michael scarpone, do / justin baker, dc perry pritchard ... · michael scarpone, do / justin baker,...
TRANSCRIPT

Use of Diagnostic Ultrasound in the Treatment and Rehabilitation of Upper Extremity : Multidisciplinary Case Review
Michael Scarpone, DO / Justin Baker, DC Perry Pritchard, PT, ATC
Progression of Diagnostic Ultrasound
Standard of Care-Direct
Visualization
•Tendionoplathy
•Intrinsic Changes
•Calcific Changes
Needle Placement
Dynamic Testing
•Impingement
•Bicep tendon subluxation
•Subluxation of glenoid labrum
Neovascularity Elastography
Is MSKUS Evidence Based?
Retrospective study of 1,012 patients treated by MSK and sports physicians over a 10-month period by Sivan et al. concluded that the use of clinic-based MSK US enables a one-stop approach, reduces repeated hospital appointments and improves quality of care.
Musculoskeletal Care. 2011;9(2):63-8

Improved Outcomes
RCT by Sibbitt et al. in 148 painful joints were randomized.
US guided had 43% reduction (p<0.001) in procedural pain.
58% reduction (p<0.001) in absolute pain scores at the 2 wks outcome.
75% reduction (p<0.001) in significant pain and 62% reduction in non-responder rate.
Increased detection of effusion by 200% and volume of aspirated fluid by 337%.
Journal of Rheumatology. 2009: 36(9):1892-902
MSKUS vs. MRI In a prospective study of 124 patients, US and
MRI had comparable accuracy for identifying and measuring the size of full-thickness and partial-thickness rotator cuff tears, with arthroscopic findings used as the standard.
J Bone Joint Surg Am. 2004; 86-A(4):708-16
Advantages of Ultrasound
No Radiation
Directed, real time
Patient Feedback is helpful
Dynamic
Multiplainer Capability
Dynamic Motion Assessment
Tendon Subluxation
Guided needle aspiration, injection
Contralateral Comparison
Not affected by implanted devices / metal
No Claustrophobia
Cost-effective
Color/Power Doppler sonography for vascularity
Non-radiopaque FB

Limitations of MSK US Limited Field of View
Detailed picture of relatively small area
Limited Penetration
Lower Resolution at greater depths
Unable to penetrate bone
Operator Dependent
Education (anatomy), scanning skills, and interpretation.
Requires Patient Cooperation
Body habitus dependent
> 5 cm deep hard to evaluate
When to Evaluate with Ultrasound ?
Shoulder Indications
Rotator Cuff Tears
Calcified tendinitis of the cuff
Subdeltoid-subacromial bursitis
Biceps tendinitis / tenosynovitis
Glenohumeral effusion
Impingement Syndrome
Acromiclavicular Joint
Suprascapular Ganglion Cyst

Ultrasound Accuracy for RTC Imaging
Difficult to differentiate
Partial-thickness articular vs tendinopathy
High-Grade partial vs full-thickness
With Modern Equipment
Full-Thickness
Sensitivity: 95 – 100 %
Specificity: 94 %
Partial-Thickness
Sensitivity: 93 %
Specificity: 87 %
Van Holsbeeck et al. Radiology 1995; 197: 443-446. Teefey et al. JBJS 2000; 82:498
Rotator Cuff :Partial Thickness Tear
Rotator Cuff Tear: Full Thickness

Elbow
Ulnar collateral Ligament evaluation
Unknown accuracy vs MRI
Triceps / Biceps tendons
Epicondylosis
Olecranon Bursa
Effusion
US-Guided aspiration / injection
Ulnar Collateral Ligament
Elbow – Flexor Bundle

Elbow – Extensor Tendon
Use of Diagnostic Ultrasound in Rehabilitation
Inexpensive Can be used more frequently to monitor progress and
thus give feedback for continued rehabilitation and management
1. Multidiscipline Case Review – Elbow – UCL 2. Multidiscipline Case Review – Shoulder - RTC
Multidisciplinary Case Study : Right Elbow Jan. 2015
o 21 year old Male o Right Handed College Pitcher o History of various elbow,
shoulder complaints over the last two years.
o Completed traditional physical therapy for 4-6 weeks once year prior
o Was doing well until the beginning of this baseball pre-season
o Significantly frustrated since he was in a starting role for his team

History
– Pre-Season Throwing
developed significant
elbow pain
Unable to throw or hold
on to the ball with
activities
Pain Level 6-8 out of 10
Complaints of tightness /
Swelling
Complaints of constant
achy pain even at rest.
Multidisciplinary Case Study : Right Elbow Jan. 21, 2015
Multidisciplinary Case Study : Right Elbow Jan. 21, 2015
Examination
Mild swelling medial
elbow
Normal pulses
(-) tinels
(+) tenderness medial
epicondyle and UCL
(+) ULC stress /
Bounce Test
(+) Wrist Resisted
Flexion
MRI Arthrogram Right Elbow
Mild Scarring of UCL w/o
Acute Tear
Thickening of UCL
Intermediate signal of UCL
attachment
Ulnar Nerve somewhat
prominent
Multidisciplinary Case Study : Right Elbow Jan. 28, 2015

Plan of Care : Multidisciplinary Approach
to give him the best possibility to pitch
this season:
1. Diagnostic Ultrasound with Placental
Cell Injection into damaged tissues
2. Pre-Work Up for Outcomes
A. Quick Dash Questionnaire
B. Pain Level
C. Patient Rated Elbow Evaluation
3. Grip Strength / Goniometry / Scapula
Levels
4. Functional Movement Screen
5. Kinesotape Post injection
6. K-Laser 2-3 times a week
Multidisciplinary Case Study : Right Elbow Jan. 28, 2015
Multidisciplinary Case Study : Right Elbow Jan. 29, 2015
Quick Dash Sports 81.25
% Disability
Quick Dash Shoulder 28
% Disability
Patient Rated Elbow
Evaluation 70 %
Disability
Physical Therapist / ATC
Grip Strength : WNL –Avg 117 lbs
Shoulder Rom
1.Shoulder Arc (IR/ER = 180 : WNL)
2. Sleeper Rom- 56 deg – restriction noted
Scapula Position= WNL=dif of 1.1 cm –right
lower than left
Elbow Rom –lacking 2 degrees of extension
Multidisciplinary Case Study : Right Elbow Jan. 29, 2015

Multidisciplinary Case Study : Right Elbow Jan. 29, 2015
Functional Movement Screen
o Identify individuals at risk, who are attempting to maintain / increase activity level
o Assist in program design by systematically using corrective exercises to improve fundamental movement patterns
o Systematic tool to monitor progress and movement pattern development in the presence of changing fitness goals
o Create a movement baseline – allowing – rating/ranking movement pattern
o Not used to diagnose, simply to identify or screen
Multidisciplinary Case Study : Right Elbow Jan. 29, 2015
Raw Score Final Score
Deep Squat 2 2
Hurdle Step 18 ½ L=2 R=3 2
InLine Lunge 2 2
Shoulder Mob 3 3
Active SLR 2 2
Trunk Stab push up
3 3
Rotatory Stab L=2 R=3 2
Total 16
Functional Movement Screen
Multidisciplinary Case Study : Right Elbow Jan. 29, 2015
FMS – Correction Hierarchy
# 1 =Address Mobility / Symmetry First before stability Mobility patterns will identify asymmetries thru shoulder
girdle, hip, core & spine, which can cause disruption thru the other patterns
Elbow Case- Addressed Active SLR correctives - Brettzel, Bridge single leg
#2 +Address Stability Second Stability is reflex driven and can’t be improved when mobility
is limited or impaired Elbow Case – Addressed Rotary Stability Correctives
Curl to press Half kneeling D1 flex/ext patterns
# 3 Address Functional Test Deficits – Lunge, Hurdle step, Deep
Squat
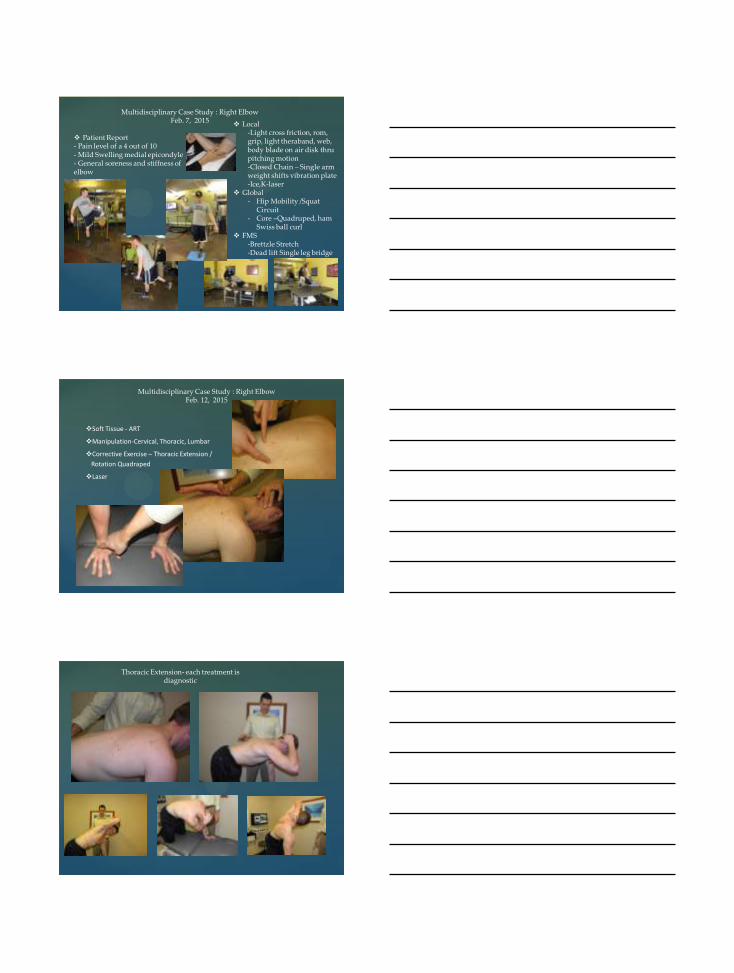
Multidisciplinary Case Study : Right Elbow Jan. 29, 2015
Diagnostic Ultrasound : Partial Cortical irregularity, mild tear of UCL at medial epicondyle
Pre-Injection
Pre-Injection
Pre-Injection

Pre-Injection
Injection of Placental Cells
Placental Injection
Multidisciplinary Case Study : Right Elbow Jan. 29, 2015
Post Treatment (next 5 days) - Ice - Active Rest - Avoid anti-inflammatores - K-Tape - K-Laser

Multidisciplinary Case Study : Right Elbow Feb. 3, 2015
Patient is determined to pitch a few innings Feb 7 on their opener in the south. So he performed Light throwing in the Bull Pen Feb 1, 2015 against better judgment.
Reported he had mild pain and did not have good strength but that it felt much better than prior to the injection. He did decreased his number of pitches for the bull pen session and utilized ice x 20 min post
Today’s Treatment ( Local Concerns – Inflammation Management )
- Ice - K laser - Kinesio-Taping - Range of motion Exercises
Multidisciplinary Case Study : Right Elbow Feb. 5, 2015
Treatment A. Local Concerns
- Inflammation Management - Modalities - light strengthening – isometrics, TB shoulder - dynamic stabilization – Grip in throwing pattern
and body blade in three positions B. Global Concerns
- ART -Soft Tissue Correction - Core Activation - OMT – Cervical, Thoracic, Lumbar
C. K-Laser D. Kinesiotape
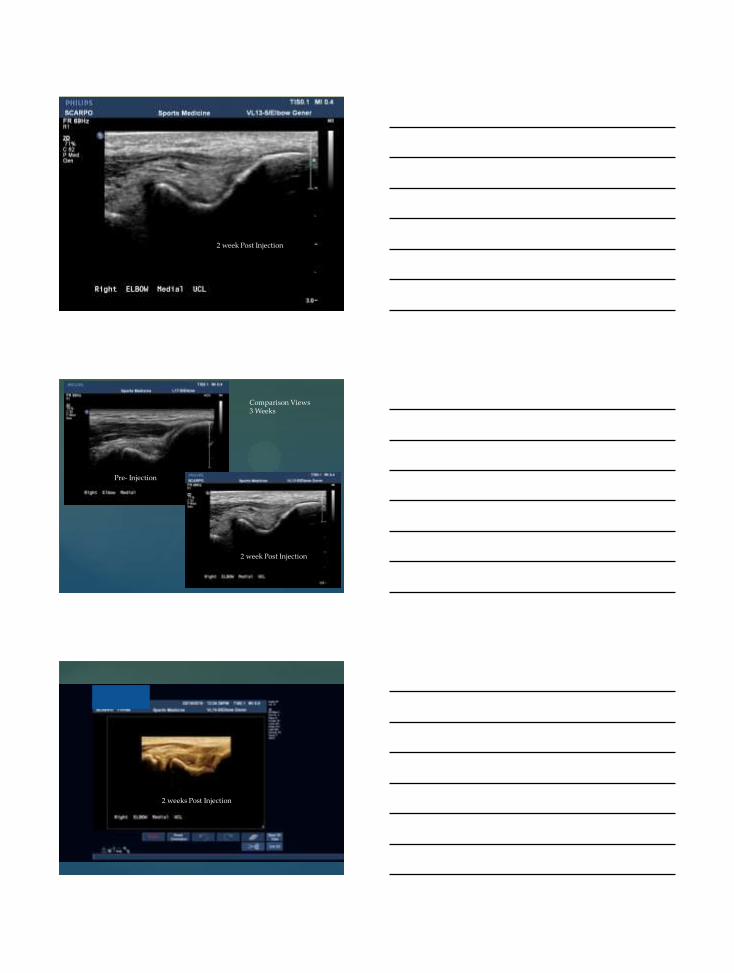
Multidisciplinary Case Study : Right Elbow Feb. 7, 2015
Warm-up at game Kinesiotape Pitched full game with K tape - 100 pitches—no sliders 0 @ 90 % - Gun speed 88 / 89 mph and finished 84 mph Won the game Reported he felt good during the
beginning and started to feel sore and loss strength toward the end. He admitted that it wasn’t a good idea to pitch
Use Ice post
Multidisciplinary Case Study : Right Elbow Feb. 7, 2015
Patient Report - Pain level of a 4 out of 10 - Mild Swelling medial epicondyle - General soreness and stiffness of elbow
Local -Light cross friction, rom, grip, light theraband, web, body blade on air disk thru pitching motion -Closed Chain – Single arm weight shifts vibration plate -Ice,K-laser
Global - Hip Mobility /Squat
Circuit - Core –Quadruped, ham
Swiss ball curl FMS
-Brettzle Stretch -Dead lift Single leg bridge
Multidisciplinary Case Study : Right Elbow Feb. 12, 2015
Soft Tissue - ART
Manipulation-Cervical, Thoracic, Lumbar
Corrective Exercise – Thoracic Extension /
Rotation Quadraped
Laser
Thoracic Extension- each treatment is diagnostic

DNS / Voijta
Multidisciplinary Case Study : Right Elbow Feb. 17, 2015
Local-cross friction, putty,
therabar, dumbbell, body
blade, vibration plate,
Laser
FMS- Curl to press double
arm
P3 – Hip / Squat circuit and
Core activation.
Multidisciplinary Case Study : Right Elbow Feb. 19, 2015
Ultrasound US
Quick Dash = 28.33 % to 18.8 % disability
Quick Dash Sports = 81.25 % to 75.1 % Disability
Patient Report Elbow Evaluation = 70 % to 47.1 % Disability
Continued Multidisciplinary Rehab
Multidisciplinary Case Study : Right Elbow Feb. 19, 2015
2 week Post Injection
Pre- Injection
Comparison Views 3 Weeks
2 week Post Injection
2 weeks Post Injection

Post Injection
2 weeks Post Injection
Pre- Injection
2 weeks Post Injection
Comparison Views 3 Weeks

Multidisciplinary Case Study : Right Elbow
Feb. 24, 2015
Progression cross
friction, general
strengthening,
dynamic stabilization
FMS –D1 patterns –
Tall kneeling , split
kneeling
Global-ART,
Manipulation,
Corrective exercise
Laser
Multidisciplinary Case Study : Right Elbow
March 3 , 2015
Quick Dash= 28.33 % to 18.88% to 11.37% Quick Dash Sports=81.25 % to 75.1% to 31.25 % Patient Reported Elbow Evaluation= 70 % to 47 % to 28 %
Local- Continued progression addressing elbow/shoulder K-Laser FMS –Curl to Press Single Arm from Single leg with one
DB Global-Corrective Exercise Core, hip, Thoracic Continue resistance in advanced positions

6 week Post Injection
Multidisciplinary Case Study : Right Elbow
March 10 , 2015
6 Week Ultrasound Evaluation-
6 week Post Injection
Pre- Injection
Multidisciplinary Case Study : Shoulder
75 yo man History of right rotator cuff
injury Previous PX 50 Placental
cell injection Followed by BMAC / AFG Previous specifics of case
presented in earlier matrices lecture
After the pain was becoming controlled this man was referred into the our multidisciplinary treatment protocol – local vs global
Injury
Local concern
Compensation
Global
concern
Dysfunction
Shoulder – 4 weeks post BMAC / AFG Physical Therapy : 4 weeks
Observations Forward head, Kyphotic posture Tight pectoralis / Lats Bilateral
Palpation Tenderness RC insertion and bicepital groove
ROM Flexion 135 Degrees ( painful arc 90-120) ABD 155 Degrees ER (POS) – 60 Degrees IR (POS)-64 Degrees
MMT – with pain complaints Flexion 4 /5 Abd 4 /5 ER 3+ / 5
Joint Mobility – Decreased inferior glide with pain
Spadi Score – 52 % disability
Shoulder – 4 weeks post BMAC / AFG Physical Therapy : 4 weeks
Treatment- address local concerns, scap stab, strength
Modalities of choice pre
ROM progression – AAROM, Pulleys, Flexband traction
GH Mobilization (inf / post)
Scap Lift – scap PNF
Strengthening Progression for RTC & Postural – isometric, Dumbbell, TB – PNF patterns
Proprioception progression – swiss ball on wall, rhythmic stab, body blade
K-Laser – used in conjunction with Physical therapy visits
YMCA – Last 5 visits – incorporating cybex circuit and Upper extremity cardio and general wellness program
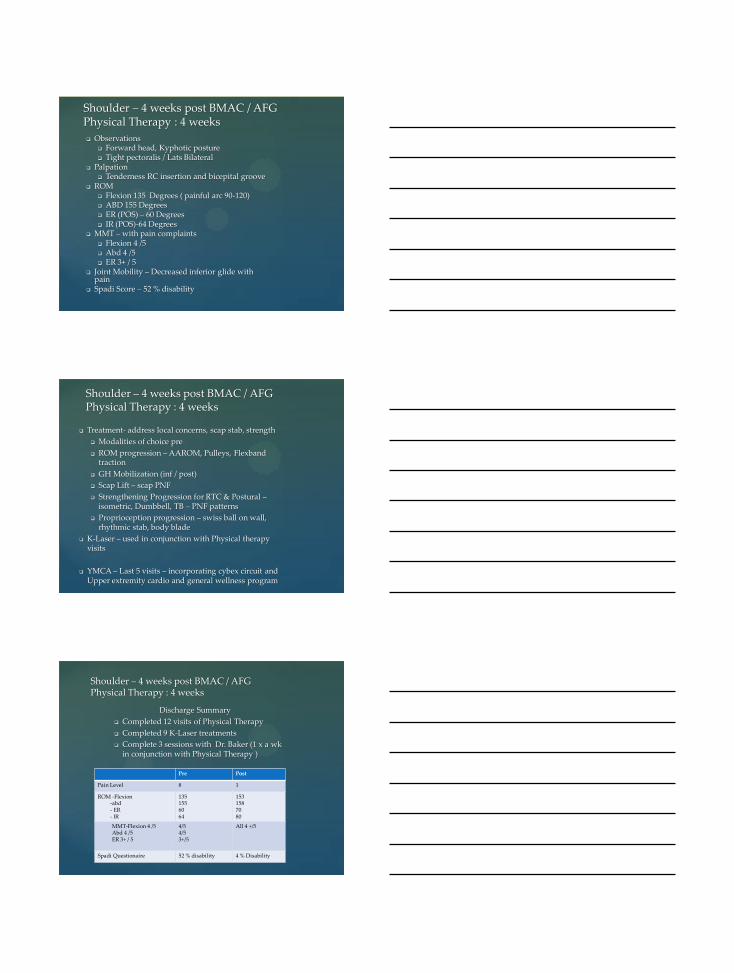
Shoulder – 4 weeks post BMAC / AFG Physical Therapy : 4 weeks
Discharge Summary
Completed 12 visits of Physical Therapy
Completed 9 K-Laser treatments
Complete 3 sessions with Dr. Baker (1 x a wk in conjunction with Physical Therapy )
Pre Post
Pain Level 8 1
ROM -Flexion -abd - ER - IR
135 155 60 64
153 158 70 80
MMT-Flexion 4 /5 Abd 4 /5 ER 3+ / 5
4/5 4/5 3+/5
All 4 +/5
Spadi Questionaire 52 % disability 4 % Disability

Shoulder – 4 weeks post BMAC / AFG Dr. Baker –Sports Chiropractic Physician
Referred for scapular stabilization, manual techniques, and DNS post rehabilitation cellular therapy
Restricted ROM- flexion, abduction, IR
Moderate tenderness / spasm
Cervical paraspinals
Upper trap
Levator scap – bilateral
Right pec mnor
Stingy pain at 90 degrees of abduction
Inability to bear sustained pressure right supraspinatus
Joint mobility
Considerable decrease C5 into right lateral flexion
Functional Tests
Poor right scap stability
Right scalene inhibition
Positive tests – supraspinatus press test
Treatment Plan – Once a week for 3-4 weeks Muscle Energy –C5 into right flexion
ART / Myofascial Release to involved structures
Corrective Exercise – side scapular stability, neck strengthening
Plan – Once a week for 3-4 weeks
Shoulder – 4 weeks post BMAC / AFG Dr. Baker –Sports Chiropractic Physician
Functional Assessment Shoulder
Impingement
Environment Development
Impingement comes from two places
Postural Otogenesis Anatomy Genetics
Upper Thoracic
Eccentric Loss
Scalene Inhibition
Neurological
Inhibition
Movement
Dysfunction
Mechanical
Problem
Articular
Dysfunction
Compression

Reports he is doing well
Pain Scale is 0-1
No limitations at this point
Vague pain with full abduction
Taking no pain medications
Shoulder Quick Dash – 2.3 % Disability
Completed his physical therapy, K-Laser, and referral session with Dr. Baker
Exam- full ROM, Strength WNL, (-) impingement tests
US Findings
Mild tendinosis with resolution of hypoechoic areas previously noted
Some hyoechoic areas where the graft was placed
Small calcification in the supraspinatus @ 1.5 cm from the insertion
Dynamic Impingement Test – (-)
Treatment Plan
FU Ultrasound in 3 months
Shoulder : Placenta & BMAC/ AFG 16 week FU post BMAC / AFG