nepal report 2015 - home - · pdf file3 the world breastfeeding trends initiative wbti nepal...
TRANSCRIPT

1International Baby Food Action Network (IBFAN) AsiaBP-33, Pitam Pura, Delhi-110034, India
Phone: 91-11-27343608, 42683059 Fax : 91-11-27343606, E-mail: [email protected] , [email protected]
Website : www.worldbreastfeedingtrends.org
Nepal Report 2015
2
Name of the country: NepalYear: 2015
The World Breastfeeding Trends Initiative (WBTi)
Nepal Breastfeeding Promotion Forum(NEBPROF)
G.P.O. Box 2533, Kathmandu, NepalPhone: +977-1-4412202
E-mail: [email protected]

3
The World Breastfeeding Trends Initiative WBTi
Nepal Report 2015
Core Group:-• Prof. Dr. Prakash Sunder Shrestha
PresidentNepal Breastfeeding Promotion Forum (NEBPROF)
• Mr. Giri Raj SubediChiefNutrition Section, Child Health Division, Ministry of Health and Popula-tion (MOHP)
• Dr. Rameswar Man ShresthaChairmanKanti Hospital Development Committee
• Dr.Kalpana TiwariChairpersonNutrition Health Research & Community Services (NHRCS)
• Dr.Merina ShresthaAsst. Professor, Dept. of Child Health, Institute of Medicine (IOM)
• Dr. Srijana BasnetAsst. Professor, Dept. of Child Health, IOM
Prepared By:Dr.Kalpana TiwariDr.Merina ShresthaDr. Srijana Basnet
Published by:- Supported by:-
4
Acknowledgements
I am extremely thankful to all the member of Executive committee of Nepal Breastfeeding Promotion Forum (NEBPROF) for helping me to form the core group to conduct assessment of WBTi 2015.
I am very much grateful to the core group members Mr. Giri Raj Subedi, Chief, Nutrition Section Child Health Division, Dr. Rameswar Man Shrestha, Chairman, Kanti Hospital Development Committee, Dr. Kalpana Tiwari, Chairperson,. Nutrition Health Research & Community Services (NHRCS), Dr. Merina Shrestha, Asst. Professor Dept. of Child Health, IOM, Dr. Srijana Basnet, Asst. Professor Dept. of Child Health, IOM for their valuable efforts in going through the detail of available document to identify the gaps and come out with the valuable recommendation. My special thanks goes to Dr. Kalpana Tiwari, Dr. Merina Shrestha and Dr. Srijana Basnet for preparing the report card and detail report of WBTi 2015.
I would like to thank Dr. Rajendra Prasad Pant, Director Child Health Division, Dr. R.P. Biccha, Director, Family Health Division for their active participation in the WBTi 2015 workshop and their valuable suggestion.
I would also like to thank the partner organization and participants in WBTi 2015 workshop who have actively participated and given their valuable suggestion without which it won’t have been possible for us to prepare this report.
I would personally thank Dr. Arun Gupta, Founder and Central Coordinator, Breastfeeding Promotion Network India (BPNI), Dr. J.P. Dadhich, Regional Co-ordinator, Dr. Sobha Suri, Policy & Programme Coordinator and Ms. Beena Bhatta from BPNI for their continued encouragement and guidance for preparing this report.
Prof. Prakash S. ShresthaPresidentNepal Breastfeeding Promotion Forum

5
Preface
The Benefits of human milk for human infants are so obvious, and so well established, supported time and again by rigorous science that organization like IBFAN should not need to gather yet more figures, or mount yet more arguments for investing on breastfeeding. The simple stark facts are that breastfeeding saves lives, lack of human milk means human babies die.
This natural way of Nurturing the future was unfortunately wickedly, irresponsibly and even some would say, criminally under mind by those whose increasing hunger for profits promoted so called “breast milk substitute carelessly and callously all over the globe. Many thousands of babies die each year because they did not enjoy the benefit of breastfeeding and multiple thousands more grow up deprived of the many wonders of this special gift of god of nature and of the mother.
The persistent failure of governments to invest significantly in breastfeeding is hard to comprehend. Further quality of life is at issue. strong evidence from randomized trials show the average effect of early weaning from exclusive breastfeeding is to reduce a child IQ by 3-7 IQ points. This is comparable with prenatal lead exposure, with cognitive damage akin to several months of wasted schooling.
The Global Strategy set forth nine operational target related to both breastfeeding and complementary feeding. To track the progress of program through the implementation of the Global Strategy, the World Health Organization developed a tool for assessing national practice, policies and program in support of infant and young child feeding. The International Baby Food Action Network (IBFAN) Asia developed the WBTi to assess and monitor Infant and Young Child Feeding Practice, Policies and Program by developing a guideline for scoring and color rating assessment finding. In the beginning network of south asia decided to use tool in eight countries including Nepal. Later this assessment tool was used by different other countries for of their policies and programs on Infant and Young child feeding. The gaps, they found helped in advocacy which resulted in national actions. Finding and result of WBTi was shared with Global Breastfeeding Partners meeting, IBFAN Co-ordination Council meeting, IBFAN Strategic planning meeting in 2006. In 2008-2009 it became an integral and central part of the Global Breastfeeding initiative for child survival (gBICC) a joint IBFAN and WABA initiatives to enhance and generate new momentum of Infant feeding worldwide.
Till December 2015, WBTi has been introduced in 79 countries and More than 51 countries have already completed WBTi around in 2012.
Nepal Breastfeeding Promotion Forum (NEBPROF) has been conducting WBTi assessment since it was originally started in Eight South Asian Countries, till date we have completed four assessments (2005, 2008, 2012 & 2015). The WBTi report of 2015 has identified the existing gap with key factors associated with breastfeeding and complementary feeding practices. It has also come out with the possible recommendations which will be shared with the UN, organization, Government, Non Government organization and relevant stakeholders which will help in developing National Strategy and Plan of action on Infant and Young Child feeding to improve the nutritional status of Children in Nepal.
Prof. Prakash S. ShresthaPresidentNepal Breastfeeding Promotion Forum (NEBPROF)

6
Executive Summary
World Breast feeding trend initiative (WBTi) assessment of Nepal for the year 2015 report is accomplished in collaboration of the World Breast Feeding Trends Initiative (WBTi) of IBFAN Asia.
The WBTi serves as a lens to show gaps in policy and programmes and guide nation to initiate action to bridge the gaps. More than 51 countries have already completed WBTi around in 2012. The brain child of IBFAN Asia, WBTi is an integrated part of two global projects jointly funded by Norwegian Agency for Development Cooperation (NORAD) and Swedish International Development Cooperation Agency (SIDA).
Nepal Breastfeeding Promotion Forum (NEBPROF) had coordinated this 2015 assessment activity. This report reviewed relevant documents with intensive analysis of existing policy and programmes and its implementation in the country.
The core group critically reviewed key documents, websites and published information and interaction with key informants in the areas. The findings presented in the report is mainly within the scope of , the web based toolkit, WBTi guidelines, Nepal score 92.5 out of total 150 and stands in BLUE based in grid of RED, YELLOW, BLUE and GREEN in ascending order of performance or achievement.
Once the report was prepared by the core group, it was shared and discussed with larger group and consensus was achieved in identification of gaps and recommendations for bridging the gaps.
The report has found gaps in both policy and programme . The report 2015 has shown some improvement since 2012 assessment. However, more improvement was observed in the situation of IYCF in emergency and IYCF in HIV particularly in policy, strategies and guidelines.
The key findings for indicator 1-15 are summarized below. Major gaps and recommendations are reported for indicators 1-10. A comparative table is given for comparison of progress from 2008, 2012 and 2015 for indicator 11-15 (Table 1)
Indicator 1: National Policy, Programme and Co-ordinationConcerns national policy, plan of action, funding and coordination
Total score-7.5/10
Gaps:• Budgets had not been adequate for implementation of policy and programs
• Inadequate co-ordination mechanism though the Nutrition Technical Committee and Breast feeding promotion and protection committee (BPPC) at high level
Recommendations:• Strengthening for effective implementation of National Nutrition Policy and Strategy and
guidelines along with clear plan of action with budget allocation
• Strengthening of coordination mechanism between BPPC and Nutrition Technical Committee and inclusion of other sectors in the committee for effective implementation of all components of Breastfeeding.
Indicator 2: Baby Friendly Hospital Initiative (Ten steps to successful breastfeeding in the maternity services)
• Qualitative Criteria- concerns percentage of BFHI hospitals- 0/5

7
• Quantitative Criteria- concerns BFHI training, standard monitoring, assessment and reassessment system-0.5/5
Total score- 0.5/10Gaps:
• BFHI policy has not been completely adopted by hospitals and there is lack of monitoring of hospitals for BFHI.
• Though, large numbers of health staff had been trained on lactation management, still the training is not adequate for BFHI policy implementation throughout the country.
Recommendations:• There is an urgent need to revitalize BFHI hospitals.
• Regular preservice and in-service training of health staff on BFHI is needed. The training package like lactation management training should be integrated into national child health strategy.
• Regular monitoring of BFHI activities is required in health care setting and it should be incorporated in the national health programs for longterm sustainability.
Indicator 3: Implementation of the International CodeConcerns Legal Measures that are in Place in the Country, system of enforcement and monitoringTotal score- 5/10Gaps:
• Lack of Monitoring and enforcement of existing Act 2049 (1992 A.D) on the infant milk substitutes, feeding bottle and infant foods
• Inadequate understanding on IMS Act in all levels
• Inactive authority to implement BMS, lack of a system for monitoring practices and identifying violations and take actions.
Recommendations:All articles of the code as law and its regular monitoring and enforcement have to be implemented.The monitoring system for BMS situation and reporting violations should be developed.
Indicator 4: Maternity ProtectionConcerns paid maternity leave, paid breastfeeding breaks, national legislation encouraging work site accommodation for breastfeeding and/or childcare and ratification of ILO MPC No 183
Total score- 1/10
Gaps:• Weak policy and legislation regarding breastfeeding that covers employees in Government,
Private and informal sectors
• Maternity leave in governmental and private sector is inadequate.
• Inadequate provision of breastfeeding break/creche in all sectors including formal ones.
Recommendations:• Strengthening advocacy from governmental and non-governmental organization on maternity
protection act is needed.
• There should be increased awareness programs for women regarding maternity protection.
• Provision of breastfeeding break and places in formal and informal sectors is required.

8
Indicator 5: Health and Nutrition Care SystemsConcerns health provider schools and preservice education programmes, standards and guidelines for mother-friendly childbirth procedures, in-service training programmes.Total score- 5.5/10Gaps:
• Adequate number of health professionals has not received practical training on IYCF in pre-services education program.
• Health workers are not adequately trained on Code implementation.
Recommendations:• Implementation and integration of IYCF practical skills in curriculum of health professionals
• Lactation management training should be incorporated as a part of continuous medical education.
Indicator 6: Mother support and community based support for the pregnant and breastfeeding motherConcerns skilled counseling service on infant and young child feeding, and its access to all women (Dur-ing pregnancy and after birth)Total score- 6/10Gaps:
• There are inadequate services on counseling pregnant and breastfeeding mothers in outreach clinic
• Inadequate counseling and listening skills among community level workers
• Lack of crèche facilities in both government and private sectors.
Recommendations:• There should be more training on lactation management skills for village Level Health Workers
for comprehensive intervention on IYCF to support at community level or outreach clinic.
Indicator 7: Information SupportConcerns national IEC strategy for improving infant and young child feeding, actively implemented at local levelsTotal score-8/10Gaps:
• IEC materials are not adequate with emphasis on risks of artificial feeding.
Recommendations:• There should be increased number of IEC materials about the risk of artificial feeding.
• To promote IEC strategy electronic and print media should be utilized more.
Indicator 8: Infant Feeding and HIVConcerns policy and programmes to address infant feeding and HIV issues and on-going monitoring of the effect of interventions on infant practices and health outcomes for mother and infantsTotal score- 5.5/10Gaps:
• Inadequate advocacy and implementation of policy and guidelines at all levels.
• Lack of trainings to health workers on infant feeding in HIV.
• Lack of monitoring system to determine the effects of intervention to prevent HIV transmission through BF on infant feeding practices who are unknown of the situation.

9
Recommendations:• Review on existing situation of implementation of infant feeding in HIV is needed.
• Revitalized BFHI required inclusion of training on PMTCT
• Strengthen implementation of policy and strategies and initiate regular monitoring of it.
Indicator 9: Infant Feeding During Emergencies-Concerns policy and programmes on infant and young child feeding in emergencies and materials on IYCF in emergencies integrated into pre-service and in-service training for emergency managementTotal score- 9/10Gaps:
• Still there is inadequate human resources and implementation experiences in infant feeding during emergency.
Recommendations:• Advocacy for its inclusion in pre-service curriculum of medical and paramedical including
refreshment training in-service is required.
• User friendly separate IEC materials containing BMS code should be developed for emergencies.
Indicator 10: Mechanisms of Monitoring and Evaluation System-Concerns monitoring, management and information system (MIS) as part of planning and management processTotal score- 7/10Gaps:
• A national level monitoring and evaluation system has integrated three core BF indicators in program activities but there is lack of regular monitoring and evaluation in terms of baseline and follow –up data to measure outcomes.
Recommendations:• Initiation and establishment of regular monitoring and evaluation system with focus on key all
IYCF indicators suggested
• Integration of adequate indicators of complementary feeding into national health management information system by seggregation of data by age
Table 1: Comparison of Key Finding Indicators 11 – 15 of last three WBTi.S.N. Indicators 2008 2012 2015
1 Percentage of babies breastfed within a one hour of birth
35.4% 45% 45%
2 Percentage of babies<6 months of age exclusive breastfed in the last 2 years
53% 70% 70%
3 Babies are breastfed for a median duration of how many month
34 months 33.6 months 33.6 months
4 percentage of breastfed babies less than 6 month old receiving other foods or drinks from bottle in the last 24 hours
3% 6% 6%
5 Percentage of breastfed babies receiving complementary foods at 6-9 months of age
75 % 70% 70%
Gaps:• More than half of the newborn in Nepal have delay in initiation of breast feeding.
• Still only 2/3rd newborn are exclusively breastfed and/or had timely initiation of complementary

10
feeding.
• Small numbers of infants are still being fed by bottles.
Recommendations:• There should be effective action plan to improve initiation of breastfeeding practices emphasizing
initiation of breast feeding, exclusive breast feeding and timely initiation of complementary feeding.

11
Introduction
The World Breastfeeding Trends Initiative (WBTi) 2015 report presents detail finding on the 15 indicators of the tool, first 10 indicators are related to policy and programmes on infant and young child feeding and last five indicators are related to the Infant feeding practice in Nepal. The core group team used the WBTi tool and questionnaire to assess the national status on the implementation of the global strategy for Infant and Young Child Feeding. The existing gaps, identified in the report are the key factors for the improvement of breast feeding and complementary feeding policies, programmes and practice.
The report provides background information on the issues such as the role of breastfeeding and complementary feeding as key interventions to enhance nutrition development and survival of Infants and Young Children. The section about WBTi and the process describe the details how it works. The section on finding gives micro details of each indicator in the country with color coding. The reports focus on policies and programmes and provide objective scoring of the achievement of each indicator. The findings are based on county assessment conducted and agreed upon by the representative national team. The report analysis these findings in the context of current science and global guideline. The state of policy and programmes and presents a way forward and recommendation. It also describe the impact of the process, shows how the initiative has been an instrumental of changes in the country, lessons learnt from WBTi and way forward are also shared.

12
About WBTiWorld Breastfeeding Trends Initiative (WBTi) BackgroundThe World Breastfeeding Trends Initiative (WBTi) is an innovative initiative, developed by IBFAN Asia, to assess the status and benchmark the progress of the implementation of the Global Strategy for Infant and Young Child Feeding at national level.The tool is based on two global initiatives, the first is WABA’s (GLOPAR) and the second the WHO’s “Infant and Young Child Feeding: A tool for assessing national practices, policies and programmes”. The WBTi is designed to assist countries in assessing the strengths and weaknesses of their policies and programmes to protect, promote and support optimal infant and young child feeding practices. The WBTi has identified 15 indicators in two parts, each indicator having specific significance.
Part-I deals with policy and programmes (indicator 1-10)
Part –II deals with infant feeding practices (indicator 11-15)
1. National Policy, Programme and Coordination2. Baby Friendly Hospital Initiative (Ten steps to
successful breastfeeding)3. Implementation of the International Code of
Marketing of Breastmilk Substitutes4. Maternity Protection5. Health and Nutrition Care Systems (in support
of breastfeeding & IYCF)6. Mother Support and Community Outreach 7. Information Support 8. Infant Feeding and HIV9. Infant Feeding during Emergencies10. Mechanisms of Monitoring and Evaluation
System
11. Early Initiation of Breastfeeding12. Exclusive breastfeeding13. Median duration of breastfeeding 14. Bottle feeding15. Complementary feeding
Once assessment of gaps is carried out, the data on 15 indicators is fed into the questionnaire using the WBTi web based toolkit© which is specifically designed to meet this need. The toolkit objectively quantifies the data to provide a colour- coded rating in Red, Yellow, Blue or Green. The toolkit has the capacity to generate visual maps or graphic charts to assist in advocacy at all levels e.g. national, regional and international.
Each indicator used for assessment has following components; • The key question that needs to be investigated.
• Background on why the practice, policy or programme component is important.
• A list of key criteria as subset of questions to be considered in identifying achievements and areas needing improvement, with guidelines for scoring, colour-rating, and ranking how well the country is doing.
Part I: A set of criteria has been developed for each target, based on Global Strategy for Infant and Young Child Feeding (2002) and the Innocenti Declaration on Infant and Young Child Feeding (2005). For each indicator, there is a subset of questions. Answers to these can lead to identify achievements and gaps in policies and programmes to implement Global Strategy for Infant and Young Child Feeding . This shows how a country is doing in a particular area of action on Infant and Young Child Feeding.

13
Part II: Infant and Young Child Feeding Practices in Part II ask for specific numerical data on each practice based on data from random household survey that is national in scope.
Once the information about the indicators is gathered and analyzed, it is then entered into the web-based toolkit through the ‘ WBTi Questionnaire’. Further, the toolkit scores and colour- rate each individual indicator as per IBFAN Asia’s Guidelines for WBTi.

14
Background Nepal context
Nepal has made considerable progress to reduce infant mortality over the last 15 years. Nepal is in track to achieve the Millennium Development Goals for maternal and child morbidity. Significant improvements have also been made in child nutrition and breastfeeding practices have improved in the last five years. However its sustainablility in urban and rural is a challenge. Currently infant mortality rate in Nepal is 46 per 1,000 live births (NDHS, 2011). However, this figure is still high, masks disparities within the regions and ecologies, and there is a concern that the rate of decline in infant mortality has slowed over the last five years. Furthermore, neonatal mortality has remained stagnant over the same time period and is representing more than two-third of infant deaths. The prevailing serious level of child under-nutrition in the country is one of the major contributing factors. Therefore, without significant improvement especially in young child nutrition, accelerated reduction of infant and neonatal mortality (MDG 4) is not likely to be achieved in the country; accelerated attainment of all the other MDGs is also under threat.
In Nepal, growth impairment associated with poor nutrition occurs primarily during the first two years of life, a period when adequate nutrient intake is needed to avoid lifelong effects of malnutrition (HKI, Nepal, 2010). Despite improvements in the nutritional status of children in Nepal over the last 15 years, 41% of Nepalese children less than five years of age are stunted, 11% are wasted and 39% are underweight (NDHS 2011).
The Nepal Demographic Health Survey NDHS 2011 indicates that exclusive breastfeeding in children has increased to 70 percent from 53% in 2006, and almost all children are still breastfed at 2 years of age. Prelacteal feeding has fallen such that only 28% of children receive a pre-lacteal and 85% of children have initiated breastfeeding within 24 hours of birth. Although breastfeeding practices have improved, there is still need to improvement, initiation of breastfeeding within one hour of birth which is currently only 45% and only 70% of children are exclusively breastfed. In order to sustain the achievement made in Initiation of breastfeeding within an hour of birth needs activities addressing avoidance of prelacteal feeding practices and provision of support for initiation of breastfeeding at hospitals to community level. Children under six months who are not exclusively breastfeeding are consuming water, other milks and complementary foods, in roughly equal proportions, in addition to breast milk. It is interesting to note that about 20% of infants 2-3 months old are given water or other milks in addition to breast milk (NDHS 2011).
Breastfeeding is prevalent in Nepal, where 70% of infants under six months of age are exclusively breastfed (NDHS 2011). Continued breastfeeding up to 24 months of age is also high; ninety-three percent of infants 12-15 months of age are breastfed in Nepal, with the rate of breastfeeding remaining high for children 21- 23 months of age. However, pre-lacteal feeding is common; approximately 28% of Nepalese children residing in urban areas have been fed something other than breast milk in the first three days after birth (MOHP, 2011).
Additionally, complementary feeding practices in Nepal show room for improvement. Early introduction of complementary foods, which has the potential to negatively affect a child’s nutritional status by displacing breast milk in the diet, is common in Nepal; three percent of breastfeeding children aged 2-3 months receive some kind of solid or semisolid food, a figure which rises to 23% by 4-5 months of age (MOHP, 2011). With regard to infant and young child feeding (IYCF) minimum standards, which account for dietary diversity, feeding frequency and consumption of breast milk, milk or other milk products, only 37% of children in urban households and 24% of Nepalese all overall are fed in accordance with recommended practices (MOHP, 2011).
15
National Commitments
Nepal has made several commitments in line with global commitments related to the survival, adequate nutrition, growth and development of infants and children as fundamental rights.
A national consensus for a multi-sectoral action plan address for reduction of chronic malnutrition in Nepal and it focuses on actions needed to improve maternal and child nutrition, accessible to everyone, especially during the first 1,000 days of life, ensuring equity, and facilitating access to information, to promoting behaviour change, with a focus to reach the most marginalized, poorest segments of the population, and taking into account gender related factors. Government prioritizes and that there is a strong link between poverty reduction, food insecurity and nutrition and chronic malnutrition.
The Nepal Strategy for Infant and Young Children Feeding been developed in line with the Nepal multi-sector nutrition plan (2013-2017) and is in final stage. The strategy has identified comprehensive actions that are crucial for improving infant feeding in the country. It has focused on the need to act upon the implementation of advocacy, policy, partnership and coordination to enhance political commitments in support of improving all components of IYCF including legislation and standards to protect promote and support IYCF including breastfeeding and BFHI/CBFI in country.
Strategic communication approach is taking and integrated approach to health for women and children, focusing on the critical time from pregnancy through the first 1000 days of a baby’s life. Health Priority linked to MNCH includes newborn care, early initiation and exclusive breastfeeding (Communication Strategy 2011-2016).
Promotion of breastfeeding and behavior-change communication for improved complementary feeding is also addressed in National Communication Strategy and National HIV/AIDs strategies.
Improving infant and young child feeding is one of the most important nutrition strategies for Nepal however; efforts in this area are fragmented and not intensive. Although exclusive breastfeeding has improved substantially since 2006, there is no data on what has caused this improvement as effective monitoring and evaluation system is weak, and none of the recent efforts to improve IYCF practices have been evaluated at national level.
Therefore, this assessment finds that IYCF interventions helps to prioritize intervention be refined interventions and intensified implementations at all level. The national IYCF strategy needs to be strengthened to be more comprehensive and detailed and efforts need to be made for its implementation at local levels.
The assessment felt the gap of national commitment mainly for an oversight and coordinating structure of fully operation and functional high level within the National Technical Committee on Nutrition. Emphasis needs to be placed on building up the capacity of the health system to provide quality skilled counseling and support to caregivers and their families for improved IYCF behaviors .World Bank Review 2012 on IYCF also recommends in line with this gap. The existing National Committee on promotion, protection and support for breastfeeding should be reactivated and coordinated with Nutrition Technical Committee currently existed under Child Health Division, Ministry of Health and Population.

16
Assessment process followed by the country
First a core group of 6 persons was formed, by bringing together stakeholders including government, professional bodies, civil society organizations and institute of medicine. A coordinator was identified to lead the process. The core group well understood the indicators of the assessment and questionnaires available at WBTi website.
Coordination at National level was the major part of the assessment which was very well undertaken by Nepal Breastfeeding Promotion Forum (NEBPROF). The Core Group was comprised of 6 persons:
1. Prof. Prakash S. Shrestha
2. Mr Giri Raj Subedi
3. Dr. Rameshwor Man Shrestha
4. Dr. Kalpana Tiwari Pant
5. Dr. Merina Shrestha
6. Dr. Srijana Basnet
The core group met several times to discuss each issues in details. Then the core group studied and assesses each indicator, list findings and identified existing gaps. In order to share the findings in the the larger group of the country and to achieve consensus, the National Workshop was organized on 14th March 2016.
Dr. Kalpana Tiwari highlighted on the background of WBTi, global situation and its initiation in Nepal - Annex 1. Dr. Srijana Basnet shared on the situation and scores under the each indicator – Annex 2. Workshop Schedules is attached (Annex – 3).
Based on the presentations and working experiences of the stakeholders, the discussion was initiated and facilitated by Dr. Prakash Sunder Shrestha. All the members present in the workshop, actively participated in the discussion and all the inputs given in workshop by participants and members were incorporated in the report.
The participant intensively discussed on the score and verification of each finding on the each indicator was done. Consensus was build on the findings and recommendations on how to bridge the existing gaps for each indicator was finalized.
17
List of the partners for the assessment process
(Details reported in Annex – 4)
Ministry of Health, Child Health Division
Nepal Paediatric Society, Perinatal Society (NEPAS)
Department of Paediatrics, Institute of Medicine, Teaching Hospital
Maharajgunj Nursing Campus
Kanti Children’s Hospital
Mother and Infant Research Activity (MIRA)
Nutrition Health Research & Community Services (NHRCS)
Civil service hospital
Helen Keller International (HKI)

18
Assessment Findings
Indicator 1: National Policy, Programme and Coordination
Key question: Is there a national infant and young child feeding/breastfeeding policy that protects, Promotes and supports optimal infant and young child feeding and the policy is supported by a Government programme? Is there a mechanism to coordinate like National infant and young child feeding committee and a coordinator for the committee?
Background:The Innocenti Declaration recommended (1990) that all governments have national breastfeeding committee and coordinators as established mechanism to protect, promote and support breastfeeding in the country. Further, in 2000, The World Summit for Children recommended to develop national breastfeeding policies in the country. Similarly, The Global Strategy for Infant and Young Child Feeding calls for urgent action from all member states to develop, implement, monitor and evaluate a comprehensive policy on IYCF. The indicator 1 deals with issues related to national policy and IYCF, national plan of action based on the national policy, national breastfeeding committee and financial allocations for IYCF. The larger group agreed that the country has a national IYCF policy and has approved by the government. National policy promotes early initiation, exclusive breastfeeding for the first six months, complementary feeding initiated after completion of six months, and it also promotes to continue breastfeeding to at least 2 years. A noticeable progress in this period is that a concrete national Plan of Action has been included into the policy. In last five years it was observed that a plan of action was developed with costing for its effective implementation. However, currently in IYCF is the high national priority. IYCF activities are integrated in large scale projects funded by USAID. Multi-sectoral Nutrition Plan of National Planning Commission targets to Golden 1000 days of human life in the highest priority that has led breastfeeding agenda in all sector plan of different ministries as nutrition sensitive and specific interventions in the country (MSNP 2010)
A separate comprehensive national IYCF strategy is in the process of developed and endorsed by the government. The table below depicts the existing situation of National Policy, Program and Coordination in Nepal.
National level Breastfeeding Promotion and Protection Committee (BPPC) has committed for regular meeting and activated recently. However, there is IYCF committee under Nutrition Technical Committee under Nutrition Section Child Health Division and it meets as per the need. It takes care of Breastfeeding and infant feeding linking with other IYCF activities such as MNP, CMAM, IMAM and CBIMCI. A coordinator responsible for Nutrition Technical Committee is also responsible to coordinate on IYCF including breastfeeding. The group agreed upon the terms of reference of coordinator also take care the issues related to breastfeeding. Nutrition Technical Committee links with other sectors like health, nutrition, information effectively through MSNP representation of Nutrition Section and Child Health Division.
19
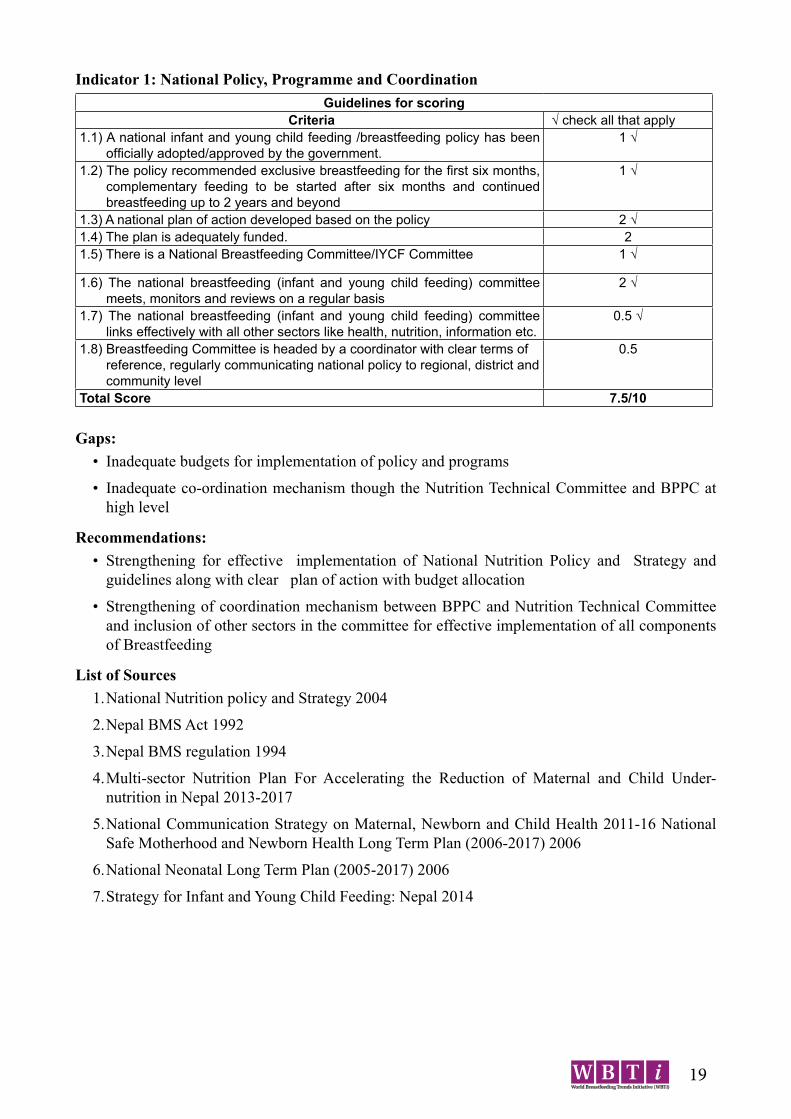
Indicator 1: National Policy, Programme and Coordination Guidelines for scoring
Criteria √ check all that apply1.1) A national infant and young child feeding /breastfeeding policy has been
officially adopted/approved by the government.1 √
1.2) The policy recommended exclusive breastfeeding for the first six months, complementary feeding to be started after six months and continued breastfeeding up to 2 years and beyond
1 √
1.3) A national plan of action developed based on the policy 2 √ 1.4) The plan is adequately funded. 21.5) There is a National Breastfeeding Committee/IYCF Committee 1 √
1.6) The national breastfeeding (infant and young child feeding) committee meets, monitors and reviews on a regular basis
2 √
1.7) The national breastfeeding (infant and young child feeding) committee links effectively with all other sectors like health, nutrition, information etc.
0.5 √
1.8) Breastfeeding Committee is headed by a coordinator with clear terms of reference, regularly communicating national policy to regional, district and community level
0.5
Total Score 7.5/10
Gaps:• Inadequate budgets for implementation of policy and programs
• Inadequate co-ordination mechanism though the Nutrition Technical Committee and BPPC at high level
Recommendations:• Strengthening for effective implementation of National Nutrition Policy and Strategy and
guidelines along with clear plan of action with budget allocation
• Strengthening of coordination mechanism between BPPC and Nutrition Technical Committee and inclusion of other sectors in the committee for effective implementation of all components of Breastfeeding
List of Sources1. National Nutrition policy and Strategy 2004
2. Nepal BMS Act 1992
3. Nepal BMS regulation 1994
4. Multi-sector Nutrition Plan For Accelerating the Reduction of Maternal and Child Under-nutrition in Nepal 2013-2017
5. National Communication Strategy on Maternal, Newborn and Child Health 2011-16 National Safe Motherhood and Newborn Health Long Term Plan (2006-2017) 2006
6. National Neonatal Long Term Plan (2005-2017) 2006
7. Strategy for Infant and Young Child Feeding: Nepal 2014

20
Indicator 2: Baby Friendly Care and Baby-Friendly Hospital Initiative (BFHI) (Ten Steps to Successful Breastfeeding)The Innocenti Declaration calls for all maternity services to fully practice all the Ten Steps to Successful Breastfeeding set out in Protecting, Promoting and Supporting Breastfeeding: the special role of maternity services, a Joint WHO/UNICEF Statement. The Global Strategy for Infant and Young Child Feeding indicates that revitalization of BFHI is necessary and its assessment is also carried out periodically to sustain this programme and contribute to increase exclusive breastfeeding .BFHI was launched in 1989 by UNICEF and WHO to ensure that hospitals protect, promote and support breastfeeding. BFHI means practicing of ten steps to successful breastfeeding which includes written breastfeeding policy, training all health staff including lactation management, inform all pregnant women about the benefits of breastfeeding, supporting mothers for initiation of breastfeeding within an hour of birth even in case of cesarean sections and establishing breastfeeding support groups in the community.
In Nepal BFHI activities were started in 1994 with the training of health workers from 22 hospitals all over the country till 1996. After training, these hospitals were assessed by external and internal assessors in 1997-98 through Nepal Pediatric Society and seven of the hospitals were certified as Baby Friendly Hospitals. These seven hospitals were: Tribhuvan University Teaching Hospital, Maharajgunj,Kathmandu, Maternity Hospital, Thapathali, Kathmandu,Patan Hospital, Lalitpur, Bhaktapur Hospital, Bhaktapur, Hetauda Hospital, Makawanpur, BP Koirala Institute of Health Science, Dharan and Koshi Zonal Hospital, Bitratnagar.
Although there is a need of continuous monitoring and supervision of BFHI activities to ensure proper implementation, it was about 13 years that no any monitoring and assessment activities were carried out in Nepal. In 2011, an assessment was carried out in all of the 7 BFHI hospitals initiated by Child Health Division, Department of Health Services which used the revised tools developed by WHO/ UNICEF. For the assessment, interview was done with Head of the Institutions, hospital staffs, pregnant women and lactating mothers and observation in different units of the hospitals, followed by a market survey. The study drew some interesting findings. All the hospitals certified as BFHI were found not fulfilling all the 10 steps of BFHI activities. There was no display of policy on BFHI in the hospitals, health workers were very limited or were not trained, demand feeding was not strictly followed and mother support group or mother friendly care did not exist in any of these hospitals but these hospitals had good practice of rooming-in and pacifier and teats were not provided to newborns. Pre test counseling on HIV testing was not done for all pregnant mothers. Proper counseling on infant feeding was not done to HIV positive mothers. Hospital staffs were not aware of international code of Breast Milk Substitutes (BMS). BMS were abundantly available in the pharmacies around the hospital and in the market. Some of the BMS products were found violating the International Code of Breast Milk Substitutes.
There could be many reasons for not fulfilling the ten steps of BFHI by hospitals in Nepal. The main reason could be lack of monitoring and supervision activities since a long time, from the time the hospitals were certified. Transfer of almost all the trained staffs and lack of training to the new staffs could be the other reason. Reluctance of the hospital administration and concerned government authority and less priority on breastfeeding could be the other possible reasons.
21
BFHI activities in Nepal in past 3 years
Lactation Management TrainingMoHP in collaboration with Hellen keller international had conducted several trainings on lactation management for hospital workers. In total, 575 health workers from 10 hospitals1 of Kathmandu Valley were trained, which mostly included nurses working in maternity ward and few medical officers. The training content focused on increasing knowledge and skills in Lactation Management in Early Postpartum for hospital staff in order to support mothers to optimally breastfeed their newborns in the early postpartum period. The organization had plan to conduct similar training throughout Nepal as well.
Similarly Nepal breast feeding promotion forum conducted two master trainings on infant and young child feeding in the year 2014 and 2015. Total of 67 health workers working at different hospitals in Kathmandu velley were trained on IYCF.
Interaction program on BFHIThe Civil Society Alliance for Nutrition, Nepal (CSANN) organized an interaction programme with the objective to advocate hospital staffs on baby Friendly Hospital Initiative (BFHI) components and bring a discussion for creating favorable environment to protect, promote and sustain breastfeeding. The specific objectives of the event are: To orient hospital staffs on components of baby friendly hospital initiatives and interact with hospital staffs on hospital situation/practice to implement BFHI components; To celebrate the breastfeeding week 2015 with slogan of the year and To engage media and journalist for campaigning on BFHI.
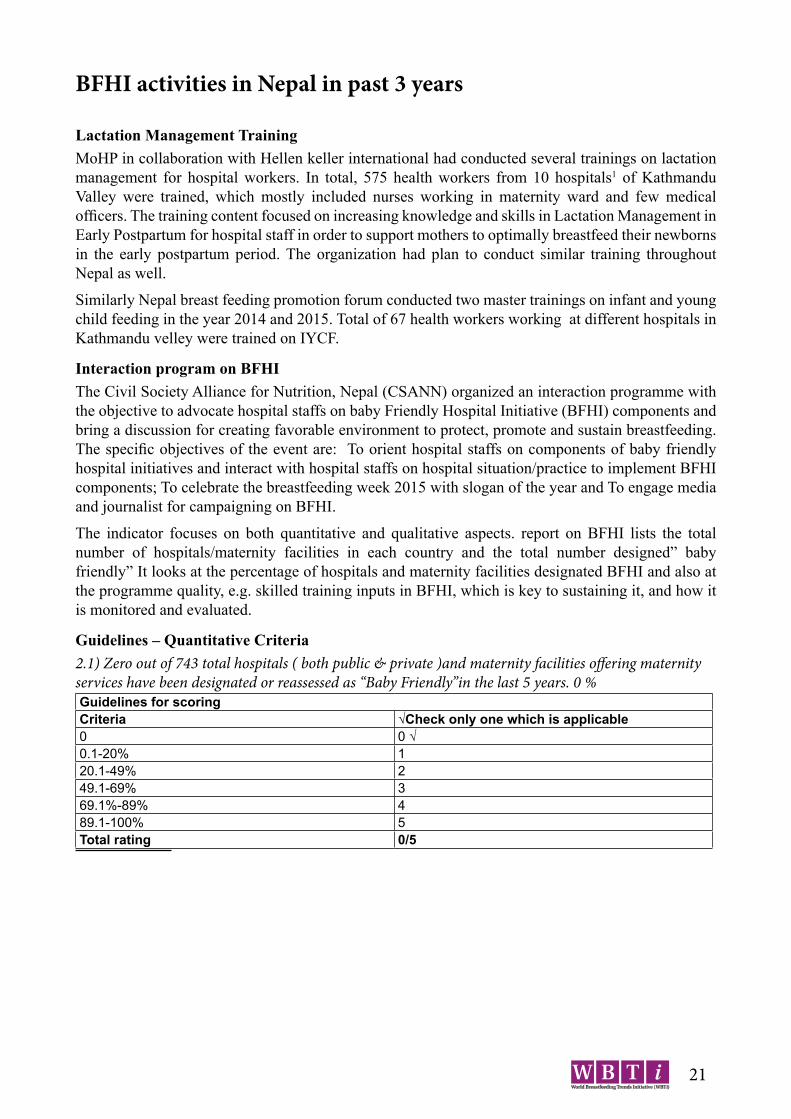
The indicator focuses on both quantitative and qualitative aspects. report on BFHI lists the total number of hospitals/maternity facilities in each country and the total number designed” baby friendly” It looks at the percentage of hospitals and maternity facilities designated BFHI and also at the programme quality, e.g. skilled training inputs in BFHI, which is key to sustaining it, and how it is monitored and evaluated.
Guidelines – Quantitative Criteria2.1) Zero out of 743 total hospitals ( both public & private )and maternity facilities offering maternity services have been designated or reassessed as “Baby Friendly”in the last 5 years. 0 %Guidelines for scoringCriteria √Check only one which is applicable0 0 √0.1-20% 120.1-49% 249.1-69% 369.1%-89% 489.1-100% 5Total rating 0/5
22
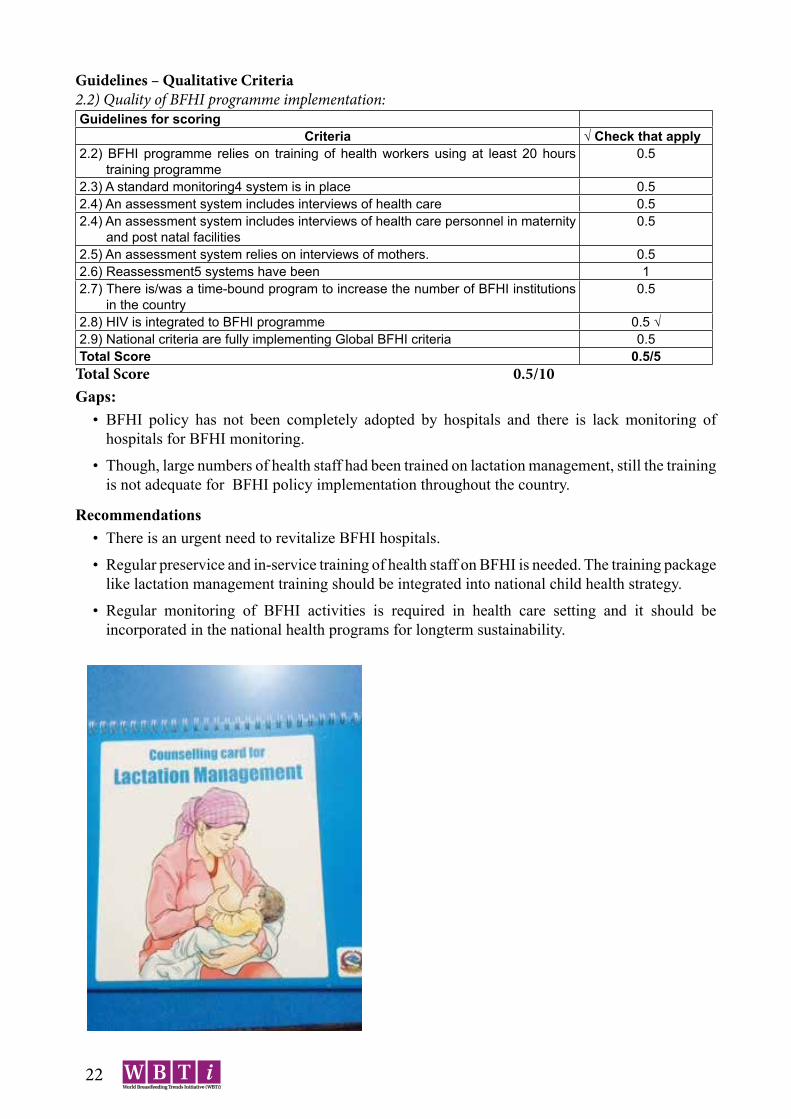
Guidelines – Qualitative Criteria2.2) Quality of BFHI programme implementation:Guidelines for scoring
Criteria √ Check that apply2.2) BFHI programme relies on training of health workers using at least 20 hours
training programme0.5
2.3) A standard monitoring4 system is in place 0.52.4) An assessment system includes interviews of health care 0.52.4) An assessment system includes interviews of health care personnel in maternity
and post natal facilities0.5
2.5) An assessment system relies on interviews of mothers. 0.52.6) Reassessment5 systems have been 12.7) There is/was a time-bound program to increase the number of BFHI institutions
in the country0.5
2.8) HIV is integrated to BFHI programme 0.5 √2.9) National criteria are fully implementing Global BFHI criteria 0.5Total Score 0.5/5
Total Score 0.5/10Gaps:
• BFHI policy has not been completely adopted by hospitals and there is lack monitoring of hospitals for BFHI monitoring.
• Though, large numbers of health staff had been trained on lactation management, still the training is not adequate for BFHI policy implementation throughout the country.
Recommendations• There is an urgent need to revitalize BFHI hospitals.
• Regular preservice and in-service training of health staff on BFHI is needed. The training package like lactation management training should be integrated into national child health strategy.
• Regular monitoring of BFHI activities is required in health care setting and it should be incorporated in the national health programs for longterm sustainability.

23
List of Sources1. Shrestha PS et al. Assessment and Strengthening the Implementation of the Code on Breast Milk
Substitutes and the Baby Friendly Hospital Initiative (BFHI), 2011. Child Health Division, MoHP.2. Key activities of Assessment and Research on Child Feeding (ARCH) project of Helen Keller
International (HKI)3. Interaction program on Baby Friendly hospital Initiatives (BFHI) with hospital staffs. Nepal
nutrition and food security portal. Downloaded from www. Nnfsp.gov.np/portalcontent.aspx4. www. Hki.org/sites/default/ files/attach/2015/17/Nepal HSS Country Report_Final_Sept5 (2) (2).
pdf5. Report on Master training on IYCF conducted at Kathmandu, Nepal. www.bpni.org/traing/TOT-
Report-Delhi.pdf6. Annual report. Department of health services 2070/71, Govt of Nepal.

24
Indicator 3: Implementation of the International Code of Marketing of Breast milk SubstitutesThe Innocenti Declaration calls for all governments to take action to implement all the articles of the International Code of Marketing of Breast Milk Substitutes and the subsequent World Health Assembly resolutions. The aim of the Code is to contribute to the provision of safe and adequate nutrition for infants, by the protection and promotion of provision of safe and adequate nutrition for infants, by the protection and promotion of breastfeeding, and by ensuring the proper use of breast milk substitutes, when these are necessary, on the basis of adequate information and through appropriate marketing and distribution. The “State of the Code by Country” by the International Code Documentation Centre (ICDC) on countries’ progress in implementing the Code provides sufficient information on the action taken.
Nations are supposed to enact legislation as a follow-up to this. Several relevant subsequent World Health Assembly resolutions, which strengthen the International Code of Marketing of Breast milk Substitute have been adopted since then and have the same status as the Code and should be considered. The Global Strategy for Infant and Young Child Feeding calls for action on this target.
The table below highlights the existing situation of implementing of the International Code in Nepal. Nepal has national legislation on the marketing of breast milk substitutes which was passed in 1992 and it is supported by national Regulation that was passed in 1994. The scope of the Act defines breast milk substitutes as “any food marketed for partial or total replacement of breast milk”
In exercise of the powers conferred by Section 17 of the Mother’s Milk Substitutes (Control of Sale and Distribution) Act, 1994 (2051), Government of Nepal has framed rules which is cited as “Mother’s Milk Substitutes (Control of Sale and Distribution) Regulation, 1994 (2051)”. Under the mother’s milk substitute rules of Nepal, Nepal Government has formed a Breast Feeding protection and promotion Committee to supervise the compliance of this Act and to protect and promote Breast Feeding and for the regulation of sale and distribution of products. Functions, Duties and powers of the committee had been given under the approved policy of Nepal Government. The Ministry, in consultation with the Committee, shall give permission to publicize the information and educational materials about infant food. The heads of Health Care Agencies, and National and Local health Officers should take appropriate measure in promoting the principles of this Act and in protecting and promoting breast feeding and they should impart appropriate information and advice to Health workers about their responsibilities, and the Health worker must be informed about the matters that is mentioned in this clause. This act had also identified appropriate way of advertising the product by the manufacturer and the distributor. This act had also made compulsory certification for feeding bottle and nipple from the central food research Laboratory for the certification of the product:
The Manufacturer or the Distributor should approve the labels of such products from the Breastfeeding promotion and protection committee before selling it in Nepal. While manufacturing, selling or distributing in other ways, the products should be of the standard quality prescribed or recommended by the Nepal Quality Standard Office. The Ministry, on the recommendations of the Committee that was formed to monitor and investigate the compliance of this Act or the rules framed under this Act by Manufacturers, Distributors, Monitoring, Agencies and Health Workers can appoint Monitors as per the requirements or Government employees can be deputed to work as monitors after obtaining the approval of the concerned departments of Nepal Government. As per the sub- Clause (2) of Clause 13, if any Manufacturer, Distributor, health Monitoring Agency or health Worker is found violating this Act or the rules framed under this Act in the reports, submitted by the Monitors, the Ministry, on the recommendations of the Committee, can write to concerned Department to suspend or cancel the License, permit or Authority letter given by Nepal Government or any other Department to carry their business or trade. Duties and the Rights of Monitor: Monitors will be having other directed duties and rights apart from the duties and rights mentioned in this Act.
25
Child Health Division and Helen Keller International conducted study to assess promotion practices occurring within maternity and child health centers related to breastfeeding and foods consumed by young children. Promotion within the health system (advice and support on infant and young child feeding practices, prescription of breast-milk substitutes and complementary foods, provision of samples of products or gifts) and mothers’ reported exposure to promotion outside the health system was documented.
These assessments found the following:• Breast milk substitute use within 3 days of delivery was found to be very high in public (48%) as
well as private (74%) hospitals in Kathmandu Valley. The public hospitals in the study include 5 of 7 hospitals in the country certified as Baby Friendly Hospitals in the past.
• Mother’s reported exposure to breast milk substitute promotion by health worker after delivery was high, and was correlated to its use among newborn within 3 days of delivery.
• Breast milk substitutes are widely available in stores in Kathmandu Valley such as local grocery shop and large supermarkets. Their general availability in local grocery shop and supermarkets is not against the BMS Act. However, point of sale promotions of such breast milk substitutes in these stores is against the BMS Act and there were violation of the codes.
• Breast milk substitutes were available in a few pharmacies inside hospital premises. Their availability inside hospital premises, including pharmacies in the hospitals, is against the BMS Act. Also, promotion inside hospitals and the point of sale promotion of such breast milk substitute anywhere is against the BMS Act.
Mother’s milk Substitue Act –Nepal, implementation of this act has never been done satisfactorily due to various reasons, the most important being lack of skilled manpower to monitor on the violation of this code. Hence, the workshop was organized with the aim to develop skill on the monitoring of Mother milk substitute code.
Workshop on BMS code at TUTHTribhuvan University Teaching hospital (TUTH) and Nepal Breast Feeding Promotion Forum (NEBROF) with support from BPNI and IBFAN Asia organized a two days workshop on “Implementation of Mothers’ Milk Substitute Act of Nepal” at Kathmandu, Nepal on 13th and 14th of September 2014. It brought together 23 participants working in the various sectors related to childhood nutrition in Nepal. The participants included government officials, Nepal Pediatric society representatives, Consumer’s right protection forum, Pediatricians, representatives of civil society and various organizations from Nepal.
Orientation on BMS Act by MOHPAround 400 health workers from 10 hospitals of Kathmandu Valley were oriented on BMS act in July 2015. The orientation was conducted in the respective 10 Hospitals. Along with the Hospital Director, the participants included the Head and health workers from Pediatric, Obstetrics/Gynecology and Nursing Department. Staff from administrative department was also included. A team comprised of a pediatrician, an obstetrician/gynecologist and a lawyer conducted the orientation. The purpose of the orientation was to make health workers aware of BMS act. Additionally, a breastfeeding committee comprising of hospital director as a chairperson, a focal person and few members was also formed in each hospital.
All articles of the code as law and its regular monitoring and enforcement have not been implemented but some articles of the Code as law exist. During the year 2015, revitalization of the breastfeeding Protection and Promotion Committee had been started with an attempt to make the law into function specified in the Act is not functioning and there are no systems for monitoring the situation and reporting violations. Nepal has been in the forefront for developing the Code and legislation. But proper monitoring could not be done due to lack of identification of nodal point at the centre level

26
as well as district. Even though there is clear clause to ban sponsorship of the medical personnel, companies continue to fine way and means to reach out to doctors to support their activities. This area needs effective enforcement of the Infant milk substitutes, feeding bottles and infant foods (Regulation of Production, supply and distribution) BMS Act 2049 (A.D 1992).
Media MonitoringA retrospective monitoring of breast milk substitutes and complementary foods in Nepalese media was conducted. Max-pro was contracted for this purpose. Advertisement of Breast Milk Substitute was not found in Nepalese TV channels.
Guidelines for scoringCriteria (Legal Measures that are in Place in the Country) Scoring3a: Status of the International Code of Marketing√ (Check that apply.If more than one is applicable, record the highest score.)3.1 No action taken 03.2 The best approach is being considered 0.53.3 National Measures awaiting approval (for not more than three years) 13.4 Few Code provisions as voluntary measure 1.53.5 All Code provisions as a voluntary measure 23.6 Administrative directive/circular implementing the code in full or in part in health
facilities with administrative sanctions3
3.7 Some articles of the Code as law 4 3.8 All articles of the Code as law 5√3.9 Relevant provisions of World Health Assembly (WHA) resolutions subsequent to the
Code are included in the national legislation6a. Provisions based on at least 2 of the WHA resolutions as listed below are includedb. Provisions based on all 4 of the WHA resolutions as listed below are included
5.56
3b: Implementation of the Code/National legislation
3.10 The measure/law provides for a monitoring system 13.11 The measure provides for penalties and fines to be imposed to violators 13.12 The compliance with the measure is monitored and violations reported to concerned
agencies1
3.13 Violators of the law have been sanctioned during the last three years 1Total Score (3a + 3b) (4+0) 5/10
Gaps:• Lack of Monitoring and enforcement of existing IMS Act 2049 (A.D 1992) on the infant milk
substitutes, feeding bottle and infant foods• Inadequate understanding on IMS Act by health professionals at all levels.• Inactive authority to implement BMS, lack of a system for monitoring practices and identifying
violations and take actions.
Recommendations• All articles of the code as law and its regular monitoring and enforcement have to be implemented.• The monitoring system for BMS situation and reporting violations should be developed.

27
List of Sources1. www. Hki.org/sites/default/ files/attach/2015/17/Nepal HSS Country Report_Final_Sept5 (2) (2).
pdf2. www.moadwto.gov.np/infantmilksubstituesact_1322220410.pdf3. Nepal Breast milk Substitute regulation 1994. Nnfsp.gov.np/portalcontent.aspx4. Substitute for the breast Milk (Sale, Distribution and control) Act 2049. http://dx.doi.org/10.3126/
jnps.v28i1.14075. Assessment and research in child feeding (arch): Labeling study report Nepal. www.nnfsp.gov.np6. Workshop on implemention of Mothers’ Milk substitute Act in Nepal. Bpni.org/project/BMS-
code-workshop-Nepal.pdf7. ibfan.org/code-watch-reports

28
Indicator 4: Maternity ProtectionKey Question: is there legislation and are there other measures (policies, regulations, practices) that meet or go beyond the International Labor Organization (ILO) standards for protecting and supporting breastfeeding for mothers, including those working mothers in the informal sector?
Background:• The Innocenti Declaration (1999,2005) and WHO Global Strategy for IYCF (2002) call for
provision of imaginative legislation to protect the breastfeeding rights for working women and further monitoring of its application consistent with ILO Maternity Protection Convention No. 183, 2000 (MOC No. 183) and recommendation 191. MPC No. 183 specifies that women workers should receive:
• At least 14 weeks of paid maternity leave• Provision of Paternity Leave• Employment protection and non discrimination that includes:
» The guaranteed right to return to work » Protection during a period following a woman’s return to work » Burden of proof i.e. dismissal is unrelated to pregnancy, child birth or nursing. » Non- discrimination in relation to maternity: right if all women not to be treated less favorably in a work situation
» Prohibition of pregnancy test at the time of application for employment• Health Protection at the workplace should have provisions for
» Arrangement of working time » Time off for prenatal health care » Provisions on hazardous or unhealthy work
• Breastfeeding at work and childcare should include » One or more paid breastfeeding breaks daily » Provision of Crèches
• Encourage facilities for breastfeeding to be set up at or near the workplace.• Only a limited number of countries have certified C 183, but quite a few countries have ratified
C103 and /or have national legislation and practices which are stronger than the provisions of any of the ILO conventions.
• Maternity protection for all women implies that women imply that women working in the informal economy should also be protected. Innocenti Declaration 2005 calls for urgent attention to the special needs of women in the non-formal sector. Adequate maternity protection also recognizes the fathers’ role in nurturing and thus the need for paternity leave.
• The Civil Service Rules 2050 (1993) has provision of a total of 60 days paid maternity leave prior to or after delivery. Father employees are entitled to paternity leave of 15 days. However, there is no provision for breastfeeding breaks or facilities. The Companies Act 2006 covers private sector and it needs to be in line with civil employee. No legislation that protects women working in the informal sector.
• Recently lots of advocacy programs are initiated and in few of the government offices, creche has been started and specially in NGOs and INGOs, there is provision of six months maternity leave. However, these efforts are very minimal and inadequate.

29
Indicator 4: Maternity ProtectionCriteria4.1) Women covered by the national legislation are allowed the
following weeks of paid maternity leavea. Any leave less than 14 weeksb. 14 to 17weeksc. 18 to 25 weeksd. 26 weeks or more
0.5√1
1.52
4.2) Women covered by the national legislation are allowed at least one breastfeeding break or reduction of work hrs /d
a. Unpaid breakb. Paid break
0.51
4.3) Legislation obliges private sector employers of women in the country to
a. Give at least 14 weeks paid maternity leaveb. Paid nursing breaks.
0.50.5
4.4) There is provision in national legislation that provides for work siteaccommodation for breastfeeding and/or childcare in work places in theformal sector.
a. Space for Breastfeeding/Breastmilk expressionb. Crèche
10.5
4.5) Women in informal/unorganized and agriculture sector are:a. accorded some protective measuresb. accorded the same protection as women working in the formal
sector
0.51
4.6) a.Information about maternity protection laws, regulations, or policies ismade available to workers.
b. There is a system for monitoring compliance and a way for workers to complain if their entitlements are not provided.
0.5
0.5
4.7) Paternity leave is granted in public sector for at least 3 days. 0.5√4.8) Paternity leave is granted in the private sector for at least 3
days.0.5
4.9) There is legislation providing health protection for pregnant and breastfeeding workers: they are informed about hazardous conditions in theworkplace and provided alternative work at the same wage until they are no longer pregnant or breastfeeding.
0.5
4.10) There is legislation prohibiting employment discrimination and assuring job protection for women workers during breastfeeding period
1
TOTAL SCORE 1/10Gaps:
• Weak policy and legislation regarding breastfeeding that covers employees in Governmental and Private and informal sectors
• Maternity leave in governmental and private sector is inadequate.• Inadequate provision of breastfeeding break/creche in all sectors including formal ones.
Recommendations:• Strengthening advocacy from governmental and non-governmental organization on maternity
protection act is needed.• There should be increased awareness programs for women regarding maternity protection.• Provision of breastfeeding break and places in formal and informal sectors is required.
List of Sources:1. http://www.ilo.org/dyn/normE:C18 3 2. Civil Service Regulation, 2050 (1993) 3. Maternity Benefit Act 200

30
Indicator 5: Health and Nutrition Care Systems (in support of breastfeeding & IYCF)Key question: Do care providers in these systems undergo skills training, and do their pre-service education curriculum support optimal infant and young child feeding; do these services support mother and breastfeeding friendly birth practices, do the policies of health care services support mothers and children, and whether health workers responsibilities to Code are in place?
Background:The Global Strategy for infant and young child feeding indicates clearly how to achieve its targets and improving these services through strengthening health and Nutrition Care Systems. Reviews of existing curriculum of health providers showed the inadequate skills of training in counseling for infant and young child feeding. Health Service providers of all the levels who are in contacts of mothers and their young children either in health facilities or in communities need to be equipped with knowledge, attitudes, and skill necessary to integrated breastfeeding counseling, lactation management, and infant and young child feeding into their health care system.
In few of the hospitals in capital city do have in service training on IYCF for their staffs but because of new recruits and transfer of staffs all the staffs do not get training on regular basis.
Criteria Yes To some degree No
5.1) A review of health provider schools and preservice education programmes for health professionals, social and community workers in the Country indicates that infant and young child feeding curricula or session plans are adequate/inadequate
2 1√ 0
5.2) Standards and guidelines for mother-friendly childbirth procedures and support have been developed and disseminated to all facilities and personnel providing maternity care.
2 1√ 0
5.3) There are in-service training programmes providing knowledge and skills related to IYCF for relevant health/nutrition care providers
2 1√ 0
5.4) Health workers are trained on their responsibility under the Code implementation / national regulation throughout the country.
1 0.5√ 0
5.5) IYCF information and skills are integrated, as appropriate, into training programmes
1√ 0.5 0
5.6) In-service training programmes referenced in 5.5 are being provided throughout the country
1 0.5√ 0
5.7) Child health policies provide for mothers andbabies to stay together when one of them is sick.
1 0.5√ 0
TOTAL SCORE 5.5/10Gaps:
• Adequate number of health professionals has not been received practical training on IYCF in pre-services education program.
• Health workers are not adequately trained on Code implementation.
Recommendations:• Implementation and integration of IYCF practical skills in curriculum of health professionals eg:
nursing and paramedics.• Lactation management training should be incorporated as a part of continuous medical education.
List of Sources:• Strategy for Infant and Young Child Feeding: Nepal 2014. Draft. Child Health Division.
Department of Health Services, Ministry of Health and Population, Government of Nepal.• Curriculum for M.Sc Nursing Paediatrics. Institute of Medicine 2003.• Curriculum for MD (Paediatrics),BPKIHS 2000.

31
Indicator 6: Mother Support and Community Outreach – Community based Support for the pregnant and breastfeeding mother
Key question: Are there mother support and community outreach systems in place to protect,
Promote and support optimal infant and young child feeding?
Background:Mother Support is defined by the Global initiative for Mother Support (GIMS) is “any support provided to mothers for the purpose of improving breastfeeding practices for both mother and infant and young child.” Women need the support of evidence-based public health policies, health providers, employers, friends, family, the community, and particularly of their women and mothers.
Step 10 of BFHI and the Global Strategy for IYCF recognizes the need of mother support and peer support based in the community for succeeding in optimal breastfeeding practices.
Mother support not only covers mother to mother but it also includes accurate and timely information to help a woman build confidence; sound recommendations based up to date research; compassionate care before, during and after childbirth; empathy and active listening, hands-on assistance practical guidance. It also means support and counseling by health professional and health care workers including community outreach services for optimal feeding.
In Nepal, although mothers group do exist in all wards supported by FCHVs but all women do not have access to community-based support system and services on infant and young child feeding. Women get suggestion from FCHVs on importance of breastfeeding and complementary feeding but not practical supports for optimal IYCF. Majority of mothers deliver at home and 1/5 only deliver at health facilities where they are supposed to receive infant and young child feeding counseling after birth. However, this is not practices in any hospital even though they were certified as BFHI in 1997 – 1998 (BFHI Assessment report 2011). Although IYCF services have national coverage and some project districts are focus more and others are not, hence practical skilled support to mothers for optimal IYCF is inadequate at National Level. Currently, some staff (600) of the maternity hospitals in Kathmandu Valley were trained on lactation management and 3 Day lactation management training manual is published in support of HKI.
Indicator 6: Mother Support and Community Outreach – Community based support for the pregnant and breastfeeding motherGuidelines for scoringCriteria Scoring √ Check that apply
Yes To some degree No6.1) All pregnant women have access to community based antenatal
and post natal support systems with counseling services on infant and young child feeding.
2 1√ 0
6.2) All women receive support for infant and young child feeding at birth for breastfeeding initiation.
2 1√ 0
6.3) All women have access to counseling support for IYCF counseling and support have national coverage.
2 1√ 0
6.4) Community based counseling through Mother Supports Groups (MSG) and support services for the pregnant and breastfeeding woman are integrated into an overall infant and young child health and development policy IYCF/Health/Nutrition Policy.
2√ 1
6.5) Community based volunteers and health workers are trained in counseling skills infant and young child feeding.
2 1√
Total Score 6/10

32
Gaps:• There are inadequate services on counseling pregnant and breastfeeding mothers in outreach
clinic• Inadequate counseling and listening skills among community level workers• Lack of crèche facilities in both government and private sectors.
Recommendations:• There should be more training on lactation management skills for village Level Health Workers
for comprehensive intervention on IYCF to support at community level or outreach clinic.
List of sources1. National Maternity Care Guideline Nepal 20042. Neonatal and Infant Nutrition Training Manual for Health Workers 20073. National Maternity Care Guidelines Nepal4. National Essential Maternal and Neonatal health Care Services Package for Nepal 20055. A Report of Nepal Maternal and neonatal and Neonatal Forum 20056. Annual Report 2071/727. CBIMCI Programme Health Sector Strategy 20048. Community Based Maternal Newborn Care Package (CBMNCP) 2007

33
Indicator 7: Information Support
Key question: Are comprehensive Information, Education and Communication (IEC) strategies for improving infant and young child feeding (breastfeeding and complementary feeding) being implemented?Behaviour Change is an important strategy, often used in counseling sessions, home visits, action-oriented group discussions and drama focused on problem based solution. Information, education and communication (IEC) strategies are crucial to improve IYCF practices. IEC approaches include the use of electronic media, print media, interpersonal, dramas and community activities for motivational material to mothers, families and community to communicate important appropriate , action oriented messages or information .
Communication ActivitiesIn Nepal, the communication strategies for interventions on nutrition are focused on three mutually supporting communication approaches namely advocacy communication, social mobilization communication and behavioural change communication.
Advocacya. Nutrition Committee. Hold regular coordination meetings of key strategic partners in nutrition for joint planning, technical updates and to ensure media and materials sharing and regular lessons learned.
b. Develop advocacy tool kits for policy makers, parliamentarians and ministries to demonstrate the importance of nutrition programmes for contributing to the MDGs/SDG and make a case for increased investments and coordinated efforts. Monitor, promote, and coordinate the use of advocacy tools across organizations working in the nutrition and maternal/child health sectors
c. Policy. Review, revise and reactivate breastfeeding act to include a leave provision for working mothers till 6 months after delivery and provision of breast feeding space at workplace
d. Engage the media. Train media persons to stimulate use of media outlets, raise awareness and report of critical issues related to nutrition programme.
A national Comprehensive IEC strategy includes messages on IYCF in Nepal. Nutrion division of Ministry of health and population in coordination with its partners had been reviewed IYCF training modules of WHO and translated in Nepal for the district level training on lactation management.
In Nepal every year World Breastfeeding Week is celebrated nationally with allocation of the budget for all 75 districts. Individual counseling and group education services related to IYCF are available within the health/nutrition care system or through community outreach but the implementation is not adequate.
IEC distributionSeveral sets of flex posters on Maternal, Infant and Young Child Nutrition (MIYCN) message was distributed to various hospitals of Kathmandu Valley during lactation management training.

34
Guidelines for scoringCriteria Scoring √ Check that apply
Yes To some degree No7.1) There is a national IEC strategy for improving infant and young child
feeding that ensures all information and materials are free from commercial influence/ potential conflicts orinterest are avoided.
2√ - 0
7.2a) National health/nutrition systems include individual counseling on infant and young child feeding
1√ 0.5 0
7.2b) National health/nutrition systems include group education and counseling services on infant and young child feeding
1√ 0.5 0
7.3) IYCF IEC materials are objective, consistent and in line with national and/or international recommendations and include information on the risks of artificial feeding
2√ 1 0
7.4. IEC programmes (eg World Breastfeeding Week) that include infant and young child feeding are being implemented at local level and are free from commercial influence
2√ 1 0
7.5 IEC materials/messages to include information on the risks of artificial feeding in line with WHO/FAO Guidelines on preparation and handling of powdered infant formula (PIF).11
2 0√ 0
Total Score: 8/10Gaps:
• IEC materials are not adequate with emphasis on risks of artificial feeding.
Recommendations:• There should be increased number of IEC materials about the risk of artificial feeding.• National communication strategy for infant and young child feeding should be implemented to
the community level.• To promote IEC strategy electronic and print media should be utilized more.
List of resources:1. National communication strategies. Dohs.gov.np/…/National_communication_Strategy__for_
MNCH_2011_2016_EN.pdf2. HKI training package on “lactation management training”.

35
Indicator 8: Infant Feeding and HIVKey Question: Are policies and programmes in place to ensure that HIV - positive mothers are supported to carry out the national recommended Infant feeding practice?
Background:In Nepal, there are 761,661 pregnancies per year with estimated 0.09% prevalence of HIV among pregnant women. 679 pregnancies estimated to occur in HIV positive women every year.Estimated rate of transmission 25-45%; 136 to 306 babies infected annually ( NCASC 2013 estimates)
Global Strategy for IYCF recommends the country to have a comprehensive policy on infant and young child feeding that includes infant and HIV. This strategy is adopted by Nepal as well. In 2014, Government of Nepal with support from World Health Organization has updated guidelines, “National Consolidated Guidelines for Treating and Preventing HIV in Nepal” and the guideline includesprevention of mother to child transmission (PMTCT), breastfeeding and infant feeding strategies in relation to HIV/AIDS along with guidelines for anti-retroviral therapy for children and adults .
Although implementation of HIV and infant feeding counseling in Nepal has improved, still there is inadequate counseling to HIV positive mothers because of lack of training for PMTCT in all levels.
Criteria Yes To Some degree No8.1) The country has a comprehensive updated policy in line with international
Guidelines on IYCF that includes infant feeding and HIV2√ 1 0
8.2) The infant feeding and HIV policy gives effect to the International Code/ National Legislation
1√ 0.5 0
8.3) Health staff and community workers receive training on HIV and infant feeding policies, the risks associated with various feeding options for infants of HIV-positive mothers and how to provide counselling and support.
1 0.5√ 0
8.4) HIV Testing and Counselling (HTC)/ Provide Initiated HIVTesting and Counselling (PIHTC)/ Voluntary and Confidential Counselling and Testing (VCCT) is available and offered routinely to couples who are considering pregnancy and to pregnant women and their partners.
1 0.5√ 0
8.5) Infant feeding counselling in line with current international recommendations and appropriate to local circumstances is provided to HIV positive mothers.
1 0.5√ 0
8.6) Mothers are supported in carrying out the recommended national infant feeding practices with further counselling and follow-up to make implementation of these practices feasible.
1 0.5√ 0
8.7) HIV positive breastfeeding mothers, who are supported through provision of ARVs in line with the national recommendations, are followed up and supported to ensure their adherence to ARVs uptake.
1 0.5√ 0
8.8) Special efforts are made to counter misinformation on HIV and infant feeding and to promote, protect and support 6 months of
Exclusive breastfeeding and continued breastfeeding in the general population.
1 0.5 0
8.9) On-going monitoring is in place to determine the effects of interventions to prevent HIV transmission through breastfeeding on infant feeding practices and overall health outcomes for mothers and infants, including those who are HIV negative or of unknown status.
1 0.5 0
TOTAL 5.5/10Gaps:
• Inadequate advocacy and implementation of policy and guidelines at all levels.• Lack of trainings to all health workers on infant feeding in HIV.• Lack of monitoring system to determine the effects of intervention to prevent HIV transmission
through BF on infant feeding practices who are unknown of the situation.

36
Recommendations:• Review on existing situation of implementation of infant feeding in HIV is needed.• Revitalized BFHI required inclusion of training on PMTCT• Strengthen implementation of policy and strategies and initiate regular monitoring of it.
List of resources:1. HIV Situation of Nepal. Updated 2015. National Centre for AIDs and STD control. Ministry of
Health. Government of Nepal.2. National Consolidated Guidelines for treating and preventing HIV in Nepal.2014. National Cen-
tre for AIDS and STD control. Ministry of Health and Population. Government of Nepal.

37
Indicator 9: Infant and Young Child Feeding during Emergencies
Key question: Are appropriate policies and programmes in place to ensure that mothers, infants and young children will be provided adequate protection and support for appropriate feeding during emergencies.
BackgroundMaintaining breastfeeding and appropriate complementary feeding of any child in emergency and relief situations is a challenge. During these situations,infants and young children are greater risks of malnutrition, illness and mortality. Thus protecting, promoting and supporting optimal infant and young child feeding practices during such situation in any country is crucial. Global experiences commonly revealed that donations of breast milk substitutes and bottles feeding practices increases that undermine breastfeeding and cause illness. Ensuring proper IYCF practices during emergencies is hard in the countries where IYCF is not effectively implemented even in normal situation.
Nepal has made a notable progress in development of emergency prepared plans and responses which clearly address the infant feeding during emergency. It has also identified a national coordinator with UN, donors, military and NGOs and related clusters working for emergency situation. The infant feeding in emergency plan ensures exclusive breastfeeding and to minimize the risk of artificial feeding
Nepal was hit by a powerful earthquake of 7.8 magnitude on April 25th, 2015. Fourteen districts were severely affected(5.6 million people) with causalities of 8897 and 22310 people injured.
Immediately after the earthquake Government of Nepal mobilized Nutrition Cluster led by the Ministry of Health and Population including 28 national and international partners. Aims of Emergency Nutrition Response were to
1. Protect, promote, and support breastfeeding for children aged 0–23 months and avoid the distribution or use of unsolicited donations of breast milk substitutes;
2. Improve complementary feeding for children aged 6–23 months through information, counseling, and the distribution of multiple micronutrient powders (MNPs) for home fortification of child foods;
3. Identify and treat children aged 6–59 months with severe acute malnutrition through community management of acute malnutrition;
4. Improve the micronutrient intake of children aged 6–59 months through MNPs and vitamin5. Improve the micronutrient intake of women during pregnancy and the early post- partum period.
With above mentioned aims “Child Nutrition Week” was formulated by Emergency Nutrition Response to deliver a package of essential nutrition services for children younger than 5 years and their mothers.
Nepal’s Child Nutrition Week was planned as a fixed-day, village-based strategy to deliver a package of six nutrition interventions to at least 80% of a target population including 4,67,425 children aged 0-59 months, pregnant women, and breastfeeding mothers. The Ministry of Health and Population, supported by the Nutrition Cluster, developed district-level guidelines for the implementation of Child Nutrition Week. In each district, Child Nutrition Week was planned and implemented by the district officials of the Ministry of Health and Population with the support of a Health and Nutrition Cluster partner in coordination with the District Disaster Relief Committee, and the Village Development Committee (municipality) and ward (village) authorities. An on-site coaching approach was used to train over 15000 implementers: health workers, female community health volunteers, and volunteers from civil society organizations. A mobilization strategy through Radio Nepal and 63 local radios before and during Child Nutrition Week raised awareness about the importance of the programme and when and where to avail its services.

38
Nepal’s Child Nutrition Week has been an effective platform to deliver a package of essential nutrition services to the most vulnerable children and mothers in the earthquake-affected districts .This is the first time that a Child Nutrition Week approach has been used in South Asia as part of an emergency response. Building on the successful implementation of Child Nutrition Week, the Government of Nepal is considering the implementation of bi-annual Child Nutrition Weeks to deliver an integrated package of nutrition services as an extension of the routine services provided by the primary health-care system.
In this recent emergency situation, Nepal has done a commendable job and has set an example which can be copied in future for different emergency situations even in different parts of the world.
Yes To some degree No9.1) The country has a comprehensive policy on IYCF that includes infant
feeding in emergencies and contains all basic elements included in the IFE Operational Guidance
2√ 1 0
9.2) Person(s) tasked with responsibility for national coordination with all relevant partners such as the UN, donors, military and NGOs regarding IYCF in emergency situations have been appointed
2√ 1 0
9.3) An emergency preparedness and response plan based on the practical steps listed in the operational Guidance has been developed and put into effect in most recent emergencysituations, and covers:a) basic and technical interventions to create an enabling
environement for breastfeeding, including counseling by appropriately trained counselors,support for relactation and wet-nursing, and protected spaces for breastfeeding
b) measures to minimize the risks of artificial feeding, including an endorsed statement on avoidance of donations of breastmilk substitutes, bottles and teats,and standard procedures for handling unsollicited nations, and procurement management and use of any infant formula and BMS, in accordance withstrict criteria, the IFE Operational Guidance, and theInternational Code and subsequent relevant WHAresolutions.
1
1√
0.5√
0.5
0
0
9.4) Resources have been allocated for implementation ofthe emergency preparedness and response plan
2√ 1 0
9.5)a) Appropriate orientation and training material on IYCF in emergencies
has been integrated into pre-service and in-service training for emergency management and relevant health care personnel.
b) Orientation and training is taking place as per the national emergency preparedness and response plan
1
1√
05√
0.5
0
0
TOTAL SCORE 9/10
Gaps:• Still there is inadequate human resources and implementation experiences in infant feeding
during emergency.
Recommendation:• Advocacy for its inclusion in pre-service curriculum of medical and paramedical including
refresher training for in-service is required.
• User friendly separate IEC materials containing BMS code should be developed for emergencies.
List of Sources1. Delivering essential nutrition services for children after the Nepal earthquake. The Lancet. Vol
13 November 20152. Strategy for Infant and Young Child Feeding: Nepal 2014. Draft. Child Health Division,
Department of Health Services, Ministry of Health and Population, Government of Nepal.
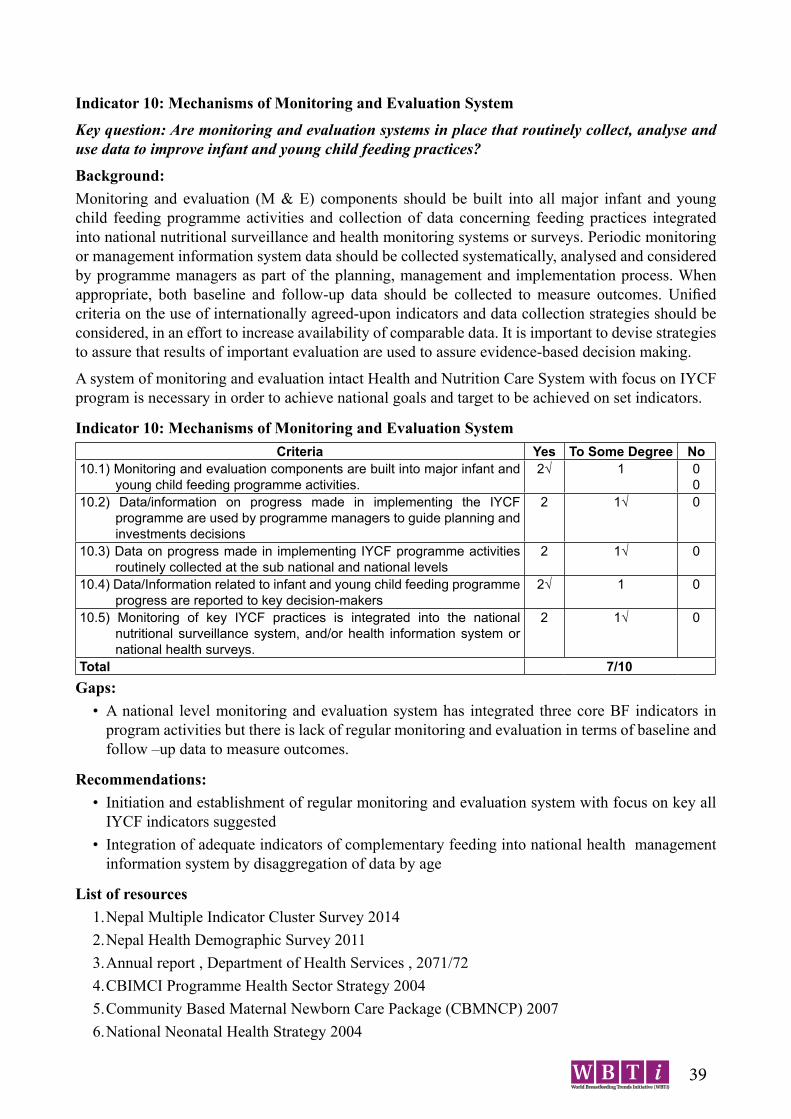
39
Indicator 10: Mechanisms of Monitoring and Evaluation System
Key question: Are monitoring and evaluation systems in place that routinely collect, analyse and use data to improve infant and young child feeding practices?
Background:Monitoring and evaluation (M & E) components should be built into all major infant and young child feeding programme activities and collection of data concerning feeding practices integrated into national nutritional surveillance and health monitoring systems or surveys. Periodic monitoring or management information system data should be collected systematically, analysed and considered by programme managers as part of the planning, management and implementation process. When appropriate, both baseline and follow-up data should be collected to measure outcomes. Unified criteria on the use of internationally agreed-upon indicators and data collection strategies should be considered, in an effort to increase availability of comparable data. It is important to devise strategies to assure that results of important evaluation are used to assure evidence-based decision making.
A system of monitoring and evaluation intact Health and Nutrition Care System with focus on IYCF program is necessary in order to achieve national goals and target to be achieved on set indicators.
Indicator 10: Mechanisms of Monitoring and Evaluation SystemCriteria Yes To Some Degree No
10.1) Monitoring and evaluation components are built into major infant and young child feeding programme activities.
2√ 1 00
10.2) Data/information on progress made in implementing the IYCF programme are used by programme managers to guide planning and investments decisions
2 1√ 0
10.3) Data on progress made in implementing IYCF programme activities routinely collected at the sub national and national levels
2 1√ 0
10.4) Data/Information related to infant and young child feeding programme progress are reported to key decision-makers
2√ 1 0
10.5) Monitoring of key IYCF practices is integrated into the national nutritional surveillance system, and/or health information system or national health surveys.
2 1√ 0
Total 7/10Gaps:
• A national level monitoring and evaluation system has integrated three core BF indicators in program activities but there is lack of regular monitoring and evaluation in terms of baseline and follow –up data to measure outcomes.
Recommendations:• Initiation and establishment of regular monitoring and evaluation system with focus on key all
IYCF indicators suggested• Integration of adequate indicators of complementary feeding into national health management
information system by disaggregation of data by age
List of resources1. Nepal Multiple Indicator Cluster Survey 20142. Nepal Health Demographic Survey 20113. Annual report , Department of Health Services , 2071/724. CBIMCI Programme Health Sector Strategy 20045. Community Based Maternal Newborn Care Package (CBMNCP) 20076. National Neonatal Health Strategy 2004
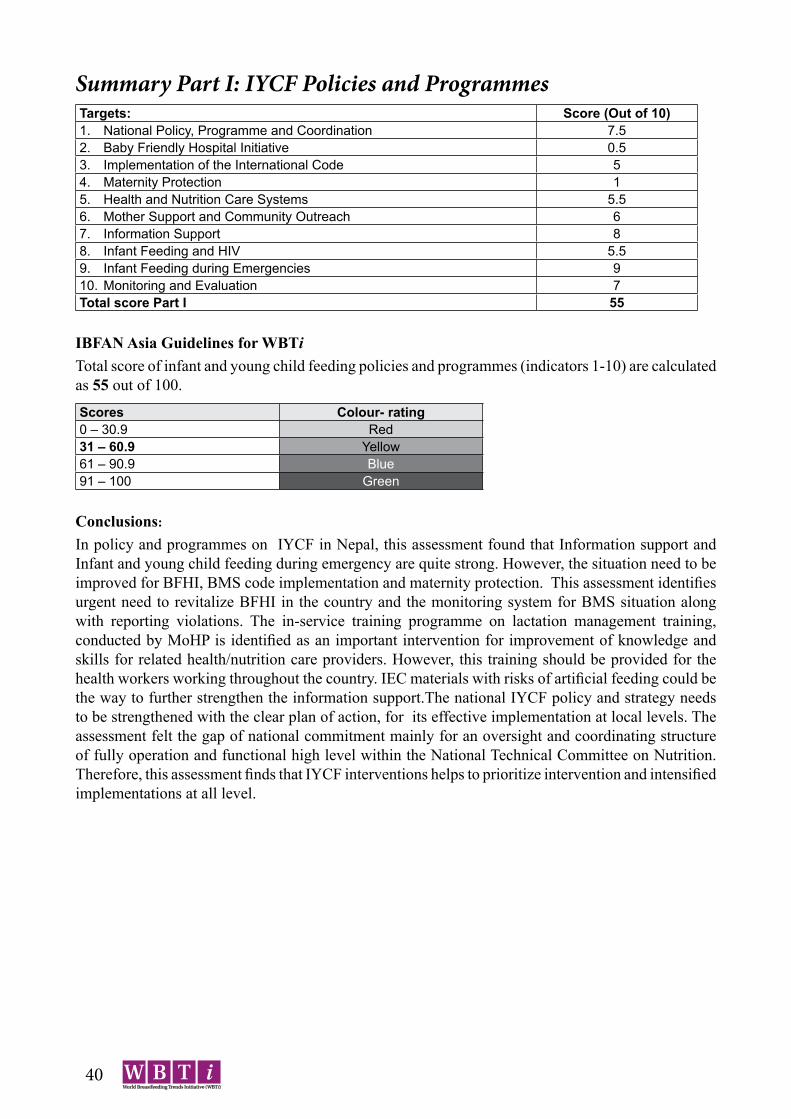
40
Summary Part I: IYCF Policies and ProgrammesTargets: Score (Out of 10)1. National Policy, Programme and Coordination 7.52. Baby Friendly Hospital Initiative 0.53. Implementation of the International Code 54. Maternity Protection 15. Health and Nutrition Care Systems 5.56. Mother Support and Community Outreach 67. Information Support 88. Infant Feeding and HIV 5.59. Infant Feeding during Emergencies 910. Monitoring and Evaluation 7Total score Part I 55
IBFAN Asia Guidelines for WBTi Total score of infant and young child feeding policies and programmes (indicators 1-10) are calculated as 55 out of 100.
Scores Colour- rating0 – 30.9 Red31 – 60.9 Yellow61 – 90.9 Blue91 – 100 Green
Conclusions:
In policy and programmes on IYCF in Nepal, this assessment found that Information support and Infant and young child feeding during emergency are quite strong. However, the situation need to be improved for BFHI, BMS code implementation and maternity protection. This assessment identifies urgent need to revitalize BFHI in the country and the monitoring system for BMS situation along with reporting violations. The in-service training programme on lactation management training, conducted by MoHP is identified as an important intervention for improvement of knowledge and skills for related health/nutrition care providers. However, this training should be provided for the health workers working throughout the country. IEC materials with risks of artificial feeding could be the way to further strengthen the information support.The national IYCF policy and strategy needs to be strengthened with the clear plan of action, for its effective implementation at local levels. The assessment felt the gap of national commitment mainly for an oversight and coordinating structure of fully operation and functional high level within the National Technical Committee on Nutrition. Therefore, this assessment finds that IYCF interventions helps to prioritize intervention and intensified implementations at all level.
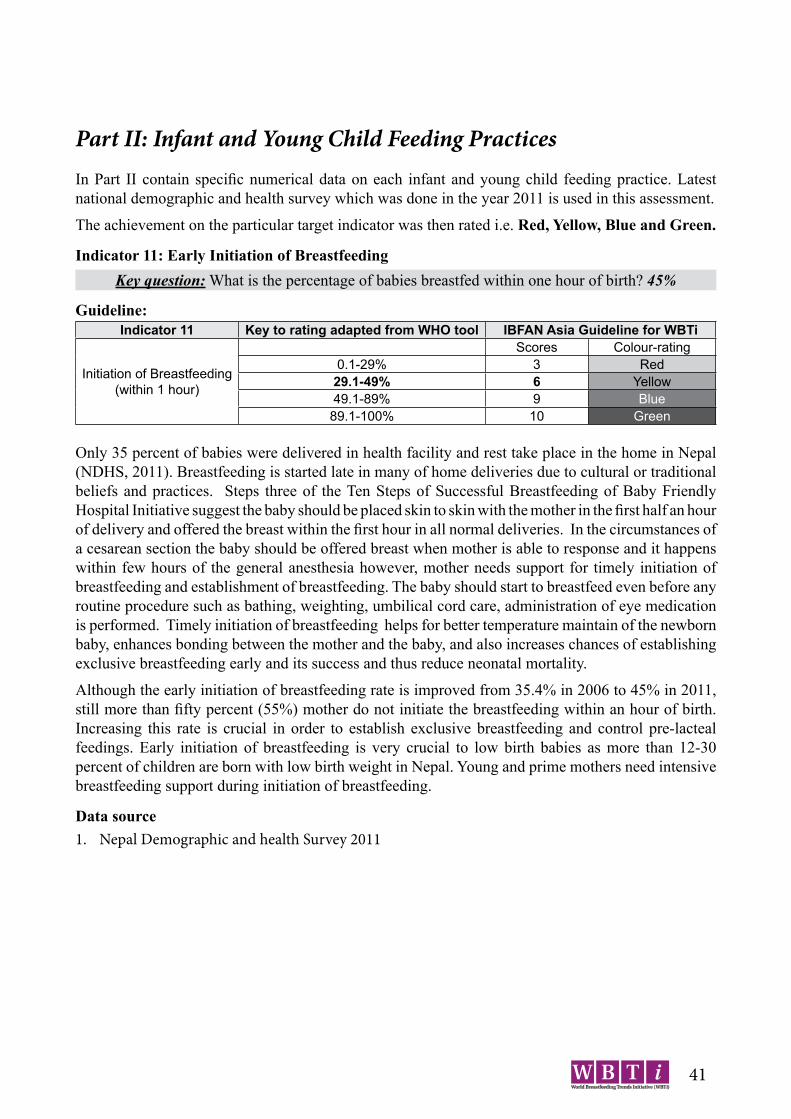
41
Part II: Infant and Young Child Feeding PracticesIn Part II contain specific numerical data on each infant and young child feeding practice. Latest national demographic and health survey which was done in the year 2011 is used in this assessment.
The achievement on the particular target indicator was then rated i.e. Red, Yellow, Blue and Green.
Indicator 11: Early Initiation of BreastfeedingKey question: What is the percentage of babies breastfed within one hour of birth? 45%
Guideline:Indicator 11 Key to rating adapted from WHO tool IBFAN Asia Guideline for WBTi
Initiation of Breastfeeding (within 1 hour)
Scores Colour-rating 0.1-29% 3 Red
29.1-49% 6 Yellow49.1-89% 9 Blue
89.1-100% 10 Green
Only 35 percent of babies were delivered in health facility and rest take place in the home in Nepal (NDHS, 2011). Breastfeeding is started late in many of home deliveries due to cultural or traditional beliefs and practices. Steps three of the Ten Steps of Successful Breastfeeding of Baby Friendly Hospital Initiative suggest the baby should be placed skin to skin with the mother in the first half an hour of delivery and offered the breast within the first hour in all normal deliveries. In the circumstances of a cesarean section the baby should be offered breast when mother is able to response and it happens within few hours of the general anesthesia however, mother needs support for timely initiation of breastfeeding and establishment of breastfeeding. The baby should start to breastfeed even before any routine procedure such as bathing, weighting, umbilical cord care, administration of eye medication is performed. Timely initiation of breastfeeding helps for better temperature maintain of the newborn baby, enhances bonding between the mother and the baby, and also increases chances of establishing exclusive breastfeeding early and its success and thus reduce neonatal mortality.
Although the early initiation of breastfeeding rate is improved from 35.4% in 2006 to 45% in 2011, still more than fifty percent (55%) mother do not initiate the breastfeeding within an hour of birth. Increasing this rate is crucial in order to establish exclusive breastfeeding and control pre-lacteal feedings. Early initiation of breastfeeding is very crucial to low birth babies as more than 12-30 percent of children are born with low birth weight in Nepal. Young and prime mothers need intensive breastfeeding support during initiation of breastfeeding.
Data source1. Nepal Demographic and health Survey 2011

42
Indicator 12: Exclusive Breastfeeding for the First Six MonthsKey question: What is the percentage of babies 0<6 months of age exclusively breastfed1 in the last 24 hours? 70 %
Guideline:Indicator 12 Key to rating adapted from WHO tool IBFAN Asia Guideline for WBTi
Exclusive Breastfeeding (for first 6 months)
Scores Colour-rating0.1-11% 3 Red11.1-49% 6 Yellow49.1-89% 9 Blue89.1-100% 10 Green
Although it has been strongly recommended that exclusive breastfeeding for the first six months is very crucial for survival, growth and development of infants and young children. It lowers the risk of diarrheal diseases. Nepal Demographic Health Survey (NDHS 2011) indicates that exclusive breastfeeding in children 0-6 months has increased to 70% in 2011, from 53% in 2006. Children who are not exclusively breasted are given water, other milks and foods in addition to breast milk. These negative practices are prevailing even among very young children.
Data source1. Nepal Demographic and health Survey 2011
Indicator 13: Median Duration of BreastfeedingKey question: Babies are breastfed for a median duration of how many months?33.6 months
Guideline:Indicator 13 Key to rating adapted from WHO tool IBFAN Asia Guideline for WBTi
Median Duration of Breastfeeding
Scores Colour-rating0.1-18 Months 3 Red
18.1-20 ’’ 6 Yellow20.1-22 ’’ 9 Blue
22.1- 24 or beyond ’’ 10 Green
The Innocenti Declaration 1990 and the Global Strategy for Infant and Young Child feeding 2002 recommend that babies continue to be breastfed for two years of age or beyond along with adequate and appropriate complementary foods starting after six months of age. Breast milk continues to be an important source of nutrition and fluids and immunological protection for the infant and the young child. Breastfeeding practice brings mother and child into a bonding and interaction between mother and child leading to an optimal development of the infant and young child.
It is interesting to note that median duration of breastfeeding in Nepal is exceptionally high i.e. 33.6 months and it needs to be maintained in future as well. Such longer duration of breastfeeding is the result of tradition of it throughout Nepal.
Data Source (including year): 1. Nepal Demographic and health Survey 2011

43
Indicator 14: Bottle feeding Key question: What percentage of breastfed babies 0-12 months of age, who are fed with any foods or drinks (even breast milk) from bottles? 6%
Guideline:Indicator 14 Key to rating adapted from WHO tool IBFAN Asia Guideline for WBTi
Bottle Feeding (0-12 months)
Scores Colour-rating29.1-100% 3 Red4.1-29% 6 Yellow2.1-4% 9 Blue0.1-2% 10 Green
Babies should be breastfed exclusively for first 6 months of age and they need not be given other fluids, fresh or tinned milk formulas or animal milk would cause more harm to babies and deprive the child from the inevitable benefits of breast milk. However, after six months babies should ideally receive mother’s milk along with solid complementary foods. Baby should be fed with a cup or from infant feeding tube even if a baby is unable to feed the breast milk form mothers breast. After six months of age, the child should be given any liquids or water using cup but not by bottle because feeding bottles with artificial nipples and pacifiers (teats or dummies) may cause nipple confusion and infant’s refusal of the breast after their use. Further, feeding bottles are more difficult to keep clean than cups and easily contaminated leading to illness of you children. Nepal data revealed that 6% of baby is bottle fed which is almost doubled as compared to 3% in 2006.
Data Source1. Nepal Demographic and health Survey 2011

44
Indicator 15: Complementary feeding - Introduction of solid, semi-solid or soft foodsKey question: Percentage of breastfed babies receiving complementary foods at 6-8 months of age? 70%
Guideline: Indicator 15 WHO’s IBFAN Asia Guideline for WBTi
Complementary Feeding (6-8 months)
Key to rating Scores Colour-rating0.1-59% 3 Red59.1-79% 6 Yellow79.1-94% 9 Blue94.1-100% 10 Green
Mother’s milk alone is not enough after completion of 6 months as babies grows continuously and need additional nutrients. Complementary feeding should begin with locally available, affordable and easily prepared indigenous foods. Babies should be offered soft or mashed foods in small quantities 3-5 times per day recommended energy dense and food diversity depending upon their age. The foods those are complementary to breast milk to the babies increase should gradually increase as the baby grows. Maintaining basic hygiene in food preparation and feeding is crucial. Responsive feeding is also recommended for child feeding that helps interact with child for overall development and mental development through stimulation.
Data source1. Nepal Demographic and health Survey 2011
Summary Part II: Infant and young child feeding (IYCF) practicesIYCF Practice Result ScoreIndicator 11 Starting Breastfeeding (Initiation) 45 % 6Indicator 12 Exclusive Breastfeeding for first 6 months 70 % 9Indicator 13 Median duration of Breastfeeding 33.6 % 10Indicator 14 Bottle-feeding 6% 6Indicator 15 Complementary Feeding 70% 6Score Part II (Total) 37
IBFAN Asia Guidelines for WBTi Total score of infant and young child feeding Practice (indicators 11-15) are calculated out of 50.
Scores Colour-rating0 – 15 Red16 - 30 Yellow31 - 45 Blue46 – 50 Green
Conclusions Regarding breastfeeding practices, the median duration of breastfeeding is being practiced for satisfactory duration. Howevere, there is still need to improve on initiation of breastfeeding within one hour of birth and exclusively breastfeeding. In order to sustain the achievement made, initiation of breastfeeding within an hour of birth needs activities addressing avoidance of prelacteal feeding practices and provision of support for initiation of breastfeeding at hospitals to community level.

45
Total of Part I and Part II (indicator 1-15): IYCF Practices and Policies and Programmes
Total score of infant and young child feeding practices, policies and programmes (indicators 1-15) are calculated as 92 out of 150. Countries are then rated as:Scores Colour- rating0 – 45.5 Red46 – 90.5 Yellow91 – 135.5 Blue136 – 150 Green
Key Gaps• Budgets had not been adequate for implementation of policy and programs• Inadequate co-ordination mechanism though the Nutrition Technical Committee and Breast
feeding promotion and protection committee (BPPC) at high level• BFHI policy has not been completely adopted by hospitals as there is lack of monitoring of
hospitals for BFHI.• Weak policy and legislation regarding breastfeeding that covers employees in Governmental,
Private and informal sectors• Inadequate provision of breastfeeding break/creche in all sectors including formal ones.• Adequate number of health professionals has not received practical training on IYCF in pre-
services education program.• There are inadequate services on counselling pregnant and breastfeeding mothers in outreach
clinic• IEC materials are not adequate with emphasis on risks of artificial feeding.• Still there is inadequate human resources and implementation experiences in infant feeding
during emergency.• A national level monitoring and evaluation system has integrated three core BF indicators in
program activities but there is lack of regular monitoring and evaluation in terms of baseline and follow up data to measure outcomes.
Key Recommendations• Strengthening for effective implementation of National Nutrition Policy and Strategy and
guidelines along with clear plan of action with budget allocation• Strengthening of coordination mechanism between BPPC and Nutrition Technical Committee
and inclusion of other sectors in the committee for effective implementation of all components of Breastfeeding.
• There is an urgent need to revitalize BFHI hospitals.• Strengthening advocacy from governmental and non-governmental organization on maternity
protection act is needed.• There should be increased awareness programs for women regarding maternity protection.• There should be increased number of IEC materials about the risk of artificial feeding.• National communication strategy for infant and young child feeding should be implemented to
the community level.• To promote IEC strategy electronic and print media should be utilized more.• Review on existing situation of implementation of infant feeding in HIV is needed.

46
• Initiation and establishment of regular monitoring and evaluation system with focus on key all IYCF indicators suggested
• Integration of adequate indicators of complementary feeding into national health management information system by segregation of data by age
• There should be effective action plan to improve initiation of breastfeeding practices emphasizing initiation of breast feeding, exclusive breast feeding and timely initiation of complementary feeding.

47
Workshopon
World Breastfeeding Trends Initiative (WBTi) 2015Kathmandu, Nepal
Date: 1st Chaitra, 2072 (14th March, 2016)
Day: Monday
Venue: National Health Training Centre, Teku, Kathmandu
Time: 11:00 AM – 1:00 PM
Programme: Time Particulars11:00-11:30 A.M Inauguration of Workshop
Welcome speech by • Prof. Prakash Sunder Shrestha,
President NEBPROF
Remarks by • Dr. Rajendra Prasad Pant
Director, Child Health Division• Dr. R.P. Biccha
Director, Family Health Division• Mr. Giri Raj Subedi
Chief, Nutrition Section, Child Health Division
11:30-11:45 A.M Overview of WBTi Dr. Kalpana TiwariChairpersonNutrition Health Research & Community Services
11:45-12:30 P.M WBTi 2015 Dr. Srijana BasnetAsst. ProfessorDept. of Child HealthInstitute of Medicine
12:30-12:55 P.M Interaction with the Participants12:55-1:00 P.M Vote of Thanks Dr. Merina Shrestha
Asst. ProfessorDept. of Child HealthInstitute of Medicine
1:00-1:30 P.M Refreshment
Master of Ceremony:
Mrs. Tulashi AdhikariAsst. ProfessorMaharajgunj Nursing Campus

48
World Breastfeeding Trend Initiative (WBTi)
Kalpana Tiwari, Ph.D (Foods and Nutrition)Chairperson, Nutrition Health Research and Community Services
What is World Breastfeeding Trends Initiative(WBTi)?
Global Initiative and a system led by IBFAN Participatory, assessment and analysis of GS
for IYCF Identify gaps and build consensus on
actions to bridge them
Why WBTi needed?
• A worldwide civil society-led initiative aiming to accelerate progress in attaining the health-related MDGs-4
• Tracking, assessment and Monitoring(TAM) GS for IYCF (2002) for advocacy and programing
• Each country urged to develop, implement, monitor and evaluate a PoA on IYCF
• Innocent Declaration on IYCF (2005)
Objectives of WBTi• To provide governments , other agencies and their
international development assistance partners with critical information needed to bridge gaps in IYCF Policy and Practice
• To provide evidence for IBFAN groups to advocate for greater effort and investment to promote early and exclusive breastfeeding in respective countries
• To contribute to attaining MDG-4 reducing under five child mortality and MDG -5 improving women’s health
What is the Basis for WBTi?
• Methodology and approach of GLOPAR 1993• WBTi is an extension of GLOPAR and
GLOPAR initiative encourage groups to assess breastfeeding practices in each countries and use information for advocacy to impact policy development
• WHO’s tool “Infant and Young Child: A tool for assessing national practices, policies, and programs” ( 2014)
How WBTi works?Phase 1- National assessmentPhase 2 – Ranking the country/regionPhase 3- Reassessment to analyze trends
Assessment
Gap Identification
Action
Policy Changes
Practices Changes
Slide 1
Slide 2
Slide 3
Slide 4
Slide 5
Slide 6

49
What is the assessment process?
• Using 15 indicators-quantitative• Documenting achievements and gaps in
the existing policy, program and practices in reference to IYCF
What goes in?• Coordination• Training/orientation• Organizing consultations and discussions
leading to national assessment• Analyzing and publishing the country report
cards• Compiling and publishing state of world’s
breastfeeding nationally and regionally• Publishing results through WBTi web tool
Cont……….
• Follow up and offer IBFAN services for capacity building in code implementation, planning, and programs related to IYCF
• Advocacy with the use of report cards at national, regional and global levels to seek support for bridging gaps in program and policy
Indicator- Part I1. National Policy Program and Coordination2. BFHI ( 10 Steps)3. Implementation of BMS Code4. Maternity Protection5. Health and Nutrition care system6. Mother support and community outreach7. Information support8 Infant feeding and HIV9. Infant feeding during emergencies10. Monitoring and Evaluation
Indicator Part-II
11. Early initiation rate12. Exclusive breastfeeding rates <6
months13. Median duration of breastfeeding14. Bottle feeding rates15. Timely complementary feeding rates
Indicator Part-II
11. Early initiation rate12. Exclusive breastfeeding rates <6
months13. Median duration of breastfeeding14. Bottle feeding rates15. Timely complementary feeding rates
Slide 7
Slide 8
Slide 9
Slide 10
Slide 11
Slide 12

50
Colour rating of IYCF Policies and Programmes
IBFAN Asia Guidelines for WBTiScores Colour-rating
0 – 30.9 Red
31 – 60.9 Yellow
61 – 90.9 Blue
91 – 100 Green
Colour Rating of One indicator of IYCF Policies and Programmes
IBFAN Asia Guidelines for WBTiScores Colour - rating
0-3.5 Red4-6.5 Yellow7-9 Blue>9 Green
Thank You
Slide 13
Slide 14
Slide 15
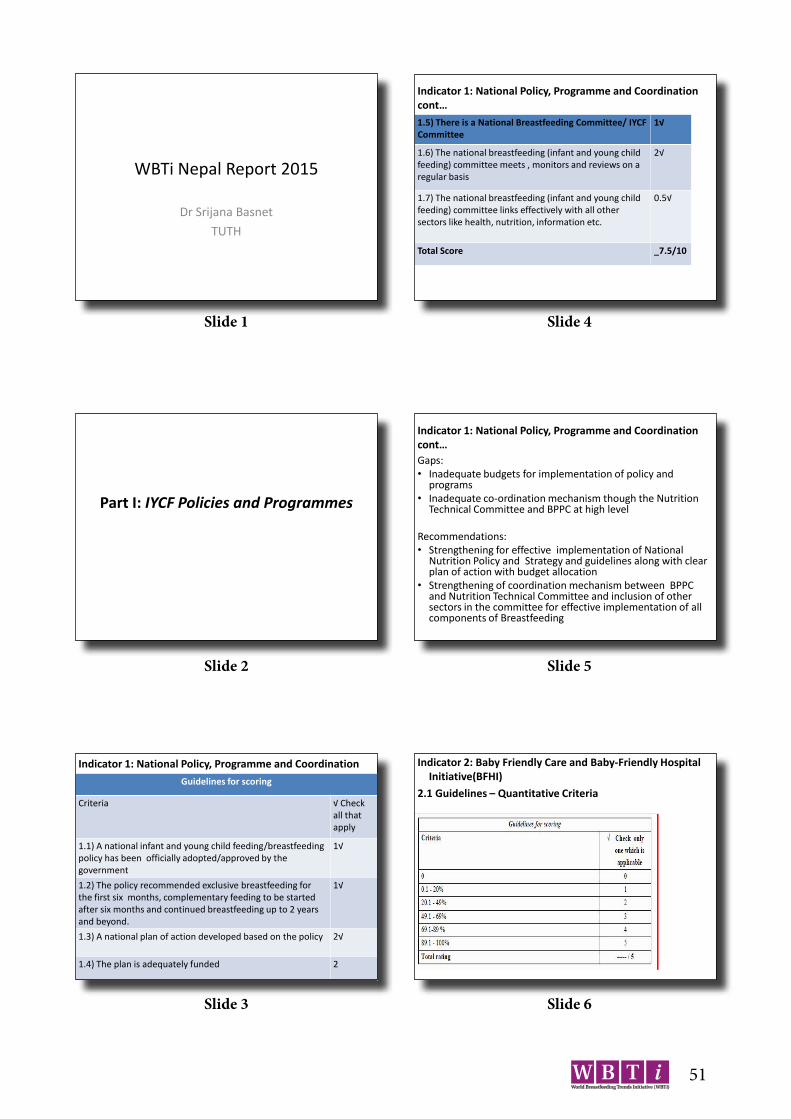
51
Indicator 1: National Policy, Programme and Coordination cont…1.5) There is a National Breastfeeding Committee/ IYCF Committee
1√
1.6) The national breastfeeding (infant and young child feeding) committee meets , monitors and reviews on a regular basis
2√
1.7) The national breastfeeding (infant and young child feeding) committee links effectively with all other sectors like health, nutrition, information etc.
0.5√
Total Score _7.5/10
Indicator 1: National Policy, Programme and Coordination cont…Gaps: • Inadequate budgets for implementation of policy and
programs• Inadequate co-ordination mechanism though the Nutrition
Technical Committee and BPPC at high level
Recommendations:• Strengthening for effective implementation of National
Nutrition Policy and Strategy and guidelines along with clear plan of action with budget allocation
• Strengthening of coordination mechanism between BPPC and Nutrition Technical Committee and inclusion of other sectors in the committee for effective implementation of all components of Breastfeeding
Indicator 2: Baby Friendly Care and Baby-Friendly Hospital Initiative(BFHI)
2.1 Guidelines – Quantitative Criteria
Part I: IYCF Policies and Programmes
Indicator 1: National Policy, Programme and CoordinationGuidelines for scoring
Criteria √ Check all that apply
1.1) A national infant and young child feeding/breastfeeding policy has been officially adopted/approved by the government
1√
1.2) The policy recommended exclusive breastfeeding for the first six months, complementary feeding to be started after six months and continued breastfeeding up to 2 years and beyond.
1√
1.3) A national plan of action developed based on the policy 2√
1.4) The plan is adequately funded 2
WBTi Nepal Report 2015
Dr Srijana BasnetTUTH
Slide 1
Slide 2
Slide 3
Slide 4
Slide 5
Slide 6
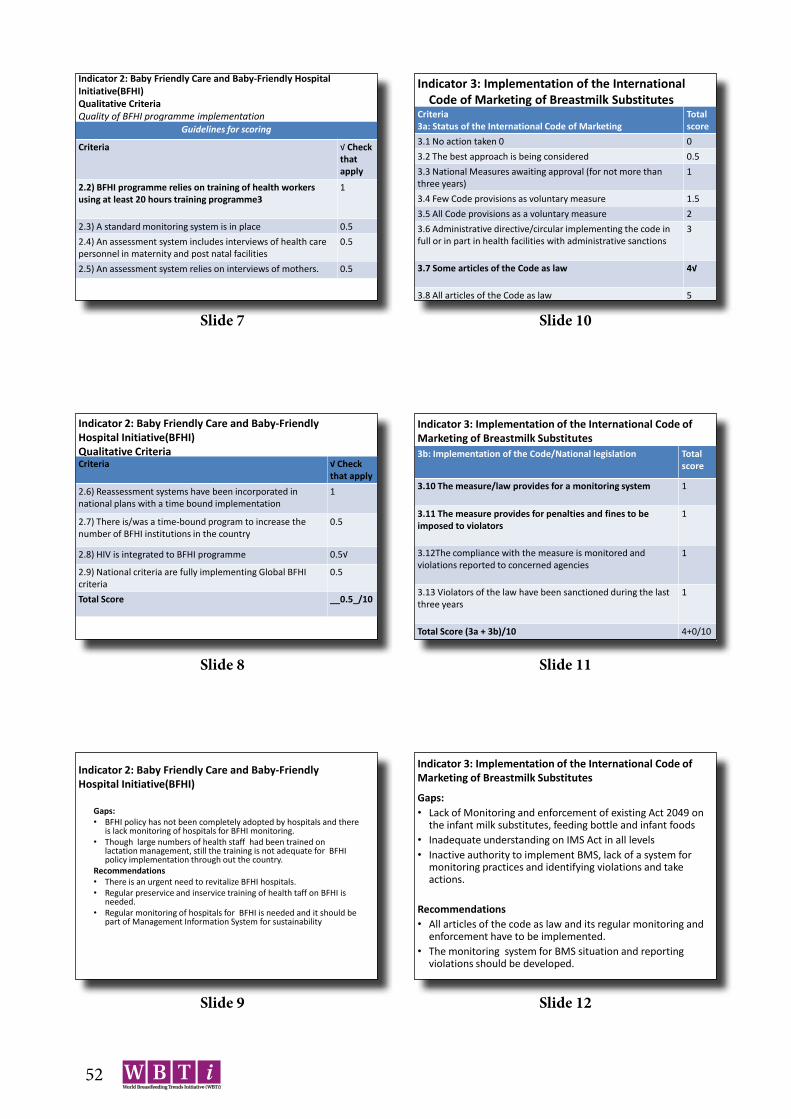
52
Indicator 2: Baby Friendly Care and Baby-Friendly Hospital Initiative(BFHI)Qualitative CriteriaQuality of BFHI programme implementation
Guidelines for scoring
Criteria √ Check that apply
2.2) BFHI programme relies on training of health workers using at least 20 hours training programme3
1
2.3) A standard monitoring system is in place 0.52.4) An assessment system includes interviews of health carepersonnel in maternity and post natal facilities
0.5
2.5) An assessment system relies on interviews of mothers. 0.5
Indicator 2: Baby Friendly Care and Baby-Friendly Hospital Initiative(BFHI)Qualitative CriteriaQuality of BFHI programme implementationCriteria √ Check
that apply2.6) Reassessment systems have been incorporated in national plans with a time bound implementation
1
2.7) There is/was a time-bound program to increase the number of BFHI institutions in the country
0.5
2.8) HIV is integrated to BFHI programme 0.5√
2.9) National criteria are fully implementing Global BFHI criteria
0.5
Total Score __0.5_/10
Indicator 2: Baby Friendly Care and Baby-Friendly Hospital Initiative(BFHI)
Gaps:• BFHI policy has not been completely adopted by hospitals and there
is lack monitoring of hospitals for BFHI monitoring.• Though large numbers of health staff had been trained on
lactation management, still the training is not adequate for BFHI policy implementation through out the country.
Recommendations• There is an urgent need to revitalize BFHI hospitals.• Regular preservice and inservice training of health taff on BFHI is
needed.• Regular monitoring of hospitals for BFHI is needed and it should be
part of Management Information System for sustainability
Indicator 3: Implementation of the International Code of Marketing of Breastmilk Substitutes
Criteria3a: Status of the International Code of Marketing
Totalscore
3.1 No action taken 0 03.2 The best approach is being considered 0.53.3 National Measures awaiting approval (for not more than three years)
1
3.4 Few Code provisions as voluntary measure 1.53.5 All Code provisions as a voluntary measure 23.6 Administrative directive/circular implementing the code in full or in part in health facilities with administrative sanctions
3
3.7 Some articles of the Code as law 4√
3.8 All articles of the Code as law 5
Indicator 3: Implementation of the International Code of Marketing of Breastmilk Substitutes3b: Implementation of the Code/National legislation Total
score
3.10 The measure/law provides for a monitoring system 1
3.11 The measure provides for penalties and fines to be imposed to violators
1
3.12The compliance with the measure is monitored and violations reported to concerned agencies
1
3.13 Violators of the law have been sanctioned during the last three years
1
Total Score (3a + 3b)/10 4+0/10
Indicator 3: Implementation of the International Code of Marketing of Breastmilk Substitutes
Gaps: • Lack of Monitoring and enforcement of existing Act 2049 on
the infant milk substitutes, feeding bottle and infant foods • Inadequate understanding on IMS Act in all levels• Inactive authority to implement BMS, lack of a system for
monitoring practices and identifying violations and take actions.
Recommendations• All articles of the code as law and its regular monitoring and
enforcement have to be implemented.• The monitoring system for BMS situation and reporting
violations should be developed.
Slide 7
Slide 8
Slide 9
Slide 10
Slide 11
Slide 12

53
Indicator 4: Maternity Protection Guidelines for scoring
Criteria Tick one
4.1) Women covered by the national legislation are allowed the following weeks of paid maternity leavea. Any leave less than 14 weeksb. 14 to 17weeksc. 18 to 25 weeksd. 26 weeks or more
0.5√11.52
4.2) Women covered by the national legislation are allowed at least one breastfeeding break or reduction of work hrs /da. Unpaid breakb. Paid break
0.51
4.3) Legislation obliges private sector employers of women in the country toa. Give at least 14 weeks paid maternity leaveb. Paid nursing breaks.
0.50.5
Indicator 4: Maternity protection contd…..
Gaps:• Weak policy and legislation regarding breastfeeding that covers
all employers in Governmental and Private and informal sectors• Maternity leave in governmental and private sector is
inadequate.• There has not been adequate provision of breastfeeding
break/crèche in all sector including formal ones.Recommendations:• Strengthening advocacy from governmental and non-
governmental organization on maternity protection act is needed.
• There should be increased number of awareness programmesregarding maternity protection.
• Provision of breastfeeding break and places in formal and informal sectors is required.
Indicator 4: Maternity protection contd….4.4) There is provision in national legislation that provides for work siteaccommodation for breastfeeding and/or childcare in work places in theformal sector. a. Space for Breastfeeding/Breastmilk expressionb. Crèche
10.5√
4.5) Women in informal/unorganized and agriculture sector are:a. accorded some protective measuresb. accorded the same protection as women working in the formal sector
0.51
4.6) a. Information about maternity protection laws, regulations, or policies ismade available to workers.b. There is a system for monitoring compliance and a way for workers to complain if their entitlements are not provided.
0.5
0.5
Indicator 5: Health and Nutrition Care Systems (in support ofbreastfeeding & IYCF)
√ Check that apply
Criteria adequate inadequate No reference
5.1) A review of health provider schools and preservice education programmes for health professionals, social and community workers in the Country indicates that infant and young child feeding curricula or session plans are adequate/inadequate
2 1√ 0
5.2) Standards and guidelines for mother-friendly childbirth procedures and support have been developed and disseminated to all facilities and personnel providing maternity care.
2 1√ 0
Indicator 4: Maternity protection contd…..4.7) Paternity leave is granted in public sector for at least 3 days.
0.5√
4.8) Paternity leave is granted in the private sector for at least 3 days.
0.5
4.9) There is legislation providing health protection for pregnant and breastfeeding workers: they are informed about hazardous conditions in theworkplace and provided alternative work at the same wage until they are nolonger pregnant or breastfeeding.
0.5
4.10) There is legislation prohibiting employment discrimination and assuringjob protection for women workers during breastfeeding period.
1
Total Score: 1.5/10
Indicator 5: Health and Nutrition Care Systems (in support ofbreastfeeding & IYCF)5.3) There are in-service training programmes providing knowledge and skills related to IYCF for relevant health/nutrition care providers
2 1√ 0
5.4) Health workers are trained on their responsibility under the Code implementation / national regulation throughout the country.
1 0.5√ 0
5.5) IYCF information and skills are integrated, as appropriate, into training programmes
1√
0.5 0
5.6) In-service training programmes referenced in 5.5 are being provided throughout the country
1 0.5√ 0
5.7) Child health policies provide for mothers andbabies to stay together when one of them is sick.
1 0.5√ 0
Total Score: _5.5_/10
Slide 13
Slide 14
Slide 15
Slide 16
Slide 17
Slide 18

54
Indicator 5: Health and Nutrition Care Systems (in support ofbreastfeeding & IYCF)Gaps:• Adequate number of health professionals has not been
received practical training on IYCF in pre-services education program.
• Health workers are not adequately trained on Code implementation.
Recommendations:• Implementation and integration of IYCF practical skills
in curriculum of health professionals eg: nursing and paramedics.
• Lactation management training should be incorporated as a part of continuous medical education.
Indicator 6: Mother Support and Community Outreach –Communitybased support for the pregnant and breastfeeding mother contd..
Gaps:• There are inadequate services on counseling
pregnant and breastfeeding mothers in outreach clinic
• Inadequate counseling and listening skills among community level workers
• Lack of crèche facilities in both government and private sectors.
Recommendations:• There should be more trainings on lactation
management skills for village Level Health Workers for comprehensive intervention on IYCF to support at community level or outreach clinic.
Indicator 6: Mother Support and Community Outreach – Communitybased support for the pregnant and breastfeeding mother
Guidelines for scoring
Criteria Scoring √Check that apply
Yes To some degree
No
6.1) All pregnant women have access to community-based ante-natal and post -natal support systems with counseling services on infant and young child feeding.
2 1√ 0
6.2) All women receive support for infant and young child feeding at birth for breastfeeding initiation.
2 1√ 0
6.3) All women have access to counseling support for IYCF counseling and support services have national coverage.
2 1√ 0
Indicator 7: Information Supportcriteria yes To some
degreeNo
7.1) There is a national IEC strategy for improving IYCF that ensures all information and materials are free from commercial influence/ potential conflicts or interest are avoided.
2√ - 0
7.2a) National health/nutrition systems include individual counseling on IYCF
1√ 0.5 0
7.2b) National health/nutrition systems include group education and counseling services on IYCF
1√ 0.5 0
7.3) IYCF IEC materials are objective, consistent and in line with national and/or international recommendations and include information on the risks of artificial feeding
2√ 1 0
Indicator 6: Mother Support and Community Outreach –Communitybased support for the pregnant and breastfeeding mother contd..6.4) Community-based counseling through Mother Support Groups (MSG) and support services for the pregnant and breastfeeding woman are integrated into an overall infant and young child health and development policy IYCF/Health/Nutrition Policy.
2√ 1 0
6.5) Community-based volunteers and health workers are trained in counseling skills for infant and young child feeding.
2 1√ 0
Total Score: _6_/10
Indicator 7: Information support contd…..
7.4. IEC programmes (eg World Breastfeeding Week) that include IYCF are being implementedat local level and are free from commercial influence
2√ 1 0
7.5 IEC materials/messages to include information on the risks of artificial feeding in line with WHO/FAO Guidelines on preparation and handling of powdered infant formula (PIF).
2 0√ 0
Total ------8--/10
Slide 19
Slide 20
Slide 21
Slide 22
Slide 23
Slide 24

55
Indicator 7: Information support contd…..Gaps:IEC materials is not adequate with emphasis on
risks of artificial feeding.Recommendations:• There should be increased number of IEC
materials about the risk of artificial feeding.• There should be a IEC materials with guidelines
on preparation and handling of artificial feeding in specified conditions.
• Adequate budget allocation to IEC on IYCF at central / district level
Indicator 8: Infant Feeding and HIVcriteria Yes To some
DegreeNo
8.1) The country has a comprehensive updated policy in line with international Guidelines on IYCF that includes infant feeding and HIV
2√ 1 0
8.2) The infant feeding and HIV policy gives effect to the International Code/ National Legislation
1√ 0.5 0
8.3) Health staff and community workers receive training on HIV and infant feeding policies, the risks associated with various feeding options for infants of HIV-positive mothers and how to provide counsellingand support.
1 0.5√ 0
8.4) HIV Testing and Counselling (HTC)/ Provide Initiated HIVTesting and Counselling (PIHTC)/ Voluntary and Confidential Counselling and Testing (VCCT) is available and offered routinely to couples who are considering pregnancy and to pregnant
1 0.5√ 0
Indicator 8: Infant feeding and HIV contd….
8.5) Infant feeding counselling in line with current international recommendations and appropriate to local circumstances is provided to HIV positive mothers.
1 0.5√ 0
8.6) Mothers are supported in carrying out the recommended national infant feeding practices with further counselling and follow-up to make implementation of these practices feasible.
1 0.5√ 0
Indicator8: Infant feeding and HIV contd….
8.8) Special efforts are made to counter misinformation on HIV and infant feeding and to promote, protect and support 6 months ofexclusive breastfeeding and continued breastfeeding in the general population.
1 0.5√ 0
8.9) On-going monitoring is in place to determine the effects of interventions to prevent HIV transmission through breastfeedingon infant feeding practices and overall health outcomes for mothers and infants, including those who are HIV negative or ofunknown status.
1 0.5√ 0
Total _6_/10
Indicator8: Infant feeding and HIV contd….
Gaps:• Iinadequate advocacy and implementation of policy and
guidelines at all levels.• Lack of trainings to health workers on infant feeding in HIV.• Lack of monitoring system to determine the effects of
intervention to prevent HIV transmission through BF on infant feeding practices who are unknown of the situation
Recommendations:• Review on existing situation of implementation of infant
feeding in HIV is needed• Revitalized BFHI required inclusion of training on PMTCT • Strengthen implementation of policy and strategies and
initiate regular monitoring of it.
Indicator 9:IYCF during Emergencies
criteria Yes To someDegree
No
9.1) The country has a comprehensive policy on IYCF that includes infant feeding in emergencies and contains all basic elements included in the IFE Operational Guidance
2√ 1 0
9.2) Person(s) tasked with responsibility for national coordination with all relevant partners such as the UN, donors, military and NGOs regarding iIYCF in emergency situations have been appointed
2√ 1 0
Slide 25
Slide 26
Slide 27
Slide 28
Slide 29
Slide 30
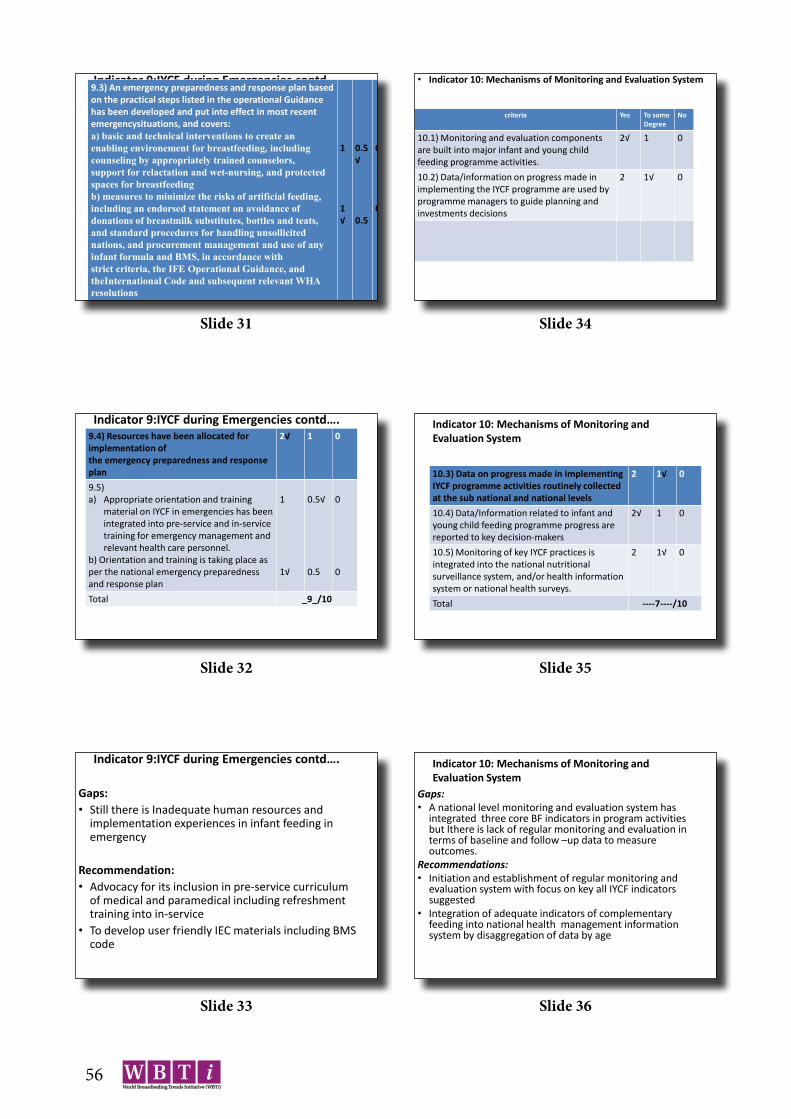
56
Indicator 9:IYCF during Emergencies contd….9.3) An emergency preparedness and response plan based on the practical steps listed in the operational Guidance has been developed and put into effect in most recent emergencysituations, and covers:a) basic and technical interventions to create an enabling environement for breastfeeding, including counseling by appropriately trained counselors,support for relactation and wet-nursing, and protected spaces for breastfeedingb) measures to minimize the risks of artificial feeding, including an endorsed statement on avoidance of donations of breastmilk substitutes, bottles and teats,and standard procedures for handling unsollicitednations, and procurement management and use of any infant formula and BMS, in accordance withstrict criteria, the IFE Operational Guidance, and theInternational Code and subsequent relevant WHAresolutions
1
1√
0.5√
0.5
0
0
• Indicator 10: Mechanisms of Monitoring and Evaluation System
criteria Yes To someDegree
No
10.1) Monitoring and evaluation components are built into major infant and young child feeding programme activities.
2√ 1 0
10.2) Data/information on progress made in implementing the IYCF programme are used by programme managers to guide planning and investments decisions
2 1√ 0
Indicator 9:IYCF during Emergencies contd….9.4) Resources have been allocated for implementation ofthe emergency preparedness and response plan
2√ 1 0
9.5)a) Appropriate orientation and training
material on IYCF in emergencies has been integrated into pre-service and in-service training for emergency management and relevant health care personnel.
b) Orientation and training is taking place as per the national emergency preparedness and response plan
1
1√
0.5√
0.5
0
0
Total _9_/10
Indicator 10: Mechanisms of Monitoring and Evaluation System
10.3) Data on progress made in implementing IYCF programme activities routinely collected at the sub national and national levels
2 1√ 0
10.4) Data/Information related to infant andyoung child feeding programme progress are reported to key decision-makers
2√ 1 0
10.5) Monitoring of key IYCF practices is integrated into the national nutritionalsurveillance system, and/or health information system or national health surveys.
2 1√ 0
Total ----7----/10
Indicator 9:IYCF during Emergencies contd….
Gaps:• Still there is Inadequate human resources and
implementation experiences in infant feeding in emergency
Recommendation:• Advocacy for its inclusion in pre-service curriculum
of medical and paramedical including refreshment training into in-service
• To develop user friendly IEC materials including BMS code
Indicator 10: Mechanisms of Monitoring and Evaluation System
Gaps:• A national level monitoring and evaluation system has
integrated three core BF indicators in program activities but lthere is lack of regular monitoring and evaluation in terms of baseline and follow –up data to measure outcomes.
Recommendations:• Initiation and establishment of regular monitoring and
evaluation system with focus on key all IYCF indicators suggested
• Integration of adequate indicators of complementary feeding into national health management information system by disaggregation of data by age
Slide 31
Slide 32
Slide 33
Slide 34
Slide 35
Slide 36

57
Indicator 12 Key to rating adapted fromWHO tool
IBFAN Asia Guideline for WBTi
ExclusiveBreastfeeding (forfirst 6 months)
scores Colour rating Existing status
0.1-11.1% 3 Red
11.1-49% 6 Yellow
49.1-89% 9 Blue 70%
89.1-100% 10 green
Part II: Infant and Young Child Feeding Practices
Indicator 13 Key to rating adapted fromWHO tool
IBFAN Asia Guideline for WBTi
MedianDuration ofBreastfeeding
scores Colour rating Existing status
0.1-18 Months
3 Red
18.1-20 Months
6 Yellow
20.1-22 Months
9 Blue
22.1-24Months
10 green 33.6 months
Indicator 11 Key to rating adapted fromWHO tool
IBFAN Asia Guideline for WBTi
Initiation of Breastfeeding(within 1 hour)
scores Colourrating
Existing status
0.1-29% 3 Red
29.1-49% 6 Yellow 45%
49.1-89% 9 Blue
89.1-100% 10 green
Indicator 14 Key to rating adapted fromWHO tool
IBFAN Asia Guideline for WBTi
Bottle Feeding(0-12 months)
scores Colour rating Existing status
29.1-100% 3 Red
4.1-29% 6 Yellow 6%
2.1- 4% 9 Blue
0.1-2% 10 green
Slide 37
Slide 38
Slide 39
Slide 40
Slide 41
Slide 42

58
Indicator 15
Key to rating adapted fromWHO tool
IBFAN Asia Guideline for WBTi
Complementary Feeding(6-8 months)
scores Colourrating
Existing status
0.1-59% 3 Red
59.1-79% 6 Yellow 70%
79.1-94% 9 Blue
94.1-100% 10 green
Slide 43
59
List of the participantsWorkshop on
World Breastfeeding Trends Initiative (WBTi) 2015Date: 14th March 2016Time: 11:00-01:00 P.MVenue: National Health Training Centre, TekuS.N. Name Designation Organization Email Address
1 Shree Laxmi Singh Sister TUTH2 Kalpana Rajbhandari Sister TUTH3 Dr. Dhana Raj Aryal [email protected] Dr. Prakash S. Shrestha Professor NEBPROF [email protected] Dr. Merina Shrestha Asst. Prof TUTH/NEBPROF6 Nina Rijal Advocate NPCS [email protected] Tulashi Adhikari Lecturer IOM, Maharajgunj [email protected] Dr. Kalpana Upadhyay
SubediChief Consulstant Peditrician
PMWH [email protected]
9 Dr.Kalpana Tiwari Chairperson, NHRCS
Nutrition Health Research & Community Services
10 Dr. Srijana Basnet Asst. Prof IOM, TUTH [email protected] Giri Raj Subedi Sr. PHO CHD [email protected] Sumit Karn Nutrition Specialist FAO [email protected] Smriti Bartaula NPO CHD [email protected] Sarita Paudel Admin Assistant CHD [email protected] Dr. R.M Shrestha Chief Pediatric
Dept.Civil Hospital [email protected]
16 Mr. Hari K. Shrestha Ad. Officer NEPAS [email protected] Dr. Atul Upadhya Sr. Project Manager Helen Keller
18 Dr. Dharma S. Manandhar President MIRA [email protected] Rajan Mandal NPO MI [email protected] Durga Das Ulak PHO CHD [email protected] Dr. K.P. Bista NEPAS/G.S NEPAS [email protected] R.L. Dhabhadel NEBRPOF
TreasureNEBPROF
23 Yogendra Neupane PHO CHD24 Dr.M.R.Baral Professor, PESON [email protected] Uma Koirala Professor TU26 Asha Rai Prog. Officer Jhpiego [email protected] Dr. Bhesh Raj Pokhrel SIMO NCASC [email protected] Chuda Mani Bhandari Chief/IMNCI CHD29 Dr. R.P. Pant Director CHD30 Jyoti Saran Shrestha M&E Asst. CHD shresthajyotisaran@gmail.
com31 Dr. Arjun Sapkota Sr. EMU CHD [email protected] Bhinsen Pant PHI CHD [email protected] Bindu Shrestha PHO CHD34 Ashesh Regmi PHO CHD [email protected] Sheela Shrestha HEO NHEICC36 Dr. R.P. Bichha Director FHD37 Kopila Shrestha Nsg. Director TUTH [email protected] Mina Sarju Nsg. Supervisor TUTH [email protected] Sushila Adhikari Sister TUTH40 Prem L. Khagi Nsg. Officer TUTH [email protected] Ramesh Kumar Pokhrel A.D CHD42 Sharada Adhikari C. Officer CHD a.sharada772gmail.com