mm-1 fda advisory committee april 26, 2001 ketek ™ (telithromycin)
TRANSCRIPT
MM-1
FDA Advisory CommitteeFDA Advisory CommitteeApril 26, 2001April 26, 2001
KETEKKETEK™™ (telithromycin) (telithromycin)
MM-2
Telithromycin – Presentation Agenda
Introduction Mindell Seidlin, MDVP, Clinical Development, Anti-Infectives, Aventis
Microbiology André Bryskier, MD
Human Pharmacology Vijay Bhargava, PhD
Clinical Efficacy and Safety Bruno Leroy, MD
ECG Analysis Claude Benedict, MD
Conclusions Mindell Seidlin, MD
MM-3
Need for New Antibiotics in Respiratory Tract Infections
• Driven by the emergence of multi-resistant strains
• Availability of a new class reduces resistance pressure on any existing classes
• Maintain coverage of all key RTI pathogens
• Simple, short course of therapy
• Recent Policy statements recommend NEW drug development:– WHO– HHS
MM-4
Pathogens of Community RTIs in 2001
• Most significant– S. pneumoniae
• multidrug resistance
• Other ‘bacterial’– H. influenzae
• beta-lactamase +ve
– M. catarrhalis• beta-lactamase +ve
– S. pyogenes
• Atypical / Intracellular– C. pneumoniae– M. pneumoniae– L. pneumophila
Importance ofintracellular levels
Importance of plasmaand ECF levels
MM-5
Recognition of Clinical Relevance of Penicillin Resistance
• Impact of penicillin G nonsusceptibility was readily demonstrated in meningitis
• Recent outcome studies show impact for ‘high-level’ resistance in pneumonia– Turett et al., Feikin et al. showed associated mortality
– Metlay et al. showed association with increased suppurative complications
– PRSP relevant for pneumonia at MIC 2 µg/mL,Heffelfinger et al.
• >60% of PRSP are multidrug resistant
MM-6
Recognition of Clinical Relevance of Erythromycin-Resistant S. pneumoniae
• 6 cases reported through 1992 (Lonks and Medeiros, Infect Med 1994;11:415-424)
• Reports of failure are increasing Fogarty et al (3 azithromycin failures)Kelley et al (1 clarithromycin and 3 azithromycin failures)Waterer (azithromycin failure)
• All recently reported failures had S. pneumoniae with MIC 8 µg/mL to erythromycin A
MM-7
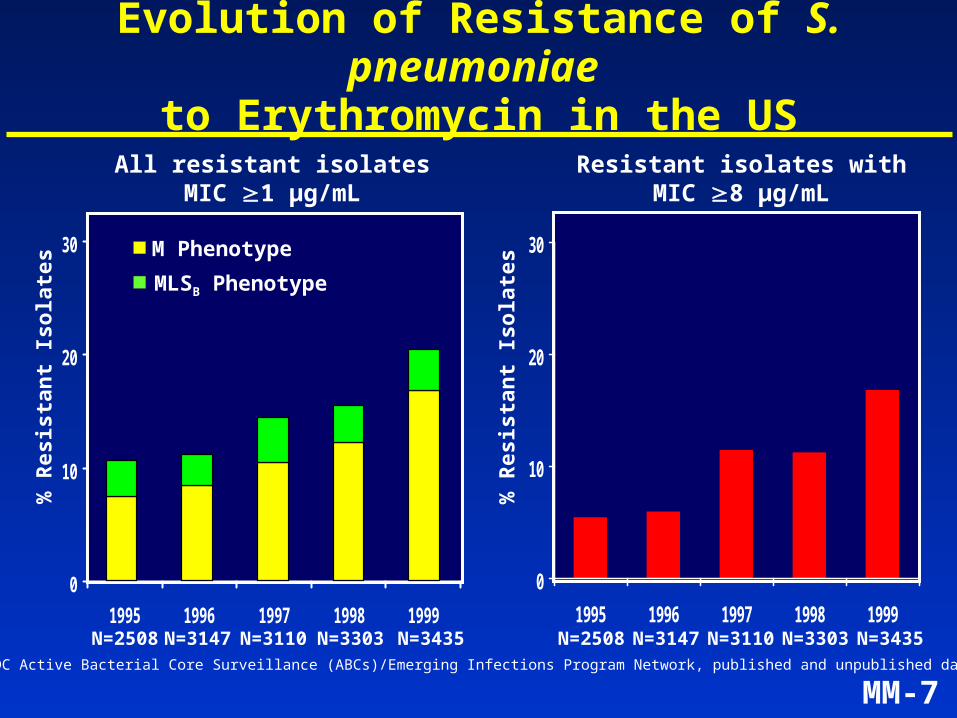
Evolution of Resistance of S. pneumoniae to Erythromycin in the US
Source: CDC Active Bacterial Core Surveillance (ABCs)/Emerging Infections Program Network, published and unpublished data.
% R
esis
tan
t Is
ola
tes
0
10
20
30
1995 1996 1997 1998 1999
M Phenotype
MLSB Phenotype
All resistant isolatesMIC 1 µg/mL
N=2508 N=3147 N=3110 N=3303 N=3435
0
10
20
30
1995 1996 1997 1998 1999N=2508
% R
esis
tan
t Is
ola
tes
N=3147 N=3435
Resistant isolates withMIC 8 µg/mL
N=3110 N=3303
MM-8
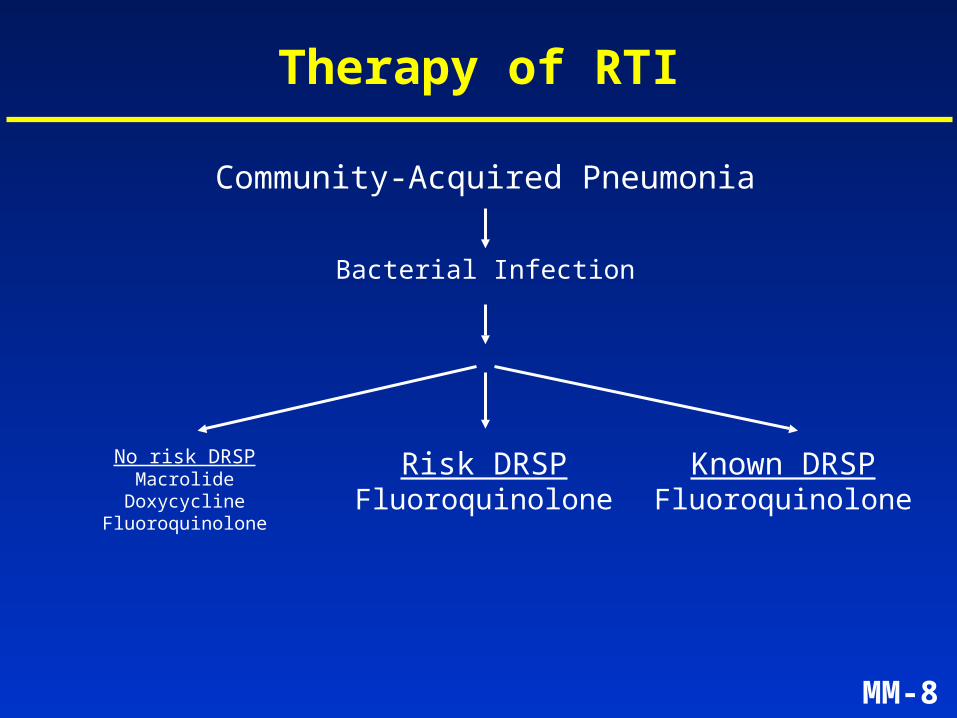
Therapy of RTI
Community-Acquired Pneumonia
Bacterial Infection
Risk DRSPFluoroquinolone
Known DRSPFluoroquinolone
No risk DRSPMacrolide
DoxycyclineFluoroquinolone
MM-9
Telithromycin
• Novel mechanism of action
• Excellent antipneumococcal activity
• Activity against Ery-R and Pen-R S. pneumoniae
• Activity against other common, intracellular, and atypical pathogens
• Short, simple course of treatment
MM-10
Telithromycin – Proposed Indications
• Community-acquired pneumonia (CAP)
• Acute exacerbation of chronic bronchitis (AECB)
• Acute sinusitis
• Tonsillitis/Pharyngitis due to Group A beta-hemolytic streptococci (GABHS)
MM-11
Telithromycin – Presentation Agenda
Introduction Mindell Seidlin, MD
Microbiology André Bryskier, MDSenior Director, Clinical Microbiology, Aventis
Human Pharmacology Vijay Bhargava, PhD
Clinical Efficacy and Safety Bruno Leroy, MD
ECG Analysis Claude Benedict, MD
Conclusions Mindell Seidlin, MD
MM-12
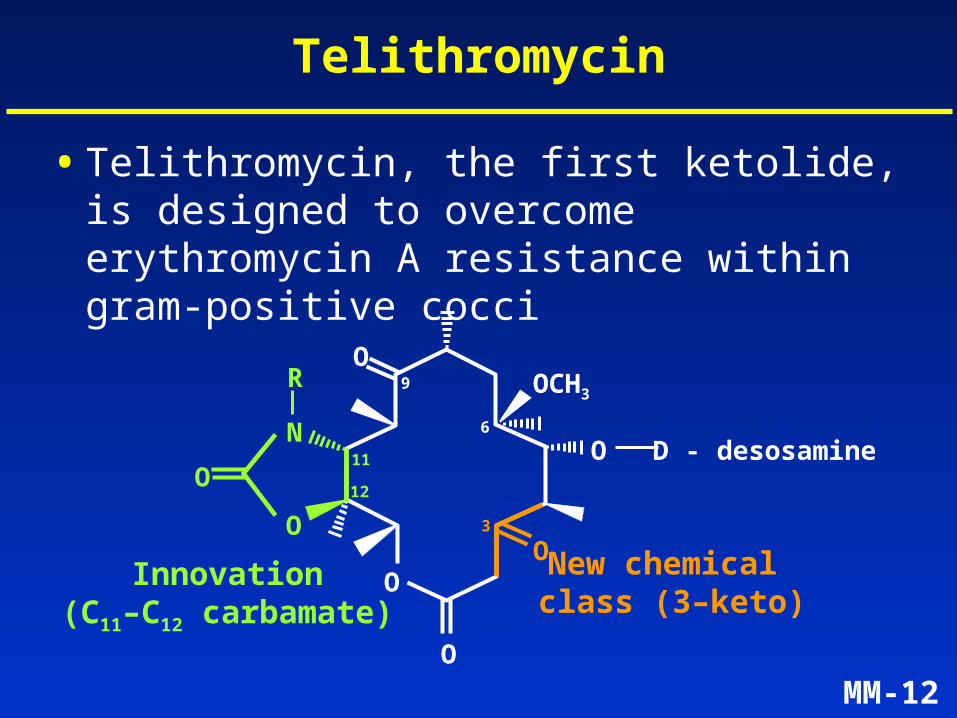
Telithromycin
• Telithromycin, the first ketolide, is designed to overcome erythromycin A resistance within gram-positive cocci
O
O
O
OOCH3
O
9
6N
R
3
OO D - desosamine
New chemical class (3–keto)
Innovation(C11–C12 carbamate)
11
12
MM-13
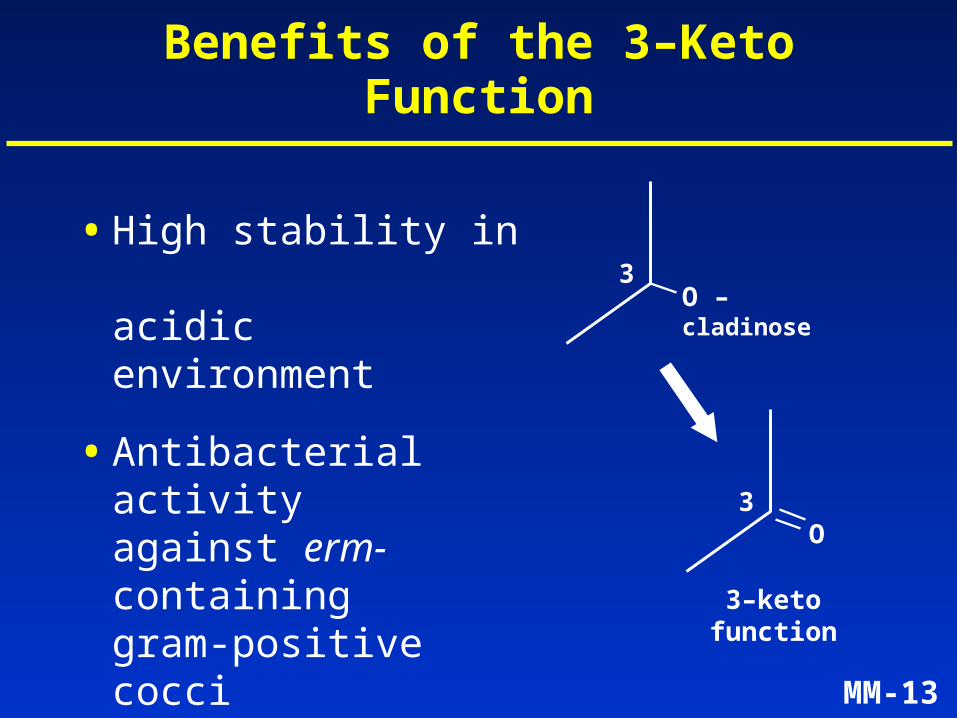
Benefits of the 3–Keto Function
• High stability in acidic environment
• Antibacterial activity against erm-containing gram-positive cocci
• Inability to induce MLSB resistance
3O – cladinose
3–keto function
3O
MM-14
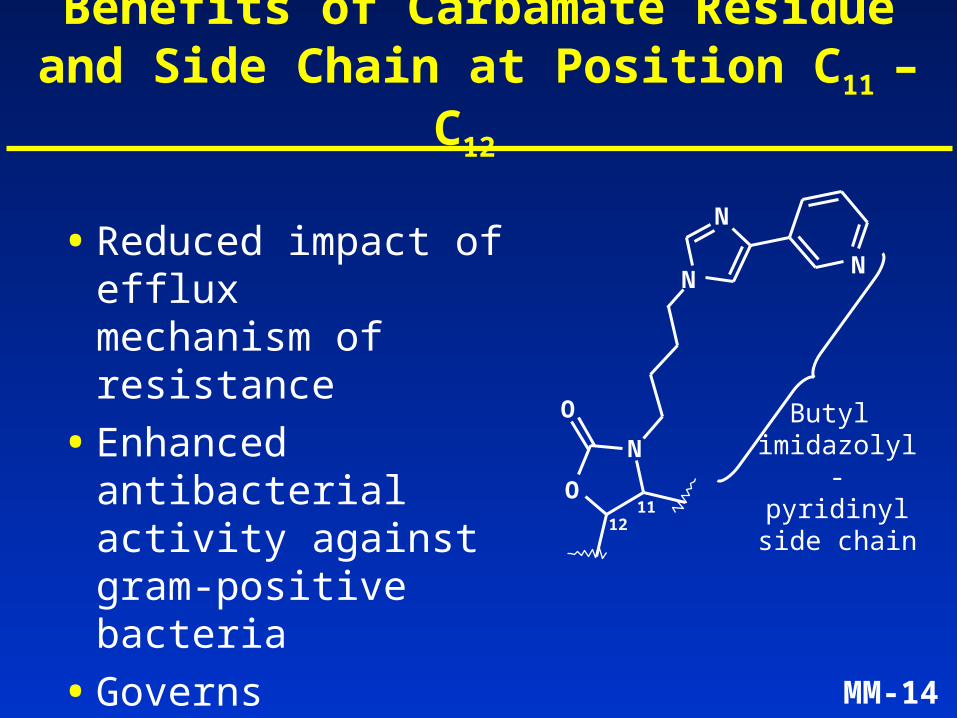
Benefits of Carbamate Residue and Side Chain at Position C11 – C12
• Reduced impact of efflux mechanism of resistance
• Enhanced antibacterial activity against gram-positive bacteria
• Governs intracellular accumulation and efflux in phagocytes
N
N
N
N
O
O
1211
Butyl imidazolyl-pyridinyl
side chain
MM-15
Telithromycin: Mode of Action
• Inhibition of protein synthesis
• Depletion of ribosomes in bacterial cell
MM-16
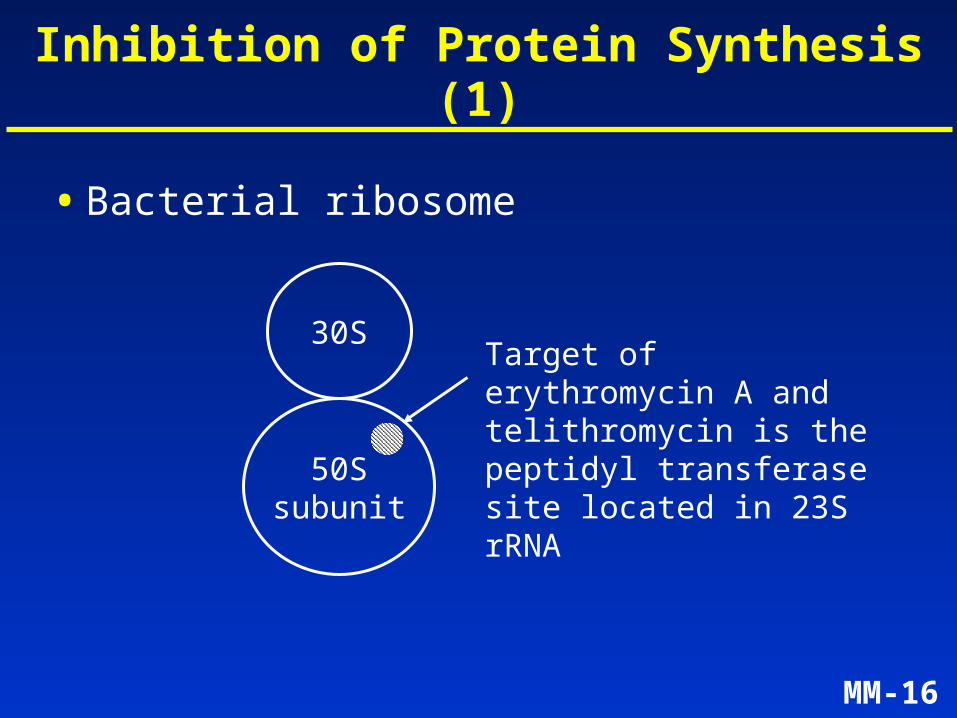
Inhibition of Protein Synthesis (1)
• Bacterial ribosome
30S
50Ssubunit
Target of erythromycin A and telithromycin is the peptidyl transferase site located in 23S rRNA
MM-17
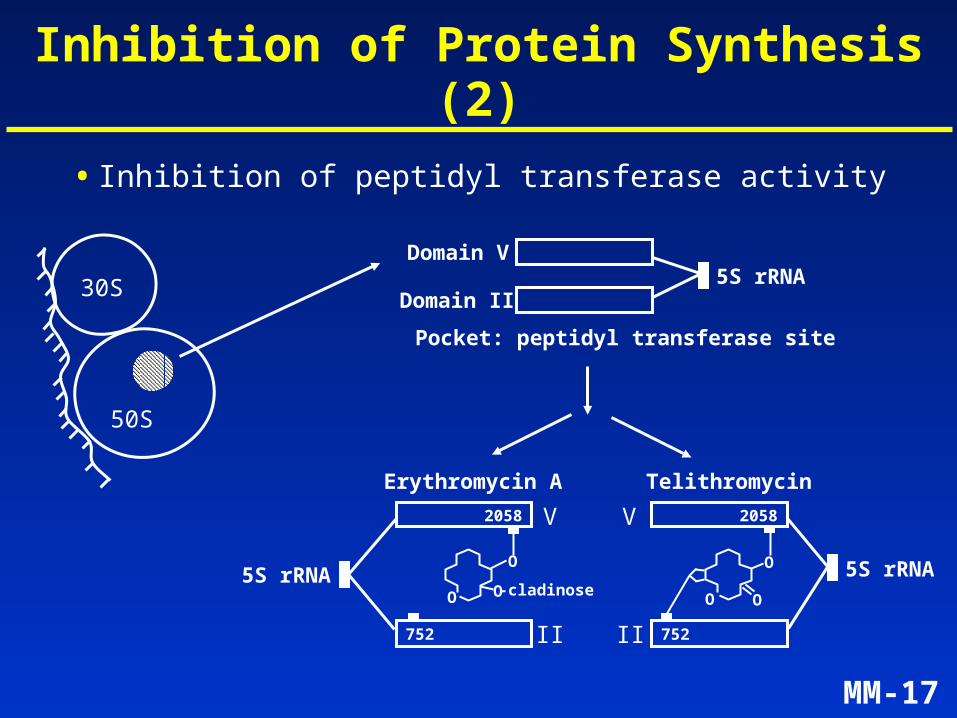
Inhibition of Protein Synthesis (2)
• Inhibition of peptidyl transferase activity
5S rRNADomain V
Domain II
Pocket: peptidyl transferase site
5S rRNA5S rRNA
2058
752
V
II
V
II
Erythromycin A Telithromycin
2058
752
30S
50S
O O
O
OO
O
-cladinose
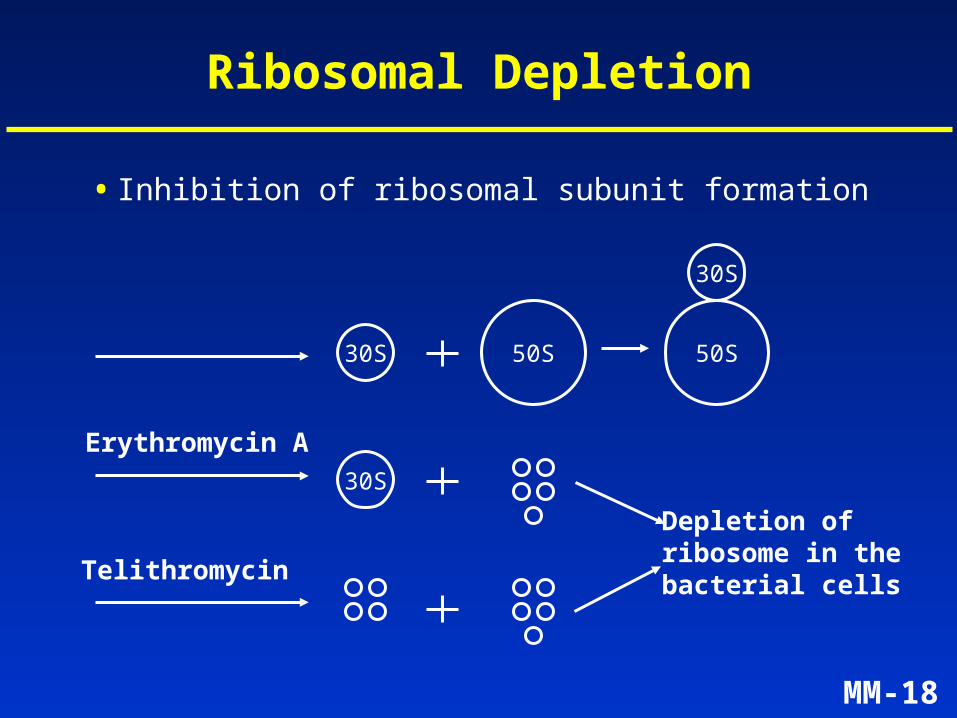
MM-18
Ribosomal Depletion
30S 50S
30S
50S
30S
Depletion ofribosome in thebacterial cells
Erythromycin A
Telithromycin
• Inhibition of ribosomal subunit formation
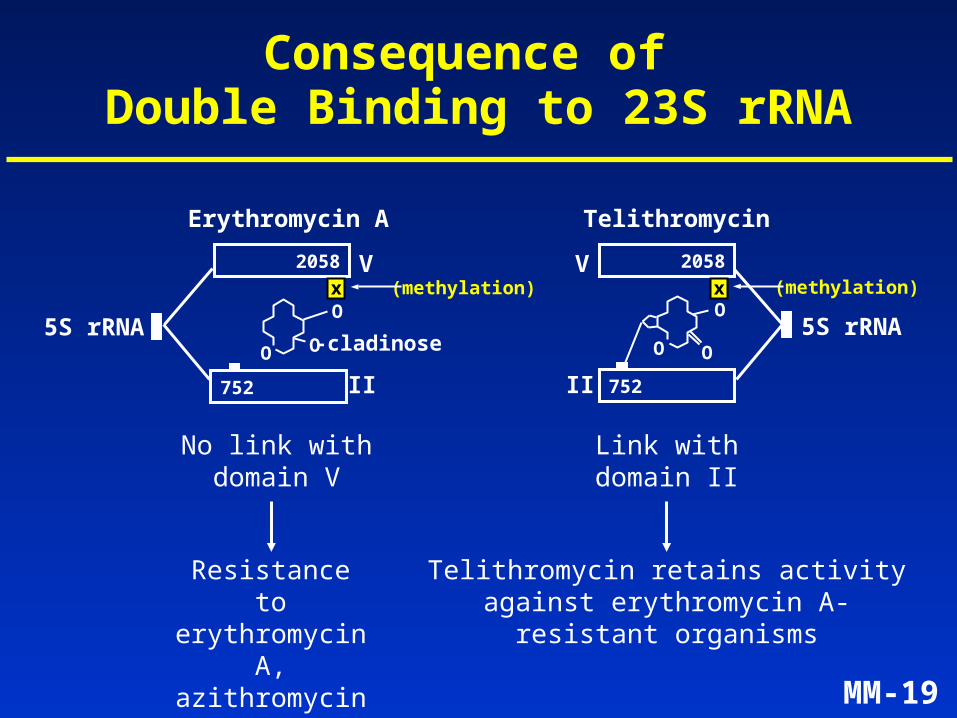
MM-19
Consequence of Double Binding to 23S rRNA
2058
752
V
II
V
II
Erythromycin A Telithromycin
2058
752
No link withdomain V
Resistance to erythromycin A,azithromycin, clarithromycin
Link withdomain II
Telithromycin retains activityagainst erythromycin A-
resistant organisms
5S rRNA5S rRNA-cladinoseOO
O
O O
O(methylation) (methylation)x x
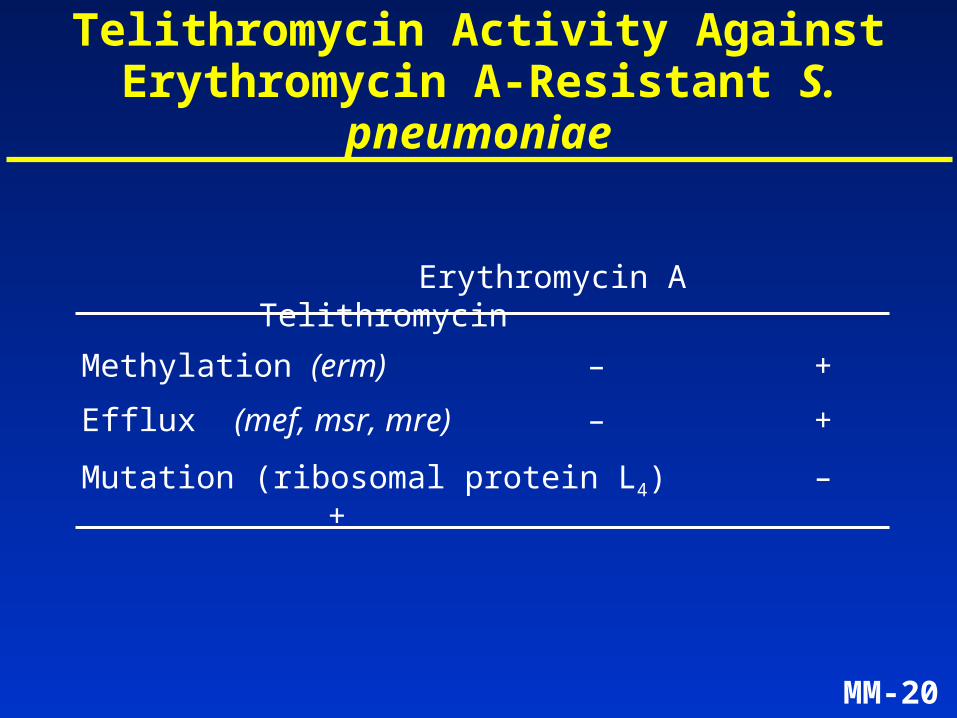
MM-20
Telithromycin Activity Against Erythromycin A-Resistant S. pneumoniae
Erythromycin A Telithromycin
Methylation (erm) – +
Efflux (mef, msr, mre) – +
Mutation (ribosomal protein L4) – +
MM-21
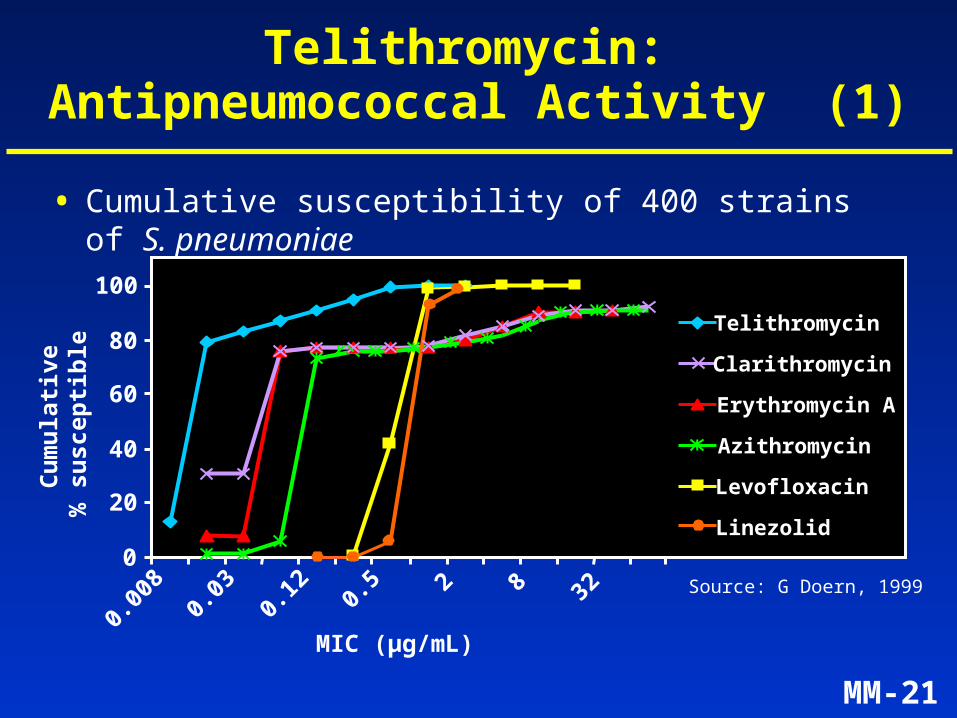
Telithromycin: Antipneumococcal Activity (1)
• Cumulative susceptibility of 400 strains of S. pneumoniae
0
20
40
60
80
100
0.00
80.
030.
12 0.5 2 8 32
MIC (µg/mL)
Cu
mu
lati
ve%
su
scep
tib
le Telithromycin
Levofloxacin
Erythromycin A
Clarithromycin
Azithromycin
Linezolid
Source: G Doern, 1999
MM-22
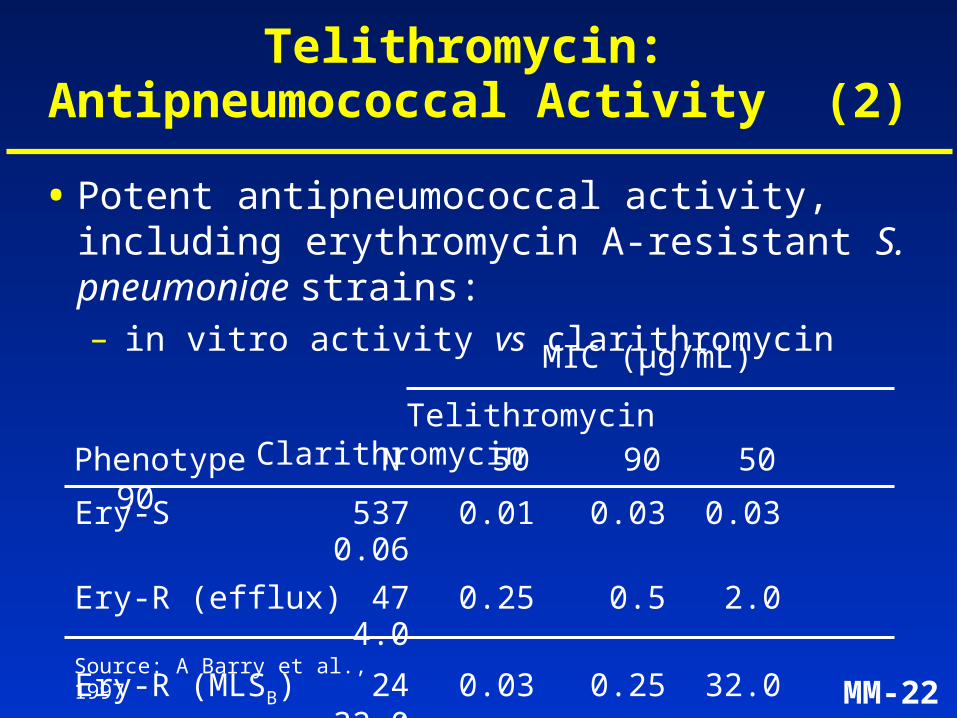
Telithromycin ClarithromycinPhenotype N 50 90 50
90Ery-S 537 0.01 0.03 0.030.06
Ery-R (efflux) 47 0.25 0.5 2.04.0
Ery-R (MLSB) 24 0.03 0.25 32.032.0
Source: A Barry et al., 1997
MIC (µg/mL)
Telithromycin: Antipneumococcal Activity (2)
• Potent antipneumococcal activity, including erythromycin A-resistant S. pneumoniae strains:– in vitro activity vs clarithromycin
MM-23
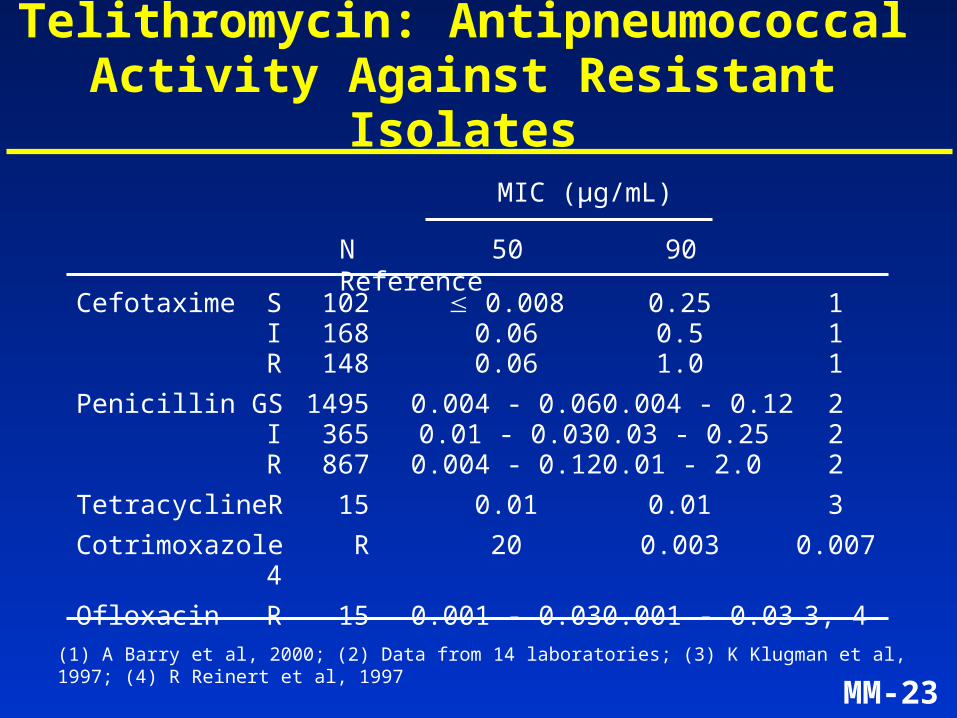
Telithromycin: Antipneumococcal Activity Against Resistant Isolates
N 50 90 Reference
Cefotaxime S 102 0.008 0.25 1I 168 0.06 0.5 1R 148 0.06 1.0 1
Penicillin G S 1495 0.004 - 0.06 0.004 - 0.12 2I 365 0.01 - 0.03 0.03 - 0.25 2R 867 0.004 - 0.12 0.01 - 2.0 2
Tetracycline R 15 0.01 0.01 3
Cotrimoxazole R 20 0.003 0.007 4
Ofloxacin R 15 0.001 - 0.03 0.001 - 0.03 3, 4
(1) A Barry et al, 2000; (2) Data from 14 laboratories; (3) K Klugman et al, 1997; (4) R Reinert et al, 1997
MIC (µg/mL)
MM-24
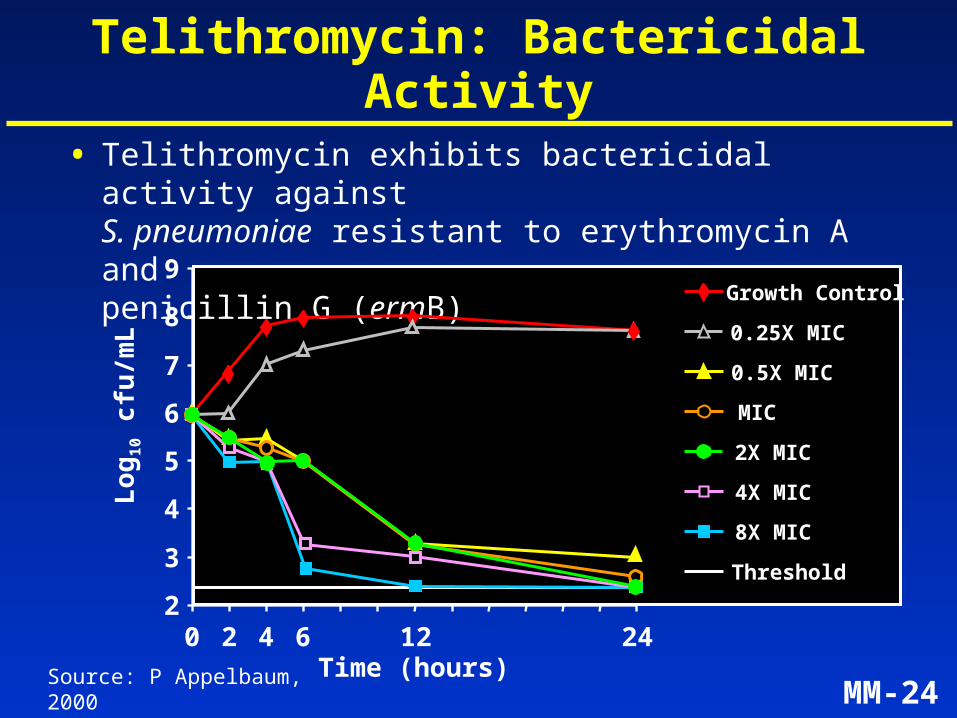
Telithromycin: Bactericidal Activity
• Telithromycin exhibits bactericidal activity against S. pneumoniae resistant to erythromycin A and penicillin G (ermB)
2
3
4
5
6
7
8
9
0 2 4 6 12 24Time (hours)
Lo
g1
0 cf
u/m
L
8X MIC
4X MIC
2X MIC
MIC
0.5X MIC
0.25X MIC
Growth Control
Threshold
Source: P Appelbaum, 2000
MM-25
Telithromycin: In VivoAntipneumococcal Activity
• Efficacy confirmed in animal models:– disseminated infections in mice– lung infections in mice
using:• erythromycin A–susceptible strains• erm– and mef–containing strains
MM-26
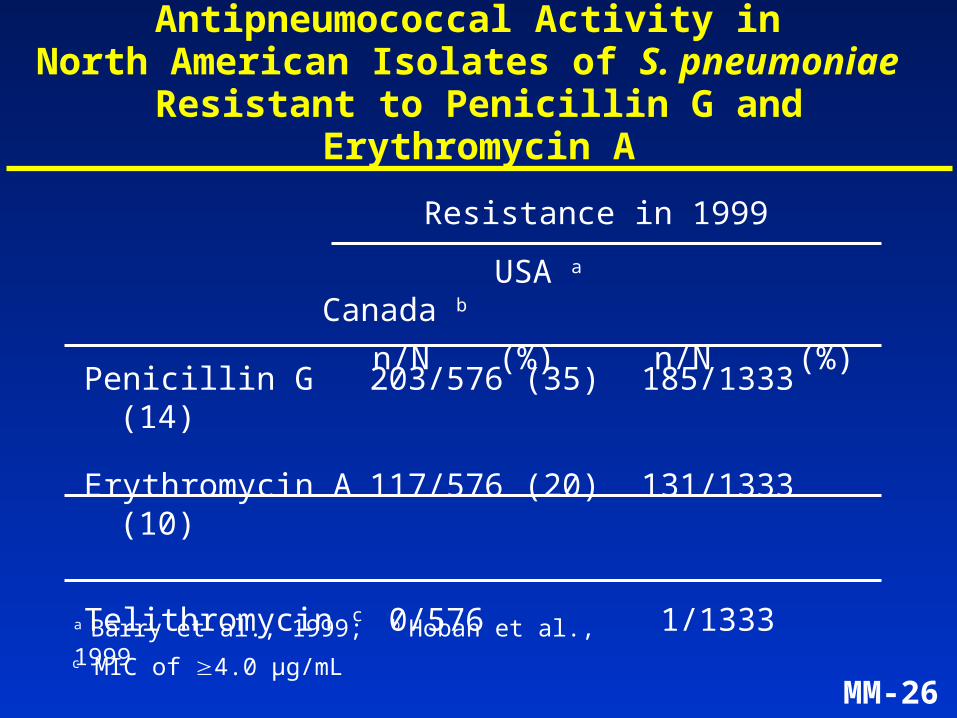
Antipneumococcal Activity in North American Isolates of S. pneumoniae
Resistant to Penicillin G and Erythromycin A
a Barry et al., 1999; b Hoban et al., 1999
USA a Canada b
n/N (%) n/N (%)
Penicillin G 203/576 (35) 185/1333(14)
Erythromycin A 117/576 (20) 131/1333(10)
Telithromycin c 0/576 1/1333c MIC of 4.0 µg/mL
Resistance in 1999
MM-27
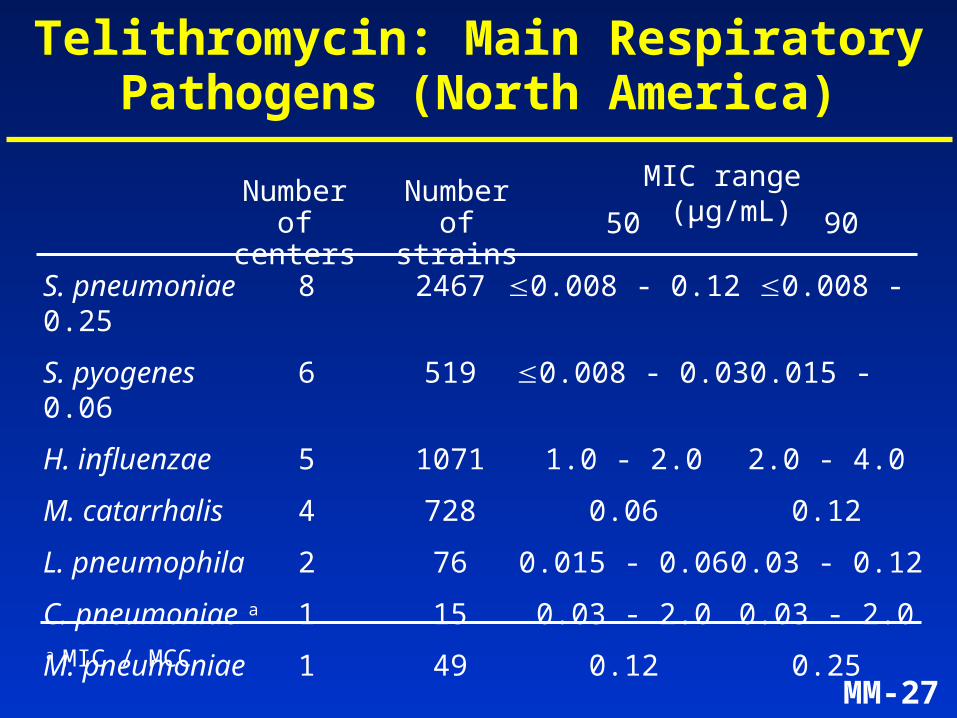
Telithromycin: Main Respiratory Pathogens (North America)
S. pneumoniae 8 2467 0.008 - 0.12 0.008 - 0.25
S. pyogenes 6 519 0.008 - 0.03 0.015 - 0.06
H. influenzae 5 1071 1.0 - 2.0 2.0 - 4.0
M. catarrhalis 4 728 0.06 0.12
L. pneumophila 2 76 0.015 - 0.06 0.03 - 0.12
C. pneumoniae a 1 15 0.03 - 2.0 0.03 - 2.0
M. pneumoniae 1 49 0.12 0.25
Number of centers
Number of strains 50 90
MIC range (µg/mL)
a MIC / MCC
MM-28
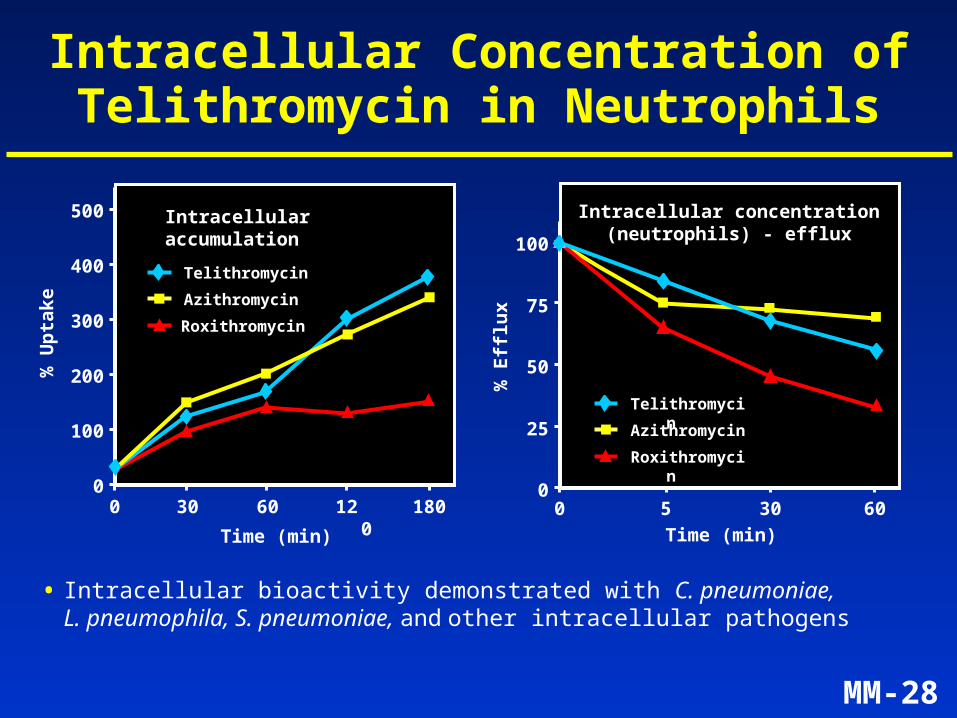
Intracellular Concentration of Telithromycin in Neutrophils
• Intracellular bioactivity demonstrated with C. pneumoniae, L. pneumophila, S. pneumoniae, and other intracellular pathogens
500
0
100
200
300
0 18030 60
Time (min)
% U
pta
ke
400
120
Intracellular accumulation
100
0
25
50
75
0 5 30 60
Time (min)
% E
fflu
x
Intracellular concentration(neutrophils) - efflux
Telithromycin
Azithromycin
Roxithromycin
Telithromycin
Azithromycin
Roxithromycin
MM-29
Microbiology of Telithromycin: Summary (1)
• Telithromycin, the first ketolide, has a novel antibacterial mechanism of action
• Telithromycin exhibits antibacterial activity against common, atypical, and intracellular pathogens involved in community-acquired respiratory tract infections
• Telithromycin overcomes erythromycin A resistance
MM-30
Microbiology of Telithromycin: Summary (2)
• Telithromycin has rapid bactericidal activity against S.pneumoniae
• Does not induce MLSB resistance
• Low frequency of selection of resistant mutants
• Active against S. pneumoniae strains resistantto erythromycin A, penicillin G, tetracycline, cotrimoxazole, fluoroquinolones and cefotaxime
MM-31
Telithromycin – Presentation Agenda
Introduction Mindell Seidlin, MD
Microbiology André Bryskier, MD
Human Pharmacology Vijay Bhargava, PhD Senior Director,
Drug Metabolism and Pharmacokinetics, Aventis
Clinical Efficacy and Safety Bruno Leroy, MD
ECG Analysis Claude Benedict, MD
Conclusions Mindell Seidlin, MD
MM-32
Clinical Pharmacology Program
• Clinical pharmacology, bioavailability, and drug metabolism of telithromycin:– plasma and tissue pharmacokinetic
characteristics– multiple pathways of disposition and exposure
in special populations– pharmacokinetic/pharmacodynamic
rationale for doses used in Phase III clinical efficacy program
MM-33
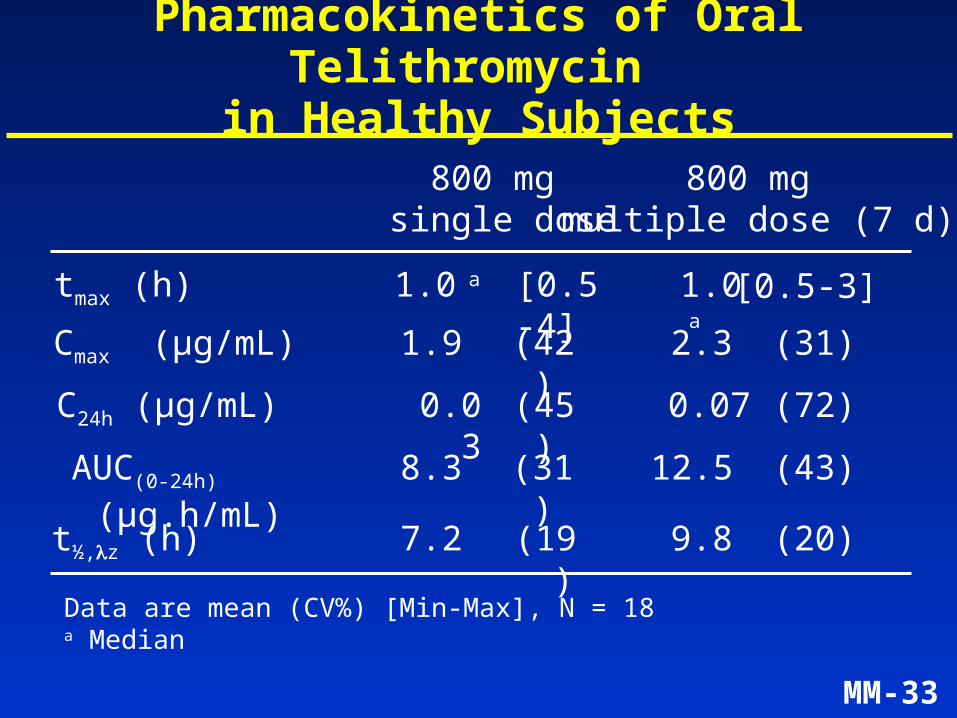
Pharmacokinetics of Oral Telithromycin in Healthy Subjects
800 mg single dose
800 mg multiple dose (7 d)
C24h (µg/mL) 0.03 (72)
AUC(0-24h) (µg.h/mL) 8.3 (43)
7.2 (20)t½,z (h)
Data are mean (CV%) [Min-Max], N = 18a Median
(19)
(31)
(45)
Cmax (µg/mL) 1.9 2.3(42) (31)
tmax (h) 1.0 a 1.0 a [0.5-4] [0.5-3]
0.07
12.5
9.8
MM-34
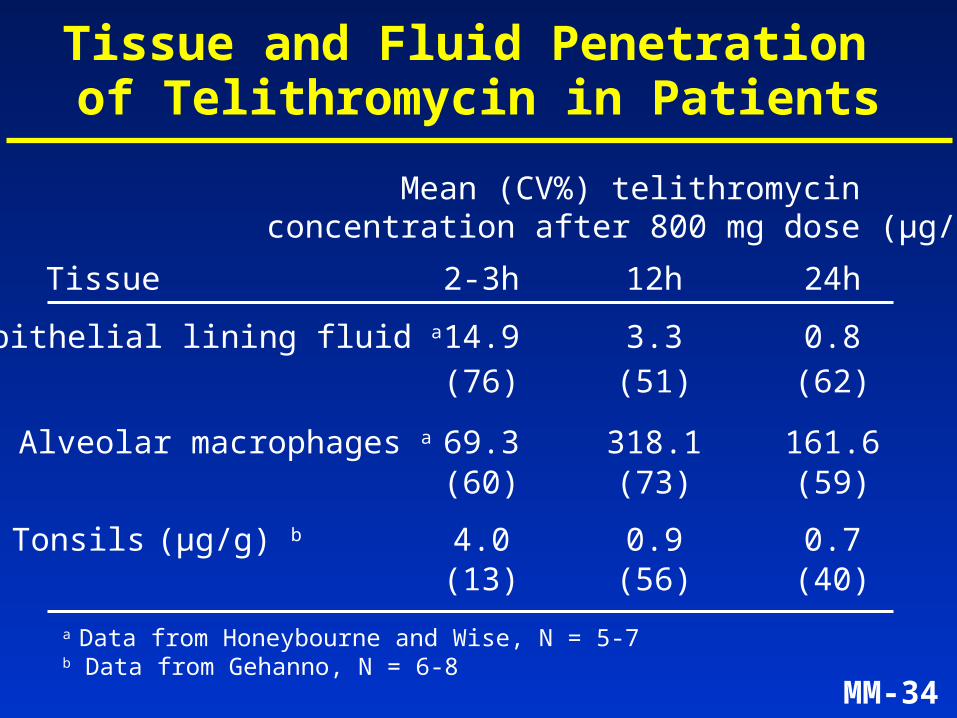
Tissue and Fluid Penetration of Telithromycin in Patients
Tissue
Mean (CV%) telithromycin concentration after 800 mg dose (µg/mL)
2-3h 24h
Alveolar macrophages a 69.3 161.6
Tonsils (µg/g) b 4.0 0.7
a Data from Honeybourne and Wise, N = 5-7b Data from Gehanno, N = 6-8
Epithelial lining fluid a
12h
0.9
14.9 0.83.3
318.1
(76) (62)(51)
(60) (59)(73)
(13) (40)(56)
MM-35
Other Key Pharmacokinetic Features
• Absolute bioavailability ~60%
• Serum protein binding ~70%
• Similar pharmacokinetics in men and women
• Similar pharmacokinetics with or without food
MM-36
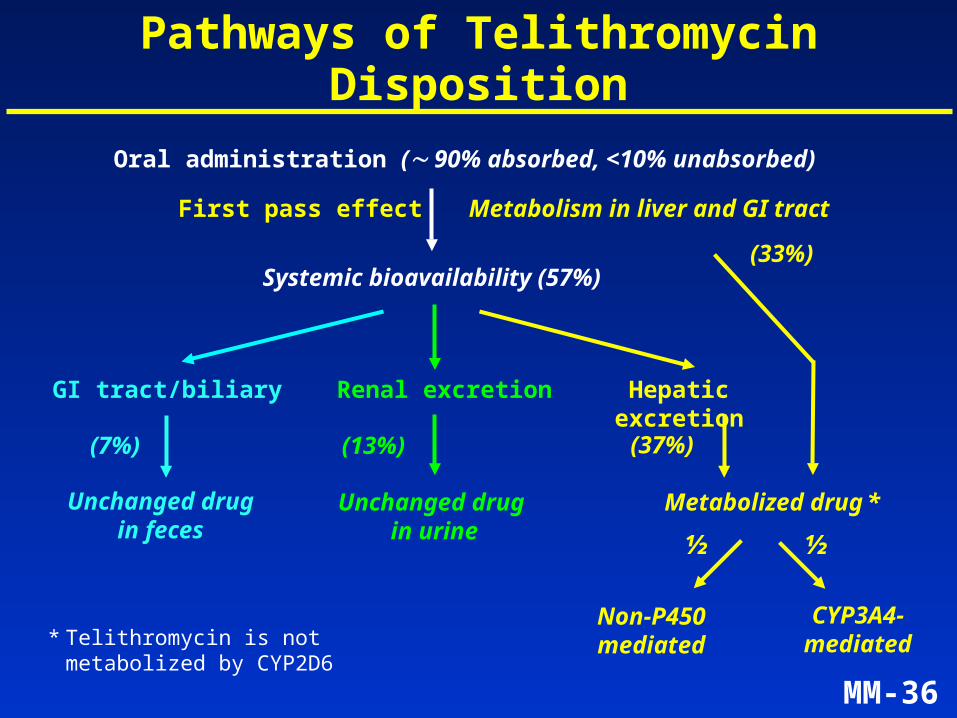
Oral administration ( 90% absorbed, <10% unabsorbed)
Systemic bioavailability (57%)
Renal excretion
Unchanged drug in urine
GI tract/biliary Hepatic excretion
Unchanged drugin feces
Metabolized drug *
Metabolism in liver and GI tract First pass effect
Pathways of Telithromycin Disposition
(13%) (37%)(7%)
(33%)
Non-P450 mediated
CYP3A4-mediated
½ ½
* Telithromycin is not metabolized by CYP2D6
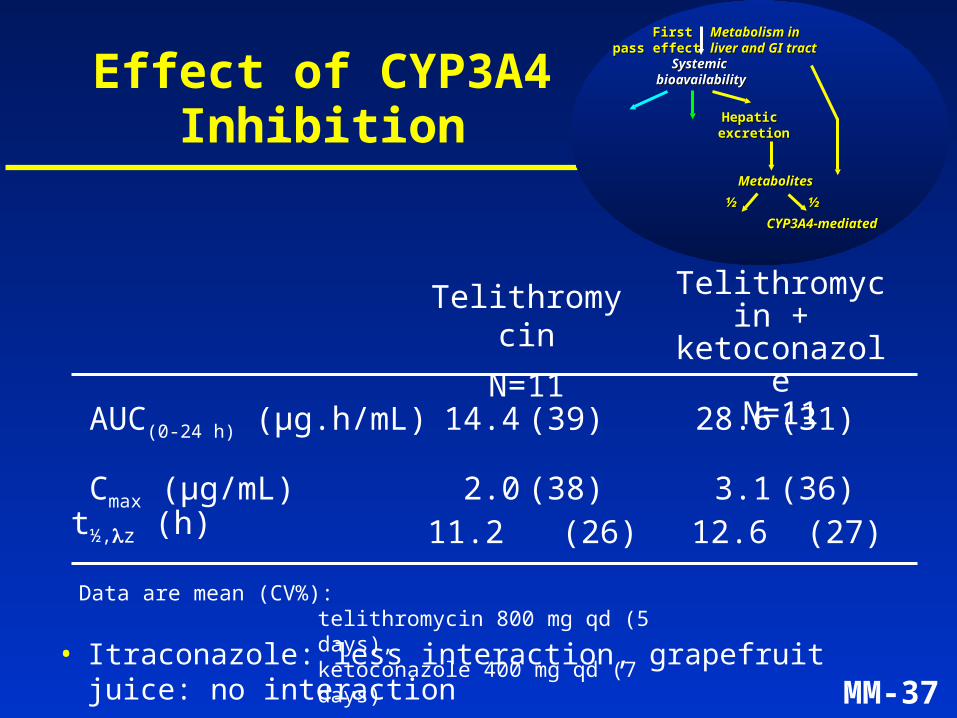
MM-37
First First pass effectpass effect
Telithromycin
N=11
Telithromycin +
ketoconazoleN=11
AUC(0-24 h) (µg.h/mL) 14.4 (39) 28.6 (31)
Cmax (µg/mL) 2.0 (38) 3.1 (36)
Data are mean (CV%): telithromycin 800 mg qd (5 days), ketoconazole 400 mg qd (7 days)
• Itraconazole: less interaction, grapefruit juice: no interaction
Effect of CYP3A4 Inhibition
Systemic Systemic bioavailabilitybioavailability
Hepatic Hepatic excretionexcretion
MetabolitesMetabolites
Metabolism in Metabolism in liver and GI tract liver and GI tract
CYP3A4-mediatedCYP3A4-mediated
½½½½
t½,z (h) 11.2 (26) 12.6 (27)
MM-38
Hepatic impairment
N=12HealthyN=12
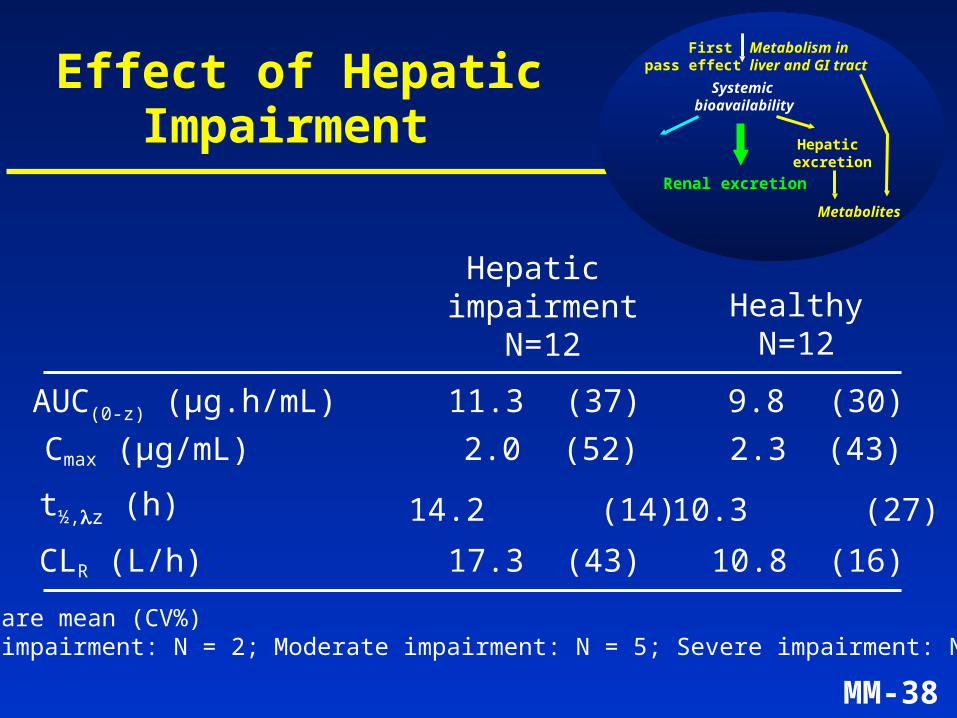
Data are mean (CV%)Mild impairment: N = 2; Moderate impairment: N = 5; Severe impairment: N = 5
Effect of Hepatic Impairment
Cmax (µg/mL) (52) (43)2.0 2.3
AUC(0-z) (µg.h/mL) (37) (30)11.3 9.8
CLR (L/h) (43) (16)17.3 10.8
Systemic bioavailability
Renal excretion
Hepatic excretion
Metabolites
Metabolism in liver and GI tract
First pass effect
t½,z (h) 14.2 (14) 10.3 (27)
MM-39
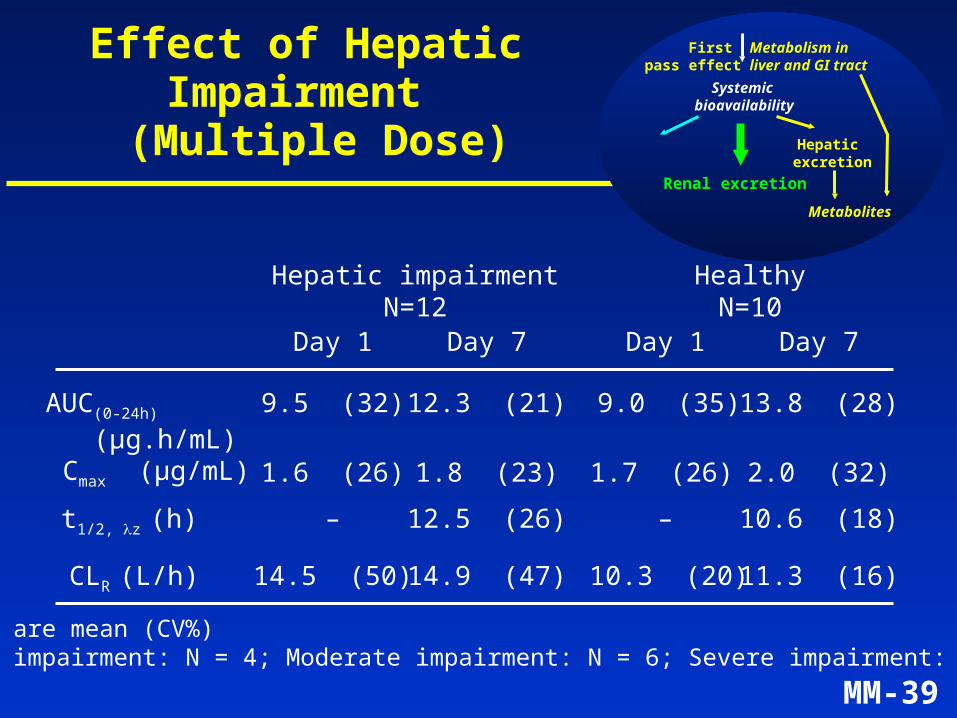
Hepatic impairmentN=12
HealthyN=10
Day 1 Day 7 Day 1 Day 7
t1/2, z (h) 12.5 (26) – 10.6 (18)
CLR (L/h)
Cmax (µg/mL) 1.6 (26) 1.8 (23) 1.7 (26) 2.0 (32)
AUC(0-24h)
(µg.h/mL)9.5 (32) 12.3 (21) 9.0 (35) 13.8 (28)
–
14.5 (50) 14.9 (47) 10.3 (20) 11.3 (16)
Data are mean (CV%)Mild impairment: N = 4; Moderate impairment: N = 6; Severe impairment: N = 2
Effect of Hepatic Impairment
(Multiple Dose)
Systemic bioavailability
Renal excretion
Hepatic excretion
Metabolites
Metabolism in liver and GI tract
First pass effect
MM-40
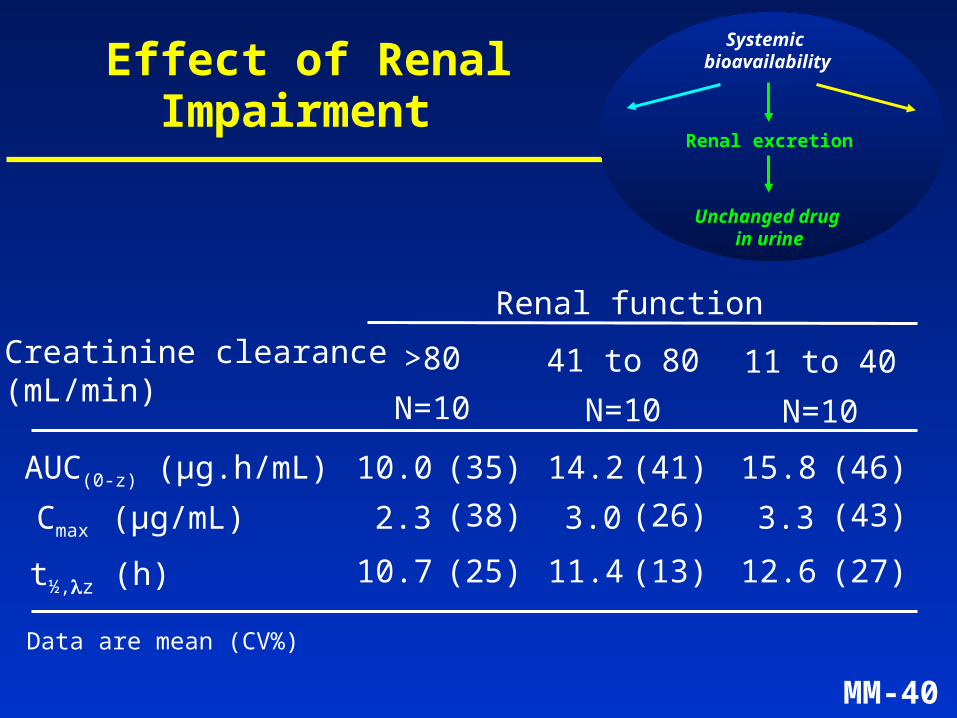
>80
N=10
41 to 80
N=10
11 to 40
N=10
Creatinine clearance(mL/min)
Data are mean (CV%)
Effect of Renal Impairment
Systemic bioavailability
Renal excretion
Unchanged drug in urine
Renal function
Cmax (µg/mL) 2.3 3.0 3.3(38) (26) (43)
AUC(0-z) (µg.h/mL) 10.0 14.2 15.8(35) (41) (46)
t½,z (h) 10.7 11.4 12.6(25) (13) (27)
MM-41
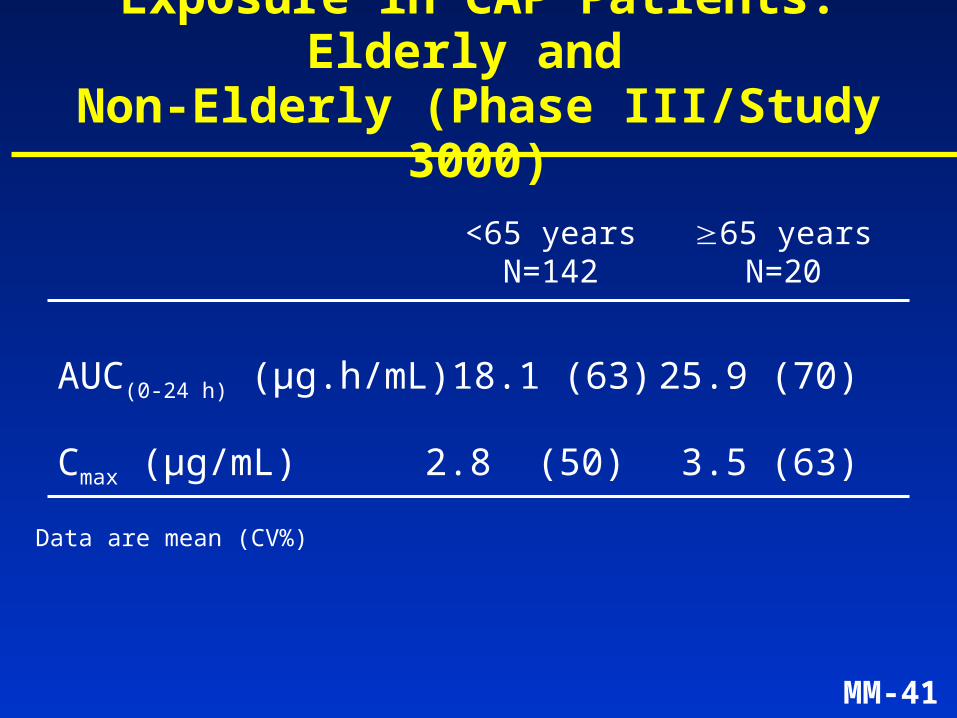
AUC(0-24 h) (µg.h/mL) 18.1 (63) 25.9 (70)
Cmax (µg/mL) 2.8 (50) 3.5 (63)
Data are mean (CV%)
<65 yearsN=142
65 yearsN=20
Exposure in CAP Patients: Elderly and Non-Elderly (Phase III/Study 3000)
MM-42
Selection of Telithromycin Dose Regimen
(Mouse Thigh Infection Model - Craig)
• Effective dose was similar, irrespective of dosing frequency (3, 6, 12, 24 hours)
• Efficacy of telithromycin is concentration-dependent rather than time-dependent:– AUC/MIC and Cmax/MIC are better predictors of
efficacy than time above MIC
MM-43
• Dose in humans was chosen to give unbound AUC/MIC values similar to, or higher than, AUC/MIC values at effective dose in mice
• 800 mg once-daily dose regimen is supported by high tissue levels in humans
Selection of Telithromycin Dose Regimen Based on PK/PD Model
MM-44
Dose Selection: H. influenzae
• No well-validated animal model of lower RTI
• ELF peak levels (up to 14.9 µg/mL) exceed MIC90 of H. influenzae
• Plasma and extracellular (ELF) levels for telithromycin (Cmax ELF/MIC = 3.6 to 7.2) are well above those reported for azithromycin
MM-45
Summary of Human Pharmacology
• Telithromycin rapidly achieved targeted plasma and respiratory tissue concentrations
• Telithromycin has a well-characterized and reproducible PK profile
• Multiple elimination pathways limit the potential for increased exposure in special populations
• The PK/PD profile of telithromycin supports an 800 mg once-daily regimen
MM-46
Telithromycin – Presentation Agenda
Introduction Mindell Seidlin, MD
Microbiology André Bryskier, MD
Human Pharmacology Vijay Bhargava, PhD
Clinical Efficacy and Safety Bruno Leroy, MDSenior Director, Clinical Development,Anti-Infectives, Aventis
ECG Analysis Claude Benedict, MD
Conclusions Mindell Seidlin, MD
MM-47
Clinical Efficacy of Telithromycin
• Study design across indications
• Clinical efficacy by indication:
– Community-acquired pneumonia (CAP)
– Acute exacerbation of chronic bronchitis (AECB)
– Acute sinusitis
– Tonsillitis/Pharyngitis
MM-48
Telithromycin Dosage Regimens in Phase III Studies
CAP 800 mg qd7-10 days
AECB 800 mg qd5 days
Acute sinusitis 800 mg qd5 days
800 mg qd10 days
Tonsillitis/Pharyngitis 800 mg qd
5 days
Indication Dosage Duration
MM-49
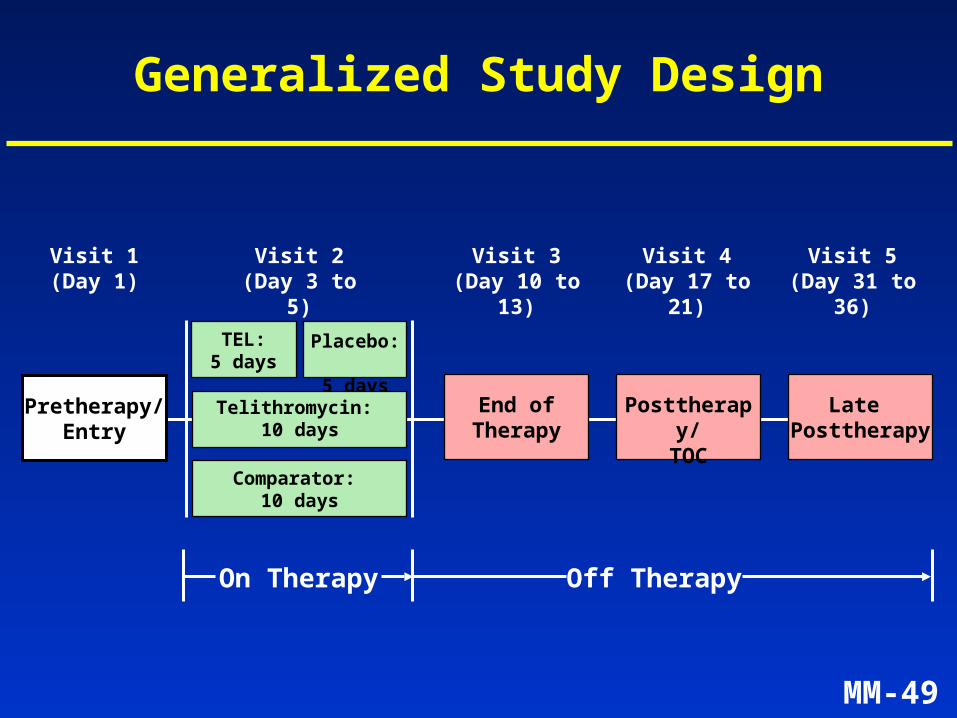
Generalized Study Design
Pretherapy/Entry
Comparator: 10 days
TEL:5 days
Placebo: 5 days
Posttherapy/TOC
Late Posttherapy
Telithromycin: 10 days
Visit 5(Day 31 to 36)
End ofTherapy
Visit 1(Day 1)
Visit 2(Day 3 to 5)
Visit 3(Day 10 to 13)
Visit 4(Day 17 to 21)
On Therapy Off Therapy
MM-50
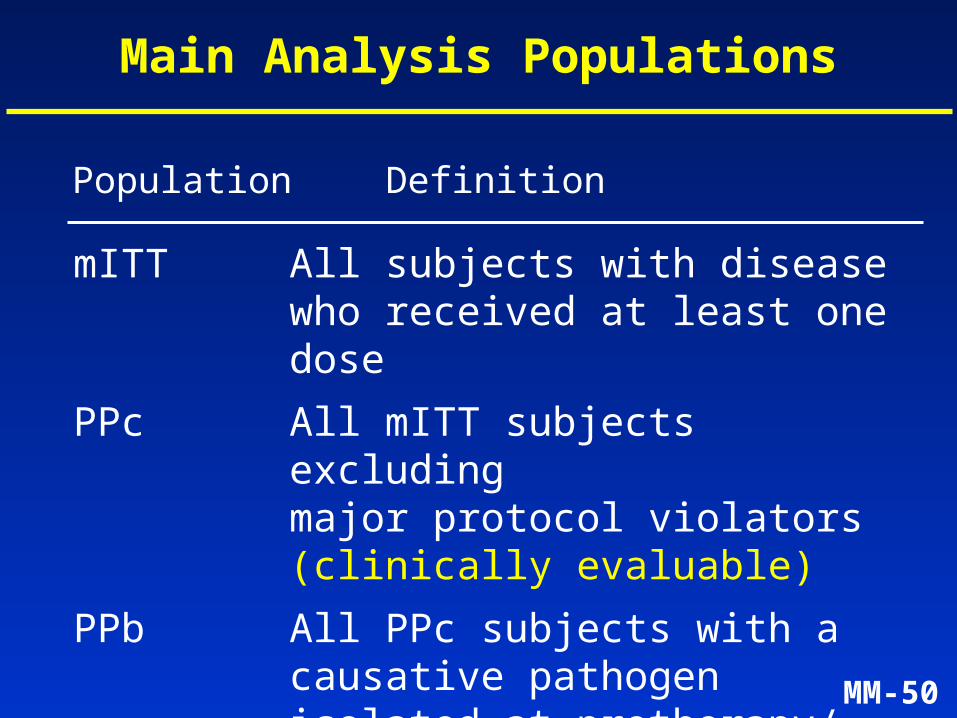
Main Analysis Populations
Population Definition
mITT All subjects with disease who received at least one dose
PPc All mITT subjects excluding major protocol violators (clinically evaluable)
PPb All PPc subjects with a causative pathogen isolated at pretherapy/ entry (microbiologically evaluable)
MM-51
Clinical Efficacy of Telithromycin
• Study design across indications
• Clinical efficacy by indication:– Community-acquired pneumonia (CAP)
– Acute exacerbation of chronic bronchitis (AECB)
– Acute sinusitis
– Tonsillitis/Pharyngitis
MM-52
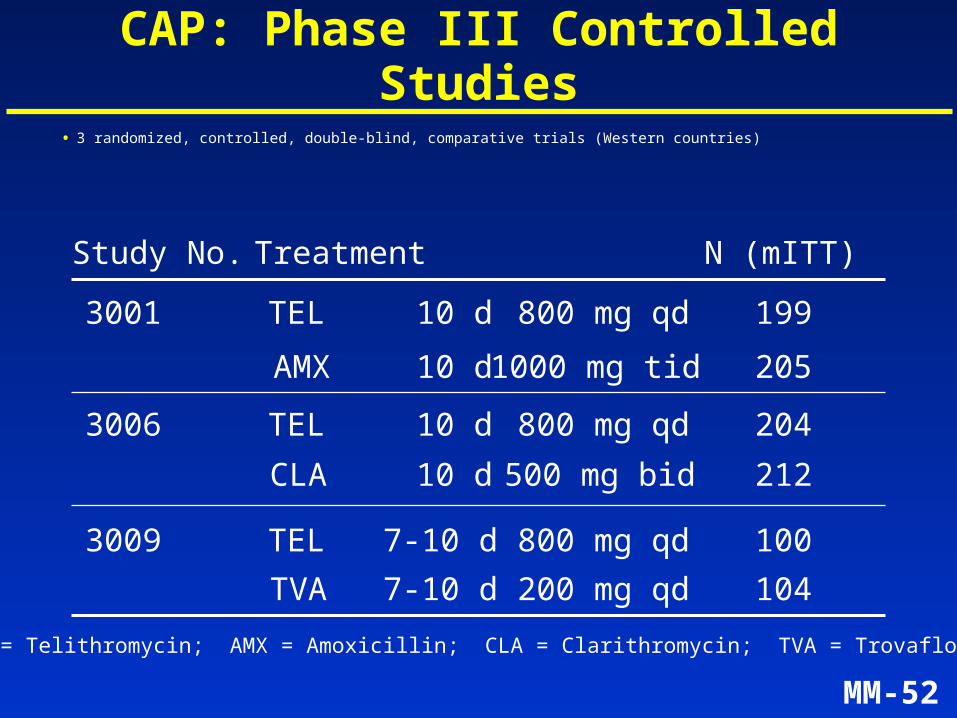
CAP: Phase III Controlled Studies
Study No. Treatment
3001 TEL 10 d 800 mg qd
AMX 10 d 1000 mg tid
3006 TEL 10 d 800 mg qd
CLA 10 d 500 mg bid
TEL = Telithromycin; AMX = Amoxicillin; CLA = Clarithromycin; TVA = Trovafloxacin
3009 TEL 7-10 d 800 mg qd
TVA 7-10 d 200 mg qd
• 3 randomized, controlled, double-blind, comparative trials (Western countries)
N (mITT)
199
205
204
212
100
104
MM-53
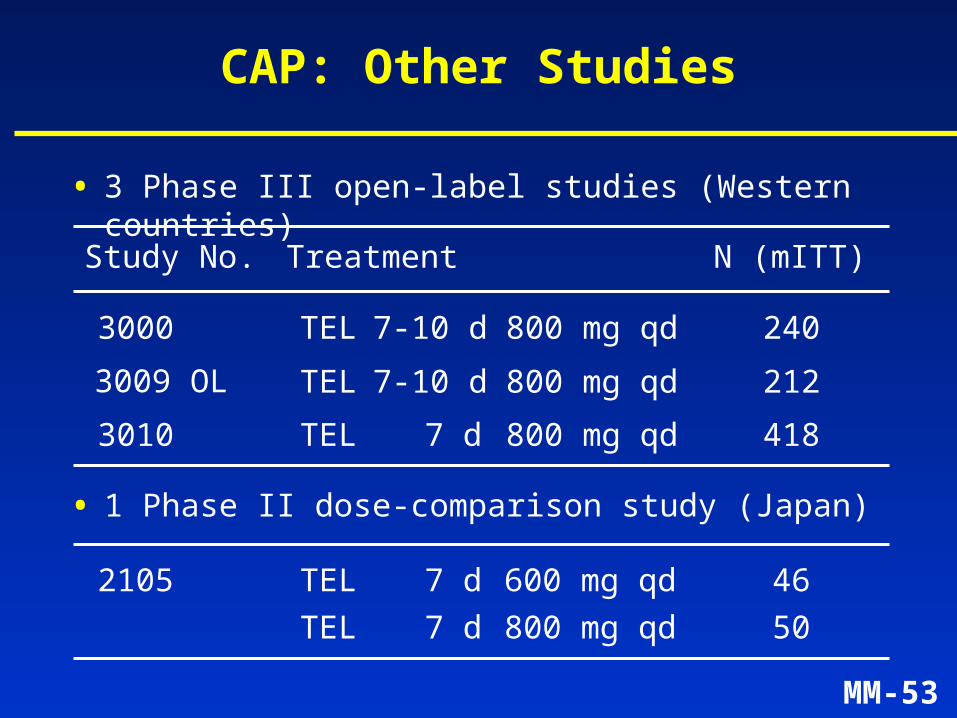
CAP: Other Studies
Study No. Treatment
3000 TEL 7-10 d 800 mg qd
3009 OL TEL 7-10 d 800 mg qd
• 3 Phase III open-label studies (Western countries)
N (mITT)
240
212
• 1 Phase II dose-comparison study (Japan)
3010 TEL 7 d 800 mg qd 418
2105 TEL 7 d 600 mg qd
TEL 7 d 800 mg qd
46
50
MM-54
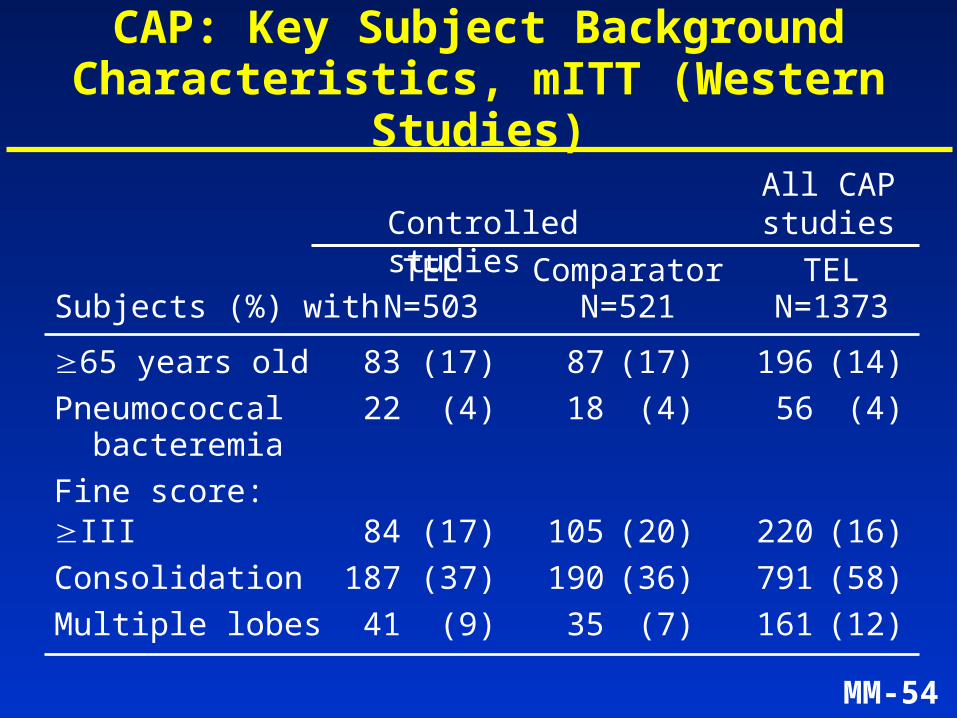
CAP: Key Subject Background Characteristics, mITT (Western Studies)
65 years old 83 (17) 87 (17) 196 (14)
Pneumococcal 22 (4) 18 (4) 56 (4) bacteremia
Fine score:III 84 (17) 105 (20) 220 (16)
Consolidation 187 (37) 190 (36) 791 (58)
Multiple lobes 41 (9) 35 (7) 161 (12)
Controlled studies
TEL Comparator TELSubjects (%) with N=503 N=521 N=1373
All CAPstudies
MM-55
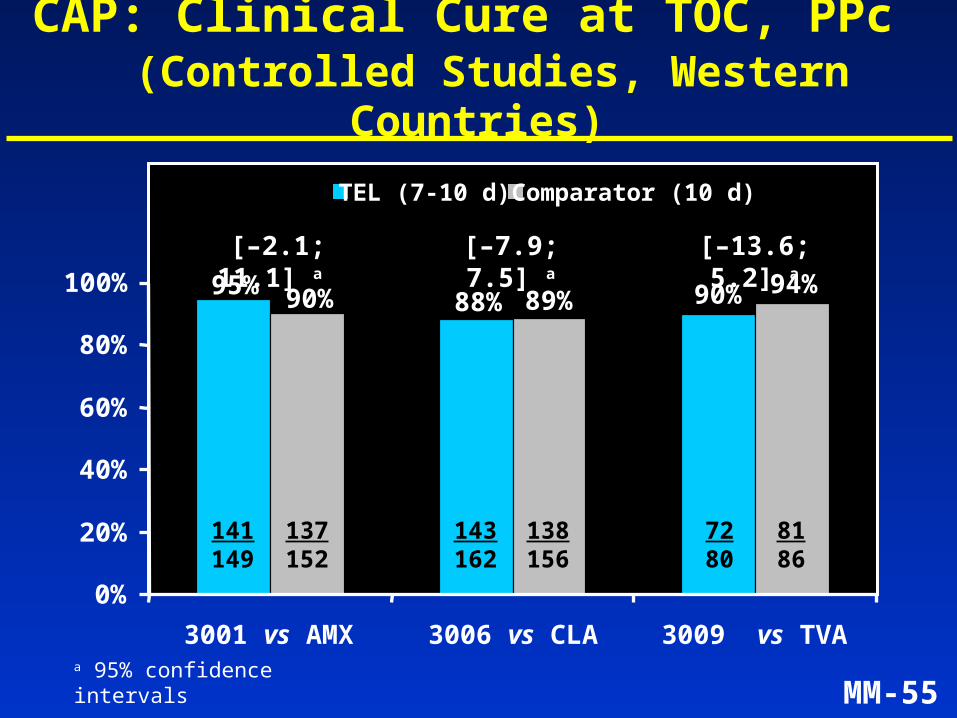
CAP: Clinical Cure at TOC, PPc (Controlled Studies, Western Countries)
95%88%
94%90%89%90%
0%
20%
40%
60%
80%
100%
3001 vs AMX 3006 vs CLA 3009 vs TVA
TEL (7-10 d) Comparator (10 d)
[–2.1; 11.1] a
143162
138156
141149
137152
7280
8186
a 95% confidence intervals
[–7.9; 7.5] a [–13.6; 5.2] a
MM-56
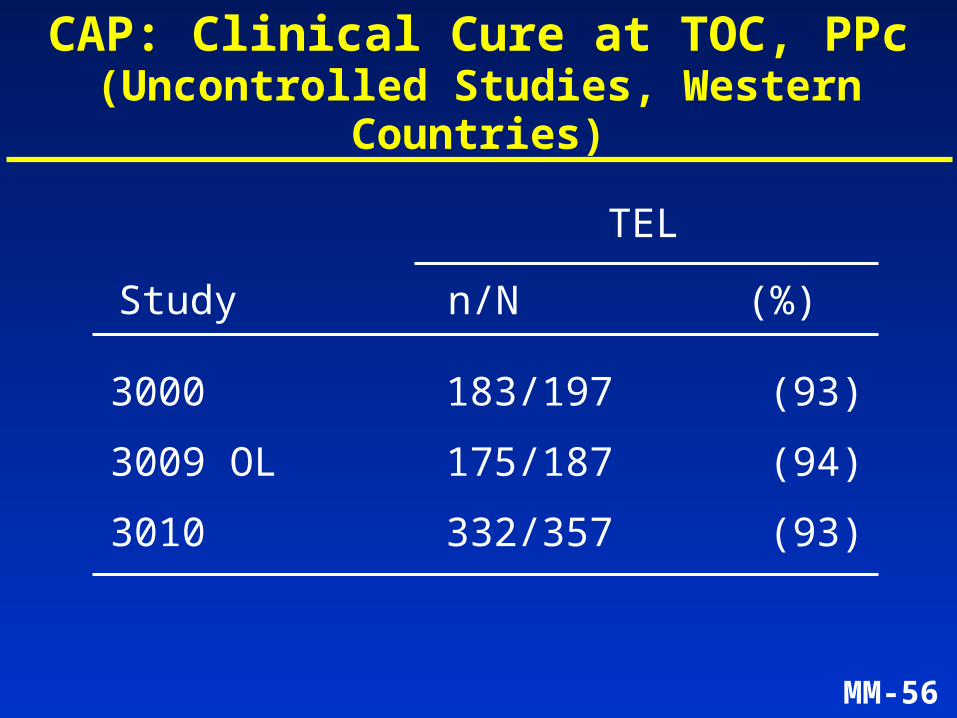
CAP: Clinical Cure at TOC, PPc(Uncontrolled Studies, Western Countries)
3000 183/197 (93)
3009 OL 175/187 (94)
3010 332/357 (93)
TEL
n/N (%)Study
MM-57
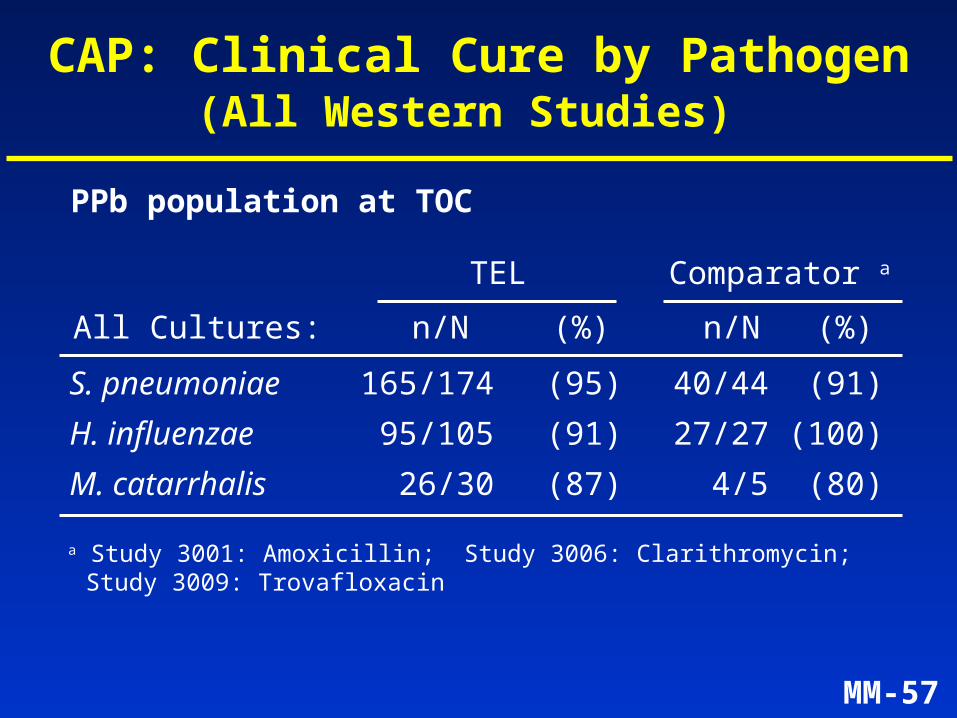
S. pneumoniae 165/174 (95) 40/44 (91)
H. influenzae 95/105 (91) 27/27 (100)
M. catarrhalis 26/30 (87) 4/5 (80)
TEL Comparator a
All Cultures: n/N (%) n/N (%)
CAP: Clinical Cure by Pathogen(All Western Studies)
a Study 3001: Amoxicillin; Study 3006: Clarithromycin; Study 3009: Trovafloxacin
PPb population at TOC
MM-58
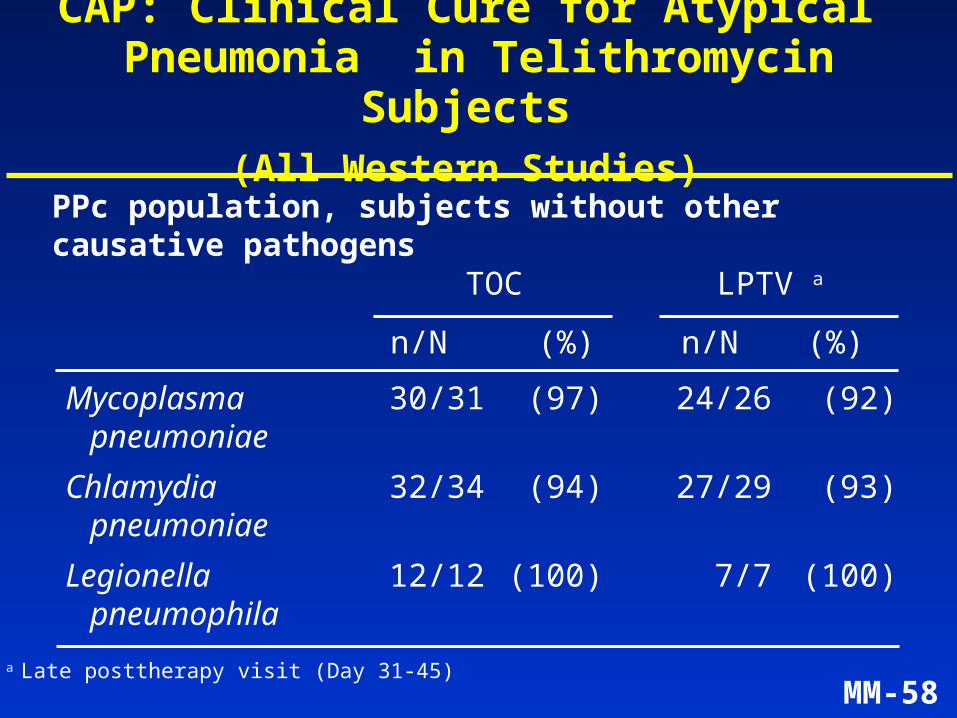
Mycoplasma 30/31 (97) 24/26 (92)pneumoniae
Chlamydia 32/34 (94) 27/29 (93)pneumoniae
Legionella 12/12 (100) 7/7 (100)pneumophila
TOC LPTV a
n/N (%) n/N (%)
CAP: Clinical Cure for Atypical Pneumonia in Telithromycin Subjects
(All Western Studies)
a Late posttherapy visit (Day 31-45)
PPc population, subjects without other causative pathogens
MM-59
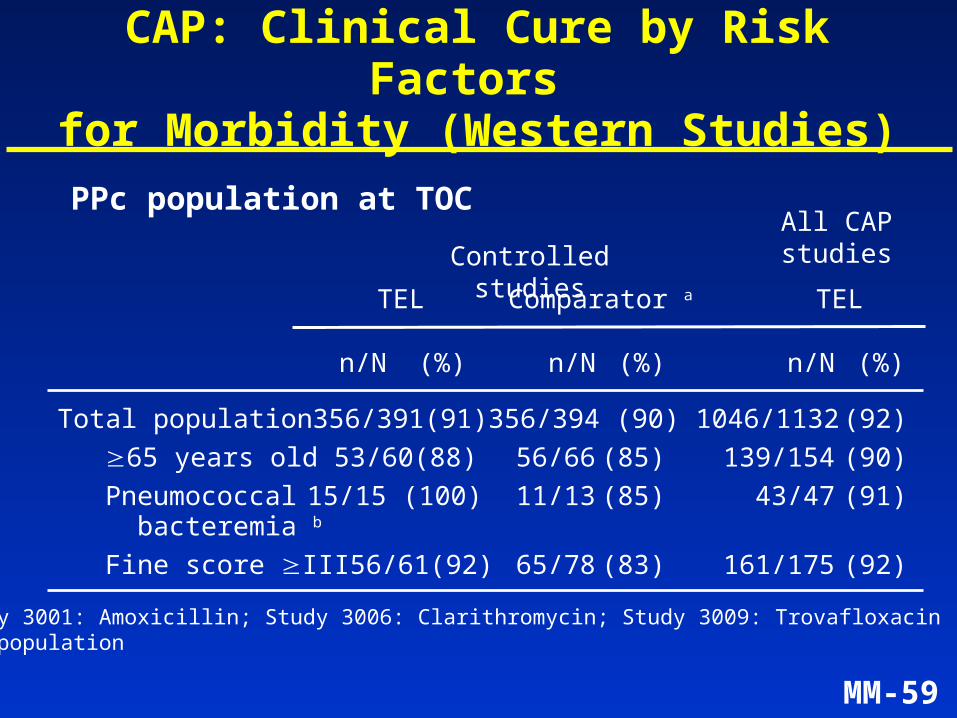
CAP: Clinical Cure by Risk Factors for Morbidity (Western Studies)
Total population 356/391 (91) 356/394 (90) 1046/1132 (92)
65 years old 53/60 (88) 56/66 (85) 139/154 (90)
Pneumococcal 15/15 (100) 11/13 (85) 43/47 (91) bacteremia b
Fine score III 56/61 (92) 65/78 (83) 161/175 (92)
Controlled studies
n/N (%) n/N (%) n/N (%)
All CAPstudies
PPc population at TOC
TEL Comparator a TEL
a Study 3001: Amoxicillin; Study 3006: Clarithromycin; Study 3009: Trovafloxacin b PPb population
MM-60
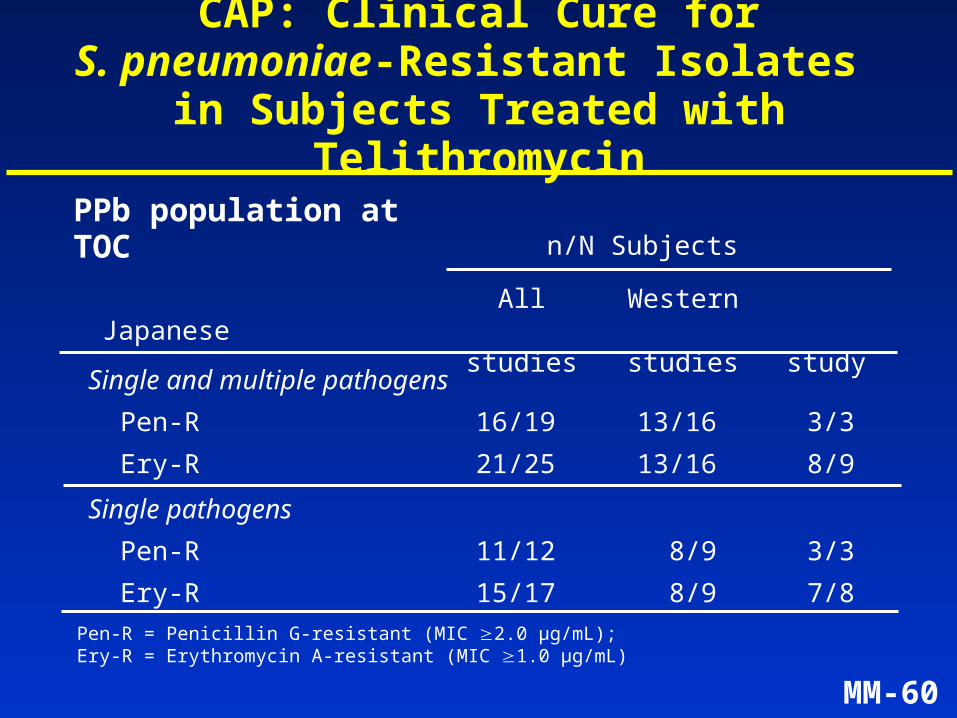
CAP: Clinical Cure forS. pneumoniae-Resistant Isolates
in Subjects Treated with Telithromycin
Single and multiple pathogens
Pen-R 16/19 13/16 3/3
Ery-R 21/25 13/16 8/9
Single pathogens
Pen-R 11/12 8/9 3/3
Ery-R 15/17 8/9 7/8
n/N SubjectsPPb population at TOC
All Western Japanesestudies studies study
Pen-R = Penicillin G-resistant (MIC 2.0 µg/mL); Ery-R = Erythromycin A-resistant (MIC 1.0 µg/mL)
MM-61
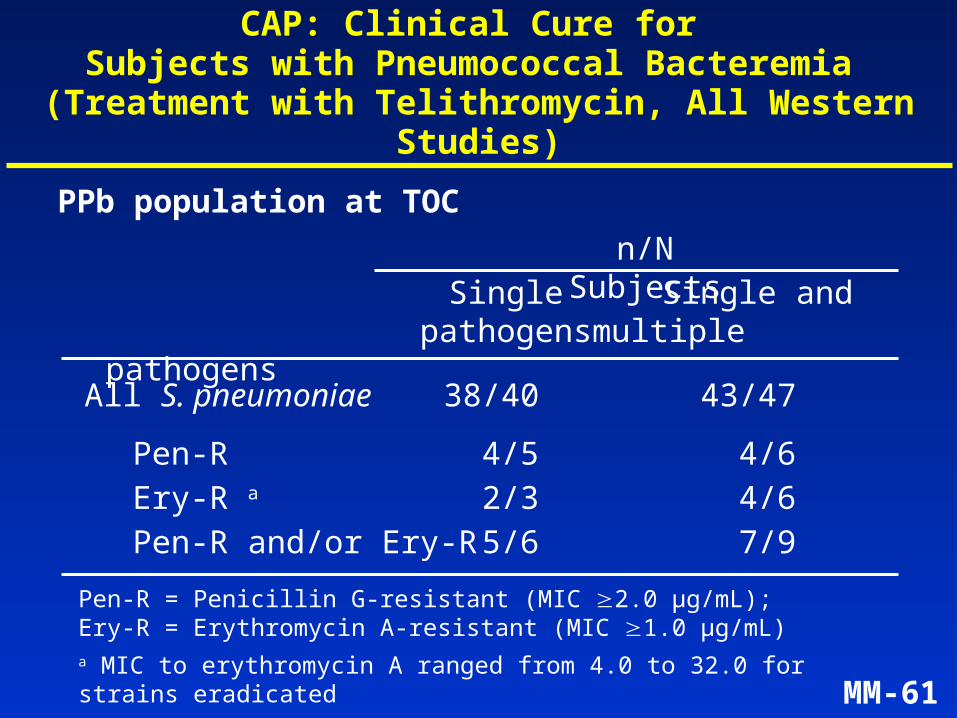
CAP: Clinical Cure for Subjects with Pneumococcal Bacteremia
(Treatment with Telithromycin, All Western Studies)
All S. pneumoniae 38/40 43/47
Pen-R 4/5 4/6Ery-R a 2/3 4/6Pen-R and/or Ery-R 5/6 7/9
PPb population at TOC
Single Single andpathogens multiple
pathogens
Pen-R = Penicillin G-resistant (MIC 2.0 µg/mL); Ery-R = Erythromycin A-resistant (MIC 1.0 µg/mL)a MIC to erythromycin A ranged from 4.0 to 32.0 for strains eradicated
n/N Subjects
MM-62
Summary of Efficacy in CAP
• Effective in outpatients at risk for complications (elderly, pneumococcal bacteremia, Legionella)
Common pathogens– S. pneumoniae
• Pen-R strains• Ery-R strains
– H. influenzae– M. catarrhalis
Atypical pathogens– M. pneumoniae– C. pneumoniae– L. pneumophila
• Treatment with telithromycin 800 mg once daily for 7 to 10 days is effective in CAP due to:
MM-63
Clinical Efficacy of Telithromycin
• Study design across indications
• Clinical efficacy by indication:– Community-acquired pneumonia (CAP)
– Acute exacerbation of chronic bronchitis (AECB)
– Acute sinusitis
– Tonsillitis/Pharyngitis
MM-64
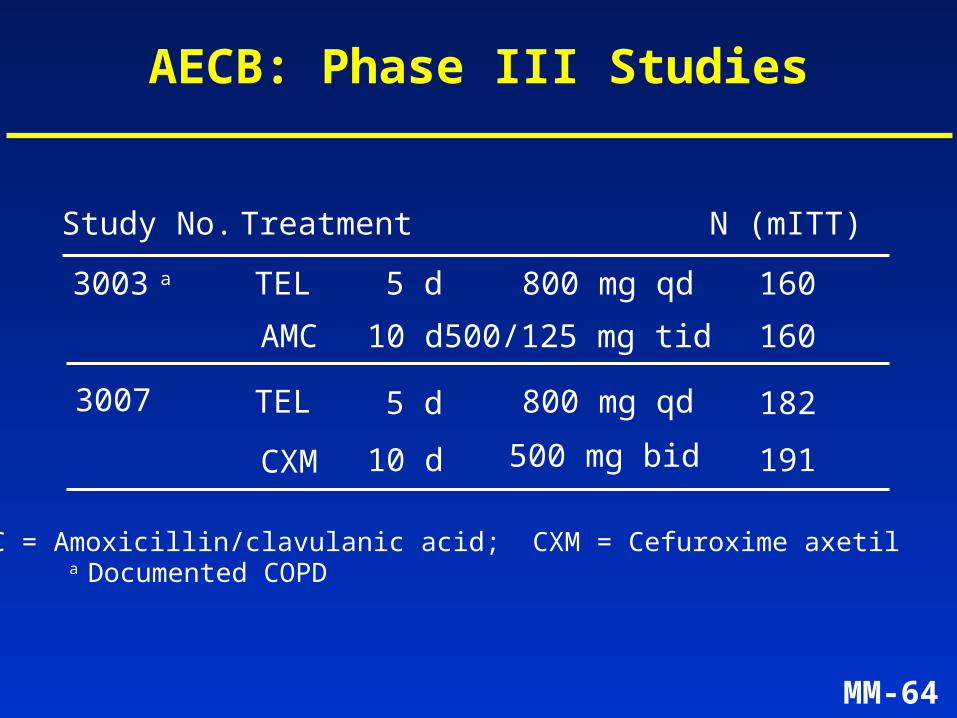
AECB: Phase III Studies
3003 a TEL 5 d 800 mg qd
AMC 10 d 500/125 mg tid
3007 TEL 5 d 800 mg qd
CXM 10 d 500 mg bid
AMC = Amoxicillin/clavulanic acid; CXM = Cefuroxime axetil
Study No. Treatment N (mITT)
160
160
182
191
a Documented COPD
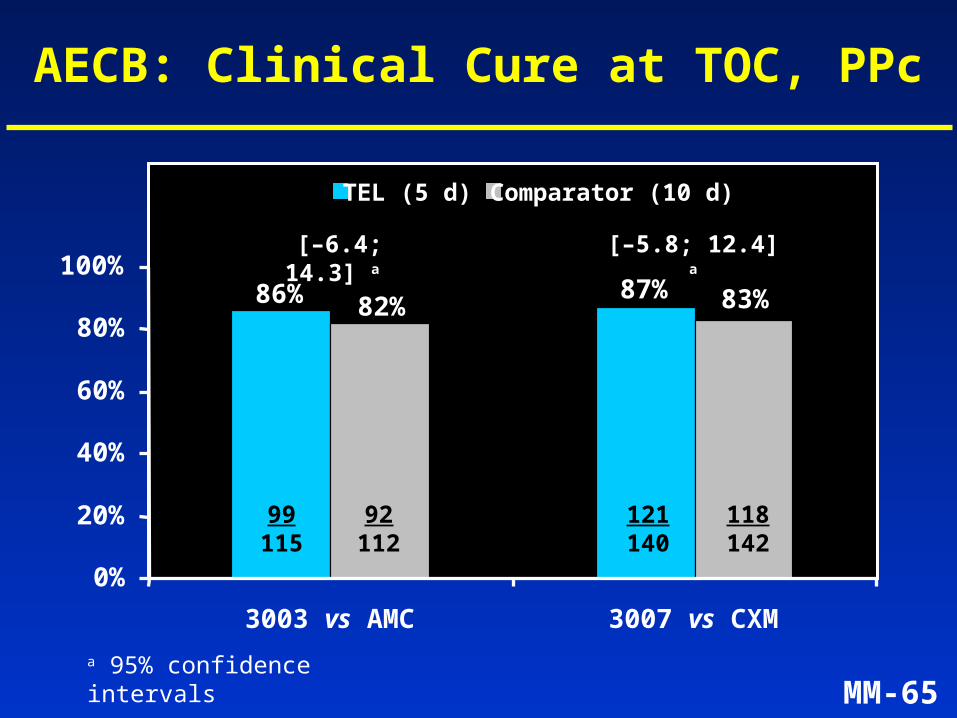
MM-65
AECB: Clinical Cure at TOC, PPc
86% 87% 83%82%
0%
20%
40%
60%
80%
100%
3003 vs AMC 3007 vs CXM
TEL (5 d) Comparator (10 d)
99115
92112
121140
118142
[–6.4; 14.3] a
a 95% confidence intervals
[–5.8; 12.4] a
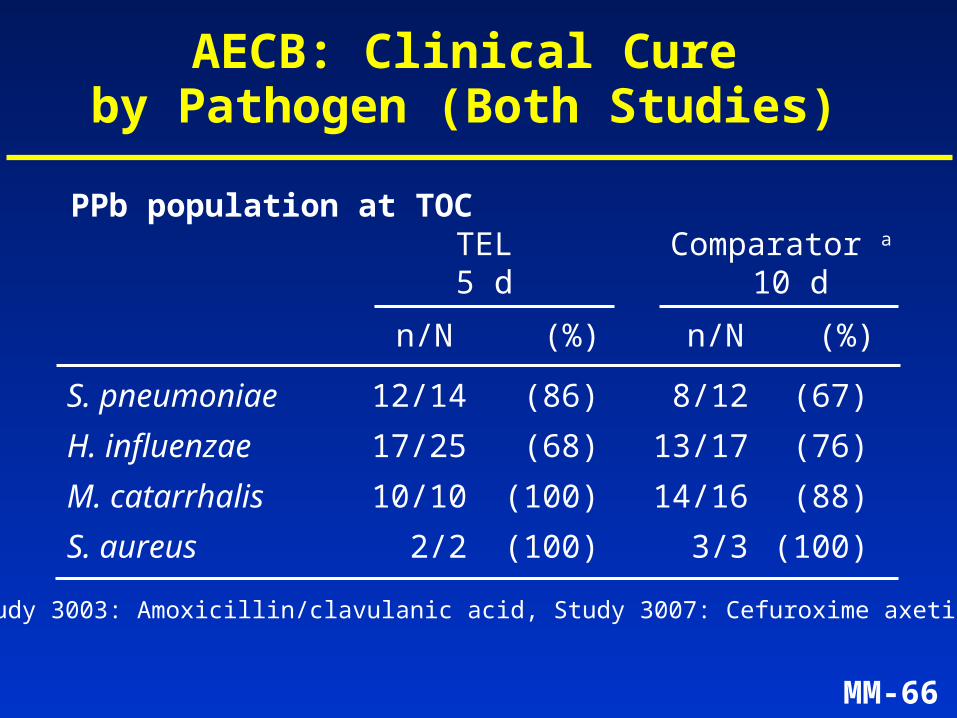
MM-66
S. pneumoniae 12/14 (86) 8/12 (67)
H. influenzae 17/25 (68) 13/17 (76)
M. catarrhalis 10/10 (100) 14/16 (88)
S. aureus 2/2 (100) 3/3 (100)
TEL Comparator a 5 d 10 d
n/N (%) n/N (%)
AECB: Clinical Cure by Pathogen (Both Studies)
PPb population at TOC
a Study 3003: Amoxicillin/clavulanic acid, Study 3007: Cefuroxime axetil
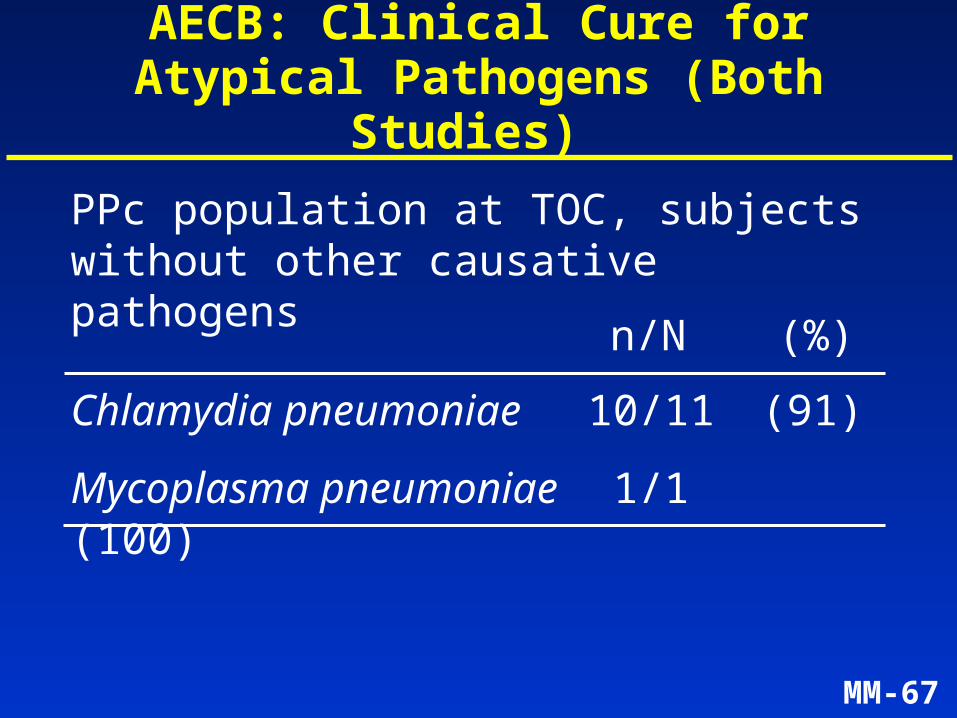
MM-67
Chlamydia pneumoniae 10/11 (91)
Mycoplasma pneumoniae 1/1 (100)
n/N (%)
AECB: Clinical Cure for Atypical Pathogens (Both Studies)
PPc population at TOC, subjects without other causative pathogens
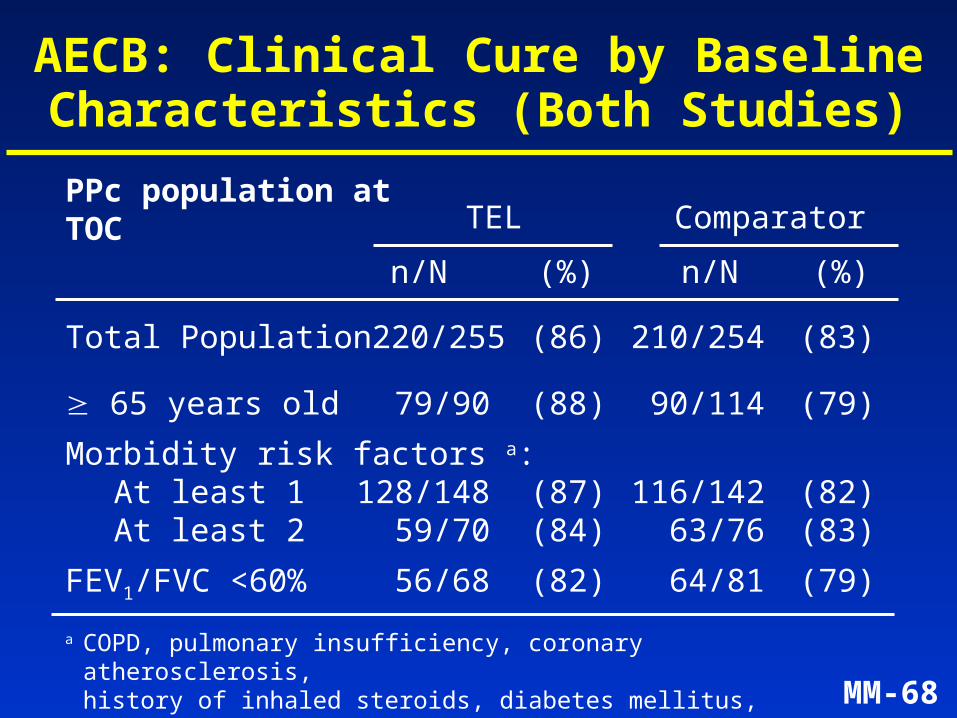
MM-68
AECB: Clinical Cure by Baseline Characteristics (Both Studies)
Total Population 220/255 (86) 210/254 (83)
65 years old 79/90 (88) 90/114 (79)
Morbidity risk factors a: At least 1 128/148 (87) 116/142 (82)At least 2 59/70 (84) 63/76 (83)
FEV1/FVC <60% 56/68 (82) 64/81 (79)
TEL Comparator
n/N (%) n/N (%)
a COPD, pulmonary insufficiency, coronary atherosclerosis, history of inhaled steroids, diabetes mellitus, etc.
PPc population at TOC
MM-69
Summary of Efficacy in AECB
• Treatment with telithromycin 800 mg once daily for 5 days is effective in AECB due to:– S. pneumoniae– H. influenzae– M. catarrhalis– S. aureus– C. pneumoniae
• Effective in outpatients at risk for complications (elderly, significant obstruction)
MM-70
Clinical Efficacy of Telithromycin
• Study design across indications
• Clinical efficacy by indication:– Community-acquired pneumonia (CAP)
– Acute exacerbation of chronic bronchitis (AECB)
– Acute sinusitis
– Tonsillitis/Pharyngitis
MM-71
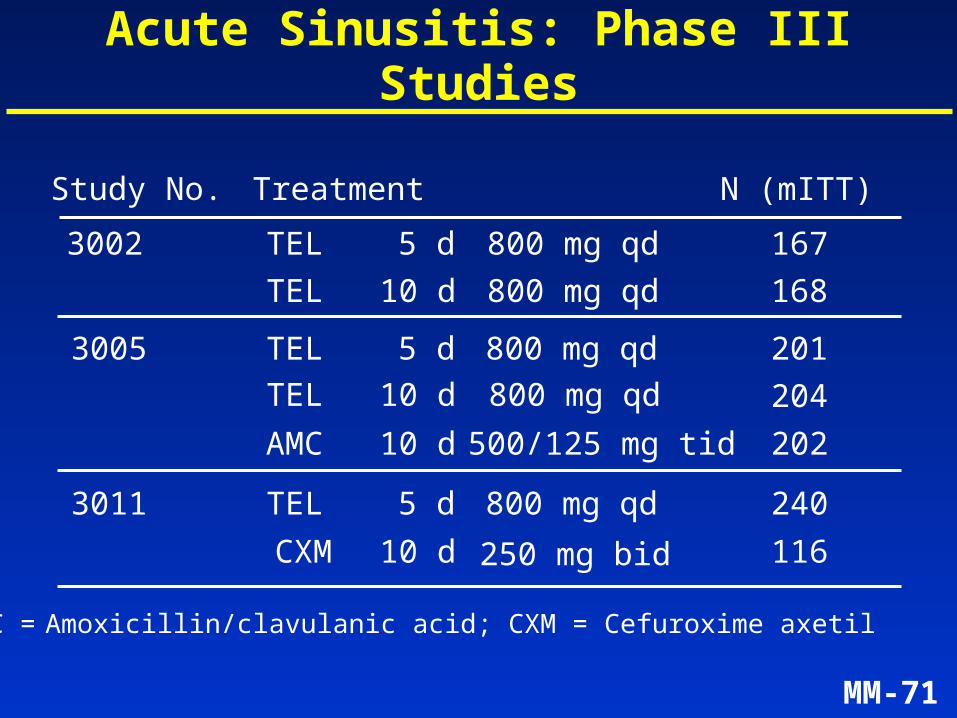
Acute Sinusitis: Phase III Studies
3002 TEL 5 d 800 mg qd
TEL 10 d 800 mg qd
AMC 10 d 500/125 mg tid
3005 TEL 5 d 800 mg qd
TEL 10 d 800 mg qd
AMC = Amoxicillin/clavulanic acid; CXM = Cefuroxime axetil
Study No. Treatment N (mITT)
3011 TEL
202
240
167
168
201
204
CXM 116
5 d
10 d 250 mg bid
800 mg qd
MM-72
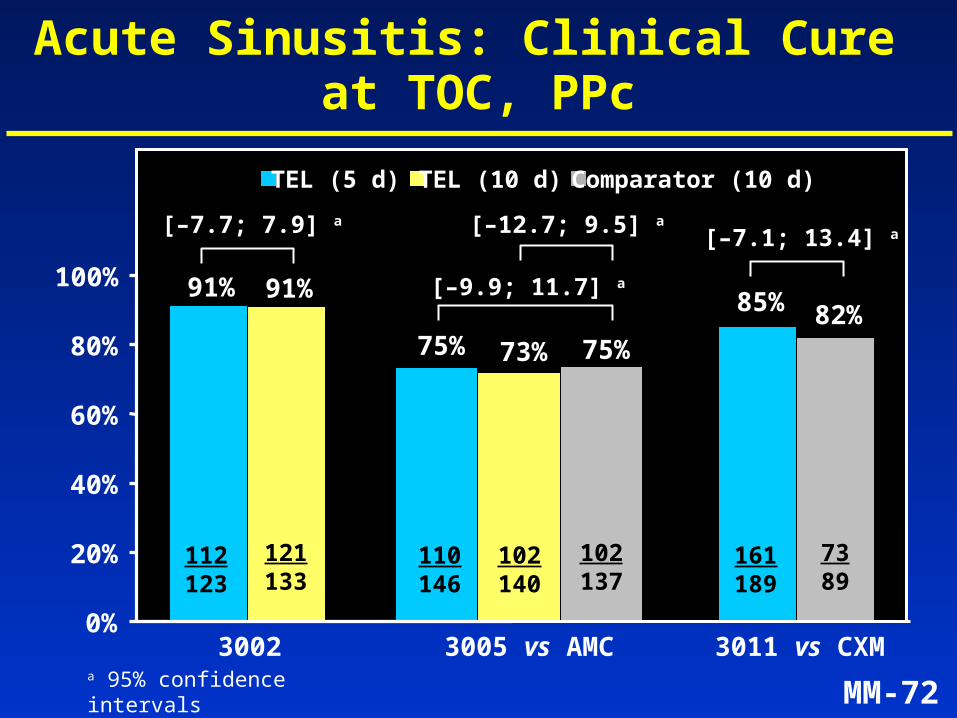
Acute Sinusitis: Clinical Cure at TOC, PPc
0%
20%
40%
60%
80%
100%
TEL (5 d) TEL (10 d) Comparator (10 d)
91% 91%
3002
112123
121133
[–7.7; 7.9] a
75% 73% 75%
3005 vs AMC
110146
102137
102140
[–12.7; 9.5] a
[–9.9; 11.7] a
a 95% confidence intervals
85% 82%
3011 vs CXM
161189
7389
[–7.1; 13.4] a
MM-73
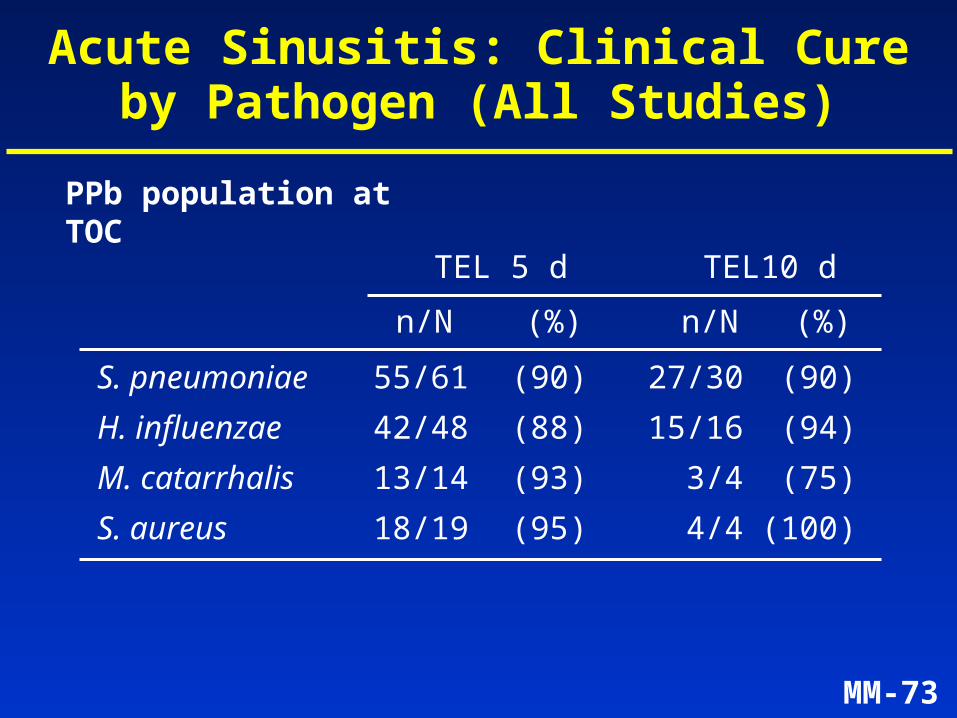
S. pneumoniae 55/61 (90) 27/30 (90)
H. influenzae 42/48 (88) 15/16 (94)
M. catarrhalis 13/14 (93) 3/4 (75)
S. aureus 18/19 (95) 4/4 (100)
TEL 5 d TEL10 d
n/N (%) n/N (%)
Acute Sinusitis: Clinical Cureby Pathogen (All Studies)
PPb population at TOC
MM-74
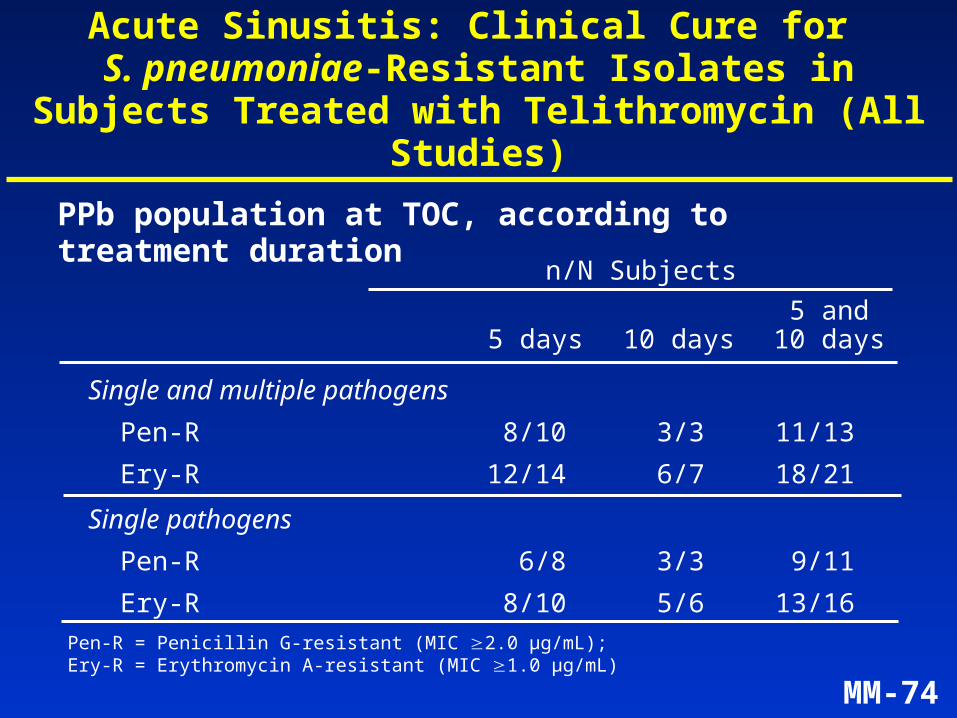
Acute Sinusitis: Clinical Cure for S. pneumoniae-Resistant Isolates in Subjects
Treated with Telithromycin (All Studies)
Single and multiple pathogens
Pen-R 8/10 3/3 11/13
Ery-R 12/14 6/7 18/21
Single pathogens
Pen-R 6/8 3/3 9/11
Ery-R 8/10 5/6 13/16
n/N Subjects
PPb population at TOC, according to treatment duration
5 and5 days 10 days 10 days
Pen-R = Penicillin G-resistant (MIC 2.0 µg/mL); Ery-R = Erythromycin A-resistant (MIC 1.0 µg/mL)
MM-75
Summary of Efficacy in Acute Sinusitis
• Treatment with telithromycin 800 mg once daily for 5 days is equivalent to 10 days of standard treatment given 2 to 3 times daily (amoxicillin/clavulanic acid, cefuroxime axetil)
• Telithromycin 800 mg once daily for 5 days is effective in acute sinusitis due to: – S. pneumoniae
• Pen-R strains• Ery-R strains
– H. influenzae– M. catarrhalis– S. aureus
MM-76
Clinical Efficacy of Telithromycin
• Study design across indications
• Clinical efficacy by indication:– Community-acquired pneumonia (CAP)
– Acute exacerbation of chronic bronchitis (AECB)
– Acute sinusitis
– Tonsillitis/Pharyngitis
MM-77
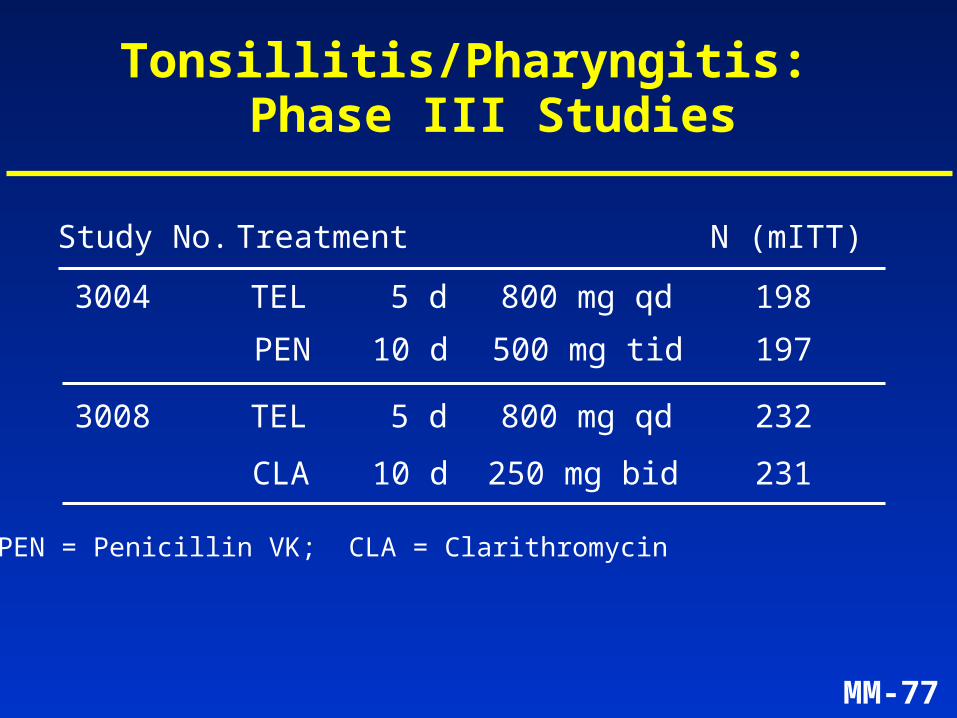
Tonsillitis/Pharyngitis: Phase III Studies
3004 TEL 5 d 800 mg qd
PEN 10 d 500 mg tid
3008 TEL 5 d 800 mg qd
CLA 10 d 250 mg bid
PEN = Penicillin VK; CLA = Clarithromycin
Study No. Treatment N (mITT)
198
197
232
231
MM-78
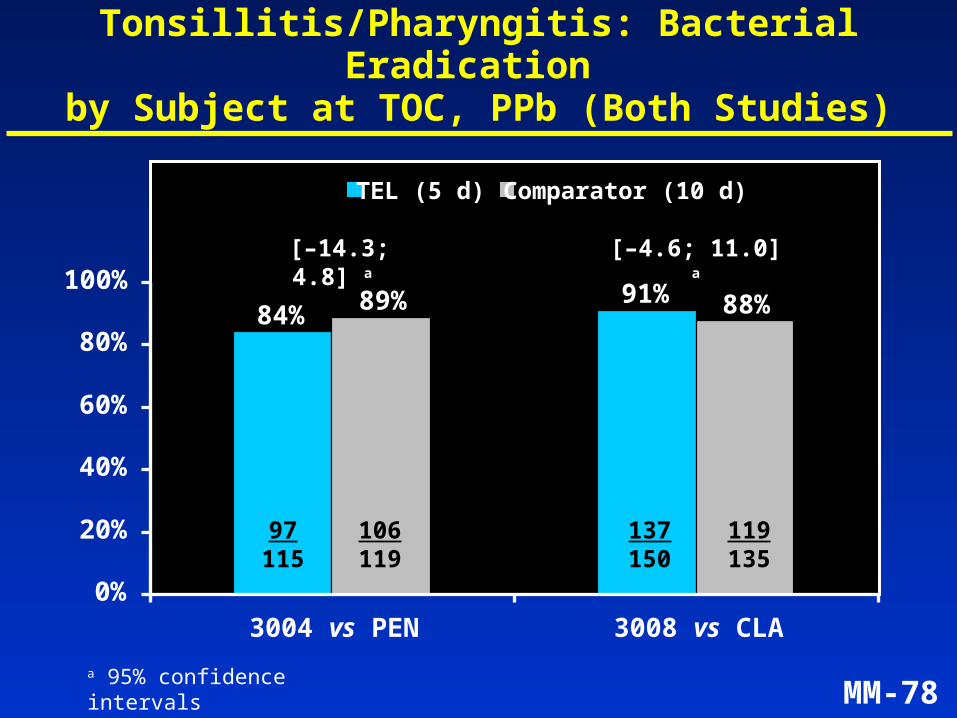
Tonsillitis/Pharyngitis: Bacterial Eradication by Subject at TOC, PPb (Both Studies)
84%91% 88%89%
0%
20%
40%
60%
80%
100%
3004 vs PEN 3008 vs CLA
TEL (5 d) Comparator (10 d)
97115
106119
137150
119135
[–14.3; 4.8] a
a 95% confidence intervals
[–4.6; 11.0] a
MM-79
Summary of Efficacy in Tonsillitis/Pharyngitis
• Treatment with telithromycin 800 mg once daily for 5 days is effective in GABHStonsillitis/pharyngitis
• Equivalence demonstrated between 5-day telithromycin treatment and 10-day standard treatment (penicillin VK 500 mg tid or clarithromycin 250 mg bid)
MM-80
Summary of Efficacy in RTIs (1)
• Efficacy results consistent across analysis populations in 13 studies in 4 indications
• 5-day treatment effective in AECB, acute sinusitis and tonsillitis/pharyngitis vs 10-day treatment with comparators
• 7 to 10-day treatment effective in CAP
MM-81
Summary of Efficacy in RTIs (2)
• Effective in subjects at risk for complications:
– CAP: elderly, pneumococcal bacteremia, Legionella infection
– AECB: elderly, significant obstruction (FEV1/FVC < 60%)
• Effective in infections (CAP, acute sinusitis) due to S. pneumoniae resistant to penicillin G and erythromycin A
MM-82
Safety Results
• Phase III:– general adverse event profile
– serious adverse events
– laboratory abnormalities
• ECG analysis
MM-83
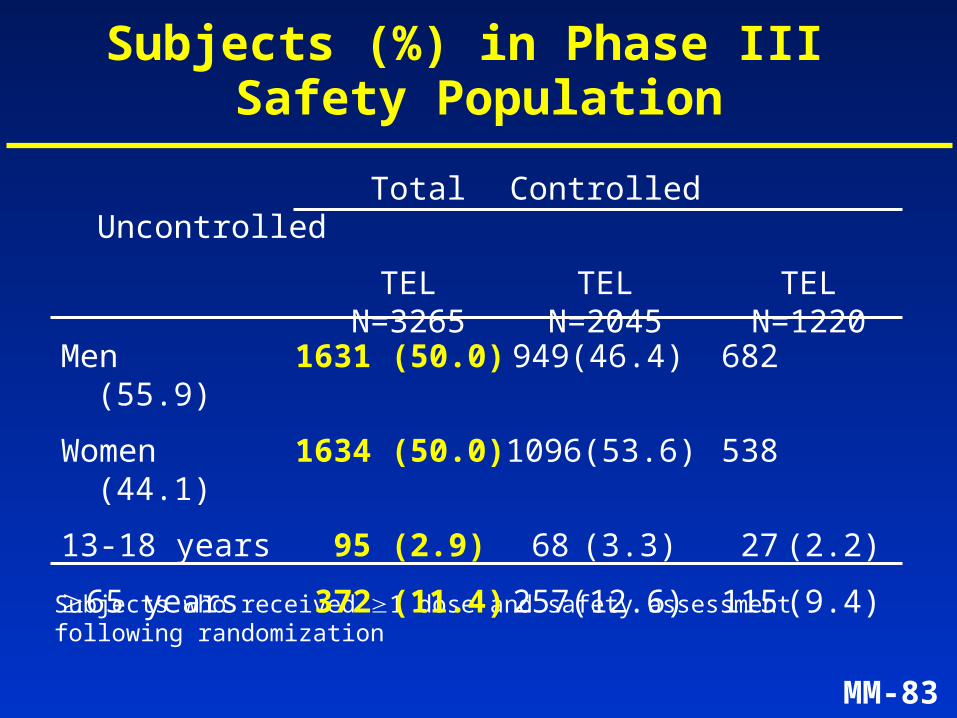
Total Controlled Uncontrolled
TEL TEL TEL N=3265 N=2045 N=1220
Subjects (%) in Phase III Safety Population
Subjects who received 1 dose and safety assessment following randomization
Men 1631 (50.0) 949 (46.4) 682 (55.9)
Women 1634 (50.0) 1096 (53.6) 538 (44.1)
13-18 years 95 (2.9) 68 (3.3) 27 (2.2)
65 years 372 (11.4) 257 (12.6) 115 (9.4)
MM-84
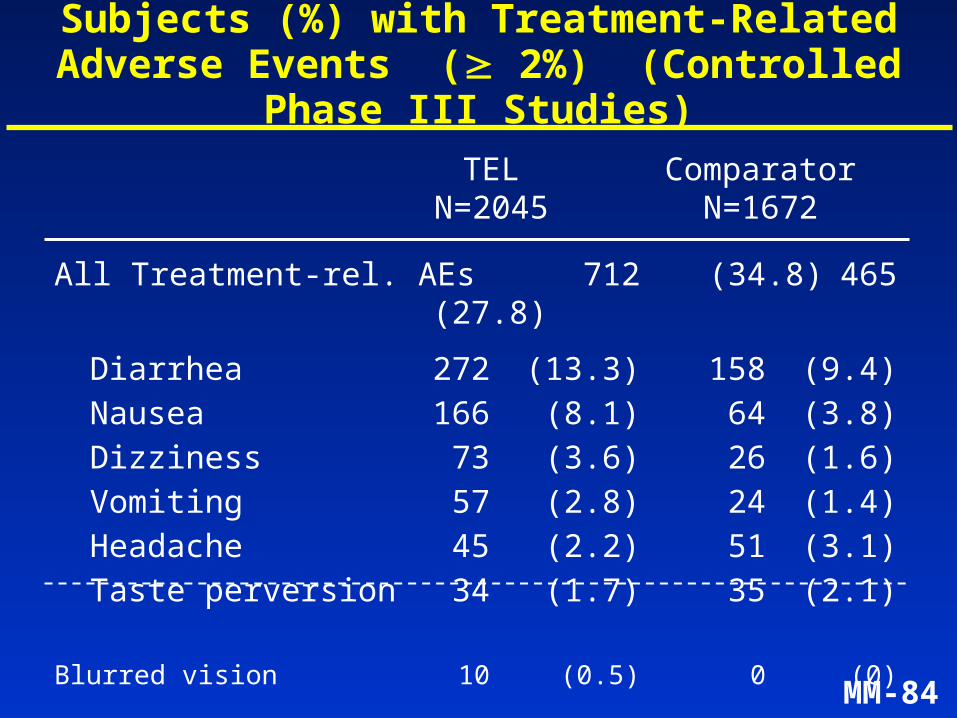
Subjects (%) with Treatment-Related Adverse Events ( 2%) (Controlled Phase III Studies)
TEL Comparator N=2045 N=1672
All Treatment-rel. AEs 712 (34.8) 465 (27.8)
Diarrhea 272 (13.3) 158 (9.4)Nausea 166 (8.1) 64 (3.8)Dizziness 73 (3.6) 26 (1.6)Vomiting 57 (2.8) 24 (1.4)Headache 45 (2.2) 51 (3.1)Taste perversion 34 (1.7) 35 (2.1)
Blurred vision 10 (0.5) 0 (0)
MM-85
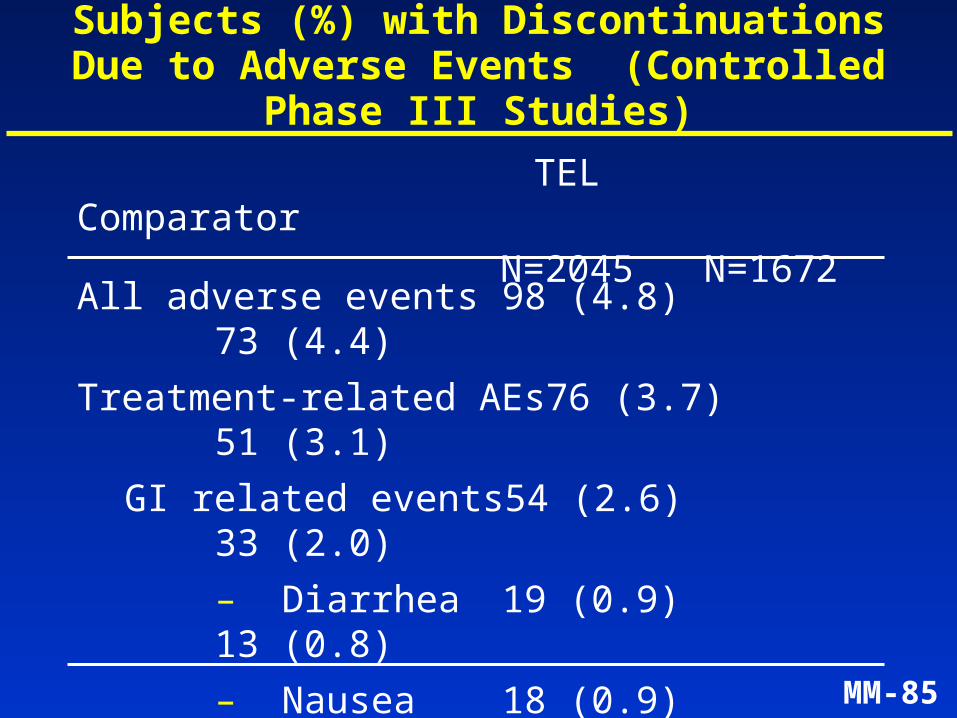
All adverse events 98 (4.8)73 (4.4)
Treatment-related AEs 76 (3.7)51 (3.1)
GI related events 54 (2.6)33 (2.0)
– Diarrhea 19 (0.9)13 (0.8)
– Nausea 18 (0.9)9 (0.5)
– Vomiting 19 (0.9)6 (0.4)
Other events 25 (1.2)18 (1.1)
Subjects (%) with Discontinuations Due to Adverse Events (Controlled Phase III Studies)
TEL Comparator N=2045 N=1672
MM-86
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 10
TEL 5-day
TEL 7-10 day
Clarithromycin
Amoxicillin/clavulanic acid
Day
% Subjects
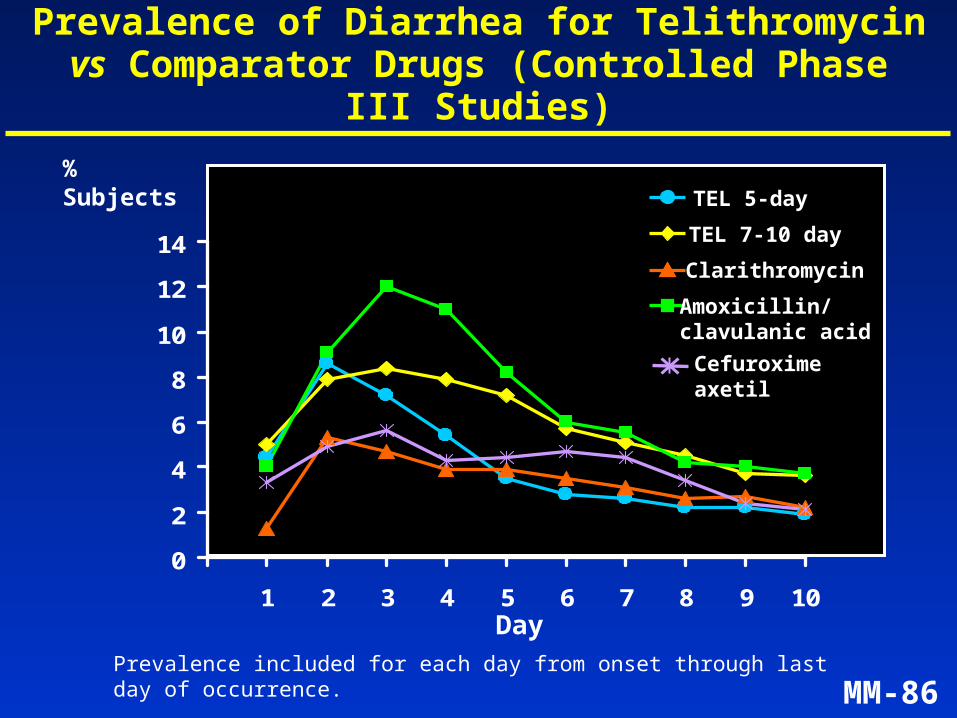
Prevalence of Diarrhea for Telithromycin vs Comparator Drugs (Controlled Phase III Studies)
Prevalence included for each day from onset through last day of occurrence.
Cefuroximeaxetil
MM-87
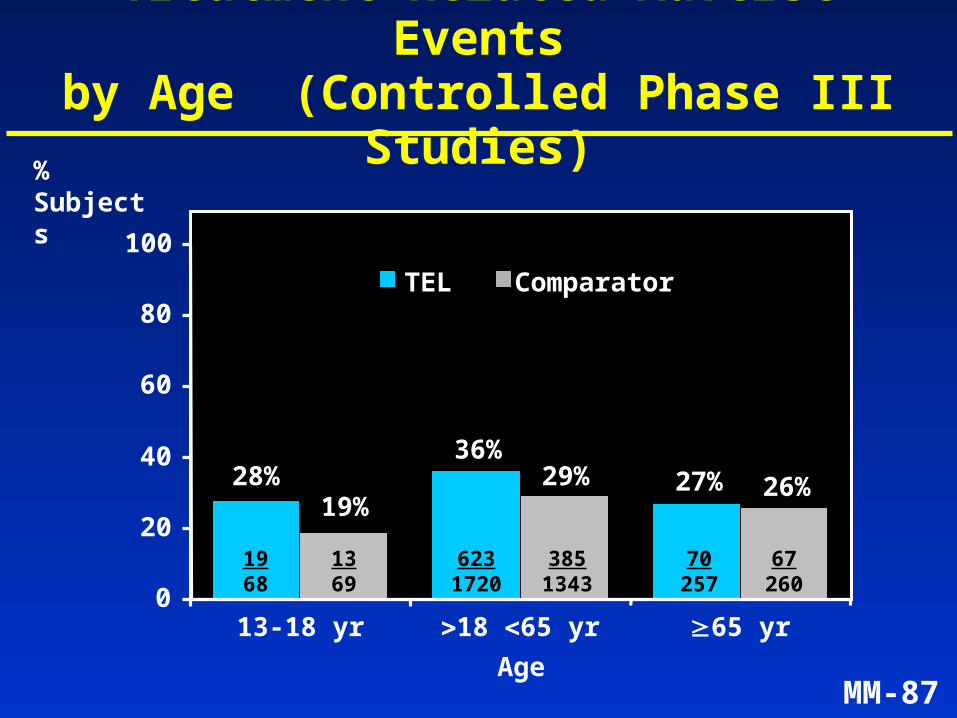
Treatment-Related Adverse Eventsby Age (Controlled Phase III Studies)
28%36%
27%19%
29% 26%
0
20
40
60
80
100
13-18 yr 18 65 yr 65 yr
TEL Comparator
1968
1369
6231720
3851343
70257
67260
Age
% Subjects
MM-88
Summary of Mortality(All Phase III Studies)
• Controlled studies: Telithromycin = 2Comparator = 4
• Uncontrolled studies: Telithromycin = 5
• No treatment-related deaths
• Deaths occurred in CAP subjects(telithromycin 7/1415; 0.5%)
MM-89
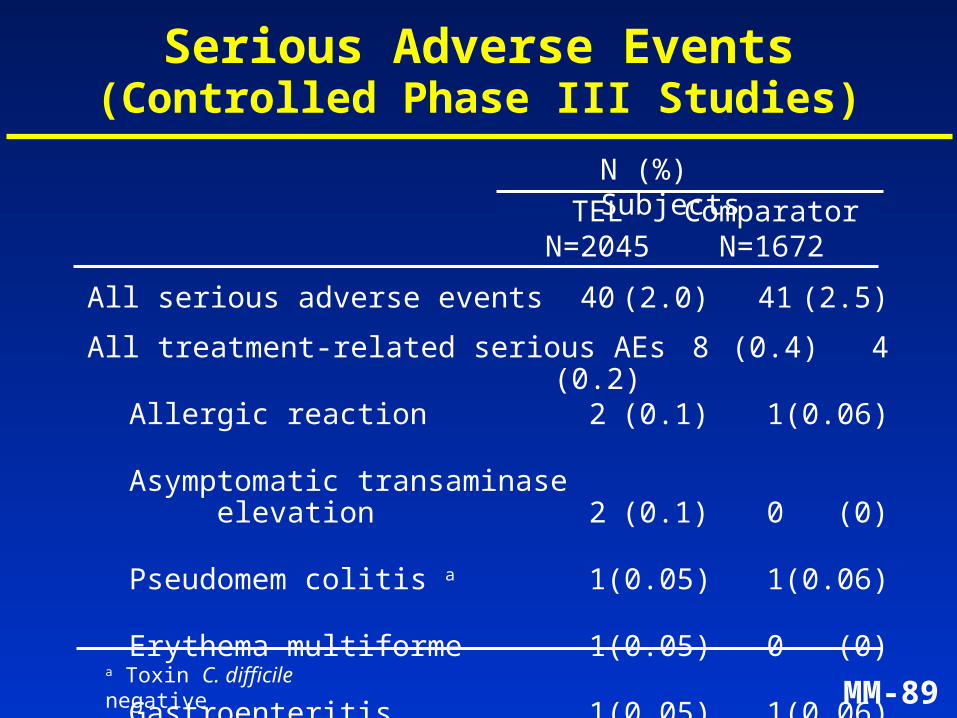
All serious adverse events 40 (2.0) 41 (2.5)
All treatment-related serious AEs 8 (0.4) 4 (0.2)
Allergic reaction 2 (0.1) 1 (0.06)
Asymptomatic transaminase elevation 2 (0.1) 0 (0)
Pseudomem colitis a 1 (0.05) 1 (0.06)
Erythema multiforme 1 (0.05) 0 (0)
Gastroenteritis 1 (0.05) 1 (0.06)
Vomiting 1 (0.05) 0 (0)
Dyspnea 0 (0) 1 (0.06)
Serious Adverse Events(Controlled Phase III Studies)
TEL ComparatorN=2045 N=1672
N (%) Subjects
a Toxin C. difficile negative
MM-90
Subject 0502/1069
53 year-old man with CAP and baseline elevated transaminases,eosinophilia, history of diabetes, asthma, 3 recent courses of macrolides
• Episode 1: four days after completing telithromycin, new onset of fever and diarrhea; peak ALT 1529 U/L 8 days later – Biopsy (6 days after peak transaminase): centrilobular necrosis,
granulomas, eosinophil/plasma cell infiltration
– Resolved with return to baseline levels 8 weeks after starting therapy
• Episode 2: asymptomatic transaminase increase (1331 U/L ALT) 9 months after telithromycin therapy, with normalization 10 weeks later– Second biopsy (~7 weeks after peak transaminase): centrilobular
hepatic cell depletion without frank necrosis, plasma cell infiltration, bridging fibrosis
MM-91
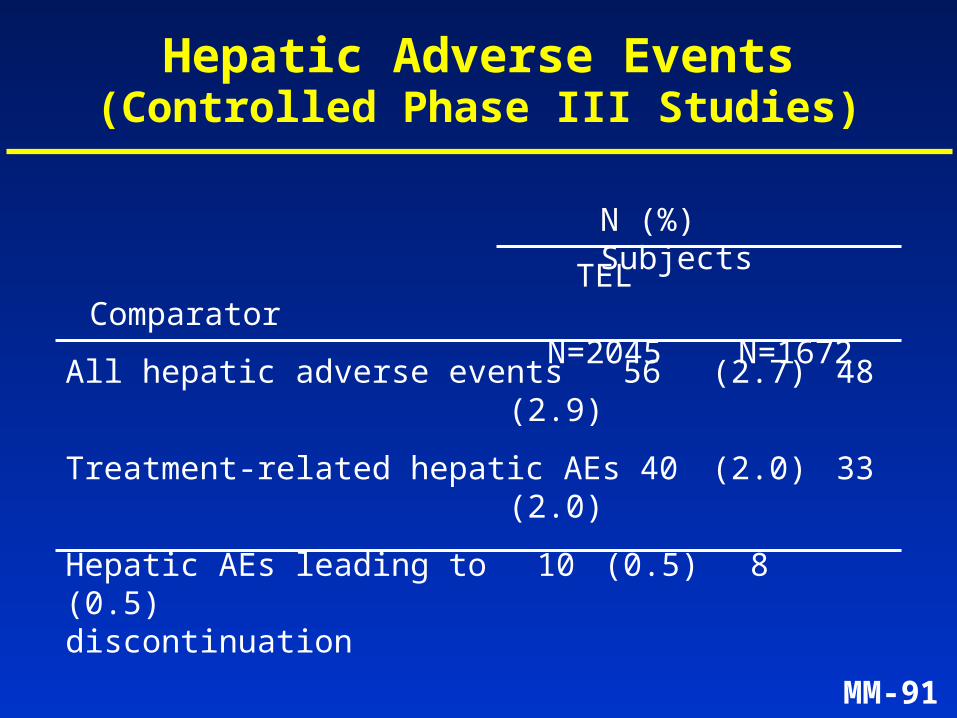
All hepatic adverse events 56 (2.7) 48 (2.9)
Treatment-related hepatic AEs 40 (2.0) 33 (2.0)
Hepatic AEs leading to 10 (0.5) 8 (0.5) discontinuation
Hepatic Adverse Events(Controlled Phase III Studies)
TEL ComparatorN=2045 N=1672
N (%) Subjects
MM-92
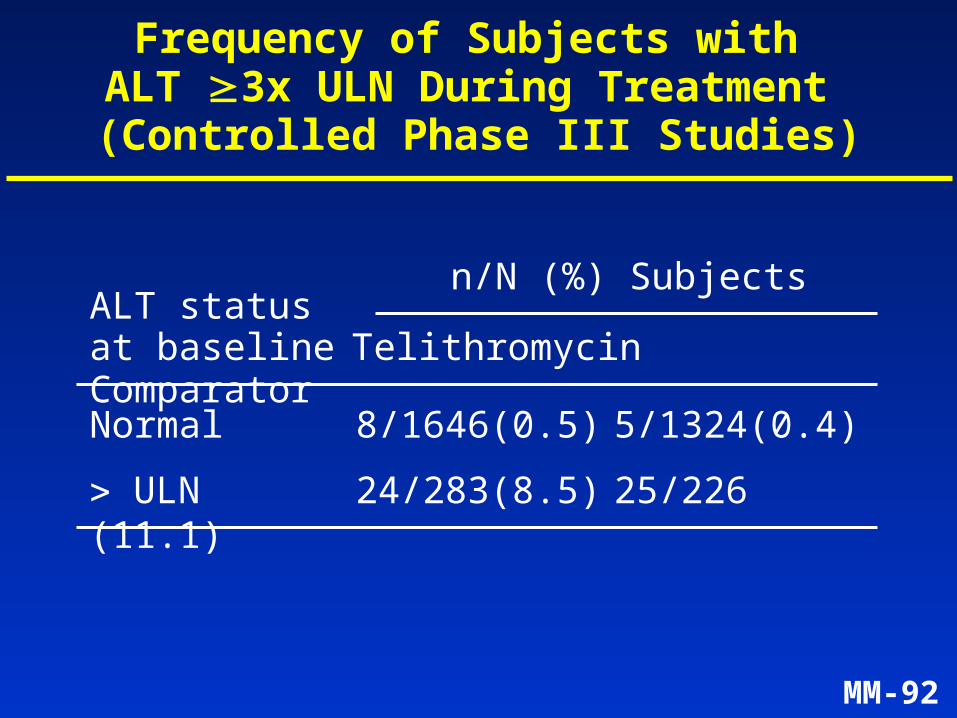
Frequency of Subjects with ALT 3x ULN During Treatment
(Controlled Phase III Studies)
n/N (%) SubjectsALT statusat baseline Telithromycin Comparator
Normal 8/1646 (0.5) 5/1324 (0.4)
ULN 24/283 (8.5) 25/226 (11.1)
MM-93
0
20
40
60
80
100
0
20
40
60
80
100
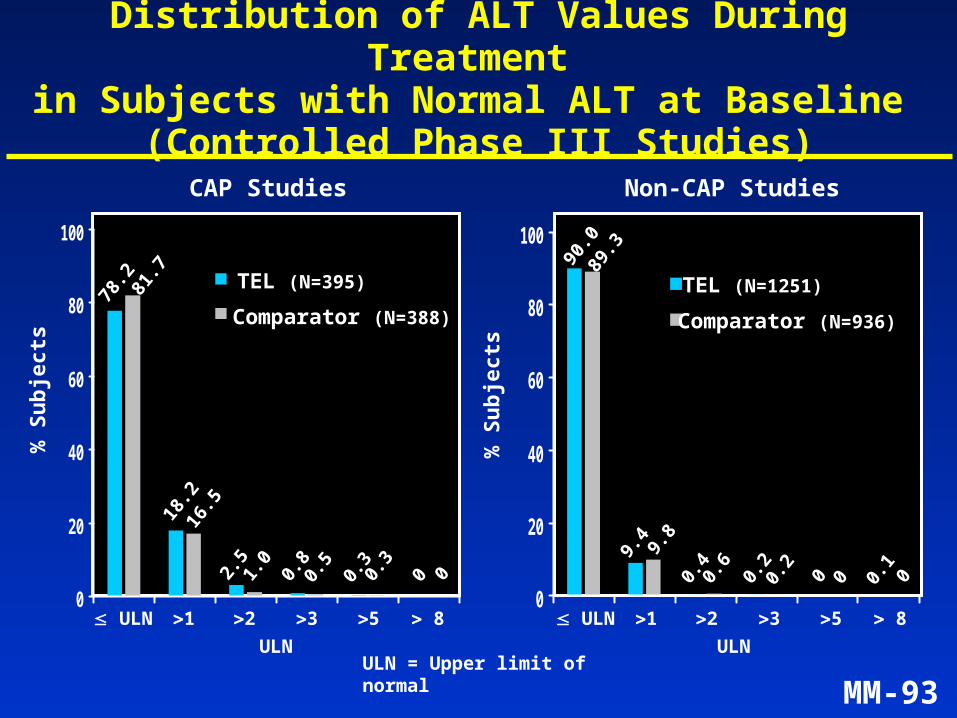
Distribution of ALT Values During Treatment in Subjects with Normal ALT at Baseline
(Controlled Phase III Studies)
CAP Studies Non-CAP Studies
ULN ULN
% S
ub
ject
s
% S
ub
ject
s
ULN = Upper limit of normal
TEL (N=1251)
Comparator (N=936)
TEL (N=395)
Comparator (N=388)
1 2 3 5 8 ULN ULN 1 2 3 5 8
2.5
1.0
0.8
0.5
0.3
0.3
0 0 0.4
0.6
0.2
0.2
0 0 0.1
0
18.2
16.5
78.2 81.7
9.4 9.8
90.0
89.3
MM-94
Summary of Phase III Safety
• Well tolerated:– pattern of adverse events similar to macrolides
– GI events in the range seen with other antibiotics
– adverse event profile similar in different age groups
– rates of transaminase elevation similar to comparators
• Low incidence of serious adverse events and discontinuations, similar to comparators
MM-95
Telithromycin – Presentation Agenda
Introduction Mindell Seidlin, MD
Microbiology André Bryskier, MD
Human Pharmacology Vijay Bhargava, PhD
Clinical Efficacy and Safety Bruno Leroy, MD
ECG Analysis Claude Benedict, MDSenior VP,Preclinical and Early Clinical Development, Aventis
Conclusions Mindell Seidlin, MD
MM-96
Background
• Macrolides have been associated with changes in cardiac repolarization
• Telithromycin is structurally derived from macrolides
• Extensive preclinical and prospective clinical investigation of potential effect of telithromycin on cardiac repolarization and comparison to macrolides and non-macrolides
• Program was designed in accordance with EU guidelines and FDA recommendations
MM-97
Telithromycin: Preclinical Studies
• Binding to membrane ionic channels (KATP, Kvoltage-dependent, KCa, Na, L-type Ca)
• Interaction with cloned channels(Ikr (HERG), Kv1.5, IKS)
• Studies on isolated human atrial cells(Ito, Ikur, AP duration)
• Rabbit Purkinje fibers:– bradycardia, hypokalemia– interaction with sotalol and quinidine
• Studies in awake dogs
MM-98
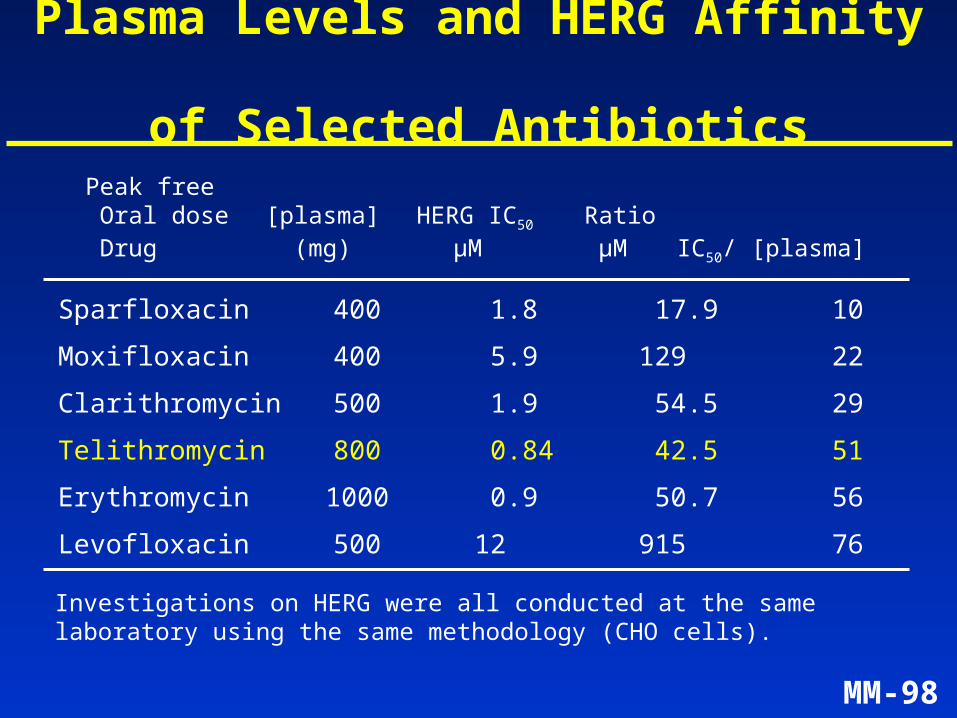
Plasma Levels and HERG Affinity of Selected Antibiotics
Peak free Oral dose [plasma] HERG IC50 Ratio
Drug (mg) µM µM IC50/ [plasma]
Investigations on HERG were all conducted at the same laboratory using the same methodology (CHO cells).
Sparfloxacin 400 1.8 17.9 10
Moxifloxacin 400 5.9 129 22
Clarithromycin 500 1.9 54.5 29
Telithromycin 800 0.84 42.5 51
Erythromycin 1000 0.9 50.7 56
Levofloxacin 500 12 915 76
MM-99
ECG Phase III Analysis
• ECGs performed pre- and on-therapy (Day 3 to 5) and read by a single central reader in 10 Phase III studies (N=1872 patients)
• 625 patients at risk for QT prolongation (33.4%) included in Phase III program
• 1512 patients with a PK sample drawn within one hour of ECG
• QT measured as mean of longest and shortest QT intervals, corrected for heart rate by Bazett Formula (QTc)
MM-100
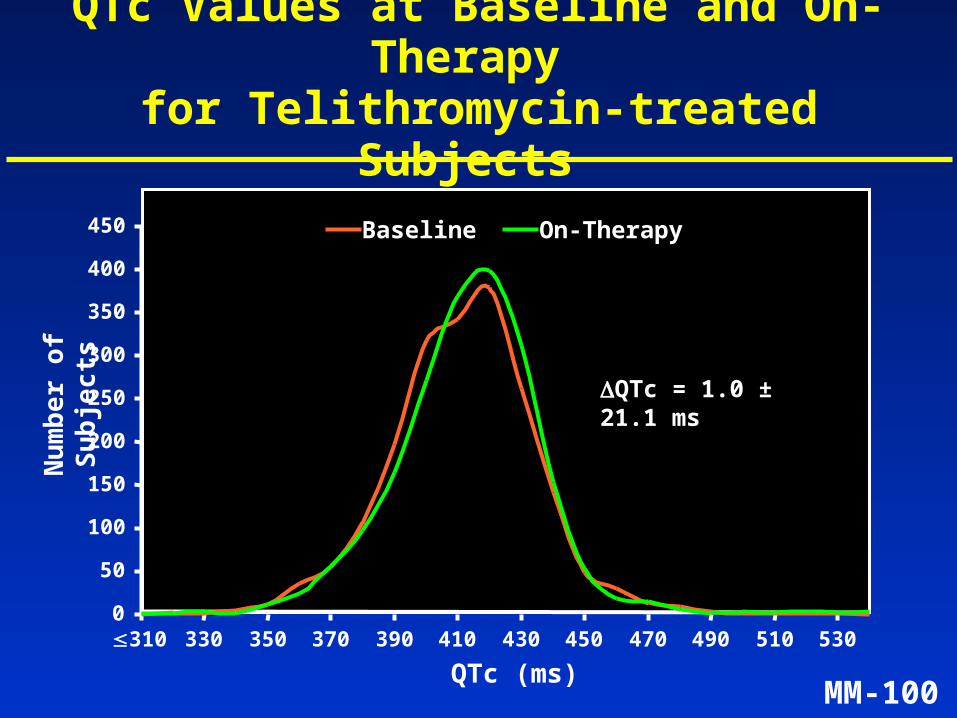
QTc Values at Baseline and On-Therapy for Telithromycin-treated Subjects
Baseline On-Therapy
Nu
mb
er
of
Su
bje
cts
QTc = 1.0 ± 21.1 ms
0
50
100
150
200
250
300
350
400
450
310 330 350 370 390 410 430 450 470 490 510 530
QTc (ms)
MM-101
QTc QT dispersionTreatment N (ms) (ms)
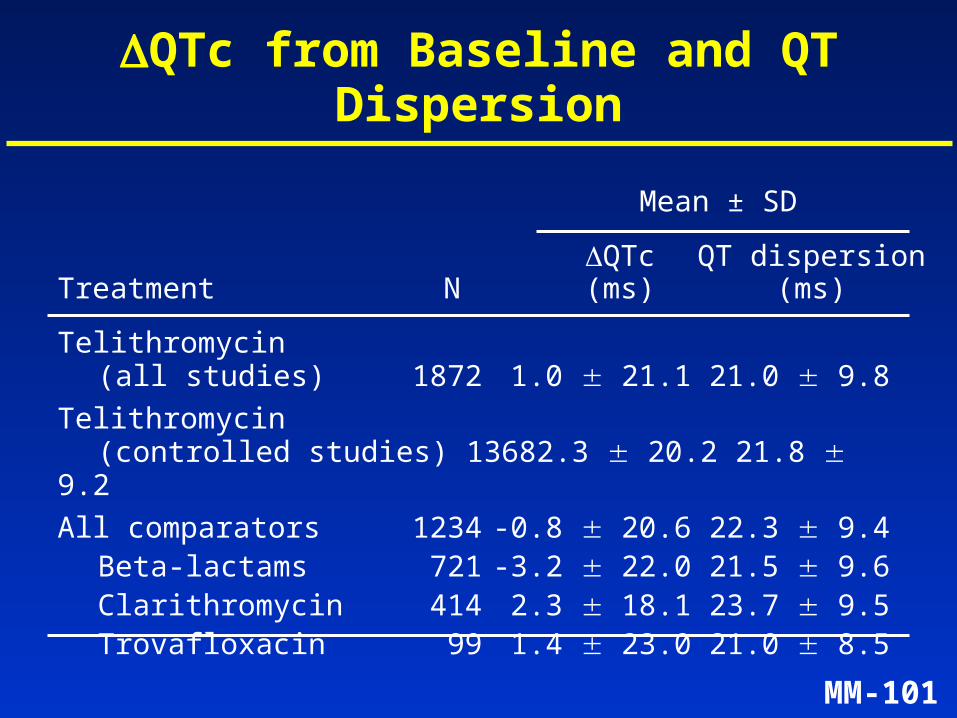
QTc from Baseline and QT Dispersion
Telithromycin (all studies) 1872 1.0 21.1 21.0 9.8
Telithromycin (controlled studies) 1368 2.3 20.2 21.8 9.2
All comparators 1234 -0.8 20.6 22.3 9.4Beta-lactams 721 -3.2 22.0 21.5 9.6Clarithromycin 414 2.3 18.1 23.7 9.5Trovafloxacin 99 1.4 23.0 21.0 8.5
Mean ± SD
MM-102
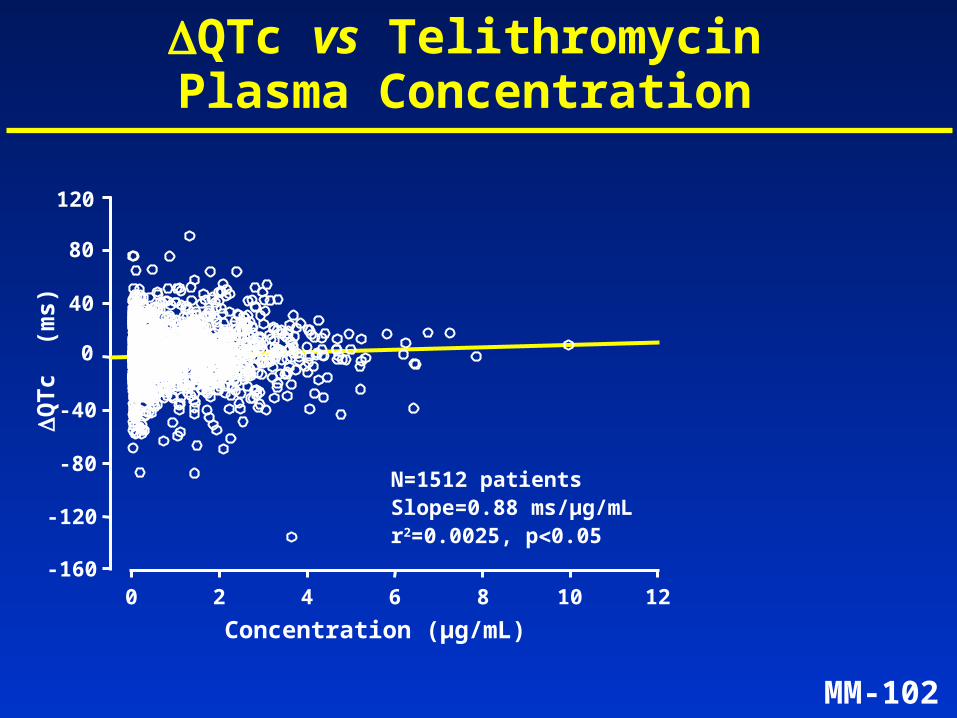
QTc vs Telithromycin Plasma Concentration
Concentration (µg/mL)
QT
c (
ms)
0 2 4 6 8 10 12-160
-120
-80
-40
0
40
80
120
N=1512 patientsSlope=0.88 ms/µg/mLr2=0.0025, p0.05
MM-103
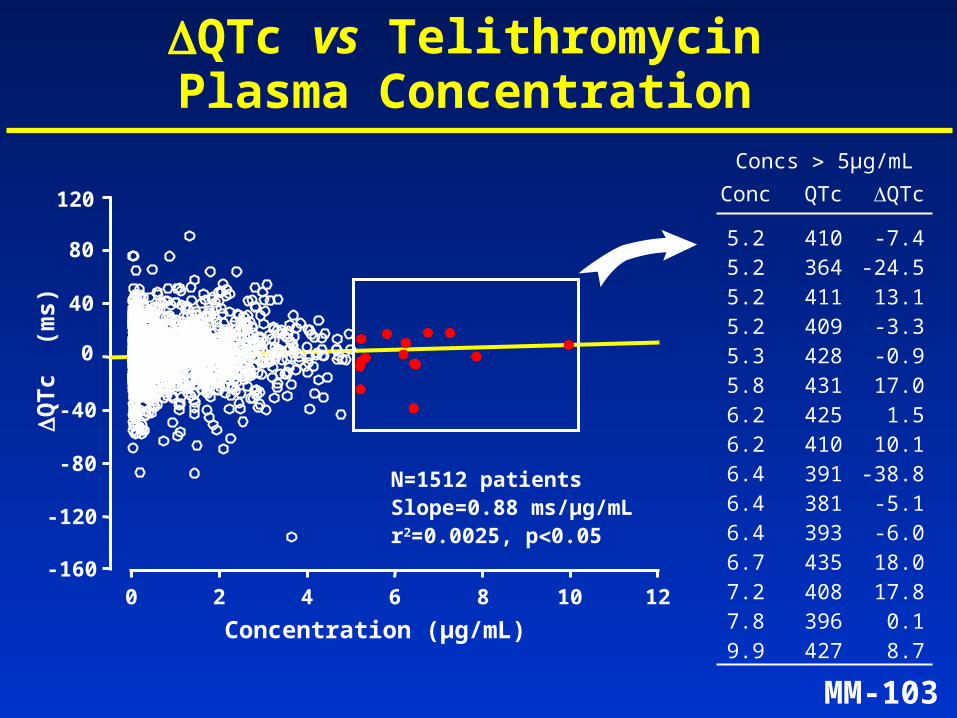
QTc vs Telithromycin Plasma Concentration
Concentration (µg/mL)
QT
c (
ms)
0 2 4 6 8 10 12-160
-120
-80
-40
0
40
80
120
Concs 5µg/mL
Conc QTc QTc
5.2 410 -7.45.2 364 -24.55.2 411 13.15.2 409 -3.35.3 428 -0.95.8 431 17.06.2 425 1.56.2 410 10.16.4 391 -38.86.4 381 -5.16.4 393 -6.06.7 435 18.07.2 408 17.87.8 396 0.19.9 427 8.7
N=1512 patientsSlope=0.88 ms/µg/mLr2=0.0025, p0.05
MM-104
Telithromycin Clarithromycin
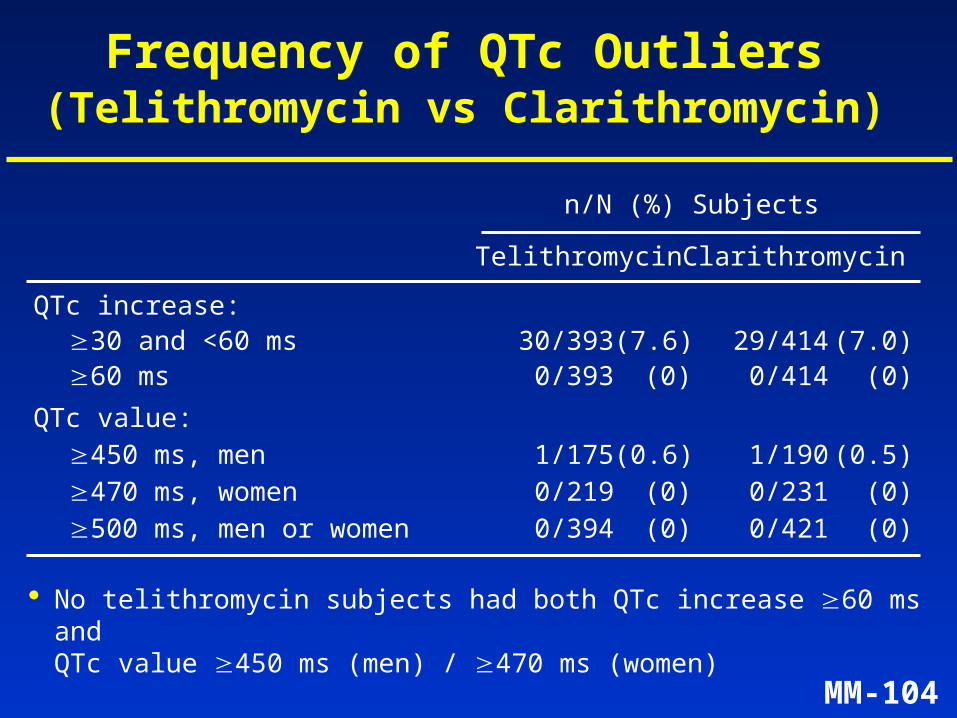
Frequency of QTc Outliers (Telithromycin vs Clarithromycin)
n/N (%) Subjects
No telithromycin subjects had both QTc increase 60 ms and QTc value 450 ms (men) / 470 ms (women)
QTc increase:30 and <60 ms 30/393 (7.6) 29/414 (7.0)60 ms 0/393 (0) 0/414 (0)
QTc value:450 ms, men 1/175 (0.6) 1/190 (0.5)470 ms, women 0/219 (0) 0/231 (0)500 ms, men or women 0/394 (0) 0/421 (0)
MM-105
Telithromycin Non-macrolidesa
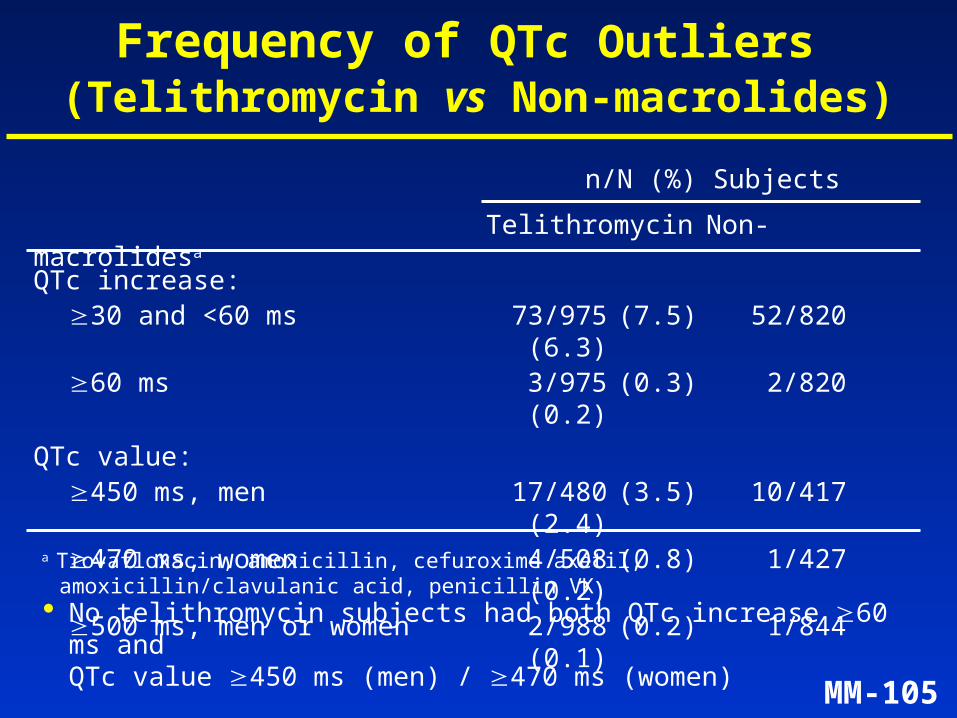
Frequency of QTc Outliers (Telithromycin vs Non-macrolides)
a Trovafloxacin, amoxicillin, cefuroxime axetil, amoxicillin/clavulanic acid, penicillin VK
n/N (%) Subjects
No telithromycin subjects had both QTc increase 60 ms and QTc value 450 ms (men) / 470 ms (women)
QTc increase:30 and <60 ms 73/975 (7.5) 52/820
(6.3)60 ms 3/975 (0.3) 2/820
(0.2)
QTc value:450 ms, men 17/480 (3.5) 10/417
(2.4)470 ms, women 4/508 (0.8) 1/427
(0.2)500 ms, men or women 2/988 (0.2) 1/844
(0.1)
MM-106
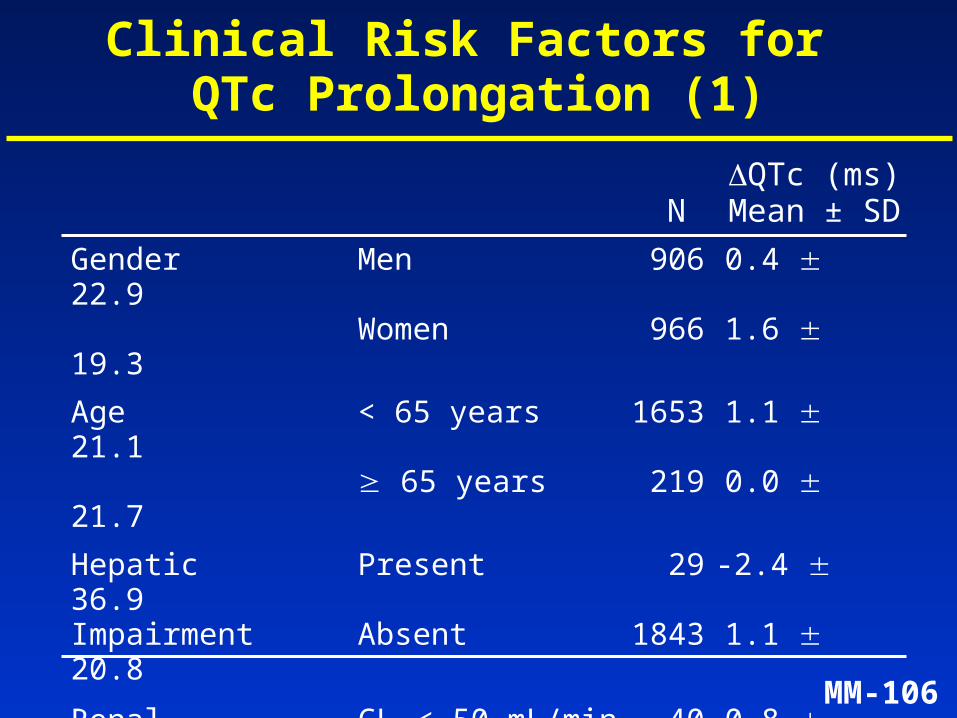
Gender Men 906 0.4 22.9Women 966 1.6 19.3
Age < 65 years 1653 1.1 21.1 65 years 219 0.0 21.7
Hepatic Present 29 -2.4 36.9Impairment Absent 1843 1.1 20.8
Renal CLCR< 50 mL/min 40 0.8 20.6Impairment CLCR 50 mL/min 1832 1.0 21.2
Concomitant Taking 154 3.2 19.7CYP3A4 inhibitors Not taking 1718 0.8 21.3
Clinical Risk Factors for QTc Prolongation (1)
QTc (ms) N Mean ± SD
MM-107
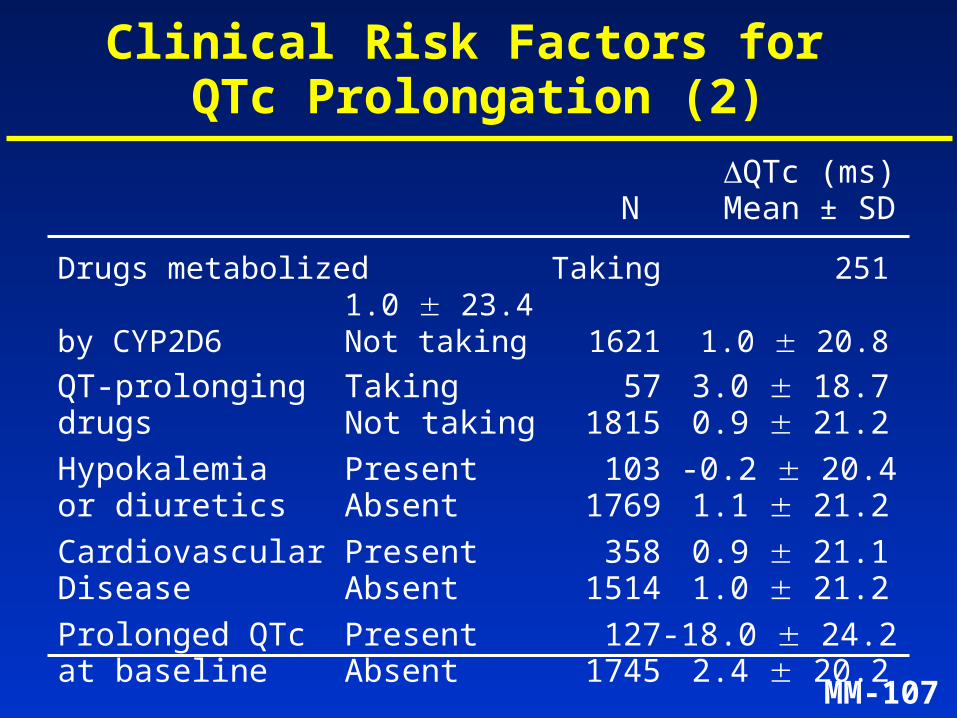
Drugs metabolized Taking 251 1.0 23.4by CYP2D6 Not taking 1621 1.0 20.8
QT-prolonging Taking 57 3.0 18.7drugs Not taking 1815 0.9 21.2
Hypokalemia Present 103 -0.2 20.4or diuretics Absent 1769 1.1 21.2
Cardiovascular Present 358 0.9 21.1Disease Absent 1514 1.0 21.2
Prolonged QTc Present 127 -18.0 24.2at baseline Absent 1745 2.4 20.2
QTc (ms) N Mean ± SD
Clinical Risk Factors for QTc Prolongation (2)
MM-108
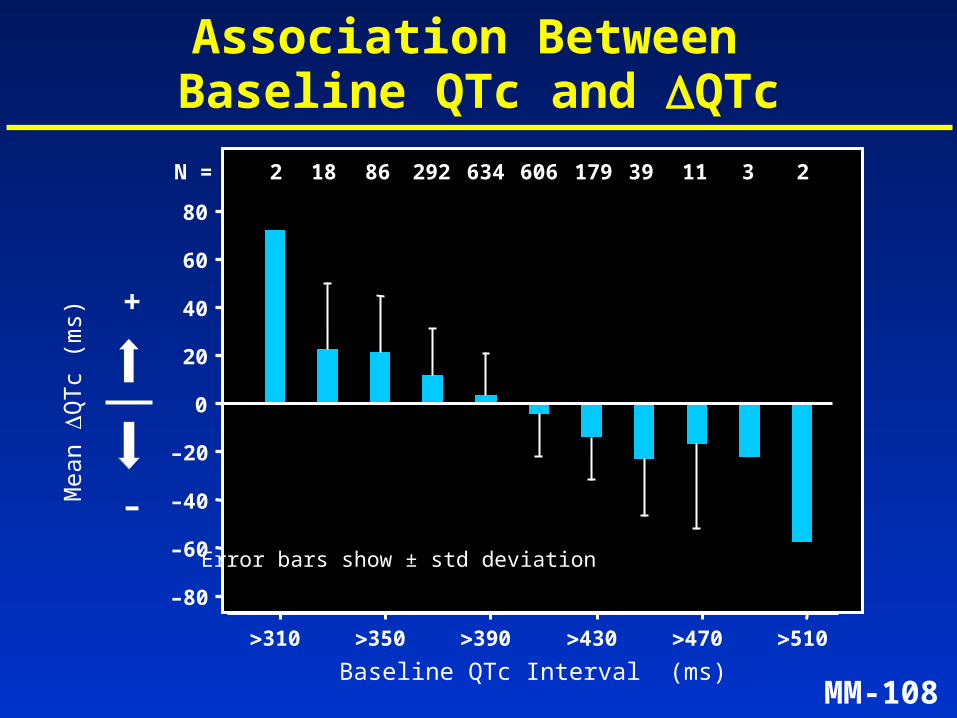
Association Between Baseline QTc and QTc
Baseline QTc Interval (ms)
Mea
n Q
Tc
(ms)
–60
–40
–20
0
20
40
60
310 350 390 430 470 510
+
–
Error bars show ± std deviation
N = 2 18 86 292 634 606 179 39 11 3 2
–80
80
MM-109
Telithromycin Comparators
Adverse Event (N = 2045) (N = 1672)
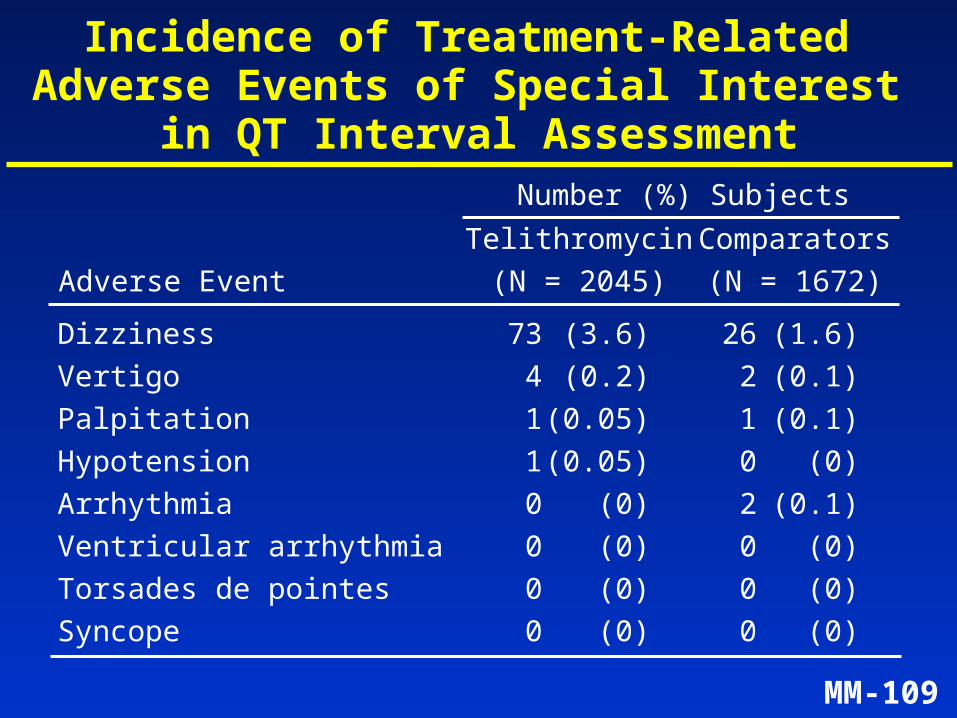
Incidence of Treatment-Related Adverse Events of Special Interest
in QT Interval AssessmentNumber (%) Subjects
Dizziness 73 (3.6) 26 (1.6)
Vertigo 4 (0.2) 2 (0.1)
Palpitation 1 (0.05) 1 (0.1)
Hypotension 1 (0.05) 0 (0)
Arrhythmia 0 (0) 2 (0.1)
Ventricular arrhythmia 0 (0) 0 (0)
Torsades de pointes 0 (0) 0 (0)
Syncope 0 (0) 0 (0)
MM-110
Further Characterization of Telithromycin Effect on
Cardiac Repolarization
• Evaluation of concentration vs QT at up to 4 times the therapeutic dose
• Evaluation of heart rate correction formulas for QT
MM-111
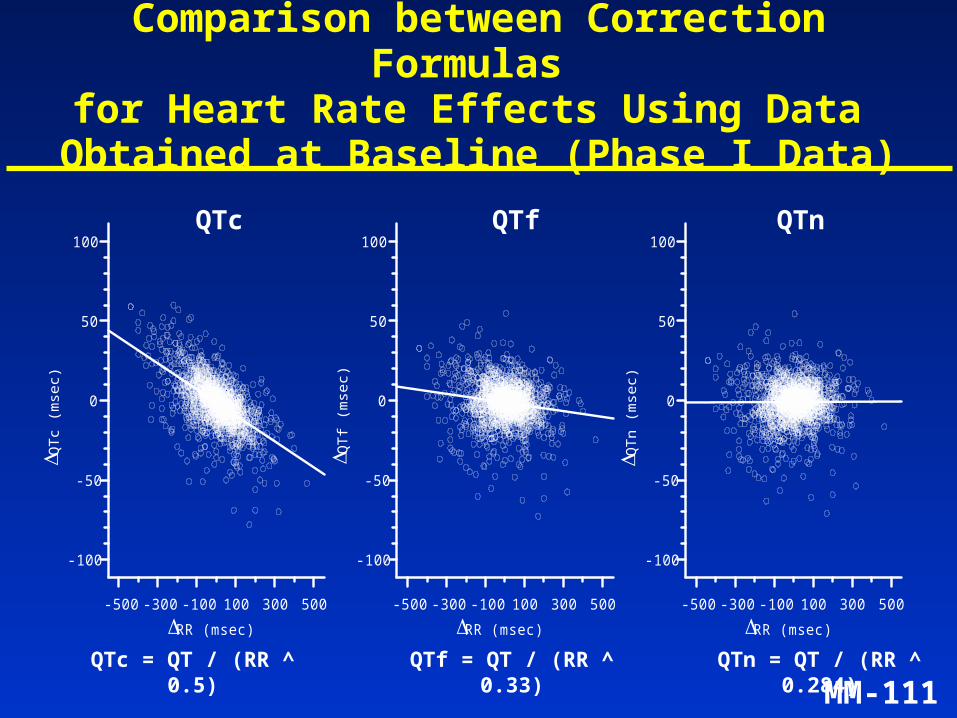
Comparison between Correction Formulas for Heart Rate Effects Using Data
Obtained at Baseline (Phase I Data)
QTc QTf QTn
QTc = QT / (RR ^ 0.5) QTf = QT / (RR ^ 0.33) QTn = QT / (RR ^ 0.284)
-500 -300 -100 100 300 500RR (msec)
-100
-50
0
50
100
QTc
(mse
c )
corrected by Bazett's formula
-500 -300 -100 100 300 500RR (msec)
-100
-50
0
50
100
QTf
(mse
c )
corrected by Fridericia's formula
-500 -300 -100 100 300 500RR (msec)
-100
-50
0
50
100
QTn
(mse
c)
corrected by the New formula
MM-112
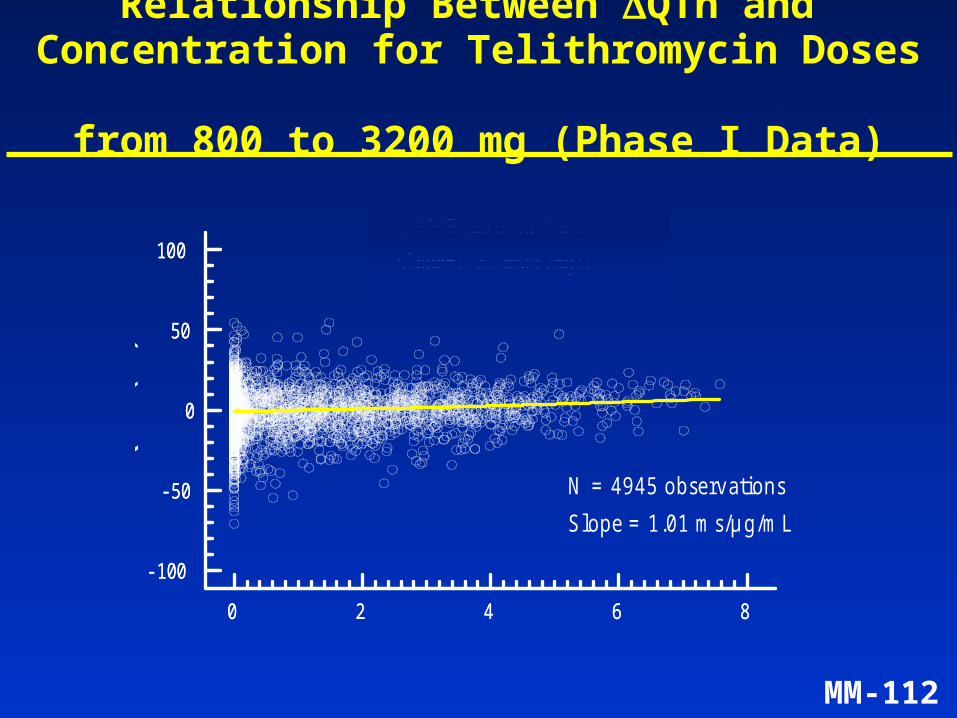
Relationship Between QTn and Concentration for Telithromycin Doses
from 800 to 3200 mg (Phase I Data)
0 2 4 6 8Concentration (mg/L)
-100
-50
0
50
100
QTn
(m
sec)
Slope=1.01 msec/mg/Ln=4945 observations
0 2 4 6 8
-100
-50
0
50
100
N = 4 9 4 5 o b se rv a tio n s
S lo p e = 1 .0 1 m s /µ g /m L
C o n c e n tr a tio n (µ g /m L )
QT
n (
ms)
MM-113
Drug Interactions of Special Interest
• Ketoconazole (potent CYP3A4 inhibitor)
• Cisapride (exclusively metabolized by CYP3A4)
• Sotalol (class III antiarrhythmic drug)
MM-114
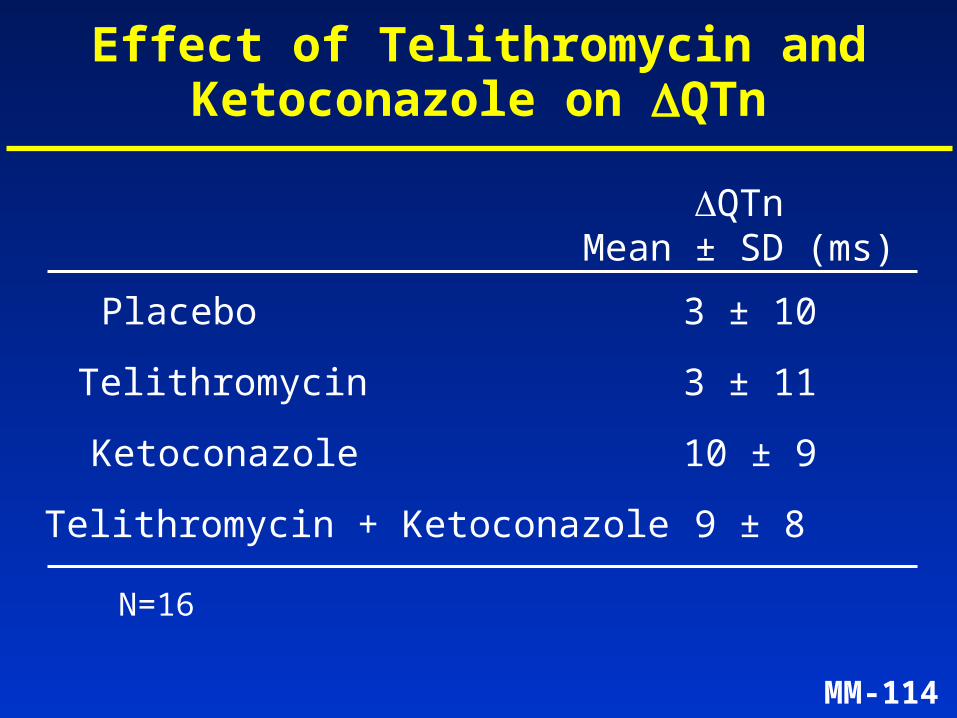
Effect of Telithromycin and Ketoconazole on QTn
QTn Mean ± SD (ms)
Telithromycin 3 ± 11
Ketoconazole 10 ± 9
Telithromycin + Ketoconazole 9 ± 8
Placebo 3 ± 10
N=16
MM-115
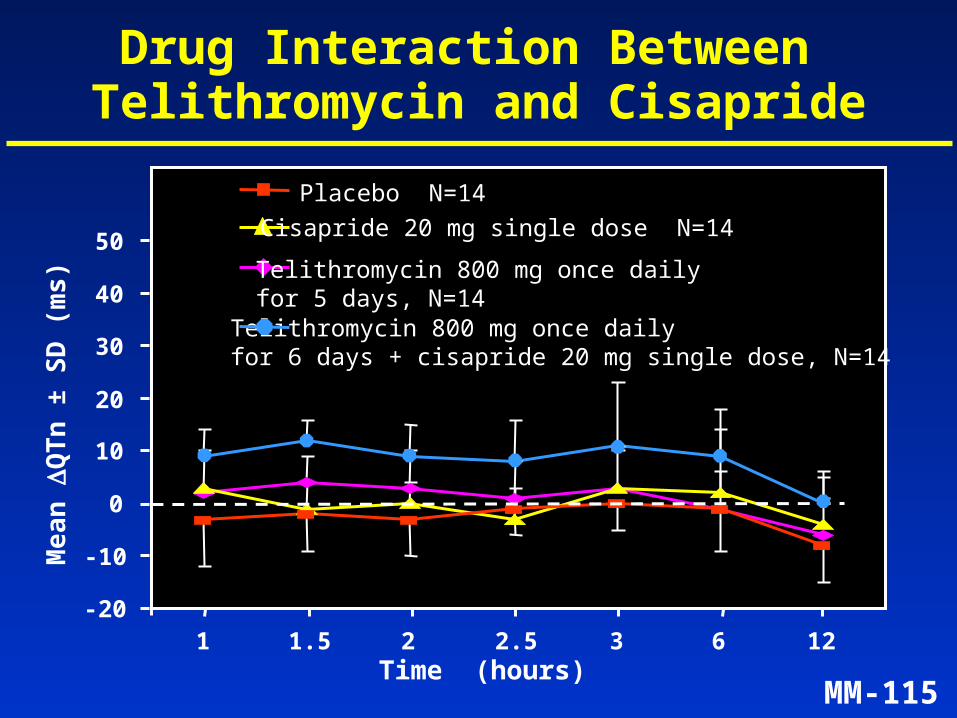
Drug Interaction Between Telithromycin and CisaprideM
ea
n
QT
n ±
SD
(m
s)
-20
-10
0
10
20
30
40
50
1 1.5 2 2.5 3 6 12
Telithromycin 800 mg once daily for 6 days + cisapride 20 mg single dose, N=14
Telithromycin 800 mg once daily for 5 days, N=14
Cisapride 20 mg single dose N=14
Placebo N=14
Time (hours)
MM-116
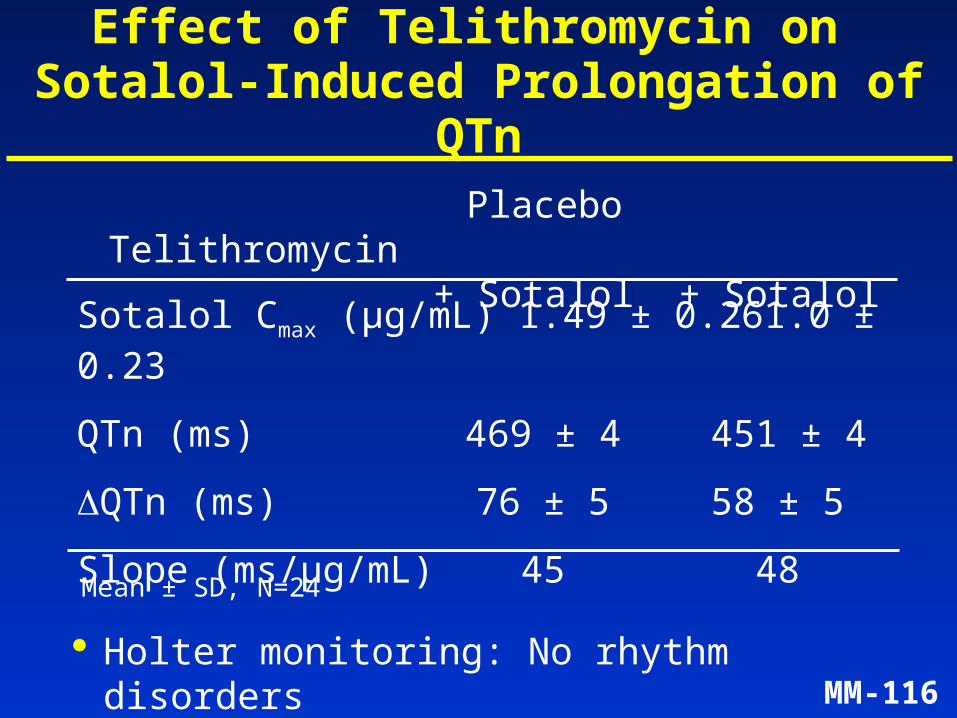
Effect of Telithromycin on Sotalol-Induced Prolongation of QTn
Placebo Telithromycin+ Sotalol + Sotalol
Sotalol Cmax (µg/mL) 1.49 ± 0.26 1.0 ± 0.23
QTn (ms) 469 ± 4 451 ± 4
QTn (ms) 76 ± 5 58 ± 5
Slope (ms/µg/mL) 45 48
Mean ± SD, N=24
Holter monitoring: No rhythm disorders
MM-117
Study in Subjects with CV Disease: Design/Population
• Single-dose, double-blind, randomized, placebo-controlled, 4-way crossover study
• Telithromycin 800 and 1600 mg, clarithromycin 500 mg x2, placebo
• 24 high-risk subjects with underlying cardiovascular disease
• ECG and 24-hour Holter recording before and after dosing

MM-118
Subjects with CV Disease: Mean Changes in QTn and QTc
TEL TEL CLA 800 mg 1600 mg 500 mg
Cmax (µg/mL) 1.8 ± 0.9 3.1 ± 1.0 2.5 ± 1.2
QTn (ms) -0.8 ± 10 1.0 ± 9.0 2.0 ± 9.0
QTc (ms) 3.0 ± 13 6.5 ± 13.5 3.2 ± 15• Holter: No arrhythmias recorded
Mean ± SD
Data corrected for placebo
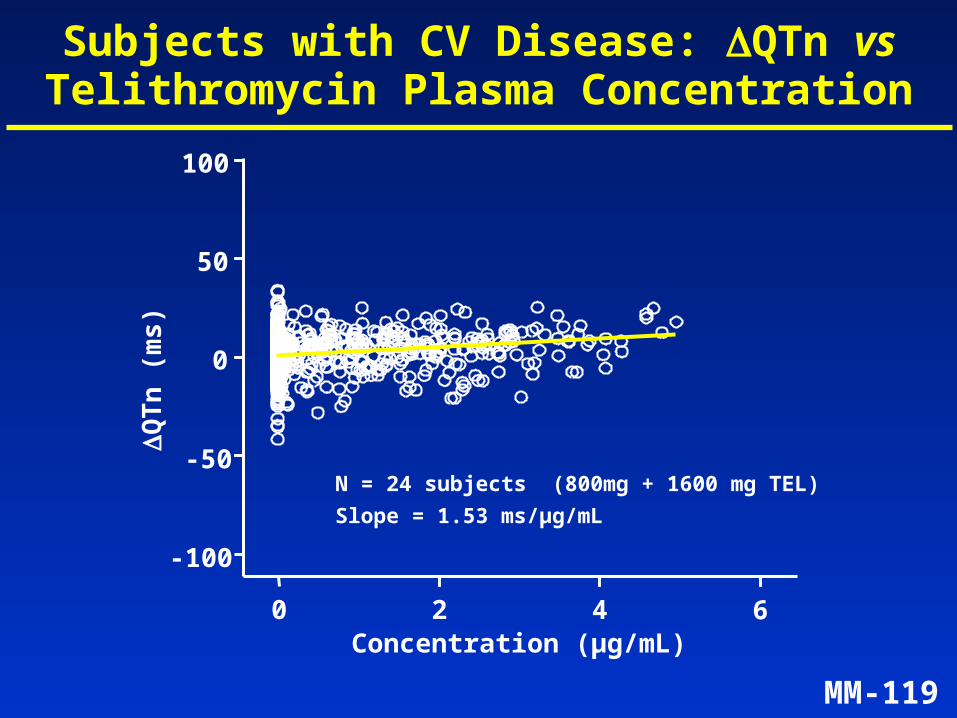
MM-119
Subjects with CV Disease: QTn vs Telithromycin Plasma Concentration
Concentration (µg/mL)
QT
n (
ms
)
0 2 4 6
-100
-50
0
50
100
N = 24 subjects (800mg + 1600 mg TEL)
Slope = 1.53 ms/µg/mL
MM-120
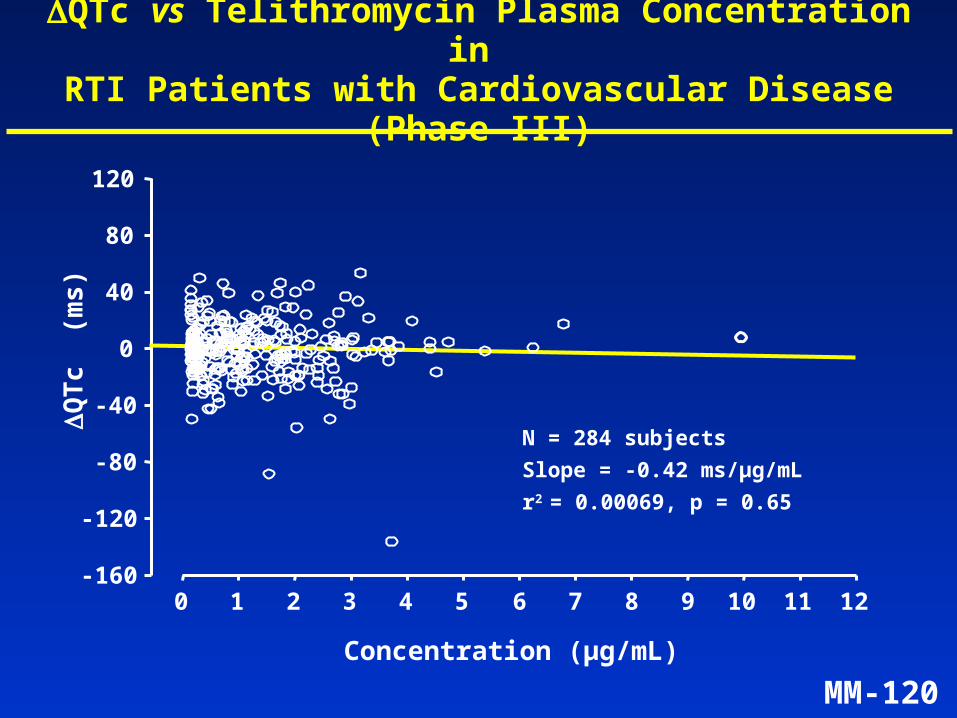
QTc vs Telithromycin Plasma Concentration in RTI Patients with Cardiovascular Disease (Phase III)
QT
c (
ms
)
0 1 2 3 4 5 6 7 8 9 10 11 12-160
-120
-80
-40
0
40
80
120
N = 284 subjects
Slope = -0.42 ms/µg/mL
r2 = 0.00069, p = 0.65
Concentration (µg/mL)
MM-121
Summary of ECG Analysis (1)
• Telithromycin has a weak effect on IKr channels
• In patients with respiratory infections, the mean change in QTc observed was small (~1 ms)
• Shallow relationship between QTc and plasma telithromycin concentrations over a wide range of concentrations
• No difference in the frequency of QTc outliers between telithromycin and macrolide and non-macrolide antibiotics
MM-122
Summary of ECG Analysis (2)
• Analysis of at-risk subpopulations did not reveal a propensity for enhanced effect on cardiac repolarization
• No increase in the incidence of cardiovascular adverse events, including no torsades de pointes, no ventricular tachycardias, and no syncope associated with QT prolongation
• Limited risk due to brief duration of treatment and multiple pathways of elimination that limit exposure
MM-123
Telithromycin – Presentation Agenda
Introduction Mindell Seidlin, MD
Microbiology André Bryskier, MD
Human Pharmacology Vijay Bhargava, PhD
Clinical Efficacy and Safety Bruno Leroy, MD
ECG Analysis Claude Benedict, MD
Conclusions Mindell Seidlin, MDVP, Clinical Development, Anti-Infectives, Aventis
MM-124
Medical Need for New Antibiotics
• Resistance in respiratory tract pathogens is increasing– S. pneumoniae: High level penicillin or macrolide resistance in >15%
strains– threat of multi-drug resistance– beta-lactamase + strains of M. catarrhalis and
H. influenzae– increasing importance of atypical pathogens
• Respiratory infections are associated with significant morbidity and mortality– more patients with underlying illness are being
treated in the community
MM-125
Microbiological and PK Features
• Telithromycin, the first ketolide, has:– two sites of interaction with 50S ribosomal
subunit; also interferes with assembly of both ribosomal subunits
– potent in vitro antipneumococcal activity
– activity against erythromycin-resistant strains
– activity against common, intracellular, and atypical respiratory pathogens
• Well-characterized pharmacokinetic profile, with therapeutic plasma and sustained tissue levels
MM-126
Summary of Efficacy in Respiratory Tract Infections
• Consistently effective in all analyses in 13 Phase III trials
• CAP:– elderly: cure rate 90% – pneumococcal bacteremia: cure rate 91% – atypical infections (including Legionella: cure rate 100%)
• AECB, Acute Sinusitis, Tonsillitis/Pharyngitis:– 5-day once-daily telithromycin treatment was equivalent to
10-day, 2-3 doses per day comparator treatment
• Efficacy in resistant S. pneumoniae infections in CAP and Acute Sinusitis
MM-127
Summary of Safety
• Safety studied in a broad spectrum of patients:
– incidence of GI events comparable to other widely used antibiotics
– hepatic events and transaminase elevation similar to comparators
– discontinuations and serious events equivalent to comparators
– small effect on QTc (~1 ms mean increase) in patients with RTIs
MM-128
The Advantages that Telithromycin Brings
• Highly effective in pneumococcal infections
• No cross-resistance in pneumococci to macrolides, beta-lactams, quinolones
• Effective against common, atypical, and intracellular RTI pathogens
• 5-day once-daily regimen for common infections
• Expands the options for outpatient management of RTIs