modified directly observed therapy for first virologic failure: actg a5234 pi dr a chisada...
TRANSCRIPT

Modified Directly Observed Therapy for First Virologic
Failure: ACTG A5234
PI Dr A Chisada
Presenter: Dr W Samaneka
MBChB, MSc
UZ-UCSF ARD
17 April 2015

• Sustained and consistent adherence is a key factor for durable ART success
• 2nd line therapy is typically more complex and expensive than 1st line
• Conventional DOT is logistically challenging• Enhanced partner support may benefit
patients with prior treatment failure.
Background
Main Objective
To test whether a partner-based modified DOT (mDOT) intervention would result in higher rates of virologic suppression compared with standard of care after first-line treatment failure

Methods
• Study duration: Apr 2009 – Sep 2011• Confirmed virologic failure on 1st line
• Identifiable mDOT partner (family, friend, etc.)• 1:1 allocation to mDOT and standard of care
• 2nd line: lopinavir/r (400 mg/100 mg) BID +
TDF/FTC (300 mg/200 mg) qD
Brazil, Botswana, Haiti, Peru, SA, Uganda, Zambia, Zimbabwe

End Points
Primary efficacy endpoint• Confirmed Virologic Failure HIV RNA>400
cpm by week 48 Secondary endpoints• Confirmed virologic failure HIV RNA>400
cpm by week 24• Adherence measured using electronic
monitors[MEMS] summarized quarterly as % of doses taken

mDOT Intervention Design• Single training session of mDOT partner (1.5
hrs) Drug regimen
Adherence &handling missed doses Side effects
Examples of +ve and –ve social support Documentation of observed doses How and when to contact site for help
Provision of airtime (buddie)
Duration of active phase: 24 weeks (total follow up 52 wks)

Participant Flow Diagram

RESULTSBaseline Characteristics
Characteristic mDOT SOC
n =129 N=128
Median age (IQR) 38 y (34,44) 37 y (33, 45)
Female sex 62 (48%) 65 (51%)
Black race 101 (78%) 103 (80%)
Hispanic ethnicity 27 (21%) 25 (20%)
Prior rx duration 153 wks 144 wks
(IQR) (82, 230) (89, 245)
Entry CD4 (median) 164 c/mm3 201 c/mm3
(IQR) (91, 250) (97, 292)
Nadir CD4 (median) 122 c/mm3 109 c/mm3
(IQR) (37, 187) (45, 202)
HIV RNA (median) 4.2 log cpm 4.2 log cpm
(IQR) (3.8, 4.9) (3.8, 4.9)
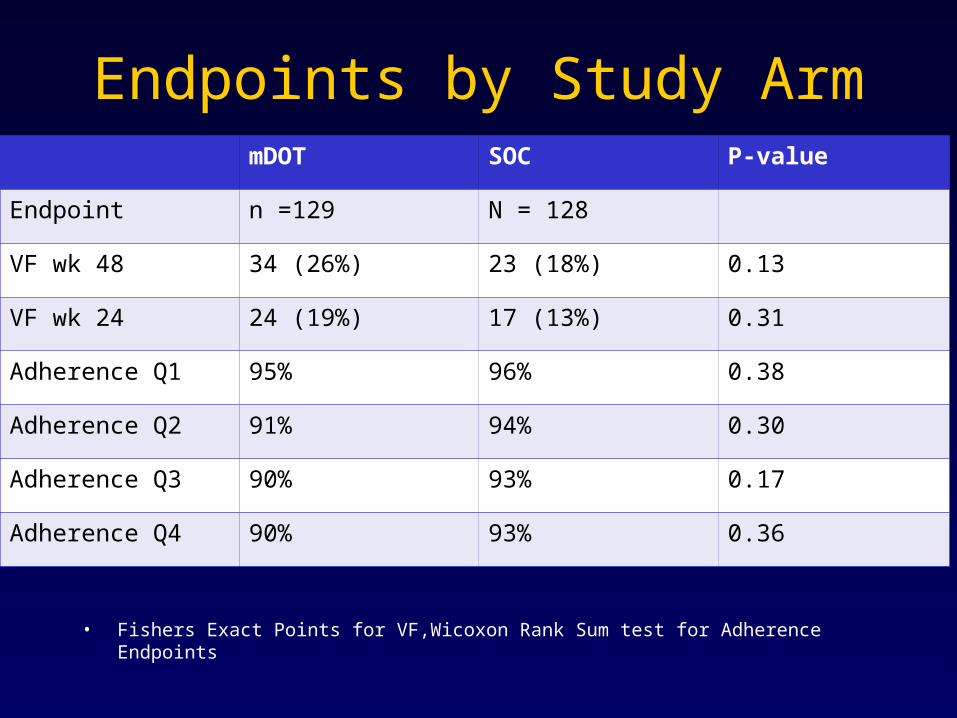
Endpoints by Study Arm
• Fishers Exact Points for VF,Wicoxon Rank Sum test for Adherence Endpoints
mDOT SOC P-value
Endpoint n =129 N = 128
VF wk 48 34 (26%) 23 (18%) 0.13
VF wk 24 24 (19%) 17 (13%) 0.31
Adherence Q1 95% 96% 0.38
Adherence Q2 91% 94% 0.30
Adherence Q3 90% 93% 0.17
Adherence Q4 90% 93% 0.36

Virologic suppression ≤ 400
• At all time points after week 12 undetectable VL was higher in SOC, however not significant
• Week 48, 75% (CI 67-83) in mDOT and 82% in SOC (CI 74-89) had VL ≤ 400, (p=0.37)
• No sig diff between groups at week 24; p=0.18

Virologic Suppression (HIV-RNA ≤ 400 cpm)over time

Conclusion
• mDOT had no significant impact on virologic failure
High rate of suppression in both arms• mDOT had no significant impact on
adherence High rate of adherence in both arms• Other interventions still need to be
tested in this setting

• Although mDOT intervention not successful findings are encouraging > high rates of virologic success on second line therapy in RLS
Acknowledgements
• Sponsors – NIAID
- Abbott Laboratories
- Gilead Sciences• Study participants + partners• CAB• CRS Leader- Prof JG Hakim• ACTG site staff• UZ-UCSF
