neonatal transitional physiology: a new paradigm...neonatal transitional physiology: a new paradigm...
TRANSCRIPT

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology:A New Paradigm
Early clamping of the umbilical cord at birth, a practice developed without adequate evidence,causes neonatal blood volume to vary 25% to 40%. Such a massive change occurs at no othertime in one’s life without serious consequences, even death. Early cord clamping may impedea successful transition and contribute to hypovolemic and hypoxic damage in vulnerable new-borns. The authors present a model for neonatal transition based on and driven by adequate bloodvolume rather than by respiratory effort to demonstrate how neonatal transition most likely oc-curs at a normal physiologic birth. Key words: capillary erection, cardiopulmonary adaptation,the first breath, hypovolemia, neonatal blood volume, neonatal transition, nuchal cord, placentaltransfusion, polycythemia, postpartum placental respiration, umbilical cord clamping
Judith S. Mercer, CNM, DNSc, FACNMAssociate Clinical ProfessorUniversity of Rhode IslandKingston, Rhode Island
Rebecca L. Skovgaard, CNM, MSAssociate in the Department of
Obstetrics and GynecologyUniversity of Rochester at Highland
HospitalRochester, New YorkAssistant Professor in the School
of NursingUniversity of RochesterEditorial Staff, Strong Perifax
CURRENT ANALYSIS OF knowledgerelated to neonatal transitional phys-
iology reveals that early cord clampingmay interfere with completion of a normalphysiologic neonatal transition. An endresult of this interference with transitionalphysiology is a 25% to 40% reduction inthe neonate’s blood volume.1,2 In othercircumstances over the life span, sucha massive restriction in blood volumewould result in severe consequences,even death. Human babies are remarkablyadaptable, and in most cases no appar-ent harm is initially evident. However,practitioners are obligated to establish arationale for early neonatal managementand then to apply it in practice. The exist-ing evidence suggests that the interventionof early cord clamping evolved withoutadequate evidence-based rationale and,accordingly, is deserving of careful sci-entific review.3 The debate remains:what is optimal care—what do all babiesneed initially? Do some babies experience
The authors would like to thank Margaret McGrath,PhD, RN, for her inspiration, encouragement, andguidance throughout the development of this work.
Submitted for publication: November 9, 2000Accepted for publication: April 20, 2001
56
J Perinat Neonat Nurs 2002;15(4):56–75c© 2002 Aspen Publishers, Inc.

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 57
harm because of inadequate blood andred cell volume? Synthesizing knowledgefrom several disciplines, this articlepresents a new model for explainingphysiologic neonatal transition that pro-motes an alternative view about placentaltransfusion and the importance of delayedcord clamping in the first minutes of life.The application of this model to practicemay lead to benefits for all newborns andmay be especially important for compro-mised infants who do not have adequateperfusion.
Two factors, the singular role of thered blood cell (RBC) in the body and theidea that a significant reduction in RBCsat birth does no harm, must be exploredin examining any relationship betweenneonatal transition and cord clampinginterval. In recent years, advances inphysiological measurement tools andunderstanding of physiologic and patho-logic processes have been made that maysubstantiate the evidence against earlycord clamping. Application of this newknowledge to the issue of fetus-to-neonatetransition argues for a reformulation ofcurrent practice and presents a rationalbasis for optimal clinical practice. Of keyimportance are these two facts: that theonly oxygen-carrying component in thebody is the RBC,4 and that, in a typicalapproach to early neonatal managementtoday, immediate cord clamping, a reser-voir of RBCs is routinely, according totradition, discarded with the placenta.The problem occurs when oxygen deliv-ery is the primary concern in neonatalillness. These include respiratory dis-tress syndrome, persistent pulmonaryhypertension, necrotizing enterocolitis,and hypoxic-ischemic encephalopathy.Discovery of any potential relationshipof the pathologic processes of theseconditions to essential hypovolemia
in the newborn has been hamperedby the fact that there is no reliable, avail-able, clinically useful measure for RBC orblood volume in the neonate.2 The lackof evidence to guide practice, the assump-tion that early cord clamping can “do noharm,” and the relative connection thatthe RBC is the only transporter of oxygenlead to the conclusion that reexamina-tion of the consequences of early versusdelayed cord clamping is warranted.
The second key issue in explaining thenormal neonatal transition is the rationalefor the establishment of breathing. Tradi-tional views for causality of first breathhave focused exclusively on the respi-ratory and neurological system.5–8 Thesetheories have claimed asphyxia at birth,touch, cold and sensory stimulation, frogbreathing, and chest recoil as potentialexplanations for the first breath.7,8 Thesetheories were developed prior to thediscovery that fetuses perform breathingmovements in utero. None of these ex-planatory theories have held up to scrutinyupon closer examination.9 While earlycord clamping appears to hasten an in-fant’s first breath, severely depressed ba-bies do not breathe spontaneously—an in-teresting paradox worthy of investigation.Alternate analysis and synthesis of cur-rent knowledge can produce a more plau-sible model for the pathways to successfulextrauterine respiration.
LITERATURE REVIEW
In the last decade, there has been aresurgence of interest in the issue ofoptimal cord clamping time and itseffect on neonatal transition. Recentstudies show the benefits of delayed cordclamping as improving the neonate’scardiopulmonary adaptation,10 blood

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
58 JOURNAL OF PERINATAL AND NEONATAL NURSING/MARCH 2002
Table 1. Effects of placental transfusion on human neonatal systems in the first 6 hoursafter birth
Blood volume/Component measures• Blood volume17–21 +• Red cell mass17–21 +• Plasma volume17–19,21 +• Hematocrit15,16,21–24 =, +Vascular pressures• Atrial pressure25 +• Pulmonary artery26 +• Systolic blood pressure11,12,23 +Blood flow• Right and left ventricular output21 =• Renal blood flow27 +• Cutaneous blood flow (skin temperature)28 +• Systemic and pulmonary resistance10,29 +• Blood viscosity10,21,30 +• Vascular hinderance10 −• Red blood cell flow10 +• Cerebral red blood cell flow10 +• Gastrointestinal red blood cell flow10 +Other cardiac effects• Heart rate26,31 =• Cardiac size23 +• EKG signs of cardiac load22 +• Preejection period22,32 +•Murmurs23 −Renal function• Effective renal blood flow27 +• Glomerular filtration rate27 +• Urine flow27 +• Urinary sodium excretion27 −Respiration• Respiratory rate31,33 +• Lung compliance33,34 −• Function residual capacity33,34 −• Expiratory grunting31 +
Key: + = increased; − = decreased; == no change found.
pressures,11–13 oxygen transport andred blood cell flow,10,14 days on oxygenand ventilation,15 and anemia.16 Earlierstudies demonstrated consistent physio-
logical effects in newborns.17–34 Table 1summarizes the findings.
What is not agreed upon by cliniciansand researchers is the meaning of the

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 59
findings—are they harmful or beneficial?Delayed cord clamping seems to preventshock-like parameters and anemia (refer toTable 1). However, concerns exist aboutvolume overload and polycythemia.35–37
Unfortunately, the wide range of study de-signs and definitions of variables preventsa meaningful meta-analysis of the stud-ies. An additional shortcoming is that fewstudies evaluate outcomes beyond the firstfew hours after birth. The volume of di-verse studies and the lack of an organiz-ing framework for understanding this re-search thwart any attempt to synthesizethe literature or direct further knowledgedevelopment. A theoretical model for thetransition from fetus to neonate is essen-tial to establish the blueprint for under-standing this critical physiologic process.A gap exists because no current modelfor neonatal transition adequately explainsthe relationships among oxygen transport,RBC volume, and initiation of breathing, orpredicts the effects of early versus delayedcord clamping.
The goal of a theoretical model is toconnect and find meaning in a groupof related concepts for the purpose ofunderstanding, describing, or explaininga phenomenon.38 Such models provideand dictate hypotheses for research. Test-ing and further development may lead toprediction of outcomes and prescriptionfor practice. Clinical sciences need pre-scriptive models to guide interventionsand to provide underlying rationale for
A gap exists because no current modelfor neonatal transition adequatelyexplains the relationships among oxygentransport, RBC volume, and initiation ofbreathing, or predicts the effects ofearly versus delayed cord clamping.
practice.39 The development and use ofmodels to direct research reduces the riskthat a single factor, examined out of con-text, will direct interventions. The fol-lowing situation-specific model presentsa description of and explanation for thephysiologic processes of normal neonataltransition.
The hypothesis proposed is that a suc-cessful neonatal transition is dependentupon a newborn having an adequate bloodvolume to recruit the lung for respiratoryfunction through capillary erection andan adequate red cell volume to provideenough oxygen delivery to stimulate andmaintain respiration. The mechanism thatinitiates fetal breathing in utero is cur-rently unknown, but it is thought to besensitive to oxygen.9,40 This same oxygen-sensitive mechanism is the more likelycandidate to begin and maintain neona-tal breathing at birth. Capillary erectionmay also be important for other vulnera-ble structures in the neonate’s body. Theexplanation of origins for this model restsupon the development of an adequateblood volume in the neonate—a substan-tially greater blood volume than is neces-sary for the fetus during intrauterine life,when maternal “life support” obviates theneed for much fetal organ function.
This model for successful neonataltransition takes into account the researchfindings related to timing of cord clampingand the evidence for physiological mecha-nisms underlying this dramatic transitionto life after birth. The model is dia-grammed and the relevant documentationto support the model is summarized.
OVERVIEW OF THE MODEL
Figure 1 presents an overview of theBlood Volume Model for physiologic
P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
60 JOURNAL OF PERINATAL AND NEONATAL NURSING/MARCH 2002
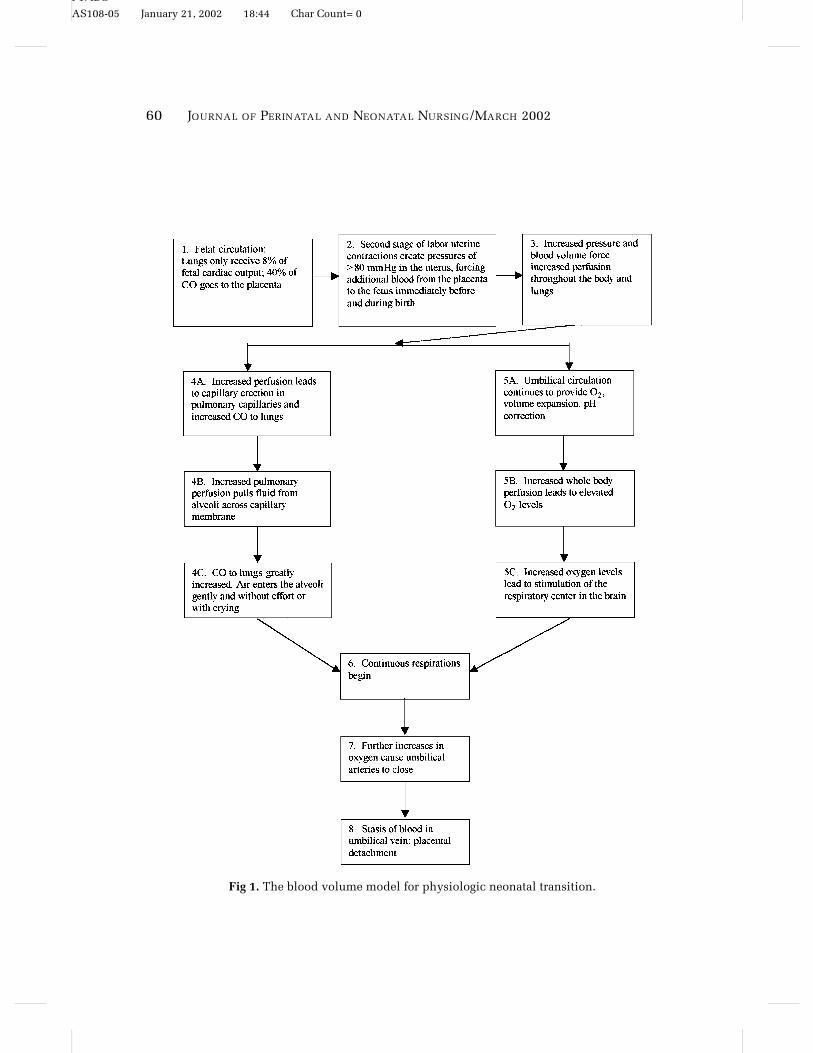
Fig 1. The blood volume model for physiologic neonatal transition.

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 61
neonatal transition. The following para-graphs detail the processes summarized inthe model.
In the fetal state, one third to one halfof the fetal-placental blood volume is inthe placenta (Step 1). The essential processof respiration, gas exchange, takes placein the placenta. Within the fetus, the pul-monary circulation receives only 8% of thecardiac output (CO). The vast majority ofblood volume contained within the fetussupports systemic circulation. There is noapparent indication that demands for sys-temic circulation decrease at the time ofbirth. In fact, the opposite is most likelytrue, as the gut and all other organs gainincreased function at birth. A dramatic in-crease in pulmonary circulation occurs,demanding 40% to 55% of the neonatalCO for extrauterine respiration. This tran-sition requires a redirection of the CO andan increase in blood volume if adequateperfusion to other vital structures is to bemaintained.
During birth, the uterine myometriumcontracts around the emptying uterinecavity, causing compression of the pla-centa and transfer of blood to the fetus/neonate (Step 2). Second stage contrac-tions generate intrauterine pressures of 80to 100 mmHg and force blood from the pla-centa to the fetus. This process is depen-dent on three factors: (1) a patent umbilicalvein; (2) a decrease in the blood volumeremaining in the placenta; and (3) an in-crease in the corporal fetal/neonatal bloodvolume, blood pressure, and oxygen lev-els. The rise in fetal/neonatal blood pres-sure (due to increased blood volume,Step 3) overrides the high pulmonary vas-cular resistance to begin the process oflung recruitment via capillary erection(Step 4). Increased blood pressure andblood flow cause the erection of alveo-lar capillaries that support the alveolar
structure and recruit the lung tissue.41 Es-sentially, a capillary network surroundseach alveolus as a collapsed, fluid-filledsphere in the fetal state. When the capillarynetwork is perfused at birth, hydrostaticpressure expands the sphere secondaryto increased pressure from full expansion(erection) of the capillary plexuses cover-ing each alveolus. Each alveolus, attachedto the capillary network through elasticfibers in the extracellular matrix, is pas-sively pulled open to an expanded state(see Fig 2) allowing effortless entry or air(Step 4C).42
The alveolus is further made ready forthe first breaths as lung fluid diffusesacross the alveolar-capillary membranes,driven by the higher colloid concentrationwithin the capillaries (Step 4B). When theunclamped umbilical cord continues topulsate, it allows the newborn to equili-brate blood volume, oxygen levels, andpH through ongoing placental exchange(Step 5A). The increased red blood cellflow raises the level of oxygen (Step 5B),stimulating the respiratory center toinitiate breathing—exactly the samemechanism used to initiate fetal breathingmovements in utero (Steps 5C and 6).Compression of the placenta continues asthe uterus empties, transferring more ofthe placental-fetal blood to the baby. Gasexchange and acid-base adjustment maycontinue during this transition. Whenthe oxygen level in the newborn’s venousblood is elevated from 15 mmHg (fetal lev-els) to 36 mmHg, the normal extrauterinelevel, the umbilical arteries close, shuttingdown any further blood flow from theinfant’s body to the placenta (Step 7). Thenext few uterine contractions may squeezea small amount of additional remainingblood through the umbilical vein to theinfant, ensuring maximum RBCs for oxy-genation and normal infant blood volume.

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
62 JOURNAL OF PERINATAL AND NEONATAL NURSING/MARCH 2002
Fig 2. Schema of respiratory unit: relationship of alveoli and capillary plexuses. Source: Copyright,1999. Icon Learning Systems, LLC, a subsidiary of Hava MediMedia USA Inc. Reprinted with per-mission from ICON Learning Systems, LLC, illustrated by Frank H. Netter, MD. All rights reserved.
Documentation and support for each stepin the model follow.
Documentation and References for Model
The following section presents the ra-tionale, documentation, and references forthe processes in the model shown inFigure 1. Each process in the model is re-iterated before discussion. Although cre-ation of a model allows for conjecture,most of the concepts included here arewell documented in published studies. Bynecessity, each step in the model is dis-cussed as though it happens in linear or-der, although, in fact, the model functionsin a recursive pattern until equilibrium isreached.
Step 1: In the fetal state, 40% of the COgoes to the placenta while only 8% goes tothe fetal lungs.
In the fetal state, one third (full-term) toone half (pre-term) of the blood in the fetal-placental circulation (FPC) at any pointin time is in the placenta fulfilling therespiratory function of gas exchange.2,17
Within the fetus, the circulation to thelungs receives 8% to 10% of the CO. A dra-matic increase of 32% to 47% in respira-tory circulation occurs at birth, demanding40% to 55% of the CO. Adequate perfusionof both the respiratory and systemic cir-culations in the neonate requires a partialtransfusion of the placental blood volumeto the neonate.

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 63
Step 2: Second stage uterine contractionscreate pressures of 80 mmHg or more inthe uterus, transferring blood volume tothe fetus.
Caldeyro-Barcia and colleagues43 docu-mented uterine contractions of approxi-mately 80 mmHg pressure within the uter-ine cavity as the fetus descends into thebirth canal. This pressure, exerted inter-mittently on the placenta acts to force addi-tional placental blood into the fetus duringcontractions before and immediately afterbirth while still allowing for fetal-maternalexchange between contractions.44 As theuterus extrudes the fetal head (one fourthof fetal mass) and body, it effectivelycompresses the placenta, causing more ofthe fetal-placental blood volume to trans-fer to the infant. The pressure of 80 mmHgis equal to Jaykka’s findings that pressuresof 80 mmHg are required to overcome thepulmonary vascular resistance in cadaver-ous fetal lungs45,46 (see below).
Step 3: Increased pressure on the pla-centa forces increased perfusion and be-gins to open the pulmonary vessels.
Increased uterine pressures of secondstage labor and birth may begin theprocess of increasing perfusion.43 Yao,Hirvensalo, and Lind documented in-creased placental transfusion in babies af-ter maternal contractions.44 Higher atrialand pulmonary artery pressures werefound in late-clamped (LC) versus early-clamped (EC) infants in the first few hoursafter birth, demonstrating increased perfu-sion and more pulmonary capillary fillingin the LC infants.25,26
Step 4A: Increased perfusion leadsto capillary erection in the pulmonaryvessels.
Jaykka’s45,46 physiologic adaptationtheory of capillary erection in the lungsoffers a logical explanation for the phe-nomenon of lung recruitment at birth.
Jaykka concluded that, at birth, the sud-den entry of blood under pressure intothe pulmonary capillaries that surroundeach alveoli causes the alveoli to becomeindividually symmetrically erect (re-cruited), thus easing entry of air. Jaykkadesigned an experiment to test theprocess of inflation using accompa-nying microscopic anatomy of thelung from stillborn infants and fetallambs. He tested the effect of inflationalone, the effect of forcing dye throughthe pulmonary artery to mimic pulmonaryperfusion, and a combination of these twomethods.
First, he inflated the lungs with air aloneand found that the expansion did not pro-ceed uniformly. He had difficulty injectingthe India ink to mimic capillary circulationwhen he attempted to do so after the in-flation. On microscopic examination,alveolar walls were found to be irregularand thin in shape and stretched aroundglobular air spaces with considerableareas remaining unstained (unrecruited),as demonstrated in Figure 3. Next, inother lungs, he forced India ink in thepulmonary artery at 80 mmHg pressureand found that the capillary system inthe excised lung became rigid or erectfrom the liquid forming a frameworkthat supported the respiratory unit. Theresulting microscopic picture resem-bled that of a normal aerated lung (seeFig 4). Last, he injected the India inkunder pressure first and then inflatedthe lungs. He needed much less pressureto inflate the lungs when the vascu-lar system was already distended withthe India ink. With these “perfused”lungs, he was able to inflate so muchair that the lungs became buoyant. Themicroanatomical picture of these lungsresembled those of a normally aerated lungand was similar to the lung that had been

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
64 JOURNAL OF PERINATAL AND NEONATAL NURSING/MARCH 2002
Fig 3. Inflation with air. Note irregular disten-sion with over-distended alveoli in one areaand atelectasis in other areas. Source: Reprintedwith permission from Acta Paediatr; 47, JaykkaS. Capillary erection and the structural ap-pearance of fetal and neonatal lungs, 484–500,1958.
experimentally treated with only liquidinjected into the vascular system underpressure (refer to Fig 5). He concludedthat this process of capillary erectionis an essential step in normal neonatalcardiopulmonary adaptation. In a modi-fication of this experiment, Avery47 alsofound that lungs were easier to inflate atlower pressures if they were first perfused.These studies support the concept thatthe establishment of normal neonatalrespiration is based on the adequate flowof blood into the lung bed.
Recent studies detailing ultrastructuraldevelopment of the lung in rats from fetalthrough neonatal stages seem to verifyJaykka’s work and, if anything, suggest thatadequate pulmonary blood flow maintainsan important role in effective respiratoryfunction from birth to some time after.48
In the rat lung, which is often used as
Fig 4. Thin section from lung with forcedcapillary distension using India ink. Source:Reprinted with permission from Acta Paediatr;47, Jaykka S. Capillary erection and the struc-tural appearance of fetal and neonatal lungs,484–500, 1958.
a model for the study of human lungstructure and function, three morpholog-ical phases precede the development ofa mature, alveolar lung. At term and forthe first few days after birth, the terminallung is in a saccular phase, with relativelysmaller air spaces and thick intrasaccularsepta containing multiple capillaries (seeFig 6). Not until seven days of life does thetypical alveolar structure begin to develop,with thin intra-alveolar septa in whichthere lies a single capillary in contact withthe air space on each side of the septum.The thick, vascular septa present at birthand for the following week may play animportant role in the structural support ofrespiratory function in early neonatal lifeand may be similar to what Jaykka saw

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 65
Fig 5. Capillary erection. Note distended, full capillaries bulging into the alveolar spaces. Source:Reprinted with permission from Acta Paediatr; 47, Jaykka S. Capillary erection and the structuralappearance of fetal and neonatal lungs, 484–500, 1958.
in his experiments (refer to Fig 4 andFig 5). Progress to normal alveolar struc-ture and function may rest upon adequatepulmonary blood flow. Further, the effi-ciency of gas exchange across the thickintrasaccular septa would necessarily belower than that in a mature alveolar lungand would likely function best in thepresence of generous pulmonary bloodvolume.
Step 4B: Increased pulmonary perfusionpulls lung fluid from the alveoli across thecapillary membrane.
Fetal lung fluid, which is in essence am-niotic fluid, contains very little proteinand has a low colloid osmotic pressure.Once the capillaries are filled with blood,which has a high colloid osmotic pressure,the alveolar fluid is rapidly absorbed into
the pulmonary capillaries. The fluid has tocross only one alveolar cell and one bloodcapillary cell, constituting a distance ofless than 2 µm (refer to Fig 2).49 Thus,the process of capillary erection is proba-bly an essential part of the rapid changefrom the “wet” lung of the fetus to the“dry” lung needed by the neonate for gasexchange. Capillary erection may be thestimulus for the lung to change both struc-ture and function immediately at birth
Capillary erection may be the stimulusfor the lung to change both structure andfunction immediately at birth from anorgan of fluid secretion to an organ ofgas exchange.

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
66 JOURNAL OF PERINATAL AND NEONATAL NURSING/MARCH 2002
Fig 6. Left: the lung of a 2-day-old rat newborn with saccular structure. Intrasaccular septa are thickwith capillaries located on both sides of the septa (large arrows). Right: Lung of a 21 day old rat new-born with alveolar structure. Alveolar septa are mainly thin; they accommodate only one capillary(small arrows). Original magnification X 400. Source: Reprinted with permission from Folia Histo-chemica et Cytobiologica, 36(1). Wasowicz M, Biczysko W, Marszalek A, Yokoyama S, Nakayama I.Ultrastructural studies on selected elements of the extracellular matrix in the developing rat lungalveolus, 3–13, 1998.
from an organ of fluid secretion to an or-gan of gas exchange.9
Step 5A: Umbilical circulation contin-ues to provide oxygenation, volume ex-pansion, and pH correction.
Significant blood flow in the umbilicalcord after birth can be palpated easilyand has been documented. Stembera andcolleagues50 developed a unique methodto study the actual volume of blood flow
through the human umbilical cord in thefirst few minutes after birth. From 113measurements of thermodilution taken be-tween 20 and 265 seconds after birthin 17 neonates, they were able to doc-ument blood flow of 248 mL/min inthe average 3 kg newborn (approximately75± 7 mL/min per kilogram). In the first100 to 120 seconds, the rate of flow didnot change in comparison with the first

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 67
reading at approximately 20 to 40 seconds.After 1.5 to 2 minutes, they found a markeddecrease of flow in most, but not all, cases.In distressed infants, they recorded a flowof 50 mL/min per kilogram.51 This studysupports the idea that the transition to ex-trauterine respiration may be made grad-ually and without undue stress, as theneonate is able to rely on blood flowthrough the placenta for oxygenation dur-ing the first minutes of life while blood vol-ume is equilibrating.
Yao and Lind18 clearly documented theincreased blood volume that occurs whenthe umbilical circulation is left intact.They estimated that 50% of the transfusionoccurs within one minute if the infantis at the level of the introitus and 100%by 3 minutes. Lowering the baby at least30 cm speeds the transfusion so that max-imum transfusion occurs in 1 minute.This additional blood volume has beenshown to increase perfusion,52 raise bloodpressure,11,12 and increase RBC deliveryto the vital organs.10 Higher blood pres-sures have been consistently documentedin preterm and full term babies with de-layed cord clamping by several sourcesin older23,24 and more recent studies.11,12
Arcilla et al26 have shown higher pul-monary artery pressures along with higherblood pressures in babies with delayedclamping.
Steps 5B and C: Increased systemic per-fusion leads to elevated oxygen levels thatinitiate continuous respiration.
Increased perfusion leads to better cap-illary distention,52 higher blood pre-ssure,11–13 and additional RBCs to carrymaximum oxygen.18 Increased oxygen lev-els have been shown to stimulate contin-uous fetal breathing movements in uterowhile the administration of low oxygengas mixtures to the ewe caused fetalbreathing to cease.40 Ventilation of fetal
lambs with 100% oxygen initiated contin-uous breathing.9 “Breathing [movements]can occur in the fetus [lamb] in the ab-sence of transient hypoxemia to stimulatethe chemoreceptors and without any ofthe sensory stimuli thought to be impor-tant for the establishment of continuousbreathing at birth.”9(p 1122) It is probablethat this adaptive process continues afterbirth to assist in initiating breathing inthe neonate. Babies who are well-perfusedbreathe spontaneously while pale, limp in-fants require resuscitation and often in-tubation. While this information appearscounterintuitive, suppression of breath-ing by low oxygen levels may be aphysiologic response in a stressed infant,assuming uninterrupted umbilical circula-tion. In this circumstance, the infant canrely on the placenta for essential oxy-genation while circulatory corrections aremade to establish adequate pulmonary per-fusion effecting capillary erection beforebreathing.
Steps 4C and 6: Air enters erect alveoligently or with crying and continuous res-pirations begin.
With placental gas exchange supportingthe neonate immediately after birth, thefirst breathing efforts may develop grad-ually and gently. Immediate cord clamp-ing may stimulate earlier, more aggressivebreathing efforts; however, these efforts arelikely to be ineffective at gas exchange andin fact may be counterproductive.53
A major hypothesis of this paper isthat time to accomplish capillary erec-tion is essential for adequate lung per-fusion. Capillary erection appears to beessential to the process of establishingextrauterine respiration. This is consis-tent with the finding that babies with de-layed cord clamping have been found totake the first breath later than babies withearly cord clamping.54 Evidence for this

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
68 JOURNAL OF PERINATAL AND NEONATAL NURSING/MARCH 2002
hypothesis is found in the work of Marquisand Ackerman,53 who devised a techniqueto examine placental respiratory functionin the immediate neonatal period. Theyclamped one umbilical artery (UA) im-mediately after birth and measured bloodgases. They clamped the second UA up to37 seconds after birth and found no changein the blood gases, even though several ba-bies had breathed over six times. They con-cluded that little gas exchange takes placein the neonate’s first few breaths. Dunn55
reported higher 5-minute Apgar scores ina group of babies with delayed clampingwhen compared to a similar group whohad early clamping. Thus, when the cordis left intact, the baby’s first cry may notoccur until there has been adequate trans-fer of blood volume to recruit the lung,fully perfuse the body, and stimulate therespiratory center with the higher oxy-
Fig 7. Cross section of early clamped umbilical cord on the left (within 10 sec) and late-clampedcord (over 3 min postpartum) on the right. Source: Reprinted from European Journal of Cardiology,Vol. 5/3, Lind J, Human fetal and neonatal circulation, 265–281, c© 1977; with permission fromElsevier Science.
gen levels. Even in babies who cry ear-lier, the first breaths are not effective at gasexchange.53
Step 7: Increased oxygen levels causeclosure of umbilical arteries and umbilicalcirculation ceases.
The umbilical arteries, but not the vein,are sensitive to oxygen and will closewhen adequate oxygenation is achieved.Figure 7 compares cross sections of earlyand late clamped umbilical cords showingclosure of the umbilical arteries after cordclamping at 3 minutes.56 McGrath et al57
examined sections of the umbilical cordexposed to oxygen and found that the ar-teries, but not the vein, were sensitiveto oxygen at 36 mmHg. After birth, oxy-gen tension in the venous circulation (um-bilical arteries) increases from the fetallevel of 15 mmHg to the neonatal levelof 40 mmHg. This rise in venous oxygen

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 69
is most likely an adequate stimulus to ef-fect closure of the umbilical arteries. In thephysiological range, increased oxygen didnot contract the umbilical vein that carriesoxygenated blood to the fetus/neonate.
It is likely that this same level ofoxygenation also begins to close othersimilar oxygen-sensitive structures, suchas the ductus arteriosus, thus promot-ing the transition to neonatal circulationand respiration. Buckels et al found mur-murs in all 17 early clamped babies andnone in the 15 late clamped babies theystudied.23 The increase in blood volumethat follows physiologic closure of theumbilical vessels is also likely to con-tribute to neonatal circulatory changes.Linderkamp19 states, “Studies in newbornlambs have shown that an increase of 50%in blood volume causes the ductus arte-riosus to close as a result of decreasingpressure gradient between the aorta andarteria pulmonalis.”(p.580) Thus, increasedblood volume, with its higher oxygen de-livery capacity, appears to support moresuccessful neonatal transition.
Cord pulsations may continue for sev-eral minutes after birth and can be read-ily palpated. The flow slows immenselybut does not close entirely in some cases,perhaps providing for further equilibra-tion if needed.50 Spontaneous closure ofthe umbilical arteries within a few min-utes after birth may be a protective mech-anism that would have guarded againstunregulated blood loss in newborns inmore primitive settings. The longer pa-tency of the umbilical vein may serve toprotect the most stressed infants and of-fer a small amount of additional RBCsand nutrients. Yao and colleagues44 docu-mented that maternal uterine contractionseffected complete placental transfusion byapproximately 3 minutes after birth. Thirdstage administration of oxytocic medica-
tion reduces that time by half, confirm-ing the role of the uterus in placentatransfusion.44
Step 8: Stasis of blood in the umbilicalvein occurs; the placenta separates.
Typically, the placenta separates fromthe uterus within a few minutes afterbirth. In the 1930s, Brandt,58 using dyeand X-rays, documented that the placentararely separated before 3 minutes. Whileseparation ends the exchange of gaseswithin the placenta, blood volume is stillavailable for the infant.
DISCUSSION
To date, our knowledge related to thephysiology of neonatal transition has beensegmented and scattered among differentdisciplines. The development of thismodel is an effort to synthesize what isknown into a whole. Its core concept isthat an uninterrupted umbilical circula-tion will assist in the establishment of anadequate blood volume to perfuse the bodyand an adequate RBC flow to oxygenateand stimulate the respiratory center.
The model underscores the value ofmaintaining umbilical circulation in thefirst minutes after birth. This approachprovides for adequate neonatal blood vol-ume and allows a gradual and gentle,but effective, physiologic transition to ex-trauterine breathing. This interpretation ofthe neonatal transition process runs con-trary to some long-held beliefs of many ob-stetric and pediatric care providers. Thesebeliefs often (and necessarily) have beenbased on limited or conflicting empiri-cal data. Reasonable consideration of thismodel will require reevaluating currentknowledge relevant to several related is-sues. These include beliefs about neonatalpolycythemia and jaundice and issues re-lated to neonatal resuscitation procedures.

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
70 JOURNAL OF PERINATAL AND NEONATAL NURSING/MARCH 2002
Neonatal Polycythemia and Jaundice
The belief that delayed cord clampingcauses polycythemia and jaundice willprobably be the single greatest obstacle toresearch on and acceptance of this model.Currently, this belief is so prevalent thatone often finds it stated in the literatureas accepted unreferenced fact.36,37,59 Con-cerns about the potential for polycythemiaand neonatal jaundice when cord clamp-ing is delayed were initially raised in pub-lications by Saigal et al60–61 who reportedsymptomatic polycythemia in 2 of 42 ba-bies held 30 cm (12 in) below the per-ineum for 5 minutes. In contrast, there arelarger studies from the 1960s and 1970sthat report no symptomatic polycythemiawhen infants were held at the level ofthe perineum and cord clamping wasdelayed until pulsations ceased.17,18,23–29
A comprehensive review of the literatureon cord clamping shows that most re-cent controlled trials do not support thisconcern.62
Polycythemia has long been a perplex-ing disorder that is difficult to manage andeven to diagnose. It does have associa-tions that are clearly unrelated to the tim-ing of cord clamping. Pregnancy compli-cations such as preeclampsia/eclampsia,maternal diabetes, small or large for ges-tational age conditions, and fetal geneticabnormalities all bear increased risk forneonatal polycythemia.37,38,63,64 Kurlat63
found that the risk of polycythemia inappropriate size infants of hypertensivemothers was 12.6-fold greater than that
The belief that delayed cord clampingcauses polycythemia and jaundice willprobably be the single greatest obstacleto research on and acceptance of thismodel.
of the general newborn population. Ina study of diabetic mothers, 5% of in-fants had polycythemia.65 Diagnostic dif-ficulties have persisted due to problemsrelated to the unreliability of labora-tory indicators for blood volume andhemoconcentration.65,66 The blood testmost commonly used for diagnosis, thehematocrit, can be influenced by factorsas simple as site of sampling or time oftesting.67,24
One new hypothesis has been put forththat may better explain the pathophysio-logic processes and lead to more effectivetreatment. Jones et al65 and Wardrop et al66
suggest that an elevated hematocrit oc-curs when hypoxia induces a failure of thevascular endothelial integrity, leading tocapillary leakage. This failure of the en-dothelium allows components of plasmasuch as salt, water, and albumin to leakfrom the intravascular space, causing a sec-ondary hemoconcentration and poor cor-relation between the hematocrit and bloodvolume.65,66 Their findings raise doubtsabout the results of older studies that usedalbumin markers such as radioactive I125
to measure blood volumes.17,19,60,61 Leak-age of tracer attached to albumin across thecapillary membranes would lead to falselyhigh blood volume results—especially insick or hypoxic infants.2,65,66
Polycythemia appears to be a multifac-torial problem—it occurs most often in ba-bies who have other serious problems—yetit is often assumed to be the cause,rather than a result, of any overarchingproblem.37 This scientific flaw, as Werner37
so aptly points out, causes polycythemia tocontinue to vex the neonatologists.
Issues Related to Neonatal Resuscitation
This model raises several issues relatedto neonatal resuscitation. These include

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 71
the development of techniques for bedsideresuscitation that dispense with the needfor immediate cord ligation, inquiry intothe possible risks of ventilation efforts thatprecede adequate pulmonary perfusion,and the potential of placental transfusionfor avoiding the need for volume expan-sion in resuscitative efforts.
Successful resuscitation can occur at theperineum with an intact umbilical cord. Inmany hospital settings, this would requirea new, but perhaps beneficial, interdisci-plinary team effort. A neonate can be keptwarm and dry and monitored for respira-tory effort, heart rate, and color on the bednearly as easily as anywhere else. Whenindicated, equipment for positive pressureventilation can be brought to the infant.Lowering the infant as much as cord lengthwill allow for 30 to 60 seconds while dry-ing the baby can speed placental transfu-sion and provide volume expansion beforeclamping the cord when it must happenquickly.18 Optimal management in caseswhere meconium is present in amnioticfluid needs further investigation. Immedi-ate clamping of the cord may be likely toinduce a first breath prior to adequate suc-tioning after birth. A better approach maybe to keep the baby unstimulated, withcord intact at the perineum, while the na-sopharynx is carefully suctioned.
Jaykka’s work decades ago suggested thatforceful ventilation prior to recruitmentof the lung brought about by pulmonaryperfusion and capillary erection damagedthe alveoli. Clark68 suggests that the lungsof ventilated newborns are most dam-aged when the lung is recruited and dere-cruited with each breath—exactly whatwould happen without adequate supportfrom the full capillary plexuses. Allowingtime and blood volume for adequate capil-lary perfusion and erection to occur, even(or perhaps especially) in premature in-
fants, may help protect the delicate tissueof the neonatal lung and promote effectiverespiratory function. The need for imme-diate intubation is under study for preterminfants.69
A poor response to resuscitative mea-sures in the delivery room is often at-tributed to neonatal volume depletion.70
The ideal volume expander, and theonly one with oxygen-carrying capacity,is whole blood. If one places a pale, limpbaby at the level of the perineum or lower,the baby will get about 10 mL/kg of wholeblood while resuscitation is being per-formed, as long as the heart rate is goodand the cord is pulsating.1
CONCLUSION
Since the beginning of mammalian life,young have been born attached to a life-line which supports their transition to ex-trauterine life. The process of birth invari-ably involves a period of maternal andneonatal rest before any active measure re-sults in a severing of the umbilical cord.There have been two exceptions to the nor-mal recovery process: human birth in somesettings of recent times, and the attendedbirths of thoroughbred foals.
In 1959, equine researchers Mahaffeyand Rossdale71 reported on an often fa-tal “convulsive syndrome” in newbornthoroughbred foals that occurred onlyto “foals born indoors, under humansupervision.”(p 1224) Human supervision offoaling at that time included rapid cordclamping, contrary to natural (unsuper-vised) settings, in which a mare and foaltypically rest for about a half hour. Thecord is then broken when either the mareor the foal rises. Pathology findings fromfoals that died of convulsive syndromeincluded an absence of aeration of thealveoli, with lung tissue so dense that it

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
72 JOURNAL OF PERINATAL AND NEONATAL NURSING/MARCH 2002
rapidly sank in fixative, and presence ofhyaline structures.72
Foal or baby, “human supervision” atbirth should, at the least, do no harm.While the United States remains at 25th73
in the worldwide ranking of infant mor-tality, with little change in the past sev-eral years, we must consider all possiblesources of potential harm to babies. A dif-ference in blood volume of 25% to 40% isnot insignificant. The current typical prac-tice of immediate cord clamping, espe-cially of those infants potentially in mostneed of additional red blood cells, needs tobe reconsidered.74 Examination of short-term and long-term neonatal outcomeswith variations in cord clamping practicesand methods of resuscitation is essential.These issues demand a better understand-ing of and respect for the normal physi-ologic processes involved in labor, birth,and the neonatal transition. Continued re-search on the issue of neonatal transitionfor full-term and premature infants and theeffect of cord clamping timing is urgentlyneeded.
In fact, the current knowledge baseis limited even to the extent that typ-ical practices and the beliefs on whichthey are based are mostly undocumented.
A survey of American certified nurse-midwives revealed that one-third feelstrongly that clamping should be delayeduntil the newborn has completed a suc-cessful transition.75 They believe that thisdelay allows time for the neonate to gentlymake the transition to extrauterine respi-ration and to self-regulate blood volume.Midwives who practice early clamping(26%) believe that delay has no benefitand often fear it will cause polycythemiaand jaundice.75 Similar descriptions ofpractices or beliefs among other groupsof obstetric and pediatric practitionersare not available. International practicesand experiences are not shared in theliterature.
Research-based evidence for practice islacking. Management of the umbilical cordat the time of birth is probably most fre-quently done without thought, and clamp-ing of the cord is often seen as merely atask. The presentation of the blood volumemodel for neonatal transition is a frame-work presented as an alternative to com-monly held beliefs. It is put forth in an ef-fort to encourage the application of criticalthinking to this potentially significant is-sue, and to foster and frame the researchthat will answer the questions raised.
REFERENCES
1. Morley G, Morley GM. Cord closure: canhasty clamping injure the newborn? OBGManage. 1998;7:29–36.
2. Wardrop CAJ, Holland BM. The rolesand vital importance of placental bloodto the newborn infant. J Perinat Med.1995;23:139–143.
3. Enkin M, Keirse M, Renfrew M, Neilson J.A Guide to Effective Care in Pregnancy andChildbirth, 2nd ed. Oxford: Oxford MedicalPublications; 1995.
4. Dixon LR. The complete blood count: phys-iologic basis and clinical usage. J PerinatNeonatal Nurs. 1997;11(3):1–18.
5. Gabbe SG, Niebyl JR, Simpson JL, (eds.)Obstetrics: Normal and Problem Pregnan-cies. New York: Churchhill-Livingstone;1996.
6. Cunningham FG, McDonald P, Gant N,et al. Williams Obstetrics, 20th Edition.Stamford, CT: Appleton & Lange; 1997,Chapter 16, p. 399.

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 73
7. Milner AD, Vyas H. Medical progress:Lung expansion at birth. J Pediatr.1982;101(6):879–886.
8. Adamson SL. Regulation of breathing atbirth. J Dev Physiol. 1991;15:45–52.
9. Rigatto H. Control of breathing in fetal lifeand onset and control of breathing in theneonate. In Polin R, Fox W, (eds). Fetal andNeonatal Physiology, 2nd ed. Philadelphia:WB Saunders; 1998.
10. Nelle M, Zilow E, Bastert G, LinderkampO. Effect of Leboyer childbirth on cardiacoutput, cerebral and gastro-intestinal bloodflow velocities in full term neonates Am JPerinatol. 1995;12:212–216.
11. Nelle M, Fischer S, Conze S, Beedgen B,Brischke EM, Linderkamp O. Effectsof later cord clamping on circulationin prematures (Abstract), Pediatr Res.1998;44:420.
12. Rabe H, Wacker A, Hulskamp G,Homig-Franz I, Jorch G. Late cord clampingbenefits extrauterine adaptation (Abstract).Pediatr Res. 1998;44:454.
13. Ibrahim H, Krouskop R, Lewis D,Dhanireddy R. Placental transfusion:umbilical cord clamping and preterminfants. J Perinatol. 2000;20:351–354.
14. Nelle M, Hocker C, Zilow E, Linderkamp O.Effect of red cell transfusion on cardiac out-put and blood flow velocities in cerebraland gastrointestinal arteries in prematureinfants. Arch Dis Child. 1994;71:F45–F48.
15. Kinmond S, Aitchison TC, Holland BM,Jones JG, Turner TL, Wardrop CA. Umbil-ical cord clamping and preterm infants: arandomized trial. BMJ. 1993;306:172–175.
16. Grajeda R, Perez-Escamilla R, Dewey K. De-layed clamping of the umbilical cord im-proves hematologic status of Guatemalaninfants at 2 months of age. Am Clin Nut.1997;65:425–431.
17. Usher R, Shephard M, Lind J. Blood volumein the newborn infant and placental trans-fusion. Acta Paediatr Scand. 1963;52:497–512.
18. Yao AC, Moinian M, Lind J. Distributionof blood between infant and placenta afterbirth. Lancet. 1969;626(2):871–873.
19. Linderkamp OL. Placental transfusion: de-terminants and effects. Clin Perinatol.1982;9:559–592.
20. Narenda A, Beckett C, Aitchison T, et al.Is it possible to promote placental transfu-sion at preterm delivery? (Abstract), Pedi-atr Res. 1998;44:453.
21. Nelle M, Zilow EP, Kraus M, Bastert G,Linderkamp O. The effect of Leboyer deliv-ery on blood viscosity and other hemorhe-ologic parameters in term neonates.Am J Obstet Gynecol. 1993;69(1):189–193.
22. Nelle M, Kraus M, Bastert G, LinderkampO. Effects of Leboyer childbirth on left- andright-systolic time intervals in healthy termneonates. J Perinat Med. 1996;24(5):513–520.
23. Buckels LJ, Usher R. Cardiopulmonary ef-fects of placental transfusion. J Pediatr.1965;67:239–246.
24. Oh W, Lind J. Venous and capillaryhematocrit in newborn infants and pla-cental transfusion. Acta Paediatr Scand.1966;55:38–48.
25. Arcilla RA, Oh W, Lind J, Blankenship W.Portal and atrial pressures in the newbornperiod. Acta Paediatr Scand. 1966;55:615–625.
26. Arcilla RA, Oh W, Lind J, Gessner IH. Pul-monary arterial pressures of newborn in-fants with early and late clamping of thecord. Acta Paediatr Scand. 1966;55:305–315.
27. Oh W, Oh MA, Lind J. Renal functionand blood volume in newborn infant re-lated to placental transfusion. Acta Paedi-atr Scand. 1966;55:197–210.
28. Oh W, Lind J. Body temperature of the new-born infant in relation to placental transfu-sion. Acta Paediatr Scand. 1967;172S:137–145.
29. Oh W, Lind J, Gessner IH. Circulatory andrespiratory adaptation to early and latecord clamping in newborn infants. ActaPaediatr Scand. 1966;55:17–25.
30. Linderkamp O, Nelle M, Kraus M, ZilowE. The effects of early and late cordclamping on blood viscosity and other

P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
74 JOURNAL OF PERINATAL AND NEONATAL NURSING/MARCH 2002
hemorheological parameters in full-term neonates. Acta Pediatr Scand.1992;81:745–750.
31. Yao AC, Lind J, Vuorenkoski V. Expiratorygrunting in the late clamped neonate. Pedi-atr 1971;48(6):865–870.
32. Yao AC, Lind J. Effect of early and late cordclamping on the systolic time intervals ofthe newborn infant. Acta Paediatr Scand.1977;69:489–493.
33. Oh W, Wallgren G, Hanson J, Lind J. Theeffect of placental transfusion on respira-tory mechanisms of normal term newborninfants. Pediatr 1967;40(1):6–12.
34. Daily W, Olsson T, Victorin L. Transtho-racic impedence: V. Effects of early andlate clamping of the umbilical cord withspecial reference to the ratio air-to-bloodduring respiration. Acta Paediatr Scan.1970;207(Suppl):57–72.
35. Yao AC, Lind J. Placental transfusion [Re-view]. Amer J Dis Child. 1974;127(1):128–141.
36. Oh W. Neonatal polycythemia and hyper-viscosity. Pediatr Clin North Am. 1986;33:523–532.
37. Werner EJ. Neonatal polycythemia andhyperviscosity. Clin Perinatol. 1995;22(3):693–710.
38. Kim HS. The Nature of Theoretical Think-ing in Nursing. New York: Springer Pub-lishing; 2000.
39. Im EO, Meleis AI. Situation-specific the-ories: philosophical roots, properties, andapproach. Adv Nurs Sci. 1999;22(2):11–24.
40. Baier RJ, Hasan SU, Cates DB, Hooper D,Nowaczyk B, Rigatto H. Effects of vari-ous concentrations of O2 and umbilicalcord occlusion on fetal breathing and be-havior. J Appl Physiol. 1990;68(4):1597–1604.
41. Netter F. Atlas of Human Anatomy. 2ndedition. East Hanover, NJ: Novartis; 1997.
42. Dunsmore SE, Rannels DE. Extracellularmatrix biology in the lung. Am J Physiol.1996;270(14):L3–L27.
43. Caldeyro-Barcia R, Alvarez H, ReynoldsS. A better understanding of uterine con-tractility through simultaneous recording
with an internal and a seven-channelexternal method. Surg Gynecol Obstet.1950;91:641–646.
44. Yao AC, Hirvensalo M, Lind J. Placentaltransfusion rate and uterine contraction.Lancet. 1968;539(1):380–383.
45. Jaykka S. Capillary erection and the struc-tural appearance of fetal and neonatallungs. Acta Paediatr. 1958;47:484–500.
46. Jaykka S. An experimental study of the ef-fect of liquid pressure applied to the cap-illary network of excised fetal lungs. ActaPaediatr. 1957;Supp 112:2–91.
47. Avery ME, Frank R, Gribetz I. The inflation-ary force produced by pulmonary vascu-lar distension in excised lungs. The pos-sible relation of this force to that neededto inflate the lungs at birth. J. Clin. Invest.1959;38:456–460.
48. Wasowicz M, Biczysko W, Marszalek A,Yokoyama S, Nakayama I. Ultrastructuralstudies on selected elements of the ex-tracellular matrix in the developing ratlung. Folia histochemica et Cytobiologica1998;36(1):3–13.
49. Van De Graaff KM, Fox SI. RespiratorySystem in Concepts of Human Anatomyand Physiology. Dubuque, IA: William C.Brown; 1992;Chapter 24.
50. Stembera Z, Hodr J, Janda J. Umbilicalblood flow in healthy newborn infants dur-ing the first few minutes after birth. Am JObstet Gynecol. 1965;91:568–574.
51. Stembera Z, Hodr J, Janda J. Umbilicalblood flow in newborn infants who suf-fered intrauterine hypoxia. Am J ObstetGynecol. 1968;101:546–553.
52. Pietra GG, D’Amodio MD, Leventhal MM,Oh W, Braudo JL. Electron microscopy ofcutaneous capillaries of newborn infants:Effects of placental transfusion. Pediatr.1968;42(4):678–683.
53. Marquis L, Ackerman B. Placental respira-tion in the immediate newborn period. AmJ Obstet Gynecol. 1973;117:358–363.
54. Yao A, Lind J. Placental Transfusion,Springfield, IL: Charles C. Thomas; 1984.
55. Dunn PM. Postnatal placental respiration.Dev Med Child Neurol. 1966;8:607–608.
P1: IBC
AS108-05 January 21, 2002 18:44 Char Count= 0
Neonatal Transitional Physiology 75
56. Lind J. Human fetal and neonatal circula-tion. Eur J of Cardiol. 1977;5/3:265–281.
57. McGrath JC, MacLennan S, Mann A, Stuart-Smith K, Whitle M. Contraction of humanumbilical artery, but not vein, by oxygen.J Physiol. 1986;380:513–519.
58. Brandt ML. Mechanism and man-agement of the 3rd stage of labor.Am J Obstet Gynecol. 1933;25:662–670.
59. Blackburn S, Loper D. Maternal, Fe-tal, and Neonatal Physiology. Philadel-phia: WB Saunders Company; 1992,Chapter 5, p. 191.
60. Saigal S, Usher RH. Symptomatic neonatalplethora. Biol Neonate. 1977;32(1–2):62–72.
61. Saigal S, O’Neill A, Surainder Y, Chua L,Usher R. Placental transfusion and hyper-bilirubinemia in the premature. Pediatr.1972;49(3):406–19.
62. Mercer J. Current best evidence: A re-view of the literature on umbilical cordclamping. J Midwifery Wom Health.2001;46(6):402–414.
63. Kurlat I, Sola A. Neonatal polycythemiain appropriately grown infants of hyper-tensive mothers. Acta Pediatr. 1992;81(9):662–664.
64. Codero L, Treuer SH, Landon MB, GabbeSG. Management of infants of diabeticmothers. Arch Pediatr Adolesc Med.1998;152(3):249–254.
65. Jones JG, Holland BM, Hudson IR, WardropCA. Total circulating red cells versushaematocrit as the primary descriptor ofoxygen transport by the blood. Br J Haema-tol. 1990;76(2):288–294.
66. Wardrop CAJ, Holland BM, Jones JG.Consensus on red cell transfusion. BMJ.1995;311:962–963.
67. Shohat M, Merlob P, Reisner S. Neonatalpolycythemia: 1. Early diagnosis and inci-dence relating to time of sampling. Pediatr.1984;71(3):7–10.
68. Clark R, Slutsky A, Gertsmann D. Lungprotective strategies of ventilation in theneonate: what are they? Pediatr 2000;105(1):112–114.
69. Lindner W, Vobeck S, Hummler H,Pohlandt F. Delivery room managementof extremely low birth weight infants:spontaneous breathing or intubation?Pediatr. 1999;103(5):961–967.
70. Bloom RS, Cropley C. AHA/AAP NeonatalResuscitation Program Steering Commit-tee. Textbook of Neonatal Resuscitation.Illinois: American Academy of Pediatrics;1995.
71. Mahaffey LW, Rossdale PD. A convulsivesyndrome in newborn foals resemblingpulmonary syndrome in the newborn in-fant. Lancet. 97:1223–1226.
72. Mahaffey LW, Rossdale PD. Convulsive andallied syndromes in newborn foals. VetRec. 1957;69:1277–1289.
73. Peristats, March of Dimes Perinatal DataCenter, 1998. Available at Modimes.org/HealthLibrary2/Infant-HealthStatistics/mortal.htm.
74. World Health Organization. Care in Nor-mal Birth: Report of the Technical WorkingGroup Meeting on Normal Birth. Geneva,Switzerland: World Health Organization,Maternal Health and Safe Motherhood Pro-gram; 1996.
75. Mercer J, Nelson C, Skovgaard R. Um-bilical cord clamping: beliefs and prac-tices of American nurse-midwives. JMidwifery Wom Health. 2000;45(1):58–66.