monitoraggio della funzione piastrinica durante … · monitoraggio della funzione piastrinica...
TRANSCRIPT

MONITORAGGIO DELLA FUNZIONE PIASTRINICA DURANTE TERAPIA CON
TIENOPIRIDINE
Rossella Marcucci30 novembre 2013
CardioLucca 2013

CLOPIDOGREL:
A MODEL FOR PERSONALIZED MEDICINE
High on-treatment platelet reactivity

ACUTE CORONARY SYNDROME PATIENTSUNDERGOING PCI WITH STENT IMPLANTATION
ISCHAEMIC
EVENTSBLEEDING
DUAL ANTIPLATELET THERAPY
ACUTE PHASE

Buonamici P, JACC 2007 n=804
10 micromol ADP LTA
RECLOSE TRIAL

1.00
0.98
0.96
0.94
0.92
0 2 4 6 8 10 12
Time (months)
CV death-free Survival
RPR (PRU ≥240)
No RPR (PRU <240)
log-rank test p=0.02
Cardiovascular death and nonfatal myocardial infarction in acutecoronary syndrome patients receiving coronary stenting are
predicted by residual platelet reactivity to ADP detected by a point-of-care assay: a 12 month follow-up
Marcucci R et al, Circulation 2009
n= 683 ACS patients
VerifyNow P2Y12
HR=2.55 (95%CI 1.08-6.07), p=0.034

Iperattività piastrinica “misurata” con i comuni test di
aggregazione piastrinica e prognosi: metanalisi

Impact of Platelet Reactivity on Clinical Outcomes After Percutaneous
Coronary Intervention Somjot S. Brar et Al. JACC 2011

JAMA 2011;306(11):1215-1223
Prospective observational single center cohort study

JAMA 2011;306(11):1215-1223
STUDY FLOW
n= 1789
n= 1525
n= 24714%

Kaplan Meier survival curves for primary end point events
JAMA 2011;306(11):1215-1223
Estimate risk
27.5% (18.3-36.7) in HRPR group
14.5% (12.1-16.9) in LRPR group
2 YRS FOLLOW-UP


CLOPIDOGREL:
A MODEL FOR PERSONALIZED MEDICINE
- Genetic Factors

CYP1A2 (35.8%)CYP2B6 (19.4%)CYP2C19 (44.9%)
CYP2B6 (32.9%) CYP2C9 (6.8%)CYP2C19 (20.6%)CYP3A4 (39.8%)
Kazui M et al, Drug Metab Dispos 2009
Simon T et al, N Engl J Med 2009
Roles in clopidogrel activity of proteins with known genetic
polymorphisms
C3435TIle1145IleABCB1
A672TQ192RPON1
T196CLeu59Pro
ITGB3
T744CH1/H2P2Y12

CYP2C19*2 genotypes
*1/*1 *1/*2 *2/*2 p (overall)
*1/*2+*2/*2p (vs. *1/*1)
SubjectsN (%)
974 (68.6%)
405 (28.6%)
40(2.8%)
445(31.4%)
Aggregation accordingto stimulus
%
ADP(2µM)
26 (1-100) 32 (1-94)* 41 (5-84)*§ <0.0001 33 (1-94) <0.0001
ADP(10µM) 49 (1-100) 54 (2-100) * 62 (26-100)*# <0.0001 56 (2-100) <0.0001
AA(0.5
mg/mL)11 (1-100) 12 (1-100) 14 (5-85) 0.060 12 (1-100) 0.043
Distribution of maximal platelet aggregation after different stimuli in
the overall study population according to CYP2C19*2 genotypes
Giusti B et al, Pharmacogenetics and Genomics 2007; 17(12):1057-1064
1419 ACS patients on dual antiplatelet therapy undergoing percutaneous
coronary intervention (PCI) and stent implantation
*p<0.0001 vs *1/*1; §p=0.028 vs *1/*2; #p=0.015 vs *1/*2;

Cardiovascular death,MI or ischemic stroke
JAMA 2010

Stent Thrombosis
JAMA 2010


JAMA , 2011
ELEVATE TIMI 56
Conclusion Among patients with stablecardiovascular disease, tripling the maintenance dose of clopidogrel to 225 mg daily in CYP2C19*2 heterozygotes achieved levels of platelet reactivity similar to that seen with the standard 75-mg dose in noncarriers;in contrast, for CYP2C19*2 homozygotes, doses as high as 300mg daily did not result in comparable degrees of platelet inhibition.

CLOPIDOGREL:
A MODEL FOR PERSONALIZED MEDICINE
- Genetic Factors
-Acquired Factors:
clinical characteristics

HIGH ON TREATMENT PLATELET REACTIVITY BY ADP AND INCREASED RISK OF MACE IN GOOD CLOPIDOGREL METABOLIZERS: BEYOND PHARMACOGENETIC APPROACH
n= 892 patients NON carriers of CYP2C19*2 polymorphism12 month follow-up
Marcucci R et al, Platelets 2012

High on-treatmentplatelet reactivity
TRANSIENT
Chronic
Systolic function
Age,sex
Diabetes
PERSISTENT
Acute phase
Reticulated platelets
Platelet turn-over
Erythrocytedeformability ADAMTS-13
activity
Inflammation
ComplianceDrug interactions
CYP2C19polymorphism
DRUG RESISTANCEPERMANENT

4OR 95%CI
Multivariate logistic regression analysis on risk of Multivariate logistic regression analysis on risk of
having RPR *having RPR *
10 2
IPF vs. AA-RPR
H-IPF vs. AA-RPR
IPF vs. ADP-RPR
H-IPF vs. ADP-RPR
1.77 (1.05-2.99)
1.62 (1.05 -2.51)
1.76 (1.07-2.90)
1.74 (1.14-2.64)
p=0.03
p=0.03
p=0.02
p=0.01
*Adjusted for age, gender, family history of CAD, smoking habit, hypertension, diabetes, dyslipidemia, hematocrit,
STEMI/NSTEMI, use of GpIIb/IIIa inhibitors and platelet count
3
Cesari et al, Thromb Haemost 2008
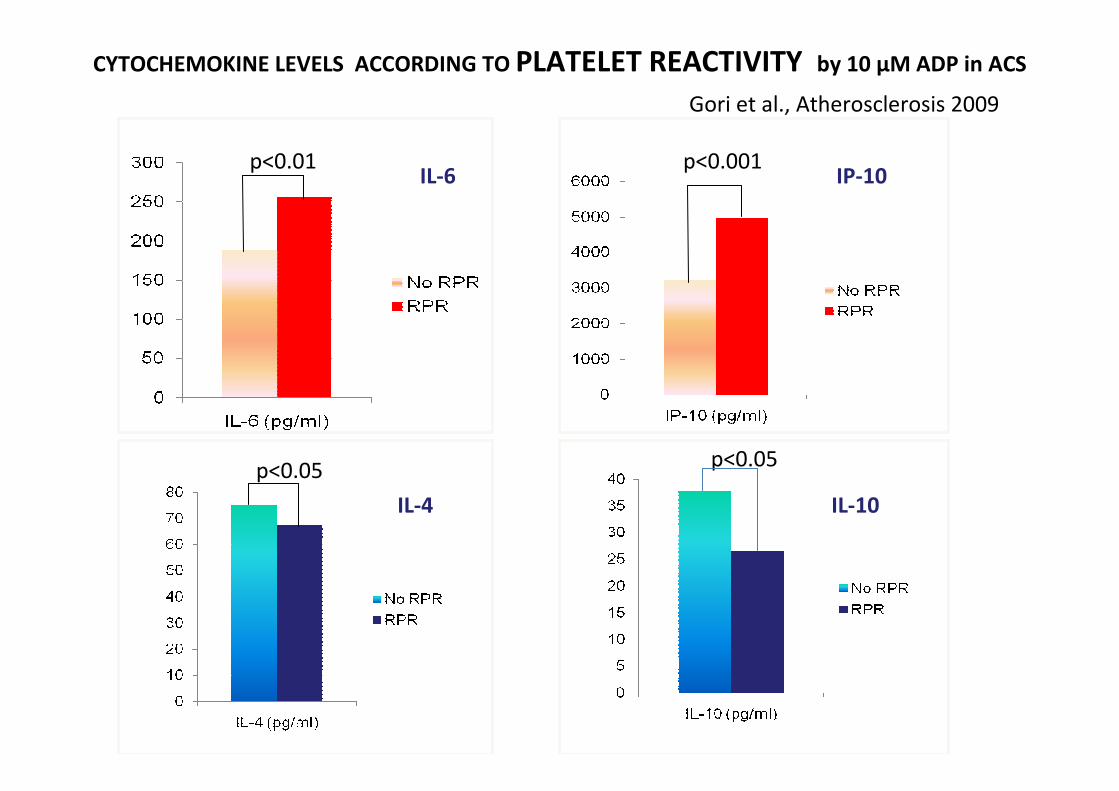
CYTOCHEMOKINE LEVELS ACCORDING TO PLATELET REACTIVITY by 10 µM ADP in ACS
p<0.01 p<0.001IL-6 IP-10
p<0.05p<0.05
IL-10IL-4
Gori et al., Atherosclerosis 2009

High on-thienopyridine platelet reactivity in elderly coronary patients: the
SENIOR-PLATELET study
Silvain L, EHJ 2011
Rate of high platelet reactivity
(PRU . 235) (Figure 2A) and
mean inhibition (%) (Figure 2B)
in patients treated with an MD
of 75 mg of clopidogrel
according to decades of age
identified with the VN-P2Y12
assay. Mean inhibition
corresponds to the ratio PRU
iso-TRAP/PRU ADP-PGE .
Asterisks indicate P , 0.05 with
Kruskall – Wallis test for
multiple comparison.

ACS patients(n=386)
Elective PCI(n=482)
WithRPR (n=99)
WithoutRPR (n=287)
p WithRPR (n=93)
WithoutRPR (n=389)
P
Age 68.3(65.7-70.8) 68.3(66.9-69.8) ns 68.4(66.2-70.6) 67.7(66.6-68.8) ns
Sex (M/F) 69/30 206/81 ns 70/23 294/95 ns
Smoking habit (%) 45.6 48.1 ns 40.5 47.3 ns
Hypertension (%) 63.6 64.7 ns 64.5 70.2 ns
Diabetes (%) 44.3 20.6 .0001 34.2 16.6 .001
Dyslipidemia (%) 25.0 28.5 ns 13.4 22.4 .04
PAD (%) 13.9 7.8 ns 24.6 27.6 ns
AF(%) 15.2 14.8 ns 14.4 15.8 ns
Previous useof clopidogrel (%)
4.4 7.7 ns 28.9 41.8 .02
Ejection Fraction ≤40% (%)
61.2 41.0 .003 38.3 26.0 .04
Leukocytes (x 109/L)
12882(12023-13804)
10000(9550-10471)
.0001 8318(7762-8709)
7244(7079-7413)
.0001
ESR (mm/h)
45.7(39.8-52.5)
29.5(26.9-31.6)
.0001 23.9(20.9-28.2)
18.2(17.0-19.5)
.0001
Clinical and laboratory characteristics according to platelet reactivity by 10 microM ADP-PA
Marcucci R et al, Atherosclerosis 2007

CLOPIDOGREL:
A MODEL FOR PERSONALIZED MEDICINE
- Genetic Factors
-Acquired Factors:
Drug-drug interactions

Hulot et al, JACC 2010
ORs for MACE according to PPI use (n=46,037)
CLOPIDOGREL:
HOW TO OVERCOME HIGH PLATELET REACTIVITY

Iperattività piastrinica e “tailored antiplatelets therapy”
I GRANDI TRIAL
Standard- vs High-Dose Clopidogrel Based on Platelet Function Testing After Percutaneous Coronary Intervention.
Matthew J. Price et Al. JAMA, March 16, 2011

CV Events and Post-PCI PRU In Patients With High and Not High Reactivity Treated With Clopidogrel 75-mg Daily
500
400
300
200
100
0
PRU 12 - 24 hrs post-PCI
High ResidualReactivity
Not HighResidual Reactivity
N=1105 N= 586
ITT population
Red dots: patients with CV death, MI, or ST
230 PRU
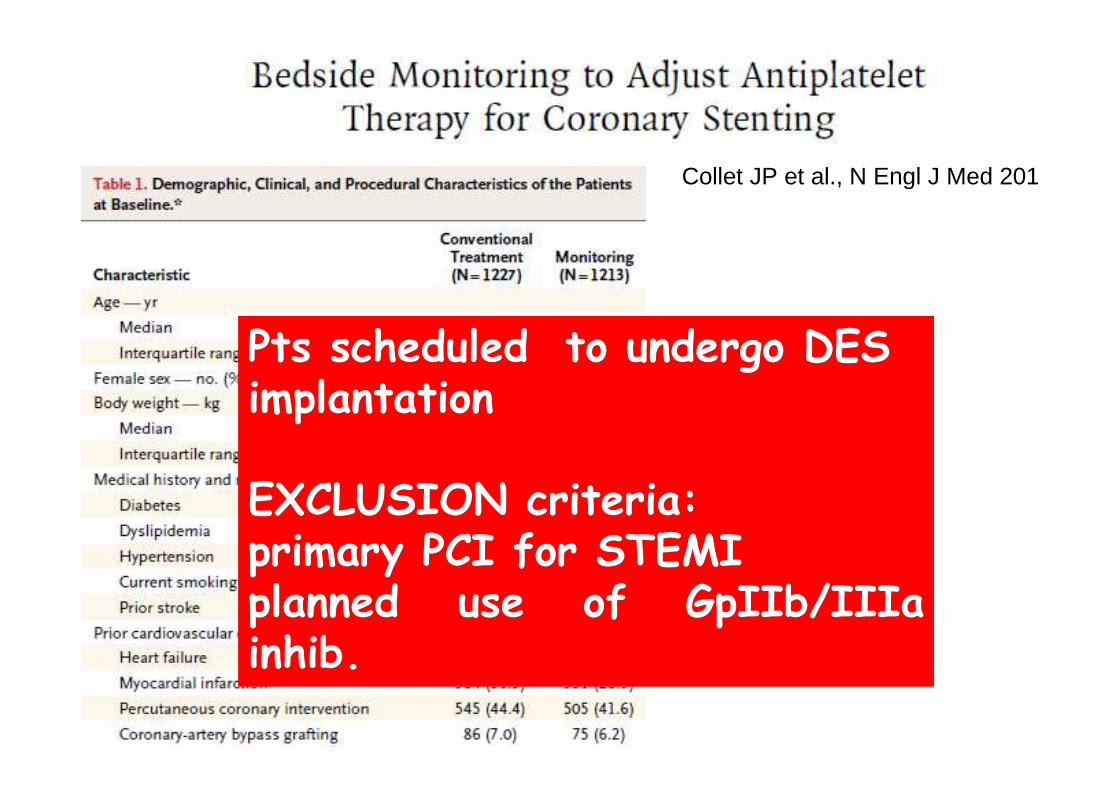
Pts scheduled to undergo DES implantation
EXCLUSION criteria:primary PCI for STEMIplanned use of GpIIb/IIIa inhib.
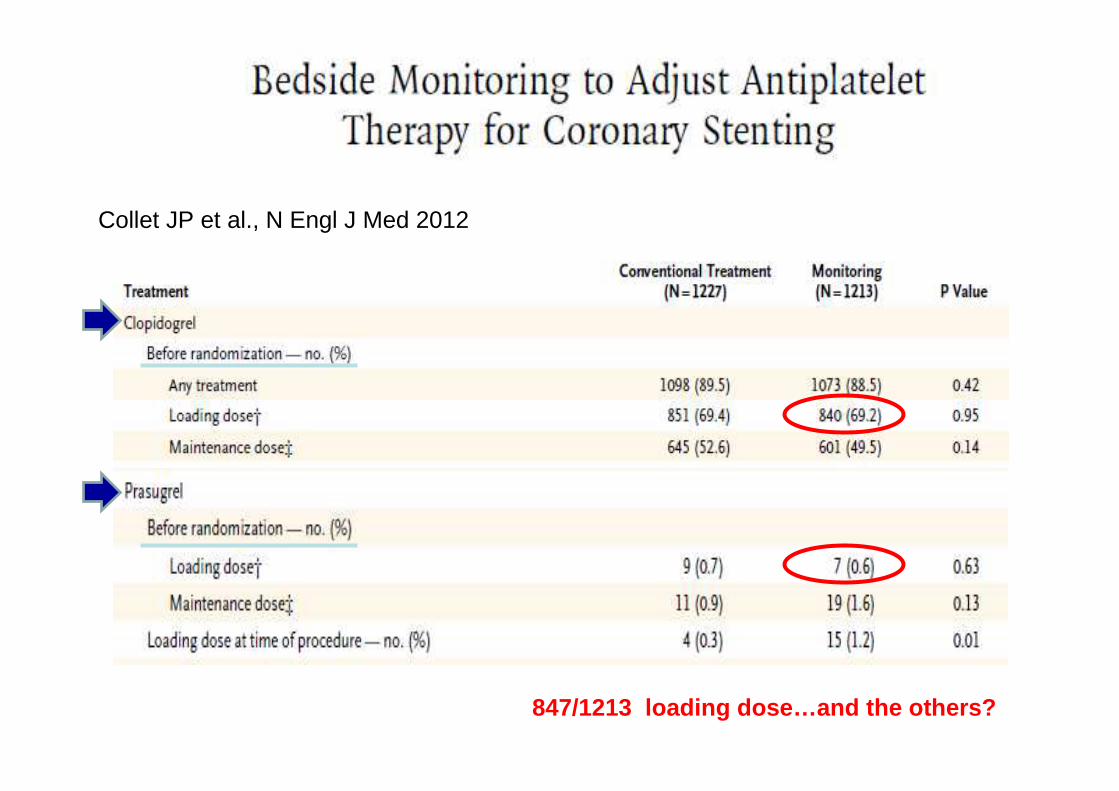
Collet JP et al., N Engl J Med 2012
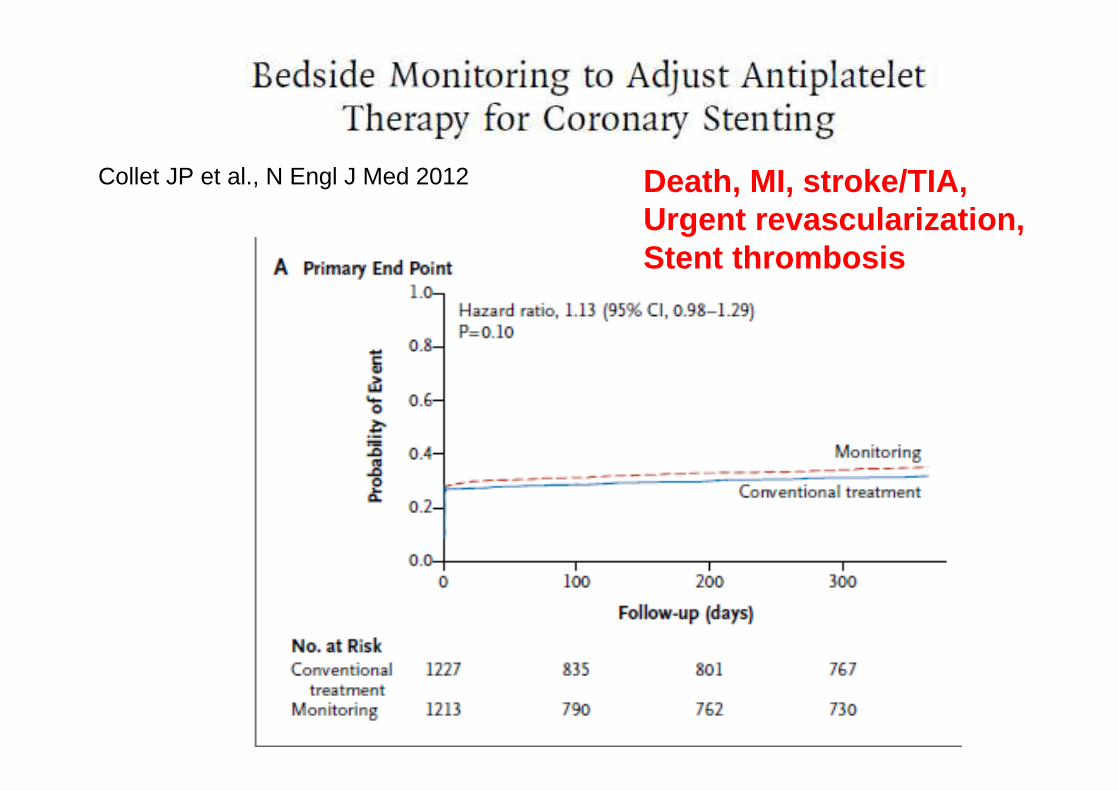
Collet JP et al., N Engl J Med 2012 Death, MI, stroke/TIA,Urgent revascularization, Stent thrombosis
Collet JP et al., N Engl J Med 2012
847/1213 loading dose…and the others?
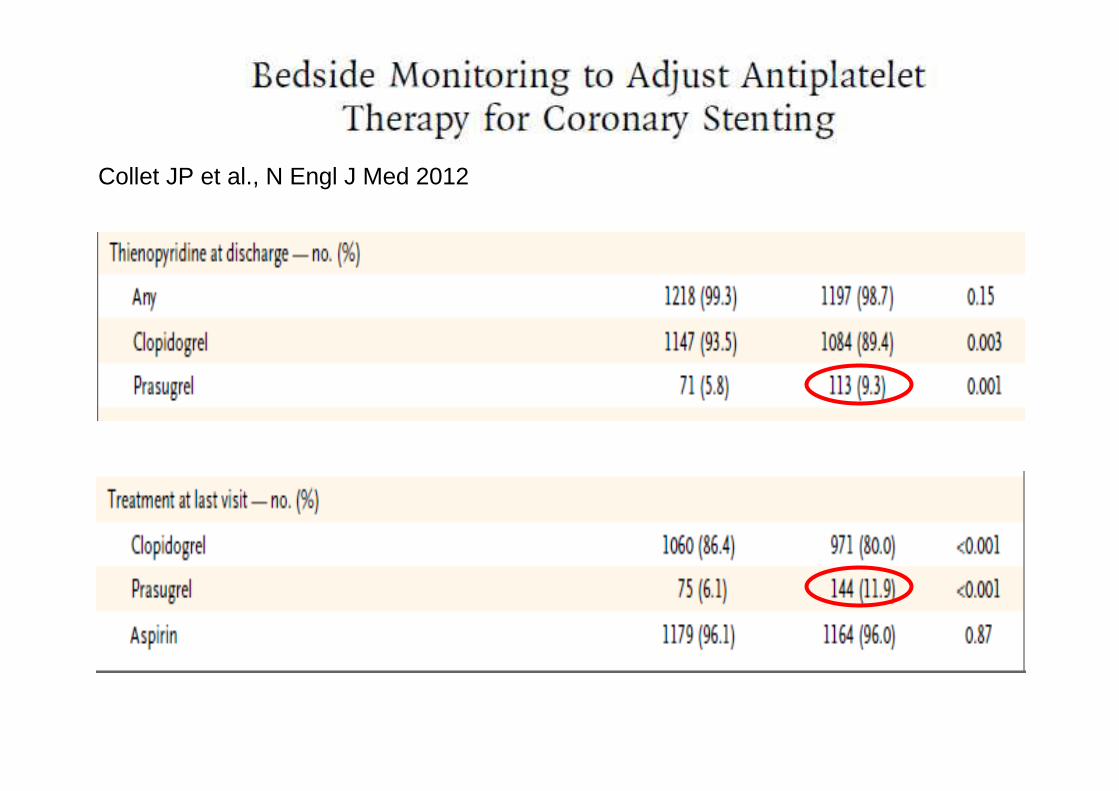
Collet JP et al., N Engl J Med 2012

Collet JP et al., N Engl J Med 2012


Whole cohort
Non carriers
of CYP2C19*2
Carriers
of CYP2C19*2
Roberts, Lancet 2012

Roberts, Lancet 2012

Point of care genetic testing after PCI can
be done effectively at the bedside and
treatment of identified CYP2C19*2
carriers with prasugrel can reduce high
on-treatment platelet reactivity
Roberts, Lancet 2012

GIANT STUDYClopidogrel Genotyping for Antiplatelet Guidance in MI Stenting: Maybe Reduced Ischemic RiskNovember 06, 2013TCT
In the prospective GIANT trial with 1445 patients, it was discretionary whether clinicians raised the clopidogrel dosage or switched thienopyridine agents based on the assay results, which they had in hand within 48 hours after stenting.
Such changes were made in 86% of the 316 who tested positive for the LOF genotype, a group known to be at increased ischemic risk on standard clopidogrel-containing antiplatelet therapy after stenting.

Among those 272 patients with assay-guided antiplatelet changes, the one-year composite risk of death, MI, or stent thrombosis closely matched that of patients lacking the high-risk genotype
GIANT STUDYClopidogrel Genotyping for Antiplatelet Guidance in MI Stenting: Maybe Reduced Ischemic RiskNovember 06, 2013TCT
Of note, the composite end point was about five times higher forthe remaining 14% of LOF-genotype patients whose antiplatelet therapy wasn't changed based the assay
End point
Normal
n=1118
LOF, treatment is adjusted,
n=272
LOF, treatment is not adjusted,
n=55
Primary 3.04 3.3* 15.6

TRANSIENT
Acute phase
High on-treatmentplatelet reactivity

NATURAL HISTORY OF HPR BY ADP IN ACS PATIENTS
AMI FLORENCE STUDY

Atherosclerosis 2013

Atherosclerosis 2013

The next FUTURE….
- Prasugrel / Ticagrelor for ALL patients?
- Prasugrel/Ticagrelor: duration of therapy?

NSTEMI 2011

NSTEMI 2011

2012


What about costs?
In Italy:
1 year
CLOPIDOGREL (generic drug) 0.57 E/cp 205E
PLAVIX 0.65 E/cp 234E
PRASUGREL 2.57 E/cp 925E
TICAGRELOR 1.80 E/cp 648E

CLOPIDOGREL HYDROGEN SULFATE
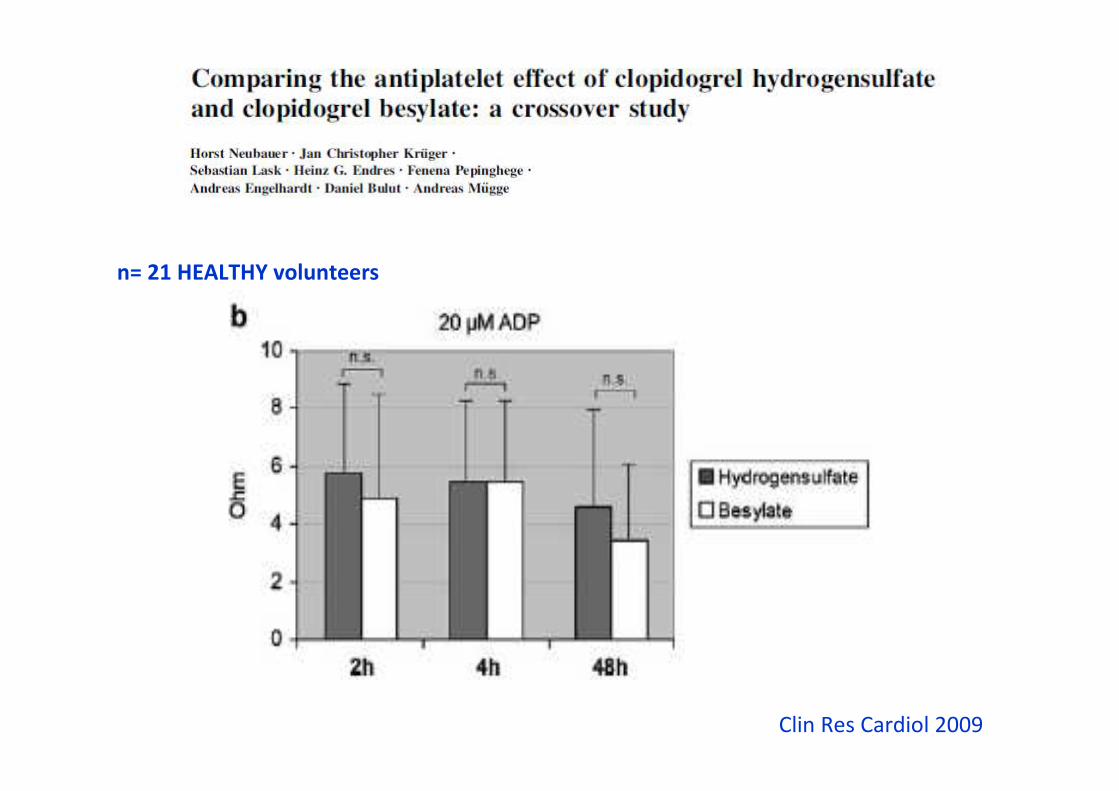
n= 21 HEALTHY volunteers
Clin Res Cardiol 2009

CHS= Clopidogrel Hydrogensulfate
CB= clopidogrel besylate
n=150 pts
Thromb Res 2011


CLOPIDOGREL
BASE
(n=741)
CLOPIDOGREL
HYDROGENSULFATE
(n=838)
p
Age (yrs) 72±12 71±12 0.108
Sex (M/F) 521/220 590/248 0.999
Hypertension, n (%) 510 (68.8) 570 (68) 0.745
Diabetes, n (%) 163 (21.9) 192 (22.9) 0.673
Smoking, n (%) 373 (50.3) 415 (495) 0.762
Dyslipidemia, n (%) 290 (39.1) 330 (39.3) 0.959
STEMI/NSTEMI 363/378 402/436 0.724
HPR by ADP n (%) 314 (42.2) 213 (25.4) <0.0001
10 µM/L ADP-PA 58%±20% 52%±19% <0.001
1 mM arachidonic acid-PA 18%±7% 17%±9% 0.715
2 µg/ml collagen-PA 36.7%±15.2% 33.5%±16.6% <0.001
Marcucci R et al. JACC 2013

2010
2011Oct.
45/166 (27 %)
58/144 (40 %)
0 10 20 30 40 50
(%)
ADP (%)
2010
2011Nov.
43/144 (30 %)
53/126 (42 %)
2010
2011Dec.
38/133 (29 %)
51/135 (38 %)
2011
2012Jan.
37/124 (30 %)
50/114 (44 %)
2011
2012Feb.
31/130 (24 %)
45/99 (44%)
2011
2012Mar.
19/141 (13%)
57/123 (45%)
TOTAL
213/838 (25.4 %)
314/741 (42.4%)
56.7±19.5
57.2±17.9
58.2±18.3
60.8±19.6
54.5±19.4
61.6±19.2
54.2±19.6
56.9±20.5
51.1±19.4
56.5±19.1
46.3±18.2
57.7±20.8
52.3±19.4
57.9±19.8
= Clopidogrel hydrogensulfate = Clopidogrel base
P<0.05
P<0.05
P=0.060
P<0.05
P<0.05
P<0.005
P<0.0001
Marcucci R et al. JACC 2013

A company press release reports that Dr. Reddy’s launched bioequivalent
generic clopidogrel tablets, 75 mg and 300 mg, in the United States on May 18,
2012.
The US version appears to be clopidogrel bisulphate, and not the base form.
In June 2009, the EMEA gave the go-ahead to 6 generic versions of
clopidogrel bisulfate and the drug is now available in several European
countries.
On June 2, 2010, the EMEA approved the generic version clopidogrel base,
stating that 75-mg tablets possess adequate quality and benefit/risk ratio
and are comparable to the reference clopidogrel product.
Italian Generic Clopidogrel Worse Than Brand
Name at Suppressing Platelets
Marcucci R et al. JACC 2013


The next FUTURE….
- Prasugrel / Ticagrelor for ALL patients?
- Prasugrel/Ticagrelor: duration of therapy?

ISCHAEMIC
EVENTS BLEEDING
CHRONIC PHASE

Tantry US, Bonello L, Aradi D, Price MJ, Jeong YH, Angiolillo DJ, Stone GW, Curzen N, Geisler T, Ten Berg J, Kirtane A, Siller-Matula J, Mahla E, Becker RC, Bhatt DL, Waksman R, Rao SV, Alexopoulos D, Marcucci R, Reny JL, Trenk D, Sibbing D, Gurbel PA.
J Am Coll Cardiol. 2013 Sep 26. doi:pii: S0735-1097(13)05380-1.
Consensus and Update on the Definition of On-Treatment Platelet Reactivity to ADP Associated with Ischemia and
BLEEDING


Sibbing D et al, J Thromb Haemost 2010

Campo G, JACC 2011
Prospective Evaluation of On-Clopidogrel Platelet Reactivity Over Time in
PatientsTreated With Percutaneous Coronary Intervention Relationship With Gene
Polymorphisms and Clinical Outcome

Residual Platelet Reactivity, Bleedings, and Adherence toTreatment in Patients Having Coronary Stent Implantation
Treated With PrasugrelParodi et al., AJC Oct 2011
LTA 10 µm ADP < 40% : 96/298 (32%)Multivariate analysis
OR FOR BLEEDING EVENTS Female gender: OR= 2.2 (1.08-4.45),
p=0.029
Low RPR: OR= 0.91 (0.88-0.95), p=0.001

From clopidogrel – through drug resistance – to NEW antiplatelets
from MONITORING antiplatelet therapyto the identification of
a risk marker ON dual antiplatelets
….Toward a tailored antiplatelet treatment based on symptoms,
clinical and procedural characteristics and platelet function testing…..