myocardial repair by percutaneous cell transplantation of autologous skeletal myoblasts as a stand...
TRANSCRIPT

Myocardial repair by percutaneous cell transplantation of autologous
skeletal myoblasts as a stand alone procedure in post myocardial
infarction chronic heart failure patients: the SEISMIC trial
Pilar Jiménez Quevedo MD on behalf of the BIOHEART European SEISMIC study investigators
4th International Symposium on Stem Cell Therapy and Applied Cardiovascular Biology,
Madrid april 2007
(Safety and Effects of Implanted (Autologous) Skeletal Myoblasts (MyoCell™) using an Injection Catheter)
CARDIOVASCULARINSTITUTO
HOSPITAL CLINICO SAN CARLOS
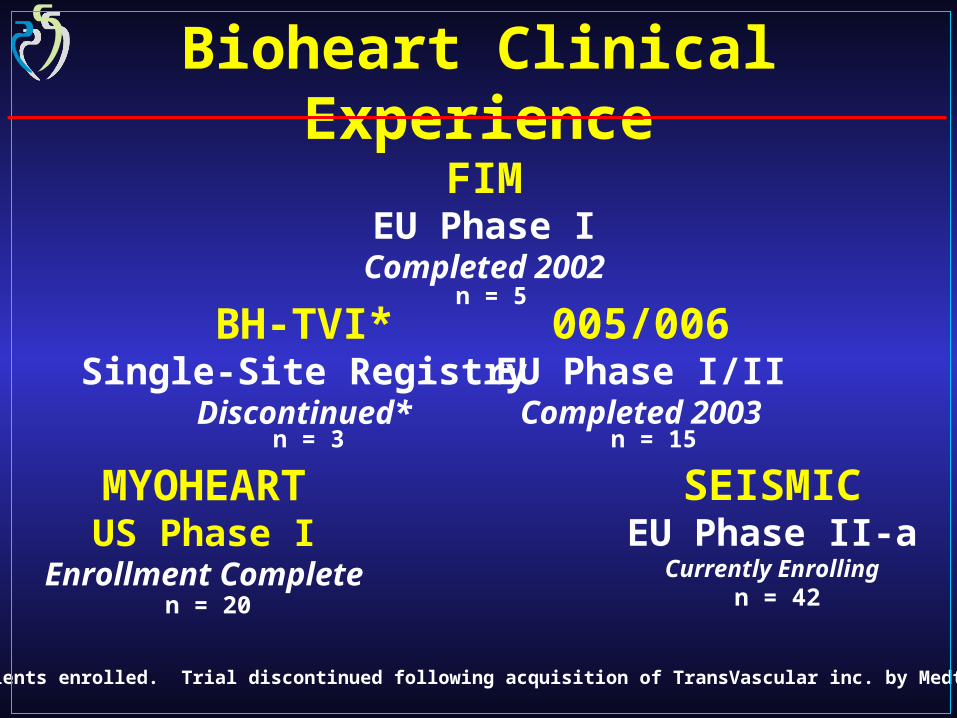
Bioheart Clinical Experience
MYOHEARTUS Phase I
Enrollment Complete
SEISMICEU Phase II-a
Currently Enrolling
FIMEU Phase I
Completed 2002
005/006EU Phase I/IICompleted 2003
BH-TVI*Single-Site Registry
Discontinued*
* 3 patients enrolled. Trial discontinued following acquisition of TransVascular inc. by Medtronic Inc.
n = 5
n = 3 n = 15
n = 20 n = 42

Phase IIOpen-label, Randomized, Controlled, Multi-Center Study P.I.: P.W. SerruysHealth Decisions – Data Management/StatisticsSynarc – Core-Lab Echo, MUGAHertford Cardiology – Core-Lab, HolterSponsor: Bioheart, Inc. Sunrise, Florida, USA
Percutaneous Intramyocardial Transplantation of Autologous Myoblasts:
BIOHEART SEISMIC* Trial

Overall Objective:
To assess the safety and efficacy of MYOCELL™ therapy on myocardial function in CHF patients post MI(s).
Bioheart EU Phase II Trial – SEISMIC

Primary Safety Endpoint:– Defined Serious Adverse Events (SAEs) at 3 & 6 mos.
Secondary Safety Endpoints:– Number and mean length of stay for hospitalizations– Holter monitoring, 12-lead ECG data, frequency of
ventricular arrhythmias– Safety of the use of the MyoCath™ injection catheter
by Adverse Event (AE) assessment
Bioheart EU Phase II Trial – SEISMIC

Primary Efficacy Endpoint:– Change in LVEF at 3 & 6 mos. by MUGA compared
with baseline
Secondary Efficacy Endpoints:– QOL assessment, 6-min. walk, NYHA class– Hospitalization, readmissions or the need for
medical treatment outside of hospitalizations– Improvements in global contractility, wall thickness,
coronary perfusion and change in infarct size
Bioheart EU Phase II Trial – SEISMIC
SEISMIC Significant Adverse Events
• Study protocol defines SAEs as any adverse events meeting one or more of the following:
• Fatal• Life-threatening• Requiring in-patient hospitalization not specifically required
by the protocol or is elective• Resulting in permanent impairment or surgical intervention
to preclude permanent impairment of a body function
• Additionally, medical events that may not result in death, be life-threatening, or require hospitalization may be considered SAEs when they jeopardize the patient.
• Medical and scientific judgment is exercised when classifying events as serious
• Relation between an adverse event and the test article will be determined by the Investigator on the basis of his or her clinical judgment

Pr. Patrick Serruys, Rotterdam, the Netherlands (PI)
Dr. Jozef Bartunek, Aalst, Belgium
Pr. Victor Legrand, Liege, Belgium
Dr. Walter Van Mieghem, Genk, Belgium
Pr. Christoph Nienaber, Rostock, Germany
Pr. Joachim Schofer, Hamburg, Germany
Pr. Christoph Hehrlein, Freiburg, Germany
Dr. Johannes Waltenberger, Maastricht, the Netherlands
Dr. Carlos Macaya, Madrid, Spain
Dr. Anthony Gershlick, Leicester, UK
Pr. Nicholas Peters, London, UK
Pr. Tomasz Siminiak, Poznan, Poland
Dr. Peter Smits, Rotterdam, the Netherlands
SEISMIC Trial Investigators
13 investigative sites, 6 European countries
*
** *
** **

SEISMIC Committees
Independent Data Safety & Monitoring Board
– J. Tijssen, Chair – Amsterdam, The Netherlands– G. Steg – Paris, France– F. Verheugt – Nijmegen, The Netherlands– H. Wellens, EP – Maastricht, The Netherlands
SEISMIC Steering Committee
– P.W. Serruys, Chair – Rotterdam, The Netherlands– J. Bartunek – Aalst, Belgium– A. Gershlick – Leicester, UK– N. Peters, EP – London, United Kingdom

SEISMIC Patient Selection
Inclusion Criteria:
– Age ≥ 18 and ≤ 75 years old – Placement of ICD 6 months prior to study entry – Prior MI > 90 days with region of myocardial dysfunction
involving the anterior, lateral, posterior or inferior walls– LVEF at screening of ≥ 20% ≤ 45% (by MUGA scan)– New York Heart Association (NYHA) Symptom Class II or III– Patients on optimal medical drug therapy for at least 2
months prior to study entry– Need or feasibility for re-vascularization has been ruled out
within 30 days of screening– Minimum myocardial wall thickness of 5mm
SEISMIC Patient Selection
Exclusion Criteria:
– CABG within 180 days OR PCI within 90 days prior to scheduled MyoCell™ implantation
– Aortic valve replacement– Exposure to any investigational drug or procedure within 1
month prior to study entry or enrolled in any concurrent study that could confound the data
– ICDs implanted less than 180 days or reprogrammed less than 90 days prior to cellular implantation
– Patients fitted with a Bi-V pacers– Patients unable to take anti-arrhythmic medications– Evidence of left ventricular mural thrombus
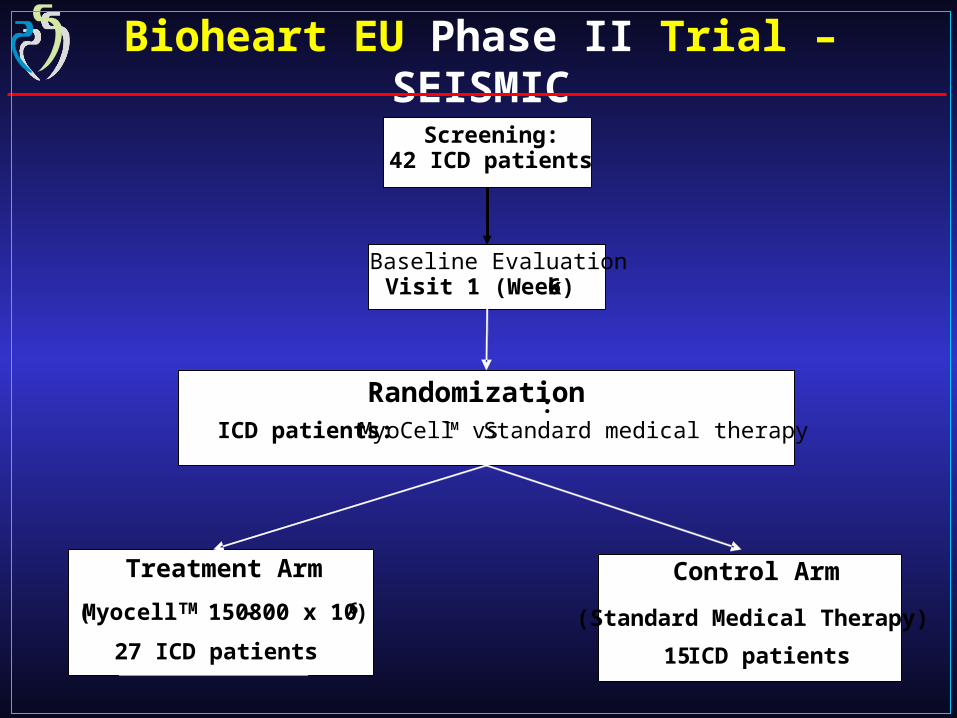
Randomization :ICD patients: MyoCell™ vs Standard medical therapy
Treatment Arm
(Myocell TM 150- 800 x 106)
27 ICD patients-
Control Arm
(Standard Medical Therapy)
15 ICD patients
Baseline EvaluationVisit 1 (Week 6)
Screening: 42 ICD patients
Bioheart EU Phase II Trial – SEISMIC

SEISMIC Study Flow
Days 1-2 Days 7-8 Days 14-15 Days 21-22 Day 28(±2) Day 35 (Implantation) 30 Days (±2 days) post implantation
90 Days (±2 days) post implantation
180 Days (±2 days) post implantation
Visit 1 Screening
ICF Biopsy Request Form HX/Med Review PE ECG NYHA Class 6-min walk Min QOL MUGA DSE TDI ICD Review Amiodarone Pivitol Core Lab · Viral Screen · Serum Chemistry · Hematology · Coagulants
Local Lab · Urinalysis · Cardiac Panel
Screening 24 hr Holter
Monitoring # 1
Screening 24 hr Holter
Monitoring # 2
Visit 2 Biopsy/Assessment
HX/Med Review PE AE Assessment ECG ICD Review Amiodarone Cont. Holter Monitoring Weekly Pivitol
· Serum Chem · Hematology · Coags
Local Lab · Urinalysis · Cardiac Panel
Treatment Group Muscle Biopsy
Visit 4 1 Month Follow-up
HX/Med Review PE ECG NYHA Class 6-min walk Min QOL ICD Review Holter Monitoring Monthly amiodarone D/C’d Pivitol · Serum Chem · Hematology · Coags
Local Lab · Urinalysis · Cardiac Panel
Visit 6 6 Month Follow-up
HX/Med Review PE ECG NYHA Class 6-min walk Min QOL MUGA DSE TDI ICD Review Pivitol · Serum Chem · Hematology · Coags
Local Lab · Urinalysis · Cardiac Panel
Screening 24 hr Holter
Monitoring # 3
Screening 24 hr Holter
Monitoring # 4
Randomization
Visit 3 Treatment - Implantation
Pre-Procedure PE AE Assessment ECG ICD Review Resting Echo (prior) ICD Review Local Lab · Cardiac Panel (6 hrs prior)
Post-Procedure Telemetry (8 hrs in hospital) Local Lab · Cardiac Panel (6 hrs post)
Resting ECHO (6 hrs post) 72 hr Holter Monitoring Discharge Instructions amiodarone Cont. Frequent Telephone Contacts ICD Review Weekly Holter Monitoring Weekly
Visit 3 Control - Assessment
HX/Med Review PE AE Assessment ECG ICD Review amiodarone Cont. 72 hr Holter Monitoring Holter Monitoring Weekly Pivitol · Serum Chem · Hematology · Coags
Local Lab · Urinalysis · Cardiac Panel
Visit 5 3 Month Follow-up
HX/Med Review PE ECG NYHA Class 6-min walk Min QOL MUGA DSE TDI ICD Review Holter Monitoring Monthly Pivitol · Serum Chem · Hematology · Coags
Local Lab · Urinalysis · Cardiac Panel
Visit 2a Re -Biopsy (if needed) Vital Signs AE Assessment ICD Review Amiodarone Cont. Muscle Biopsy

MyoCell™ Specifications
• Skeletal myoblasts suspended in organ transport media
• 30 ml bag is sterilized prior to filling with cells and handled aseptically thereafter
• Concentration: 50 million cells / 1 cc
• Temperature controlled delivery
• Cell Viability: 4-days from harvest

MyoCath™ Specifications
• Sheath Compatibility – 8f
• Usable Catheter Length – 115 cm
• Core Needle Diameter – 25 gauge
• Core Needle “dead space” – 0.5cc
• Adjustable Needle Length 3mm – 6mm
• Syringe Compatibility – 1cc Luer Lock
•
• Curve Size – Medium and Large

Apical
BasalAA BB
EpiEpi
EndoEndo InjectionsInjections
Cell Implant Procedure(From Animal Training)

Interim Analysis (n=25)

0123456789
10
Ser
ruys
Bar
tun
ekW
alte
nb
erge
rV
an M
iegh
emL
egra
nd
Nie
nab
erH
ehrl
ein
Sch
ofer
Ger
shli
ckP
eter
sM
acay
aS
imin
iak
Sm
its
Patients Randomized
SEISMIC Enrollment By Site
0123456789
10
Ser
ruys
Bar
tun
ekW
alte
nb
erge
rV
an M
iegh
emL
egra
nd
Nie
nab
erH
ehrl
ein
Sch
ofer
Ger
shli
ckP
eter
sM
acay
aS
imin
iak
Sm
its
Patients Consented

SEISMIC Baseline Characteristics Interim Analysis, n=25
Mean±SD Range Mean±SD Range
Age (years) 56 8.7 32-66 60 8.9 44-72
Male – no. (%) 14 (88) n/a 7 (78) n/a
Race: Caucasian – no. (%) 16 (100) n/a 9 (100) n/a
Diabetes Type II – no. (%) 6 (38) n/a 1 (11) n/a
Prior MI – no. (%) 16 (100) n/a 9 (100) n/a
Years Since Last MI 9.3 5 2-21 7.1 4 2-16
Prior History of VT – no. (%) 10 (63) n/a 6 (67) n/a
Years. ICD in Place 2.4 1-4 2.3 1-5
NYHA Class III – no. (%) 8 (50) n/a 3 (33) n/a
LVEF (%) 30.0 10.4 19-38 32.8 + 11.1 20-40
TREATMENT (n=16) CONTROL (n=9)
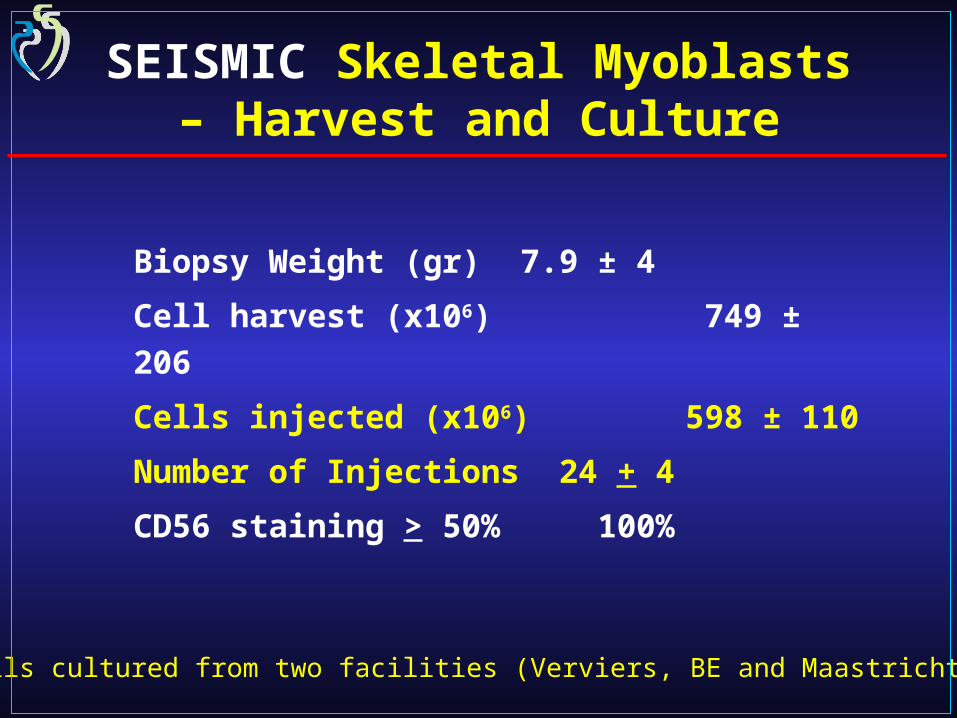
SEISMIC Skeletal Myoblasts – Harvest and Culture
Biopsy Weight (gr) 7.9 ± 4
Cell harvest (x106) 749 ± 206
Cells injected (x106) 598 ± 110
Number of Injections 24 + 4
CD56 staining > 50% 100%
Cells cultured from two facilities (Verviers, BE and Maastricht, NL)

SEISMIC Significant Adverse Events Interim Analysis, 25 patients
(16 treatment, 9 control) • 1+ month follow-up at time of analysis (December 2006)
• 6/16 patients (37.5%) in Treatment Arm Experienced 12 SAEs
– Death: 1 (multiple organ failure)– Worsening HF: 1 (hospitalization, recovered)– Pericarditis: 1 (hospitalized, recovered)– NSVT: 1 (self-resolving)– VT w/ ICD firing: 6 (5 possibly related, all resolved)*– Haematoma post-biopsy: 1 (recovered)– Herpes Zoster: 1 (recovered)
• 2/9 patients (22.2%) in Control Arm Experienced 2 SAEs– NSVT: 1 (self-resolving)– Diverticulitis: 1
* 3 of the 4 patients with VT (6 total events) were non-compliant with Amiodarone use per protocol

SEISMIC Arrhythmia Detail• 6 VTs w/ ICD firing (4 patients)
– Patient 12008: 2 separate single-firing events at days 5 and 11 post-procedure. Patient had history of VT prior to procedure (2 events in 2001). Patient allergy to Amiodarone prevented prophylactic administration per protocol. After 1st firing, was placed on Class I anti-arrhythmic, then on Amiodarone drip following 2nd firing. Arrhythmia fully resolved. After appearing to recover, patient subsequently declined and died of multiple organ failure 30 days post-procedure.
– Patient 14001: single firing at 8 days post-implant, full resolution. Patient had history of VT prior to procedure (2 events in 1996 and 1999 requiring cardioversion). Patient confirmed non-compliant with Amiodarone post cell implantation.
– Patient 14004: single firing, full resolution. Patient had history of VT prior to procedure (3 events in 2003 and 2005). ICD fired prior to cell implantation (patient not yet placed on Amiodarone).
– Patient 15001: 2 separate firing events at days 12 and 25 post-procedure, full resolution. Patient had history of VT, VF with multiple ICD firings (4 firing events since receiving ICD but prior to cell therapy). Patient treated with IV and oral Amiodarone.
* 3 of the 4 patients with VT (6 total events) were non-compliant with Amiodarone use
per protocol

SEISMIC LVEF (MUGA) Interim Analysis
27
28
29
30
31
32
33
34
35
Baseline 3 Months 6 Months
Treatment
Control
• 50% of treated patients exhibit improvement in LVEF
• 57% of control patients exhibit reduction in LVEF
(n=25) (n=13) (n=6)
Mean %
30.0+
10.4
32.8+
11.1
30.2+
8.2
32.4+
8.9 31.7+
21.8
31.7+
8.3

SEISMIC NYHA Class Improvement Interim Analysis
1
1.3
1.6
1.9
2.2
2.5
2.8
Baseline 3 Months 6 Months
Treatment
Control Treated Patients:
• 37.5% improved at 3 mos.• 50.0% improved at 6 mos.• No patients worsened at 3 or 6 mos.
Control Patients:
• 0% improved at 3 mos.• 25% improved at 6 mos.• 33% worsened at 3 mos.• 25% worsened at 6 mos.
(n=25) (n=14) (n=6)(Mean)

SEISMIC 6-Minute Walk Interim Analysis
-50
-25
0
25
50
75
100
125
TreatmentControl
Meters 97+
51.4
-20
Treated patients improved their 6-minute walk time at 6 mos. (n=7)
(Mean)
+147.1

SEISMIC – Conclusions
Interim analysis suggests arrhythmias largely manageable with close observation and prophylactic use of ICDs and Amiodarone
Limited amount of follow-up at this time prevents meaningful insight to efficacy analysis, though preliminary trends appear encouraging
Final 6-month data expected to be available for presentation at a medical symposium Q4 2007


SEISMIC Time to First SAE / Death

SEISMIC Injection Guide
0.5 3.0 150
0.5 4.0 200
0.5 6.0 300
0.5 8.0 400
0.5 10.0 500
0.5 12.0 600
0.5 14.0 700
0.5 16.0 800
(mL) (mL) (x 10 6 cell)
Volume/
Injection
Total VolumeTotal Cells
0.5 3.0 50 150
0.5 4.0 50 200
0.5 6.0 50 300
0.5 8.0 50 400
0.5 10.0 50 500
0.5 12.0 50 600
28 0.5 14.0 50 700
0.5 16.0 50 800
(L ) (mL) (x 10 6 cell)
Volume/
Injection
Total Volume(mL)
Concentration(x 106 cells/mL)
Total CellsX 106 cell
Number of Injections
6
8
12
16
20
24
28
32
6
8
12
16
20
24
32
(x 106 cells/mL)