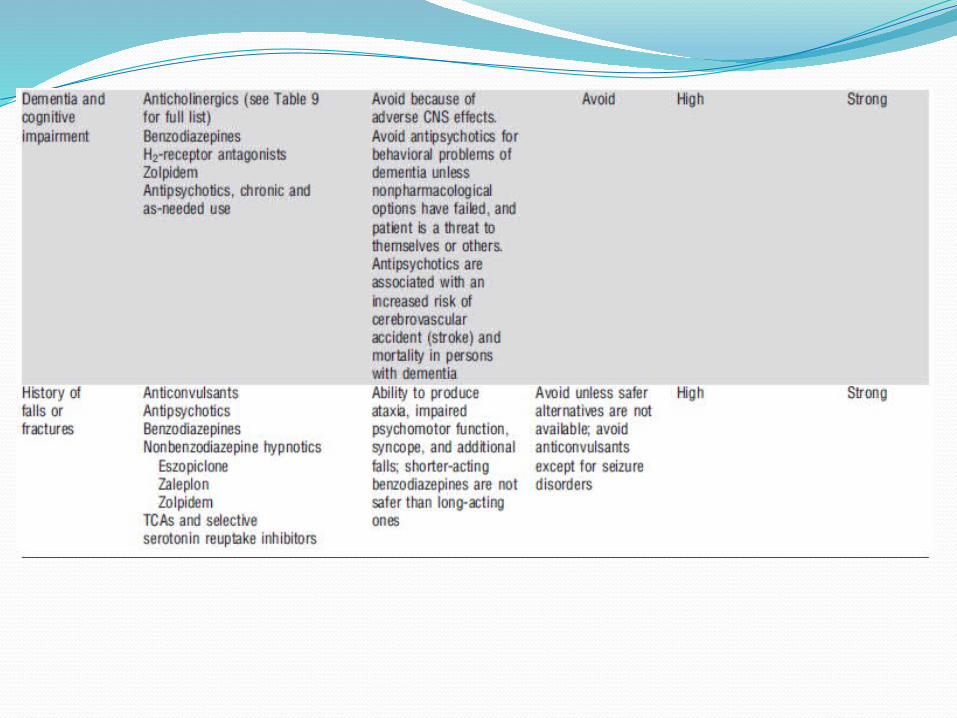
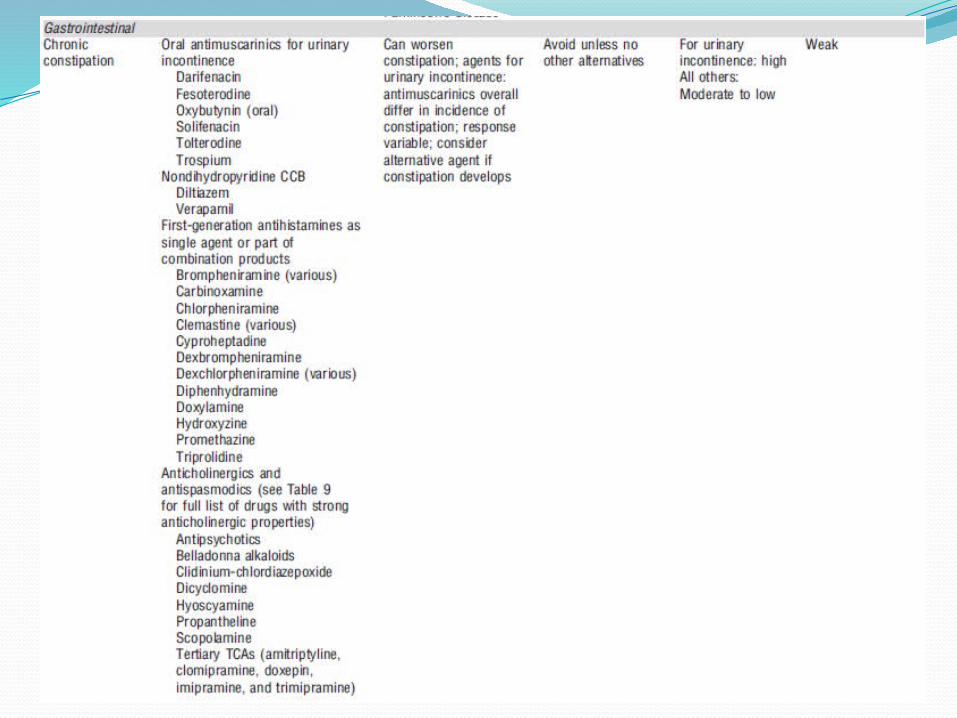
Potentially Inappropriate Medications and Classes to Avoid in Older Adults with Certain Diseases and Syndromes
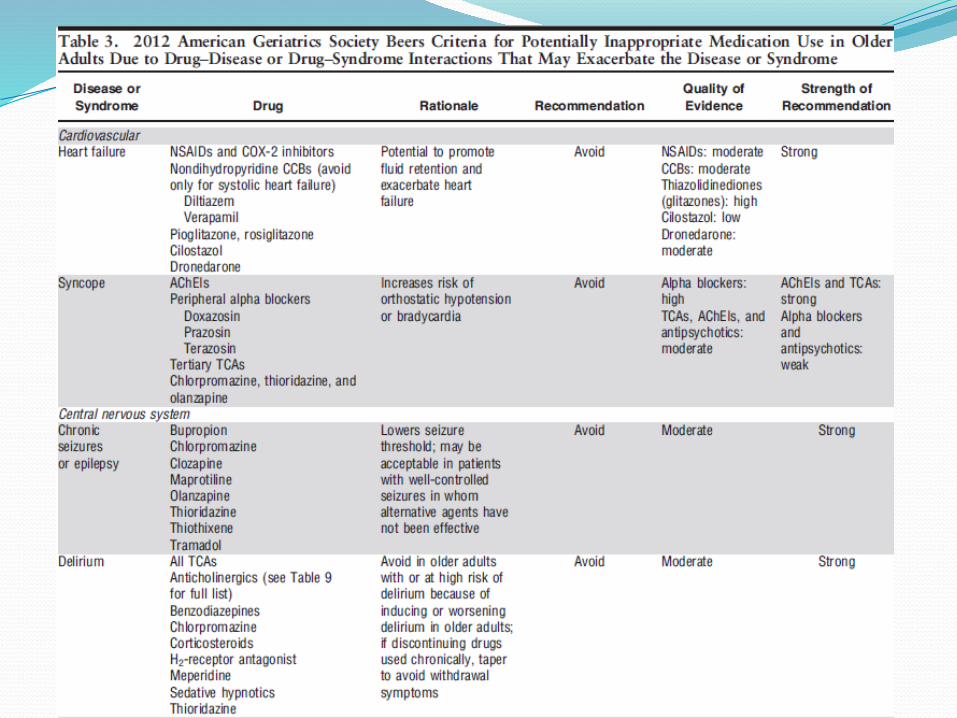

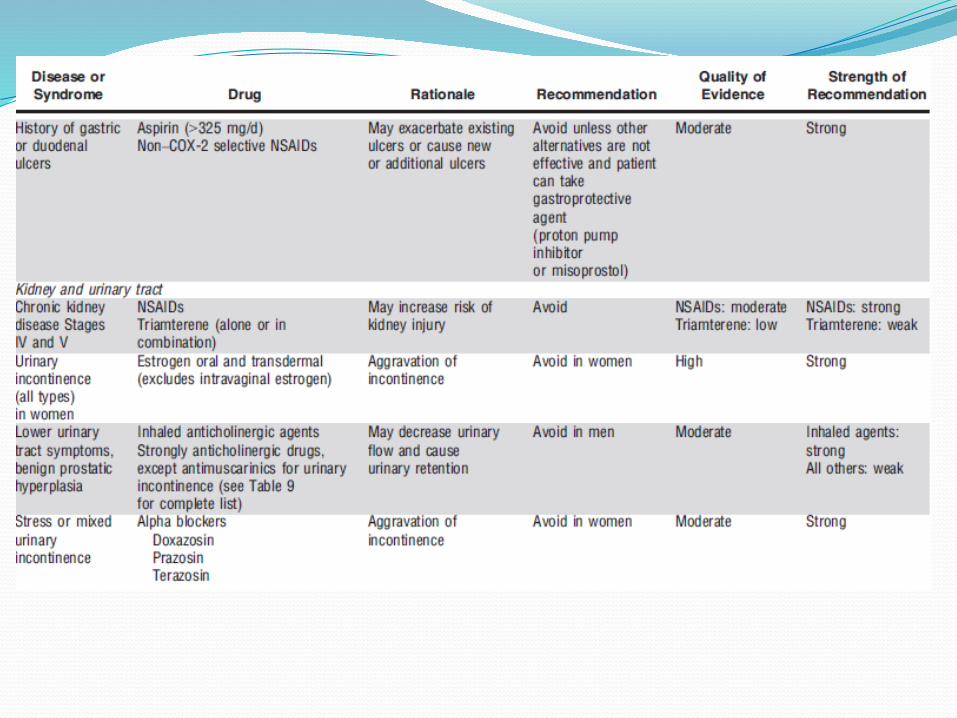
New AdditionsThiazolidinediones or Glitazones with CHFAcetylcholinesterase inhibitors with history of
syncopeSSRIs with falls and fractures
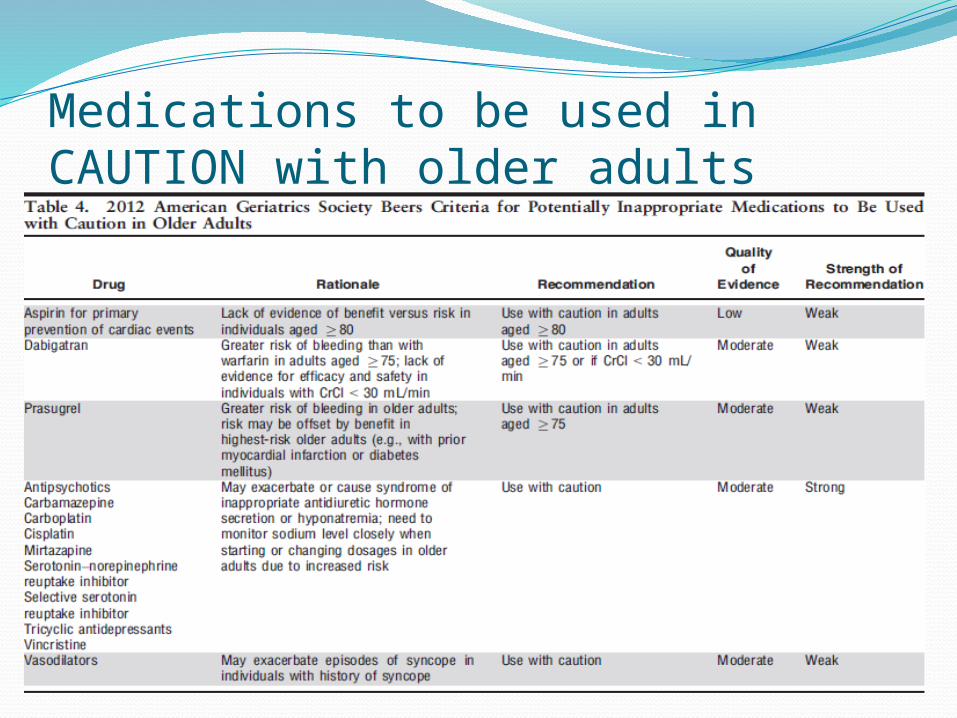
Medications to be used in CAUTION with older adults

New AdditionsAnti-thrombotics – caution in 75 years and
older

Removed Since 2003 (Last Update)

ConclusionsPreviously, ~40% of patient have received 1
or more drugs from this listNew update is based upon methods for
determining best-practice guidelinesThis list should serve as a guideline and risk
vs. benefit should always be assessedThis list is not meant to supersede clinical
judgment

ConclusionsPrescribing and managing disease states
should be individualizedIf a medication on the list cannot be avoided
and the physician feels it is necessary, the patient should be closely monitored for ADEs
Regular updates of this list allow for the evidence for medications to be assessed regularly, making it more relevant and sensitive to patient outcomes

ReferenceAmerican Geriatrics Society Updated Beers
Criteria for Potentially Inappropriate Medication Use in Older Adults. Journal of American Geriatric Society, 2012.