mesa 1.5 jose luis lopez campos
TRANSCRIPT

Mesa 1. EPOC epidemiología y diagnóstico
Dr. José Luis
López-CamposHospital Virgen del Rocío. Sevilla

Mesa 1. EPOC epidemiología y diagnóstico
[ATS] Correlates Of 5 Year
Decline In 6-Minute Walk
Distance In The
COPDGene Cohort
Gordon JA
COPDGene Investigators

Mesa 1. EPOC epidemiología y diagnóstico
La P6MM es un test submaximal simple, objetivo y clínicamente útil que permite estimar
la capacidad funcional del paciente con EPOC, y aporta información de 3 variables
principales:
• Distancia recorrida (D6MM).
• Desaturación de O2.
• Disnea percibida por el propio paciente evaluada con la escala de Borg, como reflejo de
diferentes dimensiones de la enfermedad.
Titular tabla

Mesa 1. EPOC epidemiología y diagnóstico
El análisis multivariante demostró que
las siguientes variables tenían un valor predictivo
estadísticamente significativo de la D6MM: sexo,
edad, VEMS (% de su teórico), puntuación en la
escala de disnea de la MRC, comorbilidades (índice
de Charlson) y limitación al esfuerzo físico.
Mesa 1. EPOC epidemiología y diagnóstico
D6MM se asocia con la frecuencia de exacerbaciones, la
gravedad de la enfermedad (según criterios GOLD), la difusión
(TLCO), el atrapamiento aéreo y grado de enfisema
cuantificado por la TC torácica.
Estudio NETT y ECLIPSE

Mesa 1. EPOC epidemiología y diagnóstico
Correlates Of 5 Year Decline In 6-Minute Walk Distance
In The COPDGene Cohort
We utilized a large cohort studied over a 5-year interval to determine epidemiologic
and clinical variables that predict 6MWD decline.
Methods: We sought correlates of 6MWD decline in a large longitudinal cohort of
current or ex-smokers; subjects with and without spirometric evidence of COPD were
included. Data were gathered in the COPDGene study, at baseline and 5-year follow-
up, at 21 United States hospitals.
Predictors of 6MWD decline from among baseline assessments, and also among
changes seen over the 5-year follow-up period, were sought using univariable and
multivariable linear regression.
Mesa 1. EPOC epidemiología y diagnóstico
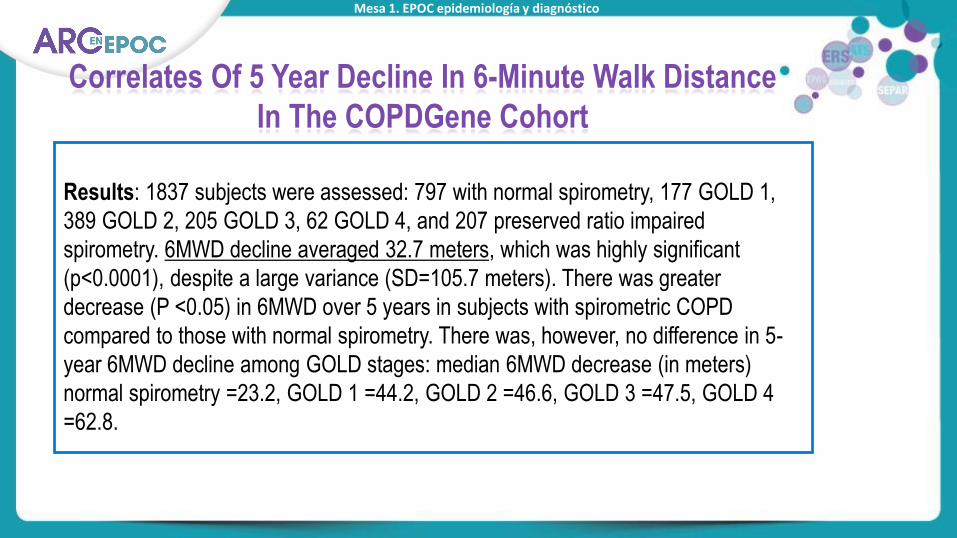
Correlates Of 5 Year Decline In 6-Minute Walk Distance
In The COPDGene Cohort
Results: 1837 subjects were assessed: 797 with normal spirometry, 177 GOLD 1,
389 GOLD 2, 205 GOLD 3, 62 GOLD 4, and 207 preserved ratio impaired
spirometry. 6MWD decline averaged 32.7 meters, which was highly significant
(p<0.0001), despite a large variance (SD=105.7 meters). There was greater
decrease (P <0.05) in 6MWD over 5 years in subjects with spirometric COPD
compared to those with normal spirometry. There was, however, no difference in 5-
year 6MWD decline among GOLD stages: median 6MWD decrease (in meters)
normal spirometry =23.2, GOLD 1 =44.2, GOLD 2 =46.6, GOLD 3 =47.5, GOLD 4
=62.8.

Mesa 1. EPOC epidemiología y diagnóstico
Correlates Of 5 Year Decline In 6-Minute Walk Distance
In The COPDGene Cohort
Results: In multivariable regression analysis of 5-year change predictors, only 5 %
of variance in 6MWD decline was predicted by change in (in order of significance)
total SGRQ, FEV1, BMI, and FEV1 /FVC. A regression analysis restricted to the 656
GOLD 2-4 subjects yielded qualitatively similar results.
Conclusion: These results demonstrate that 6MWD declines significantly over a 5-
year period in a large cohort of smokers and ex-smokers, but the decline is highly
variable. Spirometric, CT, health status and anthropometric measures account for
only modest portions of this variance.

Mesa 1. EPOC epidemiología y diagnóstico
[SEPAR] ¿Es el fenotipo
exacerbador de la EPOC
un fenotipo estable en el
tiempo?
Serrano L

Mesa 1. EPOC epidemiología y diagnóstico
Título de la diapositiva
Subtítulo de la diapositiva
•Cabecera párrafo
Titular tabla

Mesa 1. EPOC epidemiología y diagnóstico
Subtítulo de la diapositiva
Cabecera párrafo
Tercer apartado
• Tercer apartado
• Tercer apartado

Mesa 1. EPOC epidemiología y diagnóstico
• 78 pacientes inician el estudio.
• 13 fallecieron y 1 se abandonó en los 2 años seguimiento.
• A los 2 años, 18/64 (28 %) no ingresan y 46/64 (72 %) habían
precisado al menos una hospitalización.

Mesa 1. EPOC epidemiología y diagnóstico

Mesa 1. EPOC epidemiología y diagnóstico
Lange P, et al 2012. Am J Respir Crit Care Med. 2012;186(10):975-81.
Mesa 1. EPOC epidemiología y diagnóstico
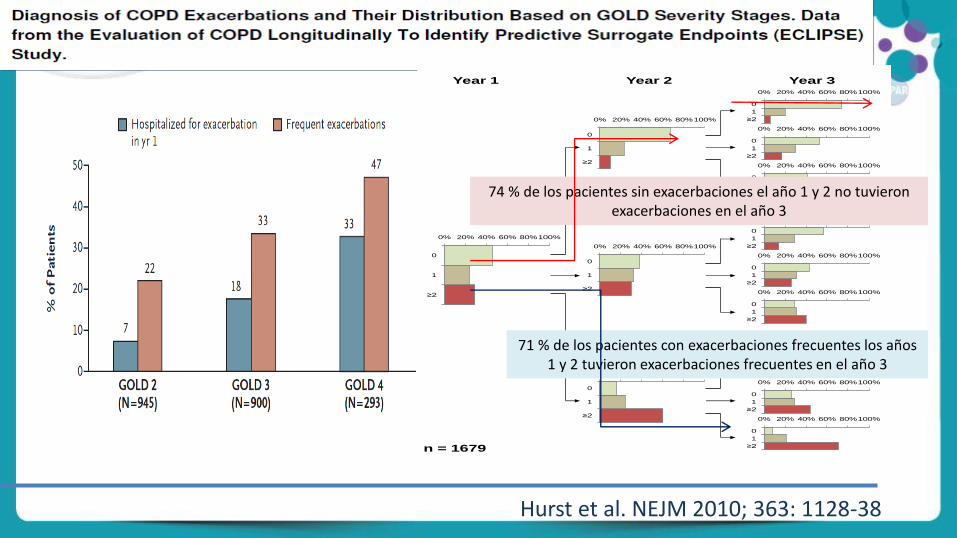
Hurst et al. NEJM 2010; 363: 1128-38
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
0% 20% 40% 60% 80%100%
≥2
1
0
Year 3Year 2Year 1
n = 1679
74 % de los pacientes sin exacerbaciones el año 1 y 2 no tuvieronexacerbaciones en el año 3
71 % de los pacientes con exacerbaciones frecuentes los años1 y 2 tuvieron exacerbaciones frecuentes en el año 3
Mesa 1. EPOC epidemiología y diagnóstico
[ERS] Co-morbidities of
adult smokers at risk of
COPD evaluated in a 6-
year prospective study
Toljamo T

Mesa 1. EPOC epidemiología y diagnóstico
Disfunción
mucociliar
(bronquitis
crónica)
Inflamación de la vía
aéreaOCFA
Inflamación
sistémica
Cambios
estructurales
(enfisema)
Agusti AGN. Respir Med 99 (6):670-682, 2005
•Pérdida de peso (caquexia)
• Disfunción muscular
• Enfermedad cardiovascular
• Otros
• Osteoporosis
• Depresión
• Cáncer
Efectos sistémicos de la EPOC
Las consecuencias de la inflamación
Mesa 1. EPOC epidemiología y diagnóstico
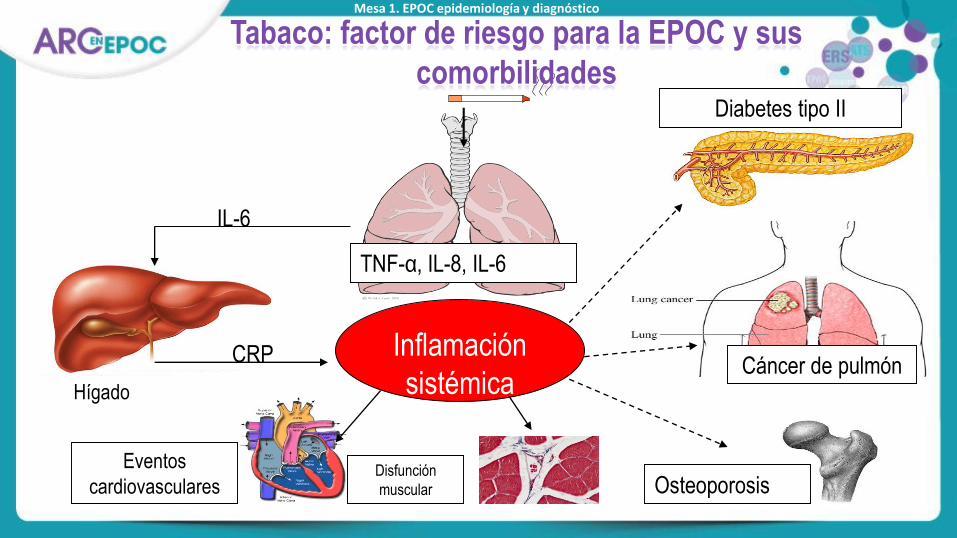
Hígado
Eventos
cardiovasculares OsteoporosisDisfunción
muscular
Inflamación
sistémica
Diabetes tipo II
IL-6
CRP
TNF-α, IL-8, IL-6
Cáncer de pulmón
Tabaco: factor de riesgo para la EPOC y sus
comorbilidades

Mesa 1. EPOC epidemiología y diagnóstico
La inflamación pulmonar y sistémica no se
correlacionan
0
1
2
3
4
50
100
150
200
250
Med
ian
valu
es
*
*
0
1
2
7
8
9
10
11
NDND
*(n=4)
*
IL-8
(pg/ml)
sTNF-R75
(pg/ml)
sTNF-R55
(pg/ml)
Total TNF
(pg/ml)
Med
ian
valu
es
Sputum
IL-8
(pg/ml)
sTNF-R75
(ng/ml)
sTNF-R55
(ng/ml)
Total TNF
(pg/ml)
Plasma
COPD (n=18, FEV1 56%)
Healthy smokers (n=17)
Vernooy JH et al. AJRCCM 2002; 166: 1218
Los valores no son diferentes entre fumadores activos y EPOC exfumadores

Mesa 1. EPOC epidemiología y diagnóstico
Titular tabla
Describe the co-morbidities of adult smokers at risk of COPD during a 6-year
follow-up
Methods:
•Healthy asymptomatic subjects (n = 513) with >20 years of smoking history
and no chronic diseases were followed longitudinally for six years.
•Smoking, symptoms and COPD status were assessed during the follow-up
period. Daily medications for possible comorbidities were self-reported. Co-
morbidities that emerged during the follow-up causes of death were
ascertained from hospital discharge records.
Co-morbidities of adult smokers at risk of COPD
evaluated in a 6-year prospective study

Mesa 1. EPOC epidemiología y diagnóstico
Titular tabla
Results: •As many as 43.1 % suffered from at least one co-morbidity during daily medication
after the 6-year follow up.
•As many as 20 % of these smokers were taking daily medication for metabolic
syndrome diseases e.g. high blood pressure, adult-onset diabetes or
hypercholesterolemia, and 9.7 % were taking drugs for arteriosclerotic disease such
as coronary artery heart disease.
•At the end of the study, only 8.4 % of COPD subjects admitted to having used
some type of inhalers on a daily basis.
•Overall, 4 % (n= 27) of all smokers died during the 6 year follow-up, half of them
from cancers and the others mainly from arteriosclerosis disease.
Co-morbidities of adult smokers at risk of COPD
evaluated in a 6-year prospective study

Mesa 1. EPOC epidemiología y diagnóstico
Titular tabla
Co-morbidities of adult smokers at risk of COPD
evaluated in a 6-year prospective study
Discussion: After the 6-year period approximately nearly half of the middle-
aged heavy smokers who had considered themselves symptom-free and
healthy at the baseline had been diagnosed with some chronic disease; this
may increase the risk of all-cause mortality in the long run.
Conclusion: There are as many co-morbidities in adult daily smokers as
encountered in COPD patients.

Muchas gracias
por su atención