myocardial perfusion imaging. physiological alteration vs. stress rest stress perfusion abnormality...
TRANSCRIPT

Myocardial Perfusion ImagingMyocardial Perfusion Imaging
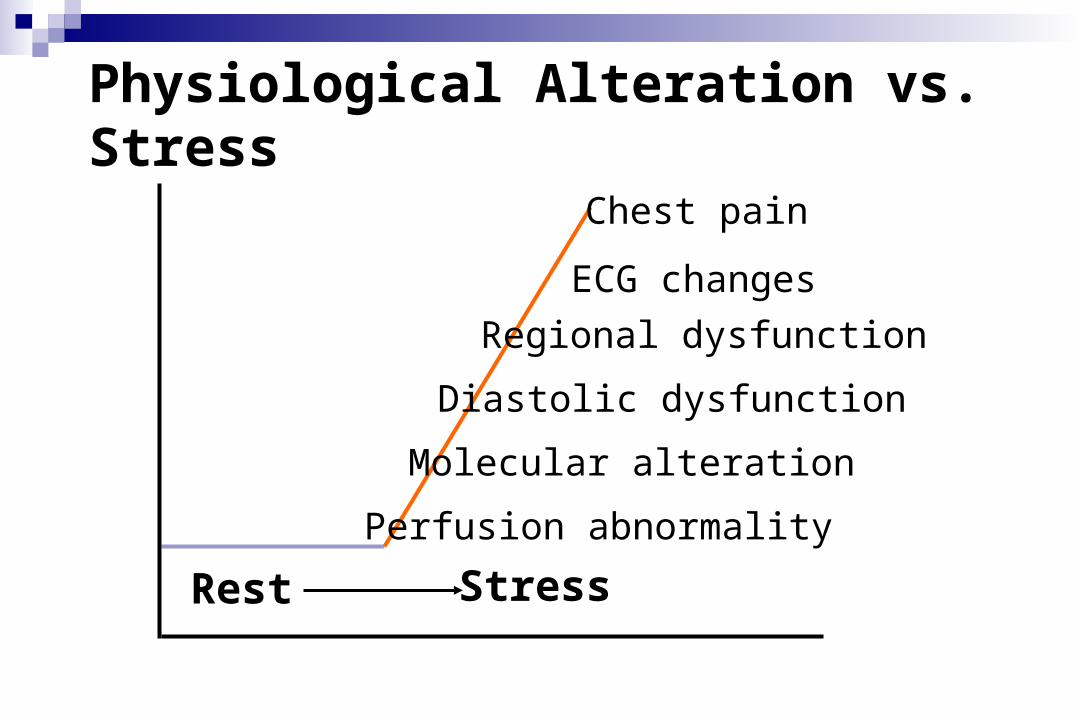
Physiological Alteration vs. Stress
Rest Stress
Perfusion abnormality
Molecular alteration
Diastolic dysfunction
Regional dysfunction
ECG changes
Chest pain
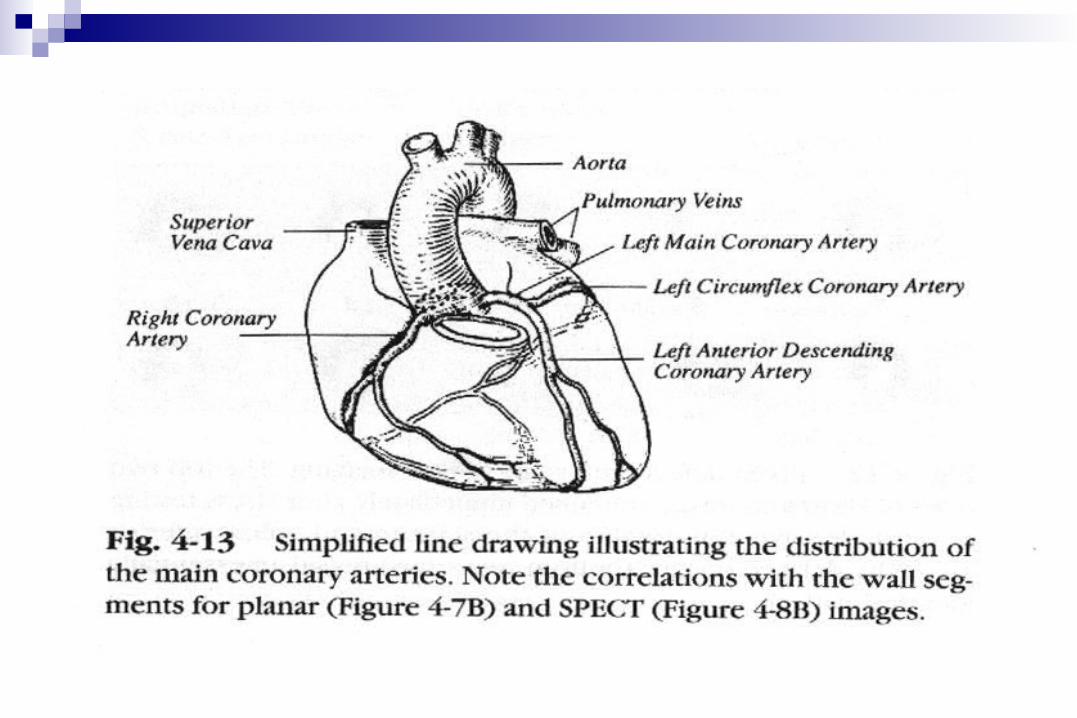

Myocardial perfusion scintigraphy Overview
Myocardial blood flow 80-100 ml/min/100g at rest, 3-5 fold while demand When tachycardia, absolute flow , but inner-to-outer flow ratio
1973 Zaret et al. 43K NEJM 1973;288:809
1977 Botvinick et al. 81Rb AJC 1977;39:364
1973 Lebowitz et al. 201Tl JNM 1973;14:421
Heo et al. 99mTc Cardiology 1994;12:187
1989 Najm et al. Function EHJ 1989;10:142
Cooke et al. SPECT AJCI 1993;7:152
Maddahi et al. Quantitative JACC 1989;114:1689



Myocardial perfusion Radiotracers
Mechanism, Extraction, and Linearity with flow



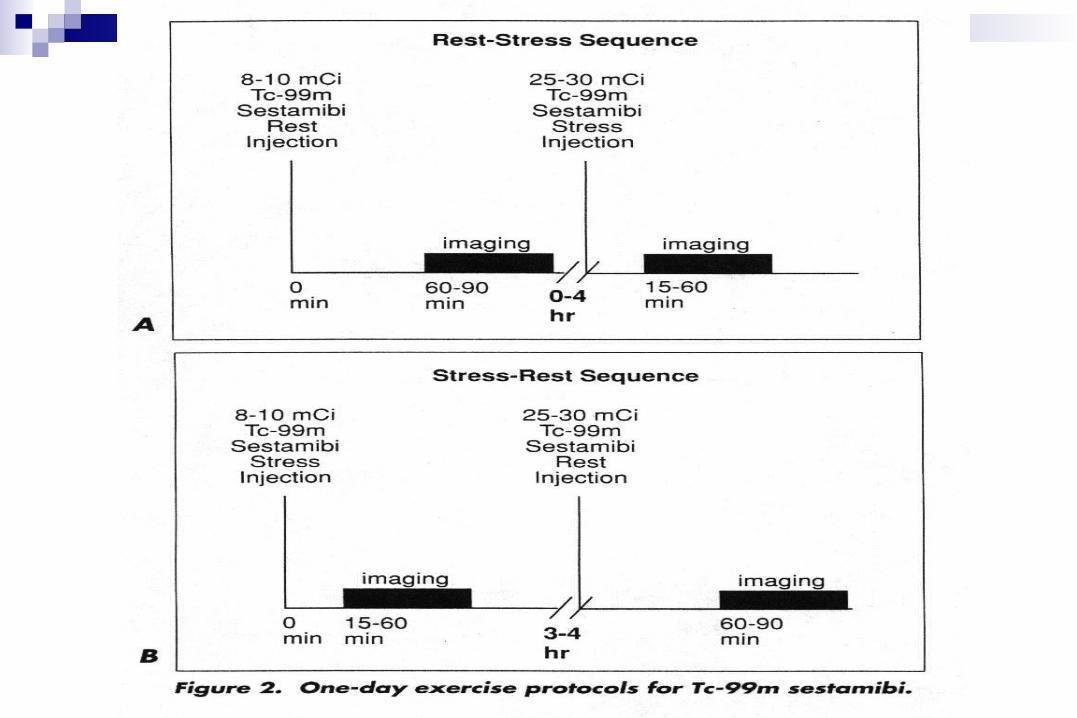
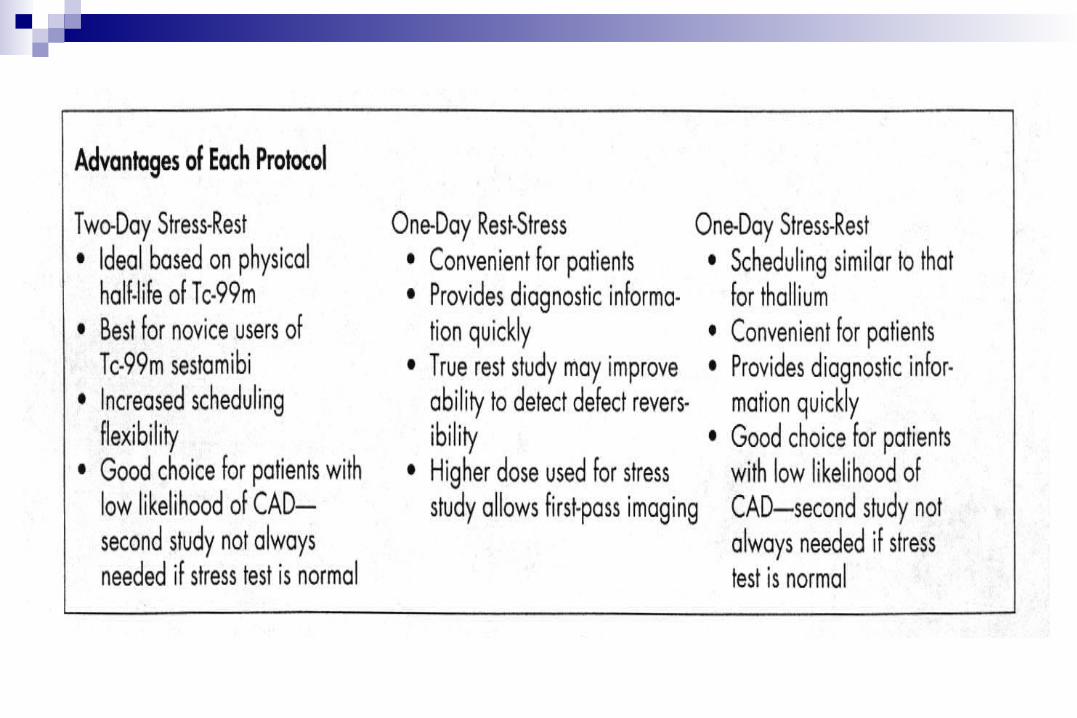
Comparison of MPS protocols 201Tl stress-rest protocol
Long half-life, low dose, low count, poor spatial resolution, low energy, not well gated images, high scatter, attenuation
Stress always first Probably optimal viability agent
201Tl rest-redistribution protocol Likely optimal and most cost-effective viability study
99mTc sestamibi / tetrofosmin protocols Better imaging characteristics, high resolution, least attenuation, no signific
ant redistribution Dual isotope 201Tl rest / 99mTc stress protocol
Brief with high throughput 24-hr 201Tl imaging to maximize viability assessment Difficulties in comparing 201Tl and 99mTc images

Tl-201 Myocardial imaging
Patient preparation: fasting for 4 hours. Dosage: 2-3 mCi, i.v. Stress imaging: 10 min post Tl-201 admi
nistration. Rest imaging: 3-4 hr later.

Cardiac drugs that may interfere with stress testing and
recommended withdrawal interval
Beta blockers 72 hr Ca++ channel blockers 48-72 hr Nitrates (long acting) 12 hr


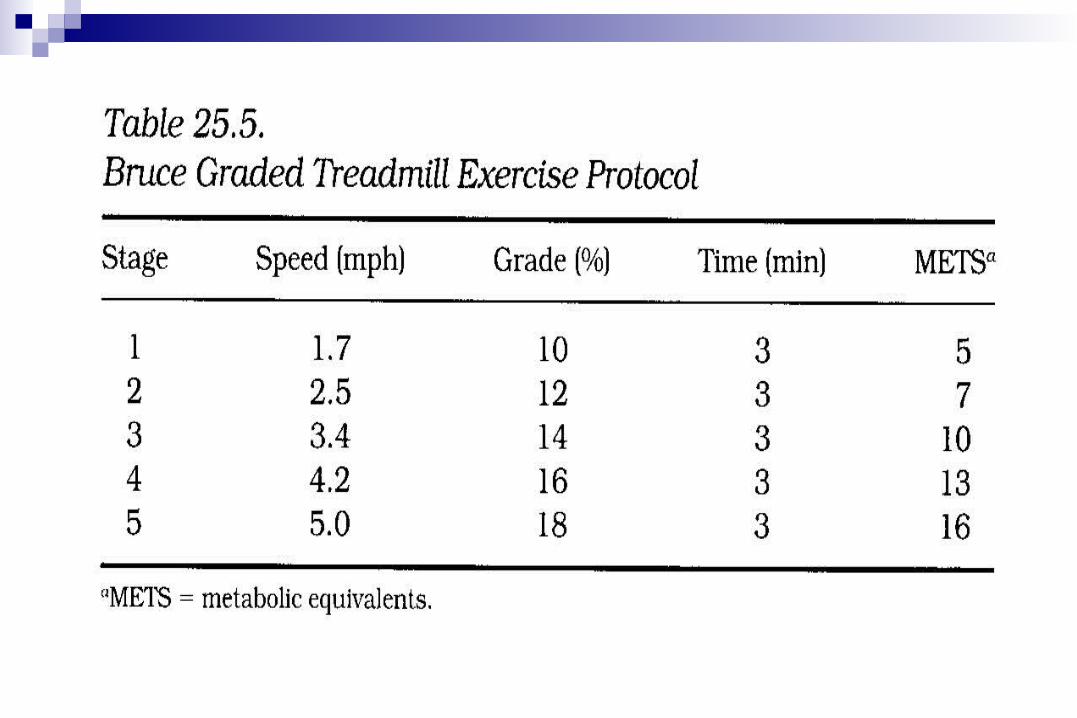


Alternatives to leg exercise in cardiac stress testing Isometric (handgrip) exercise Atrial pacing Esophageal pacing Cold pressor testing Ventricular stimulation; postextrasystolic pot
entiation Pharmacologic stress






SPECT processing stepsProcess Utilization
Filtering
Timing Prereconstruction Standard
with Reconstruction Optional
Types Adaptive Optional
Conventional Standard
Reconstruction
Transverse Analytic (backprojection) Standard
Iterative Optional
Oblique angle Manual / Automatic
Display
Cine review Screen Mandatory
Study review Screen Preferred
Hard copy Optional

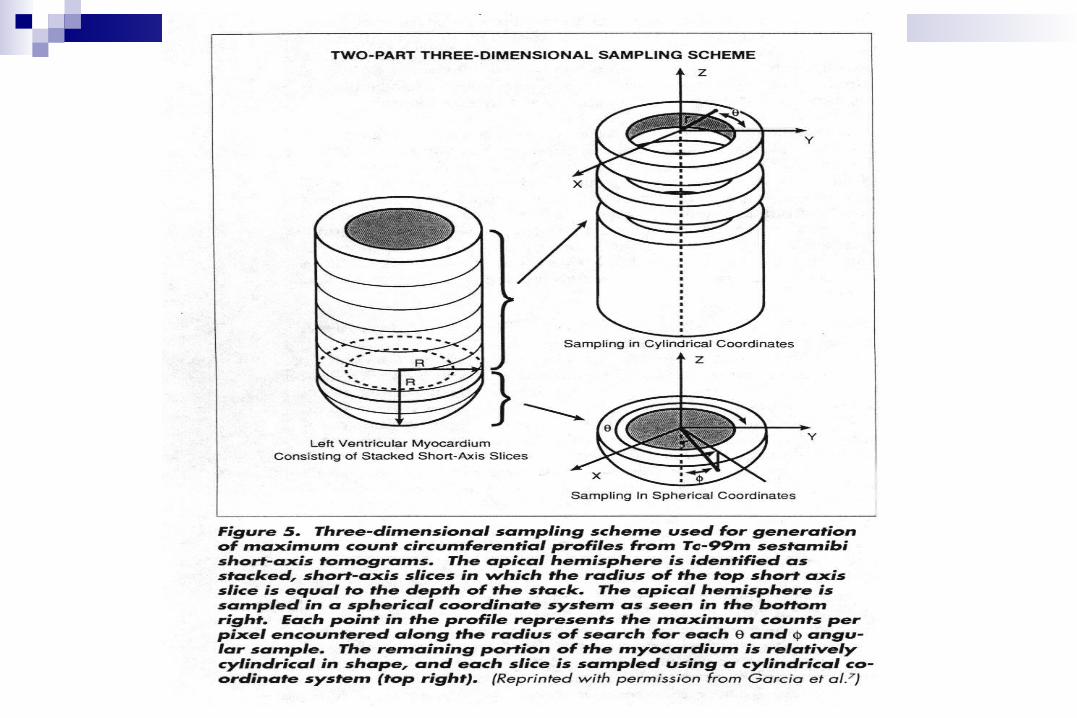
Methods of MPS QuantitationOperation Method Utilization
Sampling Circumferential profile
Cylindrical Standard
Cylindrical and Spherical Optional
Maximum count Standard
Average count Optional
Normalization Maximum count Standard
Average region Optional
Maximum count (%) Optional
Analysis Normal database Standard
Threshold Optional
Variables Extent, Severity, Reversibility Standard
Transient dilation, Lung washout Optional
Display 2D polar maps (Bullseye maps) Standard
Circumferential profiles Optional