myth busters: answering difficult questions about single payer healthcare snahp annual summit...
TRANSCRIPT
Myth Busters: Answering Difficult Questions about Single Payer Healthcare
SNaHP Annual SummitFebruary 2015
Xin GuanAlbany Medical College, M3
Danny AshOhio State U. College of Medicine, M4

“The most important thing is to show people that change is possible.”
Gerald FriedmanProfessor of EconomicsUniversity of Massachusetts, Amherst

MYTH…“The uninsured get free health care. They can just go to the emergency room.”
MYTH… REALITY• Among families with at least one uninsured
member, less than ¼ report getting free or discounted care in any given year.
• Financial pressures to provide charity care are reducing the ability of private physicians to provide charity care.
• Emergency department care is not free! Hospitals bill the uninsured at higher prices than insurance companies pay
• EDs are ill-suited to provide primary care
MYTH…“Single payer is fundamentally anti-American because America is a capitalist and individualistic society.”
MYTH… REALITY• Anti American: ‐ our current system that
discourages entrepreneurship because health insurance is tied to employment
• Anti-American: our current system that leaves Americans vulnerable to skyrocketing healthcare costs, so that 78% of all bankruptcies are related to medical bills
• Single payer will boost our economy, reduce healthcare expenditures in the long run and help us remain a strong nation.
MYTH…“Single payer is socialized medicine.”

MYTH… REALITY• A single payer national health program is NOT socialized medicine• Socialized medicine: a system in which doctors and hospitals work
for and draw salaries from the government. – American examples: VA, Armed Services. – Other examples: Great Britain and Spain
• Single payer: the government pays for most healthcare (hence single payer) but does not own or manage medical practices or hospitals– American examples: Medicare– Other examples: Canada, Australia, Japan
• This is why our motto for single payer is “improved Medicare for all”

MYTH…“We have the best health care system in the world! Why change it?”

MYTH… REALITY• Our life expectancy and infant mortality rates are worse
than that of many countries• International rankings:
– 19th out of 19 nations in deaths from medically-treatable causes– WHO: 37th on overall performance and 24th on health attainment
• We spend more than any other nation in the world per capita on health care
• Only a select few who can afford it get some of the best care in the world. Americans get less of most kinds of care (doctor, hospital, surgery, etc.) than the citizens of other industrialized nations.

Our current system: worse outcomes…Female life expectancy at birth
Turkey
HungaryChile
Poland
Estonia
Ireland
Greece
United Kingdom
Germany
Slove
nia
Luxe
mbourg
Finland
Austria
Iceland
KoreaIta
ly
France
74
76
78
80
82
84
86
Figure: Gerald Friedman from data at http://www.oecd.org/els/health-systems/oecdhealthdata2013-frequentlyrequesteddata.htm
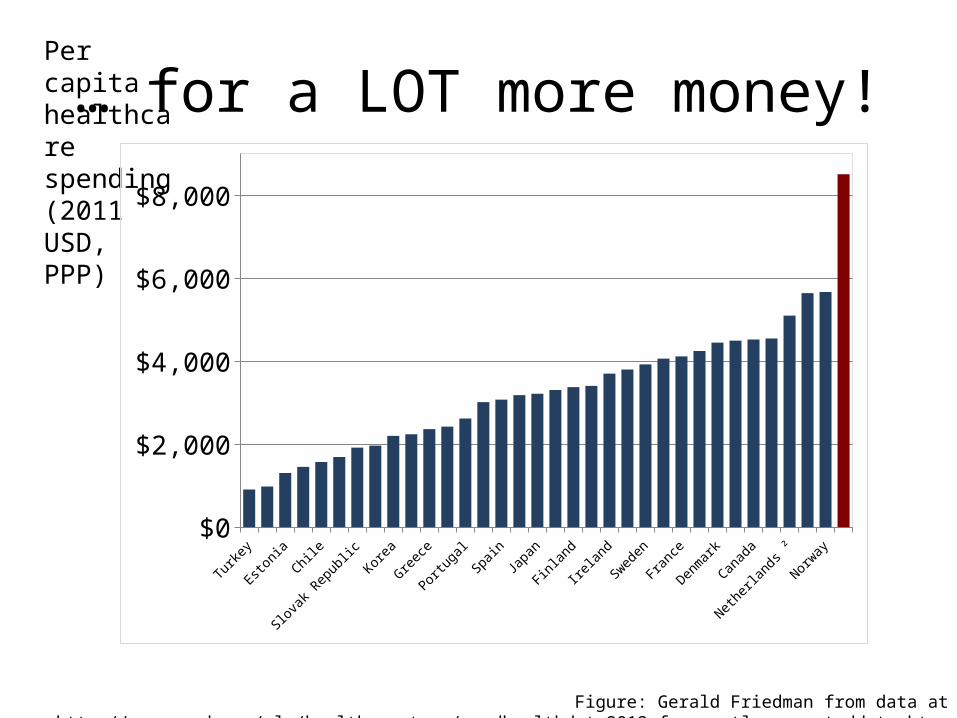
… for a LOT more money!Per capita healthcare spending (2011 USD, PPP)
Turk
ey
Esto
nia
Chile
Slov
ak R
epub
lic
Korea
Greec
e
Portu
gal
Spai
n
Japa
n
Finla
nd
Irela
nd
Swed
en
Fran
ce
Denm
ark
Canad
a
Nethe
rland
s ²
Norway
$0
$2,000
$4,000
$6,000
$8,000
Figure: Gerald Friedman from data at http://www.oecd.org/els/health-systems/oecdhealthdata2013-frequentlyrequesteddata.htm

Paying more… for less!
0
2
4
6
8
10
12
14
An
nu
al p
er
Cap
ita D
oct
or
Vis
its
Figure: Gerald Friedman from data at http://www.oecd.org/els/health-systems/oecdhealthdata2013-frequentlyrequesteddata.htm
MYTH…“We already have healthcare reform. The ACA will cover everybody who is uninsured.”

MYTH… REALITY• The ACA will cover some uninsured
Americans… but the job’s not finished!• CBO projections for 2019: 23 million Americans
still without coverage• CBO estimates do not include the
underinsured, who are still vulnerable to financial ruin due to growing out-of-pocket costs
• Underinsurance will worsen under ACA

MYTH…“Single payer will restrict provider choice.”

MYTH… REALITY• Provider choice is already restricted under
current system!• Many private insurers severely limit patients’
ability to choose their health care provider• Single payer would promote increased patient
autonomy and choice of providers by removing all “network” restrictions
MYTH…“Quality of care will suffer under single payer.”

MYTH… REALITY• Single payer provides the most effective
financial structure for increasing the quality and efficiency of care
• Facilitates large-scale adoption of quality improvement initiatives such as surgical checklists
• Makes it possible to identify "outliers" who are practicing outside community norms

Perverse incentives and fragmented payment system: a recipe for trouble
MYTH…“Doctors will never buy into single payer because it will interfere with their autonomy and decrease their salaries.”

MYTH… REALITY• More than 60% of physicians already support a single payer
system • Canada is experiencing a net influx of physicians – both
Canadian and American• Private companies currently restrict physicians’ ability to
practice medicine (network restrictions, precert, etc)• Under single payer, decision making will be returned to
healthcare providers and their patients• Based on Canadian experience, average physician incomes
should change little, though income disparity between specialties is likely to shrink

Healthcare job growth since 1970...
Physicians Administrators
3000%
2500%
2000%
1500%
1000%
500%
01970 1980 1990 2000 2010
Figure: Gerald Friedman from data provided by Bureau of Labor Statistics, Occupational Employment Statistics, at bls.org.

… a uniquely American phenomenon!
USA Canada$0
$1,000
$2,000
$3,000
$4,000
$3,006
$787
Per capita administrative spending (2014 USD)
Figure: Gerald Friedman from Woolhandler/Himmelstein/Campbell NEJM 2003;349:769 (updated 2013)

MYTH…“Single payer is politically unfeasible – look what happened in Vermont!”

MYTH… REALITY• There are still single payer bills in many state
legislatures and a national bill, HR 676• Single payer has growing support from health
professional, labor, business, and faith-based groups• Vermont’s plan had veered away from a true single
payer model, so is not representative of single payer’s political prospects
• Effective grassroots organizing got real healthcare reform on the political radar screen in Vermont, and can get it back on the radar elsewhere!
MYTH…“Health care is not a right.”

MYTH… REALITY• Even if healthcare is not a right, single payer might still be the
wisest public policy because of its moral and economic benefits.
• Moral benefits - tens of thousands of Americans die each year because they do not have adequate access to healthcare
• Economic benefits - The United States spends 50% more as a percentage of its GDP than most other developed countries, but we insure a lower percentage of our population. Under single payer, the average taxpayer would have thousands of dollars more in discretionary income.

We die young because we lack access to careAnd it is getting worse!
Had a medica
l pro
blem, did not v
isit d
octor o
r clin
ic
Did not fill a
prescr
iption
Skipped reco
mmended test,
treatm
ent or f
ollow-u
p
Did not get n
eeded specia
list c
are
Any of the above acc
ess pro
blems0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
200120052010
Slide by Gerald FriedmanSource: Commonwealth Fund survey reported in Cathy Schoen, et al., "Access, Affordability, and Insurance Complexity" Health Affairs, Nov. 18, 2013

Cost of health insurance, Ohio private-sector workers with health insurance and
single payer savings
Cost of health insurance, Ohio private-sector workers with health insurance and single payer savingsAverage premium worker with health insurance $ 9,584 Average deductible $ 1,777 Total: $ 11,361 Average wages $ 43,170 ratio 26.3%Savings under single-payer $ 7,044
Slide by Gerald Friedman
MYTH…“Single payer will create waiting lists.”
“Single payer would result in rationing of care.”

MYTH… REALITY• We are already rationing healthcare in the United
States.• All scarce goods are rationed. The only choice we have is
how.– Rationing in single payer system: according to need– Rationing in the current system: according to income
• This is an inefficient allocation of healthcare resources. • In European-style single-payer systems, some elective
procedures have waiting lists, but there are rarely, if ever waiting lists for medically necessary or emergent procedures
MYTH…“How can we possibly transition from our current system to single payer? It seems impossible!”

MYTH… REALITY• The payment and provider structures already exist within
the Medicare program to permit a relatively smooth transition to a single payer health care system in this country
• Many people now working in the insurance industry are, in fact, already health professionals (e.g. nurses) who will be able to find work in the healthcare field again
• Many insurance and health administrative workers will need a job retraining and placement program. Cost: ~$20B/yr during transition (a small fraction of the administrative savings from transition)

THANK YOU!
Photos © Ian Hayhurst, Bob Estremera, and Joe Newman