mespa ppt - wordpress.com€“ features of vibratory behavior wnl ... – connected speech (rainbow...
TRANSCRIPT
4/1/16
1
NormalAnatomy/PhysiologyofVoice,AssessmentParametersfora
VoiceEvalua=onPartII:Videostroboscopy
ErinGuidera,MS,CCC-SLPMoffiJCancerCenter
LearningObjec=vesAJendeeswillbeableto:• Haveabasicunderstandingoftheroleofvideostroboscopy
aspartofacomprehensivevoiceevalua=on• Haveabasicunderstandingofthebenefitsandlimita=onsof
videostroboscopy• Haveabasicunderstandingofindica=onsfor
videostroboscopy
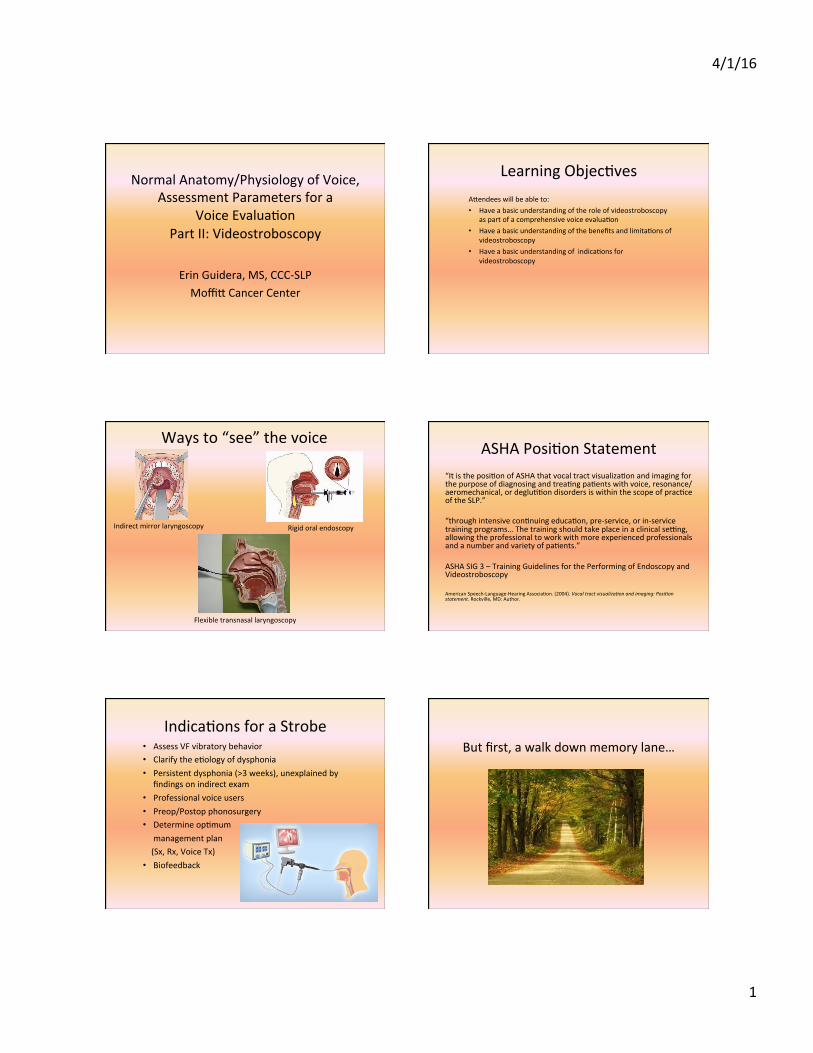
Waysto“see”thevoice
Indirectmirrorlaryngoscopy Rigidoralendoscopy
Flexibletransnasallaryngoscopy
ASHAPosi=onStatement“Itistheposi=onofASHAthatvocaltractvisualiza=onandimagingforthepurposeofdiagnosingandtrea=ngpa=entswithvoice,resonance/aeromechanical,ordeglu==ondisordersiswithinthescopeofprac=ceoftheSLP.”“throughintensivecon=nuingeduca=on,pre-service,orin-servicetrainingprograms…Thetrainingshouldtakeplaceinaclinicalse[ng,allowingtheprofessionaltoworkwithmoreexperiencedprofessionalsandanumberandvarietyofpa=ents.”ASHASIG3–TrainingGuidelinesforthePerformingofEndoscopyandVideostroboscopyAmericanSpeech-Language-HearingAssocia=on.(2004).Vocaltractvisualiza.onandimaging:Posi.onstatement.Rockville,MD:Author.
Indica=onsforaStrobe• AssessVFvibratorybehavior• Clarifythee=ologyofdysphonia• Persistentdysphonia(>3weeks),unexplainedby
findingsonindirectexam• Professionalvoiceusers• Preop/Postopphonosurgery• Determineop=mummanagementplan(Sx,Rx,VoiceTx)• Biofeedback
Butfirst,awalkdownmemorylane…

4/1/16
2
VFAnatomy/Physiology
• Cover– Epithelium– Superficiallaminapropria
• Transi=on(vocalligament)– Intermediatelaminapropria– Deeplaminapropria
• Body– Vocalismuscle
TheoriesofVibra=on• Body-CoverTheory
– Hirano,1975– Vibra=onproducedbydifferenceins=ffnessbetweenthebodyandthecover
• Myoelas=cAerodynamicTheory– Muller,1843– BernoulliEffect:VFsaresuckedtogetherbynega=ve
pressureandblowbackopenbyairpressurethroughglo[s
• Non-LinearDynamics– Interac=onbetweenvibra=onandresonance
ViewingVFVibra=on
• TheVFsvibratetoofastfortheeyetosee– Women:~200Hz(cycles/sec)– Men:~100Hz– Children:~300Hz– SingingfalseJo(highC):>1000Hz
ViewingVFVibra=on• Humaneyeisunabletodiscriminatebetweenseparate
imagesthatoccurfasterthan5=mespersecond(wecanperceive5dis=nctimagespersecond)
• Avisualimagelingersonthere=nafor0.2secondsakerexposure
• Talbot’sLaw-If>6images/secondarevisualized,thebrainwill“fuse”theimagestogetherandappeartobemovingàstroboscopicillumina=on
StroboscopicIllumina=on• Anillusionofmo=on• Providesarepresenta=onofvibra=on• VisualizeindividualpointsfromsuccessivegloJalcycles
• Usepersistenceofvisiontofusetheimagesintoaslowmo=onpicture
WhatAreWeLookingAt-Supraglo[c
• Larynx/pharynxstructures– Vallecula,epiglo[s,AEfolds,falseVFs,arytenoids,pyriformsinuses,etc.
– Interarytenoidpachydermia,erythema,edema,etc.
• Laryngealsecre=ons– Pooling,loca=on,aspira=on– Copious,frothy,thick/s=cky,ropey,inspissated
• Supraglo[chyperfunc=on
4/1/16
3
WhatAreWeLookingAt–VocalFolds
• Mobility– WNL,limitedABD,limitedADD,fixa=on,unilateral/bilateral
• VFappearance– Edges(smooth,straight,bowed)– Color(white,erythema,vasculariza=on)
• Lesions– Loca=onoflesion– Translucent/opaque,hard/sok,sessile/pedunculated,smooth/rough,
round/pointed/ellip=cal,hemorrhagic,etc.…
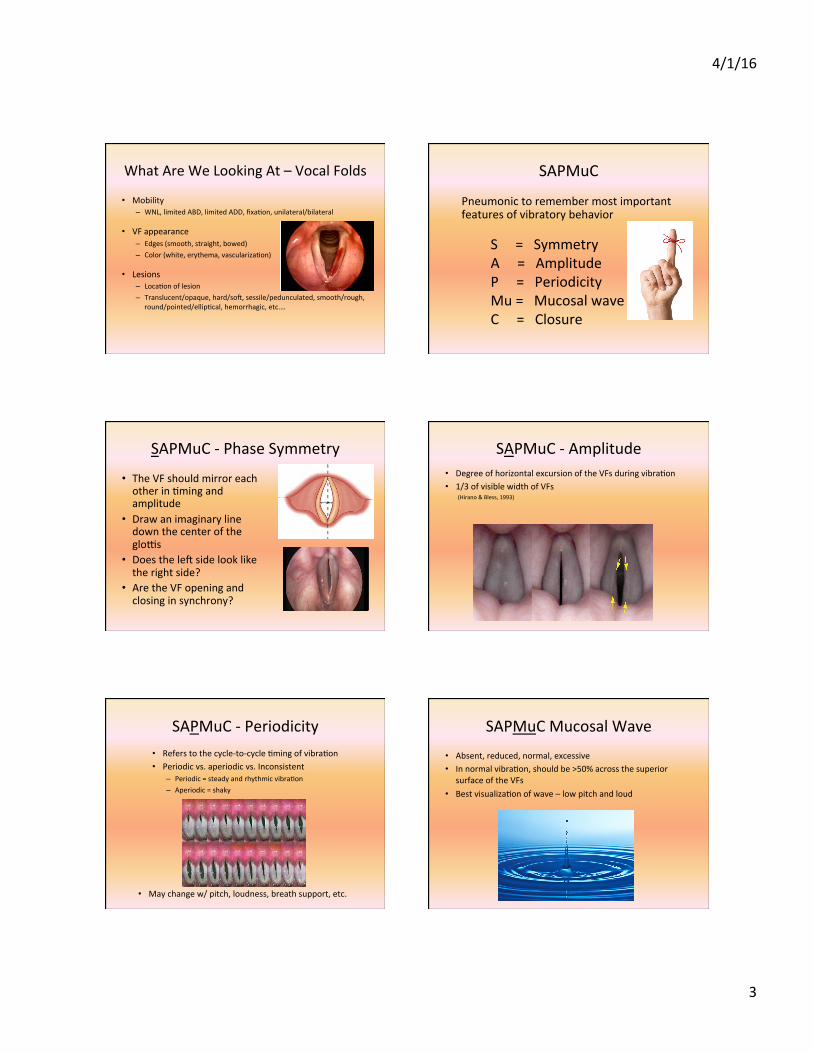
SAPMuC
Pneumonictoremembermostimportantfeaturesofvibratorybehavior
S=SymmetryA=AmplitudeP=PeriodicityMu=MucosalwaveC=Closure
SAPMuC-PhaseSymmetry
• TheVFshouldmirroreachotherin=mingandamplitude
• Drawanimaginarylinedownthecenteroftheglo[s
• Doestheleksidelookliketherightside?
• AretheVFopeningandclosinginsynchrony?
SAPMuC-Amplitude• DegreeofhorizontalexcursionoftheVFsduringvibra=on• 1/3ofvisiblewidthofVFs(Hirano&Bless,1993)
SAPMuC-Periodicity• Referstothecycle-to-cycle=mingofvibra=on• Periodicvs.aperiodicvs.Inconsistent
– Periodic=steadyandrhythmicvibra=on– Aperiodic=shaky
• Maychangew/pitch,loudness,breathsupport,etc.
SAPMuCMucosalWave• Absent,reduced,normal,excessive• Innormalvibra=on,shouldbe>50%acrossthesuperior
surfaceoftheVFs• Bestvisualiza=onofwave–lowpitchandloud

4/1/16
4
SAPMuC-Glo[cClosure
• Completevs.Incomplete
• Ifincomplete…– Hourglass,spindle,anteriorgap,posteriorchink,bowed,irregularclosurepaJern
• Bewareofpitch=maygetfalseclosurepaJern
Sonowwe’rereadytoscope.
Justafewsugges=ons….
Bridge3eErin
Pa=entPosi=on–RigidScope
• Slidehipstobackofchair• Leanforwardfromthewaist• Armsonkneesorarmrests• Chinup
HoldingTheTongue• Horizontally
– Thumbbeneathtongue– Indexfingerontopoftongue– Stabilizescopebetweenindexand
middlefinger
• Ver=cally– Thumbontopoftongue– Indexfingerbeneathtongue– Stabilizescopeontopofthumb
• Begentlewithtongue!
• Don’t“ride”tongue=gag
• Mayneedtowarmscopeuptopreventfogging
Horizontal
Ver=cal
Say/i/
• High,frontclosedvowel• Raiseslarynx• Tonguemovesforward• Velumraises• Haveptsmilearoundthescope
Don’tGetSlimed
Tipstominimizegagging:• Don’t“ride”tongue• Don’thitvelum• Anchorscope• Keeptongueoutwhenbreathing• /i/totongueBOT
4/1/16
5
SuggestedFlexProtocol• VPITasks
– “puhpuhpuh”– “ssssssssssss”– Dryswallow– Hum
• Respiratory/VFMobilityTasks– Sniff– Lightbreathhold– Tightbreathhold– Throatclear– Cough– Alterna=ngphona=on/inhala=on(/i/-sniff-/i/-sniff)
• VoicingTasks– Modal/i/– Lowpitch/i/– Highpitch/i/– Glidinglowtohighpitch/i/– Short/i/repe==ons– Loudphona=on– Connectedspeech(rainbowpassage)– S=mulability(e.g.,SDtasks,easyonset,humming,etc.)
SuggestedprotocolVideo
BenefitsofaStrobe
• Bridgefromtheearstotheeyes• Assesslaryngealanatomy• AssessVFvibra=onpaJerns• ProvidesimageofVFpathology• Permanentvideorecordoftheevalua=on• Pa=enteduca=on/biofeedback
Limita=onsofaStrobe
• Op=calillusion,notreal=me• Aperiodicvibra=oncanbedifficulttoassess• 2-Drepof3-Dprocess• Coloringandresolu=onvariesfromscopetoscope• Rigidscopeonlyforsustainedphona=on• Ar=factualmuscletension• AssessmentofSAPMuCissubjec=ve
Ques=ons?
References• AmericanSpeech-Language-HearingAssocia=on.(2004).Vocaltractvisualiza.onand
imaging:Posi.onstatement.Rockville,MD:Author.
• AmericanSpeech-Language-HearingAssocia=onSIG3,VoiceandVoiceDisorders.(1997).TrainingGuidelinesforthePerformingofEndoscopyandVideostroboscopy,Vol3,395-402.
• Gartner-Schmidt,J.(DateUnknown).StroboscopyPrinciple,ConceptsandEvalua.on.ContemporaryVoiceCare:APrac.calApproach.PPTPresenta=on.
• Hapner,E.&Johns,M.(2007).RecognizingandUnderstandingtheLimita.onsofLaryngealVideostroboscopy.SIG3Perspec=veonVoiceandVoiceDisorders.March2007.Vol17,3-7.
• Hirano,M.&Bless,D.(1993).VideostroboscopicExamina.onoftheLarynx.SingularPublishingGroup.
• Rosen,C&Simpson,B.(2008).Opera.veTechniquesinLaryngology.Videostroboscopy
andDynamicVoiceEvalua=onwithFlexibleLaryngoscopy,17-20.
• Stemple,J.,Glaze,L.&Klaben,B.(2000).InstrumentalMeasurementofVoice.ClinicalVoicePathology:TheoryandManagement,ThirdEdi=on,179-255.