nhi teveten
TRANSCRIPT

Cardiovascular and Cerebrovascular health in the management of hypertensive patients

Not all ARBs looks after your patient heart as well as
his mind

Cardiovascular Disease: A Worldwide Epidemic
World Health Organization Burden of Disease Estimates 2002.
0 5 10 15 20 25 30 35 40 45 50
CVDs
Infectious/parasitic diseases
Malignant neoplasms
Respiratory infections
Respiratory diseases
Unintentional injuries
Perinatal conditions
Digestive diseases
Intentional injuries
Neuropsychiatric conditions
Diabetes mellitus
Cause of death
Worldwide
Developed world
CVD is responsible for one third of all deaths worldwide and almost half of all deaths in the developed world

Contribution of Risk Factors to Burden of Disease Mortality*
*Based on The World Health Report 2003. *Based on The World Health Report 2003. Yach et al. Yach et al. JAMAJAMA. 2004;291:2616-2622.. 2004;291:2616-2622.
0 5 10 15 20
Percentage of Mortality Attributable to Risk Factors
Developing Developing
countries countries Developed Developed countriescountries
Blood pressureBlood pressure
TobaccoTobacco
UnderweightUnderweight
AlcoholAlcohol
CholesterolCholesterol
Unsafe sexUnsafe sex
OverweightOverweightUnsafe water, sanitation, Unsafe water, sanitation,
hygienehygieneLow fruit and vegetable Low fruit and vegetable intakeintake
Indoor smoke from solid fuelsIndoor smoke from solid fuels
Physical inactivityPhysical inactivity

Hypertension: A Growing Problem
Prevalence (%)
United StatesUnited States77
EgyptEgypt99
JapanJapan88
ItalyItaly77
SwedenSweden77
EnglandEngland77
SpainSpain77
FinlandFinland77
GermanyGermany77
00 1010 2020 3030 4040 5050
TaiwanTaiwan99
CanadaCanada77
South KoreaSouth Korea99
*Defined as systolic/diastolic blood pressure *Defined as systolic/diastolic blood pressure ≥≥140/90, (140/90, (≥≥160/95 for Taiwan)160/95 for Taiwan) or receiving treatment. or receiving treatment. ††South Korea is defined as men, aged 30 to 59. South Korea is defined as men, aged 30 to 59. 7. Wolf-Maier et al. 7. Wolf-Maier et al. JAMAJAMA. 2003;289:2363-2369; 8. Data on file. Pfizer Inc, New York, NY;. 2003;289:2363-2369; 8. Data on file. Pfizer Inc, New York, NY;9. 9. WHO Collaborating Centre on Surveillance of Cardiovascular Disease Web site. Available at: www.cvdinfobase.ca. Accessed February 22, 2005.WHO Collaborating Centre on Surveillance of Cardiovascular Disease Web site. Available at: www.cvdinfobase.ca. Accessed February 22, 2005.

Lewington et al. Lancet 2002 ; 360 : 1903–13.
CARDIOVASCULAR MORTALITY DOUBLES FOR EVERY INCREMENT IN SBP/DBP OF 20/10 mm Hg

Meta-analysis of 61 prospective, observational studies 1 million adults 12.7 million person-years
BENEFITS OF BP DECREASE
Lewington S, et al. Lancet. 2002;360:1903-1913.

Effect of antihypertensive therapy on all CV events: Comparison of more or less
intensive BP control
Relative risk (95% CIs)1.0 1.25
More intensive BP control better
Less intensive BP
control better
0.5
Stroke
Coronary heart disease
Heart failure
Major CV events
CV death
Total mortality
BPLTTC Lancet 2003

Benefits of Lowering BP
Average Percent ReductionAverage Percent Reduction
Stroke incidence Stroke incidence 35–40% 35–40%
Myocardial infarction Myocardial infarction 20–25% 20–25%
Heart failureHeart failure 50% 50%

SBP-Associated Risks: MRFIT
Adapted from Neaton JD et al. Arch Intern Med. 1992;152:56-64.
SBP versus DBP in Risk of CHD Mortality
Diastolic BP(mm Hg)
Systolic BP(mm Hg)
CHD Death Rate
100+90–99
80–8975–79
70–74<70 <120
120–139
140–159
160+
48.3
20.6
10.311.8
8.88.5
9.2
23.8
16.9
13.912.8
12.611.8
31.0
25.524.6 25.3
25.224.9
37.434.7
43.8
38.1
80.6

Pulse Pressure
• Increase in pulse pressure (PP) indicates greater stiffness in large conduit arteries, primarily the thoracic aorta.
• PP may be a better marker of increased CV risk than either systolic BP or diastolic BP alone in older persons.
PP = SBP – DBPPP = SBP – DBP

2007 ESH/ESC Hypertension Guidelines2007 ESH/ESC Hypertension GuidelinesFirst Choice Drug TreatmentFirst Choice Drug Treatment
DiureticsDiuretics
ACE-inhibitorsACE-inhibitors
Calcium antagonistsCalcium antagonists
Angiotensin receptor antagonistsAngiotensin receptor antagonists
Beta-blockersBeta-blockers

Rationale for Use of ARB’s in Hypertension

Rationale for Use of ARB’s in Hypertension
• Specific blockade of the renin-angiotensin-aldosterone system provides:– More complete blockade of BP response to angiotensin
II (specific for ATII receptor blockade)
– Reduced potential for target organ damage– Reduced potential for bradykinin “cough”
– Best tolerability (specific for ATII receptor blockade)– Some studies suggest a reduced risk of vascular events
compared with other BP lowering regimens
Guidelines recognize the additive positive effect of ARBs in hypertensives with:• Type 2 diabetes• End-organ disease, particularly that affecting the kidney

RR (95% CI)Favors ARB
Favors Other
0.5 1.0 2.0Relative risk
0.79 (0.69,0.90)Stroke
0.96 (0.85,1.09)CHD
Heart failure 0.84 (0.72,0.97)
Major CV events 0.90 (0.83,0.96)
CV death 0.96 (0.85,1.08)
Total mortality 0.94 (0.86,1.02)
Outcome
BP difference(mmHg)
-2/-1
-2/-1
-2/-1
-2/-1
-2/-1
-2/-1
Angiotensin Receptor Antagonists Reduce Risk Angiotensin Receptor Antagonists Reduce Risk of Vascular Events And Total Mortalityof Vascular Events And Total Mortality
BPLTTC Lancet 2003; 362: 1527-35Based on analysis of data from the SCOPE, IDNT, RENAAL and LIFE trials

Diuretics
β-blockers
Ca-antagonists
ACE-Inhibitors
LV
Mas
s r
edu
cti
on
, %
-16
-14
-12
-10
-8
-6
-4
-2
0
- 8%
- 6%
- 11%- 10% ARBs
- 13%
80 randomized controlled trials; 4113 patients
Meta-analysis of Randomized, Controlled Trialsof LV Hypertrophy Regression in Essential Hypertension
Klingbeil AU et al. Am J Med 2003; 115:41-46

ARBs significantly increased probability of maintaining sinus rhythm
0
20
40
60
80
100
Probability of maintaining
sinus rhythm (%)
ARB+ amiodarone
Madrid A et al. Circulation 2002;106:331–6.
p = 0.008 vs. amiodarone
Amiodarone
85%
63%
159 patients with persistent atrial fibrillation were randomized 159 patients with persistent atrial fibrillation were randomized to either amiodarone or amiodarone + ARB to either amiodarone or amiodarone + ARB Results are taken at 2-month follow-up visitResults are taken at 2-month follow-up visit

Mancia G et al. J Hypertens 2007; 25:1105-1187.
Antihypertensive treatment: Preferred drugs as
per new European guidelines Clinical event Clinical event TreatmentTreatmentAtrial f ibri l lationAtrial f ibri l lation •RecurrentRecurrent Angiotensin receptor blockers, ACE Angiotensin receptor blockers, ACE
inhibitorsinhibitors•PermanentPermanent Beta blockers, nonhydropyridine Beta blockers, nonhydropyridine
calcium antagonistscalcium antagonistsESRD/proteinuriaESRD/proteinuria ACE inhibitors, angiotensin receptor ACE inhibitors, angiotensin receptor
blockers, loop diureticsblockers, loop diureticsPADPAD Calcium antagonistsCalcium antagonistsLVH=left ventricular hypertrophyESRD=end-stage renal diseasePAD=peripheral arterial diseaseISH=isolated systolic hypertension

ESH/ESC Guidelines “A blocker of the renin-angiotensin system should be a regular component of combination treatment and the one preferred when monotherapy is sufficient”

Others 2.2%
(-13.9%) ACEi26.9%(-4.0%)
CCB13.9%
(+4.8%)
DIU15.7%
(+3.0%)
ARB 17.7%
(+17.9%)
BB 23.5%
(+9.1%)
Overall Hypertension Market in EgyptARBs are most rapidly growing group
Source: IMS Rx Audit MAT QIII’2007
HT Market Definition: C2, C3, C7, C8, C9

Teveten among other ARBs

Change in mean SBP and DBP from baseline after 8 weeks of treatment with eprosartan (600mg/day) or placebo in patients with mild-to-moderate hypertension
Eprosartan vs Placebo in Mild-to-Moderate HTN
-26
-17.1-12.6 -13.5
-50
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
mmHg SBP
MBPDBPPP

Sega. Blood Press 1999;8:114
Red
uct
ion
in
sit
SB
P (
mm
Hg
)
p=0.025
–29.1
–21.2
–15
–25
–20
–30
0
–5
–10
Red
uct
ion
in
sta
SB
P (
mm
Hg
)
p=0.032
–27.8
–20.0
–15
–25
–20
–30
0
–5
–10
Eprosartan
Enalapril
Eprosartan reduces sitSBP and staSBP in patients with severe hypertension

Argenziano & Trimarco. Curr Med Res Opin 1999;15:9
<65 years (n=201)
≥65 years(n=63)
0
–2
–4
–6
–8
–10
–12
–14
–16
–18
–20
Mea
n c
han
ge
fro
m b
asel
ine
in s
itS
BP
(m
mH
g)
Eprosartan has similar efficacy in young and elderly patients
0
–2
–4
–6
–8
–10
–12
–14
–16
–18
–20
<65 years(n=201)
≥65 years(n=63)
Mea
n c
han
ge
fro
m b
asel
ine
in s
itD
BP
(m
mH
g)

Puig et al. J Hypertens 1999;17:1033
Red
uct
ion
in s
itB
P (
mm
Hg
)
–18
–15
–12
–9
–6
–3
0Diastolic Systolic
–12.4
–9.6
–12.7
–10.9
0
20
40
60
80
Res
po
nse
rat
e (%
)
73
53
100
Eprosartan
Losartan
Eprosartan is more effective than losartan in mild hypertension

PULSE PRESSURE REDUCTION
Robles NR, et al. Int J Clin Pract 2005;59(4):478-484
Reduction in mean pulse pressure, arterial pressure, SBP and DBP in a 16-week open-label study (n=566)

Teveten effect on fibrinolytic/hemostatic variables: Comparative study to losartan
In conclusion, the results indicate that 6-month monotherapy with an angiotensin II type 1 receptor blocker, eprosartan, is associated with a more favorable modification of hemostatic & fibrinolytic status than with losartan
Drugs Exp Clin Res. 2004;30(3):125-32

Effect of Teveten on cytoplasmic free calcium mobilization, platelet activation, and
microparticle formation in hypertension
CONCLUSIONS: Teveten significantly reduces blood pressure and normalizes undesirable changes in platelet function
Am J Hypertens. 2004 Sep;17(9):757-63.


CEREBROVASCULAR RISK EPIDEMIOLOGY
Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease andstroke statistics—2009 update: a report from the American Heart Association Statistics
Committee and Stroke Statistics Subcommittee.Circulation 2009;119:e21–181.
CVD is the 3rd leading cause of death in the U.S. and the first cause of long-term major disability
There are 795,000 incident strokes in the U.S. each year 8–12% of individuals die within the first 30 days of their initial
stroke Patients who survive the initial attack face an increased risk of
subsequent vascular events and stroke (21.5%) The consequences of stroke are socioeconomic Therefore, in light of this disease burden, prevention of initial
and recurrent stroke is a major priority for healthcare providers

STROKE IS MORE FREQUENT THAN AMI
Gentil, A et al. J Neurol Neurosurg Psychiatry 2009;80:1006-1011C
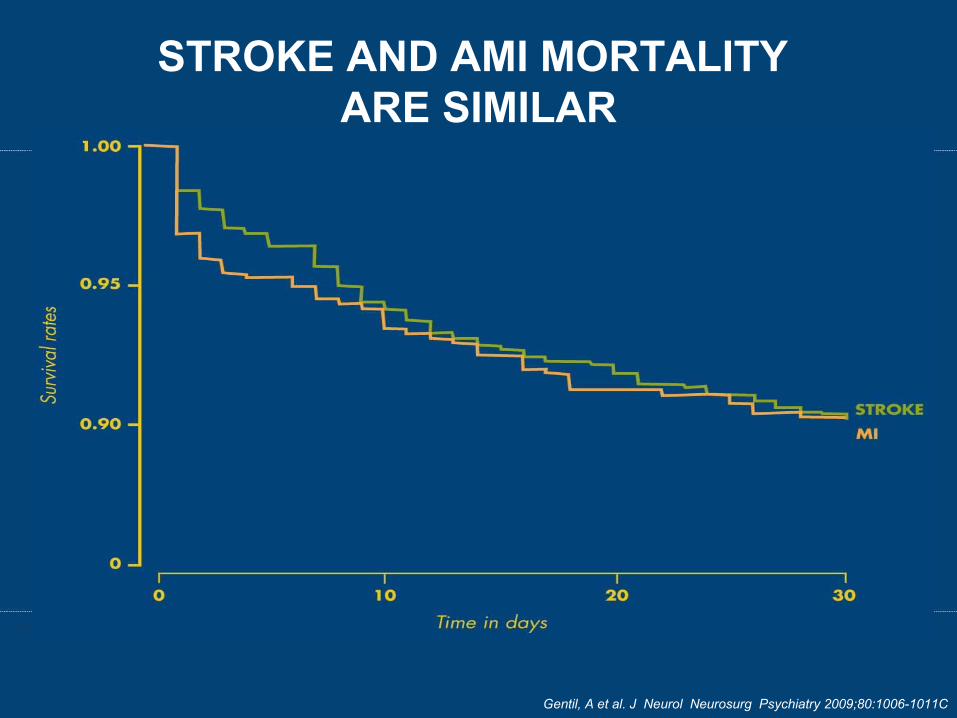
STROKE AND AMI MORTALITY ARE SIMILAR
Copyright ©2009 BMJ Publishing Group Ltd.
Gentil, A et al. J Neurol Neurosurg Psychiatry 2009;80:1006-1011C

RISK FACTORS FOR STROKE

SYSTOLIC BLOOD PRESSURE AND RISK OF STROKE
Lewis et al. Lancet 2002;360:1903–13

CAN WE EXTRAPOLATE DATA FROM PRIMARY PREVENTION
TRIALS TO SECONDARY PREVENTION IN STROKE ?

DECREASING BP DECREASE THE RISK OF STROKE
Law, M R et al. BMJ 2009;338:b1665

ANTIHYPERTENSIVES DO NOT HAVE THE SAME BENEFICIAL EFFECT ON PREVENTING STROKE
Law, M R et al. BMJ 2009;338:b1665

PROGRESS
Lancet 2001; 358:1033

ANTIHYPERTENSIVE THERAPY AFTER STROKEPROFESS TRIAL
N Engl J Med 2008; 359 (12) : 1225-37

POST STROKE TRIAL
ACCESS: candesartan, post acute STROKE, positive but pilot study
SCAST: candesartan, negative.
PROFESS: telmisartan, post stroke negative
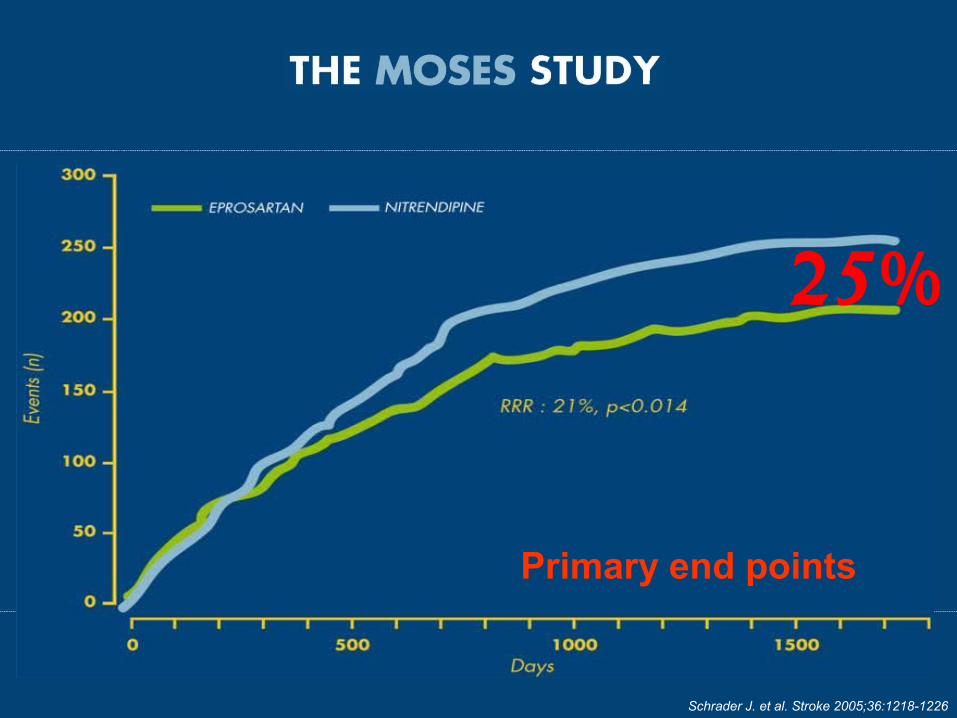
MOSES: eprosartan, post stroke only positive trial with an active comparator, benefits beyond simple BP reduction.
Primary endpoint:
Total mortality plus total number of cardiovascular and cerebrovascular events
Secondary endpoints:
Change in mental capacity and functional status (Barthel Index and Rankin Scale)
Individual elements of the combined primary endpoint
Mean follow-up:
2.5 years

29 in total:14 withdrew consent priorto first intake of study drug
1 without known vital status14 lost for follow-up monitoring
24 in total:10 withdrew consent prior to first intake of study drug2 without known vital status12 lost for follow-up monitoring
1,405 patients eligible for randomization
710 assigned to eprosartan-based
regimen
695 assigned to nitrendipine-based
regimen
681 available for intention-to-treat analyses
671 available for intention-to-treat analyses

Schrader J. et al. Stroke 2005;36:1218-1226
Schrader J. et al. Stroke 2005;36:1218-1226
25%
Primary end points
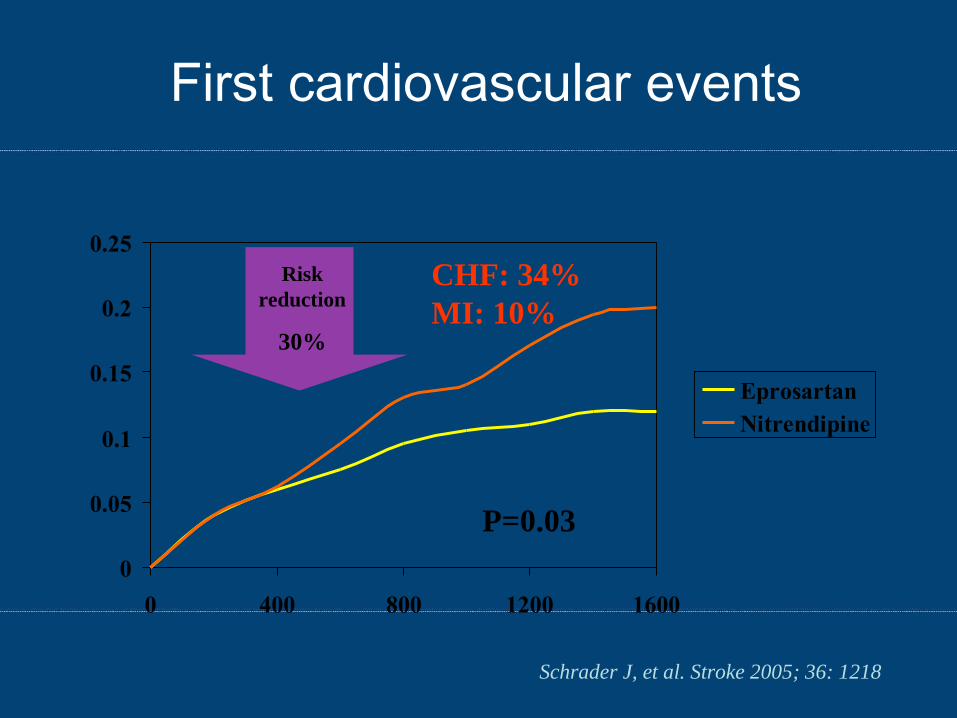
First cardiovascular events
0
0.05
0.1
0.15
0.2
0.25
0 400 800 1200 1600
EprosartanNitrendipine
Risk reduction
30%
P=0.03
Schrader J, et al. Stroke 2005; 36: 1218
CHF: 34%MI: 10%

Is it BP reduction effect ?

Blood pressure Blood pressure
Ris
k of
cor
onar
y he
art d
isea
se
NitrendipineNitrendipine
TevetenTeveten
-25% vs CCB
-31% vs CCB)1st time occurrence(
Risk of Stroke and CHD – MOSES StudyRisk of Stroke and CHD – MOSES StudyBenefits beyond BP LoweringBenefits beyond BP Lowering
Ris
k of
cer
ebro
vasc
ular
eve
nts

Adverse Remodeling of the VasculatureAdverse Remodeling of the Vasculature
Alpha-1vasoconstriction
Ang II
DoxazosinPrazosin
Eprosartan
NE
Eprosartan(ARBs)
Vasoconstriction
VasoconstrictionMedia hypertrophyCollagen deposition
Dual mechanism of action

CONCLUSIONS Cerebrovascular health protection is cardiovascular
prevention Prevention is primary, secondary prevention of stroke but
also dementia and global cardiovascular protection Evidence based approach: Eprosartan
Efficient in BP reduction Specific and dual mode of action Prevention of cardiovascular and cerebrovascular
Health
Prevention of dementia
